social aspects of malaria in heping, hainan
TRANSCRIPT

Acta Tropica, 59(1995)41-53 41 © 1995 Elsevier Science B.V. All rights reserved 0001-706X/94/$09.50
ACTROP 00451
Social aspects of malaria in Heping, Hainan
Tang Linhua a*, Lenore M a n d e r s o n b', D e n g Daa,Wu Kaichen b, Cai Xianzheng% Lan Changxiong c, G u Zhengcheng ~ and Wang Ke-an d
alnstitute of Parasitic Diseases, Chinese Academy of Preventive Medicine, 207 Rui Jin Er Lu, Shanghai 200025, China
bTropieal Health Program, University of Queensland Medical School, Brisbane, Herston Road, Herston 4006, Qld Australia
~Hainan Provincial Institute of Tropical Diseases, Haikou, China dChinese Academy of Preventive Medicine, Belting, China
(Received 8 December 1994; Accepted 19 December 1994
Abstract This paper presents findings from a study conducted in Heping Town, Qiongzhong County, Hainan
Province, China. The study, conducted in 1992, used qualitative as well as quantitative methods to gather social, cultural and behavioural data associated with the acquisition, transmission and prevention of malaria, and the diagnosis and treatment of disease. These methods included focus groups, key informant and other in-depth interviews, and observations, a household survey and tests of school children of knowledge of malaria. The study is among the first to our knowledge that has utilized this broad mix of methods for tropical disease research in China.
Key words: Malaria; Social risk factors of infection; Cultural and behavioral factor; Community
1. Introduction
Malaria continues to be a major public health problem world-wide. Biological, medical and economic problems have impeded its eradication; these problems include the high cost and logistic problems associated with environmental management limiting the efficacy of currently available control measures, mosquito resistance to DDT, and transmission of malaria to non-immune populations as a result of increased population mobility to and from endemic areas (Gomes, 1993). Additional problems are associated with the delivery of health services and diagnostic services, and the irrational use of anti-malarials implicated in the development of parasite resistance to such drugs. Community participation for environmental control, aimed at reducing vector breeding sites, has also been problematic and the sustain- ability of such programs remains questionable (Manderson, 1992; Sornmani and Manderson, 1992). In the absence of a vaccine or cost-effective means of vector control, social and behavioural interventions at a household level are the most viable means of controlling malaria; these include the timely diagnosis and appropriate
*Corresponding author
SSDI 0001-706X (94) 00086-7

42
treatment of malaria and the use of bed nets to avoid mosquito bites and hence reduce transmission.
Social and economic research issues relevant to understanding the transmisson, diagnosis, treatment and prevention of malaria, including in relation to these house- hold interventions, have been described by a number of authors (Rosenfield et al., 1981; Rosenfield et al., 1984; Koss and Kloos, 1989; Singer, 1989; Vlassoff, 1991; Gomes and Litsios, 1993). Although compared to some other infectious diseases, empirical research is limited, a number of studies have now been published that document the direct and indirect costs of malaria to communities (e.g. various papers in Gomes, 1993; Ruiz and Kroeger, 1994), that describe folk understandings of malaria and the implications of this for diagnosis and treatment (e.g. Agyepong, 1992; Helitzer-Allen et al., 1993; Helitzer-Allen et al., 1993; Manderson and Agyepong, in press), and have addressed strategies aimed at reducing transmission, improving case detection and treatment, and ensuring the cost-effectiveness of such approaches (Kaewsonthi et al., 1984; Ettling et al., 1989; Ruebush et al., 1990; Okanurak et al., 1991; Mills, 1992).
In China, endemicity of malaria is low and hence household interventions are in theory the most cost-effective means of control. In line with world-wide interest in bed net acceptability and use, particularly as a result of the apparent success in The Gambia of the use of insecticide-impregnated bed nets in reducing child mortality (Snow, 1988; MacCormack et al., 1989; Alonso et al., 1990; Gyapong et al., 1992; Greenwood and Baker, 1993), there has been interest especially in the applicability of bed nets in China. Field trials of insecticide-impregnated bed nets have demon- strated a reduction in vector density and incidence of malaria (Li et al., 1989; Curtis et al., 1990), and their use, combined with prompt treatment of clinical malaria, appears to be most appropriate in areas where malaria continues to be transmitted. This includes Hainan Province, the site of the study reported in this paper.
