testosterone cardiovascular disease and osteoporosis
TRANSCRIPT

J. Endocrinol.lnvest. 28 (Suppl. to no. 10): 73-79, 2005
A.M. Isidori, E. Giannetta, C. Pozza, V. Bonifacio, and A. IsidoriDepartment of Medica! Physiopathology, "La Sapienza" University, Rome, Italy
ABSTRACT. Epidemiological studies correlatedthe age-related decline of serum testosteronelevels to the concomitant increase of cardiovascu-lar diseases, osteoporosis and bone fractures. Forthis reason, testosterone replacement therapy(TRT) in older men with late-onset hypogonadismhas been advocated. Testosterone has an anti-re-sorptive effect that may increase bone density atlumbar spine. Androgens may also have cardio-protective effects by improving endothelial func-tion and reducing the risk factors for atheroscle-rosis. It has been proposed that atherosclerosisand osteoporosis share common pathophysi-ological mechanisms. The role of inflammatorycells, citokynes and calcium deposition into thevascular walls has been reviewed to explore the
causal nexus between these frequently associ-ated diseases. Experimental studies indicate thata deregulation in the commitment of pluripotentmesenchimal stem cells toward specialized phe-notypes might participate in the development ofthese conditions. The crossed-over beneficial ef-fect of bisphosphonate on the cardiovascular sys-tem and statins on bone metabolism supports theresearch for a unitary pharmacological approachto both conditions. The findings that androgensregulate mesenchimal cell differentiation, as wellas body composition, lipid profile and bone me-tabolism, have claimed a role for TRT in aging menwith late onset-hypogonadism.[J. Endocrinol. Invest. 28 (Suppl. to no. 10): 73-79, 2005]@2005, Editrice Kurtis
studies in support of this hypothesis and the use oftestosterone replacement therapy (TRT) in late onsethypogonadism (LOH) are briefly reviewed.
ANDROGENS AND BONEAndrogens act directly on bone cells and indirectly onlocal and systemic production of cytokines and growthfactors (3). In addition, androgens regulate musclemass and body composition which are important de-terminants of bone density (4). Several studies showedthat androgen receptors are expressed in osteoblasts,bone marrow stromal cells, osteocytes, hypertrophicchondrocytes and osteoclasts. Osteoblasts also con-tain the Sa-reductase and aromatase enzymes in orderto metabolize androgens to dihydrotestosterone orestrogens locally (5). It is well known that aromatiza-tion is crucial for the development and maintenanceof male skeleton. However, the presence of androgenreceptors in bone cells suggests that androgens mayalso act independently of estrogens. In vitro, andro-gens regulate proliferation (6), differentiation (7, 8)and mineralization of osteoblastic lineage cells, andmodulate the expression of several cytokines (5). Oneof these is IGF-I, an important autocrine/paracrine me-diator of the anabolic effects of sex steroids (9). Testo-sterone augment GH secretion and IGF-I generation.Androgens increase IGF-I mRNA expression within
INTRODUCTION
The aging process in men is accompanied by a pro-gressive decline in serum testosterone levels (1). Oldage is also associated with a growing prevalence ofcardiovascular disease (CVD) and osteoporosis, bothregarded as leading public health problems affectingmorbidity and mortality of elderly men. Although tradi-tionally viewed as separate entities, accumulating evi-dence indicates that osteoporosis and atherosclerosisshare common pathophysiological mechanisms andepidemiological studies revealed they are frequentlyassociated. The risk factors for CVD, such as immobil-ity, dyslipidemia, oxidative stress, hyperhomocysteine-mia, hypertension and diabetes, were also found topredispose to low bone mineral density (LBMD) (1,2).These conditions and the medications used to treatthem contribute further to lowering testosterone lev-els in elderly men (1).Whether androgen deficiency plays a role in the de-scribed association between CVD and LBMD is still un-der investigation. The recent clinical and exp~imental
Key-woras: Anorogens, testosterone, atllerosclerosls, osteoporosIS, Intla.mation.
Correspondence: A.M. Isidori, Dipartimento di Fisiopatologia Medica,Universita"La Sapienza, ViaJedel Policlinico 1S5, 00161 Roma,ltaly.
