novità su dolori addominali ricorrenti, stipsi e malattia ... fimp 2018... · ricorrenti, stipsi e...
TRANSCRIPT

OSVALDO BORRELLI
Department of Paediatric Gastroenterology, Head
Division of Neurogastroenterology & Motility
Great Ormond Street Hospital (GOSH)
London, UK
Novità su dolori addominali
ricorrenti, stipsi e malattia
da reflusso

GASTRO-OESOPHAGEAL
REFLUX DISEASE

BACKGROUND: DEFINITION
GER: the passage of gastric contents into the
esophagus with or without regurgitation and
vomiting.
GERD: when GER leads to troublesome symptoms and/
or complications.
Responsive GERD GERD responding to optimal treatment
Refractory GERD: GERD not responding to optimal treatment after 8
weeks.
Optimal Therapy: Maximum pharmacologic and/or nonpharmacologic
therapy based on the region of practice of the
subspecialist
INFANT REGURGITATION
(OR UNCOMPLICATED GOR)
• Daily regurgitation (occasionally vomiting)
• Normal growth pattern (“happy spitting out”)
• Parental anxiety – Doctor shopping
• Frequent formula changes
• Failure of empiric therapy
• Spontaneous resolution around 12 months
Must include all of the following in otherwise healthy infants 3 weeks to 12
months of age:
1. Regurgitation 2 or more times per day for 3 or more weeks
2. No retching, hematemesis, aspiration, apnea, failure to thrive,
feeding or swallowing difficulties, or abnormal posturing
Hyman et al Gastroenterol 2006;130:1519–1526

Infant with Suspicion of GERD
HISTORY AND PHYSICAL
EXAMINATION WARNING SIGNALS
JPGN 2018;66: 516–554

Warning signals requiring investigation in infants
with regurgitation or vomiting
Vandenplas 2017
Bilious vomiting
GI bleeding
– Hematemesis, Hematochezia
Consistently forceful vomiting
Onset of vomiting after 6 months of life
Failure to thrive
Diarrhoea, Constipation
Fever
Lethargy
Hepatosplenomegaly
Bulging fontanelle, Macro/microcephaly, Seizures
Abdominal tenderness or distension
Documented or suspected genetic/metabolic syndrome

HISTORY AND PHYSICAL
EXAMINATION WARNING SIGNALS EVALUATE FURTHER
SYMPTOMS/SIGNS OF GOR DISEASE
no
yes
JPGN 2018;66: 516–554
Infant with Suspicion of GERD

SYMPTOMS AND SIGNS SUGGESTIVE OF GORD
JPGN 2018;66: 516–554
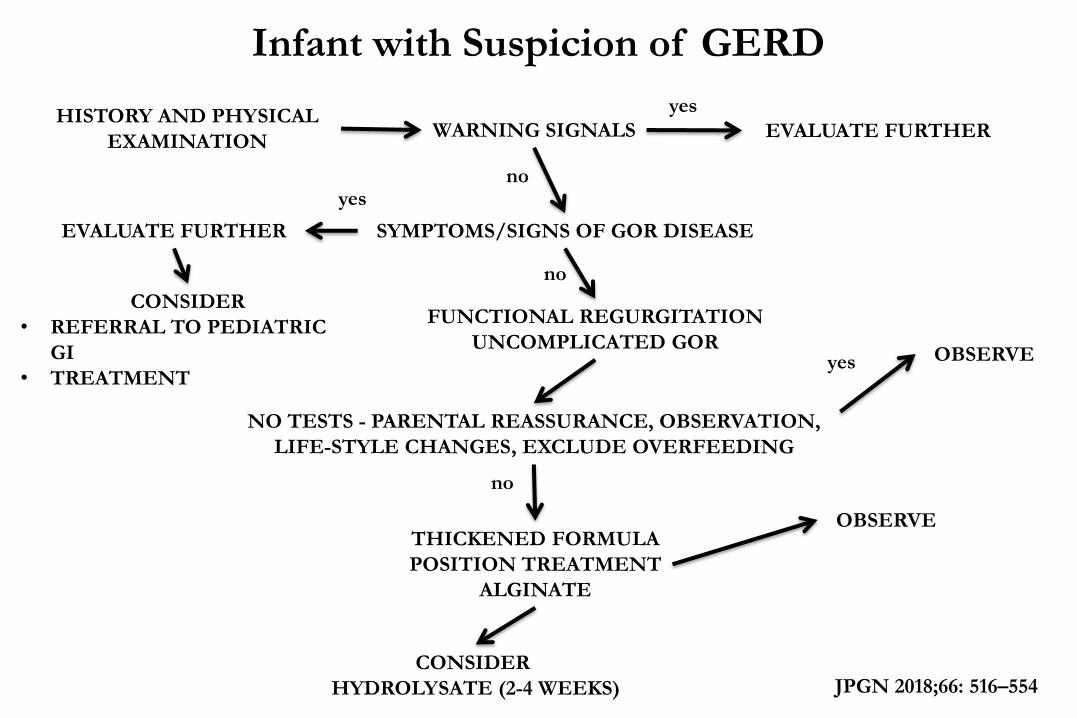
HISTORY AND PHYSICAL
EXAMINATION WARNING SIGNALS EVALUATE FURTHER
SYMPTOMS/SIGNS OF GOR DISEASE
FUNCTIONAL REGURGITATION
UNCOMPLICATED GOR
NO TESTS - PARENTAL REASSURANCE, OBSERVATION,
LIFE-STYLE CHANGES, EXCLUDE OVERFEEDING
CONSIDER
• REFERRAL TO PEDIATRIC
GI
• TREATMENT
EVALUATE FURTHER
yes
no yes
no
JPGN 2018;66: 516–554
yes
THICKENED FORMULA
POSITION TREATMENT
ALGINATE
OBSERVE
no
OBSERVE
CONSIDER
HYDROLYSATE (2-4 WEEKS)
Infant with Suspicion of GERD

