chinese herbs nephropathy: a clue to balkan endemic nephropathy?
TRANSCRIPT

Kidney International, Vol. 45 (1994), pp. 1680—1688
Chinese herbs nephropathy: A clue to Balkan endemicnephropathy?
JEAN-PIERRE COSYNS, MICHEL JADOUL, JEAN-PAUL SQUIFFLET, JEAN-FRANç0Is DE PLAEN,DUSAN FERLUGA, and CHARLES VAN YPERSELE DE STRIHOU
Departments of Pathology, Nephrology and Renal Transplantation, University of Louvain Medical School, Brussels, Belgium, and Institute ofPathology, Medical Faculty, University of Ljubljana, Ljubljana, Slovenia
Chinese herbs nephropathy: A clue to Balkan endemic nephropathy?Rapidly progressive interstitial renal fibrosis has recently been reportedin young women who have been on a slimming regimen includingChinese herbs. We examined four nephroureterectomies performed inthree patients prior to or at the time of transplantation to determine thenature and topography of the kidney and urinary tract lesions inChinese herbs nephropathy (CHN). Extensive, hypocellular, interstitialsclerosis, tubular atrophy and global sclerosis of glomeruli decreasingfrom the outer to the inner cortex, including the columns of Bertin,were observed in the four kidney specimens, together with severefibromucoid to fibrous intimal thickening, mainly of interlobular arter-ies, normal or collapsed residual glomeruli, and mild to moderate atypiaand atypical hyperplasia of the urothelium. In addition, bilateral pelvi-ureteric sclerosis was observed in one case. With the exception of thelatter, these lesions are very similar to those described in Balkanendemic nephropathy (BEN). The clinical presentation of the patientswas also similar to that observed in BEN: normal blood pressure,aseptic leukocyturia, low grade low molecular weight proteinuria, earlyand severe anemia. In conclusion, on morphological and clinicalgrounds, CHN appears similar to BEN. A common etiologic agent,aristolochic acid, is suspected. The known carcinogenic potential of thiscompound, taken together with our finding of multiple foci of cellularatypia of the urothelium suggest that CHN patients should undergo aregular follow-up for urothelial malignancy.
Rapidly progressive interstitial renal fibrosis has been re-cently reported in young women who have been on a slimmingregimen including Chinese herbs [1]. Available pathologicaldata are limited by the small size of renal cortical biopsies. Wereport a detailed pathological description of four nephroure-terectomy specimens obtained in three patients suffering fromChinese herbs nephropathy (CHN). Our observations confirmthe earlier findings of cortical fibrosis without primary glomer-ular abnormalities and demonstrate that this pattern is homo-geneous, follows a marked corticomedullary gradient, withrelative sparing of the medulla. They furthermore demonstratethe topography of significant vascular lesions involving mainlythe interlobular arteries, the presence of atypia and metaplasiaof the urothelium, and, in one case, a severe pelviureteralfibrosis. These findings are compared with those reported in the
Received for publication October 14, 1993and in revised form January 3, 1994Accepted for publication January 3, 1994
© 1994 by the International Society of Nephrology
Balkan endemic nephropathy (BEN). The similarity of themorphological and clinical pattern raises the possibility of acommon etiologic toxic agent, aristolochic acid.
Methods
Four nephroureterectomies were performed as part of thepretranspiantation program or at the time of transplantation inthree women with severe renal failure due to the ingestion ofslimming pills containing Chinese herbs [1]. A renal biopsy wasalso available in one patient.
Biopsy and kidney samples were fixed in Duboscq-Brasil andembedded according to the usual procedures for light micros-copy. Three micron thick sections were stained by hematoxylineosin, Masson's trichrome, periodic acid Schiff, periodic acidsilver methenamine, phosphotungstic acid hematoxylin andWeigert's elastic van Gieson.
A semiquantitative analysis was done according to Pirani,Pollak and Schwartz [2]. Glomerular pathology was evaluatedfor cellularity, thickening and double contour appearance ofglomerular basement membrane (GBM), hyalinosis, segmentaland global sclerosis. Tubular pathology was graded accordingto the degree of atrophy and regeneration. The grading ofcortical interstitial damage was based on an estimation of theseverity and extent of fibrosis/sclerosis, and on an evaluation ofthe distribution, severity and type of the interstitial inflamma-tory cell infiltrate. Arteriolar and arterial changes were evalu-ated: distribution and extent of hyaline and fibrinoid deposits(hyalinosis), increased amount of basement membrane materialaccompanied by thickening of vessel wall layers (sclerosis),mucinofibrous and elastofibrous intimal thickening.
Kidney samples were quick-frozen in liquid nitrogen and 3m thick cryostat sections were incubated with phosphatebuffered saline pH 7.2 for 20 minutes at room temperature andoverlaid with fluorescein isothiocyanate conjugated anti-IgG,anti-IgA, anti-IgM, anti-Clq, anti-C3, anti-fibrinogen antiserafor immunofluorescent microscopy.
For electron microscopy, fixation was made in 2.5% glutar-aldehyde buffered with 0.1 M cacodylate containing 7.5% su-crose at pH 7.4 and 4°C. The specimens were rinsed in coldbuffer, postfixed in 0.1 M cacodylate-buffered 1% 0s04 at 4°C,dehydrated in a graded series of alcohols, propylene oxide andembedded in Epon 812. Ultrathin sections were contrasted withuranyl acetate and lead citrate according to Reynolds and were
1680
Cosyns et a!: Chinese herbs nephropathy 1681
Table 1. Clinical data
Case 1 Case 2 Case 3
Age 32 28 27Sex F F FPast medical story
Creatinine pino!/!iter 53 (6/90) 97 (10/91) 75 (8/85)(date)Formula I — 12/88—6/89 5/89—5/90Formula 2 5/90—12/91 7/90—8/91 5/90—1/92
Data of presentationDate 3/92 10/91 6/92BP mm Hg 130/80 120/80 120/75Creatinine 185 101 801Hbg/d! 8.7 9.6 5.9Proteinuna g/day 0.6 0.3 0.6Urine analysis
RBC/hpf 0 10—20 2—3
WBC/hpf 8—10 5—10 5—6Glucose + — +
X-raysRight cm 11 US bilateral 8Left cm 14 hydronephrosis 9
Follow-up3 months
intervention — —bilateralureteral JJ
—3 packed red cells(4/92)
—
BP 144/80 144/94 HDCreatinine 519 202 HDHb 8.5 6.9 HD
6 monthsCreatinine TP 176 HD
LaterHD — 1/93 7/92TP 9/92 4/93 5/93Creatinine (9/93) 122 99 103
Abbreviations are:transplantation.
US, ultrasound; HD, hemodialysis; and TP,
examined in a Zeiss EM 109 electron microscope operated at 80kV.
