spectroscopic and histological evaluation of wound healing progression following low level laser...
TRANSCRIPT
FULL ARTICLE
Spectroscopic and histological evaluationof wound healing progression followingLow Level Laser Therapy (LLLT)
Vijendra Prabhu1, Satish B. S. Rao2, Subhash Chandra1, Pramod Kumar3, Lakshmi Rao4,Vasudeva Guddattu5, Kapaettu Satyamoorthy6, and Krishna K. Mahato*; 1
1 Biophysics Unit, Manipal Life Sciences Centre, Manipal University, Manipal 576104, Karnataka, India2 Division of Radiobiology & Toxicology, Manipal Life Sciences Centre, Manipal University, Manipal 576104, India3 Department of Plastic Surgery & Burns, Kasturba Medical College, Manipal University, Manipal 576104, India4 Department of Pathology, Kasturba Medical College, Manipal University, Manipal 576104, India5 Department of Statistics, Manipal University, Manipal 576104, India6 Department of Biotechnology, Manipal Life Sciences Center, Manipal University, Manipal 576104, India
Received 30 September 2011, revised 23 November 2011, accepted 23 November 2011Published online 16 December 2011
Key words: Spectroscopic and microscopic technique, fluorescence in biophysics, therapeutic application,collagen biomolecules.
1. Introduction
Wound by definition is a disruption of normal ana-tomical structure of a tissue and its specific functionassociated with loss of body fluid leading to infec-tion. Healing can be defined as the restoration ofanatomical continuity and function through a very
well-orchestrated dynamic process regulated by cer-tain biological molecules such as cytokines, andgrowth factors [1]. Orderly advancement of cellsthrough four known phases of healing namely he-mostasis, inflammation, proliferation and remodelingor maturation are thus becoming very essential forthe successful acute healing process [2]. On the con-
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim
Journal of
BIOPHOTONICS
The present study focuses on the evaluation of the effectof He-Ne laser on tissue regeneration by monitoring col-lagen synthesis in wound granulation tissues in Swiss al-bino mice using analysis of laser induced fluorescence(LIF) and light microscopy techniques. The spectral ana-lyses of the wound granulation tissues have indicated adose dependent increase in collagen levels during thepost-wounding days. The histological examinations onthe other hand have also shown a significant increase incollagen deposition along with the reduced edema, leu-kocytes, increased granulation tissue, and fibroblastnumber in the optimal laser dose treated group com-pared to the non-illuminated controls. The block diagram of the experimental setup used to
monitor the wound healing progression following LLLTby fluorescence spectroscopy and light microscopy.
* Corresponding author: e-mail: [email protected], Phone: +91-820-2922425, Fax: +91-820-2571919
J. Biophotonics 5, No. 2, 168–184 (2012) / DOI 10.1002/jbio.201100089

trary, chronic wounds often fail to heal in the orderlyfashion, and become the leading cause of physicaland emotional stress to the patients and the clini-cians. Marked reduction in the angiogenesis, col-lagen synthesis, activation and migration of fibro-blasts and prolonged inflamatory reaction in chronicwounds are considered to be the major reasons forfailure of tissue repair process [3]. The wound heal-ing in mammalian system is of prime interest andstudied extensively because of its underlying clini-cal importance. Of late, several promising physicalmethods have been attempted to modulate theevents in all phases of the wound healing processwhich includes the use of stem cells, growth factors,drugs [4], vacuum-assisted wound closure [5], treat-ment with magnetic field pulses [6], light emittingdiode irradiation [7] and low level laser therapy(LLLT) [8, 9].
The LLLT is being widely used in biomedicinefor the treatment of a variety of skin injuries such asburns, surgical wounds, diabetic wounds and ulce-ration [10–13]. Increased ATP production [14], in-creased mitochondrial membrane potential [15] andits activity [16], transformation of fibroblasts intomyofibroblasts [17, 18], increased cell proliferation[19], cell differentiation [20] and collagen productionare the key biological effects witnessed followingLLLT. Our previous studies on the laboratory ani-mals, have shown the photobiomodulatory effectwith He–Ne laser irradiation [21] on the healing ofacute and diabetic wounds with increased collagensynthesis [22, 23]. Even though different laser treat-ment modalities have been used for tissue regenera-tion, histological inspections of the wound tissuebiopsy indicated the formation of new collagen afterthe laser treatments [24]. Thus in LLLT, it is very es-sential to explore the combination of optimal lasertreatment parameters for the most effective collagenremodeling. Collagen is a major protein componentof the extracellular matrix (ECM) responsible forproviding normal skin with tensile strength, integrityand structure. Tensile strength generation is consid-ered to be an important element for successful woundhealing and due to its direct role, periodic and accu-rate monitoring of collagen in this regard may be ofdirect relevance.
Electron microscopy [25], X-ray diffraction [26],biochemical assay [23, 27], High Performance LiquidChromatography (HPLC) [28] and histological ana-lysis [29–31] are the presently available methods tostudy collagen deposition. Although these methodscan identify the presence and types of collagen, theyare destructive and identification could be done onlywith the tissue biopsy samples [32]. Thus, there is aneed for non-destructive technique to monitor col-lagen synthesis during the progression of woundhealing. Laser induced fluorescence (LIF) is one ofsuch techniques which has the potential in monitor-
ing the biochemical, metabolic, and morphologicalchanges in various tissue types [33]. Nicotinamideadenine dinucleotide reduced form (NADH), col-lagen, elastin, aromatic amino acids (tryptophan, tyr-osine, phenylalanine), and flavins are the most com-mon endogenous fluorophores responsible for thetissue autofluorescence [34]. This technique is oftenused in vivo or ex vivo for the diagnosis and dis-crimination of various types of cancers [35–43] andother tissue pathologies [44–46] including woundhealing [33]. However, LIF technique remains to befully explored to evaluate wound healing [33].
Histopathological examination of the tissue oftenconsidered as “gold standard” for the identificationof the various pathological stages during the diseaseprogression. To understand the efficacy of the vari-ous treatment modalities, histopathological studies ofthe wound granulation tissues are routinely beingperformed in the laboratories [47]. Regular inspec-tion of the collagen fibers during wound healingthrough histopathology is believed to be essential[48], as it plays leading role in maintaining the struc-tural integrity of the healed tissues [49]. In addition,several other wound characteristics such as depthand length of healed wounds, degree of neutrophils,macrophages, fibroblasts and epithelialization weremonitored through histopathology [47]. Semi quanti-tative measurements of various histological featuresrelated to inflammation, proliferation and remodel-ing were also used previously, to assess photobiomo-dulatory effects of LLLT on wound healing progres-sion [3, 31, 50–52].
Presented here is a novel approach of combiningtwo different optical techniques – LIF and Lightmicroscopy to investigate the photobiomodulatoryeffect of He-Ne laser on wound healing process.The LIF will provide the information about thechanges in collagen and NADH, while histologicalexaminations of the wound granulation tissues willprovide the detail insight of the changes broughtabout by laser irradiation during healing progres-sion. The correlation between these two sensitivetechniques may provide more information about thebiochemical changes at the tissue level which maybe of ample help in developing a robust LIF basedtechnique for monitoring wound healing in an invivo setting.
2. Materials and methods
2.1 Animal selection
This study was approved by Institutional AnimalEthical Committee, Kasturba Medical College, Man-ipal University, Manipal, India. Six to eight weeks
J. Biophotonics 5, No. 2 (2012) 169
FULLFULLARTICLEARTICLE
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheimwww.biophotonics-journal.org

old Swiss albino mice of either sex weighing 25–30 gwere selected from an inbred colony maintained un-der the controlled conditions of temperature (23 �2 �C) humidity (50 � 5%) and light (14 and 10 h oflight and dark respectively). They were allowed ac-cess to sterile food and water ad libitum. Animalcare and handling were carried out according to theguidelines of the World Health Organization andthe Indian National Science Academy, New Delhi.Each animal was housed in a separate polypropy-lene cage containing sterile paddy husk bedding.All the animals were closely monitored for the signsof infection during the experimental period andthose which exhibited, were eliminated from the ex-periment.
2.2 Wound inducement
Prior to wounding, the dorsal hairs (below the ribcage) of each animal were shaved using cordless elec-tric mouse clipper (Philips Electronics India Ltd.).The animals were then anesthetized by administer-ing a cock tail of Ketamine (65 mg/kg body weight)(Aneket, Neon Laboratories, India) and Diazepam(8 mg/kg body weight) (Calmpose, Ranbaxy Labora-tories, India) intraperitonially. The shaved portion ofthe skin was swabbed with sterillium solution (BodeChemie, Hamburg, Germany). The cleared dorsalsurface of the skin was marked (15 mm diameter)with a template for consistency. Under the asepticcondition, a single full thickness excision wound wasinflicted using scissors and forceps. Wounds werekept open without dressing for control as well astreatment group animals throughout the entire ex-periment. All the wounding was done by the sameperson in an effort to limit the variability in thewounding procedure.
2.3 Study design
2.3.1 Granulation tissue digestion
This experiment was carried out to digest the majorextracellular component, collagen from the granula-tion tissue using collagenase enzyme. A total 5 ani-mals were used to conduct this experiment. The ani-mals were wounded as described previously, andexposed to single exposure of laser dose (2 J/cm2)immediately following wounding. The animals weresacrificed on 15th day post-wounding, granulationtissues were harvested and stored in at �80 �C tillfurther use.
2.3.2 Study of storage effect onspectral characteristics
This experiment was conducted to study the effectof freezing (storage) over the detectable spectralchanges in the wound granulation tissues. A total of5 animals were used to conduct this experiment. Allthe animals were wounded according to the methodsexplained earlier and subsequently exposed to singleexposure of 2 J/cm2 laser dose. The animals were sa-crificed on 15th day post-wounding and granulationtissues were harvested. Spectral measurements werecarried out on the freshly excised wound granulationtissues. Subsequently, the same tissues were frozento �80 �C for ten days. Following the brief storageperiod, tissues were defrosted to room temperatureand spectral measurements were repeated again.
2.3.3 Monitoring of granulation tissuefluorescence
This experiment was conducted to observe thechanges in levels of two major tissue fluorophores,NADH and collagen by monitoring the correspond-ing fluorescence signatures from the granulation tis-sue at different post-wounding days. The NADH/collagen ratio for each experimental group was cal-culated and compared for collagen deposition duringthe healing progression. A total of 75 animals wereused for this experiment. Animals were randomlydistributed into 5 groups of 15 animals in each.Group 1-Non-illuminated control; Group 2 to 5-laserdose variants i.e., 0.5, 1, 1.5 and 2 J/cm2 respectively.Five animals from each experimental group were sa-crificed to harvest the granulation tissues on threedifferent post-irradiation time points (5th, 10th and15th days). The granulation tissues were harvestedand stored at �80 �C until further analysis.
2.3.4 Histological studiesof granulation tissues
This experiment was conducted to study the histolo-gical changes brought about by the optimum laserdose irradiation (2 J/cm2) on the progression of heal-ing at different post-wounding time points (5th, 10th
and 15th day). For this experiment, the animals weregrouped into 2 groups of 15 animals in each. A totalof 30 animals were used for this experiment. Group 1served as the non-illuminated control and the group 2served as optimum laser treatment group. The gran-
V. Prabhu et al.: Spectroscopic and histological studies on wound healing progression170
Journal of
BIOPHOTONICS
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.biophotonics-journal.org
ulation tissues from 5 animals was excised followingeuthanization on day 5, day 10 and day 15 post-wounding, and were fixed in Bouin’s fixative forfurther histological analysis.
