b9 acute renal failure, toxic nephropathy
TRANSCRIPT

Wednesday, June 11 B9. Acute renal failure, toxic nephropathy 651
haematuria occurred in 217 patients (15%). Haemorragic complicationsappeared to be related to some kidney disease such as acute tubular necrosisand end stage kidney (OR 2.369, IC 95% 0.945), lupus erythematosussystemicus and vasculitis (OR 1.973, IC 1.342), to prolonged bleedingtime (>7 min, but always < 9 min) (OR 1.628, IC 0.945), to arterialhypertension (>140/90 mmHg, but always <160/100 mmHg) (OR 1.257,IC 0.950).Haemorragic complications were not directly related to: low platelet count(<150.000/mm3), sex, anemia (Haemoglobin < 10 g/dl), reduced renalfunction (creatinine > 1.3 mg/dl, azotemia > 50 mg/dl, or dialysis at thetime of biopsy) and age of patient.In our experience clinical suspicion predicted histological diagnosis in67% of biopsies; the greatest rate of agreement between clinical guessand confirmed pathological feature has been obtained in cast nephropathyand acute tubular necrosis (100%), in lupus erythematosus and vasculitis(90%).In conclusion the review of our clinical and histological data of 30 yearsof kidney biopsy experience, confirmed this extended manoeuvre as a suc-cessful procedure with a low incidence of serious complications even inold and difficult patients. Nowadays renal biopsy is still useful not onlyfor diagnosis of kidney disease but its importance is above all reflectedto estimate the extent of activity or chronicity of nephropathy and this isessential for therapeutical decisions and prognostic evaluation.
W330 PREDICTORS OF BLEEDING COMPLICANCES INPERCUTANEOUS ULTRASOUND GUIDED RENAL BIOPSY
Carlo Manno1, Loredana Arnesano1, Giovanni F.M. Strippoli1,2,Nicla Campobasso1, Loreto Gesualdo3, Francesco P. Schena1. 1Dept. ofEmergency and Organ Transplantation, University of Bari, Bari, BA,Italy; 2Centre for Kidney Research, Cochrane Renal Group, TheChildren’s Hospital at Westmead, Westmead, NSW, Australia; 3Division ofNephrology, University of Foggia, Foggia, FG, Italy
Tecnhnical advances have greatly improved and simplified the percuta-neous renal biopsy (PRB); however biopsy-realted bleeding complicationsstill occurr.We evaluated the prevalence of post-biopsy bleeding complications in anattempt to assess which factors were predictive indicators in a cohort of416 (244 male and 172 female) patients who underwent PRC in our Unitbetween January 1995 and December 2001. Renal biopsies were peformedby semiautomated or automated needle with direct ultrasound guidance.The following data were obtained and collected at the time of renal biopsy:age of patient, sex, blood pressure, hemoglobin and hematocrit value, PT,PTT, bleeding time, serum creatinine and daily proteinuria, type and sizeof needle (14 G or 16 G). Transplant biopsies were excluded from ouranalysis. Univariate and multivariate analysis (logistic regression) wereused to evaluate the influence of these variables on bleeding complicationsat the time of PRB. Clinical and ultrasound evaluation were used to identifythe presence of post-biopsy bleeding.One-hundred and fourty-seven patients (35.3%) presented bleeding com-plications following PRB. These were, respectively: 144 (34.6%) casesof hematomas, 2 (0.5%) cases of macrohematuria and 1 (0.2%) case ofartero-venous fistula. According to univariate analysis, the only distinctiveparamether between patients with complications and those without com-plications was age (p=0.0098). No significant differences were evident forany of the other investigated paramethers. Multivariate analysis indicateda statistically significant correlation between sex (male) and post-biopsybleeding (odds ratio: 1.92; confidence intervals: 1.17-3.15, p=0.0099). In-creased pre-biopsy hemoglobin levels were associated with a reduction ofbleeding risk (odds ratio: 0.88, confidence intervals: 0.78-0.99, p=0.05).No other parameter had an influence on post-biopsy bleeding.In conclusion, even with current improvement in the methods of PRB, thisis still not a risk-free procedure and bleeding complications still occur.According to our multivariate analysis, the only indipendent predictors ofbleeding complications in PRB are sex and pre-biopsy hemoglobin levels.
W331 ISOLATED MICROHEMATURIA IN CHILDREN: VALUEOF RENAL BIOPSY
Danica Batinic1, Mira Scukanec-Spoljar2, Danko Milosevic1,Ljiljana Nizic1, Kristina Vrljicak1, Maja Matkovic1, Danko Batinic1,Lana Grkovic1. 1Department of Pediatric Nephrology, 2Department ofPatology, Medical Faculty, Yagreb, Croatia
Isolated microscopic hematuria (IMH) in children always raises the ques-tion whether, besides other examinations, there is a need of performing arenal biopsy. Many authors consider IMH to be a minor abnormality wherepathological glomerular changes are not likely to be found, however, gen-eral agreement has not yet been achieved. The aim of the study was toevaluate the contribution of the renal biopsy to the diagnosis of the diseasein IMH. Renal biopsy was performed in 54 children with IMH (22 boysand 32 girls, mean age 8.2 and 8.3 years, respectively) in whom urologi-cal abnormalities, hypercalciuria, systemic diseases, coagulopathy or overtfamily history of renal disease were excluded. Mean duration of IMH priorto biopsy was 2.8 years. Biopsy specimens were examined by light (LM),immunofluorescent (IF) and electron microscopy (EM). Fortythree (79.6%)patients were found to have glomerular abnormalities. On LM 18 patientshad normal glomeruli (NG), 22 mesangial proliferative glomerulonephritis(MEPGN), 9 focal glomerulosclerosis (FGS), 3 focal glomerulonephritis(FGN) and 2 membranoproliferative glomerulonephritis (MPGN). IF re-vealed 2 cases of NG, 5 cases of MEPGN, and all 3 cases of FGN as IgAnephropathy. EM discovered GBM changes consistent with Alport syn-drome in 21 patients, 7 of them with NG, 9 with MEPGN and 5 with FGSon LM. Diffuse thinning of GBM was found in 10 children, 7 with NG and3 with MEPGN on LM. In 5 cases subepithelial hump-like deposits, whichwere considered to be the sign of acute postinfectious glomerulonephritisin resolution, were found. One of 2 cases of MPGN showed to be type II(DDD). On follow-up, 6 of 21 children with changes consistent with Alportsyndrome developed clinical signs of the syndrome. Further surveillance isneeded to confirm the significance of EM findings in others. We concludethat in children with IMH renal biopsy is justified and should always beanalyzed by light, immunofluorescent and electron microscopy.
B9 Acute renal failure, toxic nephropathy
W332 CHANGING CAUSES AND PROGNOSIS INNONTRAUMATIC ACUTE RENAL FAILURE REQUIRINGDIALYSIS TREATMENT COMPARING THE YEARS1981-1990 AND 1991-2000
Georg Biesenbach, Bernhard Schmekal. 2nd Department of Medicine,General Hospital, Linz, Austria
Despite advanced techniques of renal replacement therapy as well as im-proved medical care and control over the last decade, the overall mortalityof patients with nontraumatic acute renal failure (ARF) requiring replace-ment therapy is still high. In a retrospective study we compared causes ofnontraumatic ARF, risk factors for the development of renal failure andmortality rates in patients with nontraumatic ARF who received hemodial-ysis therapy from 1981 to 1990 (n=278) and from 1991 to 2000 (n=232). Inthe latter period there was a significant reduction in the prevalence of acuteglomerulonephritis (3.0 vs. 8.3%, p<0.01) and acute interstitial nephritis(2.6 vs. 7.6%, p<0.01) as well as acute pancreatitis (1.7 vs. 7.6%, p<0.01).On the other hand, the prevalence of drug-induced ARF increased duringthe latter period (10.8 vs. 4.7%, p<0.05). Other etiologies of nontraumaticARF did not significantly differ between the two decades. Patients treatedfrom 1991 to 2000 had chronic risk factors for the development of ARF,namely diabetes (14.6 vs. 6.8%), coronary artery disease (28.0 vs 9.3%)and pre-existing renal impairment (51.7 vs. 17.6%, p<0.001), more fre-quently than did patients dialysed from 1981-1990. The overall mortality(41.8 vs. 44.6%, NS) and mortality secondary to causes of nontraumaticARF were similar in both periods. Conclusion: The prevalence of sev-eral causes of nontraumatic ARF has changed during the last decades, butthe overall prognosis of the patients has not been significantly improved.Furthermore, patients treated in the 90’s had chronic risk factors for re-nal failure, namely diabetes and pre-existing renal impairment as well as
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022
652 B9. Acute renal failure, toxic nephropathy Wednesday, June 11
coronary artery disease, more frequently than did subjects treated in thepreceding time period.
W333 ACUTE RENAL FAILURE IN THE TROPICS: EMERGINGTRENDS FROM A TERTIARY CARE HOSPITAL IN SOUTHINDIA
Urmila Anandh, S. Renuka, Lloyd Vincent. Nephrology, St. John’sMedical College Hospital, Bangalore, Karnataka, India
Acute renal failure forms a major cause of admissions in hospitals in India.This study was undertaken to note the epidemiology laboratory parameters,outcome and factors determining outcome of patients presenting with acuterenal failure in our hospital.A prospective follow up study from December 1997 to January 2000 wasconducted in all patients presenting with acute renal failure was done.Demographics, laboratory parameters, etiology, outcome and prognosticfactors determining outcome were studied. 642 patients were included inthe study. The predominant underlying cause was sepsis (153/642) fol-lowed by acute gastroenteritis (96/642). Dialysis was offered in 1/3rd ofthe patients. Most of them underwent hemodialysis. Intermittent peritonealdialysis was the preferred mode of renal replacement therapy in the criti-cally ill patients. The overall mortality was 26.5%. A multiple regressionanalysis showed that presence of sepsis, who were admitted in the ICU,and presence of oliguria were associated with a poorer outcome (Table).
Logistic regression analysis for factors determining outcome
SE Wald p Value
ICU Admission 0.04 16.35 0.0001Sepsis 1.95 40.03 0.00005Ventilatory support 2.15 15.43 0.001Oliguria 0.71 4.71 0.03
Acute renal failure is a common admitting diagnosis in tropical countries.With changing medical facilities sepsis is becoming a predominant cause.However, mortality figures compare favourably with the west because ofrelatively benign diseases like acute gastroenteritis still form a major etio-logical factor.
W334 ACUTE RENAL FAILURE IN ROMANIA: NEW PATTERNSPOINTING A CHANGING SOCIETY
Dan-Stefan Vladutiu, Mirela Gherman, Costel Spanu, Ioan-Mihai Patiu,Simona Racasan, Liliana Parvu. Nephrological Clinic, MedicalUniversity, Cluj-Napoca, Cluj, Romania
Comprehensive studies on acute renal failure (ARF) are scarce in formercommunist countries and almost absent in Romania. The present work ana-lyzes etiology, clinical features and outcome of ARF in 1688 patients (pts)treated from 1970 to 2002 in the Nephrological Clinic of Cluj-Napoca,capital city of the province of Transylvania. The Hemodialysis Departmentwas founded in 1960, being the second one in Romania. The departmentprovided medical care for patients with ARF from 9 districts of Transylva-nia; therefore data are representative for a large part of the country.The mean age of the pts increased steadily (42.7±14.7 years in 1979-89;50.7±16.8 in 1991-9; 55.2±15.8 in 2000-1). The etiology of ARF changeddramatically after 1989 (table 1). During Ceausescu’s era, draconian lawsinterdicting birth control transformed surreptitious abortion in the maincause of ARF. After 1989, other causes, important before, lost in preva-lence: nephrotoxins (- 8.5%), rifampicin (-2.91%), leptospirosis (- 3.71%),blood transfusions (-3.77%). Surgery (especially cardiovascular) becamean important etiology. At present, Romania situates between underdevel-oped countries, where infections and toxics prevail, and developed ones,where trauma and surgery are prominent. In spite of significant techni-cal improvement, mortality increased (1979-89: 24.75%; 2000-2: 37.5%),being highest in patients with sepsis and after surgery. In a univariatedregression analysis, death associated significantly with anuria, MSOF andhemodynamic instability at dialysis; in bivariated analysis, there was a sig-nificant correlation between poor outcome and hemodynamic instabilityduring dialysis, associated with either of MSOF, infection, high creatininelevel and hyperkalemia.
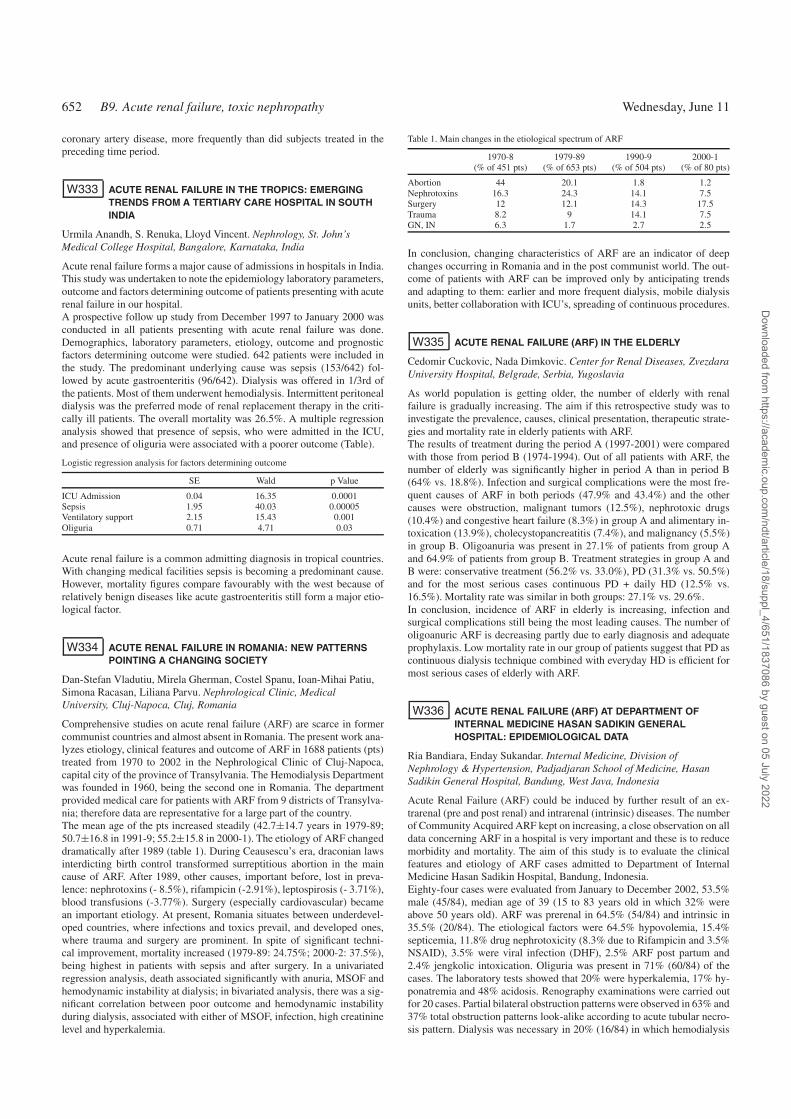
Table 1. Main changes in the etiological spectrum of ARF
1970-8 1979-89 1990-9 2000-1(% of 451 pts) (% of 653 pts) (% of 504 pts) (% of 80 pts)
Abortion 44 20.1 1.8 1.2Nephrotoxins 16.3 24.3 14.1 7.5Surgery 12 12.1 14.3 17.5Trauma 8.2 9 14.1 7.5GN, IN 6.3 1.7 2.7 2.5
In conclusion, changing characteristics of ARF are an indicator of deepchanges occurring in Romania and in the post communist world. The out-come of patients with ARF can be improved only by anticipating trendsand adapting to them: earlier and more frequent dialysis, mobile dialysisunits, better collaboration with ICU’s, spreading of continuous procedures.
W335 ACUTE RENAL FAILURE (ARF) IN THE ELDERLY
Cedomir Cuckovic, Nada Dimkovic. Center for Renal Diseases, ZvezdaraUniversity Hospital, Belgrade, Serbia, Yugoslavia
As world population is getting older, the number of elderly with renalfailure is gradually increasing. The aim if this retrospective study was toinvestigate the prevalence, causes, clinical presentation, therapeutic strate-gies and mortality rate in elderly patients with ARF.The results of treatment during the period A (1997-2001) were comparedwith those from period B (1974-1994). Out of all patients with ARF, thenumber of elderly was significantly higher in period A than in period B(64% vs. 18.8%). Infection and surgical complications were the most fre-quent causes of ARF in both periods (47.9% and 43.4%) and the othercauses were obstruction, malignant tumors (12.5%), nephrotoxic drugs(10.4%) and congestive heart failure (8.3%) in group A and alimentary in-toxication (13.9%), cholecystopancreatitis (7.4%), and malignancy (5.5%)in group B. Oligoanuria was present in 27.1% of patients from group Aand 64.9% of patients from group B. Treatment strategies in group A andB were: conservative treatment (56.2% vs. 33.0%), PD (31.3% vs. 50.5%)and for the most serious cases continuous PD + daily HD (12.5% vs.16.5%). Mortality rate was similar in both groups: 27.1% vs. 29.6%.In conclusion, incidence of ARF in elderly is increasing, infection andsurgical complications still being the most leading causes. The number ofoligoanuric ARF is decreasing partly due to early diagnosis and adequateprophylaxis. Low mortality rate in our group of patients suggest that PD ascontinuous dialysis technique combined with everyday HD is efficient formost serious cases of elderly with ARF.
W336 ACUTE RENAL FAILURE (ARF) AT DEPARTMENT OFINTERNAL MEDICINE HASAN SADIKIN GENERALHOSPITAL: EPIDEMIOLOGICAL DATA
Ria Bandiara, Enday Sukandar. Internal Medicine, Division ofNephrology & Hypertension, Padjadjaran School of Medicine, HasanSadikin General Hospital, Bandung, West Java, Indonesia
Acute Renal Failure (ARF) could be induced by further result of an ex-trarenal (pre and post renal) and intrarenal (intrinsic) diseases. The numberof Community Acquired ARF kept on increasing, a close observation on alldata concerning ARF in a hospital is very important and these is to reducemorbidity and mortality. The aim of this study is to evaluate the clinicalfeatures and etiology of ARF cases admitted to Department of InternalMedicine Hasan Sadikin Hospital, Bandung, Indonesia.Eighty-four cases were evaluated from January to December 2002, 53.5%male (45/84), median age of 39 (15 to 83 years old in which 32% wereabove 50 years old). ARF was prerenal in 64.5% (54/84) and intrinsic in35.5% (20/84). The etiological factors were 64.5% hypovolemia, 15.4%septicemia, 11.8% drug nephrotoxicity (8.3% due to Rifampicin and 3.5%NSAID), 3.5% were viral infection (DHF), 2.5% ARF post partum and2.4% jengkolic intoxication. Oliguria was present in 71% (60/84) of thecases. The laboratory tests showed that 20% were hyperkalemia, 17% hy-ponatremia and 48% acidosis. Renography examinations were carried outfor 20 cases. Partial bilateral obstruction patterns were observed in 63% and37% total obstruction patterns look-alike according to acute tubular necro-sis pattern. Dialysis was necessary in 20% (16/84) in which hemodialysis
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

