bulletin - who | world health organization
TRANSCRIPT

Bulletinof the World Health Organization
Incorporating World Health Forumand World Health Statistics Quarterly
The International Journal
of Public Health
lll
if
hld
lhi
i
V O L U M E 7 7 , N U M B E R 1 , 1 9 9 9 , 1 – 1 0 0
EditorialsMaking a difference 1
Gro Harlem Brundtland
A new role for the Bulletin 2Richard G.A. Feachem
ResearchMumps and mumps vaccine: a global review 3
A.M. Galazka, S.E. Robertson, & A. Kraigher
Diagnosing anaemia using the Haemoglobin 15Colour Scale
N.R. van den Broek et al.
Unrecognized sexually transmitted infections 22in rural South African women
D. Wilkinson et al
Use of an autodestruct syringe compared 29with a disposable syringe
C.M. Nelson, A. Sutanto, & I.G.P. Suradana
In vivo and in vitro tests of chloroquine 34resistance
P. Ringwald & L.K. Basco
Policy and PracticeTowards evidence-based health care reform 44
M. Vienonen, D. Jankauskiene & A. Vask
Prizes for weight loss 50L. Englberger
Round TableAnimal-to-human organ transplants 54
A.S. Daar
Discussion 62J.S. Allan; A.P.R. Aluwihare; F.H. Bach;A.Caplan; L.Chapman; B.M. Dickens;J.A. Fishman; C.G. Groth & M.E. Breimer;A.Menache; P J. Morris; E. Van Rongen
Public Health ClassicsMeasuring the health hazards of tobacco: 82Commentary
A.D. Lopez
Smoking and carcinoma of the lung 84R. Doll & A. Bradford Hill
News 94
Books & Electronic Media 96
Readers’ Forum 97

Bulletin of the World Health Organization, 1999, 77 (1) i
Bulletinof the World Health Organization
Incorporating World Health Forumand World Health Statistics Quarterly
The International Journal
of Public Health
V O L U M E 7 7 , N U M B E R 1 , 1 9 9 9 , 1 – 1 0 0
World Health OrganizationGeneva

ii Bulletin of the World Health Organization, 1999, 77 (1)
The World Health Organization welcomes requests for permission to reproduce or translate itspublications, in part or in full. Applications and enquiries should be addressed to the Office ofPublications, World Health Organization, Geneva, Switzerland, which will be glad to provide thelatest information on any changes made to the text, plans for new editions, and reprints andtranslations already available.
© World Health Organization 1999
Publications of the World Health Organization enjoy copyright protection in accordance with theprovisions of Protocol 2 of the Universal Copyright Convention. All rights reserved.
The designations employed and the presentation of the material in this publication do not implythe expression of any opinion whatsoever on the part of the Secretariat of the World HealthOrganization concerning the legal status of any country, territory, city, or area or of its authorities,or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps representapproximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that theyare endorsed or recommended by the World Health Organization in preference to others of asimilar nature that are not mentioned. Errors and omissions excepted, the names of proprietaryproducts are distinguished by initial capital letters.
Authors alone are responsible for views expressed in signed articles.
ISSN 0043-9686Printed in Switzerland.
Bulletin of the World Health Organization, 1999, 77 (1) iii
Contents
EditorialsMaking a difference 1
Gro Harlem Brundtland
A new role for the Bulletin 2Richard G.A. Feachem
ResearchMumps and mumps vaccine: a global review 3
A.M. Galazka, S.E. Robertson, & A. Kraigher
Diagnosing anaemia in pregnancy in rural clinics: assessing the potential of 15the Haemoglobin Colour Scale
N.R. van den Broek, C. Ntonya, E. Mhango, & S.A. White
Unrecognized sexually transmitted infections in rural South African women: 22a hidden epidemic
D. Wilkinson, S.S. Abdool Karim, A. Harrison, M. Lurie, M. Colvin,C. Connolly, & A.W. Sturm
Use of SoloShot autodestruct syringes compared with disposable syringes, 29in a national immunization campaign in Indonesia
C.M. Nelson, A. Sutanto, & I.G.P. Suradana
Comparison of in vivo and in vitro tests of resistance in patients treated 34with chloroquine in Yaoundé, Cameroon
P. Ringwald & L.K. Basco
Policy and PracticeTowards evidence-based health care reform 44
Mikko Vienonen, Danguole Jankauskiene, & Arvi Vask
The Ljubljana Charter on Reforming Health Care 48
Prizes for weight loss 50Lois Englberger
Round TableAnimal-to-human organ transplants – a solution or a new problem? 54
A.S. Daar
Discussion 62Jonathan S. Allan; A.P.R. Aluwihare; Fritz H. Bach; Arthur Caplan;Louisa Chapman; Bernard M. Dickens; Jay A. Fishman; C.G. Groth &M.E. Breimer; André Menache; Peter J. Morris; Eric van Rongen
Public Health ClassicsMeasuring the health hazards of tobacco: Commentary 82
A.D. Lopez
Smoking and carcinoma of the lung 84Richard Doll & A. Bradford Hill
News 94
Books & Electronic Media 96
Readers’ Forum 97
Directions to Contributors 98


Bulletin of the World Health Organization, 1999, 77 (1) 1
Editorials
© World Health Organization 1999
Making a differenceGro Harlem Brundtland1
1 Director-General, World Health Organization,Geneva, Switzerland.
A new era is beginning. The imminentnew millennium reflects only one wayof recording history, but it does serveto heighten our awareness of transi-tion. This is a time that brings with itunprecedented risks and opportunitiesfor human health. As a result of globalinterdependence, epidemics canbecome pandemics more rapidly thanever before, but protection against anincreasing number of diseases can bemore inclusive than ever before. Withtechnological development comes thepower to destroy, but with it alsocomes the power to solve problemsthought until now to be insoluble.With economic turmoil come hard-ship and insecurity for the healthsector in many parts of the world, butwith it also comes intense pressure onpolicy-makers to find better ways toprotect people’s health.
Whatever our expectations maybe, the future depends to a largeextent on the choices we make today.The task of the World Health Organi-zation is to help find ways of con-structing that future to avert thethreats and use the opportunities itholds for health. To do so moreeffectively, WHO itself is goingthrough an intense period of change.We are redefining our work as theglobal agency for public health, andreorganizing our activities to get itdone.
This work has four dimensions:building healthy communities,combating ill-health, sustaininghealth, and reaching out to partners indevelopment. These are the themesaround which we have arranged theactivities of WHO headquarters,placing them in nine clusters ofrelated programmes. My guidingconviction in this whole reform effort
is that each of us individually and theOrganization as a whole can make adifference. We can make a differenceto the health of the people in ourMember States, to the health systemsthat serve them, and to the policies onwhich their well-being depends.
Commitment to making apositive difference requires us to baseour decisions on the best evidence.“Evidence and information for policy”is the name of one of our nineprogramme clusters. It includesdeveloping research policy, managinginformation, and building up a solidbase of evidence on the best ways topromote health. The Bulletin of theWorld Health Organization plays a keypart in carrying out these functions,and it has been expanded and re-designed to do so more effectively.
The Bulletin now places researchfindings and policy-relevant discus-sions side by side in the same publica-tion. In doing so it is making animportant point: people with differentresponsibilities for health cannotafford to ignore each other’s work.Health decisions are aimed at savinglives, reducing suffering and promot-ing well-being. It is hard to think ofany area of decision-making that canbe more important for individuals andfor society as a whole. Clearly, suchdecisions must be based on the mostrigorous analysis possible of thetechnical and scientific factorsinvolved. But equally clearly, theymust be based on how people seethings. Perceptions of such matters asjustice, desirability and acceptabilitydiffer. Different kinds of informationand different points of view must beincluded if the right decision is to bemade.
Recent examples of the need fordebate include the control of some ofthe emerging diseases, and the use ofnew genetic technologies. Here therisk–benefit ratio cannot always bequantified, so it has to be weighed upin other ways. Even where the num-bers are available there may be noagreement on what an “acceptable”level of risk would be, or whatpreventive measures should be taken.More general questions of publichealth policy and practice, such asfinancing and priority-setting, requirea similar interaction of disciplines andviewpoints. It is clear that povertyincreases ill-health and that ill-healthincreases poverty. The vicious circlecannot be broken by health workersalone any more than it can by econo-mists and politicians alone. Educa-tion, lifestyle and environment alsohave a direct bearing on most of thepressing health problems of today.
The Bulletin in its new form willbe open to every perspective that canincrease our understanding of healthproblems and how to solve them. Inthis way it will reflect our decision tomake WHO not only a participantbut a leader in the current fast-movinginteractive process of global change. Itwill provide valuable information onthe hard work the health communityis doing around the world, and at thesame time try to convey some of theexcitement this work brings with it,and some of the courage and imagina-tion it requires of all of us. ■

2 Bulletin of the World Health Organization, 1999, 77 (1)
With this issue, the Bulletin of theWorld Health Organization has a newlook. As it starts its 52nd year, WHO’sBulletin also takes on a new and biggerrole in public health, appearingmonthly and covering an even widerrange of topics than before. Digestscontaining selected articles will alsoappear twice a year in Chinese, Frenchand Spanish.
Since 1948, the Bulletin has beenreporting internationally importanthealth research, much of it fromdeveloping countries. Now two ofWHO’s other journals, the Worldhealth statistics quarterly and the Worldhealth forum, have been incorporatedinto the Bulletin to make it, as itssubtitle states, “the internationaljournal of public health”. By mergingthese journals with their separateemphases on epidemiology, informa-tion exchange and science, WHOaims to bring together all that is bestin the theory and practice of publichealth worldwide. It is a mark of theOrganization’s commitment to seeinghealth from a broad perspective thatintegrates disciplines and combinesscientific enquiry with policy analysis.
Building on its well-establishedfoundation, the Bulletin will be theplace to find not just articles on thelatest internationally relevant scientificresearch but also reports and commen-taries on a wide range of health-relatedtopics of direct interest to healthpractitioners and policy-makers. It willreport regularly on WHO’s ownresearch, such as that on the globalburden of disease and injury, and willencompass issues such as health ethics,the financing of health care, and
research policy. Readers will be invitedto express their views in letters to theeditor, there will be round tablediscussions on timely and controver-sial issues, and reviews of books andelectronic media will keep readers upto date with the latest sources ofinformation in international publichealth.
While regular Bulletin readers willnotice many changes in this issue —both in content and in presentation— the aim of the Bulletin remainssimple and straightforward. It is toprovide a sound basis of evidence thatwill contribute to the achievement ofbetter health for all. The Bulletin willnot shrink from publishing well-founded arguments that are critical ofcurrent paradigms or the policies ofgovernments and agencies, includingWHO. To support this ambitioustask, a number of internationallyrecognized figures are being recruitedto serve on the journal’s editorialboard to guide policy and provideexpert assessment of all materialsubmitted for publication. Togetherwith an internal WHO team ofexperts, the board will ensure thehighest possible standards for theOrganization’s flagship journal.
WHO’s standpoint is clear: as aplatform for the widest range ofhealth-related information and analy-sis, the Bulletin will further thegreatest equity and efficiency, and thehighest quality, in health policies andprogrammes worldwide. We cannot besatisfied with less. ■
Editorials
A new role for the BulletinRichard G.A. Feachem1
1 Editor-in-Chief

Bulletin of the World Health Organization, 1999, 77 (1) 3© World Health Organization 1999
1 Professor of Medicine, National Institute of Hygiene, Warsaw, Poland.2 Medical Officer, Vaccines and Other Biologicals, World HealthOrganization, 1211 Geneva 27, Switzerland. Requests for reprintsshould be sent to this author.
3 Head, Centre for Communicable Diseases, Institute of PublicHealth of Slovenia, Ljubljana, Slovenia.
Research
Mumps and mumps vaccine: a global reviewA.M. Galazka,1 S.E. Robertson, 2 & A. Kraigher 3
IntroductionMumps is an acute infectious disease caused by aparamyxovirus closely related to parainfluenza vi-rus. Although the disease is usually mild, its burdenshould not be underestimated. Up to 10% of mumpspatients developed aseptic meningitis; a less com-mon but more serious complication is encephalitis,which can result in death or disability; and perma-nent deafness, orchitis and pancreatitis are otheruntoward effects that can be prevented by vaccina-tion. As of mid-1998, mumps vaccine was routinelyused by national childhood immunization pro-grammes in 82 countries. Where high coverage hasbeen achieved, countries have shown a rapid declinein mumps morbidity. Furthermore, in many coun-tries encephalitis associated with mumps has almosttotally vanished.
In this article we review the disease burdencaused by mumps; summarize studies on theimmunogenicity, efficacy, and safety of differentstrains of mumps vaccine; and highlight lessonslearned about implementing mumps immunizationfrom countries in different regions of the world.Guidance is provided for countries contemplatingthe introduction of mumps vaccine and for coun-tries already using this vaccine.
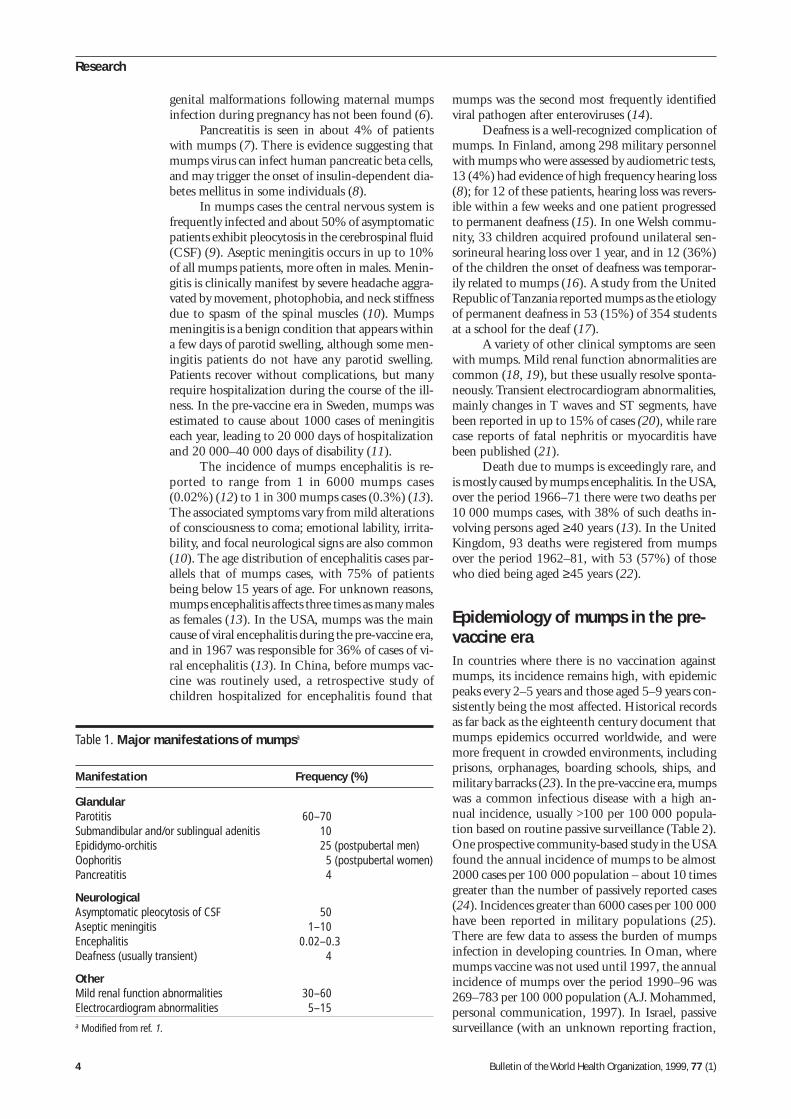
Disease burden due to mumpsHumans are the only natural hosts for mumps vi-rus, which is usually spread by respiratory droplets.The incubation period of mumps averages 16–18days, with a range of about 2–4 weeks (1). Infectionwith mumps virus is asymptomatic in one-third ofcases. Nonspecific prodromal symptoms include low-grade fever, anorexia, malaise, and headache. Thedisease can vary from a mild upper respiratory ill-ness to viraemia with widespread systemic involve-ment (Table 1). Classic mumps is characterized byenlargment of the parotid and other salivary glands;parotitis is bilateral in three-quarters of cases; andother salivary glands are involved in 10% of cases(1).
Epididymo-orchitis occurs in about 25% ofpostpubertal men who contract mumps. In one largecohort study the median age for mumps orchitis was29 years (range, 11–64 years) (2). Testicular atro-phy occurs in about one-third of patients withmumps orchitis, but sterility is rare. Mumps orchi-tis appears to be a risk factor for testicular cancer,though not a major one (3). In postpubertal women,mastitis and oophoritis can occur; one study foundmastitis in 31% of women over 14 years of age (4).Among women who acquire mumps during the first12 weeks of pregnancy, more than a quarter sufferspontaneous abortion; in a large cohort study, therate of spontaneous abortion in the first trimesterdue to mumps infection was higher than that due torubella infection (5). An increased incidence of con-
Mumps is an acute infectious disease caused by a paramyxovirus. Although the disease is usually mild, up to 10%of patients can develop aseptic meningitis; a less common but more serious complication is encephalitis, whichcan result in death or disability. Permanent deafness, orchitis, and pancreatitis are other untoward effects ofmumps. Based on data reported to WHO up to April 1998, mumps vaccine is routinely used by national immuniza-tion programmes in 82 countries/areas: 23 (92%) of 25 developed countries, 19 (86%) of 22 countries witheconomies in transition (mainly the Newly Independent States of the former Soviet Union), and 40 (24%) of 168developing countries. Countries that have achieved high coverage have shown a rapid decline in mumps morbid-ity. Furthermore, in many of these countries, mumps-associated encephalitis and deafness have nearly vanished.This review considers the disease burden due to mumps; summarizes studies on the immunogenicity, efficacy, andsafety of different strains of mumps vaccine; and highlights lessons learned about implementing mumps immuni-zation in different countries. Countries already using mumps vaccine should monitor immunization coverage andestablish routine mumps surveillance with investigation of outbreaks. Where mumps is targeted for elimination,countries need to add a second dose of mumps vaccine for children, keeping in mind that the disease may stilloccur in susceptible adults.
Voir page 11 le résumé en français. En la página 12 figura un resumen en español.
4 Bulletin of the World Health Organization, 1999, 77 (1)
Research
genital malformations following maternal mumpsinfection during pregnancy has not been found (6).
Pancreatitis is seen in about 4% of patientswith mumps (7). There is evidence suggesting thatmumps virus can infect human pancreatic beta cells,and may trigger the onset of insulin-dependent dia-betes mellitus in some individuals (8).
In mumps cases the central nervous system isfrequently infected and about 50% of asymptomaticpatients exhibit pleocytosis in the cerebrospinal fluid(CSF) (9). Aseptic meningitis occurs in up to 10%of all mumps patients, more often in males. Menin-gitis is clinically manifest by severe headache aggra-vated by movement, photophobia, and neck stiffnessdue to spasm of the spinal muscles (10). Mumpsmeningitis is a benign condition that appears withina few days of parotid swelling, although some men-ingitis patients do not have any parotid swelling.Patients recover without complications, but manyrequire hospitalization during the course of the ill-ness. In the pre-vaccine era in Sweden, mumps wasestimated to cause about 1000 cases of meningitiseach year, leading to 20 000 days of hospitalizationand 20 000–40 000 days of disability (11).
The incidence of mumps encephalitis is re-ported to range from 1 in 6000 mumps cases(0.02%) (12) to 1 in 300 mumps cases (0.3%) (13).The associated symptoms vary from mild alterationsof consciousness to coma; emotional lability, irrita-bility, and focal neurological signs are also common(10). The age distribution of encephalitis cases par-allels that of mumps cases, with 75% of patientsbeing below 15 years of age. For unknown reasons,mumps encephalitis affects three times as many malesas females (13). In the USA, mumps was the maincause of viral encephalitis during the pre-vaccine era,and in 1967 was responsible for 36% of cases of vi-ral encephalitis (13). In China, before mumps vac-cine was routinely used, a retrospective study ofchildren hospitalized for encephalitis found that
mumps was the second most frequently identifiedviral pathogen after enteroviruses (14).
Deafness is a well-recognized complication ofmumps. In Finland, among 298 military personnelwith mumps who were assessed by audiometric tests,13 (4%) had evidence of high frequency hearing loss(8); for 12 of these patients, hearing loss was revers-ible within a few weeks and one patient progressedto permanent deafness (15). In one Welsh commu-nity, 33 children acquired profound unilateral sen-sorineural hearing loss over 1 year, and in 12 (36%)of the children the onset of deafness was temporar-ily related to mumps (16). A study from the UnitedRepublic of Tanzania reported mumps as the etiologyof permanent deafness in 53 (15%) of 354 studentsat a school for the deaf (17).
A variety of other clinical symptoms are seenwith mumps. Mild renal function abnormalities arecommon (18, 19), but these usually resolve sponta-neously. Transient electrocardiogram abnormalities,mainly changes in T waves and ST segments, havebeen reported in up to 15% of cases (20), while rarecase reports of fatal nephritis or myocarditis havebeen published (21).
Death due to mumps is exceedingly rare, andis mostly caused by mumps encephalitis. In the USA,over the period 1966–71 there were two deaths per10 000 mumps cases, with 38% of such deaths in-volving persons aged ≥40 years (13). In the UnitedKingdom, 93 deaths were registered from mumpsover the period 1962–81, with 53 (57%) of thosewho died being aged ≥45 years (22).
Epidemiology of mumps in the pre-vaccine eraIn countries where there is no vaccination againstmumps, its incidence remains high, with epidemicpeaks every 2–5 years and those aged 5–9 years con-sistently being the most affected. Historical recordsas far back as the eighteenth century document thatmumps epidemics occurred worldwide, and weremore frequent in crowded environments, includingprisons, orphanages, boarding schools, ships, andmilitary barracks (23). In the pre-vaccine era, mumpswas a common infectious disease with a high an-nual incidence, usually >100 per 100 000 popula-tion based on routine passive surveillance (Table 2).One prospective community-based study in the USAfound the annual incidence of mumps to be almost2000 cases per 100 000 population – about 10 timesgreater than the number of passively reported cases(24). Incidences greater than 6000 cases per 100 000have been reported in military populations (25).There are few data to assess the burden of mumpsinfection in developing countries. In Oman, wheremumps vaccine was not used until 1997, the annualincidence of mumps over the period 1990–96 was269–783 per 100 000 population (A.J. Mohammed,personal communication, 1997). In Israel, passivesurveillance (with an unknown reporting fraction,
Table 1. Major manifestations of mumpsa
Manifestation Frequency (%)
GlandularParotitis 60–70Submandibular and/or sublingual adenitis 10Epididymo-orchitis 25 (postpubertal men)Oophoritis 5 (postpubertal women)Pancreatitis 4
NeurologicalAsymptomatic pleocytosis of CSF 50Aseptic meningitis 1–10Encephalitis 0.02–0.3Deafness (usually transient) 4
OtherMild renal function abnormalities 30–60Electrocardiogram abnormalities 5–15a Modified from ref. 1.
Bulletin of the World Health Organization, 1999, 77 (1) 5
but possibly as low as 20%) found the annual inci-dence of mumps to be 80–162 per 100 000 popula-tion over the period 1977–88 prior to introductionof mumps vaccine (26).
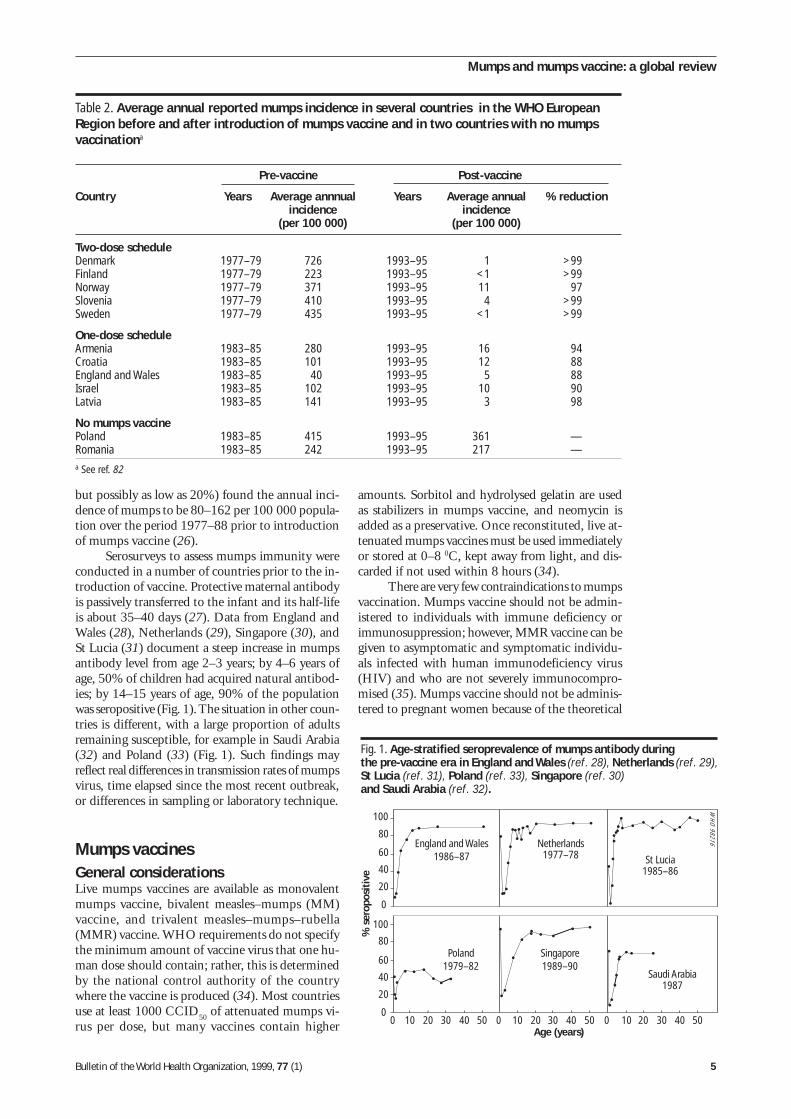
Serosurveys to assess mumps immunity wereconducted in a number of countries prior to the in-troduction of vaccine. Protective maternal antibodyis passively transferred to the infant and its half-lifeis about 35–40 days (27). Data from England andWales (28), Netherlands (29), Singapore (30), andSt Lucia (31) document a steep increase in mumpsantibody level from age 2–3 years; by 4–6 years ofage, 50% of children had acquired natural antibod-ies; by 14–15 years of age, 90% of the populationwas seropositive (Fig. 1). The situation in other coun-tries is different, with a large proportion of adultsremaining susceptible, for example in Saudi Arabia(32) and Poland (33) (Fig. 1). Such findings mayreflect real differences in transmission rates of mumpsvirus, time elapsed since the most recent outbreak,or differences in sampling or laboratory technique.
Mumps vaccinesGeneral considerationsLive mumps vaccines are available as monovalentmumps vaccine, bivalent measles–mumps (MM)vaccine, and trivalent measles–mumps–rubella(MMR) vaccine. WHO requirements do not specifythe minimum amount of vaccine virus that one hu-man dose should contain; rather, this is determinedby the national control authority of the countrywhere the vaccine is produced (34). Most countriesuse at least 1000 CCID
50 of attenuated mumps vi-
rus per dose, but many vaccines contain higher
amounts. Sorbitol and hydrolysed gelatin are usedas stabilizers in mumps vaccine, and neomycin isadded as a preservative. Once reconstituted, live at-tenuated mumps vaccines must be used immediatelyor stored at 0–8 0C, kept away from light, and dis-carded if not used within 8 hours (34).
There are very few contraindications to mumpsvaccination. Mumps vaccine should not be admin-istered to individuals with immune deficiency orimmunosuppression; however, MMR vaccine can begiven to asymptomatic and symptomatic individu-als infected with human immunodeficiency virus(HIV) and who are not severely immunocompro-mised (35). Mumps vaccine should not be adminis-tered to pregnant women because of the theoretical
Fig. 1. Age-stratified seroprevalence of mumps antibody duringthe pre-vaccine era in England and Wales (ref. 28), Netherlands (ref. 29),St Lucia (ref. 31), Poland (ref. 33), Singapore (ref. 30)and Saudi Arabia (ref. 32).
% s
erop
osit
ive
Age (years)
England and Wales1986–87
100
Netherlands1977–78
Poland1979–82
Singapore1989–90
Saudi Arabia1987
St Lucia1985–86
80
60
40
20
0
100
80
60
40
20
010 20 30 40 50 0 10 20 30 40 50 0 10 20 30 40 500
WH
O 98216
Table 2. Average annual reported mumps incidence in several countries in the WHO EuropeanRegion before and after introduction of mumps vaccine and in two countries with no mumpsvaccinationa
Pre-vaccine Post-vaccine
Country Years Average annnual Years Average annual % reductionincidence incidence
(per 100 000) (per 100 000)
Two-dose scheduleDenmark 1977–79 726 1993–95 1 >99Finland 1977–79 223 1993–95 <1 >99Norway 1977–79 371 1993–95 11 97Slovenia 1977–79 410 1993–95 4 >99Sweden 1977–79 435 1993–95 <1 >99
One-dose scheduleArmenia 1983–85 280 1993–95 16 94Croatia 1983–85 101 1993–95 12 88England and Wales 1983–85 40 1993–95 5 88Israel 1983–85 102 1993–95 10 90Latvia 1983–85 141 1993–95 3 98
No mumps vaccinePoland 1983–85 415 1993–95 361 —Romania 1983–85 242 1993–95 217 —a See ref. 82
Mumps and mumps vaccine: a global review

6 Bulletin of the World Health Organization, 1999, 77 (1)
Research
risk of fetal damage, and pregnancy should beavoided for 3 months after vaccination (35). Indi-viduals with common forms of allergy (atopic ec-zema, asthma, cow’s milk allergy) can be vaccinatedsafely with MMR vaccine (36). In the past, egg al-lergy was considered a reason not to administermumps vaccine; however, recent studies documentthat among 1227 known egg-allergic individuals whoreceived a standard dose of mumps vaccine only two(0.16%) had any symptoms suggesting anaphylaxis(37). Other components of MMR vaccine, such asgelatin (38) and neomycin (39), can produce hy-persensitivity to the vaccine in some individuals.
Immunogenicity, efficacy, and safetyWe review data on immunogenicity, efficacy, andsafety for the five most commonly used mumps vac-cine strains below. The scope of this article does notpermit comparisons of serological methods, case defi-nitions, or methods of surveillance. Information onsafety is limited to reported rates of vaccine-associ-ated aseptic meningitis, which have been recalcu-lated as rates per 100 000 vaccine doses.
Jeryl Lynn strain mumps vaccine. The JerylLynn strain, named after the child from whom thevirus was isolated, was developed in the USA bypassaging the virus in embryonated hen’s eggs, thenin chick embryo cell cultures (40). The strain waslicensed in the USA in 1967, and by 1992 it hadbeen administered to approximately 135 millionchildren and adults around the world (34).
Clinical studies in industrialized countriesshow that a single dose of Jeryl Lynn strain mumpsvaccine leads to initial seroconversion rates of 80–100% (41). Further studies document persistenceof antibody in a large proportion of vaccinees. InSweden, 73% of 229 children who received MMRvaccine containing Jeryl Lynn strain mumps vaccineat 18 months of age remained seropositive 10.5 yearslater (42). In Finland, 4 years after the second MMRvaccine dose (with Jeryl Lynn mumps strain) and 9years after the initial dose the seropositivity rate was86% (43). The clinical protective efficacy of the JerylLynn strain of mumps vaccine in outbreak-basedstudies in the USA has ranged from 75% to 91%(44). Two recent outbreak investigations in the USAfound that the risk of mumps increased with timeelapsed since vaccination, suggesting possible wan-ing of vaccine-induced immunity (45, 46). Few stud-ies of Jeryl Lynn vaccine have been conducted indeveloping countries; however, in the DominicanRepublic, a study of this vaccine reported 94%seroconversion among 72 seronegative children aged1–6 years (47).
In the USA, a 10-year retrospective study ofhospitalized cases of mumps found one case of asep-tic meningitis per 100 000 doses of MMR vaccine(with Jeryl Lynn mumps strain) in a cohort of chil-dren aged 12–23 months (48). Although these find-ings are reassuring, further prospective studies areplanned. In Germany, the Jeryl Lynn strain was
associated with 0.1 aseptic meningitis cases per100 000 vaccine doses (49).
Leningrad-3 strain mumps vaccine. The Len-ingrad-3 mumps attenuated strain was developed inthe Soviet Union in guinea-pig kidney cell culture,with further passages in Japanese quail embryo cul-tures (50). Vaccines based on the Leningrad-3 strainhave been used since 1974 in the former SovietUnion and other countries. Approximately 8–11million doses of Leningrad-3 mumps vaccine areproduced annually (34). Studies have shown 89–98% seroconversion among children aged 1–7 yearsfollowing receipt of Leningrad-3 mumps vaccine,and a protective efficacy of 92–99% (50). A large-scale efficacy trial that enrolled more than 100 000children found the vaccine to have 97% protectiveefficacy in the outbreak setting (51).
In Slovenia, passive surveillance over the pe-riod 1979–85 identified 20 cases of aseptic menin-gitis per 100 000 doses of MM vaccine with theLeningrad-3 mumps strain (52). Further retrospec-tive review of the medical records of Slovenian pa-tients hospitalized for aseptic meningitis during1979–86 found an incidence of 100 cases of asepticmeningitis per 100 000 doses of MM vaccine con-taining Leningrad-3 mumps strain; however, at thetime of discharge, all symptoms had resolved andno patient had any sequelae (53).
L-Zagreb strain mumps vaccine. In Croatia,the L-Zagreb strain was obtained by further attenu-ation of Leningrad-3 mumps virus by adaptation andpassage on chick embryo fibroblast cell culture (54).Over the period 1976–87, more than 10 milliondoses of L-Zagreb mumps vaccine were distributedin the former Yugoslavia and elsewhere (54).
Studies in Croatia showed 87–100%seroresponse to L-Zagreb mumps vaccine and a vac-cine efficacy of 97–100% (54). In India, a singledose of locally produced MMR vaccine containingthe L-Zagreb mumps strain increased mumps sero-positivity from 12% to 92% among 15–24-month-olds (55).
In Slovenia, MMR vaccine containing the L-Zagreb mumps strain has been used since 1990, andpassive surveillance over the period 1990–96 revealedtwo cases of aseptic meningitis per 100 000 doses(A. Kraigher, unpublished data, 1997). In Croatia,there were 90 cases of aseptic meningitis per 100 000doses of MMR vaccine containing the L-Zagrebmumps strain over the period 1988–92 (56).
Rubini strain mumps vaccine. The Rubinimumps virus strain was passaged first in a humandiploid cell line, serially passaged in embryonatedhen’s eggs, then adapted to the MRC-5 human dip-loid cell line (57). Mumps vaccine based on theRubini strain was licensed in Switzerland in 1985,and by 1990 more than 4 million people aroundthe world had been immunized with it (34).
A study in Germany of children aged 14–24months who received a dose of MMR vaccine foundthat 95% seroconverted when the mumps strain was

Bulletin of the World Health Organization, 1999, 77 (1) 7
Rubini, compared with 100% when the strain wasJeryl Lynn (58). Recent studies in Switzerland, Italy,and Portugal provide evidence that mumps vaccinebased on the Rubini strain does not appear to offerlong-term protection against the disease. In Swit-zerland, a study of secondary attack rates among thefamily contacts 16 y ears of age (median age, 6.9years) of confirmed mumps cases (median age, 6.2years) found a protective efficacy of 6% for theRubini strain mumps vaccine compared with 73%for the Urabe strain vaccine and 62% for the JerylLynn strain vaccine (59). Several other Swiss studiesconfirm the low efficacy of the Rubini strain vac-cine (60, 61). In Italy, a case–control study con-ducted during 1995–96 found that, compared withchildren vaccinated with Jeryl Lynn or Urabe strainmumps vaccine, children vaccinated with the Rubinistrain vaccine had a higher risk of contractingmumps: 1.2 for children aged <4 years; 3.0 for 4–6-year-olds; and 12.8 for 7–12-year-olds (62). In Por-tugal, MMR coverage of children aged 12–23months has been >90% since 1991; despite this, alarge mumps epidemic occurred in 1995–96 withthe highest incidence among children aged 1–4 years.A plot of the number of cases according to their prob-able month and year of vaccination showed that therewas a large increase in mumps incidence among chil-dren vaccinated after October 1992, which corre-sponded to the date when Portugal began to use theRubini strain of mumps vaccine exclusively (63).
Urabe strain mumps vaccine. The Urabe strainof live mumps vaccine was first licensed in Japan in1979, and thereafter in Belgium, France, and Italy(34). It is produced either in the amnion of embryo-nated hen’s eggs or in chick embryo cell cultures. By1991, more than 60 million persons around theworld had been immunized with the Urabe strain ofmumps vaccine (34).
In a study in Finland, among children whoreceived mumps vaccine at 14–20 months of age,95% seroconverted with the Urabe strain, comparedwith 97% with the Jeryl Lynn strain (64). Severalstudies have assessed the immunogenicity of theUrabe strain mumps vaccine in developing coun-tries. Among seronegative children who receivedUrabe strain mumps vaccine at 9 months of age,99% seroconverted in Brazil (65), 98% in SouthAfrica (66), and 75% in India (67). Among chil-dren aged 12 months, 100% responded in Brazil(65), 98% in China (Province of Taiwan) (68), and92% in India (67). At 15 months of age, 100% ofrecipients responded in South Africa (66), and at14–18 months, 98% responded in China (Provinceof Taiwan) (68).
In the United Kingdom, a study showed that4 years after a single dose of MMR vaccine the sero-positivity rates were 85% for the Urabe strain, com-pared with 81% for the Jeryl Lynn strain (69). InCanada, a study found that 5–6 years after one doseof MMR vaccine the seropositivity rate was 93%for the Urabe strain, compared with 85% for theJeryl Lynn strain (70).
Following reports of aseptic meningitis casestemporally associated with the administration ofMMR vaccine containing Urabe mumps virus strain,Canada initiated molecular studies, which showedthat the Urabe vaccine is a mixture of viruses, withwild type A and variant G. Spinal fluid from Urabestrain vaccinees who developed aseptic meningitis orparotitis showed predominately wild type A (71). MMRvaccine containing the Urabe strain was therefore with-drawn from the market in Canada in 1990 (72).
Several studies in the United Kingdom haveexamined rates of aseptic meningitis following vac-cination with Urabe strain vaccine. A study in Not-tingham was followed by a multi-centre confirmatorystudy, which showed a rate of 9 aseptic meningitiscases per 100 000 vaccine doses (73). As a result,the Public Health Service in the United Kingdomstopped purchasing Urabe strain vaccine in 1992.
In Japan, nationwide surveillance conductedby the Ministry of Health and Welfare during 1989demonstrated an overall rate of 49 cases of asepticmeningitis per 100 000 doses of domestically pro-duced MMR vaccine containing Urabe mumpsstrain (74). Subsequent studies up to 1993 identi-fied an incidence of approximately 100 aseptic men-ingitis cases per 100 000 doses of MMR containingUrabe mumps strain (although rates differed bymanufacturer), and in April 1993 the Ministry ofHealth and Welfare of Japan withdrew all domesti-cally produced MMR vaccines (75).
Use of mumps vaccine around theworldBased on data reported to WHO up to April 1998,a total of 82 countries/areas (38%) are using mumpsvaccine in their national immunization programme.This is similar to the situation for rubella vaccine,which is used on a national basis in 78 countries/areas (76). Based on the United Nations countryclassification scheme (77), mumps vaccine is usedby 23 (92%) of 25 developed countries; 19 (86%)of 22 countries with economies in transition (mainlythe Newly Independent States of the former SovietUnion); and 40 (24%) of 168 developing countries.Among the 82 countries/areas using mumps vaccine,52 (63%) schedule one dose of mumps vaccine and30 (37%) have a two-dose schedule. Mumps vac-cine use varies widely by region (Table 3), as de-tailed below.
African RegionNo countries in the WHO African Region includemumps vaccine in their national immunizationschedule.
Region of the AmericasIn the WHO Region of the Americas, 21 (45%)countries/areas use mumps vaccine: 15 give one doseof MMR vaccine and 6 give two doses of MMR vac-cine (Table 3). Use of MMR vaccine is receiving
Mumps and mumps vaccine: a global review
8 Bulletin of the World Health Organization, 1999, 77 (1)
Research
increasing attention in the Americas, and regionaltargets for mumps control and eventual eliminationare under discussion.
Canada. In Quebec Province, one dose ofMMR vaccine was introduced in 1976 for childrenat 12 months of age; coverage has been >95% since1980. The annual number of reported mumps caseshas fallen from 6858 in 1977 to fewer than 100 peryear since 1981, with the exception of an outbreakin 1988–89 (78). Cases in the outbreak occurredlargely among unvaccinated students aged 15–19years, who were born prior to the introduction ofvaccine. Because of the low incidence of mumps inQuebec, the province has elected not to add a sec-ond dose of mumps vaccine.
USA. Use of mumps vaccine began in the USAin 1967, when the incidence of the disease was al-most 90 per 100 000 population (79). However,during the next decade mumps immunization wasconsidered a low priority. In 1977, routine mumpsimmunization was recommended at 12 months ofage or older, and this was facilitated by the availabil-ity of MMR vaccine. During 1985–86 large mumpsoutbreaks occurred among underimmunized cohortsborn in the period 1967–77, resulting in a shift inpeak incidence from 5–9-year-olds to 10–19-year-olds. In 1989, a second dose of MMR vaccine wasrecommended at 4–6 years of age. The incidence ofmumps fell from 2 per 100 000 population in 1988to 0.7 per 100 000 population in 1993 (79).
Eastern Mediterranean RegionIn the WHO Eastern Mediterranean Region, 11countries/areas (48%) include mumps vaccine in thenational immunization schedule: six countries useone dose and five countries use two doses of MMRvaccine (Table 3).
European RegionOf the 51 countries/areas in the WHO EuropeanRegion, 43 (84%) use mumps vaccine on a national
basis (Table 3). In western Europe, most countriesschedule one or two doses of MMR vaccine. Amongthe Newly Independent States of the former SovietUnion, 14 countries administer a single dose ofmonovalent mumps vaccine. In 1991, the EuropeanRegion set a target of mumps elimination by theyear 2000; and in 1993 this was defined as an an-nual mumps incidence of <1 case per 100 000 popu-lation in each country (80). The Health for Alldatabase of the European Regional Office includesthe annual number of reported mumps cases andincidence by country (81). These data show that inthe pre-vaccine era mumps incidence generally ex-ceeded 100 per 100 000 population (Table 2). Fol-lowing the introduction of mumps vaccine, theaverage annual incidence of the disease dropped sig-nificantly in countries using a one-dose immuniza-tion schedule, and reached levels <1 per 100 000population in several countries using a two-doseschedule.
Croatia. In the Rijeka region (population,340 000 in 1990), mumps immunization started in1976. At 15 months of age children receive a doseof MMR vaccine containing the L-Zagreb strain;coverage has been ≥92% (82). In 1977 and 1981–82 mumps outbreaks occurred, and then there wasan 8-year period with lower incidence (31–78mumps cases per 100 000 population). Mumps vac-cination led to a shift in the age distribution of cases,with the highest incidence being among 5–9-year-olds over the period 1976–82, and among 15–19-year-olds over the period 1983–90.
England and Wales. From 1962 to 1981 Eng-land and Wales had an annual mumps incidence of160–1011 cases per 100 000 population (22).Mumps vaccine was introduced in October 1988,when MMR vaccine was scheduled for all childrenaged 12–15 months (83). In addition, all pre-schoolchildren were offered MMR vaccine in a 3-yearcatch-up programme. Since 1991, mumps vaccinecoverage of children by their second birthday hasexceeded 90%. The annual incidence of mumps fellto 5 per 100 000 population in the period 1993–95(Table 2). The number of hospital admissions formumps fell by 92% compared with the pre-vaccineera (83). Nevertheless, studies in vaccinated pre-school cohorts showed that 15% of children wereseronegative for mumps. Therefore, in 1997 a sec-ond dose of MMR vaccine was added at age 4 years(83).
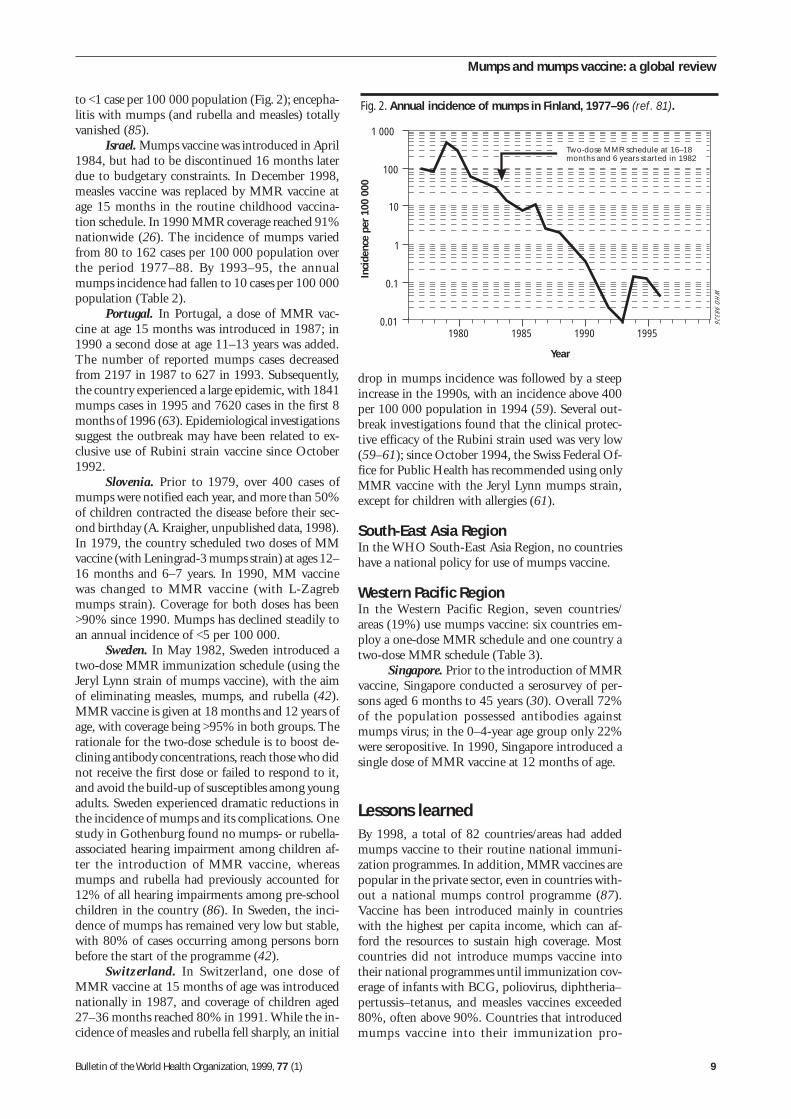
Finland. In the 1970s the mean annual inci-dence of mumps was 240 cases per 100 000 popula-tion, meningitis and orchitis were commoncomplications, and occasional deaths were reported.In 1982 a national immunization programme wasbegun, with two doses of MMR vaccine (with JerylLynn mumps strain) at age 14–18 months and 6years (84). Over a period of 12 years, 1.5 million ofthe 5 million Finnish population were vaccinated.As a result, there was a 99% decrease in the inci-dence of mumps and the annual incidence dropped
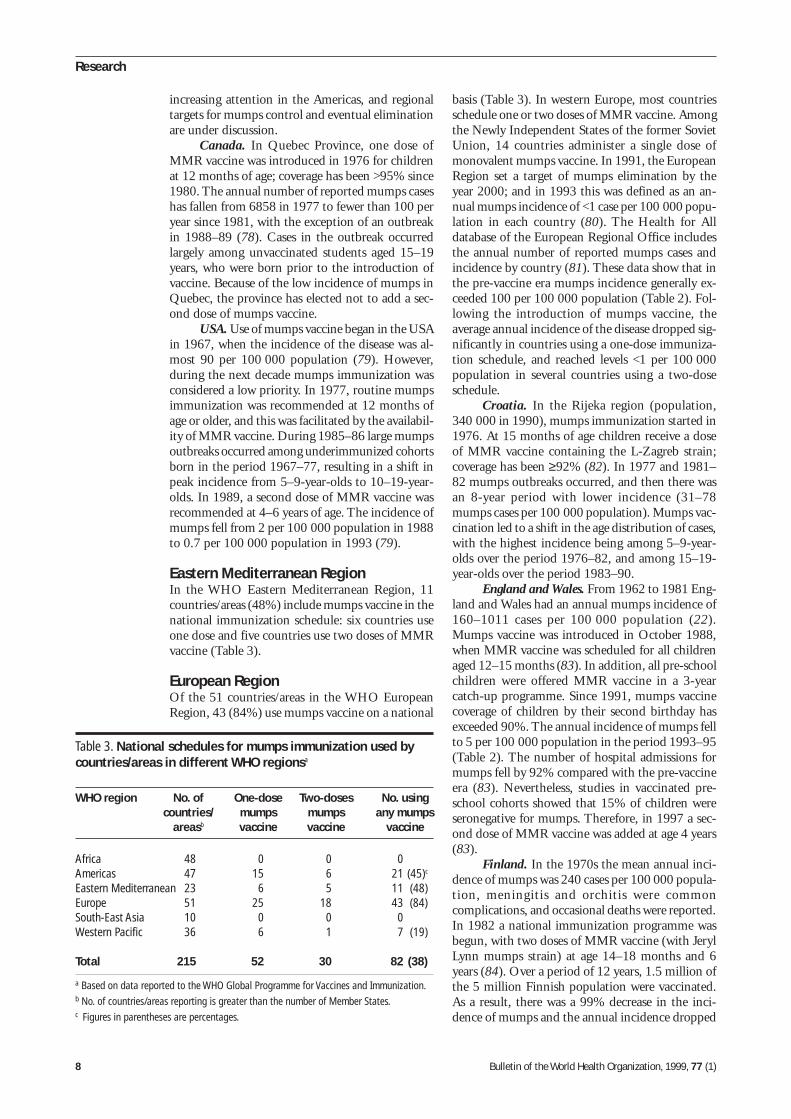
Table 3. National schedules for mumps immunization used bycountries/areas in different WHO regionsa
WHO region No. of One-dose Two-doses No. usingcountries/ mumps mumps any mumps
areasb vaccine vaccine vaccine
Africa 48 0 0 0Americas 47 15 6 21 (45)c
Eastern Mediterranean 23 6 5 11 (48)Europe 51 25 18 43 (84)South-East Asia 10 0 0 0Western Pacific 36 6 1 7 (19)
Total 215 52 30 82 (38)
a Based on data reported to the WHO Global Programme for Vaccines and Immunization.b No. of countries/areas reporting is greater than the number of Member States.c Figures in parentheses are percentages.
Bulletin of the World Health Organization, 1999, 77 (1) 9
to <1 case per 100 000 population (Fig. 2); encepha-litis with mumps (and rubella and measles) totallyvanished (85).
Israel. Mumps vaccine was introduced in April1984, but had to be discontinued 16 months laterdue to budgetary constraints. In December 1998,measles vaccine was replaced by MMR vaccine atage 15 months in the routine childhood vaccina-tion schedule. In 1990 MMR coverage reached 91%nationwide (26). The incidence of mumps variedfrom 80 to 162 cases per 100 000 population overthe period 1977–88. By 1993–95, the annualmumps incidence had fallen to 10 cases per 100 000population (Table 2).
Portugal. In Portugal, a dose of MMR vac-cine at age 15 months was introduced in 1987; in1990 a second dose at age 11–13 years was added.The number of reported mumps cases decreasedfrom 2197 in 1987 to 627 in 1993. Subsequently,the country experienced a large epidemic, with 1841mumps cases in 1995 and 7620 cases in the first 8months of 1996 (63). Epidemiological investigationssuggest the outbreak may have been related to ex-clusive use of Rubini strain vaccine since October1992.
Slovenia. Prior to 1979, over 400 cases ofmumps were notified each year, and more than 50%of children contracted the disease before their sec-ond birthday (A. Kraigher, unpublished data, 1998).In 1979, the country scheduled two doses of MMvaccine (with Leningrad-3 mumps strain) at ages 12–16 months and 6–7 years. In 1990, MM vaccinewas changed to MMR vaccine (with L-Zagrebmumps strain). Coverage for both doses has been>90% since 1990. Mumps has declined steadily toan annual incidence of <5 per 100 000.
Sweden. In May 1982, Sweden introduced atwo-dose MMR immunization schedule (using theJeryl Lynn strain of mumps vaccine), with the aimof eliminating measles, mumps, and rubella (42).MMR vaccine is given at 18 months and 12 years ofage, with coverage being >95% in both groups. Therationale for the two-dose schedule is to boost de-clining antibody concentrations, reach those who didnot receive the first dose or failed to respond to it,and avoid the build-up of susceptibles among youngadults. Sweden experienced dramatic reductions inthe incidence of mumps and its complications. Onestudy in Gothenburg found no mumps- or rubella-associated hearing impairment among children af-ter the introduction of MMR vaccine, whereasmumps and rubella had previously accounted for12% of all hearing impairments among pre-schoolchildren in the country (86). In Sweden, the inci-dence of mumps has remained very low but stable,with 80% of cases occurring among persons bornbefore the start of the programme (42).
Switzerland. In Switzerland, one dose ofMMR vaccine at 15 months of age was introducednationally in 1987, and coverage of children aged27–36 months reached 80% in 1991. While the in-cidence of measles and rubella fell sharply, an initial
drop in mumps incidence was followed by a steepincrease in the 1990s, with an incidence above 400per 100 000 population in 1994 (59). Several out-break investigations found that the clinical protec-tive efficacy of the Rubini strain used was very low(59–61); since October 1994, the Swiss Federal Of-fice for Public Health has recommended using onlyMMR vaccine with the Jeryl Lynn mumps strain,except for children with allergies (61).
South-East Asia RegionIn the WHO South-East Asia Region, no countrieshave a national policy for use of mumps vaccine.
Western Pacific RegionIn the Western Pacific Region, seven countries/areas (19%) use mumps vaccine: six countries em-ploy a one-dose MMR schedule and one country atwo-dose MMR schedule (Table 3).
Singapore. Prior to the introduction of MMRvaccine, Singapore conducted a serosurvey of per-sons aged 6 months to 45 years (30). Overall 72%of the population possessed antibodies againstmumps virus; in the 0–4-year age group only 22%were seropositive. In 1990, Singapore introduced asingle dose of MMR vaccine at 12 months of age.
Lessons learnedBy 1998, a total of 82 countries/areas had addedmumps vaccine to their routine national immuni-zation programmes. In addition, MMR vaccines arepopular in the private sector, even in countries with-out a national mumps control programme (87).Vaccine has been introduced mainly in countrieswith the highest per capita income, which can af-ford the resources to sustain high coverage. Mostcountries did not introduce mumps vaccine intotheir national programmes until immunization cov-erage of infants with BCG, poliovirus, diphtheria–pertussis–tetanus, and measles vaccines exceeded80%, often above 90%. Countries that introducedmumps vaccine into their immunization pro-
WH
O 98326
Fig. 2. Annual incidence of mumps in Finland, 1977–96 (ref. 81).
1 000
100
10
1
0.1
0.011980 1985 1990 1995
YearIn
cide
nce
per
100
000
Two-dose MMR schedule at 16–18months and 6 years started in 1982
Mumps and mumps vaccine: a global review
10 Bulletin of the World Health Organization, 1999, 77 (1)
Research
grammes exhibited a rapid decline in mumps mor-bidity. Countries implementing a one-dose sched-ule at high coverage levels reported reductions inmumps incidence of ≥88% (Table 2). Countries im-plementing a two-dose schedule at high levels ofcoverage for both doses show reductions in mumpsincidence of ≥97%, and several countries reachedthe elimination target of <1 mumps case per 100 000population (Table 2). Sustained high levels of vacci-nation against mumps can be expected to lengthenthe inter-epidemic period, while susceptibles accu-mulate in the population; thus, mumps outbreakscan be expected 10–20 years after the introductionof routine mumps immunization. Such outbreaksare more likely to be seen among older age groups,especially those aged 15–30 years, who were too oldto receive vaccine and whose exposure to wildmumps virus was reduced by the herd effect of thevaccination programme.
Guidance for countries consideringusing mumps vaccineSo far, mumps vaccine has not been recommendedas part of the global Expanded Programme on Im-munization. Countries considering the use ofmumps vaccine should review the WHO guidelinesfor introduction of new vaccines (88), paying care-ful attention to the aspects discussed below.
• Consider the disease burdenInformation on the incidence of mumps and the agegroups affected should be examined. Data on theproportion of encephalitis and meningitis due tomumps can help in determining the importance ofthe disease. In some countries, Japanese encephali-tis, dengue, varicella, or tick-borne encephalitis maybe the primary causes of encephalitis, but local dataneed to be examined to determine the relative dis-ease burden due to mumps. Studies to assess hear-ing disabilities should consider mumps as a possibleetiology.
• Decide on an appropriate routineschedule
Mumps vaccine can be most efficiently incorporatedinto the immunization schedule by using MMR vac-cine. Separate delivery of single-antigen mumps vac-cine is less practical, since this requires an extrainjection and may also lead to an additional healthcare visit. Serological studies show that vaccine re-sponse rates are excellent from the age of 12 months.For the Urabe strain mumps vaccine, theseroresponse rates appear high from the age of 9months. An initial target of mumps control wouldsuggest use of a single dose of MMR vaccine at 9–15 months of age, and countries should aim for cov-erage of ≥80%. Using MMR instead of measlesvaccine will require further considerations aboutwhat strategy is appropriate to prevent congenital
rubella syndrome (76). If a large proportion of theadult population remains seronegative for mumps,care should be taken to provide mumps vaccine toadults who may be at special risk, including healthworkers, teachers, and military personnel.
• Select the mumps vaccineSeveral mumps vaccines based on different attenu-ated strains are available. Recent studies indicate thatthe Rubini strain does not provide sufficient long-term clinical protection, although several othermumps vaccine strains do provide better long-termprotection as demonstrated in outbreak investiga-tions. Among the available strains, the rates of vac-cine-associated aseptic meningitis vary; however,vaccine-associated meningitis resolves spontaneouslyin less than a week, and there are no sequelae. Natu-ral mumps infection leads to aseptic meningitis inup to 10% of patients, and this also resolves sponta-neously within a week without sequelae. It is of fargreater concern that natural mumps infection canlead to encephalitis, with a risk of death or perma-nent disability. Thus, countries need to consider thatthe incidence and severity of meningitis and en-cephalitis following natural infection greatly exceedthose associated with any protective mumps vaccinecurrently available in international commerce (89).
• Assess costsStudies in several countries have found that the in-troduction of routine mumps vaccine is economi-cally justifiable. In Austria, the benefit–cost ratio was3.6 for routine immunization using Jeryl Lynnmumps vaccine (90). In Israel, the benefit–cost ra-tio was 5.9 for routine immunization with MMRvaccine at 15 months of age (91). The results ofbenefit–cost analyses may, however, differ from onecountry to another, and countries should considerlocal estimates of disease burden, costs of treatment,costs of vaccination, and the rates of adverse eventsfor the vaccine strain of interest. Some countrieswhich have attained high measles vaccine coverageand have concerns about the burden of mumps dis-ease may find that they cannot afford to replacemonovalent measles vaccine with MMR because ofthe cost of the vaccine. Benefit–cost analysis mayhelp in approaching potential donors.
Recommendations for countriesalready using mumps vaccineFor countries already using mumps vaccine, mumpscontrol programmes should include the activitiesdiscussed below.
• Monitor immunization coverageWhere mumps vaccine is delivered as MMR vac-cine, immunization coverage monitoring is likelyalready to be in place. Countries that deliver single-antigen mumps vaccine need to be certain that the

