radiologie interventionnelle oncologique · radiologie interventionnelle • guidage par imagerie...
TRANSCRIPT

Radiologie Interventionnelle Oncologique
Pr Frank Boudghene
Radiologie Hôpital Tenon
APHP.6 - Sorbonne Université
PARIS

Radiologie Interventionnelle
• Guidage par imagerie => Mini invasif • Induit moins de complications, et réduit la durée d’hospitalisation
Movable gantryputs cliniciansin controlThe Discovery IGS provides full flexibility in your clinical
space. Controls available at tableside and at the back
of the gantry let you maneuver the system easily and
conveniently. When in position for imaging, the gantry
swivels around the table on a defined path, with
precise laser guidance. Combined gantry and GE OR
table movement enables you to stop and image at any
point for coverage from head to toe.
6 Discovery IGS Discovery IGS 7
One-touch back-in and back-out means fully
flexible procedures
With the Discovery IGS, you can t ruly have it both
ways: Move the gantry to the table for imaging,
move it aside when not needed – and all at the
touch of a button. From seven posit ions at the
table, you can back the gantry out to predefined
locat ions. Back-out distances are customizable to
suit different room sizes.
Customized parking provides the maximum
freedom
When it ’s not needed for imaging, you can move
the gantry aside completely, allowing complete
pat ient access at the table and enabling easy
room cleaning. You can pre-configure two parking
spaces to suit your room size and shape.
Teams work better with nothing in their way
The Discovery IGS gives physicians, nurses,
anesthesiologists and technologists ample space
to work together effect ively. Clinicians can
posit ion on either side of the pat ient according
to preference. With the offset C-arm, the
anesthesiologist can work comfortably at the
patient’s head. Addit ionally y ou can work with the
system posit ioned slight ly to the left to facilitate
access to the patient when using TEE.
La RI n’est pas de la Chirurgie : elles sont complémentaires
1

Radiologie Interventionnelle dédiée à la prise en charge des cancers Comprend toutes les techniques percutanées et/ou endovasculaires/endoluminales guidées par l’image:
– Diagnostic – Traitement – Management des incidents
• Sous guidage par l’image (US, TDM, IRM, PET)
• Très liée à la recherche comme à l’ innovation
• «Optimisation de la prise en charge»
- ambulatoire - sans anesthésie générale - récupération rapide
«activité préservée »
2
Oncologie Interventionnelle

Quelles procédures ?
Biopsies guidées
Drainages
Stents, filtres caves
Embolisations
Ablations tumorales
patient à jeun, perfusé
crase sanguine, groupe sanguin …..
consultation RI (48h)
antalgiques + anti inflammatoires
3
Oncologie Interventionnelle

BIOPSIES et médecine de précision
Biopsie du FOIE sous TDM
Biopsie OSSEUSE sous PET-CT
Biopsie liquide (CTC)
Biopsie solide
4
Biopsie du SEIN sous ECHO
Biopsie du SEIN sous IRM

Quels équipements? => CBCT
5



Procédures ENDOLUMINALES
Drainages

Procédures ENDOVASCULAIRES
PIC et PAC Filtres Caves

Stents Emboles
Procédures ENDOVASCULAIRES

Quels traitements? EMBOLISATIONS
CHIMIO Embolisation
RADIO Embolisation
TACE - LIPIODOL
HCC
11

Quels traitements? ABLATIONS
Radio Frequence Micro Ondes
Cryotherapie Electroporation
TOUS ORGANES
(initialement pour tumeurs du foie)

Ablations = Médecine personnalisée

Ablations thermiques
Techniques « chaudes » Techniques « froides »
Apoptose Nécrose

Résultats
3 mois de suivi
CBCT de planification
Même dans des zones difficiles d’accès

Radio Fréquence ou Cryothérapie?
Radio Fréquence Cryothérapie
Accessibilité X 0
Volume d’ablation 0 X
Proximité des structures « sensibles » (nerfs, peau, vaisseaux)
0 X
Anesthesie locale 0 X
Injection de ciment X 0
Durée de la procedure X 0
Cout = =
En pratique courante nous avons souvent à choisir