2. Background
Hainan Island, in the far south of China, is endemic for malaria. Qiongzhong County, where field research was conducted, in the past was hyperendemic; the central highway that transects the island and the county, built in the 1950s, is reputed to have claimed one life from malaria for each kilometer of road laid. A survey conducted in 1956 in the neighbouring county of Baisha, among a population of 435, indicated a parasite rate of 91% (China, Institute of Parasitic Diseases, 1957). Although DDT spraying in the late 1950s and early 1960s led to a dramatic decline in the main vector population and consequently in the prevalence of malaria through- out the province, effectively eliminating the disease from mesoendemic areas, still over 10.3% of all malaria cases in China, and 40.7% of cases of Plasmodium falciparum malaria, occur here. Transmission remains especially high in Qiongzhong and adjacent counties (Deng et al., 1991; Wu et al., 1992).
The primary burden of malaria infection and disease is carried by the Li and Miao minorities; this paper is concerned with these groups. Li people comprise approximately 15% of Hainan's population (c. 1 million of a total of 6.7 million). Most live in the hinterland hills and lower levels of the mountains of Qiongzhong, Baisha, Baoting and Dongfang Counties, and Tongzha City, practising - depending

43
on altitude - wet or dry rice farming and supplementing this through hunting, gathering and the cash crop production of cassava, rubber and tea (Liao, 1991). The Miao, comprising only 50 000 people, live in the highest levels of the mountains of these counties and are predominantly shifting agriculturalists who supplement dry rice production through hunting and gathering. The use of forest resources by both Li and Miao to gather subsistence foodstuffs, to generate some income (for example, collecting wild vegetables and hunting wild boar for sale to restaurants), to collect fuel, and to maintain hill rice and other crops, renders them especially vulnerable to malaria from the primary vector, Anopheles dirus, which resides in mountain fields and forests. Anopheles minimus has also been an important vector in this area in the past, although its population has decreased over recent years.
3. Research methods
Qiongzhong County comprises a small population of 200 000, one-sixth of whom live and work as production teams of the state farms (e.g. Chengpo Farm). Heping Township in this county consists of a population of 6175, which includes 42 rural villages, of which 39 have road access, 22 electricity, and 12 with piped water.
The res.zarch was conducted in 6 villages of Heping Town and 3 production teams (residential areas) of Chengpo Farm (hereafter, referred to as "farms"), sampled purposively to take account of geography and prevalence (Fig. 1). A total of 226 households, totalling 1100 persons, were investigated in four residential areas, each ethnically homogenous and of which two were Li, one Miao and one Han. One Li study site (5 villages: Yiazhao, Xingxingli, Beiwan, Gexin, Shunzuo) and one Miao study site (1 village: Xingxingmiao) were natural villages, within which production and hence income is privatized, with a mix of subsistence and income-generating activity. The second Li site (1 residential area: No. 27 production team) and the Hart study site (2 residential areas: No. 7 and No. 26 production team) were farms, where income generated from the sale of cash crops is equally distributed among all workers. As we shall describe below, the differences in wealth between villages and farms are marked. As a consequence of sampling procedure, the study data enables us to differentiate not only between ethnicity or "minority status", but also according to socio-economic status.
Both qualitative and quantitative research methods were used in this study, which allowed the research team to collect quantifiable data and to gain in-depth informa- tion about the social, economic and personal context of reported behaviour. Based on earlier work in the field, a questionnaire was developed for a household survey, with revisions made to the study protocol after arrival in the field; survey households were randomly selected within the study villages. In-depth interviews and focus group discussions were held to explore issues that arose from the survey instrument and to identify new areas for enquiry, thus facilitating iteration (Jick, 1979). In-depth interviews were also conducted specifically on the diagnosis and management of malaria and strategies of resort for treatment. Five focus groups of 8-9 participants each were conducted, one in a Miao village, two in Li villages, one in a combined Li and Han farm, and one with village health workers. The latter focus group was designed to explore issues related to the role of the primary health care system in the prevention, diagnosis and treatment of malaria. A separate questionnaire, estab-

44
I o.,NA I
Beibu Gulf
1123m X
Haikou Yiazhao
Hainan Island
1867m A Wuzhi Mountain~
Fig. 1. Map of Heping District, Hainan Province
lishing the level of knowledge of malaria, was administered to primary and secondary school children (n = 251) and to health workers. Finally, a malariometric survey was conducted to establish the malaria parasite rate and malaria antibody (IFA) levels in the study sites, and data were collected with regard to malaria incidence and the mosquito vector.
