to cut or not to cut: a modeling approach for assessing the role of male circumcision in hiv control
TRANSCRIPT

Bulletin of Mathematical Biology (2007) 69: 2447–2466DOI 10.1007/s11538-007-9226-9
O R I G I NA L A RT I C L E
To Cut or Not to Cut: A Modeling Approach for Assessingthe Role of Male Circumcision in HIV Control
C.N. Poddera, O. Sharomia, A.B. Gumela,∗, S. Mosesb
aDepartment of Mathematics, University of Manitoba, Winnipeg, MB, R3T 2N2, CanadabDepartment of Medical Microbiology and Medicine, University of Manitoba, Winnipeg,MB, R3T 2N2, Canada
Received: 11 October 2006 / Accepted: 25 April 2007 / Published online: 8 June 2007© Society for Mathematical Biology 2007
Abstract A recent randomized controlled trial shows a significant reduction in women-to-men transmission of HIV due to male circumcision. Such development calls for a rigor-ous mathematical study to ascertain the full impact of male circumcision in reducing HIVburden, especially in resource-poor nations where access to anti-retroviral drugs is lim-ited. First of all, this paper presents a compartmental model for the transmission dynam-ics of HIV in a community where male circumcision is practiced. In addition to havinga disease-free equilibrium, which is locally-asymptotically stable whenever a certain epi-demiological threshold is less than unity, the model exhibits the phenomenon of backwardbifurcation, where the disease-free equilibrium coexists with a stable endemic equilibriumwhen the threshold is less than unity. The implication of this result is that HIV may persistin the population even when the reproduction threshold is less than unity. Using partialdata from South Africa, the study shows that male circumcision at 60% efficacy level canprevent up to 220,000 cases and 8,200 deaths in the country within a year. Further, it isshown that male circumcision can significantly reduce, but not eliminate, HIV burden ina community. However, disease elimination is feasible if male circumcision is combinedwith other interventions such as ARVs and condom use. It is shown that the combineduse of male circumcision and ARVs is more effective in reducing disease burden thanthe combined use of male circumcision and condoms for a moderate condom compliancerate.
Keywords HIV/AIDS · Male circumcision · Reproduction number · Backwardbifurcation · Condoms · ARVs
∗Corresponding author.E-mail address: [email protected] (A.B. Gumel).
2448 Podder et al.
1. Introduction
Since its emergence in the 1980s, the human immune deficiency virus (HIV) has claimedthe lives of millions of people (20 million), and continues to exert a significant socio-economic and public health burden around the globe. The current UNAIDS report es-timates about 38.6–46 million people living with HIV at the end of 2005, and an es-timate of 4.1 million new infections recorded in that year (Report on the global AIDSepidemic, 2006). Further, sexual intercourse accounts for 80% of all cases (Robert et al.,2001).
Various preventive and therapeutic strategies have been embarked upon, aimed atcombating the HIV pandemic. These include the use of life-saving anti-retroviral drugs(ARVs), condom use, HIV testing, counseling and education about safer sex practices,etc. (Report on the global AIDS epidemic, 2006; USAID, 2004; WHO, UNAIDS, 2005;Wilson et al., 2005). Although the use of ARVs has led to significant reductions inHIV burden (new cases, morbidity and HIV-related mortality) in many nations, theiraccessibility and efficient delivery in resource-poor nations remain quite problematic.This, coupled with the absence of an anti-HIV vaccine (although a number are in var-ious stages of clinical trials), calls for the use of other affordable programs for con-trolling HIV spread especially in nations with limited resources and public health effi-ciency.
A number of studies have provided clear evidence that male circumcision (MC) sig-nificantly reduces female-to-male transmission of HIV (Aubert et al., 2005; Bailey etal., 1999; Fink, 1986; Hutchinson, 1885; Moses et al., 1998; Siegfried et al., 2005;Weiss et al., 2000). For instance, using a randomized controlled trial, Auvert et al., (Aubertet al., 2005) shows that male circumcision reduces 60% of women-to-men HIV transmis-sion (32%–76%; 95% CI).
The aim of this paper is to use mathematical modeling to assess the potential impactof male circumcision in controlling the spread of HIV in a community. A deterministicsex-structured model (basic model), simulated using partial data from South Africa, is de-signed and analysed to monitor the temporal dynamics of the associated sub-populations.The extended model is formulated and qualitatively analysed in Section 2. The modelis extended, to incorporate condom use and ARVs, in Section 3. Simulation results arepresented in Section 4.
2. Formulation of basic model
The total sexually-active female population, denoted by Nf (t), is divided into threemutually-exclusive sub-populations of susceptible Sf (t), HIV-infected individuals withno clinical symptoms of AIDS If (t) and HIV-infected individuals with clinical symp-toms of AIDS (i.e., people in the AIDS stage of infection) Af (t) individuals, so thatNf (t) = Sf (t) + If (t) + Af (t). Similarly, the total sexually active male population,denoted by Nm(t), is also divided into five mutually-exclusive sub-populations of un-
To Cut or Not to Cut: A Modeling Approach for Assessing the Role 2449
circumcised susceptible Smu(t), circumcised susceptible Smc(t), uncircumcised infectedImu(t), circumcised infected Imc(t) and AIDS Am(t) individuals, so that Nm(t) = Smu(t)+Smc(t) + Imu(t) + Imc(t) + Am(t). For mathematical convenience, the infected classes If ,
Imu and Imc are defined to include individuals in both the acute stage (first few weeks ofHIV infection) and the chronic stage (lasting many years) of HIV disease (these two stagesare asymptomatic stages). Although individuals in the acute stage of infection have highviral load (due to the high viremia that characterizes the early stage of HIV infection), thelong chronic stage is characterized by reduced viral load (see Elbasha and Gumel, 2006;Gumel et al., 2006 and the reference therein). Thus, it is plausible to assume that the av-erage viral load in the total population of individuals in the acute and chronic stage (If
for example) is less than that of its corresponding AIDS stage (Af for example). In otherwords, this study assumes that individuals in the AIDS stage (A) are more infectious thanthose in the corresponding acute/chronic stage (I ).
The susceptible female, uncircumcised male and circumcised male populations (Sf (t),Smu(t) and Smc) are increased via the recruitment of new sexually-active individuals, intothese classes at rates Π1, Π2 and Π3, respectively. The parameter Π3 models the recruit-ment of circumcised children who become sexually active. Individuals in the Sf (t) classacquire HIV infection at a rate λm = βm(Imu+Imc+ηAm)
Nm, where βm is the effective contact
rate of males, and the modification parameter, η ≥ 1, accounts for the aforementionedrelative infectiousness of individuals in the AIDS class, in relation to uncircumcised (Imu)and circumcised (Imc) infected males. Thus, male individuals in the AIDS stage (Am) areassumed to be more infectious than those in the asymptomatic stages (Imu and Imc). Al-though the parameter η is typically taken to be greater or equal to unity, the model isrobust enough to allow for values of η less than unity (this would correspond to the casewhere individuals in the asymptomatic pre-AIDS classes are assumed to be more infec-tious than those in the AIDS classes). It is worth emphasizing that one of the key noveltiesof this model is the incorporation of the contribution of AIDS patients in the transmissionof HIV. Although this aspect is often ignored in many HIV transmission models, epi-demiological evidence supports the hypotheses that AIDS patients are capable of, and doengage in, risky sexual behavior (e.g., inconsistent condom use or having multiple sexpartners) (Lansky et al., 2000).