2.4 Laser treatment procedures
The laser delivery setup for the present study wasdescribed in detail elsewhere [21–23]. Our recentreport demonstrated that the illumination source iscapable of delivering uniform power distributionover the entire wound area under study [22]. Thetreatment groups were illuminated with the singleexposures of pre-assigned He––Ne laser (power� 7 mW; power density � 4.02 mW/cm2) doses of0.5, 1, 1.5 and 2 J/cm2 by exposing them for differenttime durations (2 min 0.8 sec � 0.5 J/cm2; 4 min15 sec � 1 J/cm2; 6 min 23 sec � 1.5 J/cm2; 8 min32 sec � 2 J/cm2) immediately following wounding.The details of the source and other experimentalconditions were listed in Table 1. The laser irradia-tion was carried out after 15 min of the laser warm-up time to avoid any possible error in the laserpower stability. The laser power was monitored be-fore and after each exposure using a laser power me-
ter (Gentec, Canada) to ensure proper energy deliv-ery to the wounded site. The laser beam was carriedvia an optical fiber of core diameter 200 mm (trans-mittance �90%; Ocean Optics, USA) and coupledto a beam expander (2.5X–15X; CVI Melles Griot,USA) held at a constant distance of 20 mm abovethe wound surface (non-contact mode) providing alaser spot size of diameter 15 mm at the surface ofthe wound using a focusing lens. Before each experi-ment, it was confirmed that the laser beam wasspread out uniformly over the entire wound includ-ing the wound boundaries. Control animals were notgiven any laser treatment. Anesthesia and animalhandling procedures including wounding were simi-lar for control as well as laser treatment groups toensure observed changes in spectroscopic data andhistology could not be due to procedure differ-ences.
2.5 Spectroscope system and spectralmeasurements
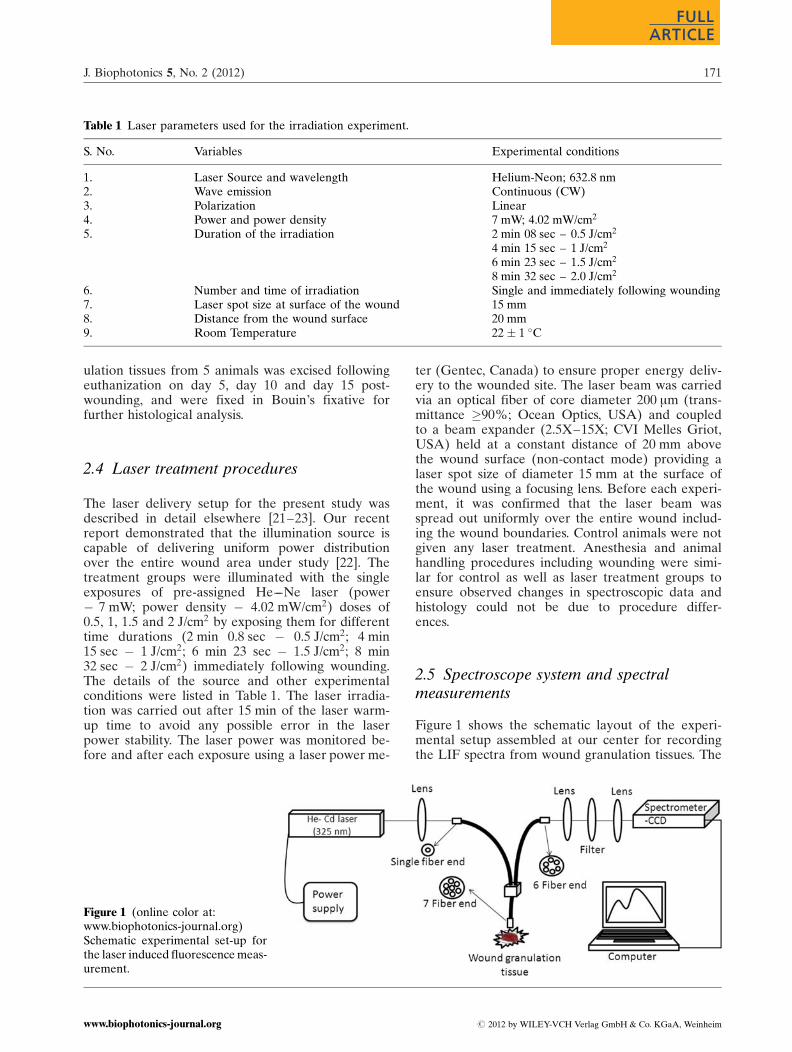
Figure 1 shows the schematic layout of the experi-mental setup assembled at our center for recordingthe LIF spectra from wound granulation tissues. The
Table 1 Laser parameters used for the irradiation experiment.
S. No. Variables Experimental conditions
1. Laser Source and wavelength Helium-Neon; 632.8 nm2. Wave emission Continuous (CW)3. Polarization Linear4. Power and power density 7 mW; 4.02 mW/cm2
5. Duration of the irradiation 2 min 08 sec – 0.5 J/cm2
4 min 15 sec – 1 J/cm2
6 min 23 sec – 1.5 J/cm2
8 min 32 sec – 2.0 J/cm2
6. Number and time of irradiation Single and immediately following wounding7. Laser spot size at surface of the wound 15 mm8. Distance from the wound surface 20 mm9. Room Temperature 22 � 1 �C
Figure 1 (online color at:www.biophotonics-journal.org)Schematic experimental set-up forthe laser induced fluorescence meas-urement.
J. Biophotonics 5, No. 2 (2012) 171
FULLFULLARTICLEARTICLE
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheimwww.biophotonics-journal.org

setup consists of a He––Cd laser (Kimmon Koha Co.,Ltd, Japan) emitting at 325 nm radiation with 8 mWstable output power, a seven fiber assembly (oneexcitation and six for fluorescence collection) ofcore diameter of 200 mm, numerical aperture 0.22having transmittance >90% (Ocean Optics, USA)and spectrometer with Hamamatsu back thinnedFFT-CCD detector (QE-65000, Ocean Optics, USA).The 325 nm laser light with spot size of 0.75 mm wascoupled to a single fiber using a 5 cm focal lengthfocusing length. The typical 7 fiber probe (centralfiber for excitation and surrounding six fibers forcollection) used in this study was fabricated and op-timized in-house in our lab. Autofluorescence signalfrom the granulation tissues under study were col-lected by the six fibers, were made to fall on an F1lens for collimation. This signal was then allowed topass through a UV cut off filter (365 nm long passfilter, Schneider Kreuznach, Germany) to block theexcitation wavelength and was further focused at theslit of the spectrograph using an F4 lens. The resul-tant spectrum was recorded using micro spectrometer(1044 � 64 pixels, detection range 200–1100 nm) andspecialized spectra suite software (Ocean Optics,USA).
It is a well-known fact that the detected signal inLIF depend greatly on the stability of the excitationsource. Thus, a stable source with constant outputpower is always desirous for a reliable device. Wehave carried out the laser power stability study as afunction of time using low power thermophile de-tector (Gentec Electro-optics, Inc., Canada). All thepower stability measurements were carried out byplacing the power meter sensor head at a distance of30 cm from the fiber end. Multiple experimentalmeasurements after 45 min of laser warming up haveshown a stable output power with only less than 2%fluctuations. Therefore, all the fluorescence measure-ments mentioned in the study were conducted after45 min of laser warm up time. The tissue sampleswere thawed to room temperature prior to fluores-cence measurement. All the fluorescence measure-ments were recorded at room temperature (22 �2 �C) within ten days of its excision. During thefluorescence measurements the tissue samples weremoistened periodically with normal saline solution,as drying of samples could lead to errors due to scat-tering [53]. The spectra were recorded from four dif-ferent sites of the wound granulation tissues andfour spectra were recorded from each measurementsite. An average spectrum of all the recorded spectrafrom a site was used for further analysis. A constantdistance of 3 mm was maintained between the tip offiber probe and the tissue surface using a transla-tional stage to avoid any influence of distance varia-tion on the tissue fluorescence pattern. All the spec-tra were recorded in the 350–700 nm spectral regionwith 10 s integration time.
2.6 Spectral measurement with Standardfluorophores
The major tissue endogenous fluorophores NADHand collagen were procured from Sigma Aldrich(Sigma Aldrich, MO, USA). 1% collagen (in aceticacid) and NADH (in 0.01 M NaOH) solutions wereprepared and the corresponding fluorescence spec-tra were recorded using 325 nm excitation from aHe––Cd laser source. The resultant spectra from purecollagen and NADH were overlapped with granula-tion tissue spectrum for comparison.
2.7 Granulation tissue digestion
Fresh 0.5% collagenase (GIBCO, Invitrogen Corpo-ration, USA) solution in phosphate buffered saline(PBS- pH-7.4) was used for granulation tissue diges-tion. Granulation tissues (15th day post-wounding)were defrosted to room temperature and soaked inthe freshly prepared collagenase solution at 37 �Cfor 24 h. Fluorescence measurements of tissue sam-ples were performed before and after the digestionexperiments.
2.8 Tissue processing and histologicalevaluation
Wound granulation tissues were collected from fif-teen animals of control and laser treatment groups,five each from day 5, 10 and 15 post-wounding re-spectively. Wound specimen with a volume equal tothe original wound size together with underlyingmuscle layers were excised and immediately fixed inBouin’s fixative. Tissues were subjected to dehydra-tion with different grades of alcohol, cleared in xy-lene and embedded in paraffin wax. Samples weresectioned into thin slices of 5 mm thickness usingLeica rotary microtome (Leica RM 2125 RT, LeicaMicrosystems, Germany). Pairs of slides underwentsubsequent staining with Hematoxylin-eosin [54],and Masson’s Trichome stain kit as per the manu-factures protocol (Trichome Stain kit, HT-15, SigmaAldrich, St. Louis, MO, USA) [55]. From each speci-men colour images were acquired using a light mi-croscope with digital camera (Motic BA 400, MoticMicrosystems, China) running under image analysisprogramme (Motic images plus 2.0, Multifunctionalmicroscopy software, China). These images fromeach animal were qualitatively assessed for sevendifferent parameters related to acute inflammatoryresponse, proliferation and remodeling: edema, leu-
V. Prabhu et al.: Spectroscopic and histological studies on wound healing progression172
Journal of
BIOPHOTONICS
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.biophotonics-journal.org

kocytes, macrophages, granulation tissue, fibroblasts,collagen deposition and epithelialization. Masson’sTrichome staining was performed specifically to mo-nitor the collagen deposition. The list of assessingparameters is given in Table 2. Each feature wassemi-quantitatively graded from 0–3 grading systembased on the histological feature as described byMcMinn [56].