4. The study community
Details of survey households, and summary of demographic and socio-economic data, are set out in Table 1. The table indicates disparity between people according to both social status (ethnicity) and mode of production. This is indicated by housing type (cement-rendered brick walls with rooves, predominant on the state farm, compared with bamboo-slat or mud and fibre walls with a thatch roof, typical in the Miao and Li villages). It is also indicated by income. However, the measure presented here - per capita income - is not a good equivalent of disposable household
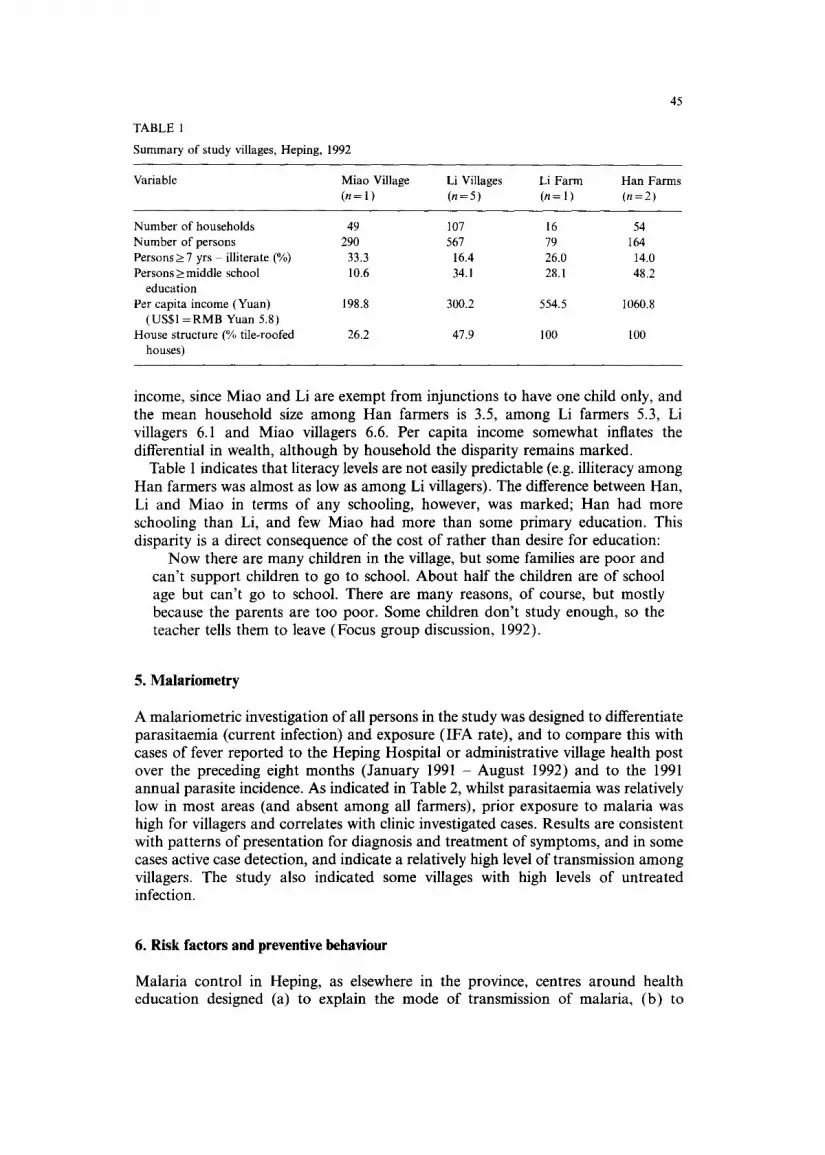
TABLE 1
Summary of study villages, Heping, 1992
45
Variable Miao Village Li Villages Li Farm Han Farms (n = 1 ) (n = 5) (n = 1 ) (n =2)
Number of households 49 107 16 54 Number of persons 290 567 79 164 Persons>7 yrs illiterate (%) 33.3 16.4 26.0 14.0 Persons _> middle school 10.6 34.1 28.1 48.2
education Per capita income (Yuan) 198.8 300.2 554.5 1060.8
(US$1 = RMB Yuan 5.8) House structure (% tile-roofed 26.2 47.9 100 100
houses)
income, since Miao and Li are exempt from injunctions to have one child only, and the mean household size among Han farmers is 3.5, among Li farmers 5.3, Li villagers 6.1 and Miao villagers 6.6. Per capita income somewhat inflates the differential in wealth, although by household the disparity remains marked.