E-mail: [email protected]
/3

Testosterone, heart and bone
the osteoblasts promoting their proliferation (10). In
addition, androgens down-regulate osteoclastogen-esis probably by making these cells less vulnerable toother cytokines, such as interleukin-6 (11-13).Androgens not only inhibit osteoclastogenesis, andtherefore bone resorption, but also increase corticalbone formation mainly by stimulating periosteal syn-thesis. Cortical bone seems to contain more androgenreceptors than trabecular bone (13). Higher androgenconcentrations in men may provide a sufficient expla-nation for the thicker cortical bone mass compared towomen (14). Indeed, studies on animals suggest thatandrogens regulate periosteal bone formation dif-ferentially in male and female rats, which may justifythe sexual dimorphism of bone size developing afterpuberty (15). Male mice lacking androgen receptorshave reduced trabecular and cortical bone mass with-out alteration in shape or length. In ovariectomizedrats, the administration of non-aromatizable andro-gens had a beneficial effect in preserving bone mass,suggesting a direct action on bone in females (15-18).Surprisingly, in these studies the predominant effectof androgen treatment was found on bone formation,rather than bone resorption. In summary, experimen-tal studies support the anabolic action of androgenson bone cells that, in vivo, adds up to the known anti-catabolic effect due to its aromatization.In view of the recent interest in TRT, several studies ex-amined the effects of testosterone treatment in oldermen, identifying bone as a possible target organ. Themost encouraging results were found at lumbar spine,which is a typical site of bone loss in men, but only afterprolonged treatment with generous doses of aroma-tizable testosterone preparations (19, 20). A recentmeta-analysis (21) of 29 randomized controlled trials(RCTs) on TRT, evaluating a total of 1083 subjects (625randomized to testosterone), showed an improve-ment at lumbar spine density only, with an estimatedincrease of 3.7% over baseline after a minimum of12-36 months of treatment. However, discrepancieswere found among the various studies largely due tothe heterogeneity in patients' baseline testosteronevalues and the delta of increases in serum T and estra-diol (E2) achieved with the different preparations. Thebeneficial effects on bone density were confirmed bythe results on bone markers: testosterone treatmentsignificantly decreased N-telopeptydes and the deox-ypyridinoline (DPD)/creatinine ratio -the most sensi-tive markers of bone resorption.
increasing interest. The principal sites of androgen ac-tion can be identified as follows.
Effects on the vascular wall
Androgen receptors (AR)s are widely expressed inthe endothelial cells and smooth muscle cells ofarterial vessels, but also in the macrophages andplatelets. These cells are activated or recruited inresponse to vascular damage and, when the repair-ing process is protracted, they participate in the de-velopment of the atherosclerotic plaque. Androgensmay act on these components either directly or indi-rectly through aromatization into estrogens, as thearomatase and 17-(3 OH dehydrogenase enzymesare locally expressed.It is generally accepted that testosterone exerts itsactions through a genomic mechanism. However, ithas been recently demonstrated that sex hormonescan also bind their receptors at cellular membranelevels and modulate ATP-dependent and calciumand potassium voltage-independent channels, witha non-genomic signaling (22). Through differentsignaling pathways or endothelium-dependent and-independent mechanisms, testosterone may inducevasodilatation or vasoconstriction. Studies performedon penile vasculature demonstrated that testosteroneaffects the nitric oxide (NO) cascade at several sites byregulating both NO generation (23) and cGMP deg-radation (24). In general, it has been proposed thattestosterone might be protective against endothe-lial dysfunction and therefore contribute to reducingcoronary events caused by vasospasm, plaque ruptureand thrombosis (25).Endothelial dysfunction is thought tQ be responsiblefor the decreased vasodilatation and enhanced vaso-constriction underlying angina pectoris (26). In a vari-ety of small uncontrolled studies, therapeutic dosesof testosterone reduced the severity and frequency ofangina improving ECG signs of myocardial ischemia.The beneficial effect of acute and chronic testosteroneadministration with physiological or supra-physiologi-cal doses was observed in older men with decreasedbaseline levels of testosterone. Short-term intracoro-nary administration of testosterone, at physiologicalconcentrations, induces coronary artery dilatation andincreases coronary blood flow in men with establishedcoronary artery disease (22).Several studies directly analyzed the effects ofTRT onCVD and indirectly those on cardiovascular risks. Datapublished on endothelial response to testosterone ad-ministration showed that physiological dose of testo-sterone cypionate in men with positive-exercise ECGreduced ST-segment depression by 32% (at 4 weeks)and 51% (at 8 weeks) compared to placebo (27). Thiseffect was confirmed by Webb et al. (28) that demon-
ANDROGENS ANDTHE CARDIOVASCULAR SYSTEM
The effects of androgens on the cardiovascular systemand the development of atherosclerosis are gaining
/4
A.M. Isidori, E. Giannetta, C. Palla, et al.
