men's knowledge, attitudes and beliefs about medical male circumcision: a qualitative study in...
TRANSCRIPT
1
Men’s knowledge, attitudes and beliefs about medical male circumcision: A
qualitative study in rural northern KwaZulu-Natal, South Africa.
Authors: Sicelo F Sengwayo1,2,3 , Christopher J Colvin2, Marie-Louise Newell1,4,
John Imrie1,5,6
1. Africa Centre for Health and Population Studies, University of KwaZulu-Natal,
Somkhele 3935, KwaZulu-Natal, South Africa;
2. School of Public Health and Family Medicine, Faculty of Health Science,
University of Cape Town, Cape Town 7925, South Africa;
3. Department of Health Studies, UNISA 0003, University of South Africa, South
Africa;
4. University College London Institute of Child Health, London, UK;
5. Health4Men, Anova Health Institute, Parktown 2193, Johannesburg, South
Africa;
6. Centre for Sexual Health and HIV Research, Faculty of Population Health
Sciences, University College London, London, UK.
Correspondence and requests for reprints to:
Mr. Sicelo F Sengwayo
Department of Health Studies
University of South Africa
Theo Van Wyk Building
7 Floor, 7-181
UNISA Main Campus
0003
Tel: +27 12 429 8450
Cell: +27 72 310 6882
Email: [email protected]
Date of submission: 19/10/2012
2
Source of support
The study was completed as part of an MPH training programme and funded by the
Africa Centre for Health and Population Studies, the South African Medical Research
Council and the Umthombo Youth Development Foundation. The Africa Centre for
Health and Population Studies receives core funding from the Wellcome Trust (UK).
The South African Medical Research Council improves the nation’s health and
quality of life through promoting and conducting relevant and responsive health
research. The Umthombo Youth Development Foundation supports the training of
rural youth to become health professionals and address the human resource
shortages in rural hospitals and to improve health care in rural communities.

3
Men’s knowledge, attitudes and beliefs about medical male circumcision: A
qualitative study in rural northern KwaZulu-Natal, South Africa.
Abstract:
Medical male circumcision (MMC) is a key component of comprehensive HIV
prevention strategies for countries with heterosexually-driven epidemics and is being
rapidly rolled-out in South Africa. This study was conducted in 2011 - one-year after
the KwaZulu-Natal Department of Health launched its MMC programme - to assess
rural men’s knowledge, understanding and beliefs about circumcision and inform
development of supportive interventions to optimise MMC uptake. Six focus group
discussions and 27 in-depth interviews with circumcised and uncircumcised men
from three remote, rural areas of northern KwaZulu-Natal, and one focus group with
public sector healthcare workers in the same area, were conducted. Knowledge of
the HIV prevention benefits of MMC was high. Uncircumcised men expressed
willingness to be circumcised to ‘obtain’ the perceived health benefits, but articulated
preference for the procedure to be performed in hospitals or health facilities because
of concern about safety and pain management. Factors influencing men’s
willingness to be circumcised were the perceived health benefit in terms of reduced
sexually transmitted infections and the belief that MMC enhanced sexual pleasure.
Barriers to MMC uptake included the requirement to undergo HIV testing (with an
HIV-negative result) before MMC would be performed and the extended period of
sexual abstinence during healing. Men’s generally positive attitudes and beliefs
could be enhanced by women’s endorsement and increased participation in MMC
promotion and by additional investment in capacity to deliver MMC programmes in
rural areas.
Word count: 233
Key words: Medical male circumcision, HIV prevention, Knowledge, Attitudes and
beliefs, South Africa
4
Men’s knowledge, attitudes and beliefs about medical male circumcision: A
qualitative study in rural northern KwaZulu-Natal, South Africa.
Introduction:
The HIV epidemic in South Africa continues to be primarily heterosexually-driven,
with the highest prevalence reported from KwaZulu-Natal, where the general
population prevalence increased from 38.7% to 39.5% between 2008 and 2010
(National Department of Health, 2010). Additional strategies to help curb the
pandemic are needed, and medical male circumcision (MMC) is one that is currently
being rolled-out. Compelling evidence exists to support MMC as a public health HIV
prevention intervention for men, with more than 40 observational and three
randomized controlled trials demonstrating that MMC reduces HIV acquisition in men
(Herman-Roloff et al., 2011; Weiss et al., 2008; Bailey et al., 2007). Data from these
trials have also shown circumcision reduces men’s risk of acquiring other sexually
transmitted infections (STI), and in some cases, the risks to their female partners’
(Morris, 2010; Auvert et al. & Tobian et al., 2009; Weiss et al., & Gray et al., 2008;
Western & Bailey, 2007).
Such is the strength of evidence that MMC has become an essential part of
comprehensive HIV prevention programming in high-prevalence countries with
primarily heterosexually-driven epidemics. However MMC implementation
programmes in South Africa are still relatively new and significant knowledge gaps
remain about how men, particularly in rural areas where the programmes are just
beginning, understand and perceive MMC and what, if any, are the barriers to uptake
(Scott et al., 2005).
There have been numerous studies of MMC acceptability in both traditionally
circumcising and non-circumcising communities in Africa. In general these studies
show high levels of acceptability, despite fears expressed by men of pain, excessive
bleeding and death (Harman-Roloff et al., 2011; Westercamp & Bailey, 2007).
However some studies have also noted a false sense of security among some newly
circumcised men and belief that MMC provides an HIV prevention panacea reducing
the need for condom use; this would be of concern to public health programmes
(Lagarde et al., 2003).
5
Men’s perceptions of MMC have been associated with beliefs about improved
personal health, hygiene and sexual performance. In South Africa, Taljaard and
collegues (2000) found health-related beliefs to be strong motivators for men to take
up circumcision – beliefs such as that the uncircumcised penis collects dirt which
promotes disease and is generally unhealthy. Beliefs that circumcision enhances
sexual pleasure and perfomance and makes sex more appealing to women have
also been noted (Grund and Hennink, 2011; Tobian et al., 2009; Weiss et al., 2008).
While still other studies have observed that in traditional circumcising communities,
men are often not respected if they have been medically circumcised and not gone
through the appropriate traditional circumcision rituals and would thus not be
considered to have completed the transition from boyhood (inkwenkwe) to manhood
(ubudoda) (Tenge, 2009). All of these factors have the potential to influence men’s
willingness to participate in a large scale MMC roll-out programme.
Ethnicity has also been highlighted as a potentially important consideration. Studies
in South Africa have examined men’s attitudes to MMC through the lens of ethnicity
as part of the feasibility assessment of a national roll-out programme. According to
Scott et al., (2005) and Taljaard et al., (2000) among adults from non-circumcising
communities participating in their studies, more than 70% said they would like to be
medically circumcised if it reduced the chance of getting HIV and STIs. Both of these
studies concluded MC acceptability was highest among Xhosa men (72%), a group
with a tradition of male circumcision, but also popular among Tswana men (52%),
who have no such tradition and generally much lower circumcision prevalence
(15%)(Taljaard et al., 2000). Although traditional male circumcision practices vary,
these studies conclude ethnicity per se, does not seem to be a determinant of
acceptability and as a result should not impede the roll-out of MMC nationally
(Herman-Roloff et al., 2011; Lagarde et al. & Bailey et al., 2003; Taljaard et al.,
2000)
However, nearly all the South African research looking at the acceptability of medical
male circumcision pre-dates the South African Government’s 2010 decision to roll-
out MMC in a national programme, led by the nine provincial Departments of Health.