Uncircumcised susceptible males (Smu) acquire HIV infection at a rate λf = βf (If +ηAf )
Nf,
with βf being the effective contact rate of females. Here too, it is assumed that infectedfemales in the AIDS stage (Af ) are more infectious than those in the asymptomaticstage (If ). A fraction, q , of sexually-active adults in the Smu(t) class is circumcised (ata rate of ξ, with efficacy ε). Circumcised male susceptible individuals acquire infectionat a rate λf (1 − ε), where 0 < ε < 1 is the efficacy of male circumcision in preventingfemale-to-male transmission. Infected individuals (whether female, uncircumcised or cir-cumcised male) progress to AIDS at a rate σ (0 < σ < 1). Individuals suffer natural death(at a rate μ) and those in AIDS stages suffer an additional disease-induced death (at arate δ).

2450 Podder et al.
Combining the above descriptions and assumptions, the basic circumcision model isgiven by the following deterministic system of differential equations.
dSf
dt= Π1 − λmSf − μSf ,
dSmu
dt= Π2 − λf Smu − ξqεSmu − μSmu,
dSmc
dt= Π3 + ξqεSmu − λf (1 − ε)Smc − μSmc,
dIf
dt= λmSf − σIf − μIf ,
(1)dImu
dt= λf Smu − σImu − μImu,
dImc
dt= λf (1 − ε)Smc − σImc − μImc,
dAf
dt= σIf − δAf − μAf ,
dAm
dt= σImu + σImc − δAm − μAm,
where,
λf = βf (If + ηAf )
Nf
and λm = βm(Imu + Imc + ηAm)
Nm
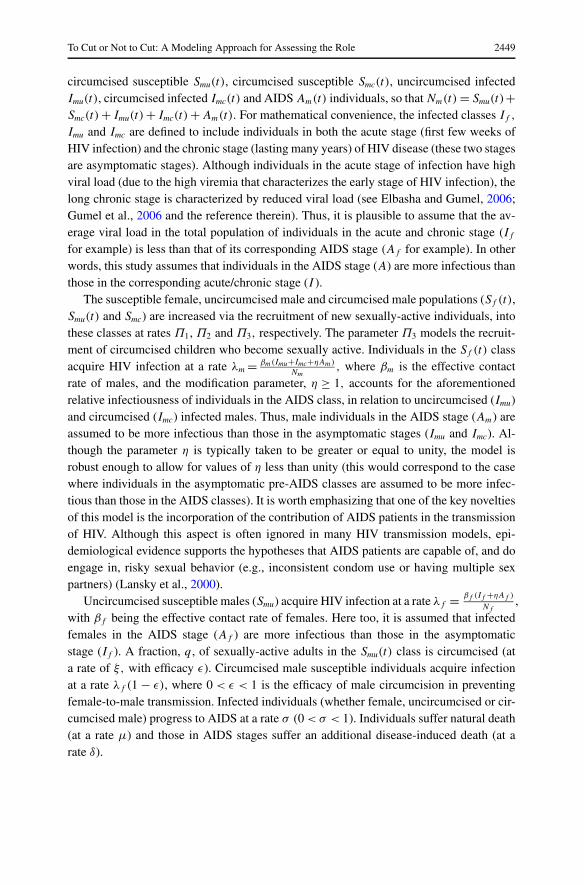
are the forces of infection for females and males, respectively (see Fig. 1a for a schematicdiagram and Table 1 for description of the variables and parameters).
2.1. Stability analysis of disease-free equilibrium
Since the model (1) monitors human populations, it is assumed that the variables and asso-ciated parameters are non-negative for all t ≥ 0. The model has a disease-free equilibrium(DFE) given by
E0 = (S∗f , S∗
mu, S∗mc, I
∗f , I ∗
mu, I∗mc,A
∗f ,A∗
m)
=(
Π1
μ,
Π2
μ + ξqε,Π3(μ + ξqε) + ξqεΠ2
μ(μ + ξqε),0,0,0,0,0
). (2)
To Cut or Not to Cut: A Modeling Approach for Assessing the Role 2451
Fig. 1 (a) Schematic diagram of model (1). (b) Schematic diagram of model (9).
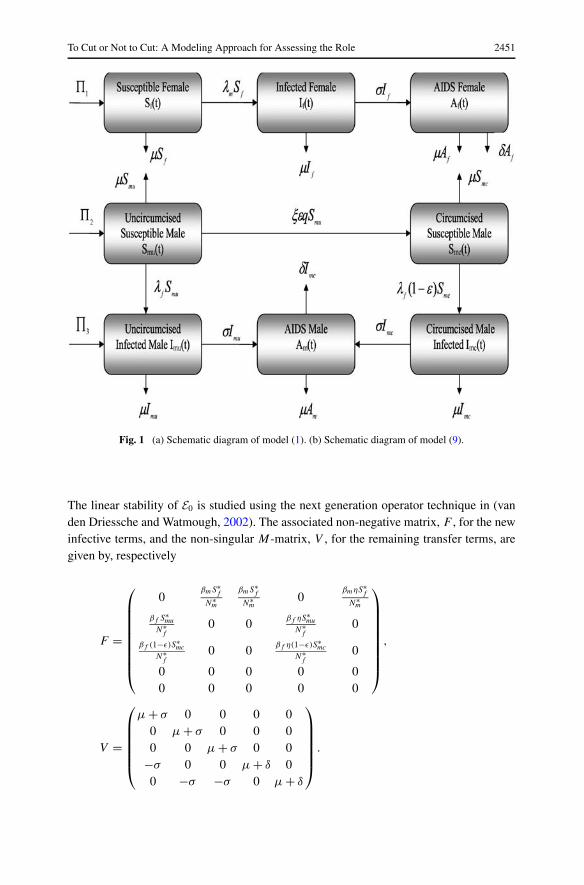
The linear stability of E0 is studied using the next generation operator technique in (vanden Driessche and Watmough, 2002). The associated non-negative matrix, F , for the newinfective terms, and the non-singular M-matrix, V , for the remaining transfer terms, aregiven by, respectively
F =
⎛⎜⎜⎜⎜⎜⎜⎜⎜⎝
0βmS∗
f
N∗m
βmS∗f
N∗m
0βmηS∗
f
N∗m
βf S∗mu
N∗f
0 0βf ηS∗
muN∗
f0
βf (1−ε)S∗mc
N∗f
0 0βf η(1−ε)S∗
mcN∗
f0
0 0 0 0 00 0 0 0 0
⎞⎟⎟⎟⎟⎟⎟⎟⎟⎠
,
V =
⎛⎜⎜⎜⎜⎜⎝
μ + σ 0 0 0 00 μ + σ 0 0 00 0 μ + σ 0 0
−σ 0 0 μ + δ 00 −σ −σ 0 μ + δ
⎞⎟⎟⎟⎟⎟⎠
.