lytic effects may be opposed to the pro-aggregatoryeffects exerted on platelets, since high doses of andro-gens were found to decrease cyclooxygenase activityand increase aggregability (22).Numerous observations suggest that serum tes-tosterone is inversely related to body mass index(8M I), waist circumference, waist-to-hip ratio (WHR),visceral fat, free fatty acids and serum leptin andinsulin levels (38, 39). Therefore in men, a low se-rum testosterone is a component of the metabolicsyndrome, the clinical entity characterized byobes-ity, glucose intolerance of Type 2 diabetes mellitus,arterial hypertension, hypertriglyceridemia, hype-ruricemia, low HDL-C and a pro-coagulatory andantifibrinolytic status.During the aging process, lipid accumulation canbe observed in several tissues and an increase andredistribution of fat occurs from subcutaneous tovisceral deposits (40-42). As an increase in intra-ab-dominal fat is associated with greater mortality forcardiovascular events (39), it could be argued thattestosterone treatment, by reducing fat mass, im-proves cardiovascular risk. In a recent meta-analysisfrom our group, it was estimated that testosteronedependent fat mass reduction accounted for a6.2% loss of initial body fat content, and an increaseof 2.7% in initial fat free mass (21). Therefore, thechanges induced by testosterone administrationon body composition may exert an additional ben-eficial effect on bone density and quality. However,data about the effects of testosterone on serum lipidprofile are controversial. When they were pooledin the meta-analysis, a significant decrease in totalcholesterol was revealed that, however, should beweighted against a reduction in HDL-C detectable infew studies performed using high doses or non-aro-matizable testosterone preparations (21). It seemsthat aromatization of exogenous testosterone has itsrole in maintaining HDL concentration in men, coun-teracting the effects of testosterone on lipoproteinlipase (LPL) activity (43).
strated a significant increase in coronary and brachialvessel diameter and blood flow after testosterone infu-sion at supraphysiological doses (8 ~mol/l) over 3 mininto the coronary arteries.The association between testosterone and atherogen-esis is strengthened further by the effect of testoster-one on the immune system. Activated macrophagesproduced several cytokines, such as interleukin (IL)-1,-10, tumor necrosis factor (TN F)-a and platelet-derivedgrow-factor-1. These molecules promote the recruit-ment of other inflammatory cells into the vascularwall,the proliferation and migration of smooth-muscle cellsand alterations of endothelial function (26, 29). Theeffect of testosterone on cytokine productions hasnot been studied in foam cells, although testosteroneexerts potentially anti-inflammatory effects by modu-lating IL-1 0/IL-6 synthesis and inhibiting TNF-a andreactive oxygene species (ROS) release from macro-phages (29,30).Finally, arterial smooth muscle cell proliferation, mi-gration and extracellular matrix production all affectendothelium-independent vasoreactivity. Rat arterialsmooth muscle cells were found to express the ARs(26). The effects of testosterone on these processesare currently under investigation.As already shown for bone metabolism, androgensmay also affect cardiovascular system indirectly bymodulating the products of other neuroendocrineaxis which are dependent on sex hormones levels.Regarding this, the importance of the GH-IGF-I axison maintenance of healthy cardiovascular functionin men's adult life has recently been highlighted. Re-duced circulating androgen and IGF-llevels are oftenassociated and both correlate with a higher cardiovas-cular and cerebrovascular risk (31). The role oflGF-1 onCV system became evident from studies on adult GHdeficiency, where an increase in vascular intima-mediathickness and a higher occurrence of atheromatouseplaques were shown (32).
Effects on cardiovascular risk factors
Testosterone inhibits tryglicerid uptake and lipopro-teine lipase activity in abdominal but not in femoralsubcutaneous fat (33), suggesting that it may contrib-ute to sexual dimorphism in fat distribution betweencentral and peripheral sites. In men, serum testoster-one is positively correlated to serum levels of HDL-Cand inversely to triglycerides, total cholesterol, LDL-C,fibrinogen and plasminogen activator inhibitor 1 (PAI-1) (22, 34-36). In agreement with the lowering effects oftestosterone on PAI-1 concentrations, in vitro studiesshowed that testosterone inhibits PAI-1 secretion frombovine aortic endothelial cells. Current data indicatethat testosterone reduces fibrinogen and PAI-1 levels(37). However, these anti-coagulatory and pro-fibrino-
AGING AND THE ADIPOGENETIC PROJECT
Aging in men is associated with an increase in vis-ceral fat mass and a redistribution of fat cells towardheterotopic sites such as muscles and bones. In vitrostudies showed that myoblasts isolated from mouseskeletal muscle exhibited an increased adipogenicpotential as a function of age. It has been hypoth-esized that this is due to a change in differentiationpotential toward an adipogenic default program.It seems that with aging there is abundance of themRNA encoding a transcription factor (clEBPa) andrelative abundance of peroxisome proliferator-acti-
75

Testosterone, heart and bone
Mesenchymal stem cell
Osteoblasts Pre-adipocytes Myoblasts Condroblasts
Fig. 1 -Deregulation of mesenchymal stemcell differentiation with aging and the effectsof androgen deficiency on this process.
