modulating conjunctival wound healing
TRANSCRIPT

M.F. Cordeiro
L. Chang
K. Sheng Lim
n. Daniels
R.D. Pleass
D. Siriwardena
P.T. Khaw
Wound Healing Research
Unit
Department of Pathology & Glaucoma
Moorfields Eye Hospital and
Institute of Ophthalmology
London, UK
L. Chang
Department of Immunology
Royal Free and University
College Medical School
London, UK
M. Francesca Cordeiro, PhD,
MRCP, FRCOphth I';!(l Wound Healing Research
and Glaucoma Units
Institute of Ophthalmology
11-43 Bath Street
London EC 1V gEL, UK
536
Modulating
conjunctival wound healing
Abstract
Advances in molecular and cell biology have
led to an expansion in our knowledge and
understanding of the processes involved in
wound healing. We review existing and
potential therapies modulating the
conjunctival scarring response, with particular
reference to glaucoma filtration surgery. We
discuss how the refinement of present
antimetabolite regimens can minimise
complications and improve surgical results,
and advocate their use in carefully selected
patient groups. Perhaps the most promising
approach is targeting biological molecules.
Hence, use of fully human neutralising
monoclonal antibodies to the growth factor
TGFf3 has potential as a useful strategy for
modifying conjunctival scarring. Combination
therapies may also afford an improved
therapeutic index. It is hoped that future
therapies can offer safer, more specific, focal
and titratable treatment, with far-reaching
clinical applications.
Key words Antimetabolites, Conjunctival scarring, Glaucoma surgery, Growth factors, Wound healing
The impact of primary glaucoma world-wide means that it is now the leading cause of irreversible vision loss, estimated to account for 15% (6.7 million) of world blindness.1-3 The treatment of this disease is directed towards the reduction of intraocular pressure (the main identifiable risk factor in glaucoma)4 and includes topical medication, laser and surgery. Of all available therapies, filtration surgery has been shown to be the most effective.s,6 However, the major determinant of the longterm outcome of glaucoma surgery is the conjunctival wound healing response -excessive post-operative scarring significantly reducing surgical success,s 8 and inadequate healing being associated with thin-walled filtration blebs, wound leakage, hypotony and infection.9-11
The introduction of the antiproliferative drugs mitomycin C and 5-fluorouracil as conjunctival anti-scarring treatments has revolutionised filtration surgery, and these
M. FRANCESCA CORDEIRO, LYDIA CHANG, K. SHENG LIM, JULIE T. DANIELS, ROBERT D. PLEASS,
DILANI SIRIWARDENA, PENG T. KHAW
agents are now in widespread use. These antimetabolites significantly reduce postoperative fibrosis and, in patients known to be at high risk of scarring, can prevent surgical failureY-15 (Fig. 1) However, they do so by causing widespread cell death and apoptosis/6,17 and are associated with severe and potentially blinding complications.9-11 Currently, more specific anti-scarring treatments are being investigated, as these antiproliferative drugs provide just one strategy of modulating the wound healing response.
The processes regulating scarring, as illustrated in Fig. 2, are both numerous and complex. Modulation of the healing response can occur at various stages. However, it is only recently with the expansion in our knowledge of the mechanisms underlying these processes, that refinement of existing therapies and the development of potential new therapies have been achieved. Below, we summarise the biology of wound healing, following which we
review existing and potential therapies modulating the scarring response, with particular reference to glaucoma filtration surgery.
The wound healing process
Wound healing is a complex, dynamic process which may be simplified by dividing it into three phases: inflammatory, proliferative and remodelling (Fig. 2).18,19
The inflammatory phase is characterised by an inflammatory response, with an influx of neutrophils and monocytes to the wound area, and haemostasis. Injury (e.g. surgical conjunctival incisions) results in both connective tissue and blood vessel damage. Following the extravasation of blood, plasma proteins and extracellular matrix fragments are released into the damaged site, with activation of the clotting cascade. The formation of haemostat plugs from the aggregation of platelets is further stimulated by the presence of
factors such as thrombin, adenosine diphosphate (ADP), fibrinogen, and collagen, thrombospondin and von Willebrand factor VIII, all helping to achieve haemostasis. Activation of platelets and the blood clotting cascade results in the release of a variety of
Eye (2000) 14, 536-547 © 2000 Royal College of Ophthalmologists
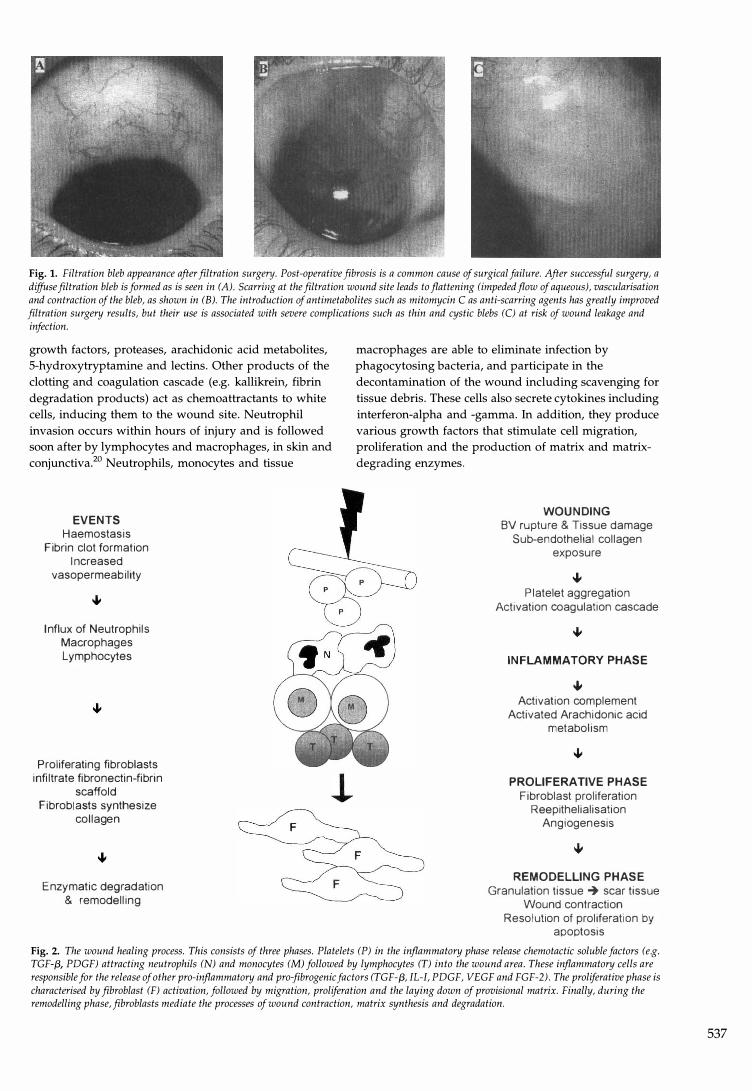
Fig. 1. Filtration bleb appearance after filtration surgery. Post-operative fibrosis is a common cause of surgical failure. After successful surgery, n
diffuse filtration bleb is formed as is seen in (A). Scarring at the filtration wound site leads to flattening (impeded flow of aqueous), vascularisation and contraction of the bleb, as shown in (B). The introduction of antimetabolites such as mitomycin C as anti-scarring agents has greatly improved filtration surgery results, but their llse is associated with severe complications such as thin and cystic blebs (C) at risk of wound leakage and infection.
growth factors, proteases, arachidonic acid metabolites, 5-hydroxytryptamine and lectins. Other products of the clotting and coagulation cascade (e.g. kallikrein, fibrin degradation products) act as chemoattractants to white cells, inducing them to the wound site. Neutrophil invasion occurs within hours of injury and is followed soon after by lymphocytes and macrophages, in skin and conjunctiva?O Neutrophils, monocytes and tissue
EVENTS Haemostasis
Fibrin clot formation Increased
vasopermeability
Influx of Neutrophils Macrophages Lymphocytes
Proliferating fibroblasts infiltrate fibronectin-fibrin
scaffold Fibroblasts synthesize
collagen
Enzymatic degradation & remodelling
macrophages are able to eliminate infection by phagocytosing bacteria, and participate in the decontamination of the wound including scavenging for tissue debris. These cells also secrete cytokines including interferon-alpha and -gamma. In addition, they produce various growth factors that stimulate cell migration, proliferation and the production of matrix and matrixdegrading enzymes.
WOUNDING BV rupture & Tissue damage
Sub-endothelial collagen exposure
� Platelet aggregation
Activation coagulation cascade
INFLAMMATORY PHASE
� Activation complement
Activated Arachidonic acid metabolism
PROLIFERATIVE PHASE Fibroblast proliferation
Reepithelialisation Angiogenesis
REMODELLING PHASE Granulation tissue -+ scar tissue
Wound contraction Resolution of proliferation by
apoptosis
Fig. 2. The wound healing process. This consists of three phases. Plate/ets (P) in the inflammatory phase release chemotactic soluble factors (e.g. TGF-(3, PVGF) attracting neutrophils (N) and monocytes (M) followed by lymphocytes (T) into the wound area. These inflammatory cells are responsible for the release of other pro-inflammatory and pro-fibrogenic factors (TGF-(3, IL-I, PVGF, VEGF and FGF-2). The proliferative phase is characterised by fibroblast (F) activation, followed by migration, proliferation and the laying down of provisional matrix. Finally, during the remodelling phase, fibroblasts mediate the processes of wound contraction, matrix synthesis and degradation.