JPGN 2018;66: 516–554
CONSIDER HYDROLYSATE
(2-4 WEEKS)
Infant with Suspicion of GERD
CONTINUE MANAGEMENT
AND DISCUSS MILK PROTEIN
REINTRODUCTION AT
FOLLOW UP
Improved Not Improved
REFERRAL TO
PAEDIATRIC GI
Referral not
Possible
CONSIDER 4-8 WEEEK TRIAL
OF ACID SUPPRESSION
THEN WEAN IF SYMPTOMS
IMPROVED
Referral
REVISIT THE DIFFERENAL
DIAGNOSES, CONSIDER TESTING
AND/OR SHORT MEDICATION
TRIAL
NO FURTHER
TREATMENT
Symptoms not
Improved or Recur
Successful Weaning
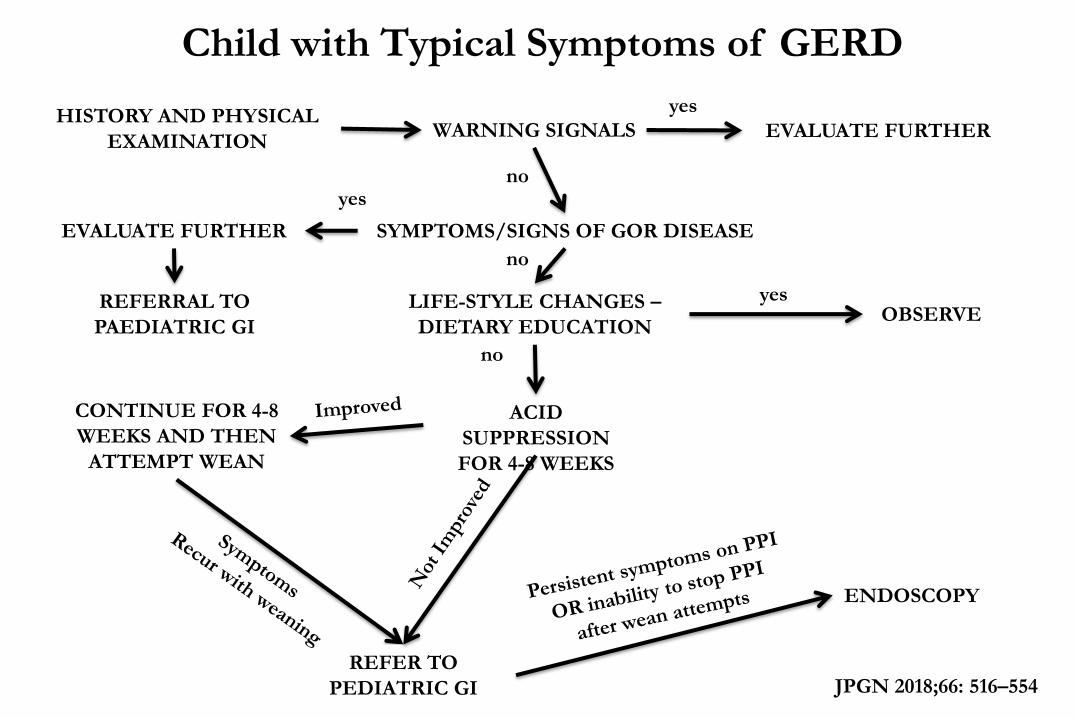
HISTORY AND PHYSICAL
EXAMINATION WARNING SIGNALS EVALUATE FURTHER
SYMPTOMS/SIGNS OF GOR DISEASE
LIFE-STYLE CHANGES –
DIETARY EDUCATION
ACID
SUPPRESSION
FOR 4-8 WEEKS
REFERRAL TO
PAEDIATRIC GI
EVALUATE FURTHER
yes
no yes
no
JPGN 2018;66: 516–554
yes
CONTINUE FOR 4-8
WEEKS AND THEN
ATTEMPT WEAN
OBSERVE
ENDOSCOPY
Child with Typical Symptoms of GERD
no
REFER TO
PEDIATRIC GI

JPGN 2018;66: 516–554
ENDOSCOPY
TREAT
APPROPRIATELY
pH-MII or pHMETRY
NERD
NO SYMPTOM
CORRELATION
POSITIVE SYMPTOM
CORRELATION
CONTINUE PPI FOR
RESPONSIVE
SYMPTOMS WITH
PERIODIC
WEANING ATTEMPTS
No Erosions,
Persistent
symptoms
despite PPI
ABNORMAL ACID EXPOSURE NORMAL ACID EXPOSURE
FUNCTIONAL
HEARTBURN
REFLUX
HYPERSENSITIVITY
Child with Typical Symptoms of GERD

