immunosuppressive treatment for idiopathic membranous nephropathy: a systematic review
TRANSCRIPT

R
●
momwiwoeErciCwnh©
It
sBs
1
bwr
The Official Journal of the
National Kidney Foundation
VOL 44, NO 3, SEPTEMBER 2004
AJKD American Journal ofKidney Diseases
A
EVIEW
Immunosuppressive Treatment for Idiopathic MembranousNephropathy: A Systematic Review
Annalisa Perna, StatSciD, Arrigo Schieppati, MD, Javier Zamora, PhD,Giovanni A. Giuliano, DiplStat, Norbert Braun, MD,
and Giuseppe Remuzzi, MD
Background: This study aims to assess whether immunosuppression is beneficial in the treatment of idiopathicembranous nephropathy (IMN). Methods: We reviewed randomized controlled trials (RCTs) addressing the effectf immunosuppression on histologically proven IMN in adults with nephrotic syndrome followed up for at least 6onths. The literature was searched according to Cochrane Collaboration guidelines. Four therapeutic classesere considered: (1) steroids (alone), (2) alkylating agents (alone or in combination with steroids), (3) calcineurin
nhibitors (alone or in combination with steroids), and (4) antiproliferative agents (alone). Results: Eighteen RCTsere selected (1,025 patients). Overall, no differences were found between immunosuppressive treatment and placebor no treatment. For oral glucocorticoid therapy, no beneficial effect was observed. For alkylating agents, a beneficialffect was observed on complete remission (relative risk [RR], 2.37; 95% confidence interval [CI], 1.32 to 4.25; P � 0.004).xcluding patients with particularly well-preserved renal function, there was no significant difference in completeemission. Cyclophosphamide therapy resulted in a lower rate of adverse-event discontinuations compared withhlorambucil (8 versus 21 discontinuations, respectively; RR, 2.34; 95% CI, 1.25 to 4.39; P � 0.008). For calcineurinnhibitors, no difference was observed. For antiproliferative agents, a paucity of data did not allow a conclusion.onclusion: The meta-analysis failed to show a long-term effect of treatment on patient and/or renal survival. There iseak evidence that the immunosuppressive regimen increased the remission rate. The review of safety showed a higherumber of discontinuations for adverse events in immunosuppressive-treatment groups and that cyclophosphamidead fewer side effects than chlorambucil. Am J Kidney Dis 44:385-401.2004 by the National Kidney Foundation, Inc.
NDEX WORDS: Idiopathic membranous nephropathy (IMN); adult; nephrotic syndrome (NS); immunosuppressiveherapy; systematic review.
Ips
cb
CDsd
Editorial, p. 562
From Mario Negri Institute for Pharmacological Re-earch; Nephrology and Dialysis Unit, Ospedali Riuniti diergamo, Italy; and Section of Nephrology and Hyperten-ion, University of Tuebingen, Germany.
Received January 14, 2004; accepted in revised form May0, 2004.This review is excerpted from a Cochrane Review that will
e published in The Cochrane Library 2004, Issue 4 (http://ww.update-software.com/cochrane). Cochrane Reviews are
egularly updated as new evidence emerges in response to
merican Journal of Kidney Diseases, Vol 44, No 3 (September),
DIOPATHIC MEMBRANOUS nephropathy(IMN) is the most common form of ne-
hrotic syndrome (NS) in adults.1 The diseasehows a benign or indolent course in the majority
omments and criticisms, and The Cochrane Library shoulde consulted for the most recent version of the Review.Address reprint requests to Annalisa Perna, StatSciD,
linical Research Centre for Rare Diseases Aldo e Celeaccò, Mario Negri Institute for Pharmacological Re-
earch, Via Gavazzeni 11, 24125 Bergamo, Italy.Email ad-ress: [email protected]© 2004 by the National Kidney Foundation, Inc.0272-6386/04/4403-0001$30.00/0
doi:10.1053/j.ajkd.2004.05.0202004: pp 385-401 385

oomprtgairmttdiwbtm
ttaf“ooosa(crtNaptmcwsrtcptrsbs
eRdo
sDuartdmaalanawaatdenwes
T
alol(cpssafibamouawa
PERNA ET AL386
f patients, with a rate of spontaneous completer partial remission of NS as high as 30% orore.2 However, a non-negligible proportion of
atients (30% to 40%) progress toward end-stageenal failure in 5 to 15 years.3 Several therapeu-ic regimens have been proposed; namely, orallucocorticoids, alkylating agents (chlorambucilnd cyclophosphamide), and, lately, cyclospor-ne.4 The uncertain risk-benefit ratio of corticoste-oid and cytotoxic therapy in the treatment ofembranous nephropathy and the lack of defini-
ive evidence that cytotoxic drugs alter the long-erm course of the disease make optimal therapyifficult to determine. Because almost all studiesnvolved at most only a few tens of patients, dataere combined through different approaches,5-7
ut yielded conflicting conclusions and still main-ained uncertainty on the most appropriate treat-ent.Couchoud et al5 combined 8 randomized con-
rolled trials (RCTs) of glucocorticoid and cyto-oxic and antiproliferative immunosuppressivegents, including 526 randomized patients, andound that with 2 surrogate criteria, such asimprovement in proteinuria” and “impairmentf renal function,” there was a tendency in favorf immunosuppressive treatment, but no effectn the 2 absolute criteria of “complete remis-ion” and “renal death.” Hogan et al6 performedpooled analysis of 35 studies of 1,815 subjects
of whom 475 were included in RCTs)8-13 onorticosteroid and alkylating therapy, combiningetrospective and prospective studies, both con-rolled and uncontrolled. Complete remission ofS was observed more frequently with the use of
lkylating agents, combining retrospective androspective studies, both controlled and uncon-rolled. Complete remission of NS was observedore frequently with the use of alkylating agents
ompared with no treatment or corticosteroids,hich were no better than no treatment. Cortico-
teroids or alkylating agents did not improveenal survival. Imperiale et al7 included 5 prospec-ive studies, 4 RCTs, and 1 non-RCT in whichytotoxic agents were compared with steroids,lacebo, or symptomatic treatment. Response toherapy was assessed by means of short-termesponses, achieving complete or partial remis-ion of proteinuria. The investigators found aeneficial effect of cytotoxic agents on these
hort-term responses among the 228 subjects hnrolled, of whom 202 were included inCTs.11-14 Conversely, they were unable to ad-ress the question of the effects of this therapyn long-term renal function.The 2 more recent meta-analyses6,7 based their
earch strategy on MEDLINE, 1968 to 1993. Byecember 15, 2003, we developed a new andpdated bibliographic search.15 This sensitivepproach allowed the identification of 1 moreelevant trial before 1994 on a comparison be-ween alkylating agents and steroids in 71 ran-omized patients16 not identified in the previouseta-analyses, 1 trial of azathioprine,17 1 trial of
lkylating agents,18 and 8 more randomized tri-ls from 1994 to December 15, 2003; 5 pub-ished19-23 as full articles and 3 published24-26 inbstract form, regarding approximately 400 moreew patients. Apart from the use of steroidslone compared with placebo or no treatment, forhich the new search strategy did not show
dditional trials since the publication of the meta-nalysis by Hogan et al,6 we considered thathere was a substantial increase in available newata for an updated systematic review of theffect of different immunosuppressive agents oneed for dialysis, death, and remission of NS, asell as on changes in 24-hour urinary protein
xcretion, glomerular filtration rate (GFR), anderum creatinine level.