In this regard, current knowledge, attitudes and beliefs about medical male
6
circumcision, particularly in communities without a tradition of circumcision needs
updating (Peters, 2010; Auvert et al., 2009; WHO, 2008; Scott et al., 2005), while the
impact on acceptability of programmes actually rolling-out needs to be assessed
(Westercamp, 2007). It would seem that widespread knowledge of adverse events
associated with traditional circumcision practices (WHO, 2008) has ensured a strong
preference for MMC performed by trained health providers and delivered in health
care contexts, but the extent to which this is a requirement for a successful national
roll-out is unclear (Scott, Weiss & Viljoen, 2005).
Cultural beliefs and practices are important considerations that may also affect
programme roll-out (WHO, 2010 & Kwata, 2009). They provide a useful platform
through which to engage traditional leaders, authorities, religious leaders and the
Departments of Health to work together. King Zwelenthini, the Zulu monarch, called
for the return to the custom of rite of passage for boys at the annual Umkhosi
Wokweshwama (First Fruit Cerenony) held in December 2009 (KZN Department of
Health, 2010). Since then, King Goodwill has become a key champion of MMC in
South Africa, particularly in KwaZulu-Natal. With the Zulu King as champion and
spokesperson, the KwaZulu-Natal Department of Health launched its campaign to
extend circumcision provision in April 2010 (KZN Department of Health, 2010). Since
then close to 176,000 circumcisions have been performed among the more than 3.0
million eligible men in the province, but there is still substantial unmet demand and
areas where the programme is just starting (Mail & Guardian (Health Supplement) 5
– 11 October 2012:4). As MMC programmes are rolled-out into new areas,
understanding men’s underlying knowledge, attitudes and beliefs about the
procedure is essential to ensure appropriate continuing professional training for
programme staff and adequate education interventions for men and their
communities. In this study we explored knowledge, attitudes, beliefs and potential
factors influencing successful roll-out of MMC among Zulu men in three rural
communities adjacent to the traditional home of Zulu monarch where the Department
of Health’s programme had been in place for approximately one-year at the time of
the study.
7
Methods
Focus group discussions (FGDs) and in-depth interviews (IDIs) were carried out with
circumcised and uncircumcised men in the Hlabisa, Nongoma and Vryheid areas of
northern KwaZulu-Natal. An additional focus group was convened with
representatives of public sector health care providers from the three health sub-
districts. The Ethics Committee of the University of Cape Town, Health Science
Faculty, Groote Schuur Hospital approved the project (Protocol number 189/2010).
Individual interviews were conducted to allow participants to share their personal
views and perceptions, while the focus groups aimed to illuminate how men discuss
MMC together, and to gain an appreciation for community beliefs about the
procedure, its benefits and shortcomings. The aim of utilizing these methods in
tandem was to ensure that comparable individual and group level knowledge and
perceptions data were collected. The aim of the focus group discussion with
Department of Health frontline staff was to obtain insights regarding implementation
of the MMC programme and narratives of staff experiences of the innovative delivery
model using mobile circumcision camps to reach underserved areas.
Data were collected approximately one-year after the launch of the KZN Department
of Health’s MMC programme (February-May 2011), but still in the early days of the
programme in each of the sites. The FGDs were facilitated by a skilled male Zulu-
speaking facilitator (SMF) from the area (the researcher), with detailed local
knowledge of the communities and facilities available. Observational notes were
compiled simultaneously by trained research assistants. Similar topic guides,
characterized by open-ended questions with probes were used for both focus groups
and interviews. Guides were originally drafted in English and translated into Zulu.
Participants were recruited using a purposive sampling frame from sports grounds,
homes, and shops to, obtaining a diversity of community opinions across different
demographic, age and social characteristics (King, 2004). A recruitment team
including six community members attended community soccer grounds during
games and also visited individuals in their homes and met men around shops where
they tended to congregate. The sample size was based on the notion of theoretical
8
saturation as a process in which the researcher continues to sample relevant cases
until no new theoretical insights are being gleaned from the data.
Eligibility was limited to men 18 years and older, and residents living in the area for
five years or more. The study was explained to participants individually in their
language of choice (English or Zulu). Men interested in participating were given a
minimum of two hours for consideration and reflection before being enrolled and
providing written informed consent in their language of choice. Focus groups lasted
approximately 60 minutes and involved 10-13 men. Three focus groups involving a
total of 80 men were conducted with older men (aged 30-89 years) and with young
men (18-30 years). The additional focus group with public sector health care
representatives involved 10 participants from across the three areas. These health
care providers were selected based on their active involvement in the roll-out of
MMC. All study participants were offered refreshments and ZAR100.00
(approximately US$ 8.50) as compensation for their time and to cover transport
costs. Focus groups and individual interviews were held in private where it was
possible to ensure and maintain confidentiality. The focus group with health care
providers was limited to male service providers - nurses and traditional health
practitioners.
Interviews and focus groups were digitally audio-recorded, transcribed and
translated by experienced bilingual transcribers. A thematic analytic approach was
used for the data analysis. Initial categories were drawn from the interview guide,
and from themes and patterns that emerged after repeated reviewing the data. Key
themes identified during IDIs and FGDs included: general knowledge of MMC;
understanding of local MMC programme; the connection between HIV and MMC;
primary facilitators and inhibitors of MMC uptake; and attitudes towards MMC and
being circumcised. Three of the authors reviewed the data independently to confirm
the themes and categories.
Once themes were identified, all transcripts were read and re-read until consensus
was reached on the overall meaning of the text. The second step was to prepare the
transcript by dividing the original text into “meaning units” and “single thought units”.
9
Thematic analysis encouraged re-reading of master transcripts with the identified
themes in mind. Theme words or phrases were revised to fit the overall meaning of
the original meaning units. The main aim of thematic analysis was to write out a
summary of themes accurately without software use (King, 2004).