OMEPRAZOLO:
1 mg/kg/die
(adulto 20-40 mg),
LANSOPRAZOLO :
Dose iniziale: 1.5 mg/kg/die
(adulto 30-60 mg)
ESOMEPRAZOLO
0.5-1 mg/kg/die
(adulto 20-40 mg)
30-45 min prima della colazione/cena.
Romano C et al Current Clinical Pharmacology, 2011;6:41-47
Gli Inibitori di Pompa Protonica nelle Malattie Acido-correlate
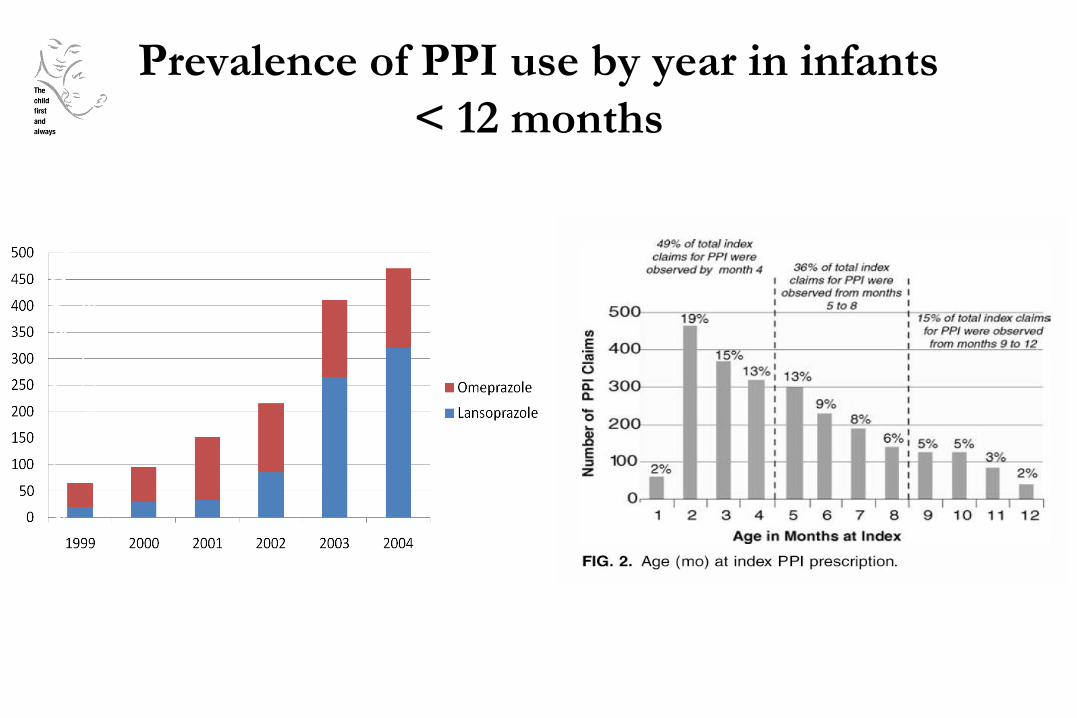
Prevalence of PPI use by year in infants
< 12 months
Pre
vale
nce o
f P
PI
use /
100,0
00
insure
d infa
nts
Barron et al JPGN 2007; 45: 421-427

Concerns about long-term therapy with PPIs
in children
De Bruyne et al Arch Dis Child 2018;103:78–82

Gli Inibitori di Pompa Protonica nelle Malattie Acido-correlate
• Give PPIs to children with acid-
related GERD symptoms
• Regularly reassess the child’s
response to PPIs and taper off
dose with the aim to wean after
8 weeks of treatment
• Substitute PPIs with other
antireflux medications when it
is difficult to wean off
(H2-receptor antagonists or
alginates)
Nikaki Nat Rev Gastr Hepatol 2016
DO
• Do not prescribe PPIs in
infants without proven acid-
related GERD symptoms
• Do not abruptly stop PPIs;
taper dose down to avoid
rebound hyperacidity
• Do not continue to represcribe
PPIs; question their use and
aim to wean off
• Do not treat children with
atypical or extraoesophageal
symptoms with PPIs unless
there is an increased
oesophageal acid exposure
DO NOT
L’uso appropriato – MRGE Considerazioni generali

FUNCTIONAL
ABDOMINAL PAIN

………..

BURDEN OF THE ILLNESS
• Prevalence 0.3-19%
• Bi-modal peak
•Age 4-6
•Age 8-12
• Female preponderence
• 2%-4% of all office visits
Chitkara et al Am J Gastro, 2005
15%
9%
0.3-19%
23%

DEFINITIONS
• Recurrent abdominal pain
• Chronic abdominal pain
• Non-organic abdominal pain
• Psychogenic abdominal pain
• FUNCTIONAL ABDOMINAL PAIN DISORDERS


FUNCTIONAL DYSPEPSIA
Must include 1 or more of the following
bothersome symptoms at least 4 days/month:
1. Postprandial fullness
2. Early satiation
3. Epigastric pain or burning not associated
with defecation
4. After appropriate evaluation, the symptoms
cannot be fully explained by another medical
condition.
*Criteria fulfilled for at least 2 months before diagnosis.
Hyams et al Gastroenterology 2016
Postprandial distress syndrome
Epigastric pain syndrome
IRRITABLE BOWEL SYNDROME (IBS) Must include all of the following:
1. Abdominal pain at least 4 days per month
associated with one or more of the following:
• related to defecation
• a change in frequency of stool
• a change in form (appearance) of stool
2. In children with constipation, the pain does
not resolve with resolution of the constipation
(children in whom the pain resolves have
functional constipation, not IBS)
3. After appropriate evaluation, the symptoms
cannot be fully explained by another medical
condition
*Criteria fulfilled for at least 2 months before diagnosis. Hyams et al Gastroenterology 2016

ABDOMINAL MIGRAINE
Must include all of the following at least twice
1. Paroxysmal episodes of intense, acute
periumbilical pain, midline or diffuse pain ≥1 hr
(should be the most severe/distressing symptom)
2. Episodes are separated by weeks to months
3. The pain is incapacitating and interferes with
normal activities
4. Stereotypical pattern and symptoms in the
individual patient
5. The pain is associated with ≥2 of the following:
a. Anorexia b. Nausea c. Vomiting
d. Headache e. Photophobia f. Pallor
6. After appropriate evaluation, the symptoms cannot
be fully explained by another medical condition.
*Criteria fulfilled for at least 6 months before the diagnosis Hyams et al Gastroenterology 2016