METHODS
rial Inclusion CriteriaData were searched for from reports of RCTs, published
s full articles, in abstract form, or partially/totally unpub-ished, addressing the effect of immunosuppressive agentsn patients with NS. Studies should have a planned fol-ow-up of at least 6 months. Both parallel and the first periodof at least 6 months) of cross-over randomized studiesould be eligible for the review. In case of only 1 reportublished as a full article, interim data not followed by aubsequent publication were considered suitable for inclu-ion. In the case of more than 1 report published as fullrticles on the same patients, the primary reference showingnal results was chosen for the meta-analysis, excludingoth interim and follow-up reports. For results published inbstract form, the first investigator was contacted to deter-ine whether a publication was published recently, in press,
r submitted to a medical journal or, alternatively, whethernpublished material could be released for the present meta-nalysis. Because of limitations of reporting, abstract dataere included only if an implementation through additional
dequate information was provided by the investigators.The selected patients were adult subjects with IMN who
ad NS. The definition of adult was according to the single

sycchtdiree
S
DCocfRtmMmplATgcNtRfsNiap
D
JiTacbtsiwcgtfeGaa
aaatrrtAtl
rqfietmgetcrtmtCcbpssbtnrsisinucferqcbcowia
T
wac
IMMUNOSUPPRESSION IN IDIOPATHIC MEMBRANOUS NEPHROPATHY 387
tudies’ inclusion criteria: usually the cutoff value of 18ears was considered, but some trials referred to a lowerutoff value.8-10,12,22 The diagnosis of IMN was histologi-ally proven. Secondary forms of membranous nephropathyad to be excluded. NS assessment relied on that chosen byhe investigators in the single studies. It must be said that thisefinition was heterogeneous. In trials that included a minor-ty of non-nephrotic subjects, when possible, analyses wereestricted to nephrotic patients only. In the absence of anxplicit NS definition, a cutoff value for urinary proteinxcretion greater than 3.5 g/24 h was used.
earch TechniquesElectronic databases, MEDLINE, EMBASE (1966 to
ecember 15, 2003), and the Cochrane Central Register ofontrolled Trials (issue 4, 2003) were searched, regardlessf the article language, with the Cochrane Renal Group trialoordinator using the optimally sensitive strategy developedor the Cochrane Collaboration for the identification ofCTs.15 The following medical subject heading terms and
ext words were used: glomerulonephritis, membranous,embranous nephropathy, membranous glomerulopathy,GN, extramembranous glomerulopathy, membranous glo-erulonephropathy, idiopathic membranous glomerulone-
hritis, and idiopathic membranous nephropathy. Referenceists of retrieved reports were checked. Abstract books of themerican Society of Nephrology, the European Dialysis andransplantation Society, and the Gesellschaft für Nephrolo-ie (Germany, Switzerland, and Austria) were systemati-ally hand searched. Electronic search in the Journal ofephrology was supplemented by hand searching from 1989
o February 1997. Furthermore, several investigators ofCTs in the field of nephrology were contacted since 1994
or identifying planned and ongoing RCTs with the aim toet up and update a “Prospective Registry of RCTs inephrology.”27 Other sources for identifying ongoing stud-
es were the metaRegister of Current Controlled Trials Ltd28
nd The Lancet29 Web site specifically devoted to RCTrotocols.
ata CollectionThe review was undertaken by 6 reviewers (A.P., A.S.,
.Z., G.A.G., N.B., and G.R.). The search strategy wasndependently performed by 2 reviewers (A.P. and G.A.G.).wo independent reviewers (A.P. and J.Z.) inspected allrticles identified in their abstract form. For studies thatould possibly have been RCTs or in case of disagreementetween the 2 reviewers, the full article was obtained. Inurn, the same reviewers, who were not blinded to author-hip or journal, compiled an ad hoc questionnaire andndependently revised these articles. The questionnaires thenere cross-checked, and disagreements were resolved by
onsensus or with a third reviewer (A.S.). The followingeneral descriptive information was extracted from eachrial: number, age, and sex of participants; baseline renalunction evaluated by means of 24-hour urinary proteinxcretion, serum creatinine level, creatinine clearance, andFR; number of participants assigned to each intervention;
nd definite and surrogate end points. Outcomes were evalu-
ted at the last available follow-up. For articles published in tbstract form,24-26 it was possible to retrieve all relevantdditional information by contacting the first investigator25
nd considering, when available, a later publication of therial as full article.30 In 1 case,24 data from the abstracteferred to final results and therefore were used for theeview, supplemented with some unpublished material. Forhe other study,26 the abstract reported preliminary data.lthough no substantial differences occurred compared with
he subsequent unpublished data, it was decided to use theatter because it was defined “final” by the investigators.
First, trials were inspected for 3 principal aspects of theandomization process: (1) generation of allocation se-uence, (2) allocation concealment, and (3) blinding. Therst and second aspects refer to the prevention of foreknowl-dge of treatment assignment.31 The latter refers to measuresaken to mask group identity after allocation. Following theethod of Shultz et al,31 the following approaches to the
eneration of allocation sequences were considered ad-quate: computer, random number table, shuffled cards orossed coins, and minimization. The following allocationoncealment strategies were considered adequate: centralandomization; numbered or coded containers; or sequen-ially numbered, opaque, or sealed envelopes.31 Further-
ore, it was assessed whether the analysis was by intentiono treat and the completeness of follow-up. The followingochrane quality checklist was compiled: (1) allocationoncealment: adequate/unclear/inadequate; (2) blinding:linding of investigators (yes/no/not stated), blinding ofarticipants (yes/no/not stated), blinding of outcome asses-ors (yes/no/not stated), blinding of data analysis (yes/no/nottated); (3) intention-to-treat: (A) yes; specifically reportedy investigators that intention-to-treat analysis was under-aken and this was confirmed on study assessment; (B) yes;ot stated, but confirmed on study assessment; (C) no; noteported and lack of intention-to-treat analysis confirmed ontudy assessment (patients who were randomized were notncluded in the analysis because they did not receive thetudy intervention, withdrew from the study, or were notncluded because of protocol violation); (D) no; stated, butot confirmed on study assessment; and (E) not stated;nable to be determined on study assessment; and (4)ompleteness of follow-up: percentage of participants lost toollow-up or with no data for the primary outcome offfectiveness. Furthermore, 2 additional important aspectsegarding the diagnosis of IMN32 were evaluated in theuestionnaire: whether the article described the diagnosticriteria used in the trial and if the diagnosis was confirmedy using immunohistochemical microscopy or electron mi-roscopy. A recent methods meta-analysis evaluating studiesn the prognosis of IMN32 discovered that several RCTsere not of higher quality compared with some nonrandom-
zed ones. Some of the RCTs evaluated by Marx and Marx32
re included in the present review.8-10,14,33
ypes of InterventionsThe following 4 classes of immunosuppressive treatments
ere identified: (1) glucocorticoids (alone), (2) alkylatinggents (alone or in association with glucocorticoids), (3)alcineurin inhibitors (alone or in association with glucocor-
icoids), and (4) antiproliferative agents (alone).
m
wic(((tss
O
eetpsnG
rUra(p2hcIg
soc
S
rtrmdaat(vttptmwais
pFbpitbasfca
sLBCttSntadoTgttlRitrTfttacaidmacrowa
PERNA ET AL388
Control groups were administered placebo or no treat-ent other than supportive therapy.The following interventions, nonimmunologic in nature,
ere excluded: drugs aimed to reduce proteinuria throughnhibition of the renin-angiotensin system (eg, angiotensin-onverting enzyme [ACE] inhibitors), antialdosterone drugseg, spironolactone), nonsteroidal anti-inflammatory drugseg, indomethacin), and drugs aimed to correct dyslipidemiaeg, statins, diet). Conversely, it was attempted to considerhe possible confounding effect of these nonimmunosuppres-ive treatments as concomitant medications used in thetudies included in the review.