vated receptor (PPAR)y-2 to PPARy-1 mRNAs. Fur-thermore, adipogenic gene expression in myoblastsfrom aged animals was activated, presumably inresponse to PPARy and dEBra, without an effectiverepression of myogenic gene expression (44). Thesame process occurs in bones. In fact, an inverserelationship between adipogenic and osteoblasticprecursors has been demonstrated in bone marrowmesenchymal stromal cells, and in vivo studies dem-onstrated decreased osteoblastogenesis accom-panied with increased adipogenesis in aging bone(45). Altogether these results suggest a switch in thedifferentiation program of multipotent mesenchymalprogenitors during aging. It provides a potential ex-planation for the association between a decreasedbone formation and an increased adiposity of bonemarrow seen with advancing age (46, 47). Numer-ous experimental systems have demonstrated thepotential of stem cells to give rise to a variety ofdifferentiated cell types (48-50). It is supposed thata default program may be activated in mesenchy-mal cells with increasing age by a variety of agentsincluding growth factors, substrate, density and pas-sage number, resulting in a more adipogenic-likephenotype (44). In this view, the balance that existsbetween differentiation programs into the myob-lasts, osteoblasts, condrocytes, and osteoclasts line-ages with age appears to be shifted predominantlytoward adipogenesis (Fig. 1). Since androgens, butalso GH, have been recently demonstrated to beable to redirect the differentiation of mesenchymalcells, and both hormones are reduced with aging, weproposed that they are involved in the age-relatedchanges in body composition and its consequences(including the increased cardiovascular risk).
OSTEOPOROSIS AND CVD: THE LINKS
In a recent analysis, from the Rotterdam study,LBMD was found to be associated with increasedrisk of peripheral arterial disease (51). Atheroscle-rosis and osteoporosis are traditionally viewed asseparate entities, however these conditions sharetwo important pathophysiological processes thatmay be linked with advancing age: inflammationand calcification. The evidence supporting thishypothesis is briefly reviewed (Fig. 2). The arterywall and the osteon of cortical bone both have acommon endothelium-lined lumen (52, 53). Also,resident and rec;:ruited macrophages, monocytes,and lymphocytes play key roles in the atheroscle-rotic plaque calcification and osteoporosis (53,54). Monocytes may differentiate into osteoclastsin bone, and macrophages or foam cells withinarteries. Interestingly, Parhami et al. (55) showedthat in animals, the same oxidised lipids that induceosteoblast differentiation in calcifying vascular cellsinhibit osteoblast differentiation in bone. Therefore,oxidiseq lipid accumulation in the sub-endothelialspace of bone will inhibit bone mineral formation.This has been confirmed, using advanced tech-nologies, by the association found between BMDand coronary calcium (54, 55). The dysfunctionalendothelium is impaired in its abilities to serveas a barrier against atherogenic lipoproteins, toregulate vascular tone via NO and other vasoac-tive molecules and to control thrombosis. Recently,it has been proposed that NO has a role in bonemetabolism, and the constitutive expression of NOsynthetase endothelial isoform (eNOS) and induc-ible isoform (iNOS) in cells of osteoblast/osteocytelineage was demonstrated (56-58). Investigations in
76
A.M. Isidori, E. Giannetta, C. Pozza, et al.
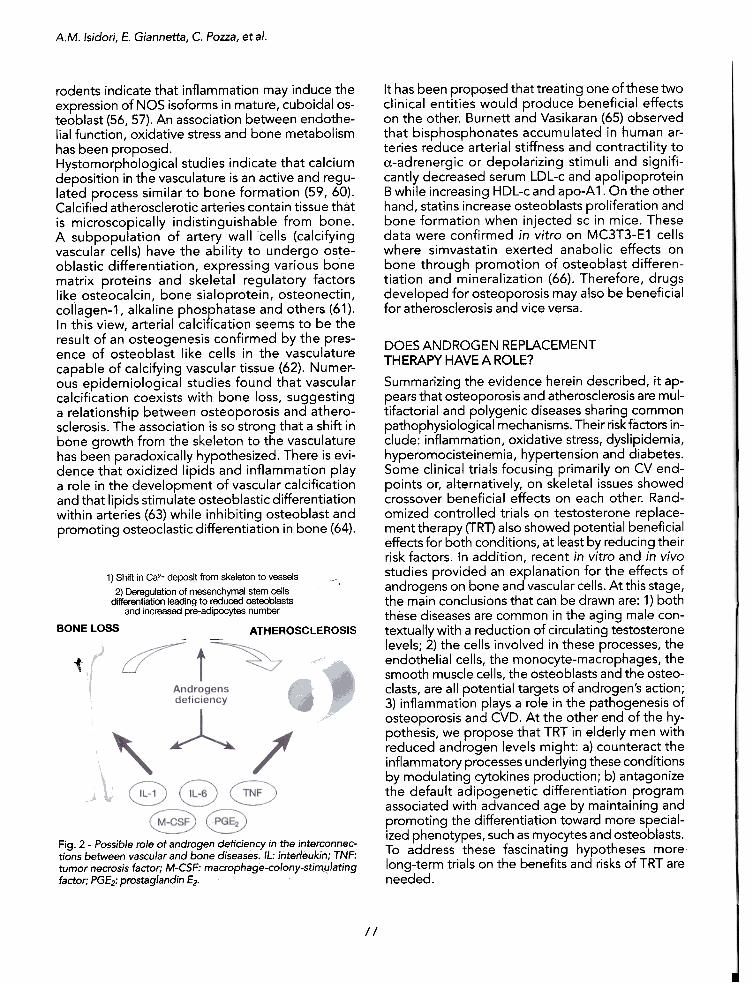