FUNCTIONAL ABDOMINAL PAIN
NOT OTHERWISE SPECIFIED
Must be fulfilled at least 4 times per month
and include all of the following:
1. Episodic or continuous abdominal pain
that does not occur solely during
physiologic events (eg eating, menses)
2. Insufficient criteria for irritable bowel
syndrome, functional dyspepsia,
or abdominal migraine
3. After appropriate evaluation, the
abdominal pain cannot be fully explained
by another medical condition
*Criteria fulfilled for at least 2 months before diagnosis. Hyams et al Gastroenterology 2016

The clinical problem
La bambina mi sembra stia benissimo
Dr Borrelli…..il prossimo paziente è uno di quelli
con dolori addominali ricorrenti
Il papà è grosso ed
alto 1.90 cm
La mamma mi sembra molto
preoccupata

Adesso passerà tutto il pomeriggio a parlare!
Oh…Yippy…Yippy….il mio paziente preferito
Forse chiedo al mio specializzando di vederla
Richiederò direttamente degli esami bioumorali
e una ecografia

identificare un possibile trigger
Discriminare tra una patologia organica e funzionale
Identificare la terapia con maggiore possibilità di successo
Classificare il sottotipo di DFGI
Capire le loro preoccupazione ed aspettative


DIAGNOSTIC ALGORITHM
CHRONIC ABDOMINAL PAIN HISTORY AND PHYSICAL EXAMINATION
PRESENCE OF ALARM SIGNS

ALARM SIGNS IN ABDOMINAL PAIN
Historical findings
• Persistent right upper or right
lower quadrant pain
• Persistent vomiting
• Gastrointestinal blood loss
• Chronic severe diarrhoea
• Dysphagia
• Involuntary weight loss
• deceleration of linear growth
• Delayed puberty
• Unexplained fever
• Family history of IBD, CD or
familial Mediterranean fever
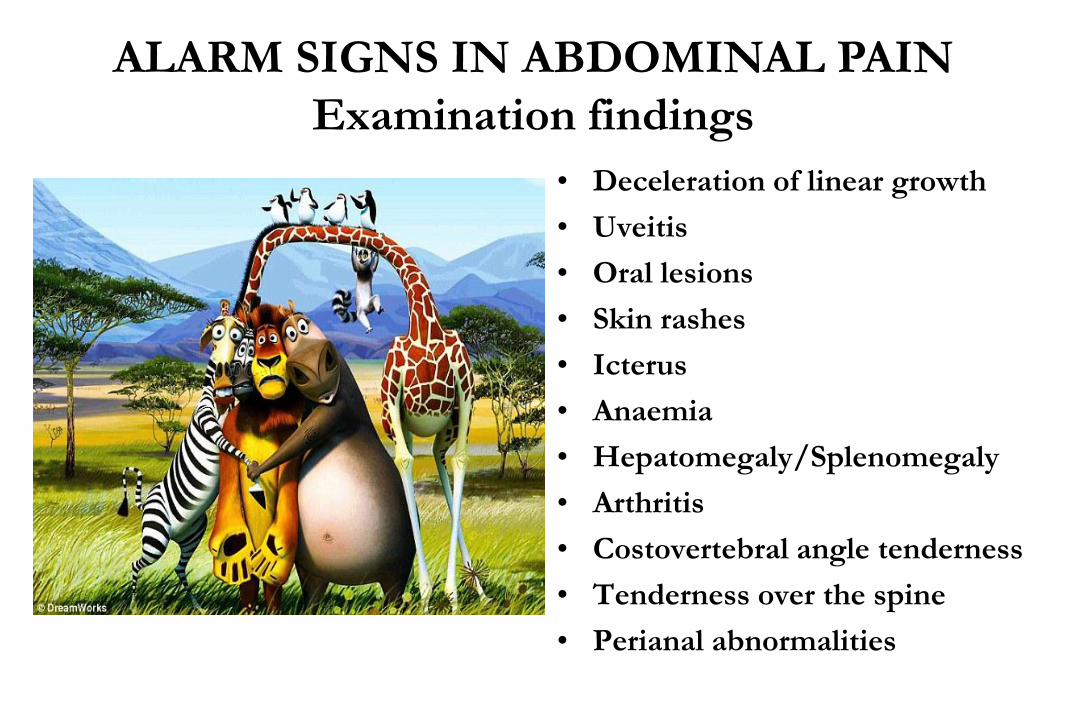
• Deceleration of linear growth
• Uveitis
• Oral lesions
• Skin rashes
• Icterus
• Anaemia
• Hepatomegaly/Splenomegaly
• Arthritis
• Costovertebral angle tenderness
• Tenderness over the spine
• Perianal abnormalities
ALARM SIGNS IN ABDOMINAL PAIN
Examination findings

DIAGNOSTIC ALGORITHM
CHRONIC ABDOMINAL PAIN HISTORY AND PHYSICAL EXAMINATION
PRESENCE OF ALARM SIGNALS EVALUATE
FURTHER
FULFILLS CRITERIA
OF CONSTIPATION
TREAT
CONSTIPATION
WORKING DIAGNOSIS OF FUNCTIONAL
ABDOMINAL PAIN DISORDERS
DIAGNOSIS ACCORDING
ROME IV CRITERIA
Pain alone: Functional abdominal pain (NOS)
Pain in upper abdomen Functional dyspepsia
Pain + abnormal bowel habit IBS
Paroxysmal episodes of Pain Abdominal Migraine
DIAGNOSTIC TESTS
FBC, ESR, CRP
Coeliac screening
Food Allergy
Urinalysis
Calprotectin
Stool O&P
Stool H. Pylori antigen
EVALUATE
FURTHER
APPROPRIATE
TREATMENT
yes
yes
yes no
no
no

