successful brief captopril treatment in experimental radiation nephropathy
TRANSCRIPT

Successful brief captopril treatment in experimental radiation nephropathy
ERIC P. COHEN, BRIAN L. FISH, and JOHN E. MOULDER MILWAUKEE, WISCONSIN
Experimental renal irradiation is followed by a well-defined sequence of events leading to kidney failure. Inhibitors of angiotensin-converting enzyme can prevent the structural and functional changes that occur after renal irradiation, which sug- gests that the renin-angiotensin system plays a key role in their evolution. We therefore evaluated captopril, used for short intervals, in a total body irradiation model of radiation nephropathy. Irradiated 7- to 8-week-old rats that were treated with captopril from 3.5 to 9.5 weeks after irradiation had better kidney function and survival than irradiated animals treated at earlier or later intervals. At 26 weeks after irradiation, kidney function of these animals was similar to that of irradiated animals treated continuously with captopril, but their subsequent survival was less. Animals irradiated at 7 to 8 weeks of age and treated with captopril from 6 to 9 weeks after irradiation had better function and survival than animals treated at earlier or later intervals. Irradiated 15-week-old animals had significant functional and survival benefit from continuous captopril treatment but no protection from a 6-week inter- val of therapy. We conclude that radiation nephropathy may be significantly at- tenuated by the use of captopril from 3.5 to 9.5 weeks after irradiation in young animals. Although older animals did not appear to benefit from a short course of captopril, these data suggest that the renin-angiotensin system is important in the sequential expression of renal radiation injury, particularly between 3.5 and 9.5 weeks after irradiation. (J Lab Clin Med 1997; 129:536-47)
Abbreviations: ACE = angiotensin-converting enzyme; BMT = bone marrow transplant; BP = blood pressure; BUN = blood urea nitrogen; SH = spontaneously hypertensive; TEl = total body irradiation; UP/UC = urine protein to creatinine ratio
R adiation nephropathy occurs predictably af- ter sufficient local kidney or total body irra- diation, l'z Until recently, such radiation in-
jury to normal tissue had been deemed to be inexorably progressive. 3 We successfully used angio-
From the Departments of Medicine and Radiation Oncology, Medical College of Wisconsin, Milwaukee. Supported by U. S. National Institutes of Health grant CA24652. Submitted for publication Oct. 25, 1996; revision submitted Dec. 23, 1996; accepted Jan. 02, 1997. Reprint requests: Eric P. Cohen, MD, Froedtert Memorial Lu- theran Hospital, Medical College of Wisconsin, Nephrology Di- vision, 9200 W. Wisconsin Ave., Milwaukee, WI 53226. Copyright © 1997 by Mosby-Year Book, Inc. 0022-2143/97 $5.00 + 0 5/1/80225
tensin-converting enzyme (ACE) inhibitors, includ- ing captopril, in the treatment of established radia- tion nephropathy caused by local kidney and total body irradiation (TBI). 4'5 Captopril was also effec- tive in preventing radiation nephropathy, 6'7 and an angiotensin II type I receptor blocker was even more effective. 8 In addition, antihypertensive agents that did not antagonize the renin-angiotensin system were ineffective in preventing radiation nephropa- thy. 3'6'9 These results not only established that radi- ation nephropathy may be successfully treated, but also implicated the renin-angiotensin system in its pathogenesis.
10 12 Recent studies by Harrap and colleagues - have shown long-term functional and survival benefits with ACE inhibitors used in spontaneously hyper-
536

J Lab Clin Med Volume 129, Number 5
tensive (SH) rats aged between 2 and 10 weeks. This effect could be el iminated by simultaneous angio- tensin I I administration. The A C E inhibitors had fewer, and only transient, benefits when used later in the life of the SH rat. Recent ly we demons t ra ted in our rat bone mar row transplant (BMT) model that A C E inhibitors are effective in the prevent ion of radiat ion nephropa thy even when initiation of A C E inhibitor therapy is delayed until 25 days after i r rad ia t ion) 3 Fur the rmore we showed that when A C E inhibitor therapy was discontinued 28 weeks after irradiation, the protective effect was not lost if adequate control of azotemia had been main- tained. 13
Viewed together, these data suggest that the re- nin-angiotensin system, either at the whole body or at the tissue level, may be involved in the sequential expression of injury in bo th the SH rat and in radi- at ion nephropathy, and that there might be an op- timal t ime after irradiation for using A C E inhibi- tors. W e therefore tested the effect of captopril when used for only brief intervals after TBI.
METHODS Rat syngeneic BMT model. These studies were per-
formed with WAG/Rij/MCW rats that were bred and housed in a moderate security barrier. These animals were free of Mycoplasma pulmonis, Pseudomonas, and common rat viruses. No antibiotics or immunosuppressive drugs were used. The animals were maintained in the Animal Care Facilities of the Medical College of Wisconsin, which are fully accredited by the American Association of Ac- creditation of Laboratory Animal Care. Seven- to eight- week-old male rats underwent TBI with 17 Gy, given in six fractions over 3 days at a dose rate of 0.48 Gy/minute. For irradiation, unanesthetized rats were immobilized in a specially constructed jig. 2 Immediately after the end of the radiation course, the animals received a syngeneic BMT. 2 For defining time after TBI/BMT, the day of BMT was considered to be day zero. Captopril was administered in the drinking water at 500 mg/L; when continuous capto- pril therapy was used, it started 10 days before BMT.
Experimental design. In a pilot study, the effect of a 6.5-week course of captopril given after TBI/BMT was evaluated in parallel with larger studies of the use of continuous captopril therapy to prevent radiation ne- phropathy 6 (Fig. 1). Ten animals were given captopril from 3.5 to 10 weeks after TBI/BMT. These animals were compared with 11 healthy (no drug, BMT, or TBI) ani- mals, 9 animals that received TBI/BMT only, and 6 ani- mals that were continuously treated with captopril.