Bulletin of the World Health Organization, 1999, 77 (1) 11
coverage is monitored. When second doses are de-livered to pre-school or school-aged populations,coverage should also be monitored.
• Conduct routine surveillance ofmumps
Mumps should be a notifiable disease, recognizingthat passive surveillance generally underreports dis-ease incidence but it can monitor trends and signaloutbreaks. It is important to remember that mumpsaffects adults; WHO surveillance guidelines, whichinclude recommended case definitions, are beingdeveloped.
• Investigate outbreaksMumps outbreaks should be investigated to the ex-tent that resources allow.
• Assess (and re-assess) control versuselimination strategies
Countries already using a single dose of mumps vac-cine may eventually contemplate including a sec-ond dose. The potential benefit will depend onwhether the objective of the programme is controlor elimination of the disease. As countries use masscampaigns to deliver extra doses of measles vaccineto particular target groups, measles vaccine can be
substituted by MMR vaccine; however, mass cam-paigns with MMR vaccine should be planned onlywhere long-term routine immunization against ru-bella and mumps is being implemented.
• Conduct researchWhen new mumps vaccine strains are introduced,studies on their immunogenicity should be carriedout in both industrialized and developing countries.The field effectiveness of vaccines, especially newerstrains, needs to be monitored. A more difficult taskis to establish and maintain sufficiently sensitivemonitoring systems that can provide reliable dataon rare adverse events. In countries where mumpsvaccine has been in use for many years, there is aneed for continued study of the duration of protec-tion following vaccination in childhood, particularlyif there is little natural boosting from exposure towild mumps virus. ■
AcknowledgementsThis review was conducted at the request of the Steer-ing Committee on Epidemiology and Field Research,with support from the WHO Global Programmefor Vaccines and Immunization. We thank A.M.Henao-Restrepo and J.-M. Olivé for their helpfulcomments.
Résumé
Les oreillons et le vaccin antiourlien : la situation dans le mondeLes oreillons sont une maladie infectieuse aiguë due àun paramyxovirus très proche des virus parainfluenza.En l’absence de vaccination, c’est une affection cou-rante dont l’incidence annuelle est élevée : en généralplus de 100 cas pour 100 000 habitants. La surveillanceà base communautaire donne de son côté un taux d’in-cidence de 2000 pour 100 000 – soit environ 10 foisplus de cas que n’en dénombre la notification passive.Des épidémies d’oreillons se produisent tous les 2 à5 ans.
Sous sa forme habituelle, la maladie se caracté-rise par une tuméfaction parotidienne avec atteinteassociée des autres glandes salivaires. Elle est le plussouvent bénigne mais peut se compliquer d’une mé-ningite aseptique dans 10% des cas. L’encéphalite estune complication moins fréquente mais plus grave etpeut entraîner la mort ou du moins une invalidité per-manente. Après la puberté, il peut se produire uneépididymo-orchite dans 25% des cas. Chez la femmeenceinte, la maladie provoque dans un quart des casun avortement spontané lorsqu’elle est contractée aucours du premier trimestre. Chez 4% des malades, onobserve une surdité passagère qui, chez un petit nom-bre d’entre eux, peut évoluer vers une perte auditiveimportante et définitive. Les pays qui ont inscrit la vac-cination contre les oreillons à leur programme nationalde vaccinations courantes et sont parvenus à assurerune bonne couverture, ont vu la morbidité ourliennedécliner rapidement. En outre, dans nombre d’entre eux,
les encéphalites et les surdités consécutives aux oreillonsont presque totalement disparu.
Selon les données communiquées à l’OMS jus-qu’en avril 1998, la vaccination antiourlienne fait par-tie des vaccinations de l’enfance dans 82 pays (38%).Selon le système de classification des pays adopté parles Nations Unies, la vaccination antiourlienne est pra-tiquée dans 23 pays développés sur 25 (92%), dans19 pays en transition économique sur 22 (86%) (prin-cipalement les nouveaux Etats indépendants del’ancienne Union soviétique) et dans 40 pays en déve-loppement sur 168 (24%).
Dans 52 pays, la vaccination comporte l’admi-nistration d’une seule dose de vaccin alors que dans 30autres elle en comporte deux.
Les pays qui envisagent d’introduire la vaccina-tion antiourlienne pour lutter contre la maladie, doi-vent évaluer la charge que cette maladie représente,définir l’âge de vaccination systématique et choisir lasouche vaccinale de virus vivant atténué à acquérir. Uneanalyse coût-avantages ne serait pas inutile à cet égard.Les pays qui pratiquent déjà la vaccination contre lesoreillons doivent contrôler la couverture vaccinale, met-tre en place une surveillance systématique des oreillonset faire une enquête chaque fois qu’une flambée seproduit. Là où l’on s’est fixé pour but d’éliminer la ma-ladie, il faut ajouter une seconde dose de vaccin chezl’enfant, sans perdre de vue que les oreillons peuventaussi frapper les adultes sensibles.
Mumps and mumps vaccine: a global review

12 Bulletin of the World Health Organization, 1999, 77 (1)
Research
Resumen
La parotiditis y la vacuna antiparotidítica: situación mundialasociados a la parotiditis han desaparecido casi porcompleto.
Según los datos notificados a la OMS hasta abrilde 1998, la vacuna contra la parotiditis se utilizasistemáticamente en los programas nacionales de in-munización de 82 países (38%). Según el sistema em-pleado por las Naciones Unidas para clasificar los países,utilizan la vacuna antiparotidítica 23 (92%) de 25 paí-ses desarrollados, 19 (86%) de 22 países con econo-mías en transición (principalmente los nuevos Estadosindependientes de la antigua Unión Soviética) y 40(24%) de 168 países en desarrollo.
En 52 países se administra una sola dosis de lavacuna, mientras que en los otros 30 se emplean dosdosis.
Los países interesados en implantar la vacuna-ción contra la parotiditis para combatir esa enferme-dad tendrán que evaluar la carga de morbilidad querepresenta, determinar la edad idónea para la vacuna-ción sistemática, y seleccionar la cepa de vacuna vivaatenuada que deba comprarse. Los análisis costo-be-neficio pueden ser de utilidad a ese efecto. Los paísesque ya utilizan la vacuna contra la parotiditis deberíanseguir de cerca la cobertura de inmunización y estable-cer mecanismos de vigilancia sistemática de la enfer-medad, incluida la investigación de los posibles brotes.Allí donde se haya fijado la meta de eliminar laparotiditis, los países habrán de añadir una segundadosis de vacuna para los niños, sin olvidar que la enfer-medad puede afectar con todo a adultos susceptibles.
La parotiditis, o paperas, es una enfermedad infecciosaaguda causada por un paramixovirus estrechamenterelacionado con el virus parainfluenza. Si no se vacunacontra ella, la parotiditis es una enfermedad común,con una alta incidencia anual, generalmente superior a100 casos por 100 000 habitantes. La vigilancia comu-nitaria ha revelado cifras de incidencia del orden de2000 casos por 100 000 habitantes, esto es, unas diezveces más que el número de casos notificados pasiva-mente. Cada 2-5 años se declaran epidemias deparotiditis.
La parotiditis clásica se caracteriza por una infla-mación de la glándula parótida y de otras glándulassalivales. Aunque suele ser benigna, hasta un 10% delos pacientes desarrollan meningitis aséptica. Una com-plicación menos frecuente, pero más grave, es la ence-falitis, que puede ser causa de muerte o de discapacidadpermanente. Además, un 25% de los hombres que con-traen la enfermedad tras la pubertad sufren epididimor-quitis. Entre las mujeres afectadas durante el primertrimestre de embarazo, una cuarta parte sufren abortoespontáneo. Aparece sordera transitoria en un 4% delos pacientes, una pequeña proporción de los cualesqueda aquejado permanentemente de pérdida deoído profunda. Los países que han incluido la vacunacontra la parotiditis en sus programas nacionales deinmunización sistemática y han logrado una alta co-bertura han mostrado un rápido descenso de lamorbilidad por la enfermedad. Por añadidura, en mu-chos de esos países los casos de encefalitis y sordera
References1. Baum SG, Litman N. Mumps virus. In: Mandell GL, Bennett
JE, Dolin R, eds. Principles and practice of infectious disease,4th edit. London, Churchill Livingston, 1995: 1496–1501.
2. Beard CM et al. The incidence and outcome of mumpsorchitis in Rochester, Minnesota, 1935 to 1974. Mayo Clinicproceedings, 1977, 52: 3–7.
3. Swerdlow AJ, Huttly SRA, Smith PG. Testicular cancer andantecedent diseases. British journal of cancer, 1987,55: 97–103.
4. Philip RN, Reinhard KR, Lackman DB. Observations on amumps epidemic in a “virgin” population. American journal ofhygiene, 1959, 69: 91–111.
5. Siegel M, Fuerst HT, Peress NS. Comparative fetalmortality in maternal virus diseases: a prospective study onrubella, measles, mumps, chicken pox and hepatitis. NewEngland journal of medicine, 1966, 274: 768–771.
6. Siegel M. Congenital malformations following chickenpox,measles, mumps and hepatitis: results of a cohort study.Journal of the American Medical Association, 1973,226: 1521–1524.
7. Falk WA et al. The epidemiology of mumps in southernAlberta, 1980–1982. American journal of epidemiology, 1989,130: 736–749.
8. Stratton KR, Howe CJ, Johnston RB, eds. Adverse eventsassociated with childhood vaccines: evidence bearing oncausality. Washington, DC, National Academy Press, 1994:155–159.
9. Bang HO, Bang J. Involvement of the central nervous systemin mumps. Acta medica scandinavica, 1943, 113: 487–505.
10. Grist NR et al. Diseases of infection, 2nd edit. Oxford, OxfordUniversity Press, 1993.
11. Bjorvatn B, Skoldenberg B. Mumps and its complicationsin Stockholm. British medical journal, 1979, 1: 788.
12. Russell RR, Donald JC. The neurological complications ofmumps. British medical journal, 1958, 2: 27–30.
13. Mumps surveillance, January 1972–June 1974. Atlanta, USA,Center for Disease Control, 1974 (DHEW Publication No. CDC75-8178).
14. Xu Y et al. Viral etiology of acute childhood encephalitis inBeijing diagnosed by analysis of single samples. Pediatricinfectious disease journal, 1996, 15: 1018–1024.
15. Vuori M, Lahikainen EA, Peltonen T. Perceptive deafnessin connection with mumps: a study of 298 servicemensuffering from mumps. Acta otolaryngology, 1962,55: 231–236.
16. Hall R, Richards H. Hearing loss due to mumps. Archives ofdisease in childhood, 1987, 62: 189–191.
17. Minja BM. Aetiology of deafness among children at theBuguruni School for the Deaf in Dar es Salaam, Tanzania.International journal of pediatric otorhinolaryngology, 1998,42: 225–231.
18. Utz JP, Houk VN, Alling DW. Clinical and laboratory studiesof mumps. IV. Viruria and abnormal renal function. NewEngland journal of medicine, 1964, 270: 1283–1286.
Bulletin of the World Health Organization, 1999, 77 (1) 13
19. Lin CY, Chen WP, Chiang H. Mumps associated withnephritis. Child nephrology and urology, 1990, 10: 68–71.
20. Rosenberg DH. Electrocardiographic changes in epidemicparotitis (mumps). Proceedings of the Society for ExperimentalBiology and Medicine, 1945, 58: 9–11.
21. Özkutlu S et al. Fatal mumps myocarditis. Japanese heartjournal, 1989, 30: 109–114.
22. Galbraith NS et al. Mumps surveillance in England andWales 1962–81. Lancet, 1984, 1: 91–94.
23. Hirsch A. Mumps (Parotitis epidemica s. polymorpha). In:Handbook of geographical and historical pathology, vol III.London, New Syndenham Society, 1886: 277–283.
24. Levitt LP et al. Mumps in a general population: a sero-epidemiologic study. American journal of diseases of children,1970, 120: 134–138.
25. Gordon JE, Kilham L. Ten years in the epidemiology ofmumps. American journal of medical science, 1949,218: 338–359.
26. Slater PE, Roitman M, Costin C. Mumps incidence inIsrael— impact of MMR vaccine. Public health reviews, 1991,18: 88–93.
27. Sato H, et al. Transfer of measles, mumps, and rubellaantibodies from mother to infant: its effect on measles,mumps, and rubella immunization. American journal ofdiseases of children, 1979, 133: 1240–1243.
28. Morgan-Capner P et al. Surveillance of antibody tomeasles, mumps, and rubella by age. British medical journal,1988, 297: 770–772.
29. Wagenvoort JHT et al. Epidemiology of mumps in theNetherlands. Journal of hygiene, 1980, 85: 313–326.
30. Seroepidemiology of measles, mumps and rubella, Singapore.Weekly epidemiological record, 1992, 67(31): 231–233.
31. Cox MJ et al. Seroepidemiological study of the transmissionof the mumps virus in St. Lucia, West Indies. Epidemiology andinfection, 1989, 102: 147–160.
32. Bakir TMF et al. Seroepidemiology of mumps, measles, andsubacute sclerosing panencephalitis in Saudi Arabia. Journalof tropical pediatrics, 1988, 34: 254–256.
33. Imbs D, Loza-Tulimowska M, Rudnicka H. [Occurrence ofantibodies against mumps in the population of Poland].Przeglad epidemiologiczny, 1984, 38: 361–368 (in Polish).
34. WHO Expert Committee on Biological Standardization. Forty-third report. Geneva, World Health Organization, 1994 (WHOTechnical Report Series No. 840).
35. Recommendations of the Immunization Practices AdvisoryCommittee. Measles, mumps, and rubella—vaccine use andstrategies for elimination of measles, rubella, and congenitalrubella syndrome and control of mumps. Morbidity andmortality weekly report, 1998, 47 (RR-8): 1–57.
36. Juntunen-Backman K et al. Safe immunization of allergicchildren against measles, mumps, and rubella. Americanjournal of diseases of children, 1987, 141: 1103–1105.
37. James JM et al. Safe administration of the measles vaccineto children allergic to eggs. New England journal of medicine,1995, 332: 1262–1266.
38. Kelso JM, Jones RT, Yunginger JW. Anaphylaxis tomeasles, mumps, and rubella vaccine mediated by IgE togelatin. Journal of allergy and clinical immunology, 1993,91: 867–872.
39. Kwittken PL, Rosen S, Sweinberg SK. MMR vaccine andneomycin allergy. American journal of diseases of children,1993, 147:128–129.
40. Buynak EB, Hilleman MR. Live attenuated mumps virusvaccine: 1. Vaccine development. Proceedings of the Societyfor Experimental Biology and Medicine, 1966, 123: 768–775.
41. Fahlgren K. Two doses of MMR vaccine—sufficient toeradicate measles, mumps and rubella? Scandinavian journalof social medicine, 1988, 16: 129–135.
42. Broliden K et al. Immunity to mumps before and after MMRvaccination at 12 years of age in the first generation offeredthe two–dose immunization programme. Vaccine, 1997,16: 323–327.
43. Davidkin I, Valle M, Julkunen I. Persistence of anti-mumpsvirus antibodies after a two-dose MMR vaccination: a nine-year follow-up. Vaccine, 1995, 13: 1617–1622.
44. Cochi SL, Wharton M, Plotkin SA. Mumps vaccine. In:Plotkin SA, Mortimer EA Jr, eds. Vaccines, 2nd edit.Philadelphia, PA, WB Saunders, 1994: 277–301.
45. Briss PA et al. Sustained transmission of mumps in a highlyvaccinated population: assessment of primary vaccine failureand waning vaccine–induced immunity. Journal of infectiousdiseases, 1994, 169: 77–82.
46. Hersh BS et al. Mumps outbreak in a highly vaccinatedpopulation. Journal of pediatrics, 1991, 119: 187–193.
47. Ehrenkranz NJ et al. Clinical evaluation of a new measles–mumps–rubella combined live virus vaccine in the DominicanRepublic. Bulletin of the World Health Organization, 1975,52: 81–85.
48. Black S et al. Risk of hospitalization because of asepticmeningitis after measles–mumps–rubella vaccination in one-to two-year-old children: an analysis of the Vaccine SafetyDatalink (VSD) Project. Pediatric infectious disease journal,1997, 16: 500–503.
49. Fescharek R et al. Measles–mumps vaccination in the FRG:an empirical analysis after 14 years of use. II. Tolerability andanalysis of spontaneously reported side-effects. Vaccine,1990, 8: 446–456.
50. Smorodintsev AA, Nasibov MN, Jakovleva NV.Experience with live rubella virus vaccine combined with livevaccines against measles and mumps. Bulletin of the WorldHealth Organization, 1970, 42: 283–289.
51. Unanov SS et al. [Results of studying a live mumps vaccinefrom strain L-3 manufactured by the Moscow ResearchInstitute of Viral Preparations: the epidemiologicaleffectiveness of the vaccine]. Voprosy Virusologii, 1977,1: 59–61 (in Russian).
52. Kraigher A. [Monitoring side-effects and adverse eventsfollowing immunization against measles and mumps in anational vaccination programme in Slovenia from 1982 to1986]. Dissertation, Medical Faculty, Zagreb, Croatia, 1990 (inSlovenian).
53. Cizman M et al. Aseptic meningitis after vaccination againstmeasles and mumps. Pediatric infectious disease journal,1989, 8: 302–308.
54. Beck M et al. Mumps vaccine L-Zagreb, prepared in chickfibroblasts: I. production and field trials. Journal of biologicalstandardization, 1989, 17: 85–90.
55. Bhargava I et al. Immunogenicity and reactogenicity ofindigenously produced MMR vaccine. Indian pediatrics, 1995,32: 983–988.
56. Tesovic G, Begovac J, Bace A. Aseptic meningitis aftermeasles, mumps, and rubella vaccine. Lancet, 1993,341: 1541.
57. Gluck R et al. Rubini, a new live attenuated mumps vaccinevirus strain for human diploid cells. Developments inbiological standardization, 1986, 65: 29–35.
58. Schwarzer S et al. Safety and characterization of theimmune response engendered by two combined measles,mumps and rubella vaccines. Vaccine, 1998, 16: 298–304.
59. Chamot E, et al. [Estimation of the efficacy of three strainsof mumps vaccine during an outbreak in Geneva State(Switzerland)]. Epidemiology and public health, 1998,46:100–107 (in French).
60. Paccaud MF et al. [Two mumps outbreaks in retrospect].Sozial- und Präventivmedizin, 1995, 40: 72–79 (in German).
61. Toscani L et al. Comparaison de l’efficacité de différentessouches de vaccin ourlien: une enquête en milieu scolaire.Sozial- und Präventivmedizin, 1996, 41:1–7.
Mumps and mumps vaccine: a global review

14 Bulletin of the World Health Organization, 1999, 77 (1)
Research
62. Benevento and Compobasso Pediatricians Networkfor the Control of Vaccine-Preventable Diseases. Fieldevaluation of the clinical effectiveness of vaccines againstpertussis, measles, rubella and mumps. Vaccine, 1998,16: 818–822.
63. Dias JA et al. Mumps epidemic in Portugal despite highvaccine coverage— preliminary report. Eurosurveillance,1996, 1: 25–28.
64. Vesikari T et al. Evaluation in young children of the UrabeAm 9 strain of live attenuated mumps vaccine in comparisonwith the Jeryl Lynn strain. Acta paediatrica scandinavica,1983, 72: 37–40.
65. Forleo-Neto E et al. Seroconversion of a trivalent measles,mumps, and rubella vaccine in children aged 9 and 15months. Vaccine, 1997, 15: 1898–1901.
66. Schoub BD et al. Measles, mumps and rubella immunizationat nine months in a developing country. Pediatric infectiousdisease journal, 1990, 9: 263–267.
67. Singh R et al. Immune response to measles, mumps &rubella vaccine at 9, 12 & 15 months of age. Indian journal ofmedical research, 1994, 100: 155–159.
68. Huang L-M et al. Effect of monovalent measles and trivalentmeasles–mumps–rubella vaccines at various ages andconcurrent administration with hepatitis B vaccine. Pediatricinfectious disease journal, 1990, 9: 461–465.
69. Miller E et al. Antibodies to measles, mumps and rubella inUK children 4 years after vaccination with different MMRvaccines. Vaccine, 1995, 13: 799–802.
70. Boulianne N et al. Measles, mumps, and rubella antibodiesin children 5–6 years after immunization: effect of vaccinetype and age of vaccination. Vaccine, 1995, 13: 1611–1616.
71. Brown EG, Dimock K, Wright KE. The Urabe AM9 mumpsvaccine is a mixture of viruses differing at amino acid 335 ofthe hemagglutinin–neuraminidase gene with one formassociated with disease. Journal of infectious diseases, 1996,174: 619–622.
72. Furesz J, Contreras G. Vaccine–related mumps meningitis—Canada. Canadian diseases weekly report, 1990,16(50): 253–254.
73. Miller E et al. Risk of aseptic meningitis after measles,mumps, and rubella vaccine in UK children. Lancet, 1993,341: 979–982.
74. Sugiura A, Yamada A. Aseptic meningitis as a complicationof mumps vaccination. Pediatric infectious disease journal,1991, 10: 209–213.
75. Ueda K et al. Aseptic meningitis caused by measles–mumps–rubella vaccine in Japan. Lancet, 1995, 346: 701–702.
76. Robertson SE et al. Control of rubella and congenitalrubella syndrome (CRS) in developing countries, part 2:vaccination against rubella. Bulletin of the World HealthOrganization, 1997, 75: 69–80.
77. WHO Division of Health Situation and Trend Assessment.Demographic data for health situation assessment andprojections. Geneva, World Health Organization, 1996.
78. De Serres G et al. Epidemiology of mumps in Quebec,1970–1995. Canada communicable disease report, 1997,23(2): 1–4.
79. van Loon FPL et al. Mumps surveillance—United States,1988–1993. Morbidity and mortality weekly report, 1995,44, SS-3, 1–14.
80. WHO Regional Office for Europe. Operational targets for EPIdiseases. Unpublished document EUR/ICP/CMDS 01 01 14Rev.1. Copenhagen, World Health Organization, 1996.
81. Health for all database. Copenhagen, WHO Regional Office forEurope, 1998.
82. Bakasun V. Mumps in the region of Rijeka, Croatia. Europeanjournal of epidemiology, 1997, 13: 117–119.
83. Gay N et al. Mumps surveillance in England and Walessupports introduction of a two dose vaccination schedule.Communicable disease report, 1997, 7: R21–R26.
84. Peltola H et al. The elimination of indigenous measles,mumps, and rubella from Finland by a 1-year, two-dosevaccination program. New England journal of medicine, 1994,331: 1397–1402.
85. Koskiniemi M, Vaheri A. Effect of measles, mumps, rubellavaccination on pattern of encephalitis in children. Lancet,1989, 1: 31–34.
86. Darin N, Hanner P, Thiringer K. Changes in prevalence,aetiology, age at detection, and associated disabilities inpreschool children with hearing impairment born in Göteborg.Developmental medicine and child neurology, 1997, 39: 797–802.
87. Topal B, Kanra G, Ceyhan M. Serological evaluation of 52children immunized with the combined measles, mumps andrubella vaccine. Turkish journal of pediatrics, 1991, 33: 13–18.
88. Expanded Programme on Immunization. Framework forevaluating a vaccine for the EPI. Unpublished document WHO/EPI/GEN/93.5. Available upon request from Director, GlobalProgramme for Vaccines and Immunization, World HealthOrganization, 1211 Geneva 27, Switzerland.
89. Meningitis associated with measles–mumps–rubella vaccines.Weekly epidemiological record, 1992, 67(41) : 301–302; and1992, 67(51/52): 387.
90. Wiedermann G, Ambrosch F. Cost–benefit calculations ofvaccinations against measles and mumps in Austria.Developments in biological standardization, 1978,43: 273–277.
91. Berger SA, Ginsberg GM, Slater PE. Cost–benefit analysisof routine mumps and rubella vaccination for Israeli infants.Israel journal of medical sciences, 1990, 26: 74–80.

Bulletin of the World Health Organization, 1999, 77 (1) 15
Diagnosing anaemia in pregnancy in rural clinics:assessing the potential of the HaemoglobinColour ScaleN.R. van den Broek,1 C. Ntonya,2 E. Mhango,3 & S.A. White4
© World Health Organization 1999
1 Wellcome Trust Centre for Research, Department of Obstetricsand Gynaecology, College of Medicine, PO Box 30096, Blantyre 3,Malawi. Requests for reprints should be sent to this author.2 Field Research Nurse, Wellcome Trust, Blantyre, Malawi.3 Laboratory Technician, Wellcome Trust, Blantyre, Malawi.4 Lecturer in Statistics, University of Malawi, Blantyre, Malawi.
Anaemia in pregnancy is a common and severe problem in many developing countries. Because of lack of re-sources and staff motivation, screening for anaemia is often solely by clinical examination of the conjunctiva or isnot carried out at all. A new colour scale for the estimation of haemoglobin concentration has been developed byWHO. The present study compares the results obtained using the new colour scale on 729 women visiting ruralantenatal clinics in Malawi with those obtained by HemoCue haemoglobinometer and electronic Coulter Counterand with the assessment of anaemia by clinical examination of the conjunctiva. Sensitivity using the colour scalewas consistently better than for conjunctival inspection alone and interobserver agreement and agreement withCoulter Counter measurements was good. The Haemoglobin Colour Scale is simple to use, well accepted, cheapand gives immediate results. It shows considerable potential for use in screening for anaemia in antenatal clinicsin settings where resources are limited.
Voir page 20 le résumé en français. En la página 20 figura un resumen en español.
IntroductionIn most developing countries anaemia in pregnancymakes an important contribution to maternal mor-tality and morbidity (1, 2). A haemoglobin concen-tration ([Hb]) of < 11.0 g/dl is commonly taken asindicative of anaemia in pregnancy (3).
Successful management of anaemia in preg-nancy depends on accurate and acceptable methodsof detecting anaemia, assessing its severity and moni-toring response to treatment (4). In women withmild-to-moderate anaemia, timely treatment is likelyto prevent the development of more severe anaemiaand therefore reduce the need for blood transfusionwith its associated risks. Prevention of severe anae-mia also has more direct benefits for both motherand child.
In developed countries, where the prevalenceof anaemia is below 20%, an accepted standard ofpractice is that all women have at least one measure-ment of [Hb] during the course of pregnancy. Thisis usually performed by electronic counter. In devel-oping countries with reported prevalences of 40–70% these methods are often not available, even atthe tertiary level. Screening for anaemia may not becarried out at all, or may be limited to inspection ofthe conjunctiva for the presence of pallor. There areno published reports of the accuracy of screeningfor anaemia using clinical inspection of conjunctiva
alone in pregnant women in the rural antenatal clinicsetting. Studies in children (5) and healthy ambula-tory adults (6) have demonstrated poor accuracy.Even when used in combination with a conjuncti-val or anaemia recognition card, sensitivity remainslow except when anaemia is severe (7, 8). There is aneed for a simple, cheap but accurate method forthe estimation of haemoglobin concentration.
A new colour scale for assessing [Hb] has re-cently been developed by WHO (9). We have con-ducted a study to determine the value of thistechnique as a screening method for anaemia in ru-ral antenatal clinics when used by local staff. Theresults are compared with values estimated for thesame individuals by clinical examination of the con-junctiva and by measurements of [Hb] using a bat-tery-operated HemoCue machine. As a standard forcomparison, [Hb] measurements were obtained onvenous blood samples using a Coulter Counter(Onyx, Coulter Counters, Johannesburg, SouthAfrica).
Materials and methodsA total of 44 nurse–midwives from five different sites(three rural hospitals and two health centres) insouthern Malawi each attended a one-day trainingsession on the use of the HemoCue machine andthe Haemoglobin Colour Scale. Training was givenaccording to a standard format. As all staff were al-ready familiar with conjunctival assessment no ex-tra training was given in this method. All five siteswere subsequently revisited three to four times eachover a period of 3 months. At each antenatal clinic,three nurse–midwives independently assessed
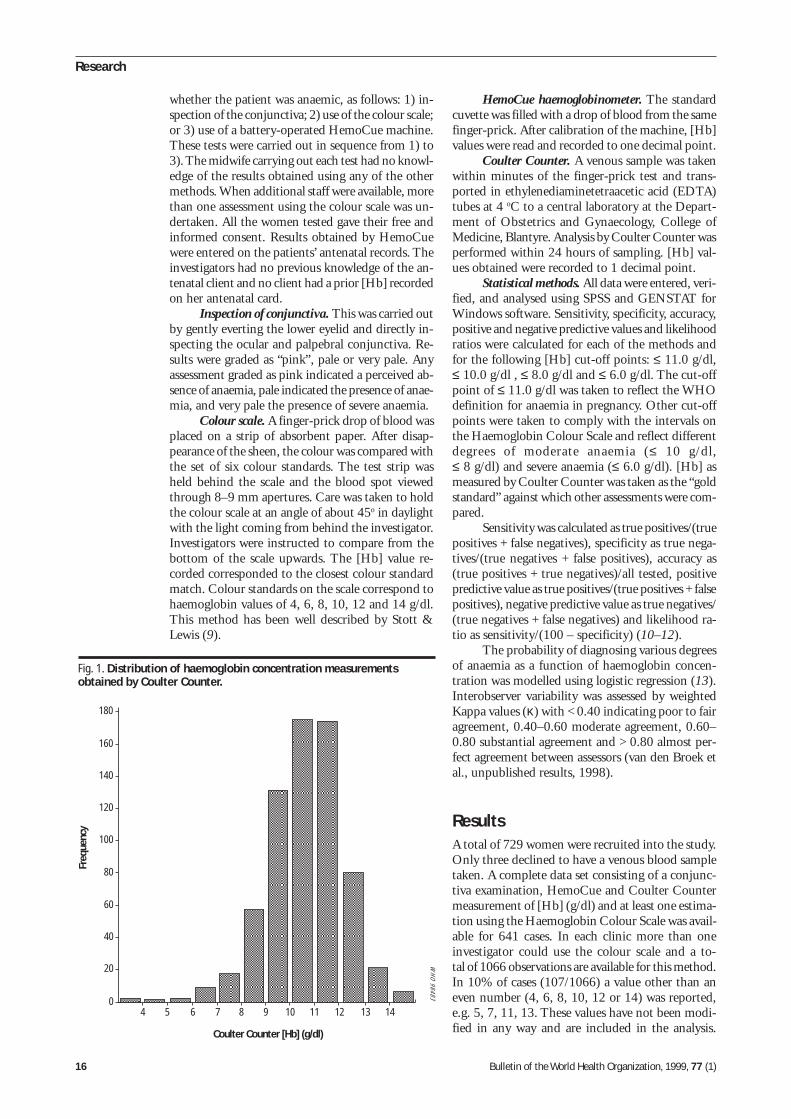
16 Bulletin of the World Health Organization, 1999, 77 (1)
Research
whether the patient was anaemic, as follows: 1) in-spection of the conjunctiva; 2) use of the colour scale;or 3) use of a battery-operated HemoCue machine.These tests were carried out in sequence from 1) to3). The midwife carrying out each test had no knowl-edge of the results obtained using any of the othermethods. When additional staff were available, morethan one assessment using the colour scale was un-dertaken. All the women tested gave their free andinformed consent. Results obtained by HemoCuewere entered on the patients’ antenatal records. Theinvestigators had no previous knowledge of the an-tenatal client and no client had a prior [Hb] recordedon her antenatal card.
Inspection of conjunctiva. This was carried outby gently everting the lower eyelid and directly in-specting the ocular and palpebral conjunctiva. Re-sults were graded as “pink”, pale or very pale. Anyassessment graded as pink indicated a perceived ab-sence of anaemia, pale indicated the presence of anae-mia, and very pale the presence of severe anaemia.
Colour scale. A finger-prick drop of blood wasplaced on a strip of absorbent paper. After disap-pearance of the sheen, the colour was compared withthe set of six colour standards. The test strip washeld behind the scale and the blood spot viewedthrough 8–9 mm apertures. Care was taken to holdthe colour scale at an angle of about 45o in daylightwith the light coming from behind the investigator.Investigators were instructed to compare from thebottom of the scale upwards. The [Hb] value re-corded corresponded to the closest colour standardmatch. Colour standards on the scale correspond tohaemoglobin values of 4, 6, 8, 10, 12 and 14 g/dl.This method has been well described by Stott &Lewis (9).
HemoCue haemoglobinometer. The standardcuvette was filled with a drop of blood from the samefinger-prick. After calibration of the machine, [Hb]values were read and recorded to one decimal point.
Coulter Counter. A venous sample was takenwithin minutes of the finger-prick test and trans-ported in ethylenediaminetetraacetic acid (EDTA)tubes at 4 oC to a central laboratory at the Depart-ment of Obstetrics and Gynaecology, College ofMedicine, Blantyre. Analysis by Coulter Counter wasperformed within 24 hours of sampling. [Hb] val-ues obtained were recorded to 1 decimal point.
Statistical methods. All data were entered, veri-fied, and analysed using SPSS and GENSTAT forWindows software. Sensitivity, specificity, accuracy,positive and negative predictive values and likelihoodratios were calculated for each of the methods andfor the following [Hb] cut-off points: ≤ 11.0 g/dl,≤ 10.0 g/dl , ≤ 8.0 g/dl and ≤ 6.0 g/dl. The cut-offpoint of ≤ 11.0 g/dl was taken to reflect the WHOdefinition for anaemia in pregnancy. Other cut-offpoints were taken to comply with the intervals onthe Haemoglobin Colour Scale and reflect differentdegrees of moderate anaemia (≤ 10 g/dl,≤ 8 g/dl) and severe anaemia (≤ 6.0 g/dl). [Hb] asmeasured by Coulter Counter was taken as the “goldstandard” against which other assessments were com-pared.
Sensitivity was calculated as true positives/(truepositives + false negatives), specificity as true nega-tives/(true negatives + false positives), accuracy as(true positives + true negatives)/all tested, positivepredictive value as true positives/(true positives + falsepositives), negative predictive value as true negatives/(true negatives + false negatives) and likelihood ra-tio as sensitivity/(100 – specificity) (10–12).
The probability of diagnosing various degreesof anaemia as a function of haemoglobin concen-tration was modelled using logistic regression (13).Interobserver variability was assessed by weightedKappa values (κ) with < 0.40 indicating poor to fairagreement, 0.40–0.60 moderate agreement, 0.60–0.80 substantial agreement and > 0.80 almost per-fect agreement between assessors (van den Broek etal., unpublished results, 1998).
ResultsA total of 729 women were recruited into the study.Only three declined to have a venous blood sampletaken. A complete data set consisting of a conjunc-tiva examination, HemoCue and Coulter Countermeasurement of [Hb] (g/dl) and at least one estima-tion using the Haemoglobin Colour Scale was avail-able for 641 cases. In each clinic more than oneinvestigator could use the colour scale and a to-tal of 1066 observations are available for this method.In 10% of cases (107/1066) a value other than aneven number (4, 6, 8, 10, 12 or 14) was reported,e.g. 5, 7, 11, 13. These values have not been modi-fied in any way and are included in the analysis.
Fig. 1. Distribution of haemoglobin concentration measurementsobtained by Coulter Counter.
Coulter Counter [Hb] (g/dl)
Freq
uenc
y
WH
O 98483
180
4
160
140
120
100
80
60
40
20
05 6 7 8 9 10 11 12 13 14
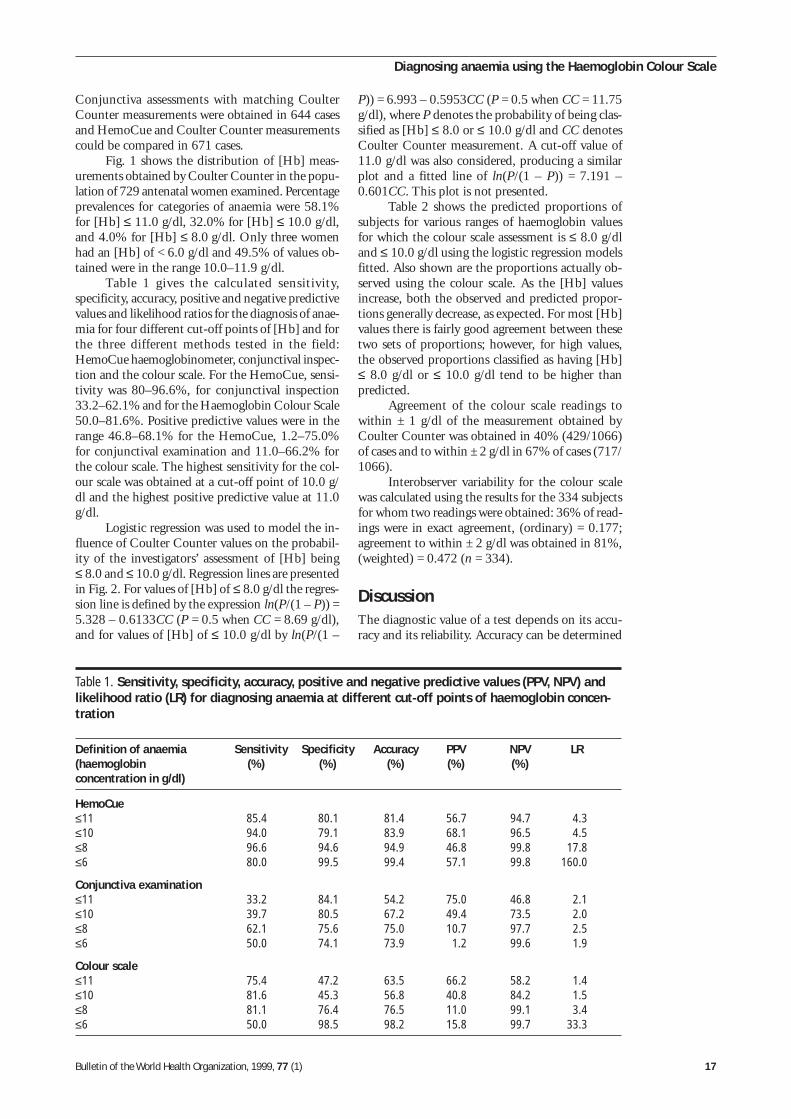
Bulletin of the World Health Organization, 1999, 77 (1) 17
Conjunctiva assessments with matching CoulterCounter measurements were obtained in 644 casesand HemoCue and Coulter Counter measurementscould be compared in 671 cases.
Fig. 1 shows the distribution of [Hb] meas-urements obtained by Coulter Counter in the popu-lation of 729 antenatal women examined. Percentageprevalences for categories of anaemia were 58.1%for [Hb] ≤ 11.0 g/dl, 32.0% for [Hb] ≤ 10.0 g/dl,and 4.0% for [Hb] ≤ 8.0 g/dl. Only three womenhad an [Hb] of < 6.0 g/dl and 49.5% of values ob-tained were in the range 10.0–11.9 g/dl.
Table 1 gives the calculated sensitivity,specificity, accuracy, positive and negative predictivevalues and likelihood ratios for the diagnosis of anae-mia for four different cut-off points of [Hb] and forthe three different methods tested in the field:HemoCue haemoglobinometer, conjunctival inspec-tion and the colour scale. For the HemoCue, sensi-tivity was 80–96.6%, for conjunctival inspection33.2–62.1% and for the Haemoglobin Colour Scale50.0–81.6%. Positive predictive values were in therange 46.8–68.1% for the HemoCue, 1.2–75.0%for conjunctival examination and 11.0–66.2% forthe colour scale. The highest sensitivity for the col-our scale was obtained at a cut-off point of 10.0 g/dl and the highest positive predictive value at 11.0g/dl.
Logistic regression was used to model the in-fluence of Coulter Counter values on the probabil-ity of the investigators’ assessment of [Hb] being≤ 8.0 and ≤ 10.0 g/dl. Regression lines are presentedin Fig. 2. For values of [Hb] of ≤ 8.0 g/dl the regres-sion line is defined by the expression ln(P/(1 – P)) =5.328 – 0.6133CC (P = 0.5 when CC = 8.69 g/dl),and for values of [Hb] of ≤ 10.0 g/dl by ln(P/(1 –
P)) = 6.993 – 0.5953CC (P = 0.5 when CC = 11.75g/dl), where P denotes the probability of being clas-sified as [Hb] ≤ 8.0 or ≤ 10.0 g/dl and CC denotesCoulter Counter measurement. A cut-off value of11.0 g/dl was also considered, producing a similarplot and a fitted line of ln(P/(1 – P)) = 7.191 –0.601CC. This plot is not presented.
Table 2 shows the predicted proportions ofsubjects for various ranges of haemoglobin valuesfor which the colour scale assessment is ≤ 8.0 g/dland ≤ 10.0 g/dl using the logistic regression modelsfitted. Also shown are the proportions actually ob-served using the colour scale. As the [Hb] valuesincrease, both the observed and predicted propor-tions generally decrease, as expected. For most [Hb]values there is fairly good agreement between thesetwo sets of proportions; however, for high values,the observed proportions classified as having [Hb]≤ 8.0 g/dl or ≤ 10.0 g/dl tend to be higher thanpredicted.
Agreement of the colour scale readings towithin ± 1 g/dl of the measurement obtained byCoulter Counter was obtained in 40% (429/1066)of cases and to within ± 2 g/dl in 67% of cases (717/1066).
Interobserver variability for the colour scalewas calculated using the results for the 334 subjectsfor whom two readings were obtained: 36% of read-ings were in exact agreement, (ordinary) = 0.177;agreement to within ± 2 g/dl was obtained in 81%,(weighted) = 0.472 (n = 334).
DiscussionThe diagnostic value of a test depends on its accu-racy and its reliability. Accuracy can be determined
Table 1. Sensitivity, specificity, accuracy, positive and negative predictive values (PPV, NPV) andlikelihood ratio (LR) for diagnosing anaemia at different cut-off points of haemoglobin concen-tration
Definition of anaemia Sensitivity Specificity Accuracy PPV NPV LR(haemoglobin (%) (%) (%) (%) (%)concentration in g/dl)
HemoCue≤11 85.4 80.1 81.4 56.7 94.7 4.3≤10 94.0 79.1 83.9 68.1 96.5 4.5≤8 96.6 94.6 94.9 46.8 99.8 17.8≤6 80.0 99.5 99.4 57.1 99.8 160.0
Conjunctiva examination≤11 33.2 84.1 54.2 75.0 46.8 2.1≤10 39.7 80.5 67.2 49.4 73.5 2.0≤8 62.1 75.6 75.0 10.7 97.7 2.5≤6 50.0 74.1 73.9 1.2 99.6 1.9
Colour scale≤11 75.4 47.2 63.5 66.2 58.2 1.4≤10 81.6 45.3 56.8 40.8 84.2 1.5≤8 81.1 76.4 76.5 11.0 99.1 3.4≤6 50.0 98.5 98.2 15.8 99.7 33.3
Diagnosing anaemia using the Haemoglobin Colour Scale
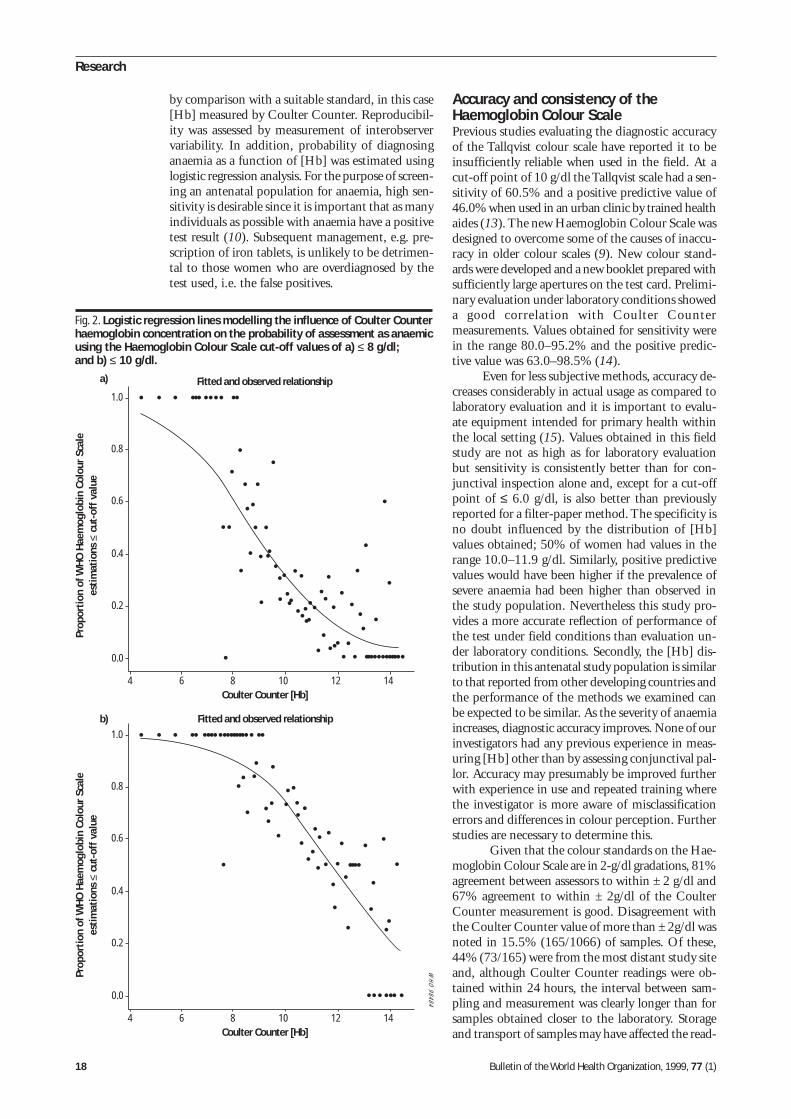
18 Bulletin of the World Health Organization, 1999, 77 (1)
Research
by comparison with a suitable standard, in this case[Hb] measured by Coulter Counter. Reproducibil-ity was assessed by measurement of interobservervariability. In addition, probability of diagnosinganaemia as a function of [Hb] was estimated usinglogistic regression analysis. For the purpose of screen-ing an antenatal population for anaemia, high sen-sitivity is desirable since it is important that as manyindividuals as possible with anaemia have a positivetest result (10). Subsequent management, e.g. pre-scription of iron tablets, is unlikely to be detrimen-tal to those women who are overdiagnosed by thetest used, i.e. the false positives.
Accuracy and consistency of theHaemoglobin Colour ScalePrevious studies evaluating the diagnostic accuracyof the Tallqvist colour scale have reported it to beinsufficiently reliable when used in the field. At acut-off point of 10 g/dl the Tallqvist scale had a sen-sitivity of 60.5% and a positive predictive value of46.0% when used in an urban clinic by trained healthaides (13). The new Haemoglobin Colour Scale wasdesigned to overcome some of the causes of inaccu-racy in older colour scales (9). New colour stand-ards were developed and a new booklet prepared withsufficiently large apertures on the test card. Prelimi-nary evaluation under laboratory conditions showeda good correlation with Coulter Countermeasurements. Values obtained for sensitivity werein the range 80.0–95.2% and the positive predic-tive value was 63.0–98.5% (14).
Even for less subjective methods, accuracy de-creases considerably in actual usage as compared tolaboratory evaluation and it is important to evalu-ate equipment intended for primary health withinthe local setting (15). Values obtained in this fieldstudy are not as high as for laboratory evaluationbut sensitivity is consistently better than for con-junctival inspection alone and, except for a cut-offpoint of ≤ 6.0 g/dl, is also better than previouslyreported for a filter-paper method. The specificity isno doubt influenced by the distribution of [Hb]values obtained; 50% of women had values in therange 10.0–11.9 g/dl. Similarly, positive predictivevalues would have been higher if the prevalence ofsevere anaemia had been higher than observed inthe study population. Nevertheless this study pro-vides a more accurate reflection of performance ofthe test under field conditions than evaluation un-der laboratory conditions. Secondly, the [Hb] dis-tribution in this antenatal study population is similarto that reported from other developing countries andthe performance of the methods we examined canbe expected to be similar. As the severity of anaemiaincreases, diagnostic accuracy improves. None of ourinvestigators had any previous experience in meas-uring [Hb] other than by assessing conjunctival pal-lor. Accuracy may presumably be improved furtherwith experience in use and repeated training wherethe investigator is more aware of misclassificationerrors and differences in colour perception. Furtherstudies are necessary to determine this.
Given that the colour standards on the Hae-moglobin Colour Scale are in 2-g/dl gradations, 81%agreement between assessors to within ± 2 g/dl and67% agreement to within ± 2g/dl of the CoulterCounter measurement is good. Disagreement withthe Coulter Counter value of more than ± 2g/dl wasnoted in 15.5% (165/1066) of samples. Of these,44% (73/165) were from the most distant study siteand, although Coulter Counter readings were ob-tained within 24 hours, the interval between sam-pling and measurement was clearly longer than forsamples obtained closer to the laboratory. Storageand transport of samples may have affected the read-
Fig. 2. Logistic regression lines modelling the influence of Coulter Counterhaemoglobin concentration on the probability of assessment as anaemicusing the Haemoglobin Colour Scale cut-off values of a) ≤ 8 g/dl;and b) ≤ 10 g/dl.
Prop
orti
on o
f WH
O H
aem
oglo
bin
Colo
ur S
cale
esti
mat
ions
≤ c
ut-o
ff v
alue
a)
1.0
Coulter Counter [Hb]
0.8
0.6
0.4
0.2
0.0
4 6 8 10 12 14
Fitted and observed relationship
WH
O 98484
Prop
orti
on o
f WH
O H
aem
oglo
bin
Colo
ur S
cale
esti
mat
ions
≤ c
ut-o
ff v
alue
b)1.0
Coulter Counter [Hb]
0.8
0.6
0.4
0.2
0.0
4 6 8 10 12 14
Fitted and observed relationship

Bulletin of the World Health Organization, 1999, 77 (1) 19
ings. To reflect field conditions, we have not excludedthese values from our analysis, but had we done sothe accuracy of the scale could be expected to bebetter than indicated here.
Other simple screening methodsAs mentioned earlier, accuracy is low when anaemiais diagnosed by conjunctival inspection alone. Forunder-5-year-olds, a definite diagnosis of anaemiawas correctly made in 5–42% of cases and a diagno-sis of probable anaemia was correctly made in 24–64% of cases by conjunctival inspection (5). Whenpalm, tongue and nailbed were examined in addi-tion, accuracy improved. However, in this paediat-ric study a low [Hb] cut-off point of 8 g/dl was usedto define anaemia. Similarly, Gjorup et al. obtaineda sensitivity of 27–44% at cut-off points of 10.0 g/dl and 11.0 g/dl, and the expected probability ofdetecting anaemia did not exceed 0.75 even wheninspection was carried out by trained physicians (12).Substantial interobserver variability has also beenreported (6, 12, 16, 17). In the current study, sensi-tivity was 33.2% and 39.7% for [Hb] values of≤ 11.0 and ≤ 10.0 g/dl, respectively. Values obtainedwere better for the lower range of [Hb] values butdid not exceed 62.1%. Conjunctival inspection inpregnant women may be particularly inaccurate as aresult of increased peripheral vasodilatation. It maybe possible to improve the accuracy of screening foranaemia using conjunctival inspection in pregnantwomen by improved training and assessment of morethan one physical sign of pallor. However, in ourstudy no extra training in this method was given tothe investigators.
The HemoCue method had excellent sensi-tivity and specificity at all cut-off levels of [Hb]tested. Values obtained were comparable with thosepreviously reported for field studies (88.5% sensi-tivity and 77.6% specificity) (15). It must be notedthat a small bias is possible when the results of fin-ger-prick samples (HemoCue) are compared withthose of a venous blood sample (Coulter Counter).The HemoCue method was well liked by health careworkers but in practice it is still too expensive foruse in the primary health care setting in most devel-oping countries.
Recently the use of the copper sulfate (18, 19)and undiluted Lovibond (20, 21) methods has beenre-evaluated and recommended for screening pur-poses. The values obtained for sensitivity with theHaemoglobin Colour Scale (50–81.6%) are com-parable to those reported for these methods (75.8–87.5% and 87.4%, respectively), both of whichrequire standard solutions and/or standardizedequipment.
Operational and logistic appealThe Haemoglobin Colour Scale is simple to use,cheap, and gives an immediate result. Health careworkers appreciated having a method which gavean actual measurement of [Hb] as opposed to in-
spection of conjunctiva with categories of pink, paleor very pale only (van den Broek et al., unpublishedresults, 1998). Patients were curious to see their “col-our of blood” a phrase which is commonly used toexplain anaemia in developing countries. Hencecompliance with the test was excellent. A better un-derstanding of the concept of anaemia by pregnantwomen is likely to lead to improved compliance withprophylactic or therapeutic measures, such as irontablets.
Potential clinical usefulnessScreening for anaemia in pregnancy is useful for avariety of reasons. It may be helpful to collect base-line data on prevalence and severity in a given popu-lation, and to assess the effects of supplementationwith iron tablets, antimalarial prophylactics orantihelminthic treatment. At primary care level, es-timation of [Hb] can help decide whether referral isnecessary for more detailed investigation and treat-ment.
The value of each screening test within a spe-cific setting depends on the necessity of performingan assessment in the absence of a more accuratemethod and on cost–benefit considerations. Anymethod of screening for anaemia at primary healthcare level in a developing country should be accept-able to both patients and staff, simple to operate,require a minimum of materials, be cheap and giveimmediate accurate results. In situations with lim-ited resources and poor technical support, a simplescreening tool is likely to perform better than so-phisticated methods that depend on correct dilu-tion and preparation of standards or on power supply.From this perspective, the Haemoglobin ColourScale has considerable potential as an exciting newtool for use in antenatal clinics. Further field testingis necessary to evaluate whether use of the colourscale can permit health staff to detect the effect oftherapy, be similarly successful in recognition andmanagement of anaemia in other patient groups, andallow the identification of potential blood donors. ■
Diagnosing anaemia using the Haemoglobin Colour Scale
Table 2. Observed and predicted proportions of Coulter Counterreadings (n = 1066) correctly classified as haemoglobinconcentrations [Hb] of ≤8.0 g/dl and ≤10.0 g/dl by the Haemo-globin Colour Scale (logistic regression analysis)
Coulter Counter Colour scale ≤8.0 g/dl Colour scale ≤10.0 g/dl
[Hb] (g/dl) n Predicted Observed Predicted Observed
3.5–4.4 2 0.947 1.000 0.990 1.0004.5–5.4 2 0.906 1.000 0.982 1.0005.5–6.4 4 0.839 1.000 0.968 1.0006.5–7.4 11 0.738 0.909 0.944 1.0007.5–8.4 50 0.604 0.700 0.903 0.9008.5–9.4 130 0.452 0.438 0.837 0.8319.5–10.4 256 0.309 0.273 0.739 0.750
10.5–11.4 291 0.195 0.165 0.609 0.58811.5–12.4 234 0.116 0.128 0.462 0.46212.5–13.4 55 0.066 0.182 0.322 0.43613.5–14.4 31 0.037 0.161 0.207 0.226
20 Bulletin of the World Health Organization, 1999, 77 (1)
Research
AcknowledgementsWe would like to thank Dr S.M. Lewis and Dr G.J.Stott for preparation of a training protocol for theColour Scale, Dr E.A. Letsky for help in preparingthe study, and Professor M. Molyneux for help with
the manuscript. This study was made possible by agrant from the Division of Reproductive Health,World Health Organization, Geneva. Dr van denBroek is a Wellcome Trust Research Fellow.
L’anémie chez la femme enceinte est courante dans denombreux pays en développement. Au niveau des soinsde santé primaires, le dépistage de l’anémie, quand ilest pratiqué, se limite souvent à l’examen clinique de laconjonctive. L’OMS a mis au point une nouvelle échellecolorée pour déterminer l’hémoglobinémie (échelle decoloration pour le dosage de l’hémoglobine). Nousavons formé à son emploi les agents de santé des dis-pensaires ruraux de soins prénatals dans le sud duMalawi et effectué une étude de terrain auprès de 729femmes venues dans ces dispensaires pour évaluer saprécision diagnostique, sa fiabilité et son acceptabilitéen tant que méthode de dépistage de l’anémie danscette population. Les dosages de l’hémoglobine parl’échelle de coloration ont été comparés aux valeursobtenues au moyen d’un hémoglobinomètre à pilesHemoCue et à l’évaluation de l’anémie par l’examenclinique de la conjonctive. Pour chaque sujet, une me-sure au Coulter Counter a été effectuée sur un prélève-ment de sang veineux et utilisée comme étalon aux finsde comparaison. Les résultats sont présentés pour les
seuils [Hb] < 11,0 g/dl, < 10,0 g/dl, < 8,0 g/dl et < 6,0g/dl. Pour chaque seuil, la sensibilité était systémati-quement plus élevée pour l’échelle de coloration(50,0%–81,6%) que pour l’examen clinique de la con-jonctive (33,2%–62,1%). L’influence de la distributiondes taux de [Hb] dans la population étudiée sur les va-leurs diagnostiques est examinée. On a calculé par ré-gression logistique les proportions observées et prévuesdes mesures obtenues par le Coulter Counter, classéesen fonction des seuils [Hb] < 8,0 g/dl et < 10,0 g/dl,ainsi que l’influence de [Hb] sur la probabilité d’un dia-gnostic d’anémie. Dans 67% des cas, les mesures ob-tenues au moyen de l’échelle colorée de l’OMScorrespondaient à + 2 g/dl près à la mesure enregis-trée par le Coulter Counter. L’intérêt clinique et logisti-que de la nouvelle échelle de coloration est examiné.L’échelle de coloration est simple à utiliser, bien accep-tée, bon marché et elle donne des résultats immédiats.Elle paraît très prometteuse pour le dépistage de l’ané-mie dans les dispensaires prénatals là où les ressourcessont limitées.
Resumen
Diagnóstico de la anemia gestacional en los dispensarios rurales: evaluacióndel potencial de la nueva escala cromática para la estimación de la hemoglobinaLa anemia durante el embarazo es un problema comúnen muchos países en desarrollo. A nivel de la atenciónprimaria, la detección de la anemia, cuando se hace,suele consistir en la inspección clínica de la conjuntivasolamente. La OMS ha ideado una nueva escalacromática para estimar la concentración de hemoglo-bina en la sangre ([Hb]), cuyo uso se ha enseñado a losagentes de salud de los dispensarios rurales de aten-ción prenatal del sur de Malawi. Para determinar sugrado de exactitud de diagnóstico, fiabilidad yaceptabilidad como método de detección de la anemiase hizo un estudio sobre el terreno con 729 mujeres deesos dispensarios. Las estimaciones de [Hb] con la es-cala cromática se compararon con las mediciones ob-tenidas con el hemoglobinómetro HemoCue y con losresultados del examen clínico de la conjuntiva. A partirde una muestra de sangre venosa de las pacientes seobtuvieron valores de referencia con el contador deCoulter para fines de comparación. Los resultados sepresentan para valores límite de [Hb] de < 11,0, < 10,0,< 8,0 y < 6,0 g/dl. Respecto de cada valor límite, la
sensibilidad fue sistemáticamente mayor en el caso dela escala cromática (50,0%–81,6%) que en el del exa-men clínico de la conjuntiva (33,2%–62,1%). El efectoque la distribución de los valores de [Hb] en la pobla-ción estudiada tiene sobre los valores de diagnósticoobtenidos es objeto de discusión. Se utilizó la regresiónlogística para calcular las proporciones observadas ypredichas de los datos obtenidos con el contador deCoulter clasificados correctamente como [Hb] < 8,0 y< 10,0 g/dl, así como la influencia de la [Hb] sobre laprobabilidad de que se diagnostique anemia. En el 67%de los casos hubo correspondencia, dentro de un mar-gen de + 2 g/dl, entre las lecturas de la escala cromáticay la medición registrada por el contador de Coulter. Seexaminan la posible utilidad clínica y el interés logísticode la nueva escala cromática, que es fácil de utilizar,tiene buena aceptación, es barata y da resultados in-mediatos. Sus posibilidades de uso para detectar laanemia en los dispensarios prenatales con recursos li-mitados son considerables.
Résumé
Diagnostic de l’anémie chez la femme enceinte dans les dispensaires ruraux :évaluation du potentiel de la nouvelle échelle colorée