Table 1 indicates that literacy levels are not easily predictable (e.g. illiteracy among Han farmers was almost as low as among Li villagers). The difference between Han, Li and Miao in terms of any schooling, however, was marked; Han had more schooling than Li, and few Miao had more than some primary education. This disparity is a direct consequence of the cost of rather than desire for education:
Now there are many children in the village, but some families are poor and can't support children to go to school. About half the children are of school age but can't go to school. There are many reasons, of course, but mostly because the parents are too poor. Some children don't study enough, so the teacher tells them to leave (Focus group discussion, 1992).
5. Malariometry
A malariometric investigation of all persons in the study was designed to differentiate parasitaemia (current infection) and exposure (IFA rate), and to compare this with cases of fever reported to the Heping Hospital or administrative village health post over the preceding eight months (January 1991 - August 1992) and to the 1991 annual parasite incidence. As indicated in Table 2, whilst parasitaemia was relatively low in most areas (and absent among all farmers), prior exposure to malaria was high for villagers and correlates with clinic investigated cases. Results are consistent with patterns of presentation for diagnosis and treatment of symptoms, and in some cases active case detection, and indicate a relatively high level of transmission among villagers. The study also indicated some villages with high levels of untreated infection.
6. Risk factors and preventive behaviour
Malaria control in Heping, as elsewhere in the province, centres around health education designed (a) to explain the mode of transmission of malaria, (b) to

46
TABLE 2
Malariometric investigation by type of residential area, Heping District, 1992
Type of residents Miao village Li villagers Li farmers Han farmers
No of residential spots surveyed 1 5 1 2 No of persons surveyed 290 567 79 164 Parasite rates % 1.8 2.9 0 0 IFA rates (>__ 1:40) 24.2 20.1 10.2 2,1 Annual incidence in 1991 (%) 16.9 9.5 0.9 0.4 % of population with malaria 22.4 25.2 13.9 1.2
history, 1991-1992
encourage people to present themselves at clinics for blood smears, and where positive identification is made, for treatment (as first line drugs, with chloroquine and primaquine for P. vivax and piperaquine for P. falciparum), and (c) to sleep under impregnated bed nets. These interventions are supplemented by some residual spraying of houses and mountain huts and by occasional focal spraying. The ideal with respect to community participation has been that villagers assist in the impreg- nation of nets (as depicted in malaria control program posters displayed in village health centres), although in practice the nets are dipped annually by Anti-Epidemic Station staff with the assistance of the village health workers.
The provision of primary health care services is central to the effectiveness of these measures. In total, there are 73 "residential spots" or natural villages in Heping (including Chengpo Farm). Table 3 summarizes the primary health care facilities available to each, and indicates the advantage of farm residence in terms of access to care. This is significant given the higher use by farm workers of health facilities, as reflected in this table and as discussed below in terms of malaria treatment.
7. Knowledge of malaria
Table 4 summarizes risk factors and preventive behaviours, focusing on knowledge of transmission of malaria, presentation of signs of fever and health seeking behavi- our, ownership and use of nets, and temporary mountain residence. As indicated, the survey indicated that around half the respondents had heard of malaria. This needs amplification. Firstly, the question varied to take account of differences in language. Han respondents were asked whether they had heard of nueji, Li
TABLE 3
Primary health care services in villages and state-run farms in Heping District
Place Heping town Chengpo farm
No. of residential spots No. of health workers % of health workers with certificate No. of residential spot per health workers No. of consultations (per health workers per month)
42 31 13 31 23,1 67.7
3.2 1 36.7 187.7

TABLE 4
Risk factors and preventive behaviour, Heping, 1992
47
Variable Miao Village Li Villages Li Farms Han Farms (n = 1 ) (n = 5) (n = 1 ) (n = 2)
Household heads who knew 57.1 41.4 56.2 64.0 malaria was transmitted by mosquitoes (%)
Household heads who would 76.3 89.5 100 100 seek medical advice if someone were ill (%)
Number of nets owned per 0.47 0.5 0.66 0.63 person
Reported utilisation rate of nets 85.0 76.1 84.6 91.1 (%)
Observed utilisation rate of nets 79.2 64.4 70.4 81.5 (%)
Persons who ever stayed 29.0 17.5 14.8 7.4 overnight in forest (%)
respondents baigua, and Miao respondents fusang. The terms used in Han and Li appear to be used exclusively for "malaria", and are a reasonable gloss for clinical malaria. However, the Miao term fusang is used for any variation in temperature (hot-cold) and so might be understood to refer to fevers other than or in addition to malaria. Further research is required to explore this point.