Wednesday, June 11 B9. Acute renal failure, toxic nephropathy 653
were used in 70% (11/16) of the cases. The mortality of ARF associatedmainly to septicemia was about 11%.More attention should be given to drug-induced ARF. The prognosis couldbe markedly improved if the diagnoses is made in the earlier stage andtreats the patients as early as possible.
W337 EPIDEMIOLOGY OF ACUTE RENAL FAILURE IN ANELDERLY POPULATION IN TERUEL (SPAIN)
Luis Miguel Lou1, Beatriz Boned2, Ana Cruz3, José Antonio Gimeno4,Ricardo Gómez1. 1Nephrology, Alcañiz Hospital, Alcañiz, Teruel, Spain;2Clinical Biochemistry, Alcañiz Hospital, Alcañiz, Teruel, Spain;3General Medicine, Alcañiz Health Center, Alcañiz, Teruel, Spain;4Internal Medicine, Alcañiz Hospital, Alcañiz, Teruel, Spain
Acute renal failure (ARF) epidemiology in developped countrys is chang-ing due to increase of elderly patients with cardiovascular pathology. Thereare few studys about this fact. The objective of this work is to assess ARFfeatures in our population in order to recognize incidence, etiological fac-tors and to establish adequate preventive measures.The study was done in the Alcañiz area (Teruel, Spain), comprising apopulation of 79.963 served by our general hospital. Ageing rate was high(>65 years/<15 years=103,2).In a 12-month prospective study, all patientsserum creatinine≥2 mg/dl were extracted by computer from all results is-sued by our laboratory and brought to the attention of the renal team.ARF was defined as a temporary rise in serum creatinine to≥2 mg/dl ora rise of at least 50% above their initial value in patients with previouslyknown impaired renal function. We analysed age, sex, diuresis, etiology,type of ARF, pre-existing chronic diseases and ARF outcome. Ninety-ninepatients with ARF (58 males, 41 females) were identified, a crude inci-dence rate of 1.238 cases/million/year. Mean age at presentation was 80,3± 10 years (87%≥70 years). Previous chronic diseases were frequent (hy-pertension 54%, heart failure 41%, diabetes 39%, cerebrovascular disease34%, chronic renal failure 25%). Previous cardiovascular treatment (35,4%renin-angiotensin system (RAS) blockade, 50,5% diuretics) and NSAIDs(10%) were frequent too. ARF prerenal were 60%, renal 31% and postrenal9%. 34,7% were caused by volume depletion, 23,4% by low cardiac outputand 23,4% by infection. 44,4% were oligoanuric. 79% were contracted out-side hospital and 21% in hospital. ARF had an iatrogenic element in 35,2%.RAS blockade, diuretics and NSAIDs were frequently implicated, particu-larly associated with fluid depletion. The commonest causes of ARF aris-ing in hospital were prerenal uraemia and acute tubular necrosis, derivedfrom an inadequate volume repletion, incorrect aminoglucosides dosageand NSAIDs. A mortality rate of 36,4% was registered. Comorbid condi-tions, oligoanuria, renal ARF and albumin level were significant mortalityfactors.ARF is most frequent caused by an isquemic or nephrotoxic insult to thekidney and a significant proportion is preventable. In the next years, theincrease of elderly patients with cardiovascular pathology, cardiovasculartreatment (RAS blockade and diuretics) and NSAIDs treatment could causean increase of ARF incidence and modify the etiology. In our study, ARFincidence is higher than in previous series, and these features associatedwith moderate fluid depletion, heart failure and infections are the maincauses. An important ARF ratio is extrahospitalary. Clear guidelines, easilyaccessible at the point of care, could aid the prevention and diagnosis. Anadequate volume repletion and prevention of aminoglucosides and NSAIDsnephrotoxicity are necessary to prevent hospitalary ARF.
W338 DIALYSIS DEPENDENT ACUTE RENAL FAILURE ONINTENSIVE CARE UNIT - PROGNOSIS AFTER SURGERYAND IN PATIENTS WITH MEDICAL REASONS
Thomas Rath, Martina Gradinger, Bernd Weber, Ulla Albert,Franz-Werner Albert. Department of Nephrology and TransplantationMedicine, Klinikum-Kaiserslautern, Kaiserslautern, Germany
Acute renal failure (ARF) is a frequent complication in patients on intensivecare unit (ICU) with substantial influence on mortality of these patients.It may be assumed that pts. with ARF would have higher mortality ratesthan pts. with kown end-stage-renal-disease (ESRD-pts.) treated on ICU.Therefore we analysed the in-hospital mortality of dialysis dependent ARF
after surgery and in ARF-patients with medical reasons without surgery incomparison to ESRD-pts.treated on ICU.Retrospective analysis of all adult ICU-patients with dialysis dependentARF in a tertiary care hospital and of all adult ICU patients with knownend-stage- renal-disease (ESRD-pts.) from 1.1.2001 until 31.12.2002.There were 201 pts. with dialysis dependent ARF and 85 pts. with ESRDon ICU. Main indication for dialysis was fluid management followed byelectrolyte disorder and acidosis. 106 of 201 (52,7%) ARF-pts. were treatedon ICU because of medical reasons and 95 of 201 (47,2%) of ARF-patientshad prior surgery, the majority of these (88%) had undergone cardiovascu-lar surgery. The in-hospital mortality was 42,1% for patients with ARF and29,4% for pts. with ESRD (p < 0,05). Mortality after surgery for all pts.was 43,9% and for pts. with medical reasons 35,3% (p < 0,05). Mortalityin pts. with ARF after surgery was 50,5% whereas mortality after ARFon medical reasons was 34,9% (p < 0,05). In ESRD-pts. mortality aftersurgery was 14,2% and after medical reasons 35,9% (p< 0,05). 54 (18,1%)of all pts. were treated at least once with CRRT on ICU, 65% after surgerywith 66% mortality and 35% without surgery and a mortality rate of 36%.In general pts. with ARF were older than patients with ESRD on ICU(68,4±10,6 vs. 62,4 ± 12,7 years; p < 0,05). There was no influence ofage on mortality either in pts. with ARF nor in pts. with ESRD regardlessof precedent surgical intervention. Mortality of dialysis-dependent ARFafter surgery, especially after cardiovascular surgery, is remarkably highcompared with mortality of ESRD-pts. after surgical interventions. TheMortality-rates in pts. with ARF induced by medical reasons showed nodifference compared to ESRD-pts. on ICU. Patients selected for CRRTshowed additional higher in-hospital mortality.
W339 AGE AS A ONE OF THE SIX RISK FACTORS IN THE NEWPREDICTIVE SCORE FOR OUTCOME IN PATIENTS WITHACUTE RENAL FAILURE
Liljana Tozija, Olivera Stojceva-Taneva, Zvezdana Antova,Koco Cakalaroski. Department of Nephrology, Medical Faculty, Skopje,The Former Yugoslav Republic of Macedonia
Unpredictability of the outcome as well as high expenses of the treatmentfor patients with acute renal failure (ARF) were the causes for statisticalanalysis of the risk factors (RF) that can have important role in outcome ofthis syndrome. In a period of 4 yrs, in our population of 112 patients (pts),prospectively, were analyzed 68 clinical and laboratory RF. With univariantand diskriminant statistical analysis, we find that 27 Rf were determined asstatistical significance with the outcome of ARF. One of these was age withp=0.0075, and the possibility that patients older than 53 years could be-long to group1 (Gr1/nonsurvivals). With diskriminant analysis 27 Rf wereselected to 8. Statistical parameters for inclusion were: mean value F statis-tic 32, p<0.05 and number of appearance of selected RF in 32 models ofpopulation. In the definitive predictive score for ARF (PS-ARF) we have 6parameters, selected RF with logistic regression, influencing the outcome inARF. One of these is age, coded in 8 groups according with the decades ofyears. The others were: number of trombocytes, values of bilirubin, Glas-gow coma scale, hematocrit, mean arterial preassure. The equation was:PS-ARF (predictive score-Acute renal failure)= 2*GCS_M0SF (Glasgowcoma scale) + BILIRUBIN(S)-_SOFA + MAP_SOFA + 0.5*TROMBO-CYTES_SOFA + 0.5*AGE_COD + 0.5*HEMATOCRIT_COD. Compar-ing the new system with the previously determined and accepted systemhas shown that the new system has higher classification possibilities withless numbers of parameters for assessment
W340 CLINICAL-PATHOLOGICAL FEATURES OF DIFFERENTDRUG-ASSOCIATED ACUTE TUBULOINTERSTITIALNEPHRITIS
Xiaomei Li, Jinrong Ma, Siqin Bao, Li Yang, Haiyan Wang. RenalDivision, Department of Medicine, First Hospital and Institute ofNephrology, Peiking Universtity, Beijing, China
Previous survey from cases with renal biopsy has shown that the preva-lence of acute tubulointerstitial nephritis in our hospital rise from a aver-age 1% to 5% in the recent decade. It has also been noticed that drug-associated acute tubulointerstitial nephritis (D-ATIN) is account for more
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

654 B9. Acute renal failure, toxic nephropathy Wednesday, June 11
than 70% of whose acute renal failure(ARF) caused by ATIN or acutetubular necrosis(ATN). The purpose of this study was to investigate theincidence, clinical-pathological features and outcome of D-ATIN causedby different drugs. 362 in-patients with intrinsic ARF (Scr ≥ 177mmol/Land BUN≥ 9.4mmol/L)were studied retrospectively. 67 cases defined asD-ATIN were further analyzed. Their outcome was evaluated as extremelyeffective(Scr<177mmol/L), effective(recovered more than 30% of highestlevel but Scr ≥ 177mmol/L) or inefficiency(no change at all) after treat-ment for two months. The results shown that incidence of D-ATIN was22.1% in 362 cases with intrinsic ARF. In 67 cases with D-ATIN who hadcomplete record, responsible drugs for ATIN included antibiotics (35%),antipyretic analgesics (8.8%), antibiotics combined with antipyretic anal-gesics(12.5%), different kinds of Chinese Herbs or pills(27.5%), and othertoxic drugs(16.2%). In 85% cases, D-ATIN onset was at one week up toone month after taken drug. The unifying presentation in D-ATIN was thatan abrupt onset of urine abnormality and renal dysfunction. Clinical man-ifestations of antibiotics- or antipyretic analgesics-induced ATIN usuallyfirst presented as decreased urinary volume or oliguria(40-80%). Skin rashwas found mostly in b-lactams antibiotics-(25%) and Macrolides-(27.3%),especially in combination of antibiotics and antipyretic analgesics-inducedATIN(43%). Drug related fever mainly was found in Quinolone-inducedD-ATIN(50%). Anemia, accompanied by renal tubular dysfunction with orwithout non-oliguric ARF, was seen in most Chinese herb GMT-induced D-ATIN. Pathological characteristics of antibiotics-ATIN was revealed tipicalAIN or ATN. However, there were severe degradation, necrosis and col-lapse of the renal tubular epithelial cells leaving the basement membranenaked in Chinese herb GMT induced-ATIN. Marked tubular atrophy andearly occurrence diffuse interstitial fibrosis were detected in both Chineseherbs GMT- and antipyretic analgesics-induced ATIN. Based on withdraw-ing the suspected drug and supportive therapy, renal function could full orpartially recovered in 85.9%of D-ATIN patients after a prednisone therapy(20∼40mg/d) for 2∼4 weeks with or without hemodialysis. In conclusion,D-ATIN has become one of important cause of ARF in the adults. An-tibiotics, antipyretic analgesics and specific Chinese herb have to be paidmore attention as main cause of D-ATIN. Most of patients with D-ATINare clinical reversible if early diagnosis and theraputic interventions couldbe done. It is warned that D-ATIN induced by Chinese herb GMT andantipyretic analgesics may have tendency to the early emerged and rapidlyprogressed fibrosis.
W341 PREDICTION OF OUTCOME IN PATIENTS WITH SEPSIS
Wim Van Biesen1, Itir Yegenaga2, Raymond Vanholder1,Francis Colardyn3, Norbert Lameire1. 1Renal Division, UniversityHospital Ghent, Ghent, Belgium; 2Department of Nephrology, KocaeliUniversity Medical School, Izmit, Turkey; 3Intensive Care Department,University Hospital Ghent, Ghent, Belgium
Sepsis has a high morbidity and mortality. Knowledge on risk factors formortality in this specific patients is important for prediction of outcome,and for risk stratification. We wanted i) to test two existing scores foroutcomes in patients with sepsis on the ICU, and ii)develop our own scor-ing system. All patients treated at the ICU of the Univ Hosp between1/1/2001and 31/12/2001 were included if they had a Screa < 2mg% onadmission, and developed de novo sepsis, which was defined accordingto ACCP/SCCM criteria. Discriminant analysis was used to construct theUZG survival score. RoC curves were constructed for prediction of in-hospital mortality. 257 patients developed de novo sepsis during their stayon ICU. Survivors compared to non-survivors, were older (62.9± 17.1 vs53.4± 16.6, p<0.0001), had a lower Salbumin (2.3± 0.6 vs 2.7± 1.5,p=0.039), a higher INR (2.9± 1.7 vs 2.3± 1.3, p=0.006), a lower dias-tolic and mean RR (48.1± 9.4 vs 51.4± 9.9, p=0.013 and 65.3± 12.9 vs68.4± 12.5, p=0.076), a higher Screatinine (11.0± 3.9 vs 9.5± 3.2, p=0.001), and a higher colloid fluid loading over the first 3days (1529± 1521vs 1095± 1196, p= 0.018). In the non-survivors, there was a higher inci-dence of ARF (27.6 vs 4.6%, p<0.0001), of liver failure (14.5 vs 6.7%,p=0.0001), a higher need for mechanical ventilation (88% vs 21.5%, p=0.07), and use of vasopressors (71.3% vs 54.2%, p= 0.007), and of diuretics(28.9 vs 16.1%, p=0.02). In the logistic regression, presence of ARF (B=2.1, p= 0.0001), liver failure (B= 1.3, p= 0.01) and need for mechanicalventilation (B=1.12, p= 0.04) were included in a stepforward model. The
following standardized canonical discriminant function contained 100% ofthe variability: (ATN*0.81) + (ventilation*0.29) + (age * 0.131) – (albumin* 0.096) + (INR * 0.049) – (vasopressors * 0.042) – (diastolic RR * 0.35)+ (mean RR * 0.395) + (Screa at day 0 * 467) – (Screa at day 1 * 727)+ (colloid fluid loading * 0.209) + (use of diuretics * 0.279) + (bilirubin* 0.346), and this score was used to create the UZG survival score. Usingbootstrapping techniques, a correct classification overall of 70.4% with theUZG survival score was obtained. However, 20.9% of patients who sur-vived, were predicted to die. There was a good correlation of the UZGsurvival score with the ApacheII score (Rho= 0.2, p= 0.006), but not withthe SOFA score (Rho= 0.042, p= 0.6). In conclusion, the correct predic-tion of survival in patients with sepsis remains difficult, and no treatmentsshould be stopped based on these scores. This lack of a good risk strat-ification in sepsis has also important implications for the comparison ofdifferent patient groups.
W342 ACUTE RENAL FAILURE AND PROGNOSIS. APROSPECTIVE OBSERVATIONAL STUDY
Javier Lavilla1, Astrid Hernandez1, Juaquin Manrique1, Esther Rossich1,Dolores Pujante1, Nuria Garcia-Fernandez1, Pedro Errasti1,Andres Purroy1, Jokin De Irala2. 1Nephrology, Clinica UniversitariaNavarra, Pamplona, Navarra, Spain; 2Epidemiology, Facultad deMedicina, Pamplona, Navarra, Spain
Objective We performed a prospective study to determine prognostic fac-tors in Acute Renal Failure (ARF).Methods: A total of 828 patients with acute renal failure (creatinine in-crease> 20%) were included. 69.4% were men and mean age was 59 years(SE 0.563). Mortality rate was 22.3%. The main cause of death was cardio-vascular diseases (53.8%) and respiratory diseases (21.1%). We determi-nated epidemiological, clinical variables (ARF etiology, underlying diseaseand ARF treatment) and prognotic scores (Liaño‘s Individual Severity In-dex -ISI- and Multiple Organ Dysfunction Score -MODS-). ARF etiologyclassification criteria was: prerenal (renal hypoperfusion), renal (intrinsicrenal failure, acute tubular necrosis), mixed (prerenal and renal factors)and postrenal (obstruction). Statistical analysis were performed with SPSS9.0 software (chi square, ANOVA and multiple regression analysis). P lessthan 0.05 was considered statiscally significant.Results: The study was conducted from January 1999 through June2002. The age neither the sex had a significant effect on mortality. Mor-tality rate according to ARF etiology was: mixed renal and prerenalARF (37.2%), prerenal ARF (18.3%), renal ARF (14.9%) and postrenalARF (2.9%), p<0.001. Mixed ARF was associated with an inflamma-tory process, p<0.001. Mortality rate was higher in this group of patients(57.8%), p< 0.001. The ARF treatment was: conservative (69.2%), in-termittent hemodialysis (15.1%), continuous renal replacement therapy(CRRT) (12.9%) and both of them (7%). In the group which recievedCRRT mortality was higher (69.2%), p< 0.001. Mean ISI score was 0.32(SE 0.02) and this had an area under the ROC curve of 0.875 (IC 95%0.842-0.907). ISI score was higher in patients with mixed ARF (0.4483SE 0.0, p<0.001), inflammatory process (0.4552 SE 0.02, p<0.001) andtreated with CRRT (0.7302 SE 0.03, p<0.001). ISI clinical variables asso-ciated with prognosis by multivariate analysis were coma (OR 13.8 IC 95%8.5-22.5, p<0.001), jaundice (OR 3.6 IC 95% 2.17-5.98, p<0.001) andoliguria (OR 3.57 IC 95% 2.23-5.73, p<0.001). Organ nonrenal failuresassociated with outcome in ARF by multivariant analysis were respiratory
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

Wednesday, June 11 B9. Acute renal failure, toxic nephropathy 655
(OR 2.99 IC 95% 2.22-4.01, p<0.001), neulologic (OR 2.62 IC 95% 1.56-4.4, p=0.003), cardiovascular (OR 1.84 IC 95% 1.38-2.45, p<0.001) andhepatic failure (OR 1.76 IC 95% 1.37-2.26, p<0.001).Conclusions: Acute renal failure has high mortality. The mortality in thesepatients depend on underlying disease. ARF with the presence of multi-organ dysfuction syndrome, oliguria, and treated with CRRT have a pooroutcome. ISI score is a good prognosis index.
W343 ACUTE RENAL FAILURE (ARF) TREATED WITHHEMODIALYSIS (HD) IN INTENSIVE CARE UNIT (ICU):RETROSPECTIVE MONOCENTRIC STUDY
Antonio Santoro1, Elena Mancini1, Graziella Marvasi2, Chiara Zanzani2,Rossella Gaggi1, Cristina Canova1, Stefano Faenza2.1Malpighi-Nephrology and Dialysis, Policlinico S:Orsola-Malpighi,Bologna, Italy; 2Institute of Anesthesiology and Intensivce CareMedicine, Policlinico S.Orsola-Malpighi, Bologna, Italy
ARF in the critical patient on ICU is considered to be a factor making prog-nosis worse. In order to identify the epidemiology and predictive outcomefactors, we have analysed all the ARF cases needing HD we followed upat the Adult Intensive Care Unit of the Policlinico S. Orsola-Malpighi (notincluding heart surgery patients). Out of 128 cases (93 M, 35 F; 63.4±15years; intermittent dialysis (ID) in 85 and continuous (CD) in 44) the over-all mortality was 40.6% (30.9% in ID, 60.4% in CD). Access to ICU wasdue to medical causes in 41.7% of the cases, with a 54% mortality rate,and in the remaining cases due to surgical reasons (32% emergency and26.3% first-choice treatment, with a mortality of 48.3% and 29.2%, respec-tively). The aetiology of ARF was multifactorial in 64.8% of the cases. Itsdistribution, in relation to mortality, was the following:
Aetiological factor Prevalence Observed mortality
Hypovolemia 68.3% 37%Sepsis 26.3% 66.7%Pharmacological nephrotoxicity 24.2% 63.7%Myocardial insufficiency 24.2% 54.5%
Diuresis upon entry was < 200 ml/die in 23 patients, 16 of whom (69.6%)subsequently died.No differences emerged between survivors (S) and non-survivors (non-S)in terms of age, the presence of major concomitant pathologies (APACHEIII), the number of hospitalisation days, the overall number of dialysis ses-sions and the number of days elapsing between ICU entry and the deliveryof the first HD. The trends in urea, creatinine, diuresis and the APACHE II,SAPS II, SOFA scores, resulted to be significantly different between S andnon-S at the time of the first dialysis and at exit (death or transfer to an-other ambient), but not upon entering ICU. Severe respiratory insufficiencyrequiring assisted mechanical ventilation for over 96 hours accompanied a78% mortality rate.In conclusion, the analysis of these data shows that: 1) hypovolemia isthe most frequent aetiological factor in ARF, but has a lower mortalityrate compared with nephrotoxicity and sepsis; 2) the presence of oliguriaupon entering ICU is a strong predictive factor of a very poor prognosis;3) the severity scores upon entrance are not capable of predicting the out-come, while they acquire a good predictive value at the start of dialysistreatment; 4) prolonged respiratory insufficiency is the co-morbidity factormost closely linked to disease development; 5) the high mortality rate incontinuous dialyses is affected by the negative patient selection.
W344 THE INCIDENCE AND 90 DAY OUTCOME OF ACUTERENAL FAILURE REQUIRING RENAL REPLACEMENTTHERAPY IN SCOTLAND
Jyoti Baharani1, Wendy Metcalfe3, Heather Martin1, Lawson Loraine1,W. Cairns Smith3, Keith Simpson2, Alison MacLeod1, Izhar Khan1.1Medicine and Therapeutics, University of Aberdeen, Aberdeen, UnitedKingdom; 2Public Health Medicine, University of Aberdeen, Aberdeen,United Kingdom; 3Scottish Renal Registry, Glasgow, United Kingdom
We have conducted the first comprehensive, prospective national studyof the incidence of ARF receiving RRT in Scotland. The Acute Renal
Failure in Scotland study (ARFS) has registered adult patients in Scotland(population 5 122 500) with ARF, acute on chronic renal failure (ACRF)and CRF receiving their first RRT over a 9-month period. The aim of thisstudy was to establish the incidence of ARF receiving RRT in a definedpopulation and to determine the outcome of these patients at a 90-dayperiod.All adult patients in Scotland receiving their first RRT were identifiedby regular phone calls and visits to all 20 Scottish hospitals offering thistreatment. In addition to this, some Scottish patients may occasionallyreceive RRT in the north of England and these hospitals were included inour study. For the purpose of data collection we divided Scotland into 3regions.
We completed a standard data collection form for each patient registeredinto the study.Over a recruitment period of 36 weeks, 878 patients fulfilling study criteriafor ARF and ACRF were identified (mean age 62.1 years, 61% male).The results are shown in the table below.
ARF and ACRF in Scotland
NORTH SOUTH-EAST WEST
Number of ARF 189 145 261Number of ACRF 65 89 129Total number of patients 254 234 390Number of Hospitals offering RRT for
ARF in this region 3 6 11Population 1 200 500 1 373 900 2 548 100Incidence of ARF and ACRF p.m.p/year 282.1 227.1 204.1
We found an incidence of 223 p.m.p/year for ARF and ACRF receivingRRT; a third of these cases occur in patients with a degree of pre-existingrenal impairment (ACRF). 54% of all patients received their first treatmentin the intensive care unit and mortality in ARF for all patients by 90 dayswas 47%.In this first comprehensive prospective national study of ARF receivingRRT in a defined population we have found that the incidence of ARFrequiring RRT is much higher than that previously reported from the UK(Khan et al, QJM 1997 90: 781-785). The mortality for patients with ARFcontinues to remain high and over half the patients have their initial treat-ment in the intensive care unit.
# EPIDEMIOLOGY, RISK FACTORS AND OUTCOME OFHOSPITAL-ACQUIRED RENAL FAILURE
Pascal Meier1, Daniel Teta1, Georges Halabi1, Frederic Barbey1,Jean-Blaise Wasserfallen2, Michel Burnier1. 1Division of Nephrology,CHUV; 2Department of Medicine, CHUV, Lausanne, Switzerland
Acute renal failure (ARF) is a serious condition that often develops inhospital. The goal of this analysis was to obtain data on the incidence,etiology, associated risk factors and prognosis of hospital-acquired renalfailure (HARF) in a 3-year (2000-2002) computer-assisted retrospectivestudy. ARF was defined as a sudden rise in serum creatinine (Scr) > 177µmol/L in patients with a previously normal renal function or a suddenrise (>50%) in Scr in patients with previous mild-to-moderate chronicrenal failure (CRF) (Scr < 264 µmol/L). Decreased renal perfusion wasconsidered if there was a weight loss accompanied by signs of volumedepletion or a decrease in blood pressure to < 90/60 mmHg. Radiographiccontrast media were incriminated when Scr increased within 48 h of the
# Author declined to present
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