2.9 Statistical analysis
In the spectroscopic measurements, 16 spectra wererecorded from each animal from 4 different sites ofa granulation tissue and averaged for further analysis.A total of 1200 spectra were recorded from 75 ani-mals. All the spectra were smoothed, base line cor-rected and normalized to their highest peak intensityusing GRAMS/AI 8.0 spectroscopy software (ThermoElectron Corporation, USA). The fluorescence ratioof NADH/collagen was calculated for individualspectrum and average of the same was representedfor respective experimental groups. The NADH/col-lagen ratios of different post-wounding days (5, 10
and 15) for non-illuminated controls and treatmentgroups were compared for the collagen depositionduring the healing progression. All the data wereexpressed as mean � SEM. For spectroscopic stud-ies, statistical significance among the experimentalgroups was determined using repeated measuresANOVA with Bonferroni’s post hoc test. For histolo-gical studies, the scores for each assessing parameterwere averaged. Comparisons of values were per-formed by the Student’s unpaired two tailed t-test.GraphPAD Prism-4 (GraphPAD software Incorpo-ration, USA) was used for the statistical analysis.Values of P < 0.05 were considered significant.
3. Results
3.1 Fluorescence of Standard fluorophores
The normalized fluorescence spectra of pure collagenand NADH along with the fluorescence spectrum ofwound granulation tissue are shown in Figure 2. Theemission maxima for pure collagen and NADH wererecorded at 405 and 455 nm respectively. The tissue
Table 2 Scoring system for histological assessment of wound healing.
Characteristic Score Features
Edema 0 No evidence1 Only present at the wound boundaries2 Present in <50% of the tissue inspected3 Present in >50% of the wound tissue inspected
Leukocytes 0 No evidence1 Mild Presence2 Moderate number of cells3 Prominent feature
Macrophages 0 No evidence1 Mild Presence2 Moderate number of cells3 Prominent feature
Granulation tissue 0 No evidence1 Occurrence at the wound margins2 Occurrence in <50% of the tissue examined3 Occurrence in >50% of the wound tissue examined
Fibroblasts 0 No indication1 Present only in the perivascular spaces2 Present in <50% of the tissue observed3 Present in >50% of the wound tissue observed
Collagen 0 No evidence1 Focal presence in fibroblast around new capillaries2 Moderate amount in the repair tissue3 Dominant feature
Epithelialization 0 No evidence1 Epidermal thickening and cell migration at wound margins2 >50% of wound epithelialized3 Epithelialization complete
J. Biophotonics 5, No. 2 (2012) 173
FULLFULLARTICLEARTICLE
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheimwww.biophotonics-journal.org
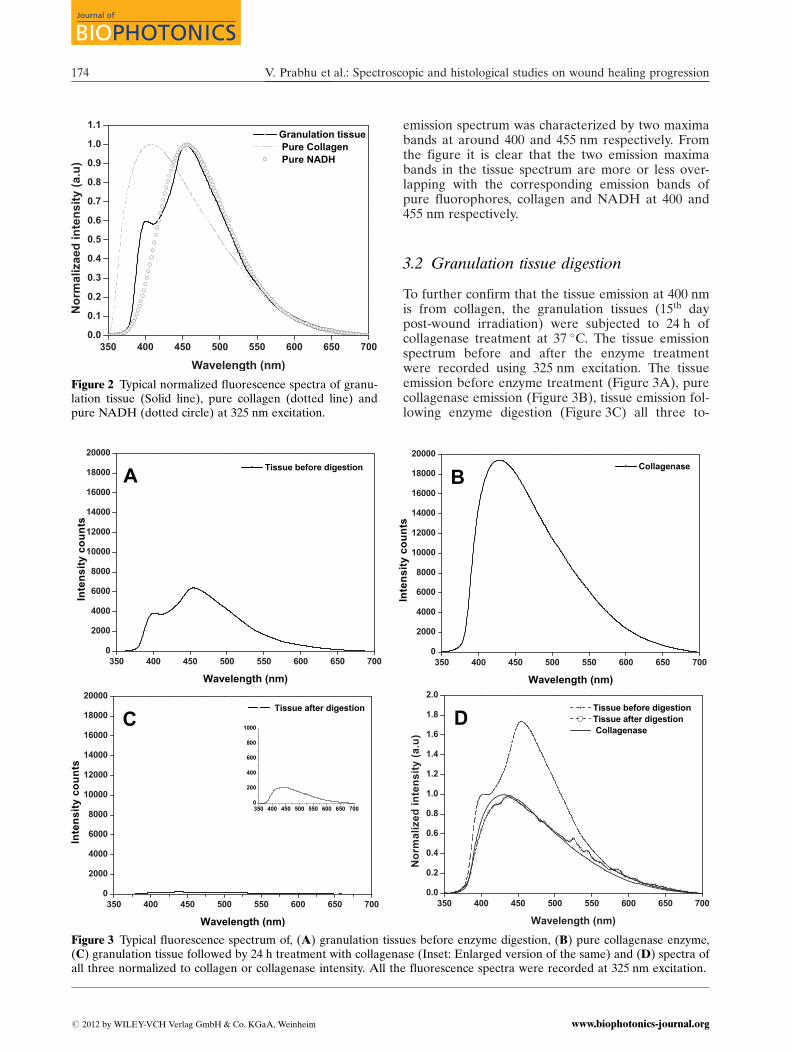
emission spectrum was characterized by two maximabands at around 400 and 455 nm respectively. Fromthe figure it is clear that the two emission maximabands in the tissue spectrum are more or less over-lapping with the corresponding emission bands ofpure fluorophores, collagen and NADH at 400 and455 nm respectively.
3.2 Granulation tissue digestion
To further confirm that the tissue emission at 400 nmis from collagen, the granulation tissues (15th daypost-wound irradiation) were subjected to 24 h ofcollagenase treatment at 37 �C. The tissue emissionspectrum before and after the enzyme treatmentwere recorded using 325 nm excitation. The tissueemission before enzyme treatment (Figure 3A), purecollagenase emission (Figure 3B), tissue emission fol-lowing enzyme digestion (Figure 3C) all three to-
Figure 2 Typical normalized fluorescence spectra of granu-lation tissue (Solid line), pure collagen (dotted line) andpure NADH (dotted circle) at 325 nm excitation.
Figure 3 Typical fluorescence spectrum of, (A) granulation tissues before enzyme digestion, (B) pure collagenase enzyme,(C) granulation tissue followed by 24 h treatment with collagenase (Inset: Enlarged version of the same) and (D) spectra ofall three normalized to collagen or collagenase intensity. All the fluorescence spectra were recorded at 325 nm excitation.
V. Prabhu et al.: Spectroscopic and histological studies on wound healing progression174
Journal of
BIOPHOTONICS
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.biophotonics-journal.org
gether normalized corresponding to their collagen/collagenase emission band (Figure 3D) are shown inFigure 3. It could be noted that, before digestion thetissue had two fluorescence maxima bands at around400 and 455 nm respectively (Figure 3A), which weredisappeared subsequently following 24 h of colla-genase treatment (Figure 3C). The pure collagenasehas shown an emission maximum approximately at430 nm (Figure 3B) which was almost overlappingwith the tissue spectrum after enzyme treatment.The main finding of this study was the disappearanceof the major tissue emission peak at 400 nm due toits digestion following collagenase treatment. Thus,this experiment further confirms that the tissue emis-sion at 400 nm is only due to collagen component ofthe tissue.
3.3 Effect of tissue storage on spectralcharacteristics
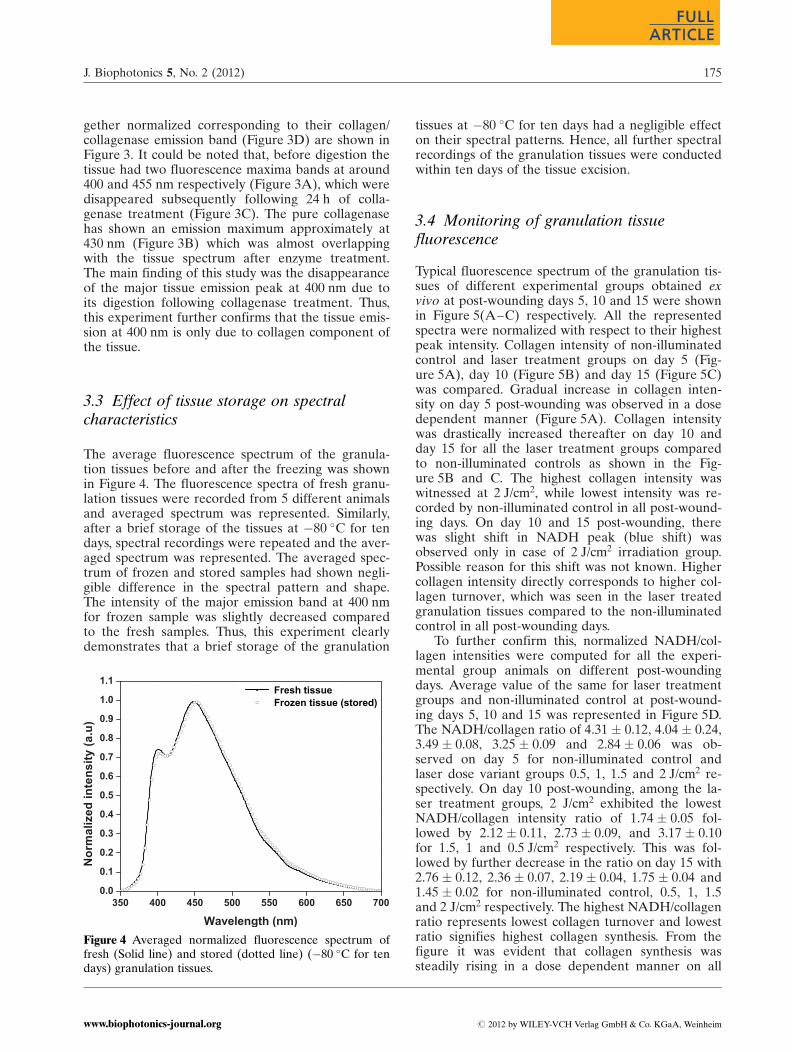
The average fluorescence spectrum of the granula-tion tissues before and after the freezing was shownin Figure 4. The fluorescence spectra of fresh granu-lation tissues were recorded from 5 different animalsand averaged spectrum was represented. Similarly,after a brief storage of the tissues at �80 �C for tendays, spectral recordings were repeated and the aver-aged spectrum was represented. The averaged spec-trum of frozen and stored samples had shown negli-gible difference in the spectral pattern and shape.The intensity of the major emission band at 400 nmfor frozen sample was slightly decreased comparedto the fresh samples. Thus, this experiment clearlydemonstrates that a brief storage of the granulation
tissues at �80 �C for ten days had a negligible effecton their spectral patterns. Hence, all further spectralrecordings of the granulation tissues were conductedwithin ten days of the tissue excision.