A second study evaluated the use of captopril at different 5- to 6-week intervals after TBI/BMT (Fig. 1). Sixty-eight animals received TBI/BMT. Eight of these received no captopril, 5 were continuously treated with captopril, and 15 were treated with captopril from 1.5
Cohen, Fish, and Moulder 537
weeks before BMT to 3.5 weeks after BMT (a 5-week interval). The remaining 40 animals were treated with captopril for 6-week intervals, beginning at 3.5 weeks (n = 10), 9.5 weeks (n = 15), or 15.5 weeks (n = 15) after TBI/BMT.
In a third study, a briefer course of captopril was eval- uated (Fig. 1). Fifty-eight animals received TBI/BMT. Ten of these animals received no captopril. The remaining 48 were treated with captopril for 3-week intervals, beginning at BMT (n --- 10), or at 3 (n = 9), 6 (n = 10), 9 (n = 10) or 12 (n = 9) weeks after BMT.
A fourth study (Fig. 1) used 52 animals that were 15 weeks old when they received TBI/BMT (as opposed to the 7- to 8-week-old animals used in the first three stud- ies). The older animals were tested because of studies showing that the radiosensitivity of the kidney decreased when age at irradiation increased from 5 to 12 weeks of age. 14 Eight animals were given captopril for the 6 weeks before TBI, and 15 animals were given captopril from 3.5 to 9.5 weeks after BMT. These animals were compared with 14 animals that received TBI/BMT only, and 15 animals that were continuously treated with captopril. The 6-week treatment starting 6 weeks before TBI was chosen to overlap the time of life at which captopril therapy was most effective in animals irradiated at 7 to 8 weeks of age in the pilot and in the second study.
Monitoring the development of BMT nephropathy. An- imals were monitored daily in all experiments. Develop- ment of severe nephritis (uremia) was assessed up to 70 weeks after TBI, except in the pilot study, which was terminated at 26 weeks. Animals with symptomatic ure- mia or other lethal conditions (such as tumors) were killed. Severe nephritis (uremia) was the major cause of death in this model. 2 Levels of blood urea nitrogen (BUN), urine protein, and urine creatinine, and the sys- tolic blood pressure (BP) were assessed at 26 weeks after TBI in all animals. Urine was collected in metabolic cages, and blood was collected by orbital bleeding. Levels of BUN, urine protein, and urine cre- atinine were determined with commercial kits. 6 The systolic BP was measured with a tail-cuff. The animals were conditioned to the apparatus and the reported BP value was the average of the readings on 3 consecutive days. 6
Some animals were discontinued from the study before the assessment of their physiologic condition at 26 weeks. Before 26 weeks, one animal was discontinued because of the development of a tumor. Another animal was discon- tinued because of tooth problems, and four animals were killed or died of severe uremia. An additional seven ani- mals were killed or died of severe uremia before the blood pressure assessment could be completed. No more than one animal was lost from any treatment group before the 26-week assessment, except in the following two cases. In the group treated with TBI/BMT alone in the second study (n = 8), one animal with uremia was killed before 26 weeks, and two others (with BUN levels > 360 mg/dl at 26 weeks) died before the assessment of

5 3 8 Cohen, Fish, and Moulder J Lab Clin Med
May 1997
Weeks of Life
i I , , I , , , , I , , I I I I I I , , i , , , , i , , 0 10 20 30
TBI/BMT -1.5 ~ 3.5 9.5 wks relative to BMT
i
Pilot I " E ~ f o ~ { ~ I ~////////////////~~f~p.~(~/////////////////////////////////A I I
TBI/BMT -1.5 ~ 3.5 9.5
I
J ,
Study 2
i i I I i I )
4O
15.5 21.5 wks relative to BMT
. . . . . . . . . [~'captoprif~. "///////////~///////////////////~///////////////~ ~ ~pt~ ~ ~ V//////////////l/////~
Study 3
TBI/BMT 6 9 12 15 wks relative to BMT
Study 4
TBI/BMT /
-6 t 3.5 9.5 wks relative to BMT
W//////////////////~ ~ ~ (~ ~ # ! "////////////////////////////////~
Fig. 1. Schema of the experimental protocol Chronologic age of the animals is shown as the top arrow. The intervals of captopril treatment for each study are shown as shaded boxes. The numbers in italics are the number of weeks relative to the time of BMT. BMT, bone marrow transplant; TB1, total body irradiation.
the BP was completed. Also in the second study, 2 of 15 animals in the group treated with captopril from 15.5 to 21.5 weeks were killed because of uremia before 26 weeks.
S t a t i s t i c a l m e t h o d s . The four studies reported here were conducted over a number of years. Each of the four studies used a fully randomized design, where animals were randomly assigned to the different regimens of cap- topril treatments and were then given TBI/BMT as a group. Follow-up studies were conducted in a masked fashion. In all but the pilot study, the number of animals was large enough that each study had to be done in two groups. Within a given study, all treatment arms were equally represented in each of the two groups, and no significant differences in outcome (survival and azotemia at 26 weeks) were seen between these pairs of groups.
Cross-study comparisons were generally not done (excep- tions are specifically noted in the text).
Physiologic data are shown as geometric means with 95% confidence intervals. The Kruskal-Wallis test was used for analysis of differences among three or more groups, and comparisons between pairs of groups were made using the Mann-Whitney test. Correlations of physiologic parameters with survival times were done using the Kendall rank correlation test. Thep values for all comparisons are stated and are not corrected for multiple comparisons unless otherwise indicated. Where multiple comparison issues are relevant, they are discussed and p values corrected by the method of Beck-Bernholdt and Dubben. 15 The method of Kaplan- Meier was used to evaluate survival, which is shown as the incidence of severe nephritis requiring the killing of

J Lab Clin Med Volume 129, Number 5 Cohen, Fish, and Moulder 539
150
100
50
0 30
20
10
0
200
150
100
UPAJC (gm/gm)
BP (mm Hg)
age-matched normal animals
age-matched normal animals
age-matched normal animals
Fig. 2. Kidney function 26 weeks after TBI/BMT in the pilot study of a 6.5-week interval of captopril therapy in animals irra- diated at 7 to 8 weeks of age. Physiologic data are shown as geometric means with 95% confidence intervals; the 95% confi- dence interval for age-matched normal animals is shown by hor- izontal bars. A 6.5-week interval of captopril therapy is effective in reducing azotemia, proteinuria, and hypertension after TBI/ BMT, but the short treatment is generally less effective than continuous captopril therapy. BUN, blood urea nitrogen; BP, blood pressure; UP/UC, urine protein to creatinine ratio.
animals, and survival times were compared using an extension of the Kruskal-Wallis test.