656 B9. Acute renal failure, toxic nephropathy Wednesday, June 11
procedure. Medications were implicated when the increase in Scr was tem-porally related to their administration. Renal failure was considered post-operative when Scr increased within 48 h of a surgical procedure. Sepsiswas defined by positive blood cultures accompanied by hemodynamic in-stability. Obstruction was deemed responsible for ARF if it was evidenton radiographic studies with improvement in renal function with relief ofobstruction. To be included, the patients with HARF should have followingoutcomes: complete recovery of renal function, partial recovery, dischargewith an increasing Scr, discharge on dialysis therapy, or death. One hun-dred thirty nine episodes of HARF were identified (131 patients, 0.52%of admissions, and 5.2% in ICU populations). Daily urine output and uri-nalysis was performed in 97% and 93% of episodes, respectively. Themean±SD age of the patients was 61±13 years with a 65% male predom-inance. The most common cause of HARF was decreased renal perfusion(49%). Twenty episodes (15%) were attributed to medications (aminogly-coside 5%) and 10% to radiocontrast. Five % of cardiac surgery patients(18% heart transplant), 15% of liver transplant patients and 28% of traumapatients developed HARF. In our population, 52% of HARF cases occurredin patients over 65 years (38% of the hospitalised population). In a multi-variate analysis, Scr> 177mmol/L, oliguria, urine sediment abnormalities,cardiovascular failure and infection were independent risk factors for bothHARF and higher mortality. Acute tubular necrosis (ATN) (47%), prerenalARF (22%), acute-onset CRF (15%) and obstructive ARF (8%) were themost frequent clinical forms. Six patients (7.9%) required long-term dial-ysis. Total mortality associated with HARF was 19% (76% ICU). One inevery 59 patients who died within the hospital did so in the course of anARF episode (ICU excluded). Patients requiring RRT (42%) had a highermortality rate (p = 0.012). The highest mortality was observed in ATNcases (60%), followed by vascular, vasculitis, prerenal and acute-onsetCRF. HARF is a serious condition induced at a high rate resulting from arelatively small number of processes. Epidemiologic data are particularlyuseful in identification of at-risk patients, where preventative therapies andearly interventions might be employed.
W346 SURVIVAL RATES IN PATIENTS WITH ACUTE RENALFAILURE: SINGLE CENTER 15 YEARS RESULTS
Milan Radovic1, Mina Tomovic2, Sanja Simic-Ogrizovic1,Vladimir Ostric1, Visnja Lezaic1, Ljubica Djukanovic1. 1Clinic ofNephrology, Clinical Center of Serbia, Belgrade, Serbia, Yugoslavia;2Institute of Anesthesiology, Clinical Center of Serbia, Belgrade, Serbia,Yugoslavia
Acute renal faliure (ARF) outcome is one of the most important issuessin nephrology. The aim of the study was to compare the frequencies ofdeadly outcome in ARF patients (pts), who needed intermittent hemodial-ysis (IHD) treatment, during 15 years’ period (1987-2001). From the pop-ulation of 583 pts (age 49.4 ± 15.2,428 male,155 female), 233 (40%) outof pts had medical and 288 (49%) surgical causes of ARF occurrence.Mortality in surgical group (62.5%) was significantly higher than medical(43%) χ2=19.08, P<0.0001. In surgical group, ARF treated by IHD af-ter aortic surger had highest mortality (73%), folowed by general surgery(67.5%) and polytrauma (54%), but not with significant difference com-paring each other. In group of patients with medical causes of ARF, ptswith liver failure had highest mortality rate (85%), followed by pts withARF caused by cardiovascular diseases (68%), sepsis (56%), HUS (46%),hemoragic fever with renal syndrome (24%), toxic (22%) and leptospirosis(19%). Significant difference in mortality was found between liver faliure,cardiovascular, septic and HUS pts who did not differ significanlty betweeneach other (p>0.05), comparing to HFRS, toxic and leptospirosis pts onthe other side (p<0.05). These results stressed the influence of preexsistingatherosclerotic and diffuse endothelial diseases on ARF outcome.
W347 PREDICTORS OF MORTALITY IN ELDERLY PATIENTSWITH ACUTE RENAL FAILURE
H.S. Kohli, A. Bhat, K. Sud, V. Jha, K.L. Gupta, V. Sakhuja. Departmentof Nephrology, PGIMER, Chandigarh, UT, India
Patients of acute renal failure (ARF) have an increased morbidity and mor-tality not only due to renal failure per se but also due to associated illnesses.
There is ongoing debate on the risk for mortality from ARF in the elderly.This prospective study was undertaken to study the predictors of mortal-ity in elderly population from India with ARF. All elderly patients (>60years) with ARF who were hospitalized at this tertiary care centre be-tween July 2001 to June 2002 were studied. Various predictors of mortalitystudied included type of ARF (medical or surgical;hospital or commu-nity acquired), causes of ARF (sepsis, hypoperfusion, toxic nephropathy,acute interstitial nephritis), presence of co-existing diseases [cardiovas-cular disease (CVSD) respiratory system disease (RSD), central nervoussystem disease (CNSD), malignancy, liver disease, hypertension, diabetes}, severity of renal failure (initial and peak serum creatinine, oliguria, needfor dialysis), complications of ARF (bleeding and infection), serum albu-min levels and number of organ failure.Of 33301 patients admitted to the hospital over 1 year 4255 (12.7%) wereelderly, of these 69 (1.6%) had ARF. Mean age was 65.1± 45.9 (60-80years). Forty two (60.9%) patients died. Hospital acquired ARF was as-sociated with significantly higher mortality as compared to communityacquired ARF [19/24 (79.2%) vs 23/45 (51.1)% p < 0.05], sepsis as causeof ARF was also associated with higher mortality [37/42 (88%) vs15/27(55.5%) p<0.05]. Amongst coexisting diseases, RSD [21/42 (50%) vs 4/27(15%) p < 0.05], CNSD [15/42 (35.7%) vs 3/27 (11.1%) p< 0.05], sepsis[37/42 (88.1%) vs 15/27 (55.5%) p<0.05] were more frequent in non sur-vivors than survivors. Need for dialysis [29/42 (69.1%) vs 12/27 (44.4%)p<0.051], occurrence of bleeding [13/42 (30.9%) vs 1/27 (3.7%) p<0.05]and infection [35/42 (83.3%) vs 4/27 (14.8%) p<0.05] during the courseof ARF were significantly higher in non survivors. Serum albumin was sig-nificantly lower amongst non survivors than survivors ((3 ±0.6 gm/dl vs3.4±0.6 gm/dl, p<0.05). Presence of multiorgan failure in addition to ARFwas associated with significant higher mortality (90%vs20.7% p<0.05).On logistic regression analysis, occurrence of sepsis during the course ofillness (odds ration 55.5 p 0.007) and presence of multiorgan failure (oddsratio 25.6 p 0.01) were the only significant independent risk factors ofmortality.To conclude, ARF complicates only 1.6% of hospitalised elderly patientsbut is associated with a high mortality rate of 61%. occurrence of sepsisduring the course of ARF and presence of multiorgan failure are indepen-dent risk factors of mortality.
W348 DETERMINANTS OF ACUTE RENAL FAILURE (ARF) POSTCARDIOTHORACIC SURGERY (CTS): A PILOT STUDYUTILIZING THE NEW YORK STATE CARDIAC SURGERYREPORTING SYSTEM (CSRS)
Jorge Cerda1, David S. Strogatz2, Javid Saifi3, Jayne Prendergast1. 1Dept.of Nephrology, St. Peters Hospital, Albany, NY, United States; 2School ofPublic Health, SUNY- Albany, Albany, NY, United States; 3AlbanyCardiothoracic Surgeons, Albany, NY, United States
Except for cardiac arrest, ARF is associated with the largest increase inmortality of all post CTS complications. Every effort to avoid its develop-ment is the best strategy to decrease morbidity, mortality, use of resourcesand cost. Previous studies on the determinants of ARF in this setting weredone in the 1980s analyzing predominantly male patients. To our knowl-edge, no studies have addressed the impact of contrast-induced ARF inthis setting. The CSRS is the largest, oldest and most complete prospectivedatabase in the US. Up until now, no studies on ARF have been done utiliz-ing this database because underreporting of ARF made data on incidenceand determinants unreliable. The present study is a pilot analysis of thedeterminants of ARF in a well-defined setting; its results will be utilized toexpand the search into a much larger and diverse population of patients. Inthe years 1999 thru 2001, 43 St Peters Hospital CTS patients were identifieddeveloping de novo dialysis-requiring ARF. Risk factor (RF) analysis uti-lized a case-control design, where 3 patients controls matched by age, sexand time of surgery were randomly chosen for each case (129 controls). Inaddition to the CSRS data, the date of cardiac catheterization (cath), creati-nine clearance (Ccr) calculated by Gaults formula and standard laboratorydata was collected by retrospective chart review. Matched analysis wasconducted and organized to facilitate comparison with published literature.Preoperatively impaired renal function (Ccr<60) was strongly associatedwith ARF (OR=19.2). The presence of CHF was a predictor (OR=15.0)while low LVEF<35%, peripheral vascular disease and COPD were asso-
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

Wednesday, June 11 B9. Acute renal failure, toxic nephropathy 657
ciated with modest increases of risk (OR=2.5, 2.1 and 1.5 respectively). Ashort interval (≤ 2 days) between cath and CTS was associated with onlya slight increase in ARF (OR=1.4). Among preoperative factors, acute res-piratory failure was most strongly associated with ARF (OR=63.0). Post-operative re-bleed requiring operative revision (OR=3.0) and the use ofIABP (OR=3.0) also increased the risk of ARF. Valvular or CABG+valvereplacement surgery, compared with CABG alone (OR=2.0) and a longerextracorporeal bypass time >120 minutes (OR=3.9) were also associatedwith increased risk. Ongoing analysis will include logistic regression mod-els to assess the statistically independent relationship of these and otherRF with ARF. While some of these results agree with previous reports, theimpact of hemodynamic and respiratory instability is particularly signifi-cant. While small, the association between shorter cath to surgery and ARFpoints to a possibly avoidable relationship worth of additional study. Theresults of this study will form the basis for the analysis of a much largersample involving the CSRS database, to enable more effective subgroupanalysis and the possible development of a prediction instrument.
W349 PREDICTION OF ARF IN PATIENTS WITH SEPSIS ON THEICU
Itir Yegenaga1, Wim Van Biesen2, Raymond Vanholder2,Francis Colardyn3, Norbert Lameire3. 1Dept of Nephrology, KocaeliUniversity Medical School, Izmit, Turkey; 2Renal Division, 3IntensiveCare Department, University Hospital Ghent, Ghent, Belgium
Sepsis is is a frequent condition in ICU patients, with a high morbidityand mortality, which are still further enhanced by the development of ARF.Prevention of ARF in sepsis patients is therefore of importance. Knowledgeon the risk factors for ARF in this patient group is therefore important. Wewanted to evaluate different existent predictive scoring systems and todevelop a centre-specific prediction model.All patients on the ICU of the University Hospital Ghent between 1/1/2001and 31/12/2001 were eligible for inclusion, if they had a normal renal func-tion (Screa < 2mg%) on admission, and developed de novo sepsis whichwas defined according to the criteria of ACCP/SCCM. A wide array of bio-chemical and physiological parameters was used to calculate Liano score,SHARF score, SOFA score and APACHE II score on a daily basis. ARFwas determined as a doubling of Screa, or the increase of Screa>2mg%, oroliguria <500ml/24hrs. Data were analysed for the development of ARFby unpaired T test, Chi Square and discriminant analysis to develop an ownprediction model.During the observation period, 257 patients developed sepsis, 29 of whomwith ARF. A standardized discriminant function with the following com-ponents contained 100% of the variability present in the study population:Vasopressor use*0.214 + Liverfailure*0.278 + CVD day0 * 0.433 - CVDday1*0.057 - colloid*0.128 - albumin day 0*0.047 – Screa day 0* 0.166- diuresis *0.162 + age*0.4 - thrombocytes*0.033 + Screa day 1*0.864- cristalloid*0.001. The figure shows the RoC curves for Liano score,SHARF score at day 0, SOFA score at day 0 and the UZG score. Areaunder the curves were 91± 7% for UZG score, 76± 7% for SHARF score,73± 10% for Liano score, 58.5± 5.5% for the APACHEII score, and 51±10% for SOFA score.
Using bootstrapping techniques, correct classification by the UZG scoredecreased from 91.6% in the original population to a mean of 89.8% in thetest population.
Conclusion: Liano and SHARF score have an acceptable predictive powerto predict ARF also in septic patients, despite the fact that these scores werenot specifically developed for this patient group. Our own score, based ondiscriminant analysis, was superior, which is of course partly due to the factthat it was developed at our own unit, a draw back we tried to reduce usingbootstrapping. Prospective testing in another centre is warranted. ApacheII score and SOFA score did not have a discriminative power for ARF inthis population of septic patients.
W350 RISK FACTORS OF RENAL IMPAIRMENT IN PATIENTSUNDERGOING CARDIOPULMONARY BYPASS GRAFTSURGERY
Asli Donmez1, Cigdem Erkaya1, Zubeyde Arat2, Atilla Sezgin3,F. Nurhan Ozdemir2. 1Department of Anesthesiology, Baskent UniversityFaculty of Medicine, Ankara; 2Department of Nephrology, BaskentUniversity Faculty of Medicine, Ankara; 3Department of CardiovascularSurgery, Baskent University Faculty of Medicine, Ankara
Although the incidence of dialysis dependent acute renal failure (ARF) inpatients undergoing open heart surgery is low, milder degrees of renal dys-function are more common. Even though this state is associated with lessmorbidity than overt ARF, they too have a higher number of complicationscompared to patients with normal renal function. In this study we evaluatedthe risk factors for renal impairement before and during open heart surgery.We included, randomly selected 200 patients (men 158/women 42, meanage was 60.4 ±10 years) with preoperative normal renal function whohad coronary artery bypass graft surgery (CABG) during year 2002. Weevaluated preoperative (co-existing disease, age, blood pressure, fluid bal-ance, chronic heart failure, low cardiac output (CO), radiocontrast dyes,drugs), intraoperative (cardiopulmonary bypass (CPB) time, hypoperfu-sion, hemodilution ratio, hemolysis) and postoperative data (extubationtime, blood loss, blood pressure, low CO). Additionally we recordedchanges of serum glucose, s.BUN, s.creatinine, Hb, Htc, fluid balance,urine output/hour and central venous pressure (CVP) variability during the3 stages. According to our data there were 104 patients (group I) with olig-uria (less than 0.5mL/kg/hour urine output during postoperative 72 hours)and 96 (group II) had urine output in normal ranges.Longer CPB and extubation times, postoperative low CO with preopera-tive risk factors and perioperative decline in CVP significantly influencedoliguria according to univariate regression analysis. Among these multi-variante analysis revealed that the preoperative risk factors (being olderthan 60 years RR:1.890, presence of hypertension RR:1.834, preop crea-tinine higher than 1.2 mg/dL RR:3.553 and Hb < 11g/dL RR:2.745) andperioperative decline in CVP (RR:2.830) were the most important ones.Theidentification of the high risk patients and maintenance of optimal hemody-namics are the major factors behind the prophylaxis of ARF in associationwith CABG.
W351 ACUTE RENAL FAILURE AND MORTALITY IN ANINTENSIVE CARE UNIT: USEFULNESS OF A RECENTSEVERITY INDEX SCORE OF THE PROGNOSIS
Piero Dionisio1, Barbara Agostini1, Nadia Chiappini1, Elisa Caramello1,Roberto Bergia1, Michelangelo Valenti1, Mauro-Ilario Berto1,Raffaella Cravero1, Enrico Schillaci1, Alessandro Albani2,Ermanno Spagarino2. 1Department of Nephrology and Dialysis, Ospedaledegli Infermi, Biella, Italy; 2Department of Intensive Care, Ospedale degliInfermi, Biella, Italy
Acute renal failure (ARF) is frequently observed in patients in IntensiveCare Units (ICU) with an incidence varying from 1-25% and is oftenpresent as one of the aspects of multiple organ failure (MOF). In spite of theimprovement in the procedure of diagnosis and treatment, the incidence ofARF and the death-rate connected with it in ICU, has remained relativelyconstant and notoriously high in the past 2 decades arriving up to 80% inpatients recovered in ICU.Aim of this work is to point out the incidence of mortality in patientsin ICU affected with ARF that need a renal replacement therapy (RRT).With this end in view, we have examined retrospectively our case historiesfrom January 2000 to the 31st of December 2002, taking only those patients
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

658 B9. Acute renal failure, toxic nephropathy Wednesday, June 11
affected with acute tubular necrosis (ATN) in the light of a recent prognosticindicator (acute tubular necrosis – index severity score) ATN-ISS proposedby Liano e Coll. (Liano F et al. Nephron 1993).We studied 50 patients (8F-42M) average age 68.92±11.82 subjected toRRT with a death-rate (D) of 68% and functional recovery (FR) in 16cases equal to 32%. We have compared the values of blood urea nitrogen(BUN), creatininemia (Crs), total proteins, albumin, Ks, Nas, HCO3 in 2groups of patients that have had outcome D or FR observing that only thealbuminemia was significantly different in the FR group in respect to theD group 2.79±0.07 vs 2.24±0.07 p<0.0045. The patients were dividedin groups according to the score ATN-ISS and we observed a progressiveincrease of D according to the increase of the severity of the score. Themortality examined shows a very high correlation with the index of Lianop<0.000 in comparison with SAPS II° p<0.032.In conclusion, despite a precocious beginning of RRT, with parametersexamined such as BUN, Crs, total proteins, albumin, Ks, Nas, HCO3, infe-rior to those considered imperative for initiating RRT (Burchardi H, ContrNephrol 2001), the mortality of patients afflicted with ARF is still veryhigh. The index of Liano ATN-ISS is able to predict the outcome of pa-tients affected with ARF and subjected to RRT in ICU. The values ofalbuminemia seem to be important in conditioning the outcome of patients.
W352 RENAL DOPPLER IN EVALUATION OF ACUTE RENALFAILURE (ARF)- A PROSPECTIVE STUDY
Balasubramaniam Jeyaraj, Shanthi Balasubramaniam,Palaniappan Nainar. Nephrology, Kidney Care Centre, Tirunelveli,Tamilnadu, India
ARF is a medical emergency where the outcome depends on early diag-nosis and intervention. Diagnosis based on clinical, laboratory and ultra-sound examination is still imperfect and renal biopsy remains the only goldstandard. Renal biopsy cannot be performed in all situtions. Any new non-invasive investigation, increasing the sensitivity and specificity of clinicaldiagnosis is welcome. Colour Doppler study is a simple, reproducible andeasily available investigation in most centres.We undertook to do Doppler study of intra renal vasculature in non ob-structive ARF and to analyze the usefulness in diagnosis and prognosis ofARF.1. Consecutive cases of non obstructive ARFs were included.2. Clinical classification of ARF into glomerular disease(AGN) and tubu-lointerstitial disease(TI) was made using the clinical setting, quantity ofproteinuria, type of urinary sediments, ASO, C3 level and renal biopsywherever available.3. Cases which could not be clearly categorized into AGN or TI wereexcluded.4. Doppler estimation of Resistive Index (RI) and Pulsatile Index (PI)in the interlobar branches of both renal arteries were done. The resultswere analyzed statistically to see if the indices correlated with the type ofunderlying lesion and the severity of renal failure.Results: Total - 93; AGN - 43; TI - 40
RI Mean PI Mean Creat Mean
AGN 0.675 1.131 4.1TI 0.753 1.454 4.9p p< 0.05 p< 0.05 p> 0.1
AGN TI p value
RI > 0.8 0 22 <0.01RI > 0.75 5 27 <0.01RI < 0.7 31 14 <0.05
1. In ARF, RI and PI of interlobar artery is significantly higher in Tubulointerstitial than Glomerular disease.2. There is a positive correlation between RI/PI and severity of renal failurein ARF due to tubulo interstitial lesion and not glomerular lesion.3. Attention to this variable expression of renal doppler might throw morelight into research of the pathophysiology of ARF due to different lesions.3. Doppler study is a useful tool in evaluation and management of ARF.
W353 PLASMA LEPTIN CONCENTRATION IS NOT INCREASED INPATIENTS WITH NONINFLAMMATORY ACUTE RENALFAILURE
Rafal Ficek, Franciszek Kokot, Jerzy Chudek, Marcin Adamczak,Joanna Ficek, Andrzej Wiecek. Department of Nephrology,Endocrinology and Metabolic Diseases, Silesian University MedicalSchool, Katowice, Poland
Background: Noninflammatory acute renal failure (NARF) is character-ized by impairment of excretory, endocrine, homeostatic and metabolicfunction of the kidneys. Leptin is an adipose derived polypeptide hormonewhich is predominantly eliminated by the kidneys. Plasma leptin concen-tration is increased in chronic renal failure (CRF) but its concentration inpatients with NARF was not investigated until now.The aim of present study was to evaluate plasma leptin concentration inpatients with NARF.Patients and Methods: 27 patients with NARF (age 44±4 years; BMI26.0±0.9 kg/m2; 17 patients: 15M, 2F recovered kidney function and 10patients: 7M, 3F died during the anuric phase), 27 hemodialyzed patients(22M, 5F; age 45±2 years; BMI 26.2±0.8 kg/m2) with chronic renal failure(CRF) and 27 healthy subjects (HS) (22M, 5F; age 42±3 years; BMI25.9±0.6 kg/m2) were examined. Blood samples for plasma leptin androutinely assessed biochemical parameters were withdrawn before the firstHD session (I), and in patients who survived a second time 5 days later atthe anuric/oliguric phase (II) and a third one at the polyuric phase beforethe discharge the patient from hospital (III). In CRF the same parameterswere estimated once before the subsequent HD session.Results: Patients with NARF (before the first HD session) and CRF did notdiffer significantly in respect to BMI, serum creatinine and blood hydrogenion concentrations. Plasma leptin levels in patients with NARF before thefirst HD session were similar to values obtained in HS, but significantlylower (p<0.01) than in patients with CRF (2.5 (1.9-8.2) vs. 3.4 (2.5-8.3)vs. 8.4 (2.9-16.9) ng/ml in NARF, HS and CRF respectively). There wasno significant difference in leptinaemia between patients with NARF whosurvived and who died. Patients with NARF showed lower serum levels ofcholesterol, triglycerides, Na and Ca but higher ones of phosphorus andwhite blood count than patients with CRF. Improvement of renal functionwas accompanied by a slightly declining tendency in plasma leptin con-centration (5.6±2.2 vs. 4.8±1.7 vs. 4.5±1.3 ng/ml; I, II, III respectively).Conclusion: The influence of impaired kidney function on plasma leptinconcentration is less pronounced in patients with NARF then CRF sug-gesting participation of factors others than glomerular filtration rate onleptinaemia in patients with CRF.
W354 PRE-OPERATIVE MICROALBUMINURIA IS ANINDEPENDENT PREDICTOR FOR ACUTE RENAL FAILUREFOLLOWING CORONARY ARTERY BYPASS GRAFT
Haidong Luo1, Sylvia Ramirez1,2, Reida El Oakley1, Stephen Hsu1,2.1Faculty of Medicine, National University of Singapore, Singapore;2Center for Prevention and Research, National Kidney FoundationSingapore, Singapore
Background: Acute renal failure (ARF) after coronary artery bypass graft-ing (CABG) is associated with high morbidity and mortality. Predictors forpost-op ARF are important to define in order to identify high-risk popu-lations. We investigated the predictors of post-op ARF in a multi-racialSoutheast Asian population undergoing CABG. Microalbuminuria (MA)is an established risk factor for adverse cardiovascular and renal outcomesin the general population. We sought to determine whether pre-operativeMA is also an independent predictor of post-op ARF following CABG.Method: Over a 7-month period, 65 consecutive elective and urgent CABGpatients from a major tertiary referral center were enrolled in a largerprospective cohort study to identify predictors and long-term outcomes ofpost-op ARF. Demographic, clinical and pre-op laboratory characteristicswere identified and patients were followed until discharge. MA was definedas a 24-hour urine albumin excretion of 30-300 mg. Control group wasdefined as a 24-hour urine albumin excretion <30mg. ARF was definedas a change in serum creatinine (cr) level of ≥0.5 mg/dl when baselinecr is <2.0 mg/dl (177 umol/l) or ≥1.5 mg/dl when baseline cr is ≥2.0mg/dl.
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

