glomerular fcαr expression and disease activity in iga nephropathy
TRANSCRIPT

Glomerular FctxR Expression and Disease Activity in IgA Nephropathy
Abul Kashem, MD, Masayuki Endoh, MD, Naohiro Yano, MD, Fumio Yamauchi, MD, Yasuo Nomoto, MD, Hideto Sakai, MD, and Kiyoshi Kurokawa, MD
0 In this study, we examined the receptors for the Fc portion of immunoglobulin A (IgA) (Fc&) in the glomeruli as well as circulating polymorphonuclear leukocytes and monocytes at the mRNA level by reverse transcription- polymerase chain reaction (RT-PCR) assay and at the protein level by an immunohistochemistry/flow cytometry technique using a specific anti-FccuR monoclonal antibody (My 43). Glomeruli were isolated from biopsy specimens of renal tissues from IgA nephropathy (IgAN; 20 cases) and non-IgA mesangial proliferative glomerulonephritis (PGN; 13 cases) patients, and from normal renal tissue specimens obtained from kidneys removed because of malignancies (five cases) applying the microdissection method. There was a relative increase in FccuR in the circulating phagocytes from IgAN patients compared with those from PGN and healthy controls. FcctR expression was present in approximately 40% of glomeruli samples from IgAN patients at the message levels. FccuR-positive specimens were also strongly positive for expression of tumor necrosis factor-a, interleukin-1, and interleukin-6 mRNA. Specimens from PGN patients and healthy controls did not show any detectable FccuR message. Serum IgA levels and severity of hematuria were significantly higher in patients with positive FccvR expression. A message for FccuR was detected in the tissues that were more damaged histologically. Our data suggest that there is some in vivo induction of glomerular FccuR expression, possibly mediated by a synergistic stimulus from IgA and inflammatory cytokines, and the expressed receptor is likely to be involved in the disease process of IgAN. 0 1997 by the National Kidney Foundation, Inc.
INDEX WORDS: IgA nephropathy; glomerular FccuR expression; hematuria; tissue damage.
P RIMARY immunoglobulin A nephropathy (IgAN) is an immunologically mediated ne-
phropathy characterized by a predominance of IgA deposits in the mesangium,’ which are thought to represent the counterpart of the circu- lating IgA immune complexes (IgA-ICs) that are often detectable in the sera of IgAN patients.2’3 Although it is suspected that the deposition of IgA-ICs in the mesangium may mediate tissue injury, the mechanism(s) by which these immune complexes are deposited in the mesangium and thus cause tissue injury is unknown. Many inves- tigators speculated that receptors for the Fc por- tion of IgA (FcatR) are responsible for binding of IgA-ICs in the glomerular regions, and the existence of such a receptor on a variety of cell types, including human neutrophils, monocytes, macrophages, and eosinophils, and probably on certain populations of lymphocytes has been re- ported.4 FcorR has been defined as a variable gly- cosylated protein of 55 to 75 kd that can bind IgAl and IgA2 antibodies via their Fc regions5
Although glomerular deposition of IgA-ICs is one of the diagnostic criteria and their receptor- specific interaction with IgA receptor-bearing cells is one of the likely routes of pathogenesis in IgAN, there has been no direct evidence of FccuR expression in the human glomemli. Re- cently, Gomez-Guerrero et al6 described a spe-
cific IgA receptor in rat and human mesangial cells, and the expression was shown to be aug- mented by IgA in cultured human mesangial cells. However, whether such a receptor exists in human glomeruli (in vivo), and if present, what its functional significance is in IgAN remain to be determined. Therefore, it is necessary to eluci- date the existence of FccrR and its functional significance in IgAN. In this study, we investi- gated FcaR expression in the glomeruli and cir- culating phagocytes (polymorphonuclear leuko- cytes [pMNLs] and monocytes/macrophages) from patients with IgAN and proliferative glo- merulonephritis (PGN) as well as healthy con- trols, and the clinicopathologic significance of such receptor expression in IgAN was examined
From the Division of Nephrology und Metabolism, Depart- ment of Internal Medicine, Tokai University School of Medi- cine, Isehara, Kanagawa, Japan.
Received May 21, 1996; accepted in revised form April 21, 1997.
Supported by grants from the Ministry of Health and Wel- fare, Ministry of Education, Science and Culture of Japan and u Tokai University research grant.
Address reprint requests to Masayuki Endoh, MD, Division of Nephrology and Metabolism, Tokui University School of Medicine, Isehara 259-11, Japan.