RESULTS Renal function 26 weeks after 6-week intervals of cap-
topril therapy. In a pilot experiment, captopril given for 6.5 weeks, from 3.5 to 10 weeks after TBI/BMT, was effective in limiting azotemia (as indicated by
300
200
100
0
30
20
10
0
200
150
100
UP/UC (gm/gm)
I
Fig. 3. Kidney function 26 weeks after TBI/BMT in the second study of 6-week intervals of captopril therapy in animals irradi- ated at 7 to 8 weeks of age. Physiologic data are shown as geometric means with 95% confidence intervals. Blood pressure could not be evaluated in the animals given TBI/BMT alone (see METHODS). Survival data for these animals are shown in Fig. 6. A 6-week interval of captopril therapy starting at 3.5 weeks after TBI/BMT is effective in reducing azotemia and proteinuria, but other 6-week intervals are not as effective.
the BUN value), proteinuria (as determined by the urine protein to creatinine ratio [UP/UC]), and hy- pertension (as the BP value), compared with ani- mals given TBI/BMT alone (Fig. 2) (all p values = 0.0002). Azotemia in animals treated with captopril for 6.5 weeks was not significantly different (p > 0.20) from that in animals receiving continuous cap- topril therapy (Fig. 2). Continuous captopril treat- ment was, however, significantly more effective than the 6.5-week treatment in controlling hypertension and proteinuria (both p values < 0.003) (Fig. 2).

540 Cohen, Fish, and Moulder J Lab Clin Med
May 1997
200
100
0 20
BUN (mg/dl)
I
UP/UC (gm/gm)
10
200
150
100
Illi lull ¢at~ ca,~
Fig. 4. Kidney function 26 weeks after TBI/BMT in a study of 3-week intervals of captopril therapy in animals irradiated at 7 to 8 weeks of age. Physiologic data are shown as geometric means with 95% confidence intervals. Survival data for these animals are shown in Fig. 7. A 3-week interval of captopril therapy starting at 6 weeks after TBI/BMT is effective in reducing azotemia, but other 3-week intervals are not effective.
The second set of experiments (Fig. 1) was de- signed to confirm the first, and to test whether other intervals of captopril therapy were also ef- fective in limiting the severity of radiation ne- phropathy. The 3.5- to 10-week treatment interval was slightly shortened, to 3.5 to 9.5 weeks, to avoid weekend treatment changes. Continuous captopril treatment was again significantly effec- tive in preventing azotemia and proteinuria in irradiated rats (both p values < 0.008) (Fig. 3). Hypertension could not be formally evaluated at 26 weeks in the animals treated with irradiation alone because three of the eight animals died of end-stage renal disease before the blood pressure measurements could be completed (see METH-
100 BUN (mg/dl)
50
0
20 UP/UC (grrdgm)
10
0
200
BP (mm Hg)
150
100
ur~
Fig. 5. Kidney function 26 weeks after TBI/BMT in a study of 6-week intervals of captopril therapy in animals irradiated at 15 weeks of age. Physiologic data are shown as geometric means with 95% confidence intervals. Survival data for these animals are shown in Fig. 8. Continuous captopril therapy is effective in reducing azotemia, proteinuria, and hypertension in older ani- mals, but 6-week intervals of therapy are ineffective.
ODS). However, the BP levels in the animals that were given continuous captopril in this phase of the study (Fig. 3) were lower than in the animals treated with irradiation alone in the other phases of the study (Figs. 2 and 4).
In all four groups in which 6 weeks of captopril

J Lab Clin Med Volume 129, Number 5 Cohen, Fish, and Moulder 541
Continuous Cap
r.¢1
20
k ~ Cap 15.5 to 21.5 wks
40
60 ; [hllll
Cap -1.5 to 3.5 wks r , ~ 80
17 Gy TBI @ 7 to 8 weeks-of-age
100 0 10 20 30 40 50
Weeks post TBI/BMT
3.5 to 9.5 wks
19.5 to 15.5 wks
60 70
Fig. 6. Development of severe nephritis after 17 Gy TBI plus BMT in animals irradiated at 7 to 8 weeks of age. Actuarial incidence curves are shown for animals given TBI/BMT alone (gray curve), animals given TBI/BMT plus continuous captopril therapy (black line), and for animals given TBI/BMT plus various 6-week intervals of captopril therapy (patterned lines). Incidence curves stop when fewer than four animals are still at risk. These are the same animals whose 26-week physiologic data are shown in Fig. 3. Six-week intervals of captopril therapy are effective in delaying the development of severe nephritis, with the interval beginning at 3.5 weeks being the most effective.
therapy was given, azotemia at 26 weeks after TBI/ BMT was less than in animals given TBI/BMT alone ( a l p values < 0.002) (Fig. 3). Although the UP/UC ratio in some of the groups treated with 6 weeks of captopril was less than in the animals given TBI/ BMT alone, the differences were not statistically significant (all p values > 0.04, which is not signifi- cant when corrected for the fourfold comparison) (Fig. 3). As discussed above, hypertension could not be formally evaluated at 26 weeks in the animals given TBI/BMT alone, but the BP levels in the four groups treated with captopril for 6 weeks (Fig. 3) were comparable with those observed in animals treated with TBI/BMT alone in the other phases of the study (Figs. 2 and 4).
Although the animals treated with 6-week inter- vals of captopril had significantly less azotemia at 26 weeks than the animals treated with TBI/BMT alone, the results were not comparable with contin- uous captopril treatment (Fig. 3). For all four groups that received 6 weeks of captopril therapy, proteinuria at 26 weeks was significantly elevated compared with animals given continuous captopril (all p values < 0.003). Blood pressure values at 26 weeks were greater in the groups that received cap- topril for 6 weeks than in the animals given contin- uous captopril (all p values -< 0.037) (Fig. 3). For three of the groups that received 6 weeks of capto- pril therapy, the BUN levels at 26 weeks also were significantly elevated compared with the levels in
the animals given continuous captopril treatment (all p values < 0.004). The exception was the group whose 6-week interval of therapy started at 3.5 weeks, in which the BUN levels at 26 weeks were not significantly elevated (p = 0.19) compared with the levels in the animals given continuous captopril therapy (Fig. 3). The observation that a 6-week course of captopril therapy starting at 3.5 weeks was effective in controlling azotemia, but not hyperten- sion or proteinuria, confirms the results of the pilot study.