Wednesday, June 11 B9. Acute renal failure, toxic nephropathy 659
Results: Out of the 65 patients (71% Chinese), 12 (18.5%) developedARF. The mean duration of ARF was 3.5±1.5 days. None of the patientsrequired initiation of dialysis. The mean age of the study population was59.3±8.7 yrs, and 84.6% were done electively. On crude analysis, post-opARF was significantly associated with older age (65.5±7.2 vs 57.9±8.4yrs,p=0.005), higher pre-op cr (122±33.8 vs 96.9±21.4umol/l, p=0.03), lowerpre-op ejection fraction (EF) (36±19% vs 46±14%, p=0.03), and lowercreatinine clearance (CrCl) (41±22 vs 70±23 ml/min, p=0.005). MA wassignificantly associated with post-op ARF [10 out of 17 patients (58.8%)in MA vs 2 out of 48 patients (4.2%) in non-MA, p=0.0005], althoughmean duration of ARF did not differ between these two groups (3.8±1.5 vs2.0±0 days, p=0.13). Race (Chinese vs Malay vs Indian, 17.4% vs 26.7%vs 9.1%, p=0.5), pre-op hypertension [21.2%(Yes) vs 10%(No), p=0.22],pre-op diabetes (15.2% vs 23.1%, p=0.4), requirement for urgent surgery(30% vs 16.4%, p=0.27), requirement for intra-op pump use (18.2% vs16.7%, p=0.9) and pre-op ACE inhibitor use (17.5% vs 20%, p=0.52) werenot significantly associated with post-op ARF. After adjusting for age, race,pre-exiting hypertension, diabetes, pre-op CrCl and baseline EF, only MAremained an independent predictor for post-op ARF (OR=51.4, 95% CI:2.3 to 1152.9, p=0.013).Conclusion: Our results suggest that pre-op MA is a strong predictor forARF after CABG surgery, independent of pre-op renal function and pre-existing diabetes and hypertension. Whether or not interventions to reduceMA will lead to a reduction in the risk for post-op ARF remains to bestudied. Nevertheless, our results indicate that patients undergoing CABGwho have pre-op MA are at high risk for post-op ARF, independent of otherrisk factors.
W355 THE EFFECT OF PRE-PROCEDURAL CAPTOPRIL ONCONTRAST-INDUCED NEPHROPATHY IN PATIENTS WHOUNDERWENT CORONARY ANGIOGRAPHY
Omer Toprak, Mustafa Cirit, Serdar Bayata. Internal Medicine, AtaturkResearch and Training Hospital, Izmir, Turkey; Nephrology, AtaturkResearch and Training Hospital, Izmir, Turkey; Cardiology, AtaturkResearch and Training Hospital, Izmir, Turkey
Purpose: Contrast media induced nephropathy (CIN) is diagnosed as theacute renal failure developed following intravenous contrast media usagewhen all other causes of renal failure are excluded. In this study, we inves-tigated the effects of captopril given before coronary angiography (CAG)on CIN development.Method: A total of 80 patients, 43 male and 37 female, mean age: 58 ±8 years (range: 18-80), with serum creatinine level below 2 mg/dl, whounderwent coronary angiography in Cardiology Clinic of Izmir AtaturkTraining and Research Hospital between October 2000- February 2002,were included into the study. Captopril was administered in 48 patientsbefore 8 hours and an hour before CAG (captopril group). Remaining 32patients had no captopril treatment (control group). There was no signifi-cant difference between the groups by means of clinical and biochemicalparameters. The levels of serum creatinine and serum urea and creatinineclearence in 24 hours urine were measured before CAG application and 48hours after the procedure.Results: Five patients (8.3%) in captopril group and 1 patient (3%) in con-trol group developed CIN and this difference was statistically significant(p=0.02).Conclusion: Captopril is a risk factor of developing CIN.
Abstract W355 – Table: The Creatinin Level Change in Control and Captopril Groups
Parameters Captopril Group � Control Group � p of �
Before CAG After CAG Before CAG After CAG
Serum Creatinine 0.91 ± 0.28mg/dl 1.01 ± 0.33mg/dl 0.08 ± 0.27 1.05 ± 0.36mg/dl 1.20 ± 0.4mg/dl 0.145 ± 0.21 0.06
CAG: Coronary Angiography, �: The serum creatinine level after CAG - before CAG
Abstract W355 – Table: Distribution of CIN Developed Patients
Captopril Group (n=48) Control Group (n=32) p
Number and Percent of CIN Developed Patients 5/8.3% 1/3% 0.02
W356 LESSONS LEARNED FROM THE CATASTROPHICMARMARA EARTHQUAKE: FACTORS INFLUENCING THEFINAL OUTCOME OF RENAL VICTIMS
Mehmet Sukru Sever1, Ekrem Erek2, Raymond Vanholder3,Mehmet Koc4, Mahmut Yavuz5, Nilgun Aysuna1, Hulya Ergin6,Rezzan Ataman2, Mujdat Yenicesu7, Basol Canbakan8,Celalettin Demircan9, Norbert Lameire3. 1Nephrology, Istanbul School ofMed., Istanbul, Turkey; 2Nephrology, Cerrahpasa School of Med.,Istanbul, Turkey; 3Nephrology, University Hospital, Ghent, Belgium;4Nephrology, Marmara School of Med., Istanbul, Turkey; 5Nephrology,Uludag School of Med., Bursa, Turkey; 6Nephrology, Goztepe SocialSecurity Hosp., Istanbul, Turkey; 7Nephrology, Gulhane Military Hosp.,Ankara, Turkey; 8Nephrology, Numune Hosp., Ankara, Turkey;9Nephrology, Bursa State Hosp., Bursa, Turkey
During catastrophic earthquakes, crush syndrome is the second most fre-quent cause of death after the direct impact of trauma. The Marmara Earth-quake, which struck Northwestern Turkey in August 1999, was character-ized by 639 crush syndrome victims with acute renal problems. The factorsinfluencing their final outcome have been the subject of this study.Within the first week of the disaster, questionnaires asking about 63 clinicaland laboratory variables were sent to 35 reference hospitals that treated thevictims. Information obtained by means of these questionnaires, includingthe factors with a potential influence on outcome was submitted to analysis.Overall mortality rate was 15.2%. In univariate analysis, nonsurvivors wereolder (p=0.048); and the highest mortality rates were observed among thevictims coming from the closest cities to the reference hospitals. Admissionwithin the first three days of the disaster (p=0.016), with oliguria (p=0.042),lower figures for blood pressure (p<0.001), platelets (p=0.004) and serumalbumin (p=0.005) were associated with mortality. Also, higher body tem-perature (p=0.013) and serum potassium (p<0.001) as well as sufferingfrom thoracic or abdominal traumas, extremity amputations and medicalcomplications other than renal failure (for all four, p<0.0001) in addi-tion to the need of dialysis support (p=0.015) and mechanical ventilation(p<0.0001) indicated higher risk of death. In the multivariate analysis, age(p=0.030, o.r.=1.02), presence of disseminated intravascular coagulation(p=0.001, o.r.=4.49), abdominal trauma (p=0.012, o.r.=4.05) and amputa-tions (p=0.010, o.r.=2.81) were predictors of death. Dialyzed patients werecharacterized by higher mortality rates than nondialyzed victims (17.2%versus 9.3%, p=0.015).Outcome of the renal victims of catastrophic earthquakes is influenced bythe type of trauma, co-morbid events and complications observed duringthe clinical course as well as epidemiological features such as age, distanceto reference hospitals, and time lapse between disaster and admission toreference hospitals. Fasciotomies should be performed only by objectivecriteria.
W357 MANAGEMENT OF CRUSH SYNDROME FOLLOWINGGUJARAT EARTHQUAKE – JAN.2001
Divyesh Viroja, Pravina Shah, H.L. Trivedi, Vina Shah, Aruna Vaniker.Nephrology, IKDRC, Ahmedabad, Gujarat, India
We conducted retrospective analysis of 35 patients admitted with acuterenal failure (ARF) at IKDRC-Ahmedabad following Gujarat earthquake-01, to assess the treatment and outcome of patients with crush syndrome.Out of 35 patients 34 (97.1%) had crush syndrome and one patient hadprerenal ARF. Male:Female ratio 24:11. Mean age of these patients was31.6±10.65 years (16-65). 25 (71.4%) patients were from Kutch district,
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

660 B9. Acute renal failure, toxic nephropathy Wednesday, June 11
10 (28.6%) from other area. Mean period under the debris was 11.64 ±10.03 hours and initiation of primary treatment was 28.71 ± 25.35 hours.Clinically all patients presented with oligoanuria, 28 (80%) with smokyurine and 2 (5.71%) with hypotension. 19 (54.29%) patients sustained frac-tures. 12 (34.28%) involved only lower limb, 1 (2.85%) only upper limb, 2(5.71%) both limbs, 3 (8.57%) vertebral injuries, 1 (2.85%) rib fracture and1 (2.85%) had pelvic bone involvement. Out of them 13 (37.14%) requiredorthopaedic procedures and 6 were treated conservatively. 19 (54.29%)patients had compartment syndrome. 11 (31.43%) patients required fas-ciotomy, 2 (5.71%) were amputed, 5 (14.28%) treated conservatively andone patient expired before amputation. 2 (5.71%) sustained renal traumaand were treated conservatively. 19 (54.29%) patients developed septi-caemia and 17 (48.57%) had disseminated intravascular coagulation duringthe course of treatment. All had high S. creatinine (6.53 ± 2.29mg/dl). 22(62.86%) patients had hyperkalaemia (S.K+>5.5mmol/l) and mean S.K+
was 5.983 ± 1.201mmol/l. S.Ca++, S.phosphate and S.uric acid were 0.898± 0.165mmol/l, 5.817 ± 1.669mmol/l and 9.689 ± 3.674mmol/l respec-tively. SGPT (351.2 ± 252.2 U/l), SGOT (535.9 ± 408.9 U/l) and S.CPK(12645 ± 18840 U/l) were correlating with each other. 33 (94.28%) pa-tients required dialysis. Mean hemodialysis session per patient was 5.05 ±3.96 and mean duration to open up was 9.71 ± 7.99 days. 6 (17.14%) pa-tients were expired (4 with renal failure and 2 were recovering from ARF),all these patients had septicaemia, DIC and wound infection. There wasno correlation between duration of burried under debris, s.creatinine andduration of recovery.Majority of earthquake victims were young. 97.1% of ARF was due tocrush syndrome. All developed oligo-anuria and majority had haema-turia. 54.29% had fractures and required orthopaedic treatment. 54.29%had compartment syndrome and 31.43% required fasciotomy. Amputationwas done in 8 (22.86%) patients. 82.86% patients recovered and weanedfrom dialysis. 6 (17.14%) patients were expired. This showed that timelyorthopaedic treatment and dialysis support markedly improved the survivalof earthquake victim with crush syndrome.
W358 INFLUENCE OF GENDER ON VARIOUS PARAMETERS INTHE CRUSH SYNDROME VICTIMS OF THECATASTROPHIC MARMARA EARTHQUAKE
Mehmet Sukru Sever1, Raymond Vanholder2, Ekrem Erek3,Norbert Lameire1. 1Nephrology, Istanbul School of Med., Istanbul,Turkey; 2Nephrology, University Hospital, Ghent, Belgium; 3Nephrology,Cerrahpasa School of Med., Istanbul, Turkey
Crush syndrome resulting from earthquakes is a major cause of mortality,while detailed analyses on this patient population is scarce. In this study, weaimed to analyze the influence of gender on various parameters in the renalvictims of the catastrophic Marmara earthquake that struck NorthwesternTurkey, in August 1999.To analyze the extent of nephrological problems, questionnaires were pre-pared within the first week of disaster and sent to 35 reference hospitalsthat treated the victims. Relation between gender and various epidemiolog-ical, clinical and laboratory parameters as well as treatment modalities andoutcome is then investigated.Of the 639 victims, 348 (54%) were males and 291 (46%) females. Overall,mean age was 32±15 yrs., which was 33±14 and 31±15 yrs. in males andfemales, respectively. At admission, male victims were characterized byhigher Hct [(34.3±9.3 vs 32.4±8.7%), (p=0.013)] and higher serum levelsof creatinine [(4.9±3.1 vs. 4.0±2.7 mg/dl), (p<0.001)], BUN [(62.8±36.8vs 57.8±36.8 mg/dl), (p=0.024)], potassium [(5.5±1.3 vs 5.2±1.3 mEq/L),(p=0.014)] and phosphorus [(5.6±2.0% vs 5.2±1.8 mg/dl), (p=0.042)],while other clinical and laboratory parameters as well as the number of fas-ciotomized and amputated extremities did not differ significantly betweenthe two genders. Both the numbers of haemodialysis sessions (8.9±8.7vs. 7.0±8.0) and days for dialysis support (10.6±10.1 vs. 8.3±9.1) werehigher in the male victims (p=0.002 and p=0.003, respectively). Consid-ering the clinical course, males suffered from longer periods of oliguria[(8.5±8.1 vs. 6.7±7.4 days), (p=0.007)], higher rates of sepsis [22.1%(77/348) vs %15.1 (44/291), (p=0.024)] and hypertension [7.5% (26/348)vs 2.1% (6/291), (p=0.002)]. 269 of the 348 male patients (77.3%) neededdialysis support, while this figure was 71.5% (208/291) in the females(p=0.092). Need for mechanical ventilation, hyperbaric oxygen treatment,
blood, fresh frosen plasma and human albumin transfusions did not dif-fer between the genders. Last serum creatinine in nephrology clinics washigher in males [(1.3±1.1 mg/dl) vs. (1.2±1.0 mg/dl), p=0.021)], whilemortality rates were similar in both genders [14.4% (50/348) and 16.2%(47/291), (p=0.53)].Although males more frequently suffer from sepsis and hypertension andneed more intensive dialysis support, gender is not a prognostic indicatorof final outcome in the renal victims of disasters.
W359 NON-TRAUMATIC RHABDOMYOLYSIS AND THE ROLE OFMYOGLOBINEMIA IN ACUTE RENAL FAILURE IN PATIENTSOF SURGICAL PROFILES
Natalia Teplova. Anesthesiology Department, Kirov State MedicalAcademy, Kirov, Kirov Region, Russian Federation
Currently, impairments of skeletal muscles caused by mechanic traumassuch as crash syndrome, syndrome of positional ischemia and syndrome offascial space are well known. Endotoxemia caused by products of myolysismay result in the development of acute renal failure (ARF).Complex evaluation of 117 surgicalprofile patients’ skeletal muscles wascarried put. The patients were in severe conditions. Those were patientswith peritonitis, sepsis, destructive pancreatitis, mediastenitis. Concentra-tion of myoglobin (MG) in blood serum and serum activity of creatinephosphokinase enzyme (CPK). Structural impairments of skeletal muscles(biopsy of the rectut abdominal muscle) were evaluated by means of lightmicroscopy. MG and CPK of blood serum were studied in the early post-operative period (on the 1st, 3nd and 5th days after the operation). Biopsywas performed during laparotomy.The results and findings of the study showed that the patients in criticalconditions had significant increase of myoglobinemia and activity of CPKas well as structural non-specific changes of skeletal muscles (necrosis,dystrophy and inflammation of muscular fibers) that were evidence of my-olysis.The patients in complicated post-operative periods had purulent septiccomplications on the 5th day after surgery. They had secondary increaseof the above parameters in blood serum – the second attack of myogloben-imia and activity of CPK. The registration of this fact allowed us to useMG as one of the criteria of the post-operative course and a predictor ofpurulent septic complications.18 patients developed ARF that was considered as a secondary organ im-pairment that resulted from non-traumatic myolysis. Use of hemodialysisas a pathogenetic treatment method in combination withother therapies didnot result in statistically significant decrease of MG and CPK in bloodserum.A complex of causes resulted in indirect rhabdomyolysis. The most signif-icant causes were endotoxicosis, stress of operative procedures and anes-thesia as well as mediators of inflammation.Indirect rhabdomyolysis is a frequent finding in patients with acute surgicalpathologies in critical cinditions. Indirect rhabomyolysis is involved in thedevelopment of secondary organ impairments (ARF) and adequate therapyis required to eliminate products of myolysis.
W360 RHABDOMYOLYSIS: INCIDENCE, ETIOLOGY, RENALINVOLVEMENT AND TREATMENT OPTIONS IN APROSPECTIVE STUDY
Giacomo Quattrocchio1, Massimo Comune2, Cristiana Rollino1,Roberto Boero1, Giulietta Beltrame1, Michela Ferro1,Francesco Quarello1. 1Nephrology, Ospedale S.G.Bosco, Turin, Italy;2Critical Care Medicine, Ospedale S.G.Bosco, Turin, Italy
Rhabdomyolysis (R) defines an injury of skeletal muscle. Its real incidenceis unknown, it may have various etiologies and it can cause acute renalfailure (ARF). Furthermore, its treatment is not univocal.In our study we performed a prospective analysis of patients (pts) with R,identified among people older than 18 years, who were admitted in ourhospital from February 1st to July 31st, 2002. R was divided into twodegrees of severity: moderate (creatine kinase - CK - levels = 1.000-5.000UI/L) and severe (CK> 5.000 UI/L). We evaluated the etiologic factors,the incidence of ARF (defined as a 50% increase of serum creatinine -Scr)
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

