vitamins and minerals: efficacy and safety”2
TRANSCRIPT

Am J Cliii Niar 1997:66:427-37. Printed in USA. 0 1997 Anierican Society fuir Clinical Nutrition 427
Vitamins and minerals: efficacy and safety”2
John N Hatlu’o’k
Review Articles
ABSTRACT Safety and efficacy are crucial but separate is-
sues for vitamin and mineral supplements. Misinterpretation of
“safe and adequate” to mean “safety limit” would impose restric-
tions on vitamin and mnineral intakes that are not needed to ensure
safety. Substantial evidence indicates that intakes greater than the
recommended dietary allowances (RDAs) of’ certain vitamins and
minerals such as calcium, fblic acid, vitamin E, selenium. and
chromium reduce the risk of certain diseases for some people.
Limitation of’ intakes to the RDAs would preclude reductions iii
disease risk from these nutrients. The margin of safety between the
usual dietary intake and the intake that would produce adverse
effects varies greatly amilong the different nutrients. Very high
intakes of vitamins A and D, niacin, pynidoxine, and selenium have
produced adverse effects. Many widely discussed putative adverse
ef’fects of vitamin C. vitamiiin E, and trivalent chromium have little
factual basis. There is no evidence of adverse effects fromii a-car-
otene supplements except in current heavy smokers. Ant J
Cliii Nuir 1997:66:427-37.
KEY WORDS Vitamins, tiiinenals, benefits. ef’ficacy. safety.
adverse effects
INTRODUCTION
Efficacy and safety are the health issues that determine
whether dietary supplements should be recommended and con-
sumed. E,flk’acv is the ability of a supplement to provide a
health benefit related to either prevention of deficiency or a
reduction in the risk of chronic disease (1-4). Safrtv is a
reasonable certainty that there will be no adverse effects from
excessive intake of a nutrient ( I , 3. 5). Most consumers likely
consider both by assuming safety and judging efficacy in their
individual decisions. Moreover, safety related to avoidance of
adverse effects of excessive intake and efficacy to provide
health benefits are addressed separately under federal labeling
and safety regulations. Nonetheless. the two concepts aresometimes treated in a manner that does not clearly separate
them. For example. the Food and Nutrition Board has set
estimated safe and adequate daily dietary intakes (ESADDIs)
of selected vitamins and minerals as an alternative to recoin-
mended dietary allowances (RDAs) when the data are made-
quate for setting an RDA (6, 7). Also, the term “safe and
adequate” has been misinterpreted as “safety limit” by the
Codex Alimentarius Commission (8). A more accurate defini-
tion of “safe and adequate” and the ESADDI would be “the
recommended intake, an amount that is also safe” (5).
It has long been conventional wisdom that dietary supple-
ments are not needed by persons who eat varied diets, and also
that use of suppletiients may carry significant risk of adverse
effects if’ intakes exceed the RDAs (9-I I ). The issue of need
raises the question “Needed flr what?” The potential benefits
of nutrients in reducing the risk of diseases not recognized as
classic deficiency diseases generally have not been considered
thus far in setting the RDAs or ESADDIs. Recognizing the
important role of same vitaniins and niinenals beyond that (if
preventing deficiency. the Food and Nutrition Board is now
considering use of evidence for decreased risk of chronic
disease it-isetting the RDAs ( I).
Safety is of’ course an important issue. especially at nutrient
intakes well above the RDAs on ESADDIs. A safe intake of
any substance is one that provides an adequate margin below
amounts that cause adverse effects (4. 5). The Environmental
Protection Agency’s ref’erence dose concept of safe intakes has
been applied t(i essential minerals ( I 2). A similar approach that
takes nutritional recommendations into account before calcu-
lation of a safety limit has been applied to both vitamins andminerals (4. 5). The Food and Nutrition Board is currently
evaluating procedures and standards for identifying “safe tipper
limits” or “tipper reference intakes” for nutrients.
For selected vitamins and minerals. this paper examined the
scientific evidence fr benefits other than meeting classical
nutritional needs as well as the concepts and evidence related
to safety concerns, The nutrients reviewed fir safety were
selected because they have been the source of practical safety
problems or the subject of controversy about safety. Similarly.
the nutrients reviewed fir efficacy were selected because cur-
rent evidence on them challenges the conventional wisdom that
“the RDA is always enough.” The criteria for nutrient selection
for safety and efficacy intersect in the conclusion that if’ there
are benefits at intakes above the RDAs, the RDAs should not
be used as sal’ety limits.
EVIDENCE OF EFFICACY
Calcium and osteoporosis
The role (if dietary calcium in achieving higher bone mass
and thereby reducing the risk or delaying the onset of osteo-
porosis is iiow well recogmiized (13) and a health claim on this
nutrient-disease relation has been authorized by the Food and
I From the Council for Resptinsihle Nutrition, Washington. IX’.
2 Address reprint requests to iN Hathcock. Council for Responsible
Nutrition. 13(M) l9th Street NW. Suite 310, Washington. DC 2(8)36-1609.
E-iiiail: hathcock @crnusa.org.
Received November 19. 1996.Accepted fir publication March 6, 1997.
Dow
nloaded from https://academ
ic.oup.com/ajcn/article/66/2/427/4655754 by guest on 14 February 2022

428 HATHCOCK
Drug Administration ( 14). Because bone loss accompanies the
aging process, sufficient calcium intakes during early adult-
hood increase peak bone mass, thereby reducing the risk of
osteoporosis decades later. Increases in calcium intake in post-
menopausal women delay calcium loss from bone, thus low-
ering the risk of bone density declining to osteoporotic levels.
Daily calcium intakes of l0(X)-2000 mg slow the decline of
bone density. thus reducing risk of osteoporosis (13, 14). These
amounts are well above the 800-mg RDA for nonpregnant.
nonlactating adult women in the United States (7).
Folic acid and risk of neural tube defects and heart
disease
There is clear evidence that sufficient intakes of dietary folic
acid before conception and very early in pregnancy decrease
the risk of a baby developing neural tube defects (NTDs) that
include spina bifida. anencephaly, and encephalocele ( I 5). The
daily intake of folic acid thought to be effective for a sensitive
subset of the population is 400 p.g (0.4 mg), an amount above
the RDA in most countries. Although folic acid can reduce the
risk for NTDs, these defects are not solely attributable to folic
acid deficiency. Folic acid supplementation generally reduces
the risk by 50-75%.
Increasing evidence suggests that sufficient dietary folic acid
can decrease the plasma concentration of homocysteine. a
substance that is gaining scientific recognition as a risk factor
for heart disease ( 16-18). The data are not yet sufficient to
make a reliable estimate of the amount of folic acid needed to
generate this benefit, but the amount identified as possibly
effective is in the same range as that shown to be effective
against NTDs.
Antioxidant nutrients and risk of cancer and heart
disease
Vitamin E
Results from several research approaches studying the effect
of vitamin E on heart disease and its risk factors have shownprotective effects associated with intakes well above the RDA
(19-25). Epidemiologic evidence indicates a strong dose-ne-
sponse relation between decreased risk of heart disease and
increased vitamin E intakes from both diet and supplements.
Significant protection begins at daily intakes of 67 mg a-to-
copherol equivalents (19). Low-density-lipoprotein (LDL)-
cholesterol oxidation decreased significantly in blood taken
from subjects receiving � 400 IU/d but not � 200 IU/d (21). In
addition, a double-blind, placebo-controlled intervention trialshowed a significant decrease in nonfatal myocardial infarcts in
high-risk subjects consuming either 400 or 800 IU vitamin E/d
as a supplement (23).
In comparison. another clinical trial did not observe any
benefit on heart disease from a supplement of 50 mg all-rae-
a-tocopherol acetate/d given for 5-7 y to middle-aged Finnish
men who were long-term, heavy smokers (26). One recent
epidemiologic study observed a decrease in heart disease with
increased intakes from foods but not from supplements (27).
The study population involved very few who took vitamin E
supplements and there may have been insufficient statistical
power to detect any effects of supplements. The preponderanceof evidence contradicts these results. Considerable epidemio-logic evidence also links vitamin E with a reduced risk of
cancer (28). These data are supported by the results of animal
experiments (29) but the evidence is not as strong as for the
reduction of heart disease risk by vitamin E.
Vitamin C
Vitamin C inhibits chemical synthesis of nitrosamines (most
of which are animal carcinogens) in the gastric contents, but
inhibition is not complete until dietary intakes reach � 1000 mg
(30-33). Considerable evidence from both epidemiologic stud-
ies and clinical trials suggests that intakes of vitamin C much
higher than the RDA may reduce the risk or risk factors for
chronic diseases such as heart disease and cancer, especially
when combined with higher intakes of vitamin E (34-39).
13-Carotene
Epidemiologic studies have shown that people with high
intakes of 13-carotene or high blood concentrations of this
nutrient have a reduced risk of various diseases, including
cancer and heart disease (40). The chemical abilities of 13-car-
otene to quench singlet oxygen and inhibit peroxyl free radical
reactions are well established (41). In addition to this antioxi-
dant property, 13-carotene and some other carotenoids may play
an important role in facilitating normal cell-to-cell communi-
cation through gap junctions (42). Because many carcinogens
inhibit gap junction communications (43), protection of this
activity by dietary substances could be an important function in
protection against cancer.