Clear differences are evident when the four groups of animals that were treated with captopril for different 6-week intervals are compared with each other. The Kruskal-Wallis test shows large dif- ferences in azotemia (p = 0.0027), and slight differ- ences in hypertension (p -- 0.035) and proteinuria (p = 0.011). Analysis of the azotemia data in Figure 3 shows that the group whose 6-week interval started at 3.5 weeks had significantly less azotemia than the other groups (all p -- 0.004). When that group was excluded from the Kruskal-Wallis analy- sis, no statistically significant differences were ob- served in azotemia (29 > 0.20) or hypertension (p = 0.12) among the remaining groups, although differ- ences still existed in proteinuria (p = 0.02). The control of azotemia after TBI/BMT that was achieved by a 6-week course of captopril therapy starting at 3.5 weeks was not equaled by other 6-week intervals of captopril therapy (Fig. 3).

542 Cohen, Fish, and Moulder J Lab Clin Med
May 1997
20
40
60
80 17 Gy TBI @ 7 to 8 weeks-of-age
TBI only a J~.l
Cap 3 to .6 wks L l
Cap 12 to 15 wks 1 wks
Cap 0 to 3 wks
100 • • ' " - - ' ' ' - • ~ , , , { . , . , . . , , • . • 0 10 20 30 40 50 60 70
Weeks post TBUBMT
Fig. 7. Development of severe nephritis after 17 Gy TBI plus BMT in animals irradiated at 7 to 8 weeks of age and treated with 3-week intervals of captopril. Actuarial incidence curves are shown for animals given TBI/BMT alone (gray curve), and for animals given TBI/BMT plus various 3-week intervals of captopril therapy (patterned lines). Incidence curves stop when fewer than four animals are at risk. These are the same animals whose 26-week physiologic data are shown in Fig. 4. A 3-week interval of captopril therapy beginning at 6 weeks after BMT is effective in delaying the development of severe nephritis; a 3-week interval starting at 9 weeks is less effective, and other intervals are ineffective.
Renal function 26 weeks after 3-week intervals of cap- topril therapy. The third group of studies (Fig. 1) evaluated the efficacy of 3-week intervals of capto- pril treatment after TBI/BMT. When compared with animals given TBI/BMT alone, the animals given a 3-week course of captopril starting at 6 weeks after TBI/BMT had a significant reduction in azotemia (p = 0.007, p = 0.035 when adjusted for the fivefold multiple comparison) (Fig. 4). No sig- nificant reductions in azotemia were observed in the other groups of animals treated with 3-week courses of captopril (allp -> 0.04) (Fig. 4). No reductions in BP levels or UPAJC values (compared with animals given TBI/BMT alone) were seen in any of the groups treated with 3-week intervals of captopril (all p -> 0.04) (Fig. 4). It is noteworthy that the 3-week course of captopril therapy that had some beneficial effect on azotemia (6 to 9 weeks after TBI, Fig. 4) fell within the 6-week course of therapy that showed the maximum efficacy (3.5 to 9.5 weeks after TBI, Fig. 3).
Renal function 26 weeks after captopril therapy in older animals. Animals irradiated at 15 weeks of age (Study 4, Fig. 1) had less severe BMT nephropathy than animals irradiated at a younger age. The 26- week physiologic data of these animals are pre- sented in Figure 5 (survival data are shown in Figure 8). A similar dependence of renal tolerance on age- at-irradiation had been observed in other studies in
this model) 4 In the 15-week-old animals, continu- ous captopril therapy gave significant protection against azotemia, proteinuria, and hypertension as compared with animals given TBI/BMT alone (allp values < 0.0001) (Fig. 5). In these 15-week-old an- imals, however, captopril given from 3.5 to 9.5 weeks after TBI/BMT was ineffective in controlling azotemia, proteinuria, or hypertension (all p val- ues -> 0.08) (Fig. 5). Captopril given from 9 to 15 weeks of age, an age interval that overlaps the most effective interval for captopril therapy in younger animals, was also ineffective in controlling azotemia, proteinuria, or hypertension (all p -> 0.10) (Fig. 5).