utcome MeasuresOne or more of the following outcome measures for
fficacy were considered: (1) definite end points: death ornd-stage renal failure that requires initiation of dialysisherapy or renal transplantation; and (2) surrogate end points:artial remission; complete remission; final proteinuria, mea-ured as grams of protein per 24 hours; final serum creati-ine level, measured as micromoles per minute; and finalFR, measured as milliliters per minute per 1.73 m2.We adopted the same definitions of partial and complete
emission of NS as those used by the study investigators.sually, the most frequent definitions adopted were: partial
emission, proteinuria with protein between 0.2 and 2 g/24 hnd a serum creatinine level of 2.0 mg/dL or less�180 �mol/L); and complete remission, proteinuria withrotein less than 0.2 g/24 h and a serum creatinine level of.0 mg/dL or less (�180 �mol/L). We found the definitionseterogeneous, and although this outcome measure can beonsidered an acceptable “definite” outcome measure inMN, we decided to include this outcome among “surro-ate,” and not “definite,” end points.The number of patients at risk usually was the same for
urrogate and hard end points and for safety; however,ccasionally, for the evaluation of surrogate end points (ie,omplete and/or partial remission), it may differ.
tatistical AnalysisData were quantitatively combined by 2 independent
eviewers (A.P. and G.A.G.) through a meta-analysis under-aken using Review Manager 4.2. The calculated relativeisk (RR) with 95% confidence interval (CI) for dichoto-ous data and a weighted mean difference for continuous
ata were determined. A random-effects model was used fornalyses of both dichotomous and continuous data. Addition-lly, robustness of the model chosen was evaluated by usinghe fixed-effects model. When analyzing unfavorable eventsdeath, need for dialysis therapy or transplantation, or ad-erse events), an RR less than 1 favors the experimentalreatment, whereas an RR greater than 1 favors the controlreatment. In the case of favorable events (partial or com-lete remission), an RR less than 1 favors the controlreatment, whereas an RR greater than 1 favors the experi-ental treatment. Statistical heterogeneity across studiesas explored by using chi-squared test for heterogeneity,
utomatically performed by Review Manager. Because thiss a low-power test, the � level was set at 0.10. Two main
ources of heterogeneity across trials were considered a iriori: trial quality and characteristics of study participants.urthermore, it can be argued that although recommendedy the Cochrane Collaboration, the inclusion of totally orartially unpublished material can be questionable becauset is not possible to verify unpublished trial data. To addresshis issue, studies providing partially unpublished data wereoth included and excluded for sensitivity analysis. Addition-lly, the following potential confounding factors were con-idered: inclusion/exclusion criteria regarding baseline renalunction (preserved/declining), unbalances in main baselineharacteristics, and use of concomitant medication(s), suchs ACE inhibitors or statins.
RESULTS
Figure 1 shows progress through the differenttages of this systematic review. From MED-INE, 753 citations were retrieved; from EM-ASE, 254 citations; and from the Cochraneentral Register of Controlled Trials, 60 cita-
ions. Overall, 943 potentially relevant publica-ions were identified, discarding duplications.ubsequently, 896 articles were excluded, beingonrandomized, retrospective series, review ar-icles, and so on. Forty-seven studies were evalu-ted in a closer inspection: 16 studies wereiscarded because they were non-RCTs, and 6ther RCTs were excluded34-39 (Fig 1; Table 1).wenty-five trial reports were considered eli-ible to be included in the meta-analysis: 4 ofhese subsequently were excluded, being duplica-ions or interim/early reports of main pub-ications12,40-42 (Fig 1; Table 1). Overall, 18CTs8-11,13,14,16-26,33 published as full articles or
n abstract form were identified and included inhe present review. The total number of patientsandomized in the included trials was 1,025.en studies provided data on 1 or more outcomesor the comparison between immunosuppressivereatment versus placebo or no treatment. Ofhese, 3 trials tested the effect of steroidslone8-10; 4 trials, of alkylating agents alone or inombination with steroids11,13,26,33; 1 trial, ofzathioprine17; and 3 trials, of cyclospor-ne.21,24,26 Five studies14,16,18,19,25 compared 2ifferent classes of immunosuppressive treat-ents: 4 studies evaluated the effect of adding an
lkylating agent14,16,18,19 and 1 study, of addingyclosporine,25 to therapy based on steroids. Theemaining 3 studies20,22,23 compared the effectf 2 specific immunosuppressive treatmentsithin the class of alkylating agents. Main trial
nd patient characteristics of the RCTs are listed
n Table 2. The median average follow-up period
s
IMMUNOSUPPRESSION IN IDIOPATHIC MEMBRANOUS NEPHROPATHY 389
Fig 1. Flow diagram of the
ystematic review.
r6
M
t3roir
gbapdfiuiro1
CV
iosiwcopv12ecPcog(T�o9(3u0cs
amvc
A
L
M
N
T
Y
I
P
P
P
PERNA ET AL390
eported in the trials was 24 months (range, 12 to0 months).
ethod Quality of Included Studies
Reporting of trial method details was unsatisfac-ory and incomplete for the majority of trials (Table). Nine9-11,14,17,22,24-26 of the 18 studies includedeported, or additional information was provided,n adequate allocation concealment. In the remain-ng 9 trials, it was reported that the trial was
Table 1. Excluded Studies
Study Identification Reason for Exclusion
mbalavanan et al34 Randomized crossover study ofcyclosporine v ACE inhibitor;excluded because the firstcrossover period was � 6 mo(3 mo)
agrue et al35 RCT of chlorambucil,azathioprine, and placebo,excluded because it waspossible to isolate the NSsubgroup for 1 of thetreatment groups only
edical ResearchCouncil WorkingParty36
RCT; excluded because it wasnot possible to identifypatients with NS
and et al37 RCT; excluded because it wasnot possible to identifypatients with NS
ejani et al38 RCT; excluded because allparticipants were children
ao et al39 RCT; excluded because thecontrol group wasadministered ACE inhibitor
mbasciati et al40 RCT; excluded because it wasan early report of Ponticelli,198933
onticelli et al41 RCT; excluded because it wasan early report of Ponticelli,198933
onticelli et al12 RCT; although at first sight, thisreport seemed to be theprimary reference, Ponticelli,1989,33 reported morecomplete results with anincreased number of patientsof the same protocol;therefore, Ponticelli, 1984,12
was considered an interimanalysis of Ponticelli, 198933
onticelli et al42 RCT; this is a longer follow-upreport corresponding to thePonticelli 198933 study
andomized, but no information on the method was d
iven. Three trials8,9,17 only reported blinding ofoth investigators and participants. Three tri-ls11,24,26 reported, or additional information wasrovided, on the blinding of outcome assessors orata analysts. Intention-to-treat analysis was con-rmed in 7 trials,9,10,14,17,20,24,33 whereas it was notndertaken in 6 trials11,13,16,22,23,26 and was unclearn the remaining 5 trials.8,18,19,21,25 Informationegarding completeness of follow-up was reportedr deducible in all trials, ranging from 81% to00%.
omparison of Immunosuppressive Regimensersus Placebo or No Treatment
We analyzed the efficacy of all combinedmmunosuppressive regimens versus placebor no treatment. Some unbalances were ob-erved in the proportion of males, serum creat-nine levels, and proteinuria at randomization,hich were greater in the treatment versus
ontrol groups. Fourteen deaths and 49 casesf end-stage renal failure were reported. Sevenatients died in the immunosuppressive groupsersus 7 patients in the control groups (RR,.00; 95% CI, 0.34 to 2.90; P � 0.99), whereas3 patients required dialysis therapy in thexperimental group versus 26 patients in theontrol group (RR, 0.74; 95% CI, 0.38 to 1.44;
� 0.37). Overall, 30 patients reached theombined end point of death, dialysis therapy,r transplantation in the immunosuppressiveroups versus 32 patients in the control groupsRR, 0.82; 95% CI, 0.49 to 1.40; P � 0.47).here was no heterogeneity between trials (P0.38; Fig 2). No significant differences were
bserved in the number of partial (RR, 1.25;5% CI, 0.83 to 1.88; P � 0.29), completeRR, 1.36; 95% CI, 0.82 to 2.24; P � 0.23; Fig), or complete or partial remissions of protein-ria (RR, 1.30; 95% CI, 0.86 to 1.96; P �.21), as far as in final proteinuria, final serumreatinine level, and final GFR (data nothown).
