the effects of cardiorespiratory biofeedback and - stresseraser
TRANSCRIPT

TheEffectsofCardiorespiratoryBiofeedbackandDialec9calBehavioralSkillsTrainingwithSertralineonPostMyocardialInfarc9onMajorDepressionandLowHeartRateVariability
ADisserta9onPresentedbyPriyaChaudhri,M.A.

CardiovascularDisease
• CVDistheleadingcauseofmorbidityandmortalityintheU.S.sincethe1940’s(AHA,2005)
• 2,600peopledieofCVDintheU.S.eachday,whichisapproximately1deathevery30seconds(AHA,2005)
• ThisyearanesMmated1.2millionAmericanswillhaveaneworrecurrentcoronaryaNack(WHO,2006)

CardiovascularDiseaseandDepression
• ItisesMmatedthat40‐65%ofMIpaMentshavecomorbiddepression(AHA,2005)
• 1outof5MIpaMentshavediagnosableMDDandaquarterhaveminordepression(Carneyetal.,1987)
• Depressionisassociatedwitha2‐7foldelevatedriskofcardiacevents(Molinarietal.,2006)
• Post‐MIdepressionisassociatedwitha2‐3foldincreasedriskforcardiacmortality(vanJoostetal.,2004)
• DepressioncontributestopooradherencetocardiacrehabilitaMon(Kessleretal.,1997)

DepressionandANSDysregula9onDepressionisassociatedwith…• Elevatedheartrate• Lowheartratevariability• Exaggeratedheartrateresponsestophysicalandpsychologicalstressors
• HighvariabilityinventricularrepolarizaMon
• LowbaroreceptorsensiMvity• Elevatedinflammatoryresponse• Elevatednorepinephrine(NE)whichincreasesSNSacMvity (Carneyetal.,2005)

CVDandHeartRateVariability• HRVisdefinedasthefluctuaMonsorbeattobeatalteraMonsinHRasmeasuredinms
• HRVisthesinglegreatestpredictorofmorbidityandmortalityinCVDpaMents(Kleiger,etal.,2000)
• LowHRVisassociatedwitha2‐4foldincreasedriskofmortalityinpost‐MIpaMents(Biggeretal.,1993)
• HRVissignificantlylowerindepressedpopulaMons(Carney,etal.,2000)
Limita9onsofCurrentTreatmentOp9ons
• ThecurrentstandardofcaretotreatdepressionforcardiacpaMentsisSSRImedicaMon,whichhasbeenshowntobeonly40‐60%effecMveinreducingdepressivesymptoms.(Carneyetal.,2005)
• Betablockershavebeenshowntohavemodesteffectsonincreasingheartratevariability.(Sandroneetal.,1994)
• AlthoughpharmacologicaltreatmenthasbeenparMallyeffecMvefordepressionandlowHRV,therearemajorconcernswithlongtermconsequences,sideeffects,compliance,andlifeMmecost.
StudyObjec9veToexaminetheefficacyofcardiorespiratorybiofeedbackwithdialec9calbehavioraltherapy(DBT)inconjunc9onwithsertralinemedica9onforthetreatmentofmajordepressivedisorderandlowheartratevariabilityinpost‐MIpa9ents.

DailyPoints
Every9meapointisobtaineditisaddedintheleRhandcorner.Thegoalistoget2or3squarescon9nuouslyinordertoreachthedailygoalof50‐100pts.
Squarestellyouwhetheryouarerelaxed…
3squares=1point
2squares=½point
1square=1point
PulseRateWave
Reflectstheac9vityofthenervoussystemorRSAandrepresentsthespontaneousrhythmicincreaseanddecreaseoftheheartrate.
InfraredFingerSensor
TheStressEraser,Helicor,Inc.