Recent clinical trials-the Physicians’ Health Study (PHS)
(44), the Carotenoid and Retinol Efficacy Trial (CARET) (45),
and the Alpha-Tocopherol Beta-Carotene (ATBC) Cancer Pre-
vention Study (26)-failed to find any benefit of 13-carotene in
reducing the risk of cancer or heart disease. In fact, the ATBC
trial and the CARET found increases in lung cancer incidence
in smokers who were administered 13-carotene. The results of
these highly publicized clinical trials were without a doubt
disappointing to those expecting 13-carotene to lower the risk of
cancer. but the current data should not be overgeneralized. The
results do not show that 13-carotene has no anticarcinogenic
effect under any circumstance. Because the ATBC trial and the
CARET studied populations at very high risk of lung cancer,
and because the duration of treatment was far shorter than the
induction time for this cancer, these trials do not support, but
also do not disprove. the hypothesis that 13-carotene may be
anticancinogenic in early stages of cancer.
There are several credible reasons for hypothesizing that
13-carotene might reduce the risk of cancer: I) increased con-
sumption of 13-carotene is strongly associated with reduced risk
of cancer (40), 2) 13-carotene is a dietary antioxidant (4 1 , 46),
3) antioxidants inhibit early stages of carcinogenesis (47), and
4) 13-carotene reduces cancer in some experimental animal
models (48).
For modifying cancer risk. the importance of early adminis-
tration of an antioxidant in relation to the time of exposure to
the initiating carcinogen is well established through studies
with butylated hydnoxytoluene and butylated hydroxyanisole
(49, 50). It is widely thought that lung cancer requires two
decades for development from the first initiating events to
clinically diagnosed cancer. Thus, even with the most powerful
known protective action against lung cancer. cessation of
smoking. decreases in risk become significant only over a
10-l5-y period (51).
Dow
nloaded from https://academ
ic.oup.com/ajcn/article/66/2/427/4655754 by guest on 14 February 2022

VITAMIN AND MINERAL SAFETY 429
Seleniuni
The epidemiologic association of higher selenium intakes
with reduced cancer risk and the antioxidant role of selenium in
glutathione peroxidase (as well as several other possible mech-
anisms) have provided a basis for research on possible antican-
cinogenic effects of selenium. Several selenium compounds
have antitumorigenic activities in a variety of animal models
when administered at amounts greater than those associated
with nutritional need (52).
Only two clinical intervention trials published to date were
designed to determine whether selenium in combination with
other nutrients will reduce cancer risk. In one, 50 pg Se (in
yeast) in combination with vitamin E and 13-carotene moder-
ately reduced the risk of total mortality. total cancer mortality,
and stomach cancer mortality (53). In the other, inorganic
selenium together with a wide spectrum of other minerals and
vitamins did not significantly protect against cancer (54). An
additional placebo-controlled. randomized clinical trial was
stopped recently for ethical reasons after it became clear that
treattnent with 200 j.tg Se in yeast significantly decreased total
and lung cancer mortality and total colorectal and prostate
cancer incidence (55-57). The amount of selenium used in the
study was 200 j.�g. an amount nearly three times the RDA for
adult males (7). The primary objective of the trial was to
determine the effect of selenium on nonmelanoma skin cancer.
but there was no effect. either negative or positive, on this
disease-in contrast with effects on cancer at three other sites.
SAFETY: ISSUES AND EVIDENCE
Safety cannot be absolutely proven for any substance be-
cause such proof would require demonstration of a negative-
that an adverse effect does not occur. Any substance would be
expected to produce adverse effects if the intake were suffi-
ciently high, and therefore safety or lack of it must be related
to a specified intake. Published evidence is sufticient for safety
assessment of vitamins and minerals over a range of intakes.
This evidence is reviewed for some genuine and some bogus
safety concerns for different vitamins and minerals.
Vitamin A
The potential for adverse effects from excessive vitamin A
intake is well documented. Potential risk is based on the
ingestion of excessive amounts of preformed vitamin A in the
forms of retinol or retinyl esters. and not from provitamin A
forms such as 13-carotene or other vitamin A-forming carote-
noids. Consumption of 7500-15 000 p.g preformed netinol
equivalents (RE) daily for periods of several months or more
can produce multiple adverse effects, including liver toxicity
and possibly birth defects (58). The smallest daily supplement
of vitamin A reported to be associated with liver cirrhosis is
7500 pg RE (25 000 IU), which had been taken for 6 y (59).
The smallest daily supplement generally considered to generate
any risk of birth defects is also 7500 �g RE (25 000 IU) (58).
One recent report. however, described a significantly increased
risk of neural crest birth defects at daily supplement amounts of
> 3()00 p�g RE (> 10 000 IU) (60). The average supplement
intake by this group was 6509 �g RE (21 675 IU) but unfor-
tunately the authors did not identify individual supplement
intakes. Several issues have been raised about the validity of
the defect classification scheme used and the resulting likeli-
hood that the study overestimated the risk associated with
vitamin A at the intakes identified in this study (61-63).
Some reports suggest that there may be some risk of vitamin
A toxicity at supplement intakes < 6(X)0 �g REId (20 (XX)
IU/d). One report to the US Food and Drug Administration
suggested a characteristic birth defect associated with maternal
supplementation at 5400 �g REid (18 000 IU/d) (64). Another
report found marginal indications in elderly subjects of adverse
effects on the liver associated with chronic supplementation
providing intakes of 1500-3000 �g REId (5(XX)-l() (XX) IU/d
(65). However, the same laboratory was unable to repeat this
finding in later research (66).
In summary. there is no evidence that vitamin A supplements
of 3 0(X) i,�g RE (10000 IU) are harmful to normal adults.
including pregnant women and the elderly. Adverse effects of
vitamin A are sometimes observed when supplement intakes
reach 7500 p�g RE (25 000 IU) and one report suggests that
such effects may occur with somewhat lower intakes (60).
fl-Carotene
13-Carotene is widely considered to be virtually nontoxic
because humans tolerate high doses without apparent harm,
and animal studies have also failed to find any toxic effects (58.
67, 68). There is no evidence that conversion of 13-carotene to
vitamin A contributes to vitamin A toxicity, even when 13-can-
otene is ingested in large amounts (69).
The only consistent adverse or undesirable effect of high
13-carotene intakes has been coloration of the skin related to
hypencarotenemia, which occurs only at extremely high in-
takes. Doses as high as 180 mg/d have been given to humans
for several months without observed adverse effects other than
skin discoloration (70).
Because of the extensive safety record of 13-carotene. major
clinical trials have been designed with the implicit assumption
that the only likely effects would be benefits. But subsequently.
questions about the safety of 13-carotene have been raised by
the results of the ATBC trial (26) and the CARET (45). which
observed significant increases in lung cancer risk in high-risk
populations (long-term smokers or asbestos workers) given
supplements of 13-carotene (20 mg/d in the ATBC trial and 30
mg/d in the CARET). On the other hand. there was evidence in
the CARET that 13-carotene may reduce the risk of lung cancer
in former smokers. In contrast with the results of the ATBC
trial and the CARET, no increased risk was observed in the
longer-term PHS (44), which included > 2000 smokers. or in
three other shorten-term trials (53, 71, 72). Moreover, observa-
tional studies found no risk of lung cancer or other disease
associated with increased 13-carotene intakes (20. 73, 74).
The effects of alcohol or high intakes of retinol on the liver
have been postulated to explain the adverse outcomes with
13-carotene in the ATBC trial and the CARET (75). This
hypothesis is supported by recently published subgroup anal-
yses of the ATBC and CARET data. indicating that the pro-
moting effects of 13-carotene on lung cancer were seen pniman-
ily in subjects who consumed alcohol and smoked more (76.
77). All data available suggest that heavy concurrent smoking
is a necessary condition for a promotional effect of 13-carotene
(78). Former smokers, whose tissues would presumably have
been subjected to the mutagenic and carcinogenic effects of
cigarette smoke, show decreased, not increased, rates of lung
Dow
nloaded from https://academ
ic.oup.com/ajcn/article/66/2/427/4655754 by guest on 14 February 2022
430 HATHCOCK
cancer with 13-carotene treatment (77). A review of all pub-
lished evidence on 13-carotene shows that the ATBC trial and
the CARET suggest adverse effects but this conclusion is not
supported by other clinical trials or epidemiologic data.
Nicotinic acid
The flushing reaction produced by nicotinic acid has been
recognized for more than half a century (79). When taken on an
empty stomach, crystalline nicotinic acid (but not nicoti-
namide) in doses as small as 10 mg may produce a mild but
noticeable flushing reaction. Although not desirable. such re-
actions produce no known adverse consequences and they are
seldom perceptible when small amounts of nicotinic acid are
taken in tablet or capsule f’orm or consumed with ftod.
Side effects such as liver toxicity and serious gastrointestinal
reactions have occurred when gram quantities of nicotinic acid
were taken to lower serum lipids (80). Gastrointestinal side
effects include indigestion, nausea, vomiting, and diarrhea.
and. in some persons necessitate discontinuation of nicotinic
acid. Liver toxicity is most commonly manifested by increases
in serum transaminase enzymes of liver origin released as a
result of damage to liver cells. High doses have produced
jaundice. fatigue. and, in at least one case, fulminant liver
failure.
There is strong agreement between the minimum adverse
effect level identified through clinical trials and that suggested
by published case reports. Many severe reactions to nicotinic
acid. especially liver toxicity, have involved ill-advised or
inadvertent switching from unmodified to slow-release formu-
lations (80). Most reported adverse reactions to niacin have
occurred with intakes of 2-6 g/d. There are only two anecdotal
cases reported in which intakes were < 1000 mg. one for
slow-release nicotinic acid at 5(X) mg/d and another for un-
iiiodified tiiacin at 750 mg/d (80). In a clinical trial two groups
of adult subjects. one taking immediate-release and one taking
slow-release nicotinic acid, were observed initially and for 6
wk at each dosage level: 500. 1000, 1500, 2000, and 3000 mg/d
(8 1 )‘ The data showed no adverse reactions at 500 mg/d for
either form of nicotinic acid, but significant effects beginning
at l(XX) irig/d (gastrointestinal effects with unmodified nico-
tinic acid and mild liver toxicity with slow-release nicotinic
acid).