Survival after 3- and 6-week intervals of captopril ther- apy. The survival of 7- to 8-week-old animals treated with 6-week intervals of captopril therapy is superior to that of animals given TBI/BMT alone (all p val- ues < 0.001) (Fig. 6). These 6-week intervals of treatment, however, did not give survival times equivalent to those achieved with continuous capto- pril therapy (allp values < 0.025) (Fig. 6). Animals treated for the 6-week interval starting at 3.5 weeks after TBI/BMT had longer survival times than ani- mals treated for the other three intervals (all p values < 0.002). Animals treated for the intervals starting at 1.5 weeks before, 9.5 weeks after, and 15.5 weeks after TBI/BMT did not differ from each other with regard to survival (all p values > 0.20). The survival data (Fig. 6) show the same pattern
J Lab Clin Med Volume 129, Number 5 Cohen, Fish, and Moulder 543
20
40
60
80
| I l L
TBI only (you~
| Continuous Cap
to 9.5 wks
1. ~ C ~ o 0 wks
TBI only
t7 Gy TBI @ 15 weeks-of-age 100 . . . . . . . . . . . . . . . . . . . I , , , v , , ,
0 10 20 30 40 50 60 70
Weeks Post TBUBMT
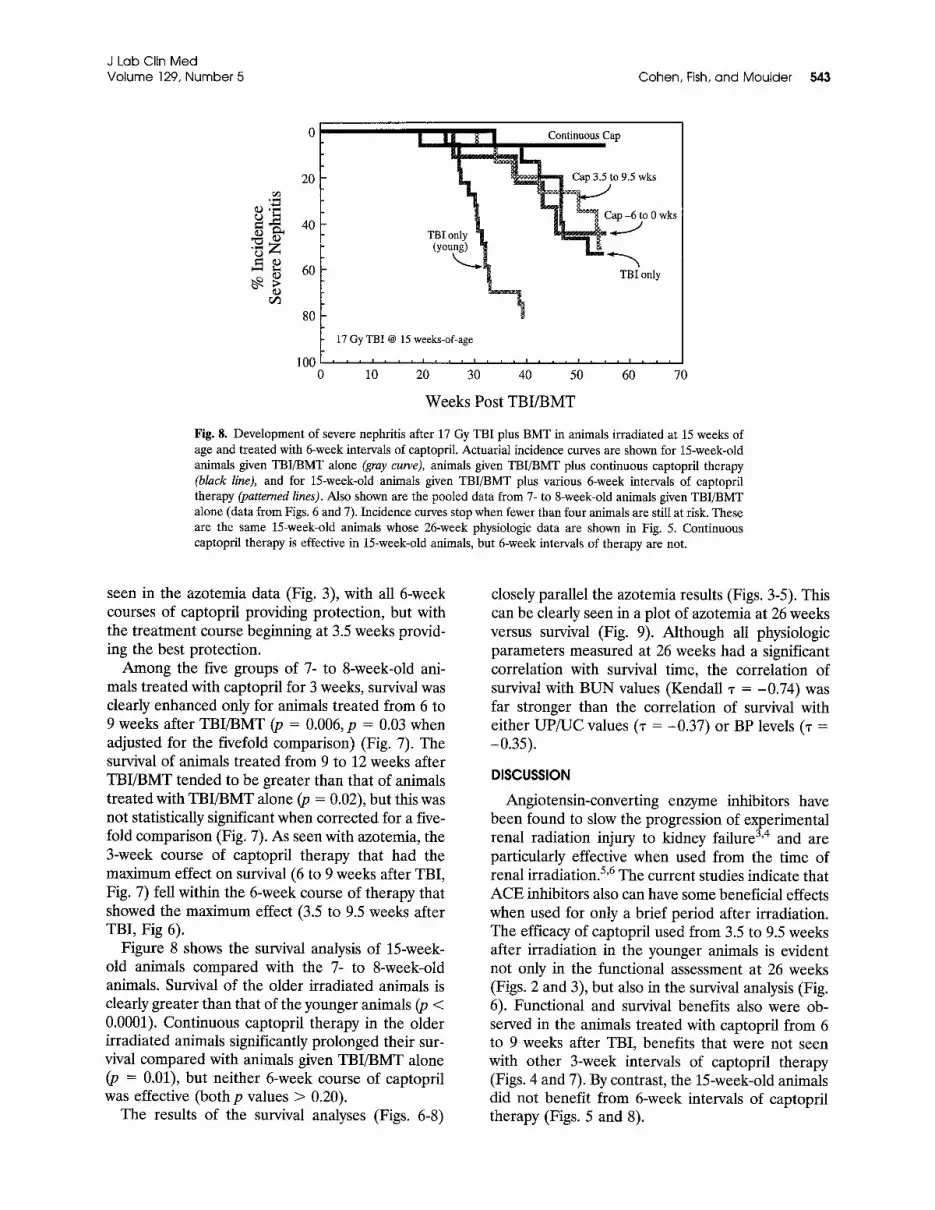
Fig. 8. Development of severe nephritis after 17 Gy TBI plus BMT in animals irradiated at 15 weeks of age and treated with 6-week intervals of captopril. Actuarial incidence curves are shown for 15-week-old animals given TBI/BMT alone (gray curve), animals given TBI/BMT plus continuous captopril therapy (black line), and for 15-week-old animals given TBI/BMT plus various 6-week intervals of captopril therapy (patterned lines). Also shown are the pooled data from 7- to 8-week-old animals given TBI/BMT alone (data from Figs. 6 and 7). Incidence curves stop when fewer than four animals are still at risk. These are the same 15-week-old animals whose 26-week physiologic data are shown in Fig. 5. Continuous captopril therapy is effective in 15-week-old animals, but 6-week intervals of therapy are not.
seen in the azotemia data (Fig. 3), with all 6-week courses of captopril providing protection, but with the treatment course beginning at 3.5 weeks provid- ing the best protection.
Among the five groups of 7- to 8-week-old ani- mals treated with captopril for 3 weeks, survival was clearly enhanced only for animals treated from 6 to 9 weeks after TBI/BMT (p = 0.006, p = 0.03 when adjusted for the fivefold comparison) (Fig. 7). The survival of animals treated from 9 to 12 weeks after TBI/BMT tended to be greater than that of animals treated with TBI/BMT alone (p = 0.02), but this was not statistically significant when corrected for a five- fold comparison (Fig. 7). As seen with azotemia, the 3-week course of captopril therapy that had the maximum effect on survival (6 to 9 weeks after TBI, Fig. 7) fell within the 6-week course of therapy that showed the maximum effect (3.5 to 9.5 weeks after TBI, Fig 6).
Figure 8 shows the survival analysis of 15-week- old animals compared with the 7- to 8-week-old animals. Survival of the older irradiated animals is clearly greater than that of the younger animals (p < 0.0001). Continuous captopril therapy in the older irradiated animals significantly prolonged their sur- vival compared with animals given TBI/BMT alone (p = 0.01), but neither 6-week course of captopril was effective (both p values > 0.20).
The results of the survival analyses (Figs. 6-8)
closely parallel the azotemia results (Figs. 3-5). This can be clearly seen in a plot of azotemia at 26 weeks versus survival (Fig. 9). Although all physiologic parameters measured at 26 weeks had a significant correlation with survival time, the correlation of survival with BUN values (Kendall -r = -0.74) was far stronger than the correlation of survival with either UP/UC values (-r = -0.37) or BP levels ('r = -0.35). DISCUSSION
Angiotensin-converting enzyme inhibitors have been found to slow the progression of experimental renal radiation injury to kidney failure 3'4 and are particularly effective when used from the time of renal irradiation. 5'6 The current studies indicate that ACE inhibitors also can have some beneficial effects when used for only a brief period after irradiation. The efficacy of captopril used from 3.5 to 9.5 weeks after irradiation in the younger animals is evident not only in the functional assessment at 26 weeks (Figs. 2 and 3), but also in the survival analysis (Fig. 6). Functional and survival benefits also were ob- served in the animals treated with captopril from 6 to 9 weeks after TBI, benefits that were not seen with other 3-week intervals of captopril therapy (Figs. 4 and 7). By contrast, the 15-week-old animals did not benefit from 6-week intervals of captopril therapy (Figs. 5 and 8).