Results
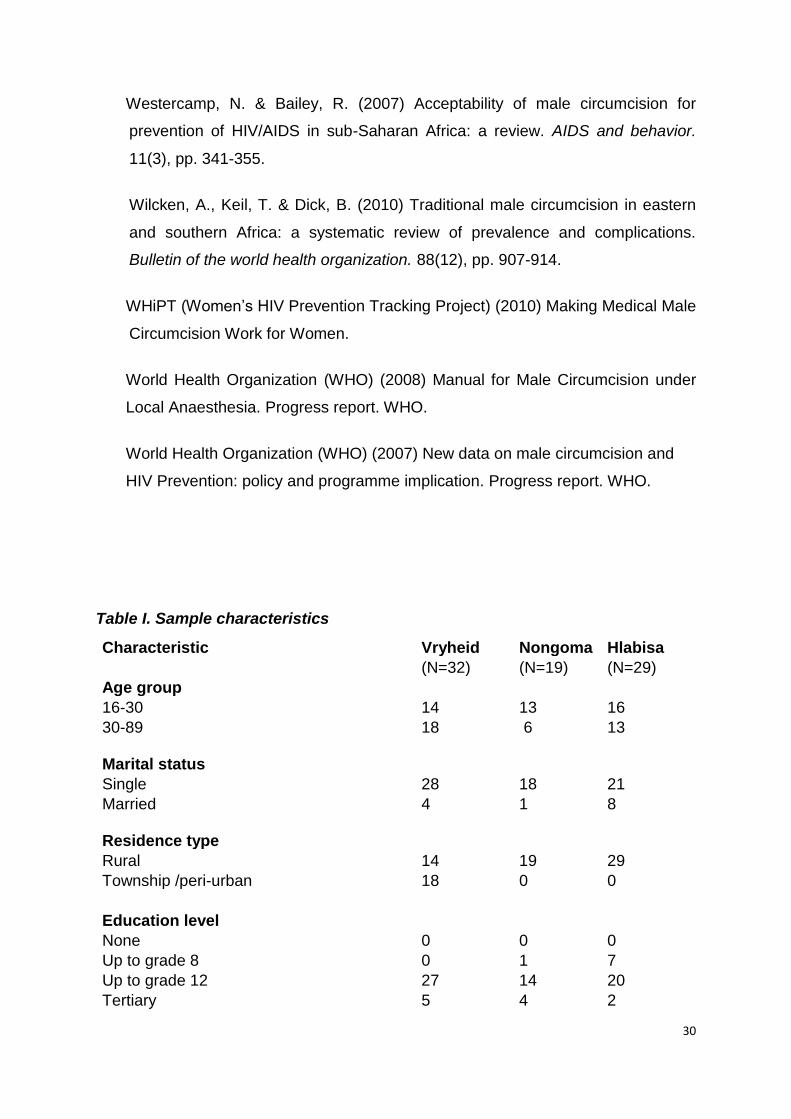
Sample Characteristics
The study took place in three rural communities: Kwa-Hlabisa, a deep rural
community, Bhekuzulu and Hlobane, semi-rural townships near the town of Vryheid,
and Nongoma, a rural village and traditional home of the Zulu monarch. Kwa-Hlabisa
and Nongoma share similar socio-economic development centred on tourism
focused in a nearby game reserve, while Bhekuzulu and Hlobane is a coal mining
centre with a substantial cattle farming sector. In total 80 men participated in the
study, 32 from Bhekuzulu and Hlobane, 19 from Nongoma and 29 from Kwa-Hlabisa.
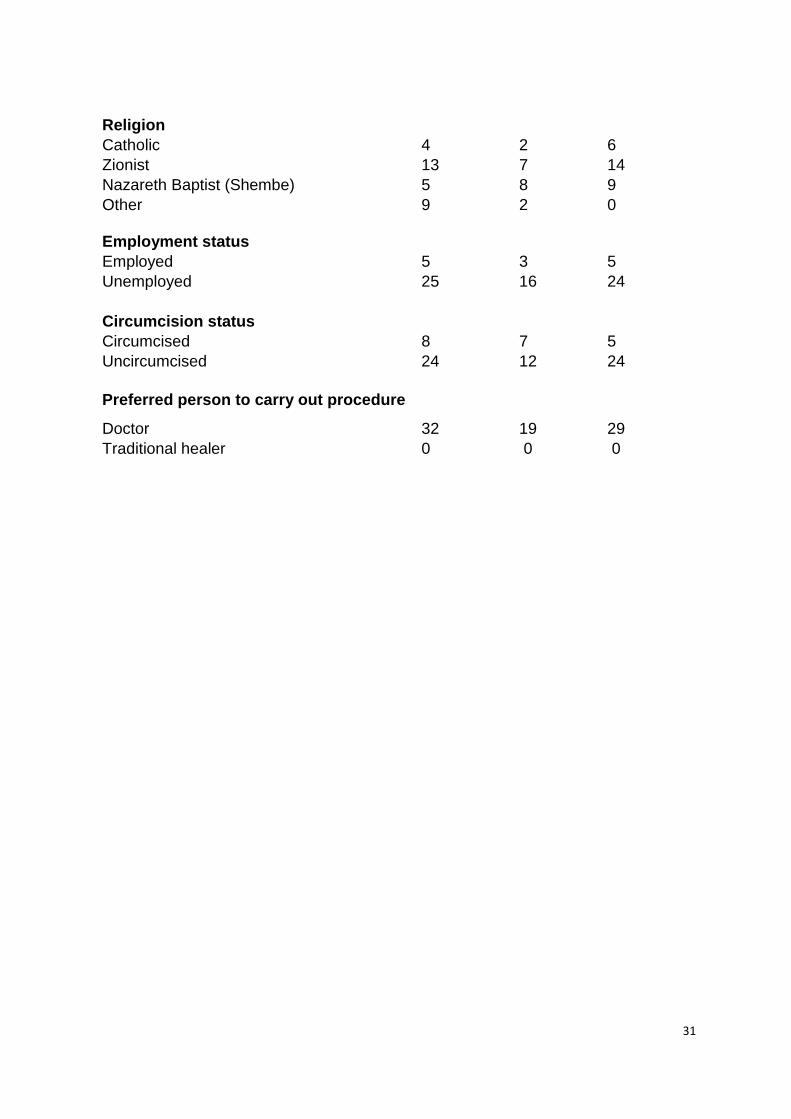
Key characteristics of the sample are included in Table 1. The prevalence of
circumcision in these communities was low with only 22 men (28%) reporting that
they had been either medically or traditionally circumcised. Half of the sample self-
reported that they knew their HIV status, although participants were not required or
encouraged to disclose.
Table 1: Sample characteristic (attached)
General knowledge of male circumcision
In the in-depth interviews and focus group discussions men demonstrated high
levels of knowledge of the male circumcision (MC) practice. Participants described
male circumcision using the term ukuqhatha, a Zulu word referring to being
traditionally circumcised “at the mountain”, a reference to cutting off the foreskin on
the tip of the penis in a traditional setting according to traditional practice (Bailey et
al., 2001). Participants described a foreskin as ‘a trap’ or ‘a host’ for dirt and bacteria.
This general knowledge existed despite the very limited practice of traditional male
10
circumcision (TMC) among Zulu men. Many participants remarked that MC had
health benefits specific to HIV and sexual transmitted infections (STIs), details
regarding the nature of these benefits varied by age with young men being better
able to articulate them than older men.
In individual interviews men were asked to describe the distinction between
traditional and medical circumcision. All the participants shared a common
understanding that traditional circumcision is performed on adolescents or young
men, ‘at the mountain’, in non-clinical settings, by traditional health care providers,
for cultural or religious reasons. In contrast medical circumcision is carried out in a
clinic or hospital setting, by trained health professionals with the use of anesthetic.
“Traditional circumcision is done in mountains, usually by izinyanga
(traditional health practitioners) whereas medical circumcision happens in the
hospital, doctors help to do it”. [Male FGD Participants (18-30 years),
Nongoma].
Older and younger focus group participants characterised traditional circumcision as
“… dangerous and painful … Some men do not come back from the mountain, they
die there”. They were concerned about the safety of traditional circumcision as they
believed the practice had led to high death rates among young boys, particularly in
the Xhosa population. In contrast, medical circumcision was seen as a safe
procedure performed by doctors.
“I have heard that circumcision at the mountain is performed by people who
are not trained and it is painful, there are no treatments like tablets and
injections and some boys don’t come back. But circumcision done at the
hospital is safe, there are trained doctors and they can inject you so that you
feel better, you see?” [Male FGD Participants (18-30 years), Vryheid].