Bulletin of the World Health Organization, 1999, 77 (1) 21
References1. The prevalence of anaemia in women: a tabulation of
available information. Geneva, World Health Organization,1992 (unpublished document WHO/MCH/MSM/92.2; availableupon request from Division of Reproductive Health, WorldHealth Organization, 1211 Geneva 27, Switzerland).
2. van den Broek NR. Anaemia in pregnancy in developingcountries. Review. British journal of obstetrics andgynaecology, 1998, 105: 385–390.
3. Nutritional anaemias. Report of a WHO Group of Experts.Geneva, World Health Organization, 1972 (WHO TechnicalReport Series, No. 503).
4. Prevention and management of severe anaemia in pregnancy.Geneva, World Health Organization, 1993 (unpublisheddocument WHO/FHE/MSM/93.5; available upon request fromDivision of Reproductive Health, World Health Organization,1211 Geneva 27, Switzerland).
5. Luby SP et al. Using clinical signs to diagnose anaemia inAfrican children. Bulletin of the World Health Organization,1995, 73: 477–482.
6. Sanchez-Carrillo CI. Bias due to conjunctiva hue and theclinical assessment of anaemia. Journal of clinicalepidemiology, 1989, 42: 751–754.
7. Sanchez-Carrillo CI et al. Test of a non-invasive instrumentfor measuring haemoglobin concentration. Internationaljournal of technical assessment in health care, 1989,5: 659–667.
8. Ghosh S, Mohan M. Screening for anaemia. Lancet, 1978,1: 823.
9. Stott GJ, Lewis SM. A simple and reliable method forestimating haemoglobin. Bulletin of the World HealthOrganization, 1995, 73: 369–373.
10. Hennekens CH, Buring JE. In: Mayrent SL, ed. Epidemiologyin medicine. Boston, Little, Brown & Company, 1987.
11. Jaeschke R, Guyatt GH, Sackett DL. Users’ guide to themedical literature III. How to use an article about a diagnostic
test. What are the results and will they help me in caring formy patients? Journal of the American Medical Association,1994, 271: 703–707.
12. Gjorup T et al. A critical evaluation of the clinical diagnosisof anaemia. American journal of epidemiology, 1986,124: 657–665.
13. Agresti A. Categorical data analysis. New York, John Wiley &Sons, 1990.
14. Stone JE et al. An evaluation of methods for screening foranaemia. Bulletin of the World Health Organization, 1984,62: 115–120.
15. Neville RG. Evaluation of portable hemoglobinometer ingeneral practice. British medical journal, 1987, 294:1263–1265.
16. Jacobs HD et al. Observer bias and error in integumentaryclinical diagnosis of anaemia. South African medical journal,1979, 55: 1031–1034.
17. Strochbach et al. The value of the physical examination inthe diagnosis of anemia. Archives of internal medicine, 1988,148: 831–832.
18. Politzer WM, Myburgh WM, van der Merwe JF.Haemoglobin estimation – reliability of the copper sulphatespecific gravity v. the cyanhaemoglobin colorimetric method.South African medical journal, 1988, 73: 111–112.
19. Pistorius LR et al. Screening for anaemia in pregnancy withcopper sulphate densitometry. International journal ofgynaecology and obstetrics, 1996, 52: 3–36.
20. van Lerberghe W et al. Haemoglobin measurement : thereliability of some simple techniques for use in a primaryhealth care setting. Bulletin of the World Health Organization,1983, 61: 957–965.
21. Kegels G et al. Haemoglobin and packed cell volumemeasurement: the reliability of some simple techniques foruse in surveys or rural hospitals. Annales des Sociétés Belgesde Médecine Tropicale, 1984, 64: 413–419.
Diagnosing anaemia using the Haemoglobin Colour Scale

22 Bulletin of the World Health Organization, 1999, 77 (1)
Research
Unrecognized sexually transmitted infections inrural South African women: a hidden epidemicD. Wilkinson,1 S.S. Abdool Karim,1 A. Harrison,1 M. Lurie,1 M. Colvin,1
C. Connolly,1 & A.W. Sturm2
1 Centre for Epidemiological Research in South Africa, MedicalResearch Council, PO Box 198, Mtubatuba 3935, South Africa;and Hlabisa Hospital, Hlabisa, South Africa. Requests for reprintsshould be sent to Dr Wilkinson at the former address.2 Department of Medical Microbiology, University of Natal,Durban, South Africa.
IntroductionNot all people with a sexually transmitted infection(STI) are symptomatic; not all those who are symp-tomatic recognize the meaning or importance of theirsymptoms and seek care; and not all those who doseek care are adequately treated (1). The proportionsthat are asymptomatic, symptomatic but not seek-ing care, and symptomatic and seeking care, haveimportant implications for disease control. If mostpatients are symptomatic and present for treatment,a priority is high-quality case management. If mostare symptomatic, but symptom recognition andtreatment-seeking behaviour is poor, health promo-tion becomes especially important. However, ifthe majority are asymptomatic, strategies such asscreening and mass treatment may assume highestpriority.
But where does the true burden of diseaselie? It is well established that 60–70% of gonococcaland chlamydial infections in women are asympto-matic (2, 3), and recent data suggest that a similarproportion of men may have asymptomatic infec-tions (4). A model proposed by Piot, and modifiedversions of it (5, 6), suggest that only a minor pro-
portion of STIs in developing countries are evertreated adequately because most cases never presentfor care. However, the proportion of cases that areasymptomatic, symptomatic but not seeking care,and symptomatic and seeking care has not been de-fined for an African population.
To design cost-effective STI control strate-gies, we used data from studies conducted in a ruralSouth African health district to estimate the pointprevalence of STIs among women, and the propor-tion who, on any given day, are asymptomatic, symp-tomatic but not seeking care, and symptomatic andseeking care. Clinic surveys were used to estimatefurther the proportion of infected women who wereadequately treated.
MethodsSettingHlabisa health district is situated in northernKwaZulu/Natal, South Africa. The populationserved in 1996 was estimated at 205 463 based onthe 1991 census data. Most residents are rural peo-ple living in widely scattered kraals, and are depend-ent on migrant labour, pension remittances, andsubsistence farming for money and food. Migrantlabour is a particularly strong feature of life; we esti-mate that in 60% of households the male head isabsent most of the time (Medical Research Council,unpublished data, 1997).
© World Health Organization 1999
Sexually transmitted infections (STIs) are of major public health concern in developing countries, not least becausethey facilitate transmission of human immunodeficiency virus (HIV). The present article presents estimates of theprevalence, on any given day, of STIs among women in rural South Africa and the proportion who are asympto-matic, symptomatic but not seeking care, and symptomatic and seeking care. The following data sources fromHlabisa district were used: clinical surveillance for STI syndromes treated in health facilities, microbiological stud-ies among women attending antenatal and family planning clinics, and a community survey. Population censusprovided denominator data. Adequacy of drug treatment was determined through quality of care surveys.
Of 55 974 women aged 15–49 years, a total of 13 943 (24.9%) were infected on any given day with atleast one of Trichomonas vaginalis, Neisseria gonorrhoeae, Chlamydia trachomatis, or Treponema pallidum. Ofthe women investigated, 6697 (48%) were asymptomatic, 6994 (50%) were symptomatic but not seeking care,238 (1.7%) were symptomatic and would seek care, and 14 (0.3%) were seeking care on that day. Only 9 of the14 women (65%) were adequately treated.
STIs remained untreated because either women were asymptomatic or the symptoms were not recognizedand acted upon. Improved case management alone is therefore unlikely to have a major public health impact.Improving partner treatment and women’s awareness of symptoms is essential, while the potential of mass STItreatment needs to be explored.
Voir page 27 le résumé en français. En la página 27 figura un resumen en español.
Bulletin of the World Health Organization, 1999, 77 (1) 23
Patients with STIs are treated either in pub-lic sector primary care clinics staffed by nurses or byprivate sector general practitioners. Care is free inthe public sector, but private practitioners charge afee that averages R 25 (US$ 5). The provincial healthdepartment recommends syndromic case manage-ment, and modern drugs such as quinolones are in-cluded in the treatment protocols. There are few dataavailable on the epidemiology of STIs in rural SouthAfrica (7), but the country is in the midst of a rap-idly escalating human immunodeficiency virus(HIV) epidemic (8). Prevalence of HIV infectionamong women attending antenatal clinics in Hlabisadistrict increased from 4.2% in 1992 (8) to 22% in1997 (Medical Research Council, unpublished data,1997).
Data sourcesIn order to estimate the proportion of women withSTIs who are asymptomatic, symptomatic but notseeking care, and symptomatic and seeking care onany given day, we applied data from four differentstudies conducted in Hlabisa to population estimatesderived from the 1991 census. Definitions used areshown in Table 1.
STI syndrome surveillance. Passive surveillancefor STI syndromes in all primary care settings in thedistrict has been carried out since February 1996(9), and in the first year 5069 female residents aged15–49 years were treated for symptomatic STIs. Thisrepresents an average of 14 women each day (5069/365) and hence, with a mean symptom duration of18 days (9), we estimate that on any one day thereare 252 (14 x 18) women in the district with a symp-tomatic STI who will present at some time duringthat illness episode for treatment.
Symptoms and STIs in women attendingantenatal clinics. A total of 327 women bookingfor antenatal care in four district primary care clin-ics were questioned about symptoms and examinedfor STIs using standard microbiology on vaginal andcervical specimens, and syphilis serology (MedicalResearch Council, unpublished data, 1996). Mostwomen (271; 83%) reported abnormal symptoms(Table 2), and 170 (52%) were infected with at leastone STI (Trichomonas vaginalis, Neisseriagonorrhoeae, Chlamydia trachomatis, or Treponemapallidum). As shown in other studies (10, 11) theassociation between elicited symptoms and labora-tory-confirmed infection was weak.
Symptoms and STIs in women attending fam-ily planning clinics. A total of 189 women attend-ing the Hlabisa family planning clinic werequestioned and examined in the same way and forthe same organisms as those attending the antenatalclinic (12). Fewer women (125; 39%) reported typi-cal symptoms; 47 (25%) had at least one STI, and60% of these women were asymptomatic. The asso-ciation between elicited symptoms and infection wasweak (12).
Community prevalence survey. A communitysurvey (13), which included residents being ques-
tioned about symptoms, having their urine testedby ligase chain reaction for gonococcal andchlamydial infection, and being tested by serologyfor syphilis, was used to supplement the antenataland family planning studies. Of 149 women exam-ined, 23 (15%) had either active syphilis or gono-coccal or chlamydial infection. Infection with T.vaginalis was not measured. No women reportedsymptoms.
Census and population data. The resident dis-trict female population aged 15–49 years for 1996(55 974) was estimated from the 1991 census (Ta-ble 2). From antenatal clinic records and a commu-nity survey (14) we estimated that 9057 womenbecome pregnant each year. Assuming an averagenumber of 24.8 women (9057/365) becoming preg-nant each day and an average pregnancy duration of280 days, a total of 6948 women (12.4%) will bepregnant on any given day in Hlabisa.
AssumptionsThe assumptions shown below were made.• The Hlabisa district STI surveillance system was
assumed to detect all symptomatic STIs present-ing for care. The completeness of the surveillancesystem has not been validated; however, surveil-lance returns show internal consistency over timeand between surveillance sites. While it is inevi-table that some cases were not captured, it seems
Table 1. Definition of terms
Terms Definition
Symptoms Patient-reported abnormalities
Typical symptoms Genital itch, vaginal discharge, genital ulcer, lowerabdominal pain, dysuria, dyspareunia
Signs Abnormal physical signs observed by a clinician
STI Laboratory-confirmed infections with either Trichomonasvaginalis (by culture), Neisseria gonorrhoeae (by culture),Chlamydia trachomatis (by direct immunofluorescence), orTreponema pallidum (defined serologically as rapidplasma reagin (RPR) positivity plus T. pallidumhaemagglutination (TPHA positivity))
STI syndrome A combination of symptoms and signs typically associatedwith sexually transmitted microorganisms. Genital ulcersyndrome, which may be due to syphilis, chancroid, herpesetc; vaginal discharge syndrome, which may be due toinfection with either T. vaginalis, N. gonorrhoeae, orC. trachomatis; pelvic inflammatory disease, which maybe due to the same organisms as those responsible forvaginal discharge syndrome
Symptomatic STI STI syndrome in a woman with typical symptoms whopresents to the health service for treatment
Symptomatic Microbiologically confirmed STI in a woman with typicalbut untreated STI symptoms who does not present for treatment
Asymptomatic STI Microbiologically confirmed STI in a woman without anysymptoms
Unrecognized sexually transmitted infections in rural South African women
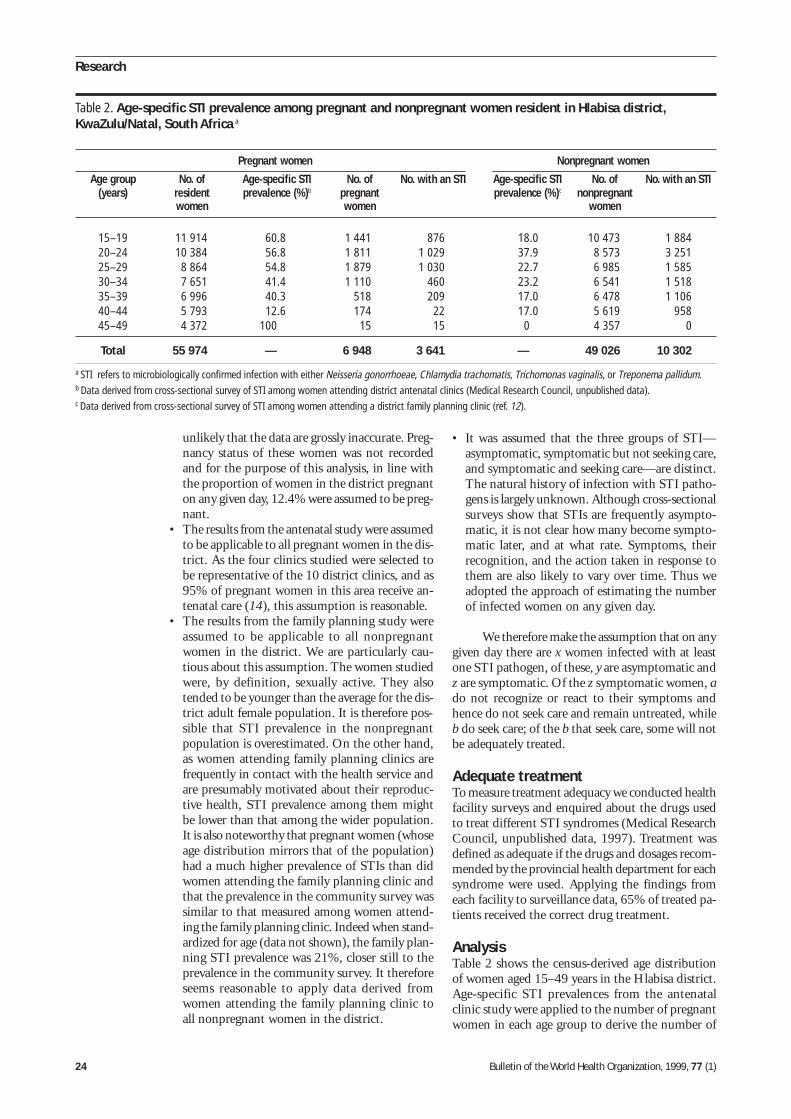
24 Bulletin of the World Health Organization, 1999, 77 (1)
Research
unlikely that the data are grossly inaccurate. Preg-nancy status of these women was not recordedand for the purpose of this analysis, in line withthe proportion of women in the district pregnanton any given day, 12.4% were assumed to be preg-nant.
• The results from the antenatal study were assumedto be applicable to all pregnant women in the dis-trict. As the four clinics studied were selected tobe representative of the 10 district clinics, and as95% of pregnant women in this area receive an-tenatal care (14), this assumption is reasonable.
• The results from the family planning study wereassumed to be applicable to all nonpregnantwomen in the district. We are particularly cau-tious about this assumption. The women studiedwere, by definition, sexually active. They alsotended to be younger than the average for the dis-trict adult female population. It is therefore pos-sible that STI prevalence in the nonpregnantpopulation is overestimated. On the other hand,as women attending family planning clinics arefrequently in contact with the health service andare presumably motivated about their reproduc-tive health, STI prevalence among them mightbe lower than that among the wider population.It is also noteworthy that pregnant women (whoseage distribution mirrors that of the population)had a much higher prevalence of STIs than didwomen attending the family planning clinic andthat the prevalence in the community survey wassimilar to that measured among women attend-ing the family planning clinic. Indeed when stand-ardized for age (data not shown), the family plan-ning STI prevalence was 21%, closer still to theprevalence in the community survey. It thereforeseems reasonable to apply data derived fromwomen attending the family planning clinic toall nonpregnant women in the district.
• It was assumed that the three groups of STI—asymptomatic, symptomatic but not seeking care,and symptomatic and seeking care—are distinct.The natural history of infection with STI patho-gens is largely unknown. Although cross-sectionalsurveys show that STIs are frequently asympto-matic, it is not clear how many become sympto-matic later, and at what rate. Symptoms, theirrecognition, and the action taken in response tothem are also likely to vary over time. Thus weadopted the approach of estimating the numberof infected women on any given day.
We therefore make the assumption that on anygiven day there are x women infected with at leastone STI pathogen, of these, y are asymptomatic andz are symptomatic. Of the z symptomatic women, ado not recognize or react to their symptoms andhence do not seek care and remain untreated, whileb do seek care; of the b that seek care, some will notbe adequately treated.
Adequate treatmentTo measure treatment adequacy we conducted healthfacility surveys and enquired about the drugs usedto treat different STI syndromes (Medical ResearchCouncil, unpublished data, 1997). Treatment wasdefined as adequate if the drugs and dosages recom-mended by the provincial health department for eachsyndrome were used. Applying the findings fromeach facility to surveillance data, 65% of treated pa-tients received the correct drug treatment.
AnalysisTable 2 shows the census-derived age distributionof women aged 15–49 years in the Hlabisa district.Age-specific STI prevalences from the antenatalclinic study were applied to the number of pregnantwomen in each age group to derive the number of
Table 2. Age-specific STI prevalence among pregnant and nonpregnant women resident in Hlabisa district,KwaZulu/Natal, South Africa a
Pregnant women Nonpregnant women
Age group No. of Age-specific STI No. of No. with an STI Age-specific STI No. of No. with an STI(years) resident prevalence (%)b pregnant prevalence (%)c nonpregnant
women women women
15–19 11 914 60.8 1 441 876 18.0 10 473 1 88420–24 10 384 56.8 1 811 1 029 37.9 8 573 3 25125–29 8 864 54.8 1 879 1 030 22.7 6 985 1 58530–34 7 651 41.4 1 110 460 23.2 6 541 1 51835–39 6 996 40.3 518 209 17.0 6 478 1 10640–44 5 793 12.6 174 22 17.0 5 619 95845–49 4 372 100 15 15 0 4 357 0
Total 55 974 — 6 948 3 641 — 49 026 10 302
a STI refers to microbiologically confirmed infection with either Neisseria gonorrhoeae, Chlamydia trachomatis, Trichomonas vaginalis, or Treponema pallidum.b Data derived from cross-sectional survey of STI among women attending district antenatal clinics (Medical Research Council, unpublished data).c Data derived from cross-sectional survey of STI among women attending a district family planning clinic (ref. 12).
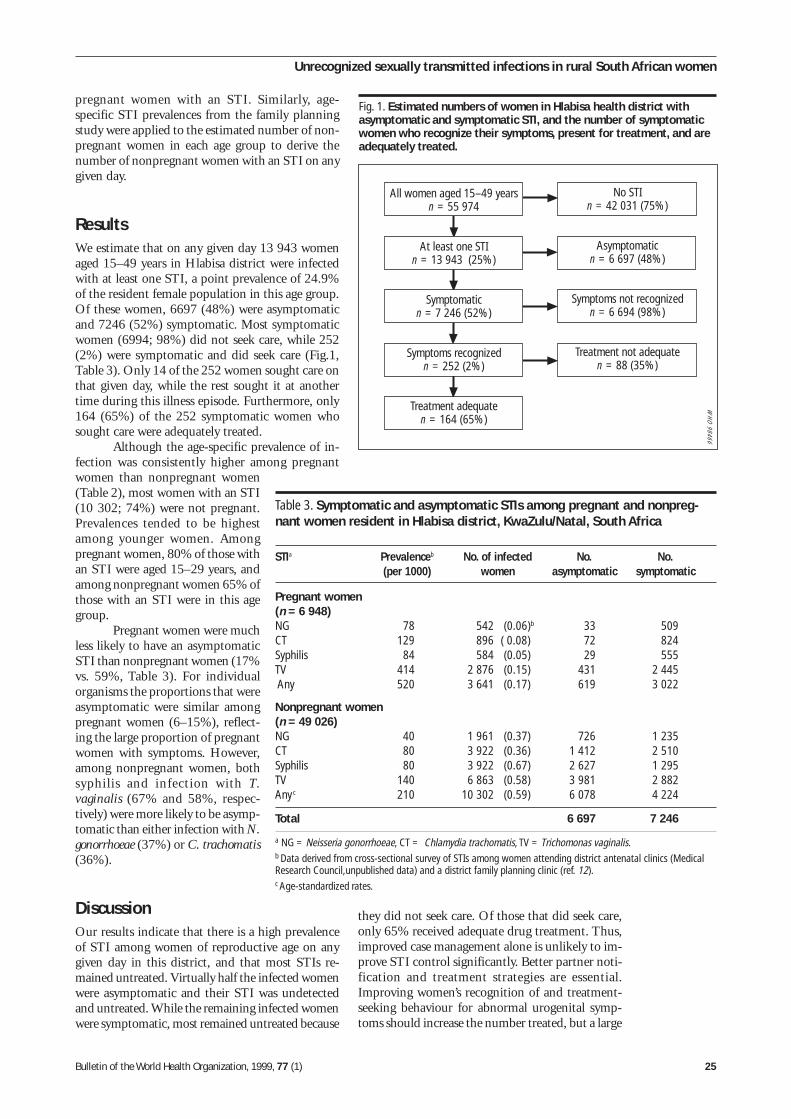
Bulletin of the World Health Organization, 1999, 77 (1) 25
pregnant women with an STI. Similarly, age-specific STI prevalences from the family planningstudy were applied to the estimated number of non-pregnant women in each age group to derive thenumber of nonpregnant women with an STI on anygiven day.
ResultsWe estimate that on any given day 13 943 womenaged 15–49 years in Hlabisa district were infectedwith at least one STI, a point prevalence of 24.9%of the resident female population in this age group.Of these women, 6697 (48%) were asymptomaticand 7246 (52%) symptomatic. Most symptomaticwomen (6994; 98%) did not seek care, while 252(2%) were symptomatic and did seek care (Fig.1,Table 3). Only 14 of the 252 women sought care onthat given day, while the rest sought it at anothertime during this illness episode. Furthermore, only164 (65%) of the 252 symptomatic women whosought care were adequately treated.
Although the age-specific prevalence of in-fection was consistently higher among pregnantwomen than nonpregnant women(Table 2), most women with an STI(10 302; 74%) were not pregnant.Prevalences tended to be highestamong younger women. Amongpregnant women, 80% of those withan STI were aged 15–29 years, andamong nonpregnant women 65% ofthose with an STI were in this agegroup.
Pregnant women were muchless likely to have an asymptomaticSTI than nonpregnant women (17%vs. 59%, Table 3). For individualorganisms the proportions that wereasymptomatic were similar amongpregnant women (6–15%), reflect-ing the large proportion of pregnantwomen with symptoms. However,among nonpregnant women, bothsyphilis and infection with T.vaginalis (67% and 58%, respec-tively) were more likely to be asymp-tomatic than either infection with N.gonorrhoeae (37%) or C. trachomatis(36%).
DiscussionOur results indicate that there is a high prevalenceof STI among women of reproductive age on anygiven day in this district, and that most STIs re-mained untreated. Virtually half the infected womenwere asymptomatic and their STI was undetectedand untreated. While the remaining infected womenwere symptomatic, most remained untreated because
they did not seek care. Of those that did seek care,only 65% received adequate drug treatment. Thus,improved case management alone is unlikely to im-prove STI control significantly. Better partner noti-fication and treatment strategies are essential.Improving women’s recognition of and treatment-seeking behaviour for abnormal urogenital symp-toms should increase the number treated, but a large
Table 3. Symptomatic and asymptomatic STIs among pregnant and nonpreg-nant women resident in Hlabisa district, KwaZulu/Natal, South Africa
STIa Prevalenceb No. of infected No. No.(per 1000) women asymptomatic symptomatic
Pregnant women(n = 6 948)NG 78 542 (0.06)b 33 509CT 129 896 ( 0.08) 72 824Syphilis 84 584 (0.05) 29 555TV 414 2 876 (0.15) 431 2 445 Any 520 3 641 (0.17) 619 3 022
Nonpregnant women(n = 49 026)NG 40 1 961 (0.37) 726 1 235CT 80 3 922 (0.36) 1 412 2 510Syphilis 80 3 922 (0.67) 2 627 1 295TV 140 6 863 (0.58) 3 981 2 882Any c 210 10 302 (0.59) 6 078 4 224
Total 6 697 7 246
a NG = Neisseria gonorrhoeae, CT = Chlamydia trachomatis, TV = Trichomonas vaginalis.b Data derived from cross-sectional survey of STIs among women attending district antenatal clinics (MedicalResearch Council,unpublished data) and a district family planning clinic (ref. 12).c Age-standardized rates.
Unrecognized sexually transmitted infections in rural South African women
All women aged 15–49 yearsn = 55 974
At least one STIn = 13 943 (25%)
Symptomaticn = 7 246 (52%)
Symptoms recognizedn = 252 (2%)
Treatment adequaten = 164 (65%)
No STIn = 42 031 (75%)
Asymptomaticn = 6 697 (48%)
Symptoms not recognizedn = 6 694 (98%)
Treatment not adequaten = 88 (35%)
WH
O 98466
Fig. 1. Estimated numbers of women in Hlabisa health district withasymptomatic and symptomatic STI, and the number of symptomaticwomen who recognize their symptoms, present for treatment, and areadequately treated.

26 Bulletin of the World Health Organization, 1999, 77 (1)
Research
burden of asymptomatic infection will remain un-less screening or mass treatment is considered.
The assumption that the three groups con-sidered (symptomatic and seeking care, symptomaticbut not seeking care, and asymptomatic) are distinctneeds further consideration. Understanding of thenatural history of STIs is not complete: for exam-ple, while many gonococcal and chlamydial infec-tions were asymptomatic, it is not clear whether theseinfections were ever symptomatic or will becomesymptomatic or at what rate. Even if asymptomaticSTIs do become symptomatic and patients presentfor treatment, the delay in doing so may be consid-erable, and this delay may allow continued trans-mission. It is not clear how infectious asymptomaticSTIs are, and thus how relevant they are, comparedwith symptomatic cases. The prevalence of STIs maybe even higher than we estimated, because we didnot use the most sensitive microbiological tests thatare available. We were unable to study men, but datafrom the United Republic of Tanzania suggest thatasymptomatic infection is at least as frequent amongmen as women (4).
Whatever the temporal relationship betweenthese groups, they are probably in equilibrium sincethe rates of infection that we observed are similar tothose reported from neighbouring districts severalyears ago (15), and the prevalence of syphilis amongantenatal women has not declined in recent years(Medical Research Council, unpublished data, 1990–96). Thus modelling the prevalence of STIs on anygiven day seems to be a reasonable way of gainingsome insight into aspects of STI epidemiology.
What are the transmission dynamics thatmaintain this large reservoir of prevalent and un-treated infection? We believe that there are threemain factors.
First, case management is poor. Thosewomen given inadequate drug treatment probablyremain infectious and continue to spread disease.Furthermore, as our clinical surveillance indicatesthat only about 4% of patients treated for an STIare asymptomatic contacts (9), partner treatmentstrategies are clearly inadequate and this also per-petuates transmission.
Second, if most cases never present for treat-ment, transmission will continue unchecked. Fewsymptomatic women seem to realize that they areinfected and hence they do not seek care. The corre-lation between infection and symptoms has beenshown in many studies to be poor (9–12) and ifsymptoms are both common and nonspecific it isperhaps unreasonable to expect women consistentlyto suspect an STI. This is especially so in pregnancywhen urogenital symptoms not due to infection arecommon. Conversely, some women may suspect anSTI, but decide not to seek care because of perceivedshame, cost, or unpleasant services. This issue needsfurther study. However, even at the risk of consider-able overtreatment, improving women’s recognition
of abnormal urogenital symptoms and encouragingpresentation for syndromic management are poten-tially important for improving STI control.
The third reason for the continued highprevalence of STIs is the considerable circular mi-gration by men between an urban workplace and arural home (13). We have previously shown that theprevalence of HIV infection among male migrantsin Hlabisa is considerably higher than that amongresidents (13). Female-controlled methods such asvaginal microbicides could be an important way ofprotecting the female partners of migrants and ofinterrupting STI transmission.
What are the immediate implications of ourfindings for STI control in African populations?Clearly, high quality case management is importantfor those patients who seek treatment. Other com-ponents of syndromic management (partner treat-ment, condom promotion, and counselling toprevent new infections) must be successfully imple-mented to reduce the prevalence of asymptomaticinfection and the number of incident cases.
However, it is difficult to see how a substan-tial reduction in STI prevalence can be achieved ina reasonable time frame without some form of massor presumptive treatment. Two options exist; pre-sumptive treatment of the whole population of re-productive age, or the treatment of high-risk oraccessible groups (16). As most STIs in our settingare found among nonpregnant women, mass treat-ment only of women attending antenatal clinics isunlikely to be sufficient. Surveys to define the pro-portion of women of reproductive age who havecontact with the health service, and under what cir-cumstances, would help further define the potentialutility of presumptive treatment delivered in servicesettings.
There are few data on the cost-effectivenessof alternative STI control strategies and more re-search is needed. Mass treatment would be expen-sive; giving a single dose of azithromycin to allpregnant women in Hlabisa and their partners wouldcost R 800 000 (US$ 200 000), equivalent to 80%of the total district pharmacy budget. However, itcould be a highly cost-effective intervention as preg-nancy outcome might also be improved (17), andboth STI sequelae and STI and HIV transmissionmight be considerably reduced. Mass treatmentmight only be needed once, with the aim of sub-stantially reducing STI prevalence before conven-tional measures are used to maintain any gainachieved (16). How sustained the effect of a singleround of mass treatment would be depends on theeffectiveness of supporting interventions, particularlythose aimed at migrants.
If we are serious about controlling STIs thereare three clear steps to follow (see Fig.1). The first isto improve the management of patients who seekcare, to encourage them to seek care early, and totreat their partners. The second is to increase the

Bulletin of the World Health Organization, 1999, 77 (1) 27
number of symptomatic people who seek care, in-cluding core groups; and the third is to develop ascreening or mass treatment strategy that will reachasymptomatic people and those with symptoms who
do not seek care. Multiple strategies that operatebeyond health facilities are required if a substantialand sustained reduction in community STI preva-lence is to be achieved. ■
Résumé
Infections sexuellement transmissibles non détectées chez les Sud-Africaines vivanten milieu rural : une épidémie invisibleLes infections sexuellement transmissibles (IST) sont ungrave problème de santé publique dans les pays en dé-veloppement, notamment parce qu’elles facilitent latransmission du virus de l’immunodéficience humaine(VIH). Cet article donne des estimations de la prévalencedes IST, quel que soit le jour, chez les femmes vivantdans les zones rurales d’Afrique du Sud et indique lepourcentage de sujets asymptomatiques, de sujetssymptomatiques qui ne se font pas soigner et de sujetssymptomatiques qui se font soigner. On a utilisé lessources suivantes dans le district de Hlabisa : surveillanceclinique des syndromes d’IST soignés dans les établis-sements de santé, études microbiologiques chez les fem-mes qui consultent les services prénatals et deplanification familiale, et enquête dans la communauté.Le recensement de la population a fourni les donnéesservant de dénominateur. Des enquêtes sur la qualitédes soins ont permis de déterminer si la pharmaco-thérapie était adaptée ou non.
Sur 55 974 femmes âgées de 15 à 49 ans, etquel que soit le jour, 13 943 au total (soit 24,9%) étaientinfectées par au moins un des germes suivants : Tricho-monas vaginalis, Neisseria gonorrhoeae, Chlamydiatrachomatis et Treponema pallidum. Sur les femmes étu-diées, 6697 (48%) n’avaient pas de symptômes, 6994(50%) avaient des symptômes mais ne se faisaient passoigner, 238 (1,7%) présentaient des symptômes et seferaient soigner, et 14 (0,3%) se faisaient soigner lejour même. Seules 9 de ces 14 femmes (65%) rece-vaient un traitement adéquat.
Les IST n’étaient pas soignées parce que les fem-mes n’avaient pas de symptômes ou parce que les symp-tômes n’étaient pas correctement identifiés et traitésen conséquence. Il est donc peu probable qu’unemeilleure prise en charge des cas ait à elle seule uneincidence majeure sur le plan de la santé publique. Ilest indispensable de mieux soigner les partenaires etd’apprendre aux femmes à reconnaître les symptômes,tout en étudiant la possibilité d’un traitement de massecontre les IST.
Resumen
Infecciones de transmisión sexual no reconocidas en las campesinas sudafricanas:una epidemia ocultaLas infecciones de transmisión sexual (ITS) son un im-portante problema de salud pública en los países endesarrollo, especialmente porque facilitan la transmi-sión del virus de la inmunodeficiencia humana (VIH).En el presente artículo se ofrecen estimaciones de laprevalencia de las ITS entre las campesinas sudafricanasen un día dado, y la proporción de las que sonasintomáticas, sintomáticas que no solicitan asistencia,y sintomáticas que solicitan asistencia. Las fuentes dedatos del distrito de Hlabisa que se utilizaron fueronlas siguientes: la vigilancia clínica de los síndromes deITS tratados en los establecimientos de salud, los estu-dios microbiológicos de las mujeres que acuden a losdispensarios de atención prenatal y de planificación fa-miliar, y una encuesta comunitaria. El censo demográfi-co proporcionó los datos denominadores. La idoneidaddel tratamiento medicamentoso se determinó median-te encuestas sobre la calidad de la atención.
De 55 974 mujeres de edades comprendidas en-tre 15 y 49 años, 13 943 (24,9%) estaban infectadas
en un día dado por al menos uno de los siguientes agen-tes: Trichomonas vaginalis, Neisseria gonorrhoeae,Chlamydia trachomatis o Treponema pallidum. De lasmujeres investigadas, 6697 (48%) eran asintomáticas,6994 (50%) eran sintomáticas pero no habían solicita-do asistencia, 238 (1,7%) eran sintomáticas y busca-rían asistencia, y 14 (0,3%) habían solicitado asistenciaese día. De estas 14 mujeres, sólo 9 (65%) eran trata-das adecuadamente.
La falta de tratamiento de las ITS se debía bien aque las mujeres eran asintomáticas o bien a que lossíntomas no se reconocían y, en consecuencia, no sehacía nada al respecto. Por lo tanto, no es probableque un mejor manejo de casos tenga, por sí solo, gran-des repercusiones en la salud pública. Es esencial me-jorar el tratamiento de la pareja y aumentar losconocimientos de las mujeres acerca de los síntomas,estudiando al mismo tiempo la posibilidad de un trata-miento masivo de las ITS.
Unrecognized sexually transmitted infections in rural South African women

28 Bulletin of the World Health Organization, 1999, 77 (1)
Research
References1. Abdool Karim SS. Challenges to the control of sexually
transmitted diseases in Africa. American journal of publichealth, 1994, 84: 1891–1893.
2. Mabey D. Sexually transmitted diseases in developingcountries. Transactions of the Royal Society of TropicalMedicine and Hygiene, 1996, 90: 97–99.
3. De Schryver A, Meheus A. Epidemiology of sexuallytransmitted diseases: the global picture. Bulletin of the WorldHealth Organization, 1990, 68: 639–654.
4. Grosskurth H et al. Asymptomatic gonorrhoea andchlamydial infection in rural Tanzanian men. British medicaljournal, 1996, 312: 277–280.
5. Fransen L. Meet the experts. Paper presented at:International Conference on AIDS and STDs, Berlin.
6. Mayaud P, Ka-Gina K, Grosskurth H. STD casemanagement in prevention and management of sexuallytransmitted diseases in Eastern and Southern Africa. Currentapproaches and future directions. (NARESA Monograph 3).
7. Pham-Kanter GB, Steinberg MH, Ballard RC. Sexuallytransmitted diseases in South Africa. Genitourinary medicine,1996, 72: 167–171.
8. Coleman R, Wilkinson D. Increasing HIV prevalence in arural district of South Africa. Journal of acquiredimmunodeficiecy syndrome and human retrovirology, 1997,16: 50–53.
9. Wilkinson D et al.. Sexually transmitted disease syndromesin rural South Africa: results from health facility surveillance.Sexually transmitted diseases, 1998, 25: 20–23.
10. Vuylsteke B et al. Clinical algorithms for the screening ofwomen for gonococcal and chlamydial infection: evaluation ofpregnant women and prostitutes in Zaire. Clinical infectiousdiseases, 1993, 17: 82–88.
11. Mayaud P et al. Risk assessment and other screeningoptions for gonorrhoea and chlamydial infections in womenattending rural Tanzanian antenatal clinics. Bulletin of theWorld Health Organization, 1995, 73: 621–630.
12. Wilkinson D et al. Family planning services in developingcountries: an opportunity to treat asymptomatic andunrecognised genital tract infections? Genitourinary medicine,1997, 73: 558–560.
13. Colvin M, Abdool Karim SS, Wilkinson D. Migration andAIDS. Lancet, 1995, 46: 1303.
14. Wilkinson D. et al. Maternal and child health indicators in arural South African health district. South African medicaljournal, 1997, 87: 456–459.
15. O’Farrell N et al. Sexually transmitted pathogens inpregnant women in a rural South African community.Genitourinary medicine, 1989, 65: 276–280.
16. Adler M. et al. Sexual health and care. Sexually transmittedinfections. Guidelines for prevention and treatment. London,Overseas Development Administration, 19 (Health andPopulation Occasional Paper).
17. Temmerman M et al. Mass antimicrobial treatment inpregnancy. A randomised placebo-controlled trial in apopulation with high rates of sexually transmitted diseases.Journal of reproductive medicine, 1995, 40: 176–180.
Bulletin of the World Health Organization, 1999, 77 (1) 29
Use of SoloShot autodestruct syringes comparedwith disposable syringes, in a nationalimmunization campaign in Indonesia*
C.M. Nelson, 1 A. Sutanto,2 & I.G.P. Suradana 3
* SoloShot is a trademark of Becton Dickinson and Company.1 Program Manager, Program for Appropriate Technology inHealth/Lombok, Mataram, Lombok, Indonesia. Requests forreprints should be sent to this author at the following address:Program for Appropriate Technology in Health (PATH), 4 NickersonStreet, Seattle, WA 98109, USA.2 Head, Disease Prevention and Health Promotion, NTB Province,Ministry of Health, Indonesia.3 Field Manager, Program for Appropriate Technology in Health/Lombok; Mataram, Lombok, Indonesia.
Autodestruct syringes can reduce the improper reuse of syringes, which present a significant risk in the transmis-sion of bloodborne pathogens in developing countries, especially during immunization campaigns owing to thehigh number of injections given per session. SoloShot is an autodestruct syringe, distributed by UNICEF, which hasbeen shown to be safer and easier to use than standard syringes. This study analyses the accuracy and dose-efficiency of SoloShot, compared with disposable syringes, during a national tetanus toxoid immunization cam-paign on the Indonesian island of Lombok. Observation and dose measurements revealed that SoloShot syringesdelivered more precise and consistent doses and 15% more doses per vial than disposable syringes. Vaccinesavings may partially be offset by the higher price of SoloShot. Vaccinators preferred SoloShot, describing it aseasier to use, faster, and more accurate than the disposable syringe. The study indicates that SoloShot is highlyappropriate for use in immunization campaigns by reducing vaccine wastage and improving injection safety.
Voir page 32 le résumé en français. En la página 33 figura un resumen en español.
IntroductionThe reuse and improper sterilization of syringespresent significant risks in the transmission ofbloodborne pathogens (1–4). Surveys in developingcountries have shown that up to 30% of injectionsfor immunizations are not sterile (5).
Immunization campaigns present their ownrisks of unsafe injection practices. The influx of largequantities of disposable syringes, usually purchasedor donated for these campaigns, could easily lead toimproper syringe reuse once the campaign is over.WHO and UNICEF have therefore called for theuse of autodestruct syringes in mass immunizationcampaigns (6). WHO prefers the autodestruct typeof disposable syringe for administering vaccines, es-pecially for conducting mass immunizations (7).Such syringes present the lowest risk of person-to-person transmission of bloodborne pathogens be-cause they cannot be reused.
One type of autodestruct syringe, SoloShot,was developed under the USAID-funded HealthTechproject and studied in a trial in Pakistan in 1987(8). It was determined to be safe and effective in pre-venting reuse, as well as easier and quicker to usethan a conventional disposable syringe. The SoloShotsyringe, which is available commercially, is distrib-
uted through UNICEF’s Supply Division in Copen-hagen and is being increasingly used in immuniza-tion programmes in developing countries.
SoloShot syringes were used in Indonesia fora national immunization campaign in 1996 as partof the neonatal tetanus elimination programme;approximately 13 million of these syringes were usedin the campaign to deliver two doses of tetanus tox-oid to women of childbearing age. This article in-vestigates the appropriateness of SoloShot in theIndonesian campaign, compared to a standard dis-posable syringe, in terms of vaccine wastage, doseaccuracy, and user acceptability.
Materials and methodsSyringes and vaccinesSoloShot (Fig. 1) is a plastic disposable syringeequipped with an internal metal clip. After permit-ting a single filling and injection, the clip locks theplunger and prevents refilling. The clip is set to en-gage when a dose of 0.5 ml is withdrawn. A 23-gauge, 25-mm needle, suitable for intramuscularinjection, is permanently attached. A conventional3-ml disposable syringe (Becton Dickinson) fittedwith a 23-gauge, 30-mm needle was used for com-parison in the trial. Ten-dose vials of tetanus toxoid(Perum Bio Farma, Bandung, Indonesia) were usedin the study as well as throughout the Indonesiancampaign.
Vaccinators and study sitesVaccinators were regular Indonesian Ministry ofHealth service personnel and midwives from sub-district-level health centres. All were experienced
© World Health Organization 1999

30 Bulletin of the World Health Organization, 1999, 77 (1)
Research
vaccinators in Indonesia’s Expanded Programme onImmunization and had delivered at least 100 injec-tions using SoloShot prior to the data collectionperiod.
Training for the national immunization cam-paign consisted of a one-day session for all vaccinatorsand managers, including the proper use and disposalof SoloShot. The present study was not announcedprior to training, and the training given was consid-ered representative of that conducted throughoutIndonesia. The vaccinators received no explanationsabout the study prior to or during data collection.
The study was conducted during regular na-tional immunization campaign sessions over a 4-dayperiod in December 1996. Observations were madeby two provincial-level Ministry of Health supervi-sors. Each day, one supervisor observed a vaccinatordelivering only SoloShot injections, and the othersupervisor observed a vaccinator delivering only dis-posable-syringe injections. Each observer alternatedbetween observing SoloShot injections and dispos-able-syringe injections on sequential days. Study ob-servations were made at rural immunization postsset up specifically for the national campaign in two
districts on Lombok Island within the province ofNusa Tenggara Barat (NTB). Sites were randomlyassigned to SoloShot or the disposable syringe onthe day of data collection.
Data collectionDuring immunization sessions, observers noted thenumber of doses taken from each vial. To collectsamples for dose accuracy, the observers asked thevaccinator to inject one dose from each vial into apre-weighed container. To minimize possible full-or empty-vial effects on dose accuracy, the third,fourth or fifth dose from each vial was randomlyselected for sampling. The vaccinator was asked toinject a dose into the container only after the dosehad been withdrawn for regular injection. Only vac-cine doses injected into clients and doses collectedin bottles were counted as having been delivered.Any unusual event—such as malfunctioning syringesor syringes discarded without being used—was re-corded. After injections were complete, the observerused a questionnaire to ask the vaccinators aboutthe syringe they used that day.
ResultsA total of 385 doses of vaccine were delivered withSoloShot, while 433 doses were delivered with thedisposable syringe. Eight different vaccinators wereobserved, four using SoloShot and four using dis-posable syringes (Table 1). Eleven SoloShot syringes(2.8% of the total used) were rendered unusablewhen the vaccinator tried to expel air from thembefore complete filling of the device, thereby acti-vating the non-reuse device and preventing completefilling. No disposable syringes were unnecessarilydiscarded during the study. Three of the fourSoloShot vaccinators delivered more doses per vialthan their disposable-syringe counterparts. Less in-ter-vaccinator variation in the mean-dose deliveredwas recorded among SoloShot users.
SoloShot delivered an average of 1.02 (15%)more doses per vial than the disposable syringe (Ta-ble 2). A total of 46 SoloShot doses and 48 dispos-able-syringe doses were collected and measured.SoloShot provided a mean dose closer to the desired0.5-ml dose as well as a smaller dose variation.
The volume of full vials was measured anddetermined to contain 5.01 ml. To determine theamount of vaccine left in discarded vials, 24 dis-carded vials from each syringe type were collectedand the volume of the contents measured. There wereno significant differences between the vial residuesfor the two syringe types, averaging less than onedose per discarded vial. The dead space of each sy-ringe was 0.005 ml for SoloShot and 0.080 ml forthe disposable syringe. As a result, an average of 2.6doses of vaccine per vial used were wasted by usersof the disposable syringe, while users of SoloShotwasted 1.2 doses of vaccine per vial used (Table 3).
Fig. 1. The SoloShot plastic disposable syringe. After a single filling andinjection the internal clip locks the plunger and prevents refilling.
Table 1. Injection data using SoloShot and disposable syringes
Syringe type and No. of Mean doses No. of Mean dosedoses delivered vials used delivered syringes delivered per
per vial discarded injection (ml)
SoloShot98 12 8.17 0 0.5288 11 8.00 0 0.5285 12 7.08 8 0.51
114 13 8.77 3 0.52
Disposable108 17 6.35 0 0.58115 16 7.19 0 0.60132 18 7.33 0 0.55
86 12 7.17 0 0.50
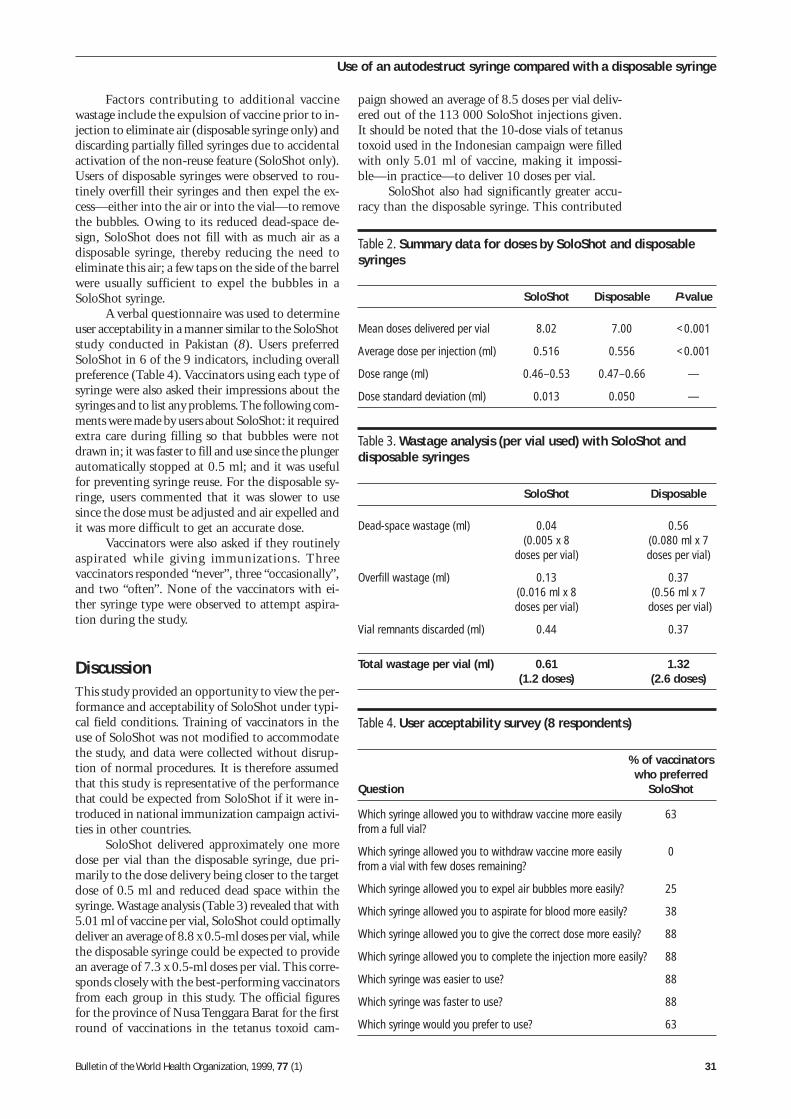
Bulletin of the World Health Organization, 1999, 77 (1) 31
paign showed an average of 8.5 doses per vial deliv-ered out of the 113 000 SoloShot injections given.It should be noted that the 10-dose vials of tetanustoxoid used in the Indonesian campaign were filledwith only 5.01 ml of vaccine, making it impossi-ble—in practice—to deliver 10 doses per vial.
SoloShot also had significantly greater accu-racy than the disposable syringe. This contributed
Table 4. User acceptability survey (8 respondents)
% of vaccinatorswho preferred
Question SoloShot
Which syringe allowed you to withdraw vaccine more easily 63from a full vial?
Which syringe allowed you to withdraw vaccine more easily 0from a vial with few doses remaining?
Which syringe allowed you to expel air bubbles more easily? 25
Which syringe allowed you to aspirate for blood more easily? 38
Which syringe allowed you to give the correct dose more easily? 88
Which syringe allowed you to complete the injection more easily? 88
Which syringe was easier to use? 88
Which syringe was faster to use? 88
Which syringe would you prefer to use? 63
Table 2. Summary data for doses by SoloShot and disposablesyringes
SoloShot Disposable P-value
Mean doses delivered per vial 8.02 7.00 <0.001
Average dose per injection (ml) 0.516 0.556 <0.001
Dose range (ml) 0.46–0.53 0.47–0.66 —
Dose standard deviation (ml) 0.013 0.050 —
Table 3. Wastage analysis (per vial used) with SoloShot anddisposable syringes
SoloShot Disposable
Dead-space wastage (ml) 0.04 0.56(0.005 x 8 (0.080 ml x 7
doses per vial) doses per vial)
Overfill wastage (ml) 0.13 0.37(0.016 ml x 8 (0.56 ml x 7doses per vial) doses per vial)
Vial remnants discarded (ml) 0.44 0.37
Total wastage per vial (ml) 0.61 1.32(1.2 doses) (2.6 doses)
Factors contributing to additional vaccinewastage include the expulsion of vaccine prior to in-jection to eliminate air (disposable syringe only) anddiscarding partially filled syringes due to accidentalactivation of the non-reuse feature (SoloShot only).Users of disposable syringes were observed to rou-tinely overfill their syringes and then expel the ex-cess—either into the air or into the vial—to removethe bubbles. Owing to its reduced dead-space de-sign, SoloShot does not fill with as much air as adisposable syringe, thereby reducing the need toeliminate this air; a few taps on the side of the barrelwere usually sufficient to expel the bubbles in aSoloShot syringe.
A verbal questionnaire was used to determineuser acceptability in a manner similar to the SoloShotstudy conducted in Pakistan (8). Users preferredSoloShot in 6 of the 9 indicators, including overallpreference (Table 4). Vaccinators using each type ofsyringe were also asked their impressions about thesyringes and to list any problems. The following com-ments were made by users about SoloShot: it requiredextra care during filling so that bubbles were notdrawn in; it was faster to fill and use since the plungerautomatically stopped at 0.5 ml; and it was usefulfor preventing syringe reuse. For the disposable sy-ringe, users commented that it was slower to usesince the dose must be adjusted and air expelled andit was more difficult to get an accurate dose.
Vaccinators were also asked if they routinelyaspirated while giving immunizations. Threevaccinators responded “never”, three “occasionally”,and two “often”. None of the vaccinators with ei-ther syringe type were observed to attempt aspira-tion during the study.
DiscussionThis study provided an opportunity to view the per-formance and acceptability of SoloShot under typi-cal field conditions. Training of vaccinators in theuse of SoloShot was not modified to accommodatethe study, and data were collected without disrup-tion of normal procedures. It is therefore assumedthat this study is representative of the performancethat could be expected from SoloShot if it were in-troduced in national immunization campaign activi-ties in other countries.
SoloShot delivered approximately one moredose per vial than the disposable syringe, due pri-marily to the dose delivery being closer to the targetdose of 0.5 ml and reduced dead space within thesyringe. Wastage analysis (Table 3) revealed that with5.01 ml of vaccine per vial, SoloShot could optimallydeliver an average of 8.8 x 0.5-ml doses per vial, whilethe disposable syringe could be expected to providean average of 7.3 x 0.5-ml doses per vial. This corre-sponds closely with the best-performing vaccinatorsfrom each group in this study. The official figuresfor the province of Nusa Tenggara Barat for the firstround of vaccinations in the tetanus toxoid cam-
Use of an autodestruct syringe compared with a disposable syringe