0 1997 by the National Kidney Foundation, Inc. 0272~6386/97/3003-001 I $3.00/O
American Journal of Kidney Diseases, Vol 30, No 3 (September), 1997: pp 389-396 389

390 KASHEM ET AL
by evaluating different clinical and histologic pa- rameters.
MATERIALS AND METHODS
Subjects
This study protocol was approved by the Ethics Committee of Tokai University and individual informed consent was obtained. Open renal biopsy tissue specimens from 33 pa- tients were enrolled in this study after exclusion of specimens of systemic diseases, such as systemic lupus erythematosus, liver cirrhosis, and diabetes mellitus. None of the patients was on prednisolone or immunosuppressive drugs at the time of renal biopsy. The part of the renal tissue remaining after routine diagnostic study (light, immunofluorescence, and electron microscopy) was used in the study. Twenty patients had IgAN (16 males and four females) and 13 patients had PGN (nine males and four females) as diagnosed histologi- cally. The advantages and detailed procedures of open renal biopsy have been reported elsewhere.7 Normal renal tissue specimens were obtained from five different kidneys nephrec- tomized for renal carcinoma. The clinical status of the patients was evaluated by proteinuria, hematuria, blood urea nitrogen (BUN), serum creatinine, and glomerular filtration rate (Ccr; creatinine clearance) at the time of biopsy. Severity of renal tissue damage was evaluated by semiquantitative analysis of light microscopic glomerular changes (mesangial prolifera- tion, mononuclear/polymorphonuclear infiltration, mesangial sclerosis, and crescent formation/adhesion to the capsule), tubulointerstitial changes (tubular atrophy, mononuclear/ polymorphonuclear infiltration, and interstitial fibrosis), and vascular changes. All specimens were independently interpre- ted without knowledge of clinical and experimental informa- tion. The degree of tissue lesions was graded on a scale of minus (-) for almost normal tissue, + for mild (changes affecting <20%), ++ for moderate (changes affecting <40%), and +++ for severe (changes affecting >40% of the samples) lesions.
Glomeruli Isolation
Glomeruli were isolated from fresh renal tissues immedi- ately after biopsy applying the microdissection method as previously described8 with a slight modification. The micro- dissection solution (solution I) was a Hepes-buffer solution of the following concentrations: 135 mmol NaCl, 5 mmol KCl, 1 mm01 NaZHP04 (7H,O), 12 mmol MgS04 (7H20), 2 mm01 CaC12, 1.2 mmol Na2S04, 55 mm01 glucose, and 5 mmol Hepes added after pH adjustment to 7.4 by NaOH. Solution II was of the same composition as microdissection solution I, except that it contained 5% vanadyl ribonucleoside complex (VRC; Life Technologies, Grand Island, NY). cDNA was prepared from equal numbers of isolated glomer- uli and studied by the polymerase chain reaction (PCR) method.
Cell Separation Heparinized peripheral venous blood from IgAN patients
(n = 16), PGN patients (n = 14), and healthy controls (n =
16) was used as a source of cells. To reduce nonspecific activation of neutrophils, a one-step separation procedure was used. Blood was centrifuged on Polymorphprep (Accurate Chemical and Scientific Corp, Westbury, NY). The plasma and peripheral blood mononuclear cell layers were carefully removed, the lower neutrophil layer was collected, and eryth- rocyte contamination was removed by hypotonic shock. The cells were washed twice with ice-cold RPM1 solution (GIBCOiBRL, Gaithersburg, MD), and the final cell prepara- tion consisted of 98% neutrophils as assessed by a morpho- logic study using the cytospin method (Diff-quick stain; Green Cross Co, Osaka, Japan). Monocyte isolation was per- formed as previously described.’ Briefly, peripheral blood mononuclear cells were isolated by Ficoll-Hypaque (Phar- macia, Piscataway, NJ) density gradient centrifugation and applied to gelatin-coated culture flasks for 1 hour of incuba- tion at 37°C with 5% CO*. After removal of the nonadherent cells by suction, flasks were washed gently several times with DME medium prewarmed at 37°C. A mixture of 10 mmol/ L ethylenediaminetetraacetic acid (EDTA) in calcium, mag- nesium-free phosphate-buffered saline (PBS) with DME 20% horse serum (Gibco Laboratories, Chagrin Falls, OH) was added and the adherent cells were isolated after another 15- minute incubation period. Cell surface phenotype was as- sessed using monoclonal antibody anti-human CD14 (Bec- ton-Dickinson, Mountain View, CA). More than 90% of the cells reacted with monoclonal antibody. The cells were kept on ice until flow cytometric analysis.