Understanding of KwaZulu-Natal MMC programme
Nearly all respondents were aware that MMC was available in health care settings
like hospitals and that a programme was being rolled-out in KwaZulu-Natal by the
Department of Health. Older men praised the Zulu King for bringing the circumcision
11
tradition back to hospitals as part of preventing HIV. Their belief was the provincial
MMC programme was safer because it was hospital-based and hospitals had the
necessary capacity to respond to excessive bleeding which could result in death as
had happened with circumcisions performed traditionally. MMC in hospital meant
access to other services such as blood pressure and weight measurement, and HIV
counseling and testing (HCT), although as discussed below the provision of HCT
was not entirely straightforward.
“To do circumcision at the hospital is safe and clean because trained doctors
are there. Should it happen that the person has prolonged bleeding the
hospital will be able to give him some injections and tablets to stop the
bleeding. That is not done at the mountain”. [FGD participant (30-89 years),
Nongoma].
Understanding the relationship between HIV and MMC
Participants also demonstrated significant knowledge and understanding of the local
HIV pandemic and understood something of the scale of the problem in their local
areas. Despite a functioning and widely available HIV treatment and care
programme (Houlihan et al., 2009), they described the impact of HIV in their
communities using a frequently repeated phrase: “Many people are dying in this
community because of this disease (HIV)”. In interviews, old men placed the blame
for HIV on young people being irresponsible in respect to condom use. When asked
“who are the most affected people in terms of the age group?” there was consensus
that it was young people because they often consume alcohol excessively and forget
to use condoms and therefore new strategies such as MMC were needed as ones
like Abstain, Be faithful and Condomise (ABC) have failed.
In focus groups the association between HIV and MMC was described more in
relation to the strong protective correlation between circumcision and reduced STIs
and HIV. But among some interviewees this was claimed to be hearsay - what had
been reported in the media – of which men had no evidence in their own experience.
Alternatively circumcision did not prevent HIV transmission or provide a cure once
one had been infected, it simply reduced the chances of being infected; and if
infected the course of disease would be the same. So while knowledge was
12
generally accurate, understanding was not grounded in either scientific evidence, or
personal experience.
“People who circumcise must be clearly told that if they are circumcising it is
not that they are preventing getting infected with HIV or you will not get HIV.
Circumcising minimizes the chances of getting infected with 60% and does
not permit a person to have unprotected sex”. [18 year old Male, IDI, Vryheid].
In contrast, older men were not certain about the relationship between HIV and MC,
except for what they had learned from the media.
“We hear that male circumcision prevents HIV. When this foreskin is cut it
helps to prevent HIV. There is also this thing called a condom as well, others
use it, others don’t use it at all, but it is used to help prevent HIV. [Male FGD
Participants (30-89 years), Hlabisa].
Focus group participants demonstrated higher-levels of knowledge about the
association between circumcision and protection against HIV and STI. Young men
particularly were clear in their beliefs that circumcision was not a substitute for a
condom; that it was only partially effective in protecting men from acquiring HIV
infection and that men must continue using condoms even if they had been
medically circumcised because MC would not protect their female partners from
acquiring HIV. Removing the foreskin eliminated many cells targeted by HIV and the
“germs” that caused STIs, and HIV could not live on a circumcised penis, but it was
not entirely effective, so condoms were still needed.
“It is not true that you can’t get HIV but the chances of getting it decrease, and
circumcising does not mean that you should have unprotected sex because
circumcising does not prevent you from impregnating your girlfriend,
circumcision only makes the chances of getting HIV lower and protects you
from STIs infection.” [18 year old Male, IDI, Nongoma].
13
Facilitators of MMC uptake
Several factors mixing health and sexual pleasure emerged as powerful motivators
for men to undergo circumcision. Unsurprisingly the health benefit of male
circumcision in reducing HIV and STI risk was the strongest of these and the
greatest motivator for most men to undergo the procedure.
“Circumcision helps you not get HIV easily, and STIs. So once a man has
removed the foreskin, chances that he can get any sort of STIs are very small
and that is why I decided to do circumcision” [Male FGD participants (30-89
years), Nongoma].
But other factors were also described as important, specifically improved sexual
performance and increased sexual pleasure. Several interview participants spoke
about an association between circumcision and increased sexual pleasure although
they were not sure what might account for this. Their beliefs, by their own admission,
were based on information from others, and few could base their beliefs on personal
experience. Older men on the other hand, stated the association was baseless.
“The truth is that there is no one who can say there is a difference unless it is
from a person who can feel this and say that it is a first time I am sleeping with
someone like this (circumcised) it is different. How can you know the
difference because it is still as it was when you were not circumcised? Unless
it is a person who has just circumcised now” [Male FGD Participants (30-89
years), Hlabisa].
However, in all the focus groups, and across the three different locations, at least
one participant referred to his own experience of increased sexual pleasure after
being medically circumcised.
“What I can say is that I used to think that I was having good sex but after
circumcising that is when I was feeling it” [18 year old Male, IDI, Vryheid].
Younger men also claimed that being circumcised enhanced sexual pleasure and
satisfaction for women - a belief that is widely held among both young men and
young women and often discussed in community gatherings of men (Wilcken, et al,.
14
2010; Sawires, et al., 2007). Somewhat worryingly, in focus groups men described
the mechanism that explained women’s enhanced sexual pleasure as being that
circumcision acted “something like a ‘natural condom’” - implying that being
circumcised eliminated the need for barrier protection and that the effect of
circumcision made consistent condom-use less important.
Pressure from peers was another important influence on the decision whether or not
to be circumcised.
“I was staying in Durban with friends who are circumcised, so I used to get
embarrassed at other times when I was taking a bath in front of them because
they were circumcised and I was not. I saw myself as someone who is not at
their level and they laughed a lot at me” [Male FGD Participants (18-30
years), Vryheid].
The nature of peer pressure was not restricted to friends and chronological peers,
men also referred to the peer pressure that came from religious association and
fellow church members, particularly those with links to the Shembe Christian Church
(Masondo, 2004). Among older men, a few participants remarked that they had been
circumcised at the mountain in line with their religious beliefs (Shembe Church).
While others described that abiding by the principles of the church and acceptance
by other men of their faith was their primary motivation for undergoing circumcision.
“I have seen a lot of circumcised people from the Shembe Church. If you are
not circumcised you do not eat with those who are circumcised, you eat alone
and they exclude uncircumcised men when discussing important matters of
the church. I have seen them from Shembe Church especially, they sit there
and you also sit here to show that you have not done this job, male
circumcision” [Male FGD Participants (30-89 years), Hlabisa].
According to these men the religious conventions around circumcision within their
mainly African Independent/Indigenous Churches, were underpinned by beliefs
about the improved hygiene afforded by circumcision. But hygiene was also
frequently mentioned by men without religious connections, as a potent motivator.

15
Without making a direct connection with the reduced HIV/STI risk, they described the
cutting of the foreskin as a symbol of cleanliness and good hygiene, and explained
this was the reason uncircumcised men need to shower after sex to avoid ‘disease
problems’[1].