Many uncertainties exist in these cases about the accuracy of
patient reports regarding the amount consumed and the pres-
ence or absence of preexisting or conf’ounding conditions such
as alcoholism or other conditions that compromise liver func-
tion (80). For these reasons, the clinical trial data are useful for
safety and risk evaluations of nicotinic acid. From the clinical
trial data it can be concluded that an intake of 10(X) mg/d
carries significant risk and that an intake of 500 mg/d carries no
identifiable risk (8 1 ). Note, however, that the adverse reactions
to 1000 mg unmodified nicotinic acidld were gastrointestinal
effects, which generally have less potential for serious out-
conies compared with the liver toxicity that can result from
1000 mg slow-release nicotinic acidld. The risks associated
with � 1(XX) mg nicotinic acid/d may be tolerable when it is
used as an antihyperlipidemic drug under the care and moni-
toring of a physician. but such risks are not acceptable for
unsupervised, selI’-selected use by consumers.
Pyridoxine
Deficient and excess intakes of pynidoxine can produce
neurologic disturbances (82). The first report of pynidoxine
neurotoxicity in humans described a sensory neuropathy of the
extremities in women with daily intakes of 2000-60(X) mg,
mostly taken in an attempt to control premenstrual symptoms
(83). The neuropathy slowly but perhaps incompletely re-
gressed after cessation of the elevated dose (84-86). Most
cases of sensory neuropathy have resulted from intakes > 60()
mg/d but some evidence suggests that neuropathy may result
from doses as low as 300-5(X) mg/d in sonic individuals (82,
87. 88). The total dose over an unspecified time may give a
better prediction of the potential for neurotoxic response than
either the daily dose or the duration of the high intake (88).
There is controversy over the validity of the single report of
adverse effects at daily intakes of � 10() mg or less (89).
Although this report is often cited as evidence that pynidoxine
intakes < 1(X) mg/d can cause sensory neuropathy. the data
showed an average intake of I 17 mg/d among women with
symptoms and an identical average intake ( I 16 mg/d) in the
control group. The group with symptoms had taken pynidoxine
longer (an average of 2.9 y) than those without symptoms ( I .6
y). Some women in each group had intakes � 50 mg/d. Pos-
sible inaccuracies in the telephone survey method and a lack of
objective neurologic assessment could have introduced bias.
The symptoms observed had no dose-response relation to pyn-
idoxine intake but did show a time-response relation.
Some reports suggest that high intakes of pynidoxine may
cause the development of oxalate kidney stones, but the re-
ported cases may have been associated with the drug pynidoxi-
late (a combination of pynidoxine and glyoxalate) (90), and a
recent prospective epidemiologic study found the relative risk
of oxalate renal stone development to be decreased for men
consuming > 40 mg pynidoxine/d compared with those con-
suniing < 3 mg/d (91).
Ascorbic acid
Many hypothetical adverse effects of high intakes of vitamin
C have been cited for decades (92-94). Most, with the excep-
tion of mild and transient gastrointestinal effects, seem to have
little or no known factual basis (82).
Co,iditioned .seu,i’v
Although this supposed phenomenon has been so widely
cited in review articles that it has become conventional wisdom
(92-94). detailed review and bibliographic tracing provide no
substantiation. Only a very few original sources can be located:
most references are secondary sources, and subsequent inter-
pretation frequently reached conclusions not supported by the
original data. The original hypothesis grew out of two cases of
infantile scurvy (95). The mothers of these infants had taken
vitamin C supplements during pregnancy and the author spec-
ulated that this might have conditioned the infants for rapid
clearance of vitamin C. resulting in scurvy. High intakes of
vitamin C can result in accelerated clearance but this does not
result in blood concentrations lower than normal (96, 97). Oral
scurvy due to withdrawal from high vitamin C intakes has been
reported but the diagnosis was not confirmed, the time to onset
was suspiciously short, and no plasma vitamin C measurements
Dow
nloaded from https://academ
ic.oup.com/ajcn/article/66/2/427/4655754 by guest on 14 February 2022

VITAMIN AND MINERAL SAFETY 43l
were made (98). Conditioned scurvy has been widely discussed
and speculated, but not substantiated.
Ova/ate kidney .stoize.s
Reported large increases in urinary oxalate concentrations
during periods of high vitamin C intakes appear to be an
artifact of analysis due to oxalate production from ascorbic acid
in an analytic procedure that involves heat (99). A more recent
report involving better assay methods indicated a significant
increase in oxalate excretion (still within the normal range) by
persons consuming l(XX) mg ascorbic acid/d (1(X)). It is not
clear whether this increased excretion of 10-15 mg oxalate/d
was due to the instability of ascorbic acid in the urine during
collection, storage. or analysis. Some reports assert that ascon-
bic acid is a risk factor for calcium oxalate kidney stones ( 101).
Other research involving alternative sample handling proce-
dures found fl() increase with a different preparatiomi of ascorbic
acid at intakes of up to 8 g/d ( 102). One study found that
oxalate was produced only in vitro in the urine sample itself
with daily oral ascorbic acid intakes up to 10 g ( 103). The
contribution of high ascorbic acid intakes to urinary oxalate is
not established ( 104), and the suggestion that oxalate kidney
stones are caused by high ascorbic acid intakes remains spec-
ulative ( 105). Indeed, epidemiologic evidence suggests a de-
creased risk of oxalate kidney stones with increased intakes of
vitamin C. For example, a recent prospective epidemiologic
study found the relative risk of oxalate renal stones to be
decreased for men consuming � 15(X) mg vitamin C in com-
parison with those consuming < 250 mg (91). These data
provide further support for an earlier retrospective that pro-
duced siniilar results (l()6).
Proo.vida,zt efft’ets, excessive iron absorptioiz, or exee.ssit’e
iron release
A potential for harm by high intakes of ascorbic acid through
prooxidant effects has been discussed widely ( 107. 108). An
original research paper ( 109) has been cited in a review article
(108) as showing that an asconbate-dniven free radical reaction
damages cells. The study used in vitro assays with phagocytes
and found that the release of iron from senescent erythrocytes
in the medium had adverse effects only at abnormally high
ascorbic acid concentrations. These concentrations were > I 0
tinies the highest plasma ascorbic acid concentrations of sub-
jects consuming 1000-25(X) mg ascorbic acidld ( 100). The
hypothesis that high intakes ofascorbic acid will produce direct
prooxidant ef’fects is not consistent with the data on iron
release, and contrasts with the antioxidant effects of vitamin C
observed under a wide variety ofconditions (1 10). The concept
that enhanced iron absorption by ascorbic acid leads to excess
iroti-related disease has been suggested (108) based on the
hypothesis that increased serum ferritin concentrations cause
heart disease ( I I 1 , I I 2). The hypothesis that excessive iron
causes heart disease is not supported by subsequent evidence
and evaluation ( 1 1 3- 1 1 8). Ascorbic acid intakes of’ 2 g/d for
2 y did not cause excessive iron uptake (1 19), providing
additional evidence that a high ascorbic acid intake is unlikely
to produce any iron-related increase in heart disease. Intakes of
up to 10 g/d for up to 3 y without observed side effects have
been evaluated in clinical trials ( 120).
Gastrointestinal distress
The most common adverse effects of’ high vitamin C intakes
are gastrointestinal symptoms such as nausea. abdominal
cramps. and diarrhea ( I 2 1 ). When these symptoms occur. the
vitamin C dosage is usually > 2 g/d but a few individuals
report such symptoms at intakes as low as 1 g. These symptoms
seem to be a direct osmotic effect because they can usually be
avoided by taking the vitamin as a buffered salt rather than as
a free acid. The symptoms usually disappear within a week or
two with no further consequences. At least some of the diarrhea
reportedly caused by ascorbic acid supplements may have been
produced by other components such as sorbitol ( I 22).
Folic acid
Three major concerns have been identified as possible ad-
verse effects from excessive folic acid intakes: I) the masking
of pernicious anemia. thus allowing the neurologic disease of
vitamin B- I 2 deficiency to progress unchecked; 2) the disrup-
tion of zinc function: and 3) the antagonism of medications.
especially antifolate agents.
�%‘fa.sking pernicious a�zeinia
Administration of high intakes of folic acid to patients with
pernicious anemia can mask the anemic manifestations while
allowing the neurologic disease (posterolateral spinal cord de-
generation) to progress. Although there are a few reports of the
masking effect related to amounts of f’olic acid � I mg (results
based almost entirely on studies with injected fblic acid). the
eftect is unusual at such low doses and predictable only at
doses � 5 mg (123).
!‘Oli(’ (l(’id-Zi?U’ intera(’tions
Certain folic acid-zinc interactions are well documented.
including the malabsorption of f�id folates in zinc deficiency
due to insuf’ficient activity of the folate conjugase enzyme that
must convert food pteroylpolyglutamates to the monoglutaniate
forni before absorption ( I 24). The crucial question for folic
acid safety in relation to zinc is whether higher intakes have
adverse consequences through a disruption of zinc bioavail-
ability or function, and. if so. what are the intakes of fblic acid
that are associated with such effects. Some reports suggest that
as little as 350 .tg of supplemental folic acid can adversely
affect zinc nutniture (125-127), but more recent reports mdi-
cate no adverse effects of f()lic acid at even higher intakes on
zinc uptake or function (128. 129). The suggestion that folic
acid intakes < 400 �g/d cause adverse outcomes of’ pregnancy
through the antagonism of zinc functions (125) has not been
supported by subsequent larger. multicenter studies involving
intakes that were either 4 mg ( I 30) or 800 �g ( I 3 1 ) before and
throughout pregnancy.