Wednesday, June 11 B9. Acute renal failure, toxic nephropathy 661
and the efficacy and safety of an experimental therapeutic protocol (A) ofprevention of renal dysfunction (consisting in a sodium chloride, sodiumbicarbonate and glucose solution + mannitol 18% + uricase + diuretics)compared to treatment with isotonic saline (B).In the six months period evaluated, we identified 129 R cases over 6.038hospitalized pts (2.1%); 95 pts (1.57% of the whole population) had mod-erate R and 34 (0.56%) had severe R; 43 pts (33% of R pts) were excludedfrom subsequent analysis since they had an acute myocardial infarction.Thirty-one (0.51% of the whole population) over the remaining 86 pts(1.42%) had severe R. The more frequent causes of R were ischemic (57%)and physical (32%) injuries. The incidence of ARF in R pts was 37.2% andit was more frequent in severe than in moderate R (51.6% versus 29.1%,p = 0.065). Mortality between the two groups was statistically different(29% in severe R versus 1.8% in moderate R, p = 0.001). Treatment with A(25 pts) was safe, but not more efficacious compared to B (61 pts). Amongthe 31 pts with severe R, the 16 subjects treated with A, compared to the15 subjects treated with B, had lower peak Scr (1.47 versus 1.91 mg/dl),percent creatinine increase (0.53 versus 0.90%) and mortality (12.5 versus46.7%), even if the differences were not statistically significant.Rhabdomyolysis is a frequent, underrecognized and protean condition. Itmay cause ARF in nearly 35% of pts. Our preliminar data suggest thenecessity of a prospective, interventional, controlled study to define thebest therapeutic option.
W361 ACUTE RENAL FAILURE DUE TO SEVERE CHOLESTASISIN A BODYBUILDER ABUSING THE ANABOLIC STEROIDSTANOZOLOL
Jochen Wilpert1, Marcel Geyer1, Sven Teschner1, Dawit Assefa2,Herrmann Pavenstädt1, Johannes Donauer1. 1Renal Division, InternalMedicine, University Hospital Freiburg, Freiburg, Germany; 2CardiologyDivision, Internal Medicine, University Hospital Freiburg, Freiburg,Germany
A 52 year old, previously healthy bodybuilder presented with malaise,weight loss of 15kg within 2 months, severe jaundice (maximum totalbilirubin 69,6 mg/dl) and intolerable pruritus. Initial workup revealedcholestasis and an acute non-oliguric renal failure requiring immediatehemodialysis (serum creatinine 10,6 mg/dl). He admitted to having usedintramuscular stanozolol, an anabolic steroid, for at least 3 months in orderto accelerate muscle build-up. The patient had discontinued the agent a fewweeks prior to developing symptoms.Transaminases were not elevated and liver synthesis parameters not im-paired. All liver-specific serologies turned out to be negative. Liver biopsywas consistent with drug-induced cholestasis.The acute non-oliguric renal failure was assessed non-invasively, as a renalbiopsy could not be performed due to prolonged bleeding time and the pa-tient’s denial. Clinical history, urine analysis and urine microscopy pointedtowards acute tubular necrosis (ATN) as the underlying pathology (2-4muddy brown casts/low power field, proteinuria 800mg/day, no hematuriaor leucocyturia and a fractional excretion of sodium of 6%). We consid-ered the toxic effects of cholestasis to be causative for this case of ATN,since immunological parameters, serological markers, renal ultrasound andduplex sonography ruled out several other etiologies.Therapy with ursodeoxycholate only moderately reduced cholestasis pa-rameters (serum bilirubin declined from 56,3 to 46,2 mg/dl within fivedays). Therefore extracorporal detoxification with an albumin dialysis(Molecular Adsorbent Recirculating System, MARS, Teraklin, Rostock,Germany) was initiated and rapidly improved cholestatic symptoms andparameters. The patient’s pruritus disappeared within the first MARS
treatment. Three consecutive treatments further reduced the total bilirubinfrom 46,2 to 16,7 mg/dl. The only adverse event observed was a drop ofplatelets from 754/nl to 544/nl.The acute renal failure demanded a series of seven intermittent hemodial-ysis treatments. Parallel with improvement of cholestasis, renal functioncontinuously improved. The patient was discharged after 18 days with aserum creatinine of 1,7 mg/dl and a total serum bilirubin of 12,2 mg/dl. Atfollow-up three months later, serum creatinine was 1,3 mg/dl and bilirubin0,7 mg/dl.We present the rare case of an acute renal failure due to acute tubularnecrosis, presumably caused by stanozolol-induced cholestasis. In this pa-
tient, albumin dialysis accelerated the elimination of endogenous biliarytoxins, significantly reduced pruritus and potentially lead to faster recoveryof renal function.
W362 CLINICAL CHARACTERISTICS OF PATIENTS DEVELOPINGACUTE RENAL FAILURE DUE TO SEPSIS/SIRS: RESULTSOF A PROSPECTIVE STUDY
Itir Yegenaga1, Eric Hoste2, Raymond Vanholder3, Wim Van Biesen3,Dominique Benoit2, Gulcin Kantarci4, Francis Verbeke3, Ann MiekeDhont3, Francis Colardyn2, Norbert Lameire2. 1Nephrology,InternalMedicine, Kocaeli University,Medical School, Izmit, Derince, Turkey;2Intensive Care, University Hospital, Gent, Belgium; 3InternalMedicine,Nephrology Division, University Hospital, Gent, Belgium;4Nephrology, Marmara University, Istanbul, Turkey
The aim of this study is to define the clinical and biochemical character-istics of sepsis/SIRS patients admitted to the ICU, in order to recognise,from the first day of sepsis on, those prone to develop ARF subsequently.During a one year period 257 sepsis/SIRS patients admitted to the med-ical and surgical ICU who met the American College of Chest Physi-cians/Society of Critical Care Medicine (ACCP/SCCM) Consensus Con-ference Criteria were included and followed prospectively regarding clini-cal, biochemical and therapeutic status. The patients who developed ARFduring this follow-up were noted, and their clinical and laboratory datawere compared to the rest of the population. In addition APACHEII, SOFA,SHARF, Liano scoring systems were calculated for two groups of patients,to define predictive factors pointing to the development of ARF.Out of 257 sepsis/SIRS patients, 29 (11%) developed ARF. Upon admis-sion, statistically significant differences between the ARF and the non-ARFgroups were age, Central Venous Pressure, serum creatinine, urea, biliru-bin, which were higher (p=0.003, 0.006, <0.001, <0.001, =0.013 respec-tively), and lowest mean arterial and diastolic blood pressure, 24 hr urinaryoutput, creatinine clearance, serum arterial pH, serum bicarbonate, andalbumin which were lower (p=0.038, 0.003, 0.006, 0.006,<0.001, 0.009,0.050 respectively). Severity scoring systems were not different betweenthe two groups.Based on our study it was possible to define the patients who most probablywill develop ARF as belonging to a higher age category, showing a rise inurea and creatinine level and low serum albumin, as well as acidosis uponadmission, having hypotension form the earliest phase on, and sufferingfrom previous hepatic failure.
W363 A PROSPECTIVE ANALYSIS OF HEMOSTASIS INSYSTEMIC INFLAMMATORY RESPONSE SYNDROME(SIRS) WITH ACUTE RENAL FAILURE
Jolanta Malyszko1, Slawomir Czaban2, Jacek Malyszko1,Jacek Krajewski2, Andrzej Siemiatkowski2, Michal Mysliwiec1.1Nephrology and Internal Medicine, Medical University, Bialystok,Podlaskie, Poland; 2Intensive Care Unit, Medical University, Bialystok,Podlaskie, Poland
Endothelial cell damage plays a central role in the development of systemicinflammatory response syndrome –SIRS due to the imbalance betweencoagulation and fibrinolysis. Acute renal failure often complicates SIRS.Hemostatic disturbances were described in patients with acute renal failurerequiring renal replacement therapy in a form of hemodialyses. However,at present only very limited data exist in patients with SIRS and acute renalfailure, particularly on conservative treatment. The aim of the study wasto assess prospectively the endothelial cell damage and hemostatic dis-turbances in SIRS and acute renal failure not requiring renal replacementtherapy. We studied 58 patients (mean age 59 years,) at the time of SIRSdiagnosis, on the 3rd and 5th day. We assessed markers of endothelial cell in-jury: von Willebrand factor (vWF), thrombomodulin, markers of ongoingcoagulation: prothrombin fragments 1+2 (F1 +2), thrombin-antihrombincomplexes (TAT), a marker of ongoing fibrinolysis: plasmin-antiplasmincomplexes (PAP), moieties of extrinsic coagulation pathway: tissue factor(TF), tissue factor pathway inhibitor (TFPI), TFPI/Xa complexes, TF/VIIacomplexes, and Thrombin Activatable Fibrinolysis Inhibitor-TAFI usingcommercially available kits. Factors related to endothelial damage did not
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

662 B9. Acute renal failure, toxic nephropathy Wednesday, June 11
change during the study as well as TAFI activity, TFPI activity and PAP.TAFI concentration, TF/VIIa and TFPI/Xa complexes decreased signifi-cantly on the 3rd day of SIRS evolution. Markers of hypercoagulabilityincreased significantly on the 3rd day, the decreased significantly on the 5th
day, reaching values lower that at the time of SIRS diagnosis. APACHE 2and SSS scores decreased significantly on the 5th day. Prothrombin time,activated partial thromboplastin time, INR did not change during the study.Fibrinogen increased significantly on 5th day of SIRS evolution. Our datashows that patients with SIRS and associated renal failure exhibit signs ofendothelial cell damage and hypercoagulability, mostly on the 3rd of SIRSevolution, followed by dampening of hypercoagulation.
W364 ACUTE RENAL FAILURE IN PATIENTS WITH FALCIPARUMMALARIA: AN AUDIT FROM A TERTIARY CARE HOSPITALIN THE TROPICS
Urmila Anandh. Nephrology, St.John’s Medical College Hospital,Bangalore, Karnataka, India
This study was undertaken to find out the incidence of acute renal failure inpatients with plasmodium falciparum infection and the prognostic factorsdetermining outcome.A prospective study which enrolled 133 patients between June 2001 to June2002 in our centre. The demographics, clinical presentation, biochemicalparameters, requirement for dialysis and outcome was studied.The mean age (SD) of the patients was 38.4 (15.7) years, and there were95 males and 38 females. 62 (46.6%) patients presented with jaundice,48 (36%) had oliguria and 64 (48%) had renal failure. The biochemicalinvestigations at presentation was mean (SD) serum creatinine (mg/dl)2.26 (2.4), bilirubin (mg/dl) 9.5 (11.71), conjugated bilirubin 5.6 (7.2) andhemoglobin (g/dl) 8.5 ± 2.8. 87 patients (65.4%) had thrombocytopenia.52 patients (39.0%) had some evidence of protein in their urine. A largenumber of patients (56/133) had parasite load >1%. 24 patients (18%)needed dialysis and there were 27 death (20%).The factors commonly associated with development of renal failure werepresence of jaundice (p<0.0001), anemia (p<0.0001), high parasitic load(P <0.0001), thrombocytopenia (P<0.0001), and chloroquine resistance(P<0.0001).A multiple regression analysis for prognostic factors predicting mortalityshowed significant association with a high parasitic load (>1%) (P<0.03)and presence of hypotension (P=0.04).A significant number of patients with falciparum malaria develop renalfailure which is associated with hematological abnormalities and evidenceof other organ dysfunction. The severity of infection as manifested by ahigh parasitic load is a major prognostic factor for mortality. Acute renalfailure in falciparum malaria occurs most commonly in patients who areresistant to chloroquine making it a serious health problem in the tropics.
W365 A PROSPECTIVE STUDY OF PROGNOSTIC FACTORS INFALCIPARUM MALARIA WITH MULTI ORGANDYSFUNCTION SYNDROME MANAGED IN INTENSIVECARE UNIT
Tarun Kumar Saha, Manoj Rai, Gopal Kanwar, Pawan Agarwal,Kanta Chatterjee. Nephrology, Apollo Hospitals, Bilaspur, Chattisgarh,India
Multiorgan dysfunction syndrome (MODS) including acute renal failure isa frequent complication of falciparum malaria. This prospective study wasdone over a 14-month period to evaluate the pattern of organ involvement,prognostic factors and the effect of treatment in intensive care unit (ICU)on the outcome of patients with MODS due to falciparum malaria. Patientswho showed ring forms of P. falciparum on examination of peripheralblood smear and developed MODS were included in the study. MODS wasdefined according to criteria laid down by the American College of ChestPhysicians and Society of Critical Care Medicine 1992 Consensus Confer-ence. All patients were admitted in the ICU and treated with quinine or arte-sunate. The clinical and laboratory parameters and outcomes were noted. Atotal of 52 patients presented with MODS due to falciparum malaria in thestudy period. The involved organs included liver (86.5%, bilirubin 15.74 ±13.95 mg/dl) followed by brain(82.7%), hematological (76.9%,Hb 6.62 ±
1.27 gm/dl, platelet 18,000 ± 9000/cumm), kidneys (75%, creatinine 7.14± 3.69 mg/dl), cardiac(21.15%) and respiratory (15.30%).Dialysis was required in 23 patients, six of whom died. Renal functionalrecovery took 14.03±-12.32 days in the surviving patients. A total of 8patients died.The mortality was directly correlated with the number of organs involved.No patient with involvement of 3 or less organs (n=25) died, whereas 5.26%of those showing involvement of four organs (n=19) and 87.57% of thosewith involvement of five or more organs (n=8) died. Other factors thatpredicted a high mortality were ARDS (85.71%), hypotension (72.72%)and a total leukocyte count > 20,000 cumm (50%). Acute renal failure(ARF) was not associated with increased mortality, but the severity of renalfailure correlated positively with the severity of jaundice and anaemia. Theparasite index correlated positively with the severity of ARF, anaemia,thrombocytopenia and jaundice.The average parasite count was significantly higher in patients who died ascompared those who survived (103.75±70.29 vs 34.06±46.73).In conclusion, good survival can be obtained with appropriate managementin MODS due to falciparum malaria. Dysfunction of five or more organsis associated with high mortality. ARF alone does not increase mortality inthese patients.
W366 RENAL INVOLVEMENT IN DENGUE FEVER - A STUDYFROM SOUTH TAMILNADU
Balasubramaniam Jeyaraj, Palaniappan Nainar. Nephrology, Kidney CareCentre, Tirunelveli, Tamilnadu, India
Dengue fever, a Flavi virus infection affecting large populations in devel-oping countries has not been well documented and studied in this area untilrecently. During the year 2002 there was an epidemic of dengue fever inTirunelveli/Tuticorin districts of south Tamilnadu.The clinical presentation of these cases were recorded with special refer-ence to renal involvement. There were 117 cases. Children -86 and adults31. Common features were Fever, thrombocytopenia, leucopenia, poly-serositis, shock.In children, inspite of severity of the disease including shock, renal in-vlevement was not prominant. Out of 86 cases only 6 cases developedrenal failure. The renal failure was not severe (mean creat 2.2) and it wasnot the cause for the mortality. 15 out of 86 did have mild prerenal azotemianot progressing to renal failure.In adults, there was a femle predominance and 11 out of 31 developed renalfailure. 6 out of this 11 developed renal failure inspite of absence of grossshock. 2 of them had severe renal failure requiring dialysis. 2 patients withsevere renal failure underwent renal biopsy. One showed features of HUSand patchy cortical necrosis and the other showed mesangial proliferativeglomerulonephritis. 6 out of the 11 cases had significant proteinuria.Renal failure in the absence of shock and presence of proteinuria indicate amechaism other than simple ischemic tubular injury, is intriguing and needsfurther look.This phenomenon is also restricted to the adult population.
Free Communication June 10
W367 THE CLINICAL PROFILE AND PREDICTORS OFMORTALITY OF WEIL’S SYNDROME SEEN AT AREFERRAL CENTRE IN KERALA
Ranjit Narayanan, Jyotish C. Gopinathan, Rajaratnam Krishnan,Ramdas Pisharody. Department of Nephrology, Calicut Medical College,Kozhikode, Kerala, India
Leptospirosis is the most common zoonoses worldwide that is assumingalarming proportions in the coastal parts of South India. Weil’s syndromebeing most common cause of ARF requiring dialytic support at our insti-tution, we decided to study the clinical profile and predictors of mortalityof leptospirosis with hepatorenal involvement seen during the year 2001.All cases of febrile illness with hepatorenal involvement presumed to bedue to leptospirosis admitted between January-December 2001 were in-cluded in this study. Clinical features, lab workup, serology and outcomewere studied. Enteric fever, malaria and Hepatitis B were ruled out in allcases.There were 232 cases during the period of study. Majority was male (M:
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

Wednesday, June 11 B9. Acute renal failure, toxic nephropathy 663
F 3:1). There was a definite rise in number of cases during the monsoonmonths with maximum cases seen during August-September. The com-mon presenting symptoms were fever (97%) with myalgia (72%), red eye(73%), jaundice, vomiting (35%) and oliguria (54%). The common clinicalfindings included icterus (92%), conjunctival congestion (71%), calf ten-derness (68%), tender hepatomegaly (56%) and dehydration (56%). Lesscommonly, subconjunctival haemorrhage (15%), hypotension (25%) andaltered mentation (10%) were observed. Meningism was distinctly un-common. The common lab findings included leucocytosis with high ESR,thrombocytopenia, mild pyuria or bland urinary sediment apart from de-ranged liver and renal function. Transaminases showed only mild to modestelevation. Serological testing (IgM Elisa) was done in 131 cases. Positiveserology was obtained in 94 cases while 37 were negative. Most cases ofoliguria were correctable with adequate hydration alone. Dialytic supportwas given in 71 cases. 59 cases underwent peritoneal dialysis (P.D.) whilehaemodialysis (H.D.) was done in 26 cases. 14 cases needing prolongeddialytic support had to be shifted from P.D. to H.D.. There were 52 deathsincluding 30 who received dialytic support.On statistical analysis, myocarditis, bleeding diathesis, degree of thrombo-cytopenia and respiratory distress significantly correlated with mortality.However there was no significant difference in clinical features or lab pa-rameters between IgM positive and negative cases.To summarize, cases of leptospirosis showed a definite peaking during themonsoon months. The most common picture was of an oliguric dehydratedicteric patient with fever, myalgia and conjunctival suffusion who recoverswith volume repletion and supportive measures. Meningism, a prominentfeature of the WHO scoring system for leptospirosis, is uncommon in oursetting. Positive serology for leptospirosis did not reflect severity. Severethrombocytopenia, bleeding manifestations and hypotension due to my-ocarditis carry poor prognosis.
Free Communication June 10
W368 BOVINE AORTIC ENDOTHELIAL CELLS ARESUSCEPTIBLE TO HANTAVIRUS INFECTION: A NEWPERSPECTIVE IN ECOLOGY OF VIRUS HOSTINTERACTION
Martin Zeier1, Walter Muranyi2, Roland Kehm2, Udo Bahr2,Muller Sandra2, Handermann Michaela2, Darai Gholamreza2.1Medicine/Nephrology, University of Heidelberg, Heidelberg, Germany;2Virology, University of Heidelberg, Heidelberg, Germany
Hantaviruses are enveloped RNA viruses that belong to the family Bun-yaviridae. They possess a three segmented, single stranded negative sensedRNA-genome that encodes for the different hantaviral proteins. Theseviruses are the causative agents of hemoragic fever with renal syndrome(HFRS) and hantavirus pulmonary syndrome (HPS). The mortality rate ofHFRS is ranging from 0.1-10%, whereas the mortality of HPS is about50%. Hantaviruses have a worldwide distribution with specific host (ro-dents) as transmission vector. It is known that rodents transmit the virus tohumans. However, antibodies against hantavirus serotype were also foundin domestic animals. Danes and co-worker documented a prevalence of2% of high IgG titers of hantavirus antibodies in cattles (Danes L. et al.,Rep. Cesk. Epidemiol Mikrobiol. Immunol. 41, 15-18, 1992). In order toclarify the possibility of non-rodent hantavirus infection, the susceptibilityof bovine endothelial cells (BAEC) to a Puumala virus serotype (CG18-20) infection was investigated. The hantaviral nucleocapsid protein wasdetected sixty days post infection in 95% of infected BAEC by immunoflu-orescence assay. The expression of Puumalavirus nucleocapsid protein ininfected cells was confirmed by western blot analysis and by immunopre-cipitation. The presence of all three genomic viral RNAs (L, M, and S)were identified in infected BAEC cultures and in cell free culture mediumby RT-PCR. The identity of the amplified cDNAs of the individual vi-ral RNA-segments were verified by cDNA nucleotide sequence analysis,showing a 99-100% homology to the input virus. BAEC- infected cellsrevealed no major cytopathic effects as assayed by immunofluorescencestaining of the cytoskeleton (actin and microtubules). Additionally, the vi-ral receptor α3Vβ integrin was downregulated.In the present study we documented for the first time that a non-rodentendothelial cell culture of bovine origin (BAEC) can be efficiently infectedwith hantavirus serotype Puumala. This finding is of particular importance,
since it focuses attention on viral host interaction, host barrier, viral reser-voir, virus transmission, and ecology of hantavirus infection.
W369 ACUTE RENAL FAILURE DUE TO BEE STINGS
Enrique Klahr1, John Serna2. 1Centro de Terapia Renal de Medellin, RTS,Medellin, Antioquia, Colombia; 2Nefrosalud, RTS, Armenia, Quindio,Colombia
Acute Renal Failure due to Bee Stings is a relatively frequent event in somerural areas of Colombia, mainly in the Coffee Zone.A longitudinal prospective study was developed for an 8-year period, be-ginning on January 1992 until January 2000. The patients we studied hadsuffered multiple stings by Africanized Bees and they were submitted totwo renal clinics from Colombia. We found out 35 patients fulfilled the in-clusion criteria which is multiple stings by Africanized Bees. Of those 35,fourteen patients developed Acute Renal Failure. This means the creatininevalue was above 1,5 mg/dl at beginning or during its first evolution.All the accidents occurred in rural area and the patients were coffee horti-culturists. Eleven were men and three were women with ages between fourand 86 years old, for an average of 58,3 years. They received an initial med-ical treatment in the local hospitals. After an average time of 24 hours, allthe patients were sent to the renal clinics and evaluated by a nephrologist.They presented more than a hundred bee stings.The patients responded to the medical treatment, which consisted in IVfluid with normal saline solution 0,9% bicarbonate and diuretic (furosemidetype). From the fourteen patients with Acute Renal Failure, four requiredhemo-dialysis for their treatment. One of the patients died. The creatininevalues were between 1,5 mg/dl and 15 mg/dl as maximum level. The urinechemistry revealed mioglubinury, proteinury of less than one gram in 24hours, hematury, cilindrury and leukocitury in all the cases in which thesample was possible to obtain. The average CPK value was 13557,8, andthe levels were between 31600 for the highest case, and 937 for the lowest.There is no data for two patients, one of those, the patient who died.
PATIENTS DATA LAB
DATA/PATIENTS 1 2 3 4 5 6 7
AGE 4 78 40 77 60 40 72SEX F M M M M M MCPK 31600 NA 16000 10570 5600 3000 28457
PATIENTS DATA LAB (2)
DATA/PATIENTS 8 9 10 11 12 13 14
AGE 37 60 65 50 71 77 86SEX M F M M M M MCPK NA 937 18800 9470 21510 10570 23100
Therefore, the experience acquired in the cases of this study has allowedthe professional staff of the hospitals where the initial attention is provided,to be prepared for this sort of accidents. Now they are able to give a quickand efficient first handle treatment to the patients with multiple bee stings.Also, they are now warned about the need of remission within the nextsix hours after the stings, in order to avoid the possible evolution of AcuteRenal Failure.
W370 HIGH AND LOW OSMOLALITY, AND NONIONICRADIOCONTRASTS INHIBIT NITRIC OXIDE IN CULTUREDRENAL ARTERY SMOOTH MUSCLE CELLS
Luciane Ribeiro1, Fábio de Assunção e Silva1, Giovana S. Di Marco1,Nestor Schor1, Elisa Mieko Suemitsu Higa1,2. 1Nephrology Division,UNIFESP-Escola Paulista de Medicina, São Paulo, SP, Brazil;2Emergency Division, UNIFESP-Escola Paulista de Medicina, São Paulo,SP, Brazil
The aim of the present study was to evaluate the NO production in ratrenal artery smooth muscle cells (rVSMC) primary culture, exposed toradiocontrast (RC).The cells were treated during 72 hr with mannitol, an osmotic control,at 10% (MT10; 600 mOsm/kg H2O) or 35% (MT35; 2,100 mOsm/kgH2O). They were also treated with the RC (4.6x10-4M): iobitridol (IBT)
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