3.4 Monitoring of granulation tissuefluorescence
Typical fluorescence spectrum of the granulation tis-sues of different experimental groups obtained exvivo at post-wounding days 5, 10 and 15 were shownin Figure 5(A–C) respectively. All the representedspectra were normalized with respect to their highestpeak intensity. Collagen intensity of non-illuminatedcontrol and laser treatment groups on day 5 (Fig-ure 5A), day 10 (Figure 5B) and day 15 (Figure 5C)was compared. Gradual increase in collagen inten-sity on day 5 post-wounding was observed in a dosedependent manner (Figure 5A). Collagen intensitywas drastically increased thereafter on day 10 andday 15 for all the laser treatment groups comparedto non-illuminated controls as shown in the Fig-ure 5B and C. The highest collagen intensity waswitnessed at 2 J/cm2, while lowest intensity was re-corded by non-illuminated control in all post-wound-ing days. On day 10 and 15 post-wounding, therewas slight shift in NADH peak (blue shift) wasobserved only in case of 2 J/cm2 irradiation group.Possible reason for this shift was not known. Highercollagen intensity directly corresponds to higher col-lagen turnover, which was seen in the laser treatedgranulation tissues compared to the non-illuminatedcontrol in all post-wounding days.
To further confirm this, normalized NADH/col-lagen intensities were computed for all the experi-mental group animals on different post-woundingdays. Average value of the same for laser treatmentgroups and non-illuminated control at post-wound-ing days 5, 10 and 15 was represented in Figure 5D.The NADH/collagen ratio of 4.31 � 0.12, 4.04 � 0.24,3.49 � 0.08, 3.25 � 0.09 and 2.84 � 0.06 was ob-served on day 5 for non-illuminated control andlaser dose variant groups 0.5, 1, 1.5 and 2 J/cm2 re-spectively. On day 10 post-wounding, among the la-ser treatment groups, 2 J/cm2 exhibited the lowestNADH/collagen intensity ratio of 1.74 � 0.05 fol-lowed by 2.12 � 0.11, 2.73 � 0.09, and 3.17 � 0.10for 1.5, 1 and 0.5 J/cm2 respectively. This was fol-lowed by further decrease in the ratio on day 15 with2.76 � 0.12, 2.36 � 0.07, 2.19 � 0.04, 1.75 � 0.04 and1.45 � 0.02 for non-illuminated control, 0.5, 1, 1.5and 2 J/cm2 respectively. The highest NADH/collagenratio represents lowest collagen turnover and lowestratio signifies highest collagen synthesis. From thefigure it was evident that collagen synthesis wassteadily rising in a dose dependent manner on all
Figure 4 Averaged normalized fluorescence spectrum offresh (Solid line) and stored (dotted line) (�80 �C for tendays) granulation tissues.
J. Biophotonics 5, No. 2 (2012) 175
FULLFULLARTICLEARTICLE
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheimwww.biophotonics-journal.org
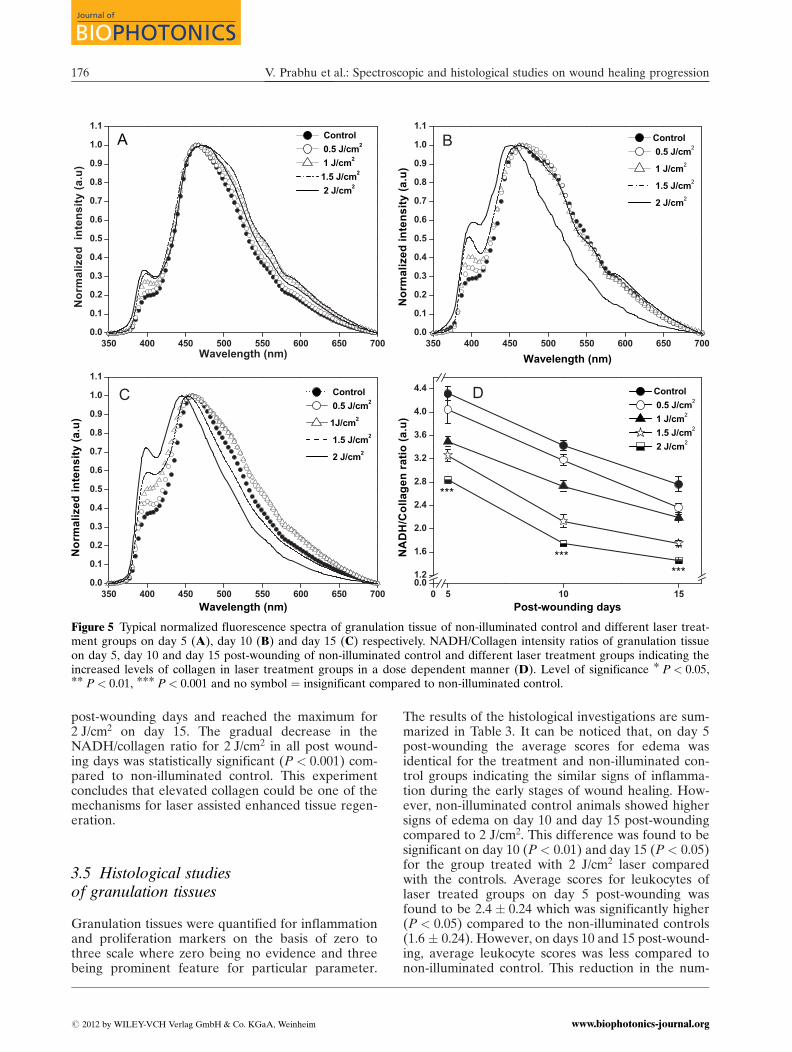
post-wounding days and reached the maximum for2 J/cm2 on day 15. The gradual decrease in theNADH/collagen ratio for 2 J/cm2 in all post wound-ing days was statistically significant (P < 0.001) com-pared to non-illuminated control. This experimentconcludes that elevated collagen could be one of themechanisms for laser assisted enhanced tissue regen-eration.
3.5 Histological studiesof granulation tissues
Granulation tissues were quantified for inflammationand proliferation markers on the basis of zero tothree scale where zero being no evidence and threebeing prominent feature for particular parameter.
The results of the histological investigations are sum-marized in Table 3. It can be noticed that, on day 5post-wounding the average scores for edema wasidentical for the treatment and non-illuminated con-trol groups indicating the similar signs of inflamma-tion during the early stages of wound healing. How-ever, non-illuminated control animals showed highersigns of edema on day 10 and day 15 post-woundingcompared to 2 J/cm2. This difference was found to besignificant on day 10 (P < 0.01) and day 15 (P < 0.05)for the group treated with 2 J/cm2 laser comparedwith the controls. Average scores for leukocytes oflaser treated groups on day 5 post-wounding wasfound to be 2.4 � 0.24 which was significantly higher(P < 0.05) compared to the non-illuminated controls(1.6 � 0.24). However, on days 10 and 15 post-wound-ing, average leukocyte scores was less compared tonon-illuminated control. This reduction in the num-
Figure 5 Typical normalized fluorescence spectra of granulation tissue of non-illuminated control and different laser treat-ment groups on day 5 (A), day 10 (B) and day 15 (C) respectively. NADH/Collagen intensity ratios of granulation tissueon day 5, day 10 and day 15 post-wounding of non-illuminated control and different laser treatment groups indicating theincreased levels of collagen in laser treatment groups in a dose dependent manner (D). Level of significance * P < 0.05,** P < 0.01, *** P < 0.001 and no symbol ¼ insignificant compared to non-illuminated control.
V. Prabhu et al.: Spectroscopic and histological studies on wound healing progression176
Journal of
BIOPHOTONICS
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.biophotonics-journal.org
ber of leukocytes for the laser treated groups wasfound to be significant on day 10 (P < 0.001) andday 15 (P < 0.01) post-wounding respectively. Withregard to macrophages, a reduction in the averagescores on day 5 and 10 post-wounding was noticedwhen compared with the control groups. It can alsobe noticed that on day 15 post-wounding, averagescores for macrophages for non-illuminated controland laser treatment groups were similar. There wasno statistically significant difference observed in themacrophage numbers among the control and lasertreatment groups on all the post-wounding days.
The animals subjected to optimal laser treatmentdose, healthy granulation tissues were observed inthem on all the post-wounding days compared to thenon-illuminated controls. The presence of healthy
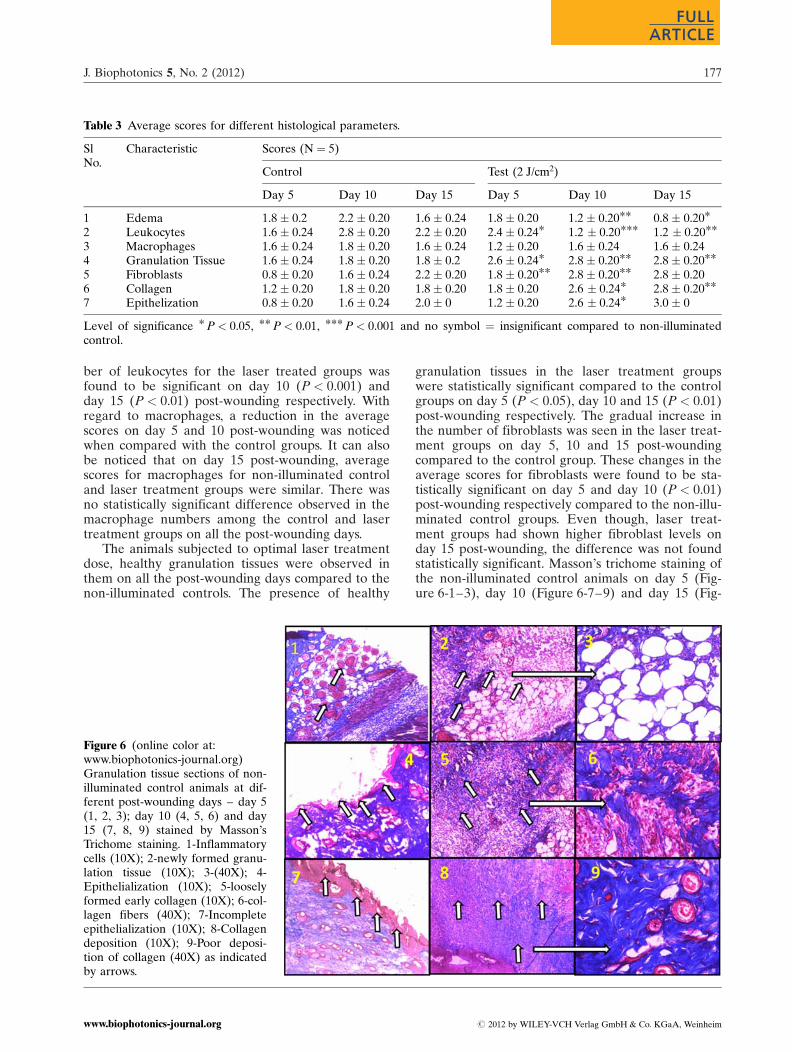
granulation tissues in the laser treatment groupswere statistically significant compared to the controlgroups on day 5 (P < 0.05), day 10 and 15 (P < 0.01)post-wounding respectively. The gradual increase inthe number of fibroblasts was seen in the laser treat-ment groups on day 5, 10 and 15 post-woundingcompared to the control group. These changes in theaverage scores for fibroblasts were found to be sta-tistically significant on day 5 and day 10 (P < 0.01)post-wounding respectively compared to the non-illu-minated control groups. Even though, laser treat-ment groups had shown higher fibroblast levels onday 15 post-wounding, the difference was not foundstatistically significant. Masson’s trichome staining ofthe non-illuminated control animals on day 5 (Fig-ure 6-1–3), day 10 (Figure 6-7–9) and day 15 (Fig-
Table 3 Average scores for different histological parameters.