There were 17 discontinuations caused bydverse events in immunosuppressive treat-ent. The most frequently experienced ad-
erse events were leukopenia (5 events),ushingoid features (5 events), and gastric
isorders (2 events).
I
T
T
IMMUNOSUPPRESSION IN IDIOPATHIC MEMBRANOUS NEPHROPATHY 391
Table 2. Summary of Included Studies
ReferenceNo. of
Patients
MeanFollow-Up
(mo)
Mean Age atRandomization
(y)Sex
(% men)
Declining RenalFunction atBaseline
Use of ACE InhibitorsDuring Follow-Up
mmunosuppressivetreatment v notreatment
Steroids v no treatmentCameron et al9 103 52 45 84 No Not mentionedCattran et al10 158 48 45 66 No Not mentionedCoggins8 72 23 39 58 No Not mentioned
Alkylating agents v notreatment
Braun et al26 53 60 44 72 No Yes, no confounding effectDonadio et al11 22 12 44 77 No Not mentionedMurphy et al13 40 24 43 65 No Not mentionedPonticelli et al33 81 60 43 78 No Not mentioned
Cyclosporine v notreatment
Braun et al*26 66 60 44 52 No Yes, no confounding effectCattran et al21 17 21 42 82 Yes Yes, no confounding effectPisoni et al*24 21 12 49 81 Yes Yes, no confounding effect
Azathioprine v notreatment
Silverberg17 9 12 43 67 No Not mentionedwo different classes of
immunosuppressivetreatments
Steroids v alkylatingagents
Ahmed et al19 20 15 35 80 No Not mentionedFalk et al18 26 24 45 62 Yes Yes, no confounding effectPahar et al16 71 46 34 69 No Not mentionedPonticelli et al14 92 48 47 64 No Not mentioned
Cyclosporine v steroidsCattran et al25 51 18 48 82 No Yes, no confounding effect
Cyclosporine valkylating agents
Braun et al*26 75 60 43 61 No Yes, no confounding effectwo different
immunosuppressivetreatments withinthe same class
Chlorambucil vcyclophosphamide
Branten et al20 32 26 52 94 Yes Not mentionedPonticelli et al22 95 36 49 69 No Discouraged, but not
prohibited; noconfounding effect
Reichert23 18 12 47 94 Yes Yes, no confounding effect
*Partially unpublished data provided by the study investigators.
CIP
sgwat
sw0a9c9wh
ua
c
ot(Cr09fs
e
e
CI
psas
ABBCCCCCDFMPPPPPRS
aoa
PERNA ET AL392
omparison of Each Class ofmmunosuppressive Regimen Versuslacebo or No Treatment
Baseline serum creatinine level was greater interoid-treated patients compared with controlroups, whereas increased baseline proteinuriaas observed in groups treated with alkylating
gents or cyclosporine versus placebo or noreatment.
No beneficial effect on total mortality or end-tage renal failure was observed in patients treatedith glucocorticoids (combined end point: RR,.88; 95% CI, 0.39 to 1.97; P � 0.75; Fig 2),lkylating agents (combined end point: RR, 0.56;5% CI, 0.18 to 1.70; P � 0.3; Fig 2), oryclosporine (combined end point: RR, 0.93;5% CI, 0.32 to 2.71; P � 0.89; Fig 2) comparedith placebo or no treatment. There was noeterogeneity between trials.There were no deaths or end-stage renal fail-
re within the trial period in the only trial ofzathioprine.
Glucocorticoids had no effect on partial or
Table 3. Quality Asse
ReferenceAllocation
ConcealmentBlinding of
Investigators
hmed et al19 Not stated Not statedranten et al20 Not stated Not statedraun et al26 Adequate Noameron et al9 Adequate Yesattran et al10 Adequate Noattran et al21 Not stated Noattran et al25,30 Adequate Nooggins et al,8 1979 Not stated Yesonadio et al,11 1974 Adequate Noalk et al,18 1992 Not stated Not statedurphy et al,13 1992 Not stated Not statedahari et al,16 1993 Not stated Not statedisoni et al,24 2000 Adequate Noonticelli et al,33 1989 Not stated Noonticelli et al,14 1992 Adequate Noonticelli et al,22 1998 Adequate Noeichert et al,23 1994 Not stated Not statedilverberg et al,17 1976 Adequate Yes
Abbreviation: ITT, intention to treat.*1 � yes, specifically reported by investigators that IT
ssessment; 2 � yes, not stated, but confirmed on study asn study; 4 � no, stated, but not confirmed on study asssessment.
omplete remission. w
Alkylating agents showed a significant effectn complete remission (RR, 2.37; 95% CI, 1.32o 4.25; P� 0.004; Fig 3) and final proteinuriaweighted mean difference, �2.36 g/24 h; 95%I, �4.27 to �0.46; P � 0.02), but not on partial
emission (RR, 1.22; 95% CI, 0.63 to 2.35; P �.56) or complete or partial remission (RR, 1.55;5% CI, 0.72 to 3.34; P � 0.27). Final renalunction was similar in the 2 groups (data nothown).
In cyclosporine-treated patients, no beneficialffect was observed.
The only trial of azathioprine showed no differ-nce for any of the chosen end points.
omparison of 2 Different Classes ofmmunosuppressive Regimens
Information was available for 3 kinds of com-arisons: steroids versus alkylating agents, cyclo-porine versus steroids, and cyclosporine versuslkylating agents. Baseline characteristics wereimilar.
For each of the 3 comparisons, no clear effect
t of Included Studies
ofnts
Blinding ofOutcome
Assessor(s)
Blinding ofData
AnalysisITT
Analysis*n/N Lost toFollow-Up
ted Not stated Not stated 5 0/20ted Not stated Not stated 2 0/32
No No 3 18/97Not stated Not stated 1 7/103Not stated Not stated 1 27/158Not stated Not stated 5 0/17Not stated Not stated 5 2/51Not stated Not stated 5 5/72No No 3 3/22
ted Not stated Not stated 5 2/26ted Not stated Not stated 3 1/40ted Not stated Not stated 3 10/71
No No 1 1/21Not stated Not stated 1 3/81Not stated Not stated 1 1/92Not stated Not stated 3 5/95
ted Not stated Not stated 3 0/18Not stated Not stated 2 0/9
lysis was undertaken, and this was confirmed on studynt; 3 � no, not reported and lack of ITT analysis confirmedent; 5 � not stated, unable to be determined on study
ssmen
BlindingParticipa
Not staNot staNoYesNoYesYesYesNoNot staNot staNot staNoNoNoNoNot staYes
T anasessmesessm
as seen as far as hard end points are concerned.

IMMUNOSUPPRESSION IN IDIOPATHIC MEMBRANOUS NEPHROPATHY 393
Fig 2. Outcome: end-stage renal failure or death.

PERNA ET AL394
Fig 3. Outcome: complete remission.