2452 Podder et al.
Fig. 1 (Continued.)
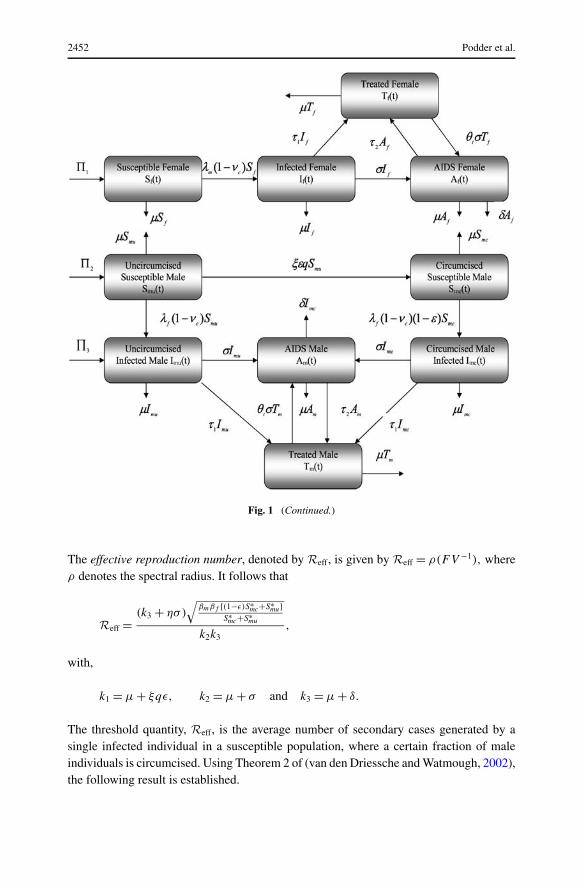
The effective reproduction number, denoted by Reff, is given by Reff = ρ(FV −1), whereρ denotes the spectral radius. It follows that
Reff =(k3 + ησ)
√βmβf [(1−ε)S∗
mc+S∗mu]
S∗mc+S∗
mu
k2k3,
with,
k1 = μ + ξqε, k2 = μ + σ and k3 = μ + δ.
The threshold quantity, Reff, is the average number of secondary cases generated by asingle infected individual in a susceptible population, where a certain fraction of maleindividuals is circumcised. Using Theorem 2 of (van den Driessche and Watmough, 2002),the following result is established.

To Cut or Not to Cut: A Modeling Approach for Assessing the Role 2453
Table 1 Description of variables and parameters for the models.
Variables Description Initial values
Sf (t) Susceptible female individuals 9.972 mSmu(t) Uncircumcised susceptible male 7 m
individualsSmc(t) Circumcised susceptible male 2.2 m
individualsIf (t) Infected female individuals 1.4 mImu(t) Uncircumcised infected male 1.4 m
individualsImc(t) Circumcised infected male individuals 1.018 mAf (t) AIDS infected female individuals 1.005 mAm(t) AIDS infected male individuals 1.005 mTf (t) Treated female individuals 0Tm(t) Treated male individuals 0
Parameters Description Baseline values Ref.
Π1 Rate of recruitment into the susceptible 1000 Estimatedfemale population
Π2 Rate of recruitment into the 1000 Estimateduncircumcised male population
Π3 Rate of recruitment into the circumcised 1000 Estimatedmale population
βf Transmission coefficient for females 0.45 Estimatedβm Transmission coefficient for males 0.4 Brian et al. (2006)q Fraction of susceptible males 0.6 Estimated
circumcisedη,ηf , ηm Modification parameters 1.1, 0.02, 0.02 Estimatedθt Progression rate of treated individuals to 0.1 Estimated
AIDSε Efficacy of circumcision 0.6 Aubert et al. (2005)ξ Circumcision rate of susceptible 1 Estimated
individualsν Condom efficacy 0.87 David and Weller (1999)c Condom compliance 0.6 Estimatedσ Progression rate to AIDS 0.1 Perelson and Nelson
(1999)τ1, τ2 Treatment rates 5 Estimatedμ Natural death rate 0.037 Brian et al. (2006)δ Disease-induced mortality rate 0.102 Brian et al. (2006)
Lemma 1. The DFE, E0, of the system (1), given by (2), is locally asymptotically stable(LAS) if Reff < 1 and unstable if Reff > 1.
The epidemiological implication of Lemma 1 is that HIV can be eliminated from thecommunity when Reff < 1, provided the initial sizes of the sub-populations of the model(1) are in the basin of attraction of E0. In other words, an influx of small number of infected

2454 Podder et al.
individuals into the population (community) will not generate large outbreaks if the malecircumcision can make Reff < 1.
2.1.1. Impact of circumcisionA theoretical expression for the measure of circumcision impact can be obtained by re-writing the effective reproduction number of the model as
R2eff = R2
0
S∗mu
S∗mu + S∗
mc
+R2oc
S∗mc
S∗mu + S∗
mc
=(
1 − S∗mc
S∗mu + S∗
mc
)R2
0 +R2oc
S∗mc
S∗mu + S∗
mc
= R20
[1 − S∗
mc
S∗mu + S∗
mc
(1 − R2
oc
R20
)],
where
R0 = (k3 + ησ)√
βmβf S∗mu
k2k3
is the basic reproduction number, which measures the average number of new secondarycases generated by an infected individual in a completely susceptible population (whenno individual in the community is circumcised), and
R2oc = (k3 + ησ)
√βmβf (1 − ε)
k2k3
is the circumcision reproduction number when every male member of the community iscircumcised. Using the notation in (Blower et al., 2002; Elbasha and Gumel, 2006), thecircumcision impact factor, denoted by φ, is given by
φ = S∗mc
S∗mu + S∗
mu
(1 + Roc
R0
)(1 − Roc
R0
). (3)
It follows from (3) that if Roc ≤ R0, then the impact factor (φ) is positive (meaningthat male circumcision will reduce the basic reproduction number, and, therefore, reduceHIV burden in the community). The factor is negative if Roc > R0. These results aresummarized below.