Results
Clinical dataCase 1. This 32-year-old woman (patient 9 in [11) was referred
in March 1992 for evaluation of mild renal failure (serumcreatinine 132 prnol/liter) and glucosuria (Table 1).
Her previous medical history was unremarkable apart from arecent miscarriage (serum creatinine was 53 moIIliter in June1990). She had followed a slimming cure at a clinic identified asX Clinic [1], and for 20 months ingested pills whose composi-tion is referred to as formula 2 pills, which contained Chineseherbs [1].
Her blood pressure was 130/80 mm Hg. Laboratory dataincluded: serum creatinine 185 mol/liter; mild hyperchioremicacidosis; normochromic, normocytic, nonregenerative anemia;glucosuria without hyperglycemia; aseptic leukocyturia; andmild proteinuria. On intravenous pyelography, the kidneyswere asymmetric (right axis 11 cm, left axis 14 cm). A kidneybiopsy was performed.
The blood pressure remained normal but renal functiondeteriorated rapidly. In September 1992, the patient underwenta living-related donor kidney transplantation together with a
Table 2. Morphological findings
Pathological changes Case I Case 2 Case 3
Kidney weight gLeft — 80 45Right 50 90 —1
Cortical tubulointerstitialTubular atrophy 80—90% 80% 100%Interstitial sclerosis 80—90% 80—90% 90%Cell infiltration
Glomerular changesSclerosis
Global 20-30% 60% 70-80%Segmental 0% 1—2% 5%
Ischemic 30% 10—20% 15—20%
Hyalinosis 0% 0% 0%GBM double contour 0% 0% 0%Fetal-like glomeruli 0
Vascular changesHyalinosis + + +Sclerosis +++ +++ +++Fibroelastosis + + +Mucoid fibrosis + + + +
UrotheliumSquamous metaplasia +/+ + 0 +1+ +Dysplasia + + + + +
right nephroureterectomy. Twelve months later, serum creati-nine was normal; hemoglobin (Hb) was 11.1 g/dl.
Case 2. This 28-year-old woman (reported in [3]) had twouneventful pregnancies in 1988 and 1990. She was referred inOctober 1991, during the 12th week of her third pregnancy, forevaluation of sterile microscopic hematuria and leukocytuna ofrecent onset.
The patient had followed the slimming regimen of clinic Xand ingested the apparently harmless formula 1 preparation forseven months after her first pregnancy and the toxic formula 2pills for 13 months after her second pregnancy.
Her blood pressure was 120/80 mm Hg. Laboratory dataincluded: a normal serum creatinine, a normochromic normo-cytic nonregenerative anemia; aseptic leukocyturia and micro-scopic hematuria; and mild proteinuria. Ultrasonography dis-closed major bilateral ureterohydronephrosis extending to thepelvis.
Her blood pressure remained normal but her serum creatininerose from 101 to 176 molIliter at delivery in April 1992, whilehemoglobin fell from 9.6 to 6.9 g/dl, necessitating blood trans-fusions. Subsequently, ureterohydronephrosis did not regressand renal function further deteriorated despite the successfulinsertion of ureteral catheters. Hemodialysis was initiated inJanuary 1993, and the ureteral catheters were removed. A leftnephroureterectomy was performed in February as part of thepretransplantation program.
Two months later, she underwent a living-unrelated donorkidney transplantation together with a right nephrourecterec-tomy. Five months later, serum creatinine was normal, and Hbwas 12.9 g/dl.
Case 3. This 27-year-old woman was referred in June 1992 forevaluation of severe anemia. Her medical history included afew generalized seizures in 1985, treated with vaiproIc acidduring two years, and anorexia nervosa. Renal function wasnormal at that time. The patient attended the X clinic and took
1682 Cosyns et a!: Chinese herbs nephropathy
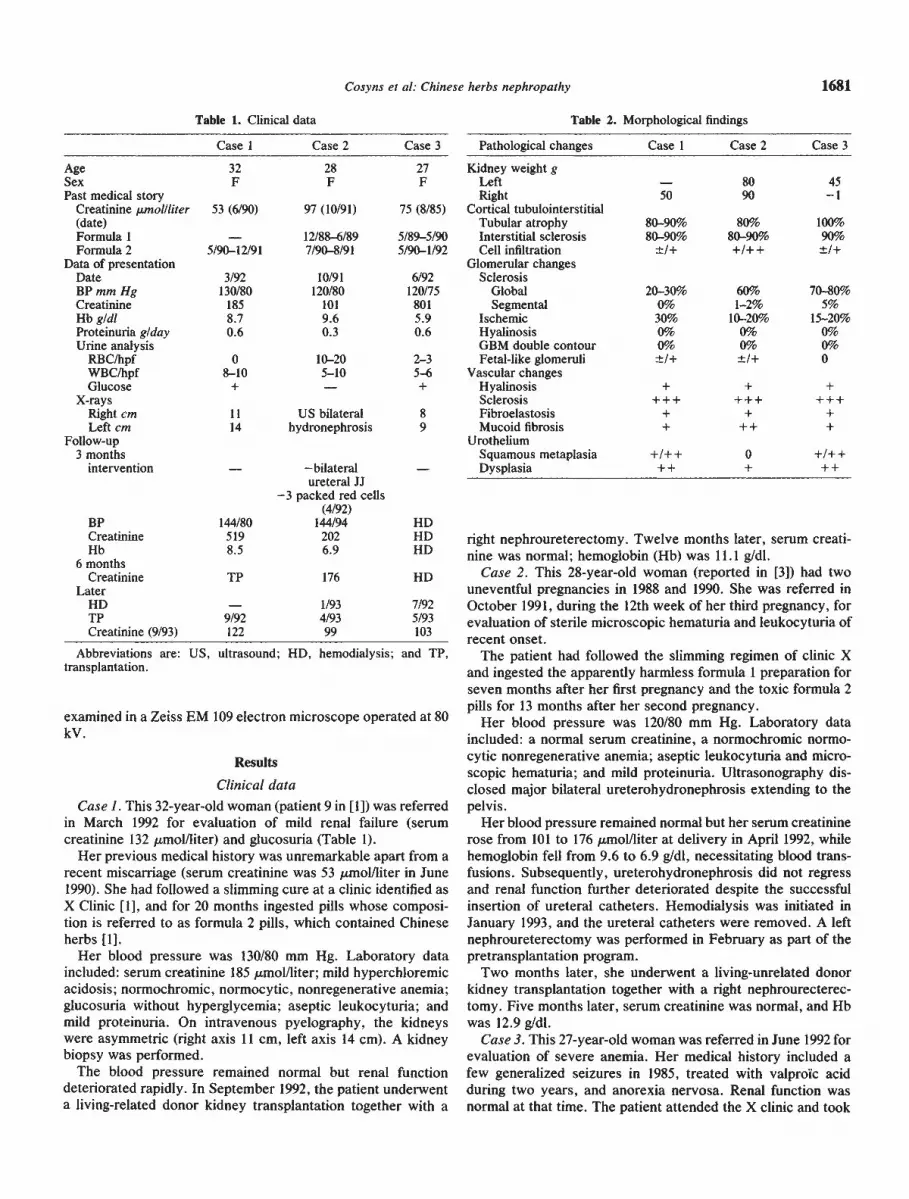
Fig. 1. Diffuse atrophy of cortex (C) including columns of Bertin (B) down to the renal sinus. Slight involvement of the pyramids (M) (case 3) (HE,x 4).
the harmless formula 1 pills for 12 months and the toxic formula2 pills for the subsequent 21 months.