Factors inhibiting MMC uptake
Issues surrounding the circumcision procedure, the healing requirements and
concerns about the delivery of services appeared to be the main factors inhibiting
men from taking up circumcision. The MMC roll-out model being implemented in
KwaZulu-Natal involves a mix of facility-based services that includes surgical
circumcisions performed in hospitals, stand-alone circumcision clinics (mainly in
urban areas), special clinics within the services of local primary healthcare clinics
and community-based seasonal circumcision camps. Currently the majority of
medical male circumcisions are performed in public hospitals with limited capacity or
private GPs (KZN Department of Health, 2010). However, before MC was carried-out
in public health hospitals the procedure was performed in Department of Health
seasonal circumcision camps. The camps were staffed by Department of Health
staff, set-up in local community halls or tents, mainly in rural communities in each
health district, often at some distance from the referral hospital, mainly on weekends
and during holiday periods. Men are mobilized and recruited from different settings -
schools, churches, taverns, Izimbizo (large community gathering), taxi ranks – to
attend the camps. The circumcision camps routinely last for at least two days, and
involve the processing of a hundred or more men per day. The minimum package of
care in the circumcision camps involves information giving, written informed consent
to undergo the procedure, HIV testing and counselling, with MMC performed
according to clinical manual/guidelines under local anesthesia and follow-up after 24-
hours. (KZN Department of Health, MMC manual 2010).
Fear of adverse events – excessive pain, bleeding and even death, during and after
a circumcision, were the most cited barrier to uptake of medically performed
circumcisions, although none of the participants actually knew of any deaths in the
provincial roll-out programme. Respondents were less concerned if the circumcision
16
was performed in a hospital compared to a clinic or circumcision camp because of
the availability of back-up.
“We understood that circumcision was going to happen at the hospital. We
looked at the deaths that were occurring in other provinces like Eastern Cape
where Xhosa boys lost their lives due to excessive bleeding. Although these
circumcisions were performed at the mountain, these instances will always
bring a second thought if one thinks of going to a camp for MC even though it
is supposed to be safe” [Male FGD Participants ( 30-89), Nongoma].
To reduce risk of HIV/STI infection and potential longer term sexual health problems,
men are instructed to abstain from sexual intercourse for a minimum of four and
optimally eight weeks, following the procedure. This is because of the increased risk
for women. This is the common recommendation of both the WHO and KwaZulu-
Natal Department of Health (KZN Department of Health, 2010; WHO, 2008). The
abstinence period was described as a major barrier for men in regular and formal
relationships, but also among those who described only having casual sexual
partners. Despite being convinced that their female partners would enjoy sex more
with them if they were circumcised, young men were concerned that their partners
might have sex with other men during this healing period. Older men and married
men viewed the abstinence period as a serious obstacle because sharing a bed with
their partners would make it impossible for them comply.
“For us is not easy, in a way that if you have a partner it is not easy that you
can do it. For me it will not just be easy because my wife is beside me all the
time. I first have to talk to her and say I am thinking of doing this thing (MMC)
and it should be something that we both agree on”. [Male FGD participants
(30-89 years), Hlabisa].
In the focus groups several recently circumcised men reported shorter wound
healing times than described by health care staff, and as such they reported
abstinence periods that varied from those recommended. Several claimed healing,
and by inference, abstinence periods of as little as two weeks, others reported longer
healing times, but still significantly less than the MMC guidance. It seemed most
17
newly circumcised men determined for themselves what constituted an adequate
period of sexual abstinence, although these same men appeared to disapprove of
any increase in risky sex following the procedure, arguing, “it would not make sense
because the primary reason for circumcision is to reduce chances of getting HIV”.
Local MMC guidance also recommends several days rest at home following the
procedure. Although this was less of a concern than the abstinence period, working
men, men in education and men who wanted to keep their circumcision choices
private identified this as a potential barrier. However, it was the ‘requirement’ of an
HIV test prior to having the procedure that caused a major problem. The KwaZulu-
Natal Department of Health circumcision patient information advises that prior to the
procedure men will receive a group counseling and can voluntarily undergo HIV
counseling and testing (HCT) (KZN Department of Health, 2010) and that this is part
of the package of ‘health checking’ offered in the public circumcision services.
However, some uncircumcised men reported they would be ‘required’ to undergo
HIV testing having been told it was compulsory, before having the procedure.
“This is surprising to me that you are first tested for HIV because people are
scared to test their blood. It means many guys (adult men) will be scared to
circumcise too”. [Male FGD Participants (18-30 years), Vryheid].
The young men understood that only HIV-negative men would be circumcised, and
that those testing HIV-positive would not be able to have the procedure immediately.
They would be told to return home and wait for an opening on a hospital surgical
waiting list. In addition to not being prepared to test, many young men attending the
camps do so as groups of friends, and the HIV testing requirement created an
obstacle because it would have the effect of indirectly disclosing both their
circumcision and HIV status to all who knew them. This was potentially the most
serious reason for young men not coming forward when MMC was being offered
locally in circumcision camps.
Concern about how MMC services were being rolled-out also worried health care
workers. All health care workers remarked that a shortage of staff was the main
barrier to better provision of MMC, especially in the most remote areas. For young
18
men, staff shortages meant long waiting-times, queues at the camps, and in turn led
them to feel health care staff lacked concern and caused distrust between patients
and providers.
“This MMC programme is a good strategy to fight against HIV but what I
noticed when I went for circumcision was that there were few doctors and
many patients waiting to be circumcised. People started complaining because
they were told not to eat anything and some guys who were behind me left
because it was getting late. The government must bring more staff” [18 year
old, IDI, Nongoma].
Health care staff noted that workload and working environments contributed to
additional pressure and strain that affected the quality of MMC services. This in turn
created barriers for men who may have wanted to come forward. The strains on the
MMC services were being felt in all the facilities, but most notably in hospitals that
had a high volume of MMC clients on daily basis.
“Getting tired is something we experience a lot because since the campaign
started it has never happened that there is additional staff provided. The staff
that works on the campaign is the staff that works from Wednesday to allocate
circumcisions that will take place on Saturday and Sunday. At the same time,
there is work at the ward; there are patients who have already circumcised
which you need to pay attention to and other people who are not visiting for
MMC. It is the same staff and you are not divided. There is a serious work
load issue” [One HCP, FGD,].
Since the introduction of the seasonal circumcision camps offering MMC on a mass
scale, many more boys and young adult men have begun to come forward. But
health care workers expressed concern that the working conditions in the camps
were affecting the quality and hygiene of the services, making them reluctant to
recommend the circumcision camps if asked.
“The other barrier I have seen is the place where the work is done at the
camps. You find that there is not enough space or the place is not very clean
and the procedures that are done need to be practiced carefully, I end up
19
seeing patients coming back here, some with septic problems and I think it is
the place where the work was done which was not clean.[HCP, FGD,].
In the health care workers’ opinion, this problem would only be resolved by
increasing capacity, establishing new dedicated MMC units and allowing trained
circumcisers to do the job in hospitals/clinics rather than surgical staff. Specific
designated staff (trained circumcisers) within hospitals was considered the most
appropriate way to strengthening the programme immediately, as health care
workers all agreed that in the coming months and years demand for the service
would only increase and what was being practiced now was not sustainable.