It is difficult to resolve differences in the scientific literature
regarding a possible adverse effect of folic acid on zinc nutni-
tune. These apparently incompatible results are likely attnibut-
able to the widely different experimental approaches used. In
general, methods based on uptake rate and plasma concentra-
tion tend to show ef’fects at lower folic acid intakes. whereas
zinc balance methods tend to show effects only at higher
intakes. Large, well-conducted clinical trials have found no
adverse effects of folic acid on pregnancy through zinc antag-
Dow
nloaded from https://academ
ic.oup.com/ajcn/article/66/2/427/4655754 by guest on 14 February 2022

432 HATHCOCK
onism or any other mechanism, although they have shown a
clear benefit in reducing the risk of NTDs (130, 131).
Folie u’id-drug interactions
At high intakes. folic acid has been reported to interfere with
the effectiveness of anticonvulsant drugs such as Dilantin (di-
phenylhydantoin; Parke-Davis, Division of Warner Lambert,
Morris Plains. NJ), used to control epilepsy (124). Folic acid
doses of 5-30 mg orally have produced some evidence of
increased frequency of seizures in epileptics, but there is no
evidence of such effects at lower intakes of folic acid. It might
be expected that increased folic acid intakes could interfere
with actions of folate-antagonizing drugs such as methotrexate.
In contrast, administration of I mg folic acid/d for 6 mo in
patients with rheumatoid arthritis treated with low-dose meth-
otrexate actually decreased methotrexate toxicity without af-
fecting its efficacy for therapy (132).
Selenium
Excess selenium intake from consumption of seleniferous
plants by animals produces a wide range of adverse effects
( 1 33). Chronic signs of toxicity in livestock include cirrhosis,
lameness, hoof malformations, hair loss, and emaciation. In
laboratory animals the signs commonly include liver cirrhosis.
The minimum dietary intake of selenium recognized to produce
adverse effects in farm animals is 4-5 �g/g dry wt of diet
(133).
An episode of human poisoning by selenium involved a
manufacturing error that resulted in a dietary supplement prod-
uct that actually contained 182 times the amount of selenium
declared on the label (I 34, 1 35). Adverse effects occurred
within a few weeks and included effects on hair, nails, and
liven. Human selenium poisoning in a high-selenium area of
China also produced adverse effects on nails. skin, the nervous
system, and teeth ( 1 36). These adverse effects occurred in
some persons with intakes > 910 �g/d. No adverse effects
have been associated with lower intakes, but the ratios of
plasma selenium to erythrocyte selenium have been found to
increase with dietary intakes � 750 �g/d ( 137, 138). Surveys
in selenifenous areas of the United States have failed to find any
signs of selenium intoxication in persons with intakes of up to
slightly > 700 �g/d (139). In the Chinese population with an
average lowest observed adverse effect level (LOAEL) of 910
I_Lg Se intake, the lower 95% confidence limit for the LOAEL
was 6(X) p�g/d ( 140). Because the chemical forms of selenium
in foods grown in seleniferous areas are not completely known,
the human data on adverse effects from chronically high in-
takes apply only to total dietary selenium and not to any
specific form. No adverse effects were observed in a l0-y
clinical trial at daily supplemental intakes of 200 p.g Se in
selenized yeast (55-57).
Chromium
No credible data or reports have shown adverse effects of
Cr3 � in humans, and animal data also suggest that orally
administered Cr� is extremely innocuous (5, 141, 142). In
addition, the MEDLINE database (National Library of Mcdi-
cine, Bethesda, MD) lists no published cases of adverse neac-
tions in humans. In contrast, chromate (Cr6� ) is clearly estab-
lished as a work-related etiologic agent in lung disease,
including lung cancer, in chromate and stainless steel workers
(143).
One report described clastogenesis (chromosome breakage
in vitro) from high concentrations of chromium picolinate
added directly to Chinese hamster ovarian cells in culture
( 144). Because Cr6� can be biologically reduced to � Cr4�,
and Cr3� but Cn� � is not oxidized to the higher valence states,
the authors suggest that Cn� � could be the actual carcinogen.
This suggestion seems to conflict with their data that indicated
clastogenic effects of chromium picolinate and picolinic acid,
but not chromium chloride, chromium nicotinate, or nicotinic
acid ( I 44). Also, other data from the same research group were
interpreted to show that Cr�� is the genotoxic and presumably
carcinogenic species of chromium ( 145-148). Moreover, the
criteria of the Environmental Protection Agency (EPA) for
interpreting in vitro clastogenesis data in cancer risk assess-
ment specify that evidence ofclastogenicity is meaningful only
if there is confirming mutagenicity data, and that these together
are sufficient only to recommend an animal bioassay to eval-
uate possible carcinogenicity ( I 49-151).
The EPA has reviewed all relevant data on chromium tox-
icity and calculated a reference dose, a safety limit involving a
margin of safety below the levels with evidence of adverse
effects, for Cn3� and also for Cr6�. Application ofa composite
safety factor of 1000 to the animal data for Cr�� gives a
reference dose of 1 .47 mg/kg (142), which with downward
rounding converts to 70 mg/d in adult males. The reference
dose for Cr” (70 000 p.g) is 350 times the upper value of the
ESADDI of 50-200 p.g for adults (7). Thus, trivalent chro-
mium has an extraordinarily wide margin of safety. In contrast,
hexavalent chromium-a form not normally found in the di-
et-has significant toxic potential. and accordingly the refer-
ence dose for Cn6�, calculated by the EPA for a 70-kg man, is
only 335 j.�g/d (142).
There is no evidence of toxicity in humans from orally
ingested trivalent chromium, and 1000 �tg Cr/d as chromium
picolinate produced no adverse effects in a clinical trial (R
Anderson, N Cheng, N Bryden, et al, unpublished observa-
tions, 1996). Extrapolation from animal data corroborates hu-
man data that trivalent chromium is extraordinarily safe but its
benign character should not be confused with the established
toxicity of hexavalent chromium.
CONCLUSIONS
The potential benefits of nutrients in reducing the risk of
diseases that are not recognized as classic deficiency diseases
have not been used thus far in setting the RDAs or ESADDIs.
Recognizing the important role of some vitamins and minerals
beyond that of preventing deficiency. the National Academy of
Science, in contrast with past practices, is now considering use
of evidence for decreased risk of chronic disease in setting the
RDAs ( I ). Evidence is rapidly accumulating that intakes above
the RDA for some micronutnients provide benefits in reducing
the risk of chronic disease, and these effects are moving toward
acceptance as an appropriate basis for future RDAs ( I , 152).
Also, it is well recognized that higher intakes of nutrients
necessitate careful evaluation of the safety of those intakes
(1, 5).
Dow
nloaded from https://academ
ic.oup.com/ajcn/article/66/2/427/4655754 by guest on 14 February 2022
VITAMIN AND MINERAL SAFETY 433
Efficacy
Calcium
The benefits of calcium in reducing the risk of osteoporosis
are recognized by health claims authorized by the US Food and
Drug Administration for intakes of 1000-2000 mg/d, but the
current RDA for most women is only 800 mg (Table 1).
Folk’ cl(’id
The intake of folic acid recognized by the Food and Drug
Administration to reduce the risk of NTDs is 400 p.g/d. but the
RDA for most women is only I 80 p.g (Table 1).
Vitamin E
Intakes of 67-30() mg a-tocopherol equivalents (100-400
IU) of vitamin E have been shown to reduce oxidation of LDL
cholesterol and lower the risk of heart disease, but the RDA for
adult males is 10 mg (15 LU) (Table 1).
Seleniuni
A recent clinical trial found reduced cancer risk with a
selenium intake of 200 �g/d. but the RDA for adult males is 70
�tg/d (Table 1 ). Limiting this nutrient to the RDA precludes
benefits from higher intakes, and such limitations are not
necessary for safety.
Safety
Safety limits should be based on a standard other than the
RDA, ESADDI, on other recommendations related to nutri-
tional policy or beneficial effects. Use of a direct scientific
approach to identify safe upper levels does not impose false
safety limits related to the RDA on ESADDI.