Her blood pressure was 120/75 mm Hg. Laboratory dataincluded: serum creatinine 801 mol/liter; severe metabolicacidosis (serum bicarbonate 14 mmollliter); severe normochro-mic, normocytic anemia; glucosuria without hyperglycemia;mild proteinuria; and aseptic leukocyturia. The kidneys wereshrunken on tomography [longitudinal axes were 8 cm (R) and9 cm (L)]. Hemodialysis was initiated in July 1992. Severeincapacitating peripheral neuropathy developed, and proved tobe resistant to an increase of the dialysis duration from 12 to 15hours weekly. In May 1993, she underwent a cadaver kidneytransplantation together with a left nephroureterectomy. Fourmonths later serum creatinine was normal; Hb was 11.7 gldl.
Morphological findings
Morphological findings in the nephroureterectomy specimensare summarized in Table 2. No significant difference was notedbetween the kidneys of case 2 despite the three month intervalbetween the two nephrouretectomies. The findings in only onespecimen (left) are thus described.
The kidneys were markedly atrophic. Their external surfacewas smooth with some retracted areas. A longitudinal sectionrevealed a homogeneously shrunken organ with a pale brownthin rim of cortex around the pyramids, which looked darkerwith still visible medullary rays (Fig. 1). The pelvis and ureter
were unremarkable in cases 1 and 3. In case 2, they wereembedded in a 0.5 to 1 cm thick sheath of dense fibrotic tissueresulting in a mild bilateral pelvi-calyceal dilatation and shortsegments of right ureteral dilatation.
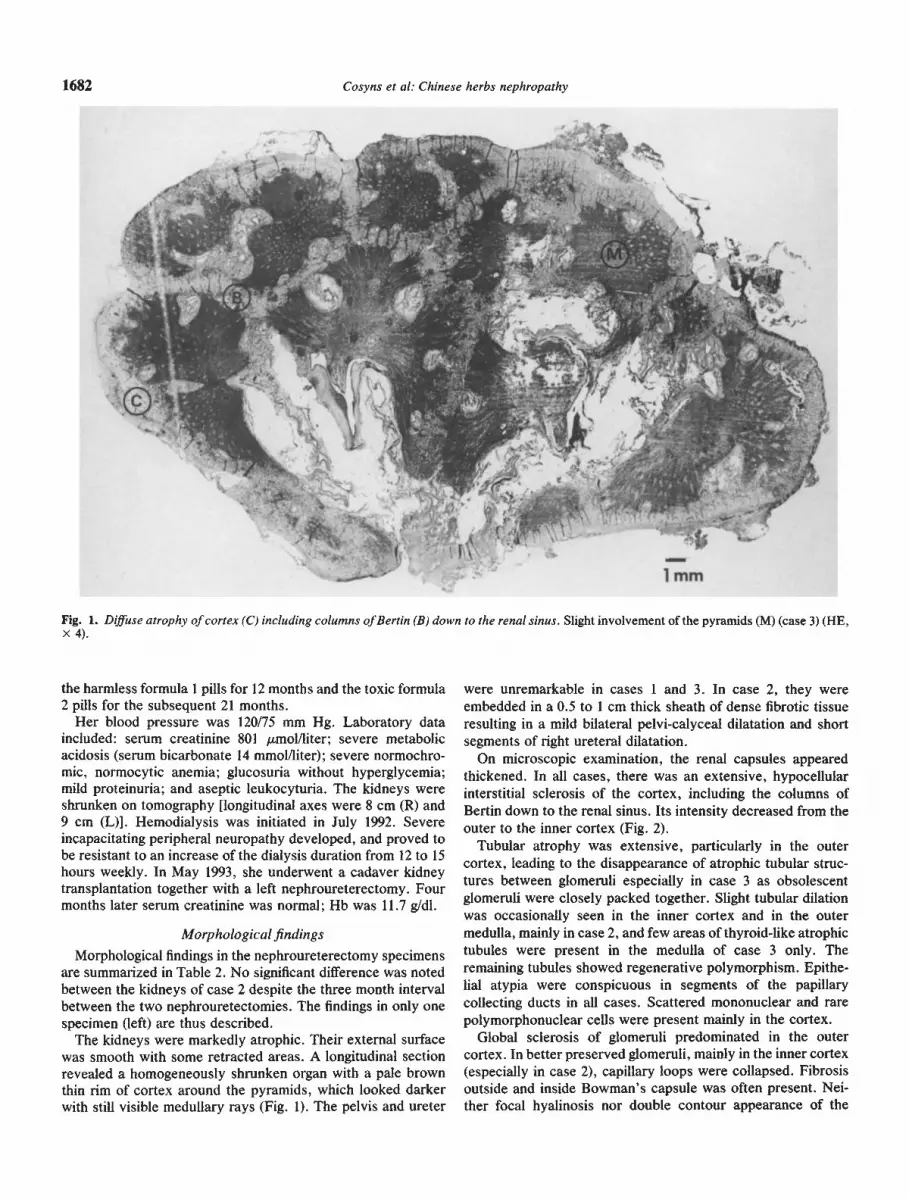
On microscopic examination, the renal capsules appearedthickened. In all cases, there was an extensive, hypocellularinterstitial sclerosis of the cortex, including the columns ofBertin down to the renal sinus. Its intensity decreased from theouter to the inner cortex (Fig. 2).
Tubular atrophy was extensive, particularly in the outercortex, leading to the disappearance of atrophic tubular struc-tures between glomeruli especially in case 3 as obsolescentglomeruli were closely packed together. Slight tubular dilationwas occasionally seen in the inner cortex and in the outermedulla, mainly in case 2, and few areas of thyroid-like atrophictubules were present in the medulla of case 3 only. Theremaining tubules showed regenerative polymorphism. Epithe-hal atypia were conspicuous in segments of the papillarycollecting ducts in all cases. Scattered mononuclear and rarepolymorphonuclear cells were present mainly in the cortex.
Global sclerosis of glomeruhi predominated in the outercortex. In better preserved glomeruli, mainly in the inner cortex(especially in case 2), capillary loops were collapsed. Fibrosisoutside and inside Bowman's capsule was often present. Nei-ther focal hyalinosis nor double contour appearance of the
I.