ttRodccdin
scP0
qtP0
C
apncntacslsdpa4wtc
S
smcpwi
intwacwfaet
btqpaittosFporeoss
aioswaLtsatnsrrscca
IMMUNOSUPPRESSION IN IDIOPATHIC MEMBRANOUS NEPHROPATHY 395
Alkylating agents induced more remissionshan steroids (complete: RR, 1.89; 95% CI, 1.34o 2.67; P � 0.0003; Fig 3; complete or partial:R, 1.45; 95% CI, 1.16 to 1.81; P � 0.001). Thenly trial reporting adverse events14 showed 4iscontinuations caused by adverse events, in-luding leukopenia, pneumonia, and gastric dis-omfort, in the alkylating-agent group versus 1iscontinuation caused by renal vein thrombosisn the steroid-treated group. This difference wasot statistically significant.
Cyclosporine induced more remissions thanteroids, which did not reach statistical signifi-ance (partial: RR, 3.70; 95% CI, 0.89 to 15.44;� 0.07; complete or partial: RR, 3.01; 95% CI,
.95 to 9.52; P � 0.06).Similarly, partial remissions were more fre-
uent with cyclosporine than alkylating agentherapy (partial: RR, 1.68; 95% CI, 1.06 to 2.65;� 0.03; complete or partial: RR, 1.46; 95% CI,
.97 to 2.20; P � 0.07).
omparison of 2 Alkylating Agents
We compared the relative efficacy of the 2lkylating agents, chlorambucil versus cyclophos-hamide. Proportions of males and baseline re-al function were similar. There was no signifi-ant difference in the incidence of death andeed for dialysis therapy or transplantation or inhe combined end point. Within the class oflkylating agents, there were no differences foromplete, partial, or complete or partial remis-ion or for final proteinuria, serum creatinineevel, or GFR. Cyclophosphamide treatment re-ulted in a statistically significantly lower rate ofiscontinuations caused by adverse events com-ared with chlorambucil (8 versus 21 discontinu-tions, respectively; RR, 2.34; 95% CI, 1.25 to.39; P � 0.008; Fig 4). Three discontinuationsere caused by leukopenia in cyclophosphamide-
reated patients versus 14 discontinuations in thehlorambucil group.
ensitivity Analysis
To assess the robustness of meta-analytic re-ults, a sensitivity analysis was conducted. Twoain sources of heterogeneity across trials were
onsidered: trial quality and characteristics ofarticipating patients. First, it was performedith the analysis excluding trials providing no
nformation on allocation concealment and blind- i
ng.13,16,18-20,23 This first sensitivity analysis didot substantially change the results referred tohe analyses versus no treatment. Modificationsere noted for the comparison of steroids versus
lkylating agents. The statistically significant in-rease in complete or partial remissions observedith alkylating agent therapy was not sustained
urther after the exclusion of trials by Ahmed etl19 and Pahari et al.16 Such discrepancy can bexplained because of the reduced power to detecthe difference (42% and 16%, respectively).
It can be argued that although recommendedy the Cochrane Collaboration, inclusion of to-ally or partially unpublished material can beuestionable because data from abstracts and notublished data were not subject to peer reviewnd validation. To address this issue, the 2 stud-es24,26 that provided unpublished data in addi-ion to those published were excluded for sensi-ivity analysis. No significant changes werebserved for the comparison of immunosuppres-ive treatment versus placebo or no treatment.or the comparison of alkylating agents versuslacebo or no treatment, by excluding the studyf Braun et al,26 the difference in completeemissions was magnified. This can be consid-red an example of publication bias.43 No changesccurred for the comparison of cyclosporine ver-us placebo or no treatment after exclusion of thetudy by Pisoni et al.24
It was found that baseline renal function evalu-ted by serum creatinine level differed across stud-es. Therefore, inclusion and/or exclusion criteriaf the studies were checked to assess whether theyystematically varied. Some trials included patientsith particularly well-preserved renal function (ie,
verage serum creatinine � 1.1 mg/dL [97 �mol/]). It was decided to exclude this kind of
rial.14,22,33 This approach resulted in several sub-tantial changes. When reanalyzing the effect oflkylating agents versus placebo or no treatment,he difference in rates of complete remission waso more statistically significant. Conversely, exclu-ion of trials with inclusion and/or exclusion crite-ia leading to the enrollment of patients with worseenal function18,20,21,23,24 did not change the re-ults. It was thought that an additional potentialonfounding factor can be represented by the use ofoncomitant medication, such as ACE inhibitorsnd/or statins.Afew more recent trials reported this
nformation (Table 1). It therefore was considered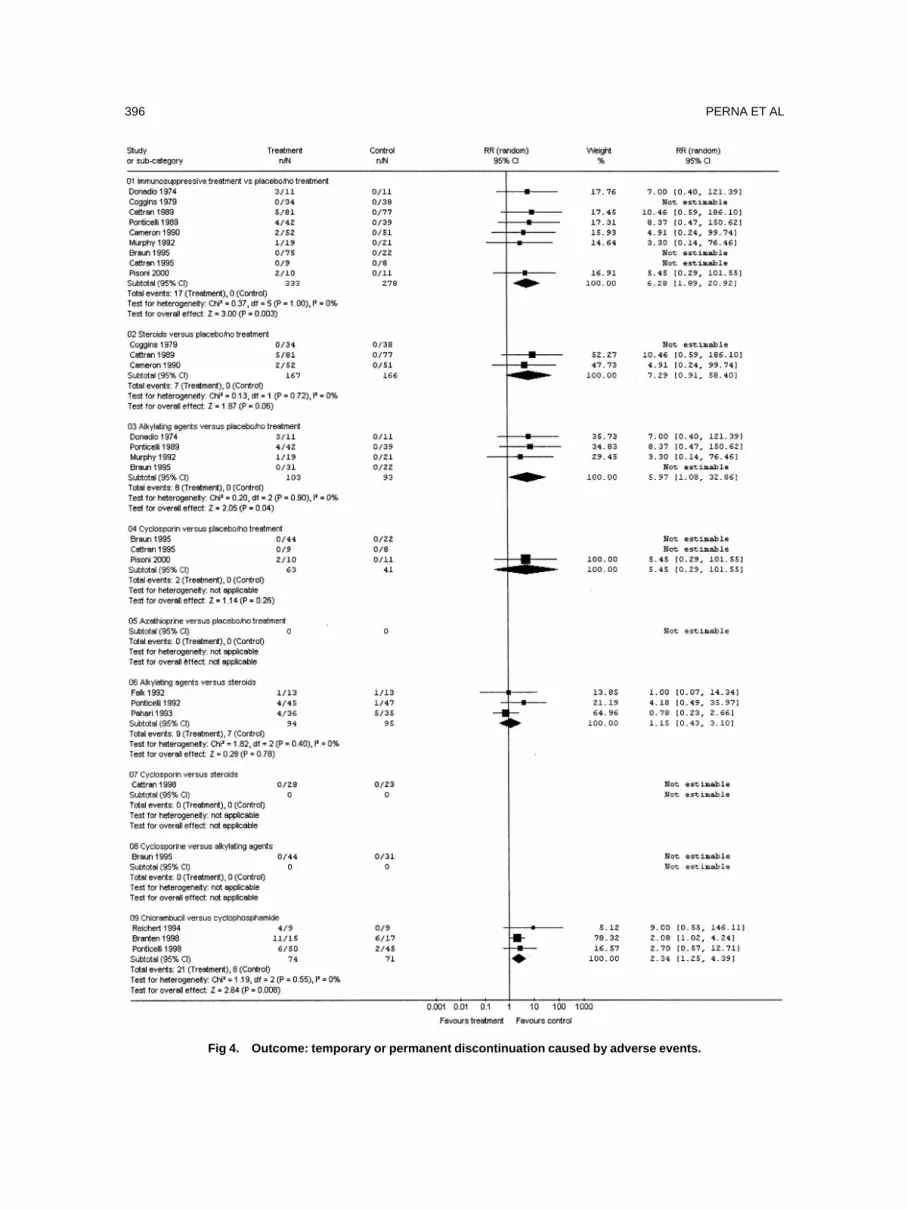
PERNA ET AL396
Fig 4. Outcome: temporary or permanent discontinuation caused by adverse events.