544 C o h e n , Fish, a n d M o u l d e r J Lab Ciin M e d
M a y 1997
>57 ,o01_ o° °o • °o°° 0 0000" 0 0
4 o ~ ~ [ o %0 ° Oo
4 / o o o o oo
r.~ ¢:~ J o o oO o o°~? % ~o 8 o8'Ooo
.,~ [-~ " ~ 30
25 1 , I , , , 20 40
O o O o o
o a Oo OOoOO ° 0 0 0 0
o ~° o ~ o o
, , I I , i00 200 400
BUN (mg/dl) at 26 Weeks
Fig. 9. Time to development of severe nephritis after TBI/BMT as a function of B U N at 26 weeks. Survival t imes are relative to TBI/BMT; animals that did not survive to 26 weeks are excluded from the analysis. B U N is a strong predictor of animal survival after TBI/BMT.
Experimentally, progressive renal injury occurs after subtotal nephrectomy, double doses of paren- teral adriamycin, streptozotocin-induced diabetes, and in other models. 16-1s Angiotensin-converting enzyme inhibitors may slow this progression and are more effective than other antihypertensive agents. 19-21 Use of ACE inhibitors has been contin- uous in such studies, beginning after subtotal ne- phrectomy or induction of diabetes, for instance, and continuing until the experiment is terminated. Recent studies in our laboratory have shown that the preventive effect of captopril in radiation ne- phropathy is not lost when the initiation of ACE inhibitor therapy is delayed until 25 days after TBI, and that the preventive effect persists even if the drug is removed from the drinking water 28 weeks after TBI. 13 Thus we hypothesized that captopril might exert a beneficial effect in radiation nephrop- athy if used for only a brief period after irradiation. The current studies have confirmed that hypothesis in young but not in older rats.
Furthermore, these studies support the notion that radiation injury of healthy tissue is not inevita- ble and that it may be significantly attenuated by clinically accepted drugs. 3 Until recently, radiation injury of normal tissue in the kidney and other organs could be modified only by relatively toxic drugs, and only when these were used at the time of irradiation. 22'23 The current results, and our previ- ous studies, 4'5A3 strongly suggest that at least in the kidney, radiation injury of normal tissue may be modified by drugs used well after irradiation. This may have direct clinical utility, either by affording treatment of existing radiation injury or by allowing
escalation of radiation doses and, thus, the promise of higher cure rates of treated cancers. 3
The pilot studies were originally designed to in- vestigate whether starting captopril after TBI would be as effective as using captopril continuously from the time of TBI. A group of 10 animals began receiving captopril 3.5 weeks after TBI/BMT and stopped receiving the drug 6.5 weeks later. These animals showed significant preservation of renal function at 26 weeks, compared with animals that were given TBI/BMT alone (Fig. 2). Moreover, the BUN levels of animals given the 6.5-week interval of captopril therapy were not significantly different from those of animals treated continuously with captopril, and BUN was a very good marker of injury in our studies (Fig. 9). 5,6 This led to consid- eration of a possible interval effect of captopril ther- apy, which was confirmed in the second set of ex- periments (Figs. 3 and 6). These studies showed significantly less azotemia and better survival in ir- radiated animals treated for any of the 6-week in- tervals, when compared with animals given TBI/ BMT alone. An intergroup comparison showed that the animals treated for 6 weeks starting at 3.5 weeks had less azotemia (Fig. 3), and correspondingly bet- ter survival (Fig. 6), than animals treated for any other interval. These data not only confirmed the value of the simple BUN measurement in predicting outcome in this model (Fig. 9), but also confirmed the results of the pilot study. In the studies of cap- topril used for a 3-week interval from 6 to 9 weeks after irradiation, we again noted the coincidence of benefit as assessed by BUN levels at 26 weeks after irradiation (Fig. 4) and long-term survival (Fig. 7). It

J Lab Clin Med Volume 129, Number 5
is noteworthy that these effects occurred despite the lack of good control of blood pressure or protein- uria. It is also important to note that although these brief intervals of captopril therapy were effective in reducing azotemia and enhancing survival, they were not nearly as effective as continuous captopril treatment.
In studies of SH rats, Harrap and colleagues 1°-12 were the first to show that a brief, 4- to 8-week treatment of young SH rats with the ACE inhibitor perindopril was effective in attenuating the develop- ment of hypertension in these animals. Concomitant angiotensin II administration appeared to eliminate the protective effect of the ACE inhibitor. When perindopril was used in SH rats aged 20 to 24 weeks, it did control the systolic BP levels during its use but the BP levels rose to control (untreated) levels after the treatment ended. Other agents used for brief intervals in young SH rats were also effective in attenuating later hypertension. These included the combination of hydralazine and hydrochlorothia- zide, and a vasopressin antagonist24'25; however, nei- ther agent was as effective as ACE inhibitors when used for brief intervals. In the SH rat, both kidney and plasma renin are higher in early life (3 to 6 weeks old) than in the adult rat. 26 It is possible that a generally higher level of activity of the entire renin-angiotensin system exists in the young SH rat, compared with healthy rats of the same age, and properly timed ACE inhibition may blunt this activ- ity with subsequent reduced hypertension.