—
rM fl..e,— e
S
4.
14e
1mm
Cosyns et a!: Chinese herbs nephropathy 1683
Fig. 2. Extensive sclerosis decreasing fromthe outer to the inner cortex (case 2) (HE, X50).
capillary basement membrane were observed. Occasional fetal-like glomeruli were seen.
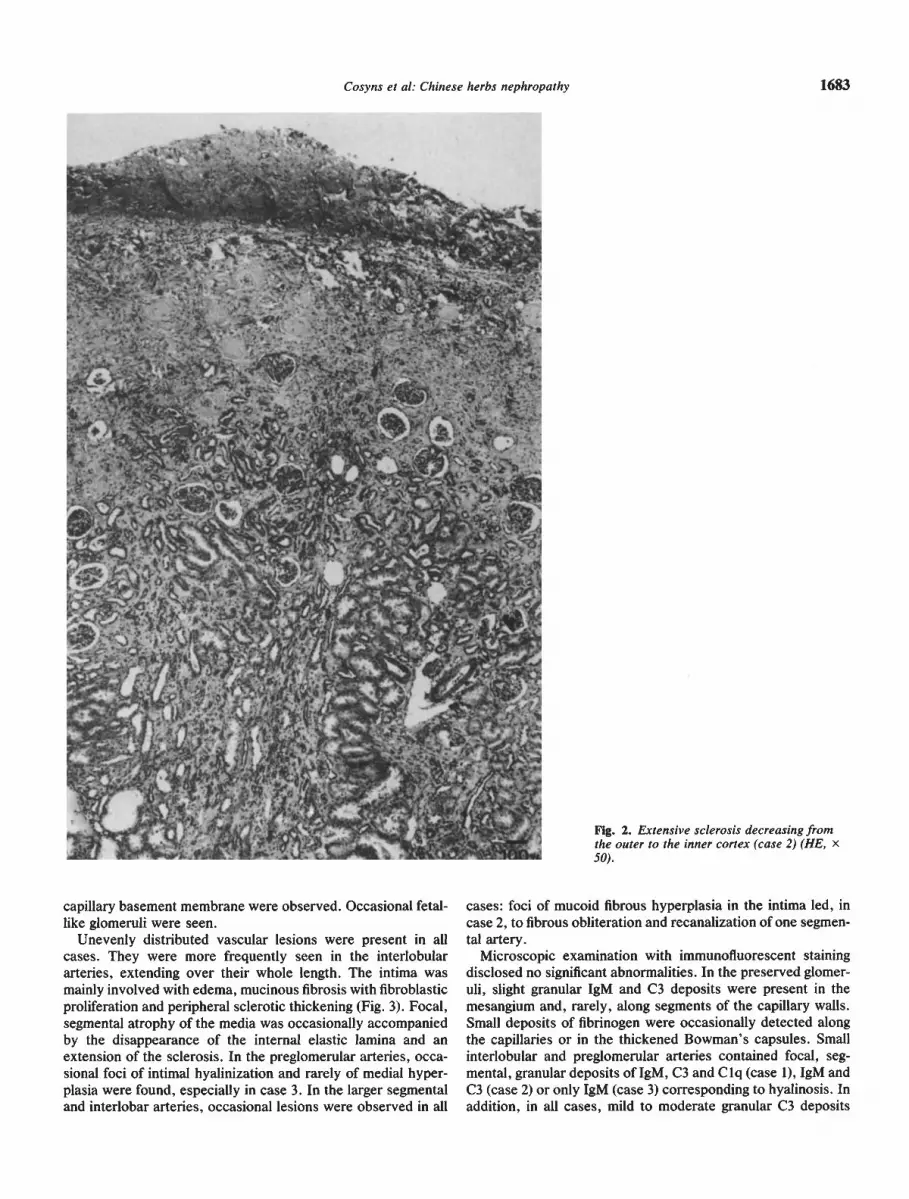
Unevenly distributed vascular lesions were present in allcases. They were more frequently seen in the interlobulararteries, extending over their whole length. The intima wasmainly involved with edema, mucinous fibrosis with fibroblasticproliferation and peripheral sclerotic thickening (Fig. 3). Focal,segmental atrophy of the media was occasionally accompaniedby the disappearance of the internal elastic lamina and anextension of the sclerosis. In the preglomerular arteries, occa-sional foci of intimal hyalinization and rarely of medial hyper-plasia were found, especially in case 3. In the larger segmentaland interlobar arteries, occasional lesions were observed in all
cases: foci of mucoid fibrous hyperplasia in the intima led, incase 2, to fibrous obliteration and recanalization of one segmen-tal artery.
Microscopic examination with immunofluorescent stainingdisclosed no significant abnormalities. In the preserved glomer-uli, slight granular 1gM and C3 deposits were present in themesangium and, rarely, along segments of the capillary walls.Small deposits of fibrinogen were occasionally detected alongthe capillaries or in the thickened Bowman's capsules. Smallinterlobular and preglomerular arteries contained focal, seg-mental, granular deposits of 1gM, C3 and C lq (case 1), 1gM andC3 (case 2) or only 1gM (case 3) corresponding to hyalinosis. Inaddition, in all cases, mild to moderate granular C3 deposits
1684 Cosyns et a!: Chinese herbs nephropathy
Fig. 3. Severe fibrous intimal thickening of interlobular artery. Acellular interstitial sclerosis with few atrophic tubules (case 2) (HE, X 280).