SlNo.
Characteristic Scores (N ¼ 5)
Control Test (2 J/cm2)
Day 5 Day 10 Day 15 Day 5 Day 10 Day 15
1 Edema 1.8 � 0.2 2.2 � 0.20 1.6 � 0.24 1.8 � 0.20 1.2 � 0.20** 0.8 � 0.20*
2 Leukocytes 1.6 � 0.24 2.8 � 0.20 2.2 � 0.20 2.4 � 0.24* 1.2 � 0.20*** 1.2 � 0.20**
3 Macrophages 1.6 � 0.24 1.8 � 0.20 1.6 � 0.24 1.2 � 0.20 1.6 � 0.24 1.6 � 0.244 Granulation Tissue 1.6 � 0.24 1.8 � 0.20 1.8 � 0.2 2.6 � 0.24* 2.8 � 0.20** 2.8 � 0.20**
5 Fibroblasts 0.8 � 0.20 1.6 � 0.24 2.2 � 0.20 1.8 � 0.20** 2.8 � 0.20** 2.8 � 0.206 Collagen 1.2 � 0.20 1.8 � 0.20 1.8 � 0.20 1.8 � 0.20 2.6 � 0.24* 2.8 � 0.20**
7 Epithelization 0.8 � 0.20 1.6 � 0.24 2.0 � 0 1.2 � 0.20 2.6 � 0.24* 3.0 � 0
Level of significance * P < 0.05, ** P < 0.01, *** P < 0.001 and no symbol ¼ insignificant compared to non-illuminatedcontrol.
Figure 6 (online color at:www.biophotonics-journal.org)Granulation tissue sections of non-illuminated control animals at dif-ferent post-wounding days – day 5(1, 2, 3); day 10 (4, 5, 6) and day15 (7, 8, 9) stained by Masson’sTrichome staining. 1-Inflammatorycells (10X); 2-newly formed granu-lation tissue (10X); 3-(40X); 4-Epithelialization (10X); 5-looselyformed early collagen (10X); 6-col-lagen fibers (40X); 7-Incompleteepithelialization (10X); 8-Collagendeposition (10X); 9-Poor deposi-tion of collagen (40X) as indicatedby arrows.
J. Biophotonics 5, No. 2 (2012) 177
FULLFULLARTICLEARTICLE
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheimwww.biophotonics-journal.org
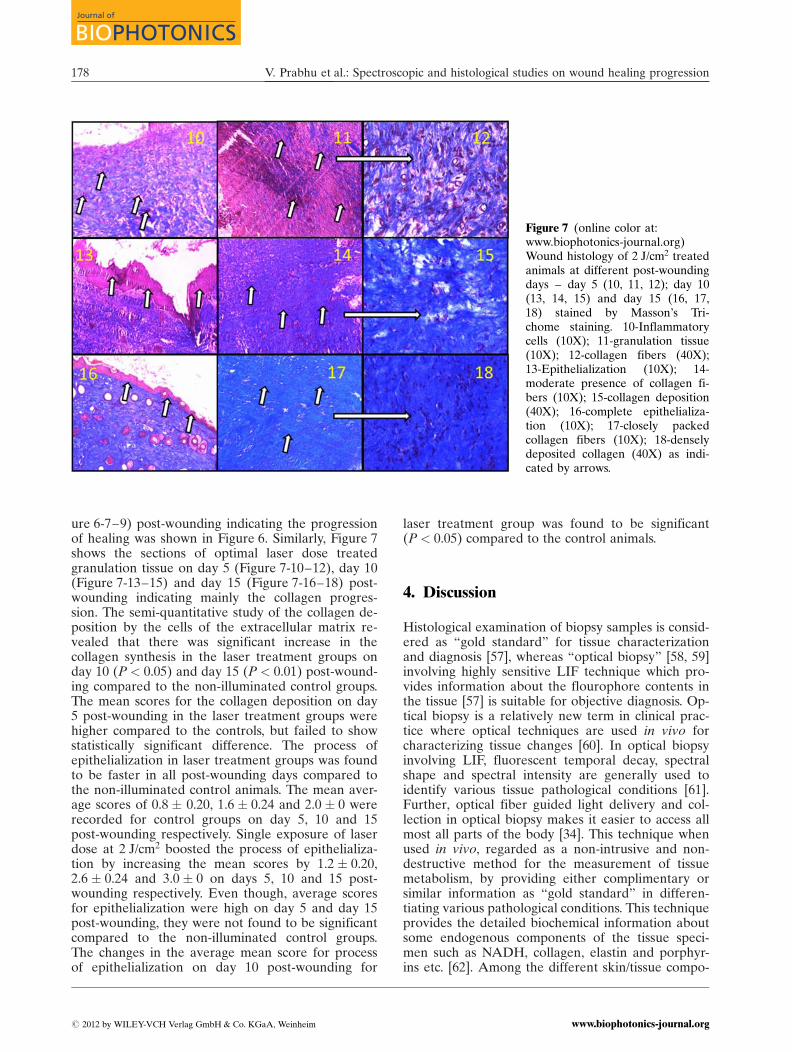
ure 6-7–9) post-wounding indicating the progressionof healing was shown in Figure 6. Similarly, Figure 7shows the sections of optimal laser dose treatedgranulation tissue on day 5 (Figure 7-10–12), day 10(Figure 7-13–15) and day 15 (Figure 7-16–18) post-wounding indicating mainly the collagen progres-sion. The semi-quantitative study of the collagen de-position by the cells of the extracellular matrix re-vealed that there was significant increase in thecollagen synthesis in the laser treatment groups onday 10 (P < 0.05) and day 15 (P < 0.01) post-wound-ing compared to the non-illuminated control groups.The mean scores for the collagen deposition on day5 post-wounding in the laser treatment groups werehigher compared to the controls, but failed to showstatistically significant difference. The process ofepithelialization in laser treatment groups was foundto be faster in all post-wounding days compared tothe non-illuminated control animals. The mean aver-age scores of 0.8 � 0.20, 1.6 � 0.24 and 2.0 � 0 wererecorded for control groups on day 5, 10 and 15post-wounding respectively. Single exposure of laserdose at 2 J/cm2 boosted the process of epithelializa-tion by increasing the mean scores by 1.2 � 0.20,2.6 � 0.24 and 3.0 � 0 on days 5, 10 and 15 post-wounding respectively. Even though, average scoresfor epithelialization were high on day 5 and day 15post-wounding, they were not found to be significantcompared to the non-illuminated control groups.The changes in the average mean score for processof epithelialization on day 10 post-wounding for
laser treatment group was found to be significant(P < 0.05) compared to the control animals.
4. Discussion
Histological examination of biopsy samples is consid-ered as “gold standard” for tissue characterizationand diagnosis [57], whereas “optical biopsy” [58, 59]involving highly sensitive LIF technique which pro-vides information about the flourophore contents inthe tissue [57] is suitable for objective diagnosis. Op-tical biopsy is a relatively new term in clinical prac-tice where optical techniques are used in vivo forcharacterizing tissue changes [60]. In optical biopsyinvolving LIF, fluorescent temporal decay, spectralshape and spectral intensity are generally used toidentify various tissue pathological conditions [61].Further, optical fiber guided light delivery and col-lection in optical biopsy makes it easier to access allmost all parts of the body [34]. This technique whenused in vivo, regarded as a non-intrusive and non-destructive method for the measurement of tissuemetabolism, by providing either complimentary orsimilar information as “gold standard” in differen-tiating various pathological conditions. This techniqueprovides the detailed biochemical information aboutsome endogenous components of the tissue speci-men such as NADH, collagen, elastin and porphyr-ins etc. [62]. Among the different skin/tissue compo-
Figure 7 (online color at:www.biophotonics-journal.org)Wound histology of 2 J/cm2 treatedanimals at different post-woundingdays – day 5 (10, 11, 12); day 10(13, 14, 15) and day 15 (16, 17,18) stained by Masson’s Tri-chome staining. 10-Inflammatorycells (10X); 11-granulation tissue(10X); 12-collagen fibers (40X);13-Epithelialization (10X); 14-moderate presence of collagen fi-bers (10X); 15-collagen deposition(40X); 16-complete epithelializa-tion (10X); 17-closely packedcollagen fibers (10X); 18-denselydeposited collagen (40X) as indi-cated by arrows.
V. Prabhu et al.: Spectroscopic and histological studies on wound healing progression178
Journal of
BIOPHOTONICS
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.biophotonics-journal.org
nents, collagen is the most studied flourophore [63].Various attempts have also been made to evaluatethe collagen deposition in the histological sections ofthe diabetic and acute wound tissues to monitor theprogression of healing following LLLT [31, 52]. Inaddition to the report of collagen deposition in tis-sues using LIF, histological examinations are alsoused to provide the information related to inflama-tory response, proliferation and remodeling duringwound healing [64]. Based on these reports, in thepresent study we have utilized the information pro-vided by these two techniques-LIF (optical biopsy)and tissue histology (gold standard) for collagen de-position in monitoring the succession of acute woundhealing in laser treated Swiss albino mice.
Traditionally mice, rats, pigs, chicken and rabbitsare the best studied animal models for studying laserinduced fluorescence in relation to tumor develop-ment or wound healing [65]. The studies on animalmodels using LIF can provide the information re-lated to the biochemical changes that take place dur-ing the disease progression or an outcome of thetherapeutic intervention as reflected by the spectralintensity and shape. Moreover, there are reports inthe literature showing main fluorophores in humanand animal skin are almost similar and variations inthem could be expected in terms of change in con-centration and content of the specific flourophoresuch as collagen [34]. Different light sources rangingfrom ultra violet to blue green spectral region suchas Nitrogen laser (337.1 nm), Helium-cadmium laser(325 and 442 nm) and Argon-ion laser (488 and514 nm) were commonly reported as an excitationsource for the autofluorescence studies in skin tissues[34, 66]. Among them, wavelength around 340 nm iswidely used as excitation source for studying auto-fluorescence [34]. Hence, in the present study325 nm laser light from a He––Cd source was usedas an excitation for investigating autofluorescenceproperties of the wound granulation tissues follow-ing LLLT in Swiss albino mice.