664 B9. Acute renal failure, toxic nephropathy Wednesday, June 11
nonionic of low osmolality; ioxaglate (IXG) ionic of low osmolality, andioxitalamate (IXT) ionic of high osmolality, and with lipopolysaccharide(LPS 100 µg/ml) as a positive control. We evaluated the cell viability (%)and in the cell culture media, the NO (nmol/mg protein) and the osmolality(mOsm/kg H2O).As shown in the tables, by the Griess method, the NO synthesis was notdifferent in MT10, it was increased in the LPS and decreased in all the RCgroups as compared to CTL.The NO was also decreased in the RC+LPSwhen compared to LPS. By chemiluminescence (NOAnalyzer) the resultswere similar as compared to the Griess method, but due to its greatersensitivity the values were higher. MT35 group presented a reduced NOsynthesis when compared to the CTL. The MT35, IXT and IXT+LPS pre-sented a significant decrease of the cellular viability, compared to the othergroups. The osmolality of the culture media was significantly increasedonly in the groups MT35 (382±4.3) and IXT (378±5.1) when comparedto the CTL (314±5.5).
Table 1
CTL MT10 MT35 IXT IXG IBT
Griess 14.6±0.7 14.3±0.7 - 4.2±0.5* 10.9±1.2*• 12.9±0.6*•†
NOAnalyzer 61.1±2.0 61.4±1.7 53.9±0.9* 26.7±1.4* 42.9±1.1*• 53.5±1.8*•†
Cell viability 96.4±0.6 96.2±0.4 81.4±1.2δ 81.2±0.6δ 95.8±0.6 95.9±0.6
n=10, all groups. For Griess and NOAnalyzer: One-Way ANOVA - Newman - Keulstest. p<0.05: * vs CTL; • vs IXT; † vs IXG. For cell viability: Kruskal-Wallis - Newman- Keuls test. p<0.05: ‡ vs CTL.
Table 2
CTL LPS IXT+LPS IXG+LPS IBT+LPS
Griess 14.6±0.7 455.2±2.3* 260.2±2.7*φ 423.6±2.2*φβ 433.7±1.4*φβω
NOAnalyzer 61.1±2.0 2758.2±2.5* 1877.4±2.5*φ 2260.4±1.3*φβ 2448.9±1.3*φβω
Cell viability 96.4±0.6 96.2±0.3 80.9±0.5δ 95.7±0.6 95.9±0.3
n=10, all groups. For Griess and NO Analyzer: One-Way ANOVA - Newman - Keulstest. p<0.05: * vs CTL; φ vs LPS; β vs IXT+LPS; ω vs IXG+LPS. For cell viability:Kruskal-Wallis - Newman - Keuls test. p<0.05: δ vs CTL.
Our data show that the RC significantly reduced NO synthesis in rVSMC,which was more pronounced after IXT treatment. This decrease in NOcaused by IXT (57.3%) was not directly related to the reduced cell viabilitycaused by them (15.8%), neither to its high osmolality, since in the groupMT35 which osmolality was similar to IXT, NO decreased only 11.0%when compared to CTL. Besides, in the groups IXG and IBT we did notobserve any change in the cell culture media osmolality, neither in the cellviability, but there was a decreased NO synthesis.The decreased NO caused by the RC could explain the vasoconstrictionand therefore, the acute renal failure related to them.
W371 CONTRAST ASSOCIATED NEPHRO TOXICITY
Shaista Hussaini, Somasekhar , Krishnan . Nephrology, Apollo Hospital,Hyderabad, Andhra Pradesh, India
To study the effect of high vs low osmolar contrast on the incidence of con-trast associated nephrotoxicity (CAN) in high risk patients. 120 patients,101 male and 19 female in the age group of 15 – 73 years who under-went coronary angiography between June – July 2000 were randomisedto receive sodium meglumine diatrizoate(group A) or Iohexol (Group B)in a dose of 50 – 200 ml. i.v. Study group included diabetics, elderly pa-tients hypertensive patients with LV dysfunction. Underlining renal insuffi-ciency children less than 15 years age haemodynamically unstable patientsand those with baseline s.creatinine more than 3.5 mg% were excluded.S.Creatinine was estimated pre and 24 hours post procedure. CAN wasdefined as a 25% increase in s.creatinine, 24 hours post procedure.There were 32 patients (27%) in group A and 88 (73%) in group B. The sexand baseline renal functions were comparable. Overall incidence of CANwas 20%, 22% in group A, 19% in group B. None of the patients requireddialytic support and recovered with conservative treatment. There were nodeaths.Overall risk of CAN was 20%. There was no difference between thosereceiving high osmolar and low osmolar contrast. None of the patients re-quired dialysis. Identifying high risk group, proper hydration using optimaldose of contrast and regular monitoring of renal functions could minimiseor prevent CAN.
W372 ROLE OF N-ACETYL CYSTEINE IN PREVENTION OFCONTRAST NEPHROPATHY IN PATIENTS OF DIABETICRENAL FAILURE: A PROSPECTIVE STUDY
Deepak Shankar Ray1, V. Srinivas2. 1Department of Nephrology, SevenHills Hospital, Visakhapatnam, Andhra Pradesh, India; 2Department ofNephrology, Care Hospital, Visakhapatnam, Andhra Pradesh, India
Contrast nephropathy is an important cause of acute renal failure in hos-pitalised patients. It is more so in the presence of background diabeticrenal failure. Recently certain studies have shown beneficial effects of N-acetylcysteine in prevention of contrast nephropathy in patients with renalimpairment.Since patients of diabetes mellitus with chronic renal failureare more likely to develop contrast induced acute renal failure. We studiedthe role of N-acetylcysteine in prevention of contrast nephropathy in thisgroup of patients.Twentytwo patients of diabetes mellitus with stable chronic renal failure(Serum Creatinine more than 1.5 mg%), requiring coronary or, periph-eral angiography and or, angioplasty were taken in to study. They wererandomised to two groups i.e. Group-A and Group-B. There were no dif-ference in the clinical settings amongst both the groups. Patients of both thegroups received hydration according to the clinical condition for 24 hoursbefore and after the procedure. In addition patients of Group-A receivedoral N-acetylcysteine at a dose of 600 mg. twice a day for 2 days starting 24hours prior to procedure. All the patients received low osmolality contrstagents. The amount of contrast agent kept to the minimum possible.Out of 22 patients 9 patients (4 in Group-A and 5 in Group-B) had detori-aration of renal function in 48 to 72 hours after use of contrast. All exceptone patient improved by 7days time. One patient of Group-B who had re-covered from cotrast nephropathy a week earlier and had a serum creatinineof 4.1mg% detoriarated significantly after coronary angioplasty requiringdialysis.In our small study we did not find any beneficial effect of N-acetylcysteinein preventing contrast nephropathy in patients of diabetes mellitus withrenal failure requiring angioplasty or, angiography.
W373 THE INFLUENCE OF GADOPENTETATE DIMEGLUMINE ONTHE RENAL FUNCTION IN PATIENTS WITH NORMAL ANDREDUCED RENAL FUNCTION
Ute Hoffmann1, Alexandra Reil1, Johann Link2, Michael Fischereder1,Bernhard K. Krämer1. 1Klinik und Poliklinik f. Innere Medizin II,University of Regensburg, Regensburg, Germany; 2Institut fürRöntgendiagnostik, University of Regensburg, Regensburg, Germany
Radiocontrast-induced nephropathy (RCIN) is a critical consideration dur-ing the performance of diagnostic and interventional radiological proce-dures in patients with renal impairment. Gadolinium-based contrast agentshave a record of causing minimal toxicity in their standard use in MRimaging (MRI). This study was performed to evaluate the influence ofgadopentetate dimeglumine injection on the renal function.Data from 181 patients with and 198 patients without pre-existing reducedrenal function undergoing magnetic resonance imaging were retrospec-tively analyzed. Serum creatinine, urea and albumin levels just before and1-8 days after the administration of gadolinium were checked and age,height, body mass, sex, preexisting illnesses such as nephropathies, arte-rial hypertension, diabetes and heart failure were monitored. Furthermore,the intake of drugs as ACE inhibitors and angiotensin-II-antagonists, cal-cium channel antagonists, diuretics and NSAIDs were assessed. GFR wasestimated by the Cockroft-Gault formula.In the 181 patients with normal serum creatinine level, there is a slight butstatistically not significant increase of mean serum creatinine [± SD] (0,72mg/dl [± 0,18] before and 0,73 mg/dl [± 0,22] after the administration ofgadolinium. In patients with pre-existing renal impairment, there is a sig-nificant decrease of serum creatinine after the administration of gadolinium(1,82 mg/dl [± 1,03] before and 1,72 mg/dl [± 1,03] after (p<0,01). Thechange of GFR in patients with normal renal function was not significantwhile in patients with reduced renal function, there is a highly significantincrease of GFR (52,60 ml/min. [± 24,53 ml/min.] before and 58,23 [±30,44 ml/min.] after the administration of gadolinium) (p<0,001).The high diagnostic value of gadolinium contrast media is associated witha very minor risk of adverse reactions in comparison to iodinated contrast
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

Wednesday, June 11 B9. Acute renal failure, toxic nephropathy 665
agents. In addition, the administration of gadolinium even leads to a de-crease of serum creatinine in patients with pre-existing renal impairment. Inconclusion, the use of gadolinium-based contrast media is a safe alternativein patients for whom iodine-based contrast agents are contraindicated.
W374 ACETYLCYSTEINE INDUCES A SIGNIFICANT INCREASE INGFR IN PATIENTS WITH NORMAL RENAL FUNCTION
Ute Hoffmann1, Bernd Krüger1, Wolfgang Drobnik2,Michael Fischereder1, Bernhard K. Krämer1. 1Klinik und Poliklinik f.Innere Medizin II, University of Regensburg, Regensburg, Germany;2Institut fur Klinische Chemie, University of Regensburg, Regensburg,Germany
Prevention of contrast nephropathy is of crucial importance in a numberof diagnostic studies using radio contrast media. Recently, acetylcysteinehas been reported to decrease serum creatinine in this setting. Although nostudies exist which demonstrate decreased incidence of dialysis therapy,ACC administration prior to radiocontrast media has been widely recom-mended. The objective of this study was to investigate the potential effectsof acetylcysteine on serum creatinine, serum urea and glomerular filtrationrate (GFR) in patients with normal renal function.We prospectively enrolled 50 healthy volunteers who had a baseline creati-nine of (mean [±SD]) 0,85 [±0,14] mg/dl. Acetylcysteine was given orallyat a dose of 600 mg daily for a total of 2 days. Serum creatinine, serumurea and albumin were checked immediately before the administration ofacetylcysteine (day 0), and 4 hours (day 1) and 48 hours (day 3) after thelast intake. GFR was estimated (eGFR) on the basis of serum creatinine,urea and albumin concentration and weight, age and sex as reported byLevey.The mean serum creatinine and urea concentrations decreased significantlyfrom 0,85 [± 0,14] mg/dl and 29,79. [± 7,47] mg/dl to 0,82 [± 0,13]mg/dl and 27,49 [± 5,92] mg/dl respectively (p=0,04 and p=0,004) 4 hoursafter the last intake of acetylcysteine. There was a significant increaseof estimated GFR (from 102,23 [±19,43] ml/min. to 105,75 [±19,88]ml/min. on day 1 (p=0,01). The changes of serum creatinine, urea andeGFR between day 0 and day 3 and between day 1 and day 3 were notsignificant.In several studies, a protective effect of acetylcysteine on renal functionafter radiocontrast media administration has been postulated. This is thefirst study that shows a positive effect of acetylcysteine on creatinine andGFR, surrogate markers of renal injury. Before renal protective effects ofACC in contrast nephropathy are considered, the direct effects of ACC oncreatinine, urea and estimated GFR have to be adressed.
W375 PREECLAMPSIA AND ACUTE RENAL FAILURE IN WOMENDURING PREGNANCY (NORTH OF IRAN)
Seddigheh Esmaelzadeh, Hadi Sorkhi, Nastaran Jalai. Nephrology,Amirkola Hospital, Babol, Mazandaran, Iran
Preeclampsia is a serious problem in pregnancy, both for mother and herneonate. Acute renal failure is one of its major problems and usuallyrequires the termination of pregnancy and premature labor. This studywas done to determine risk factors and outcome for women with severepreeclampsia and renal failure.This retrospective study was done from 1999 to 2001 in all pregnant womenwith hypertension and prteinuria who were admitted in the obstetric ward.Blood pressure grater than 160/110 mmHg was defined severe preeclamp-sia and less than 160/90mmHg was defined mild preeclampsia, too. Acuterenal failure was defined if serum creatinin was equal or grater than 1.1mg/dl.In the 125 women with preeclampsia, 75(60%) were primparous and50(40%) were multiparous. Mean age at admition was 26 years old (17-40) and mean gestation age was 35 week (28-41). 37.6% of patients hadpreterm labor.7.2% of women had acute renal failure and only one casewas treated with dialysis (hemdialysis). They’re no maternal death or per-manent complication.In order of this study, preeclampsia is higher in first pregnancy and in lowerage. Fortunately, acute renal failure was low, only one patient was treatedby dialysis, and without any permanent complications.
W376 ACUTE RENAL FAILURE IN PREGNANCY: TWENTY YEARSJOURNEY
Jai Prakash, Hemant Kumar, Bibekananda Kar, Anil Kumar Singh,Dhananjay Kumar Sinha, Laxmikant Pandey, Prashant G. Kedalaya,Shivendra Singh, Usha . Department of Nephrology, Institute of MedicalSciences,Banaras Hindu University, Varanasi, Uttar Pradesh, India
Acute renal failure (ARF) has become a rare (one in 20,000 pregnancies)complication of pregnancy in developed countries. The present study de-scribes the changing trends of pregnancy related ARF between period ofJuly 1982 to December 2002 in Eastern India. acute renal failure due toobstetrical causes were observed in 11.6%(190/1627) of total ARF cases.The patients were divided into two groups based on the period of study:Group A 65 (1982-1991) and group B 125(1992-2002) patients. Obstet-rical complications were causative factors for ARF in 15% (65/426) and10% (125/1201) of patients in the two periods respectively. ARF was ofischemic origin and caused by multiple factors either alone or in combi-nations. Obstetrical ARF declined from 15% in 1982-1991 to 10% duringthe period of 1992-2002. ARF following septic abortion showed a declin-ing trend, 9% in 1980s to 7% in 2000s of the total number of ARF cases.Puerperal sepsis contributed to 0.8% of the total ARF in recent years com-pared to 2.4% in the earlier period. Preeclampsia-eclampsia was the causeof obstetrical ARF in 23% and 14.4% of patients in group A and group Brespectively. The percentage of total ARF due to eclampsia declined from3.5% during the period from 1982-1991 to 1.4% in 1992-2002. The inci-dence of cortical necrosis decreased significantly (P<0.001) from 17% in1982-1991 to 2.4% in 2000s. The maternal mortality reduced to 6.4% in1992-2002 from initial high mortality of 20% in the period of 1982-1991.In summary, ARF due to obstetrical complications which remained high inthe initial period has decreased in recent years. This is associated with adeclining trend in post-abortal ARF and a reduction in maternal mortality.We also observed a significant fall (p<0.001) in the incidence of corticalnecrosis related to ARF in pregnancy. These changing trends in obstetricalARF were mainly due to a decrease in the number of septic abortions,puerperal sepsis and legalization of abortion.
Free Communication June 9
W377 ACUTE LIVER DISEASE AND DIALYSIS DEPENDENTRENAL FAILURE (ARF) FOLLOWING INGESTION OF RAWFISH GALL BLADDER
Saubhik Sural, Chandra Sekhar Panja, Ajay Kumar Sarkar. Nephrology,Peerless Hospital and B.K.Roy Research Centre, Calcutta, West Bengal,India
There are very few studies reporting the nephrotoxic and hepatotoxic ef-fects of raw fish bile. The largest series from Korea comprised of 13 patientsand in only 3 of them ARF was induced by bile from common carp. Someof these patients did not require dialysis. Recently over a short period of6 months 7 patients came to our centre with dialysis dependent ARF afteringestion of raw gall bladder from common carp and this needs reporting.Five patients were young diabetic(age 30,36,28,32 and 35 years)and theywere advised by a quack to ingest raw fish gall bladder to cure diabetes.Twopatients (age 45 and 40 years) ate to improve their health.All patients(6male & 1 female)presented initially with recurrent vomitingafter eating. Oliguria and jaundice in all and microhematuria in 5 followedthis. Mean serum creatinine at the time of admission was 11.3 mg%. Meanserum bilirubin was 2.9 mg% and mean serum SGPT was 286 IU. Six pa-tients recovered with conservative therapy and hemodialysis. Renal func-tion and liver function became normal at the end of 2 weeks. One patientdeveloped acute respiratory distress syndrome. He remained ventilator &dialysis dependent for 1 month and then died.Ingestion of raw fish gall bladder can lead to severe ARF and patient maydie of multi-organ failure. General practitioners and social workers mustbe alerted to prevent further spread of this false belief
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