Flow Cytometry Flow cytometric analysis was performed using a FACScan
analyzer (Becton-Dickinson) by forward light scattering pro- file and side light scattering profile. Five hundred thousand cells were stained with monoclonal antibody My-43, a spe- cific antibody for FccvR that was a gift from Dr Li Shen (Department of Microbiology, Dartmouth Medical School, Hanover, NH).” After 30 minutes on ice, cells were washed with 1% bovine serum albumin (BSA) in phosphate-buffered saline and stained with FITC-labeled goat anti-mouse Ig for another 30 minutes on ice. Mouse control Ig was used in the staining procedure as a negative control to determine the background binding of mouse Ig.
Reverse Transcription-Polymerase Chain Reaction (RT-PCR) Protocol
Total RNA was prepared from neutrophils, monocytes, and whole renal tissues using Isogen (Wake Chemical Co, Osaka, Japan) based on a guanidinium-phenol-chloroform extraction method.” RNA (3 wg) was reverse transcribed with an Oligo (dT)18 primer in 50 mmol Tris-HCI (pH 8.3), 75 mmol KCI, 3 mmol MgC12. and 0.5 mmol dNTP mixture using 40 U of Moloney murine leukemia virus (M-MLV) reverse tran- scriptase in the presence of 20 U of recombinant RNase inhibitor (Clontech Laboratories, Inc, Palo Alto, CA). Ampli- fication of each PCR was performed in a final volume of 25 PL of 10 mmol/L Tris-HCl (pH 8.3), 50 mmol/L KCI, 1.55 mmol/L MgCl,, and 0.2 mmol/L. of all four dNTPs containing 1 PL of each primer and 1 PL of templates with 2 U of AmpliTaq DNA Polymerase (Perkin-Elmer Cetus, Norwalk,

F&R IN IGA NEPHROPATHY 391
Table 1. Primers Used for PCR
Transcript Primer
GAPDH, 5’ GAPDH, 3’ FccuR, 5’ FcaR, 3’ TNF-a, 5’ TNF-a, 3’ IL-I/3, 5’ IL-I@, 3’ IL-6, 5’ IL-6, 3’
Predicted Size (base pairs)
250
216
325
388
628
Sequences
5’-GCG ACG AAG GCC GTG TGC GTG-3’ 5’-CGC TGC 7-K CGG CAC ACG CAC-3’ 5’-AGA GGA TTC AGG CAC AGG AAG-3’ 5’-GGT CAA TGA CGA ACT CAG GAT-3’ 5’-CAG AGG GAA GAG l-K CCC AG-3’ 5’-CCT TGG TCT GGT AGG AGA CG-3’ 5’-GTG AGT AGG AGA GGT GAG AGA GGC-3’ 5’-CTT GGT GAT GTC TGG TCC ATA TGA-3’ 5’-AAA AGA TGG ATG CTT CCA ATC TGG-3’ 5’-TGC TGA ATT -ITT TAA AAT GCC ATT-3’
CT). Based on the genomic sequences previously reported, oligonucleotide primers were designed using computer soft- ware (Oligo; National Biosciences, Inc, Plymouth, MN) as shown in Table 1, and synthesized products were obtained from Takara Biomedicals (Shiga, Japan). The PCR amplifi- cation reactions consisted of 1 minute denaturing at 94°C 1 minute annealing at 62°C and 1.5 minute extension at 72°C. In a preliminary experiment, 30 and 35 PCR cycles were shown to be best for optimal fluorescence of glyceraldehyde- 3-phosphate dehydrogenase (GAPDH), tumor necrosis fac- tor-a (TNF-cr). interleukin-lp (IL-l&, IL-6, and FccuR genes. Ten microliters of each PCR product was analyzed by electro- phoresis on 2% agarose gel (Takara Biomedicals) containing ethidium bromide (0.5 wL/mL) in Tris-acetate-EDTA buffer (pH 8.0). The gel was then photographed with Polaroid 667 film (Polaroid Co, Cambridge, MA), and the developed film was scanned on a flat-bed scanner (ScanJet IIcx; Hewlett Packard, Palo Alto, CA). The optical density of the gel image produced by the scanner was semiquantitated by a densito- metric method using NIH Image 1.54; a computer program for image analysis. The optical density of the target gene n&NA bands was compared with those of the housekeeping gene. Data are expressed as the mean (+SEM) fold increase in the iNOS/GAPDH or COX-2/GAPDH ratio compared with the ratio of mRNA expression in unstimulated cells per- formed under identical PCR conditions.