Attitudes of men towards MMC
Men in the study were supportive of MMC roll-out as part of the HIV prevention
response, and many young men said would be circumcised if, and so long as, they
perceived the MMC programme to be safe. There was strong support from older
men, although their desire for MMC was much lower because being in a steady
partnership, they felt they were at less risk.
“We are in support of male circumcision to be done in hospitals so that HIV
risk can be decreased and we think this is good because in hospitals
complications maybe prevented” [Male FGD Participants (30-89), Hlabisa].
However, they were enthusiastic about recommending it to young men, wherever it
might be offered, because young men, they believed, were highly sexually active,
often with multiple partners, and users of alcohol; all of which increased their HIV
and STI risk. The MMC programme was an exciting development, for which they
praised the Zulu King. It would save lives particularly of young people who were
otherwise caught in a gap between traditional values and ways of living, and the
uncertainty of an ongoing HIV pandemic that continued to cause many deaths in
their communities.
Discussion
Acceptability of MMC has been shown in numerous research studies, including one
conducted in this population (Scott, Weiss & Viljoen, 2005), and now by the high
20
volume of demand in clinical facilities. Rather than acceptability, this study instead
focused on rural men’s knowledge, attitudes and beliefs about MMC following the
initial phases of the provincial government’s roll-out programme to highlight potential
facilitators and obstacles to MMC uptake. As circumcision programmes come to
scale in different parts of South Africa and other areas of the continent, additional
qualitative data are needed to inform, improve and optimize these services, and to
guide development of the next generation of men’s health education and the
continuing professional development of health care staff.
In 2007, the WHO endorsed MMC as an additional component in national HIV
prevention strategies (WHO, 2007). Since then exploration studies of perceptions,
knowledge and beliefs have guided the scaling-up MMC programmes (Westercamp
& Bailey, 2007); Herman-Roloff et al., 2011). Support for medical circumcision in the
area where this study was conducted has been high for a number of years as Scott
et al’s demonstrated in 2005 (Scott et al., 2005). In the same approximate
geographic area as this study, they found 66% of men and 64% of women would
support re-introduction of circumcision if it could provide protection from STIs and
HIV (Scott et al., 2005). Like other men in their communities, the majority in this
study had not been circumcised, yet they were aware of medical circumcision
practice, the health benefits of the procedure and found it an acceptability
intervention. There was some variation in knowledge according to age with some
older men being less conversant with the detailed health benefits, but still being
aware that medical circumcisions reduces HIV infection risk. The high level of
acceptability and knowledge is at least partly attributable to the open discussion of
circumcision at the highest traditional and government levels in South Africa, and
effective health communication including through the news media and health
promotion.
However, these results are not consistent with those found in Uganda where older
men demonstrated greater knowledge of the health benefits of circumcision than
young people (Wilcken, Keil & Dick, 2010). One possible explanation is that as part
of the post-apartheid legacy, the older men in this study had less experience of
formal education than younger men. Nevertheless, the differences highlight the
importance of conducting context-specific research to inform local programming and
21
the need for additional health education that specifically targets older men (> 30
years).
All the men in this study were able to distinguish between traditional and medical
male circumcision, and nearly all held some type of negative beliefs about the
traditional practice. These seemed to be based primarily on stories from the media,
rather than personal experience. In contrast, they were generally positive about
medical male circumcision performed in health care settings which was seen to be
much safer. This is consistent with Scott et al’s previous findings in the area - that
among uncircumcised Zulu men, circumcision by a medical provider, in hospitals,
with adequate access to back-up and medication to deal with pain was preferred
over traditional practice and the basis on which MMC should be scaled-up (Scott et
al., 2005). In traditionally non-circumcising communities, fear of excessive pain,
bleeding, mutilation and preventable premature death during and after circumcision
are potent barriers. As much as programmatic staff may claim to be able to deal with
these issues, the patient reality and circulating knowledge in the community is a
more powerful influence. As the health care workers acknowledged, ensuring the
continued acceptability of MMC and men’s use of the public sector MMC services
depends on maintaining high standards and avoiding the potential damage
associated with highly publicized adverse outcomes and at the same time doing
everything to improve the patient experience (see for example; ‘Worries over
‘dangerous circumcisions’ http://www.news24.com/SouthAfrica/AidsFocus/Worries-
over-dangerous-circumcisions-20120823 accessed 9 October 2012 ).
The WHO and UNAIDS recommend that an HIV test is performed before medical
circumcision (WHO, 2007), but neither excludes men undergoing circumcision on the
basis of their HIV-positive status or refusal to test. In this study participants reported
fear of HIV testing as a primary barrier to taking up MMC. It was noted in the
participant focus groups and interviews, and confirmed by the health care workers.
Similar results were reported by Grund & Hennink who found that HIV counselling
and testing acted as a barrier to circumcision mainly among those fearing a potential
positive result (Grund & Hennink, 2011). A review of the current guidance concerning
medical circumcision and those who test HIV-positive may be appropriate given the
growing evidence of health benefits associated with MMC for men and their sexual
22
partners, and in the context of improved HIV treatment access, increased life
expectancy and persistent high incidence and prevalence of STI in these
communities.
Younger participants seemed to agree that having undergone circumcision their
sexual performance and sexual pleasure would be enhanced. Although this was
dismissed as baseless by older men, recently circumcised participants’ claimed this
based on their own experience. While it is possible these testimonies were in part
youthful hyperbole in the context of a focus group discussion, the finding is still in line
with other reports in the literature that conclude some men are motivated to undergo
circumcision in order to enhance their sexual pleasure (Peters et al., 2009; Lagarde
et al., 2003; Bailey et al., 2002;). Nevertheless, these findings are important for two
reasons. Firstly, because some men described the mechanism by which sexual
pleasure would be enhanced as involving reduced need for consistent condom-use,
which would be possibly indicative of behavioural disinhibition (Herman-Roloff et al.,
Grund, & Hennink, 2011). And secondly because some of the beliefs described by
men could at least in part be confirmed or refuted by greater inclusion of women’s
voices in the hypothetical discussions surrounding enhanced sexual performance
and pleasure (Gray et al., 2008; Auvert et al., 2005).
The possibility of behavioural disinhibition is also partially supported by newly
circumcised men’s decisions to resume sexual activity according to their own
timetable of wound healing, rather than following advice of health care staff. This
pattern has been observed in studies in Kenya, Uganda, Rwanda (Bailey et al.,
2002), in the South African MMC efficacy trial conducted at Orange Farm (Auvert et
al., 2005) and in a community study in Mpumalanga province (Peltzer et al., 2009).
Although current counselling and educational information emphasizes that MMC is
not a substitute for condoms, and that consistent condom-use is still required to
maximize the intervention’s protective effect; this does not appear to be consistently
reflected in men’s prevention choices. We did not specifically address risk
compensation or behavioural disinhibition with recently circumcised men, but
participants were asked about HIV risk after circumcision. Those who felt able to
comment appeared to disapprove of anyone embarking on sexually risky behavior
after undergoing circumcision because it would undermine their reason for having
23
been circumcised. What is clear in this context, like many others, is that
circumcision, condom-use, sexual pleasure, gender equity and sexual negotiation
are intertwined.