537

538
RESOLUTION OF WOUND HEAUNG REACTION
-+ Neutrophils decrease from day 3 by apoptosis
-+ Apoptosis = gene-directed cell death • Nuclear condensation • Cytoplasmic condensation • Nuclear fragmentation • Intact cell membrane
INFLAMMATORY + Cleared by phagocytosis by macrophages PHASE
+ Lymphocyte numbers increase between day 8-14
-+ Expanded population activated T cells decreases by apoptosis
-+ Fas-mediated apoptosis at peak of inflammatory response
+ Cytokine-deprivation mediated apoptosis at end of inflammatory response
PROUFERA TIVE -+ PHASE
Fibroblast numbers decrease from about day 7 by apoptosis Initiating mechanisms for fibroblast apoptosis unknown
Fig. 3. Aopoptotic processes and wound healing resolution. The inflammatory and proliferative phases of the wound-healing reaction probably resolve by apoptosis. In inflammatory cells, apoptosis probably occurs by signalling through death receptors (Fas receptor) and the withdrawal of nutrient cytokines. The initiating mechanisms for fibroblast apoptosis are not clearly known. Wound debris and apoptotic bodies are subsequently cleared by phagocytic macrophages. N, neutrophils; M, monocytes; T, lymphocytes; F, fibroblasts.
Re-epithelialisation and an increase in fibroblast activity and number occur in the proliferative phase, as do the processes of angiogenesis and the deposition of granulation tissue. The formation of fibrin, derived from plasma fibrinogen, provides an initial 'scaffold' bridging the gaps between wound edges. However, new matrix or granulation tissue begins to be laid approximately 4 days after injury and is heralded by the migration of fibroblasts to the wound site, accompanied by the ingrowth of blood vessels. Normally, the fibroblast exists within the subconjunctival connective tissue as a quiescent undifferentiated mesenchymal cell, the fibrocyte. On activation and recruitment of local fibrocytes, the scarring response is initiated: without the conjunctival fibroblast, conjunctival scarring would not be significant.21
The fibroblast is also important in the remodelling phase. It is responsible not only for wound contraction and the depOSition and synthesis of new matrix, but also for its modification. Fibroblasts produce enzymes that have proteolytic activity that allow cell migration and movement into provisional and collagenous matrix. Extracellular matrix (ECM) is degraded by these same enzymes called matrix metalloproteases (MMPs). The MMPs are also involved in the process of wound contraction, again a process mediated by fibroblasts?2,23
One aspect of the healing response that has only recently come to light is the role of apoptosis (Fig. 3). Once the wound is filled with collagenous matrix, angiogenesis ceases, and fibroblasts within the matrix stop synthesising molecules and undergo programmed cell death,24 although the signals inducing fibroblast
apoptosis in this environment are still not fully known. This accounts for the relative acellularity of a mature scar compared with that of an early wound,
Wound modulation
There are a variety of agents available which can modify the scarring response and fibroblast function. Important considerations are the length, degree and types of stimulation present in the surrounding wound area, which can influence the overall profile of healing, including fibroblast behaviour.
Many strategies are currently and potentially available for the modulation of the scarring response (Table 1), including factors specifically affecting fibroblast behaviour such as activation, migration, wound contraction, ECM synthesis and degradation, and proliferation. In addition there are factors affecting inflammation, fibrinolysis, angiogenesis, wound healing resolution, cytokines, growth factors and their receptors. Each of these will now be described in detail.
Factors affecting fibroblast behaviour
Fibroblast activation
The process of fibroblast activation is not yet understood?5 However, it is suggested that in the eye certain control mechanisms may exist that change the fibroblast phenotype leading to activation of a fibrotic response, such as activation of transcription factors and intracellular signalling pathways?6
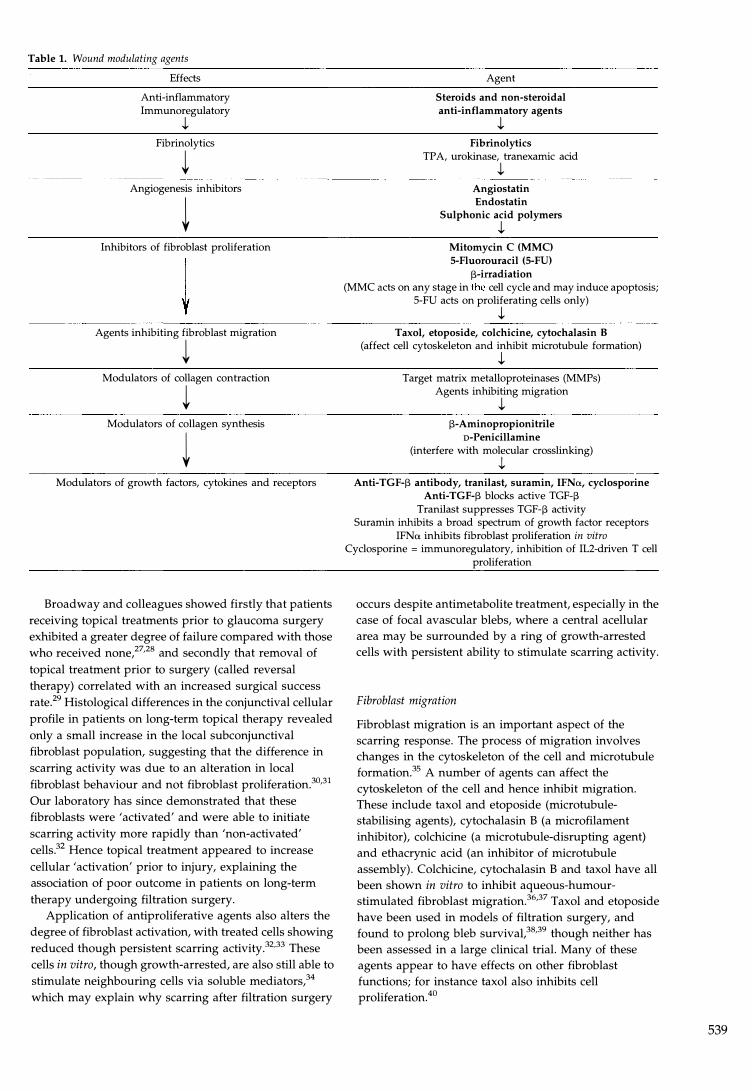
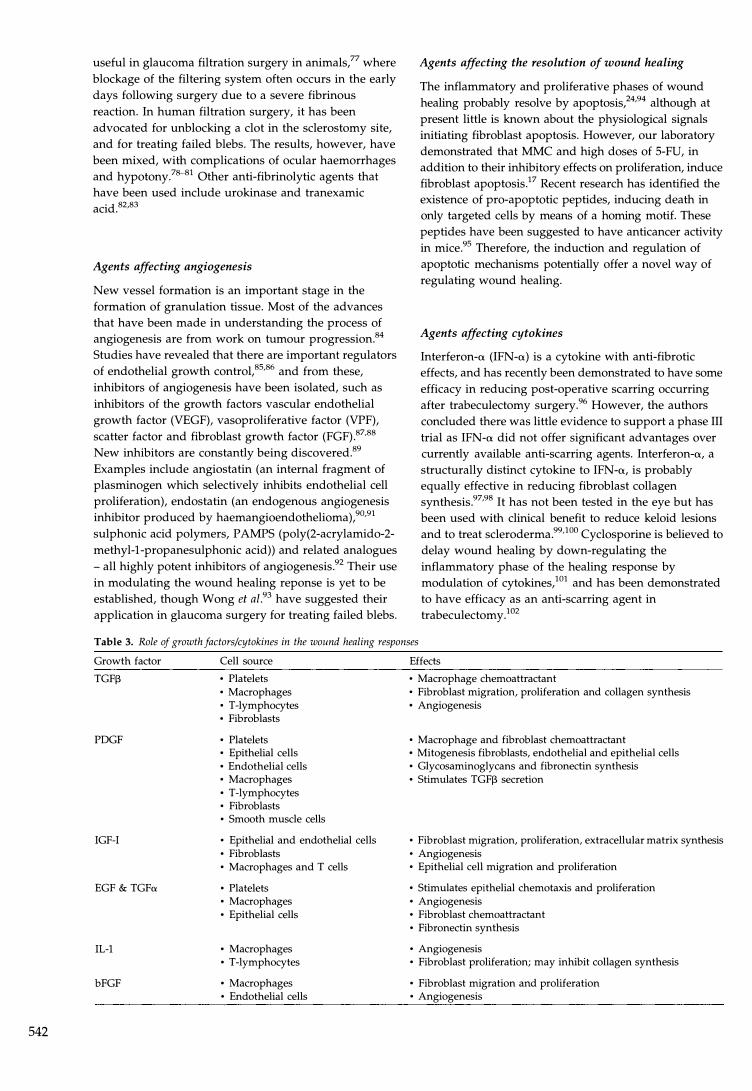
Table 1. Wound modulating agents
Effects
Anti-inflammatory Immunoregulatory
J. Fibrinolytics
� Angiogenesis inhibitors
� Inhibitors of fibroblast proliferation
Agents inhibiting fibroblast migration
� Modulators of collagen contraction
� Modulators of collagen synthesis
� Modulators of growth factors, cytokines and receptors
Broadway and colleagues showed firstly that patients receiving topical treatments prior to glaucoma surgery exhibited a greater degree of failure compared with those who received none,27,28 and secondly that removal of topical treatment prior to surgery (called reversal therapy) correlated with an increased surgical success rate?9 Histological differences in the conjunctival cellular profile in patients on long-term topical therapy revealed only a small increase in the local subconjunctival fibroblast population, suggesting that the difference in scarring activity was due to an alteration in local fibroblast behaviour and not fibroblast proliferation?0,31 Our laboratory has since demonstrated that these fibroblasts were 'activated' and were able to initiate scarring activity more rapidly than 'non-activated' cells.32 Hence topical treatment appeared to increase cellular 'activation' prior to injury, explaining the association of poor outcome in patients on long-term therapy undergoing filtration surgery.