Theorem 1. Male circumcision will have positive impact in the community if φ > 0(i.e., Roc < R0), no impact if φ = 0 (i.e., Roc = R0) and negative impact if φ < 0(i.e., Roc > R0).
Noting that
R2oc
R20
= (1 − ε) < 1 for 0 < ε < 1,
To Cut or Not to Cut: A Modeling Approach for Assessing the Role 2455
it follows (using the fact R2oc
R20
< 1) that φ > 0 always (for any 0 < ε < 1). Thus, male
circumcision will always be beneficial in curtailing HIV spread in the community (sinceit always reduces R0). However, this may not be the case if the widespread use of cir-cumcision induces an increase in risky behavior amongst circumcised males (i.e., somecircumcised males may believe that circumcision will provide immunity against HIV in-fection, and thereby relax their use of precautionary measures). For instance, using avaccination model, Elbasha and Gumel (2006) show that a HIV vaccine could have detri-mental impact if its widespread use induces increase in risky behavior (in this case, thecorresponding impact factor is negative; and the use of an HIV vaccine, under this riskybehavior scenario, increases the associated basic reproduction number).
2.2. Existence of backward bifurcation
The phenomenon of backward bifurcation, characterized by the co-existence of a stableDFE and a stable endemic equilibrium when the associated reproduction threshold is lessthan unity, has been observed in a number of disease transmission models, especiallythose that incorporate an imperfect vaccine (see Elbasha and Gumel, 2006 and the refer-ences therein). The public health implication of backward bifurcation is that the classicalrequirement of having the reproduction threshold less than unity, although necessary, isno longer sufficient for disease control (in such a case, control measures must bring thereproduction threshold, Reff, much smaller that one, so that it is outside the backwardbifurcation range, to guarantee disease elimination).
Since, in this study, male circumcision is modeled in a way that is somewhat akin toincorporating an imperfect vaccine in the model, it is instructive to determine whetheror not the model (1) undergoes backward bifurcation when Reff < 1. This is investigatedbelow. Define
λ∗∗f = βf (I ∗∗
f + ηA∗∗f )
S∗∗f + I ∗∗
f + A∗∗f
and λ∗∗m = βm(I ∗∗
mu + ηcI∗∗mc + ηA∗∗
m )
S∗∗mu + S∗∗
mc + I ∗∗mu + I ∗∗
mc + A∗∗m
(4)
as the force of infection of the female and male population at steady state, respectively.Thus, the variables of the model (1) can be expressed in terms of λ∗∗
f and λ∗∗m (at steady
state) as follows:
S∗∗f = Π1
λ∗∗m + μ
, S∗∗mu = Π2
λ∗∗f + k1
,
S∗∗mc = Π3λ
∗∗f + Π3k1 + ξqεΠ2
(λ∗∗f + k1)[λ∗∗
f (1 − ε) + μ] ,
I ∗∗f = λ∗∗
m Π1
k2(λ∗∗m + μ)
, I ∗∗mu = λ∗∗
f Π2
k2(λ∗∗f + k1)
, (5)
I ∗∗mc = λ∗∗
f (1 − ε)(Π3λ∗∗f + Π3k1 + ξqεΠ2)
[k2(λ∗∗f + k1)(λ
∗∗f (1 − ε) + μ)] ,

2456 Podder et al.
A∗∗f = σλ∗∗
m Π1
(k3k2(λ∗∗m + μ))
,
A∗∗m = σλ∗∗
f [(1 − ε)(Π3k1 + λ∗∗f Π2 + λ∗∗
f Π3 + ξqεΠ2) + Π2μ][k3k2(λ
∗∗f + k1)(λ
∗∗f (1 − ε) + μ)] .
Substituting (5) in (4) gives
λ∗∗m = βmλ∗∗
f (Aλ∗∗f + B)
Cλ∗∗f
2 + Dλ∗∗f + E
(6)
and
λ∗∗f = βf λ∗∗
m (k3 + ησ)
λ∗∗m (k3 + σ) + k2k3
, (7)
where,
A = (Π2 + Π3)(k3 + ησ)(1 − ε),
B = [(Π3k1 + Π2ξqε)(1 − ε) + Π2μ
](k3 + ησ),
C = (Π2 + Π3)(k3 + σ)(1 − ε),
D = [Π2k2k3 + (Π3k1 + Π2ξqε)(k3 + σ)
](1 − ε) + Π2μ(k3 + σ) + Π3k2k3,
E = k1k2k3(Π2 + Π3).
Using (7) in (6), it follows that the nonzero equilibria of the model satisfy the quadratic:
a0λ∗∗m
2 + a1λ∗∗m + a2 = 0, (8)
where,
a0 = C(k3 + ησ)2β2f + D(k3 + ησ)(k3 + σ)βf + E(k3 + σ)2,
a1 = (k3 + σ)[2Ek2k3 − βmβf B(k3 + ησ)
]+ (k3 + ησ)βf
[Dk2k3 − βmβf A(k3 + ησ)
],
a2 = k1k32k
33
(1 −R2
eff
).
The quadratic (8) can be analysed for the possibility of multiple endemic equilibria.It is worth noting that the coefficient a0 is always positive, and a2 is positive (negative)if Reff is less than (greater than) unity, respectively. Hence, the following result is estab-lished:
Theorem 2. The circumcision model (1) has
(i) A unique endemic equilibrium if a2 < 0 ⇔ Reff > 1;(ii) A unique endemic equilibrium if a1 < 0, and a2 = 0 or a2
2 − 4a0a2 = 0;(iii) Two endemic equilibria if a2 > 0, a1 < 0 and a2
1 − 4a0a2 > 0;(iv) No endemic equilibrium otherwise.
To Cut or Not to Cut: A Modeling Approach for Assessing the Role 2457
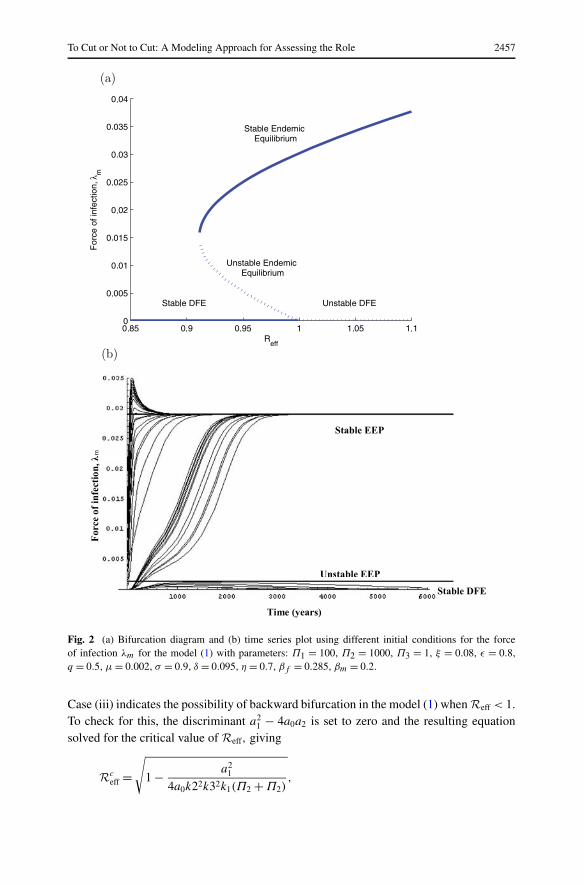
Fig. 2 (a) Bifurcation diagram and (b) time series plot using different initial conditions for the forceof infection λm for the model (1) with parameters: Π1 = 100, Π2 = 1000, Π3 = 1, ξ = 0.08, ε = 0.8,q = 0.5, μ = 0.002, σ = 0.9, δ = 0.095, η = 0.7, βf = 0.285, βm = 0.2.