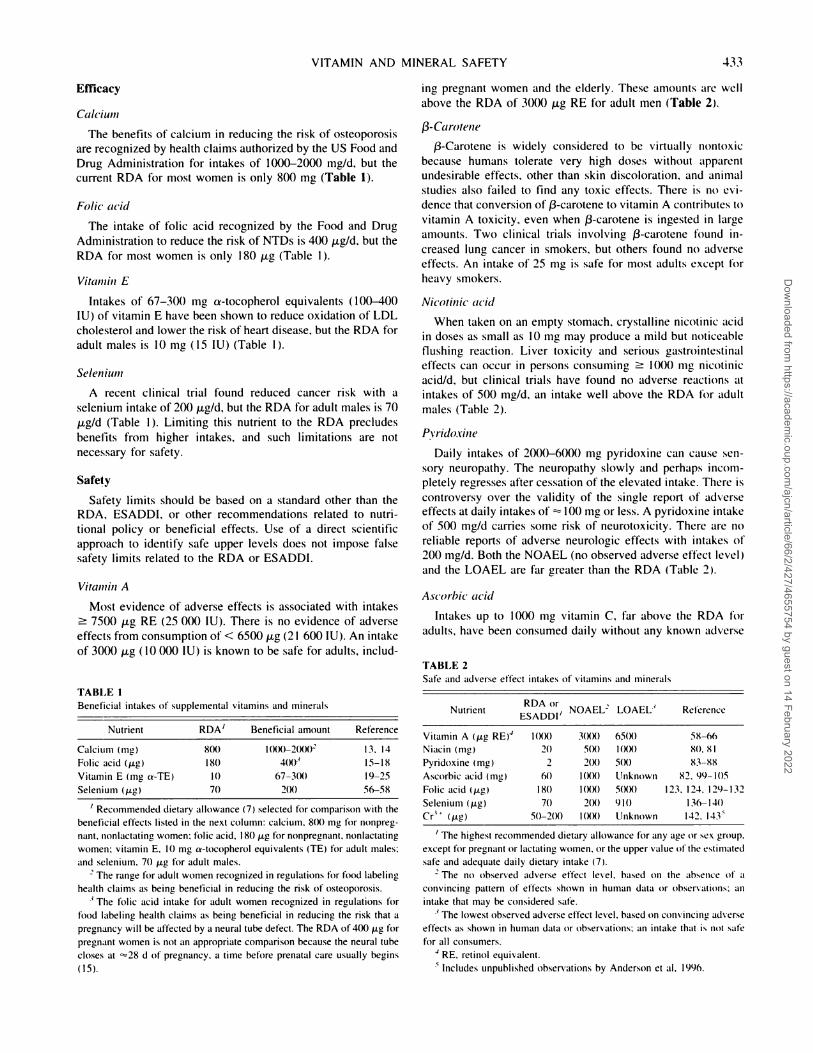
Vitanii,i A
Most evidence of adverse effects is associated with intakes
� 7500 �.tg RE (25 000 LU). There is no evidence of adverse
effects from consumption of < 6500 p.g (2 1 600 IU). An intake
of 3000 j.tg ( 10 000 IU) is known to be safe for adults, includ-
TABLE I
Beneficial intakes of supplemetital vitamins and minerals
Nutrient RDA’ Beneficial amount Reference
Calcium (mg) 800 l00()�2(X)02 13. 14
Folic acid (�.tg) 180 4(X)� 15-18
Vitamin E (mg s-TE) 10 67-3(8) 19-25
Selenium (gig) 70 2(8) 56-58
I Recommended dietary allowance (7) selected for comparison with the
beneficial effects listed in the next column: calcium, 8(8) mg for nonpreg-
nant, nonlactating women: folic acid, I 80 .tg for nonpregnant. nonlactating
women: vitamin E. 10 mg a-tocopherol equivalents (TE) for adult males:
and selenium. 70 �zg for adult males.
2 The range kr adult women recognized in regulations for food labelinghealth claims as being beneficial in reducing the risk of osteoporosis.
3 The folic acid intake for adult women recognized in regulations for
food labeling health claims as being beneficial in reducing the risk that a
pregnancy will be affected by a neural tube defect. The RDA of400 �zg for
pregnant women is not an appropriate comparison because the neural tube
closes at �28 d of pregnancy. a time before prenatal care usually begins
(15).
ing pregnant women and the elderly. These amounts are well
above the RDA of 3000 j.�g RE for adult men (Table 2.
13-Carotene
13-Carotene is widely considered to be virtually nontoxic
because humans tolerate very high doses without apparent
undesirable effects, other than skin discoloration, and animal
studies also failed to find any toxic effects. There is no cvi-
dence that conversion of 13-carotene to vitamin A contributes to
vitamin A toxicity, even when 13-carotene is ingested in large
amounts. Two clinical trials involving 13-carotene found in-
creased lung cancer in smokers, but others found no adverse
effects. An intake of 25 mg is safe for most adults except for
heavy smokers.
Nicotinic’ (U’i(l
When taken on an empty stomach, crystalline nicotinic acid
in doses as small as 10 mg may produce a mild but noticeable
flushing reaction. Liver toxicity and serious gastrointestinal
effects can occur in persons consuming � 1000 mg nicotinic
acid/d. but clinical trials have found no adverse reactions at
intakes of 500 mg/d. an intake well above the RDA for adult
males (Table 2).
Pvridoxine
Daily intakes of 20��()-600() mg pynidoxine can cause sen-
sony neuropathy. The neuropathy slowly and perhaps incom-
pletely regresses after cessation of the elevated intake. There is
controversy over the validity of the single report of adverse
effects at daily intakes of � 100 mg or less. A pynidoxine intake
of 5(X) mg/d carries some risk of neurotoxicity. There are no
reliable reports of adverse neunologic effects with intakes of
200 mg/d. Both the NOAEL (no observed adverse effect level)
and the LOAEL are far greater than the RDA (Table 2.
Ascorbic acid
Intakes up to 1000 fig vitamin C, far above the RDA for
adults, have been consumed daily without any known adverse
TABLE 2
Safe and adverse effect intakes of vitamins and minerals
NutrientRDA or
ESADDI’NOAEL LOAEL3 Relerence
Vitamin A (ftg RE)’ 1(88) 3(8%) 65(8) 58-66
Niacin (mg) 20 5(8) 1(88) 80. 81
Pyridoxine (mg) 2 2(8) 5(8) 83-88
Ascorbic acid (mg) fit) 1(88) Unknown 82. 99-lOS
Folic acid (Mg) 180 1(88) 5(8%) 123. 124, 129-132
Selenium (Mg) 70 2(8) 910 136-140
Cr� (jig) 5()-2(X) 1(8%) Unknown 142. l43�
, The highest recommended dietary allowance for any age or sex group.
except for pregnant or lactating women. or the upper value of the estimated
safe and adequate daily dietary intake (7).
2 The no observed adverse effect level, based on the absence of a
convincing pattern of effects shown in human data or observations: an
intake that may be considered safe.
3 The lowest observed adverse effect level, based on convinctng adverse
effects as shown in human data or observations: an intake that is not safe
for all consumers.
4 RE, retinol equivalent.
S Includes unpublished observations by Anderson et al, 1996.
Dow
nloaded from https://academ
ic.oup.com/ajcn/article/66/2/427/4655754 by guest on 14 February 2022
434 HATHCOCK
effects (Table 2). Most of the purported adverse effects attnib-
uted to vitamin C have no factual basis.
Folic acid
Folic acid is nontoxic but concern has been raised about high
intakes masking pernicious anemia. This effect is established
only at intakes � 5000 p.g. Intakes of 1000 �g (1 mg) total
folic acid plus food folates are without identifiable risk of any
known adverse effects. This intake is well above the RDA for
women (Table 2).
Selenium
The margin of safety for selenium is relatively narrow.
Adverse effects have occurred at intakes of 9 10 �sg/d. Some
risk of adverse effects may occur with total dietary intakes as
low as 600 �g/d. Daily supplemental intakes of 200 �.tg have
been shown to be safe (Table 2).
Chromium
No credible data or reports have shown adverse effects of
dietary trivalent chromium in humans, and animal data also
suggest that orally administered trivalent chromium is cx-
tremely nontoxic. Reports of DNA damage by chromium do
not apply to oral intakes of the forms found in foods and dietary
supplements. The benign character of oral trivalent chromium
should not be confused with the established toxicity of inhaled
hexavalent chromium, which is associated with workplace-
related lung cancer. Hexavalent chromium is not normally
found in foods and is not used in dietary supplements. There is
sufficient experience with intakes of trivalent chromium, as
chromium picolinate, up to 1000 �g Cn/d, along with the wide
margin of safety in animal studies, to establish the safety of
trivalent chroniium at this intake (Table 2). A
REFERENCES
I . Food and Nutrition Board. How should the recommended dietary
allowances be revised? Washington, DC: National Academy Press.I 994.
2. World Health Organization. Trace elements in human nutrition andhealth. Geneva: World Health Organization, 1996.
3. Hathcock JN. Risk/benefit analysis for vitamin supplements. In:
Hathcock iN, ed. Nutritional toxicology. Vol 3. Orlando. FL: Aca-
deniic Press, 1989:141-53.
4. Hathcock iN. Safety limits for nutrient intakes: concepts and data
requirements. Nutr Rev 1993:51:278-85.
5. Hathcock J. Safety limits for nutrients. J Nutr l996:126(suppl):
2386S-9S.
6. Food and Nutrition Board. Recommended dietary allowances. 9th ed.Washington. DC: National Academy Press. 1980.
7. Food and Nutrition Board. Recommended dietary allowances. 10thed. Washington. DC: National Academy Press, 1989.
8. Committee on Nutrition and FOOdS for Special Dietary Uses. Codex
Alimentanius Commission. Draft guidelines for dietary supplements
(vitamins and minerals). Rome: FAOIUNU/WHO, 1995. (ALl-
NORM 95/26.)
9. US Department of Health and Human Services. The Surgeon Gen-
eral’s report on nutrition and health. Washington, DC: US Govern-
ment Printing Office. I 988.
10. Committee on Diet and Health. Diet and health. Washington, DC:
National Academy Press. 1989.
I I . Thomas PR. Food for thought about dietary supplements. Nutr Today
I 996:31:46-54.
I 2. Dourson ML. Methods for establishing oral reference doses. In:
Mertz W, Abernathy CO. Olin 55, eds. Risk assessment of essentialelements. Washington. DC: ILSI Press, 1994:51-61.