32 Bulletin of the World Health Organization, 1999, 77 (1)
Research
to vaccine savings and could play a role in improvedvaccine efficacy where dose accuracy is important.
The 15% saving in tetanus toxoid deliveredby SoloShot may not represent a significant overallsaving—especially in light of the higher syringe wast-age that might be expected from the occasionallydiscarded SoloShot arising from air that could notbe expelled. In this study, 11 SoloShot syringes werewasted, while about 40 doses of vaccine were savedby using SoloShot. At a UNICEF price of US$ 0.10per SoloShot and a tetanus toxoid cost of US$ 0.05per dose, the vaccine cost savings were halved by thesyringe wastage. However, the increased efficiencyof SoloShot could be a significant economic benefitif it were used with more expensive vaccines such ashepatitis B, Haemophilus influenzae type B (Hib),or quadrivalent vaccines.
Vaccinators indicated a strong preference forSoloShot, considering it easier, faster, and more ac-curate to use. However, one vaccinator experiencedsignificant difficulties with SoloShot, accounting for8 of the 11 SoloShot discards. This was the oldestand most experienced vaccinator of the group, andhe had difficulty modifying his syringe-filling tech-nique so as not to withdraw large amounts of airinto the syringe. Given the small sample size of thisstudy, it is difficult to say to what extent this prob-lem may occur with other vaccinators; however, it isan indication that, during training, special attentionshould be paid to modifying the vaccine withdrawalprocedures—especially among experiencedvaccinators.
While SoloShot improves injection safety byeliminating reuse of syringes, other safety issues mayalso be considered. Disposal boxes were supplied bythe manufacturer and used in the Indonesian teta-nus toxoid campaign; occasionally, however, it wasobserved that the syringe supply exceeded the dis-
posal-box capacity, resulting in over-filled boxes andprotruding syringes. With SoloShot—as with alldisposable syringes—care must be taken to ensurecompliance with proper disposal techniques.
Recapping of both SoloShot and disposablesyringes was frequently observed. While noneedlestick injuries were observed for either syringetype, recapping presents a danger to health workers.Training should emphasize immediate insertion ofthe syringe into the disposal box without recapping.
This study indicated that use of SoloShot ishighly appropriate in a national immunization cam-paign setting. It could reduce vaccine wastage whileimproving injection safety. The study also confirmedthe findings of the SoloShot evaluation conductedin Pakistan—specifically, that it was preferred byvaccinators and can be used properly and safely witha minimal amount of training. ■
AcknowledgementsWe are grateful to the following organizations andindividuals for supporting this study: the Centraland East Lombok District Health Departments, DrKetut Artastra, Sri Heny and Sitti Hindum of theNTB Provincial Health Department, BectonDickinson and Company, and Surayah ofLaboritorium Hepatika.
The study was jointly supported by USAIDthrough the Technologies for Health (Health Tech)project under Cooperative Agreement No. HRN-A-00-96-90007-02 and by Worldwide InjectionSystems of Becton Dickinson and Company. Thedevelopment of the autodestruct device used inSoloShot was carried out by Program for Appropri-ate Technology in Health (PATH) with support fromUSAID under the Technologies for Child Healthproject, Cooperative Agreement No. DPE-5968-A-00-7035-00.
Résumé
Utilisation comparée des seringues autobloquantes SoloShot et des seringuesjetables dans le cadre d’une campagne nationale de vaccination en IndonésieL’utilisation de seringues autobloquantes pourrait fairereculer la réutilisation indue des seringues, un graveproblème pour les programmes de vaccination des paysen développement. De par leur nature même, les cam-pagnes de vaccination nécessitent de grandes quanti-tés de seringues jetables, susceptibles d’être facilementréutilisées une fois la campagne achevée. L’UNICEF dis-tribue une seringue autobloquante, la seringue SoloShot,qui s’est révélée plus sûre et d’un usage plus commodeque les seringues classiques. La présente étude a con-sisté en une analyse de la précision et de l’efficacité dedosage de la SoloShot, comparativement à la seringuejetable, lors d’une campagne nationale de vaccination parl’anatoxine tétanique dans l’île indonésienne de Lombok.
On a observé les faits et gestes de quatre vacci-nateurs titulaires qui utilisaient des seringues SoloShotet de quatre autres qui utilisaient des seringues jeta-bles classiques. Les vaccinateurs n’avaient pas reçud’instructions ni de formation particulières autres que
celles habituellement données par le Ministère indoné-sien de la Santé aux utilisateurs de ces types de serin-gue. On a noté le nombre de doses délivrées parampoule ainsi que tous les problèmes qui se posaient.Il avait été en outre demandé aux vaccinateurs d’injec-ter de temps à autre le contenu d’une seringue dansune ampoule pour mesurer la dose délivrée. Aprèschaque séance, on demandait aux vaccinateurs quelleseringue avait leur préférence.
Les seringues SoloShot on délivré 8,02 doses parampoule, contre 7,00 doses pour les seringues jetables,soit une différence de 15%. Par ailleurs, les SoloShotont délivré une dose moyenne de 0,516 ml par injec-tion contre 0,556 ml dans le cas des seringues jetables.Il n’y avait pas de différence entre les deux seringuespour ce qui est de la quantité de vaccin restant dans lesampoules après utilisation. Toutefois l’espace mort dela seringue, c’est-à-dire le volume de vaccin qui reste àl’intérieur sans pouvoir être injecté, s’est révélé être
Bulletin of the World Health Organization, 1999, 77 (1) 33
se pudo administrar 7,00 dosis por vial, lo que repre-senta una diferencia del 15%. Las jeringas SoloShotsuministraban una dosis media de 0,516 ml por inyec-ción; para las jeringas desechables, en cambio, esa do-sis era de 0,556 ml por inyección. Los restos de vacunaen los viales descartados no revelaron diferencias en-tre los dos tipos de jeringas; no obstante, se determinóque el espacio muerto de cada jeringa (la vacuna quequeda en la jeringa y no puede ser inyectada) era mu-cho menor en las jeringas SoloShot. La reducción delespacio muerto y la mayor precisión del volumen de ladosis se consideraron los factores principales que per-mitían hacer un uso más eficaz de la vacuna utilizandolas jeringas SoloShot. Sin embargo, el ahorro de vacu-na en parte puede quedar contrarrestado por el preciomás elevado de este tipo de jeringas.
Los vacunadores prefirieron la SoloShot, a la quedescribieron como más fácil de utilizar, más rápida ymás precisa que la jeringa desechable. Un vacunadortuvo dificultades con la SoloShot: varias veces dejó pa-sar aire a la jeringa y activó prematuramente el dispo-sitivo de autodestrucción al tratar de expelerlo. Duranteel adiestramiento debe prestarse especial atención a lamodificación de los procedimientos de aspiración queexige la nueva jeringa, especialmente en el caso devacunadores experimentados.
En el estudio se indica que la jeringa SoloShot esmuy apropiada para su utilización en campañas de in-munización, ya que permite reducir las pérdidas de va-cuna y mejorar la seguridad de la inyección.
beaucoup plus faible dans le cas de la SoloShot. Il ap-paraît que la réduction de l’espace mort et la meilleureprécision obtenue dans la dose délivrée sont à la basede la plus grande efficacité de la seringue SoloShot. Ilest vrai cependant que l’économie de vaccin ainsi réa-lisée pourrait être contrebalancée par le coût plus élevéde la SoloShot.
Les vaccinateurs ont donné la préférence à laseringue SoloShot pour sa plus grande facilité d’utilisa-tion et sa précision supérieure à celle de la seringuejetable. L’un d’entre eux a cependant eu des difficultés
avec la SoloShot : il aspirait systématiquement de l’airet actionnait prématurément le dispositif de blocageen tentant de l’éliminer. Lors de la formation, il faudradonc attirer l’attention des vaccinateurs – notammentde ceux qui sont expérimentés – sur la modificationde la technique d’apiration qu’impose la nouvelleseringue.
Cette étude montre que la seringue SoloShotconvient tout à fait aux campagnes de vaccination carelle réduit les pertes de vaccin et garantit une meilleuresécurité des injections.
Resumen
Comparación del uso de las jeringas autodestruibles SoloShot y de las jeringasdesechables en una campaña nacional de inmunización de IndonesiaLas jeringas autodestruibles pueden reducir lareutilización de las jeringas, que es uno de los grandesproblemas de los programas de inmunización de lospaíses en desarrollo. Para las campañas de inmuniza-ción se dispone habitualmente de grandes cantidadesde jeringas desechables, que pueden fácilmente serreutilizadas una vez finalizada la campaña. El UNICEFdistribuye una jeringa autodestruible, conocida comoSoloShot, que, según se ha comprobado, es más seguray más fácil de utilizar que las jeringas de uso corriente.En este estudio se analizaron la precisión y la eficienciade la dosificación de la jeringa SoloShot en relacióncon las jeringas desechables durante una campaña deinmunización con anatoxina tetánica realizada en la islaindonesia de Lombok.
En esa campaña se procedió a la observación decuatro vacunadores que utilizaban jeringas SoloShot ycuatro que empleaban jeringas desechables estándares.Los vacunadores no recibieron instrucciones ni adies-tramiento especial, salvo el adiestramiento habitual delMinisterio de Salud de Indonesia para el uso de ambostipos de jeringas. Se hicieron observaciones del núme-ro de dosis administradas por vial y de los problemasocurridos. Se pidió a los vacunadores que ocasional-mente inyectaran el contenido de una jeringa en unvial para medir la dosis. Después de cada sesión, serecabó la opinión de los vacunadores con respecto alas jeringas.
Las jeringas SoloShot permitieron administrar8,02 dosis por vial, mientras que con las desechables
References1. Aylward B et al. Reducing the risk of unsafe injections in
immunization programmes. Bulletin of the World HealthOrganization, 1995, 73: 531–540.
2. Anan A. India: unhealthy immunization programme. Lancet,1993, 341: 1402.
3. Aylward B et al. Model-based estimates of the risk ofhuman immunodeficiency virus and hepatitis B virustransmission through unsafe injections. International journalof epidemiology, 1995, 24: 446–452.
4. Expanded Programme on Immunization. Changingneedles but not the syringe: an unsafe practice. Weeklyepidemiological record, 1987, 62(46): 345–352.
5. Expanded Programme on Immunization. Technet News,1994, 94.1.
6. Safety of injections: WHO-UNICEF policy statement for massimmunization campaigns. Unpublished document WHO/EPI/LHIS/97.04 (available upon request from Global Programmefor Vaccines and Immunization, World Health Organization,1211 Geneva 27, Switzerland).
7. Safety of injections in immunization programmes: WHO-recommended policy. Unpublished document WHO/EPI/LHIS/96.05 (available upon request from Global Programme forVaccines and Immunization, World Health Organization, 1211Geneva 27, Switzerland).
8. Steinglass R et al. Safety, effectiveness, and ease of use ofa non-reusable syringe in a developing country immunizationprogramme. Bulletin of the World Health Organization, 1995,73: 57–63.
Use of an autodestruct syringe compared with a disposable syringe

34 Bulletin of the World Health Organization, 1999, 77 (1)
Research
Comparison of in vivo and in vitro tests ofresistance in patients treated with chloroquinein Yaoundé, CameroonP. Ringwald 1 & L.K. Basco 2
1 Researcher, Institut Français de Recherche Scientifique pour leDéveloppement en Coopération (ORSTOM) and Laboratoire deRecherches sur le Paludisme, Laboratoire Associé Francophone302, Organisation de Coordination pour la lutte contre lesEndémies en Afrique Centrale (OCEAC), Yaoundé, Cameroon.Requests for reprints should be sent to Dr Ringwald at thefollowing address: OCEAC/ORSTOM, B. P. 288, Yaoundé,Cameroon. e-mail : [email protected] Researcher, ORSTOM/OCEAC, Yaoundé, Cameroon.
The usefulness of an isotopic in vitro assay in the field was evaluated by comparing its results with the therapeuticresponse determined by the simplified WHO in vivo test in symptomatic Cameroonian patients treated with chlo-roquine. Of the 117 enrolled patients, 102 (87%) completed the 14-day follow-up, and 95 isolates obtained fromthese patients (46 children, 49 adults) yielded an interpretable in vitro test. A total of 57 of 95 patients (60%; 28children and 29 adults) had an adequate clinical response with negative smears (n = 46) or with an asymptomaticparasitaemia (n = 11) on day 7 and/or day 14. The geometric mean 50% inhibitory concentration of the isolatesobtained from these patients was 63.3 nmol/l. Late and early treatment failure was observed in 29 (30.5%) and 9(9.5%) patients, respectively. The geometric mean 50% inhibitory concentrations of the corresponding isolateswere 173 nmol/l and 302 nmol/l. Among the patients responding with late and early treatment failure, five iso-lates and one isolate, respectively, yielded a discordant result (in vivo resistance and in vitro sensitivity). Thesensitivity, specificity, and predictive value of the in vitro test to detect chloroquine-sensitive cases was 67%, 84%and 86%, respectively. There was moderate concordance between the in vitro and in vivo tests (kappa value =0.48). The in vitro assay agrees relatively well with the therapeutic response and excludes several host factors thatinfluence the results of the in vivo test. However, in view of some discordant results, the in vitro test cannotsubstitute for in vivo data on therapeutic efficacy. The only reliable definition of “resistance” in malaria parasitesis based on clinical and parasitological response in symptomatic patients, and the in vivo test provides the stand-ard method to determine drug sensitivity or resistance as well as to guide national drug policies.
Voir page 41 le résumé en français. En la página 41 figura un resumen en español.
IntroductionChloroquine-resistant Plasmodium falciparum hasbeen reported in all sub-Saharan African countries(1). The extent of such resistance is still limited inmany areas of Africa, and most reported cases of re-sistance are at the RI level (2–4). These findings,together with economic considerations and a gener-ally high level of acquired immunity, justify the rec-ommendation to use chloroquine for the first-linetreatment of acute uncomplicated falciparum ma-laria infections in indigenous patients in most sub-Saharan Africa where acceptable clinical cure ratescan be obtained (5). However, the possibility of anincreasingly ineffective chloroquine therapy, as con-firmed in other endemic areas, necessitates regularassessment of the therapeutic efficacy of chloroquineto guide drug policies in Africa.
There are two general methods to assess drugefficacy in the field: in vivo and in vitro tests (6). Inthe past, both WHO standard tests were largely ap-
plied in the field but accumulated experience hasshown that neither of these tests has been adoptedwidely for making decisions on drug policies (7).Clinical evaluation of therapeutic efficacy is basedon the determination of the proportion of treatmentfailure in a patient population at a particular studysite. The aim of in vivo tests is to detect drug resist-ance, defined as “the ability of a parasite strain tosurvive and/or multiply despite the administrationand absorption of a drug in doses equal to or higherthat those usually recommended but within the lim-its of tolerance of the subject” (8). The standard invivo tests described in 1973 allowed enrolment ofeither symptomatic patients or asymptomatic para-site carriers and required either a daily 7-day (“7-day test”) or a 28-day follow-up (daily for the first 7days, weekly thereafter; “extended test”) in a ma-laria-free zone (8). Such a test is hardly practical inAfrica, especially from the social and economic view-point if a 1-month hospitalization period is required.In addition, drug efficacy determined for sympto-matic patients cannot be extrapolated from studiesconducted on asymptomatic parasite carriers. A con-siderable improvement was introduced recently withthe development of a more practical and simplified14-day in vivo test that is performed on sympto-matic patients with acute uncomplicated falciparummalaria (7). The simplified in vivo test is performedby a regular measurement of body temperature and
© World Health Organization 1999

Bulletin of the World Health Organization, 1999, 77 (1) 35
microscopic examination of blood films. The stand-ard or simplified in vivo test is the reference methodto detect drug resistance.
In vitro assays are based on culturing P.falciparum isolates in the presence of a range of con-centrations of an antimalarial drug for one life cycleor part of a life cycle. Drug efficacy is assessed bycounting the number of parasites developing intoschizonts (WHO in vitro test) or by measuring thequantity of radiolabelled hypoxanthine, a DNA pre-cursor, incorporated into the parasites (isotopicmicrotest) (6, 9–13). Chloroquine resistance is de-duced when the parasite growth is not inhibitedbelow a threshold concentration.
It has been argued that the results of in vitrotests of resistance do not always coincide with thoseof in vivo tests and may thus be irrelevant for clini-cal studies (7). Part of the problem is associated withthe type of in vitro assay as well as insufficient dataon in vitro assays performed in parallel with in vivotests in individual patients. A comparison of in vivoand in vitro tests of resistance has not been exten-sively investigated for chloroquine because this drughad lost its efficacy in many endemic areas before invitro culture techniques were developed and its useis no longer recommended to treat P. falciparum in-fections in these areas.
In the present retrospective analysis, we com-pared the results of isotopic in vitro assays and clini-cal response (measured using the simplified WHOin vivo test) of Cameroonian patients treated with astandard regimen of chloroquine. The aim was toevaluate whether in vitro assays from a given patientactually measure in vivo chloroquine sensitivity orresistance and to assess to what extent in vitro assaysmay be complementary to the in vivo test.
Patients and methodsPatientsA total of 117 Cameroonian adults and children aged>5 years (range: 5–50 years) residing in Yaoundé wererecruited at the Nlongkak Catholic missionary dis-pensary, Yaoundé, Cameroon, between 1994 and1996, with their free and informed consent. Thefollowing inclusion criteria were used: signs andsymptoms of acute uncomplicated falciparum ma-laria (fever >37.5 0C on enrolment or a history offever within the previous 24 h), monoinfection withP. falciparum, initial parasitaemia >5000 asexual para-sites per µl blood, and negative Saker–Solomonsurine test for antimalarial drugs (14). Pregnantwomen, patients with signs and symptoms of severeand complicated malaria, as defined by WHO (15),and patients with severe anaemia (haemoglobin <6g/dl) were excluded. The study was approved by theCameroonian National Ethics Committee.
In vivo testChloroquine (total dose, 25 mg/kg body weight inthree divided doses: 10 mg/kg on days 0 and 1; 5
mg/kg on day 2) was administered under supervi-sion. The patients were followed on an outpatientbasis on days 1, 2, 3, 4, 7 and 14. The clinical con-dition, body temperature, and parasite density wereassessed at each visit. Parasite density was determinedby counting the number of infected red blood cellsagainst 20 000 red blood cells in Giemsa-stained thinblood films (on day 0) or the number of asexualparasites against 1000 white blood cells in Giemsa-stained thick blood films (from day 1 onwards) andexpressed as the number of asexual parasites per µlof blood.
In the revised 1996 WHO classification of invivo response to antimalarial treatment, patients arefollowed on days 3, 7 and 14, and both clinical andparasitological responses are monitored (7). Theclinical and parasitological responses are classifiedas early treatment failure (ETF), late treatment fail-ure (LTF), or adequate clinical response (ACR). ETFis defined by one of the following four criteria: posi-tive smear and signs and symptoms of severe ma-laria on days 1, 2 or 3; positive smear (parasite density> day 0 density) and fever on day 2; positive smearand fever on day 3; and positive smear on day 3(parasite density ≥ 25% of pre-treatment density).LTF is defined as positive smear and signs and symp-toms of severe malaria between day 4 and day 14; orpositive smear and fever between day 4 and day 14.ACR refers to patients who have completed the 14-day follow-up and have a negative smear on day 14,with or without fever; or positive or negative smearand apyrexia during the follow-up, without previ-ously meeting the criteria of ETF or LTF. Patientswho responded with either ETF or LTF were treatedwith oral halofantrine (total dose = 1500 mg foradults or 24 mg base/kg body weight for children inthree divided doses at 6-hour intervals) or oral quinine(25 mg base per kg body weight per day for 5 days).
The parasitological response was alsointerpreted using the classical S–RI–RII–RIII classi-fication system (8). The interpretation of the parasito-logical response using the WHO standard testsrequires daily monitoring of the parasite densitybetween day 0 and day 7 for the “7-day test”, fol-lowed by a weekly blood film examination until day28 for the “extended test”. Since the 1996 simpli-fied in vivo test does not require daily monitoring ofblood films and is terminated at day 14, someparasitological responses cannot be clearly distin-guished. For this reason, the definitions of parasito-logical responses were modified as described below.• Sensitive (S)/late resistant grade I (RI) response.
Asexual parasite clearance on or before day 6 andnegative smears on day 7 and day 14. As in the“7-day test”, an S response and a late RI responsecannot be distinguished since the difference be-tween the two responses depends on the presence(late RI) or absence (S) of recrudescence betweenday 15 and day 28.
• Early resistant grade I (RI) response. Asexual para-site clearance on or before day 6, followed by re-crudescence between day 7 and day 14, inclusive.
In vivo and in vitro tests of chloroquine resistance
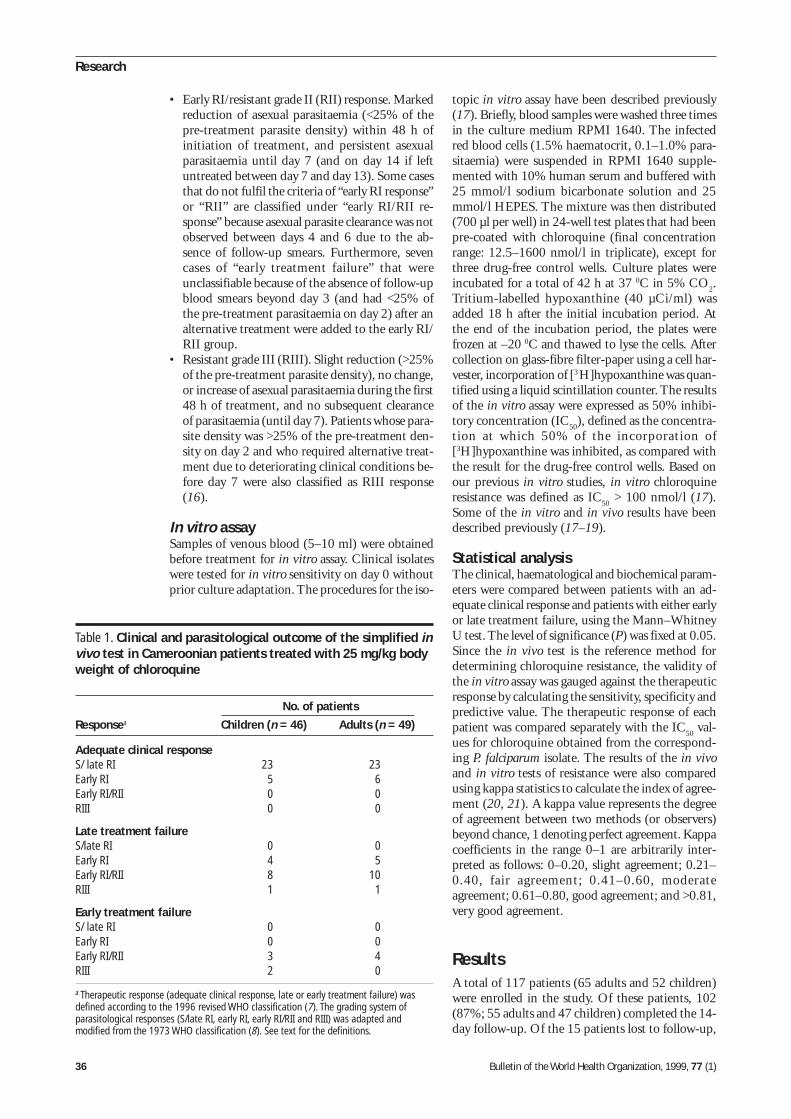
36 Bulletin of the World Health Organization, 1999, 77 (1)
Research
• Early RI/resistant grade II (RII) response. Markedreduction of asexual parasitaemia (<25% of thepre-treatment parasite density) within 48 h ofinitiation of treatment, and persistent asexualparasitaemia until day 7 (and on day 14 if leftuntreated between day 7 and day 13). Some casesthat do not fulfil the criteria of “early RI response”or “RII” are classified under “early RI/RII re-sponse” because asexual parasite clearance was notobserved between days 4 and 6 due to the ab-sence of follow-up smears. Furthermore, sevencases of “early treatment failure” that wereunclassifiable because of the absence of follow-upblood smears beyond day 3 (and had <25% ofthe pre-treatment parasitaemia on day 2) after analternative treatment were added to the early RI/RII group.
• Resistant grade III (RIII). Slight reduction (>25%of the pre-treatment parasite density), no change,or increase of asexual parasitaemia during the first48 h of treatment, and no subsequent clearanceof parasitaemia (until day 7). Patients whose para-site density was >25% of the pre-treatment den-sity on day 2 and who required alternative treat-ment due to deteriorating clinical conditions be-fore day 7 were also classified as RIII response(16).
In vitro assaySamples of venous blood (5–10 ml) were obtainedbefore treatment for in vitro assay. Clinical isolateswere tested for in vitro sensitivity on day 0 withoutprior culture adaptation. The procedures for the iso-
topic in vitro assay have been described previously(17). Briefly, blood samples were washed three timesin the culture medium RPMI 1640. The infectedred blood cells (1.5% haematocrit, 0.1–1.0% para-sitaemia) were suspended in RPMI 1640 supple-mented with 10% human serum and buffered with25 mmol/l sodium bicarbonate solution and 25mmol/l HEPES. The mixture was then distributed(700 µl per well) in 24-well test plates that had beenpre-coated with chloroquine (final concentrationrange: 12.5–1600 nmol/l in triplicate), except forthree drug-free control wells. Culture plates wereincubated for a total of 42 h at 37 0C in 5% CO
2.
Tritium-labelled hypoxanthine (40 µCi/ml) wasadded 18 h after the initial incubation period. Atthe end of the incubation period, the plates werefrozen at –20 0C and thawed to lyse the cells. Aftercollection on glass-fibre filter-paper using a cell har-vester, incorporation of [3 H]hypoxanthine was quan-tified using a liquid scintillation counter. The resultsof the in vitro assay were expressed as 50% inhibi-tory concentration (IC
50), defined as the concentra-
tion at which 50% of the incorporation of[3H]hypoxanthine was inhibited, as compared withthe result for the drug-free control wells. Based onour previous in vitro studies, in vitro chloroquineresistance was defined as IC
50 > 100 nmol/l (17).
Some of the in vitro and in vivo results have beendescribed previously (17–19).
Statistical analysisThe clinical, haematological and biochemical param-eters were compared between patients with an ad-equate clinical response and patients with either earlyor late treatment failure, using the Mann–WhitneyU test. The level of significance (P) was fixed at 0.05.Since the in vivo test is the reference method fordetermining chloroquine resistance, the validity ofthe in vitro assay was gauged against the therapeuticresponse by calculating the sensitivity, specificity andpredictive value. The therapeutic response of eachpatient was compared separately with the IC
50 val-
ues for chloroquine obtained from the correspond-ing P. falciparum isolate. The results of the in vivoand in vitro tests of resistance were also comparedusing kappa statistics to calculate the index of agree-ment (20, 21). A kappa value represents the degreeof agreement between two methods (or observers)beyond chance, 1 denoting perfect agreement. Kappacoefficients in the range 0–1 are arbitrarily inter-preted as follows: 0–0.20, slight agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderateagreement; 0.61–0.80, good agreement; and >0.81,very good agreement.
ResultsA total of 117 patients (65 adults and 52 children)were enrolled in the study. Of these patients, 102(87%; 55 adults and 47 children) completed the 14-day follow-up. Of the 15 patients lost to follow-up,
Table 1. Clinical and parasitological outcome of the simplified invivo test in Cameroonian patients treated with 25 mg/kg bodyweight of chloroquine
No. of patients
Responsea Children (n = 46) Adults (n = 49)
Adequate clinical responseS/ late RI 23 23Early RI 5 6Early RI/RII 0 0RIII 0 0
Late treatment failureS/late RI 0 0Early RI 4 5Early RI/RII 8 10RIII 1 1
Early treatment failureS/ late RI 0 0Early RI 0 0Early RI/RII 3 4RIII 2 0
a Therapeutic response (adequate clinical response, late or early treatment failure) wasdefined according to the 1996 revised WHO classification (7). The grading system ofparasitological responses (S/late RI, early RI, early RI/RII and RIII) was adapted andmodified from the 1973 WHO classification (8). See text for the definitions.
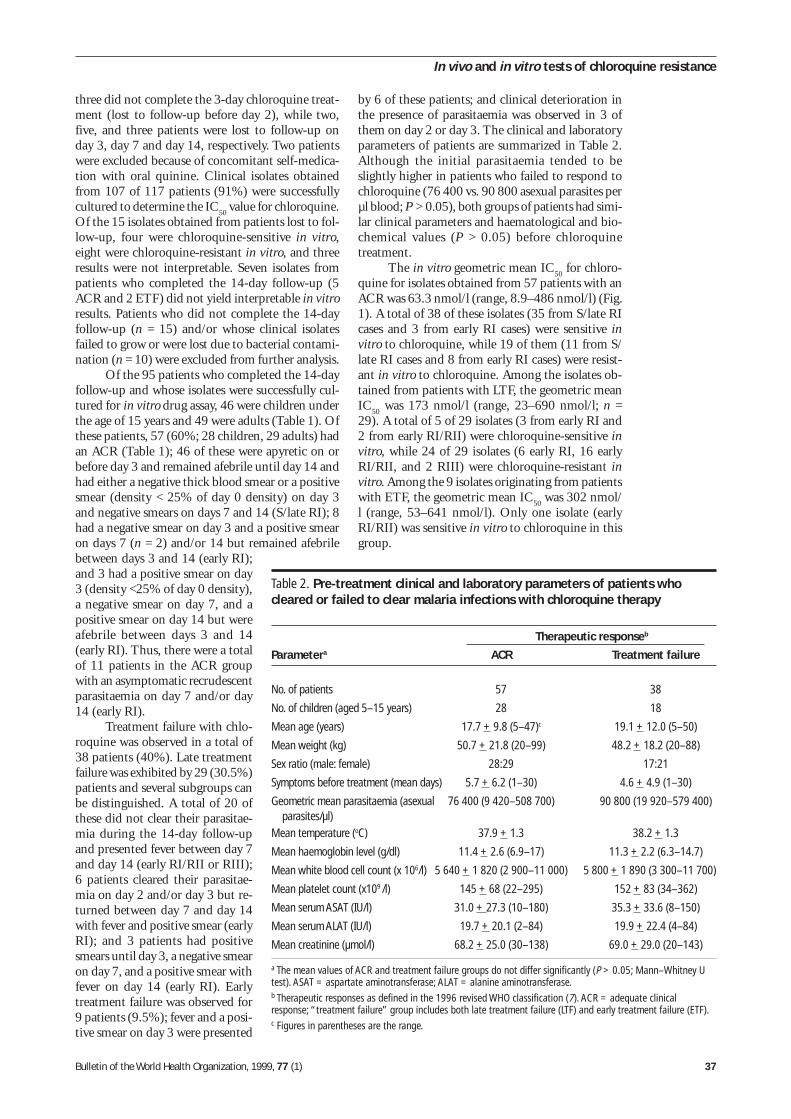
Bulletin of the World Health Organization, 1999, 77 (1) 37
three did not complete the 3-day chloroquine treat-ment (lost to follow-up before day 2), while two,five, and three patients were lost to follow-up onday 3, day 7 and day 14, respectively. Two patientswere excluded because of concomitant self-medica-tion with oral quinine. Clinical isolates obtainedfrom 107 of 117 patients (91%) were successfullycultured to determine the IC
50 value for chloroquine.
Of the 15 isolates obtained from patients lost to fol-low-up, four were chloroquine-sensitive in vitro,eight were chloroquine-resistant in vitro, and threeresults were not interpretable. Seven isolates frompatients who completed the 14-day follow-up (5ACR and 2 ETF) did not yield interpretable in vitroresults. Patients who did not complete the 14-dayfollow-up (n = 15) and/or whose clinical isolatesfailed to grow or were lost due to bacterial contami-nation (n = 10) were excluded from further analysis.
Of the 95 patients who completed the 14-dayfollow-up and whose isolates were successfully cul-tured for in vitro drug assay, 46 were children underthe age of 15 years and 49 were adults (Table 1). Ofthese patients, 57 (60%; 28 children, 29 adults) hadan ACR (Table 1); 46 of these were apyretic on orbefore day 3 and remained afebrile until day 14 andhad either a negative thick blood smear or a positivesmear (density < 25% of day 0 density) on day 3and negative smears on days 7 and 14 (S/late RI); 8had a negative smear on day 3 and a positive smearon days 7 (n = 2) and/or 14 but remained afebrilebetween days 3 and 14 (early RI);and 3 had a positive smear on day3 (density <25% of day 0 density),a negative smear on day 7, and apositive smear on day 14 but wereafebrile between days 3 and 14(early RI). Thus, there were a totalof 11 patients in the ACR groupwith an asymptomatic recrudescentparasitaemia on day 7 and/or day14 (early RI).
Treatment failure with chlo-roquine was observed in a total of38 patients (40%). Late treatmentfailure was exhibited by 29 (30.5%)patients and several subgroups canbe distinguished. A total of 20 ofthese did not clear their parasitae-mia during the 14-day follow-upand presented fever between day 7and day 14 (early RI/RII or RIII);6 patients cleared their parasitae-mia on day 2 and/or day 3 but re-turned between day 7 and day 14with fever and positive smear (earlyRI); and 3 patients had positivesmears until day 3, a negative smearon day 7, and a positive smear withfever on day 14 (early RI). Earlytreatment failure was observed for9 patients (9.5%); fever and a posi-tive smear on day 3 were presented
Table 2. Pre-treatment clinical and laboratory parameters of patients whocleared or failed to clear malaria infections with chloroquine therapy
Therapeutic responseb
Parametera ACR Treatment failure
No. of patients 57 38
No. of children (aged 5–15 years) 28 18
Mean age (years) 17.7 + 9.8 (5–47)c 19.1 + 12.0 (5–50)
Mean weight (kg) 50.7 + 21.8 (20–99) 48.2 + 18.2 (20–88)
Sex ratio (male: female) 28:29 17:21
Symptoms before treatment (mean days) 5.7 + 6.2 (1–30) 4.6 + 4.9 (1–30)
Geometric mean parasitaemia (asexual 76 400 (9 420–508 700) 90 800 (19 920–579 400)parasites/µl)
Mean temperature (oC) 37.9 + 1.3 38.2 + 1.3
Mean haemoglobin level (g/dl) 11.4 + 2.6 (6.9–17) 11.3 + 2.2 (6.3–14.7)
Mean white blood cell count (x 106/l) 5 640 + 1 820 (2 900–11 000) 5 800 + 1 890 (3 300–11 700)
Mean platelet count (x109 /l) 145 + 68 (22–295) 152 + 83 (34–362)
Mean serum ASAT (IU/l) 31.0 + 27.3 (10–180) 35.3 + 33.6 (8–150)
Mean serum ALAT (IU/l) 19.7 + 20.1 (2–84) 19.9 + 22.4 (4–84)
Mean creatinine (µmol/l) 68.2 + 25.0 (30–138) 69.0 + 29.0 (20–143)
a The mean values of ACR and treatment failure groups do not differ significantly (P > 0.05; Mann–Whitney Utest). ASAT = aspartate aminotransferase; ALAT = alanine aminotransferase.b Therapeutic responses as defined in the 1996 revised WHO classification (7). ACR = adequate clinicalresponse; “treatment failure” group includes both late treatment failure (LTF) and early treatment failure (ETF).c Figures in parentheses are the range.
In vivo and in vitro tests of chloroquine resistance
by 6 of these patients; and clinical deterioration inthe presence of parasitaemia was observed in 3 ofthem on day 2 or day 3. The clinical and laboratoryparameters of patients are summarized in Table 2.Although the initial parasitaemia tended to beslightly higher in patients who failed to respond tochloroquine (76 400 vs. 90 800 asexual parasites perµl blood; P > 0.05), both groups of patients had simi-lar clinical parameters and haematological and bio-chemical values (P > 0.05) before chloroquinetreatment.
The in vitro geometric mean IC50
for chloro-quine for isolates obtained from 57 patients with anACR was 63.3 nmol/l (range, 8.9–486 nmol/l) (Fig.1). A total of 38 of these isolates (35 from S/late RIcases and 3 from early RI cases) were sensitive invitro to chloroquine, while 19 of them (11 from S/late RI cases and 8 from early RI cases) were resist-ant in vitro to chloroquine. Among the isolates ob-tained from patients with LTF, the geometric meanIC
50 was 173 nmol/l (range, 23–690 nmol/l; n =
29). A total of 5 of 29 isolates (3 from early RI and2 from early RI/RII) were chloroquine-sensitive invitro, while 24 of 29 isolates (6 early RI, 16 earlyRI/RII, and 2 RIII) were chloroquine-resistant invitro. Among the 9 isolates originating from patientswith ETF, the geometric mean IC
50 was 302 nmol/
l (range, 53–641 nmol/l). Only one isolate (earlyRI/RII) was sensitive in vitro to chloroquine in thisgroup.
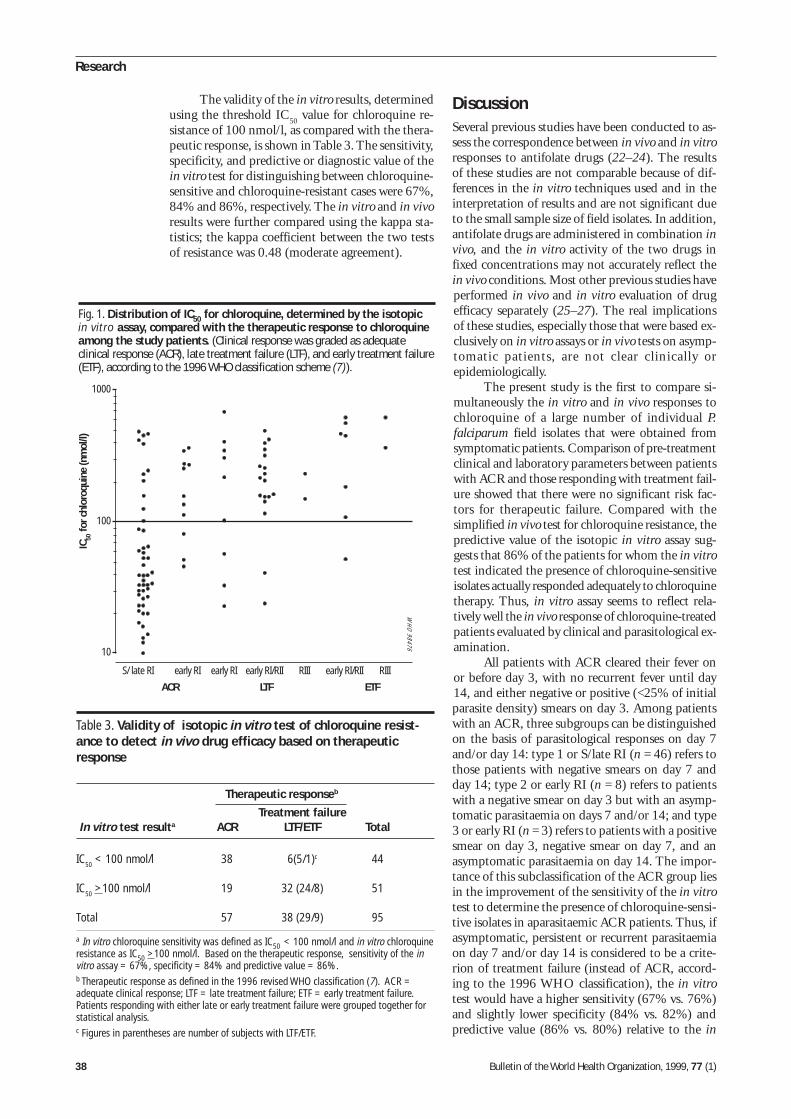
38 Bulletin of the World Health Organization, 1999, 77 (1)
Research
The validity of the in vitro results, determinedusing the threshold IC
50 value for chloroquine re-
sistance of 100 nmol/l, as compared with the thera-peutic response, is shown in Table 3. The sensitivity,specificity, and predictive or diagnostic value of thein vitro test for distinguishing between chloroquine-sensitive and chloroquine-resistant cases were 67%,84% and 86%, respectively. The in vitro and in vivoresults were further compared using the kappa sta-tistics; the kappa coefficient between the two testsof resistance was 0.48 (moderate agreement).
DiscussionSeveral previous studies have been conducted to as-sess the correspondence between in vivo and in vitroresponses to antifolate drugs (22–24). The resultsof these studies are not comparable because of dif-ferences in the in vitro techniques used and in theinterpretation of results and are not significant dueto the small sample size of field isolates. In addition,antifolate drugs are administered in combination invivo, and the in vitro activity of the two drugs infixed concentrations may not accurately reflect thein vivo conditions. Most other previous studies haveperformed in vivo and in vitro evaluation of drugefficacy separately (25–27). The real implicationsof these studies, especially those that were based ex-clusively on in vitro assays or in vivo tests on asymp-tomatic patients, are not clear clinically orepidemiologically.
The present study is the first to compare si-multaneously the in vitro and in vivo responses tochloroquine of a large number of individual P.falciparum field isolates that were obtained fromsymptomatic patients. Comparison of pre-treatmentclinical and laboratory parameters between patientswith ACR and those responding with treatment fail-ure showed that there were no significant risk fac-tors for therapeutic failure. Compared with thesimplified in vivo test for chloroquine resistance, thepredictive value of the isotopic in vitro assay sug-gests that 86% of the patients for whom the in vitrotest indicated the presence of chloroquine-sensitiveisolates actually responded adequately to chloroquinetherapy. Thus, in vitro assay seems to reflect rela-tively well the in vivo response of chloroquine-treatedpatients evaluated by clinical and parasitological ex-amination.
All patients with ACR cleared their fever onor before day 3, with no recurrent fever until day14, and either negative or positive (<25% of initialparasite density) smears on day 3. Among patientswith an ACR, three subgroups can be distinguishedon the basis of parasitological responses on day 7and/or day 14: type 1 or S/late RI (n = 46) refers tothose patients with negative smears on day 7 andday 14; type 2 or early RI (n = 8) refers to patientswith a negative smear on day 3 but with an asymp-tomatic parasitaemia on days 7 and/or 14; and type3 or early RI (n = 3) refers to patients with a positivesmear on day 3, negative smear on day 7, and anasymptomatic parasitaemia on day 14. The impor-tance of this subclassification of the ACR group liesin the improvement of the sensitivity of the in vitrotest to determine the presence of chloroquine-sensi-tive isolates in aparasitaemic ACR patients. Thus, ifasymptomatic, persistent or recurrent parasitaemiaon day 7 and/or day 14 is considered to be a crite-rion of treatment failure (instead of ACR, accord-ing to the 1996 WHO classification), the in vitrotest would have a higher sensitivity (67% vs. 76%)and slightly lower specificity (84% vs. 82%) andpredictive value (86% vs. 80%) relative to the in
Table 3. Validity of isotopic in vitro test of chloroquine resist-ance to detect in vivo drug efficacy based on therapeuticresponse
Therapeutic responseb
Treatment failure In vitro test resulta ACR LTF/ETF Total
IC50 < 100 nmol/l 38 6(5/1)c 44
IC50 >100 nmol/l 19 32 (24/8) 51
Total 57 38 (29/9) 95
a In vitro chloroquine sensitivity was defined as IC50 < 100 nmol/l and in vitro chloroquineresistance as IC50 >100 nmol/l. Based on the therapeutic response, sensitivity of the invitro assay = 67%, specificity = 84% and predictive value = 86%.b Therapeutic response as defined in the 1996 revised WHO classification (7). ACR =adequate clinical response; LTF = late treatment failure; ETF = early treatment failure.Patients responding with either late or early treatment failure were grouped together forstatistical analysis.c Figures in parentheses are number of subjects with LTF/ETF.
WH
O 98476
Fig. 1. Distribution of IC50 for chloroquine, determined by the isotopicin vitro assay, compared with the therapeutic response to chloroquineamong the study patients. (Clinical response was graded as adequateclinical response (ACR), late treatment failure (LTF), and early treatment failure(ETF), according to the 1996 WHO classification scheme (7)).
S/ late RI
1000
IC50
for c
hlor
oqui
ne (n
mol
/l)
ACR
100
10
LTF ETF
early RI early RI early RI/RII RIII early RI/RII RIII

Bulletin of the World Health Organization, 1999, 77 (1) 39
vivo test. The kappa coefficient between the two testswould also increase from 0.48 to 0.58. All three type3 (early RI) ACR patients had chloroquine-resistant isolates, as determined by the in vitro assay(chloroquine IC
50 > 100 nmol/l; 137, 272, and 348
nmol/l). Five type 2 (early RI) ACR patients wereinfected with chloroquine-resistant isolates (IC
50 =
114, 158, 258, 278, and 368 nmol/l), while threetype 2 patients harboured chloroquine-sensitive iso-lates (IC
50 = 46, 51 and 81 nmol/l). Of the 46 type
1 (S/late RI) ACR-patients, 35 chloroquine-sensitive isolates and 11 chloroquine-resistant iso-lates were obtained.
If we suppose that types 2 and 3 (early RI)ACR responses should be chloroquine-resistant, dis-cordant results between the therapeutic response andin vitro response are observed in three type 2 ACR-patients and 11 type 1 ACR-patients. Of the type 2patients, two were children and one was adult. Onechild had a chloroquine-sensitive isolate with dimin-ished in vitro sensitivity (81 nmol/l). In the otherpatients, there seem to be no obvious reasons forthe failure to clear parasitaemia, other than possibleindividual variations in the chloroquine pharmacoki-netics, unreported vomiting, and, most importantly,reappearance of asexual parasites due to reinfection.Type 1 patients were clinically and parasitologicallycured on day 14. A total of 35 patients with chloro-quine-sensitive isolates were cured, as expected, while11 patients were cured despite the presence of chlo-roquine-resistant parasites. The discordance in type1 ACR-patients may also be related to age. Of the11 patients with discordant results (range, 125–486nmol/l), one was aged 6 years, four were aged 11–14 years, and six were adults. Although we have nobiological proof, we hypothesize that discordancemay be related to a high level of acquired immunitythat enhances the clearance of parasites, independ-ently of drug sensitivity.
In contrast, with the ACR group, which con-sisted of several subgroups, fewer discordant casesbetween the therapeutic response and in vitro re-sponse were observed in the treatment failure groups.A total of 24 LTF patients had chloroquine-resist-ant isolates, while five discordant cases of LTF pa-tients (3 children and 2 adults; 3 early RI and 2 earlyRI/RII) were infected with chloroquine-sensitive iso-lates. The situation for three of five LTF patientsmay be analogous to that of three type 2 (early RI)ACR patients who responded with asymptomaticparasitaemia on day 7 and/or day 14, despite thepresence of chloroquine-sensitive isolates. Two of fivediscordant LTF patients (a 5-year-old and a 7-year-old) had persistent parasitaemia during the 14-dayfollow-up period despite the presence of chloro-quine-sensitive isolates.
Patients responding with ETF were not easilyclassifiable on the basis of the definitions of RI, RIIand RIII applied to the standard “7-day test” or the“28-day extended test”. Two types of parasitologicalresponses were observed in patients with ETF. Thefirst subset of patients (two children) had a modest
diminution of parasitaemia on day 2 (>25% of thepre-treatment parasitaemia) which was classified asan RIII response according to the criteria set byRieckmann (16), even though follow-up until day 7was not possible due to a requirement for an alter-native treatment on day 3 or day 4. Retrospectively,this classification appeared justified on the basis ofhigh levels of IC
50 values for chloroquine obtained
from the isolates from these patients (373 nmol/land 641 nmol/l). The second subset of patients (3children and 4 adults) in the ETF group wereunclassifiable in the S–RI–RII–RIII system becausean alternative treatment was administered on day 2or day 3 and their parasitological response did notfulfil the criteria for RIII. The response of these sevenpatients was considered to be late RI/RII based ontwo observations. First, compared with the pre-treat-ment levels the mean parasitaemias on day 2 were1.6%, 2.4% (excluding one patient with 180%),3.7%, 7.3% and 56% in the S/late RI, early RI, earlyRI/RII, 7 unclassifiable patients, and RIII groups,respectively. Second, analysis of the distribution ofthe day 2 parasitaemia compared with the initial lev-els showed that the 50th percentiles were, in the sameorder, 0.4%, 1.3%, 1.7%, 3.4% and 51%. Thus,the parasitological response of the seven unclassifiablepatients on day 2 was closest to that of those whoexhibited an early RI/RII response.
Six of seven isolates from ETF patients dis-played high levels of IC
50 for chloroquine (110, 187,
461, 477, 575 and 635 nmol/l). Only one case of invivo/in vitro discordance was observed in the ETFgroup. This patient was a 5-year-old child present-ing with a low-grade fever (37.8 0C) and a positivesmear on day 3 (131 760 asexual parasites per µl onday 0 and 9 asexual parasites per µl on day 3). Thisparticular patient may have been treated too hastilywith an alternative drug on day 3 and probablyshould have been re-examined on day 4 without analternative treatment on day 3. These cases of ETFillustrate the importance and responsibility of theattending clinicians to administer an alternative treat-ment as soon as early clinical deterioration or feverassociated with a positive smear is observed on orbefore day 3. Although only a small number of ETFcases were observed in our study, the subjective cri-terion of ETF (aggravated clinical condition) doesseem to be supported by parasitological criteria inthe majority of cases and potentially represents mostsevere cases of drug failure.
In vivo testing is an accurate and valid meas-ure of therapeutic efficacy and is the most reliablemeans for detecting drug resistance. Compared within vitro assays, the in vivo test of resistance may beconducted in remote areas by qualified personnelwith minimal training. It also permits working di-rectly with malaria-infected patients, deriving clini-cal data, monitoring clinical response over a shorttime frame, and modifying treatment in case of atherapeutic failure. However, the test is not entirelyfree of potential problems of bias and precision.When therapeutic failure is observed using an in vivo
In vivo and in vitro tests of chloroquine resistance

40 Bulletin of the World Health Organization, 1999, 77 (1)
Research
test, establishment of a causal relationship betweentreatment failure and in vivo drug resistance requiresfurther investigations since various parasite and hostfactors contribute to a therapeutic failure. For ex-ample, factors related to the characteristics and dy-namics of parasite transmission include the presenceof intraerythrocytic parasites with a drug-resistantphenotype on day 0 of the treatment, late emergenceof secondary or tertiary “broods” of parasites fromthe liver after a subtherapeutic level of the drug isattained in the host, and reinfection of the host withnew populations of parasites after drug treatment.Host factors that play an important role in thera-peutic failure include variability in pharmacodynam-ics and pharmacokinetics and the level of acquiredimmunity. There may be other factors that contrib-ute to or delay parasite and fever clearance, such asintrinsic virulence of parasite strains, host geneticfactors unrelated to immunity, concomitant diseasesthat were undiagnosed at the time of patient enrol-ment, and social behaviour of the host (for exam-ple, concomitant self-medication with other classicalantimalarial drugs or traditional herbal medicine).These considerations show that, unless such factorsare excluded, a case of therapeutic failure cannot beattributed to in vivo drug resistance with certitude.These limitations may diminish the precision of thein vivo test and need to be taken into considerationin assessing our findings since they lead to decreasedmeasures of validity of the in vitro test. Furthermore,unless some of the above factors can account for invivo/in vitro discordant cases, the in vitro thresholdfor chloroquine resistance can not be redefined onthe basis of our in vivo data.
In addition to the difficulties in establishing acausal relationship between therapeutic failure andin vivo drug resistance, the revised WHO criteriathemselves may not be appropriate in all cases. Oneof the criteria for treatment failure (aggravation ofclinical conditions requiring an alternative treat-ment) is based on a subjective clinical evaluation thatmay introduce a bias towards an increased propor-tion of “resistant” cases. In our experience, the crite-rion of persistent or recurrent fever on day 3sometimes leads to a wrong classification of patients.When left untreated, some patients with fever andpositive thick film on day 3 (“treatment failure” ac-cording to the WHO classification) cleared the para-sites and became afebrile on day 4 and remained soand aparasitaemic until day 14 (ACR). These casesillustrate the limits of the in vivo test of resistance.Despite these potential shortcomings, the in vivo test(“7-day test”, “28-day extended test”, or simplifiedtest) must be considered to be the only currentlyavailable, valid measure of drug resistance that maybe used to guide national antimalarial drug policy.
In vitro assays may be a more objective methodto detect drug resistance since in vitro tests elimi-nate several host factors that interfere with the clearinterpretation of results, including reinfections, im-munity, pharamacodynamics, and pharmacokinet-ics. In vitro assays are complementary to in vivo tests,
and their results are theoretically more directly asso-ciated with drug resistance (28). However, most spe-cialized laboratories that conduct in vitro assays as aroutine procedure are located far from clinical studysites and require a high level of training and techni-cal capability, transport of blood samples from thefield and sophisticated equipment to perform iso-topic assays. As a result, in vitro assays have beenused to describe the epidemiology of drug resistanceindependently of clinical studies and to screen newcompounds (10, 25–29). Although these two appli-cations of in vitro assays have provided importantinformation, the results of the present study suggestthe usefulness of in vitro assays as a complementarydiagnostic tool for drug resistance but do not sug-gest that the in vitro test can replace the in vivo testin the field.
Another major problem with the in vitro testis the selection of threshold values to classify resultsin terms of sensitivity or resistance. Use of the thera-peutic plasma level as the threshold value is theo-retically plausible but disregards the technicalconstraints of the in vitro culture method (30). Theoptimal conditions for in vitro culture are markedlydifferent from those for in vivo conditions, and in-clude the composition of culture medium, haemat-ocrit (1–2.5% for in vitro, 35–45% for in vivo tests)and proportion of serum (10% for in vitro culture,55–65% for in vivo). Thus therapeutic plasma lev-els may not be appropriate for in vitro parasite growthconditions. Comparison of different clones or labo-ratory-adapted strains of parasites and determina-tion of the limiting drug concentration that producesa response in these reference strains has also beenused to estimate the threshold value. Even if the drugresponse of the original isolate from which a cloneor strain was derived is known, adaptation of para-sites to in vitro conditions alters the original pheno-type and may not reflect the characteristics of theoriginal isolate (31). In addition, threshold valuesdetermined using this method may not be clear-cutfor some isolates obtained in the field because of thepresence of mixed populations of parasites with dif-ferent phenotypes. Thus, although a clone or strainof P. falciparum with well-defined phenotype andgenotype may be useful in laboratory experiments,various in vivo factors preclude direct comparisonbetween in vitro and in vivo conditions; conse-quently, any threshold value for differentiating sen-sitive and resistant isolates may largely remainarbitrary unless large-scale trials are conducted un-der various epidemiological conditions to define si-multaneously in vitro drug sensitivity pattern,genotype, pharmacokinetic parameters and immuneresponse.
At present, chloroquine is still the rationalchoice for the first-line treatment of the majority ofcases of acute, uncomplicated malaria in indigenouspatients in Africa because it is cheap, safe, well-tol-erated, widely available, and highly effective againstP. vivax, P. ovale, P. malariae, and sensitive strains ofP. falciparum. In some endemic areas, however, con-

Bulletin of the World Health Organization, 1999, 77 (1) 41
cern is increasing about in vivo chloroquine-resist-ant cases. The extent of chloroquine resistance there-fore needs to be monitored to guide the rational useof antimalarial drugs in Africa. Both in vitro and invivo tests of resistance have their limitations and inany case do not measure the same biological phe-nomena. Our results show that the in vitro test ofresistance is a complementary tool that is moder-ately concordant with the simplified in vivo test. Theuse of in vitro tests should be limited to researchpurposes to provide baseline data on drug responseand monitor cross-resistance patterns. The in vitrotest cannot replace the in vivo test for therapeuticefficacy and should not play any role in guiding anti-malarial drug policy. Although it may be difficult to
define exactly the criteria for in vivo chloroquineresistance and to fulfil them, especially in the field,a standardized in vivo test based on all available clini-cal and epidemiological information is still the bestavailable means for defining drug resistance withina given epidemiological context. ■
AcknowledgementsWe thank Sister Solange and her nursing and labo-ratory staff at the Nlongkak Catholic missionarydispensary for their valuable aid. This study was fi-nanced by AUPELF-UREF. Leonardo Basco receiveda grant from the UNDP/World Bank/WHO Spe-cial Programme for Research and Training in Tropi-cal Diseases.
In vivo and in vitro tests of chloroquine resistance
Résumé
Comparaison des tests in vivo et in vitro de résistance chez des malades traités à lachloroquine à Yaoundé (Cameroun)La résistance de Plasmodium falciparum à la chloroquinea été décrite dans tous les pays de l’Afriquesubsaharienne. Néanmoins, la chloroquine reste le mé-dicament de première intention pour le traitement del’accès palustre simple dans la plupart des pays afri-cains. L’extension de la résistance à la chloroquine né-cessite une surveillance permanente soit par des testsin vivo, soit par des tests in vitro. Afin de rechercherune concordance entre ces deux types de test, nousavons comparé les résultats du nouveau test d’effica-cité thérapeutique introduit par l’OMS en 1996 à ceuxdu semi-microtest isotopique. Ce nouveau test in vivoest basé sur l’évolution, après un traitement standardpar la chloroquine à 25 mg/kg sur 3 jours, de l’étatclinique et de la parasitémie chez des malades atteintsd’un accès palustre simple à P. falciparum. Les résul-tats sont exprimés en réponse clinique adéquate ou enéchec thérapeutique précoce ou tardif en fonction dela disparition, de l’aggravation, de la persistance ou dela réapparition des signes cliniques, en particulier la fiè-vre, et en fonction de l’évolution de la parasitémie. Lesemi-microtest consiste à étudier la croissance in vitrodes parasites en présence de concentrations croissan-tes de chloroquine (25 à 1600 nmol/l). La croissanceest mesurée par l’incorporation d’hypoxanthine tritiée.Les résultats sont exprimés en concentration inhibitrice50% (CI50) correspondant à la concentration inhibantla croissance de 50% des parasites par rapport à untémoin. Le seuil de résistance pour la chloroquine estfixé à 100 nmol/l. Parmi les 117 malades inclus, 102(87%) ont été suivis pendant 14 jours, et 95 tests invitro réalisés avec les isolats des malades (46 enfants
et 49 adultes) ont pu être interprétés. Cinquante-sept(60%; 28 enfants et 29 adultes) malades ont présentéune réponse clinique adéquate après le traitement à lachloroquine avec une goutte épaisse négative à J14(n = 46) ou avec une parasitémie asymptomatique à J7et/ou à J14 (n = 11). La moyenne géométrique des CI50
des isolats correspondants était de 63,3 nmol/l. Leséchecs thérapeutiques tardifs et précoces ont été ob-servés chez 29 (30,5%) et 9 (9,5%) patients, respecti-vement. La moyenne géométrique des CI50 des isolatscorrespondants était de 173 nmol/l pour les échecs thé-rapeutiques tardifs et de 302 nmol/l pour les échecsthérapeutiques précoces. En considérant le test in vivocomme test de référence, la sensibilité, la spécificité etla valeur prédictive positive du test in vitro étaient de67%, 84% et 86%, respectivement. Le coefficient dekappa mesurant la concordance entre les deux testsétait de 0,48, indiquant un degré de concordance mo-déré. Contrairement au test in vitro, le test in vivo estplus le reflet de l’efficacité thérapeutique de lachloroquine qu’un test mesurant la résistance des pa-rasites. En effet, l’efficacité thérapeutique est fonctionde nombreux facteurs liés à l’hôte et aux parasites. Cesdifférents facteurs peuvent expliquer les 20% de dis-cordance observés entre les tests in vivo et in vitro.Néanmoins, nos résultats montrent que le test in vitroet le test in vivo sont des méthodes d’analyse de larésistance concordantes et complémentaires, mais seulle test in vivo pratiqué chez des malades permet dejuger de l’efficacité d’un médicament antipaludique etd’orienter les traitements antipaludiques dans le cadrede la politique nationale de lutte.
Resumen
Comparación de pruebas de resistencia in vivo e in vitro en pacientes tratados concloroquina en Yaundé (Camerún)La resistencia de Plasmodium falciparum a la cloroquinase ha observado en todos los países del Áfricasubsahariana. Sin embargo, la cloroquina sigue siendo
el medicamento más socorrido para el tratamiento dela infección palúdica no complicada en la mayor partede los países africanos. Se requiere una vigilancia per-

42 Bulletin of the World Health Organization, 1999, 77 (1)
Research
manente de la magnitud de la resistencia a la cloroquinapor medio de pruebas in vivo o in vitro. Con objeto deestablecer una concordancia entre estos dos tipos deanálisis, hemos comparado los resultados del nuevométodo de valoración de la eficacia terapéutica adop-tada por la OMS en 1996 con el semimicroanálisisisotópico. Esta nueva prueba in vivo se basa en la evo-lución del estado clínico y la parasitemia de los enfer-mos afectados por un acceso de paludismo simplecausado por P. falciparum, al cabo de un tratamientoestándar con cloroquina a razón de 25 mg/kg durantetres días. Los resultados se expresan como respuestaclínica adecuada o fracaso terapéutico precoz o tardíoen función de la desaparición, la agravación, la persis-tencia o la reaparición de las manifestaciones clínicas,en particular la fiebre, y en función de la evolución dela parasitemia. El análisis consiste en estudiar el creci-miento in vitro de los parásitos en presencia de concen-traciones crecientes de cloroquina (25 a 1600 nmol/l). Elcrecimiento se mide por la incorporación de hipoxantinatritiada. Los resultados se expresan en concentracióninhibitoria 50% (CI50), correspondiente a la concentra-ción que inhibe el crecimiento del 50% de los parásitosen relación con un testigo. El umbral de resistencia res-pecto de la cloroquina está fijado en 100 nmol/l. De los117 enfermos participantes, 102 (87%) fueron objetode seguimiento durante 14 días y se pudieron interpre-tar 95 pruebas in vitro realizadas con los aislados delos enfermos (46 niños y 49 adultos). Cincuenta y sieteenfermos (60%; 28 niños y 29 adultos) presentaron
una respuesta clínica adecuada después del tratamien-to con cloroquina, con gota gruesa negativa el día 14(n = 46) o con una parasitemia asintomática los días 7y/o 14 (n = 11). La media geométrica de las CI
50 de los
aislados correspondientes fue de 63,3 nmol/l. Se ob-servaron fracasos terapéuticos tardíos y precoces en29 (30,5%) y 9 (9,5%) pacientes, respectivamente. Lamedia geométrica de los CI50 de los aislados corres-pondientes fue de 173 nmol/l para los fracasos tera-péuticos tardíos y de 302 nmol/l para los precoces.Considerando la prueba in vivo como valoración de re-ferencia, la sensibilidad, la especificidad y el valorpredictivo positivo de la prueba in vitro fueron del 67%,el 84% y el 86%, respectivamente. El coeficiente kappa,que mide la concordancia entre las dos pruebas, fue de0,48, lo que indica un grado de concordancia modera-do. Contrariamente a la prueba in vitro, la prueba invivo es más el reflejo de la eficacia terapéutica de lacloroquina que un análisis que permita medir la resis-tencia de los parásitos. En efecto, la eficacia terapéuti-ca depende de muchos factores vinculados al huéspedy a los parásitos. Esos diferentes factores pueden expli-car el 20% de discordancia observado entre las prue-bas in vivo e in vitro. No obstante, nuestros resultadosmuestran que la prueba in vitro y la prueba in vivo sonmétodos de análisis de la resistencia concordantes ycomplementarios, aunque sólo la prueba in vivo reali-zada en enfermos permite juzgar la eficacia de un me-dicamento antipalúdico y orientar los tratamientos enel marco de la política nacional antipalúdica.
References1. International travel and health. Vaccination requirements and
health advice. Geneva, World Health Organization, 1999.2. Turaman C, Basco LK, Le Bras J. Evaluation of therapeutic
efficacy of chloroquine in febrile Guinean children infectedwith Plasmodium falciparum by simplified in vivo test. Bulletinof the World Health Organization, 1992, 70: 477–480.
3. Adagu IS et al. Antimalarial drug response of Plasmodiumfalciparum from Zaria, Nigeria. Transactions of the RoyalSociety of Tropical Medicine and Hygiene, 1995,89: 422–425.
4. Chandenier J et al. Chimiosensibilité in vivo et in vitro dePlasmodium falciparum à Brazzaville (Congo). Cahiers Santé,1995, 5: 25–29.
5. Management of uncomplicated malaria and the use ofantimalarial drugs for the protection of travellers. Geneva,World Health Organization, 1996 (unpublished documentWHO/MAL/96.1075, available upon request from Division ofControl of Tropical Diseases, World Health Organization, 1211Geneva 27, Switzerland).
6. Bruce-Chwatt LJ et al. Chemotherapy of malaria, 2nd ed.Geneva, World Health Organization, 1984.
7. Assessment of therapeutic efficacy for uncomplicatedfalciparum malaria in areas with intense transmission.Geneva, World Health Organization, 1996 (unpublisheddocument WHO/MAL/96.1077 available upon request fromDivision of Control of Tropical Diseases, World HealthOrganization, 1211 Geneva 27, Switzerland.
8. Chemotherapy of malaria and resistance to antimalarials.Report of a WHO Scientific Group. Geneva, World HealthOrganization, 1973 (WHO Technical Report Series, No. 529).
9. Payne D, Wernsdorfer WH. Development of a blood culturemedium and a standard in vitro microtest for field-testing theresponse of Plasmodium falciparum to antifolate anti-malarials. Bulletin of the World Health Organization, 1989,67: 59–64.
10. Desjardins RE et al. Quantitative assessment of antimalarialactivity in vitro by a semiautomated microdilution technique.Antimicrobial agents and chemotherapy, 1979, 16: 710–718.
11. Chulay JD, Haynes JD, Diggs CL. Plasmodium falciparum:assessment of in vitro growth by [3H]hypoxanthineincorporation. Experimental parasitology, 1983, 55: 138–146.
12. Webster HK et al. Antimalarial drug susceptibility testing ofPlasmodium falciparum in Thailand using a microdilutionradioisotope method. American journal of tropical medicineand hygiene, 1985, 34: 228–235.
13. Childs GE, Wimonwattrawatee T, Pooyindee N.Evaluation of an in vitro assay system for drug susceptibility offield isolates of Plasmodium falciparum from southernThailand. American journal of tropical medicine and hygiene,1988, 38: 19–23.
14. Mount DL et al. Adaptations of the Saker-Solomons test:simple, reliable colorimetric field assays for chloroquine andits metabolites in urine. Bulletin of the World HealthOrganization, 1989, 67: 295–300.
15. Warrell DA, Molyneux ME, Beales PF. Severe andcomplicated malaria. Transactions of the Royal Society ofTropical Medicine and Hygiene, 1990, 84: 1–65.
16. Rieckmann KH. Monitoring the response of malariainfections to treatment. Bulletin of the World HealthOrganization, 1990, 68: 759–760.