Case (iii) indicates the possibility of backward bifurcation in the model (1) when Reff < 1.To check for this, the discriminant a2
1 − 4a0a2 is set to zero and the resulting equationsolved for the critical value of Reff, giving
Rceff =
√1 − a2
1
4a0k22k32k1(Π2 + Π2),
2458 Podder et al.
from which it can be shown that backward bifurcation occurs for values of Reff suchthat Rc
eff < Reff < 1. This phenomenon is illustrated by simulating the model (1) withthe following set of parameter values: Π1 = 100, Π2 = 1000, Π3 = 1, ξ = 0.08, ε = 0.8,q = 0.5, μ = 0.002, σ = 0.9, δ = 0.095, η = 0.7, βf = 0.285, βm = 0.2 so that Reff =0.98 < 1; and Rc
eff = 0.91 (that is Rceff < Reff < 1). The bifurcation diagram, depicted
in Fig. 2a, shows that the model has a DFE (corresponding to λ∗∗m = 0) and two endemic
equilibria (corresponding to λ∗∗m = 0.029 and λ∗∗
m = 0.0012, respectively); one of the en-demic equilibria (λ∗∗
m = 0.029) is LAS, the other (λ∗∗m = 0.0012) is unstable (a saddle), and
the DFE (E0) is LAS. This clearly shows the co-existence of two stable equilibria whenReff < 1, confirming that the model (1) exhibits backward bifurcation for Rc
eff < Reff < 1.A time series plot, using different sets of initial conditions, is given in Fig. 2b to fur-ther illustrate this phenomenon. It is worth noting that the backward bifurcation in themodel can be removed if the efficacy of male circumcision is 100% (ε = 1). This result issummarized below for the model (1).
Theorem 3. The model (1) exhibits backward bifurcation when Case (iii) of Theorem 2holds and Rc
eff < Reff < 1.
Since circumcision is akin to a vaccination program, and vaccination models that un-dergo backward bifurcation are known to lose such feature if the vaccine efficacy is 100%(see Elbasha and Gumel, 2006 and the reference therein), it is instructive to determinewhether this is also the case with the basic circumcision model (1). This is explore below.
Theorem 4. The basic model (1) does not undergo backward bifurcation if the efficacy ofcircumcision is 100% (ε = 1).
Proof: Notice that backward bifurcation occurs when Reff < 1. When ε = 1, the effectivereproduction number (Reff) reduces to
R2eff = (k3 + ησ)2βf βmΠ2μ
k1k22k
23(Π2 + Π3)
.
Further, the coefficients of the quadratic (8) reduce to
a0 = D(k3 + ησ)(k3 + σ)βf + E(k3 + σ)2,
a1 = 2Ek2k3(k3 + σ) + Dk2k3(k3 + ησ)βf − βmβf B(k3 + ησ)(k3 + σ)
= Dk2k3(k3 + ησ)βf + Ek2k3(k3 + σ)
[2 − βmβf B(k3 + ησ)2
Ek2k3
]
= Dk2k3(k3 + ησ)βf + Ek2k3(k3 + σ)
[2 − βmβf Π2μ(k3 + ησ)2
k1k22k
23(Π2 + Π3)
]
= Dk2k3(k3 + ησ)βf + Ek2k3(k3 + σ)(2 −R2
eff
)> 0,
a2 = k1k32k
33
(1 −R2
eff
)> 0.

To Cut or Not to Cut: A Modeling Approach for Assessing the Role 2459
Clearly, a0 > 0 and a1, and a2 are positive provided Reff < 1. Thus, for Reff < 1 andε = 1, the coefficients of the quadratic are all positive. Thus, the quadratic has no positiveroots, ruling out backward bifurcation in this case (refer to Theorem 2). �
3. Circumcision model with condom use and ARVs
The male circumcision model, given by Eq. (1), is extended to incorporate other interven-tions, namely the use of condoms and anti-retroviral drugs. The objective is to determinewhat additional benefits (in terms of reduction in disease burden) can be achieved bycombining the male circumcision program with one or both of these interventions. Theextended model is given by (see Fig. 1b for a flow diagram)
dSf
dt= Π1 − λm(1 − νc)Sf − μSf ,
dSmu
dt= Π2 − λf (1 − νc)Smu − ξqεSmu − μSmu,
dSmc
dt= Π3 + ξqεSmu − λf (1 − νc)(1 − ε)Smc − μSmc,
dIf
dt= λm(1 − νc)Sf − σIf − τ1If − μIf ,
dImu
dt= λf (1 − νc)Smu − σImu − τ1Imu − μImu,
(9)dImc
dt= λf (1 − νc)(1 − ε)Smc − σImc − τ1Imc − μImc,
dAf
dt= σIf + θtσTf − δAf − τ2Af − μAf ,
dAm
dt= σImu + σImc + θtσTm − τ2Am − δAm − μAm,
dTf
dt= τ1If + τ2Af − θtσTf − μTf ,
dTm
dt= τ1(Imu + Imc) + τ2Am − θtσTm − μTm,
where, now,
λf = βf (If + ηAf + ηf Tf )
Nf
and λm = βm(Imu + Imc + ηAm + ηmTm)
Nm
,
with Nf = Sf + If + Af + Tf and Nm = Smu + Smc + Imu + Imc + Am + Tm. In (9), thevariables Tm and Tf represent the populations of treated males and females, respectively.Infected individuals in the pre-AIDS stage are treated at a rate τ1, whilst those in theAIDS stages (If , Imu and Imc) are treated at a rate τ2. It is assumed that treated individualstransmit the disease at a very small rate (for males, βmηm; and for females, βf ηf ; where

2460 Podder et al.
0 < ηm,ηf < 1 are modification parameters) in relation to untreated infected individuals.Further, treated individuals progress to AIDS at a slower rate (θtσ ) (here, 0 < θt < 1 isa modification parameter). The use of condoms is incorporated using the term (1 − νc),where 0 < ν < 1 is condom efficacy and 0 < c < 1 represents compliance in condom use.In other words, condom use is modeled in terms of reduction of the transmission rate forboth males and females (λm or λf ).