Sequence Analysis
The PCR amplified FcoR fragments from glomeruli, and circulating phagocytes were purified from agarose gel. Se- quencing was performed by direct cycle sequencing on an ABI 3738 automated sequencer (Applied Biosystems Inc, a division of Perkin-Elmer Cetus) using the Dye Terminator cycle sequencing kit (Perkin-Elmer Cetus).
Statistics
Analysis of variance (ANOVA) for the P values among different groups and Fisher’s test for the P values between two groups were used for statistical analysis. All data are expressed as the mean value i SD.
RESULTS
FcolR mRNA Expression in Glomeruli Figure 1 shows a representative PCR band for
GAPDH, FccrR, TNF-CY, IL-lp, and IL-6. The
GAPDH -
FcaR -
TNF-a -
IL-q3 -
IL-6 -
Fig 1. Representative expression of GAPDH, Fc(YR, TNFw, IL-lp, and IL-6 mRNA in the glomeruli detected by RT-PCR assay. Glomerular PCR products were ob- tained from healthy controls (lane l), IgAN patients (lane 2), and PGN patients (lane 3).
392
intensity of the amplified housekeeping gene GAPDH was almost uniform in all control and patient samples, confirming that the efficiency of reverse transcription did not vary significantly between samples. The target gene FccuR (size 216 base pairs) appeared in eight of 20 glomeruli samples from IgAN (40%). There was no detect- able mRNA for FccuR in the glomeruli samples from PGN patients and healthy controls. The FccuR-positive samples were also strongly posi- tive for TNF-a, IL-lfl, and IL-6 messages, al- though certain inconsistent PCR bands for TNF- (Y, IL-lo, and IL-6 were also observed in some FccrR-negative samples. Under identical condi- tions, we also verified FccwR expression in the samples from whole renal tissues (10 IgAN pa- tients, 10 PGN patients, and five healthy con- trols). No detectable FCCXR mRNA was observed in either sample, and GAPDH expression was almost uniform in all samples (data not shown).
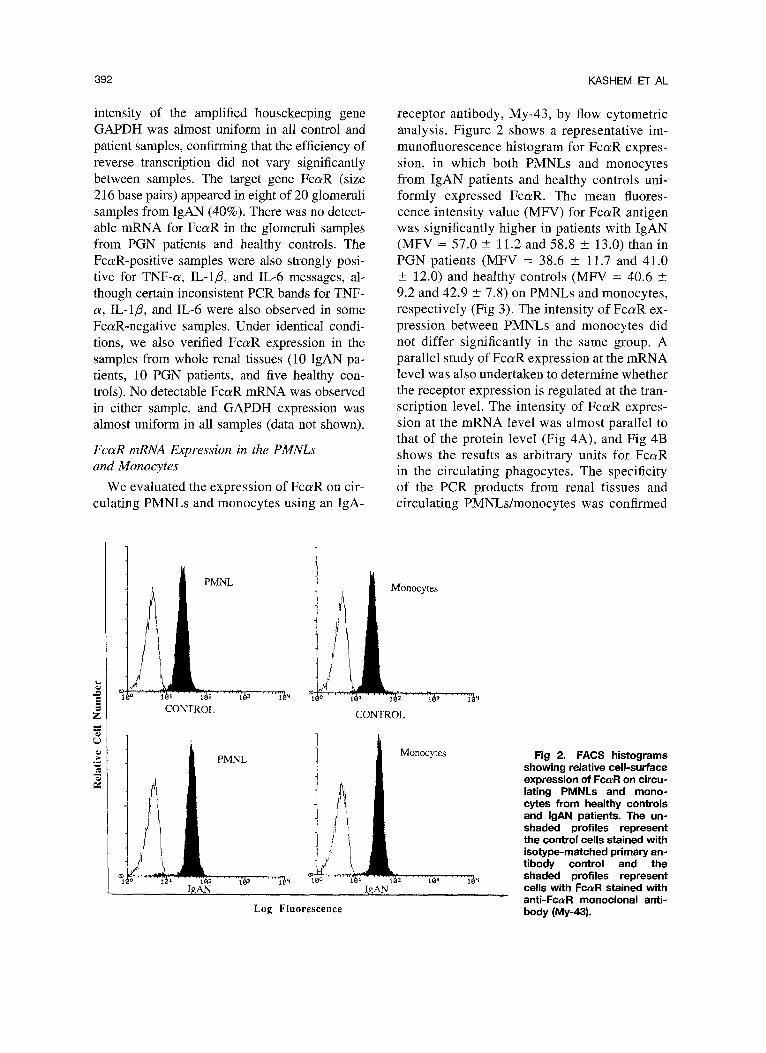
FcaR mRNA Expression in the PMNLs and Monocytes
We evaluated the expression of FccuR on cir- culating PMNLs and monocytes using an IgA-
PMNL
I 1 2 1 3
CONTROL
KASHEM ET AL
receptor antibody, My-43, by flow cytometric analysis. Figure 2 shows a representative im- munofluorescence histogram for FccuR expres- sion, in which both PMNLs and monocytes from IgAN patients and healthy controls uni- formly expressed FcaR. The mean fluores- cence intensity value (MFV) for FccuR antigen was significantly higher in patients with IgAN (MFV = 57.0 & 11.2 and 58.8 ? 13.0) than in PGN patients (MFV = 38.6 -t 11.7 and 41.0 ? 12.0) and healthy controls (MFV = 40.6 ? 9.2 and 42.9 t 7.8) on PMNLs and monocytes, respectively (Fig 3). The intensity of FcaR ex- pression between PMNLs and monocytes did not differ significantly in the same group. A parallel study of FccvR expression at the mRNA level was also undertaken to determine whether the receptor expression is regulated at the tran- scription level. The intensity of FcaR expres- sion at the mRNA level was almost parallel to that of the protein level (Fig 4A), and Fig 4B shows the results as arbitrary units for FccwR in the circulating phagocytes. The specificity of the PCR products from renal tissues and circulating PMNLsJmonocytes was confirmed