8. Health-seeking behaviour
Survey questions tend to result in responses about health-seeking behaviour that indicate that the interviewer is seeking information regarding use of formal health services. Data on health seeking behaviour in this study derives from the household survey, and consequently results indicate extremely high and prompt use of village- based clinical services in the event of fever. Respondents claimed that persistent fever, or fever with other signs (e.g. headache) would lead them to present for diagnosis and medication. Respondents were familiar with anti-malarials for prophy- lactic and therapeutic use, and were disinclined to delay presentation except where the health services were at a considerable distance from their home, or when the person with symptoms was in a mountain hut if working in upland fields, hence far from his usual residential village.
Table 4 indicates simply whether people would seek medical advice if ill. In Table 5, however, health-seeking behaviour with particular reference to malaria is amplified, with respect to those respondents who reported having had malaria in 1991 or 1992 (221 persons, 20.1%). There were few cases of farmers who had malaria, and all claimed that they had sought medical care, been tested to confirm malaria, and had complied with chemotherapy. Villagers were less likely to seek attention (although only around 5% did not), and there were fewer cases of microscopy confirmation of parasitaemia. This is consistent with data for clinical cases from Heping Town Hospital (for Li and Miao villagers) and Chengpo Farm Hospital (for Han and Li

48
TABLE 5
Diagnosis and treatment of malaria, Heping, 1992
Types of residents Miao villages Li villages Li farmers Han farmers
No. of persons surveyed 290 567 79 164 No. of persons with history of 65 143 11 2
malaria % of people seeking medical 95.3 94.2 100 100
care % of people who received blood 85.9 75.9 100 100
e x a m .
% of people taking 92.2 94.2 100 100 antimalarials
% of people taking drugs for 3 45 71.7 100 100 days
farmers) for 1990 and 1991, which indicate that blood examination was undertaken by health workers in 82.2 and 93.2 percent of cases (for Heping Town and Chengpo Farm respectively) in 1990, and 85.2 and 91.5 percent in 1991. Further, although all but one village had a village doctor and so people could be treated without travelling away from home, compliance rates for the full course were poor especially among the Miao (45% only completed the course).
9. Prevention
The primary behavioural means of reducing transmission of infection, hence morbid- ity in the community, is the promotion of use of impregnated bed nets. As Table 4 indicates, the ratio of nets to people is around 1:2.0, and this is relatively high compared with some adjacent counties, where it decreases to around 1:2.6. Householders were asked the number of bed nets they owned, and whether they used them; responses were validated through night-time spot checks of sleeping behaviour at 11 p.m. Use of nets was significantly lower than reported use (x2= 15.6, P<0.01).
10. Mountain-stays
A number of earlier studies have pointed to the impact on malaria transmission of population mobility, both in the context of resettlement (e.g. Prothero, 1965; Sawyer, 1993; Fernandez Castilla and Sawyer, 1993), and circular migration and local population movement determined by various economic and other uses of different micro-environments (e.g. Sornmani et al., 1983; Sevilla-Casas, 1993; Singhanetra- Renard, 1993). In Heping, among both Li and Miao people, residential and agricul- tural land is separate. Usually villages are located at lower altitudes than rice fields, and farmers stay in mountain huts when maintaining land, planting or harvesting rice. From this mountain base, too, they hunt and gather other forest food. This is particularly the case for the Miao, who have recently moved residential villages

49
nearer to other settlements whilst maintaining upland fields and continuing to use high altitude forests for hunting and gathering.
In this study, 29.0% of Miao villagers, on the basis of case investigation, acquired malaria in the forest, and this was an important pattern of malaria infection also among the Li. Whilst in Heping malaria was primarily transmitted in and around the village, forest-acquired malaria proved also to be important, and the use of bed nets and other methods to avoid bites in the mountains as well as in residential villages is clearly an issue for control. In order to explore further the link between mobility and infection, statistical analysis (Grey relational analysis, Deng, 1985; this approach is used extensively in China to explore the association between variables, including in demographic, agricultural and social science research) was conducted to establish the strength of association between infection and various risk factors. As indicated in Table 6, factors most strongly associated with malaria infection were staying in the mountains (r=0.869) and reported bed net use (r=0.827). Other factors - use of health services, ownership of nets, knowledge of malaria, socio-economic indicators of housing type, and per capita income - were less strongly associated although still significant.