BIOPSYCHOSOCIAL MODEL OF CARE
REASSURANCE
• Prevalence of FGID
• Benign clinical course
• Therapeutic approach directed to entire family
• Effective physician-family relationship
• Emphasize normal growth
• Genuine pain
SET REALISTIC THERAPEUTIC GOAL
• Decrease stress and tension
• Improvement of daily symptoms and quality of life
IDENTIFY AND ADDRESS OBSTACLES RELATED TO SCHOOL ATTENDANCE
• How much school has been missed
• Working with school teachers
• Initial reduction of home work
MDT APPROACH
Pediatrician, Psychologist, Psychiatrist, Dietitian, Social worker, Paediatric Gastroenterologist

DIAGNOSIS OF ABDOMINAL PAIN
RELATED FGID
Reassurance and education
Lifestyle and food habits
Discuss expectations
Abdominal pain diary Evaluate after 2-3 weeks
? intervention effective
Stop therapy and evaluate
after 2 months
Start therapy
Dependent on subtype and
preference of patient and parents
Pharmacological
Antispasmodics
Antireflux agents
Antihistaminic agents
Antidepressants
Nonpharmacological
Hypnotherapy
CBT
Probiotics
Evaluate after 2-3
weeks
Intervention effective?
Evaluate after 2-3 months
Intervention effective?
Continue or adjust therapy
Taper medication after 2–6 months
Change therapy
reconsider diagnosis
Continue
Evaluate effect
Intervention effective?
yes
yes yes yes
Korterinket al. Nat. Rev. Gastroenterol. Hepatol 2015:12:159–171
no
no
no
no no
yes

ANTIDEPRESSANTS FOR FUNCTIONAL
ABDOMINAL PAIN
Amitriptyline
Saps et al Gastroenterology 2009
90 children,
5 centers,
4 wks Rx,
5 years to complete it
CBT aims to change attitudes, cognitions, and
behavior that may play a role in generating or
maintaining symptoms
• Child
• Family
COGNITIVE BEHAVIOURAL THERAPY

GUT-BRAIN AXIS
Medial Pain System
(Spinoreticular Tract)
• Painful sensation
• Motivational –
Affective component
(suffering, anger,
response planning)
Prefrontal Cortex
(Pain Memory,
Interpretation,
Response)
Lateral Pain System
(Spinothalamic Tract)
• Non painful sensation
• Sensory – emotional
component
(location, intensity,
nature of pain)

COGNITIVE-BEHAVIORAL THERAPY FOR CHILDREN WITH
FUNCTIONAL ABDOMINAL PAIN AND THEIR PARENTS
DECREASES PAIN AND OTHER SYMPTOMS
An intervention aimed at reducing protective
parental responses and increasing child coping
skills is effective in reducing children’s pain
and symptom levels compared with an
educational control condition.
Levy et al Am J Gastroenterol 2010