3.1. Basic properties of the extended model
The extended model has a disease-free equilibrium is given by
Ect = (S∗f , S∗
mu, S∗mc, I
∗f , I ∗
mu, I∗mc,A
∗f ,A∗
m,T ∗f , T ∗
m)
=(
Π1
μ,
Π2
μ + ξqε,(Π3(μ + ξqε) + ξqεΠ2)
(μ + ξqε)μ,0,0,0,0,0,0,0
).
Using the same technique as in Section 2.1, the effective reproduction number of theextended model, denoted by Rct , is given by
Rct =√
N∗mβf βmA1A2(S∗
mc(1 − ε) + S∗mu)(1 − ν)
N∗mk2k4(δ + μ)
,
where,
k1 = μ + ξqε, k2 = σ + τ1 + μ, k3 = τ2 + δ + μ, k4 = θtσ + μ,
A1 = (δ + μ)(μ + θtσ ) + ησk4 + ησθtτ1 + ηmτ1k3 + ηmτ2σ,
A2 = (δ + μ)(μ + θtσ ) + ησk4 + ησθtτ1 + ηf τ1k3 + ηf τ2σ.
Although not shown here, the extended model (9) exhibits similar qualitative dynamics(e.g., backward bifurcation) as the basic model (1).
4. Numerical results and discussions
4.1. Circumcision-only model
To monitor the impact of male circumcision in curtailing the spread of HIV in a commu-nity, the model (1) is simulated using the parameter estimates in Table 1. Some of theseestimates are obtained from published data for South Africa (Brian et al., 2006). For ex-ample, using such data, the initial total population of sexually-active people (between theages of 15–49) is taken to be 25 million, so that N(0) = 25 million (see Table 1 for distri-bution of initial values of the state variables). With the set of parameter values in Table 1,the value of the basic reproduction number is R0 = 5.55.
The impact of the efficacy of male circumcision, to prevent women-to-men transmis-sion (ε), and the fraction of male individuals circumcised (q) on the effective reproductive
To Cut or Not to Cut: A Modeling Approach for Assessing the Role 2461
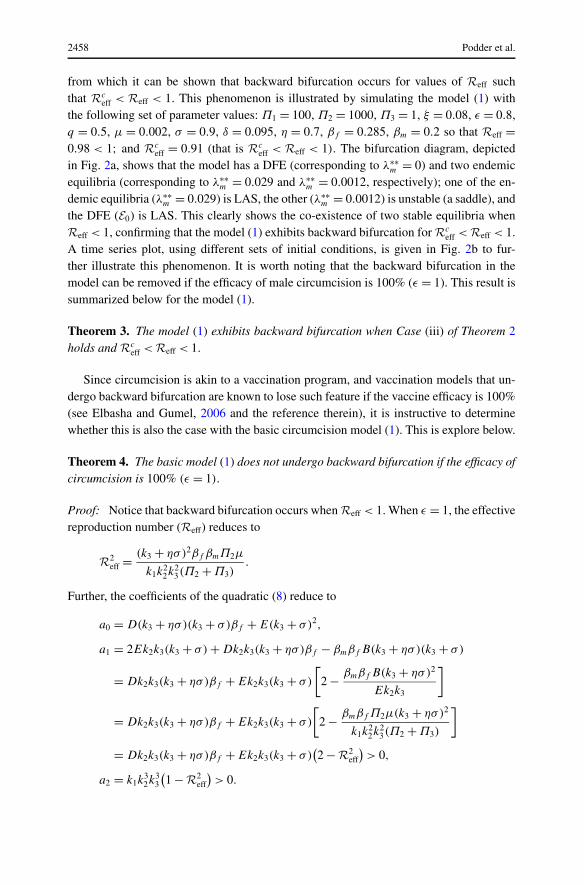
Fig. 3 Simulations of the basic model (1). Contour plot of Reff as a function of the fraction of circumcisedsusceptible males (q) and circumcision efficacy (ε). Parameters as in Table 1.
number (Reff) is evaluated, first of all, using a contour plot depicted in Fig. 3. This plotenables the evaluation of possible uncertainties in the estimates of these parameters (it isplausible to assume some uncertainties in the estimate of circumcision efficacy given inthe randomized controlled trial of Aubert et al. (2005)). As expected, the effective repro-duction number decreases with increasing efficacy and coverage rates (Fig. 3). It shouldbe noted that reduction in Reff implies reduction in disease burden. Figure 3 further showsthat although a male circumcision program with the estimated efficacy of 60% (ε = 0.6)can significantly reduce disease burden, it cannot be expected to singly eliminate HIV ina population (since it fails to make Reff < 1).
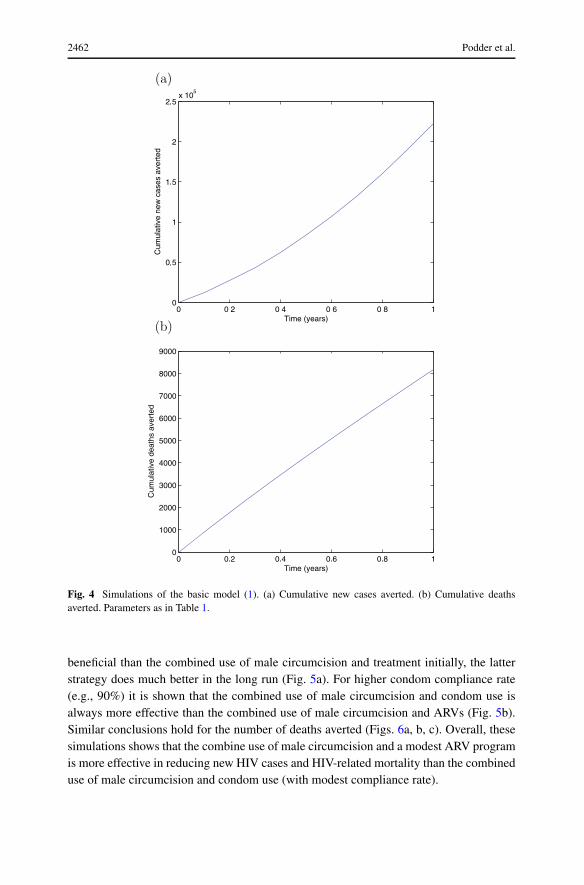
Further simulations were carried out to determine the number of cases that could beaverted using male circumcision only. These simulations show that up to 220,000 newcases (Fig. 4a) and 8,200 deaths (Fig. 4b) could be prevented in South Africa in one year.These results seem consistent with the finding in (Brian et al., 2006), which estimates thatabout 174,000 cases could be prevented in one year, and 100,000 deaths in a decade, inSouth Africa.