AnindicatorofpoorbaroreceptorfuncMoning,strainedbreathingoremoMonalstress
Synchronizedbreathingatlessthan6.5breathsperminute.
SynchronizedComfortableBreathing
StrainedBreathing

Dialec9calBehavioralTherapy
• Tradi9onalDBT(1xweekfor2.5hours)• 4ModulesofTreatment:*MindfulnessSkills
*InterpersonalEffec9venessSkills
*DistressToleranceSkills
*Emo9onRegula9onSkills
• DBTSkillsTrainingforthisstudy(1xweekfor1.5hours)• 3ModulesofTreatment:*MindfulnessSkills
*DistressToleranceSkills
*Emo9onRegula9onSkills
TreatmentProtocol
ExperimentalGroup
CardiorespiratoryBiofeedback20minutedailypracMceofStressEraserdevice
Dialec9calBehavioralSkillsTraining90minuteweeklyDBTgroup
An9depressantMedica9onsertralinetreatment
ControlGroup
An9depressantMedica9onsertralinetreatment

Hypotheses Hypothesis1:ParMcipantsintheexperimentalgroupwouldshowagreaterdecreaseindepressivesymptomsatpost‐treatmentandfollow‐uprelaMvetotheanMdepressantcontrolgroup.
Hypothesis2:Heartratevariability,asmeasuredbySDNN,LF/HFraMo,VLFwouldimprovemoreatpost‐treatmentandfollow‐upfortheexperimentalgroup,thanthecontrolgroup.
Hypothesis3:ParMcipantsintheexperimentalgroupwouldshowgreaterimprovementsinmindfulnessandemoMonregulaMonscoresatpost‐treatmentandfollow‐uprelaMvetotheanMdepressantcontrolgroup.

Hypothesis4:TheexperimentalgroupwoulddemonstrateasignificantcorrelaMonwithStressEraserbiofeedbackpointsandimprovementsindepressionscoresatpost‐treatmentandfollow‐up.
Hypothesis5:Decreasesindepressionscoreswouldbemediatedbyimprovementsinmindfulness,emoMonregulaMonandSDNNatpost‐treatmentandfollow‐up.

DepressionInterviewandStructuredHamilton(DISH)BeckDepressionInventoryII(BDI‐II)Difficul9esinEmo9onRegula9onScale(DERS)FiveFacetMindfulnessQues9onnaire(FFMQ)
Psychological
StandardDevia9onofNormal‐NormalBeats(SDNN)LowFrequency/HighFrequencyRa9o(LF/HF)
VeryLowFrequency(VLF)
HeartRateVariability
Medica9onLogBreathingLog
WeeklyLogs
AssessmentPeriodsBaseline(Week1)Post‐Treatment(Week8)Follow‐Up(Week12)
Measurements

RS
B RS
B RPBSPB
B
PRE POST Follow‐Up1 2 3 4 5 6 7 8 9 10 11
B=baseline;S=stressor;R=recovery;PB=pacedbreathing
PhysiologicalMeasurementofHRV
Baseline:10min(listenedtotravellog)
Stressor:2minuteserial7test
Recovery:3minuterecovery(siingquietly)
PacedBreathing:5minof6BPMbreathing

• DocumentedCVDandMI. • Absenceofrecentcardiacevents(MI<2months)andmedicaMonschangesinthe4weekspriortothefirsttreatmentvisit. • AprimarydiagnosisofMajorDepressiveDisorder,asassessedbyaDISHHamiltonscoreof18orgreater,withlowriskofsuicidedefinedbyaBDIscoreoflessthan2onquesMon#9. • StabilizedonsertralinemedicaMon(atleast4weeks)priortostudy. • StablecogniMvefuncMoningbasedontheMini‐MentalStatusExam(MMSE).
• Notbetweentheagesof20‐85,metthecriteriaforClassIVCongesMveHeartFailure,hadapacemaker,and/orpregnant. • ExceededadailyconsumpMonof830milligramsofcaffeine. • PresenceofanyphysicalcondiMonsormedicaMonsthatmakeheartratevariabilityuninterrupMble. • CoronaryintervenMonwithinthepast2months. • SeriouscomorbidmedicalcondiMonthatmayaffectdepressionlevels(i.e.hypothyroidism,diabetes). • PracMcedweeklyyogaormeditaMon.
InclusionCriteria ExclusionCriteria