Effet abscopal
Complémentaire de l’ablation 17
10/2015 01/2016 04/2016 09/2017
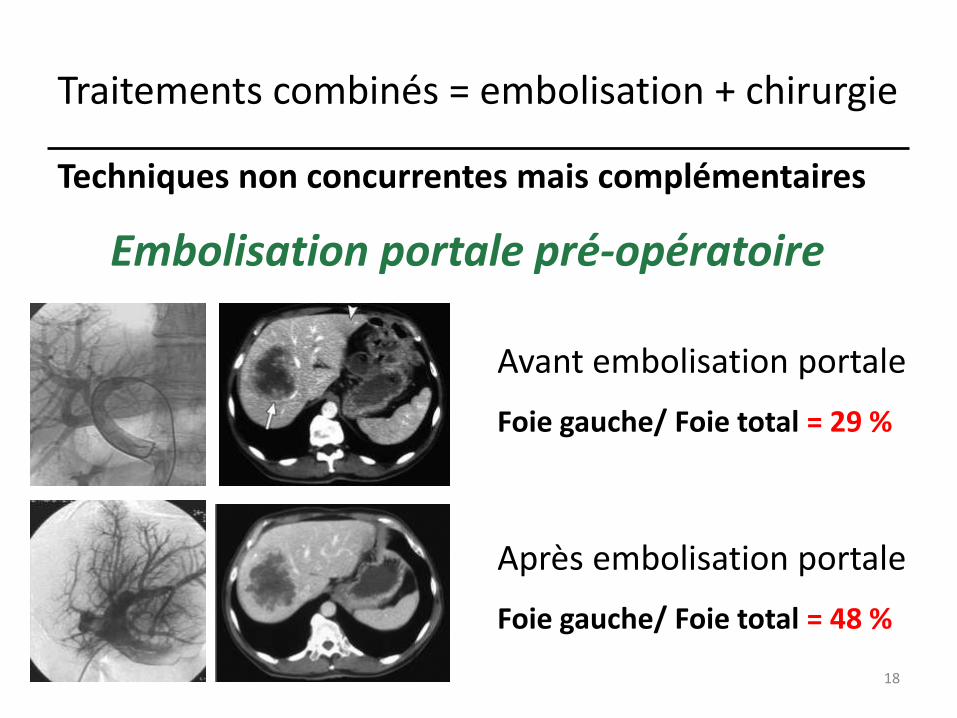
Avant embolisation portale
Foie gauche/ Foie total = 29 %
Après embolisation portale
Foie gauche/ Foie total = 48 %
Embolisation portale pré-opératoire
Techniques non concurrentes mais complémentaires
18
Traitements combinés = embolisation + chirurgie

Complémentaire de la chirurgie ce qui permet de traiter plus de patients 19
Traitements combinés = radiofréquence + chirurgie

20
Pluri étagée
Traitements combinés = cimentoplastie + chirurgie

Nouveaux matériels développés pour RIO = Kiva, Vexim, VBS, LPBS
RANDOMIZED TRIAL KAST Study: The Kiva System • Tutton et al
870 www.spinejournal.com June 2015
In the 285 AT subjects, VAS scores improved signifi cantly
over baseline in both groups after 12 months (Kiva: 70.8 ±
26.3; and BK: 71.8 ± 23.5). ODI scores also improved sig-
nifi cantly at 12 months over baseline in both groups (Kiva:
38.1 ± 19.8; and BK: 42.2 ± 21.7). A comparison of VAS
( Figure 5A ) and ODI ( Figure 5B ) scores over time across
groups is presented.
In the AT subjects at 12 months, 20.9% (28/134) of the
Kiva group and 22.3% (29/130) of the BK group had expe-
rienced a new adjacent level compression fracture (symptom-
atic and asymptomatic combined rate), meeting the endpoint
of noninferiority in the Kiva group. An analysis of the per
protocol population showed that 13.8% (16/116) of the Kiva
group and 20.2% (23/114) of the BK group had experienced
a new adjacent level fracture.
Extravasation of bone cement observed at the procedure
was assessed independently by the CL and IPA. Statisti-
cal noninferiority was met for the extravasation rate by CL
and IPA. The extravasation rate as reported by the site was
signifi cantly lower in the Kiva group when compared with
BK (Kiva: 16.9%; and BK: 25.8%). Secondary endpoints are
summarized in Table 5 .
DISCUSSION The KAST study was a prospective, multicenter, randomized
controlled trial designed to evaluate the safety and effective-
ness of the Kiva system, a novel implant-based vertebral aug-
mentation device. Given its randomized controlled design,
large cohort, and 12-month follow-up, it provides level 1
evidence in the study of 2 treatment arms for osteoporotic
compression fractures. Focal tenderness and marrow edema
on magnetic resonance imaging were required inclusion cri-
teria. These refi ned inclusion criteria identifi ed patients with
acute or subacute osteoporotic VCF-related pain, unlike ear-
lier reported randomized controlled trials without correlative
examination or strict imaging criteria. 1 , 7 The KAST study
incorporated the use of an independent CL for radiographical
evaluations and used an IPA for adjudication of safety data
in an effort to remove bias in its assessment of effi cacy and
safety.
The KAST study was able to prove that Kiva is noninferior
to BK in its ability to safely relieve pain and improve func-
tion in the treatment of osteoporotic VCFs. Pain and func-
tion were signifi cantly improved from baseline at 30 days,
6 months, and 12 months in both groups, demonstrating the
clinical success of these techniques in treating painful VCFs.
No cement-related clinical complications were reported in
the 300 subjects enrolled. The observed rate of extravasation
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
Figure 1. Image of the Kiva system used for vertebral augmentation.
Figure 2. Image under fl uoroscopy of ( A ) the Kiva implant being de-
ployed during treatment of VCF and ( B ) post-VCF treatment with the
Kiva system. The Kiva implant provides a predictable reservoir for bone
cement and the vertebra is restored. VCF indicates vertebral compres-
sion fracture.
Figure 3. Image of ( A ) polymethylmethacrylate being injected and con-
tained within the Kiva implant. ( B ) The Kiva implant.
SPINE141054_LR 870 21/05/15 10:31 AM
21