4.2. Extended circumcision model
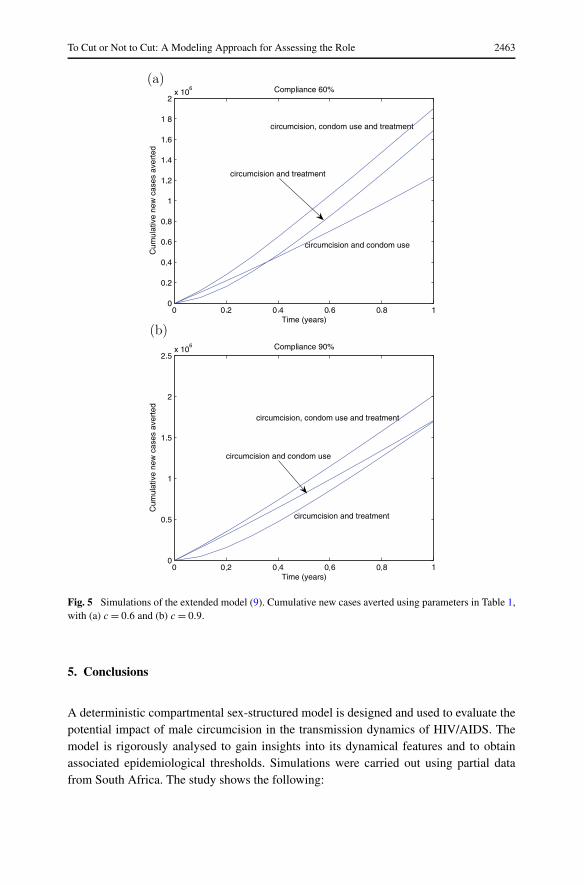
The extended model (9) is simulated with the set of parameters in Table 1 and variousvalues of the parameters associated with the use of ARVs and condoms use. Figure 5adepicts the number of new cases averted per year using male circumcision (with 60% ef-ficacy and 60% coverage rate), treatment of all infected individuals (at a rate τ1 = τ2 = 5)and condom use (with efficacy 87% and compliance rate 60%). This figure shows thatthe greatest reduction is achieved if all three interventions are used, as expected. Fur-ther, although the combination of male circumcision and condom use appears to be more
2462 Podder et al.
Fig. 4 Simulations of the basic model (1). (a) Cumulative new cases averted. (b) Cumulative deathsaverted. Parameters as in Table 1.
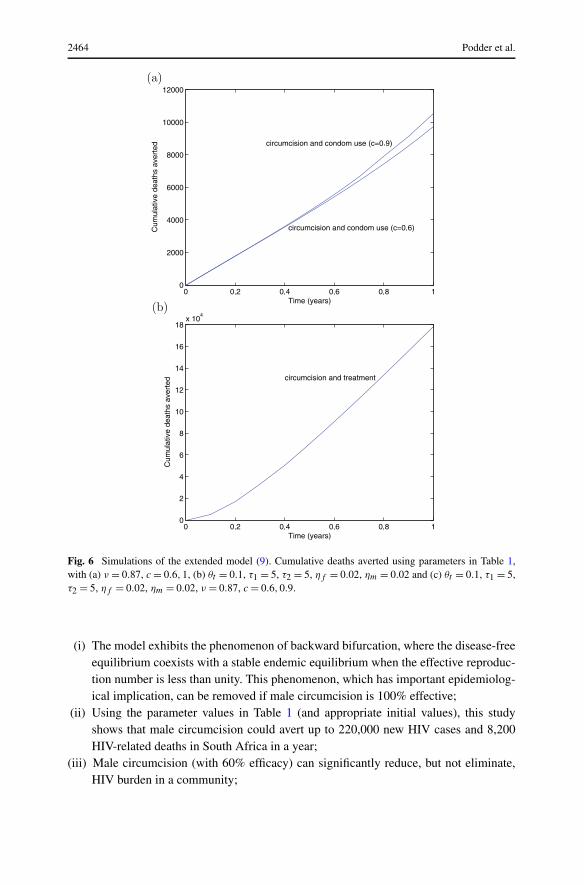
beneficial than the combined use of male circumcision and treatment initially, the latterstrategy does much better in the long run (Fig. 5a). For higher condom compliance rate(e.g., 90%) it is shown that the combined use of male circumcision and condom use isalways more effective than the combined use of male circumcision and ARVs (Fig. 5b).Similar conclusions hold for the number of deaths averted (Figs. 6a, b, c). Overall, thesesimulations shows that the combine use of male circumcision and a modest ARV programis more effective in reducing new HIV cases and HIV-related mortality than the combineduse of male circumcision and condom use (with modest compliance rate).
To Cut or Not to Cut: A Modeling Approach for Assessing the Role 2463
Fig. 5 Simulations of the extended model (9). Cumulative new cases averted using parameters in Table 1,with (a) c = 0.6 and (b) c = 0.9.
5. Conclusions
A deterministic compartmental sex-structured model is designed and used to evaluate thepotential impact of male circumcision in the transmission dynamics of HIV/AIDS. Themodel is rigorously analysed to gain insights into its dynamical features and to obtainassociated epidemiological thresholds. Simulations were carried out using partial datafrom South Africa. The study shows the following:
2464 Podder et al.
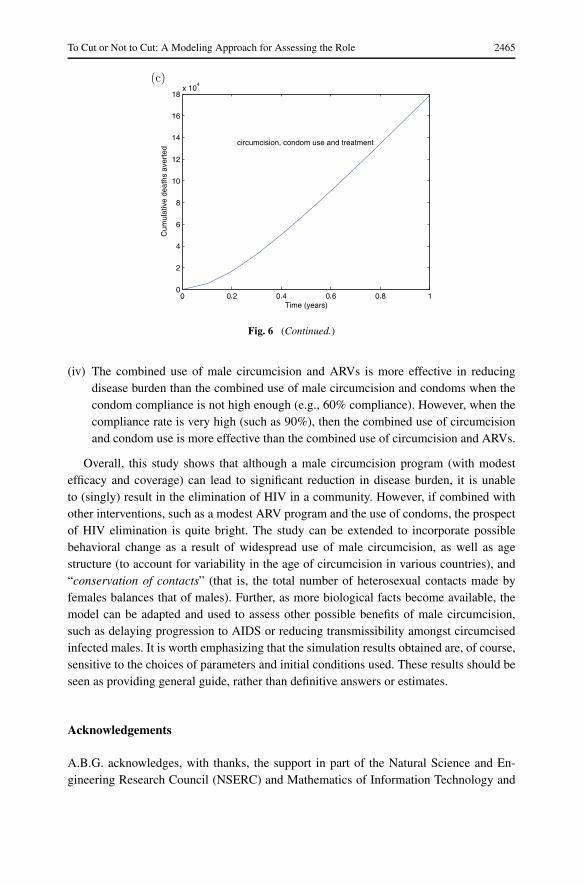
Fig. 6 Simulations of the extended model (9). Cumulative deaths averted using parameters in Table 1,with (a) ν = 0.87, c = 0.6,1, (b) θt = 0.1, τ1 = 5, τ2 = 5, ηf = 0.02, ηm = 0.02 and (c) θt = 0.1, τ1 = 5,τ2 = 5, ηf = 0.02, ηm = 0.02, ν = 0.87, c = 0.6,0.9.
