helios kliniken gmbh b.stitz, helios st. elisabeth klinik hünfeld comparison of laparoscopic and...
TRANSCRIPT

HELIOS Kliniken GmbH
B.Stitz, HELIOS St. Elisabeth Klinik HünfeldHELIOS Kliniken GmbH
Comparison of Laparoscopic and Open Hysterectomy
B. Stitz MD
HELIOS St. Elisabeth Klinik Hünfeld

B.Stitz, HELIOS St. Elisabeth Klinik HünfeldHELIOS Kliniken GmbH
The Purpose of the Study
to evaluate the procedure and the outcome of transvaginal, abdominal and laparoscopic hysterectomy
• duration of the operation and anaesthesia
• size of the uterus
• blood loss
• duration of hospitalisation
• complications

B.Stitz, HELIOS St. Elisabeth Klinik HünfeldHELIOS Kliniken GmbH
Preoperative Evaluation
• Evaluation of dysfunctional uterine bleeding, pelvic pain, dysmenorrhoe, urinary frequency, incontinence, parity status
• Inspection (pelvic floor deficiency, vaginal prolapse)
• Palpation (size and mobility of the uterus, additional findings at ovaries and tubes, peritoneal adhesions after laparotomy and redo operations)
• Sonography transvaginal and abdominal

B.Stitz, HELIOS St. Elisabeth Klinik HünfeldHELIOS Kliniken GmbH
Patient Inclusion Criteria
• Only patients treated with hysterectomy with/without salpingooophorectomy and/or McCall‘s suture were included.
• Neither reconstruction of the pelvic floor (open or laparoscopic approach) nor incontinence procedures, adhesiolysis nor any other simultaneous operations were allowed, no patients with alloplastic implants were included.
• N = 232

B.Stitz, HELIOS St. Elisabeth Klinik HünfeldHELIOS Kliniken GmbH
Operation Techniques
• Wertheim clamps and sutures
• transvaginal or abdominal removal of the uterus
• complete closure of the vagina
• no complete suture of the peritoneum parietale
• one 10mm and two 5mm trocars
• ultrasound tissue dissection
• transvaginal extraction of the uterus
• complete closure of the vagina and of the peritoneum parietale from the inside
identical material and needles for sutures in all approaches
transvaginal or abdominal laparoscopic
B.Stitz, HELIOS St. Elisabeth Klinik HünfeldHELIOS Kliniken GmbH
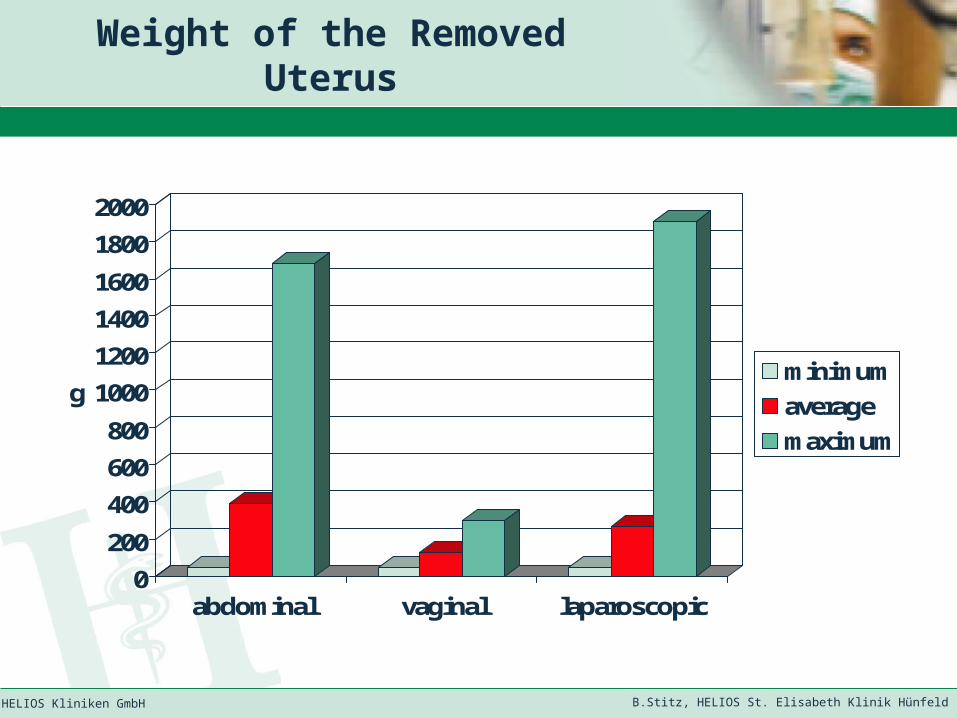
Weight of the Removed Uterus
0
200
400
600
800
1000
1200
1400
1600
1800
2000
g
abdominal vaginal laparoscopic
minimum
average
maximum
B.Stitz, HELIOS St. Elisabeth Klinik HünfeldHELIOS Kliniken GmbH
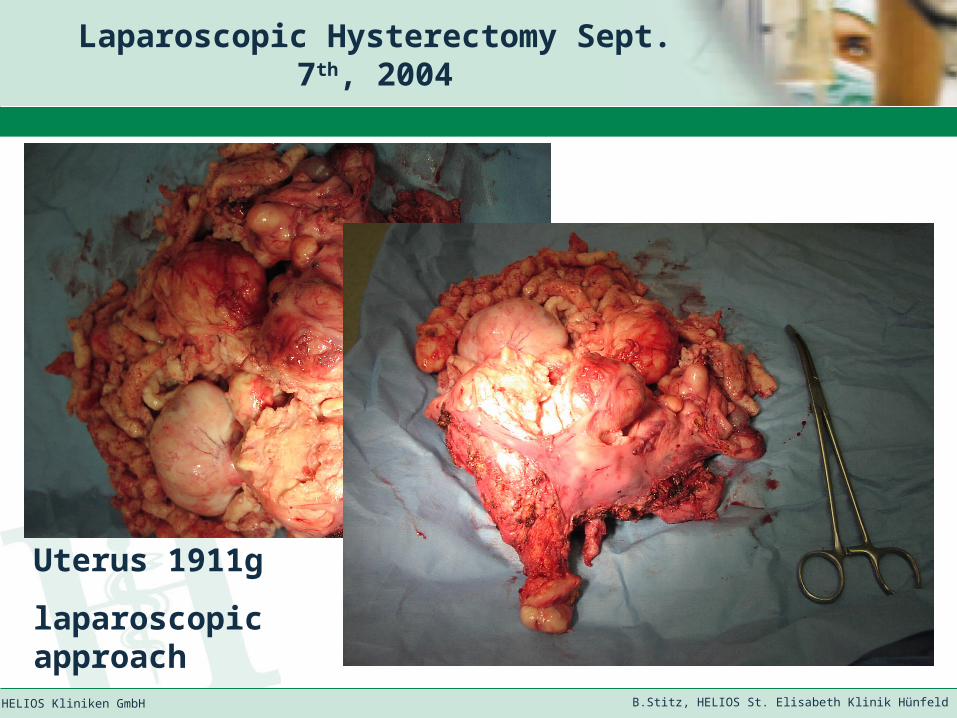
Laparoscopic Hysterectomy Sept. 7th, 2004
Uterus 1911g
laparoscopic approach