Bulletin of the World Health Organization, 1999, 77 (1) 43
17. Ringwald P, Bickii J, Basco LK. In vitro activity ofantimalarials against clinical isolates of Plasmodiumfalciparum in Yaoundé, Cameroon. American journal oftropical medicine and hygiene, 1996, 55: 254–258.
18. Ringwald P, Bickii J, Basco LK. Randomised trial ofpyronaridine versus chloroquine for acute uncomplicatedfalciparum malaria in Africa. Lancet, 1996, 347: 24–28.
19. Bickii J, Basco LK, Ringwald P. Assessment of three in vitrotests and an in vivo test for chloroquine resistance inPlasmodium falciparum clinical isolates. Journal of clinicalmicrobiology, 1998, 36: 243–247.
20. Cohen J. A coefficient of agreement for nominal scales.Educational and psychological measures, 1960, 20: 27–46.
21. Fermanian J. Mesure de l’accord entre deux juges. Casqualitatif. Revue épidémiologique et santé publique, 1984,32: 140–147.
22. Schapira A et al. The susceptibility of Plasmodiumfalciparum to sulfadoxine and pyrimethamine: Correlation ofin vivo and in vitro results. American journal of tropicalmedicine and hygiene, 1986, 35: 239–245.
23. Björkman A, Willcox M. In vivo and in vitro susceptibility ofPlasmodium falciparum to sulphadoxine/pyrimethamine inLiberia, West Africa. Transactions of the Royal Society ofTropical Medicine and Hygiene, 1986, 80: 572–574.
24. Petersen E et al. In vitro and in vivo susceptibility ofPlasmodium falciparum isolates from Liberia topyrimethamine, cycloguanil and chlorcycloguanil. Annals oftropical medicine and parasitology, 1990, 84; 563–571.
25. Warsame M et al. Positive relationship between theresponse of Plasmodium falciparum to chloroquine andpyronaridine. Transactions of the Royal Society of TropicalMedicine and Hygiene, 1991, 85: 570–571.
26. Brasseur P et al. Multi-drug resistant falciparum malaria inCameroon in 1987-1988. I. Stable figures of prevalence ofchloroquine- and quinine-resistant isolates in the original foci.American journal of tropical medicine and hygiene, 1992,46: 1–7.
27. Basco LK, Le Bras J. In vitro activity of artemisininderivatives against African isolates and clones of Plasmodiumfalciparum. American journal of tropical medicine andhygiene, 1993, 49: 301–307.
28. Wernsdorfer WH. Epidemiology of drug resistance inmalaria. Acta tropica, 1994, 56: 143–156.
29. Geary TG, Divo AA, Jensen JB. An in vitro assay system forthe identification of potential antimalarial drugs. Journal ofparasitology, 1983, 69: 577–583.
30. Trager W, Jensen JB. Human malaria parasites in continuousculture. Science, 1976, 193: 673–675.
31. Le Bras J et al. Plasmodium falciparum: Drug sensitivity invitro of isolates before and after adaptation to continuousculture. Experimental parasitology, 1983, 56: 9–14.
In vivo and in vitro tests of chloroquine resistance

44 Bulletin of the World Health Organization, 1999, 77 (1)© World Health Organization 1999
Policy and Practice
Towards evidence-based health care reformMikko Vienonen1, Danguole Jankauskiene2 & Arvi Vask3
1 Regional Adviser for Health Services Management, WHO RegionalOffice for Europe, Scherfigsvej 8, 2100 Copenhagen Ø, Denmark(tel: +45 3917 1203; fax: + 45 3917 1870; e-mail:[email protected]).2 Secretary of State, Ministry of Health, Gedimino av. 27, 2600Vilnius, Lithuania.3 Head, Health Department, Ministry of Social Affairs, Gonsiori 29,EE 0100 Tallinn, Estonia.
Health care reform in Europe is discussed in the light of the Ljubljana Charter, with particular reference to progressmade in Estonia and Lithuania.
Voir page 46 le résumé en français. En la página 47 figura un resumen en español.
In 1996 WHO organized a ministerial-level confer-ence in Ljubljana, which was attended by 46 Euro-pean Member States. On the basis of many years ofanalytical work (1), they endorsed the LjubljanaCharter on Reforming Health Care in Europe, statingthat within the European context health care sys-tems should be driven by values (such as human dig-nity, equity, solidarity and professional ethics),targeted on health, centred on people, focused onquality, based on sound financing, and oriented to-wards primary care. Additionally, the Charter iden-tifies as principles for managing change the need todevelop health policy, listen to the people’s opin-ions, reshape health care delivery, reorient humanresources for health care, strengthen management,and learn from experience.
A sceptic might ask: “What is new in theLjubljana Charter?” The main thing is that this wasthe first time that some elements of common knowl-edge about health care reforms had been presentedsimply and clearly in an agreed statement at minis-terial level. Very few politicians would have daredspeak out individually on these matters. Most so-called health care reforms have not focused on healthimprovement at all, and in fact have made thingsworse as far as the general public is concerned. Fi-nancial and administrative adjustments alone are notenough if reform is meant to have the connotationsof improvement and betterment.
First and foremost, health care reform shouldbe about reforming health. This seems to be a state-ment of the obvious, yet health has been losingground in the profound political and economicchanges sweeping through Europe. In most coun-tries the reforms have focused on cost-cutting, whiletoo little attention has been given to their longer-term effects on health.
What has worked...and what hasn’tHealth sector reform is multifaceted and multilay-ered. At one end of the continuum is the adminis-trative and managerial quest for cost containmentto keep health care expenses within sustainable lim-its. At the other end is the individual citizen’s wishto obtain the best possible care. These aspirationsmay seem irreconcilable. However, as citizens ulti-mately pay for health services—whether public orprivate—it is clearly in their interest that money bespent in the most effective and efficient ways.
There is little evidence that cost-containmentstrategies, focused on rationing, competition amonginsurers, or co-payment, have positive economic ef-fects (2). Furthermore, unless attempts to reduce thedemand for health services are accompanied by pro-tective regulations, they may substantially diminishpeople’s access to the services and thus threaten thehealth of populations. Markets are amoral (3). Oneof the drawbacks of health system markets is thathigh-risk groups such as the elderly and chronicallyill can easily be identified and excluded. Strong pub-lic action is required if this is to be avoided.
The reforms that have been best able to im-prove health and reduce costs have concentrated onchanging the behaviour of the providers of healthservices, namely health workers and hospitals. Re-forms focused on the funders of health services, i.e.patients, insurance agencies and the state, have gen-erally been less successful. New managerial roles ofthe state have emerged, including the assessment andmonitoring of the outcomes of reform. Reforms seemto work best when implemented incrementally ratherthan all at once. Evolution is better than revolution.
One of the most difficult questions is how toinvolve the public in decision-making, which tendsto become remote from people’s everyday problems.Every opportunity should be taken to facilitate dia-logue so that decision-makers remain firmly in touchwith reality.
From theory to practiceThe ability to achieve objectives in health systemsdepends on the capacity of policy-makers to respond

Bulletin of the World Health Organization, 1999, 77 (1) 45
flexibly and creatively to the policy environment theyconfront. Cross-national learning about reform ex-periences is an essential element in this process, as isthe adaptation and adjustment of reform mecha-nisms to accommodate local circumstances. Whilethe basic principles of health reform are universallyvalid, their application varies with each country’sneeds and expectations and with the understandingof reform issues by politicians, health professionalsand society as a whole.
Particular difficulties have arisen in Centraland Eastern Europe and the newly independentstates of the former Soviet Union. A major contribu-tory factor has been the deterioration of economiccircumstances, output having declined and with itthe tax base. Failing state enterprises and increaseddemand for compensatory social expenditure hasexacerbated the fiscal burden on most transitionaleconomies. Strong social and economic pressures arebuilding up in many of these countries. The medi-cal profession, moreover, has been very vocal in pro-moting changes that would strengthen the positionof doctors.
The pendulum continues to swing: dissatis-fied with an initial position, policy-makers set outto make fundamental changes, then move in the re-verse direction as the shortcomings and problemsassociated with the changes become apparent. Thecountries of Europe are in various stages of this cy-cle. Several Western European countries are settingout on major experiments. In Northern Europe,where reform began, there has been a substantialretreat from the most radical position, that of mar-ket-oriented incentives, towards the original posi-tion of publicly planned coordination andcooperation. In some of the newly independent statesthere is a tendency to compare today’s extremely dif-ficult conditions with those of the Soviet period,when the health systems as least functioned, and tohesitate about how to proceed.
A health care reform laboratoryBeing small can sometimes be an advantage. In spiteof economic constraints, the Baltic countries havemade remarkable progress in reorganizing theirhealth care delivery and financing systems. Mistakeshave been made, but in the light of themreassessments have been made and corrective meas-ures taken to the extent politically possible.
Estonia and Lithuania have received technicalassistance and material aid from major internationaland donor agencies, and have been closely involvedin WHO networks and engagements, including theanalysis and preparation for the Ljubljana Confer-ence and Charter. This has been an important fac-tor, together with internal motivation anddetermination, in both countries’ progress in healthdevelopment. They have not allowed themselves tobe unduly distracted from the main issues by theplethora of actors who sometimes advocate and, in-
deed, seek to impose their own values and systems.Estonian and Lithuanian health administrators andplanners realized at an early stage that copying oth-ers was not desirable and that quick fixes did notexist. Thus, for instance, up to the present there hasbeen only a moderate degree of privatization ofhealth care institutions. Both countries have givenspecial attention to reform of health care delivery.Lithuania has developed a strong national healthpolicy in collaboration with all major interest groups.In addition to the measures taken in primary care,public health and the pharmaceutical sector, a veryimportant principle was introduced for the remu-neration of inpatient care providers, involving per-formance-related payment (4). This is intended tobe the main tool for increasing the productivity ofhealth care providers. Payments to hospitals are basedon a cost-per-case system, cases being classified in50 diagnostic groups. The number of cases treatedis contractually agreed between each health facilityand the State Patient Fund, a newly established so-cial health insurance system. There is a ceiling onthe total payments that the Fund can make, and ifthe institutions increase their throughput of casesthe cost per case is proportionately reduced.
A new payment system has also been devel-oped for outpatient services in Lithuania. In the firsthalf of the 1990s, there was strong support, espe-cially from physicians, for adopting fee-for-serviceremuneration on the German model. A need wasfelt to increase physicians’ productivity, to improvepatient care, to reduce under-the-table payments,and to increase doctors’ job satisfaction. However,the economic recession and a dramatically reducedpublic health care budget demonstrated the impor-tance of financial affordability and the desirabilityof concentrating on health promotion and healtheducation. WHO drew attention to the disadvan-tages of creating a payment system that rewardedmaximization of the volume of medical servicesaimed at treating illness. The cautious approach wasstrongly supported by WHO and tied in with theprinciples of the Ljubljana Charter. A mixed formulafor payment of physicians was initially agreed on,whereby about 70% consisted of capitation, basedon the number of people on the lists of doctors atthe first-contact level, and additional, clearly speci-fied items were paid for on a fee-for-service basis. Inpractice, however, a system based entirely on capita-tion was adopted in 1997, and the fee-for-servicecomponent is expected to be introduced graduallyas the system develops. Time will show how well thenew scheme performs, but the focus on the deliveryside of services has a much better chance of successthan would be the case if the system were wholly atthe mercy of market forces. This transitional solu-tion does not limit access to health care but doescontain and balance the health care budget.
Estonia has been very active in establishing afunctioning family doctor system. The Departmentof Polyclinic and Family Medicine was set up in theFaculty of Medicine of the University of Tartu, and
Towards evidence-based health care reform

46 Bulletin of the World Health Organization, 1999, 77 (1)
Policy and Practice
a two-year modular training course in general prac-tice was introduced for polyclinic interns, paediatri-cians and surgeons who had worked during theSoviet period. Some 300 family doctors have beentrained and 200 graduate annually. It is expectedthat the country’s requirements in this area will bemet by 2002, when there should be 800 family doc-tors, i.e. one per 1800 inhabitants. A three-year resi-dency programme has been developed in order tosustain the pool.
In 1997 it was decided to set up a family doc-tor system throughout Estonia. This was importantin order to provide working opportunities for thenewly retrained family doctors. With the help of theEuropean Union and substantial WHO involve-ment, a comprehensive plan for rapid transition wasprepared. This consisted of registering patients withindividual family doctors, establishing a new remu-neration system for the doctors, and defining theprofile of work and equipment needed. The aim hasbeen to put primary care at the forefront of the healthcare system. The new arrangements underline therole of the family doctor at the first-contact level.Community care, health promotion and primarycare nursing still need to be strengthened.
In some parts of Estonia the secondary-levelpolyclinics were hostile to the new system. How-ever, the backing of WHO and the influence of theLjubljana Charter made it possible to proceed de-spite the opposition.
The strong backing of all European MemberStates for the Ljubljana Charter has helped to re-turn health itself (rather than economics and poli-tics) to centre stage in the European debate on healthcare reform. WHO’s Regional Office for Europe istaking the lead in working with countries to build
their health care reforms, using the scientific andethical tools that have been jointly developed. Therenewal of the health-for-all policy at both the glo-bal and the regional levels can further strengthenthis movement if health care systems are seen as anessential element and actor, indeed as a change agentin the policy.
The policy pendulum, the difficulties of policytransfer, and the lack of convergence should not leadpolicy-makers to believe that health care reform isfutile or that effective solutions cannot be found.The European experience and the outcome of re-cent supply-side initiatives have demonstrated thathealth care reform can succeed as well as fail, can bemoderate as well as radical, can strengthen primarycare and equity as well as harming them, and canreinforce the moral underpinnings of the welfarestate as well as eroding them.
About 20 European countries have alreadychosen to publicize the Ljubljana Charter. Since1996 the Charter and the analysis associated with ithave been used by health sector politicians, admin-istrators, professional groups and grass-roots organi-zations in support of their arguments with ministriesof finance and, particularly, with proponents of un-restrained privatization. Even WHO is now in a bet-ter position to provide advice to governments onthese matters.
Some countries are clearly benefiting fromputting the Ljubljana Charter into practice whileothers are not yet doing so. For WHO it is vital toconcentrate on the essential issues because the scar-city of resources does not allow action on a widerfront. The Charter can serve as a beacon guidingnavigators across difficult waters but is no substi-tute for an experienced crew and a sturdy vessel. ■
En 1996, l’OMS a organisé une conférence ministérielleà Ljubljana au cours de laquelle la Charte de Ljubljanasur la réforme des services de santé en Europe a étéapprouvée; cette Charte stipule que dans le contexteeuropéen, la réforme des systèmes de santé devait êtreguidée par certaines valeurs (dignité humaine, équité,solidarité et éthique professionnelle), être axée sur lasanté, centrée sur l’individu, inspirée par un souci dequalité, être financièrement viable et orientée vers lessoins de santé primaires. Il est également ressorti quela gestion du changement est en fin de compte l’épreuvedécisive de toute réforme. D’un côté, il y a cette ten-dance, dictée par des impératifs administratifs et ges-tionnaires, à réduire les coûts; de l’autre, il y a l’individuqui souhaite obtenir les meilleurs soins possibles. Il nesemble guère que le fait d’insister sur le rationnement,la concurrence entre compagnies d’assurance ou le co-paiement ait des effets positifs sur les réductions decoût, et à moins d’être accompagnées de mesures deprotection, ces dispositions risquent fort de menacer lasanté des populations. Les réformes qui ont le mieux
réussi à améliorer la santé et à réduire les coûts sontcelles qui se sont attachées à modifier les comporte-ments des agents de santé et du personnel hospitalier.
Les petits Etats de l’Europe centrale et de l’Estsont devenus des «laboratoires de réformes du secteurde la santé». L’Estonie et la Lituanie, deux petits Etatsbaltes, se sont particulièrement concentrés sur la ré-forme des prestations de santé. La Lituanie a su se do-ter d’une politique de santé nationale efficace et aentrepris des réformes touchant les soins de santé pri-maires, la santé publique et le secteur pharmaceutique.Les sommes perçues par les hôpitaux sont calculées surune base forfaitaire par cas et la rémunération des gé-néralistes repose sur la capitation, contrairement auxrecommandations des groupes de pression médicauxqui étaient favorables à la rémunération à l’acte. L’Es-tonie a instauré un système national d’assurance-ma-ladie obligatoire pour la population et non sélectif etnon concurrentiel pour les compagnies d’assurance. Lemédecin de famille est considéré comme le pivot dufutur système de soins de santé en Estonie, ce pays ayant
Résumé
Vers une réforme des systèmes de santé fondée sur des faits concrets

Bulletin of the World Health Organization, 1999, 77 (1) 47
Towards evidence-based health care reform
judicieusement mis en place des cours de formationuniversitaire de haut niveau à l’intention des généralis-tes. Dans un deuxième temps, un réseau de médecinsde famille a été créé et une méthode de rémunérationmotivante faisant appel au système national d’assu-rance-maladie a été mise en place. Les hôpitaux et lespolycliniques du niveau secondaire, hostiles à ce nou-veau système qui menaçait leur autorité, ont tenté degagner le public à leur cause. Mais le Gouvernementestonien est attaché à la réforme des soins de santéprimaires, et les réformes progressent avec le concoursde l’OMS.
Les exemples de l’Estonie et de la Lituanie mon-trent les difficultés pratiques que pose la gestion deschangements. Administrateurs et responsables politi-ques nationaux peuvent être largement aidés par desinstruments internationaux comme la Charte deLujbljana et aussi par l’analyse que l’OMS peut fairedes autres réformes en cours : un moyen pouvant atté-nuer les effets de balancier inutiles qui, régulièrement,entachent les réformes du secteur de la santé des paysde l’Europe centrale et de l’Est.
Resumen
Hacia una reforma de la atención de salud basada en pruebasEn 1996, la OMS organizó una conferencia de nivelministerial en Liubliana que adoptó la Carta de Liublianasobre la reforma de la atención de salud en Europa, enla que se declara que en el contexto europeo los siste-mas de atención sanitaria deben estar guiados por va-lores (como la dignidad humana, la equidad, lasolidaridad y la ética profesional), enderezados a lasalud, centrados en las personas, focalizados en la cali-dad, basados en una sólida financiación, y orientadoshacia la atención primaria. También se llegó a la con-clusión de que la gestión del cambio es la prueba deci-siva de toda reforma. En un extremo de la cadena sehalla el empeño a nivel administrativo y gerencial porcontener los costos, y en el otro el deseo de cada ciu-dadano de obtener la mejor atención posible. Hay po-cos indicios de que la insistencia en el racionamiento,la competencia entre aseguradores o los sistemas decopago tenga un efecto positivo en la contención decostos, y de no estar acompañadas por reglamentacio-nes de protección, esas medidas pueden constituir unagrave amenaza para la salud de la población. Las refor-mas que con mayor éxito han permitido mejorar la sa-lud y reducir los costos se han concentrado en el cambiodel comportamiento de los trabajadores de la salud ylos hospitales.
Los pequeños países de Europa central y orientalse han convertido en «laboratorios de la reforma de laatención de salud». Estonia y Lituania, dos pequeñosEstados bálticos, han otorgado especial atención a lareforma de la prestación de asistencia sanitaria. Lituaniaha elaborado una sólida política sanitaria nacional yreformado la atención primaria, la salud pública y elsector farmacéutico. Los hospitales cobran según el
costo por caso y los médicos generalistas son remune-rados por lo común conforme al sistema de capitación,contrariamente al deseo de los grupos de presión mé-dicos que propugnaban un método basado en el pagopor servicios prestados. Estonia estableció un sistemade seguro nacional de salud que no permite a los ase-guradores la opción de retiro ni la competencia paraapoderarse de las mejores partes de mercado. El médi-co de familia se considera una pieza fundamental delfuturo sistema de atención de salud de Estonia, que hacomenzado a construirse a partir de la base adecuada,a saber, estableciendo una formación universitaria dealto nivel para los especialistas en medicina general.En la segunda fase de la reforma, se creó una red demédicos de familia y se instauró un sistema de remu-neración atractivo mediante el seguro nacional de sa-lud. Los hospitales y policlínicas de nivel secundario hanconsiderado esta evolución como una amenaza parasu antigua hegemonía y han tratado de ganarse al pú-blico. Sin embargo, el Gobierno de Estonia está com-prometido con la reforma de la APS y, con el apoyo dela OMS, las reformas siguen adelante.
Los ejemplos de Estonia y Lituania muestran lodifícil que es en la práctica la gestión del cambio. Paralos políticos y administradores nacionales pueden seruna considerable ayuda las declaraciones de consensointernacionalmente acordadas, como la Carta deLiubliana, lo mismo que los elementos concretos queaporte el análisis de las reformas en curso que estárealizando la OMS. Esto puede atenuar el innecesarioefecto péndulo, que tan habitualmente acecha a lasreformas de la atención de salud en Europa central yoriental.
References1. Saltman RB, Figueras, J. European health care reform;
analysis of current strategies. Copenhagen, World HealthOrganization Regional Office for Europe, 1997 (WHO RegionalPublications, European Series, No. 72).
2. Saltman RB, Figueras, J. On solidarity and competition: anevidence-based perspective. Eurohealth, 1996, 2 (4): 19–20.
3. Evans RG. Health care reform: who’s selling the market andwhy? Journal of public health medicine, 1997, 19 (1): 45–49.
4. Cerniauskas G, Murauskiene L. Reforming the healthservices in Lithuania. In: Proceedings of a workshopon Reforming the Health Services in the Baltic Countries,22 August 1996. Copenhagen, Danish Institute for HealthServices Research and Development (DSI report 97.08, 1997:63–73).

48 Bulletin of the World Health Organization, 1999, 77 (1)
The Ljubljana Charter on Reforming Health Care18 June 1996
Preamble1. The purpose of this Charter is to articulate a setof principles which are an integral part of currenthealth care systems or which could improve healthcare in all the Member States of the World HealthOrganization in the European Region. These prin-ciples emerge from the experience of countries im-plementing health care reforms and from theEuropean health for all targets, especially thoserelated to health care systems.
2. This Charter addresses health care reforms in thespecific context of Europe and is centred on the prin-ciple that health care should first and foremost leadto better health and quality of life for people.
3. The improvements in the health status of thepopulation are an indicator of development in thesociety. Health services are important, but they arenot the only sector influencing people’s wellbeing:other sectors also have a contribution to make andresponsibility to bear in health, and intersectoralitymust therefore be an essential feature of health carereform.
4. In cognizance of this, we the Ministers of Health ortheir representatives from the European Member Statesof WHO (participants in the Ljubljana Conference)hereby pledge ourselves to promote the following prin-ciples and call upon all citizens and urge all govern-ments, institutions and communities to join us in thisendeavour. We further request the WHO Regional Of-fice for Europe to take the necessary action to supportMember States in giving effect to these principles.
Fundamental principles5. Within the European context, health caresystems need to be:
5.1 Driven by valuesHealth care reforms must be governed by principlesof human dignity, equity, solidarity and professionalethics.
5.2 Targeted on healthAny major health care reform should relate to cleartargets for health gain. The protection and pro-motion of health must be a prime concern of allsociety.
This document does not confer legal rights
5.3 Centred on peopleHealth care reforms must address citizens’ needs tak-ing into account, through the democratic process,their expectations about health and health care. Theyshould ensure that the citizen’s voice and choice de-cisively influence the way in which health servicesare designed and operate. Citizens must also shareresponsibility for their own health.
5.4 Focused on qualityAny health care reform must have as its aim – andinclude a clear strategy for – continuous improve-ment in the quality of the health care delivered, in-cluding its cost-effectiveness.
5.5 Based on sound financingThe financing of health care systems should enablesuch care to be delivered to all citizens in a sustain-able way. This entails universal coverage and equita-ble access by all people to the necessary care. That,in turn, requires the efficient use of health resources.To guarantee solidarity, governments must play acrucial role in regulating the financing of health caresystems.
5.6 Oriented towards primary health careReforms, with primary health care as a philosophy,should ensure that health services at all levels pro-tect and promote health, improve the quality of life,prevent and treat diseases, rehabilitate patients andcare for the suffering and terminally ill. They shouldreinforce joint decision-making by the patient andcare provider and promote the comprehensivenessand continuity of care within their specific culturalenvironments.
Principles for managing change6. The following principles are keys to managingchange effectively:
6.1 Develop health policy6.1.1 Health care reform should take place as acoherent part of an overall policy for health for allwhich is consonant with the socioeconomic condi-tions of each country. This policy development pro-cess needs to be based on a broad consensus involvingas many relevant social actors as possible.
6.1.2 Major policy, managerial and technical deci-sions on development of the health care systemshould be based on evidence where available. Re-forms must be continuously monitored and evalu-ated in a way that is transparent to the public.
Policy and Practice
Bulletin of the World Health Organization, 1999, 77 (1) 49
6.1.3 Governments must raise value-related issuesfor public debate and ensure equitable distributionof resources and access of the entire population tohealth services. They should also take facilitatinglegislative and regulatory initiatives. Whenever mar-ket mechanisms are appropriate, they should favourcompetition in ensuring quality and in using scarceresources.
6.2 Listen to the citizen’s voice and choice6.2.1 The citizen’s voice and choice should makeas significant a contribution to shaping health careservices as the decisions taken at other levels ofeconomic, managerial and professional decision-making.
6.2.2 The citizen’s voice should be heard on issuessuch as the content of health care, contracting, qual-ity of services in the provider/patient relationship,the management of waiting lists and the handlingof complaints.
6.2.3 The exercise of choice and of other patients’rights, requires extensive, accurate and timely infor-mation and education. This entails access to pub-licly verified information on health services’performance.
6.3 Reshape health care delivery6.3.1 Self care, family care and other informal care,as well as the work of a variety of social institutions,need to be brought closer together with the formalhealth care services. This requires continuous com-munication and appropriate referral and informa-tion systems.
6.3.2 Well designed strategies are needed to shiftworking capacity from acute hospital care to pri-mary health care, community care, day care andhome care, whenever necessary.
6.3.3 Regional health service networks need to bereinforced insofar as they are more cost-effective,allow for a better organization of the response tomedical emergencies and facilitate cooperation be-tween hospitals and with primary health care.
6.3.4 Continuous quality development in healthcare requires information systems based on selectedquality indicators that can be abstracted from rou-tine work and fed back to individual physicians,nurses and other health care providers.
6.4 Reorient human resources for health6.4.1 In the health services, greater attention needsto be paid to identifying and stimulating appropri-ate professional profiles that can be part of the multi-professional teams of tomorrow’s health care systems.
6.4.2 There is a need for a broader vision than thatof traditional curative care in the basic training, spe-cialization and continuing education of health carepersonnel. Quality of care, disease prevention andhealth promotion should be an integral part of train-ing.
6.4.3 Proper incentives should be introduced toencourage health personnel to be more conscious ofquality, cost and outcomes of care. Professional andpayment organizations should cooperate activelywith health authorities to promote such a develop-ment.
6.5 Strengthen management6.5.1 There is a need to develop a set of manage-rial functions and public health infrastructures en-trusted with the tasks of guiding or influencing theoverall system to achieve the desired improvementsin the population’s health.
6.5.2 Individual health care institutions shouldenjoy the maximum possible autonomy in manage-ment of their resources consistent with the princi-ples of an equitable and efficient health care system.
6.5.3 Management development needs to bestrongly promoted by strengthening individual ca-pacities to lead, negotiate and communicate and bydeveloping institutional tools to deliver health caremore effectively and efficiently.
6.6 Learn from experience6.6.1 There is a need to promote the national andinternational exchange of experience with imple-menting health care reform and supporting reforminitiatives.
6.6.2 This support must be founded on a well vali-dated knowledge base with regard to health care re-forms, with cross-cultural differences in health carebeing properly understood and appropriately valued.
Towards evidence-based health care reform

50 Bulletin of the World Health Organization, 1999, 77 (1)
Policy and Practice
Prizes for weight lossLois Englberger1
1 UNICEF Health and Nutrition Adviser, P.O. Box 2299, Kolonia,Pohnpei 96941, Federated States of Micronesia (tel: 691 320 7359;fax: 691 320 6386; e-mail: [email protected]). Formerly NutritionAdviser to the Central Planning Department of the Government ofTonga.
The Kingdom of Tonga, in the South Pacific, has apopulation of about 100 000 spread over six mainisland groups. Until relatively recently the peopleate mainly root crops, fish, other seafood, variouskinds of meat, coconut, fruit and vegetables, butincreasing quantities of fatty and refined foods arenow being consumed. Moreover, most people usedto do agricultural work involving considerable physi-cal activity, and walking was common as there werefew motor vehicles, whereas today there are moreoffice jobs than formerly, and motorized vehicleshave become comparatively common, resulting in agreat decrease in physical exercise.
In 1986, 39% of women and 10% of men wereobese, having body mass indices of $ 30 and $ 32respectively (1). The Body Mass Index is defined asweight (in kilograms) divided by height (in metres)squared, expressed as kg/m2. There was a fourfoldincrease in annual admissions of diabetic patients atVaiola Hospital between 1971 and 1991 (2). A dia-betics unit was established in 1994 to tackle the in-creased prevalence of diabetes and diabeticcomplications.
A Health and Weight Awareness Programmewas initiated in 1995 by the Tonga National Foodand Nutrition Committee, together with nationalweight loss competitions lasting six or four months.This project, which is being implemented by theNutrition Unit of the Central Planning Department,endeavours to make losing weight and gaining fit-ness an enjoyable experience.
Activities and administrationA Tongan translation of the South Pacific Commis-sion’s weight chart has been prepared, in which forboth sexes the cut-off point in body mass index valueis 27 for overweight and 32 for obesity (3). The chartis used to identify obesity and overweight and todetermine eligibility for the competitions. Adviceleaflets have been prepared which give simple guide-
lines for losing weight and starting a fitness pro-gramme (see box).
Equipment for measuring height and weighthas been obtained and a network of weigh stationshas been established. The rules for the competitionsrequire that participants be weighed monthly at des-ignated centres and that weight loss be gradual. Inthe first competition, prizes were awarded solely inrespect of total weight loss. Subsequently, the addi-tional categories of “reaching healthy weight-for-height” and “maintaining weight loss” wereintroduced. Special attention has been given to theneed for gradual and maintained weight loss.
Each weigh station is equipped with a heightmeasure, scales, a registration book, a weight-for-height poster, diet and exercise advice leaflets, ahealthy foods poster, hypertension leaflets and a com-petition flier with information on the rules, prizesand other matters. Some weigh stations are intendedonly for use by the personnel of the organizationswhere they are set up, for instance banks, whereasothers are open to the general public in the hospital,post office, some main government offices, andchurch and community groups.
Each weigh station has a manager who carriesout weighing and recording on a voluntary basis inaddition to her or his basic duties. When possible,measurements are also made of blood pressure andbody fat percentage. The managers attend meetingsat which training is provided on the measurement
© World Health Organization 1999
A programme of weight loss competitions and associated activities in Tonga, intended to combat obesity and thenoncommunicable diseases linked to it, has popular support and the potential to effect significant improvementsin health.
Voir page 52 le résumé en français. En la página 52 figura un resumen en español.
Advice on diet and exercise• Set one weight loss goal per month and one for the
duration of the competition.
• A good result is a weight loss of between 0.5 kg and1 kg per week.
• Draw up an exercise programme lasting 30–60 minutesa day.
• Eat fish, seafood, green leaves and root crops; consumereduced amounts and take three meals a day.
• Choose snacks of fresh fruit or vegetables.
• Eat less fatty, sugary and salty foods.
• Form a weight-losing group among family or friends;weigh yourselves and take exercise together.
• Think positively!

Bulletin of the World Health Organization, 1999, 77 (1) 51
of weight and height, uniformity of record-keepingis encouraged, interest is stimulated, and experiencesare shared.
Difficulties have arisen in connection with thecare and maintenance of scales; some scales have beenbroken, and it is necessary for some to be shared bydifferent stations. Either beam balances or electronicscales are used; both are satisfactory except that in afew cases it is not possible to weigh people becausethey exceed the scales’ capacity of 140 or 150 kg. Toeliminate the problem of variability between scales,each participant is required to be weighed only atone weigh station for the duration of a competition.
The project is publicized through local televi-sion, newspapers and, predominantly, radio, thismedium being used to advertise the competitions asenjoyable activities. The regular radio programmesof the Ministry of Health and the Tonga NationalFood and Nutrition Committee feature the compe-titions, and press releases are issued for the localweekly newspapers. Interviews with persons whohave succeeded in losing weight and with others in-volved in the programme stimulate much interestin the community. In the international press, spe-cial interest has been shown in what are the firstnational competitions of their kind in the world.This has lent further encouragement and has helpedto secure resources for the programme.
Exercise is encouraged as an important part ofthe weight loss competitions. Aerobics classes havebeen initiated in community groups, and an aero-bics programme has been introduced in primaryschools. The health educators of the Ministry ofHealth have been trained to give instruction in thisfield.
Special attention is given to walking as a formof exercise that can easily be incorporated into thedaily routines of people of all ages. A monthly walk-for-health programme has been started in whichmembers of the public participate in walks of eightkilometres, advance notice of which is given in themass media. Occasionally, printed T-shirts are of-fered as incentives to participate. Between 50 and200 people take part each month on the mainisland, and walks are also organized in the outerisland groups. People are also encouraged to workin gardens and agricultural plots and to engage inphysical tasks in their homes.
Local businesses have provided attractiveprizes, including overseas and domestic air tickets,cash, sports shoes and T-shirts. A local airline hasoffered a $ 10 discount on an air ticket for every kgof weight loss. Various government and nongovern-mental offices make their premises and staff avail-able so that the weigh stations can function.
The support of King Taufa’ahau Tupou IV hasgreatly boosted the programme. His weight loss of70 kg over 20 years has provided an important ex-ample of what can be achieved. In 1997 he initiateda healthy lifestyle programme in which people areencouraged to:
• have healthy diets;• take adequate exercise;• practise moderation in the consumption
of alcohol;• refrain from using tobacco and other drugs.
The King presents prizes at ceremoniesattended by dignitaries and participants in thecompetitions. Fitness displays are presented andwords of encouragement and acknowledgement aredelivered.
AchievementsThe total weight lost by the 983 participants in thefirst competition was 1168 kg, and that lost by the1313 people in the second competition was 1335 kg.Both of these competitions lasted six months. Thepercentages of participants who completed thesecompetitions were 33% and 50% respectively; 229and 367 individuals succeeded in losing weight. Thethird competition lasted only four months becauseof staff changes; 57% of the 1133 participants com-pleted it and 361 lost a total of 1143 kg.
A survey of 140 participants conducted ninemonths after the end of the second competition re-vealed that 69% of them had regained some or all ofthe weight lost. Nevertheless, the maintenance ofweight loss by 31% was a worthwhile achievement.It is hoped that the prize category “maintainingweight loss” will encourage participants to keep theirweight down.
It is hoped that a greater understanding ofTongan cultural values and attitudes concerningfood, eating, exercise and body size (4), and of theirrelevance to health programmes, will help to resolvethe obesity problem. In this connection it is note-worthy that:• more obesity occurs among girls than boys;• girls tend to be less positive than boys about
healthy food and exercise;• fatalistic views exist about health conditions;• health programmes tend to be too prescriptive.
The weight loss programme in Tonga is mak-ing a positive contribution towards combating obes-ity and associated noncommunicable diseases. Thereare difficulties connected with equipment, culturalvalues and attitudes, and weight gain following thecompetitions. Nevertheless, there is great public in-terest in the programme and a strong demand for itsactivities. ■
AcknowledgementsThe author warmly acknowledges the contributionsof: Mrs Vizo Halavatau, Ms Yoshiko Yasuda and MsRisa Yamazaki, other coordinators of the competi-tions; Mr Paula Lavulo, Director of Planning andChairman of the Tonga National Food and Nutri-tion Committee, and other members of this Com-
Prizes for weight loss

52 Bulletin of the World Health Organization, 1999, 77 (1)
Policy and Practice
mittee; the weigh station managers; the TonganMinistries of Health, Education and Agriculture; andother governmental and nongovernmental groups.Acknowledgement is also made to the New Zealandand Australian Governments, the United NationsChildren’s Fund, the South Pacific Commission, the
World Health Organization, the Japanese OverseasCooperation Volunteers, and local and overseas busi-nesses, for support with funding, the mass aware-ness campaign, technical expertise, and prizes.Finally, appreciation is expressed of the leadershipgiven by His Majesty King Taufa’ahau Tupou IV.
Résumé
La perte de poids récompenséeAux Tonga, un programme, associant des concoursd’amaigrissement et d’autres activités connexes pourcombattre l’obésité et les maladies non transmissiblesqui en découlent, recueille l’adhésion de la populationet pourrait contribuer à améliorer sensiblement la santé.
Ces dernières années, le régime alimentaire etles modes de vie des quelque 100 000 habitants duRoyaume des Tonga dans le Pacifique Sud ont subi deschangements profonds à l’origine de problèmes desanté. En 1986, 30% des femmes et 10% des hommesétaient obèses et le nombre des diabétiques était enforte hausse. Pour y remédier, le Comité national del’Alimentation et de la Nutrition des Tonga a organiséen 1995 des concours d’amaigrissement s’étalant surquatre ou six mois. Le projet, mis en oeuvre par l’Unitéde la Nutrition du Département de la Planification cen-trale, s’efforce de rendre la perte de poids et la remiseen forme aussi agréables que possible.
Chaque mois les participants se rendent aux cen-tres de pesée mis en place pour suivre l’évolution deleur poids. Lors de l’inscription, on enregistre pour cha-que personne sa taille et, si possible, sa tension arté-rielle et son pourcentage de masse grasse. Le règlementdes concours souligne que la perte de poids doit êtreprogressive. Traduite en tongan, la table des poids de laCommunauté du Pacifique précise que les seuils utili-sés pour définir les excès de poids sont un indice deQuételet de 27 pour le surpoids et de 32 pour l’obésité,ce qui permet de reconnaître les sujets en excès pondé-ral et les sujets obèses. Des directives sur la perte depoids et la remise en forme, des brochures sur l’hyper-tension et des affiches vantant les mérites d’une ali-mentation saine ont été produites. Ces concours
encouragent l’exercice, les cours d’aérobic et la mar-che, cette dernière occupant une place d’autant plusprivilégiée qu’elle peut être facilement intégrée dansles activités quotidiennes des personnes de tous âges.
Pour récompenser les lauréats, des entrepriseslocales ont offert des prix attrayants, un geste qui n’afait qu’accroître la popularité du projet. Le soutien duRoi Taufa’ahau Tupou IV a dynamisé le programme, saperte de poids de 70 kg en 20 ans donnant un aperçudes résultats qui pouvaient être obtenus. Le Roi a parti-cipé aux cérémonies de remise des prix et lancé un pro-gramme en faveur d’un mode de vie sain où l’onencourage les individus à adopter un régime alimen-taire équilibré, à faire suffisamment d’exercice, à boireavec modération et à s’abstenir de fumer et de prendredes drogues. Sur les trois concours organisés entre 1995et 1997, la perte de poids totale par concours oscillaitentre 1168 kg et 1335 kg, le nombre de participantspar concours allant de 983 à 1133. Le prix principalrécompensait la perte de poids totale. Toutefois, d’autresprix sont également venus récompenser ceux qui avaientatteint leur poids de santé par rapport à leur taille, etqui étaient parvenus à le maintenir.
Il faut espérer qu’une meilleure compréhensiondes valeurs culturelles et des comportements aidera àrésoudre le problème de l’obésité et favorisera plusencore l’adoption d’un régime alimentaire équilibré etla pratique d’un exercice. Le programme rencontre cer-tains difficultés, dont la reprise de poids des partici-pants à l’issue des concours. Mais l’intérêt populaireque le programme et ses activités suscitent est grand,ce qui laisse espérer une amélioration sensible de lasanté.
Resumen
Concursos de adelgazamientoEn Tonga, un programa de concursos de adelgazamientoy actividades conexas ideados para combatir la obesi-dad y las enfermedades no transmisibles asociadas aésta goza de apoyo popular y ofrece la posibilidad demejorar significativamente la salud.
El Reino de Tonga, situado en el Pacífico Sur, tie-ne unos 100 000 habitantes. En años recientes la ali-mentación y el modo de vida de esta población hancambiado enormemente y ello ha generado problemasde salud. En 1986, el 30% de las mujeres y el 10% delos hombres eran obesos; además, ha aumentado mu-cho el número de diabéticos. En 1995, el Comité Na-
cional de Alimentación y Nutrición de Tonga ha inicióuna serie de concursos nacionales de adelgazamientode seis o cuatro meses de duración cada uno. El pro-yecto, aplicado por la Unidad de Nutrición del Departa-mento Central de Planeamiento, se concentra enprocurar que el adelgazamiento y el mantenimiento deun buen estado físico sean actividades agradables.
Se ha establecido una red de puestos de controldel peso a los que acuden mensualmente los partici-pantes para pesarse. En el momento de la inscripciónen el concurso se determinan la altura y, en lo posible,la presión arterial y el porcentaje de grasa corporal de

Bulletin of the World Health Organization, 1999, 77 (1) 53
los participantes. El reglamento del concurso hace hin-capié en que el adelgazamiento debe ser gradual. Laversión tongana de la tabla de la Comisión del PacíficoSur relativa al peso corporal distingue entre el excesode peso y la obesidad, definiendo el exceso de peso apartir de un índice de masa corporal de 27 y la obesi-dad a partir de un índice de 32. Se han preparado di-rectrices para adelgazar y mejorar el estado físico,folletos sobre la hipertensión y carteles sobre los ali-mentos saludables. Como parte del concurso de adel-gazamiento se fomentan el ejercicio físico, las clases deaeróbica y la formación de grupos de caminantes. Serecomiendan en especial las caminatas porque se pue-den incorporar fácilmente en la actividad cotidiana acualquier edad.
Las empresas locales han donado premios atrac-tivos para los ganadores y ello ha aumentado la popu-laridad de los concursos. El apoyo del Rey Taufa’ahauTupou IV ha dado un gran impulso al programa; el Reymismo perdió 70 kilos en 20 años y constituye un ejem-plo de lo que es posible conseguir. Ha participado enlas ceremonias de entrega de los premios y ha iniciado
un programa de fomento de un modo de vida sanomediante el cual se alienta a la gente a comer alimen-tos sanos, hacer suficiente ejercicio físico, beber conmoderación y abstenerse del tabaco y de las drogas. Encada uno de los tres concursos organizados entre 1995y 1997 se perdieron un total de 1168 a 1335 kg y elnúmero de participantes por concurso osciló entre 983y 1133. Mientras que la principal categoría premiadafue la de pérdida total de peso, también se entregaronpremios al logro de un peso saludable para la altura yal mantenimiento de la pérdida de peso.
Se confía en que, mediante una comprensión másprofunda de los valores y actitudes culturales, se ayu-dará a resolver el problema de la obesidad y a promo-ver más activamente la alimentación saludable y elejercicio físico. Aunque se tropieza con dificultades, porejemplo el aumento de peso de los participantes unavez finalizado el concurso, el programa ha despertadoun gran interés popular y sus actividades, que son ob-jeto de una demanda firme, pueden mejorarsignificativamente la salud.
Prizes for weight loss
References1. Maclean E et al. The 1986 National Nutrition Survey of the
Kingdom of Tonga. Technical Report. Noumea, South PacificCommission, 1987.
2. Ministry of Health, Tonga, 1995 (unpublished data).
3. Look fit, be healthy weight-for-height chart. South PacificCommission, 1993.
4. Tupoulahi C. Sociocultural antecedents of obesity amongTongan adolescents [Ph. D thesis]. Flinders University, SouthAustralia, 1997.
54 Bulletin of the World Health Organization, 1999, 77 (1)
Round Table
Animal-to-human organ transplants – a solutionor a new problem?A.S. Daar1
1 Professor and Chairman, Department of Surgery, College ofMedicine, Sultan Qaboos University, Sultanate of Oman; andVisiting Professor in Health Policy and Society, Faculty of Law andJoint Center for Bioethics, University of Toronto.
The current definition of xenotransplantation in-cludes the grafting of cells, tissues or organs fromnon-human animal species into humans (althoughtechnically it can be the other way round or betweenany two species). It is obviously a subject that hasfascinated people for a long time because we findexamples of this kind of organ grafting in themythologies of many religions. Perhaps the one bestknown is the grafting of the head of an elephantonto the body of the boy who went on to becomethe very popular Hindu god, Ganesha. The fascina-tion seems now to have reached fever pitch, withhigh stakes for those concerned, particularly patients,scientists, the biotechnology industry, and infectiousdisease specialists. We seem to be poised on the brinkof clinical success, but with advocates on oppositesides of the argument about whether we are ready toembark on large-scale clinical trials of vascularizedwhole organs or not. In this presentation I will tryto capture the main elements that have brought usto this pass, where we have a division between “thosewho want to get it right” and “those who want toget it right now” (1).
Short historyIn modern biomedicine there have been efforts atxenotransplantation dating back to the early part ofthis century, well before we knew anything aboutthe immunological principles underlying transplan-tation in general. Most of these efforts have failed,although in one of Keith Reemtsma’s patients in the1960s a chimpanzee kidney did survive and workfor about nine months (2); we do not know whythis success occurred, as there were no powerful im-munosuppressive agents in the 1960s, and no so-
phisticated immunological or genetic manipulationsof donor or recipient. Table 1 is a summary of thesetransplants.
In the very modern era, which I will define asanything after 1980, we have had a number of well-publicized whole-organ (vascularized) xenotrans-plant attempts, as well as several less-publicizedcellular and tissue transplants. These provide us withan opportunity to examine and define the issues ofcurrent concern in xenotransplantation.
Sources of discomfortThere are many issues that make people uncomfort-able about xenotransplantation. At a very fundamen-tal level it seems to transgress those boundaries whichdefine us as human, and so challenge and threatenour identity and sense of order; the sense of orderand disorder, according to some anthropologists, isthe very basis of our entire cognitive world.
In some Eastern mythologies we do have acertain amount of fluidity between the human andanimal categories, with movement in both directions.It may be tempting to speculate on this basis thatthese cultures would easily assimilate xenotrans-plantation, but it can also be argued that this veryfluidity might make people anxious to maintainclearly distinct categories in the physical world.
In the Islamic and Judaeo-Christian traditionsthe concerns are easy to identify, and fundamentalamongst them is the question of morality: man isheld accountable because he has choice and respon-sibility. Is this responsibility as a moral agent reducedif one’s functioning depends on a foreign organ? Willthe characteristics of the animal be incorporated intothe consciousness of the human recipient? Of course,at present, there is no scientific evidence with whichto answer such questions, but as we begin to trans-plant pig neural tissue into the human brain anddemonstrate neuronal connection between the two
© World Health Organization 1999
Xenotransplantation is seen by some mainly as an opportunity and by others mainly as a danger. It could helpovercome the shortage of organs from human donors, but it raises a number of questions, particularly aboutsafety, ethics and human nature. This article reviews the progress of research, debate and decision-making in thisarea.
Voir page 59 le résumé en français. En la página 59 figura un resumen en español.
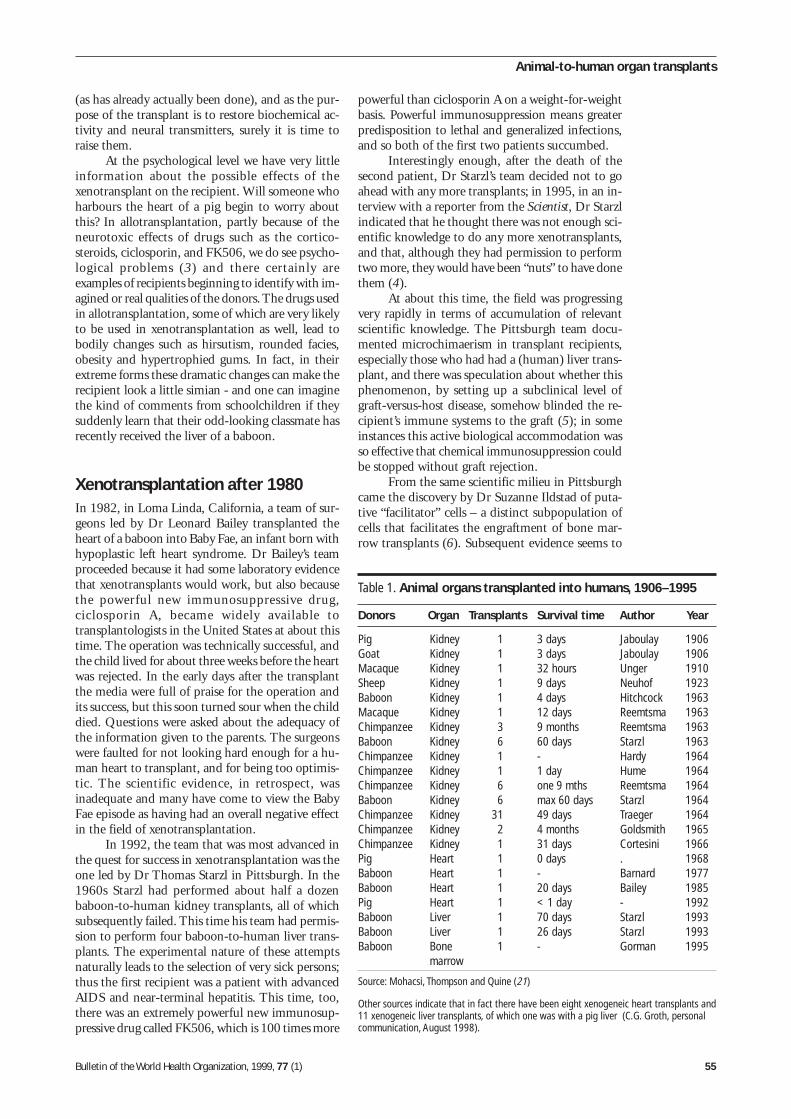
Bulletin of the World Health Organization, 1999, 77 (1) 55
powerful than ciclosporin A on a weight-for-weightbasis. Powerful immunosuppression means greaterpredisposition to lethal and generalized infections,and so both of the first two patients succumbed.
Interestingly enough, after the death of thesecond patient, Dr Starzl’s team decided not to goahead with any more transplants; in 1995, in an in-terview with a reporter from the Scientist, Dr Starzlindicated that he thought there was not enough sci-entific knowledge to do any more xenotransplants,and that, although they had permission to performtwo more, they would have been “nuts” to have donethem (4).
At about this time, the field was progressingvery rapidly in terms of accumulation of relevantscientific knowledge. The Pittsburgh team docu-mented microchimaerism in transplant recipients,especially those who had had a (human) liver trans-plant, and there was speculation about whether thisphenomenon, by setting up a subclinical level ofgraft-versus-host disease, somehow blinded the re-cipient’s immune systems to the graft (5); in someinstances this active biological accommodation wasso effective that chemical immunosuppression couldbe stopped without graft rejection.
From the same scientific milieu in Pittsburghcame the discovery by Dr Suzanne Ildstad of puta-tive “facilitator” cells – a distinct subpopulation ofcells that facilitates the engraftment of bone mar-row transplants (6). Subsequent evidence seems to
(as has already actually been done), and as the pur-pose of the transplant is to restore biochemical ac-tivity and neural transmitters, surely it is time toraise them.
At the psychological level we have very littleinformation about the possible effects of thexenotransplant on the recipient. Will someone whoharbours the heart of a pig begin to worry aboutthis? In allotransplantation, partly because of theneurotoxic effects of drugs such as the cortico-steroids, ciclosporin, and FK506, we do see psycho-logical problems (3) and there certainly areexamples of recipients beginning to identify with im-agined or real qualities of the donors. The drugs usedin allotransplantation, some of which are very likelyto be used in xenotransplantation as well, lead tobodily changes such as hirsutism, rounded facies,obesity and hypertrophied gums. In fact, in theirextreme forms these dramatic changes can make therecipient look a little simian - and one can imaginethe kind of comments from schoolchildren if theysuddenly learn that their odd-looking classmate hasrecently received the liver of a baboon.
Xenotransplantation after 1980In 1982, in Loma Linda, California, a team of sur-geons led by Dr Leonard Bailey transplanted theheart of a baboon into Baby Fae, an infant born withhypoplastic left heart syndrome. Dr Bailey’s teamproceeded because it had some laboratory evidencethat xenotransplants would work, but also becausethe powerful new immunosuppressive drug,ciclosporin A, became widely available totransplantologists in the United States at about thistime. The operation was technically successful, andthe child lived for about three weeks before the heartwas rejected. In the early days after the transplantthe media were full of praise for the operation andits success, but this soon turned sour when the childdied. Questions were asked about the adequacy ofthe information given to the parents. The surgeonswere faulted for not looking hard enough for a hu-man heart to transplant, and for being too optimis-tic. The scientific evidence, in retrospect, wasinadequate and many have come to view the BabyFae episode as having had an overall negative effectin the field of xenotransplantation.
In 1992, the team that was most advanced inthe quest for success in xenotransplantation was theone led by Dr Thomas Starzl in Pittsburgh. In the1960s Starzl had performed about half a dozenbaboon-to-human kidney transplants, all of whichsubsequently failed. This time his team had permis-sion to perform four baboon-to-human liver trans-plants. The experimental nature of these attemptsnaturally leads to the selection of very sick persons;thus the first recipient was a patient with advancedAIDS and near-terminal hepatitis. This time, too,there was an extremely powerful new immunosup-pressive drug called FK506, which is 100 times more
Table 1. Animal organs transplanted into humans, 1906–1995
Donors Organ Transplants Survival time Author Year
Pig Kidney 1 3 days Jaboulay 1906Goat Kidney 1 3 days Jaboulay 1906Macaque Kidney 1 32 hours Unger 1910Sheep Kidney 1 9 days Neuhof 1923Baboon Kidney 1 4 days Hitchcock 1963Macaque Kidney 1 12 days Reemtsma 1963Chimpanzee Kidney 3 9 months Reemtsma 1963Baboon Kidney 6 60 days Starzl 1963Chimpanzee Kidney 1 - Hardy 1964Chimpanzee Kidney 1 1 day Hume 1964Chimpanzee Kidney 6 one 9 mths Reemtsma 1964Baboon Kidney 6 max 60 days Starzl 1964Chimpanzee Kidney 31 49 days Traeger 1964Chimpanzee Kidney 2 4 months Goldsmith 1965Chimpanzee Kidney 1 31 days Cortesini 1966Pig Heart 1 0 days . 1968Baboon Heart 1 - Barnard 1977Baboon Heart 1 20 days Bailey 1985Pig Heart 1 < 1 day - 1992Baboon Liver 1 70 days Starzl 1993Baboon Liver 1 26 days Starzl 1993Baboon Bone 1 - Gorman 1995
marrow
Source: Mohacsi, Thompson and Quine (21)
Other sources indicate that in fact there have been eight xenogeneic heart transplants and11 xenogeneic liver transplants, of which one was with a pig liver (C.G. Groth, personalcommunication, August 1998).
Animal-to-human organ transplants