The sexual performance and sexual pleasure theme in these data also highlights the
relative absence of women and sexual partners’ concerns in men’s discussion of
medical circumcision. Although men believed women preferred sex with circumcised
men, and that it was more satisfying for women, they qualified their comments
saying they had only ever heard this, and never from women. There is still only a
small body of research examining women’s preferences concerning sexual partners
and circumcision status (Women’s HIV Prevention Tracking Project, 2010; Weiss et
al., 2009; Hankins, 2007; Mattson et al., 2005). Appropriate health advice about
circumcision, the protective benefits and how it works or not, for women needs wider
dissemination, especially in rural populations where much of the burden of HIV
prevention already falls on women. This may help women to become more active in
decision-making about undergoing circumcision within partnerships (Lissouba et al.,
2011). At least one of the men in this sample described including his female partner
in his decision-making which suggests there is an opportunity for effective health
promotion that is not being sufficiently exploited.
Like all studies, this work is not without limitations. Only one FGD was conducted
with healthcare providers and the group did not include surgeons or general
practitioners who are the people actually carrying out circumcisions. Healthcare
providers’ views are important in understanding what is needed next in the scale-up
of MMC and to highlight some gaps and challenges to improving quality in MMC
services. There is the possibility that different groups of health providers would have
had more varied attitudes and perception of the MMC programmes and the issues
they face or that these views would change over time. It is therefore pivotal to fill
these gaps so that all parties involved in MMC roll-out are considered to ensure
smooth delivery and expansion of the programme.
The study results should not be generalized to other countries since the sample was
not large and was specifically drawn from rural Zulu communities. This is an
important community given low-level of circumcision to date and the high HIV
24
prevalence. If the results of this study are to be used it is important to take into
consideration that the study was conducted in a non-circumcising community which
has a particular history of male circumcision and where traditional social and cultural
values are strong (Scott et al., 2005).
Conclusion
The effective roll-out of medical male circumcision requires an ongoing process of
evaluation, particularly in the early stages and while the programme is being
deployed into new areas. This study has highlighted that although men potentially
eligible for the procedure are generally knowledgeable and well-disposed, there are
educational gaps, adherence problems and systematic delivery issues that have the
potential to become significant barriers to continued success. Interventions to
address these deficiencies need to be considered, implemented and evaluated. They
need not require significant additional resources and potentially could be delivered
through the re-prioritisation of existing ones.
Acknowledgements
The authors wish to acknowledge with appreciation the contributions of the following:
South African Medical Research Council (MRC), Africa Centre for Health and
Population studies, Umthombo Youth Development Foundation, and the KwaZulu-
Natal Department of Health. The authors also thank Thembelihle Zuma, Nora
Rosenberg, the local authorities, communities, participants and research assistants
who made this study possible through their cooperation and participation.
The authors— Sicelo Sengwayo is a junior researcher in the Department of Health
Studies at the University of South Africa. Christopher J. Colvin is a Senior Research
Officer in Social Sciences and HIV/AIDS, TB and STIs at the School of Public Health
and Family Medicine at the University of Cape Town. Marie-Louise Newell is an
epidemiologist and Director of the Africa Centre for Health and Population Studies.
John Imrie is a social scientist and Social Science Lead at the Africa Centre for
Health and Population Studies.
25
Endnotes: [1]
An indirect reference to South African President, Jacob Zuma’s court testimony during his trial over
allegations of sexual assault by an HIV positive activist. Mr. Zuma claimed after having sex with the
complainant, he got up and took a shower to minimize chances of being HIV infected. In court, Zuma
was asked to elaborate on his HIV/AIDS background knowledge–what it was that he knew about the
disease and why he had chosen to have sex with someone he knew was HIV positive. Zuma
explained that he had headed a government initiative on AIDS and that he had a relatively high level
of knowledge about the disease. “I had knowledge that as a male person the chances were very slim
one would contract the disease, just because you had intercourse with a woman you would [not]
automatically be infected,” He added that he did not have HIV or any other sexually transmitted
infections so would not have put the complainant at further risk (Skeen, 2007).
References
Auvert, B., Sobngwi-Tambekou, J., Cutler, E. (2009) Effect of male circumcision
on the prevalence of high risk human papilloma virus in young men: results of a
randomized controlled trial conducted at Orange Farm, South Africa. J Infect
Dis.10:14-29.
Auvert, B., Taljaard, D., Lagarde, E. Sobngwi-Tambekou, J. & Puren, A. (2005)
Randomized, controlled intervention trial of male circumcision for reduction of
HIV infection risk: the ANRS 1265 Trial. PLoS medicine. 2(11), pp.298.
Bailey, R.C. (2001) Male circumcision and HIV prevention: current knowledge
and future research directions. The lancet infectious diseases. 1(4), pp. 223.
Bailey, R.C., Muga, R., Poulussen, R. & Abicht, H. (2002) The acceptability of
male circumcision to reduce HIV infections in Nyanza Province, Kenya. AIDS
care. 14(1), pp. 27-40.
Bailey, R.C., Moses, S., Parker, C.B., Agot, K., Maclean, I., Krieger, J.N.,
Williams, C.F.M., Campbell, R.T. & Ndinya-Achola, J.O. (2007) Male
circumcision for HIV prevention in young men in Kisumu, Kenya: a randomised
controlled trial. The Lancet. 369(9562), pp. 643-656.
26
Crowley, I.P. (1990) Ritual circumcision (Umkhwetha) amongst the Xhosa of the
Ciskei. British journal of urology. 66(3), pp. 318 330.
Gray, R.H.,Wawer, M.J., Polis, C.B., Kigozi, G. & Serwadda, D. (2008) Male
circumcision and prevention of HIV and sexually transmitted infections. Current
infectious disease reports. 10(2), pp.121-127.
Grund, J.M. & Hennink, M.M. (2011) A qualitative study of sexual behavior
change and risk compensation following adult male circumcision in urban
Swaziland.
Hankins, C. (2007) Male circumcision: Implication for women as sexual partners
and parents. Reprod Health Matters. May: 15 (29), pp. 62-7
Herman-Roloff, A., Otieno, N., Agot, K., Ndinya-Achola, J. & Bailey, R.C. (2011)
Acceptability of Medical Male Circumcision Among Uncircumcised Men in Kenya
One Year After the National Male Circumcision Program. PLoSONE 6(5), pp.
10-1371
Houlihan, C. F., Bland, R. M., Mutevedzi, P. C., Lessells, R. J., Ndirangu, J.,
Thulare, H. & Newell, M (2009) Cohort Profile: Hlabisa HIV Treatment and Care
Programme. Oxford University Press: International Journal of Epidemiology
King, N. (2004) Using Interviews in Quantitative Research. Essential guide to
qualitative methods in organizational research.
Kwata, F. (2009) Traditional male circumcision: What is its socio-cultural
significance among young Xhosa men? Aids and Society Research Unit.
KwaZulu-Natal Department of Health [South Africa] (2010) Press Release, 5
November 2010: Presentation of a progress report on male circumcision to the
Zulu King, in Durban City Hall, Main Hall.
KwaZulu-Natal Department of Health (KZNDoH) [South Africa] (2010) Medical
Male Circumcision (MMC) manual.