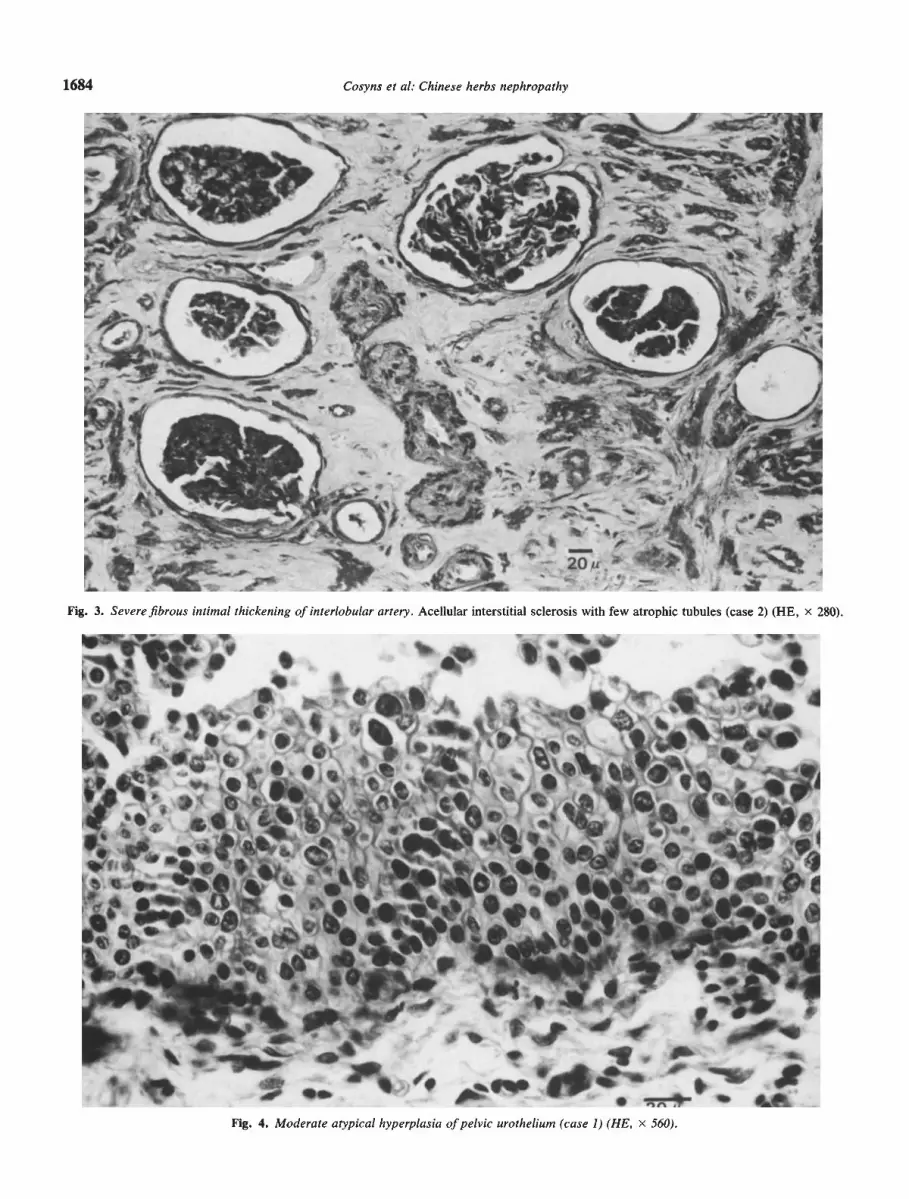
Fig. 4. Moderate atypical hyperplasia of pelvic urothelium (case 1) (HE, x 560).
V. Iis
1i,'
'.— .
.ft..J
4'
I
t , I j>.S a1i r ____ •
S 0•a[. *
I
basement membranes of atrophic tubules.On electron microscopy, most nonobsolescent glomeruli had
an ischemic appearance with diffuse collapse of capillary loops,wrinkling and thickening of glomerular basement membraneswithout areas of subendothelial swelling. In some interlobulararteries, the internal elastic lamina was fragmented and split,whereas collagen accumulated in the intima and between themuscle cells of the media. In some of these arteries, thethickened internal elastic lamina had a dense, finely granularappearance.
Significant, unevenly distributed pathological changes wereconspicuous in the pelviureteral urothelium. They includedfocal squamous metaplasia and rather extended, mild to mod-
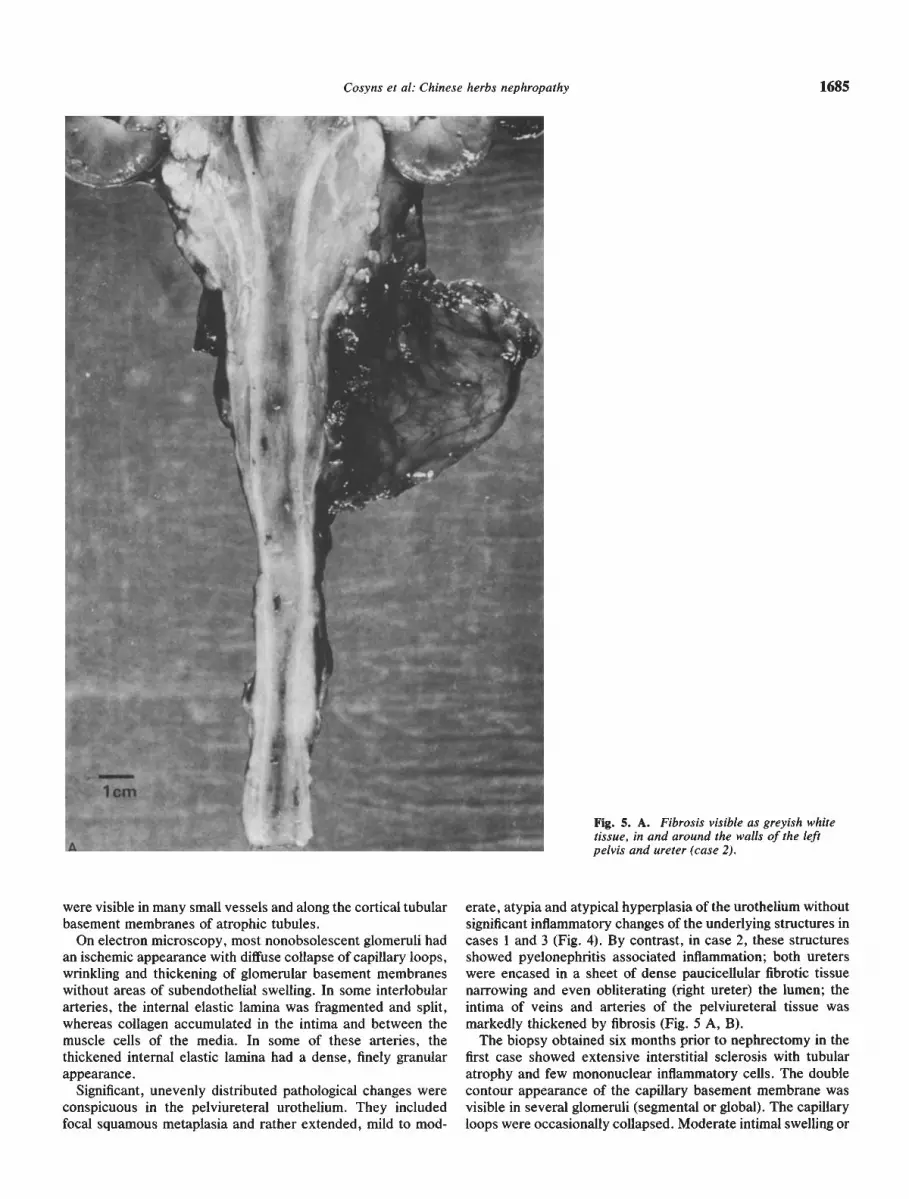
significant inflammatory changes of the underlying structures incases 1 and 3 (Fig. 4). By contrast, in case 2, these structuresshowed pyelonephritis associated inflammation; both ureterswere encased in a sheet of dense paucicellular fibrotic tissuenarrowing and even obliterating (right ureter) the lumen; theintima of veins and arteries of the pelviureteral tissue wasmarkedly thickened by fibrosis (Fig. 5 A, B).