13. Optimal calcium intake. NIH Consens Statement 1994:12:1-31.
14. Food and Drug Administration. Food labeling: health claims: calcium
and osteoporosis. Fed Regist 1994:58:2665-81.
15. Food and Drug Administration. Food labeling: health claims and
label statements: folate and neural tube defects. Fed Regist
1996:61:8752-81.
16. Boushey CJ. Beresford SA. Omenn GS, Motulsky AG. A quatititative
assessment of plasma homocysteine as a risk factor for vascular
disease: probable benefits of increasing tilic acid intakes. JAMA
1995:274:1049-57.
17. den Heijer MD. Koster T. Blom Hi. et al. Hyperhomocysteinemia as
a risk factor for deep-vein thrombosis. N EngI I Med 1996:
334:759-62.
18. Malinow MR. Plasma honiocysteitie: a risk factor for arterial oc-
elusive diseases. I Nutr I 996: 126(suppl): I 238S-43S.
19. Stampfer Mi. Rimm EB. Epidemiologic evidertce for vitamin E in
prevention of cardiovascular disease. Am I Clin Nutr 1995:
62(suppl): 1365S-9S.
20. Rimm EB. Stampfer Mi, Ascherio A. Giovannucci E. Colditz GA,
Willett WC. Vitaniiii E consumption and the risk of coronary heart
disease in men. N EngI J Med l993:328:145()-6.
21. iialal I, Fuller Ci, Huet BA. The effect of a-tocopherol supplemen-
tation (in LDL cholesterol oxidation. Arterioscler Thromb Vase Biol
1995:15:190-8.
22. Hodis HN, Mack Wi, LaBree L, et al. Serial coronary angiographic
evidence that antioxidant vitamin intake reduces progression of cor-
onary artery atherosclerosis. JAMA 199�:273:1849-54.
23. Stephens NG, Parsons A. Schofield PM, et al. Randomised controlled
trial of vitamin E in patients with coronary disease: Cambridge Heart
Antioxidant Study (CHAOS ). Lancet I 996:347:781-5.
24. Fuller Ci. Chandalia M, Garg A, Grundy SM, Jialal I. RRR-a-
tocopheryl acetate supplementation at pharmacologic doses decreases
low-density-lipoprotein oxidative susceptibility hut not protein gly-
cation in patients with diabetes mellitus. Am I Clin Nutr
1996:63:753-9.
25. Miwa K, Miyagi Y. Igawa A. Nakagawa K, lnoue H. Vitamin E
deficiency in variant angina. Circulation 1996:94:14-8.
26. Alpha-Tocopherol, Beta Carotene (ATBC) Cancer Prevention Study
Group. The effect of vitamin E and beta carotene Ofl the incidence of
lung cancer and other cancers in male smokers. N EngI I Med
I 994:330:1029-35.27. Kushi LH, Folsom AR, Prineas Ri, Mink P1, Wu Y, Bostick RM.
Dietary antioxidatit vitamins and death from coronary heart disease in
postmenopausal women. N EngI J Med 1996:334:1 156-62.
28. Knekt P. Aromaa A, Maatela I. et al. Vitamin E and cancer preven-
tion. Atii J Clin Nutr 1991:53:283S-flS.
29. Shklar G, Schwartz IL, TrickIer D, Reid S. Prevention of experimen-
tal cancer and imniunostimulation by vitamin E (imniunosurveil-
lance). J Oral Pathol Med l990:l9:6()-4.
30. Tannenbaum SR. Wishnok IS, Leaf CD. Inhibition of nitrosamine
formation by ascorbic acid. Am I Clin Nutr 1991:53:2475-505.3 1 . Schorah Ci. Sobala GM, Sanderson M, Collis N. Primrose IN.
Gastric juice ascorbic acid: effects of disease and implications t�rgastric carcinogenesis. Am I Cliii Nutr 1991:53:2875-935.
32. Cornea P. Human gastric carcinogenesis: a multistep and multifacto-
rial process-First American Cancer Society Award Lecture on Can-
cer Epidemiology and Prevention. Cancer Res 1992:52:6735-40.33. Food and Drug Administration. Food labeling: health claims and
label statements: antioxidant vitamins and cancer. Fed Regist
I 993:58:2622-60.
34. Block G. Epidemiologic evidence regarding vitamiti C and cancer.
Am I Clin Nutr 1991:54(suppl):I3IOS-4S.
35. Block G. Vitamin C and cancer preventioti: the epiderniological
evidence. Am I Clin Nutr 1991:53:270S-82S.
Dow
nloaded from https://academ
ic.oup.com/ajcn/article/66/2/427/4655754 by guest on 14 February 2022
VITAMIN AND MINERAL SAFETY 435
36. Thomas SR. Neuzil I, Mohr D, Stocker R. Coantioxidants make
a-tocophcrol an efficient antioxidant for low-density lipoprotein.
Am J Clin Nutr l995:62(suppl):l357S-64S.
37. Chamiec 1. Herhaczynska-Cedro. Ceremuzynski L. Klosiewicz-
Wasek B. Wasek W. Effects of antioxidant vitamins C and E on
signal-averaged electrocardiogram in acute myocardial infarction.
Am J Cardiol 1996:77:237-41.
38. Singh RB. Niaz MA. Rastogi 55. Rastogi S. Usefulness of antioxi-
dant vitamins in suspected acute myocardial infarction (The Indian
Experiment of Infarct Survival-3. Am J Cardiol 1996:77:232-6.
39. Losonczy KG. Harris TB. Havlik Ri. Vitamin E and vitamin C
supplement use and risk of all-cause and coronary heart disease
mortality in older persons: the Established Populations for Epidemi-
ologic Studies of the Elderly. Am J Clin Nutr 1996:64: l9()-6.
40. s an Poppel G. Goldhohm RA. Epidemiologic evidence for �-caro-
tene and cancer prevention. Am I Clin Nutr 1995:62(suppl):
I 3935-402S.
41. Sies H, Stahl W. Vitamins E and C, beta-carotene. and other carote-
noids as antioxidants. Ani J Clin Nutr l995:62(suppl):l3I5S-2lS.
42. Acevedo P. Bertram iS. Liarozole potentiates the cancer chemopre-
ventive activity of and the up-regulation of gap junctional commu-
nication and connexin 43 expression by retinoic acid and beta-
carotene in lOTl/2 cells. Carcinogenesis 1995:16:2215-22.
43. (;regus Z. Klaassen CD. Mechanisms of toxicity. In: Klaassen CD,
ed. Casarett and Doull’s toxicology: the basic science of poisons.
New York: McGraw-Hill. 1996:35-74.
44. Hennekens CH. Buring JE. Manson JE. et al. Lack of effect of
long-terni supplementation with beta carotene on the incidence of
malignant neoplasms and cardiovascular disease. N EngI J Med1996:334:1 145-90.
45. Omenn GS. Goodman GE, Thomquist MD. et al. Effects of a com-
hination of beta-carotene and vitamin A on lung cancer and cardio-
vascular disease. N EngI J Med 1996:334:1 150-S.
46. Handelman GJ. Carotenoids as scavengers of active oxygen species.
In: Cadenas E. Packer L, eds. Handbook of antioxidants. New York:
Marcel Dekker. 1996:259-314.
47. Bertram iS, Bortkiewicz H. Dietary carotenoids inhibit neoplastic
transformation and niodulate gene expression in mouse and human
cells. Am J Clin Nutr 1995:62(suppl):l327S-36S.
48. Krinsky NI. Carotenoids and cancer: basic research studies. In: Frei
B. ed. Natural antioxidants in human health and disease. San Diego:Academic Press. 1994:239-61.
49. Tatsuta M. Mikuni T, Taniguchi H. Protected effect of butylated
hydroxytoluene against induction of gastric cancer by N-methyl-N’-
nito-N-nitrosoguanidine in Wistar rats. Int J Cancer 1983:32:253-4.50. Willianis GM, Wang CX. latropoulos Mi. Toxicity studies of buty-
lated hydroxyanisole and butylated hydroxytoluene. 2. Chronic feed-ing studies. Food Chem Toxicol 1990:28:799-806.
5 I . Miller YE. Pulmonary neoplasms. In: Bennett JC. Plum F. eds. Cecil
textbook of medicine. 20th ed. Philadelphia: WB Saunders Company.
I 996:436-42.
52. Combs GF Jr. Essentiality and toxicity of selenium: a critique of the
recommended dietary allowance and the reference dose. In: Mertz W,
Abernathy CO. Olin 55, eds. Risk assessment of essential elements.
Washington, DC: ILSI Press. 1994:167-83.
53. Blot Wi, Lie J-Y. Taylor PR. et al. Nutrition intervention trials in
Linxian. China: supplementation with specific vitamin/mineral com-
binations, cancer incidence, and disease-specific mortality in the
general population. J NatI Cancer Inst 1993:85:1483-92.54. Li JY. Taylor PR. Li B. Nutrition intervention trials in Linxian.
China: multiple vitamin/niineral supplementation. cancer incidence.�md disease-specific mortality aniong adults with esophageal dyspla-
sia. J NatI Cancer Inst 1993:85:1492-8.
55. Clark LC. Combs GF Jr. Turnbull BW. The nutritional prevention of
cancer with seleniuni 1983-1993: a randomized clinical trial. FASEB
J l996:l0:A550 (ahstr).
56. Clark LC. Combs GF, Turnbull BW, et al. Effect of selenium sup-
plementation for cancer prevention in patients with carcinoma of the
skin. JAMA 1996:276:1957-68.