Application of antiproliferative agents also alters the degree of fibroblast activation, with treated cells showing reduced though persistent scarring activity?2,33 These cells in vitro, though growth-arrested, are also still able to stimulate neighbouring cells via soluble mediators,34 which may explain why scarring after filtration surgery
Agent
Steroids and non-steroidal
anti-inflammatory agents
J. Fibrinolytics
TP A, urokinase, tranexamic acid
J. Angiostatin Endostatin
Sulphonic acid polymers
J. Mitomycin C (MMC)
5-Fluorouracil (5-FU)
J3-irradiation (MMC acts on any stage in the cell cycle and may induce apoptosis;
5-FU acts on proliferating cells only)
J. Taxol, etoposide, colchicine, cytochalasin B
(affect cell cytoskeleton and inhibit microtubule formation)
J. Target matrix metalloproteinases (MMPs)
Agents inhibiting migration
J. 13-Aminopropionitrile
D-Penicillamine
(interfere with molecular crosslinking)
J. Anti-TGF-J3 antibody, tranilast, suramin, IFNrr, cyclosporine
Anti-TGF-J3 blocks active TGF-J3 Tranilast suppresses TGF-J3 activity
Suramin inhibits a broad spectrum of growth factor receptors IFNrr inhibits fibroblast proliferation in vitro
Cyclosporine = immunoregulatory, inhibition of IL2-driven T cell proliferation
occurs despite antimetabolite treatment, especially in the case of focal avascular blebs, where a central acellular area may be surrounded by a ring of growth-arrested cells with persistent ability to stimulate scarring activity.
Fibroblast migration
Fibroblast migration is an important aspect of the scarring response. The process of migration involves changes in the cytoskeleton of the cell and microtubule formation?5 A number of agents can affect the cytoskeleton of the cell and hence inhibit migration. These include taxol and etoposide (microtubulestabilising agents), cytochalasin B (a microfilament inhibitor), colchicine (a microtubule-disrupting agent) and ethacrynic acid (an inhibitor of microtubule assembly). Colchicine, cytochalasin B and taxol have all been shown in vitro to inhibit aqueous-humourstimulated fibroblast migration.36,37 Taxol and etoposide have been used in models of filtration surgery, and found to prolong bleb surviva1,38,39 though neither has been assessed in a large clinical trial. Many of these agents appear to have effects on other fibroblast functions; for instance taxol also inhibits cell proliferation. 40
539

540
Fibroblast-mediated matrix contraction
A particularly vital function of the fibroblast in the scarring response is its ability to contract the wound. This process is not fully understood, although it is known that cell migration is intrinsically involved in contraction. Hence, any anti-migration agent described above would also inhibit contraction.
Occleston et al.,22 from our laboratory, using in vitro
models of collagen contraction, have demonstrated the involvement of matrix metalloproteinases (MMPs) in the process of contraction. Recent work suggests that MMPs are particularly important in the initial 'spreading' phase of contraction.41 The importance of MMPs in contraction has been demonstrated by the fact that collagen contraction can be inhibited using MMP inhibitors.23,42 Early findings from clinical trials on the use of MMPs in cutaneous wounds have been inconclusive.43 However, as MMP inhibitors are being developed to be highly specific, non-toxic and reversible, it is hoped that further therapeutic applications will be possible, enabling more control of the degree of contraction that occurs in wound healing.44,45
Fibroblast ECM synthesis and degradation
Agents affecting ECM synthesis include the lathyrogenic agents l3-aminopropionitrile and D-penicillamine, which primarily interfere with molecular cross-linking, and inhibit the production and maturation of collagen from fibroblasts. The mechanism of action appears to be an inhibition of the enzyme lysyl oxidase, which is essential for the maturation of collagen. There is experimental and clinical evidence that this may work in filtration surgery.46 Direct antagonism of MMPs and TIMPs with specific inhibitors, as discussed above, may in future also be possible.
Table 2. MoorfieldslFlorida (More Flow) regimen
Risk group Risk factors
High risk • Neovascular glaucoma • Chronic uveitis
Fibroblast proliferation
The first antiproliferative agents advocated for use in the eye to suppress fibroblast division, were 5-fluorouracil (5-FU) and mitomycin C (MMC). Initially shown to prevent epiretinal scarring in an animal model,47,48 5-FU was found to be an effective glaucoma anti-scarring agent in a large multicentre study, where repeated subconjunctival injections after filtration surgery in patients at high risk of developing post-operative fibrosis reduced the failure rate from 50% to 27%? At the same time, use of MMC in filtration surgery was also being assessed with encouraging results.49 Our laboratory studies have demonstrated that long-term suppression of fibroblast proliferation can be obtained with single and not repeated applications of MMC and 5-FU, and this effect is both titratable (in terms of length of action) and focal.16,50,51 Clinical studies have demonstrated that in high-risk patients a single application of MMC provides better long-term pressure control than 5_FU.13-15 However, both treatments result in the production of thin avascular blebs with the incidence of bleb leakages, hypotony and endophthalmitis being slightly more prevalent with the thinner-walled MMC-treated blebs.9-11
We and several other groups have attempted to reduce the incidence of complications associated with the use of antiproliferatives in glaucoma filtration surgery, by optimising the choice of agent, its application and the surgical technique. Like other groups, we have found MMC to be particularly useful in the management of high-risk patients such as those with cicatricial conjunctiva, and in young patients with congenital glaucoma. 52-55 One method of restricting antimetabolite use is by adopting a strategy based on different, singleapplication anti-scarring agents and concentrations 'titrated' against patient risk factors. At Moorfields Eye Hospital we have designed such a regimen, called the Moorfields/Florida (More Flow) regimen, which is continuously evolving depending upon laboratory and clinical data, and is illustrated in Table 2.56
Anti-scarring regimen
None
• Previous failed trabeculectomy or tubes with 5-FU 25 or 50 mg/ml [3-irradiation 750 cGy
Intermediate risk
Low risk
5-FU / irradiation • Chronic conjunctival inflammation • Multiple risk factors • Aphakic glaucoma (tube more appropriate)
• Topical medications (adrenaline and preservatives) • Previous cataract surgery without conjunctival incision
(intact capsule) • Previous conjunctival surgery, e.g. squint, detachment surgery,
trabeculotomy • Several low risk factors • Combined glaucoma filtration surgery/cataract extraction
• No risk factors • Topical medications (beta-blockers/pilocarpine) • Elderly Afro-Caribbeans • Age < 40 years
5-FU, 5-fluorouracil; MMC, mitomycin C.
5-FU 24 or 50 mg/ml MMC 0.2 mg/ml [3-irradiation 750 cGy
MMC 0.2-0.4 mg/ml Post-operative 5-FU can be given
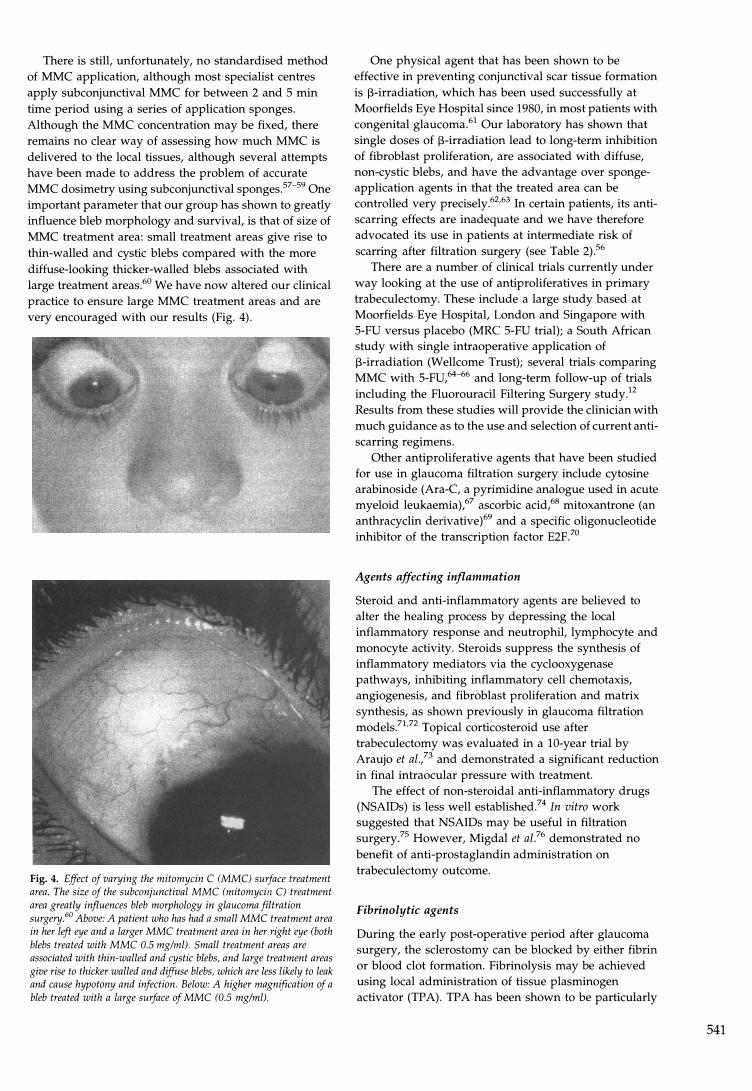
There is still, unfortunately, no standardised method of MMC application, although most specialist centres apply subconjunctival MMC for between 2 and 5 min time period using a series of application sponges. Although the MMC concentration may be fixed, there remains no clear way of assessing how much MMC is delivered to the local tissues, although several attempts have been made to address the problem of accurate MMC dosimetry using subconjunctival sponges. 57-59 One important parameter that our group has shown to greatly influence bleb morphology and survival, is that of size of MMC treatment area: small treatment areas give rise to thin-walled and cystic blebs compared with the more diffuse-looking thicker-walled blebs associated with large treatment areas.60 We have now altered our clinical practice to ensure large MMC treatment areas and are very encouraged with our results (Fig. 4).