CONSTIPATION
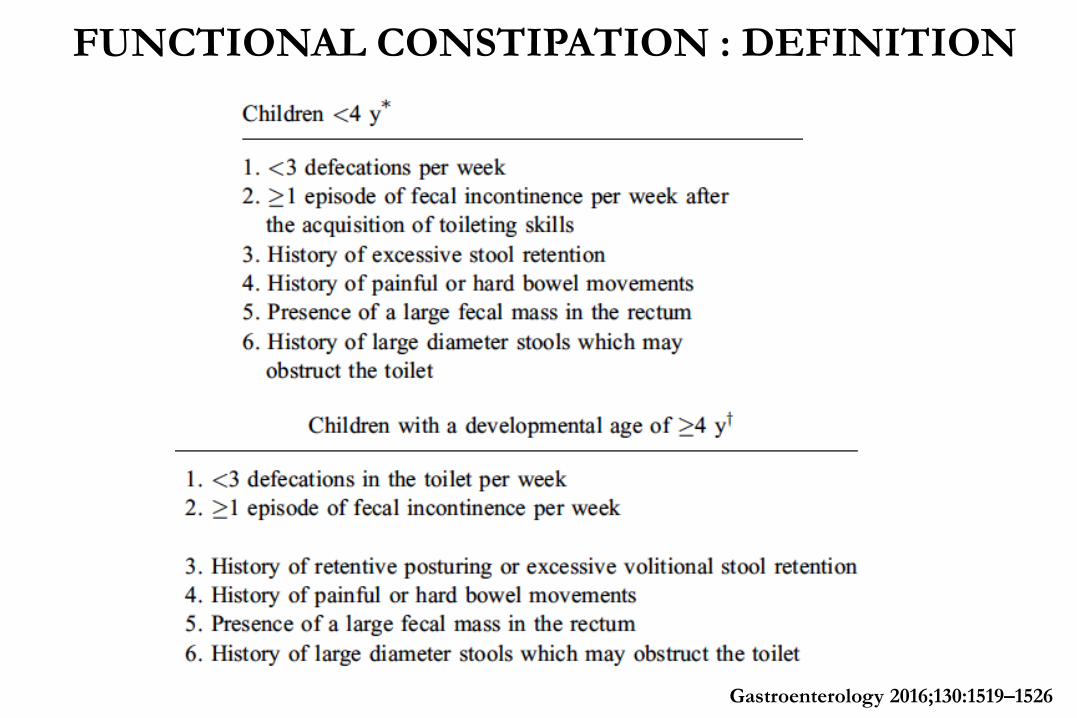
FUNCTIONAL CONSTIPATION : DEFINITION
Gastroenterology 2016;130:1519–1526
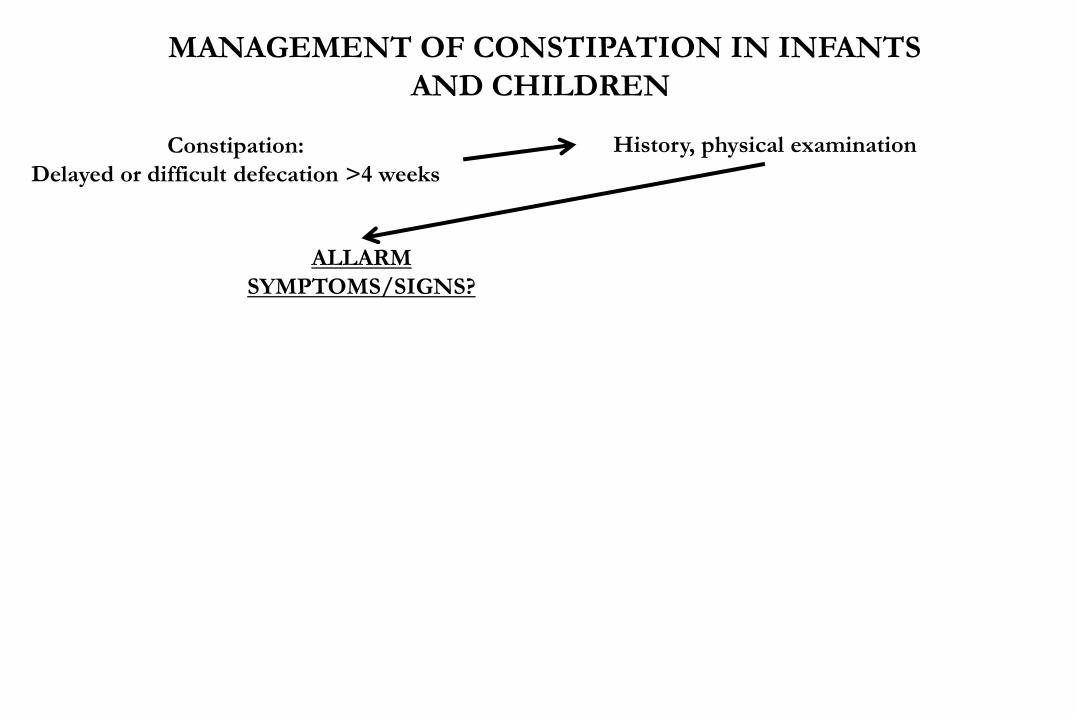
ALLARM
SYMPTOMS/SIGNS?
Constipation:
Delayed or difficult defecation >4 weeks
History, physical examination
MANAGEMENT OF CONSTIPATION IN INFANTS
AND CHILDREN
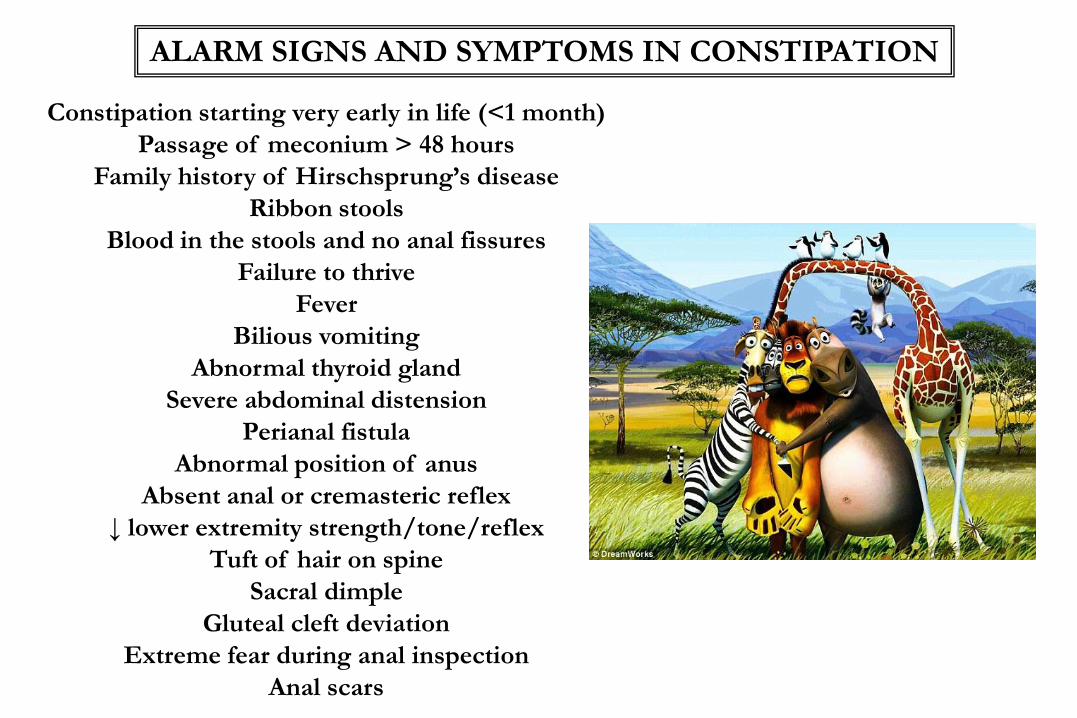
ALARM SIGNS AND SYMPTOMS IN CONSTIPATION
Constipation starting very early in life (<1 month)
Passage of meconium > 48 hours
Family history of Hirschsprung’s disease
Ribbon stools
Blood in the stools and no anal fissures
Failure to thrive
Fever
Bilious vomiting
Abnormal thyroid gland
Severe abdominal distension
Perianal fistula
Abnormal position of anus
Absent anal or cremasteric reflex
↓ lower extremity strength/tone/reflex
Tuft of hair on spine
Sacral dimple
Gluteal cleft deviation
Extreme fear during anal inspection
Anal scars