It has been proposed that treating one of these twoclinical entities would produce beneficial effectson the other. Burnett and Vasikaran (65) observedthat bisphosphonates accumulated in human ar-teries reduce arterial stiffness and contractility toa-adrenergic or depolarizing stimuli and signifi-cantly decreased serum LDL-c and apolipoproteinB while increasing HDL-c and apo-A 1. On the otherhand, statins increase osteoblasts proliferation andbone formation when injected sc in mice. Thesedata were confirmed in vitro on MC3T3-E1 cellswhere simvastatin exerted anabolic effects onbone through promotion of osteoblast differen-tiation and mineralization (66). Therefore, drugsdeveloped for osteoporosis may also be beneficialfor atherosclerosis and vice versa.
rodents indicate that inflammation may induce theexpression of NOS isoforms in mature, cuboidal os-teoblast (56, 57). An association between endothe-lial function, oxidative stress and bone metabolismhas been proposed.Hystomorphological studies indicate that calciumdeposition in the vasculature is an active and regu-lated process similar to bone formation (59, 60).Calcified atherosclerotic arteries contain tissue thatis microscopically indistinguishable from bone.A subpopulation of artery wall cells (calcifyingvascular cells) have the ability to undergo oste-oblastic differentiation, expressing various bonematrix proteins and skeletal regulatory factorslike osteocalcin, bone sialoprotein, osteonectin,collagen-1, alkaline phosphatase and others (61).In this view, arterial calcification seems to be theresult of an osteogenesis confirmed by the pres-ence of osteoblast like cells in the vasculaturecapable of calcifying vascular tissue (62). Numer-ous epidemiological studies found that vascularcalcification coexists with bone loss, suggestinga relationship between osteoporosis and athero-sclerosis. The association is so strong that a shift inbone growth from the skeleton to the vasculaturehas been paradoxically hypothesized. There is evi-dence that oxidized lipids and inflammation playa role in the development of vascular calcificationand that lipids stimulate osteoblastic differentiationwithin arteries (63) while inhibiting osteoblast andpromoting osteoclastic differentiation in bone (64).
DOES ANDROGEN REPLACEMENTTHERAPY HAVE A ROLE?
Summarizing the evidence herein described, it ap-pears that osteoporosis and atherosclerosis are mul-tifactorial and polygenic diseases sharing commonpathophysiological mechanisms. Their risk factors in-clude: inflammation, oxidative stress, dyslipidemia,hyperomocisteinemia, hypertension and diabetes.Some clinical trials focusing primarily on CV end-points or, alternatively, on skeletal issues showedcrossover beneficial effects on each other. Rand-omized controlled trials on testosterone replace-ment therapy (TRT) also showed potential beneficialeffects for both conditions, at least by reducing theirrisk factors. In addition, recent in vitro and in vivostudies provided an explanation for the effects ofandrogens on bone and vascular cells. At this stage,the main conclusions that can be drawn are: 1) boththese diseases are common in the aging male con-textually with a reduction of circulating testosteronelevels; 2) the cells involved in these processes, theendothelial cells, the monocyte-macrophages, thesmooth muscle cells, the osteoblasts and the osteo-clasts, are all potential targets of androgen's action;3) inflammation plays a role in the pathogenesis ofosteoporosis and CVD. At the other end of the hy-pothesis, we propose that TRT in elderly men withreduced androgen levels might: a) counteract theinflammatory processes underlying these conditionsby modulating cytokines production; b) antagonizethe default adipogenetic differentiation programassociated with advanced age by maintaining andpromoting the differentiation toward more special-ized phenotypes, such as myocytes and osteoblasts.To address these fascinating hypotheses morelong-term trials on the benefits and risks of TRT areneeded.