Fig. 4. Effect of varying the mitomycin C (MMC) surface treatment area. The size of the subconjunctival MMC (mitomycin C) treatment area greatly influences bleb morphology in glaucoma filtration surgery.60 Above: A patient who has had a small MMC treatment area in her left eye and a larger MMC treatment area in her right eye (both blebs treated with MMC 0.5 mg/ml). Small treatment areas are associated with thin-walled and cystic blebs, and large treatment areas give rise to thicker walled and diffuse blebs, which are less likely to leak and cause hypotony and infection. Below: A higher magnification of a bleb treated with a large surface of MMC (0.5 mg/ml).
One physical agent that has been shown to be effective in preventing conjunctival scar tissue formation is l3-irradiation, which has been used successfully at Moorfields Eye Hospital since 1980, in most patients with congenital glaucoma.61 Our laboratory has shown that single doses of l3-irradiation lead to long-term inhibition of fibroblast proliferation, are associated with diffuse, non-cystic blebs, and have the advantage over spongeapplication agents in that the treated area can be controlled very precisely.62.63 In certain patients, its antiscarring effects are inadequate and we have therefore advocated its use in patients at intermediate risk of scarring after filtration surgery (see Table 2).56
There are a number of clinical trials currently under way looking at the use of antiproliferatives in primary trabeculectomy. These include a large study based at Moorfields Eye Hospital, London and Singapore with 5-FU versus placebo (MRC 5-FU trial); a South African study with single intraoperative application of l3-irradiation (Wellcome Trust); several trials comparing MMC with 5_FU,64-66 and long-term follow-up of trials including the Fluorouracil Filtering Surgery study.12 Results from these studies will provide the clinician with much guidance as to the use and selection of current antiscarring regimens.
Other antiproliferative agents that have been studied for use in glaucoma filtration surgery include cytosine arabinoside (Ara-C, a pyrimidine analogue used in acute myeloid leukaemia),67 ascorbic acid,68 mitoxantrone (an anthracyclin derivative)69 and a specific oligonucleotide inhibitor of the transcription factor E2F?O
Agents affecting inflammation
Steroid and anti-inflammatory agents are believed to alter the healing process by depressing the local inflammatory response and neutrophil, lymphocyte and monocyte activity. Steroids suppress the synthesis of inflammatory mediators via the cyclooxygenase pathways, inhibiting inflammatory cell chemotaxis, angiogenesis, and fibroblast proliferation and matrix synthesis, as shown previously in glaucoma filtration models.71•72 Topical corticosteroid use after trabeculectomy was evaluated in a la-year trial by Araujo et al.,73 and demonstrated a significant reduction in final intraocular pressure with treatment.
The effect of non-steroidal anti-inflammatory drugs (NSAIDs) is less well established?4 In vitro work suggested that NSAIDs may be useful in filtration surgery?5 However, Migdal et az.76 demonstrated no benefit of anti-prostaglandin administration on trabeculectomy outcome.
Fibrinolytic agents
During the early post-operative period after glaucoma surgery, the sclerostomy can be blocked by either fibrin or blood clot formation. Fibrinolysis may be achieved using local administration of tissue plasminogen activator (TP A). TP A has been shown to be particularly
541
542
useful in glaucoma filtration surgery in animals,77 where blockage of the filtering system often occurs in the early days following surgery due to a severe fibrinous reaction. In human filtration surgery, it has been advocated for unblocking a clot in the sclerostomy site, and for treating failed blebs. The results, however, have been mixed, with complications of ocular haemorrhages and hypotony?8-81 Other anti-fibrinolytic agents that have been used include urokinase and tranexamic acid. 82,83
Agents affecting angiogenesis
New vessel formation is an important stage in the formation of granulation tissue. Most of the advances that have been made in understanding the process of angiogenesis are from work on tumour progression.84 Studies have revealed that there are important regulators of endothelial growth control, 85,86 and from these, inhibitors of angiogenesis have been isolated, such as inhibitors of the growth factors vascular endothelial growth factor (VEGF), vasoproliferative factor (VPF), scatter factor and fibroblast growth factor (FGF).87,88 New inhibitors are constantly being discovered.89 Examples include angiostatin (an internal fragment of plasminogen which selectively inhibits endothelial cell proliferation), endostatin (an endogenous angiogenesis inhibitor produced by haemangioendothelioma),90,91 sulphonic acid polymers, P AMPS (poly(2-acrylamido-2-methyl-l-propanesulphonic acid)) and related analogues - all highly potent inhibitors of angiogenesis.92 Their use in modulating the wound healing reponse is yet to be established, though Wong et al.93 have suggested their application in glaucoma surgery for treating failed blebs.
Agents affecting the resolution of wound healing
The inflammatory and proliferative phases of wound healing probably resolve by apoptosis,z4,94 although at present little is known about the physiological signals initiating fibroblast apoptosis. However, our laboratory demonstrated that MMC and high doses of 5-FU, in addition to their inhibitory effects on proliferation, induce fibroblast apoptosis.17 Recent research has identified the existence of pro-apoptotic peptides, inducing death in only targeted cells by means of a homing motif. These pep tides have been suggested to have anticancer activity in mice.95 Therefore, the induction and regulation of apoptotic mechanisms potentially offer a novel way of regulating wound healing.