Monocytes
Monocytes Fig 2. FACS histograms showing relative cell-surface expression of FclvR on circu- lating PMNLs and mono- cytes from healthy controls and IgAN patients. The un- shaded profiles represent the control cells stained with isotype-matched primary an- tibody control and the
Ini;; ’ 3 lY “1 0 LA- 1 ’ 1 2 shaded profiles represent
IgAN cells with FccuR stained with anti-FccuR monoclonal anti-
Log Fluorescence body (My-43).

F&R IN IGA NEPHROPATHY
by partial sequence analysis of amplified FCCVR cDNA, which displayed complete homology to the nucleotide sequence of human cell line U937 (data not shown).
Analysis of FcaR mRNA Expression With the Clinical and Histologic Data
To determine the relevance of FccrR expres- sion in the glomeruli in renal pathophysiology, clinical and histologic data of all patients at the time of renal biopsy were examined. The speci- mens that expressed detectable FccrR mRNA were considered the FccuR-positive group. Hema- turia, as assessed by two semiquantitative meth- ods (red blood cell count per high-power field and the dipstick test), was significantly more se- vere in IgAN patients with glomerular FCCXR ex- pression (Fig 5). Serum IgA levels were signifi- cantly higher in the patients with glomerular FccuR expression than in those without such an expression (Fig 6). Proteinuria, BUN, serum cre- atinine, and GFR values did not show statistical significance when compared between the positive
MFV 100 I
0 PMNL 0 Monocytes
90 * P<O.Ol
I 8 o-
7 o-
0
0
:
.T
O i 1 11
0 Q ’ 8 :
2 OJ CONTROL IgAN Pt. PGN Pt.
N=16 N=i6 N=14
Fig 3. Amount of FCCYR expression on PMNLs and monocytes in healthy controls and IgAN and PGN pa- tients. Horizontal bars indicate the mean value k SD.
A
393
0 ‘3
c2
. 5
25
_ 1
12 3 f%aiR Expression
Fig 4. (A) Analysis of FcrvR mRNA in the circulating PMNLs and monocytes from controls (lane 1) and from IgAN (lane 2) and PGN (lane 3) patients. Data show one of three representative experiments. (B) Repre- sentative data of the densitometric analysis of FcaR expression. The calculated FcoR to GAPDH ratio was used to plot the graph.
and negative groups (data not shown). FcaR ap- pearance was observed in the tissues in accor- dance with advanced damage (Fig 7) and with increased number of crescents, mostly cellular in type (five of eight patients had crescents). Three of nine (33%) and five of seven (71%) specimens with moderate and severe tissue damage, respec- tively, were positive for the FcaR mRNA signal. Other glomerular changes, such as mesangial expansion, hypercellularity, and sclerosis, did not show any particular correlation to the receptor expression (data not shown).