As in the SH rat, the mechanism of the effect of short-course captopril therapy in radiation nephrop- athy may be derived from a properly timed attenu- ation of an activated renin-angiotensin system. Ra- diation-induced activation of the kidney renin system is suggested by the finding that ACE inhibi- t o r s 6'9 and an AII receptor antagonist s are effective against BMT nephropathy, whereas other antihy- pertensive agents are not. 3'6'9
Radiation-induced activation of the kidney renin system on the tissue level also has been suggested in two histologic studies of radiation nephropathy. 27'2s Fisher and Hellstrom 28 showed that juxtaglomerular degranulation preceded hypertension in their stud- ies of radiation nephritis, which would suggest that renin release plays a role in the hypertension that is virtually uniform in this model. Blood renin, how- ever, does not appear to change over time in radia- tion nephropathy. 1 In earlier studies, we showed that proteinuria was apparent by 6 weeks after irra- diation. 6 The mechanism of this proteinuria is not known, although both endothelial and mesangial injury occur early in radiation nephropathy and
Cohen, Fish, and Moulder 545
could play a role. Endothelial injury has been shown morphologically by others 29 and we have shown an early deficit of (endothelial derived) nitric oxide, as urinary cyclic guanosine monophosphate, in radia- tion nephropathy. 3° Speculatively, the use of capto- pril from 3.5 to 9.5 weeks after TBI, at least in younger animals, reduces that endothelial injury, a mechanism that would explain the much reduced efficacy when captopril is used for other intervals. The currently reported but less impressive benefits with captopril used from 6 to 9 weeks suggest that the critical time of radiation injury includes and extends outside that interval.
Both subtotal nephrectomy and renal radiation injury set in motion a sequence of events, in part adaptive, which involves proliferation of renal epi- thelial cells, cell growth, changes in glomerular cap- illary pressure, and also enhanced matrix and colla- gen synthesis and glomerular sclerosis. The latter is the pathologic evidence of progressive scarring and kidney failure. The changes in cell proliferation and growth occur within days of subtotal nephrectomy or renal irradiation, 31'32 whereas evidence of scarring occurs weeks to months after either injury. 27'33'34 It may be particularly important to interrupt these later events if progressive kidney failure is to be preventedY
In a report in abstract, 36 transient ACE inhibitor treatment was found to be effective in limiting glo- merulosclerosis in the remaining kidney after uni- lateral nephrectomy in the rat. This suggests that brief, noncontinuous ACE inhibitor treatment may be effective in more than one model of renal injury. On the other hand, ongoing kidney injury, as in experimental or clinical diabetic nephropathy, will require uninterrupted use of ACE inhibitors.
It is worth noting the ineffectiveness of captopril used from 1.5 weeks before to 3.5 weeks after irra- diation (Figs. 3 and 6). This strongly suggests that captopril does not act as a classical radioprotector, as does the free-radical scavenger WR-2721.
Finally, the total lack of benefit from a 6-week interval of captopril therapy in older animals re- mains unexplained. One explanation for this may relate to the decreased severity of renal injury in the irradiated animals of this group compared with that of the younger animals, because younger animals are more likely to develop radiation nephropathy than older ones exposed to the same dose of radia- tion. 14'37 In previous studies, the relationship be- tween the severity of injury and the efficacy of cap- topril therapy has been somewhat paradoxical. When used therapeutically, captopril has been most effective when damage is minimal at the start of

J Lab Clin Med 546 Cohen, Fish, and Moulder May 1997
therapy4'5; but when used prophylactically, both cap- topril and enalapril had their greatest effect when the level of insult was most severe. 6 Still, continuous captopril therapy does have some protective effect in these 15-week-old animals, an effect that is not shared by a 6-week interval of captopril. The renin- angiotensin system may simply be less active in older animals. Indeed, renin mRNA and protein levels are higher in fetal and newborn rat kidneys compared with adult rat kidneys. 3s The distribution of renin expression is also more extensive in fetal and early life. 39 Thus older animals might not respond as well to a brief interval of inhibition of the renin-angio- tensin system, although continuous use of captopril still provides significant protection to these older irradiated animals.
SPECULATIONS In SH rat hypertension, as in radiation nephrop-
athy, an initial event (genetic in the first and geno- toxic in the second) is followed by a defined se- quence of events leading to severe hypertension in the first model and renal failure in the second. The current work, and that of Harrap and colleagues 1°-12 using SH rats, supports the notion that this patho- logic sequence can be interrupted, at least in the young animal. It is thus possible that a brief interval of treatment may be beneficial in other genetic mod- els of renal injury, for instance, the development of cysts in the HanSPRD rat, and not necessarily with ACE inhibitors. By extension, in any clinical hered- itary renal disease, it is theoretically possible to find a particular and crucial interval for pathologic pro- gression and, in turn, to find an optimal interval and agent for treatment.
Mary Lou Stott provided expert technical help. Cindy Ziebell and Yvonne Morauski typed the manuscript. Bristol-Myers- Squibb provided captopril as a gift.
REFERENCES 1. Robbins MEC, Campling D, Rezvaui M, Golding SJ,
Hopewell JW. Radiation nephropathy in mature pigs follow- ing the irradiation of both kidneys. Int J Radiat Biol 1989; 56:83-98.
2. Moulder JE, Fish BL. Late toxicity of total body irradiation with bone marrow transplantation in a rat model. Int J Rad Oncol Biol Phys 1989;16:1501-9.
3. Moulder JE, Robbins MEC, Cohen EP, Hopewell JW, Ward WF. Pharmacologic modification of radiation-induced nor- mal tissue injury. In: Mittal BB, Purdy JA, Aug LL, editors. Radiation Therapy, Norwell: Kluwer Academic Publishers (in press).
4. Cohen EP, Fish BL, Moulder JE. Treatment of radiation nephropathy with captopril. Radiat Res 1992;132:346-50.
5. Moulder JE, Fish BL, Cohen EP. Treatment of radiation
nephropathy with ACE inhibitors. Int J Radiat Oncol Biol Plays 1993;27:93-9.
6. Cohen EP, Moulder JE, Fish BL, Hill P. Prophylaxis of experimental bone marrow transplant nephropathy. J Lab Clin Med 1994;124:371-80.
7. Cohen EP, Molteni A, Hill P, Fish BL, Ward WF, Moulder JE. Captopril preserves function and ultrastructure in ex- perimental radiation nephropathy. Lab Invest 1996;75:349-60.
8. Moulder JE, Fish BL, Cohen EP, Bonsib SM. Angiotensin II receptor antagonists in the prevention of radiation nephrop- athy. Radiat Res 1996;146:106-10.