tsdanetticnomtaa
Iin
Iscsanal
enwapt
igtttwgpoitT
sMbpcgoito2cpcpnpwiapsoC“pacn
tqowaupuhmmde
isrt
o
IMMUNOSUPPRESSION IN IDIOPATHIC MEMBRANOUS NEPHROPATHY 397
hat an additional source of heterogeneity can beeen in the time frame of the study. It is alwaysifficult to define a clear cutoff value, but it iscceptable to identify the turning point in the semi-al observation of Lewis et al44 on the beneficialffect of ACE inhibition, published in 1993. Afterhis date, use of this important concomitant medica-ion is discussed and, relying on the assessment ofnvestigators, no major confounding effect oc-urred. In 1 case, only a publication after 1993 didot mention the use of ACE inhibitors20: removalf this study did not affect the results. It is muchore difficult to identify a similar cutoff value for
he use of statins. Few studies are available45,46 andre too recently published to allow meaningfulnalyses.
DISCUSSION
Objectives of this review of the treatment ofMN are to address the important question, whichs controversial in nephrology, of whether immu-osuppressive treatment is effective and safe.There is weak evidence that in patients with
MN and NS, treatment with an immunosuppres-ive regimen may be associated with an in-reased rate of remission. The safety of immuno-uppressive treatments must be taken intoccount. Meta-analysis showed a statistically sig-ificant number of discontinuations caused bydverse events in the treatment group, mainlyeukopenia and cushingoid features.
The meta-analysis has been unable to show anffect of immunosuppression on mortality andeed for dialysis therapy. Responses to treatmentere observed in relatively short-term studies
nd with a low incidence of these events, whichossibly prevented an observation of an effect onhese definite end points.
We attempted to minimize publication bias,ncluding unpublished data and non–English lan-uage sources, and by inspecting prospectiverial registries. Six ongoing and/or unpublishedrials were identified.47-52 Through the Prospec-ive Registry,27 we knew that Stegeman et al47
ere performing a trial (group I, ACE inhibitor;roup II, prednisolone; group III, control; totalrojected sample size, 150 patients), the protocolf which was published in 1994 before random-zation of the first patient. However, no addi-ional information was available for this trial.
28
hrough Current Controlled Trials and per- bonal communication, we became aware thatathieson et al of the University of Bristol, on
ehalf of the UK Renal Association, are studyingatients with declining renal function (20% de-line in GFR). Patients are randomized to 1 of 3roups: cyclosporine versus alternating monthsf prednisolone and chlorambucil versus support-ve therapy. The aim is to include 120 patients inotal (40 patients in each group). Another recentngoing National Institutes of Health study is a4-week, randomized, double-blind, placebo-ontrolled trial of the effect of a new immunosup-ressive drug, a genetically engineered antibodyalled h5G1.1-mAb, in reducing proteinuria inatients with IMN.48 Another study of pred-isone alone versus prednisone plus cyclophos-hamide versus prednisone plus cyclosporineas mentioned by Austin et al.49,50 No additional
nformation could be retrieved. A study by Jha etl51 has a pending classification: it is an RCTerformed in 89 subjects on the comparison ofteroids versus cyclophosphamide. Finally, an-ther ongoing trial was identified through theochrane renal group, in which “early” versusrescue” immunosuppressive therapy (cyclophos-hamide plus steroids) were compared.52 It wasttempted to examine the possible role of publi-ation bias by using funnel plots, but an adequateumber of RCTs cannot be identified.
Are there treatments among those consideredo be definitely discarded? The answer to thisuestion can be given mainly by comparing eachf the identified immunosuppressive regimensith placebo or no treatment. The role of steroids
lone, evaluated in 3 old RCTs,8-10 remains highlyncertain for both definite and surrogate endoints. Overall, this kind of therapy at the sched-les used in the trials included in the review (ie,igh-dose short-term or moderate doses for 6onths) fails to show a beneficial effect. Further-ore, the meta-analysis showed a greater inci-
ence of discontinuations caused by adversevents found under steroids.
Even data for azathioprine were not promis-ng, but it must be said that results relied on aingle trial17 that enrolled only 9 patients overall,esulting in lack of power to detect even impor-ant differences.
Clear indication on the use of a specific kindf treatment should be based on definite unam-
iguous end points, such as death or need for
dubq
pcfitTlttwcchdanw
ribitcitadnbpcoaro
epa
ssdtsc
ttce
aunittihpsaAp
bcvdor
swtpcwpdm
msdrmrramm
Idr
PERNA ET AL398
ialysis therapy.32 Complete remission of protein-ria could not be considered a hard end pointecause it was not always sustained and fre-uently was followed by relapses.32
There is evidence based on surrogate endoints that alkylating agents significantly in-reased the number of remissions and decreasednal proteinuria compared with placebo or no
reatment or in comparison with steroids alone.hese results can represent the premises for
ong-term well-designed studies of this kinds ofreatment. Among alkylating agents, there was aendency of cyclophosphamide to be associatedith fewer adverse effects compared with
hlorambucil. However, this does not mean thatyclophosphamide can be considered a safe agent,aving much toxicity. For patients with rapidlyeteriorating renal function, salvage therapy withlkylating agents may be useful, although it isot yet clear how long this salvage therapyould keep the patient off dialysis therapy.These conclusions, which confirmed previous
esults observed in a pooled analysis of random-zed and nonrandomized studies,53 are weakenedy the lack of robustness arisen after the sensitiv-ty analysis. Particularly, it was shown that 1 ofhe sources of heterogeneity found across studiesan be identified in the different degree of renalmpairment of patients at the time of randomiza-ion. Substituting 1989 data from Ponticelli etl33 with those from the 10-year follow-up42
eserves an additional comment. This change didot substantially affect the overall comparisonetween all immunosuppressive treatments withlacebo or no treatment. When focusing on thelass of alkylating agents, evidence of a tendencyf improvement in renal survival under treatmentrose. The selection of this longer follow-upeport likely accounted for an additional amountf variability.In the present review, no remarkable differ-
nces were observed between cyclosporine andlacebo. This information was based on 3 tri-ls21,24,26 involving 104 randomized patients.
Although Cattran et al25,30 reported that cyclo-porine induced more partial remissions thanteroids, and Braun, in his partially unpublishedata, showed that cyclosporine also was superioro alkylating agents in increasing partial remis-ions, it must be said that the superiority of
yclosporine in comparison to placebo or no treatment cannot be clearly shown. Furthermore,hese results arose from only a single study andonsequently need to be proven by additionalvidence.
Although it was not possible to adequatelyddress the possible confounding effect of these of ACE inhibitors and/or statins, it likely didot have a major role because studies not report-ng this information were randomized. This sys-ematic review, focusing on immunosuppressiveherapy, did not investigate the role of ACEnhibitors. However, the importance of ACE in-ibitors in reducing proteinuria and delaying therogression of renal disease should be empha-ized. Conversely, it is unlikely their role will bessessed in a specifically designed trial becauseCE inhibitors are administered routinely to allroteinuric patients, including those with IMN.We decided to perform a review addressing
roadly focused questions. Because of the pau-ity of trials, subgroup analyses allowing forariations in interventions; ie, different doses,ifferent routs of administration, different lengthsf follow-up, and in populations, ie, differentaces, cannot be carried out.