1) Shift in Ca2+ deposit from skeleton to vessels ~\
2) Deregulation of mesenchymal stem cellsdifferentiation leading to reduced osteobiasts
and increased pre-adipoc~es number
BONE LOSS ATHEROSCLEROSIS
i
Fig. 2 -Possible role of androgen deficiency in the interconnec-tions between vascular and bone diseases. IL: inter/eukin; TNF:tumor necrosis factor; M-CSF: macrophage-colony-stirTty/ating
factor; PGf2: prostaglandin f2.
II
Testosterone, heart and bone
17. Coxam V, Bowman BM, Mecham M, Roth CM, Miller MA,
Miller SC. Effects of dihydrotestosterone alone and combinedwith estrogen on bone mineral density, bone growth, and for-mation rates in ovariectomized rats. Bone 1996, 19: 107-14.
18. Tobias JH, Gallagher A, Chambers T J. 5 alpha-Dihydrotesto-sterone partially restores cancellous bone volume in osteo-penicovariectomized rats. Am J Physiol1994, 267: E853-9.
19. Amory JK, Watts NB, Easley KA, et al. Exogenoustestoster-one or testosterone with finasteride increases bone mineraldensity in older men with low serum testosterone. J ClinEndocrinol Metab 2004, 89: 503-10.
20. Snyder PJ, Peachey H, Hannoush P, etal. Effectoftestoster-one treatment on bone mineral density in men over 65 yearsof age. J Clin Endocrinol Metab 1999, 84: 1966-72.
21. Isidori AM, Giannetta E, Greco EA, et al. Effects of testo-sterone on body composition, bone metabolism and serumlipid profile in middle-aged men: a meta-analysis. Clin En-docrinol (Oxf) 2005, 63: 280-93.
22. Wu FC, von Eckardstein A. Androgens and coronary arterydisease. Endocr Rev 2003,24: 183-217.
23. Mills TM, Reilly CM, Lewis RW. Androgens and penile erec-tion: a review. J Andro11996, 17: 633-8.
24. Morelli A, Filippi S, Mancina R, et al. Androgens regulatephosphodiesterase type 5 expression and functional activityin corpora cavernosa. Endocrinology 2004,145: 2253-63.
25. Eckardstein A, Wu FC. Testosterone and atherosclerosis.Growth Horm IGF Res 2003, 13 (SuppIA): S72-84.
26. Ross R. Atherosclerosis is an inflammatory disease. AmHeartJ 1999, 138: S419-20.
27. Jaffe MD. Effect of testosterone cypionate on postexerciseST segment depression. Br Heart J 1977, 39: 1217-22.
28. Webb CM, Adamson DL, de Zeigler D, Collins P. Effectof acute testosterone on myocardial ischemia in menwith coronary artery disease. Am J Cardiol1999, 83:
437-9,A9.29. Zhu XD, Bonet B, Knopp RH. 17beta-estradiol, proges-
terone, and testosterone inversely modulate low-densitylipoprotein oxidation and cytotoxicity in cultured placentaltrophoblast and macrophages. Am J Obstet Gynecol1997 ,177: 196-209.
30. D'Agostino P, Milano S, Barbera C, et al. Sex hormonesmodulate inflammatory mediators produced by macro-phages. Ann NY Acad Sci 1999,876: 426-9.
31. Svensson J, Tivesten A, Isgaard J. Growth hormone and thecardiovascular function. Minerva EndocrinoI2005, 30: 1-13.
32. Colao A, Di Somma C, Vitale G, Filippella M, Lombardi G.Influence of growth hormone on cardiovascular health anddisease. Treat Endocrinol2003, 2: 347-56.
33. Tan KC, Shiu SW, Kung AW. Alterations in hepatic lipaseand lipoprotein subfractions with transdermal testosteronereplacement therapy. Clin Endocrinol (Oxf) 1999, 51 : 765-9.
34. Hergenc G, Schulte H, Assmann G, von Eckardstein A. Asso-ciations of obesity markers, insulin, and sex hormones withHDL-cholesterollevels in Turkish and German individuals.Atherosclerosis 1999,145: 147-56.
REFERENCES
1. Isidori AM, Lenzi A. Risk factors for androgen decline in
older males: lifestyle, chronic disease and drugs. J Endocri-
nollnvest 2005, 28 (3 Suppl): 14-22.
2. McFarlane SI, Muniyappa R, Shin JJ, BahtiyarG, Sowers JR.
Osteoporosis and cardiovascular disease: brittle bones andboned arteries, is there a link? Endocrine 2004, 23: 1-10.
3. Hofbauer LC, Khosla S. Androgen effects on bone metabo-lism: recent progress and controversies. Eur J Endocrinol
1999,140: 271-86.
4. Fabbrini E, Mencacci C, Caprio M, et al. Body composi-
tion and bone mineral density in postmenopausal women:evidence for a major effect of lean mass. Proc 83th Meetingof the Endocrine Society, ENDO 2001 2001; Denver, CO:OR45-2.