57. Combs GF Jr. Clark LC. Selenium. In: Garewal HS, ed. Antioxidant
nutrients and disease prevention. New York: CRC Press, 1997.
58. Hathcock iN. Hattan DG, Jenkins MY, McDonald IT. Sundaresan
PR. Wilkening VL. Evaluation of vitamin A toxicity. Am I Clin Nutr
I990:52:183-202.
59, Geubel AP, Dc Galocsy C, Alves N. Rahier J. Dive C. Liver damage
caused by therapeutic vitamin A administration: estimate of dose-
related toxicity in 41 cases. Gastroenterology 1991 :l0t�: 1701-9.
fit). Rothman KJ. Motre LL, Singer MR. Nguyen UDT. Mannino S.
Milunsky A. Teratogenicity of high level vitamin A intake. N EngI
J Med 1995:333:1369-73.
61. Oakley GP. Erickson JD. Vitamin A and birth defects. N EngI I Med
1995:333:1414-5.
62. Shaw GM. Wasserman CR. Block G. Lammer El. High maternal
vitamin A intake and risk of anomalies of structures with a cranial
neural crest cell contribution. Lancet 1996:347:899-900.
63. Werler MM, Lammer El, Mitchell AA. Teratology of high vitaniin A
intake. N EngI J Med 1996:334:1 195-6 (letter).
64. Rosa FW, Wilk AL. Kelsey FO. Teratogen update: vitamin A con-
geners. Teratology I 986:33:355-64.65. Krasinski SD, Russell RM. Otradovec CL. et al. Relationship of
vitamin A and vitamin E intake to fasting plasma retinol. retinol-
binding protein. retinyl esters, carotene, a-tocopherol. and cholesterol
among elderly and young adults: increased plasma retinyl esters
among vitamin A-supplement users. Am J Clin Nutr 1989;49:112-20.
66. Johnson EJ. Krall EA, Dawson-Hughes B. Dallal GE. Russell RM.Lack of an effect of multivitamins containing vitamin A on serum
retinyl esters and liver function tests in healthy women. J Am CoIl
Nutr 1992:11:682-6.
67. Bendich A. The safety of beta carotene. Nutr Cancer 1988:
I 1:207-14.
68. Diplock AT. Safety of antioxidant vitamins and 13-carotene. Am I
Clin Nutr l995:62(suppl):l5lOS-6S.
69. Olson JA. Vitamin A, retinoids and carotenoids. In: Shils ME, Olson
JA. Shike M. eds. Modern nutrition in health and disease. 8th ed.
Philadelphia: Lea and Febiger. 1994:287-307.70. Matthews-Roth MM. Beta-carotene therapy for erythrbpoietic proto-
porphyria and other photosensitivity diseases. Biochitiiie 1986:
68:875-84.
71. Greenberg ER. Baron JA. Stukel TA, et al. A clinical trial of beta
carotene to prevent basal-cell and squamous-cell cancers of the skin.
N EngI J Med 1990:323:789-95.72. Greenberg ER. Baron JA. Tosteson TD, et al. A clinical trial of
antioxidant vitamins to prevent colorectal adenoma. N EngI J Med
1994:331 :14 1-7.
73. Menkes MS. Comstock GW, Vuilleumier JP, Helsing KJ. Rider AA,
Brookmeyer R. Serum beta-carotene, vitamins A and E. selenium,
and the risk of lung cancer. N EngI J Med 1986:315:1250-4.
74, Hennekens CH. Micronutrients and cancer prevention. N EngI J Med1986:31�:1288-9.
75. Lachance PA. “Natural” cancer prevention. Science 1996:
272:1860-I.
76. Albanes D, Heinonen OP. Taylor PR. et al. cs-Tocophcrol and fi-car-
otene supplements and lung cancer incidence in the Alpha-Toco-pherol Beta-Carotene Cancer Prevention Study: effects of base-line
characteristics and study compliance. J NatI Cancer Inst 1996:
88: I 560-70.
77. Omenn GS. Goodnian GE. Thornquist MD. et al. Risk factors for
lung cancer and for intervention effects in CARET. the Beta-Cam-
tene and Retinol Efficacy Trial. I NatI Cancer Inst 1996:88: I 550-9.
78. Mayne ST. Handelman. GJ. Beecher G. p3-Carotene and lung cancer
promotion in heavy smokers-a plausible relationship? J NatI Cancer
Inst 1996:88:1513-5.
79. Bean WB. Some aspects of pharmacologic use and abuse of water-
Dow
nloaded from https://academ
ic.oup.com/ajcn/article/66/2/427/4655754 by guest on 14 February 2022
436 HATHCOCK
soluble vitaniins. In: Hathcock IN. Coon I, eds. Nutrition and drug
interrelations. New York: Academic Press, 1978:667-85.
80. Rader II. Calvert RI. Hathcock IN. Hepatic toxicity of unmodified
and time-release preparations of niacin. Am I Med 1992:92:77-81.
8 1 . McKenney iM. Proctor ID. Hamis S. Chinchilli VM. A comparisonof the efficacy and toxic effects of sustained vs immediate-release
niacin in hypercholesterolemic patients. JAMA 1994:271:672-7.
82. Hathcock IN, Rader II. Micronutrient safety. Ann N Y Acad Sci
1990:587:257-66.
83. Schaumburg H. Kaplan I. Windebank A. et al. Sensory neuropathy
froni pyridoxine abuse. N EngI I Med 1983:309:445-8.
84. Albin RL. Albers 1W, Greenberg HS. et al. Acute sensory neuropa-
thy-neuronopathy from pyridoxine overdose. Neurology I 987:37:
I 729-32.
85. Albin RL. Albers 1W. Long-term ftllow-up of pyridoxine-induced
acute sensory neuropathy-neuronopathy. Neurology I 990:40: 13 19.86. Santoro L. Ragno M. Nucciotti R, Barbieri F, Caruso G. Pyridoxine
neuropathy: a four year electrophysiological and clinical follow-up of
a severe case. Acta Neumol 1991:13:13-8.
87. Parry GI. Bredesen DE. Sensory neuropathy with low-dose pyridox-
inc. Neurology 1985:35:1466-8.
88. Bcndich A. Cohen M. Vitamin B6 safety issues. Ann N Y Acad Sci
I 990:585:321-3.
89. Dalton K. Dalton MIT. Characteristics of pyridoxine overdose neu-
ropathy syndrome. Acta Neurol Scand 1987:76:8-Il.
90. Daudon M, Reveillaud Ri. Normand M. Petit C. lungers P. Pyridoxi-
late-induced calcium oxalate calculi: a new drug-induced metabolic
nephrolithiasis. I Urol 1987:138:258-61.
91. Curhan GC. Willett WC, Rimni EB, Stampfer MI. A prospective
study of the intake of vitamins C and Be,, and the risk of kidney stones
in men. I Urology 1996:155:1847-51.
92. DiPalma JR. Ritchie DM. Vitamin toxicity. Annu Rev Pharmacol
Toxicol I977: 17: I33-48.
93. Danford DE. Munro HN. Water-soluble vitamins. In: Gilman AG,
Goodman LS. Gilman A. eds. The pharmacological basis of thera-
peutics. New York: Macmillan. 1980:1560-82.
94. Alhadeff L, Gualtieri CT. Lipton M. Toxic effects of water-soluble
vitamins. Nutr Rev 1984:42:33-40.
95. Cochrane WA. Ovemnutrition in prenatal and neonatal life: a prob-
lem� Can Med I 1965:93:893-9.96. Schrauzer GN. Rhead Wi. Ascorbic acid abuse: effects of long-term
ingestion ofexcessive amounts on blood levels and urinary excretion.
Int I Vitam Nutr Res 1973:43:201-Il.97. Tsao CS. Leung PY. Urinary ascorbic acid levels following with-
drawals of large doses of ascorbic acid in guinea pigs. I Nutr
I 988: I I 8:895-9(8).
98. Siegel C. Barker B. Kunstadter M. Conditioned oral scurvy due to
megavitaniin C withdrawal. I Periodontol 1982:53:453-5.
99. Hoffer A. Ascorbic acid and kidney stones. Can Med Assoc I1985:132:320 (letter).
100. Levine M. Conry-Cantilena C. Wang Y. et al. Vitamin C pharmaco-
kinetics in healthy volunteers: evidence for a recommended dietary
allowance. Proc Natl Acad Sci U S A 1996:93:3704-9.101 . Urivetzky M. Kessaris D, Smith AD. Ascorbic acid overdosing: a risk
factor for calcium oxalate nephrolithiasis. I Umol 1992:147:1215-8.
102. Fituri N. Allawi N, Bentley M. Costello I. Urinary and plasmaoxalate during ingestion of pure ascorbic acid: a re-evaluation. Eur
Urol 1983:9:312-5.
103. Wandzilak TR. D’Andre SD. Davis PA, Williams HE. Effect of high
dose vitamin C on urinary oxalate levels. I Urol 1994:1�1:834-7.
l()4. Costello I. Ascorbic acid overdosing: a risk factor for calcium oxalate
nephrolithiasis. I Urol 1993:149:1 146 (letter).
105. Gerster H. Do high doses of vitamin C cause kidney stones? Son-
derdrunck Ernahr/Nutr 1986:9:614-7.
l()6. Fellstrom B. Danielson BG. Karlstrom B. Lithell H. Ljunghall S.
Vessby B. Dietary habits in renal stone patients compared with
healthy subjects. Br J Urol 1989:63:575-80.
107. Herbert V. Does mega-C do more good than harm. or more harm than
good? NutrToday 1993:51:28-32.