56 Bulletin of the World Health Organization, 1999, 77 (1)
Round Table
have borne out its existence in animal models. DrIldstad suggested in 1995 that a baboon-to-humanbone marrow transplant could be used to cure a pa-tient with advanced HIV infection. She did not per-form this experiment in Pittsburgh, but was able tocollaborate with clinicians and scientists at the Uni-versity of California, San Francisco. The recipientwas a 38 year-old AIDS activist from Oakland, Cali-fornia, called Jeff Getty, who was himself sufferingfrom AIDS and was not expected to live long; thetheory was that if his marrow was partly reconsti-tuted by that of a baboon (to develop chimaerism),he would be much improved because baboonlymphocytes are not infectable with HIV.
This is a very instructive episode in the annalsof xenotransplantation from a number of differentperspectives which illustrate the current issues ofconcern in the field. From the regulatory point ofview in the United States, the freewheeling days whenany surgeon could transplant an organ from an ani-mal with the permission only of the local Institu-tional Review Board were over. All such experimentsnow required a specific Initial Notification of Drugapplication to the US Food and Drugs Administra-tion (FDA). The field was new, and so the FDA setup a panel to review the application. Arguments infavour of proceeding were that this was a valid ex-periment, that the scientific justification was ad-equate, and that if the experiment was not done inthe United States it would be done elsewhere, andthe United States would lose out. The opposing ar-guments were that the risk of infection from knownand unknown viruses in the baboon bone marrowwas just too high to ignore, and that contacts andthe public might be exposed to a risk whose extentwas unquantifiable.
Two things influenced the decision to proceed:one was the powerful lobbying from Getty’s family,and of course from the scientists and clinicians whowere advocating the transplant. The other was thepersuasive argument that the patient was likely todie anyway, and so the risk of spread of infectionwould be minimal. The transplant went ahead, andalthough it did not succeed in terms of engraftmentof the bone marrow, it did succeed in terms of mak-ing the patient better (higher T-cell count, generalwell-being in the months after the transplant). Threeyears later he is alive, apparently in fairly good health,and writing and speaking on behalf of experimentsusing animals, especially in HIV infection (7).
Increased awareness of risk ofinfectionThe emphasis in discussion of xenotransplantationhas changed from concern about the rights and wel-fare of potential non-human source animals to con-cern about the risk of xenozoonoses. One of severalthings that brought this change about was a letterpublished by Dr Jonathan Allan and about 40 otherscientists, including a number of virologists, who
pointed out the real dangers of infection from non-human primates (8). The authors of the letter andothers again reminded us that, almost certainly, HIVcame from simian sources, and that the incubationperiod of retroviruses can be many years before anyclinical symptoms are manifest. We were also re-minded that if these infections were transmitted tothe recipient, they could be rapidly lethal because ofthe heavy immunosuppression, and could also betransmitted, theoretically, to immediate contacts andeven to the public.
This widely publicized letter was written inresponse to the draft guidelines for reduction of therisk of xenozoonoses published by the Public HealthServices (9), a federal umbrella body which encom-passes both the FDA and the Centers for DiseaseControl and Prevention (CDC) in the United States.The main point of the Allan letter was that theseguidelines were not strict enough, that the risk ofinfection from non-human primates was realenough, and that we should therefore embargo theuse of primates completely.
The Public Health Service draft guidelineswere also criticized by other organizations, includ-ing the American Society of Transplant Physicians.The criticisms included the vagueness of the docu-ment regarding the funding of the regulatory instru-ments and, again, its failure to exclude the use ofprimates.
GuidelinesIn 1994 and 1995 something stirred those concernedwith ethics and public policy in both Europe andthe United States. In January 1995 in the UnitedKingdom the Nuffield Council on Bioethics set upa Working Party to look at many xenotransplant is-sues and it produced a report, which came out in1996 (10). Subsequently the United KingdomGovernment’s Advisory Group on the Ethics ofXenotransplantation examined a similar range of is-sues and came up in 1997 with the definitiveKennedy Report (11), named after its admirablycapable chairman, Professor Ian Kennedy.
The essence of the Kennedy Report was thatit was worth pursuing xenotransplantation research,and that using pigs, but not non-human primates,as source animals would be ethically acceptable.Furthermore, it was ethically acceptable to alter thepig’s genome to the extent foreseen so as to facilitatethe transplant, provided the pig remained recogniz-ably a pig. Primates could ethically be used only asrecipients, in small numbers, in animal-to-animalexperiments.
Non-human primates were not ethically ac-ceptable as source animals partly because of theemotional attachment that human beings have tothem, and partly because their being phylogeneticallycloser to man increases the risk of infection. In com-parison to the pig, there were other disadvantagessuch as their depletability, slow breeding, small lit-

Bulletin of the World Health Organization, 1999, 77 (1) 57
ters, and the fact that there are no specified-patho-gen-free (SPF) colonies of primates, while there aresuch SPF colonies of pigs. These factors also meanthat the cost of breeding non-human primates forxenotransplantation would be prohibitive. Further-more, the organs of primates are often too small forhumans.
The pig, on the other hand, has lived close toman for many generations without spreading anyserious infections (leaving aside the swine-flu epi-demic); its physiology is quite similar to man’s; itsorgans are roughly the same size; it breeds veryquickly, has large litters, and in any case is eaten bymillions of people throughout the world. The mat-ter of physiology, however, is not yet really resolved– particularly for major synthesizing organs such asthe liver, which would be pouring out pig moleculesinto the human recipient’s circulation. Also, notmuch is known about the response of these organsto normal homoeostatic signals. This is a subject thathas not received the attention that it really deserves(12).
The most significant conclusion of theKennedy Report was that the base of scientificknowledge was inadequate in 1997 to proceed toclinical trials, and that there should be an effectiveembargo until a formal regulatory authority was es-tablished, with an opportunity to review the evidenceat the time of submission of any applications to it.The Government of the United Kingdom rapidlyresponded by setting up the Xenotransplant InterimRegulatory Authority under the Chairmanship ofLord Habgood.
In the United States the consultation processwas initiated by the Institute of Medicine, whichheld a workshop in June 1995, and its report waspublished in 1996 (13). Its conclusions differed fromthe Kennedy Report’s in that non-human primateswere not excluded as source animals, and the scien-tific base was considered to be adequate to “proceedwith caution” to clinical trials. The American ap-proach was emphatically to have an advisory, not aregulatory, body to deal with xenotransplantation.
International consultationBy 1997 it was obvious that there was a risk to thepublic’s health, that the magnitude of this risk wasnot really known and was perceived differently bydifferent countries, and that there were a number ofethical, social and cultural ramifications toxenotransplantation. There was a distinct need foran international and interdisciplinary dialogue. TheWorld Health Organization responded to this glo-bal challenge by convening a consultation in Ge-neva in October 1997. Participants included expertsfrom several countries in Europe, as well as fromCanada, Cameroon, Japan, Oman, the Philippines,Sri Lanka and the United States. The main tasksgiven to the consultation were to work out techni-cal and ethical guidelines to minimize the risk of
infection, safeguard human dignity and humanrights, and ensure animal welfare.
Despite the apparent differences of approachand perceptions amongst the participants, the con-sultation was very successful, and formulated a uni-fied set of recommendations. One of the points thatbecame clear was that if xenotransplantation didsucceed, developing countries might well be amongthe main beneficiaries. This is because in most ofthe developing world organ replacement therapiessuch as haemodialysis are beyond the means of gov-ernments or individuals, and organ transplantation,especially through cadaveric donation of organs, hasnot really taken off. For many of these countries, atthe current level of expenditure, allotransplantationnecessarily has lower priority than basic public healthneeds. Here, xenotransplantation holds out the hopethat one day, when the ethical, technical, infectiousdisease and cost problems have been resolved, de-veloping countries will be able to embark on thistype of transplantation without having to divert toomuch of their scarce resources to it. The fundamen-tal need for international cooperation in research,communication and standardization was recognized.The report of the WHO Consultation was issued inFebruary 1998 (14).
Cellular and tissue xenotransplantsIn 1993 a Swedish team transplanted 10 diabeticpatients with pig islets of Langerhans. None of themsucceeded in producing pig insulin in the long term,but the experiment is nevertheless important becausethe future of xenotransplantation may well lie in suchcellular transplants for very common conditions suchas diabetes mellitus. The other significant outcomeof this experiment was important data on the pres-ence or absence of risk of viral infection. All 10 ofthe patients have developed antibodies to pig viruses,some to the influenza virus and some to picorna-virus. According to the Swedish team, none of thepatients has actually become sick with any pig vi-ruses, and they believe that there is a possibility thatthe antibodies may simply be cross-reactive (AnneTibell, personal communication, 1998).
Neural tissue transplants have been performedfrom pig to man to alleviate Parkinson disease andmore recently for intractable epilepsy. One of thepatients treated for Parkinson disease died of othercauses; a post mortem examination showed connec-tions had developed between the pig neural tissueand his brain — answering a critically importantbiological question, but at the same time raisingphilosophical and theological questions about thebrain, identity and responsibility.
Summary of current statusThe field is moving very rapidly. There are a numberof important stakeholders, and the stakes are highfor some of them. Major research is now being
Animal-to-human organ transplants

58 Bulletin of the World Health Organization, 1999, 77 (1)
Round Table
funded and carried out by venture-capitalized bio-technology companies, and one of the considera-tions in the current discussions is the part played bythese companies in determining the timing, the tech-nology and the development of xenotransplantationas a whole.
There is a distinct difference in the approachesto xenotransplantation in Europe and the UnitedStates. In Europe the feeling is that the scientificbase is inadequate to proceed to clinical trials and sothere is at present an effective embargo. In the UnitedStates the consensus seems to be that further labora-tory and animal-to-animal experiments will not an-swer the key questions, and that the only way toadvance the scientific base is to “proceed with cau-tion” (15) to clinical trials. In the United States,therefore, while the Public Health Services draftguidelines are becoming more strict in response tocomments, criticisms and consultations, the Foodand Drug Administration has been receiving appli-cations. It has already authorized a number of clini-cal trials, most of which at present involve cells andtissues rather than whole vascularized organs, al-though a number of researchers are preparing forthe latter. Furthermore, rather than completely ex-cluding the use of non-human primates, the ap-proach in the United States is to set the requirementsfor their use at levels that are virtually impossible toachieve. This effectively embargoes their use with-out actually using the dreaded term.
The question of consent to the clinical trials,especially in the early patients, is likely to be a vexedone. We have argued (16) that some of the funda-mental traditional principles of consent would needto be violated, and that because of the continuingneed to monitor the patient and perform invasiveinvestigations even if the graft failed, the agreementmay need to be more of a contract, with specificallybinding requirements, than the traditional consentwhereby the patient has the right to withdraw at anytime from the experiment. Since the community isin a sense being put at risk, there is a real argumentfor considering some form of community consentas well – but at present, with our inability to quan-tify the xenozoonotic risk (to calculate the risk–ben-efit ratio), it is not clear how far we should push thispoint. In any case, there is little experience in ob-taining such community consent.
On the purely scientific side, the evidence hasaccumulated rapidly on both sides of the divide. Onthe one hand, our understanding of the hyperacuterejection phenomenon is increasing, and scientificenquiry is already being directed to the subsequent“delayed xenotransplant reaction”. More and moreanimal models are being developed; and immuno-logical manipulations are becoming more sophisti-cated. Animal models have been developed which
no longer express on their endothelium the alpha-gal molecule, which is the main target of the anti-bodies mediating the hyperacute rejection response.Also, transgenic animals have been developed whichexpress on their endothelium human molecules suchas the decay-accelerating factor, which helps to in-activate complement components in a species-specific manner.
At the same time, however, we have growingevidence of viruses, in pigs and in primates, whichcan theoretically cause xenozoonotic infection. Newpig endogenous retroviruses, which would be verydifficult to eradicate and which have been shown toinfect human cell lines in vitro have been described(17). While it is fair to say that there is little evi-dence that such viruses will be pathogenic in man,it cannot be assumed that they will not become so,especially if introduced into an immunocompro-mised host. Evidence has also accumulated of trans-species transmission of viruses from pig to man,causing infection, for example, with paramyxovirusin Australia (18), and in the case of primates we nowknow that the simian foamy virus (and other viruses)can be transmitted via scratches and bites to animalhandlers (19).
The effect of xenotransplantation on the do-nation of cadaveric and living-donor human organsneeds to be taken into account. Xenotransplantationitself can be seen as serving one of several purposes:to be a complete substitute for human organs; tosupplement human organs, thus alleviating short-age; or to be “bridging” rather than “destination”organs. Whatever the purpose, it would be a set-back if the effect was to reduce the supply of humanorgans because the public now perceives a lack ofneed since pigs are plentiful, or for whatever otherspeculative reasons (20). We think that xenotrans-plants will be very expensive in the first decade oftheir application, and so, for at least this reason, theywill not be an adequate substitute for allotransplan-tation for at least a decade after xenotransplanatationis truly established.
One major issue for developing countries isthe phenomenon of “expatriate” experiments: it ispossible that, because of restrictions imposed in in-dustrialized countries, researchers may bring theseexperiments to be done in developing countries, withpotentially disastrous results in terms both of safetyand of human rights. This is only one of the reasonsfor which developing countries need to be repre-sented in formulating guidelines for this exciting,challenging and potentially useful new technology.Attempts are now being made to predict factors thatwould affect the response of the public toxenotransplantation (20), but surveys of public atti-tudes are beset by deficiencies and are cumulativelycontradictory at present (21). ■

Bulletin of the World Health Organization, 1999, 77 (1) 59
Résumé
Les xénogreffes : solution ou problème ?déjà suffisantes pour «procéder avec prudence» à desessais cliniques. Il était également recommandé de créerun organe consultatif (et non de réglementation) afinde veiller à ce que soient prises toutes les précautionsnécessaires. En 1997, l’OMS a organisé une consulta-tion internationale à l’issue de laquelle un certain nom-bre de recommandations ont été formulées, quisoulignaient, entre autres, le besoin d’une coopérationinternationale aux fins de la recherche, de la communi-cation et de la standardisation des principes directeursvisant à réduire le risque de transmission desxénozoonoses non pas simplement chez les receveursmais aussi chez leurs contacts et dans la population engénéral.
Des greffes de cellules et de tissus hétérologuespour le traitement de maladies courantes comme le dia-bète, la maladie de Parkinson et l’épilepsie ont déjà étéréalisées. Ce type d’opérations a permis de compren-dre certains aspects des xénogreffes, encore que sur leplan clinique, elles n’aient pas donné de résultats pro-bants. En règle générale, lorsque les enjeux sont impor-tants, par exemple, quand des recherches sont financéespar des entreprises de biotechnologie à capital à ris-que, le désir est grand de se hâter pour développer cettetechnologie et procéder à des essais cliniques. Aux Etats-Unis d’Amérique, la Food and Drug Administration adéjà autorisé un certain nombre d’essais cliniques qui,jusqu’ici, concernent des cellules et des tissus et nondes organes vascularisés entiers.
Dans la mesure où le risque d’infection n’inté-resse pas seulement l’individu mais en un sens l’en-semble de la communauté, il serait fondé d’envisagerune forme de consentement de la communauté. A cejour, les enquêtes d’opinion sur les xénogreffes ont étépeu concluantes, voire contradictoires.
Des études récentes ont montré que sur les dixmalades qui avaient reçu il y a quelques années enSuède des îlots de Langerhans de porc, aucun n’a pré-senté de signe d’infection par des rétrovirus endogè-nes porcins. Toutefois, il convient de se rappeler quedes études in vitro ont fait apparaître une infectiositéintercellulaire et que, en tout état de cause, l’absencede preuve d’infection n’est pas une preuve d’absencede risque.
Nous devons poursuivre, mais avec une grandeprudence, notamment parce que le coût des xénogreffessera très élevé au début et que seuls quelques rece-veurs pourront en bénéficier dans les premiers temps.
Animal-to-human organ transplants
Ces dernières années ont été marquées par un regaind’intérêt pour les xénogreffes. Cliniciens, scientifiques,spécialistes de l’éthique, analystes politiques et cher-cheurs ont aujourd’hui des opinions divergentes sur lerisque de transmission des xénozoonoses. Certains veu-lent dès à présent passer à l’acte et procéder à desessais cliniques alors que d’autres, partisans d’une ap-proche prudente, souhaitent d’abord évaluer les risques.Mais presque tous sont d’accord pour que la scienceprogresse dans ce domaine.
Le battage médiatique suscité en 1982 par latransplantation d’un coeur de babouin chez une petitefille «Baby Fae» en Californie, favorable dans un pre-mier temps, s’est rapidement mué en critiques lorsquel’enfant est décédée. Le Dr Thomas Starzl, qui a effec-tué deux transplantations de foie de babouin chezl’homme à Pittsburgh au début des années 90, a dé-cidé après le décès du deuxième patient que des re-cherches supplémentaires s’imposaient avant qued’autres essais cliniques puissent être réalisés. La trans-plantation de la moelle osseuse d’un babouin sur JeffGetty, un patient atteint du SIDA, a échoué du point devue de la greffe mais a été un succès en ce que l’étatdu malade s’est amélioré.
L’inquiétude suscitée par le risque de transmis-sion des xénozoonoses a conduit à exiger que lesxénogreffes fassent l’objet de contrôles d’autant plusrigoureux que le VIH, par exemple, est probablementd’origine simienne et que plusieurs années peuvents’écouler avant que la maladie ne se déclare chezl’homme : un argument venant renforcer le sentimentlargement répandu que les organes de primates nonhumains ne devraient pas être transplantés chezl’homme. Au Royaume-Uni, le rapport Kennedy indiquaiten 1996 que les xénogreffes pourraient êtreéthiquement acceptables si le donneur animal était leporc. Mais le rapport appelait à un moratoire jusqu’àce que soit créé un organe national de réglementationdes xénogreffes qui serait chargé de fixer des normes,d’examiner les demandes d’autorisation d’essais clini-ques et d’étudier au fur et à mesure les données scien-tifiques. Actuellement, tout essai clinique doit fairel’objet d’une demande d’autorisation adressée à l’Or-gane intérimaire de Réglementation des Xénogreffes(Royaume-Uni) qui indiquera au Secrétaire d’Etat à laSanté s’il convient ou non d’accorder cette autorisa-tion. A l’inverse, aux Etats-Unis d’Amérique, le rapportde l’Institut de Médecine, qui date aussi de 1996, aconclu que les données scientifiques disponibles étaient
Resumen
Trasplantes de órganos de animales: ¿solución o nuevo problema?En los últimos años se ha reavivado el interés por losxenotrasplantes. La opinión de los clínicos, especialistascientíficos, expertos en ética, analistas de las políticaspúblicas e investigadores está actualmente dividida enlo que respecta al tema del riesgo de xenozoonosis.
Algunos desean pasar a la acción y empezar ya losensayos clínicos, mientras que otros prefieren ponerprimero en marcha estructuras de evaluación y deminimización de los riesgos. Casi todos, sin embargo,desean ser testigos de avances científicos en ese terreno.

60 Bulletin of the World Health Organization, 1999, 77 (1)
Round Table
A raíz del trasplante de un corazón de babuino aBaby Fae en California, en 1982, la alternativa del xe-notrasplante tuvo gran repercusión pública, al princi-pio positiva, pero más tarde, cuando la niña falleció,negativa. El Dr. Thomas Starzl, quien llevó a cabo dostrasplantes de hígado de babuino a receptores huma-nos en Pittsburgh a principios de los años noventa, lle-gó a la conclusión, tras la muerte de su segundopaciente, de que había que llevar a cabo nuevas inves-tigaciones antes de realizar más ensayos clínicos. El tras-plante de médula ósea de babuino a Jeff Getty, unenfermo de SIDA, fracasó, pero benefició en cierta me-dida al paciente.
La preocupación suscitada por las xenozoonosisha llevado a exigir que se apliquen controles más rigu-rosos a los xenotrasplantes, sobre todo teniendo encuenta la sospecha de que el VIH procede de simios y elhecho de que los retrovirus humanos pueden tardarmuchos años en manifestarse. Ello ha conducido ademása un amplio acuerdo en el sentido de que no debe uti-lizarse a primates no humanos como fuente de órga-nos para el hombre. En el Reino Unido, el informeKennedy (1996) sostenía que el xenotrasplante a partirdel cerdo podía ser éticamente aceptable. En el infor-me, no obstante, se recomendaba aplicar una morato-ria efectiva mientras no se constituyera una autoridadnacional de regulación de los xenotrasplantes que es-tableciera normas, aceptara solicitudes y analizase losprogresos en ese campo de la ciencia. Actualmente, pararealizar cualquier ensayo clínico se debe presentar unasolicitud a la Autoridad Provisional de Regulación delos Xenotrasplantes del Reino Unido, que aconsejará alMinistro de Salud si debe o no dar su autorización. Enlos Estados Unidos, por el contrario, en el Informe delInstituto de Medicina (también de 1996) se resolvía quehabía base científica suficiente para justificar que sepasara «con las debidas precauciones» a realizar en-sayos clínicos. Se recomendaba la creación de un órga-no asesor, más que de un órgano regulador, para velarpor que se observaran las precauciones necesarias. Enuna reunión consultiva internacional organizada por laOMS en 1997 se formularon diversas recomenda-cio-
nes que resaltan la necesidad de cooperación técnicaen materia de investigación, comunicación y normali-zación de directrices a fin de reducir al mínimo el riesgode xenozoonosis, no sólo entre los receptores sino tam-bién entre sus contactos y el público en general.
Ya se han realizado xenotrasplantes de células ytejidos contra enfermedades comunes como la diabe-tes mellitus, la enfermedad de Parkinson y la epilepsia.Esas operaciones han ayudado a profundizar en el cono-cimiento de determinados aspectos de los xenotrasplan-tes, pero aún no han tenido gran trascendencia clínica.En general, cuando es mucho lo que está en juego, porejemplo en las investigaciones financiadas por empre-sas de biotecnología de capital de riesgo, hay gran in-terés en potenciar el desarrollo de esas técnicas y enpasar a realizar ensayos clínicos. En los Estados Uni-dos, la Administración de Alimentos y Medicamentosha autorizado ya varios ensayos de ese tipo, que sinembargo hasta ahora se han realizado sólo con célulasy tejidos, no con órganos enteros vascularizados. Dadoque el riesgo de infección afecta no sólo a los pacien-tes sino, teóricamente, al conjunto de la comunidad,parece lógico que deba preverse algún tipo de consen-timiento informado por parte del público. Los resulta-dos de las encuestas de opinión pública sobre losxenotrasplantes han sido hasta ahora contradictorios yno permiten extraer conclusiones.
Estudios recientes han mostrado que los diezpacientes que recibieron islotes pancreáticos porcinosen Suecia hace unos años no presentan signos de in-fección por retrovirus endógenos porcinos, según losanálisis realizados con las actuales técnicas diagnósti-cas. Sin embargo, debemos recordar que los estudios invitro realizados han revelado signos de infectividad in-tercelular, y que en cualquier caso la inexistencia depruebas no demuestra la inexistencia de riesgos aso-ciados a esos u otros agentes infecciosos.
Es necesario seguir adelante, pero con muchacautela, sobre todo considerando que el costo de losxenotrasplantes sería inicialmente muy alto, y que sóloun reducido número de pacientes podría beneficiarsede ellos en los primeros años.
References1. Daar AS. Xenotransplants: proceed with caution (letter).
Nature, 1998, 392: 11.2. Reemtsma K et al. Renal hetero xenotransplantation in
man. Annals of surgery, 1964, 160: 384–410.3. Franklin P. Psychological aspects of kidney transplantation
and organ donation. In: Morris PJ, ed. Kidney transplantation,principles and practice, 4th ed. Philadelphia, Saunders, 1994.
4. Hoke F As cross-species transplantation moves ahead, somescientists call for caution, restraint. Scientist, 1 August 1995,9 (16): 1.
5. Starzl TE et al. Donor cell chimerism permitted byimmunosuppressive drugs: a new view of organtransplantation. Immunology today, 1993,14 (6): 326–332.
6. Kaufman CL et al. Phenotypic characterization of a novelbone marrow-derived cell that facilitates engraftment ofallogeneic bone marrow stem cells. Blood, 1994,84 (8): 2436–2446.
7. Getty J. The tragic hypocrisy of “animal rights”. Wall St.journal, 1996, 13 June.
8. Allan JS et al. Letter to Beth TW, Food and DrugAdministration, Washington DC, re draft Public Health Serviceguidelines on infectious disease issues in xenotransplantation.Washington DC, Food and Drug Administration, 1996(document No. 96M–0311, available from author on request).
9. Public Health Service. Draft guidelines on infectiousdisease issues in xenotransplantation. Federal register, 1996,61 (185): 49919–49932.

Bulletin of the World Health Organization, 1999, 77 (1) 61
10. Nuffield Council on Bioethics. Animal-to-humantransplants: the ethics of xenotransplantation. London,Nuffield Council on Bioethics, 1996.
11. Advisory Group on the Ethics of Xenotransplantation.Animal tissues into humans. London, Stationery Office, 1997.
12. Hammer C. Xenotransplant physiology. Presented at the NewYork Academy of Sciences / Organisation for Economic Co-operation and Development (OECD) Joint Meeting onTransplantation Biotechnology – a workshop on internationalissues including the use of non-human cells, tissues andorgans. New York, New York Academy of Sciences,18–20 March, 1998.
13. Institute of Medicine. Xenotransplantation: science, ethicsand public policy. Washington DC, National Academic Press,1996.
14. Report of WHO consultation on xenotransplantation. Geneva,World Health Organization, 1998 (unpublished documentWHO/EMC/ZOO/98.2; available from Division of Emerging andOther Communicable Diseases Surveillance and Control,World Health Organization, 1211 Geneva 27, Switzerland).
Animal-to-human organ transplants
15. Salomon DR, Ferguson RM, Helderman JH.Xenotransplants: proceed with caution. Nature, 1998,392: 11–12 (letter).
16. Daar AS. Ethics of xenotransplantation: animal issues,consent and likely transformation of transplant ethics. Worldjournal of surgery, 1997, 21: 975–982.
17. Patience C, Takeuchi Y, Weiss RA. Infection of human cellsby an endogenous retrovirus of pigs. Nature medicine, 1997,3: 282-286.
18. Anon. Pig virus discovery underlies risks for xenotrans-plantation. Nature news, 5 March, 1998.
19. Heneine W et al. Identification of a human populationinfected with simian foamy viruses. Nature medicine, 1998,4(4): 403–407.
20. Daar AS. Analysis of factors for the prediction of the responseto xenotransplantation. Annals of the New York Academy ofSciences, 1998 (in press).
21. Mohacsi PJ, Thompson JF, Quine S. Attitudes toxenotransplantation: scientific enthusiasm, assumptions andevidence. Annals of transplantation, 1998, 3(2): 38–45.

62 Bulletin of the World Health Organization, 1999, 77 (1)
Round Table Discussion
Nonhuman primates as organdonors?Jonathan S. Allan1
Baboons and pigs are potential source animals forhuman xenotransplantation. For practical reasons,baboons have been proposed by only a handful ofUS surgeons to demonstrate “proof of concept”. TheLoma Linda paediatric heart transplant performedby Leonard Bailey in 1986 received a lot of negativepublicity because of ethical concerns about “experi-menting” on a newborn baby. Nevertheless, furtherpaediatric xenografts using baboon hearts are beingplanned (1). Two baboon liver transplants were per-formed in 1993 and they also failed for unknownreasons. This has precluded further liver transplantstudies (2).
AIDS activists helped to accelerate humanxenograft trials in the case of an AIDS patient whoreceived a baboon bone marrow in a high risk at-tempt at immune constitution (3). The monkey bonemarrow failed to grow but the patient derived somebenefit from the conditioning regimen used in pre-paring him for the procedure. This was not an abla-tive bone marrow procedure, so the patient’s ownmarrow remained fully functional. Strong criticismof the experiment, based on a lack of significant sci-entific merit and the potential infectious disease risks,was voiced by many researchers, but in this case pub-lic health policy was determined by pressure fromspecial interests. Some of these pioneering studieshave done more harm than good to thexenotransplantation field because of negative pub-licity. On the other hand, they have made the trans-plant community more aware of the problems, andsteered them towards using nonprimate species.There will always be a handful of individuals whowant to be the first to succeed using primates, how-ever, and this is where strict regulations can preventnew pandemics caused by cross-species infections.
Widespread use of nonhuman primates is nolonger foreseen, mainly because of serious riskscaused by infectious diseases naturally carried bybaboons (4). It is also unlikely that sufficient num-bers of baboons could be made available even withtremendous commitments of time and money. Cur-rently, the largest breeding colony of baboons is atthe Southwest Foundation for Biomedical Research,where there are over 3200 baboons bred for use inresearch. Unfortunately, breeding practices therehave not been developed with zoonotic infections
in mind. For example, virtually all adult baboons inthis colony carry simian foamy virus (SFV) a per-sistent retroviral infection that has recently beenfound in humans who work with primates (5,6). Anovel retroviral infection that can be transmitted tohumans via wounds or needlesticks is not a goodsign. Transplantation of tissues along with a cock-tail of immunosuppressive agents would be an idealway of transferring simian viruses to humans.
Most baboons also harbour simian T-celllymphotropic virus (STLV), another retroviral in-fection that causes leukaemia and T-cell lymphomasin baboons (7). The human form (HTLV) probablyarose from cross-species transmission from non-human primates (8). Higher rates of infection forboth retroviruses and herpesviruses are found in cap-tive colonies than in the wild, indicating that inten-sive breeding may adversely affect the pool ofnonhuman primates. Given the breadth of persist-ent infections, selecting baboons in this milieu wouldnot be good public health practice. In addition, wild-caught baboons are occasionally introduced into thebreeding programme, which could seed the estab-lished colony with new infections.
Furthermore, many viral infections remainnonpathogenic in their existing hosts only to becomepandemics when transmitted to new ones, as wasthe case with AIDS. We are currently unable to pre-dict the outcome of such zoonotic infections in xe-nograft recipients, or to predict in vivo pathogenicityon the basis of in vitro studies. Most problemati-cally, novel agents transmitted by xenotransplan-tation might circulate into the population for sometime before evidence of new clinical syndromescomes to light through changes in disease prevalence.For retroviruses the time between infection and dis-ease can span decades, and many thousands of peo-ple could be infected before a change in diseasepatterns is detected.
Preventing even some of the known infectionscan be expensive. The cost of developing a specific-pathogen-free (SPF) baboon colony, for instance, hasbeen estimated at US$ 20 million, with the first 50animals ready for donation in five to ten years.
Infectious disease risks are not equalMost of the effort and enthusiasm for xenotrans-plantation has centred on pig cells and tissues foruse in humans. Attempts are being made to over-come hyperacute and later rejection, but the ulti-mate goal of such efforts has not yet been defined.Injection of cells or tissues as a temporary measureor for use in bridging studies represents a significantrisk: if the patient survives, the viral passenger cansurvive too, and thus transmission can occur later on.
As has been the case with most whole organ
1 Scientist, Department of Virology and Immunology, SouthwestFoundation for Biomedical Research, 7620 N.W. Loop 410 atMilitary Drive, San Antonio, Texas 78228, USA. E-mail:[email protected]; tel.1(210) 670-3275, fax 1(210) 670-3332.

Bulletin of the World Health Organization, 1999, 77 (1) 63
xenografts, human patients rarely survive for longenough to get back to a way of life that would en-hance transmission. With the advent of cellulartherapies, however, such as those used to treat pa-tients with Parkinson disease, comes the prospect oflong-term survival. Still, here the risk is to some ex-tent limited by the fact that these patients are usu-ally elderly and thus less likely than others to have alifestyle that fosters the spread of sexually transmit-ted pathogens. Also, the infusion of only severalmillion fetal porcine cells reduces the risk of viraltransmission to the patient and the establishment ofinfection. Increasing the “dose” of foreign cells in-creases viral load and might result in a persistentinfection. Studies are in progress on the risk to thepopulation from pig endogenous viruses, and thereis some evidence that these may not be expressed inthe peripheral blood of human recipients of porcinecells (9,10). The same may not be true for immuno-suppressed recipients of whole organs, however.
Are we creating chimeric humans?The possibility that xenotransplantation couldchange human evolution in some profound way hasreceived little attention. The interplay of speciesgenomes through recombinational events stemmingfrom xenotransplantation is a theoretical reality.Retroviruses are in vogue as vectors for shuttlinggenes into patients to treat a variety of genetic dis-eases. More than 200 gene transfer human clinicalprotocols have been registered by the Office ofRecombinant DNA Activities and approved by theFood and Drug Administration. The admixture ofporcine cells and retroviruses produces a favourableenvironment for the transduction of porcine genesby a pig endogenous retrovirus. Several studies sup-port the notion that this retrovirus is infectious inhuman cells (9,10). Theoretically, transduced por-cine cell genes might then be spliced into the hu-man genome when the xenograft recipient is infectedwith a porcine endogenous retrovirus. If thousandsof xenotransplants were to be carried out, this mightfavour the evolution of porcine-human chimeras.
Science fiction may meet reality if a selectiveadvantage arises from some porcine gene such as achemokine, enzyme, oncogene, or chaperone. Theissue of chimerism has been discussed in the con-text of transferring donor lymphoid cells either aspart of the xenograft (leukocyte passengers) or bybone marrow transplantation in an attempt at toler-ance induction (11). Several proposed xenotrans-plants have been designed specifically to incorporatemicrochimerism as an adjunct to the induction oftolerance (12). The use of bone marrow may helpxenotransplantation to succeed, but long-lived for-eign lymphocytes derived from the donor marroware likely to harbour long-lived viruses, increasingthe chances of cross-species infection (13). If publichealth is to be protected, these concerns must be atthe forefront of any discussions on animal speciesand therapeutic modality.
History has taught us that we should restrictanimal transplants to lower nonprimate animals.Even if one were to screen baboons for the knownpathogens, emotionally charged situations, such asthe one that led to the Getty baboon transplant,would be sure to arise. For these reasons, and to avoidthe danger of rogue transplanters dumping primateorgans into humans, we should restrict our effortsin xenotransplantation to safer and more economi-cal donor resources. At a recent meeting sponsoredby the Organisation for Economic Co-operation andDevelopment (OECD) in conjunction with the NewYork Academy of Sciences, there was a clear inter-national consensus in favour of the use of porcinetissues and cells (14). From everyone except a fewUnited States officials, there was strong oppositionto the use of primates for transplants. Since virusesdo not respect national borders, we must hope thatthe US will decide to take a leadership role in plac-ing public health first in this burgeoning field. ■
1. Bailey LL, Gundry SR. Survival following orthotopic cardiacxenotransplantation between juvenile baboon recipients andconcordant and discordant donor species: foundation forclinical trials. World journal of surgery, 1997, 21:943–950.
2. Starzl TE et al. Baboon-to-human liver transplantation.Lancet, 1993, 341: 65–71.
3. Exner BG, Neipp M, Edstad ST. Baboon bone marrowtransplantation in humans: application of cross-speciesdisease resistance. World journal of surgery, 1997,21:962–967.
4. Allan LS. Xenotransplantation and possible emerginginfectious diseases. Molecular diagnosis, 1996, 1(3): 1–8.
5. Broussard SK et al. Characterization of new simian foamyviruses (SFV) from African nonhuman primates. Virology,1997, 237:349–359.
6. Heneine W et al. (1998). Identification of a humanpopulation infected with simian foamy viruses. Naturemedicine, 1998, 4:403–407.
7. Moné J et al. (1992) Simian T-cell leukemia virus type 1infection in captive baboons. AIDS research and humanretroviruses, 1992, 8(9): 1667–1675.
8. Koralnik LL et al. A wide spectrum of simian T-cellleukemia/lymphotropic virus type 1 variants in nature:evidence for interspecies transmission in Equatorial Africa.Journal of virology. , 1994, 68:2693–2707.
9. Patience C, Takeuchi Y, Weiss RA. Infection of human cellsby an endogenous retrovirus of pigs. Nature medicine, 1997,3:282–286.
10. Wilson CA et al. Type C retrovirus released from porcineprimary peripheral blood mononuclear cells infects human cells.Journal of virology, 1998, 72:3082–3087.
11. Starzl TE et al. Chimerism and donor-specific nonreactivity27 to 29 years after kidney allotransplantation.Transplantation, 1993, 55:1272–1277.
12. Greenstein JL, Sachs DH. The use of tolerance fortransplantation across xenogeneic barriers. Naturebiotechnology, 1997, 15:235–238.
13. Allan JS et al. Amplification of simian retroviral sequencesfrom human recipients of baboon liver transplants. AIDSresearch and human retroviruses, 1998, 14:821–824.
14. Allan JS. The risk of using baboons as transplant donors:exogenous and endogenous viruses. Annals of the New YorkAcademy of Sciences, 1998 (in press).
Animal-to-human organ transplants

64 Bulletin of the World Health Organization, 1999, 77 (1)
Round Table Discussion
New problems beget new solutionsA.P.R.Aluwihare1
Professor Daar has made an excellent survey of thevarious issues that arise. Acceptability of the con-cept of xenotransplantation and the sources used indifferent cultural and religious systems is an impor-tant part of the discussion. The right of recipientsto proper information about the risks and the op-portunity involved does not overrule the right ofcommunities to information on the risks involvedfor them, and to the security of knowing that rea-sonable precautions have been taken. The animalsused also must be treated in a humane manner. Theother ethical problems of priorities surroundingtransplantation in general also apply. Now that rapidprogress is being achieved in dealing with the im-mune system problems associated with xenotrans-plantation, and that assurance of the functionalcapability of suitable organs is closer, the many otherissues need continuing and urgent consideration ina pragmatic manner.
Source of organsThe patient has a right to know where an organ wasobtained. However, this might cease to be a religiousor moral issue after a time. Although catgut is ofanimal intestine origin and requires the death of theanimal for its production, it is so ubiquitous that noone objects to its use, and the matter does not evencome up for discussion with patients. Heart valvesof porcine origin, tissues of nonhuman origin storedin tissue banks for use in humans, and hormonesand enzymes of porcine origin are acceptable in manysocieties. In others they are still not acceptable onreligious grounds, but if no alternative were avail-able the reaction might be different. A potential jus-tification for acceptance may be that the complexpreparatory process would “elevate” the material intothe domain of a therapeutic device, and it wouldcease to be porcine. It would have been interestingto know Professor Daar’s views on whether the reac-tions to transplants other than those of whole or-gans might indicate less long-term opposition toxenotransplantation than one might have antici-pated. “Pseudo-rationalization” by societies is notnew. Even where organs are concerned, especiallythose whose antigenic potential is altered by geneticmanipulation, an argument could develop to facili-tate their use on the lines that the organ is no longerporcine but human as it will “take” in a human. Astrong middle-class demand could both facilitate andnecessitate the use of such rationalizations. It is ap-posite to mention that there are now many patentsfor transgenic animals and animal materials.
The major religionsProfessor Daar has mentioned some issues arisingout of religious beliefs; my comments are aimed atsupplementing his.
• In Buddhism where there is belief in reincarna-tion, there could be conflicting views on whetherthe use of a nonhuman organ confers disadvan-tage on the human or advantage on the animal asregards the next birth. This matter has not comeup for discussion, and it is unlikely that any de-bate would have an adverse effect on the use ofanimal organs.
• In Hinduism also, the pantheistic philosophies donot have any direct comment on the concept ofxenotransplantation; the use of organs of bovineorigin could raise a problem similar to the use ofporcine organs in Islam and Judaism. However,here again demand from the middle class is likelyto lead to a rationalization of use in the absenceof other alternatives.
• In the philosophies and religious systems of othersocieties such as China and Japan, where the ex-traction of organs from the brain-dead may bethought by some to be dehumanizing, it is possi-ble that implantation of a nonhuman organ maybe viewed similarly.
Basic ethicsThe basic principles of biomedical ethics such asbeneficence, non-maleficence, autonomy and jus-tice (among others) must apply in this field, both tothe individual and to the community. There is apotential conflict, for example, between the right ofa dying patient to the only available treatment andthe right of the community to avoid being exposedto an unknown and possibly nonexistent threat ofinfection. Such arguments arose in the case of theGetty marrow transplant described by ProfessorDaar.
InfectionIt is not necessary to debate here the whole vitallyimportant issue of the possibility of infection andits avoidance, prevention, monitoring, diagnosis, andcontrol in the individual or community. Suffice itto point out that host-to-donor infection or diseasetransmission has to be and is considered even whenblood transfusion is done and homografts of any kindused. Individual patients and the community have aright to expect that all reasonable precautions aretaken to ensure that such risks are lower than therisks of the illnesses for which the xenotransplantsare being done. That is to say, it is choice of thelesser risk that is required here, rather than absenceof risk.
The non-maleficence principle when appliedto individuals and communities does call for rigourin looking for possible infections. The exposure ofthe widest possible range of human tissue and cellcultures to the cells and extracts from the donoranimal would seem an essential step in such an evalu-
1 Professor of Surgery, Faculty of Medicine, University ofPeradeniya, Sri Lanka, and Human Rights Commissioner of SriLanka.

Bulletin of the World Health Organization, 1999, 77 (1) 65
ation. It might be argued that if no infection or in-festation in such tissue or cell culture (neither ofwhich has any immune competence) occurs, theninfection of the general population, whose immunesystems are normal, is much less likely than infec-tion in a host whose immune system is suppressed.The xenotransplant also has to be protected frominfection by the host’s organisms; in this respect graftsfrom gnotobiotic animals may be more susceptible(as the whole animals are) to such infection thangrafts from normal animals.
Issues of rights and resourcesThe question of priority of rights arises when deter-mining how health resources are used, and weigh-ing the need for community services against that ofexpensive therapeutic procedures. Xenotransplant-ation would be very expensive, and involve the di-version of resources from activities with a muchhigher cost–benefit ratio. Diversion even from ef-forts at increasing the availability of cadaver organsmight occur. It would be appropriate for the workto be done only in a few centres until reduction ofcosts as a result of better methodology or economiesof scale is anticipated. In the transplant field thechoice of patients in a situation of donor shortage isdone by various methods, including the ability topay for the organ or for the procedure. The choicemay be between xenotransplantation or nothing ini-tially. The category of treatment a patient would beoffered would require the same kind of ethical bal-ancing act doctors face at present. It would be un-fortunate if xenotransplants were regarded asavailable only to “the poor” (who would ironicallyalso be the least able to afford them) and the alter-native of live donor or cadaver organs were reservedfor the rich because it was perceived as “better”.
RestrictionsThe restrictions imposed on a patient fall into twocategories. In the first they would be to protect thepatient. The ethics and rights of this are no differ-ent from those that apply in the case of, say, patientswho need total body radiotherapy or have had mas-sive chemotherapy or immune suppression. In thesecond they would be to protect the community.Such restrictions might be justified, or they may beterribly wrong – as was the way in which those withleprosy were ostracized in the recent past. In the eventof an unforeseen epidemic it is conceivable that quar-antine of a community could be required. Action ofthis kind is not new, but has not been used for dec-ades. It would have to be taken at government level.In the matter of transplant ethics it is imperativethat each country be allowed to make its own ethi-cal decisions – guided by other countries’ experi-ence. In the case of organ procurement from otheranimals, international codes regarding some aspectsof preventing the risk of infection would have toapply. The “mad cow” problem provides a good il-lustration of the need for thoughtfully and imagi-natively formulated stringent controls.
Rights of disadvantaged patientsFrom historical precedent we can expect that termi-nally ill prisoners or poor people, who need trans-plantation but have no hope of access to the bestcurrently available, may be asked to be guinea pigsfor xenotransplantation. However, the quantity andtypes of drugs needed, the kinds of suffering thatmay occur, the kinds of restrictions it may be neces-sary to impose on patients, as well as many otherparameters, remain unknown. The rewards for thepatient, even if health were restored, may be small.Are the rights of the community to have access tonew treatments such that the rights of these indi-viduals can be overlooked? Or should such experi-ments be seen rather as fulfilling the individual’s rightto any treatment that might offer some hope? ■
Putting the public at riskFritz H. Bach1
Of the many important points discussed by Daar, Ishall address only one: the ethical issues raised bythe fact that xenotransplantation will put the publicat risk of an infectious epidemic. My emphasis onthis one point should not detract from other ethicalconcerns related to xenotransplantation. I have beenand continue to be in general agreement with Daar’swritings and comments regarding xenotransplant-ation. This one area I shall discuss from my ownperspective.
The possibility that xenotransplantation, suchas from pigs to humans, could lead to an infectionthat spreads to the human population, possibly notunlike the AIDS epidemic, is generally accepted.Earlier in 1998, we wrote an article suggesting thata moratorium be declared on clinical trials involv-ing xenogeneic organs, tissues and cells that involvesuch a risk (1). That moratorium, we felt, should bein place until the public has been informed aboutthe risk to which it will be exposed if xenotransplan-tation proceeds, and has had an opportunity to par-ticipate in a meaningful way in making the decisionon whether and how to proceed.
This is not different from Daar’s view. He states“Since the community is in a sense being put at risk,there is a real argument to consider some form ofcommunity consent.” The suggestion for public in-volvement in the decision-making process is analo-gous to “informed consent” as it is obtained fromindividual patients undergoing an experimental pro-cedure. We urged that research on xenotransplant-ation should continue actively (1). In that article,we discussed the question of how the “public” mightbe involved in the decision-making. I return to thattopic below.
1 Lewis Thomas Professor, Harvard Medical School, Beth IsraelDeaconess Medical Center, 99 Brookline Avenue RM 370, Boston,MA 02215, USA.
Animal-to-human organ transplants

66 Bulletin of the World Health Organization, 1999, 77 (1)
Round Table Discussion
While supporting the desirability of commu-nity consent, Daar wonders whether we should “pushthis point”, in view of two factors: first, “our inabil-ity to quantify the…risk”, and second, the fact that“there is little experience in obtaining such commu-nity consent”. I would like to take up both of thesepoints.
Our lack of knowledge about the quantitativeaspects of the risk of xenotransplantation does notdetract from the pressing ethical need to involve thepublic now. One of the most important steps in ourprogress regarding the ethics of medical experimen-tation was to insist that informed consent be ob-tained from the patient undergoing a procedure. Ourproposal that the public must have a voice in decid-ing under which conditions one could proceed withxenotransplantation essentially extends this conceptof informed consent. Such an approach attempts toensure that the public is truly represented on thisethical issue.
Daar’s argument that we should not push pub-lic discussion now, given our uncertainty about therisk, will achieve the same result as the approachproposed by some who are against a moratorium.They have argued that since we do not know theextent of the risk of xenotransplantation, we mustdo a number of xenotransplants so that it can beassessed. This argument repudiates one of the mostsacred tenets of informed consent: that consent mustbe obtained before any part of the procedure is per-formed. We often do not know how much risk weimpose on an individual patient when asking forinformed consent, and we make that fact clear tothe patient in the process of obtaining informedconsent. We do not say to the first patients under-going a new procedure that we have to go aheadwithout informed consent so that we can assess thedegree of the risk. By that logic, we would only askpatients undergoing the new procedure for informedconsent after we had performed the procedure on asufficient number of patients without such consent,in order to understand the extent of the risk. Thefact that the magnitude of the risk is not knowndoes not justify proceeding in order to find out. Thedecision by the individual patient, and in the caseof xenotransplantation by the public, must be madewhile realizing that the risk exists, even though wecannot quantify it.
The argument that we must proceed withxenotransplantation in order to assess the risk hasprofound implications. If an infection related toxenotransplantation occurs in the human popula-tion, we will have determined that there is a risk,and we will also have created a potentiallydevastatingly dangerous scenario. If there is no in-fection in the first several years, it still does not meanthat there will be no problems later. Thus, the argu-ment that we should proceed to assess the risk inthis way is proposing a potential fait accompli, anapproach that some criticize as the general insensi-tivity of medicine to the public (2).
Ethically, can we put the public at risk in or-der to help individual patients? If it is not the publicthat decides, who should? The individuals who makesuch a decision cannot be those who are stakeholdersin xenotransplantation, in the sense that they have aconflict of interests in this regard. As we have previ-ously discussed (1), they must be involved in thedecision-making but the decision should not restwith them. Nor should others who come under pres-sure from the stakeholders make the decision. TheFood and Drug Administration (FDA) properlydeals, and has dealt, with the technical issues of safety.However, that body too is under pressure from manyinterests.
I would thus reject arguments that our lack ofknowledge about the extent of risk should reduceour insistence that there be public involvement inthe decision-making prior to putting the public atrisk.
There is a logical inconsistency in the rulescurrently governing xenotransplantation. As Daarpoints out, the FDA has issued guidelines that es-sentially exclude the baboon as a donor. This hasbeen done on the basis, at least in part, of the per-ceived higher risk of infection if baboons rather thanpigs are used as donors. The baboon as a donor maywell pose a higher infectious risk than the pig, butin fact we do not know the extent of the risk pre-sented by either animal. Given this ignorance, is itnot somewhat incongruous to conclude that the riskof using baboons is too great while the risk of usingthe pig is acceptable? From the ethical point of view,both pose a risk to society and it must be societythat decides under which conditions it is willing toaccept that risk.
Daar’s second point is that there is little expe-rience in obtaining public opinion or consent. It iscorrect that public consultation is a difficult task.However, in some countries such as Switzerland, thepublic is consulted by referendum. There was sucha referendum in Switzerland on the use of geneticengineering very recently. Many expected the pub-lic to forbid the use of such techniques. However,probably because of the excellent effort that wasmade to educate the public, the referendum resultedin a solid endorsement of continued use of genetictechniques. In the United States it is hard to imag-ine holding a national referendum, although doingit at the local level is not inconceivable. For this rea-son we proposed that for the United States thereshould be a national committee composed of indi-viduals from a variety of disciplines, including eth-ics, who would try to reach a consensus on how toproceed, on behalf of the public. We have previouslydiscussed such a national committee in detail (1).In fact, there is a committee not unlike the one wesuggested now functioning: the President’s EthicsCommittee, which recently issued a report dealingwith human cloning. As discussed above, the deci-sions of the committee should not be made by indi-viduals with conflicts of interest or by those who areunder pressure from interest groups.