FUNCTIONAL CONSTIPATION
MANAGEMENT OF CONSTIPATION IN INFANTS
AND CHILDREN
IS THERE FECAL IMPACTION ?
“ GET THEM EMPTY AND
KEEP THEM EMPTY “
ALLARM
SYMPTOM/SIGNS?
Constipation:
Delayed or difficult defecation >4 weeks
History, physical examination
Evaluate further
yes no
Management of Constipation – DISIMPACTION
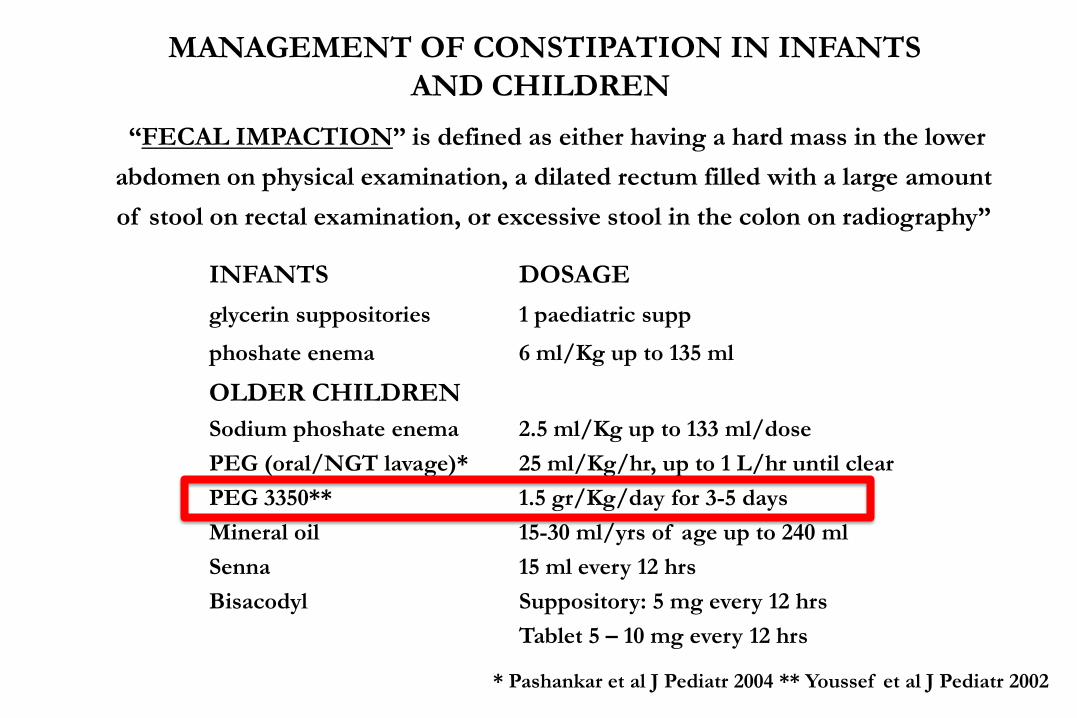
“FECAL IMPACTION” is defined as either having a hard mass in the lower
abdomen on physical examination, a dilated rectum filled with a large amount
of stool on rectal examination, or excessive stool in the colon on radiography”
CONTINUA….
INFANTS DOSAGE
glycerin suppositories 1 paediatric supp
phoshate enema 6 ml/Kg up to 135 ml
OLDER CHILDREN
Sodium phoshate enema
PEG (oral/NGT lavage)*
PEG 3350**
Mineral oil
Senna
Bisacodyl
2.5 ml/Kg up to 133 ml/dose
25 ml/Kg/hr, up to 1 L/hr until clear
1.5 gr/Kg/day for 3-5 days
15-30 ml/yrs of age up to 240 ml
15 ml every 12 hrs
Suppository: 5 mg every 12 hrs
Tablet 5 – 10 mg every 12 hrs
* Pashankar et al J Pediatr 2004 ** Youssef et al J Pediatr 2002
MANAGEMENT OF CONSTIPATION IN INFANTS
AND CHILDREN

Intake
Defe
cati
on
fre
qu
en
cy/
wk
(±S
E)
ns ns
*
Disimpaction
Defecation
Enema
PEG
Bekkali et al, J Pediatr 2009
Management of Constipation – DISIMPACTION
enema vs high dose oral PEG

Bekkali et al, J Pediatr 2009
Management of Constipation – DISIMPACTION
enema vs high dose oral PEG
Intake Disimpaction
ns *
*
Fecal
inco
nti
nen
ce /
wk
Fecal incontinence
Enema
PEG

Management of Constipation – MAINTENANCE

MEDICATION AGE DOSE
milk of magnesia
lactulose or sorbitol
Mineral Oil
PEG 3350
Senna
sodium picosulphate
Bisacodyl tablet
>6 month
1 month
> 12 months
1 month
2-6 years
6-12 years
> 12 years
1 month-4 years
>4 years
2-10 years
>10 year
1-3 ml/kg/day in 1-2 doses
1-3 ml/kg/day in 1-2 doses
1-3 ml/kg/day in 1-2 doses
0.2-0.8 gr/kg/day
2.5-5 mg 1-2 times daily
7.5-10 mg/day
15-20 mg/day
2.5-10 mg 1-2 times daily
2.5-20 mg/day
5 mg daily
5-10 mg daily
Tabbers et al JPGN 2014