Agents affecting cytokines
Interferon-a (IFN-a) is a cytokine with anti-fibrotic effects, and has recently been demonstrated to have some efficacy in reducing post-operative scarring occurring after trabeculectomy surgery,96 However, the authors concluded there was little evidence to support a phase III trial as IFN-a did not offer significant advantages over currently available anti-scarring agents, Interferon-a, a structurally distinct cytokine to IFN-a, is probably equally effective in reducing fibroblast collagen synthesis.97,98 It has not been tested in the eye but has been used with clinical benefit to reduce keloid lesions and to treat scleroderma.99,10o Cyclosporine is believed to delay wound healing by down-regulating the inflammatory phase of the healing response by modulation of cytokines,101 and has been demonstrated to have efficacy as an anti-scarring agent in trabeculectomy.lo2
Table 3. Role of growth factors/cytokines in the wound healing responses
Growth factor Cell source Effects
TGF[3 • Platelets • Macrophage chemoattractant • Macrophages • Fibroblast migration, proliferation and collagen synthesis • T-lymphocytes • Angiogenesis • Fibroblasts
PDGF • Platelets • Macrophage and fibroblast chemoattractant • Epithelial cells • Mitogenesis fibroblasts, endothelial and epithelial cells • Endothelial cells • Glycosaminoglycans and fibronectin synthesis • Macrophages • Stimulates TGF[3 secretion • T-Iymphocytes • Fibroblasts • Smooth muscle cells
IGF-I • Epithelial and endothelial cells • Fibroblast migration, proliferation, extracellular matrix synthesis • Fibroblasts • Angiogenesis • Macrophages and T cells • Epithelial cell migration and proliferation
EGF & TGFa • Platelets • Stimulates epithelial chemotaxis and proliferation • Macrophages • Angiogenesis • Epithelial cells • Fibroblast chemoattractant
• Fibronectin synthesis
IL-l • Macrophages • Angiogenesis • T-lymphocytes • Fibroblast proliferation; may inhibit collagen synthesis
bFGF • Macrophages • Fibroblast migration and proliferation • Endothelial cells • Angiogenesis
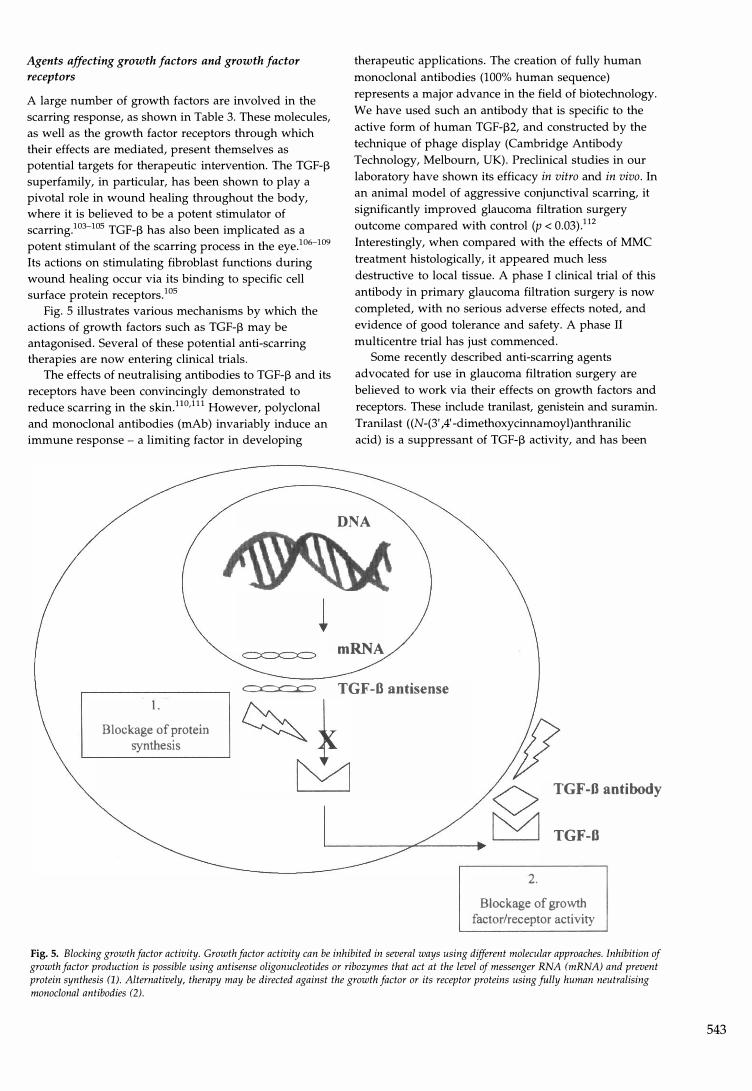
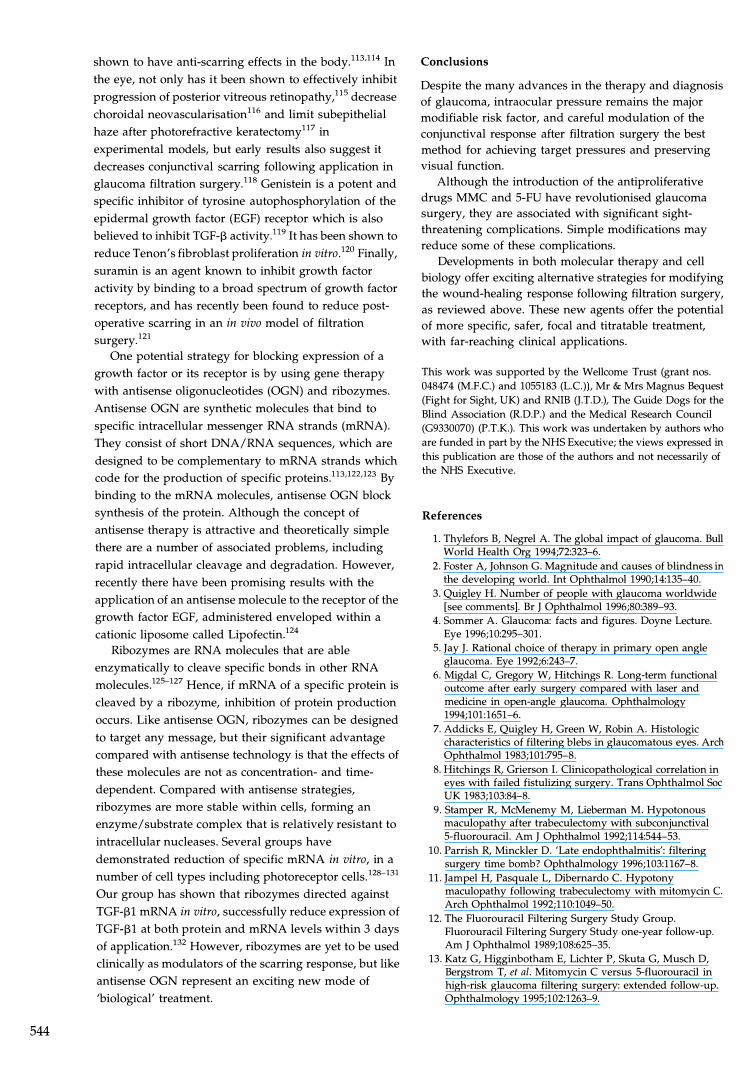
Agents affecting growth factors and growth factor receptors
A large number of growth factors are involved in the scarring response, as shown in Table 3. These molecules, as well as the growth factor receptors through which their effects are mediated, present themselves as potential targets for therapeutic intervention. The TGF-13 superfamily, in particular, has been shown to play a pivotal role in wound healing throughout the body, where it is believed to be a potent stimulator of scarring.103-lOS TGF-13 has also been implicated as a potent stimulant of the scarring process in the eye.106-109 Its actions on stimulating fibroblast functions during wound healing occur via its binding to specific cell surface protein receptors. lOS
Fig. 5 illustrates various mechanisms by which the actions of growth factors such as TGF-13 may be antagonised. Several of these potential anti-scarring therapies are now entering clinical trials.
The effects of neutralising antibodies to TGF-13 and its receptors have been convincingly demonstrated to reduce scarring in the skinYO,ll1 However, polyclonal and monoclonal antibodies (mAb) invariably induce an immune response - a limiting factor in developing
therapeutic applications. The creation of fully human monoclonal antibodies (100% human sequence) represents a major advance in the field of biotechnology. We have used such an antibody that is specific to the active form of human TGF-132, and constructed by the technique of phage display (Cambridge Antibody Technology, Melbourn, UK). Preclinical studies in our laboratory have shown its efficacy in vitro and in vivo. In an animal model of aggressive conjunctival scarring, it significantly improved glaucoma filtration surgery outcome compared with control (p < 0.03).112 Interestingly, when compared with the effects of MMC treatment histologically, it appeared much less destructive to local tissue. A phase I clinical trial of this antibody in primary glaucoma filtration surgery is now completed, with no serious adverse effects noted, and evidence of good tolerance and safety. A phase II multicentre trial has just commenced.
Some recently described anti-scarring agents advocated for use in glaucoma filtration surgery are believed to work via their effects on growth factors and receptors. These include tranilast, genistein and suramin. Tranilast ((N-(3' ,4' -dimethoxycinnamoyl)anthranilic acid) is a suppressant of TGF-13 activity, and has been
DNA
mRNA
c::x:=x::::::c: TGF -0 antisense 1.
Blockage of protein synthesis ~ 17 � TGF-B antibody
TGF-O
2.
Blockage of growth factor/receptor activity
Fig. 5, Blocking growth factor activity. Growth factor activity can be inhibited in several ways using different molecular approaches. Inhibition of growth factor production is possible using antisense oligonucleotides or ribozymes that act at the level of messenger RNA (mRNA) and prevent protein synthesis (1). Alternatively, therapy may be directed against the growth factor or its receptor proteins using fully human neutralising monoclonal antibodies (2).
543
544
shown to have anti-scarring effects in the bodyy3,114 In
the eye, not only has it been shown to effectively inhibit progression of posterior vitreous retinopathy,115 decrease choroidal neovascularisation116 and limit subepithelial haze after photorefractive keratectomyl17 in experimental models, but early results also suggest it decreases conjunctival scarring following application in glaucoma filtration surgeryy8 Genistein is a potent and specific inhibitor of tyrosine autophosphorylation of the epidermal growth factor (EGF) receptor which is also believed to inhibit TGF-13 activityY9 It has been shown to reduce Tenon's fibroblast proliferation in vitro yo Finally, suramin is an agent known to inhibit growth factor activity by binding to a broad spectrum of growth factor receptors, and has recently been found to reduce postoperative scarring in an in vivo model of filtration surgery. 121
One potential strategy for blocking expression of a growth factor or its receptor is by using gene therapy with antisense oligonucleotides (OGN) and ribozymes. Antisense OGN are synthetic molecules that bind to specific intracellular messenger RNA strands (mRNA). They consist of short DNA/RNA sequences, which are designed to be complementary to mRNA strands which code for the production of specific proteins.113,122.123 By binding to the mRNA molecules, antisense OGN block synthesis of the protein. Although the concept of antisense therapy is attractive and theoretically simple there are a number of associated problems, including rapid intracellular cleavage and degradation. However, recently there have been promising results with the application of an antisense molecule to the receptor of the growth factor EGF, administered enveloped within a cationic liposome called Lipofectin.124
Ribozymes are RNA molecules that are able enzymatically to cleave specific bonds in other RNA molecules.125-127 Hence, if mRNA of a specific protein is cleaved by a ribozyme, inhibition of protein production occurs. Like antisense OGN, ribozymes can be designed to target any message, but their significant advantage compared with antisense technology is that the effects of these molecules are not as concentration- and timedependent. Compared with antisense strategies, ribozymes are more stable within cells, forming an enzyme/substrate complex that is relatively resistant to intracellular nucleases. Several groups have demonstrated reduction of specific mRNA in vitro, in a number of cell types including photoreceptor cells.128-131 Our group has shown that ribozymes directed against TGF-131 mRNA in vitro, successfully reduce expression of TGF-131 at both protein and mRNA levels within 3 days of applicationy2 However, ribozymes are yet to be used clinically as modulators of the scarring response, but like antisense OGN represent an exciting new mode of 'biological' treatment.