27
‘KwaZulu-Natal takes healthy strides’ Mail & Guardian (Health Supplement), 5 –
11 October 2012, p.4)
Lagarde, E., Dirk, T., Puren, A., Reathe, R.T. & Bertran, A. (2003) Acceptability
of male circumcision as a tool for preventing HIV infection in highly infected
community in South Africa. AIDS. 17(6), pp. 89-95
Lissouba, P., Taljaard, D., Rech, D., Shabangu, D., Nhlapho, C., Otchere-Darko,
J., Mashigo, T., Taljaard, R., Phatedi, G., Tsepe, M., Chakela, M., Mkhwanazi,
A., Ntshnagse, P., Billy, S., Lewis, D. & Auvert, B. (2011) Knowledge, attitudes
and practices of women towards male circumcision after three years of roll-out in
Orange Farm, South Africa. Abstract Exhibition of the 6th IAS Conference on HIV
Pathogenesis Treatment and Prevention, Rome, Italy, 17-20 July 2011.Italy.
Abstract No. TUPE379.
Marck, J. (1997) Aspects of male circumcision in subequatorial African culture
history. Health transition review. 7 (3), pp. 337-360.
Masondo, S. (2004) Models of change in African Christianity: South African
Case studies. Religion, politics, and identity in a changing South Africa. 8 (5),
pp.161-181.
Mattson, C. L., Bailey, R.C., Muga, R., Poulussen, R., & Onyango, T. (2005)
Acceptability of Male circumcision and predictors of circumcision preference
among men women in Nyanza Province: Psychological and Socio-medical
aspects of AIDS/HIV. AIDS Care: 17 (2), pp. 182-194
Moodley, E.M. (2010) An assessment of students' perceptions of the ABC
prevention strategy: toward students' participation in HIV/AIDS message design
at the University of KwaZulu-Natal. Master's thesis, Department of Culture,
Communication and Media Studies, University of KwaZulu-Natal, Durban, South
Africa.
Morris, B.J. (2010) Male circumcision for doctors, parents, adults and teen Guidelines. America.
28
Peltzer, K., Banyini, M., Simbayi, L. & Kalichman, S. (2009) Knowledge,
Attitudes and Benefits about Male Circumcision and HIV by Traditional and
Medical Providers of male Circumcision and Traditionally and medically
Circumcised Men in Mpumalanga, South Africa. Gender and Behavioural. 7 (2),
pp. 132-180
Peters, F. & Marcus, T.S. (2010) Circumcision weeks: making circumcision part
of routine training and service delivery at district-level hospitals in South Africa.
South african family practice. 53(3), pp. 262-266.
Sawires, S.R., Dworkin, S.L., & Fiamma, A. (2007) Male circumcision and
HIV/AIDS: challenges and opportunities. The Lancet. 369(9562), pp. 708-713.
Scott, B.E., Weiss, H.A., & Viljoen, J.I. (2005) The acceptability of Male
circumcision as an HIV intervention among a rural Zulu population, KwaZulu-
Natal, South Africa. AIDS Care. 17(3), pp. 304-313.
Shisana, O., Rehle, T., Simbayi, L., Parker, W., Jooste, S., Pillay-van Wyk, V.,
Mbele N. & van Zyl, J. (2009) South African National HIV Prevalence,
Incidence, Behaviour and Communication Survey, 2008: Cape Town, South
Africa, Human Science Research C ouncil (HSRC).
Skeen, E. (2007) The Rape of Trial: Jacob Zuma, AIDS, Conspiracy, and
Tribalism in Neo-Liberal Post- Apartheid South Africa. Master's thesis,
Department of Anthropology, Princeton University, United State.
National Department of Health (NDoH)(2010) The National Antenatal Sentinel
HIV & Syphilis Prevalence Survey 2010 in South Africa, Pretoria.
Taljaard, R., Taljaard, D.Auvert, B. & Neilssen, G. (2000) Cutting it fine male
circumcision practises and the transmission of STDs in Carletonville. Abstract of
the 13th International AIDS Conference, Durban, South Africa, 9-14 July 2000.
Abstract no. MoOrC195.
29
Tenge, S. (2009) Xhosa teenage boys' experiences during the period prior to
circumcision ritual in East London in the Eastern Cape Province. Master’s
thesis, Department of Health Studies, University of South Africa, South Africa.
Tobian, A.R., Serwadda, D. & Quinn, T.C. (2009) Male circumcision for the
prevention of HSV-2 and HPV infections and syphilis. N Engl J Med. 360(13),
pp. 1298-1309.
Tyndall, M.W., Ronald, A.R., Agoki, E., Malisa, W., Bwayo, J.J., Ndinya-Achola,
J.O., Moses, S. & Plummer, F.A. (1996) Increased risk of infection with human
immunodeficiency virus type 1 among uncircumcised men presenting with
genital ulcer disease in Kenya. Clinical infectious diseases. 23(3), pp. 449.
United Nation AIDS (2008) Male Circumcision and HIV Prevention in Southern
Africa. Geneva.
United Nation AIDS (2009) AIDS epidemic updates. Geneva.
Vincent, L. (2008) 'Boys will be boys': traditional Xhosa male circumcision, HIV
and sexual in contemporary South Africa. Culture, health &# 38; sexuality. 10(5),
pp. 431-446.
Weiss, H.A., Quigley, M.A. & Hayes, R.J. (2000) Male circumcision and risk of
HIV infection in sub-Saharan Africa: a systematic review and meta-analysis.
Aids. 14(15), pp. 2361.
Weiss, H.A., Halperin, D., Bailey, R.C., Hayes, R.J., Schmid, G. & Haskins, C.A.
(2008) Male circumcision for HIV prevention: from evidence to action? Aids.
22(5), pp. 567.
Weiss, H.A., Hankins, C.A. & Dickson, K. (2009) Male Circumcision and risk of
HIV infection in women: A Systematic Review and Meta-Analysis. Lancet Infect
Dis. Nov: 9 (11): 669-77
30
Westercamp, N. & Bailey, R. (2007) Acceptability of male circumcision for
prevention of HIV/AIDS in sub-Saharan Africa: a review. AIDS and behavior.
11(3), pp. 341-355.
Wilcken, A., Keil, T. & Dick, B. (2010) Traditional male circumcision in eastern
and southern Africa: a systematic review of prevalence and complications.
Bulletin of the world health organization. 88(12), pp. 907-914.
WHiPT (Women’s HIV Prevention Tracking Project) (2010) Making Medical Male
Circumcision Work for Women.
World Health Organization (WHO) (2008) Manual for Male Circumcision under
Local Anaesthesia. Progress report. WHO.
World Health Organization (WHO) (2007) New data on male circumcision and
HIV Prevention: policy and programme implication. Progress report. WHO.
Table I. Sample characteristics
Characteristic Vryheid Nongoma Hlabisa
(N=32) (N=19) (N=29)
Age group 16-30 14 13 16
30-89 18 6 13 Marital status
Single 28 18 21
Married 4 1 8 Residence type
Rural 14 19 29
Township /peri-urban 18 0 0
Education level None 0 0 0
Up to grade 8 0 1 7
Up to grade 12 27 14 20
Tertiary 5 4 2
31
Religion Catholic 4 2 6
Zionist 13 7 14
Nazareth Baptist (Shembe) 5 8 9
Other 9 2 0 Employment status
Employed 5 3 5
Unemployed 25 16 24
Circumcision status Circumcised 8 7 5
Uncircumcised 24 12 24
Preferred person to carry out procedure
Doctor 32 19 29
Traditional healer 0 0 0