Demographics
• 60TotalPar9cipants• 34Males• 26Females• 55=MeanAge• 50%Caucasian• 70%Married• 70%Collegeeduca9on

PrimaryAnalyses
Correla9onAnalysesPearsoncorrelaMontests.
StructuralequaMonmodeling(SEM),SobelmediaMontest.Media9onAnalyses
Sta9s9calAnalyses
MulM‐levelModelingwasimplementedusinghierarchicallinearmodeling(HLM).ArandominterceptHLMmodelwasusedtoanalyzethepsychologicalmeasures(HAM‐D,BDI‐II,DERS,FFMQ).AnunstructuredHLMmodelusingrandominterceptandrandomslopewasusedtoanalyzeheartratevariability(SDNN),(LF/HFraMo),(VLF)acrossthreemeasurementcondiMons(baseline,stressor,andrecovery).ToassessthepotenMalimpactofmissingdata,arandomeffectspaNern‐mixtureanalysiswasimplementedwithabinarymissingdatavariable(allparMcipantsversuscompleters)whichwasenteredasapredictorintherandomregressionmodel.

ResultsoftheStudy

0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
Pre Post Follow‐up
MeanHam
ilton
HamiltonScoresAcrossTime(N=60)
biofeedbackcontrol
HLMAnalysisofHamiltonScoresAcrossTime
AllPar9cipants(N=60)
Est. SE p<
TimexTreatment ‐3.20 1.12 .006 **DropoutxTimexTreatment .591
*(p<.05)
**(p<0.01)
***(p<.001)

0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
Pre Post Follow‐up
MeanBD
I
biofeedbackcontrol
BDIScoresAcrossTime(N=60)
HLMAnalysisofBDIScoresAcrossTime
AllPar9cipants(N=60)
Est. SE p<
TimexTreatment ‐8 1.6 <.0001***DropoutxTimexTreatment 0.002 *
*(p<.05)
**(p<0.01)
***(p<.001)

DISHDepressionDiagnosisFrequencyDistribu9onatPost‐Treatment
no major / no minor dep

DISHDepressionDiagnosisFrequencyDistribu9onatFollow-Up
no major / no minor dep

MajorDepressiveDisorderAcrossTime(N=60)
0
2
4
6
8
10
12
Pre Post Follow-Up
Maj
or D
epre
ssio
n (M
ean)
Time
Major Depression Diagnosis
Exp Control

SDNN Est. SE p<Stressor
TimeXTreatment 0.009 0.005 0.055 γ DropoutXTimeXTreatment 0.134
RecoveryTimeXTreatment 12.696 4.555 0.004**DropoutXTimeXTreatment 0.138
LF/HFRa9oStressor
TimeXTreatment 0.051 0.403 0.213DropoutXTimeXTreatment 0.138
RecoveryTimeXTreatment 0.362 0.479 0.453DropoutXTimeXTreatment 0.590
VLFStressor
TimeXTreatment 0.374 2.441 0.879DropoutXTimeXTreatment 0.144
RecoveryTimeXTreatment 8.383 2.437 0.001*** DropoutXTimeXTreatment 0.130
HLMAnalysisofHeartRateVariability
*significant(p<0.05);**significant(p<0.01);***significant(p<0.0001);γ sta9s9caltrend

00.010.020.030.040.050.06
Pre‐Treatment Post‐Treatment Follow‐Up
ExpControl
StandardDevia9onofNormal‐NormalBeats(SDNN)MeanAcrossAllMeasurementCondi9ons(Baseline,Stressor,Recovery)
0
5
10
15
20
25
Pre‐Treatment Post‐Treatment Follow‐Up
ExpControl
VeryLowFrequency(VLF)MeanAcrossAllMeasurementCondi9ons(Baseline,Stressor,Recovery)

6.00
7.00
8.00
9.00
10.00
11.00
12.00
13.00
14.00
Pre Post Follow‐up
MeanFFMQ
biofeedback
control
FFMQScoresAcrossTime(N=60)
HLMAnalysisofFFMQScoresAcrossTime
AllPar9cipants(N=60)
Est. SE p<
TimexTreatment 0.28 0.05 <.0001 ***
DropoutxTimexTreatment .132
*(p<.05)
**(p<0.01)
***(p<.001)