Immunohistochemical Study
We tried to localize the distribution of FcaR in the renal tissues since its localization is of

394 KASHEM ET AL
A l-4 5-9 lo-29 >30
Fc aR +ve 0000 oooc
Fc aR -ve o&y 000 000 0
B
Fc aR +ve
Fc aR -ve 00
P<O.Ol
+ ++ +++
000 w
0000 088 0
P<O.Ol
Fig 5. A comparison between FccuR-positive and - negative IgAN patients with respect to the severity of hematuria assessed by (A) red blood cell count per high-power field and (B) the dipstick test (semiquanti- tative values).
critical importance in understanding its patho- physiologic role in IgAN. By applying mono- clonal anti-FccuR antibody (My-43), we exam- ined the renal tissues from patients with IgAN and PGN as well as healthy controls. We were unable to show any clearcut staining for the anti- body used either with immunofluorescence or the immunoperoxidase method, whereas staining for IgA was clearly observed in tissues from IgAN patients by the same staining procedure (data not shown). In the patient groups, there was a sig- nificant increase of monocyte/macrophage infil- tration in the tubulointerstitial areas. No such in- filtration was observed in the glomerular regions. There was no significant PMNL infiltration in either the interstitial or glomerular region in the tissues studied (data not shown).
DISCUSSION
Although the role of IgA and IgA-ICs in the pathogenesis of IgAN has been well documented,
9 0 o-
8 0 0.
7 0 0.
$ a 5 60~
z 2 soo- n E 2
d 400.
3 0 0.
0 0 i 0
0 2 o OJ
IgA-R (+ve) ISA-R (-ve)
Fig 6. Comparison of serum IgA levels between the FccuR-positive and -negative IgAN patients. The mean IgA level is 510 i 131 mg/dL and 336 ? 66 mg/dL in the FccuR-positive and -negative group, respectively.
the role of the Fc receptor for IgA in the develop- ment of IgAN remains uncertain. In this study, we observed the expression of FcaR at its mRNA level in the glomeruli of 40% of IgAN patients and a proportionate increase of FccvR in the circu- lating phagocytes, suggesting that there is induc- tion of FcaR in human IgA glomerulonephritis. The enhancement of Fca!R expression in the cir- culating cells was preceded by an increase in the level of FccuR-specific mRNA. This implies that the increase in FcaR levels resulted from translo-
Fc aR -ve l ee l eo 000 Egg 00
Fig 7. A comparison of renal tissue damage in IgAN patients and control tissues in the FccuR-positive and -negative groups. - = no lesion, + = mild lesion, ++ = moderate lesion, and +++ = severe lesion. 0 = normal; 0 = IgAN patient. P < 0.02.

F&R IN IGA NEPHROPATHY 395
cation of a greater amount of mRNA, which could be the result of higher gene transcription or a delay in message breakdown. Although human FcaR from glomeruli has not yet been cloned, our partial sequencing data suggest that the de- duced sequencing of FccrR product from glomer- uli is almost identical to that of human myeloid cell line U937.‘* However, the mechanism(s) by which FCCKR expression is modulated in vivo and then involved in the process of tissue damage has not been explained in this study.
Our results suggest that there is some selective in vivo induction of Fc~LR expression in the glo- meruli from IgAN patients by some inflamma- tory mediators since the majority of IgAN pa- tients (60%) with definitive mesangial IgA deposition and some with higher serum IgA lev- els, as well as some PGN patients with positive cytokine messages (TNF-a, IL-l@, and IL-6), did not show any detectable FcaR expression in their glomeruli. This might be due to the complex array of in vivo inflammatory milieu, prevailing during the disease process, and an appropriate stimulus from a combination of IgA and in- flammatory cytokines might be mandatory to modulate FccuR expression. Previous experimen- tal studies showed the involvement of IL-l and/ or IL-6 in the histologic severity of IgAN induced by passive administration of IgA-ICs.13 Recent data14’15 showed that glomerular cells themselves are capable of producing some cytokines, such as IL-l, IL-6, and TNF-a, during the disease process. Therefore, it is likely that FcczR expres- sion in the glomeruli is a result of some syner- gistic effects of IgA-ICs and inflammatory cyto- kines of glomerular origin, in which a balance of the stimuli as well as the level of each stimulus is important.