B.Stitz, HELIOS St. Elisabeth Klinik HünfeldHELIOS Kliniken GmbH
Duration of Operations
0
50
100
150
200
250
min.
abdominal vaginal laparoscopic
minimum
average
maximum
B.Stitz, HELIOS St. Elisabeth Klinik HünfeldHELIOS Kliniken GmbH
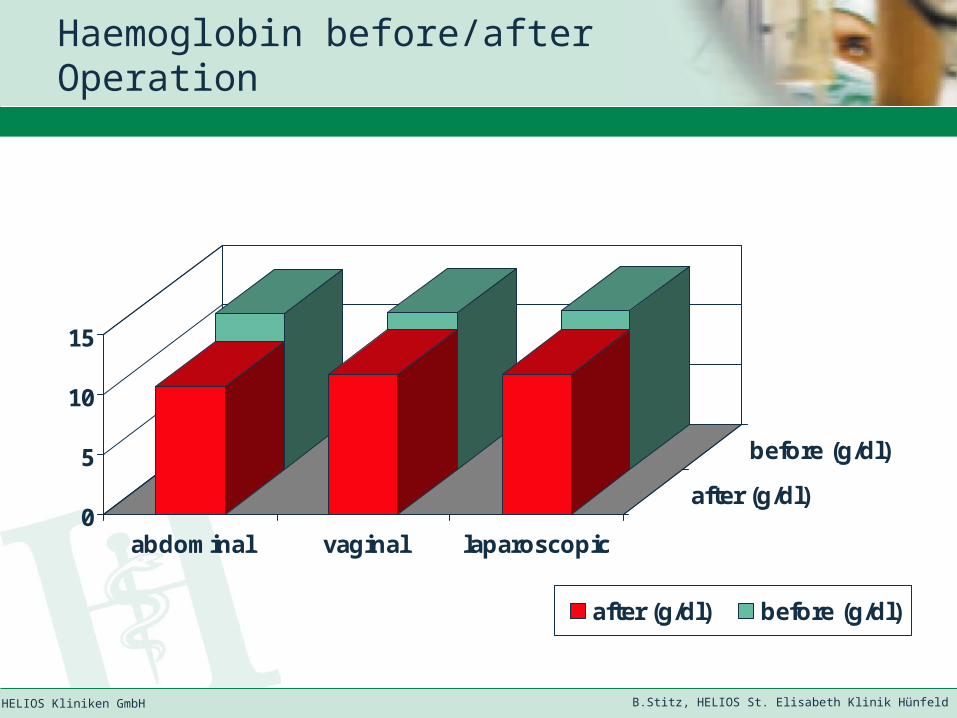
Haemoglobin before/after Operation
0
5
10
15
abdominal vaginal laparoscopic
after (g/dl)
before (g/dl)
after (g/dl) before (g/dl)