9. Juncos LI, Carrasco Duenas S, Cornejo JC, Broglia CA, Cejas H. Long-term enalapril and hydrochlorothiazide in radiation nephritis. Nephron 1993;64:249-55.
10. Harrap SB, Van der Merwe WM, Griffin SA, MacPherson F, Lever AF. Brief angiotensin converting enzyme inhibitor treatment in young spontaneously hypertensive rats reduces blood pressure long-term. Hypertension 1990;16:603-14.
11. Campbell D J, Duncan AM, Kladis A, Harrap SB. Converting enzyme inhibition and its withdrawal in spontaneously hyper- tensive rats. J Cardiovasc Pharmacol 1995;26:426-36.
12. Harrap SB, Mirakian C, Datodi SR, Lever AF. Blood pres- sure and life span following brief ACE inhibitor treatment in young spontaneously hypertensive rats. Clin Exp Pharmacol Physiol 1994;21:125-7.
13. Moulder JE, Fish BL, Cohen EP. Noncontinuous use of angiotensin converting enzyme inhibitors in the treatment of experimental bone marrow transplant nephropathy. Bone Marrow Transplant 1997;19:729-36.
14. Moulder JE, Fish BL. Age-dependence of radiation nephrop- athy in the rat. Radiat Res 1997;147:349-53.
15. Beck-Bornholdt HP, Dubben HH. Potential pitfalls in the use of p-values and in interpretation of significance levels. Radiother Oncol 1994;33:171-6.
16. Shimamura T, Morrison AB. A progressive glomerulosclero- sis occurring in partial five-sixths nephrectomized rats. Am J Pathol 1975;79:95-101.
17. Okuda S, Oh Y, Tsuruda H, Onoyama K, Fujimi S, Fuk- ishima M. Adriamycin-induced nephropathy as a model of chronic progressive glomerular disease. Kidney Int 1986;29: 502-10.
18. Zatz R, Meyer TW, Rcnnke HG, Brenner BM. Predomi- nance of hemodynamic rather than metabolic factors in the pathogenesis of diabetic glomerulopathy. Proc Natl Acad Sci U S A 1985;82:5963-7.
19. Anderson S, Rennke HG, Brenner BM. Therapeutic advan- tage of converting enzyme inhibitors in arresting progressive renal disease associated with systemic hypertension in the rat. J Clin Invest 1986;77:1993-2000.
20. Zatz R, Dunn BR, Meyer TW, Anderson S, Rennke HG, Brenner BM. Prevention of diabetic glomerulopathy by phar- macological amelioration of glomerular capillary hyperten- sion. J Clin Invest 1986;77:1925-30.
21. Brunner FP, Thiel G, Hermle M, Bock HA, Mihatsch MJ. Long-term enalapril and verapamil in rats with reduced renal mass. Kidney Int 1989;36:969-77.
22. Williams WV, Denekamp J. Modification of the radiation response of the mouse kidney by misonidazole and WR-2721. Int J Radiat Oncol Biol Phys 1983;9:1731-6.
23. Donaldson SS, Moskowitz PS, Evans JW, Fajardo LF. Pro- tection from radiation nephropathy by WR-2721. Radiat Res 1984;97:414-23.
24. Traub O, Lloyd MC, Webb RC. Long-term effects of brief

J Lab Clin Med Volume 129, Number 5
antihypertensive treatment on systolic blood pressure and vascular reactivity in young genetically hypertensive rats. Car- diovasc Drugs Ther 1995;9:421-9.
25. Burrell LM, Phillips PA, Risvanis J, Aldred KL, Hutchins AM, Johnston CI. Attenuation of genetic hypertension after short-term vasopressin VIA receptor antagonism. Hyperten- sion 1995;26:828-34.
26. Sen S, Smeby RR, Bumpus FM. Renin in rats with sponta- neous hypertension. Circ Res 1972;31:876-80.
27. Fajardo LF, Brown JM, Glatstein E. Glomerular and juxta- glomerular lesions in radiation nephropathy. Radiat Res 1976;68:177-83.
28. Fisher ER, Hellstrom HR. Pathogenesis of hypertension and pathologic changes in experimental renal irradiation. Lab Invest 1968;19:530-8.
29. Jaenke RS, Robbins MEC, Bywaters T, Whitehouse E, Rez- vani M, Hopewell JW. Capillary endothelium-target site of renal radiation injury. Lab Invest 1993;68:396-405.
30. Cohen EP, Fish BL, Moulder JE. The role of nitric oxide in radiation nephropathy. Arch Physiol Biochem 1996;104:200-6.
31. Fine L. The biology of renal hypertrophy. Kidney Int 1986; 29:619-34.
32. Robbins MEC, Sovanson JA, Wilson GD, et al. Radiation-
Cohen, Fish, and Moulder 547
induced changes in the kinetics of glomerular and tubular cells in the pig kidney. Radiat Res 1994;138:107-13.
33. Beukers JJB, Van der Wal A, Hoedemaker P J, Weening JJ. Converting enzyme inhibition and progressive glomeruloscle- rosis in the rat. Kidney Int 1987;32:794-800.
34. Robbins MEC, Wooldridge MJA, Jaenke RS, et al. A mor- phological study of radiation nephropathy in the pig. Radiat Res 1991;126:317-27.
35. Cohen EP. Fibrosis causes progressive kidney failure. Med Hypoth 1995;45:459-62.
36. Nagata M, Ito K. Transient treatment with ACE inhibitor attenuates glomerular injury following uninephrectomy in young rats [abstract]. J Am Soc Nephrol 1993;4:777.
37. Jongejan HTM, van der Kogel AJ, Provoost AP, Molenaar JC. Radiation nephropathy in young and adult rats. Int J Radiat Oncol Biol Phys 1987;13:225-32.
38. Gomez RA, Lynch KR, Sturgill BC, et al. Distribution of renin mRNA and its protein in the developing kidney. Am J Physiol 1989;257:F850-8.
39. Gomez RA, Chevalier RL, Sturgill BC, Johns DW, Peach MJ, Carey RM. Maturation of the intrarenal renin distribu- tion in Wistar-Kyoto rats. J Hypertension 1986;4(suppl 5): $31-3.