0.00
20.00
40.00
60.00
80.00
100.00
120.00
140.00
Pre Post Follow‐up
MeanDER
S
DERSScoresAcrossTime(N=60)
biofeedback
control
HLMAnalysisofDERSScoresAcrossTime
AllPar9cipants(N=60)
Est. SE p<
TimexTreatment 28.00 3.68 <.0001 ***
DropoutxTimexTreatment .150
*(p<.05)
**(p<0.01)
***(p<.001)

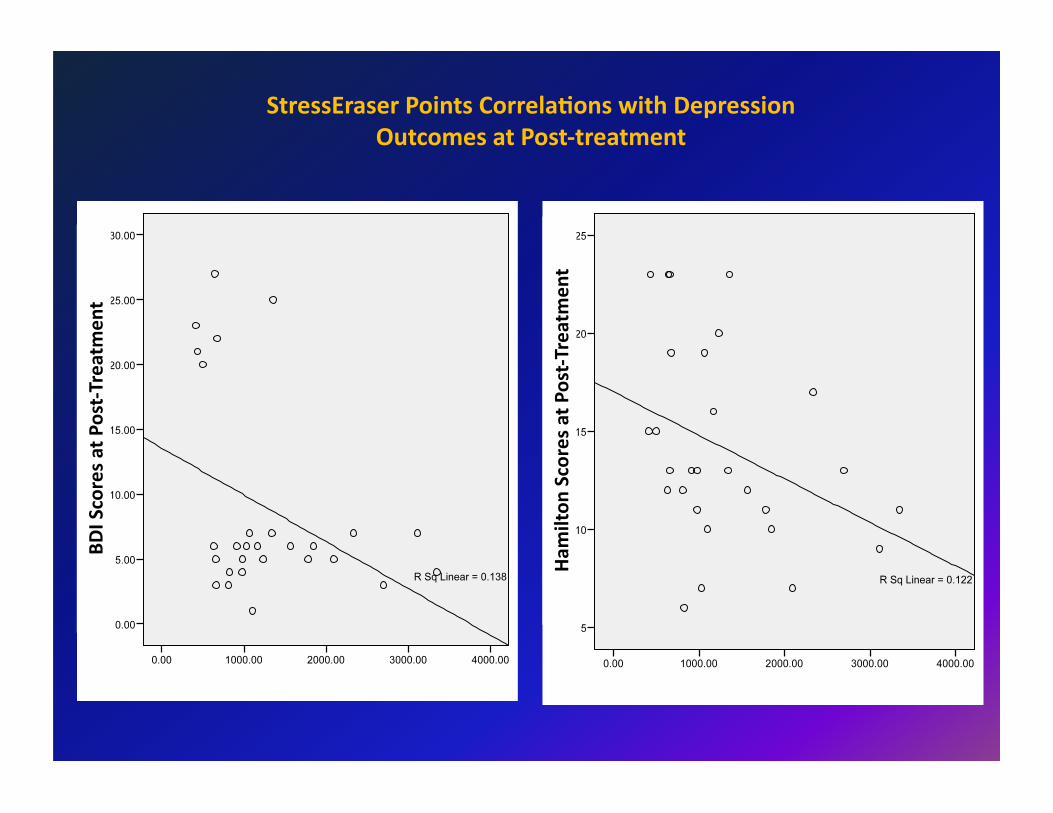
PearsonCorrela9on
pvalue n
BDI‐0.371 .052γ 28
Post‐TreatmentBDI
‐0.535 .022* 18Follow‐UpHamilton
‐0.349 .069γ 28Post‐Treatment
Hamilton‐0.476 .040* 18
Follow‐Up
*(p<.05)
γ (p<.10),sta9s9caltrend
StressEraserPointsCorrela9onwithDepressionOutcomes
Ham
ilton
ScoresatPost‐Treatm
ent
BDIScoresatPost‐Treatm
ent
StressEraserPointsCorrela9onswithDepressionOutcomesatPost‐treatment