The significance of associations between the IFA rate, used as a proxy of prior infection, and social and behavioural factors, indicate that place of sleep (staying in the mountains) and use of bed nets were the major factors affecting malaria transmis- sion and control. Thus, of the 151 persons who had stayed in the mountains overnight, the IFA rate was 25.8%, compared with 15.6% among those who had not done so (P<0.005); of the 717 person who reported frequent use of bed nets and those who did not, the IFA rate was 14.0% and 34.2% respectively (P<0.001).
11. Discussion
The significance of factors used as indexes of socio-economic status and of relevance to the prevention of malaria is as follows. Firstly, the open walls of the bamboo-
TABLE 6
Association between socioeconomic and behavioural factors, and malaria IFA rates in Heping District
Types of residents Miao villages Li villages Li farms Han farms
1FA (%) x 0 24.2 20.1 10.2 2.1 % of people staying in x 1 29.0 17.6 14.8 7.4
mounta ins % of bednet users × 2 85.0 76.1 84.6 91.1 % of households x 3 76.3 89.5 100 100
seeking medical advice
No of bednet/persons × 4 0.47 0.50 0.63 0.66 % of householdes with x 5 57.1 41.4 56.2 64.0
malaria knowledge % of households with × 6 26.2 47.9 100 100
tile-roofed houses Per capita income yuan × 7 198.9 300.2 554.5 1060.8
(RMB)

50
slat houses in particular present a problem for endophagic mosquitos, since access is very easy. Mud-plastered and cement-rendered walls, whilst they make the houses dark and hotter, discourage mosquitos. Against this, villages occasionally build shelters on poles about 10 feet off the ground, where children may rest and sleep in the cool of the evening before being removed to sleep under the net, and are at risk of being bitten there. In addition, the cost of housing more substantial than bamboo or wooden plank houses can amount to around 10 000 yuan (US$1724), well beyond the reach of most villagers.
Literacy was explored because of its possible association with knowledge of the transmission of malaria, and therefore the possible greater uptake of health education advocating treatment for fever and bed net use; in addition the poster used at the time of the study to promote bed net use included text in support of photographs. There was some association between literacy and bed net use, but this was not statistically significant.
Income data were collected because of the question of affordability of nets (the cost of a net at the time of the survey was 40 yuan (c.US$7) for a single bed net, 60-80 Yuan for a bed net to fit a double bed) and people's willingness to spend limited cash resources on bed nets, as well as the influence of disposable income on visits to the clinic and purchase of drugs. As already noted, per capita income is not equivalent to household income, and this measure does not take account of subsistence production. All communities produced at least some food for household use rather than cash sale, but even so there was a marked disparity in disposable wealth by ethnicity. The relatively high level of Han income was primarily due to income generating activities supplementary to rice production on the state farm, including growing rubber and other agricultural cash crops. However, income was not predictive of nor related to bed net use.
Models of health behavior have in the past operated on the supposition of a lineal relationship between knowledge and practice (Tang et al., 1990), but our data suggests that this is not absolutely true. Far more respondents in the survey presented for diagnosis and treatment following onset of malaria symptoms than were able to describe malaria or its association with mosquitos. Here, the most significant factor appeared to be the perceived efficacy of antimalarials, as with other pharmaceuticals, rather than an understanding of the relationship between transmission, infection, symptoms and treatment. However, respondents' claims that they seek medical care for fever do not always describe practice. First, interviews with extensive probes would yield a more complex set of behaviours, and draw attention to some house- hold-based herbal treatment at the outset of fever. Both herbal drinks (prepared from herbs either growing around the village or in the mountains) and commercial rubifacients are used, which when ingested or applied, enable temporary management of fever. Second, data from Chengpo Farm Hospital (where microscopy is provided
for both Li and Han farmers) and Heping Town Hospital (for villagers) indicate delayed presentation of 2.2 and 2.5 days respectively for the years 1990 and 1991. Delay in presentation to the town hospital for Miao villagers relates to concern about service provision and personal safety. However, some malaria knowledge was predictive of bed net use (x2=11.4791, P = <0.001); the only other statistically significant factor related to bed net use was age (x 2= 35.4478, P = <0.0001), with children < 10 years of age most likely to sleep under nets.