Hematuria is one of the prominent clinical fea- tures of IgAN, and the majority of patients show macroscopic/microscopic hematuria in either the persistent or transient form with significant pro- teinuria. Although some studies’6,‘7 reported that hematuria has no relationship with the severity of the disease, Bennett and Kincaid-Smith18 showed an association between episodes of he- maturia and lowered renal function in adult pa- tients with IgAN. Previously, a greater number of urine abnormalities with increased serum TNF-a and interferon-y levels” and a correlation be-
tween IgA-IC level and hematuria3 were ob- served in IgAN patients. Thus, qualitative esti- mates of hematuria in relation to renal function may be misleading, possibly resulting in dif- fering interpretations regarding the severity of hematuria and the importance of any associated proteinuria as predictors of a poorer prognosis. Our results suggested that the cytokines likely to be associated with hematuria are synergistic with IgA-ICs in the induction of glomeruli FccuR ex- pression in IgAN.
The functional importance of glomerular FccrR appearance in human IgAN is of some interest. We previously showed upregulation of FcaR on circulating phagocytes from IgAN patients.” Other reports showed that interaction of aggre- gated IgA with FcolR stimulates a range of func- tions, such as phagocytosis,” release of leuko- trienes (C4 and B4) and prostaglandin E2,” release of superoxide, chemiluminescence,23~z4 and antibody-dependent cellular cytotoxicity? Our findings suggest that FccuR expression in re- nal tissues and their relative increase in circulat- ing cells may be related to the disease activity in IgAN since the receptor expression was detect- able only in patients with increased hematuria and advanced tissue damage compared with those without receptor expression.
Although some investigators speculated that FccuR is ‘responsible for binding of IgA-ICs in the glomerular regions, our findings are not in favor of this hypothesis. However, other mecha- nisms, such as size and physiochemical charac- teristics of IgA-ICs,26 and/or the existence of an additional IgA receptor unrelated to FcatR may be responsible for this binding. Recently, Mon- teiro et al’ reported that IgA-binding activity is not directly reflected in the level of FccvR expres- sion; these investigators also noted a rapid in- crease in IgA-binding capacity without altering reactivity levels with the anti-FcaR monoclonal antibody in a comparative analysis.
In our immunohistochemical study, we were unable to detect FccrR expression at the protein level in the renal tissues, even in the tissue speci- mens from IgAN patients that were positive for FcorR mRNA. To date, no reports on the stain- ability of FccrR in human renal tissues are avail- able, although flow cytometric detection of FcaR protein in the circulating cells by application of

396 KASHEM ET AL
the same monoclonal antibody (My-43) has been confirmed in our previous and present experi- ments. The cause of these inconsistent findings is obscure at present, but may be due to (1) mo- lecular heterogeneity of the FccuR molecule on different cells, which is possible because of dif- ferent glycosylated FcaR created by posttransla- tion modification, (2) in vivo tissue levels of FcaR expression not detectable by the available antibodies that are too low, and (3) protein modi- fication during the fixation procedure that led to labeling insufficient for staining of FCCJLR. How- ever, further detailed studies are mandatory to resolve this vital issue, and we are now working on this field.
In conclusion, our findings of glomerular FccuR expression and their correlation with he- maturia and tissue damage might be important in the pathogenesis of glomerular injury in IgAN. However, the data must be interpreted with cau- tion, since hematurialtissue damage were also ev- idenced in some patients in the absence of detect- able FcaR expression.