Condi9on
DERS
Hamilton
Media9onPathAnalysisModel

Unstandardized Standard ZScoreRegressionCoefficient Error
Post‐Treatment(N=53)
DERSonHamilton ‐1.32 0.74 ‐1.80DERSonBDI ‐1.53 0.44 ‐3.46*FFMQonHamilton 0.72 0.4 1.81FFMQonBDI 0.20 0.23 0.85SDNNonHamilton ‐0.27 0.37 ‐0.74SDNNonBDI ‐1.48 0.38 ‐3.92*
Follow‐Up(N=30)DERSonHamilton ‐4.33 1.11 3.90*DERSonBDI ‐5.35 1.52 ‐3.53*FFMQonHamilton 1.31 0.65 2.01*FFMQonBDI ‐0.91 0.64 ‐1.42SDNNonHamilton ‐1.33 0.68 ‐2.07*SDNNonBDI ‐1.46 0.36 ‐3.90*
*Significanceis(Z>1.96)or(Z<1.96)
MediatorstoImprovementsinDepressionOutcomes

SummaryofDescrip9veDataforallOutcomeVariables

Pre‐Treatment(n=60)
Post‐Treatment(n=53)
Follow‐Up(n=30) Slope EffectSize
M (SD) M (SD) M (SD) Post‐Treatment
HamiltonExp 29.2 (4.47) 14.14 (5.05) 12.94 (3.64) ‐8.9*** 1.4
Con 27.67 (4.64) 18.64 (4.92) 17.75 (4.67) ‐5.7*** 1.0
BDI Exp 30.95 (8.69) 8.89 (7.71) 7.5 (6.99) ‐12.6*** 1.5
Con 30.53 (6.33) 24.56 (5.56) 21.95 (6.64) ‐4.5*** 0.8
FFMQ Exp 10.13 (1.96) 12.58 (1.92) 13.23 (1.23) 0.32*** 1.3
Con 10.81 (1.7) 11.01 (1.76) 11.63 (1.26) 0.04 0.4
DERS Exp 123.13 (16.54) 68.96 (20.42) 64.17 (15.00) 31.7*** 1.5
Con 103.47 (19.92) 98.04 (19.01) 93.67 (15.14) ‐3.7 0.5
SDNNAcrossphases
Exp 0.042 (0.012) 0.057 (0.020) 0.048 (0.016) 1.30** ‐0.9
Con 0.031 (0.020) 0.049 (0.021) 0.035 (0.019) 0.0046 ‐0.9
LF/HFAcrossPhases Exp 2.39 (1.79) 1.89 (0.95) 1.21 (0.71) ‐0.225 0.4
Con 1.86 (1.03) 2.32 (1.26) 1.94 (1.32) 0.297 ‐0.4
VLFAcrossPhases
Exp 19.62 (9.21) 8.98 (4.13) 7.03 (8.63) ‐8.40*** 1.6Con 11.28 (10.88) 14.01 (7.84) 14.14 (11.99) ‐0.303 ‐0.3
*significant(p<0.05);**significant(p<0.01);***significant(p<0.0001);γ sta9s9caltrend

TimexTreatmentInterac9onEffects
Measures SlopeDifferences pValue EffectSize
Hamilton ‐3.20 .006 ** 1.0
BDI ‐8.00 <.0001 *** 2.0
FFMQ 0.28 <.0001 *** 0.9
DERS 28.00 <.0001 *** 1.6
SDNN 0.6Baseline ‐0.003 .848
……..Stressor 0.0093 .055 γ Recovery ‐0.0019 .004 **
LF/HFRa9o 0.3
Baseline 0.4704 .316……..Stressor 0.0508 .213
Recovery 0.3616 .453
VLF 0.7
Baseline 8.4248 .013 *………Stressor 0.3744 .879
Recovery 8.3827 .001 **
*significant(p<0.05);**significant(p<0.01);***significant(p<0.0001);γ sta9s9caltrend

Conclusions
• ThisstudyrevealedthatthecardiorespiratorybiofeedbackandDBTorientedskillstraininginconjuncMonwithsertralineresultedinasignificantlylargerimprovementindepressionseverity,depressiondiagnosis,andheartratevariabilityatpost‐treatmentcomparedtothecontrolgroup,andthiseffectwasmaintainedatfollow‐up.InaddiMon,theexperimentalgroupshowedasignificantlylargerimprovementinemoMonregulaMonandmindfulnessscoresacrossMme.