Y-strut®
22

Non thermique = Electroporation/Electrochimiothérapie
Pour préserver nerfs and tissus sensibles
Pulses courts à haut Voltage
23

ECT = pour traverser les membranes
Tenon 01/10/2018
Première ECT Française
24
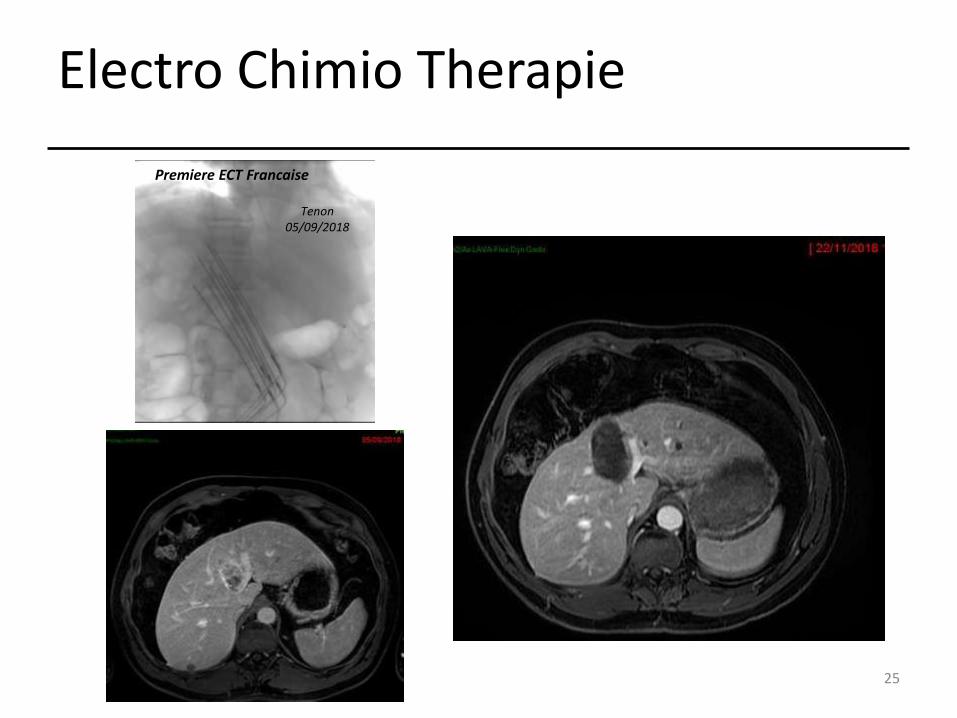
Electro Chimio Therapie
Tenon 05/09/2018
Premiere ECT Francaise
25

Outils d’aide
Prendre en compte l’Anxiété
26
Bien-être Visuel et Acoustique

27
Suite d’Oncologie Interventionnelle
Equipes/ salles dédiées
Maternité
Salles d’Endoscopie
USI
Bloc opératoire
Salle de Radiologie Interventionnelle
Oncologie

RIO = 4ème Mousquetaire contre le Cancer
Chirurgie Oncologie
Radiothérapie Oncologie Interventionnelle
Personnalisée / Précision Médecine
Encourager les jeunes radiologues à développer cette activité essentielle 28

Oncologie Interventionnelle
Radiologie Interventionnelle Avancée = Médecine de Précision OI = une des 3 surspécialités de Radiologie Interventionnelle - décret d’activité et pratique encadrée - formation spécifique (> 30% des promotions d’internes) - valorisation des actes (pas une sous spécialité chirurgicale)
Encourager les jeunes radiologues à développer la RIA
29