REFERENCES
1. Berger J, Hinglais N: Les depots intercapillaries d’IgA- IgG. J Urol 74:694-695, 1988
2. Lesavre PH, Digeon M, Bach JF: Analysis of circulating IgA and detection of immune complexes in primary IgA nephropathy. Clin Exp Immunol 48:61-69, 1982
3. Coppo R, Basolo B, Martina G, Rollino C, Marchi M, Giachino F, Mazzucco G, Messina M, Picoli G: IgA nephrop- athy and Schonlein-Henoch nephritis: Correlation with clini- cal and histological signs of activity. Clin Nephrol 18:230- 239, 1982
4. Keer MA: The structure and function of human IgA. Biochem J 271:285-296, 1990
5. Monteiro RC, Kubagawa H, Cooper MD: Cellular dis- tribution, regulation, and biochemical nature of an Fca recep- tor in humans. J Exp Med 171597-613, 1990
6. Gomez-Guerrero C, Gonzalez E, Egido J: Evidence for a specific IgA receptor in rat and human mesangial cells. J Immunol 151:7172-7181, 1993
7. Nomoto Y, Tomino Y, Endoh M, Suga T, Miura M, Nomoto H, Sakai H: Modified open renal biopsy: Results in 934 patients. Nephron 45:224-228, 1987
8. Owada A, Tomita K, Terada Y, Sakamoto H, Nono- guchi H, Marumo F: Endothelin (ET)-3 stimulates cyclic gua- nosine 3’, 5’-monophosphate production via ETB receptor by producing nitric oxide in isolated rat glomerulus, and in cultured mesangial cells. J Clin Invest 93556-563, 1994
9. Hassan NF, Campbell DE, Douglas SD: Purification of human monocytes on gelatin-coated surfaces. J Immunol Methods 95:273-276, 1986
10. Shen L: A monoclonal antibody specific for immuno- globulin A receptor triggers polymotphonuclear neutrophil superoxide release. J Leukoc Biol 51:373-378, 1992
11. Chomczynski P, Sacchi N: Single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chlo- roform extraction. Anal Biochem 162:156-159, 1987
12. Maliszewski CR, March CJ, Schoenborn MA, Gimpel S, Shen L: Expression and cloning of a human Fc receptor for IgA. J Exp Med 172:1665-1672, 1990
13. Montinaro V, Hevey K, Aventaggiato L, Fadden K, Esparaza A, Chen A, Finbloom DS, Rifai A: Extrarenal cyto- kines modulate the glomemlar response to IgA immune com- plexes. Kidney Int 42:341-353, 1992
14. Fukatsu A, Matsuo S, Tamai H, Sakamoto N, Matsuda T, Hirano T: Distribution of interleukin-6 in normal and dis- ease human kidney. Lab Invest 6561-66, 1991
15. Yoshioka K, Takemura T, Murakami K, Okada M, Yagi K, Miyazato H, Matsushima K, Maki S: In situ expression of cytokines in IgA nephritis. Kidney Int 44:825-833, 1993
16. Van der Peet J, Arisz L, Brebtjens JRH, Marrink J, Hoedemaeker PJ: The clinical course of IgA nephropathy in adults. Clin Nephrol 8:335-340, 1977
17. Kobayashi Y, Tateno S, Hiki Y, Shigematsu H: IgA nephropathy: Prognostic significance of proteinuria and histo- logical alterations. Nephron 34:146-153, 1983
18. Bennett WM, Kincaid-Smith P: Macroscopic hematu- ria in mesangial IgA nephropathy: Correlation with glomeru- lar crescents and renal dysfunction. Kidney Int 23:393-400, 1983
19. Inaba S, Takahashi T, Ishihara S, Kurose K, Arai M, Sakai Y, Yamamoto S, Matsukura H, Okada T: Serum tumor necrosis factor in mesangial IgA glomemlonephritis with macroscopic hematuria in children. Nephron 72:5 18-522, 1996
20. Kashem A, Endoh M, Nomoto Y, Sakai H, Nakazawa H: FccuR expression on polymorphonuclear leukocytes and superoxide generation in IgA nephropathy. Kidney Int 45868-875, 1994
21. Gorter A, Hiemstra PS, Leijh PCJ, van der Sluys ME, va den Barselaar MT, Van Es LA, Daha MR: IgA and secre- tory IgA-opsonized S. aureus induce a respiratory burst and phagocytosis by polymorphonuclear leukocytes. Immunology 61:303-309, 1987
22. Ferreri NR, Howland WC, Spiegelberg HL: Release of leukotrienes C4 and B4 and prostaglandin E2 from human monocytes stimulated with aggregated IgG, IgA, and IgE. J Immunol 136:4188-4193, 1986
23. Stewart WW, Kerr MA: The specificity of the human IgA receptor (FccuR) determined by measurement of chemilu- minescence induced by serum or secretory IgAl or IgA2. Immunology 71:328-334, 1990
24. Shen L, Collins J: Monocyte superoxide secretion trig- gered by human IgA. Immunology 68:491-496, 1989
25. Fanger MW, Goldstine SN, Shen L: The properties and role of receptors for IgA on human leukocytes. Ann N Y Acad Sci 409:552-563, 1983
26. Monteiro RC, Halbwachs-Mecarelli L, Roque-Barreira MC, Noel LH, Berger J, Lesavre P: Charge and size of mesan gial IgA in IgA nephropathy. Kidney Int 28:666-675, 1985