WhyDidTheExperimentalGroupHaveBererOutcomes?

Post‐Treatment(N=53)
Follow‐Up(N=30)
CategoriesExperimental
GroupControlGroup
ExperimentalGroup
ControlGroup
TimeConflict 2 1 7 4
SSRIDiscon9nued 0 1 4 5
Disinterested 0 1 0 4
CardiacReoccurrence 0 2 1 5
n=7 n=30
ReasonsForDropOut

Theresultsofthisstudycannotbeexplainedbythefollowingconfoundsatbaseline:
• Depressiondiagnosisandseverity• Medica9ons• Gender• Age• Ethnicity• Socioeconomicstatus• Par9cipants’treatmentexpectancies
AlthoughthepaNernsofdropoutmayhavebiasedtheresultsfortheBDIatfollow‐up,therewasnoevidencethattheHamilton,heartratevariability,emoMonregulaMon,andmindfulnessresultswereaffectedbydropouts.
GroupEquivalence

BererOutcomesMayBeArributedTo…..
DBTSkills*EmoMonregulaMon*Distresstolerance*Mindfulness*BehavioralacMvaMon
ImprovedHeartRateVariability*Cardiorespiratorybiofeedback*Breathingretraining
Self‐Efficacy*Empowerment

ClinicalImplicaMons• DecreasesindepressionandincreasesinHRV
canimproveANSregulaMon‐‐‐‐whichmayreduceriskofcardiacmorbidityandmortality
• DecreasesinphysiologicalreacMvitytostressorsandimprovedrecoveryfromitmayalsoprotectagainstthedevelopmentorworseningofCVD
• BeNeradherencetocardiacrehabilitaMon• MoreaNenMvetobehavioralriskfactors
(tobacco/alcoholuse,physicalinacMvity,poordiet)
• ImprovedemoMonalandphysicalhealth• Improvedqualityoflifeandself‐efficacy• ImprovedmindfulnessandemoMon
regulaMonmaypreventrelapserateswithfuturedepressiveepisodes
• ItisnoteworthythatthecontrolgrouphadmoredropoutsaNributedtocardiacreoccurrence.

Acknowledgements
ResearchAssistantsAmyMcKinneyChrisMnaHuangMishanehMarjani
CommiRee
Dr.MiltonBrown,Ph.D.Dr.RichardGevirtz,Ph.D.
Dr.RayGandhi,M.D.Dr.SharonFoster,Ph.D.
Aspecialthanksto…
Dr.FredMuench,Ph.D.Dr.DaleGlaser,Ph.D.

PostHocMedia9onwithIndividualMindfulnessFacetstoImprovementsinDepressionOutcomes
ion pValues
Hamilton BDI
IndividualFacetsofFFMQ
observing .163 .159
describing .124 .107
acMngwithawareness .077γ .045*
non‐judgingofinnerexperience .025* .028*
non‐reacMvitytoinnerexperience .070γ .049*
*significant(p<0.05);γ sta9s9caltrend

pValues
IndividualSubscalesofDERS Hamilton BDI
non‐acceptanceofemoMonalresponses 0.837 0.984
difficulMesengagingingoaldirectedbehavior 0.590 0.571
impulsecontroldifficulMes 0.509 0.936
lackofemoMonalawareness 0.918 0.805
limitedaccesstoemoMonregulaMonstrategies 0.678 0.517
lackofemoMonalclarity 0.990 0.316
PostHocMedia9onwithIndividualSubscalesforDERStoImprovementsinDepressionOutcomes