5. Kearns AE, Khosla S. Potential anabolic effects of androgens
on bone. Mayo Clin Proc 2004,79 (4 Suppl): S14-18.
6. Kasperk CH, Wergedal JE, Farley JR, et al. Androgensdirectly stimulate proliferation of bone cells in vitro. Endo-
crinology 1989,124: 1576-8.
7. Kasperk C, Fitzsimmons R, Strong D, et al. Studies of the
mechanism by which androgens enhance mitogenesis anddifferentiation in bone cells. J Clin Endocrinol Metab 1990,71:1322-9.
8. Benz DJ, Haussler MR, Thomas MA, Speelman B, KommBS. High-affinity androgen binding and androgenic regula-tion of alpha 1 (I)-procollagen and transforming growth fac-tor-beta steady state messenger ribonucleic acid levels inhuman osteoblast-like osteosarcoma cells. Endocrinology
1991,128:2723-30.
9. Riggs BL, Khosla S, Melton U, III. Sex steroids and the con-struction and conservation of the adult skeleton. Endocr Rev
2002, 23: 279-302.
10. Gori F, Hofbauer LC, Conover CA, Khosla S. Effects ofandrogens on the insulin-like growth factor system in anandrogen-responsive human osteoblastic cell line. Endo-crinology 1999, 140: 5579-86.
11. Bellido T, Jilka RL, Boyce BF, etal. Regulation ofinterteukin-6,
osteoclastogenesis, and bone mass by androgens. The roleof the androgen receptor. J Clin Invest 1995, 95: 2886-95.
12. Lin SC, Yamate T, Taguchi Y, et al. Regulation of the gp80and gp130 subunits of the IL-6 receptor by sex steroids inthe murine bone marrow. J Clin Invest 1997, 100: 1980-90.
13. Kasperk C, Helmboldt A, Borcsok I, et al. Skeletal site-de-pendent expression of the androgen receptor in humanosteoblastic cell populations. CalcifTissue Int 1997, 61:464-73.
14. Eriksen EF, Colvard DS, Berg NJ, et al. Evidence of estrogenreceptors in normal human osteoblast-like cells. Science
1988,241: 84-6.
15. Turner RT, Wakley GK, Hannon KS. Differential effects of an-drogens on cortical bone histomorphometry in gonadect-omized male and female rats. J Orthop Res 1990, 8: 612-7.
16. Mason RA, Morris HA. Effects of dihydrotestosterone onbone biochemical markers in sham and oophorectomizedrats.J Bone Miner Res 1997,12: 1431-7.
78

A.M.
Isidori, E. Giannetta, C. Pozza, et al.
35. Tchernof A, Labrie F, Belanger A, Despres JP. Obesity andmetabolic complications: contribution of dehydroepian-drosterone and other steroid hormones.J Endocrinol1996,(Suppl): 5155-64.
36. Tsai EC, Boyko EJ, Leonetti DL, Fujimoto WY. Low serumtestosterone level as a predictor of increased visceral fat inJapanese-American men. Int JObes Relat Metab Disord2000, 24: 485-91.
37. Sowers MR, Jannausch M, Randolph JF, et al. Androgensare associated with hemostatic and inflammatory factorsamong women at the mid-life. J Clin Endocrino! Metab2005,90: 6064-71.
38. Blouin K, Despres JP, Couillard C,et al. Contribution of ageand declining androgen levels to features of the metabolicsyndrome in men. Metabolism 2005, 54: 1034-40.
39. Bjorntorp P. "Portal" adipose tissue as a generatorbf riskfactors for cardiovascular disease and diabetes. Arterioscle-rosis 1990,10: 493-6.
40. Baumgartner RN, HeymsfieldSB, Roche AF. Human bodycomposition and the epidemiology of chronic disease.Obes Res 1995, 3: 73-95.
41. Horber FF, Gruber B, Thomi F, Jensen EX, Jaeger P. Effectof sex and age on bone mass, body composition and fuelmetabolism in humans. Nutrition 1997, 13: 524-34.
42. Zamboni M, Armel!ini F, Harris T, et at. Effects of age on bodyfat distribution and cardiovascular risk factors in women. AmJ Clin Nutr 1997, 66: 111-5.
43. Zmuda JM, Fahrenbach MC, Younkin BT, et al. The effect oftestosterone aromatization on high-density lip?protein cho-lesterollevel and postheparin lip?lytic activity. Metabolism1993, 42: 446-50.
44. Taylor-Jones JM, McGehee RE, Rando TA, Lecka-Czernik B,Lipschitz DA, Peterson CA. Activation of an adipogenic pro-gram in adult myoblasts with age. Mech Ageing Dev 2002,
123:649-61.