666 B9. Acute renal failure, toxic nephropathy Wednesday, June 11
W378 RENAL DYSFUNCTION EARLY IN THE COURSE OFHEMATOPOIETIC CELL TRANSPLANTATION
Yasar Caliskan, Sevgi Kalayoglu-Besisik, Gursel Acarturk, Deniz Sargin,Tevfik Ecder. Department of Internal Medicine, Istanbul School ofMedicine, Istanbul, Turkey
Renal dysfunction is a common complication during the early period ofhematopoietic cell transplantation (HCT), especially in the setting of al-logeneic HCT. The main causes of renal dysfunction after HCT are drugtoxicity, sepsis and concurrent liver disease. In the present study, renalcomplications were prospectively evaluated in patients undergoing HCTfor various hematologic diseases.Twenty-nine patients receiving HCT (18 patients allogeneic, 11 patientsautologous) in our Bone Marrow Transplantation Unit were included in thestudy. All of the allogeneic HCT patients received the same conditioningregimen, graft-versus-host-disease (GVHD) prophylaxis and antimicrobialprophylaxis. The autologous HCT patients did not receive any antimi-crobial prophylaxis and had different conditioning regimens according tothe underlying disease. The patients were evaluated during the first one-hundred-day period after the HCT. Renal dysfunction was classified asfollows: Grade 0 (Normal renal function: < 25% decrement in creatinineclearance); Grade 1 (> 25% decrement in creatinine clearance but < atwofold increase in serum creatinine); Grade 2 (> twofold rise in serumcreatinine but no need for dialysis); Grade 3 (> twofold rise in serumcreatinine and need for dialysis). Baseline characteristics and renal com-plications of the patients are shown in the table:
Allogeneic HCT (n=18) Autologous HCT (n=11)
Gender (M/F) 9/9 5/6Age (years) 29.6 ± 10.1 40.9 ± 14.9Creatinine clearance (ml/min) 132 ± 39 129 ± 57Renal Dysfunction (Grade 1) 2 (11%) 2 (18%)Renal Dysfunction (Grade 2) 8 (44%) 2 (18%)Renal Dysfunction (Grade 3) 5 (28%) 0 (0%)
Renal dysfunction occurred in 19 of the 29 patients (66%). Renal dys-function was significantly more common in allogeneic HCT (83%) thanautologous HCT (36%) (P=0.01). Severe (grade 2 and 3) renal dysfunc-tion which developed in 52% of HCT recipients was significantly morecommon in patients with allogeneic HCT than autologous HCT (72% inthe allogeneic HCT versus 18% in the autologous HCT, P=0.005). A totalof 3 patients developed veno-occlusive disease (VOD) of the liver; all ofthem had allogeneic HCT and severe renal dysfunction. Four patients withallogeneic HCT and 2 patients with autologous HCT developed sepsis, allof whom had severe renal dysfunction. The overall one-hundred-day mor-tality rate was 24% (33% in allogeneic versus 9% in autologous HCT). Themortality rate among patients with severe renal dysfunction was 40%.In conclusion, renal dysfunction, which is a common finding during theearly period after HCT, is more common in allogeneic than autologousHCT and is associated with a high risk of mortality. The use of cyclosporineA for GVHD prophylaxis and an increased incidence of VOD of the liverin allogeneic HCT may have contributed to this finding.
W379 CONTINUOUS HEMOFILTRATION VERSUS CONTINUOUSHEMODIAFILTRATION IN CRITICALLY ILL PATIENTS WITHACUTE RENAL FAILURE
Patrick Saudan1, Michel Niederberger2, Michael Zellweger1,Jerome Pugin3, Jacques Romand2, Thomas Perneger4,Pierre-Yves Martin1. 1Nephrology Unit, Geneva University Hospitals,Geneva City, Geneva, Switzerland; 2Surgical Intensive Care Unit, GenevaUniversity Hospitals, Geneva City, Geneva, Switzerland; 3MedicalIntensive Care Unit, Geneva University Hospitals, Geneva City, Geneva,Switzerland; 4Quality of Care Unit, Geneva University Hospitals, GenevaCity, Geneva, Switzerland
To study the hypothesis that continuous venovenous hemodiafiltration(CVVHDF) is associated with a better survival than continuous veno-venous hemofiltration (CVVH) among critically ill patients with acute renalfailure.Prospective randomised trial comparing these two methods in patients un-
dergoing renal replacement therapy in intensive care units (interim analy-sis).112 patients were randomised from October 2000 to November 2002 andhad either CVVH (1-2.5 L/h replacement fluid) or continuous CVVHDF(1-2.5 L/h replacement fluid + 1-1.5L/h dialysate).
CCVH (56) CVVHDF (56) p
Age (years) mean (SD) 63 (14) 63 (15) nsGender (m/f) 34/22 36/20 nsRenal failure diagnosis (surgical/trauma/medical) 13/6/37 16/2/38 nsApache II score mean (SD) 27 (9) 24 (10) nsSepsis (%) 63 55 nsARDS (%) 29 18 nsDiabetes (%) 21 27 nsPretreatment BUN (mmol/L) mean (SD) 30 (13) 32 (14) nsPretreatment creatinine (µmol/L) mean (SD) 425 (185) 485 (346) nsPrescribed ultrafiltration (ml/kg/h) mean (SD) 26 (4) 23 (6) 0.02Prescribed dialysis (ml/kg/h) mean (SD) 18 (5)Renal replacement therapy duration (days)
(median + IQR) 4 (2-7) 3 (1-5) nsOne month survival (%) (Kaplan-Meyer analysis) 39 61 0.04
The patients included in this trial have a high prevalence of sepsis andARDS. The preliminary results suggest that CVVHDF is associated at onemonth with a better survival than CVVH. CVVHDF may affect the out-come of acute renal failure by providing a more adequate renal replacementtherapy.
Free Communication June 12
W380 CONTINUOUS HEMODIALYSIS IMPROVES THEMORTALITY OF CRITICAL PATIENTS WITH ACUTE RENALFAILURE IN COMPARISON WITH CONTINUOUSHEMOFILTRATION
Tatsuo Fukushima1, Yoshisuke Haruna1, Jun-ichi Ono2,Takehiko Tokura1, Tamaki Sasaki1, Naoki Kashihara1. 1Nephrology,Kawasaki Medical School, Kurashiki, Okayama, Japan; 2Kidney Center,Kawasaki Medical School, Kurashiki, Okayama, Japan
Background: Although continuous renal replacement therapy (CRRT)is increasingly used to cure acute renal failure (ARF) including that incritical state patients with such conditions as systemic inflammatory re-sponse syndrome (SIRS) or multiple organ failure (MOF), the most suitablemethodology for these patients has been controversial. To determine whichmethod of CRRT is most suitable, we retrospectively analyzed the progno-sis of ARF patients receiving CRRT, comparing those undergoing contin-uous hemofilitration (CHF) with those receiving continuous hemodialysis(CHD).Methods: A total of 176 patients with ARF caused by MOF or SIRS,with a mean age of 68.4 years old, treated by CRRT in our intensive careunit between 1997 and 2001 were retrospectively analyzed. A total of51 patients were treated with CHF (mean APACHE-2 score: 27.1, meanfiltration dose: 19.0 ml/hr/kg, mean age: 69.5 years, M=36, F=15). A totalof 125 patients were treated with CHD (mean APACHE-2 score: 30.1,mean dialysate dose: 36.5 ml/hr/kg, mean age: 67.9 years, M=82, F=43).The primary endpoint was survival at 28 days after beginning CRRT. Thesecond endpoint was survival discharge. To assess the dose of dialysate inthe CHD group, we also evaluated the survival rate comparing a high-fluxgroup (more than 25 ml/hr/kg, n=70) and a low-flux group (less than 25ml/hr/kg, n=55).Result: There were no significant differences in age, gender and APACHE-2 score between the two groups. The survival rate at the first endpoint inthe CHD group was significantly higher than that in the CHF group (CHD:60.8%, CHF: 39.2%: p=0.0091). The survival discharge rate tended to behigher in the CHD group than in the CHF group, but the difference wasnot statistically significant (CHD: 37.6%, CHF: 23.5%, p=0.072). Regard-ing the dose of dialysate, the survival rate was 60% at the first endpointin the high-flux group and 61.9% in the low-flux group. The survival dis-charge rate was 32.9% and 45.6%, respectively. There was not significantdifference between the two groups.Conclusion: The mortality among these patients with ARF was high, butCHD significantly improved survival in comparison with CHF. CHD canremove low-molecular substances better than CHF. As for the differences
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

Wednesday, June 11 B9. Acute renal failure, toxic nephropathy 667
in the prognosis in each group, it is suspected that removal of the low-molecular substances is important. We emphasize here that the CHD is abeneficial therapy for critical patients with ARF.
W381 SLOW LOW-EFFICIENT DAILY DIALYSIS (SLED) ASRENAL REPLACEMENT THERAPY FOR ACUTE RENALFAILURE IN THE INTENSIVE CARE UNIT: COMBINATIONOF SUPERIOR DETOXIFICATION AND EXCELLENTCARDIOVASCULAR TOLERABILITY IN SEVERELY ILLPATIENTS
Jan T. Kielstein, Ulrich Kretschmer, Thomas Ernst, Carsten Hafer,Hermann Haller, Danilo Fliser. Nephrology, Medical School Hannover,Hannover, Germany
Objective: Slow low-efficient daily dialysis (SLED) theoretically offersthe advantages of intermittent and continuous renal replacement therapieson the intensive care unit, i.e. a high dialysis dose combined with cardio-vascular stability.Patients and Methods: We randomly treated 36 ventilated patients witholiguric acute renal failure either with high volume (> 35 ml/kg/h) con-tinuous veno-venous hemofiltration (hvCVVH; n = 18, 52 ± 15 years,APACHE II 32 ± 6) or SLED (n = 18, 51 ± 12 years, APACHE II 32 ± 5)for 24 hours. SLED was performed using a technically simple single-passbatch dialysis system (GENIUS, Fresenius Medical Care Germany). Weused high-flux polysulphone dialyzers for all treatments. Hemodynamicparameters were monitored on-line with an indwelling arterial catheter.Results: Hemodynamic parameters (Table) and net ultrafiltration volume(hvCVVH: 3.2 ± 1.8 l/24h; SLED: 3.7 ± 2.5 l/24h; n.s.) were comparablewith both therapies. In contrast, comparable urea blood concentrationswere achieved already after 12 hours of SLED as compared with 24h ofhvCVVH despite an average treatment dose with hvCVVH of 3.1 ± 1.1l/h.
Comparison of pre-treatment and post-treatment parameters in patients treated with ei-ther 24 hrs hvCVVH or 12 hrs SLED (GENIUS-system)
PRE-treatment POST-treatment
hv CVVH SLED hv CVVH SLED
MAP (mmHg) 74 ± 12 71 ± 16 75 ± 18 77 ± 17heart rate (b/min) 95 ± 26 101 ± 23 85 ± 19 86 ± 21CO index (l/min/m2 ) 4.1 ± 1.3 4.3 ± 1.5 4.1 ± 1.0 3.7 ± 1.8SVR index (dyn.s.cm-5.m2) 615 ± 313 671 ± 333 632 ± 358 834 ± 446S-creatinine (µmol/l) 334 ± 175 358 ± 136 131 ± 61 110 ± 45S-urea (mmol/l) 30.9 ± 16.7 29.7 ± 12.9 14.2 ± 7.3 8.5 ± 2.9*S-phosphate (mmol/l) 2.2 ± 0.9 2.2 ± 0.7 1.1 ± 0.5 1.0 ± 0.4arterial blood pH 7.31 ± 0.11 7.32 ± 0.11 7.34 ± 0.15 7.39 ± 0.08*arterial bicarbonate (mmol/l) 20.9 ± 3.5 21.6 ± 5.0 23.4 ± 5.4 25.0 ± 3.3
*p<0.01
Conclusion: SLED is a new modality of renal replacement therapy thatcombines superior detoxification with excellent cardiovascular tolerabilityeven in severely ill patients on the intensive care unit. Moreover, the tech-nically simple dialysis system used offers high treatment time flexibilityand operates at much lower costs than high volume CVVH.
W382 HAEMOFILTER LIFETIMES WITH HIGH DOSE CRRT ANDREASONS FOR HAEMOFILTER DISCONTINUATION
Detlef Kindgen-Milles1, Robert Pohlmeier2, Eckhard Mueller1. 1Klinikfür Anästhesiologie, Universitätsklinikum Düsseldorf, Düsseldorf,Germany; 2Fresenius Medical Care, Bad Homburg, Germany
Recent studies have led to the recommendation of increased dose of CRRTin the treatment of acute renal failure. We describe our experience withhigh-dose CRRT with special respect to aspects of haemofilter lifetime andreasons for filter discontinuation.Single-center, oberservational study including 67 consecutively usedhaemofilters in 20 patients. The treatments were performed using a modernCRRT device (Multifiltrate, Fresenius Medical Care) and a large surfacearea haemofilter (1.8 m2) with a polysulfone membrane (AV1000S, Fre-senius Medical Care). Depending on the individual patient, either heparinor hirudin was used as anticoagulant. The dose of CRRT was defined as
the sum of net ultrafiltration plus HF-solution turn-over and was targetedat ≥ 40 ml per kg body weight per hour. Filter lifetime and reasons forfilter discontinuation were the primary variabels. Detailed treatment pa-rameters and serum chemistry for the first 96 h of each heaemofilter usewere collected, however, filters were not discontinued automatically after96h.Postdilution-CVVHDF was the preferred treatment modality (56 haemofil-ters), additionally predilution-CVVHDF (3 haemofilters) and the combina-tion of pre- and postdilution CVVH (8 haemofilters) were used. The dosesof CRRT applied were 50 ± 15 ml/h/kg (mean ± SD) for all haemofil-ters and 46 ± 11 ml/h/kg for those used in postdilution-CVVHDF at thestart of the treatment and dropped slowly to 37 ± 10 ml/h/kg and 35 ±10 ml/h/kg at 96 h of haemofilter usage, respectively. The mean filter life-time was 49.3 ± 34.7 h for all haemofilters and 51.2 ± 35.3 h for thoseused in postdilution-CVVHDF. The Kaplan-Meier filter survival curves didnot reveal any difference between the three treatment modes (see figure),nor between heparin and hirudin anticoagulation. 49% of all haemofilterswere used for at least 48 h. 38% of the haemofilters used in postdilution-CVVHDF were discontinued for reasons not related to coagulation prob-lems (e.g. elective changes, transfer of patients), 38% were discontinuedbecause of coagulation of the system (e.g. visible coagulation, increase ofpre-haemofilter pressure, increase of transmembrane pressure), and 24%were discontinued because of other CRRT related problems (e.g. catheterchange).
We showed that a high dose of CRRT is feasible with advantageoushaemofilter lifetimes. Reasons not directly related to CRRT therapy ledto the discontinuation of more than one third of the haemofilters.
W383 EVALUATION OF THE SEVERITY OF COMPLICATIONS BYACUTE RENAL FAILURE WITH MULTIPLE ORGANFAILURE TREATED BY ON-LINE CONTINUOUSHEMODIAFILTRATION
Hideki Kawanishi, Touru Kawai, Kouji Watanabe, Misaki Moriishi,Shinichiro Tsuchiya. Artificial Organs, Akane Foundation, TsuchiyaGeneral Hospital, Hiroshima, Japan
The survival rate of patients who experienced acute renal failure (ARF)with multiple organ failure (MOF) is extremely low. In the present study,we evaluate the survival rate of ARF patients who underwent continuousrenal replacement therapy (CRRT).The subjects consisted of 348 patients (include 151 chronic hemodialysispatients (CHD) with MOF) who underwent CRRT over the last 7 years.CRRT was performed by continuous hemodiafiltration (CHDF), mainly on-line CHDF. The maximum operation condition of on-line CHDF was bloodflow: 100 mL/min, filtration flow: pre-dilution 100 mL/min, post-dilution30 mL/min, and dialysate flow: 100 mL/min used PS-filter. APACH-IIscore and SOFA scores were calculated immediately before starting CRRTand 1st, 3rd, 7th ICU days. The survival group included those who survivedfor more than 30 days after starting CRRT.The survival rate was different depend on the induced etiology of MOF;sepsis 54% in 134 patients; cardiac failure due to AMI 65% in 55 patients;post open heart operation 72% in 47 patients. There were significant dif-ferences in APACH-II scores and SOFA scores between the surviving anddead patients in the respective groups. In addition, both scores were lowerin dead patients in the CHD group than in the non-CHD group. APACH-II
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022