Conclusions
Despite the many advances in the therapy and diagnosis of glaucoma, intraocular pressure remains the major modifiable risk factor, and careful modulation of the conjunctival response after filtration surgery the best method for achieving target pressures and preserving visual function.
Although the introduction of the antiproliferative drugs MMC and 5-FU have revolutionised glaucoma surgery, they are associated with significant sightthreatening complications. Simple modifications may reduce some of these complications.
Developments in both molecular therapy and cell biology offer exciting alternative strategies for modifying the wound-healing response following filtration surgery, as reviewed above. These new agents offer the potential of more specific, safer, focal and titratable treatment, with far-reaching clinical applications.
This work was supported by the Wellcome Trust (grant nos.
048474 (M.F.C) and 1055183 (L.C», Mr & Mrs Magrms Bequest
(Fight for Sight, UK) and RNIB (J.TD.), The Guide Dogs for the
Blind Association (RD.P.) and the Medical Research Council
(G9330070) (P.T.K.). This work was undertaken by authors who
are funded in part by the NHS Executive; the views expressed in this publication are those of the authors and not necessarily of
the NHS Executive.
References
1. Thylefors B, Negrel A. The global impact of glaucoma. Bull World Health Org 1994;72:323-6.
2. Foster A, Johnson G. Magnitude and causes of blindness in the developing world. Int Ophthalmol 1990;14:135-40.
3. Quigley H. Number of people with glaucoma worldwide [see comments]. Br J OphthalmoI 1996;80:389-93.
4. Sommer A. Glaucoma: facts and figures. Doyne Lecture. Eye 1996;10:295-301.
5. Jay J. Rational choice of therapy in primary open angle glaucoma. Eye 1992;6:243-7.
6. Migdal C, Gregory W, Hitchings R Long-term functional outcome after early surgery compared with laser and medicine in open-angle glaucoma. Ophthalmology 1994;101:1651-fi.
7. Addicks E, Quigley H, Green W, Robin A. Histologic characteristics of filtering blebs in glaucomatous eyes. Arch Ophthalmol 1983;101:795-8.
8. Hitchings R, Grierson I. Clinicopathological correlation in eyes with failed fistulizing surgery. Trans Ophthalmol Soc UK 1983;103:84-8.
9. Stamper R, McMenemy M, Lieberman M. Hypotonous maculopathy after trabeculectomy with subconjunctival 5-fluorouracil. Am J Ophthalmol 1992;114:544-53.
10. Parrish R, Minckler D. 'Late endophthalmitis': filtering surgery time bomb? Ophthalmology 1996;103:1167-8.
11. Jampel H, Pasquale L, Dibernardo C Hypotony maculopathy following trabeculectomy with mitomycin C Arch Ophthalmol 1992;110:1049-50.
12. The Fluorouracil Filtering Surgery Study Group. Fluorouracil Filtering Surgery Study one-year follow-up. Am J Ophthalmol 1989;108:625-35.
13. Katz G, Higginbotham E, Lichter P, Skuta G, Musch D, Bergstrom T, et al. Mitomycin C versus 5-fluorouracil in high-risk glaucoma filtering surgery: extended follow-up. Ophthalmology 1995;102:1263-9.
14. Kitazawa Y, Kawase K, Matsushita H, Minobe M. Trabeculectomy with mitomycin: a comparative study with fluorouracil. Arch Ophthalmol 1991;109:1693-8.
15. Lamping K, Belkin J. 5-Fluorouracil and mitomycin C in pseudophakic patients. Ophthalmology 1995;102:70-5.
16. Khaw P, Doyle J, Sherwood M, Grierson I, Schultz G, McGorray S. Prolonged localized tissue effects from 5-minute exposures to fluorouracil and mitomycin C. Arch Ophthalmol 1993;111:263-7.
17. Crowston J, Akbar A, Constable P, Occleston N, Daniels J, Khaw P. Antimetabolites-induced apoptosis in Tenon's capsule fibroblasts. Invest Ophthalmol Vis Sci 1998;39:449-54.
18. Singer A, Clarke RA. Cutaneous wound healing. N Engl J Med 1999;341:738-46.
19. Clark R, Henson P. The molecular and cellular biology of wound repair. New York: Plenum Press, 1988.
20. Reichel M, Ali R, Thrasher A, Hunt D, Bhattacharya S, Baker D. Immune responses limit adenovirally mediated gene expression in the adult mouse eye. Gene Ther 1998;5:1038-46.
21. Khaw P, Occleston N, Schultz G, Grierson I, Sherwood M, Larkin G. Activation and suppression of fibroblast function. Eye 1994;8:188-95.
22. Occleston N, Tarnuzzer R, Munro P, Ravetto P, Ali R, Schultz G, et al. Inhibition of matrix metalloproteinase activity inhibits Tenon's capsule fibroblast mediated collagen contraction. Invest Ophthalmol Vis Sci 1995;36:S877.
23. Scott K, Wood E, Karran E. A matrix metalloproteinase inhibitor which prevents fibroblast-mediated collagen lattice contraction. FEBS Lett 1998;441:137-40.
24. Desmouliere A, Redard M, Darby I, Gabbiani G. Apoptosis mediates the decrease in cellularity during the transition between granulation tissue and scar. Am J Pathol 1995;146:56...u6.
25. Liu B, Connolly M. The pathogenesis of cutaneous fibrosis. Semin Cutan Med Surg 1998;17:3-11.
26. Fini E. Keratocyte and fibroblast phenotypes in the repairing cornea. Prog Retinal Eye Res 1999;18:529-51.
27. Broadway D, Grierson I, O'Brien C. Hitchings R. Adverse effects of topical anti-glaucomatous medication regimens. I. Effect on the cell profile of the conjunctiva. Arch Ophthalmol 1994;112:1446-54.
28. Broadway D, Grierson I, O'Brien C. Hitchings R. Adverse effects of topical antiglaucoma medication regimens. II. The outcome of filtration surgery. Arch Ophthalmol 1994;112:1437-45.
29. Broadway D, Grierson I, O'Brien C, Hitchings RA. Reversal of topical antiglaucoma medication effects on the conjunctiva. Arch OphthalmoI 1996;114:262-7.
30. Gwynn D, Stewart W, Pitts R, McMillian T, Hennis H. Conjunctival structure and cell counts and the results of filtering surgery. Am J Ophthalmol 1993;116:464-8.
31. Nuzzi R, Vercelli A, Finazzo C, Cracco C. Conjunctiva and subconjunctival tissue in primary open-angle glaucoma after long-term topical treatments: an immunohistochemical and ultrastructural study. Graefes Arch Clin Exp Ophthalmol 1995;233:154-62.
32. Occleston N, Alexander R, Mazure A, Larkin G, Khaw P. Effects of single exposures to antiproliferative agents on ocular fibroblast-mediated collagen contraction. Invest Ophthalmol Vis Sci 1994;35:3681-90.
33. Occleston N, Daniels J, Tarnuzzer R, Sethi K, Alexander R, Bhattacharya S, et al. Single exposures to antiproliferatives: long-term effects on ocular fibroblast wound-healing behaviour. Invest Ophthalmol Vis Sci 1997;38:1998-2007.
34. Daniels J, Occleston N, Crowston J, Khaw P. Effects of antimetabolite induced cellular growth arrest on fibroblast-fibroblast interactions. Exp Eye Res 1999;69:117-27.
35. Waterman-Storer C, Worthylake R, Liu B, Burridge K, Salmon E. Microtubule growth activates Rac1 to promote lamellipodial protrusion in fibroblasts. Nature Cell BioI 1999;1:45-50.
36. Metcalfe R, Weetman A. Stimulation of extraocular muscle fibroblasts by cytokines and hypoxia: possible role in thyroid-associated ophthalmology. Clin Endocrinol 1994;40:67-72.
37. Joseph J, Grierson I, Hitchings R. Taxo!, cytochalasin B and colchicine effects on fibroblast migration and contraction: a role in glaucoma filtration surgery? Curr Eye Res 1989;8:203-15.
38. Jampel H, Moon J. The effect of paclitaxel powder on glaucoma filtration surgery in rabbits. J Glaucoma 1998;7:170-7.
39. Jampel H, Thibault D, Leong K, Uppal P, Quigley H. Glaucoma filtration surgery in non-human primates using taxol and etoposide in polyanhydride carriers. Invest Ophthalmol Vis Sci 1993;34:3076-83.
40. Blagosoklonny M, Fojo T. Molecular effects of paclitaxel: myths and reality. Int J Cancer 1999;83:151-6.
41. Pleass R, Khaw P. Inhibition of remodelling and contraction in ocular wound healing. Keystone Symposium: Ocular cell and molecular biology, Colorado, 1999:37.
42. Daniels J, Khaw P. Synthetic matrix metalloproteinase inhibitor reduces contraction of cultured ocular tissue. Eur J Plast Surg 2000;in press.
43. Pilcher B, Wang M, Qin X, Parks W, Senior R, Welgus H. Role of matrix metalloproteinases and their inhibition in cutaneous wound healing and allergic contact hypersensitivity. Ann N Y Acad Sci 1999;878:12-24.