(i) The model exhibits the phenomenon of backward bifurcation, where the disease-freeequilibrium coexists with a stable endemic equilibrium when the effective reproduc-tion number is less than unity. This phenomenon, which has important epidemiolog-ical implication, can be removed if male circumcision is 100% effective;
(ii) Using the parameter values in Table 1 (and appropriate initial values), this studyshows that male circumcision could avert up to 220,000 new HIV cases and 8,200HIV-related deaths in South Africa in a year;
(iii) Male circumcision (with 60% efficacy) can significantly reduce, but not eliminate,HIV burden in a community;
To Cut or Not to Cut: A Modeling Approach for Assessing the Role 2465
Fig. 6 (Continued.)
(iv) The combined use of male circumcision and ARVs is more effective in reducingdisease burden than the combined use of male circumcision and condoms when thecondom compliance is not high enough (e.g., 60% compliance). However, when thecompliance rate is very high (such as 90%), then the combined use of circumcisionand condom use is more effective than the combined use of circumcision and ARVs.
Overall, this study shows that although a male circumcision program (with modestefficacy and coverage) can lead to significant reduction in disease burden, it is unableto (singly) result in the elimination of HIV in a community. However, if combined withother interventions, such as a modest ARV program and the use of condoms, the prospectof HIV elimination is quite bright. The study can be extended to incorporate possiblebehavioral change as a result of widespread use of male circumcision, as well as agestructure (to account for variability in the age of circumcision in various countries), and“conservation of contacts” (that is, the total number of heterosexual contacts made byfemales balances that of males). Further, as more biological facts become available, themodel can be adapted and used to assess other possible benefits of male circumcision,such as delaying progression to AIDS or reducing transmissibility amongst circumcisedinfected males. It is worth emphasizing that the simulation results obtained are, of course,sensitive to the choices of parameters and initial conditions used. These results should beseen as providing general guide, rather than definitive answers or estimates.
Acknowledgements
A.B.G. acknowledges, with thanks, the support in part of the Natural Science and En-gineering Research Council (NSERC) and Mathematics of Information Technology and
2466 Podder et al.
Complex Systems (MITACS) of Canada. C.N.P. and O.S. gratefully acknowledge the sup-port of the Institute of Industrial Mathematical Sciences and the Department of Mathemat-ics, University of Manitoba. The authors are grateful to the three anonymous reviewersfor their valuable comments which have enhanced the paper.
References
Aubert, B., Taljaard, D., Lagrade, E., Sobngwi-Tambekou, J., Sitta, R. et al., 2005. Randomized, controlledintervention trial of male circumcision for reduction of HIV infection risk: the ANRS 1265 trial. PLoSMed. 2, e298.
Bailey, R., Neema, S., Otheno, R., 1999. Sexual behaviors and other HIV risk factors in circumcised anduncircumcised men in Uganda. J. Acquir Immune Defic. Syndr. 22, 294–301.
Blower, S., Koelle, K., Mills, J., 2002. Health policy modeling: epidemic control, HIV vaccines, andrisky behavior. In: Kaplan, Brookmeyer (Eds.) Qualitative Evaluation of HIV Prevention Programs,pp. 260–289. Yale University Press.
Brian, G. Williams, Lioyd-Smith, J.O., Gouws, E., Hankins, C., Getz, W.M., Hargrove, J., de Zoysa, I.,Dye, C., Auvert, B., 2006. The potential impact of male circumcision on HIV in sub-Saharan Africa.PLoS Med. 3(7), e262.
David, K.R., Weller, S.C., 1999. The effectiveness of condoms in reducing heterosexual transmision ofHIV. Fam. Plann. Perspect 31(6), 272–279.
Elbasha, E.H., Gumel, A.B., 2006. Theoretical assessment of public health impact of imperfect prophy-lactic HIV-1 vaccines with therapeutic benefits. Bull. Math. Biol. 68, 577–614.
Fink, A., 1986. A possible explanation for heterosexual male infection with AIDS. N. Engl. J. Med. 314,1167.
Gumel, A.B., McCluskey, C.C. et al., 2006. Mathematical study of a staged-progression HIV model withimperfect vaccine. Bull. Math. Biol. 68(8), 2105–2128.
Hutchinson, J., 1885. On the influence of circumcision in preventing syphilis. Med. Times Gazette 1,542–543.
Lansky, A., Nakashima, A., Jones, J., 2000. Risk behaviors related to heterosexual transmission from HIV-infected persons. Sex. Transm. Dis. 27, 483–489.
Moses, S., Bailey, R.C., Ronald, A.R., 1998. Male circumcision: assessment of health benefits and risks.Sex. Transm. Infect. 74, 368–373.
Perelson, A.S., Nelson, P.W., 1999. Mathematical analysis of HIV-1 dynamics in vivo. SIAM Rev. 41(1),3–44.
Robert, C.B., Francis, A.P., Stephen, M., 2001. Male circumcision and HIV prevention: current knowledgeand future research directions. Lancet Infect. Dis. 1, 223–231.
Report on the global AIDS epidemic: Executive summary, 2006. A UNAIDS 10th anniversary specialedition.
Siegfried, N., Muller, M., Deeks, J., Volmink, J., Egger, M. et al., 2005. HIV and male circumcision—asystematic review with assessment of the quality of studies. Lancer Infect. Dis. 5, 165–173.
USAID 2004. The President’s emergency plan for AIDS relief: US five-year Global HIV/AIDS strategy.Available: http://www.usaid.gov/our_work/global_health/aids/pepfar.html, accessed 25 May 2006.
van den Driessche, P., Watmough, J., 2002. Reproduction numbers and sub-threshold endemic equilibriafor compartmental models of disease transmission. Math. Biosci. 180, 29–48.
Weiss, H.A., Quigley, M.A., Hayes, R.J., 2000. Male circumcision and risk of HIV infection in sub-Saharan Africa: a systematic review and meta-analysis. AIDS 14, 2361–2370.
WHO, UNAIDS, 2005. Progress on access to anti-retroviral therapy: an update on “3 by 5”, p. 34 WorldHealth Organization, Geneva.
Wilson, P.A., Binagwaho, A., Ruxin, J., 2005. Combating AIDS in the developing world, p. 276 Earthscan,London.