668 B9. Acute renal failure, toxic nephropathy Wednesday, June 11
scores were positively correlated with SOFA scores in both groups. Al-though 95% of the deaths patients were distributed in the area where theAPACH-II scores was above 21 and the SOFA scores was above 8 in sepsisARF, and that was 23 and 10 point in AMI–ARF, 22 and 10 point postopen heart operation-ARF, respectively. Evaluation that used target SOFAscore during ICU days, the score has improved the 7th day rapidly as theboundary in the survival casesDualism evaluation by APACHE-II score and also SOFA score is effec-tive to evaluate mortality rate in ARF with MOF. The evaluation of amore advanced lifesaving rate becomes possible, by examining to the tar-get through SOFA score. We concluded that on-line CHDF is safe andeffective at maintainig ARF patients.
W384 DIALYSIS-DEPENDENT ACUTE RENAL FAILURE (ARF) INLIVER POST-TRANSPLANT (OLT)
Antonio Santoro1, Elena Mancini1, Rossella Gaggi1, Serena Bainotti1,Silvia Pareschi2, Stefano Faenza2. 1Malpighi Nephrology and Dialysis,Policlinico S.Orsola-Malpighi, Bologna, Italy; 2Institute ofAnesthesiology and Intensive Care Medicine, PoliclinicoS.Orsola-Malpighi, Bologna, Italy
Renal dysfunction is generally considered to be a frequent complicationin the course of OLT. However, there are no data, in the immediate post-surgical phase, on the prevalence, aetiology, evolutionary characteristics ofARF needing dialysis therapy (HD). For this purpose we have retrospec-tively analysed all the cases of OLT concerning the years 1999-2001.Out of a total number of 240 OLT there were 20 cases (16 M, 4F) of ARFtreated with HD (prevalence = 8.33%). The mortality in this group was 45%(9/20). In nearly all the cases (17/20) there was already a functional multi-organ insufficiency. In 80% of the cases (16/20) ARF appeared within 5days of the OLT (early ARF), in the other cases (4/20) between the 6th andthe 14th day (late ARF). The progressive nature of ARF (12/15 in the earlyform and 1/3 in the late form) was accompanied by a high mortality (8/13,61.5%), compared with the non-progressive trend in which no deaths wereobserved. Hypovolemia was absolutely the most frequent aetiological fac-tor of ARF (15/20, 75%), followed by both endogenous (hyperbilirubine-mia, 10/20, 50%), and exogenous (drugs, 9/20, 45%) nephrotoxicity, andby sepsis (8/20, 40%). In the deceased patients (D), during their hospitali-sation at the intensive care unit, the main cause of ARF was nephrotoxityin association with hypovolemia and/or sepsis (5/9).An early development of severe ARF (creatinine increase >0.5 mg/ml/diewith urinary output< 10 ml/h) was the most frequent in patients on therapywith tacrolimus with circulating drug levels >5 ng/ml, and concomitantlygraft dysfunction.The parameters significantly different between D patients and survivors(S = transferred to another department) were: the presence of pre-surgicalrenal dysfunction (4 cases: 3 D/1 S), the kind of surgery (emergency:mortality 60%, first-choice 26.7%, p=0.05), the APACHE II score (D 24.8vs. S 17.2, p<0.05) and the urinary output (S 159.7 vs D 44.4 ml/h, p<0.05)both evaluated at the occurrence of the HD need. Instead we did not observeany differences in the type (intermittent or continuous) or the number ofdays of dialysis treatment performed.The mortality of patients developing ARF after OLT remains high. Hypo-volemia appears to be a dominant critical factor, together with endogenousand exogenous toxic factors. Nephrotoxicity due to tacrolimus seems to beparticularly severe if associated to a graft dysfunction.
W385 WHICH PATIENTS BENEFIT FROM HEMODIALYSISTHERAPY IN HEPATORENAL SYNDROME (HRS)?
O. Witzke, M. Baumann, D. Patschan, D. Eder, T. Philipp, A. Kribben.Dept. of Nephrology, University of Essen, Essen, Germany
Hepatorenal syndrome has a poor outcome. It was the aim of this study toinvestigate which patients with hepatorenal syndrome are likely to benefitfrom hemodialysis.We prospectively studied 25 patients with Child-Pugh C liver cirrhosis,hepatorenal syndrome and oliguria. Patients were either assigned to con-tinuous veno-venous hemodialysis (CVVHD) treatment (Group A) if theywere mechanically ventilated or to intermittent hemodialysis (HD) treat-
ment (Group B) if they were not mechanically ventilated. Anticoagulationwas either performed systemically with heparin or as a regional anticoagu-lation using citrate. Prognosis was assessed by the Apache-II score (withoutGlasgow coma scale) and by the Liano-Score. The primary end-point foranalysis was survival time under dialysis therapy. Secondary end-pointswere survival associated with mild (stage I and II) or severe hepatic en-cephalopathy (stage III or IV) and lethal complications due to anticoagula-tion.The Apache II score (without Glasgow coma scale) was 18.9±2.5 (range16-25) in group A and 12.1±1.2 (range 11-15) in group B (p<0.001).The Liano score was 0.98±0.05 in group A and 0.57±0.14 in group B(p<0.01). Patient’s 30-day survival was 0/12 in group A (CVVHD) and7/13 in group B (HD). The median survival time under dialysis therapywas 3 days (Range 1-10 days) in group A and 34 days (Range 1-422 days)in group B. The two patients with severe (stage III) hepatic encephalopathyin group B had with 1 and 6 days the shortest survival in this group. Threepatients from group B survived after successful liver transplantation whileall other patients from both groups died within the observation time. Weobserved two lethal intracerebral bleedings in patients receiving heparinanticoagulation, while no bleeding complication occurred with regionalcitrate anticoagulation.In conclusion, patients with HRS without mechanical ventilation and with-out severe encephalopathy may benefit from hemodialysis while hemodial-ysis seems to be futile in patients with HRS with mechanical ventilation orsevere encephalopathy (stage III).
W386 PHARMACOKINETICS AND TOTAL DIALYSATECONCENTRATION OF VANCOMYCIN IN INTENSIVE CAREUNIT PATIENTS TREATED BY SLOW LOW-EFFICIENTDAILY DIALYSIS (SLED)
Jan T. Kielstein1, David Czock2, Timo Schöpke1, StefanieM. Bode-Böger3, Hermann Haller1, Frieder Keller2, Danilo Fliser1.1Nephrology, Medical School Hannover, Hannover, Germany;2Nephrology, University Hospital Ulm, Ulm, Germany; 3Institute ofClinical Pharmacology, Otto-von Guericke University, Magdeburg,Germany
Slow low-efficient daily dialysis (SLED) has recently been introduced as anew mode of renal replacement therapy for critically ill patients. It offerssuperior detoxification and excellent cardiovascular tolerability. Hence,SLED is increasingly used in intensive care units (ICU) around the world.Objective: Vancomycin is a glycopeptide antibiotic that is used in thetreatment of severe infections especially in ICU patients. So far only dataabout dialyzability employing either intermittent or continuous renal re-placement therapies are available. The aim of the study was to investigatethe influence of SLED on the pharmacokinetics of vancomycin as well asto measure the absolute amount of the drug removed. The latter was possi-ble using the GENIUS, a simple and extremely versatile single-pass batchdialysis system. The system permits easy access to the entire amount ofsubstances that has been removed during a dialysis session.Patients and Methods: Nine adult intensive care patients with acute renalfailure being treated by SLED. All patients were anuric. Patients received a8h SLED,with a blood and dialysate flow of 160 ml/min. For all treatmentsa 1.2 m2 high-flux polysulphone dialyzer was used. The choice of theantibiotic was made on clinical grounds alone. Vancomycin (1.0g) wasinfused via infusion pump over a period of 60 min, 12 h before SLED wasstarted. Blood samples were drawn before, 0.5h, 1h, 2h, 4h, 6h and 8h afteradministration, before dialysis, during dialysis at time points 2h, 4h and 6h,at the end of the treatment as well as 0.5h, 1h, 3h and 8h after treatment. Inaddition, total drug removal was assessed by measuring drug concentrationin the spent dialysate.Results: The average vancomycin plasma concentrations of the patients isshown in the Figure. The following pharmacocinetic parameters have beencalculated. Cmax:30 ± 8 µg/mL, Tmax: 102 ± 31 min, CLanur: 22 ± 11mL/min, T1/2anur: 1739 ± 930 min (= 29 ± 15.5 h) T1/2hd: 720 ± 270 min(= 12 ± 4.5 h). The total dialysate concentration was 202 ± 59 µg/mL.Conclusion: SLED eliminates a consideralbe amount of vancomycin. Avancomycin dose of 1.0 g every does not provide an adequate serum con-centration over a period of 30 h in patients receiving SLED with a1.2m2 high-flux polysulphone dialyzer. Our data suggest that a different dos-
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022
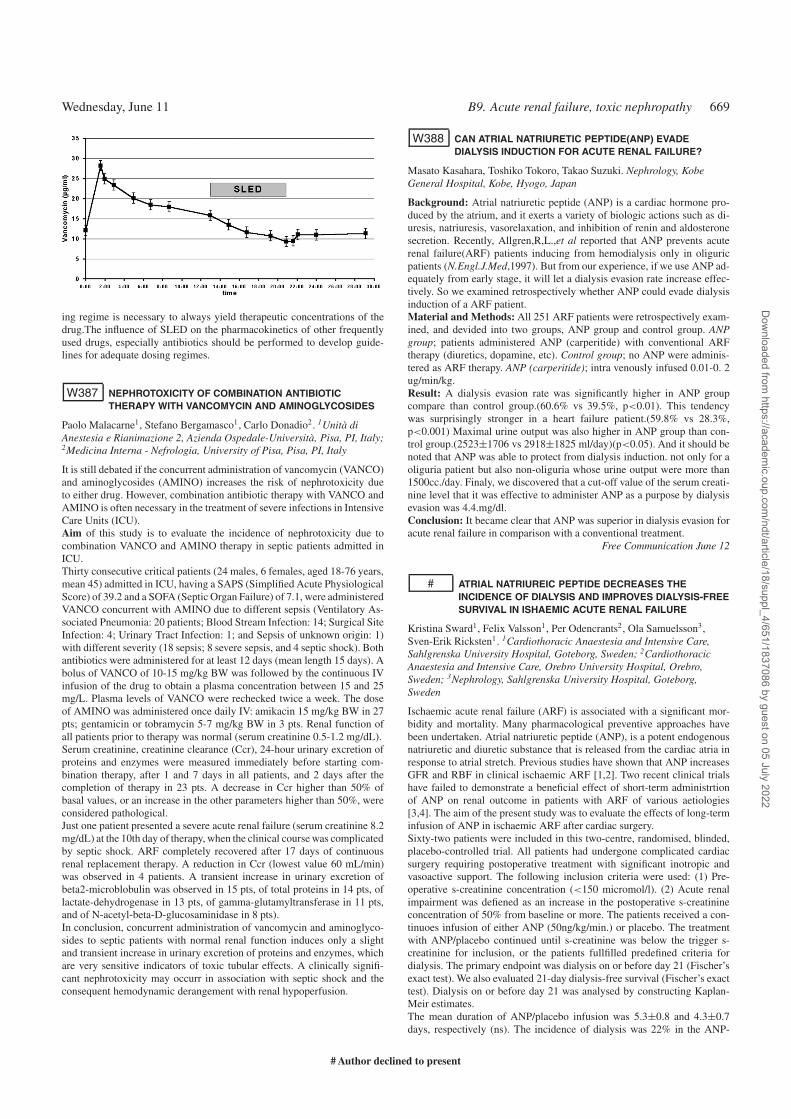
Wednesday, June 11 B9. Acute renal failure, toxic nephropathy 669
ing regime is necessary to always yield therapeutic concentrations of thedrug.The influence of SLED on the pharmacokinetics of other frequentlyused drugs, especially antibiotics should be performed to develop guide-lines for adequate dosing regimes.
W387 NEPHROTOXICITY OF COMBINATION ANTIBIOTICTHERAPY WITH VANCOMYCIN AND AMINOGLYCOSIDES
Paolo Malacarne1, Stefano Bergamasco1, Carlo Donadio2. 1Unità diAnestesia e Rianimazione 2, Azienda Ospedale-Università, Pisa, PI, Italy;2Medicina Interna - Nefrologia, University of Pisa, Pisa, PI, Italy
It is still debated if the concurrent administration of vancomycin (VANCO)and aminoglycosides (AMINO) increases the risk of nephrotoxicity dueto either drug. However, combination antibiotic therapy with VANCO andAMINO is often necessary in the treatment of severe infections in IntensiveCare Units (ICU).Aim of this study is to evaluate the incidence of nephrotoxicity due tocombination VANCO and AMINO therapy in septic patients admitted inICU.Thirty consecutive critical patients (24 males, 6 females, aged 18-76 years,mean 45) admitted in ICU, having a SAPS (Simplified Acute PhysiologicalScore) of 39.2 and a SOFA (Septic Organ Failure) of 7.1, were administeredVANCO concurrent with AMINO due to different sepsis (Ventilatory As-sociated Pneumonia: 20 patients; Blood Stream Infection: 14; Surgical SiteInfection: 4; Urinary Tract Infection: 1; and Sepsis of unknown origin: 1)with different severity (18 sepsis; 8 severe sepsis, and 4 septic shock). Bothantibiotics were administered for at least 12 days (mean length 15 days). Abolus of VANCO of 10-15 mg/kg BW was followed by the continuous IVinfusion of the drug to obtain a plasma concentration between 15 and 25mg/L. Plasma levels of VANCO were rechecked twice a week. The doseof AMINO was administered once daily IV: amikacin 15 mg/kg BW in 27pts; gentamicin or tobramycin 5-7 mg/kg BW in 3 pts. Renal function ofall patients prior to therapy was normal (serum creatinine 0.5-1.2 mg/dL).Serum creatinine, creatinine clearance (Ccr), 24-hour urinary excretion ofproteins and enzymes were measured immediately before starting com-bination therapy, after 1 and 7 days in all patients, and 2 days after thecompletion of therapy in 23 pts. A decrease in Ccr higher than 50% ofbasal values, or an increase in the other parameters higher than 50%, wereconsidered pathological.Just one patient presented a severe acute renal failure (serum creatinine 8.2mg/dL) at the 10th day of therapy, when the clinical course was complicatedby septic shock. ARF completely recovered after 17 days of continuousrenal replacement therapy. A reduction in Ccr (lowest value 60 mL/min)was observed in 4 patients. A transient increase in urinary excretion ofbeta2-microblobulin was observed in 15 pts, of total proteins in 14 pts, oflactate-dehydrogenase in 13 pts, of gamma-glutamyltransferase in 11 pts,and of N-acetyl-beta-D-glucosaminidase in 8 pts).In conclusion, concurrent administration of vancomycin and aminoglyco-sides to septic patients with normal renal function induces only a slightand transient increase in urinary excretion of proteins and enzymes, whichare very sensitive indicators of toxic tubular effects. A clinically signifi-cant nephrotoxicity may occurr in association with septic shock and theconsequent hemodynamic derangement with renal hypoperfusion.
W388 CAN ATRIAL NATRIURETIC PEPTIDE(ANP) EVADEDIALYSIS INDUCTION FOR ACUTE RENAL FAILURE?
Masato Kasahara, Toshiko Tokoro, Takao Suzuki. Nephrology, KobeGeneral Hospital, Kobe, Hyogo, Japan
Background: Atrial natriuretic peptide (ANP) is a cardiac hormone pro-duced by the atrium, and it exerts a variety of biologic actions such as di-uresis, natriuresis, vasorelaxation, and inhibition of renin and aldosteronesecretion. Recently, Allgren,R,L.,et al reported that ANP prevents acuterenal failure(ARF) patients inducing from hemodialysis only in oliguricpatients (N.Engl.J.Med,1997). But from our experience, if we use ANP ad-equately from early stage, it will let a dialysis evasion rate increase effec-tively. So we examined retrospectively whether ANP could evade dialysisinduction of a ARF patient.Material and Methods: All 251 ARF patients were retrospectively exam-ined, and devided into two groups, ANP group and control group. ANPgroup; patients administered ANP (carperitide) with conventional ARFtherapy (diuretics, dopamine, etc). Control group; no ANP were adminis-tered as ARF therapy. ANP (carperitide); intra venously infused 0.01-0. 2ug/min/kg.Result: A dialysis evasion rate was significantly higher in ANP groupcompare than control group.(60.6% vs 39.5%, p<0.01). This tendencywas surprisingly stronger in a heart failure patient.(59.8% vs 28.3%,p<0.001) Maximal urine output was also higher in ANP group than con-trol group.(2523±1706 vs 2918±1825 ml/day)(p<0.05). And it should benoted that ANP was able to protect from dialysis induction. not only for aoliguria patient but also non-oliguria whose urine output were more than1500cc./day. Finaly, we discovered that a cut-off value of the serum creati-nine level that it was effective to administer ANP as a purpose by dialysisevasion was 4.4.mg/dl.Conclusion: It became clear that ANP was superior in dialysis evasion foracute renal failure in comparison with a conventional treatment.
Free Communication June 12
# ATRIAL NATRIUREIC PEPTIDE DECREASES THEINCIDENCE OF DIALYSIS AND IMPROVES DIALYSIS-FREESURVIVAL IN ISHAEMIC ACUTE RENAL FAILURE
Kristina Sward1, Felix Valsson1, Per Odencrants2, Ola Samuelsson3,Sven-Erik Ricksten1. 1Cardiothoracic Anaestesia and Intensive Care,Sahlgrenska University Hospital, Goteborg, Sweden; 2CardiothoracicAnaestesia and Intensive Care, Orebro University Hospital, Orebro,Sweden; 3Nephrology, Sahlgrenska University Hospital, Goteborg,Sweden
Ischaemic acute renal failure (ARF) is associated with a significant mor-bidity and mortality. Many pharmacological preventive approaches havebeen undertaken. Atrial natriuretic peptide (ANP), is a potent endogenousnatriuretic and diuretic substance that is released from the cardiac atria inresponse to atrial stretch. Previous studies have shown that ANP increasesGFR and RBF in clinical ischaemic ARF [1,2]. Two recent clinical trialshave failed to demonstrate a beneficial effect of short-term administrtionof ANP on renal outcome in patients with ARF of various aetiologies[3,4]. The aim of the present study was to evaluate the effects of long-terminfusion of ANP in ischaemic ARF after cardiac surgery.Sixty-two patients were included in this two-centre, randomised, blinded,placebo-controlled trial. All patients had undergone complicated cardiacsurgery requiring postoperative treatment with significant inotropic andvasoactive support. The following inclusion criteria were used: (1) Pre-operative s-creatinine concentration (<150 micromol/l). (2) Acute renalimpairment was defiened as an increase in the postoperative s-creatinineconcentration of 50% from baseline or more. The patients received a con-tinuoes infusion of either ANP (50ng/kg/min.) or placebo. The treatmentwith ANP/placebo continued until s-creatinine was below the trigger s-creatinine for inclusion, or the patients fullfilled predefined criteria fordialysis. The primary endpoint was dialysis on or before day 21 (Fischer’sexact test). We also evaluated 21-day dialysis-free survival (Fischer’s exacttest). Dialysis on or before day 21 was analysed by constructing Kaplan-Meir estimates.The mean duration of ANP/placebo infusion was 5.3±0.8 and 4.3±0.7days, respectively (ns). The incidence of dialysis was 22% in the ANP-
# Author declined to present
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022
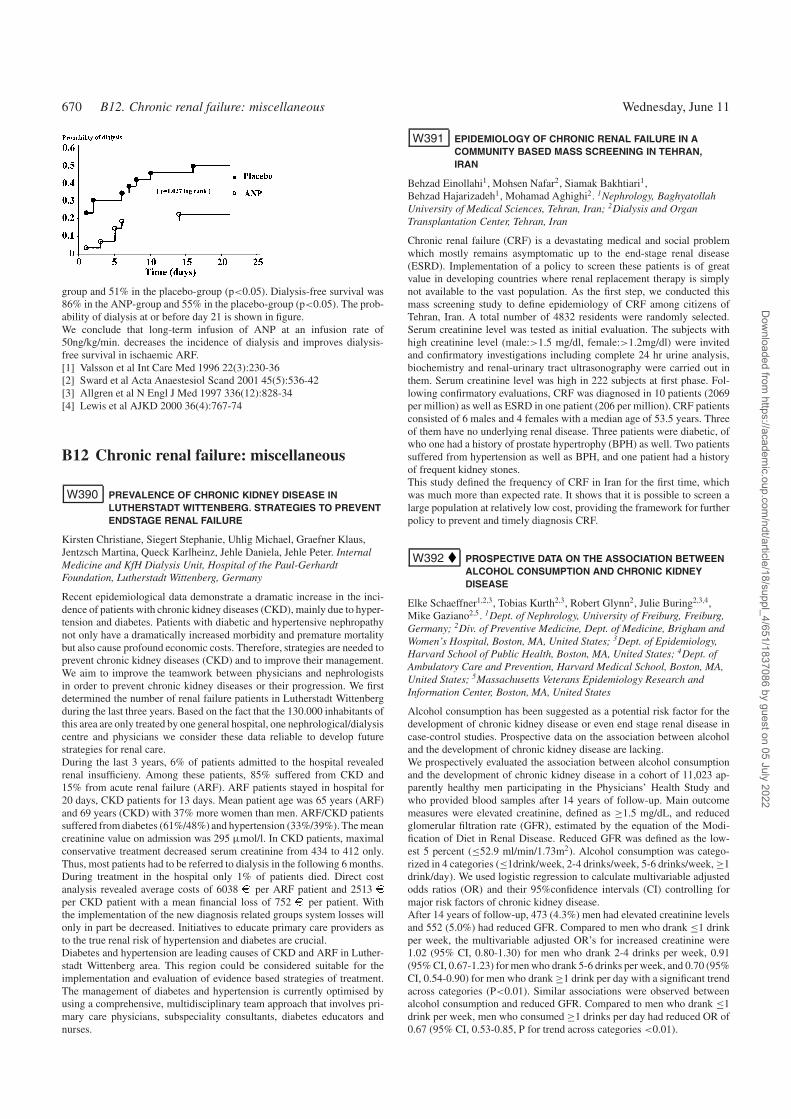
670 B12. Chronic renal failure: miscellaneous Wednesday, June 11
group and 51% in the placebo-group (p<0.05). Dialysis-free survival was86% in the ANP-group and 55% in the placebo-group (p<0.05). The prob-ability of dialysis at or before day 21 is shown in figure.We conclude that long-term infusion of ANP at an infusion rate of50ng/kg/min. decreases the incidence of dialysis and improves dialysis-free survival in ischaemic ARF.[1] Valsson et al Int Care Med 1996 22(3):230-36[2] Sward et al Acta Anaestesiol Scand 2001 45(5):536-42[3] Allgren et al N Engl J Med 1997 336(12):828-34[4] Lewis et al AJKD 2000 36(4):767-74
B12 Chronic renal failure: miscellaneous
W390 PREVALENCE OF CHRONIC KIDNEY DISEASE INLUTHERSTADT WITTENBERG. STRATEGIES TO PREVENTENDSTAGE RENAL FAILURE
Kirsten Christiane, Siegert Stephanie, Uhlig Michael, Graefner Klaus,Jentzsch Martina, Queck Karlheinz, Jehle Daniela, Jehle Peter. InternalMedicine and KfH Dialysis Unit, Hospital of the Paul-GerhardtFoundation, Lutherstadt Wittenberg, Germany
Recent epidemiological data demonstrate a dramatic increase in the inci-dence of patients with chronic kidney diseases (CKD), mainly due to hyper-tension and diabetes. Patients with diabetic and hypertensive nephropathynot only have a dramatically increased morbidity and premature mortalitybut also cause profound economic costs. Therefore, strategies are needed toprevent chronic kidney diseases (CKD) and to improve their management.We aim to improve the teamwork between physicians and nephrologistsin order to prevent chronic kidney diseases or their progression. We firstdetermined the number of renal failure patients in Lutherstadt Wittenbergduring the last three years. Based on the fact that the 130.000 inhabitants ofthis area are only treated by one general hospital, one nephrological/dialysiscentre and physicians we consider these data reliable to develop futurestrategies for renal care.During the last 3 years, 6% of patients admitted to the hospital revealedrenal insufficieny. Among these patients, 85% suffered from CKD and15% from acute renal failure (ARF). ARF patients stayed in hospital for20 days, CKD patients for 13 days. Mean patient age was 65 years (ARF)and 69 years (CKD) with 37% more women than men. ARF/CKD patientssuffered from diabetes (61%/48%) and hypertension (33%/39%). The meancreatinine value on admission was 295 µmol/l. In CKD patients, maximalconservative treatment decreased serum creatinine from 434 to 412 only.Thus, most patients had to be referred to dialysis in the following 6 months.During treatment in the hospital only 1% of patients died. Direct costanalysis revealed average costs of 6038 e per ARF patient and 2513 eper CKD patient with a mean financial loss of 752 e per patient. Withthe implementation of the new diagnosis related groups system losses willonly in part be decreased. Initiatives to educate primary care providers asto the true renal risk of hypertension and diabetes are crucial.Diabetes and hypertension are leading causes of CKD and ARF in Luther-stadt Wittenberg area. This region could be considered suitable for theimplementation and evaluation of evidence based strategies of treatment.The management of diabetes and hypertension is currently optimised byusing a comprehensive, multidisciplinary team approach that involves pri-mary care physicians, subspeciality consultants, diabetes educators andnurses.
W391 EPIDEMIOLOGY OF CHRONIC RENAL FAILURE IN ACOMMUNITY BASED MASS SCREENING IN TEHRAN,IRAN
Behzad Einollahi1, Mohsen Nafar2, Siamak Bakhtiari1,Behzad Hajarizadeh1, Mohamad Aghighi2. 1Nephrology, BaghyatollahUniversity of Medical Sciences, Tehran, Iran; 2Dialysis and OrganTransplantation Center, Tehran, Iran
Chronic renal failure (CRF) is a devastating medical and social problemwhich mostly remains asymptomatic up to the end-stage renal disease(ESRD). Implementation of a policy to screen these patients is of greatvalue in developing countries where renal replacement therapy is simplynot available to the vast population. As the first step, we conducted thismass screening study to define epidemiology of CRF among citizens ofTehran, Iran. A total number of 4832 residents were randomly selected.Serum creatinine level was tested as initial evaluation. The subjects withhigh creatinine level (male:>1.5 mg/dl, female:>1.2mg/dl) were invitedand confirmatory investigations including complete 24 hr urine analysis,biochemistry and renal-urinary tract ultrasonography were carried out inthem. Serum creatinine level was high in 222 subjects at first phase. Fol-lowing confirmatory evaluations, CRF was diagnosed in 10 patients (2069per million) as well as ESRD in one patient (206 per million). CRF patientsconsisted of 6 males and 4 females with a median age of 53.5 years. Threeof them have no underlying renal disease. Three patients were diabetic, ofwho one had a history of prostate hypertrophy (BPH) as well. Two patientssuffered from hypertension as well as BPH, and one patient had a historyof frequent kidney stones.This study defined the frequency of CRF in Iran for the first time, whichwas much more than expected rate. It shows that it is possible to screen alarge population at relatively low cost, providing the framework for furtherpolicy to prevent and timely diagnosis CRF.
W392 PROSPECTIVE DATA ON THE ASSOCIATION BETWEENALCOHOL CONSUMPTION AND CHRONIC KIDNEYDISEASE
Elke Schaeffner1,2,3, Tobias Kurth2,3, Robert Glynn2, Julie Buring2,3,4,Mike Gaziano2,5. 1Dept. of Nephrology, University of Freiburg, Freiburg,Germany; 2Div. of Preventive Medicine, Dept. of Medicine, Brigham andWomen’s Hospital, Boston, MA, United States; 3Dept. of Epidemiology,Harvard School of Public Health, Boston, MA, United States; 4Dept. ofAmbulatory Care and Prevention, Harvard Medical School, Boston, MA,United States; 5Massachusetts Veterans Epidemiology Research andInformation Center, Boston, MA, United States
Alcohol consumption has been suggested as a potential risk factor for thedevelopment of chronic kidney disease or even end stage renal disease incase-control studies. Prospective data on the association between alcoholand the development of chronic kidney disease are lacking.We prospectively evaluated the association between alcohol consumptionand the development of chronic kidney disease in a cohort of 11,023 ap-parently healthy men participating in the Physicians’ Health Study andwho provided blood samples after 14 years of follow-up. Main outcomemeasures were elevated creatinine, defined as ≥1.5 mg/dL, and reducedglomerular filtration rate (GFR), estimated by the equation of the Modi-fication of Diet in Renal Disease. Reduced GFR was defined as the low-est 5 percent (≤52.9 ml/min/1.73m2). Alcohol consumption was catego-rized in 4 categories (≤1drink/week, 2-4 drinks/week, 5-6 drinks/week, ≥1drink/day). We used logistic regression to calculate multivariable adjustedodds ratios (OR) and their 95%confidence intervals (CI) controlling formajor risk factors of chronic kidney disease.After 14 years of follow-up, 473 (4.3%) men had elevated creatinine levelsand 552 (5.0%) had reduced GFR. Compared to men who drank ≤1 drinkper week, the multivariable adjusted OR’s for increased creatinine were1.02 (95% CI, 0.80-1.30) for men who drank 2-4 drinks per week, 0.91(95% CI, 0.67-1.23) for men who drank 5-6 drinks per week, and 0.70 (95%CI, 0.54-0.90) for men who drank ≥1 drink per day with a significant trendacross categories (P<0.01). Similar associations were observed betweenalcohol consumption and reduced GFR. Compared to men who drank ≤1drink per week, men who consumed ≥1 drinks per day had reduced OR of0.67 (95% CI, 0.53-0.85, P for trend across categories <0.01).
Dow
nloaded from https://academ
ic.oup.com/ndt/article/18/suppl_4/651/1837086 by guest on 05 July 2022