Bulletin of the World Health Organization, 1999, 77 (1) 67
The fact that we do not have much experiencewith polling the public in such situations should notdissuade us from developing appropriate proceduresin this regard, or from proceeding in the best possi-ble way. We face a time in which there will be in-creasing numbers of technologies that offer greatbenefit in medicine while having potential dangersthat might affect the public. We will need mecha-nisms for handling such situations from the ethicalstandpoint. Xenotransplantation is a clear exampleof such a problem; we should use this opportunityto develop an approach to decision-making that isboth responsible and ethical.
The suggestion of a moratorium to allow usto inform the public and gauge the response of soci-ety is not anti-xenotransplantation. As we wrote ina letter answering a critique of our suggestion for amoratorium: “our call for a moratorium on clinicalwork is not anti-science; rather it is a way of respect-ing the rights of the public, thus preserving the trustof the public in science” (3). ■
1. Bach FH et al. Uncertainty in xenotransplantation:individual benefit versus collective risk. Nature medicine,1998, 4: 141–144 .
2. Beck U. Risk society. London, Sage Publications, 1992.3. Bach FH, Daniels N, Fineberg HV. Letter. Nature medicine,
1998, 4: 372–3.
The case for using pigsArthur Caplan1
The question of whether or not to use pigs, geneti-cally altered to minimize the likelihood of organ re-jection, as sources for transplantable organs seemsto hinge only on whether xenografting poses an in-tolerable danger to public health. As Dr Daar accu-rately notes in his comprehensive review of the stateof xenografting, recent debates about the moralityof xenografting in the United States and Europe,especially the United Kingdom, have arrived at dif-ferent answers to the question based on their assess-ment of the public health risk posed. The decisionin Europe has been that the threat to public healthof disease transmission is too great, given the lim-ited knowledge available, to justify clinical trials ofany xenografts at the present time. Expert panels inthe US are not so convinced of the dangers, and seethe science as more promising.
In one way the differences between the Ameri-can and European assessment of the morality ofxenografting reflect deep cultural differences in atti-tudes toward biomedicine and science. Americanstend to be more positive toward the promise of sci-ence then do Europeans, who tend toward cautionin their assessment of risk when it derives from sci-entific activities.
Strangely, it is also the case that for all the dif-ficulty that surrounds the computation of the risksposed by transmission of viruses and microorgan-isms to people from animals, questions of safety pro-vide a framework within which scientists andpolicy-makers are comfortable. Attitudes and an-swers may differ from country to country, but thereare no sticky, complex or ineffable ethical issues totackle if the debate about xenografting can be re-duced to a question of safety.
Public safety surely must be a primary consid-eration in deciding whether or not genetically modi-fied animals ought be used as sources of organs forpeople in need of transplants. The threat of a publichealth catastrophe caused by a lethal virus transmit-ted from a pig or primate to a human transplantrecipient and thence to a large segment of the hu-man population is small but real. It is a risk thatcannot be justified simply by the possibility of sav-ing a comparatively small number of lives by meansof transplants. But, as Daar correctly and insightfullyperceives, the ethics of xenografting involves morethan an analysis of the safety question.
Equally important questions in assessing themorality of xenografting are whether it is ethical tobreed and kill pigs or other animals for this pur-pose; whether it is ethical to ask a human subject toface the risks, emotional as well as physical, that willattend any attempt to xenograft; or whether the psy-chosocial issues raised for recipients are too great tobear. Each of these issues must be answered in a waythat the public finds convincing. I suspect this willrequire clinical research in xenografting to follow veryspecific protocols if it is to be an option for solvingthe problem of scarce supply in the field of organtransplantation.
There should be no doubt that serious risksare posed when organs from any animal are placedinside a human body. It is a well-established fact thatmany viral and prion agents are capable of movingfrom animal vectors to humans. The natural defencesof the human body against viruses and other micro-organisms that can be carried along in an animalorgan may well be compromised when that organcomes into direct contact with the body’s own in-ternal organs and fluids.
It might be supposed that the danger posedis greatest with the earliest experiments, butthis is not true. It may well be easier to managethe danger of transmission and infection byanimal-borne viruses and microorganisms in theearliest stages of xenografting than later in thedevelopment of the technology. The f irstexperiments can be done under very carefullycontrolled conditions. Those involved in the firstxenografts can be closely monitored. Recipientscan be rigorously isolated and those who comeinto close contact with them can be required towear appropriate protective clothing andequipment. Animal organ recipients must under-stand that they will have to be under biologicalsurveillance, undergo restrictions in living and hu-
1 Trustee Professor and Director, Center for Bioethics, University ofPennsylvania, 3401 Market Street, PA 19104, USA.
Animal-to-human organ transplants

68 Bulletin of the World Health Organization, 1999, 77 (1)
1 Centers for Disease Control and Prevention, 1600 Clifton Road,Atlanta, GA 30333, USA.
Round Table Discussion
man contact possibly for the rest of their lives andthat a postmortem will be required when they die.
It will be very difficult for the first recipientsto endure the safety precautions that must accom-pany this surgery. Still, the safety measures neededare not unprecedented, having been used in anumber of other situations in which infection fromhuman to human with dangerous agents is a realpossibility. The isolation of David the so-called “bub-ble boy”, the carefully controlled environments inwhich persons live after bone marrow transplants,and the special facilities used to handle persons be-lieved to be carrying tuberculosis and other highlyinfectious agents all provide examples.
It is only if xenografting should prove clini-cally feasible that the real question of public healthsafety will loom large as a possible stumbling block.The same exacting monitoring and environmentalcontrol standards used for a small series of experi-mental subjects, chosen in part for their capacity todeal with them, will be difficult, costly and far moreprone to failure when put to use in larger numbersof patients. The need for safety is not a barrier tothe conduct of a small number of clinical experi-ments to show the feasibility of using geneticallymodified animals as sources of organs.
If safety can be reasonably assured for an ini-tial series of experiments, the ethical focus on theuse of animals as sources of organs shifts to the ques-tion of whether it is ethical to raise and kill them forthis purpose. For many, including some prospectiverecipients, xenografting will only be morally accept-able if the animals do not suffer, are not rare or onthe verge of extinction, and are as distant as possiblephylogenetically from human beings, so that con-cerns about the moral standing of the animal to besacrificed are minimized. In addition, there wouldneed to be no other plausible alternative source oftransplantable organs.
Happily, the animals to be used for xeno-grafting at present are pigs, not primates. The factthat hundreds of millions of these animals are killedfor food each year makes it difficult to muster moraloutrage over their sacrifice to save lives. True, pigsare capable of suffering, and it might be argued thatif pigs are genetically altered to improve the chancesof transplantation success some wrong or harm isbeing done to them. But changes to the immunesystem of a small number of pigs hardly threaten toundermine the dignity or individuality of that spe-cies. To serve as sources of healthy organs, the pigsthat will be sacrificed must be very carefully raisedin safe and clean environments. So although pigswill be killed, the standard of their treatment andthe quality of their lives will be very high prior totheir deaths. Unless one believes that a human lifeand a pig life have absolutely equal value – a moralposition that is exceedingly implausible – and onceit is understood that the pigs will be very well treatedand killed in a humane manner, concerns about thewelfare of these animals are not sufficient groundsfor prohibiting their sacrifice (1).
In examining the ethics of xenografting it iseasy to overlook the issue of how much a subjectcan be asked to do. Since prospective subjects facedeath without a transplant and since there will becompetition to gain access to a clinical trial ofxenografting, there is a danger of overlooking theburden that xenografting can place upon subjects insuch research.
Subjects in proposed xenografting trials willface death, but there is a real danger that the surgerycould lead to more suffering and an earlier deaththan they would have had if they had not receivedan organ from a pig. In addition, the conditions re-quired for ensuring public safety will require greatsacrifice from subjects, who would not be able topreserve their confidentiality or the privacy of theirloved ones in an experiment of this nature. Subjectswould need to understand that in becoming sub-jects they may suffer more if the research fails orfind themselves treated as subjects for the rest of theirlives if it succeeds.
This is not to say that the risks of pigxenografting are so onerous that the experimentought not be done, but the psychosocial issues ofliving with an animal organ may prove too burden-some for some to bear. Extraordinary care must betaken in subject selection, informed consent mustbe thorough, independent sources of informationmust be available to those considering serving assubjects, and persons who wish to be candidates mustunderstand that the experiment is likely to fail.
Public health can best be protected if only asmall number of experiments are conducted, andthose in a rigorous manner. The ethical case againstxenografting, while compelling and worthy of morepublic and expert debate and discussion, is not per-suasive. Genetically altered pigs may not be able tosave human lives but the time has come to take atentative step to see whether they can. ■
1. Caplan AL. Am I my brother’s keeper? Indianapolis, IndianaUniversity Press, 1998.
Speculation, stringent reasoning,and scienceLouisa Chapman1
Dr Daar has provided a cogent review of recent de-velopments in xenotransplantation that have at-tracted public concern. In 1993, the US Centers forDisease Control and Prevention (CDC) began toassess such concerns in response to requests for lead-ership in developing a national consensus onxenotransplantation. Those chairing academic hu-man subject review committees, struggling to adoptresponsible local positions on xenotransplantation

Bulletin of the World Health Organization, 1999, 77 (1) 69
clinical trials, were foremost among the petitioners.By 1995, at the initiative of the US Food and DrugAdministration (FDA), the agencies of the US Pub-lic Health Service (USPHS) were working togetherto draw up national guidelines. An initial assessmentof the issues, published in 1995 (1), can be summa-rized as follows.
Infectious agents already endemic in humanpopulations have been transmitted from donors torecipients through allotransplantation. Xenotrans-plantation carries a risk of transmitting infectiousagents not recognized as classic zoonoses (and per-haps not capable of infecting humans under normalcircumstances) from source animals to human re-cipients. The unusual circumstances of xenotrans-plantation, in which normally intact barriers arebreached and the living xenograft serves as a persist-ent source of exposure to infectious agents, may per-mit transmission of xenogeneic infectious agents thatdo not pose a threat under normal circumstances.Once infected, the xenograft recipient may becomea source patient, introducing new infections into thelarger human community. Historic pandemics ofzoonotic human disease, including the 1918 influ-enza pandemic attributed to swine influenza and thecurrent HIV/AIDS pandemic, are precedents forthese concerns.
By September 1996 a draft USPHS guidelineon infectious disease issues in xenotransplantation hadbeen jointly drawn up by the FDA, the CDC, theNational Institutes of Health (NIH) and the HealthResources Service Administrations, and publishedfor public comment (2). As noted by Dr Daar, thisdraft provoked an extensive critical response. A re-vision of the guideline, based on this public responseand the interim advances in science and public policydevelopment, should be published in the near fu-ture. Foremost among the significant changes be-tween the draft and the revised document is therequirement that all clinical xenotransplantation tri-als in the United States proceed under FDA regula-tion. Plans have also been made for forming aNational Xenotransplantation Advisory Committee,which will have, among other responsibilities, thatof providing a forum for the consideration of per-sistently contentious issues (such as concerns aboutthe use of nonhuman primates as sources ofxenografts).
In the absence of hard data, attempts to assessrisks and develop a rational policy are exercises inreasoned speculation. Prudence requires that oneneither understate nor exaggerate risk when attempt-ing to generate public discussion of these issues. Aslong as hypotheses remain untested, there will be awide divergence of opinion among responsible sci-entists. These conditions provide an open field forsensationalism or unrealistically imaginative con-cerns by less responsible or less knowledgeablediscussants. Responsible dialogue requires stringentreasoning with the available information. In this re-gard, Dr Daar has done an admirable job of walking
a cautious line while attempting to facilitate publicdiscussion of this topic.
Dr Daar refers to the assumption thatxenografts procured from nonhuman primates posemore risk of transmitting infections to humans thando those procured from pigs. This issue has gener-ated much concern among both scientists and laypeople and is an area in which science at presentoffers inexact guidance. While the simplest solutionis to call for an absolute moratorium on the use ofnonhuman primates, the wisdom of imposing oneon the basis of fear rather than science is question-able. A moratorium would prevent the reckless useof nonhuman primate xenografts when alternativesolutions are available, but it would also prevent theuse of such xenografts for selected “niche” applica-tions that may become desirable in the future.
The assumptions implicit in the statement that“xenografts procured from nonhuman primates aremore dangerous than porcine xenografts” becomeclearer if the statement is reversed. Can we confi-dently base public policy on the assumption thatxenografts procured from pigs are safer (pose lessrisk of transmitting infection) than xenografts pro-cured form nonhuman primates? Familiarity can leadto complacency. Prudence again argues that we rec-ognize the limitations in our knowledge in this area.It is true that domesticated pigs have coexisted withhumans for centuries while captive nonhuman pri-mates are only a generation or two removed fromthe wild. It seems reasonable to deduce that the mi-crobial flora of pigs, whose husbandry has been thesubject of industrial development, is more throughlyexplored than that of nonhuman primates. How-ever, the description of a newly recognized persist-ent hepatitis E virus infection of pigs suggests thatour knowledge in this area is less than comprehen-sive (3). Likewise, it seems reasonable to argue thatthe phylogenetic proximity of human andnonhuman primates increases the probability thatcross-species infections will be facilitated by sharedcellular machinery, and epitopes retained despiteevolutionary divergence. However, available datafrom which one may infer the evolutionary historyof existing retroviruses suggest a more complex real-ity. Despite the phylogenetic divergence of primates,cats, and mice, gibbon ape leukaemia virus and fe-line leukaemia virus both appear to have evolvedthrough the cross-species transmission of an ances-tral C-type murine retrovirus (4).
The Swedish diabetic recipients of porcinepancreatic islet xenografts, to whom Dr Daar refers,have been carefully investigated for evidence of in-fection with porcine endogenous virus. No evidenceof infection was found in these patients or in anadditional two who underwent short-term extracor-poreal connection to pig kidneys (5, 6). This initialinvestigation is a promising first step, but only thefirst step in what must be a laboriously developedmultiphase process. The risk of xenogeneic infec-tion will be influenced by the species from which
Animal-to-human organ transplants

70 Bulletin of the World Health Organization, 1999, 77 (1)
Round Table Discussion
the xenograft is procured, the lifelong exposure his-tory of the individual animal, the tissue used in thexenograft, and the specific application employed.The development of clinical trials employingimmunoprotected cellular xenotransplants can beexpected to result in longer post-hospital survival oflarger numbers of xenograft recipients. These survi-vors are likely to have retained functioning xenografttissue for months or years rather than days or weeks.The presence or absence of endogenous retrovirusinfection in larger numbers of these recipients mustbe explored to develop a database with which toquantify the risk of xenogeneic infections. Existingpublic policies can then be refined in light of newknowledge.
We often have to choose an initial course ofaction based on reasoned assumptions. There is adanger, in the face of laboriously established policy,of becoming intellectually bound by early precedents.The comfort of having established policy can ob-scure the need to test the hypotheses and assump-tions underlying that policy. For this reason,adversaries who push us to refine our reasoning, ex-amine our prejudices, and be uncomfortable withconclusions not yet supported by science may bemore valuable than allies.
Dr Daar’s closing paragraph discusses the riskof expatriate experiments and introduces anotherimportant caveat. We cannot protect communitiesin the industrialized world by driving renegade ex-periments into the developing world where fewerregulatory protections may exist. Infectious diseasesintermittently remind us that we are all citizens ofan increasingly global community. Many recentevents warn us against the illusion of being protectedby geopolitical boundaries. They include:• the importation of Lassa fever from Nigeria to
Chicago in 1988 by an infected person (6);• the importation of Ebola Reston fever from the
Philippines to Reston, Virginia, in 1989 and 1990by infected nonhuman primates (7);
• the importation of malaria into the United King-dom and the United States with subsequent sec-ondary transmission (8, 9);
• the establishment of endemicity after the intro-duction of HIV/AIDS initially in Africa, subse-quently in the United States and Europe, and mostrecently in Asia (10).
For residents of industrialized countries, the preven-tion of renegade experiments in the developing worldis as much enlightened self-interest as benevolentregard for our fellow residents on this planet. ■
1. Chapman LE et al. Xenotransplantation and xenogeneicinfections. New England journal of medicine, 1995,333: 1498–1501.
2. United States Public Health Service. Draft Public HealthService guideline on infectious disease issues in xenotrans-plantation. Federal register. 23 September, 1996,61: 49920-49932.
3. Meng XJ et al. A novel virus in swine is closely related to thehuman hepatitis E virus. Proceedings of the National Academyof Science, USA, 1997, 94: 9860–9865.
4. Brown J et al. Xenotransplantation and the risk of retroviralzoonosis. Trends in microbiology, 1998, 6:411–415.
5. Heneine W et al. No evidence of infection with the porcineendogenous retrovirus in human recipients of porcine islet cellxenografts. Lancet, 1998, 352:695–699.
6. Patience C et al. No evidence of pig DNA or retroviralinfection in patients with short-term extracorporealconnection to pig kidneys. Lancet, 1998, 352: 699–701.
7. Holmes GP et al. Lassa fever in the United States.Investigation of a case and new guidelines for management.New England journal of medicine. 1990, 323: 1120–1123.
8. Jahrling PB et al. Preliminary report: isolation of Ebola virusfrom monkeys imported to USA. Lancet. 1990, 335:502–505.
9. Brabin BJ, Ganley Y. Imported malaria in children in the UK.Archives of disease in childhood. 1997, 77: 76–81.
10. Zucker JR. Changing patterns of autochthonous malariatransmission in the United States: a review of recentoutbreaks. Emerging infectious diseases. 1996, 2: 37–43.
11. Mann JM, Tarantola DJ. HIV 1998: the global picture.Scientific American. 1998, 279: 82–83.
Legal and regulatory issuesBernard M. Dickens1
The review of developments and key issues so admi-rably presented by Professor Daar raises concerns ofappropriate legal and regulatory responses at threelevels, namely governmental, clinical and social.
Governmental approachesDevelopments in medical technology need not nec-essarily induce a legislative or regulatory response.Professor Daar notes that the field of xenotrans-plantation is moving very rapidly. This may cautiongovernments against rushing to legislation that risksbeing overtaken by events, thus denying benefits tothose whose interests governments claim to serve.Such a rush could, for instance, freeze governmentsinto ill-considered positions, shaped perhaps bymisguided stereotypes or imaginary horrors that areirrational and become increasingly indefensible. Wehave recently seen how moral panic over prospectsof human cloning has resulted in demands for pro-hibitive laws that would endanger respect for valuessuch as the right to freedom of therapeutic and aca-demic enquiry, the right to reproductive choice andthe right to benefit from scientific advances.
Nevertheless, the concerns Professor Daarraises include risks to recipients of animal organsand cells, as well as to their companions and thepublic at large, that justify governmental scrutiny.The contrast is presented between the regulatoryapproach recommended in the United Kingdom bythe Kennedy Report (1) and the advisory approachfavoured by the United States Institute of Medicine(2). The regulatory approach depends on legislationthat empowers a regulatory agency to approve orreject prospective xenotransplants. It protects poten-tial recipients against their own and others’ disre-
1 Professor of Law, Faculty of Law, Faculty of Medicine and JointCentre for Bioethics, University of Toronto, Canada.

Bulletin of the World Health Organization, 1999, 77 (1) 71
gard of dangers arising from xenotransplantation,and it protects family members and others whompatients might expose to animal-derived infections,and the wider public. This approach may be criti-cized for being paternalistic, but people who in otherregards are competent adults may feel that they haveonly an infantile understanding of the scientific im-plications of xenotransplantation, and appreciate in-formed regulation of this technology. This isparticularly so if they see the technology as beingpromoted by commercial rather than therapeuticinterests.
The advisory approach favours informed, au-tonomous choice rather than governmental direc-tion. An advisory council can often be legallyconstituted under existing governmental powers, butlegislation may be required for payment of councilmembers and administrators. If public health au-thorities or public clinics incorporate advisory coun-cil recommendations into their practices, principlesof administrative law may apply. If their decisionsaffect patients’ or staff members’ legal rights or le-gitimate expectations, for instance to receive orrender appropriate treatment, the persons concernedmay be entitled to contradict advice and oppose rec-ommendations before final decisions are made.Public authorities whose decisions affect others’legal interests cannot voluntarily surrender theirduty of judgement to another agency like an advi-sory council.
Though not directly legally binding, advisorycouncil recommendations can have legal effectsthrough the professional licensing of health care pro-viders, and through private service contracts. Pro-fessional licensing authorities may consider disregardof such advice to constitute professional misconduct,and impose disciplinary sanctions such as the with-drawal or suspension of a licence. Similarly, it maybe a written or implied term of a service contractthat performance will follow such advice, and disre-gard may amount to breach of contract and justifyits termination. Accordingly, advisory council rec-ommendations on xenotransplantation can haveserious but indirect legal consequences.
Clinical approachesProfessor Daar refers to the controversy over whetherwe are ready to embark on large-scale clinical trialsof vascularized whole organs. It has become com-mon to expect that new medical technologies willbe introduced through “clinical trials”, and proceedonly with caution and due ethical reflection. In theUnited Kingdom, for instance, the Clothier Com-mittee on gene therapy recommended that, at leastinitially, somatic cell therapy should be regarded notas ordinary medical practice but as clinical research(3). Many procedures that are undertaken only forresearch purposes are performed in clinical settings.So also, however, are many innovative therapiesdesigned primarily to offer seriously ill patients per-haps their only chance of survival. Xenotransplant-ation itself will probably initially be offered only to
patients close to death. Professor Daar describes DrThomas Starzl’s 1992 baboon-to-human kidneytransplants, and observes that “the experimentalnature of these attempts naturally leads to the selec-tion of very sick persons; thus the first recipient wasa patient with advanced AIDS and near-terminalhepatitis.”
A legal and regulatory concern is whether clini-cal trials of proposed life-saving innovations are gov-erned as research or as therapy. A proposeddistinction between “therapeutic research” and“nontherapeutic research” has been condemned asillogical and harmfully confusing (4). Research andtherapy are usually distinguishable in law and inregulatory provisions. Research is undertaken fordevelopment of generalizable knowledge on peoplerather than for people who may be patients. It re-quires preliminary approval by committees that re-view proposals on ethical grounds (5). Someprocedures may require additional approval. For in-stance, Professor Daar describes the detailed reviewundertaken in 1995 by the US Food and Drug Ad-ministration (FDA) before an experimental baboon-to-human bone marrow transplant was performed,with apparent success.
In contrast, therapy, including innovativetherapy, is practised upon adequately informed pa-tients for their personal benefit. Its outcome, whethersuccessful or not, may be of considerable interest toother therapists and the research and wider scien-tific communities, but its primary purpose is to ad-vance the health interests of the sick patient whoseattending clinician judges it to be clinically appro-priate. The proposal and performance of proceduresintended as therapy constitute the practice of medi-cine. Those legally unqualified for this within a ju-risdiction, including lay members of research ethicsreview committees, are entitled neither to practisemedicine nor to veto the proposals made to theirpatients by those who are qualified.
Innovative proposals to desperately ill patientsdo indeed often require ethical review, and this iswhat the FDA may have accomplished in 1995 inthe baboon bone marrow case. There is a tendencyto describe proposed innovations such as genetherapy, as “research” in order to bring them beforeresearch ethics review committees, in the absence ofalternative means of ethical review. However, suchcommittees have no authority over therapy. Wherelaws or regulations govern therapeutic procedures,for instance because they are innovative or contro-versial, health care providers are expected to com-ply. However, when patients are facing death withno alternative means of relief, disregard of such lawsor regulations may be found legally excusable. Thereis a long history, for instance, of physicians beingacquitted of serious criminal charges for disregard-ing the legal prohibition of abortion on the groundsthat their procedures were necessary to save theirpatients’ lives (6).
In this context excusable conduct is unlawfuleven when held not to warrant judicial sanction.
Animal-to-human organ transplants

72 Bulletin of the World Health Organization, 1999, 77 (1)
Round Table Discussion
Professional licensing authorities may therefore im-pose disciplinary sanctions, since their mandate isnot to punish but to protect the public against un-ethical conduct. Performing xenotransplantation inbreach of the law and without prior ethical consid-eration may be classed as medical professional mis-conduct. Lawyers cannot advise unlawful conduct,and must inform clients of its illegality. They mayalso inform clients, however, that a court of lawmight find a certain action excusable although li-censing authorities might not. Accordingly, whetherinitial instances of xenotransplantation are charac-terized as research or as attempts at life-preservingtherapy is a matter of legal and regulatory concern.
Social approachesXenotransplantation may be presented as a meansto reduce the serious gap between the supply of trans-plantable organs of human origin and the demandfor them. Some legal or regulatory oversight of thisbiotechnology may be required, however, to ensurethat use of animal organs does not cause prejudiceto patients on waiting lists for human organs, andthat the potential benefits of xenotransplantation arefairly assessed. Prejudice may arise when patients whoagree to receive xenotransplants as therapy sufferorgan rejection, and thereby move into a categoryof need that affords them priority over other patientson the same waiting list. Rules governing assignmentof patients to priority status on the list should bedeveloped to counter strategies by a patient or phy-sician that prejudice the patients who are pre-emptedon the waiting list for therapeutic transplantationby one who has accepted xenotransplantation.
It has been seen that more experimental pro-cedures, such as Dr Starzl’s baboon kidney trans-plants, may be considered acceptable and naturalonly for patients close to death. The modern historyof transplantations of artificial hearts and humanhearts, for instance, shows their justification as meansof last resort offered to patients nearing death (7).Necessity may explain resort to desperate and un-proven medical interventions. However, there is arisk of inadequate assessment of new medical tech-nologies when their initial use in research is limitedto patients in whom alternative means have failed,and whose health is so compromised that they areliable to succumb even if the novel intervention wereotherwise able to succeed. “Last chance” interven-tions limited to treatment only of the most severe orhopeless cases, involving patients least likely to behelped, do not test a research intervention ad-equately. Social interests in acquisition of scientificknowledge about the potential of xenotransplant-ation require that the procedure should not risk be-ing discredited by regulations or practices thatconfine its use to patients at the most advanced stageof deterioration. Laws or regulations should allowpatients to approve xenotransplantation research atearlier stages in their illness.
Professor Daar discusses the risk of infectionthat explains why organs from non-human primates
such as baboons and chimpanzees may be contra-indicated for transplantation into humans, butelsewhere he has also reviewed the cultural consid-erations that underlie discomfort with use of organsfrom sources so close to the human species (8). Hewrites of the part played by “the emotional attach-ment that human beings have to them” that leads torejection of non-human primates as sources of or-gans for human recipients. This emotional attach-ment may be parallelled by a need for detachment.We can perhaps accept transplantation of pigs’ or-gans into humans because we know we are not pigs,but the prospect of non-human primates as organsources raises the issue of uncomfortable similaritiesbetween all of the walking apes (9). Sigmund Freudonce explained that the smaller the real differencebetween two peoples, the larger it looms in theirimagination. This may explain why a group’s capac-ity to esteem itself is dependent on an ability toemphasize trivial distinctions from others (10),which Freud described as the narcissism of minordifference (11).
In Canada, research ethics boards constitutedunder a new joint policy statement of the three fed-eral research councils concerned will increase thenumber of representatives of social sciences partici-pating in the ethical review of medical research (10).Further, the Industrial Biotechnology Association hasestablished an ethics committee (11) to examine ethi-cal aspects of biotechnology in a broad context. Ex-posing xenotransplantation to widely reflectivereview offers a prospect of biomedical advance thatis consistent with social values and conscience. ■
1. Advisory Committee on the Ethics of Xenotrans-plantation. Animal tissues into humans. London, StationeryOffice, 1997.
2. Institute of Medicine. Xenotransplantation: science, ethicsand public policy. Washington, DC, National Academic Press,1996.
3. Committee on the Ethics of Gene Therapy. Report:development of health. London, Stationery Office, 1992.
4. Levine RJ. Clarifying the concepts of research ethics.Hastings Center report, 1979, 9(3), 21–26.
5. Council for International Organizations of MedicalSciences, International ethical guidelines for biomedicalresearch involving human subjects. Geneva, CIOMS / WorldHealth Organization, 1993.
6. Cook RJ, Dickens BM. Abortion laws in commonwealthcountries. Geneva, World Health Organization, 1979.
7. Annas GJ. Death and the magic machine: informed consentto the artificial heart. Western New England law review,1987, 9(1):198–210.
8. Daar AS and Marshall P. Culture and psychology in organtransplantation. World health forum, 1998, 19(2): 124–132.
9. Morris D. The naked ape. London, Jonathan Cape, 1967.10. Ignatieff M. Blood and belonging: journeys into the new
nationalism. Toronto, Penguin Books Canada, 1994: 21–28.11. Freud S. Group psychology and the analysis of ego, 1921.
In: Pelican Freud library, Vol.21. London, 1961: 131.12. Medical Research Council of Canada. Tri-Council policy
statement on ethical conduct for research involving humans.Ottawa, MRC, 1998.
13. National Biotechnology Advisory Committee. Leadingin the next millennium: sixth report. Ottawa, Industry Canada,Ottawa, 1998: 67.

Bulletin of the World Health Organization, 1999, 77 (1) 73
The process of discoveryJay A. Fishman1
Questions about xenotransplantation are often posedphilosophically, in terms of right and wrong. Thisapproach contrasts with the rest of evidence-basedbiomedicine, which rarely provides absolute answersto questions of merit. Should xenotransplants beperformed? Do the potential benefits outweigh thetheoretical risks? In general, such questions are ex-amined in the light of current biological knowledge,and are subject to revision over time. As our data-base develops, hypotheses are reformulated. Cer-tainty does not exist. Thus, when allotransplantationwas introduced, knowledge of the infectious risksassociated with immune suppression was rudimen-tary. Data about infection in allotransplantation hasgrown rapidly with basic science and clinical experi-ence (1). This relatively recent information was cen-tral to the discussions on the risk to the individual(potentially great) and to society (thought to besmall) when the transplantation of baboon marrowinto a human with AIDS was reviewed for the Pub-lic Health Service in the United States. Those dis-cussions were coloured by passions about science,AIDS and individual rights, but they resulted in afar safer experiment in terms of risks of infection.They were also of benefit for more general consid-erations of clinical xenotransplantation.
The term “xenosis” was coined to reflect notonly the experience in allotransplantation, but alsothe unique epidemiological aspects of interspeciestransplantation – the potential transfer into the gen-eral human population of novel or unknown patho-gens derived from animal donors (2–6). In terms ofbasic science, the search for such novel organismshas already had a beneficial effect on studies of themicrobiology of transplantation, for example the iso-lation and sequencing of the first full-length por-cine endogenous retrovirus (7) and to virologicalstudies which suggest the ability of such organismsto infect human cells in vitro (8–10). Such data havebeen used by the US Public Health Service, and bycorporate interests, to develop testing strategies forpigs raised as potential xenograft donors. Such studiesand discussions have also made it clearer to mostinvestigators that infection is a critical considerationin the development of clinical xenotransplantation.
Further studies are likely to find additionalnew, and possibly pathogenic, organisms in xenograftdonor species, and the potential for human infec-tion can be assessed for each. This discovery processadds to our understanding of the risks of xenotrans-plantation, and of the microbiology of immuno-compromised hosts in general. It is a part of theevolution of the science of xenotransplantation.Microbiological guidelines for xenotransplantation
should therefore be devised, to indicate what is cur-rently known about infection for such procedures,and serve as a basis for future scientific investiga-tions.
Benefits of xenotransplantationThe benefits of xenotransplantation must be seen inthe light of the limitations of currently available tech-nologies. Many patients die while awaiting cadaverdonor organs. Cadaveric donors provide life-savingopportunities for a small number of fortunate re-cipients, but the organs have often been subjectedto hypoperfusion, infectious contamination, or in-jury during surgical procurement. All of these areproblems which may be eliminated by the use ofplanned xenotransplants. Allograft recipients maysuffer from chronic infection or debilitation but theseproblems could be reduced if elective transplanta-tion could be scheduled, as it is currently for livingdonor transplants. In addition to their potentiallyunlimited availability and correct size, xenogenicorgans may be resistant to infection with viral patho-gens of humans, including HIV (1 and 2), HTLV,hepatitis viruses, and herpes viruses – including hu-man cytomegalovirus (CMV), which has been shownin our laboratory to be unable to infect porcine cellsin vitro (11). Further, human hepatitis B virus doesnot appear to infect baboon in vivo (12). While suchprotection is unlikely to be observed for all poten-tial pathogens, it may provide a significant advan-tage to patients with organ failure due to viralinfection.
Assessing the risksThe central goal of infectious disease physicians intransplantation is disease prevention, given the poorclinical response of the immunocompromised hostto established infections. What types of organismsshould we be concerned about in xenotransplanta-tion? As in the case of allotransplantation, the fol-lowing points are fundamental to the assessment ofthe risks of infection in xenograft recipients.• All organisms are a potential cause of infection in
any species, but the organisms most likely to causeinfection are the ones that are similar or identicalto those that do so in the immunosuppressedhuman allograft recipient, in addition to species-specific organisms not associated with humantissues.
• The risk of infection is a direct function of theoverall level of immune suppression needed tomaintain allograft function and the nature andintensity of the epidemiological exposure of therecipient. The minimization of immune suppres-sion (for instance by tolerance induction strate-gies such as bone marrow transplantation) maysignificantly reduce the risk of infection if it doesnot increase the exposure of the recipient to do-nor-derived organisms or reduce the immune re-sponse to such organisms.
• The manifestations of infection in the xenograftrecipient will also be modified by the type (such
1 Clinical Director, Transplantation Infectious Disease Program,Infectious Disease Division, Massachusetts General Hospital, FruitStreet, Boston, Massachusetts, USA, 02114.
Animal-to-human organ transplants

74 Bulletin of the World Health Organization, 1999, 77 (1)
Round Table Discussion
as corticosteroids, antilymphocyte therapy orciclosporin), intensity and duration of the im-mune suppression needed to sustain organ func-tion, and by the clinical status of the recipientfollowing transplantation.
A number of additional factors conspire toincrease the risk of infection in xenotransplantation:• the xenograft itself serves as a nidus or “culture
plate” from which such organisms can spread inthe human host without needing a “vector” toachieve disease transmission;
• clinical laboratory tests for most organisms de-rived from non-human species (e.g., antibodies,molecular probes, culture systems for species-specific organisms, or serological tests for humanantibodies against animal pathogens) are not gen-erally available;
• the migration of cells from the graft to other sitesin the host may carry cell-associated infectionthroughout the host;
• clinical syndromes caused by new pathogens arenot necessarily recognizable;
• little is known about the behaviour of potentialpathogens from the donor species in humans;
• graft rejection and immune suppression are strongstimuli for the activation of many organisms fromlatency;
• genetic recombination, mutation, or interactionsbetween exogenous and/or endogenous organismsmay mask or alter the common manifestations ofinfection;
• the absence of pre-existing immunity in the re-cipient to novel, animal-derived organisms mayrender the host more susceptible to infection;
• species disparity of histocompatibility antigensmay be associated with diminished cellular im-mune function by the host against organismswithin the xenograft (4).
Which organisms should we fear?The organisms of greatest concern to the generalpublic are those which spread easily between immu-nocompetent individuals, which can attach to andenter human cells, which can replicate within thesecells or tissues, and which can spread with few clini-cal signs or symptoms. The ideal “stealth organism”takes on surface antigens from the host so as to re-duce the capacity of the host’s immune system toattack the pathogen. The organism must also causedisease (injury) directly or must develop pathogeniccharacteristics in the xenograft recipient so as to jus-tify concern about its spread in the general popula-tion.
The endogenous retroviruses, like the beta-herpesviruses, are almost perfect transplantationpathogens. The endogenous retroviruses are carriedin the genome of every cell, acquire host antigenswhile budding off from infected host cells, and re-quire cell-mediated immunity for clearance, whichis diminished by immune suppression of the trans-plant recipient. However, there is no clear associa-
tion of the porcine retroviruses, as yet, with clinicaldisease, infection of normal or immunocompro-mised individuals, or spread between individuals. Allretroviral assays to date (unfortunately largely basedon anecdotal reports) have been negative in termsof infection of humans exposed to porcine tissues(12–14). Preclinical studies of xenotransplantationwill be important in defining the risk of spread ofinfection between species and the factors which con-trol viral replication. However, preclinical models(e.g. pig-to-primate) may not predict the infectivityor all the manifestations of disease which may occurin human xenograft recipients.
The available data have not demonstrated riskswhich should impede measured progress towardsfurther studies of clinical xenotransplantation. How-ever, further microbiological studies of xenograft tis-sues or cells from human recipients may be veryrevealing, and are of critical importance. To this end,new molecular or antigen detection assays for knownorganisms of donor species are needed. Each ap-proved clinical trial must also be designed to optimizethe possible recovery of novel organisms and shouldnot be limited to searching for previously identifiedorganisms. Therefore, biopsies and blood samplesmust be collected from xenograft donors and recipi-ents not only for archiving but for use in an activeprogramme of microbiological investigation, includ-ing the search for unknown organisms (for instanceby representational difference analysis) and studiesof the biology of such potential pathogens. It seemslikely that new organisms will be discovered in asso-ciation with the transfer of animal tissues intoimmunocompromised or otherwise modified humanhosts, just as novel infections have been describedin association with the immune deficits of AIDS andcancer chemotherapy. Rather than being guided byfear of the unknown, we must not squander a uniqueopportunity for discovery. ■
1. Fishman JA, Rubin RH. Infection in organ transplantrecipients. New England journal of medicine, 1998,338 (June 11):1741–1751.
2. Fishman JA. Miniature swine as organ donors for man:strategies for prevention of xenotransplant-associatedinfections. Xenotransplantation, 1994, 1:47–57.
3. Fishman JA. Preventing infections in xenotransplantation:xenosis from miniature swine. Xenotransplantation, 1995,3:72–77.
4. Fishman JA. Xenosis and xenotransplantation: Addressingthe infectious risks posed by an emerging technology. Kidneyinternational, 1997, 51 (supplement 58):41–-45.
5. Michaels MG, Simmons RL. Xenotransplant-associatedzoonoses: strategies for prevention. Transplantation, 1994,57:1–7.
6. Ye Y et al. The pig as a potential organ donor for man. Astudy of potentially transferable disease from donor pig torecipient man. Transplantation,1994, 57:694–703.
7. Akiyoshi DE et al. Identification of a full-length cDNA foran endogenous retrovirus of miniature swine. Journal ofvirology, 1998, 72:4503–4507.
8. Takeuchi Y et al. Type C retrovirus inactivation by humancomplement is determined by both the viral genome and theproducer cell. Journal of virology, 1994, 68:8001–8007.

Bulletin of the World Health Organization, 1999, 77 (1) 75
9. Patience C, Takeuchi Y, Weiss RA. Infection of human cellsby an endogenous retrovirus of pigs. Nature medicine, 1997,3:276–282.
10. Wilson CA et al. Type C retrovirus released from porcineprimary peripheral blood mononuclear cells infects humancells. Journal of virology, 1998, 72:3082–3087.
11. Michaels MG et al. Lack of susceptibility of baboons toinfection with hepatitis B virus. Transplantation, 1996,61:350–351.
12. Heine W et al. No evidence of infection with porcineendogenous retrovirus by primary porcine endothelial cellsand infection of human cells. Lancet, 1998, 352:699–701.
13. Martin U et al. Expression of pig endogenous retrovirus byprimary porcine endothelial cells and infection of human cells.Lancet, 1998: 352:692–694.
14. Patience C et al. No evidence of pig DNA or retroviralinfection in patients with short-term extracorporealconnection to pig kidneys. Lancet, 1998: 352:699–701.
Xenotransplantation in SwedenC.G. Groth1 & M. E. Breimer2
Several Swedish research groups are working activelyin the field of xenotransplantation. Recently, theseefforts have resulted in two clinical pilot trials: 10diabetic patients have been transplanted with por-cine pancreatic islets, and two patients have had pigkidneys connected to their blood circulation andperfused extracorporeally.
Transplantation of porcine isletsTransplantation of isolated pancreatic islets offers asimple and safe method to provide the diabetic pa-tient with insulin-producing tissue. If such trans-plantation is to be widely applied, the supply ofhuman pancreases will not suffice. Transplantationof pig islets could then serve as an alternative. Por-cine insulin differs from human insulin only in re-gard to one amino acid, and glucose homoeostasisand the regulation of insulin secretion are similar inpig and man. Furthermore, porcine insulin has beenused for decades to treat diabetic patients. Since thetransplanted islets will become vascularized by hostvessels, hyperacute rejection should not occur.
Fetal porcine islets can be prepared in largequantities by tissue digestion and culture. After trans-plantation, the fetal cells mature and differentiateinto insulin-producing cells. Microbiological screen-ing revealed no infectious agents in the material, and,when the material was injected intraportally in dogs,no adverse effects were noted.
On the basis of the above findings, a clinicalpilot trial was conducted in the years 1990–1993 in10 diabetic renal transplant patients. All patientswere given immunsuppressive treatment because oftheir renal transplant (1). Eight patients who had
previously undergone kidney transplantation had theporcine islets injected into the portal vein. Fourof the patients excreted small amounts of porcineC-peptide for 100–400 days after transplantation,indicating porcine insulin production. In two pa-tients, the islets were placed under the capsule oftheir renal graft just after the graft had beenrevascularized. In one of the patients, a kidney bi-opsy specimen taken three weeks after transplanta-tion revealed morphologically intact epithelial cellsunder the kidney capsule. These cells stained posi-tively for insulin and glucagon. Ultrastructural andimmunocytochemical features were typical of pan-creatic islet cells; the appearance of the cells indi-cated that they were viable (2).
All patients had preformed xenoantibodiesagainst the Gal 1,3Gal, an antigen epitope presenton porcine but not on human cells. After transplan-tation there was a pronounced increase in the anti-body titres (3). The finding that the porcine isletsdid not function at all in some patients, and onlyfor a limited time in the others, probably indicatesrejection. The role of the xenoantibodies in this pro-cess remains obscure.
The patients derived no clinical benefit fromthe transplantation in that their insulin requirementsremained unaffected. A larger and longer-lastinginsulin production will be required to accomplish aclinical benefit. Recently, we have isolated adult pigislets which provide immediate function. When suchislets were transplanted into unmodified rats, rejec-tion occurred in 4–5 days. However, when the ratswere treated with novel immunosuppressive drugregimens, rejection was prevented for several weeks(4). These encouraging findings will provide the basisfor further trials with pig-to-human islet transplant-ation.
Extracorporeal (ex vivo) perfusion of pigkidneys in two patientsRemoval of the preformed xenoantibodies byimmunoadsorption, or plasmapheresis should facili-tate xenograft survival. In order to test this concept,we performed a clinical trial in 1995 where pig kid-neys were extracorporeally connected to the bloodcirculation of two volunteer dialysis patients. Theprocedure was similar to an ordinary dialysis, ex-cept that the dialysis filter was replaced by a pig kid-ney. Prior to the procedure, the patients underwentplasmapheresis with a subsequent reduction inxenoantibody titres. No immunosuppressive drugswere given (5–7).
Initially both the pig kidneys perfused well,and produced urine. However, after 65 minutes ofperfusion, the first kidney underwent rejection asevidenced by discoloration and a reduction in bloodflow, and the experiment was discontinued. The sec-ond patient developed symptoms of anaphylaxis af-ter 15 minutes of perfusion. The pig kidney appearednormal at this time but the perfusion was terminatedfor safety reasons. Histopathological examination ofthe first kidney confirmed the diagnosis of rejection,
1 Professor of Transplantation Surgery, Karolinska Institute,Huddinge Hospital, Stockholm, Sweden.2 Associate Professor of Surgery, Transplantation and Liver SurgeryUnit, Department of Surgery, Sahlgrenska University Hospital,Göteborg, Sweden.
Animal-to-human organ transplants

76 Bulletin of the World Health Organization, 1999, 77 (1)
Round Table Discussion
1 President, Doctors and Lawyers for Responsible Medicine, 104bWeston Park, London N8 9PP, England.
while there was no histological evidence of rejectionin the second case. In both kidneys, there was a pro-nounced entrapment of platelets. In the second pa-tient, analyses revealed an activation of thecomplement cascade, this presumably contributingto the symptoms that appeared. Both patients de-veloped a marked increase in their anti-pig antibodytitres, the antibodies displayed specific patterns re-garding class and subclass (6). Further pertinent sci-entific questions are currently being examined usingmaterial from these two experiments.
The aim was to proceed with perfusion experi-ments, using kidneys from transgenic pigs carryingthe human complement regulator, h-DAF, whichcounteracts hyperacute rejection. However, a UnitedKingdom Government report published in 1996,outlining the possible risks of viral transmission frompig to humans, led to a moratorium on further tri-als with pig organs in Europe. Of particular con-cern was the possibility that porcine endogenousretroviruses (PERV) would be transmitted.
In the meantime, blood samples from the 12Swedish patients who had participated in the clini-cal xenotransplantation trials have been examinedfor evidence of PERV infection by using polymer-ase chain reaction (PCR) and transcriptase assays.The findings were negative in all patients (8, 9).
In conclusion, the two pilot trials conductedin Sweden have provided important informationconcerning immunological and physiological con-sequences of transplanting porcine tissue to humans.Furthermore, they have provided a unique oppor-tunity to assess the risk for transmission of PERV inthe context of xenografting. ■
1. Groth CG et al. Transplantation of porcine fetal pancreas todiabetic patients. Lancet, 1994, 344:1402–1404.
2. Reinholt F et al. Survival of fetal porcine pancreatic isletstissue transplanted to a diabetic patient: findings byultrastructural immunocyto-chemistry. Xenotransplantation,1998, 5:222–225.
3. Satake M et al. Limited specificity of xenoantibodies indiabetic patients transplanted with fetal porcine islet cellclusters. Main antibody reactivity against linked galactose-containing epitopes. Xenotransplantation, 1994, 1:89.
4. Wennberg L et al. Efficacy of immunosuppressive drugs inislet xenotransplantation: leflunomide in combination withcyclosporine and mycophenolate mofetil prevents isletxenograft rejection in the pig-to-rat model. Transplantation,1997, 63:1234–1242.
5. Breimer ME et al. Extracorporeal (“ex vivo”) connection ofpig kidneys to humans I: clinical data and studies of plateletdestruction. Xenotransplantation, 1996, 3:328–339.
6. Rydberg L et al. Extracorporeal (“ex vivo”) connection ofpig kidneys to humans II: the anti-pig antibody response.Xenotransplantation, 1996, 3:340–353.
7. Bengtsson A et al. Extracorporeal (“ex vivo”) connection ofpig kidneys to humans III: studies of plasma complementactivation and complement deposition in the kidney tissue.Xenotransplantation, 1998, 5: 176–183.
8. Heneine W et al. No evidence of infection with porcineendogenous retrovirus in recipients of porcine islet-cellxenografts. Lancet, 1998, 352:695-699.
9. Patience C et al. No evidence of pig DNA or retroviralinfection in patients with short-term extracorporealconnection to pig kidneys. Lancet, 1998, 352:699-701.
Stop now before it’s too lateAndré Menache1
Animal-to-human organ transplantation (xeno-transplantation) did not originate in a vacuum. It isthe net result of a fundamental assumption by themedical establishment that the solution to most ofsociety’s health problems lies in the development ofever more expensive, complex and sometimes riskytechnologies. Thus, historically, the first transplantof a human heart in 1967 was widely hailed as mod-ern medicine’s supreme achievement, despite the factthat the patient died not long afterwards.
Today, human-to-human organ transplants arebecoming more routine but they are far from beinga perfect solution to the health problems they aresupposed to solve. Many patients still die as a directresult of complications from the transplant, and oth-ers describe their lives as a living hell due to the poly-pharmacy regime and lifestyle restrictions that areforced upon them (C. Ray Greek, personal commu-nication).
If human-to-human organ transplants are stillfraught with complications, animal-to-human or-gan transplants are taboo, or they should be.Transgenic transplants actually represent one experi-mental technique (the production of transgenic ani-mals) superimposed on another (the transplantationof transgenic animal organs into human beings). At-tempts to analyse the possible outcomes of this situ-ation lead to a statistical nightmare, since there is anexponential increase in unknown risks.
Although the consequences of xenotransplan-tion are far from being well understood, the publicis being led to believe that the main obstacle – for-eign organ rejection – can be overcome on the basisof earlier experiments in which monkeys receivingtransgenic pig hearts survived for 60 days. Modernmedicine still has great difficulty matching humantissue types, let alone animal tissue types.
However, a more serious public health con-sideration is that of disease transmission from ani-mal to human, and subsequently to the generalpopulation. A worst-case scenario could mean an-other AIDS-like epidemic, with little promise of con-tainment, given the difficulty of carrying outenvironmental impact studies beforehand. Over-whelming scientific evidence is now available to showthat xenotransplants represent an unquantifiable riskto the health and well-being of the general public (1).
As Murphy put it, “It will not be easy to de-termine which viruses represent a risk to the xeno-graft recipient alone, which represent a risk to societyas a whole as a result of species-jumping, and whichmay be dismissed as representing a minimal risk”(2). Equally disturbing is the well-publicized state-ment made by another US veterinary virologist,Jonathan Allan: “This is a serious mistake…it only

Bulletin of the World Health Organization, 1999, 77 (1) 77
takes one transmission from one baboon to a hu-man to start an epidemic. There’s no way you canmake it safe” (3).
Despite these and other clear warnings not toproceed with xenotransplants, the United Kingdomhealth authorities have decided, nevertheless, to “pro-ceed with caution” with pig-to-human organ trans-plants (4). It is truly ironic that these healthauthorities, which go to extremes to protect the pub-lic from importing the rabies virus are now preparedto expose that same public to an “unquantifiable”risk by transplanting known and unknown pig vi-ruses into people (2).
The situation in the US is actually far worse,since xenotransplants have already taken place, un-opposed by either the Food and Drug Administra-tion (FDA) or the Centers for Disease Control andPrevention (CDC), the very bodies whose statedpolicies are to protect the health of the public. De-spite the fact that almost all of the patients who re-ceived animal organs died soon after their operation,and despite the fact that FDA public health policieshave always been “risk averse” (i.e. against researchmethods that are not well understood), the US Gov-ernment continues to allow xenotransplants to pro-ceed. In 1984, Leonard Bailey transplanted a baboonheart into newborn “Baby Fae” at Loma Linda Uni-versity, despite the fact that a proven surgical repairtechnique could have been used instead of the high-risk baboon heart. In addition, a human heart wasavailable at the time. Also, the majority of medicalopinion at the time was against the idea of using ababoon heart at all (5).
Should society condone such unethical behav-iour? The public has been presented with a dilemmaby the medical establishment: organ transplants cansave lives, but there is a shortage of suitable humanorgans. Clearly, the idea of using animal organs istempting, but on the basis of its abysmal track record,plus the Pandora’s box of unquantifiable risks in-volved, xenotransplants cannot be the answer.
Then there are legal questions which have sofar not been answered. For example, who would beresponsible for paying compensation to persons whoare damaged as a result of the animal organ insidethem, or to secondary victims exposed to the virusesxeno-recipients transmit? A further major obstacle,which must be overcome before xenotransplants canproceed, is how to obtain the “informed consent” ofthe general population, since xenotransplantationputs not only the recipient at risk, but also the gen-eral public.
The best long-term solution to organ trans-plants in general is preventive medicine, in the wid-est possible meaning of the term (obviously, this doesnot apply to those in need of an immediate organtransplant). Several alternatives exist, although noneprovides a complete solution. There is an urgent needfor governments to invest more in preventive meas-ures (such as improved diet and lifestyle patterns,anti-smoking campaigns, and the like) in order toreduce future waiting lists to the point where
supply meets demand.Allotransplantation (human-to-human organ
transplantation) is still the best that modern medi-cine can offer the end-stage organ failure patient.From a purist medical perspective, however, organtransplants with a few exceptions are an admissionof failure, on three counts:• failure to diagnose a disease condition correctly
in the early stages;• failure to provide the correct therapeutic regimen
despite a correct diagnosis;• failure to implement corrective preventive meas-
ures (6).
The result of all these failures is a serious shortfall inthe number of suitable human organs available fortransplantation. Several schemes exist to increase thenumber of human organs available. For instance, so-called “opt-out” schemes as practised in Austria andBelgium, can increase the availability of human do-nors. However, any organ-donation scheme must beaccompanied by strict hospital protocols to fulfil allthe criteria of “brainstem” death, and the necessarywritten informed consent, before a donor’s organsare removed.
Even where these schemes are used, the de-mand for organs still far outweighs the supply. How-ever, before rushing for animal organs, there are otheroptions well worth considering. Artificial organs arestill in their infancy, but they can provide a tempo-rary substitute, or “bridge”, until a suitable humanorgan is found. In some cases, artificial organs al-ready provide a permanent solution (e.g. part-hearts).From a public health perspective, artificial organsare far superior to animal organs, because they areessentially disease-free. Indeed, research fundingwould be better spent on developing these morepromising technologies than on xenotransplantation.There are also other alternatives to xenotransplantsavailable today, some of which are already in use,such as the successful transplant of a liver lobe froma mother to her child in need of a total liver trans-plant. Similarly, cells from a particular organ cannow be cultured into cell aggregates in the labora-tory, to provide a “part-organ” as a substitute, in somecases, for a conventional organ transplant. Also, cellinjection may help some liver diseases, as recentlyreported in the New England journal of medicine.
Viable alternatives to animal organ transplantsdo exist, but they need to be explored in much greaterdepth. The present situation, whereby xenotrans-plantation is being allowed to proceed despite alarmbells ringing, is both untenable and intolerable andshould be challenged on several fronts: in the me-dia, in court, and in scientific debate. “Seldom, ifever, have we had as much knowledge to prevent afuture epidemic. What is lacking is the wisdom toact upon that knowledge” (7).
Xenotransplantation is still a dangerous andhighly experimental technique, about to be un-leashed on an uninformed, and possibly also misin-formed public, against its will. ■
Animal-to-human organ transplants

78 Bulletin of the World Health Organization, 1999, 77 (1)
Round Table Discussion
1. Animal-to-human transplants: the ethics ofxenotransplantation. London, Nuffield Council on Bioethics,1996.
2. Murphy FA. The public health risk of animal organ and tissuetransplantation into humans. Science, 273, 9 August 1996.
3. Allan JS. Time, 15 January 1996, 40.4. Advisory Group on the Ethics of Transplantation.
Animal tissue into humans. Norwich, Stationery Office, 1996.5. Of pigs, primates and plagues. New York, Medical Research
Modernization Committee, 1997.6. McKeown T. The role of medicine, Oxford, Blackwell, 1979.7. Allan JS. Xenotransplantation at a crossroads: prevention
versus progress. Nature medicine, 2 (1):20.
Current obstaclesPeter J. Morris1
I read Professor Daar’s article with considerable in-terest. He adopts a conservative stance on the ques-tion of clinical trials of animal organs in humans atthis point in time, and I must say that I would joinhim in this stance.
There is no question about the demand formore organ transplants as the numbers of patientswith end-stage organ failure awaiting kidney, liver,and heart/lung transplants grow all over the world.Indeed many patients are dying while waiting forliver and intrathoracic transplants. Furthermore,if type 1 diabetes could be cured either by wholeorgan pancreas transplantation or pancreatic islettransplantation using minimal and safe immunosup-pression, there is no way that the supply of humanorgans could meet the demand. Hence there is nodoubt about the attraction of transplanting organsfrom animals into man. Nevertheless, there are ma-jor barriers to be overcome before this is possible,and some people would consider some of these bar-riers to be insuperable.
The obstacles to successful xenotransplantationare immunological, physiological, infectious, ana-tomical and ethical. The pig, at the moment, is theanimal of choice as a donor, for, as Professor Daarpoints out, anatomically its organs are of a size ap-propriate for the human, physiologically they do notappear too dissimilar, and as much of the world’spopulation eats pork there are relatively few ethicalor cultural objections to the pig as a potential organdonor.
Among the immunological problems the firstmajor barrier is the problem of hyperacute rejectionmediated by natural cytotoxic antibodies in the pres-ence of complement to a xenoantigen (known sim-ply as the Gal antigen). These cytotoxic antibodiesare present in man and in Old World monkeys (fromEurope, Asia and Africa), as the Gal antigen is notexpressed in these species. Thus a pig organ trans-planted into man would undergo rejection within
minutes. Major advances have been made in attemptsto overcome hyperacute rejection such as the pro-duction of pigs expressing a human complementinhibitor on endothelial surfaces. Other molecularbiological approaches to this problem have also beendeveloped which suggest that the problem ofhyperacute rejection of a pig organ may have beenessentially resolved. However, less immediate but noless severe degrees of rejection, such as acceleratedvascular rejection, conventional cellular rejection,and chronic rejection, will undoubtedly prove to bea problem, which may require heavy immunosup-pression to overcome.
On the anatomical and physiological side thereis a question of the size of the organ and its workcapacity, its behaviour in an upright human com-pared to a quadruped, and of course whether pro-teins produced by the pig organ (e.g. erythropoeitinby the pig kidney) will react with human receptors.These latter problems are likely to make xenotrans-plantation of a pig liver impossible, in view of thefact that the liver produces some 1000 proteins, allof which would be foreign to man.
With respect to the transmission of infection,a major concern is the possible transfer of porcineendogenous retroviruses, and although there is noevidence yet that this has occurred in humans ex-posed to pig tissues, such as islets, it is by no meansexcluded, and indeed transfer of the virus of por-cine endogenous retroviruses to human cells has beendemonstrated in vitro. The transfer of potentialpathogens represents a danger not only to theimmunosuppressed recipient, which might well bejustifiable in the case of liver or heart transplantscarried out to save life, but also to the public at largeif a pathogenic retrovirus is introduced into thehuman species.
Finally, there are ethical problems which cer-tainly apply to the use of higher order primates asdonors, bearing in mind their similarity to humans,poor breeding in captivity and their status as endan-gered species. But many people would also see, Isuspect, an ethical problem with the use of pigs asorgan donors, and recipients might find this to beeither an ethical or a cultural issue. Nevertheless theredoes not appear to be a strong body of opinion rep-resenting this latter view.
In conclusion, although we have made veryimportant strides in finding out about the problemsthat have to be overcome to attempt xenotransplan-tation, and indeed solving some of these problems,there still does not seem to me to be sufficient knowl-edge to advocate clinical trials at this point in time.Nevertheless, if one could be as certain as possiblethat the risk of introducing a pathogenic virus intoman was highly unlikely to occur, one could con-sider trials, in the first place of certain organs as abridge to transplantation. In this scenario the heart,being the simplest of them all, would be the organof choice for the initial trials. Needless to say, therewould be tremendous potential for the transplanta-tion of tissues, particularly pancreatic islet tissue from
1 Nuffield Professor of Surgery, Nuffield Department of Surgery,University of Oxford, Oxford Radcliffe Hospitals, Oxford OX3 9DU,England.