Treatment failure?
Intractable constipation
Poor compliance
Wrong treatment
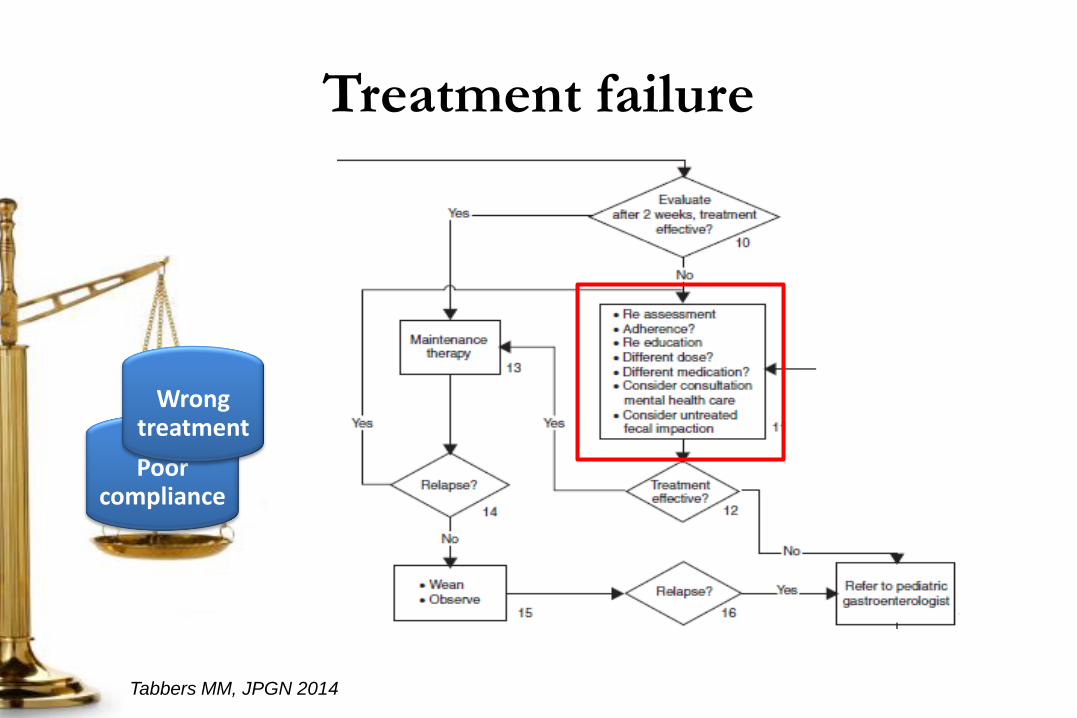
Treatment failure
Poor compliance
Tabbers MM, JPGN 2014
Wrong treatment
Treatment failure
• Re-educate
• Re-assess
• Monitor treatment adherence

Treatment adherence
• Omissions of doses or delays in the timing of doses.
• Patients commonly improve their medication-taking behavior in
the 5 days before and after an appointment with the health care
provider.
Osterberg L, Blaschke T: NEJM 2005

Treatment failure
• Re-educate
• Re-assess
• Monitor treatment adherence
• Change medications

NEWS FROM LITERATURE

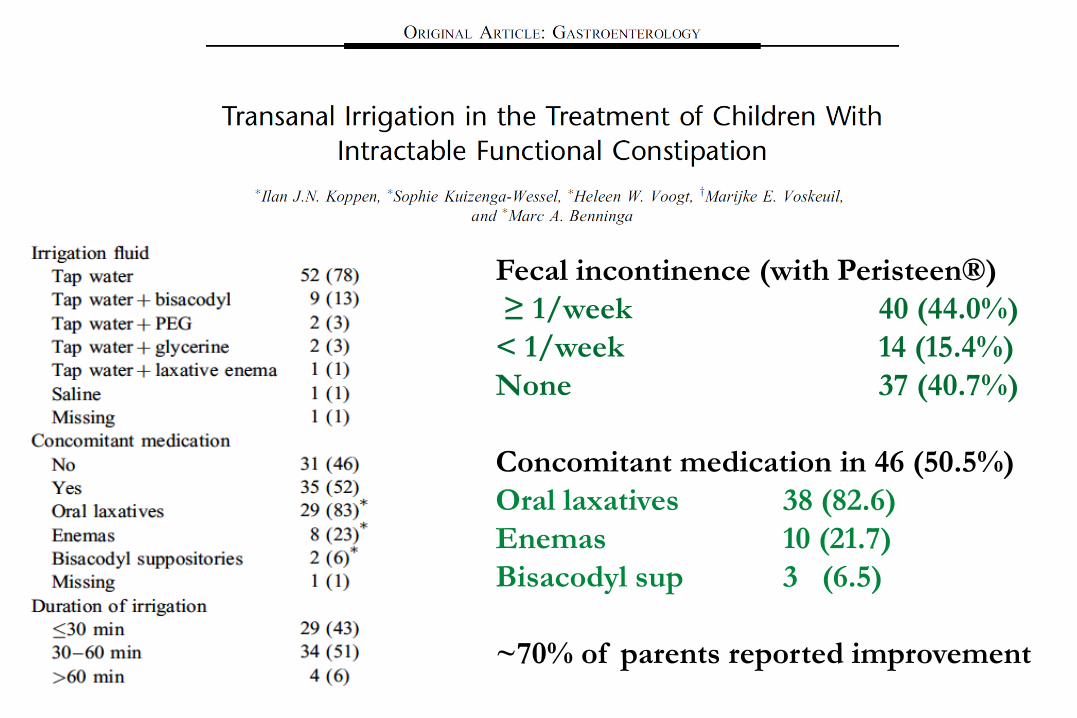
Fecal incontinence (with Peristeen®)
≥ 1/week 40 (44.0%)
< 1/week 14 (15.4%)
None 37 (40.7%)
Concomitant medication in 46 (50.5%)
Oral laxatives 38 (82.6)
Enemas 10 (21.7)
Bisacodyl sup 3 (6.5)
~70% of parents reported improvement

TAKE HOME MESSAGES
Disimpact the children before starting the maintenance
treatment
Judicious use of PPI
Role of holistic approach to FGID
Importance of red flags
Role of rectal therapy
Please, refer to a Paediatric GI for the correct diagnosis

ACKNOWLEDGEMENTS