B.Stitz, HELIOS St. Elisabeth Klinik HünfeldHELIOS Kliniken GmbH
Blood Loss Perioperative
-1
0
1
2
3
4
5
6
7
8
g/dl
abdominal vaginal laparoscopic
minimum
average
maximum
B.Stitz, HELIOS St. Elisabeth Klinik HünfeldHELIOS Kliniken GmbH
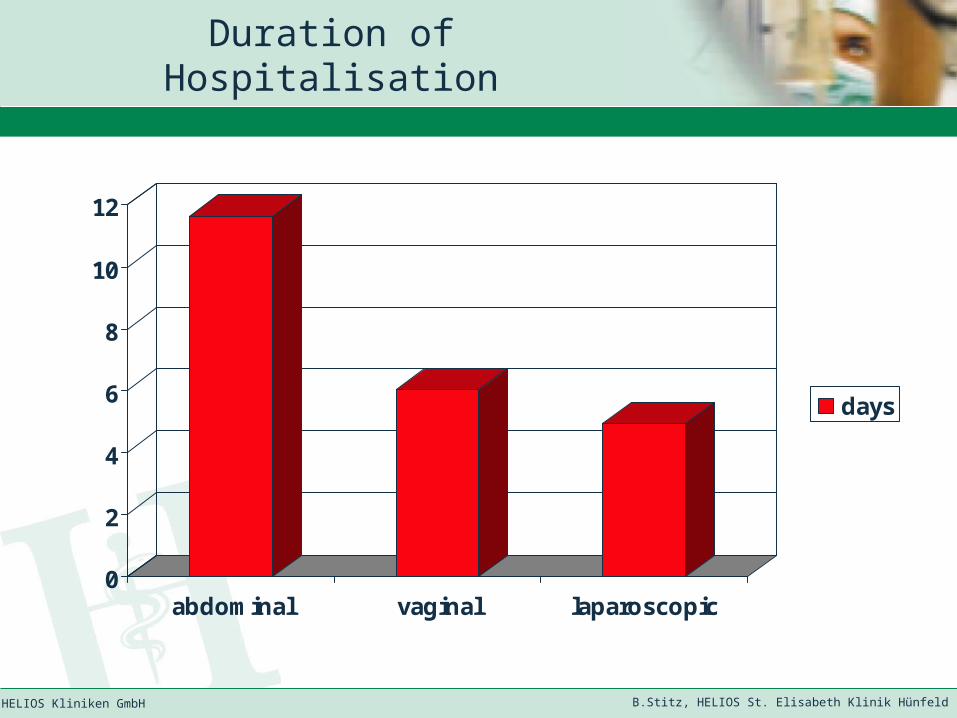
Duration of Hospitalisation
0
2
4
6
8
10
12
abdominal vaginal laparoscopic
days
B.Stitz, HELIOS St. Elisabeth Klinik HünfeldHELIOS Kliniken GmbH
Results
• As expected uteri removed by vaginal approach were significantly smaller than those removed laparoscopically or by laparotomy.
• Blood loss showed no significant difference between vaginal and laparoscopic operation. It was, however, significantly lower than in abdominal approach.
• Abdominal and laparoscopic procedures took more time than transvaginal operations.
• Patients with laparoscopic operations were discharged earlier than those with vaginal hysterectomies. After abdominal operations patients needed twice the time to recover and for being discharged.
• There was no significant difference in intra- and postoperative complications between the different approaches.

B.Stitz, HELIOS St. Elisabeth Klinik HünfeldHELIOS Kliniken GmbH
Conclusions
• Laparoscopic hysterectomy is a safe, fast and comfortable technique.
• Laparoscopic hysterectomy can particularly be recommended to replace most laparotomies done to remove even the large and heavy uterus.
• For smaller uteri we found no advantage in comparison to the vaginal approach.
• In our hospital almost 50% each of all hysterectomies following the described criteria in 2005 were performed by using vaginal and laparoscopic approach respectively. Only one laparotomy (0,55%) was needed.