The biopsy obtained six months prior to nephrectomy in thefirst case showed extensive interstitial sclerosis with tubularatrophy and few mononuclear inflammatory cells. The doublecontour appearance of the capillary basement membrane wasvisible in several glomeruli (segmental or global). The capillaryloops were occasionally collapsed. Moderate intimal swelling or
Cosyns et al: Chinese herbs nephropathy 1685
Fig. 5. A. Fibrosis visible as greyish whitetissue, in and around the walls of the leftpelvis and ureter (case 2).
were visible in many small vessels and along the cortical tubular erate, atypia and atypical hyperplasia of the urothelium without
If
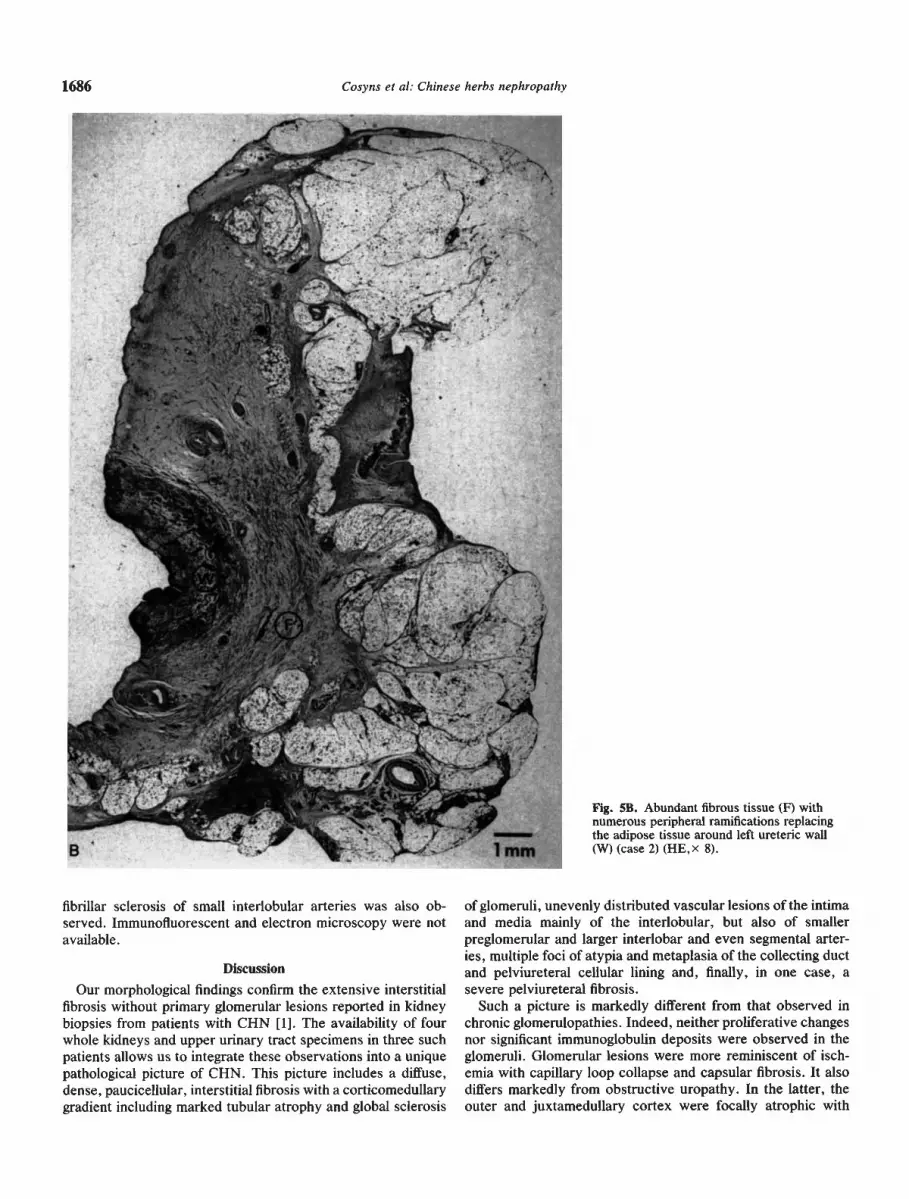
Fig. 5B. Abundant fibrous tissue (F) withnumerous peripheral ramifications replacingthe adipose tissue around left ureteric wall(W) (case 2) (HE,x 8).
fibrillar sclerosis of small interlobular arteries was also ob-served. Immunofluorescent and electron microscopy were notavailable.
Discussion
Our morphological findings confirm the extensive interstitialfibrosis without primary glomerular lesions reported in kidneybiopsies from patients with CHN [1]. The availability of fourwhole kidneys and upper urinary tract specimens in three suchpatients allows us to integrate these observations into a uniquepathological picture of CHN. This picture includes a diffuse,dense, paucicellular, interstitial fibrosis with a corticomedullarygradient including marked tubular atrophy and global sclerosis
of glomeruli, unevenly distributed vascular lesions of the intimaand media mainly of the interlobular, but also of smallerpreglomerular and larger interlobar and even segmental arter-ies, multiple foci of atypia and metaplasia of the collecting ductand pelviureteral cellular lining and, finally, in one case, asevere pelviureteral fibrosis.
Such a picture is markedly different from that observed inchronic glomerulopathies. Indeed, neither proliferative changesnor significant immunoglobulin deposits were observed in theglomeruli. Glomerular lesions were more reminiscent of isch-emia with capillary loop collapse and capsular fibrosis. It alsodiffers markedly from obstructive uropathy. In the latter, theouter and juxtamedullary cortex were focally atrophic with
1686 Cosyns et a!: Chinese herbs nephropathy
yF
t
2' -t.1 mm

Cosyns et al: Chinese herbs nephropathy 1687
relative sparing of the columns of Bertin whereas, in our cases,the sclerotic process was diffuse, extending into the columns ofBertin. The lesions were identical in the three cases, irrespec-tive of the presence of obstruction. Analgesic abuse, present insome [1] but not in our cases of CHN, leads to cortical changessimilar to those induced by obstruction and considered assecondary to papillary necrosis, also absent in our cases.
Finally, the pathological picture of CHN cannot be ascribedto the process developing in end-stage kidneys after initiation ofdialysis. Indeed, such lesions are observed only after severalmonths or years of substitutive therapy [4, 5], whereas thenephrectomy specimens were obtained from our three patientseither prior to dialysis or after less than three or 10 months ofhemodialysis.