To identify different peaks in the autofluores-cence spectra of the granulation tissues, the normal-ized spectra of the pure collagen and NADH wereoverlapped with the granulation tissue mean normal-ized spectra. The granulation tissue spectra haveshown two prominent peaks at around 400 nm and455 nm at 325 nm excitation whereas pure collagenand NADH have shown broad bands with peaks at405 nm and 455 nm respectively. Based on these ob-servations, the two major emission bands in theautofluorescence spectra of the granulation tissueswere assigned to collagen and NADH respectively.Moreover, available literatures in this area have alsoindicated that the structural protein collagen hasemission maxima at around 405 nm and co-enzymeNADH at around 455 nm [42, 67]. Hence in the pre-sent study, tissue emission bands at around 400 nm
and 455 nm could be due to the collagen and NADHemission respectively. To further confirm these un-derstanding, granulation tissues were subjected tothe collagenase digestion for 24 h at 37 �C. For thisexperiment, collagenase from the bacterial origin(Clostridium histolyticum) representing unique classof metalloproteases, were utilized to hydrolyze thecollagen chains [68, 69]. These bacterial collagenasesare known to be versatile, due to their capacity todegrade both water soluble and insoluble collagensas well as capable of acting on almost all types ofcollagens [70]. The collagen emission band around400 nm was completely disappeared following theenzymatic digestion. In addition, normalized spectraof the collagenase digested tissue have shown a veryweak band at around 430 nm overlapping with thepure collagenase emission. This observation, furtherconfirms that the granulation tissue emission peak ataround 400 nm is solely due to the collagen compo-nent of the tissue. Further, collagenase digested tis-sue spectrum even failed to show NADH band ataround 455 nm. This could be due to the interactionof phosphate and its reduced form leading to an ad-duct formation across the pyridine group resulting inthe cofactor decomposition as explained by Alivisa-tos et al. [71]. It is also known that NADH is verysensitive and is highly unstable to change in tem-perature, pH and storage conditions. In another hy-pothesis [71], it is indicated that the interaction ofphosphate with the NADH through charge trans-ferase complex could also catalyze the NADH de-composition. Laercio Rover Jr. et al. [72] have alsoshown a diminished absorption of NADH at 340 nmsuggesting it as an indicative measure of co-factordecomposition. Thus, disappearance of the NADHemission band following tissue digestion could bedue to the decomposition of the cofactor at 37 �Cand interaction with the phosphate moiety.
It is assumed that the laboratory conditions, suchas storage and handling processes could influencethe tissue autofluorescence signals. Very few studieshave been performed to show changes in the spec-tral pattern with respect to the sample storage andhanding protocols [34, 73]. Therefore, in the presentstudy, we aspired to investigate the influence offreezing on the autofluorescence signal of the granu-lation tissues. Average autofluorescence spectra ofthe fresh and frozen samples exhibited negligiblechanges in the spectral pattern. The normalized aver-aged fluorescence spectra of frozen sample hadshown a slight decrease in the collagen intensitycompared to the fresh samples. Ming G. Xu and hisassociates [73] have also observed negligible changesin the autofluorescence properties of mice skeletalmuscles when stored at �20 �C for four days in water.However, it is also reported that mouse spectral pat-tern especially NADH varied significantly when tis-sues left in water for more than four days, which is
J. Biophotonics 5, No. 2 (2012) 179
FULLFULLARTICLEARTICLE
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheimwww.biophotonics-journal.org
attributed to the degradation of the tissue in aque-ous non fixing conditions. In another study [34], nosignificance influence of freezing was detected onthe spectral pattern of pig and chicken skin samplesstored for one week. Similarly our finding suggeststhat, brief storage of the granulation tissue at �80 �Cfor ten days had minimal effects on the autofluores-cence pattern of the endogenous fluorophores.
Collagens are believed to be the key componentof the connective tissue, representing nearly 80–85%of the extracellular matrix (ECM) in the dermallayer of the normal skin tissue [28] and forms onethird of the vertebrates total proteins [74]. Till date,as many as 28 different types of collagens consistingof 46 distinct polypeptide chains were characterizedin vertebrates [75]. These collagens are broadly clas-sified into fibrillar (Types I, II, III, V and IX) andnon-fibrillar collagens. The three major fibrillar col-lagens (Type I, II and III) account for 70–80% ofthe total collagen in the human body [76]. Type Icollagen mostly found in the bone, tendon and liga-ment tissues are prone to high mechanical forces,while type III collagen predominant in the woundgranuloma tissues providing elastic properties, play avital role in wound healing. Keloids and hypertrophicscars are the result of disorganized collagen synthesisand degradation during wound healing leading tothe formation of aesthetically and functionally un-acceptable collagen fibers [77]. Thus it is essential toperiodically monitor the changes in the collagensynthesis during wound healing to avoid such clinicalcomplications. Previous work from our group [23]has demonstrated the photobiomodulatory effects ofHe––Ne laser at 2 J/cm2 via increased collagen syn-thesis compared to the other tested laser doses andnon-illuminated controls. In that study it has beenobserved that laser doses above 2 J/cm2 diminishesthe collagen production as evidenced by the biochem-ical measurements of hydroxyproline. Collagens arealso known for their fluorescent emission property,which has been extensively utilized for their trackingduring various pathological conditions [78]. It hasbeen proved that lysyl pyridinoline (LP) and hy-droxylysyl pyridinoline (HP), are the components re-sponsible for the collagen fluorescence in the UVregion. These two autofluorescent components havethe excitation maxima at 325 nm and emission max-ima at 400 nm [79, 80]. To further corroborate ourearlier findings on collagen synthesis, an attempt wasmade to compare the information provided by twooptical techniques-LIF and light microscopy. TheLIF studies have provided the information mainlyon the collagen levels in the tissue, whereas histolo-gical examinations (light microscopy) have providedthe structural information related to different stagesof wound healing following LLLT.
In the present study, the selection of laser dosesfor studying fluorescence were based on our previous
work, where single exposure of various laser doses(0.5, 1, 1.5 and 2 J/cm2), less than optimal laser dose(2 J/cm2) were only tested to monitor the spectro-scopic changes during the healing. Spectral analysisof granulation tissue spectra indicated the dose de-pendent increase in the collagen levels from 0.5 J/cm2
to 2 J/cm2 in all post-wounding days. Exact cause forBlue shift of the NADH peak in the optimum laserdose treated animals on day 10 and day 15 post-wounding was still unclear. Further studies in this di-rection may be helpful in understanding the reasonbehind this shift. The non-illuminated control groupdisplayed 1.50, 1.97 and 1.90 fold increase in theNADH/collagen ratio compared to the optimum la-ser treated groups on days 5, 10 and 15 post-wound-ing respectively. This raise in the NADH/collagenclearly reflects the decreased collagen levels in thecontrol groups compared to the optimum laser treat-ment group. Extensive LIF studies have been re-ported previously involving NADH and collagen fordiagnosis of various cancers [36, 81]. However, avery little information is known at present aboutthe applicability of fluorescence spectroscopy in themonitoring of wound healing progression [32, 82].J. Tang et al. [83], T. K. Gayen et al. [84], and A. Ali-mova and co-workers [85] have utilized Raman spec-troscopy or native fluorescence imaging to monitorcollagen deposition in tissues.
Luo and co-workers [32] have used the novel sec-ond harmonic generation (SHG) microscopy for thechanges of the collagen arrangement at the woundmargin at different post-wounding days. They havedemonstrated the potential of SHG microscopy as anon-invasive imaging tool for the analysis of collagenorganization during healing. Similarly, Morky [82]and co-workers have reported the application of fluo-rescence spectroscopy to monitor the early changesin wound healing progression by measuring corre-sponding FAD/NADH ratio till first three days ofpost-surgery in rats. They have also observed in-creased FAD/NADH ratios till 72 h following sur-gery, due to the neoangiogenesis and better bloodcirculation. Similarly, J. Tang et al. [83], T. K. Gayenand co-workers [84] assessed the efficacy of lasertissue welding (LTW) by monitoring native collagenfluorescence imaging. Likewise, A. Alimova et al.[85] evaluated the wound healing progression mainlyby collagen deposition using Raman spectroscopyand by histopathology in surgically sutured woundand LTW wounds in guinea pig. The studies con-ducted on animal models have revealed an increasedNADH levels during the early phase of epidermalwound healing [86]. It has been stated that due tohigh rate of energy metabolism, NADH is utilizedby lactate dehydrogenase (LDH) during cell migra-tion and proliferation and a-Glycerophosphate de-hydrogenase (GOPDH) during cell maturation [86].Thus this could also be one of the reasons for the
V. Prabhu et al.: Spectroscopic and histological studies on wound healing progression180
Journal of
BIOPHOTONICS
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.biophotonics-journal.org

observed decrease in the NADH/collagen ratio asthe wound healing progresses. We present the usageof two different lasers (He––Ne and He––Cd) andtwo different approaches (LLLT and LIF) first timefor the enhanced tissue regeneration and monitoringof healing in an animal model. Increased collagensynthesis recorded by LIF measurement in the opti-mal laser dose treated animals in all post-woundingdays are in agreement with our previously reportedwork [23]. The findings of the present study clearlyindicate that the LIF has enough potential in evalu-ating biochemical changes in tissue and it could beused to monitor collagen levels during differentstages of wound healing.
In the current study histological examinations ofthe granulation tissues at different stages of thewound healing were performed only for the optimallaser dose treated animals. It has been well provedthat the histological examinations provide the cleardescription of each stage of healing, thus utilizationof this technique to evaluate the efficacy of LLLTwill be more appropriate. In the present study histo-logical examination were carried out for seven differ-ent parameters related to inflammation and repair.Edema, Leukocytes, and macrophages are consideredas the key players of the inflamatory stage, While,granulation tissue, collagen, fibroblast and epithelia-lization provides information about proliferation. Ir-radiation of optimum laser dose (2 J/cm2) has con-siderably reduced edema on days 10 and 15 post-wounding compared to the non-illuminated control.Similarly, presence of leukocytes also significantlydecreased in optimal laser treated animals from day 5to 15. However, macrophages levels were found tobe much similar to the non-illuminated control ani-mals. Our current findings were in agreement withthe study conducted by Rabelo et al. [50], in whichHe––Ne laser irradiation was found to reduce theinflamatory cells in the laser treated diabetic andnon-diabetic rats. In another study, irradiation with670 nm laser light drastically reduced the number ofleukocytes on day 7 and 14 of post-wounding com-pared to the non-illuminated control animals [51]. Aseparate study conducted by Pugliese and his co-workers [13] demonstrated that, laser irradiation at4 J/cm2 could drastically decline the edema and infla-matory infiltrate thus enhance the healing process inWistar rats. Thus, based on these reports our hypoth-esis states that laser induced enhanced wound heal-ing could be by controlling the inflamatory phase, byreducing edema and disappearance of leukocytes.
Healthy granulation tissue is the sign of betterhealing. Average scores for the granulation tissue re-vealed that single exposure of optimum laser doseimmediately following wounding markedly increasedthe formation of healthy granulation tissue com-pared to non-illuminated control in all post-wound-ing days. Similarly, the laser treatment had signifi-
cant effect in increasing the number of fibroblast onpost-wounding days 5 and 10 compared to non-illu-minated control. Although, optimum laser dose irra-diation induced higher collagen deposition on day 5post-wounding, it was not significant compared tothe control group animals. Mean scores for collagenwas significantly higher in laser treatment groups onsubsequent post-wounding days indicating the laserassisted enhanced tissue regeneration. Likewise, asignificant change in the epithelialization was ob-served in the optimal laser treated animals only onday 10 post-wounding. Although, mean scores forepithelialization was higher in case of optimal laserdose treated animals on day 5 and 15, they were notfound to be significant.