Furthermore, when interpreting study results,ome unbalances in baseline characteristics,hich occurred for some comparisons, should be
aken into account. Particularly, because level ofroteinuria is known to be a predictor of out-ome, it can be of relevance that patients treatedith alkylating agents or cyclosporine had greaterroteinuria than controls: this could have in-uced a bias against seeing an effect of treat-ent.The underlying pathogenic mechanism(s) ofembranous nephropathy should be better under-
tood to allow the discovery of new selectiverugs for the treatment of this condition. Veryecently, the safety and efficacy profile of aonoclonal antibody to B-cell antigen CD-20,
ituximab, was evaluated,54,55 giving favorableesults to be studied further. Encouraging resultslso were reported with adrenocorticotropic hor-one,56 pentoxiphylline,57 and mycophenolateofetil.58
The meta-analyses of Couchoud et al5 andmperiale et al7 suggest the need for well-esigned RCTs of the long-term benefits andisks in the categories of agents considered in
6
heir articles. Hogan et al emphasized the impor-
thfoenoetisRcbtim
tthachwicacsta
m
uN
hb1
g
m4
ol
am5
Itp
spn
im
Cn
tp9
Pfl
IGwp6
st
aP
nng
oM
pnn5
Jtr
tm
ssp4
R
IMMUNOSUPPRESSION IN IDIOPATHIC MEMBRANOUS NEPHROPATHY 399
ance of identifying patients who are likely toave progressive disease and who may benefitrom treatment, understanding the contributionf prognostic variables in the long term. Hogant al6 concluded that “we must await an era ofew therapeutic agents that interfere with etiol-gy or pathogenesis of this disease before a trulyffective therapy is available.” Nine years afterhis report, there is still high uncertainty regard-ng the beneficial effect of these immunosuppres-ive agents, even after increasing the number ofCTs available. This remarkable finding indi-ates that the conclusions of Hogan et al6 possi-ly also apply 9 years later. It therefore is manda-ory to confirm the encouraging results observedn novel alternative immunosuppressive regi-ens by means of well-designed RCTs.
ACKNOWLEDGMENTThis systematic review was prepared under the aegis of
he Cochrane Collaboration, an international organizationhat aims to help people make well-informed decisions aboutealth care by preparing, maintaining, and promoting theccessibility of systematic reviews of the effects of healthare interventions. The authors thank Lisa A. Tjosvold, whoelped perform the electronic search; Luciana Tammuzzo,ho hand searched the Journal of Nephrology; and principal
nvestigators who provided additional information or clarifi-ation (Daniel C. Cattran, Peter Mathieson, Roberto Pisoni,nd Teut Risler); Ruth Mitchell, the Cochrane Trials Searchoordinator who provided us with the Cochrane libraryearch strategy and relevant information; and Narelle Willis,he Cochrane Renal Review Group coordinator, for her helpnd support.
REFERENCES1. Cameron JS: Membranous nephropathy and its treat-ent. Nephrol Dial Transplant 7:S72-S79, 1992 (suppl 1)2. Schieppati S, Mosconi L, Perna A, et al: Prognosis of
ntreated patients with idiopathic membranous nephropathy.Engl J Med 329:85-89, 19933. Honkanen E, Tornroth T, Grohagen-Riska C: Natural
istory, clinical course and morphological evolution of mem-ranous nephropathy. Nephrol Dial Transplant 7:S35-S41,992 (suppl 1)4. Glassock RJ: The therapy of idiopathic membranous
lomerulonephritis. Semin Nephrol 11:138-147, 19915. Couchoud C, Laville M, Boissel JP: Treatment ofembranous nephropathy. Nephrol Dial Transplant 9:469-
70, 19946. Hogan SL, Muller KE, Jennette JC, Falk RJ: A review
f therapeutic studies of idiopathic membranous glomeru-opathy. Am J Kidney Dis 25:862-875, 1995
7. Imperiale TF, Goldfarb S, Berns JS: Are cytotoxicgents beneficial in idiopathic membranous nephropathy? Aeta-analysis of the controlled trials. J Am Soc Nephrol
:1553-1558, 1995 w
8. Coggins CH, for the Collaborative Study of the Adultdiopathic Nephrotic Syndrome: A controlled study of short-erm prednisone treatment in adults with membranous ne-hropathy. N Engl J Med 301:1301-1306, 19799. Cameron JS, Healy MJR, Adu D: The Medical Re-
earch Council trial of short-term high-dose alternate dayrednisolone in idiopathic membranous nephropathy withephrotic syndrome in adults. Q J Med 274:133-156, 199010. Cattran DC, Delmore T, Roscoe J, et al: A random-
zed controlled trial of prednisone in patients with idiopathicembranous nephropathy. N Engl J Med 320:210-215, 198911. Donadio JV, Holley KE, Anderson CF, Taylor WF:
ontrolled trial of cyclophosphamide in idiopathic membra-ous nephropathy. Kidney Int 6:431-439, 197412. Ponticelli C, Zucchelli P, Imbasciati E, et al: Con-
rolled trial of methylprednisolone and chlorambucil in idio-athic membranous nephropathy. N Engl J Med 310:946-50, 198413. Murphy BF, McDonald I, Fairley KF, Kincaid-Smith
S: Randomised controlled trial of cyclophosphamide, war-arin and dipyridamole in idiopathic membranous glomeru-onephritis. Clin Nephrol 37:229-234, 1992
14. Ponticelli C, Zucchelli P, Passerini P, Cesana B,talian Idiopathic Membranous Nephropathy Treatment Studyroup: Methylprednisolone plus chlorambucil as comparedith methylprednisolone alone for the treatment of idio-athic membranous nephropathy. N Engl J Med 327:599-03, 199215. Robinson KA, Dickersin K: Development of a highly
ensitive search for the retrieval of reports of controlledrials using PubMed. Int J Epidemiol 31:150-153, 2002
16. Pahari DK, Das S, Dutta BN, Banerjee D: Prognosisnd management of membranous nephropathy. J Assochysicians India 41:350-351, 199317. Silverberg DS, for the Western Canadian Glomerulo-
ephritis Study Group: Controlled trial of azathioprine in theephrotic syndrome secondary to idiopathic membranouslomerulonephritis. CMAJ 115:1209-1210, 197618. Falk RJ, Hogan SL, Muller KE, Jenette C: Treatment
f progressive membranous glomerulopathy. Ann Interned 116:438-445, 199219. Ahmed S, Rahman M, Alam MR, et al: Methyl
rednisolone plus chlorambucil as compared with pred-isolone alone for the treatment of idiopathic membranousephropathy. A preliminary study. Bangladesh Ren J 13:51-4, 199420. Branten AJW, Reichert LJM, Koene RAP, Wetzels
FM: Oral cyclophosphamide versus chlorambucil in thereatment of patients with membranous nephropathy andenal insufficiency. Q J Med 91:359-366, 1998
21. Cattran DC, Greenwood C, Ritchie S, et al: A con-rolled trial of cyclosporine in patients with progressiveembranous nephropathy. Kidney Int 47:1130-1135, 199522. Ponticelli C, Altieri P, Scolari F, et al: A randomized
tudy comparing methylprednisolone plus chlorambucil ver-us methylprednisolone plus cyclophosphamide in idio-athic membranous nephropathy. J Am Soc Nephrol 9:444-50, 199823. Reichert LJM, Husmans FTM, Assmann K, Koene