108. Herbert V. Shaw 5, Iayatilleke E. Vitaniin C-driven free radical
generation frotii iron. I Nutr I 996: 126(suppl): 1213S-20S.
109. Kondo H. Saito K, Grasso IP, Aisen P. Iron metabolism in the
erythrophagocytosing Kupffer cell. Hepatology I 988:8:32-8.
I 10. Frei B. Ascorbic acid protects lipids in human plasma and low-
density lipoprotein against oxidative damage. Am J Clin Nutr
199 1:�4: 1113S-8S.I 1 1 . Sullivan IL. Iron and sex difference in heart disease risk. Lancet
1981:1:1293-4.
I 12. Salonen IT, Nyyssonen K. Korpela H, Tuomilehto I. Seppanen R.
Salonen R. High stored iron levels are associated with excess risk of
myocardial infarction in eastern Finnish men. Circulation
1992:86:803-Il.
I 13. Sempos CT, Looker AC. Gillum RF. Iron and heart disease: the
epidemiologic data. Nutr Rev 1996:54:73-84.
I 14. Liao Y. Cooper RS, McGee DL. Iron status and coronary heart
disease: negative findings from the NHANES I epidemiologic fol-
low-up study. Am I Epideniiol 1994:139:704-12.
1 15. Aronow WS. Serum femtin is not a risk factor for coronary artery
disease in men and women aged � 62 years. Am J Cardiol
1993:72:347-8.
I 16. Moore M. Folson AR. Barnes RW, Eckfeldt IH. No association
between serum ferritin and asymptomatic carotid atherosclerosis: the
Atherosclerosis Risk in Communities (ARIC) Study. Am I Epidemiol
1995: 141:7 19-23.
1 17. Baem DM. Tekawa IS. Hurley LB. Iron stores are not associated with
acute myocardial infarction. Circulation 1994:89:2915-8.
I 18. Morrison HI. Semenciw RM, Mao Y. Wigle DT. Serum iron and risk
of fatal acute myocardial infarction. Epidemiology 1994:5:243-6.
I 19. Cok JD. Watson SS, Simpson KM. Lipschitz DA, Skikne BS. The
effect of high ascorbic acid supplementation on body iron stores.
Blood I994:64:721-6.
120. Bendich A, Langseth L. The health effects of vitamin C supplemen-
tation: a review. I Am CoIl Nutr 1995:14:124-36.
I 2 1 . Miller DR. Hayes KC. Vitamin excess and toxicity. In: Hathcock IN.
ed. Nutritional toxicology. Vol 1 . New York: Academic Press,
1982:81-133.
122. Hill RE. Kamath KR. “Pink” diarrhoea: osmotic diarrhoea from a
sorbitol-containing vitamin C supplement. Med I Aust I 982:1:387-9.
123. Butterworth CE Jr. Tamura T. Folic acid safety and toxicity: a brief
review. Am I Clin Nutr 1989:50:353-8.
124. Food and Drug Administration. Food labeling: health claims and
label statements: folate and neural tube defects: proposed rules. Fed
Regist 1993:58:53254-88.
125. Mukherjee MD. Sandstead HH. Ratnaparkhi MV. Johnson LK,
Milne DB. Stelling HP. Maternal zinc, iron. folic acid. and protein
nutriture and outcome of human pregnancy. Am I Clin Nutr
I 984:40:496-507.
126. Milne DB. Canfield WK, Mahalko JR. Sandstead HH. Effect of oral
folic acid supplements on zinc. copper. and iron absorption and
excretion. Am I Clin Nutr 1984:39:535-9.
I 27. Simmer K. lames C. Thompson RPH. Are iron-folate supplementsharmful? Am I Clin Nutr 1987:45:122-5.
128. Tamura T. Goldenberg RL. Freeberg LE. Cliver SP, Cutter GR.
Hoffman Hi. Maternal serum folate and zinc concentrations and their
relationships to pregnancy outcome. Am I Clin Nutr 1992:56:
365-70.
129. Kauwell GP. Bailey LB. Gregory iF III. Bowling DW. Cousins RI.Zinc status is not adversely affected by folic acid supplementation
and zinc intake does not impair folate utilization in human subjects.
I Nutr 1995:125:66-72.
130. Wald N, Sneddon I, Densem I, Frost C, Stone R, The MRC Vitamin
Study Research Group. Prevention of neural tube defects: results of
the Medical Research Council Vitamin Study. Lancet 1991;
338: 13 1-7.
Dow
nloaded from https://academ
ic.oup.com/ajcn/article/66/2/427/4655754 by guest on 14 February 2022

Erratum
Jeppesen J, Schaaf P. Jones C, Zhou M-Y, Chen Y-DI, Reaven GM. Effects of low-fat,
high-carbohydrate diets on risk factors for ischemic heart disease in postmenopausal women.
Am J Clin Nutr 1997;65:l027-33.
The legends to Figures 1. 2, and 3 on pages 1029, 1030, and 103 1 should read as follows in part:
40% (U) and 60% (0).
VITAMIN AND MINERAL SAFETY 437
I 3 1. Czeizel A, Dudds I. Prevention of the first occurrence of neural-tube
defects by preconceptual vitamin supplementation. N EngI I Med
I992:327:1832-S.
I 32. Morgan SL. Baggott lE. Vaughn WH. et al. The effect of folic acidsupplementation on the toxicity of low-dose methotrexate in patients
with rheumatoid arthritis. Arthritis Rheum 1990:33:9-18.
133. National Research Council. Selenium in nutrition. Revised ed. Wash-ington. DC: National Academy Press, 1983.
I 34. Jensen R. Clossen W, Rothenberg R. Selenium intoxication-NewYork. MMWR Morbid Mortal WkIy Rep 1984:33:157-8.
135. Helzsouer K, Jacobs R, Morris S. Acute selenium intoxication in the
United States. Fed Proc 1985:44:1670 (abstr).
I 36. Yang G. Wang S. Zhou R. Sun S. Endemic selenium intoxication of
humans in China. Am I Clin Nutr 1983:37:872-81.
137. Yang G, Zhou R, Yin 5, et al. Studies of safe maximal daily dietary
selenium intake in a seleniferous area in China, I : selenium intake
and tissue levels of the inhabitants. I Trace Elem Electrolytes Health
Dis 1989:3:77-87.
I 38. Yang G. Yin S. Zhou R. et al. Studies of safe maximal daily dietary
selenium intake in a seleniferous area in China, 2: relation between
selenium intake and the manifestation of clinical signs and certain
biochemical alterations in blood and urine. I Trace Elem Electrolytes
Health Dis 1989:3:123-30.
I 39. Longnecker MP. Taylor PR. Levander OA. et al. Selenium in diet.
blood. and toenails in relation to human health in a seleniferous area.
Ani I Clin Nutr 1991:53:1288-94.140. Yang G. Zhou R. Further observations on the human maximuni safe
dietary seleniuni intake in a seleniferous area of China. I Trace Elem
Electrolytes Health Dis 1994:8:159-65.
141. Nielsen FW. Chromium. In: Shils ME, Olson IA. Shike M, eds.
Modern nutrition in health and disease. 8th ed. Philadelphia: Lea and
Febiger. 1994:264-8.
142. Dourson ML. The chromium reference dose. In: Mertz W, Abernathy
CO. Olin 55, eds. Risk assessment of essential elements. Washing-
ton, DC: ILSI Press. 1994:207-12.
143. Gad SC. Acute and chronic systemic chromium toxicity. Sci Total
Environ 1989:86:149-57.
144. Stearns DM. Wise IP Sr. Patiemno SR. Wetterhahn KE. Chromiuni
(III) picolinate produces chromosome damage in Chinese hamster
ovary cells. FASEB I 1995:9:1643-8.
145. Stearns DM. Kennedy U. Courtney KD. Giangrande PH. Phieffer
LS, Wetterhaun KE. Reduction ofchromium (VI) by ascorbate leads
to chromium-DNA binding and DNA strand breaks in vitro. Bin-
chemistry 1995:34:910-9.
146. Wetterhahn KE, Stearns DM. Giangrande P. Phieffer LS. CourtneyKD. The role of ascorbate in metabolism and genotoxicity of chmo-
mium (VI). Proc Annu Meet Am Assoc Cancer Res l993:34:A938
(abstr).
147. Stearns DM, Wetterhahn KE. Reaction ofchromium (VI) with ascor-
bate produces chromium (V), chromium (IV). and carbon-based
radicals. Chem Res Toxicol 1994:7:219-30.
148. Stearns DM. Courtney KD. Giagrande PH. Phieffer LS. Wetterhahn
KE. Chromium (VI) reduction by ascorbate: role of reactive inter-
mediates in DNA damage in vitro. Environ Health Perspect 1994:
I 02(suppl 3):2 I-S.
149. Cimino MC. EPA use of in vivo germ cell mutagenicity data. Environ
Mol Mutagen 1991:18:295-7.
ISO. Dearfield KL. Auletta AE. Cimino MC. Moore MM. Considerations
in the U.S. Environmental Protection Agency’s testing approach for
mutagenicity. Mutat Res 1991:258:259-83.
151 . Auletta AE. Dearfield KL, Cimino MC. Mutagenicity test schemes
and guidelines: U.S. EPA Office of Pollution Prevention and Toxics
and Office of Pesticide Programs. Environ Mol Mutagen
1993:21:38-45.
152. Lachance P. Langseth L. The RDA concept: time for a change? NutrRev 1994:52:266-70.
Dow
nloaded from https://academ
ic.oup.com/ajcn/article/66/2/427/4655754 by guest on 14 February 2022