It has been well established that fibroblast play acritical role in proliferation stage of wound healing.It is also reported that fibroblast are the essential forepithelialization, granulation tissue formation andcollagen synthesis [87]. In rabbits, higher number offibroblast proliferation was reported following laserirradiation in early stages of wound healing [88].Similarly, Carvalho and his co-workers [89] demon-strated the influence of He––Ne laser in acceleratedgranulation tissue formation and fibroblast activityin diabetic and non- diabetic rats. In another studywith 670 nm laser irradiation has reported enhancedcollagen and elastin fiber deposition as evidenced bythe histological observations during the early phasesof wound healing in Wistar rats [13]. Goez-Villaman-dos and his co-workers [90] have evidenced the en-hanced wound healing under the influence of laserradiation via increased fibroblast number, and synth-esis of collagen. It has also been reported that LLLTcould accelerate the process of epithelialization com-pared to non-illuminated counter parts [29]. Ourfindings in corroboration with other studies [31, 91,92], have clearly demonstrated the efficacy of LLLTin accelerated healing through fibroblast activity andcollagen synthesis. Also, based on the histologicalfindings of the current study it could be stated thatHe- Ne laser plays a vital role in fibroblast activity,modulating the whole process of wound healing.
Average histological scores of collagen depositionfor optimum laser dose treated animals indicatedthat there was 1.50, 1.44 and 1.55 fold increase onday 5, day 10 and day 15 post-wounding comparedto non-illuminated control. Similarly, spectroscopicexamination of the optimum laser dose treated gran-ulation tissues showed 1.44, 1.92 and 1.62 fold in-creases in collagen intensity compared to the con-trols. The findings of the present study have clearlyindicated that these two techniques are highly com-parable in monitoring collagen deposition during dif-ferent stages of wound healing. Furthermore, it isalso demonstrated that, spectroscopic measurementsare highly sensitive to minute changes in collagenlevels compared to the histological examinations as
J. Biophotonics 5, No. 2 (2012) 181
FULLFULLARTICLEARTICLE
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheimwww.biophotonics-journal.org

shown by fold increase in collagen on day 10 andday 15 post-wounding. Thus, LIF technique could beused as a promising tool to monitor collagen changesin wound granulation tissues in addition to the com-monly used biochemical and histological examina-tions for objective evaluation.
5. Conclusions
In summary, first time the LIF technique has beenutilized to evaluate tissue regeneration on acutewound healing in Swiss albino mice following LLLT.The LIF studies have demonstrated a dose depen-dent increase in the collagen synthesis up to the op-timal dose of tissue regeneration. The histologicalfindings have shown that He-Ne laser at the optimaldose, reduced the inflamatory signs, increased the fi-broblast number, granulation tissue formation, col-lagen synthesis and epithelialization, and thus mo-dulating each stage of wound healing. However, theLIF technique is specifically found to be more sen-sitive with respect to the evaluation of collagenchanges compared to the histological examinations.Therefore, it is suggested that in vivo LIF studies onpre-clinical models would certainly be of ample helpin exploiting this technique in clinical conditions formonitoring the progression of wound healing.
Acknowledgements The patronage of DRDO – GOI(Grant No. DLS/81/48222/LSRB-164/BDB/2008, 2008–2011), TIFAC-CORE (Pharmacogenomics) Manipal LifeSciences Centre, Manipal University and VGST, Karnata-ka State, Karnataka is gratefully acknowledged. The authorsare grateful to Mr. Sadanand, Department of Pathology,KMC, Manipal University for his help during the histolo-gical studies.
Vijendra Prabhu is presently pursuing his Ph.D. degreeon “Development and evaluation of fiber optic probebased Helium–Neon (He––Ne) laser radiation systemfor tissue regeneration-in vivo and in vitro studies” atBiophysics Unit, Manipal University, Manipal, after ob-taining his Master’s degree in Biotechnology from St.Aloysius College, Mangalore, India. His research inter-ests include, Low level laser therapy for tissue regen-eration on in vivo and in vitro models, Development oflaser based instrumentation for various applications inbiology and medicine.
B. S. Satish Rao is currently working as Professor andHead of Division of Radiobiology and Toxicology atManipal Life Sciences Centre, Manipal University, In-dia. He has published more than 80 full research ar-ticles in peer reviewed international journals in the
areas of toxicology, radiation biology and oncology. Hiscurrent research activities include radiation biology,experimental oncology and therapeutics, environmen-tal toxicology and wound healing using in vivo and invitro models.
Subhash Chandra is a Junior Engineer at BiophysicsUnit, Manipal Life Sciences Centre, Manipal Univer-sity. He received his Diploma in Electronics and Com-munications Engineering in 2008. His research interestsinclude developing fiber optic probe for spectroscopicand photoacoustic spectroscopic applications in diseasediagnostics.
Pramod Kumar is Professor and Head of Departmentof Plastic Surgery and Burns at Kasturba Medical Col-lage, Manipal, India. He received his Master’s degreein Surgery in 1985 and M.Ch. degree in Plastic Surgeryin 1988. He has published more than 120 scientific pa-pers and authored 2 books. His present research areaof interest includes limited access dressing (LAD) ondiabetic and burn wounds, low level laser therapy forchronic non-healing wounds.
Lakshmi Rao is Professor and Head of Department ofPathology, Kasturba Medical College, Manipal, India.She received her M.B.B.S degree in 1980 from MadrasUniversity and MD in Pathology from Mangalore Uni-versity in 1983. She has published several full researcharticles and review papers in well reputed internationaljournals.
K. Satyamoorthy is presently Professor of Biotechnol-ogy at Manipal Life Sciences Centre, Manipal Univer-sity, India. He has published more than 110 full researcharticles including reviews in journals of repute in theareas of molecular and cellular biology. His current re-search activities include epigenetic mechanisms, phar-macogenomic studies for human diseases, human popu-lation variations and diabetes.
Vasudeva Guddattu is working as a Lecturer at Depart-ment of Statistics, Manipal University, Manipal, Indiasince 2007. His areas of interest include categoricaldata analysis, secondary data analysis, multilevel mod-eling and longitudinal data analysis. He has more than12 publications in reputed national and internationaljournals. He has been resource person for many of sta-tistical workshop conducted in Manipal University andother institutions. Currently he is perusing his Ph.D. inthe area of zero inflated count models under supervi-sion of Dr. K. Aruna Rao from Mangalore University.
V. Prabhu et al.: Spectroscopic and histological studies on wound healing progression182
Journal of
BIOPHOTONICS
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.biophotonics-journal.org

References
[1] J. L. Monaco and W. T. Lawrence, Clin. Plast. Surg.30, 1–12 (2003).
[2] A. C. Gloria, F. D. Robert, and S. S. Gregory, WoundHealing (Taylor and Francis, Florida, 2005), p. 3.
[3] R. V. Goncalves, R. D. Novaes, S. L. Matta, G. P.Benevides, F. R. Faria, and M. V. Pinto, Photomed.Laser Surg. 28, 597–602 (2010).
[4] A. P. De Sousa, J. N. Santos, J. A. Dos Reis, Jr., T. A.Ramos, J. De Souza, M. C. Cangussu, and A. L. Pin-heiro, Photomed. Laser Surg. 28, 547–552 (2010).
[5] T. Toporcer and J. Radonak, Cas. Lek. Cesk. 145,702–707 (2006).
[6] J. Milgram, R. Shahar, T. Levin-Harrus, and P. Kass,Bioelectromagnetics 25, 271–277 (2004).
[7] M. A. Dall Agnol, R. A. Nicolau, C. J. De Lima, andE. Munin, Lasers Med. Sci. 24, 909–916 (2009).
[8] S. M. Rodrigo, A. Cunha, D. H. Pozza, D. S. Blaya,J. F. Moraes, J. B. Weber, and M. G. De Oliveira,Photomed. Laser Surg. 27, 929–935 (2009).
[9] A. M. Fulop, S. Dhimmer, J. R. Deluca, D. D. Johan-son, R. V. Lenz, K. B. Patel, P. C. Douris, and C. S. En-wemeka, Photomed. Laser Surg. 27, 695–702 (2009).
[10] A. V. Corazza, J. Jorge, C. Kurachi, and V. S. Bagnato,Photomed. Laser Surg. 25, 102–106 (2007).
[11] E. Mester, A. F. Mester, and A. Mester, Lasers Surg.Med. 5, 31–39 (1985).
[12] W. Posten, D. A. Wrone, J. S. Dover, K. A. Arndt,S. Silapunt, and M. Alam, Dermatol. Surg. 31, 334–340 (2005).
[13] L. S. Pugliese, A. P. Medrado, S. R. Reis, and A. An-drade Zde, Pesqui Odontol Bras. 17, 307–313 (2003).
[14] L. Wilden and R. Karthein, J. Clin. Laser Med. Surg.16, 159–165 (1998).
[15] M. Greco, R. A. Vacca, L. Moro, E. Perlino, V. A.Petragallo, E. Marra, and S. Passarella, Lasers Surg.Med. 29, 433–441 (2001).
[16] O. De Castro E. Silva, Jr., S. Zucoloto, L. A. Mene-gazzo, R. G. Granato, L. G. Marcassa, and V. S. Bag-nato, Lasers Surg. Med. 29, 73–77 (2001).
[17] N. Pourreau-Schneider, A. Ahmed, M. Soudry, J. Jac-quemier, F. Kopp, J. C. Franquin, and P. M. Martin,Am. J. Pathol. 137, 171–178 (1990).
[18] T. N. Demidova-Rice, E. V. Salomatina, A. N. Yaro-slavsky, I. M. Herman, and M. R. Hamblin, LasersSurg. Med. 39, 706–715 (2007).
[19] L. Frigo, G. M. Favero, H. J. Lima, D. A. Maria, J. M.Bjordal, J. Joensen, V. V. Iversen, R. L. Marcos, N. A.Parizzoto, and R. A. Lopes-Martins, Photomed. LaserSurg. 28 (Suppl. 1), S151–156 (2010).
[20] M. A. Ribeiro, R. L. Albuquerque, Jr., L. M. Ramalho,A. L. Pinheiro, L. R. Bonjardim, and S. S. Da Cunha,Photomed. Laser Surg. 27, 49–55 (2009).
[21] V. Prabhu, B. S. S. Rao, B. N. Rao, B. K. Aithal, B. S.Shenoy, and K. K. Mahato, Pramana–J. Phys. 75,1287–1293 (2010).
[22] V. N. Hegde, V. Prabhu, S. B. Rao, S. Chandra, P. Ku-mar, K. Satyamoorthy, and K. K. Mahato, Photo-chem. Photobiol. 87, 1433–1441 (2011).
[23] V. Prabhu, S. B. Rao, N. B. Rao, K. B. Aithal, P. Ku-mar, and K. K. Mahato, Photochem. Photobiol. 86,1364–1372 (2010).
[24] H. Liu, Y. Dang, Z. Wang, X. Chai, and Q. Ren, La-sers Surg. Med. 40, 13–19 (2008).
[25] B. Eyden and M. Tzaphlidou, Micron 32, 287–300(2001).
[26] V. J. James, L. Delbridge, S. V. Mclennan, and D. K.Yue, Diabetes 40, 391–394 (1991).
[27] V. Prabhu, S. B. S. Rao, P. Kumar, L. Rao, and K. K.Mahato, Proc. SPIE 7887, 788701–788709 (2011).