Bed net use (reported, and more significantly observed) exceeded knowledge of

51
malaria transmission, indicating that the general message ("use bed nets to avoid bites") was effective without people necessarily comprehending the rationale that lay behind the preventive measure. However, observed bed net use was significantly lower than reported use. The following account, collected in a post-survey evaluation interview, provides one reason for preferred non-use of the nets and highlights the difficulty in uptake of nets:
The husband recounted that, when the net was first impregnated with insecti- cide (deltamethrin), it smelt badly, although the smell faded after about three days. However, because of the smell, and because the net made him feel hot, he moved from the marital bed to sleep on the bench in the adjacent reception hall. His wife continued to sleep under the net, "to avoid being bitten by mosquitoes". The husband continued to sleep separately, without protection, because, he said, he was "healthy and so won't get sick anyway". This account identifies several issues worth further exploration. First, smell from
insecticide and feeling hot when sleeping under the net discourage net use; these are common complaints and difficult to counter. Second, there is no necessary association in the minds of villagers between bed net use and disease protection; the nets may be accepted or rejected because of the perceived nuisance of mosquitoes. Third, people do not necessarily understand that mosquitos are the vector of malaria, although this does not predict acceptance of nets or treatment-seeking for signs of malaria. Fourth, general health status and vulnerability to malaria infection may be confused: the man in the above account presumed his good health status was protective. Further, the comment suggests the need for a fuller exploration of sleeping patterns by sex.
Finally, it is not clear that people appreciate that a single bite from an infected mosquito is all that is necessary for transmission of infection. This becomes important in accounting for infections that occur despite bed net use (when biting occurs when the person is out of the net) and in explaining the value of impregnation to ensure "knock-down" of mosquitos poised on the surface of the net. Given vectorial habitat and behaviour, the use of nets may be the most cost effective means of malaria control, but uptake appears to be still too low to effect control.
Whilst some of these factors (social and environmental) do not lend themselves to interventions, the figure and this study highlight areas where interventions may be effective. In particular, there is a clear need to document further risks associated with mountain stays, and to develop both appropriate and acceptable interventions to reduce transmission among this mobile population.
Acknowledgement
This investigation received financial support from the UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases (WHO/TDR).
References
Agyepong, 1.A. (1992) Malaria: Ethnomedical perceptions and practice in an Adangbe farming com- munity and implications for control. Soc. Sci. Med. 35~ 131-137.

52
Agyepong, I.A. and Manderson, L. 0 The diagnosis and management of fever at household level in the Greater Accra Region, Ghana. Acta Trop. 58, 317-330.
Alonso, P.L., Lindsay, S.W., Armstrong, J.R.M., Conteh, M., Hill, A.G., David, P.H., Fegan, G., De Francisco, A., Hall, A.J., Shenton, F.C., Cham, K. and Greenwood, B.M. (1990) The effect of insecticide-treated bed nets on mortality of Gambian children. The Lancet 337, 1499-1502.
China, Institute of Parasitic Diseases, Department of Malaria (1957) Field trials of the chloroquine single dose treatment. Annual Report oflnstitute of Parasitic Diseases, Shanghai: Chinese Academy of Medical Sciences, pp. 168-182.
Deng, D., Cai, X., Qian, H., Wu, K., Liu, C., Lan, C., Tang, L , Wang, K., Chen, W., Wang, Z. and Lin, X. (1991 ) Epidemiological study of malaria in Hainan Province. Proceedings of 11 th International Conference on Agricultural Medicine and Rural Health, Beijing, 94-95.
Deng, J. (1985) Hui Se Xi Tong - She Hui, Jing Ji (Grey system for social and economic data) (lst ed.). Beijing: Guo Fang Gong Ye Chu Ban She.
Curtis, C.F., Lines, J.D., Carnevale, P., Robert, V., Boudin, C., Haina, J.-M., Pazart, L., Gazin, P., Richard, A., Mouchet, J., Charlwood, J.D., Graves, P.M., Hossain, M.I., Kurihara, T., Ichimori, K., Li, Z., Lu, B., Majori, G., Sabatinelli, G., Coluzzi, M., Njunwa, K.J., Wilkes, T.J., Snow, R.W. and Lindsay, S.W. (1990) Impregnated bed nets and curtains against malaria mosquitoes. In Curtis, C.F. (Ed.) Appropriate Technology in Vector Control, Boca Raton, FI. CRC Press.