45. Jilka RL, Weinstein RS, Takahashi K, Parfitt AM, ManolagasSC. Linkage of decreased bone mass with impaired osteob-lastogenesisina murine model of accelerated senescence.J Clin Invest 1996, 97: 1732-40. .
46. Moore SG, Dawson KL. Red and yellow marrow in the femur:age-related changes in appearance at MR imaging. Radiol-ogy 1990,175: 219-23.
47. Bianco P, Riminucci M, Gronthos 5, Robey PG. Bone marrowstromal stem cells: nature, biology, and potential applica-tions. Stem Cells 2001, 19: 180-92.
48. Gussoni E, Soneoka Y, Strickland CD, et al. Dystrophin ex-pression in the mdx mouse restored by stem cell transplan-tation. Nature 1999, 401: 390-4.
49. Jackson KA, Mi T, Goodell MA. Hematopoietic potential ofstem cells isolated from murine skeletal muscle. Proc NatlAcad Sci USA 1999, 96: 14482-6.
50. Lee JY, au-Petersen Z, Cao B, et al. Clonal isolation of mus-cle-derived cells capable of enhancing muscle regenerationand bone healing. J Cell Bioi 2000, 150: 1085-100.
51. van der KM, Pols HA, HakAE, Witteman JC, Hofman A, deLaet CEo Bone mineral density and the risk of peripheralarterial disease: the Rotterdam Study. CalcifTissue Int 2002,70: 443-9.
52. Whitney C, Warburton DE, Frohlich J, Chan SY, McKay H,Khan K. Are cardiovascular disease and osteoporosis di-rectly linked? Sports Med 2004, 34: 779-807.
53. Dhore CR, Cleutjens JP, Lutgens E, et al. Differential expres-sion of bone matrix regulatory proteins in human athero-sclerotic plaques. Arterioscler Thromb Vasc Bioi 2001, 21 :1998-2003.
54. McFarlane 51, Muniyappa R, Shin JJ, Bahtiyar G, Sowers JR.Osteoporosis and cardiovascular disease: brittle bones andboned arteries, is there a link? Endocrine 2004, 23: 1-10.
55. Parhami F, Jackson SM, Tintut Y, et al. Atherogenic diet andminimally oxidized low density lipoprotein inhibit osteo-genic and promote adipogenic differentiation of marrowstromal cells. J Bone Miner Res 1999, 14: 2067-78.
56. Helfrich MH, Evans DE, Grabowski PS, PollockJS, OhshimaH, Ralston SH. Expression of nitric oxide synthase isoformsin bone and bone cell cultures. J Bone Miner Res 1997, 12:
1108-1;'.
57. Fox SW, Chow JW. Nitric oxide synthase expression in bonecells. Bone 1998, 23: 1-6.
58. Klein-Nulend J, Hejfrich MH, Sterck JG, et al. Nitric oxideresponse to shear stress by human bone cell cu.ltures isendothelial nitric oxide synthase dependent. Biochem Bio-phys ResCommun 1998,250: 108-14.
59. Doherty TM, Asotra K, Fitzpatrick LA, et al. Calcification inatherosclerosis: bone biology and chronic inflammation atthe arterial crossroads. Proc NatlAcad Sci USA 2003, 100:11201-6.
60. Abedin M, Tintut Y, Demer LL. Vascular calcification: mecha-nisms and clinica1 ramifications. Arterioscler Thromb VascBioi 2004, 24: 1161-70.
61. Rubin MR, Silverberg SJ. Vascular calcification and oste-oporosis--the nature of the nexus. J Clin Endocrinol Metab2004, 89: 4243-5.
62. Watson KE, Bostrom K, Ravindranath R, Lam T,NortonB,Demer LL. TGF-beta 1 and 25-hydroxycholesterol stimulateosteoblast-like vascular cells to calcify. J Clin Invest 1994,93:2106-13.
63. Pohle K, Maffert R, Ropers D, eta1. Progression of aortic valvecalcification: association with coronary atherosclerosis andcardiovascular risk factors. Circulation 2001, 104: 1927-32.
64. Tintut Y, Morony 5, Demer LL. Hyperlipidemia promotesosteoclastic potential of bone marrow cells ex vivo. Arterio-scler Thromb VascBioI2004, 24: e6-10.
L~ Burnett JR, Vasikaran SD. Cardiovascular disease and oste-
oporosis: is there a link between lipids and bone? Ann ClinBiochem 2002, 39: 203-10.
66. Maeda T, Matsunuma A, Kawane T, Horiuchi N. Simvastatin pro-motes osteoblast differentiation and mineralization in MC3T3-E1 cells. Biochem Biophys Res Commun 2001,280: 874-7.
U-J
/'1