44. Skotnicki J, Zask A, Nelson F, Albright J, Levin J. Design and synthetic considerations of matrix metalloproteinase inhibitors. Ann N Y Acad Sci 1999;878:61-72.
45. De B, Natchus M, Cheng M, Pikul S, Almstead N, Taiwo Y, et al. The next generation of MMP inhibitors: design and synthesis. Ann N Y Acad Sci 1999;878:40-60.
46. McGuigan L, Mason R, Sanchez R, Quigley H. D-Penicillamine and beta-aminoproponitrile effects on experimental filtering surgery. Invest Ophthalmol Vis Sci 1987;28:1625-9.
47. Blumenkranz M, Ophir A, Claflin A, Hajek A. Fluorouracil for the treatment of massive periretinal proliferation. Am J Ophthalmol 1982;94:458-67.
48. Blumenkranz M, Hartzer M, Hajek A. Selection of therapeutic agents for intraocular proliferative disease. II. Differing antiproliferative activity of the fluoropyrimidines. Arch OphthalmoI 1987;105:396-9.
49. Chen C. Enhanced intraocular pressure controlling effectiveness of trabeculectomy by local application of mitomycin-Co Trans Asia Pacif Acad Ophthalmol 1983;9:172-7.
50. Doyle J, Sherwood M, Khaw P, McGoray S, Smith M. Intraoperative 5-fluorouracil for filtration surgery in the rabbit. Invest Ophthalmol Vis Sci 1993;34:3313-9.
51. Khaw P, Sherwood M, MacKay S, Rossi M, Schultz G. Fiveminute treatments with fluorouracil, floxuridine and mitomycin have long-term effects on human Tenon's capsule fibroblasts. Arch Ophthalmol 1992;110:1150-4.
52. Honjo M, Tanihara H, Inatani M, Honda Y. Mitomycin C trabeculectomy in eyes with cicatricial conjunctiva. Am J Ophthalmol 1998;126:823-4.
53. Ali-Hazmi A, Zwann J, Awad A, AI-Mesfer S, Mullaney P. Effectiveness and complications of mitomycin C use during pediatric glaucoma surgery. Ophthalmology 1998;105:1915-20.
54. Beck A, Wilson W, Lynch M, Lynn M, Noe R. Trabeculectomy with adjunctive mitomycin C in pediatric glaucoma. Am J Ophthalmol 1998;126:648-57.
55. Khaw P. What is the best primary surgical treatment for the infantile glaucomas? Br J Ophthalmol 1996;80:495...u.
545
546
56. Khaw P, Wilkins M, Shah P. Glaucoma surgery. In: Easty D, Sparrow J, editors. Oxford textbook of ophthalmology. Oxford: Oxford University Press, 1999: 1211-39.
57. Shin D, Reed S, Swords R, Reed A, Simone P, Birt C. Cellulose sponge punch for controlled mitomycin application. Arch Ophthalmol 1994;112:1624-5.
58. Wilkins M, Occleston N, Kotecha A, Waters L, Khaw P. Sponge delivery parameters and tissue levels of 5-fluorouracil. Br J Ophthalmol 2000;84:92-7.
59. Mehel E, Weber M, Stork L, Pechereau A. A novel method for controlling the quantity of mitomycin-C applied during filtering surgery for glaucoma. J Ocul Pharmacol Ther 1998;14:491-6.
60. Cordeiro M, Constable P, Alexander R, Bhattacharya S, Khaw P. The effect of varying mitomycin-C treatment area in glaucoma filtration surgery in the rabbit. Invest Ophthalmol Vis Sci 1997;38:1639-46.
61 . Miller M, Rice N. Trabeculectomy combined with beta irradiation for congenital glaucoma. Br J Ophthalmol 1991;75:584-90.
62. Constable P, Crowston J, Occleston N, Cordeiro M, Khaw P. Long term growth arrest of human Tenon's fibroblasts following single applications of beta radiation. Br J Ophthalmol 1998;82:448-52.
63. Constable P, Cordeiro M, Crowston J, Khaw P. The effects of single doses of beta irradiation on bleb survival and morphology in a rabbit model of filtration surgery. Invest Ophthalmol Vis Sci 1998;39(Suppl): abstract no. 3192.
64. Singh K, Group PTAS. Intraoperative 5-fluorouracil (5FU) vs mitomycin C (MMC) : the primary trabeculectomy antimetabolite study. Invest Ophthalmol Vis Sci 1999;40(Suppl) :abstract no.19.
65. Palmberg P, Escalona E, Norris E, Schiffman J. Long-term follow-up primary filtering surgery with mitomycin or 5-fluorouracil. Invest Ophthalmol Vis Sci 1999;40(Suppl):abstract no. 1416.
66. Finley C, Cantor L, Wudunn D, Hoop J, Lakhani V, Alvi N. Comparison of intraoperative 5-fluorouracil versus mitomycin C at six and twelve months in primary trabeculectomy. Invest Ophthalmol Vis Sci 1999;40(Suppl): abstract no. 5098.
67. AI-Aswad L, Huang M, Netland P. Inhibition of Tenon's fibroblast proliferation and enhancement of filtration surgery in rabbits with cytosine arabinoside. J Ocul PharmacoI 1999;15:41-9.
68. Denk P, Knorr M. In vitro effect of ascorbic acid on the proliferation of bovine scleral and Tenon's capsule fibroblasts. Eur J Ophthalmol 1998;8:37-41.
69 . Maignen F, Tilleul P, Billardon C. Xu-Van Opstal W, Pelaprat D, Elena P, et al. Antiproliferative activity of a liposomal delivery system of mitoxantrone on rabbit subconjunctival fibroblasts in an ex vivo model. J Ocul Pharmacol Ther 1996;12:289-98.
70. Akimoto M, Hangai M, Okazaki K, Kogishi J, Honda Y, Kaneda Y. Growth inhibition of cultured human Tenon's fibroblastic cells by targeting the E2F transcription factor. Exp Eye Res 1998;67:395-401 .
71 . Wahl S. Glucocorticoids and wound healing. In: Scleimer RP, Claman D, editors. Antiinflammatory steroid action: basic and clinical aspects. New York: Academic Press, 1989:280-302.
72. Miller M, Grierson I, Unger W, Hitchings R. The effect of topical dexamethasone and preoperative beta irradiation on a model of glaucoma fistulizing surgery in the rabbit. Ophthalmic Surg 1990;21 :44-54.
73. Araujo S, Spaeth G, Roth S, Starita R. A ten-year follow-up on a prospective, randomized trial of postoperative corticosteroids after trabeculectomy. Ophthalmology 1995;102:1753-9.
74. Giangiacomo J, Dueker D, Adelstein E. The effect of preoperative subconjunctival triamcinolone administration on glaucoma filtration. Arch Ophthalmol 1986;104:838-41.
75. Nguyen K, Lee D. Effect of steroids and nonsteroidal antiinflammatory agents on human ocular fibroblasts. Invest Ophthalmol Vis Sci 1992;33:2693-701 .
76. Migdal C . Hitchings R . The developing bleb: effect of topical antiprostaglandins on the outcome of glaucoma fistulizing surgery. Br J Ophthalmol 1983;67:655-60.
77. Snyder R, Lambrou F, Williams G. Intraocular fibrinolysis with recombinant human tissue plasminogen activator: experimental treatment in a rabbit model. Arch Ophthalmol 1987;105: 1277-80.
78. Lee P, Myers K, Hsieh M, Wood E, Hotaling D. Treatment of failing glaucoma filtering cystic blebs with tissue plasminogen activator (tPA). J Ocul Pharmacol Ther 1995;11 :227-32.
79. Azuara-Blanco A, Wilson R. Intraocular and extraocular bleeding after intracameral injection of tissue plasminogen activator. Br J Ophthalmol 1998;82;1345--6.
80. Lundy D, Sidoti P, Winarko T, Minckler D, Heuer D. Intracameral tissue plasminogen activator after glaucoma surgery: indications, effectiveness, and complications. Ophthalmology 1996;103:274-82.
81 . Zwann J, Latimer W. Topical tissue plasminogen activator appears ineffective for the clearance of intraocular fibrin. Ophthalmic Surg Lasers 1998;29:476-83.
82. WuDunn D. Intracameral urokinase for dissolution of fibrin or blood clots after glaucoma surgery. Am J Ophthalmol 1997;124:693-5.
83. Bramsen T. A double-blind study on the influence of tranexamic acid on the intraocular pressure and the central corneal thickness after trabeculectomy for glaucoma simplex. Acta Ophthalmol 1978;56:998-1005.
84. Bergers G, Javaherian K, Lo KM, Folkman J, Hanahan D. Effects of angiogenesis inhibitors on multistage carcinogenesis in mice. Science 1999;284:808-12.
85. D'Amore P. Mechanisms of endothelial growth control. Am J Respir Cell Mol Bioi 1992;6:1-8.
86. Favard C, Moukadiri H, Dorey C. Praloran V, Plouet J. Purification and biological properties of vasculotropin a new angiogenic cytokine. Bioi Cell 1991;73:1-6.
87. Liu J, Razani B, Tang S, Terman B, Ware J, Lisanti M. Angiogenesis activators and inhibitors differentially regulate caveolin-1 expression and caveolae formation in vascular endothelial cells. J BioI Chern 1999;274:15781-5.