The genesis of CHN lesions remains a matter of speculation.The observed vascular lesions cannot be ascribed to the age ofthe patients [6, 7] (all were below 35 years of age) or tohypertension (all 3 were normotensive). A primary vascularinsult, as observed in the hemolytic uremic syndrome, involv-ing not only renal but also extrarenal vessels such as those ofthe pelviureteral tissue, remains a distinct possibility. It mighthave led to the marked, diffuse, interstitial fibrosis of the cortexwith its outer to inner cortical gradient analogous to thatreported for global sclerosis of glomeruli in association withvascular involvement [7]. Whether it also accounts for thepelviureteral fibrosis observed in case 2 remains a matter ofspeculation. Alternatively, a primary toxic insult of the tubulesor interstitium with secondary vascular lesions remains a dis-tinct possibility. Both hypotheses imply a toxic insult whichcould account for the worrysome finding of cellular atypia andmetaplasia in the epithelial lining of collecting ducts, pelvis andureter.
Whatever their histogenesis, the pathological lesions wereport are amazingly reminiscent of another type of nephropa-thy known as the Balkan Endemic Nephropathy (BEN).
A widespread interstitial sclerosis and tubular atrophy ex-tending from the outer to the inner cortex, involving much moresignificantly the cortex than the medulla belongs indeed to thefirst description of BEN [8—12]. It is typically a hypocellularsclerosis with only focal mononuclear cell infiltrates. The latterare more pronounced when there is superimposed pyelonephri-tis, as in case 2, which is a frequent complication of advancedBEN [8, 12, 13]. The tubulointerstitial changes are alwaysassociated with sclerosis of glomeruli, typically predominant inthe outer cortex [8—12]. In the preserved glomeruli, focal doublecontour appearance of glomerular basement membrane resem-bling the chronic form of thrombotic microangiopathy wasdescribed in 22% of BEN cases [14] and was also found in thebiopsy material of case 1. Bowman's capsular fibrosis has beenfrequently reported in autopsy studies of BEN [8]. Fetal-likeglomeruli have been reported occasionally both in BEN [14]and in our cases. The cortical fibrosis is probably not ofglomerular origin in BEN in the absence of specific glomerularlesions by light microscopy [14] and of significant immunedeposits by immunofluorescent microscopy [15]. Arterial le-sions similar to those reported in our three patients have beenmentioned in most papers dealing with BEN. They weremoderate to severe in 14 of 40 biopsies of BEN [14]. Lesionswere mostly multifocal rather than diffuse and consisted ofarteriolar hyalinosis and fibroelastosis of large branches of the
interlobular arteries [14]. Although generally considered to besecondary to the tubulointerstitial changes, it is noteworthy thatthey were usually prominent and unassociated with arterialhypertension or other factors promoting vascular lesions [16,17]. Of note, focal stenosing, concentric, mucoid thickening ofthe intima of interlobular arteries was found on biopsy in twoBEN patients without obvious arterial hypertension [14]. Inter-estingly, transitional cell carcinomas of the urinary tract werefound up to 100 times more frequently in endemic than innonendemic regions [18—20]. Such carcinomas are often asso-ciated with urothelial atypia; the latter were also observed inour CHN cases. Such lesions of the upper urinary tract epithe-hum are unusual in parenchymal renal diseases. Their presenceunderlines the similarity between BEN and CHN.
The analogy between BEN and CHN is reinforced by thesimilarity of the clinical presentation. In both conditions, bloodpressure is often normal or only mildly elevated [1, 21]. Just asin our three patients, anemia is precocious and severe perhapsas a result of early destruction of cortical peritubular cellsproducing erythropoietin. In BEN, with incipient renal failure(serum creatinine <2 mgldl), anemia is more common than inpatients with other nephropathies [22]. Furthermore, in patientswith normal renal function, anemia is more prevalent in en-demic than in nonendemic villages [22]. Both BEN and CHNare characterized by an aseptic leukocyturia and a mild tubularproteinuria [23, unpublished observations in S cases of CHN].
Still, some differences between the two diseases should bepointed out. Involvement of the columns of Bertin in BENautopsied patients appears less prominent than in our cases [11,17]. On clinical grounds, three findings in CHN differ fromBEN: (1) the sex-ratio in BEN is 1/1, in contrast to the femalepreponderance in CHN; this reflects the almost exclusivefemale attendance of the X clinic. (2) CHN progresses toend-stage renal failure in a few months or years, in contrast withthe slow evolution of BEN over decades. This could reflect ahigher level of exposure to a toxic agent in CHN than in BEN.(3) Ureterohydronephrosis has not been reported in BENexcept in cases of urothehial tumors. This again may be due tothe less acute intoxication in BEN, sparing periureteral tissuewhose involvement is also uncommon in CHN.
The similarity of both pathological and clinical findings raisesthe possibility of a common cause of CHN and BEN. It is ofnote that aristolochic acid, a mutagenic and nephrotoxic alka-bid [24—26], found in the plant Aristolochia, has been incrimi-nated as the cause of BEN many years ago [21, 27], a hypoth-esis yet to be fully explored [28]. Similarly, it has beenhypothesized that aristolochic acid might be responsible for thedevelopment of CHN [29]. The Chinese herbs prescribed in theformula 2 pills were Magnolia officinalis and Stephania tetran-dra (fangji). Analysis of the incriminated pills disclosed thatmagnohiol and honokiol were contained in the first herb but notetrandrine was derived from the second one [1]. In contrast, ina sample of the herbs imported into Belgium, the ChineseMedicinal Material Research Centre at the Chinese Universityof Hong Kong recognized Aristolochia fan gchi, a nonpre-scribed aristolochic acid-containing herb [26]. A confusionbetween "fangji" and "fangchi" was postulated [1, 26], raisingthe possibility that aristolochic acid had been inadvertentlyincluded in the formula 2 pills. Indeed, Vanherweghem et al

1688 Cosyns et at: Chinese herbs nephropathy
recently confirmed in abstract form the identification of aristo-lochic acid in the incriminated formula 2 pills [29]. Interestingly,aristolochic acid has a carcinogenic effect on various tissues,including the urothelium [24, 25], and might thus account for thehigh prevalence of urinary tract epithelial atypia and transi-tional cell carcinoma complicating BEN, as well as for theurothelial atypia observed in our patients with CHN. Theamount of ingested aristolochic acid and its actual responsibilityin CHN remain to be determined. Nervertheless, the possibilitythat the same alkaloid might cause BEN and CHN is intriguing.
In conclusion, we describe a unique pathological pictureassociated with the consumption of Chinese herbs. This picturehas many similarities with that of endemic Balkan nephropathy.The possibility that both conditions are related to the toxicity ofartistolochic acid is considered. The presence of extensiveurothelial atypia in both conditions and the fact that the moreslowly progressing BEN is complicated by malignant tumors ofthe urothelium warrant a careful long-term follow-up of patientswith CHN.
Acknowledgments
Our thanks to Dr. Alenka Vizjak for helpful comments, to AnneBekaert for typing the manuscript, and to Stéphane Lagasse forpreparing the photomicrographs.