AP, Wetzels JFM: Preserving renal function in patients
ith membranous nephropathy: Daily oral chlorambucil
cc
imfN
cra
nfN
t
oc
wN
it
Acj
nI
ip1
Mm1
Tgt
tB
mp1
cvd
tM
lnc2
tcE
fa4
t1
CcN
cna
St1
ianm7
Kprnn2
M
Rnp
VpJ
imN
mO
PERNA ET AL400
ompared with intermittent monthly pulses ofyclophosphamide. Ann Intern Med 121:328-333, 1994
24. Pisoni R, Grinyo JM, Salvadori M, et al: Cyclospor-ne versus conservative therapy in patients with idiopathicembranous nephropathy (IMN) and deteriorating renal
unction: Results of the CYCLOMEN trial. J Am Socephrol 11:95A, 2000 (abstr)25. Cattran DC, Pohl M, Maxwell D, et al: Randomized
ontrolled trial of cyclosporine (D) vs. placebo (P) in steroidesistant, nephrotic patients (NS) with membranous nephrop-thy (SR MGN). J Am Soc Nephrol 9:85A, 1998 (abstr)
26. Braun N, Erley C, Benda N, et al: Therapy of membra-ous glomerulonephritis with nephrotic syndrome. 5 Yearsollow-up of a prospective, randomised multi-centre study.ephrol Dial Transplant 10:967, 1995 (abstr)27. Tognoni G, Mallick N: (Another) registry of clinical
rials? J Nephrol 6:117, 199328. Current Controlled Trials Ltd. The metaRegister
f Controlled Trials (mRCT). Available at: http://www.ontrolled-trials.com. Accessed: November 24, 2003
29. Protocol Review, The Lancet. Available at: http://ww.thelancet.com/authorinfo/Protocol�review. Accessed:ovember 24, 200330. Cattran DC, Appel GB, Hebert LA, et al: Cyclospor-
ne in patients with steroid-resistant membranous nephropa-hy: A randomised trial. Kidney Int 59:1484-1490, 2001
31. Schulz KF, Chalmers I, Grimes DA, Altman DG:ssessing the quality of randomization from reports of
ontrolled trials published in obstetrics and gynecologyournals. JAMA 272:125-128, 1994
32. Marx BE, Marx M: Prognosis of idiopathic membra-ous nephropathy: A methodologic meta-analysis. Kidneynt 51:873-879, 1997
33. Ponticelli C, Zucchelli P, Passerini P, et al: A random-zed trial of methylprednisone and chlorambucil in idio-athic membranous nephropathy. N Engl J Med 320:8-13,98934. Ambalavanan S, Fauvel J-P, Sibley RK, Myers BD:echanism of the antiproteinuric effect of cyclosporine inembranous nephropathy. J Am Soc Nephrol 7:290-298,
99635. Lagrue G, Bernard D, Bariety J, Druet P, Guenel J:
raitement par le chlorambucil et l’azathioprine dans leslomérulonéphrites primitives: Résultats d’une étude “con-rolée”. J Urol Nephrol 1975;81:655-672.
36. Medical Research Council Working Party: Controlledrial of azathioprine and prednisone in chronic renal disease.r Med J 2:239-241, 197137. Nand N, Das R, Jaswal TS: Evaluation of efficacy ofethylprednisolone, prednisolone and chlorambucil in idio-
athic glomerulonephritis. J Indian Med Assoc 95:163-165,99738. Tejani A, Suthanthiran M, Pomrantz A: A randomized
ontrolled trial of low-dose prednisone and cyclosporinersus high-dose prednisone in nephrotic syndrome of chil-ren. Nephron 59:96-99, 199139. Yao X, Chen H, Wang Q, et al: Cyclosporin A
reatment for idiopathic membranous nephropathy. Chin
ed J 114:1305-1308, 200140. Imbasciati E, Cagnoli L, Case N, et al: Studio control-ato di un trattamento a mesi alterni di steroidi e clorambucilella nefropatia membranosa e nella glomerulosclerosi fo-ale. Valutazione preliminare dei risultati. Minerva Nefrol7:571-575, 198041. Ponticelli C, Zucchelli P, Imbasciati E, et al: Con-
rolled trial of monthly alternated courses of steroid andhlorambucil for idiopathic membranous nephropathy. Procur Dial Transplant Assoc 19:717-723, 198342. Ponticelli C, Zucchelli P, Passerini P, et al: A 10-year
ollow-up of a randomized study with methylprednisolonend chlorambucil in membranous nephropathy. Kidney Int8:1600-1604, 199543. Dickersin K, Min YI: NIH clinical trials and publica-
ion bias. On-line J Curr Clin Trials [serial on line]. Apr 28,993; doc 5044. Lewis EJ, Hunsicker LG, Bain RP, Rohde RD, for the
ollaborative Study Group: The effect of angiotensin-onverting-enzyme inhibition on diabetic nephropathy.Engl J Med 329:1456-1462, 199345. Rayner BL, Byrne MJ, van Zyl Smit R: A prospective
linical trial comparing the treatment of idiopathic membra-ous nephropathy and nephrotic syndrome with simvastatinnd diet, versus diet alone. Clin Nephrol 46:219-224, 1996
46. Olbricht CJ, Wanner C, Thiery J, Basten A, for theimvastatin in Nephrotic Syndrome Study Group: Simvasta-
in in nephrotic syndrome. Kidney Int Suppl 71:S113-S116,99947. Stegeman CA, De Zeeuw D, De Jong PE: A random-
zed multicentre trial to compare the effect of symptomaticntiproteinuric treatment with an ACE inhibitor to an immu-osuppressive regimen with corticosteroids and of no treat-ent on the course of membranous nephropathy. J Nephrol
:294-300, 199448. National Institute of Diabetes and Digestive and
idney Diseases: A phase II randomized, double-blind,lacebo-controlled study of the effect of h5G1.1-mAb on theeduction of proteinuria in patients with idiopathic membra-ous glomerulopathy. Available at: http://clinicalstudies.info.ih.gov/detail/A_2000-DK-0126.html. Accessed: June 29,00149. Austin AH: Membranous nephropathy. Ann Interned 116:672-682, 199250. Austin AH, Vaughan EM, Boumpas DT, Balow JE:
andomized trial of pulse cyclophosphamide and pred-isone vs. prednisone alone in idiopathic membranous ne-hropathy. J Am Soc Nephrol 7:1327, 1996 (abstr)51. Jha V, Kohli HS, Sud K, Gupta KL, Joshi K, Sakhuja
: A randomized controlled trial of steroids and cyclophos-hamide in adults with idiopathic membranous nephropathy.Am Soc Nephrol 213A, 2001 (abstr)52. Branten AJ, du Buf Vereijken PW, Wetzel JF: Defin-
ng the optimal time of treatment start in patients withembranous nephropathy: A randomized study. J Am Socephrol 668A, 2002 (abstr)53. Schieppati A, Perna A, Remuzzi G: Recent develop-ents in the management of membranous nephropathy. Exppin Invest Drugs 6:521-532, 1997

Bm
ip
e
uK
p1
l
IMMUNOSUPPRESSION IN IDIOPATHIC MEMBRANOUS NEPHROPATHY 401
54. Remuzzi G, Chiurchiu C, Abbate M, Brusegan V,ontempelli M, Ruggenenti P: Rituximab for idiopathicembranous nephropathy. Lancet 360:923-924, 200255. Ruggenenti P, Chiurchiu C, Brusegan V, et al: Ritux-
mab in idiopathic membranous nephropathy: A one-yearrospective study. J Am Soc Nephrol 14:1851-1857, 200356. Berg AL, Nilsson-Ehle P, Arnadottir M: Beneficial
ffects of ACTH on the serum lipoprotein profile and glomer- n
lar function in patients with membranous nephropathy.idney Int 56:1534-1543, 199957. Ducloux D, Bresson-Vautrin C, Chalopin J: Use of
entoxiphylline in membranous nephropathy. Lancet 357:672-1673, 200158. Choi MJ, Eustace JA, Gimenez LF, et al: Mycopheno-
ate mofetil treatment for primary glomerular diseases. Kid-
ey Int 61:1068-1114, 2002