88. Furlong R. The biology of hepatocyte growth factor / scatter factor. Bioessays 1992;14:613-7.
89. Paper D. Natural products as angiogenesis inhibitors. Planta Med 1998;64:686-95.
90. Dhanabal M, Ramchandran R, Waterman MJ, Lu H, Knebelmann B, Segal M, Skukhatme V. Endostatin induces endothelial cell apoptosis. J BioI Chern 1999;274:11721--6.
91. O'Reilly M, Boehm T, Shing Y, Fukai N, Vasios G, Lane W, et al. Endostatin: an endogenous inhibitor of angiogenesis and tumour growth. Cell 1997;88:277-85.
92. Liekens S, Neyts J, Degreve B, De Clercq E. The sulfonic acid polymers PAMPS poly(2-acrylamido-2-methyl-1-propanesulfonic acid)] and related analogues are highly potent inhibitors of angiogenesiS. Oncol Res 1997;9:173-9l.
93. Wong J, Wang N, Miller J, Schuman J. Modulation of human fibroblast activity by selected angiogenesis inhibitors. Exp Eye Res 1994;58:439-51 .
94 . Akbar A, Salmon M. Cellular environments and apoptosis: tissue microenvironments control activated T cell death. Immunol Today 1997;18:72-6.
95. Ellerby H, Arap W, Ellerby L, Kain R, Andrusiak R, Del Rio G, et al. Anti-cancer activity of targeted pro-apoptosic peptides. Nature 1999;5:1032-8.
96. Gillies M, Brooks A, Young S, Gillies B, Simpson L Goldberg 1. A randomized phase II trial of interferon-alpha 2b versus 5-fluorouracil after trabeculectomy. Aust N Z J Ophthalmol 1999;27:37-44.
97. Nguyen K, Hoang A, Lee D. Transcriptional control of human Tenon's capsule fibroblast collagen synthesis in vitro by gamma-interferon. Invest Ophthalmol Vis Sci 1989;35:3064-70.
98. Duncan M, Berman B. Differential regulation of collagen, glycosaminoglycan, fibronectin, and collagenase activity production in cultured human adult dermal fibroblasts by interleukin I-alpha and beta and tumor necrosis factoralpha and beta. J Invest Dermatol 1989;92:699-706.
99. Berman B, Duncan M. Short-term keloid treatment in vivo with human interferon alfa-2b results in a selective and persistent normalization of keloidal fibroblast collagen, glycosaminoglycan, and collagenase production in vitro. J Am Acad Dermatol 1989;21 :694-702.
100. Kahan A, Amor B, Menkes C, Strauch G. Recombinant interferon-gamma in the treatment of systemic sclerosis. Am J Med 1989;87:273-7.
101. Petri J, Schurk S, Gebauer S, Haustein U. Cyclosporine A delays wound healing and apoptosis and suppresses activin beta-A expression in rats. Eur J Dermatol 1998;8:104-13.
102. Nuzzi R, Cerruti A, Finazzo C. Cyclosporine C: a study of wound-healing modulation after trabeculectomy in rabbit. Acta Ophthalmol Scand 1998;227(Suppl):48-9.
103. Massague J . The transforming growth factor-beta family. Annu Rev Cell BioI 1990;6:597-641 .
104. Roberts A , Sporn M , Assoian R, Smith L Roche N . Transforming growth factor beta: rapid induction o f fibrosis and angiogenesis in vivo and stimulation of collagen formation in vitro. Proc Natl Acad Sci USA 1986;83:4167-71 .
105. Critchlow M, Bland Y, Ashhurst D. The effect of exogenous transforming growth factor-beta 2 on healing fractures in the rabbit. Bone 1995;16:521-7.
106. Cordeiro M, Reichel M, Gay L D'Esposita F, Alexander R, Khaw P. TGF-131, -132 and -133 in vivo: effects on normal and mitomycin-C modulated conjunctival scarring. Invest Ophthalmol Vis Sci 1999;40:1975-82.
107. Cordeiro M, Bhattacharya S, Schultz G, Khaw P. TGF-l3l, -132 and -133 in vitro: biphasic effects on Tenon's fibroblast contraction, proliferation and migration. Invest Ophthalmol Vis Sci 2000;41:756-63.
108. Connor T, Roberts A, Sporn M, Danielpour D, Dart L, Michels R, et al. Correlation of fibrosis and transforming growth factor-beta type 2 levels in the eye. J Clin Invest 1989;83:1661-6.
109. Jampel H, Roche N, Stark W, Roberts A. Transforming growth factor-beta in human aqueous humor. Curr Eye Res 1990;9:963-9.
110. Shah M, Foreman D, Ferguson M. Neutralising antibody to TGF-beta 1,2 reduces cutaneous scarring in adult rodents. J Cell Sci 1994;107:1137-57.
111 . Shah M, Foreman D, Ferguson M. Neutralisation of TGF-beta 1 and TGF-beta 2 or exogenous addition of TGF-beta 3 to cutaneous rat wounds reduces scarring. J Cell Sci 1995;108:985-1002.
112. Cordeiro M, Gay L Khaw P. Human anti-TGF-132 monoclonal antibody: a new anti-scarring agent for glaucoma filtration surgery. Invest Ophthalmol Vis Sci 1999;40:2225-34.
113. Wu-Pong S, Weiss T, Hunt C. Antisense c-myc oligonucleotide cellular uptake and activity. Antisense Res Dev 1994;4:155-63.
114. Adachi S, Maruyama T, Kondo T, Todoroki T, Fukao K. The prevention of postoperative intraperitoneal adhesions by tranilast, N-(3',4' -dimethoxycinnamoyl)anthranilic acid. Surg Today 1999;29:51-4.
115. Ito S, Sakamoto T, Tahara Y, Goto Y, Akazawa K, Ishibashi T, et al. The effect of tranilast on experimental proliferative vitreoretinopathy. Graefes Arch Clin Exp Ophthalmol 1999;237:691-6.
116. Takehana Y, Kurokawa T, Kitamura T, Tsukahara Y, Akahane S, Kitazawa M, et al. Suppression of laser-induced choroidal neovascularization by oral tranilast in the rat. Invest Ophthalmol Vis Sci 1999;40:459-66.
1 17. Furukawa H, Nakayasu K, Gotoh T, Watanabe Y, Takano T, Ishikawa T, et al. Effect of topical tranilast and corticosteroids on subepithelial haze after photorefractive keratectomy in rabbits. J Refract Surg 1997;13(Suppl):S457-8.
118 . Chihara E, Dong L Ochiai H. Effect of TGF-131 suppressor Tranilast on filtering bleb and lOP after glaucoma surgery. Invest Ophthalmol Vis Sci 1999;40(Suppl) :abstract no. 5104.
119. Kim H, Peterson T, Barnes S. Mechanisms of action of the soy isoflavone genistein: emerging role for its effects via transforming growth factor beta signalling pathways. Am J Clin Nutr 1998;68(Suppl):SI418-25.
120. Krott R, Lebek L Grisanti S, Luke C, Esser P, Kriegelstein G. Antiproliferative effect of Genistein in cultured human Tenon-fibroblasts. Invest Ophthalmol Vis Sci 1999;40(Suppl):abstract no. 5117.
121 . Mietz H, Chevez-Barrios P, Feldman R, Lieberman M. Suramin inhibits wound healing following filtering procedures for glaucoma. Br J Ophthalmol 1998;82:816-20.
122. Beardsley T. Making antisense. Sci Am 1992;3:107-8.
123. Fakler B, Herlitze S, Amthor B, Zenner H, Ruppersberg J. Short antisense oligonucleotide-mediated inhibition is strongly dependent on oligo length and concentration but almost independent of location of the target sequence. J Bioi Chern 1994;269:16187-94.
124. Sugawa N, Ueda S, Nakagawa H, Nishino H, Nosaka K, Iwashima A, et al. An antisense EGFR oligodeoxynucleotide enveloped in Lipofectin induces growth inhibition in human malignant gliomas in vitro. J Neurooncol 1998;39:237-44.
125. Wilson C, Szostak J. In vitro evolution of a self-alkylating ribozyme. Nature 1995;374:777-82.
126. Moore M. Exploration by lamp light. Nature 1995;374:766-7.
127. Bartel D, Szostak J. Isolation of new ribozymes from a large pool of random sequences. Science 1993;261:1411-8.
128. Altman S. RNA enzyme-directed gene therapy. Proc Natl Acad Sci USA 1993;90:10898-900.
129. Dorai T, Kobayashi H, Holland L Ohnuma T. Modulation of platelet-derived growth factor-beta mRNA expression and cell growth in a human mesothelioma cell line by a hammerhead ribozyme. Mol PharmacoI 1994;46:437-44.
130. Drenser K, Timmers A, Hauswirth W, Lewin A. Ribozymetargeted destruction of RNAs associated with ADRP. Invest Ophthalmol Vis Sci 1998;39:681-9.
131 . Lewin A, Drenser K, Hauswirth W, Nishikawa S, Yasumura 0, Flannery L et al. Ribozyme rescue of photoreceptor cells in a transgenic rat model of autosomal dominant retinitis pigmentosa. Nature Med 1998;4:967-71 .
132. Ren X, Schultz G. Reduction of transforming growth factor beta-1 protein in cells transfected with plasmids expressing hammerhead and hairpin ribozymes. Invest Ophthalmol Vis Sci 1999;40(Suppl):46.
547