Reprint requests to Dr. Jean-Pierre Cosyns, Department of Pathol-ogy, University of Louvain Medical School, Cliniques St-Luc, 10Avenue Hippocrate, 1200 Brussels, Belgium.
References
1. VANHERWEGHEM JL, DEPIERREUX M, TIELEMANS C, ABRAMO-wicz D, DRATWA M, JADOUL M, RICHARD C, VANDERvELDE D,VERBEELEN D, VANHAELEN-FASTRE R, VANHAELEN M: Rapidlyprogressive interstitial renal fibrosis in young women: Associationwith slimming regimen including Chinese herbs. Lance! 341:387—391, 1993
2. Pu&NI CL, P0LLAK yE, SCHWARTZ FD: The reproducibility ofsemiquantitative analyses of renal histology. Nephron 1:230—237,1964
3. JADOUL M, DE PLAEN JF, COSYNS JP, VAN YPERSELE DE STRIHOUC: Adverse effects from traditional chinese medicine. Lance!341:892—893, 1993
4. OGATA K: Clinicopathological study of kidneys from patients onchronic dialysis. Kidney mt 37:1333—1340, 1990
5. BASILE JJ, MCCULLOUGH DL, HARRISON LH, DYER RB: Endstage renal disease associated with acquired cystic disease andneoplasia. J Urol 140:938—943, 1988
6. KAPPEL B, OLSEN S: Cortical interstitial tissue and scierosedglomeruli in the normal human kidney, related to age and sex: Aquantitative study. Virchows Arch [Al 387:271—277, 1980
7. KASISKE BL: Relationship between vascular disease and age asso-ciated changes in the human kidney. Kidney mt 31:1153—1159, 1987
8. PETRINSKA-VENKOVSKA S: Morphologic aspect of endemic ne-phropathy in Bulgaria, in international Symposium on EndemicNephropa!hy, edited by PUCHLEV A, Sofia, Bulgarian Academy ofSciences Press, 1965, p. 95
9. HALL PW III, DAMMIN GJ, GRIOGS RC, FAJGELJ A, ZIMONJIC B,GAON J: Investigation of chronic endemic nephropathy in Yugosla-via. II. Renal Pathology. Am J Med 39:210—217, 1965
10. HALL PW III, DAMMIN GJ: Balkan nephropathy. Nephron 22:281—
300, 197811. SINDJU M: Rezultati autopsijskih i biopsijskih istraivanjá
bubrenih promena u obolelih od endemske nephropatijè. Doktor-ska teza na Medicinskomfakultetu Univerze u Beogradu. Beograd,1981
12. HALL PW III, DAMMIN GJ: Balkan nephropathy, in Renal Pathol-ogy with Clinical and Functional Correlations, edited by TISHERCO. BRENNER BM, Philadelphia, J.B. Lippincott Co, 1989, p. 913
13. SINDJI* M, ZGURICAS MJ: Pyelonephritis and endemic nephropa-thy, in Endemic Nephropathy, edited by PUCHLEV A, DINEV IV,MILEv B, DOIcHIN0v D, Sofia, Publishing House of the BulgarianAcademy of Sciences, 1974, p. 178
14. FERLUGA D, HVALA A, VIZJAK A, TRNAEVal 5, HALILBAal A:Renal function, protein excretion, and pathology of Balkan en-demic nephropathy. III. Light and electron microscopic studies.Kidney mt 40 (Suppl 34):S57—S67, 1991
15. VIZJAK A, TRNAEV1 S, FERLUGA D, HALILBAU A: Renalfunction, protein excretion and pathology of Balkan endemic ne-phropathy. IV. Immunohistology. Kidney In! 40(Suppl 34):S68—S74, 1991
16. FERLUGA D, HVLA A, VIZJAK A, TRNAEVR S, HALILBAR A:Hantan nephropathy (HN) and Balkan endemic nephropathy(BEN): Tubulointerstitial or vascular renal diseases? (abstract)Path Res Pract 187:686, 1991
17. SINDJR M, ALI&PERIH N, VELIMIROVR D, ANOJH B: Renalvascular changes and their possible role in the pathogenesis andmorphogenesis of endemic Balkan nephropathy, in Endemic (Bal-kan) Nephropathy, edited by STRAHINJU S, STEFANOVI V, Pro-ceedings of the 4th Symposium, Ni, 1979, p 113
18. UKURANOVH R, IGNJAToVu M, STEFANOVII V: Urinary tracttumors and Balkan nephropathy in the South Moravia river basin.Kidney in! 40 (Suppl 34):S80—584, 1991
19. PETRONR VJ, BUKUROV NS, DJOKU MR, MILENKOVH DZ, VuK-ANOvIt AM, AVRAMOVU AD, NALE DP: Balkan endemic ne-phropathy and papillary transitional cell tumors of the renal pelvisand ureters. Kidney In! 40 (Suppl 34):S77—S79, 1991
20. RADOVANOVR Z, Jr.ucovu S, JEvREMOVH I: Incidence of tumorsof urinary organs in a focus of Balkan endemic nephropathy.Kidney In! 40 (Suppl 34):S75—S76, 1991
21. POLENAKOVH MH, STEFANOVI V: Balkan nephropathy, in Ox-ford Textbook of Clinical Nephrology, edited by CAMERON iS,DAvIsoN AM, GRUNFELD JP, KERR D, RITZ E, Oxford, OxfordUniversity Press, 1992, p. 857
22. HRABAR A, EOVI 5, ALERAJ B, tVORItEC D, HALL PW III:Relationship of anemia to Balkan endemic nephropathy. Kidney in!40 (Suppl 34):S44—S45, 1991
23. RAIEVI S, TRNAEVH 5, HRANISAVLJEVB J, VUELI D: Renalfunction, protein excretion and pathology of Balkan endemic ne-phropathy. II. Protein excretion. Kidney In! 40 (Suppl 34):S52—S56,1991
24. MENGS U, LANG W, POCH JA: The carcinogenic action of aristo-lochic acid in rats. Arch Toxicol 51:107—119, 1982
25. MENGS U: Tumour induction in mice following exposure to aristo-lochic acid. Arch Toxicol 61:504—505, 1988
26. BUT PPH: Need for correct identification of herbs in herbalpoisoning. Lance! 341:637, 1993
27. Ivu M: The problem of etiology of endemic nephropathy. Acta FacMed Naiss 1:29—37, 1970
28. STEFANOVH V, POLENAKOVH MH: Balkan nephropathy. Kidneydisease beyond the Balkans? Am J Nephrol 11:1—Il, 1991
29. VANHERWEGHEM JL, the Belgium Collaborative Group for theStudy of Chinese Herbs Nephropathy: Aristolochia nephropathy inhumans: An outbreak in Belgium. (abstract) I Am Soc Nephrol4:327, 1993