Bulletin of the World Health Organization, 1999, 77 (1) 79
the pig, if this could be achieved successfully with-out risk of infection. Furthermore the transplanta-tion of tissues, in contrast to organs, offers thepossibility of transplanting tissues encapsulated soas to allow egress of hormones such as insulin frompancreatic islets, but prevent entry of antibodies andimmunologically reactive cells which would destroythe foreign tissue. ■
The view of the Health Council ofthe NetherlandsEric van Rongen1
In the past decade, great progress has been made infinding solutions to rejection problems associatedwith xenotransplantation. In 1995 the first clinicalexperiment with genetically modified animal organsseemed close at hand. This prompted the Nether-lands Minister of Health, Welfare and Sport to re-quest the Health Council of the Netherlands tosummarize the present scientific status of xenotrans-plantation and advise her on the prospects of thetechnology for the future. The Council was alsoasked to consider ethical issues in relation to thedesirability and acceptability of research on xeno-transplantation, and of its possible clinical applica-tion. An inventory of the relevant legislation in theNetherlands was also requested, together with anevaluation of its applicability in this field. A com-mittee of the Health Council of the Netherlandsdrafted the report entitled Xenotransplantation, themain conclusions of which are presented here (1).
Viability of xenotransplantationSeveral major biotechnological problems still pre-vent the successful long-term use of xenotransplan-tation. The first is immunological rejection of thetransplanted material. Especially when discordantanimals such as pigs are used as the source of or-gans, hyperacute rejection is the main obstacle. Sincethe molecular processes associated with this type ofrejection nowadays seem to be quite well understood,the Committee felt that this problem could in duecourse be solved by using animals made adequatelytransgenic (2–4). However, for the other forms ofrejection, which become manifest within days orweeks after transplantation, the only method of pre-vention is to use immunosuppressive agents in doseswhich are not acceptable for humans, because of theassociated high risk of many serious complications(5,6). There is no obvious solution to this problemat present.
Another question that needs to be answered ishow the transplanted organ functions in the recipi-ent’s body. Certain considerations and some data
indicate that xenotransplants might not always takeover the function of the replaced organ properly (7,and C. Hammer, personal communication).
At present, a further major obstacle to the useof xenotransplantation is the risk of infection – forthe individual recipient and, more importantly, forthe human population as a whole. The Committeefeels that the use of non-human primates as sourceanimals constitutes a much larger infection risk thanthat of discordant species and therefore advisesagainst clinical experiments using primate organs.Scientific developments suggest the (transgenic) pigto be currently the most suitable source animal forxenotransplantation. However, since rejection prob-lems with primate organs are much smaller than withpig organs, the use of primates as source animalsis not a priori rejected. The technical and ethicalproblems associated with the necessary breeding ofspecific-pathogen-free (SPF) primates should not beunderestimated, however.
Recent research suggests that viruses couldmake the transition from pig to man, but it is notyet clear whether they would then cause disease(8–10). In any case this means that xenotransplant-ation of pig organs to humans is also not withoutrisks of infection. Much more understanding aboutthe processes involved is required for an assessmentof these risks.
The Committee felt that it was not possible asyet to reach any conclusion regarding the future vi-ability of xenotransplantation as a clinical technique.Clinical experiments, whether with whole organs,tissues or cells, would not be appropriate until (a)there is a good chance of operative success; (b) therejection problems have been reduced to a level com-parable to that currently associated with the trans-plantation of organs from human donors; and (c)the risk of infection is reduced to an acceptable level,for the safety of both the recipient and the popula-tion at large. For the same safety reasons, other ap-plications where intimate contact occurs between ananimal organ and a human being, such as extracor-poreal pig liver perfusion (11), should also not beperformed until the associated infection risks havebeen better determined.
EthicsThe Committee agrees with the conclusions of theelaborate ethical considerations of the NuffieldCouncil of Bioethics and the Advisory Group onthe Ethics of Xenotransplantation, both from theUnited Kingdom (12, 13). If, under the conditionsoutlined above, xenotransplantation becomes clini-cally viable, the technique will be capable of allevi-ating the suffering of people with certain medicalconditions and in many cases of prolonging life. TheCommittee therefore believes that, from a humanpoint of view, xenotransplantation is ethically ac-ceptable. Furthermore, the Committee feels that theinterests of the people who might benefit from thetechnique are sufficient to justify the possible in-convenience to or infringement upon the integrity
1 Scientific Secretary, Health Council of the Netherlands, P.O. Box1236, 2280 CE Rijswijk, Netherlands.
Animal-to-human organ transplants

80 Bulletin of the World Health Organization, 1999, 77 (1)
Round Table Discussion
of the animals concerned and that the breeding ofgenetically modified (SPF) animals for xenotrans-plantation purposes is therefore acceptable.
The Committee recognizes that some peoplemay, for cultural, religious or other reasons, disagreewith these conclusions. It would consequently liketo see more education of the public on xenotrans-plantation and more public debate on these matters.
LegislationThe use of animals is regulated in the Netherlandsby the Animal Health and Welfare Act, which stipu-lates, among other things, that performing biotech-nological procedures, including geneticmodification, is subject to licensing based on an ethi-cal judgement of the Biotechnology in AnimalsCommittee. However, the Act does not control ex-perimentation with animals or animal material ge-netically modified in other countries. TheCommittee therefore proposes to modify the Act insuch a way that the use for xenotransplantation pur-poses of organs, tissues and cells from animals ge-netically modified outside the Netherlands shouldalso be licensed and brought before the Biotechnol-ogy in Animals Committee.
Organs from genetically modified source ani-mals and the recipients of such organs are coveredby the legislation on genetically modified organisms(GMOs). This legislation, based on European regu-lations, is designed to protect the environment andhuman health from any adverse effects which theproduction or use of GMOs might have. Any re-cipient of a genetically modified animal organ wouldbe regarded under this legislation as the carrier of aGMO. As such, the recipient would be subject tothe requirements of the Environmentally Hazard-ous Substances Act and associated regulations. Thisis considered undesirable.
The Committee recommends strongly thatagreement should be sought within the EuropeanUnion regarding the application of GMO regula-tions in a way which deals specifically with theissues surrounding xenotransplantation.
According to the Committee, the governmentshould act before clinical experimentation begins,to protect individual patients and public healthagainst the risks associated with xenotransplantation,particularly the risk of possible pathogen transfer.Requirements for organ quality and for all aspectsof treatment associated with transplantation shouldbe introduced, in order to limit the risk of infectionfrom unknown pathogens.
As animal organs for xenotransplantation willbe supplied on a commercial basis, it is importantthat quality requirements applicable to such organsare included in product regulations. Given that thetrade in organs will in all probability be international,the Committee strongly favours uniform productquality standards, at the least within Europe, butpreferably worldwide.
In the Committee’s judgement, the Nether-lands’ existing medical product regulations, which
are based on European guidelines, are not adequateto regulate the trade in organs for xenotransplan-tation, mainly because they do not contain the de-sired quality standards or quality controlrequirements. The Committee therefore wishes tosee new legislation introduced, covering medicalproducts that consist at least partly of living mate-rial (biologicals). This legislation should includequality standards both for biological products in gen-eral and for particular product types. The qualitystandards included in any such legislation should beinternationally agreed.
While recognizing that new legislation of thekind described cannot be introduced in the shortterm, the Committee would like to see regulationsbrought in quickly to cover xenotransplantation in-volving human beings. Accordingly, it suggests that,as an interim solution, organs for xenotransplan-tation should be brought within the scope of thelegislation on medicines. Until the introduction ofEuropean (or global) quality standards, this moveshould be agreed with other member states of theEuropean Union.
The forthcoming Medical Research InvolvingHuman Subjects Act will cover clinical xenotrans-plantation experiments and appears to provide asound basis for the supervision of such activities. TheAct provides for local Medical Ethical Committeesthat should give permission for clinical experiments.However, it is suggested that only the central ethicalreview committee, whose establishment is also pro-vided for by the Act, should have the authority toreview protocols for research involving humanxenotransplantation. As a national body, the centralethical review committee would be well placed tomonitor developments in this field.
The new Exceptional Medical Procedures Actmakes it possible to ban xenotransplantation or tointroduce compulsory licensing. The Act could alsobe used to impose a moratorium.
Informed consentAny patient offered an animal organ should be prop-erly informed about the proposed procedure. Thepossibility of pathogen transfer, and the consequentneed for continuous and extensive monitoring fol-lowing the operation, should be clearly explained.Since an infection could be passed on to people withwhom the transplant patient has contact, the healthof such individuals would also have to be monitored.The voluntary and informed cooperation of thesepeople is therefore needed. Registration of the datacollected during the postoperative checks is essen-tial. There may, however, be problems in reconcil-ing public health interests with the individual’s rightto privacy. It should be made clear that direct con-tact between the patient and anyone who declinesto cooperate in this regard would not be possible.Furthermore, during the clinical experimentationphase at least, it will be necessary to restrict thenumber of people with whom a patient has contactfollowing a transplant operation, so as to keep the

Bulletin of the World Health Organization, 1999, 77 (1) 81
postoperative monitoring programme within toler-able proportions. As a result, the organ recipient’sfreedom of movement would need to be restricted.Xenotransplant operations should not be made gen-erally available until these problems becomemanageable. ■
1. Health Council of the Netherlands, Xenotransplant-ation Committee. Xenotransplantation. Rijswijk, HealthCouncil of the Netherlands, 1998 (Publication No. 1998/01E).
2. Cozzi E, White DJG. The generation of transgenic pigs aspotential organ donors for humans. Nature medicine, 1995,1:964–966.
3. Bach FH et al. Modification of vascular responses inxenotransplantation: inflammation and apoptosis. Naturemedicine, 1997, 3:944–948.
4. Lawson JH et al. Expression of human complementregulatory proteins CD59 and decay accelerating factor (DAF)prolongs survival and physiologic function in pig-to-baboonkidney transplants. In: The 4th International Congress forXenotransplantation. Book of abstracts. Nantes, 1997(No. O–47).
5. Bhatti FNK et al. Life supporting cardiac transplantation ina transgenic pig to primate model. In: The 4th InternationalCongress for Xenotransplantation. Book of abstracts. Nantes,1997 (No. O–52).
Animal-to-human organ transplants
6. Diamond LE et al. Transgenic pig hearts and kidneysexpressing human CD59, CD55, or CD46 are protected fromhyperacute rejection upon transplantation into baboons. In:The 4th International Congress for Xenotransplantation. Bookof abstracts. Nantes, 1997 (No. O–185).
7. Kozlowski TA et al. Clinical outcome of pig kidneytransplants in baboons treated with a tolerance inducingregimen. In: The 4th International Congress for Xenotrans-plantation. Book of abstracts. Nantes, 1997 (No. P–285).
8. Le Tissier P et al. Two sets of human-tropic pig retrovirus.Nature, 1997, 389:681–682.
9. Patience C, Takeuchi Y, Weiss RA. Infection of human cellsby an endogenous retrovirus of pigs. Nature medicine, 1997,3: 282–286.
10. Tibell A et al. Virological and clinical follow-up afterxenoislet transplantation. In: The 4th International Congressfor Xenotransplantation. Book of abstracts. Nantes, 1997(No. O–178).
11. Day M. Tainted transplants. New scientist, 1997, 2104:4.12. Advisory Group on the Ethics of Xenotransplantation.
Animal tissue into humans. Norwich, Stationery Office, 1996.13. Nuffield Council on Bioethics. Animal-to-human
transplants. The ethics of xenotransplantation. London,Nuffield Council on Bioethics, 1996.
82 Bulletin of the World Health Organization, 1999, 77 (1)
Public Health Classics
© World Health Organization 1999
This section looks back to some of the ground-breaking public health papers of the twentieth century, reproducingthem in their original form and adding a commentary on their significance from a modern-day perspective. Thismonth, Alan Lopez reviews the importance of Doll & Hill’s 1950 paper on the potential link between smoking andlung cancer. The original paper is reproduced by permission of the British medical journal.
Measuring the health hazards of tobacco:CommentaryA. D. Lopez 1
1 Acting Coordinator , Epidemiology and Burden of Disease, GlobalProgramme on Evidence for Health Policy, World Health Organiza-tion, 1211 Geneva 27, Switzerland.
“We therefore conclude that smoking is a factor, andan important factor, in the production of carcinomaof the lung ”. With this cautious statement, and anequally prudent remark on the evidence for a dose–response relationship, which while “admittedlyspeculative”, none the less suggested that “... the riskof developing the disease increases in simple pro-portion with the amount smoked”, the case waslaunched against tobacco as a leading cause of dis-ease (1). Almost five decades and thousands of sci-entific studies later, the extraordinary individual risksof smoking are now well established in populationswhere the habit is widespread, and are no longer aquestion of substantial scientific uncertainty.
But this has not always been the case, and cer-tainly was far from accepted wisdom in 1950 whenDoll & Hill published their study. Indeed, not longafter its introduction into Europe at the end of thefifteenth century, tobacco was thought to have me-dicinal value! While some undoubtedly found thesmoking of tobacco disagreeable, such was its socialacceptability that when King James I of Englandpublished a vigorous attack on the habit in 1603(Misocapnus sive de abusu tobacci lusus regius), it was“read widely, dutifully praised, and generallyignored” (see ref. 2, page 98).
The evidence that tobacco was harmful beganto accumulate during the 19th century, much of itrelating to cancer and the use of clay pipes. As theincidence of lung cancer among men began to risein the first decades of the 20th century, several epi-demiological (case–control) studies were carried outin Britain, Germany, and the USA to explore thereasons for the observed increase. For various rea-sons, these studies failed to establish unequivocallythe role of tobacco in producing lung cancer. Eventhe laboratory evidence was far from convincing, and“in 1950 ... was still not thought to support a sig-nificant role for smoking in cancer in either Britain
or the USA” ( see ref. 2 , page 91). Indeed, at thattime “ general atmospheric pollution from the ex-haust fumes of cars, from the surface dust of tarredroads, and from gas-works, industrial plants, and coalfires” was suspected as being the major cause, alongwith tobacco ( see ref.1, page 739).
The situation changed dramatically in 1950with the publication of five major case–control stud-ies (four carried out in the USA (Schrek et al. (3) ,Levin et al. (4 ), Mills & Porter (5), and Wynder &Graham (6)) and one in the United Kingdom (Doll& Hill (1)), all of which revealed a close associationbetween smoking and lung cancer. These studieswere methodologically more rigorous than previouscase–control investigations, and two studies in par-ticular (those by Doll & Hill and by Wynder &Graham) were particularly noteworthy in view ofthe numbers of cases they studied (over 600 in eachinstance), their differentiation of risk by amount andduration of smoking, the exclusion of ex-smokers(whose risks of lung cancer are intermediate betweencurrent and life-long nonsmokers), and the carefulconsideration of possible selection bias and sourcesof confounding. a
While Doll & Hill’s findings about thestrength and nature of the association between smok-ing and carcinoma of the lung were widely acceptedwhen they were published by the medical and scien-tific community, their conclusions as to cause andeffect were not. The significance of the study was, asDoll himself remarked almost 50 years later, thatthe “... idea that smoking might be an importantcause of disease had, however, been raised as a seri-ous possibility and a great deal of research into itseffects was initiated in many countries” (see ref. 2,page 97 ).
a Although the study by Doll & Hill is the focus of this commentary,the significance of Wynder & Graham’s contribution should not beunderestimated. Their conclusions, based on equally rigorousmethods, were similar to those of Doll & Hill’s; namely, that the“excessive and prolonged use of tobacco, especially of cigarettes,seems to be an important factor in the induction of bronchogeniccancer” (see ref. 6, page 336).

Bulletin of the World Health Organization, 1999, 77 (1) 83
Doll & Hill immediately followed up theirretrospective study with a large prospective study ofover 40 000 doctors registered in Britain, who werecontacted in October 1951 about their smokinghabits and other possible causes of disease. This studyeventually became a landmark in the production ofevidence on the hazards of tobacco, and, by 1954had confirmed their earlier findings from the case–control study. It is a testament to the careful scien-tific method and ingenuity of Richard Doll’s workthat today, nearly 50 years after this classic cohortstudy commenced, many of the doctors can still betraced and the relative mortality of the smokers andnonsmokers among them carefully and reliablymonitored. The results, after 40 years of follow-up,have described, perhaps better than any other re-search, the extreme hazards of persistent smoking,with the all-cause death rates of smokers being twiceas high as those of nonsmokers, and, conforming to
their prediction made almost half a century earlier,20 times higher for deaths from lung cancer (7).
The rigour, plausibility and timeliness of Doll& Hill’s retrospective study, and the vast amount ofscientific inquiry into the health hazards of tobaccothat it generated, have laid the foundations for themassive global public health response to tobacco usethat is gaining momentum, and success, as the 20thcentury draws to a close. The challenge remains,however, to accelerate public health action to reducecigarette consumption everywhere, but particularlyin the developing world. As the evidence on the haz-ards of tobacco continues to accumulate in develop-ing countries, the need for more effective tobaccocontrol programmes will become increasingly urgent.If appropriate policy and programme responses arenot implemented today, the prediction of 10 mil-lion deaths a year from tobacco consumption world-wide by 2030 (8) will, tragically, become a reality. ■
References1. Doll R, Bradford Hill A. Smoking and carcinoma of the
lung: preliminary report. British medical journal, 1950,2: 739–748.
2. Doll R. Uncovering the effects of smoking: historicalperspective. Statistical methods in medical research, 1998,7: 87–117.
3. Schrek R et al. Tobacco smoking as an etiologic factor indisease. Cancer research, 1950, 10: 49–58.
4. Levin ML, Goldstein H, Gerhardt PR. Cancer and tobaccosmoking. Journal of the American Medical Association, 1950,143: 336–338.
5. Mills CA, Porter MM. Tobacco smoking habits and cancer ofthe mouth and respiratory system. Cancer research, 1950,10: 539–542.
6. Wynder EL, Graham EA. Tobacco smoking as a possibleetiologic factor in bronchogenic carcinoma. Journal of theAmerican Medical Association, 1950, 143: 329–336.
7. Doll R et al. Mortality in relation to smoking: 40 years’observations on male British doctors. British medicaljournal, 1994, 309: 901–911.
8. Peto R et al. Mortality from smoking in developed countries,1950–2000. Oxford, Oxford University Press, 1994.

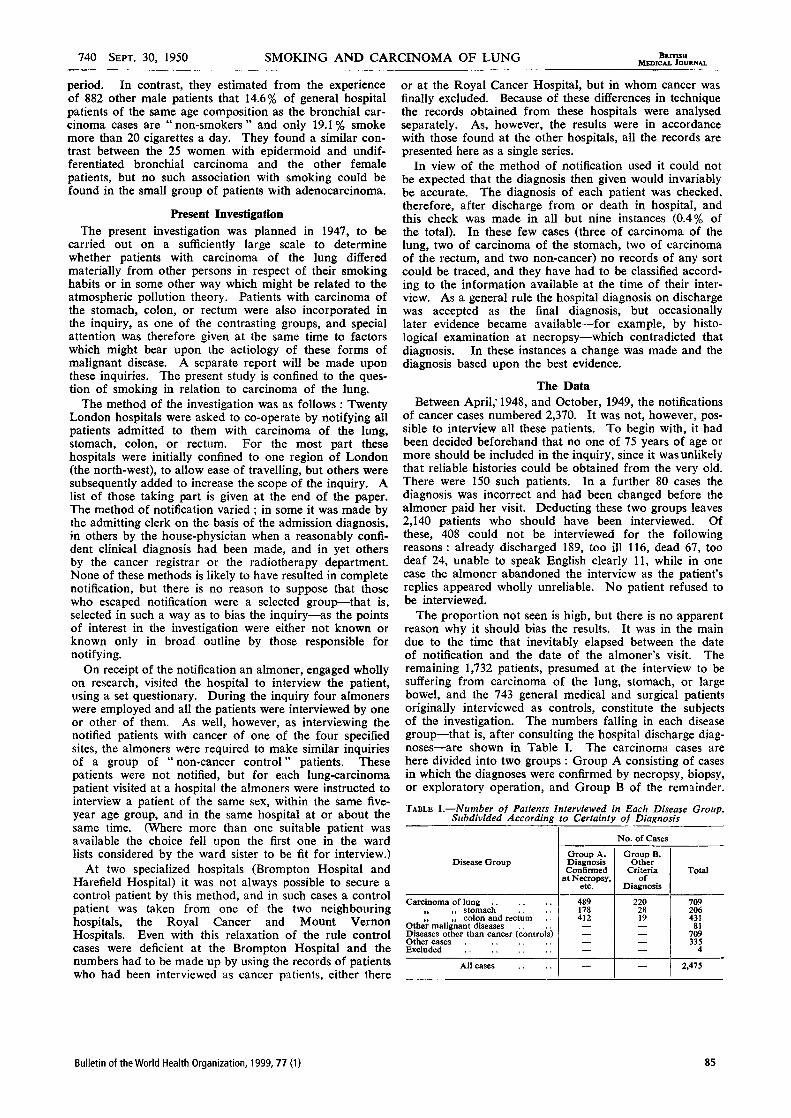
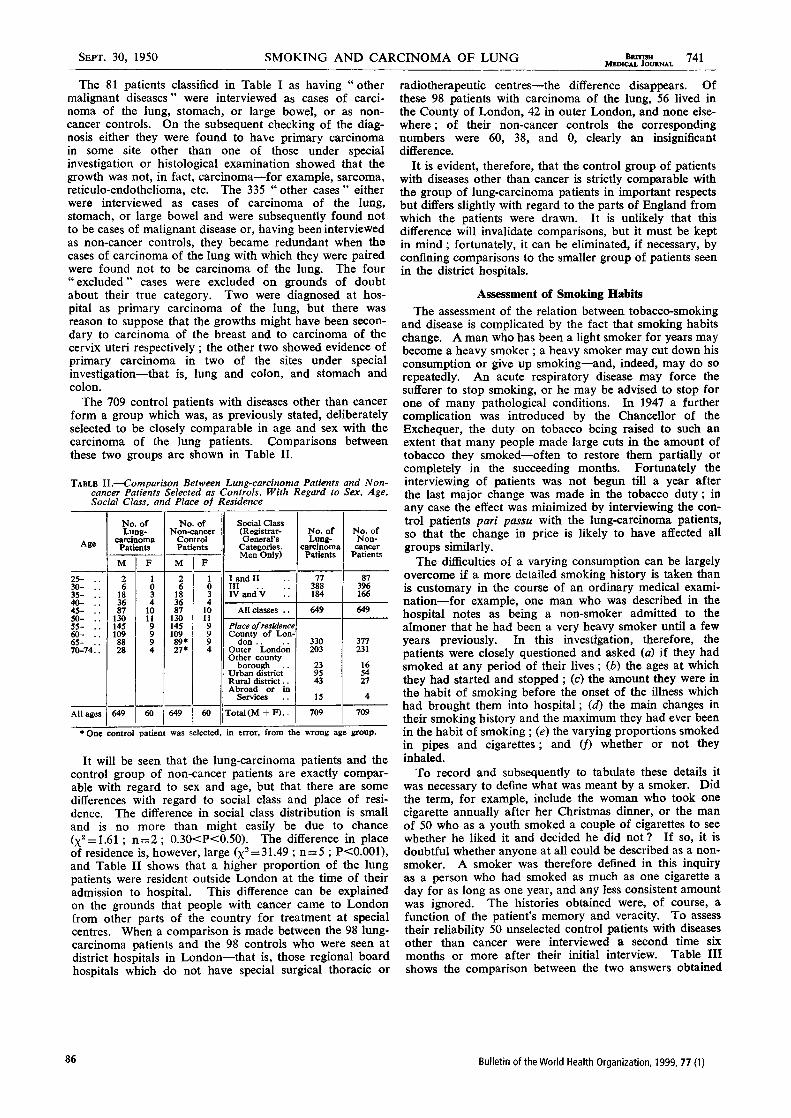
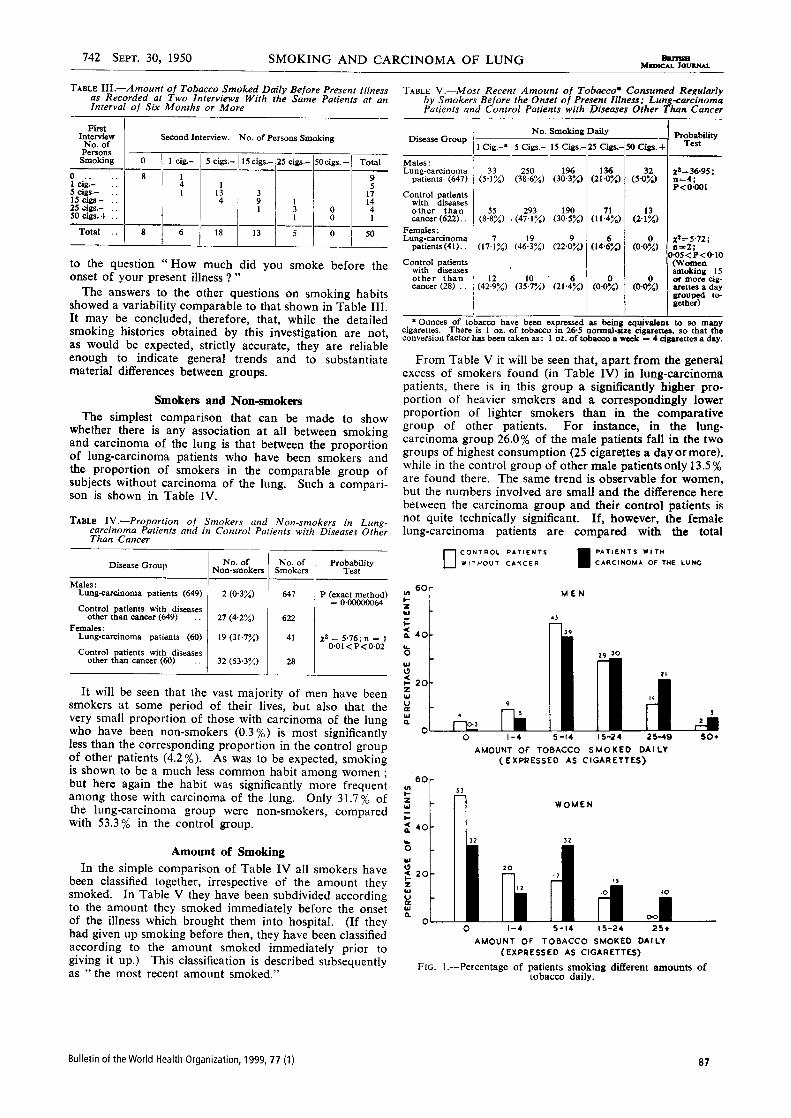
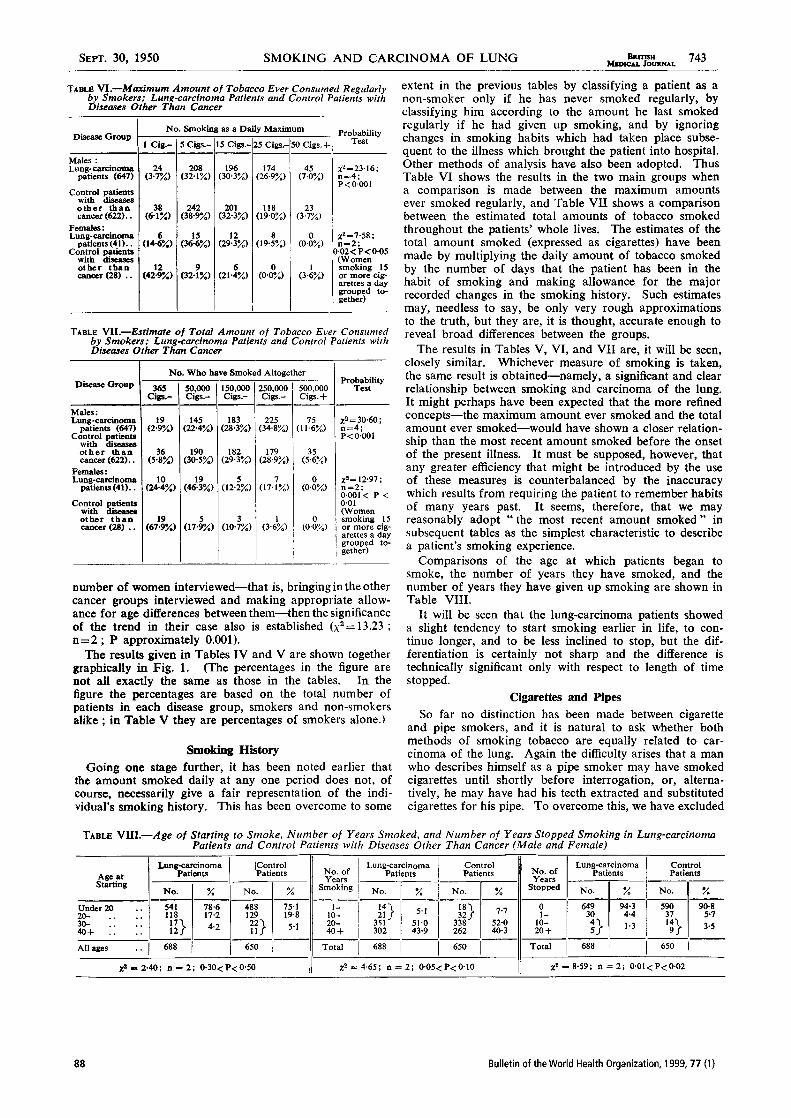
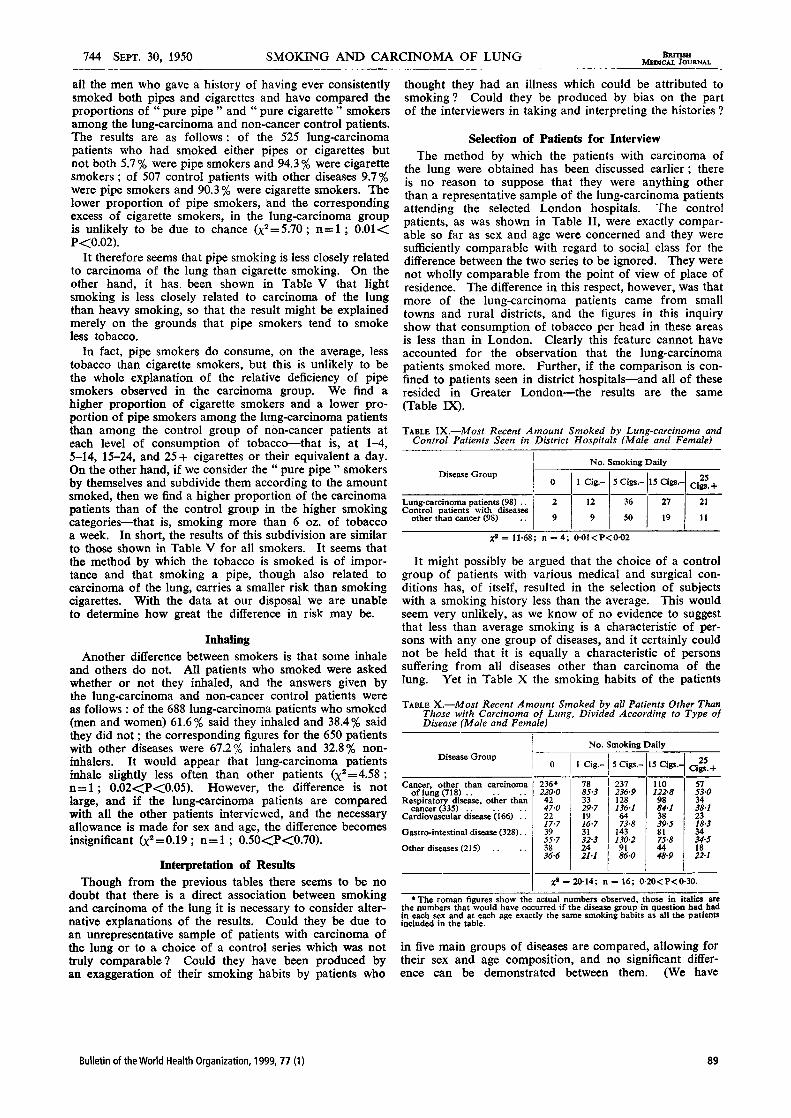

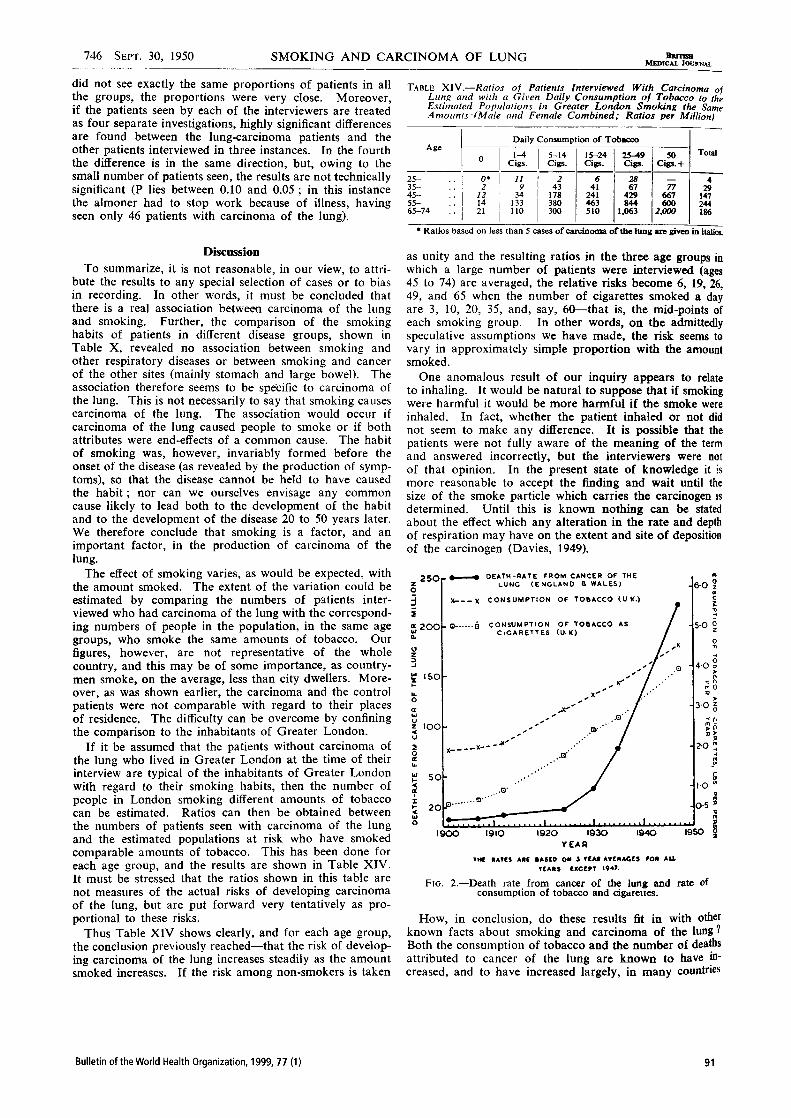
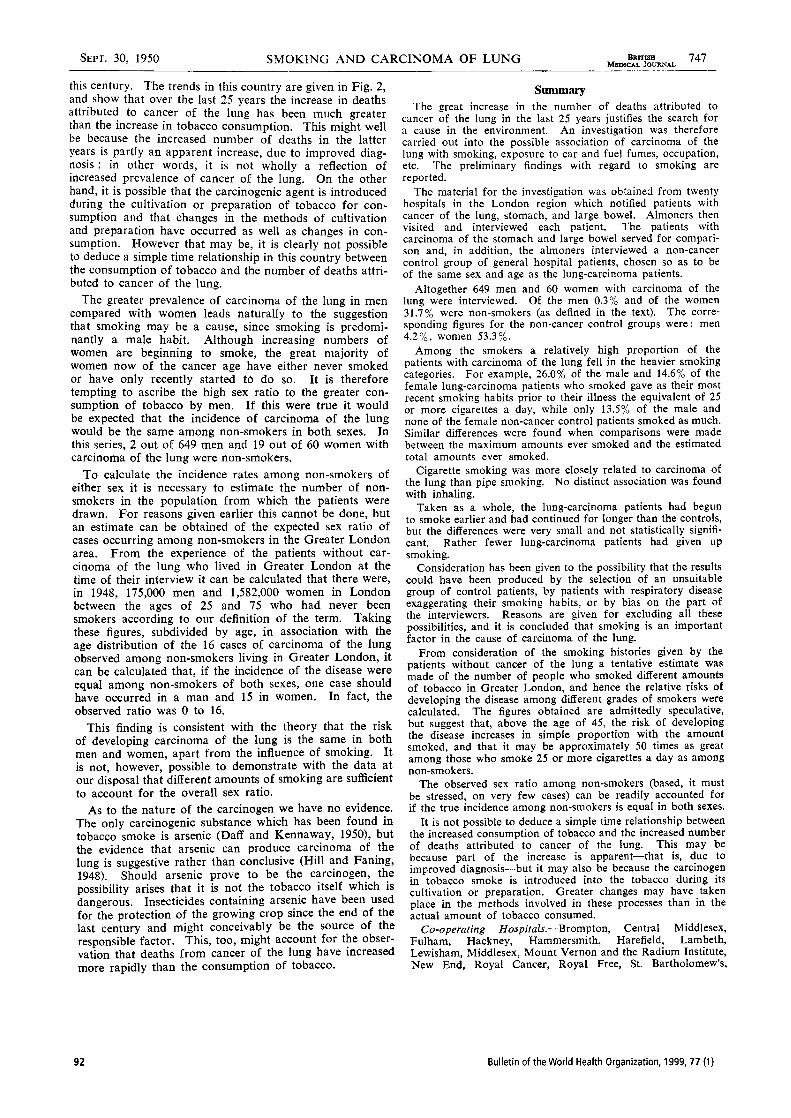

94 Bulletin of the World Health Organization, 1999, 77 (1)
News
China’s tobacco burden:large and different1
One hundred million young Chinesemen—one in three of the entire malepopulation now aged ≤29 years—willbe killed by tobacco, many of them inproductive middle age. This is theconclusion of a Chinese-led interna-tional team of epidemiologists whohave studied the impact of smokingon health in the world’s largest nation.
Their conclusions are based ontwo studies of unprecedented size, thefirst of their kind in any developingnation. In the first, the families ofalmost a million individuals who haddied across China between 1986 and1988 were interviewed to find outwhether the deceased person hadsmoked or not. Death certificates weredivided into four groups by cause ofdeath: respiratory, cancers, vasculardiseases and all other causes.
Using the “other causes” group asa reference group or baseline, theresearchers examined the excess ofsmokers in each of the other threegroups and calculated what fraction ofthe deaths in each could be attributedto tobacco.
In the second study, the epidemi-ologists interviewed some 225 000individuals about their smoking habitsand are now following their progressfor several decades. The first 10 000deaths in the cohort were analysed forthis study.
Both studies show that tobaccowas already killing 12% of Chinesemen by 1990. But, because tobacco’sdamage to a population’s health takesseveral decades to become fullyapparent, these deaths reflect thesmoking habits of the 1970s andearlier. Today’s higher rates of cigaretteconsumption by Chinese men meanthat by the middle of the next centurysome 33% of them will be killed bytobacco.
The study revealed some sur-prises. While the overall proportion ofpersistent smokers who will eventuallybe killed by tobacco is the same as inthe industrialized world — about half— the pattern of diseases that killsmokers in China is strikingly differ-ent. In China, the most commoncause of death for smokers wasrespiratory disease, mainly chronicobstructive pulmonary disease,accounting for 45% of the smoking-related deaths. In the West, ischaemicheart disease is the commonest causeof death among smokers, and respira-tory disease accounts for only 15% ofsmoking-related deaths. Importantlyfor policy-makers, tuberculosis was aslikely as heart disease to be a cause ofdeath among Chinese smokers.
Richard Peto, from the Universityof Oxford, England, one of theresearchers who carried out thestudies, said that the results under-score the importance of studying theimpact of smoking in all regions, notjust the West. “The pattern in devel-oping countries is going to be muchmore heterogeneous,” he said.
A second surprise was that youngChinese women appear to be givingup smoking. While today tobaccoaccounts for about 3% of women’sdeaths, the proportion could fall tojust 1% by the middle of next century.
The work was done by researchersat the Chinese Academy of MedicalSciences and the Chinese Academy ofPreventive Medicine in Beijing,together with the University ofOxford, England, and CornellUniversity, Ithaca, New York. Thestudies were published in November(British medical journal, 1998, 317:1411–1422; and 1998, 317: 1423–1424). The study methods used by theteam are already being adopted inIndia and elsewhere to gauge the sizeand shape of the tobacco epidemic inother nations. ■
Honours for an economistwho showed that healthmatters2
An economist who convinced hispeers of the importance of health forhuman well-being has won a Nobelprize. Amartya Sen, a citizen of Indiaand Master of Trinity College,Cambridge, England, was awarded the1998 Bank of Sweden Prize inEconomic Sciences in Memory ofAlfred Nobel for his contributions tothe study of welfare economics.
Sen is best known for his studiesof poverty and equity. He has donewide-ranging work covering thetheory of social choice, definitions ofwelfare and poverty indexes, andempirical studies of famine. His workbrings out the importance of healthcare to human well-being, anddemonstrates the centrality of thisconcern for economic and socialpolicies. He argues that what createswelfare is not goods as such, but theactivity for which they are acquired.Thus, income is significant because itcreates opportunities (or “capabili-ties”) for people. But to assess anindividual’s capabilities, the economistmust take account of other factors aswell as income, such as the individu-al’s health and level of education.
“The great thing about Sen,” saysTony Culyer, a leading health econo-mist at the University of York,England, “is that he is both aneconomist’s economist, a masterlytheorist, but also an economist forevery person... He is not only abrilliant economist but a philosopherand one who has his feet firmly on theground.”
Sen has not allowed himself to beconfined to an ivory tower, saysCulyer. His work has broadenedeconomists’ understanding of welfareinto one that takes account of indi-viduals’ state of being, says Culyer; itargues that social organizations shouldenhance people’s capabilities so thatthey can lead fruitful lives. Today,
1 For more details of the two Chinese studies seethe following Website: http://www.bmj.com
2 For more details of the Nobel prize, see thefollowing Website: http://nobelprizes.com/nobel/economics/1998a.html

Bulletin of the World Health Organization, 1999, 77 (1) 95
indicators such as those used by theUN Human Development Indexreflect this understanding that well-being is determined by many factors.
Sen, who was awarded the prizeon 14 October, heard the news inNew York at 0515 local time, hesays—“about twenty minutes before itwas announced”. He is pleased, hesays, that the Nobel committee’sdescription of his contributionemphasizes his work on theory as wellas its application to the problems ofequity and deprivation.
He was born in Bengal in 1933and has held posts in India, the USAand the UK. In 1998, he left profes-sorships in economics and philosophyat Harvard University to becomeMaster of Trinity College. ■
Malaria initiative gainsmomentumWHO’s new Director-General, GroHarlem Brundtland, acted swiftly onher arrival in office to tackle one ofsub-Saharan Africa’s greatest healththreats. She announced the start of anew initiative called Roll Back Malaria(RBM) — a campaign intended tocurb a disease that kills a millionpeople every year, most of themchildren in poor African countries.
Malaria causes up to 500 millioncases of illness each year. The eco-nomic costs, including control effortsand working days lost through illness,are estimated to be between 1% and5% of the gross domestic product ofaffected African countries. Poverty,disintegrating health services, war,rapid urbanization and the massmovement of refugees have all fuelledthe spread of the disease in recentyears.
RBM is different from previousapproaches to controlling the disease.As well as seeking to develop newtools, it is intended to strengthen thehealth systems catering for thepopulations most heavily affected bymalaria so that they can deliver theexisting tools for preventing andtreating the disease more efficientlyand equitably. This means, forexample, making insect-impregnatedbednets more widely available andimproving access to treatments with
the existing drugs, which can savemany lives. RBM’s approach will alsoseek to involve less formal healthcareproviders in communities, includingdrug vendors and traditional healers.The project is jointly sponsored byUNICEF, UNDP, the World Bank,and WHO. Its budget over the first18-month planning stage is just underUS$ 20 million.
Tore Godal, RBM’s acting projectmanager, said the first year’s prioritiesincluded the formation of clearstrategies in each affected country.These strategies would need to takeaccount of the realities of the healthsystem, he said. Godal added that theprovisional findings of assessments ofeach country’s needs had revealed that,in many cases, the situation was worsethan expected. “People are givensubstandard treatment and the use ofhealth facilities seems to be minimaleven where they exist,” he said. “Thatjust provides further justification forRoll Back Malaria.”
Within five years, he hopes, theproject “will really make a differencein the field”. He envisages morepotent combinations of drugs thatshould help to slow the emergence ofresistant malaria parasites; and,equally important, advances in thedelivery of health services that wouldenable more people to benefit fromthe existing drugs and the beststandards of existing care and preven-tion. In addition, the project’s goalsinclude more accurate measurement ofmalaria’s impact on child survival,using “sentinel” sites across the sub-Saharan African region. ■
AIDS shortens life anddents economic growthacross AfricaHIV infections continues to take asevere toll on life and health in sub-Saharan Africa, according to the latestfigures released by the United Na-tions. The UN Population Division inNew York in last autumn releasedfigures suggesting that AIDS has takenfully seven years off the average lifeexpectancy at birth of a baby borntoday in any of 29 affected Africancountries. In the absence of AIDS, lifeexpectancy for these countries would
average 54 years, but HIV has reducedthat figure to 47 years.
In certain countries where morethan 10 % of the adult population isinfected with HIV, including Bot-swana, Kenya, Malawi, Mozambique,Namibia, Rwanda, South Africa,Zambia and Zimbabwe, the UN saysthat the virus may have reduced lifeexpectancy even more sharply, by 10years. And, as the spread of the viruscontinues, its impact will worsen, withbabies born between 2010 and 2015facing lives that are on average 17years shorter than they should havebeen — 43 years instead of 60 years inthe absence of AIDS. But, becausebirth rates are generally high in theregion, no African country, howeverhard-hit, is expected to see the overallgrowth in its population reversed.
A similarly disturbing picture forsouthern Africa was described by theJoint UN Programme on HIV/AIDS(UNAIDS) on the eve of World AIDSDay, 1 December 1998, based on thesame epidemiological and demo-graphic models. In 1998 two millionpeople died of AIDS in sub-SaharanAfrica, according to the agency. Whilethese deaths reflect infections thathappened several years ago, newinfections continue to occur at“alarming” levels, says UNAIDS. Innine severely affected southern Africancountries, the agency estimates, a totalof 1.4 million adults became infectedin 1998, half of them in South Africaalone. By 2005, it is expected thatSouth African companies will bepaying out AIDS-related benefitsequivalent to 19% of their salaries’bill. Studies from other Africancountries show that households whosebreadwinner has AIDS lose most oftheir income, while their children’seducation is sharply reduced. Zimba-bwe is expected to have 0.9 million“AIDS orphans” by the year 2005. ■

96 Bulletin of the World Health Organization, 1999, 77 (1)
Books & Electronic Media
be recommended as a basic documentfor laboratory technicians, technolo-gists, and medical doctors at all levelsin developing countries, as well asmanagers and suppliers of laboratoryequipment and products.
Analytical chemistry is a compen-dium of modern analytical chemistrywhich includes:• information on quality assurance
and quality control in analyticalchemistry;
• principles of chemical analysis,covering chromatographic proce-dures, catalytic reactions,biosensors, immunoassays and otherareas;
• principles of physical analysis, insuch areas as infrared spectroscopy,nuclear magnetic resonance, massspectroscopy, and X-ray diffraction;
• statistical procedures for thevalidation of test results;
• techniques of highest metrologicalorder for the qualitative andquantitative analysis of chemicalcompounds.
This book emphasizes the entireprocess of analysis, including strategyand control, rather than confiningitself to a description of analyticalprocedures. The explanations are clear,simple and easy to follow, providing avaluable source of information forstudents and for others who are lessfamiliar with modern chemicalanalysis but want to find out moreabout it. It is a book that should be onthe shelves of all analytical chemistryand biochemistry professionals,including those who work in the areasof clinical chemistry, laboratorymedicine, pharmaceutical chemistry,environmental chemistry, foodchemistry and forensic chemistry. ■
Claus HeuckHealth Laboratory Technology UnitWorld Health Organization1211 Geneva 27Switzerland
District laboratory practice intropical countries
by Monica Cheesbrough. Published byTropical Health Technology, 1998, 464 pages,normal price £33.30, price in developingcountries £10.90. Available from 14 BevillsClose, Doddington, March, CambridgeshirePE15 OTT, United Kingdom. Tel.: 44 (0)1354740825; fax: 44 (0)1354 740013; e-mail:[email protected].
Analytical chemistry
edited by R. Kellner, J.-M. Mermet, M. Otto,H. M. Widmer. Published by Wiley-VCH VerlagGmbH, Weinheim, Germany, 1998, 916pages.
District laboratory practice in tropicalcountries takes into account advancesin laboratory technology and manage-ment that have occurred since thetextbook Medical laboratory manualfor tropical countries, 2nd ed., waspublished in 1987. The new titlereflects the current situation oflaboratories in developing countries.The author has made a considerableeffort to assess the appropriateness ofnew technologies for these laboratoriesand to update the material accord-ingly.
The author reviews the problemsfaced by laboratories in developingcountries, outlining simple practicalsolutions wherever possible. Clear andeasily understood information isprovided on the clinical biochemistryof laboratory analytes and the biologyof parasites. The book also covers themanagement of laboratory services atthe peripheral and district level,laboratory quality assurance, mainte-nance of equipment, and the localpreparation of reagents.
This book is probably the mostcomprehensive source of informationavailable today to those who work inor need to know about laboratoryservices in developing countries. It can

Bulletin of the World Health Organization, 1999, 77 (1) 97
Readers’ Forum
What do international healthconsultants need to know?
Sir – More and more consultants areoffering services in countries acrossthe globe through intergovernmental,bilateral and nongovernmentalagencies, but little systematic trainingfor such consultants is available. Thereare several important points thatconsultants need to take into consid-eration before embarking on interna-tional activities.
First, they need to be clear aboutthe assumptions underlying interna-tional aid programmes. Whose needsare being met? All too often, pro-grammes start with an assessment ofwhat the consultant or agency has tooffer, followed by a search for a willingrecipient. The offer may be hard torefuse, partly because the host countryis unable to assess the impact of theproposed programme, and partlybecause any international aid pro-gramme might bring with it a varietyof benefits irrespective of the intendedgoal. To be successful, however, theneeds of the host country must bethoroughly assessed, and the matchbetween them and the proposedprogramme must be clear to bothparties.
Consultants need to seek out thestrengths of their host country at thesame time as assessing its needs, andfind areas of mutual growth. Theirwork needs to be placed from the starton a shared power basis rather than adonor-recipient one. One way to helpachieve this is through consensusconferences, in which those whowould be involved in the proposedprogramme meet to discuss its keyconcepts, agree on which aspectsshould have priority, and express theirown views on the situation and theneeds they see for change. This processshould be repeated from time to time,since needs change and programmeshave to be flexible if they are tosucceed.
Normally, consultants are used inorder to promote change, but theprocess of change should be respectfulrather than critical. They should
remember that their task is to improvesystems, not people. One of the mostdifficult aspects of health care reformis to confront senior caregivers withthe idea that what they have beendoing for many years may be inappro-priate in the light of current knowl-edge. Sensitivity and supportivenessare needed to avoid confusing lack ofknowledge or facilities with personalfailure.
Programmes should aim forsustainability. This is easy to under-stand in relation to technologytransfer with its concomitant needs ofexpertise and supplies, but it is just asimportant if not more so for healthsystem reforms. The best way toprovide for it is to ensure that localcaregivers buy in to the new system.Buy-in is more likely to happen whenthe bulk of the relevant decision-making group, including policy-makers, clinical practitioners,academics and caregivers, see thevalidity of the new ideas. Great skillmay be needed to arrive at this,especially where some of the peopleinvolved are used to working auto-cratically and others democratically.
Most international aid pro-grammes seek to apply existingknowledge to systems that couldbenefit from it, but some healthintervention programmes are oftencarried out for the purposes ofresearch, to find out whether a certainpractice or treatment works. In thesecases the research grant often onlysupports the application of the newapproach to the experimental group. Ifthe approach proves beneficial,however, it will be desirable for thecontrol group as well. In this area as inmany others, some rethinking of theethical implications of grant fundingpolicy is needed. A general solutionmight be for research grants tostipulate that positive researchfindings must be implemented locally(and interventions with negativeresults actively withdrawn), thuscombining the aims of research andimprovement of health status.
All too often, international healthprogrammes are started with humani-tarian aims but without the means of
judging whether or when these havebeen achieved. If outcomes are notassessed, the value of the programmeremains speculative. International aidworkers therefore need to incorporateresearch components in their projectdesign and to include some teammembers with specific evaluativeexpertise. Ideally, expected outcomesshould be specified in concrete terms.
Consultants need to remainconstantly alert to their host culture.There is much that can be learntduring every moment of one’s stay inthe host country that can shed lighton the lives of programme partici-pants. Simple expedients, such asstaying in small local hotels, hospitals,and private homes, though oftenuncomfortable, will offer some of themost valuable insights into the stressesof daily living that our collaboratorsface. This also helps to build upmutual trust. In this context financialaspects of the programme, and thehuge cost differences that typicallyexist between the countries involved,should be discussed openly at theoutset, rather than left to generatehidden misunderstandings andresentment.
Finally, consultants should beaware that much of what has beenoffered with the best of intentions bypeople in industrialized countries topeople in developing ones over theyears has turned out to be less thandesirable or effective. It needs to beunder constant revision and improve-ment. Providing information for thehost country’s consideration, ratherthan advocating change in a directivemanner, is preferable, especially wherethere is uncertainty as to the efficacyof a given practice. ■
Beverley ChalmersWHO Collaborating Centre in Women’sHealth, Centre for Research in Women’sHealth, University of Toronto, Canada.Correspondence to 790 Bay Street, Toronto,Ontario, M5G 1N8, Canada. Tel: (416) 3513800 ext 2702; fax: (905) 351 3746).

98 Bulletin of the World Health Organization, 1999, 77 (1)
Directions to Contributors
The Bulletin of the World Health Organization, fromVolume 77 (1999) onwards, will have a broader fo-cus than previously. Since it now incorporates ma-terial previously published in World health forum andWorld health statistics quarterly, the Bulletin will pro-vide a platform, not only for reports of scientificresearch, but also for the exchange of information,experience, and opinions on any aspect of interna-tional public health. The Bulletin welcomes contri-butions of the following types:• research papers on topics of international public
health significance;• scholarly essays providing critical reflection on any
aspect of health development;• review articles providing state-of-the-art overviews
of public health issues;• reports outlining experiences with public health
policies and programmes, whether successful ornot; and
• letters from readers.
Contributions in the first four of the above-mentionedcategories will be peer-reviewed.
In addition, the Bulletin will publish invited contri-butions in the form of:• editorials;• round table discussions, in which a topic of cur-
rent interest is debated by individuals holdingdifferent points of view;
• reviews of books and electronic media; and• news items about health problems throughout the
world.
All papers should be addressed to the ManagingEditor, Bulletin of the World Health Organization,World Health Organization, 1211 Geneva 27, Swit-zerland.
Reprints: except for readers’ letters, authors to whomour main correspondence is addressed will receive50 free reprints of their articles. Authors will be giventhe opportunity of requesting additional copiesagainst payment.
Presentation of articles1. Papers may be prepared in accordance with thefifth edition of the Uniform Requirements for Manu-scripts Submitted to Biomedical Journals (see, forexample, New England journal of medicine, 1997,336(4):309-315; or on the World Wide Web at thefollowing URL: http://www.acponline.org).
2. Papers may be submitted in English, French orSpanish. The Bulletin is published in English, withsummaries of main articles in French and Spanish.Contributions in French or Spanish that are accepted
for publication will be translated into English by theBulletin. Twice-yearly digests of selected articles willbe published in Chinese, French, and Spanish.
3. Papers should be accompanied by a statement thatthey have not already been published and that if ac-cepted for publication in the Bulletin they will notbe submitted for publication elsewhere without theagreement of the World Health Organization. Theauthor(s) should also provide a signed statement as-signing the copyright of the manuscript, if acceptedfor publication, to the World Health Organization.
4. Papers are accepted on the understanding thatthey are subject to editorial revision, including, wherenecessary, condensation of the text and omission oftabular and illustrative material.
5. Authors are responsible for obtaining permissionfrom the copyright holder(s) to reproduce any ma-terial enjoying copyright protection. The letter grant-ing such permission should be attached to themanuscript.
6. Papers should be typewritten on A4 paper, onone side only, in double spacing, with a margin of atleast 3 cm on the left-hand side of the page. Twoclear copies should be submitted together with a3-1/2" IBM-compatible diskette containing the textand tables in MSWord or WordPerfect format, stat-ing clearly which version of the software has beenused.
7. An exact description of the post(s) held by theauthor(s) should be given. Each author should haveparticipated sufficiently in the work being reportedto take public responsibility for the content.
8. An abstract not exceeding 200 words in lengthshould be provided. A full summary, about 600words, should also be provided for translation intoFrench and Spanish.
9. Papers should be as brief as possible. As a guide, itis suggested that the length of main articles shouldnot normally exceed 6000 words, including tablesand illustrations. Contributions to the correspond-ence section are shorter and do not usually containtables or illustrations. A summary is not required.
Bibliographical references10. The number of bibliographical references shouldbe kept to a minimum. They should be numberedconsecutively as they occur in the text, the numberbeing in italic and placed in parentheses. Thus:
A recent study in India (3) showed…
Bulletin of the World Health Organization, 1999, 77 (1) 99
Directions to Contributors
11. All references should be listed in numericalorder at the end of the text. Works written by morethan three authors should be referred to by the nameof the first author only, followed by the words et al.Authors are responsible for the accuracy of all refer-ences: these are not checked by the editor.
Books and periodicals12. References to books and to articles in periodi-cals should be presented without abbreviations asshown in the following examples. A title in a for-eign language should be left in that language (ortransliterated) and followed by a translation in squarebrackets.
1. Paganini JM, Novaes HM. Hospital accredi-tation for Latin America and the Caribbean.Washington, DC, Pan American HealthOrganization/WHO and Latin AmericanHospital Federation, 1992 (SILOS series 13).
2. Cancer pain relief and palliative care. Reportof a WHO Expert Committee. Geneva, WorldHealth Organization, 1990 (WHO TechnicalReport Series, No. 804).
3. Farnsworth NR, Soejarto DD. Globalimportance of medicinal plants. In: AkereleO et al., eds. Conservation of medicinal plants.Cambridge, Cambridge University Press,1991: 25–51.
4. Videlier P, Piras P. La santé dans les bandesdessinées [Health in strip cartoons]. Paris, Edi-tions Frison-Roche/CNRS Editions/Comitéfrançais d’Education pour la Santé, 1992.
5. Hennart P. Dix programmes de santépublique [Ten public health programmes].L’enfant, 1990, 1: 8–14.
6. Kiyingi KS, Sime L. Compliance profilesof paediatrics patients in an outpatient depart-ment. Papua New Guinea medical journal,1992, 35: 95–100.
Conference proceedings and unpublishedworks13. These references should be cited as in the fol-lowing examples:
7. Ariyaratne AT. Literacy and sustainable de-velopment. In: Proceedings from the FourthWorld Assembly on Adult Education, 8–18 Janu-ary 1990. Bangkok, International Council forAdult Education, 1990: 54–55.
8. Razum O. Low valid immunization cover-age in a rural district of Zimbabwe: should themothers be blamed? Paper presented at theSecond Inter-Country Meeting on MCHFP,Juliasdale, Zimbabwe, 3–7 February 1992.
9. Chen R. A measles outbreak in a highly vac-cinated population: Health Sector Muyinga,Burundi, 1988-1989. Atlanta, GA, Centers forDisease Control, 1991 (unpublished docu-ment).
10. A one-way street? Report on Phase 1 of theStreet Children Project. Geneva, World HealthOrganization, 1993 (unpublished documentWHO/PSA/93.7, available from the Pro-gramme on Substance Abuse, World HealthOrganization, 1211 Geneva 27, Switzerland).
Information available on the World WideWeb
11. Food safety from the farm to table: a newstrategy for the 21st century. Washington, DC,United States Department of Agriculture,Department of Health and Human Services,and United States Environmental ProtectionAgency, 1997 (Internet communication, 21February 1997 at http://um.crsan. fda.gov/dms/fs-draft.html).
Tables and illustrations14. The number of tables and illustrations shouldbe strictly limited, only those that are essential to anunderstanding of the text being included. The samedata should not be presented in both tables andgraphs.
15. References in the text to tables and figures shouldalways be by number (e.g., Table 1; Fig. 3) and notin the form “the table above” or “the figure below”.
16. Tables should be typewritten, each on a separatesheet of paper, and should be numbered consecu-tively in arabic numerals. They should be groupedin sequence at the end of the text, not incorporatedinto the text.
17. Graphs or figures should be clearly drawn andall the data identified: abbreviations should beavoided or explained. Photographs should be onglossy paper, preferably in black and white. Figuretitles should be short but at the same time adequatelyexplanatory.
Research involving human subjects18. The World Health Organization publishes theresults of research involving human subjects only ifsuch research has been conducted in full accordancewith ethical principles, including the provisions ofthe Declaration of Helsinki (as amended by the 48thGeneral Assembly, Somerset West, South Africa) andthe additional requirements, if any, of the countryin which the research was carried out. Any manu-script describing the results of such research that issubmitted for publication must contain a clear state-ment to this effect, specifying that the free and in-formed consent of the subjects was obtained.

World Health OrganizationGeneva
,,
,g