[28] P. A. Villanueva, A. K. Mcnulty, H. D. Beniker, andK. Kieswetter (2010), Method for quantitation of col-lagen in tissue. Vol. US 7,713,743, B2. pp. 16. GooglePatents, USA.
[29] K. Lacjakova, N. Bobrov, M. Polakova, M. Slezak,M. Vidova, T. Vasilenko, M. Novotny, F. Longauer,L. Lenhardt, J. Bober, M. Levkut, F. Sabol, and P. Gal,Lasers Med. Sci. 25, 761–766 (2010).
[30] T. Y. Chung, P. V. Peplow, and G. D. Baxter, Photo-med. Laser Surg. 28, 251–261 (2010).
[31] K. R. Byrnes, L. Barna, V. M. Chenault, R. W. Way-nant, I. K. Ilev, L. Longo, C. Miracco, B. Johnson, andJ. J. Anders, Photomed. Laser Surg. 22, 281–290(2004).
[32] T. Luo, J. X. Chen, S. M. Zhuo, K. C. Lu, X. S. Jiang,and Q. G. Liu, Laser Phys. 19, 478–482 (2009).
[33] M. Mokry, P. Gal, B. Vidinsky, J. Kusnir, K. Duba-yova, S. Mozes, and J. Sabo, Photochem. Photobiol.82, 793–797 (2006).
[34] E. Drakaki, E. Borisova, M. Makropoulou, L. Avra-mov, A. A. Serafetinides, and I. Angelov, Skin. Res.Technol. 13, 350–359 (2007).
[35] J. Q. Brown, K. Vishwanath, G. M. Palmer, and N. Ra-manujam, Curr. Opin. Biotechnol. 20, 119–131(2009).
[36] S. D. Kamath, R. A. Bhat, S. Ray, and K. K. Mahato,Photomed. Laser Surg. 27, 325–335 (2009).
[37] P. K. Gupta, S. K. Majumder, and A. Uppal, LasersSurg. Med. 21, 417–422 (1997).
[38] N. Vengadesan, P. Aruna, and S. Ganesan, Br. J. Can-cer 77, 391–395 (1998).
[39] W. C. Lin, S. A. Toms, M. Johnson, E. D. Jansen, andA. Mahadevan-Jansen, Photochem. Photobiol. 73,396–402 (2001).
K. K. Mahato is presently working as an Associate Pro-fessor, Biophysics Unit, Manipal Life Sciences Centre,Manipal University, India. He joined the Departmentafter completing his Ph.D. from the Banaras HinduUniversity, Varanasi India and spending a short periodof few years at IIT Kanpur. His current research activ-ities include application of laser spectroscopy includingfluorescence, photoacoustic and Raman spectroscopy inbiology and medicine, low level laser therapy for tissueregeneration involving in vitro and in vivo models anddeveloping various optical instrumentations for earlydetection of various diseases.
J. Biophotonics 5, No. 2 (2012) 183
FULLFULLARTICLEARTICLE
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheimwww.biophotonics-journal.org
[40] G. A. Wagnieres, W. M. Star, and B. C. Wilson, Photo-chem. Photobiol. 68, 603–632 (1998).
[41] R. R. Alfano, A. Pradhan, G. C. Tang, and S. J. Wahl,JOSA B 6, 1015–1023 (1989).
[42] R. Richards-Kortum and E. Sevick-Muraca, Annu.Rev. Phys. Chem. 47, 555–606 (1996).
[43] L. Alchab, G. Dupuis, C. Balleyguier, M. C. Mathieu,M. P. Fontaine-Aupart, and R. Farcy, J. Biophotonics3, 373–384 (2010).
[44] K. Arakawa, K. Isoda, T. Ito, K. Nakajima, T. Shibu-ya, and F. Ohsuzu, Arterioscler Thromb. Vasc. Biol.22, 1002–1007 (2002).
[45] R. M. Korol, H. M. Finlay, M. J. Josseau, A. R. Lucas, andP. B. Canham, J. Biomed. Opt. 12, 024011-1–8 (2007).
[46] A. Christov, R. M. Korol, E. Dai, L. Liu, H. Guan,M. A. Bernards, P. B. Cavers, D. Susko, and A. Lucas,Photochem. Photobiol. 81, 457–466 (2005).
[47] A. T. Truong, A. Kowal-Vern, B. A. Latenser, D. E. Wi-ley, and R. J. Walter, J. Burns Wounds. 4, 72–82 (2005).
[48] C. B. Ballas and J. M. Davidson, Wound Repair Re-gen 9, 223–237 (2001).
[49] J. Myllyharju and K. I. Kivirikko, Ann. Med. 33, 7–21(2001).
[50] S. B. Rabelo, A. B. Villaverde, R. Nicolau, M. C. Sal-gado, S. Melo Mda, and M. T. Pacheco, Photomed.Laser Surg. 24, 474–479 (2006).
[51] E. C. De Oliveira Guirro, M. I. De Lima Montebelo,B. De Almeida Bortot, M. A. Da Costa Betito Torres,and M. L. Polacow, Photomed. Laser Surg. 28, 629–634 (2010).
[52] T. Y. Chung, P. V. Peplow, and G. D. Baxter, Photo-med. Laser Surg. 28, 251–261 (2010).
[53] M. Lagerweij, M. Van Der Veen, M. Ando, L. Lukant-sova, and G. Stookey, Caries Res 33, 220–226 (1999).
[54] Mayer, Z. f. wissenschaftl. Mikroskopie u. mikroskop.Technik 20, 409 (1903).
[55] Masson, Bulletin of the International Association ofMedicine 12, 75 (1929).
[56] R. M. H. Mcminn and J. J. Pritchard, Tissue repair.(Academic Press, New York and London, 1969),pp. 1–40.
[57] A. Johansson, K. Kromer, R. Sroka, and H. Stepp,Med. Laser App. 23, 155–174 (2008).
[58] R. Alfano, D. Tata, J. Cordero, P. Tomashefsky,F. Longo, and M. Alfano, IEEE J. Quant. Electron20, 1507–1511 (1984).
[59] R. R. Alfano, B. B. Das, J. Cleary, R. Prudente, andE. J. Celmer, Bull N Y Acad. Med. 67, 143–150 (1991).
[60] E. G. Borisova, E. Nikolova, P. P. Troyanova, and L. A.Avramov, J. Optoele. Adv. Mat. 10, 717–722 (2008).
[61] N. Ramanujam, Neoplasia 2, 89–117 (2000).[62] L. P. Hariri, A. R. Tumlinson, D. G. Besselsen, U. Ut-
zinger, E. W. Gerner, and J. K. Barton, Lasers Surg.Med. 38, 305–313 (2006).
[63] Y. P. Sinichkin, S. R. Utz, A. H. Mavliutov, and H. A.Pilipenko, J. Biomed. Opt. 3, 201–211 (1998).
[64] E. L. Nussbaum, T. Mazzulli, K. P. Pritzker, F. L.Heras, F. Jing, and L. Lilge, Lasers Surg. Med. 41,372–381 (2009).
[65] W. A. Kues and H. Niemann, Trends Biotechnol. 22,286–294 (2004).
[66] S. Andersson-Engels, J. Johansson, U. Stenram,K. Svanberg, and S. Svanberg, IEEE J. Quant. Elec-tron 26, 2207–2217 (1990).
[67] N. Kollias, G. Zonios, and G. N. Stamatas, Vib. Spec-trosc. 28, 17–23 (2002).
[68] I. Mandl, S. Keller, and J. Manahan, Biochemistry-US3, 1737–1741 (1964).
[69] M. D. Bond and H. E. Van Wart, Biochemistry-US 23,3077–3085 (1984).
[70] K. A. Mookhtiar and H. E. Van Wart, Matrix Suppl. 1,116–126 (1992).
[71] S. G. Alivisatos, F. Ungar, and G. Abraham, Nature203, 973–975 (1964).
[72] L. Rover Junior, J. C. Fernandes, G. De OliveiraNeto, L. T. Kubota, E. Katekawa, and S. H. Serrano,Anal. Biochem. 260, 50–55 (1998).
[73] M. G. Xu, E. D. Williams, E. W. Thompson, and M. Gu,Appl. Opt. 39, 6312–6317 (2000).
[74] S. P. Robins, Baillieres Clin. Rheumatol. 2, 1–36 (1988).[75] M. D. Shoulders and R. T. Raines, Annu. Rev. Bio-
chem. 78, 929–958 (2009).[76] K. Kuhn, Stru funct collagen typ, 1–42 (1987).[77] T. S. Alster and E. L. Tanzi, Am. J. Clin. Dermatol. 4,
235–243 (2003).[78] L. Marcu, D. Cohen, J. M. I. Maarek, and W. S.
Grundfest, Proc. SPIE 3917, 93–101 (2000).[79] D. R. Eyre, M. A. Paz, and P. M. Gallop, Annu. Rev.
Biochem. 53, 717–748 (1984).[80] D. Fujimoto, Biochem. Biophys. Res. Commun. 76,
1124–1129 (1977).[81] S. D. Kamath and K. K. Mahato, J. Biomed. Opt. 12,
0140281–0140289 (2007).[82] M. Mokry, P. Gal, B. Vidinsky, J. Kusnir, K. Dubayo-
va, S. Mozes, and J. Sabo, Photochem. Photobiol. 82,793–797 (2006).
[83] J. Tang, F. Zeng, J. M. Evans, B. Xu, H. Savage, P. P.Ho, and R. R. Alfano, J. Clin. Laser Med. Surg. 18,117–123 (2000).
[84] T. K. Gayen, A. Katz, H. E. Savage, S. A. Mccormick,M. Al-Rubaiee, Y. Budansky, J. Lee, and R. R. Alfa-no, J. Clin. Laser Med. Surg. 21, 259–269 (2003).
[85] A. Alimova, R. Chakraverty, R. Muthukattil, S. Elder,A. Katz, V. Sriramoju, S. Lipper, and R. R. Alfano,J. Photochem. Photobiol. B 96, 178–183 (2009).
[86] M. J. Im and J. E. Hoopes, Proc. Soc. Exp. Biol. Med.173, 17–20 (1983).
[87] H. N. Markolf, Laser Tissue Interactions-Fundamen-tals and Applications (Springer Verlag, Berlin, 2003),pp. 9–25, 45–147.
[88] A. J. Hussein, A. A. Alfars, M. A. J. Falih, and A. Has-san, North Am. J. Med. Sci. 3, 193–197 (2011).
[89] P. T. Carvalho, N. Mazzer, F. A. Dos Reis, A. C. Bel-chior, and I. S. Silva, Acta Cir. Bras. 21, 177–183(2006).
[90] R. J. Gomez-Villamandos, J. M. Santisteban Valen-zuela, I. Ruiz Calatrava, J. C. Gomez-Villamandos, andI. Avila Jurado, Lasers Surg. Med. 16, 184–188 (1995).
[91] F. A. Al-Watban and B. L. Andres, J. Clin. LaserMed. Surg. 21, 249–258 (2003).
[92] J. S. Kana, G. Hutschenreiter, D. Haina, and W. Wai-delich, Arch. Surg. 116, 293–296 (1981).
V. Prabhu et al.: Spectroscopic and histological studies on wound healing progression184
Journal of
BIOPHOTONICS
# 2012 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.biophotonics-journal.org