Etthng, M.B., Thimasarn, K., Krachiklin, S. and Bualombai, P. (1989) Evaluation of malaria clinics in Maesot, Thailand: use of serology to assess coverage. Trans. R. Soc. Trop. Med. Hyg. 83, 325-330.
Fernandez Castilla, R.E. and Sawyer, D.O. (1993) Malaria rates and fate: a socioeconomic study of malaria in Brazil. Soc. Sci. Med. 37, 9, 1137-1146.
Gomes, M. (Guest Ed.). Malaria. Special issue of Soc. Sci. Med. 37, 9. Gomes, M. and Litsios, S. (1993) Introduction. Soc. Sci. Med. 37, 9, 1091-2. Greenwood, B.M. and Baker, J.R. (Eds.) (1993) A malaria control trial using insecticide-treated bed
nets and targeted chemoprophylaxis in a rural area of The Gambia, West Africa. Trans. Roy. Soc. Trop. Med. Hyg. 87, Supp.2, 1-60.
Gyapong, M., Gyapong, J.O., Amankwa, J.A., Asedem, J.F. and Sory, E.K. (1992) "We have been looking for something like this for a long time": Acceptability of the use of insecticide impregnated bednets in an area of low bednet use. Unpublished report. Accra: Health Research Unit, Ministry of Health, Ghana.
Helitzer-Allen, D.L., Kendall, C. and Wirima, J.J. (1993) The role of ethnographic research in malaria control: An example from Malawi. Research Sociol. Health Care 10, 269-286.
Helitzer-Allen, D.L., McFarland, D.A., Wirima,J.J. and Macheso,A.P. (1993) Malaria chemoprohylaxis compliance in pregnant women: A cost-effectiveness analysis of alternative interventions. Soc. Sci. Med. 36, 403-407.
Jick, T. (1979) Mixing Qualitative and Quantitative Methods: Triangulation in Action. Admin. Sci. Quart. 24, 602-611.
Kaewsonthi, S. (1984) Cost and performance of malaria surveillance in Thailand. Soc. Sci. Med. 19, 1081-1097.
Koss, J. and Kloos, H. (1989) Social and behavioural influences on health. In Goldsmith, R. and Heyneman, D. (Eds.), Tropical Medicine and Parasitology. Englewood Cliffs, NJ, Prentice-Hall, pp.804-808.
Li, Z., Zhang, M., Wu, Y., Zhong, B., Lin, G. and Huang, H. (1989) Trials of deltamethrin impregnated mosquito nets for the control of malaria transmitted by Anopheles sinensis and Anopheles anthro- pophagus. Am. J. Trop. Med. Hyg. 40, 356-359.
Liao, P. (1991 ) Anthropological observation on economic development in Li minority. In Chen, G. (Ed.) Chinese Anthropology Today. Shanghai: Sanlian Publishing House, pp.267-273.
MacCormack, C.P., Snow, R.W. and Greenwood, B,M. (1989) Use of insecticide-impregnated bed nets in Gambian primary health care: economic aspects. Bull. WHO 67, 209-214.
Manderson, L., Valencia, L.B. and Thomas, B. (1992) Bringing the People In: Community participation and the control of tropical disease. Resource Paper No. 1, Social and Economic Research in Tropical Diseases. TDR/SER/RP/92/1. Geneva: UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases.
Mills, A. (1992) The economic evaluation of malaria control technologies: the case of Nepal. Soc. Sci. Med. 34, 9, 965-972.
Okanurak, K., Sornmani, S. and Chitprarop, U. (1991) The role of folk healers in the malaria volunteer program in Thailand. Southeast Asian J. Trop. Med. Pub. Health 22, 57-64.

53
Rosenfield, P.L., Golladay, F. and Davidson, R.K. (1984) The economics of parasitic diseases; research priorities. Soc. Sci. Med. 19, 1117-1126.
Rosenfield, P.L., Widstrand, C.-G., and Ruderman, A.P. (1981) Social and economic research in the World Bank/UNDP/Special Programme for Research and Training in Tropical Diseases. Soc. Sci. Med. 15A, 529 538.
Ruebush, T.K., Zeissig, R., Godoy, H.A. and Klein, R.E. (1990) Use of illiterate volunteer workers for malaria detection and treatment. Ann. Trop. Med. Parasitol. 84, 119-126.
Ruiz, W. and Kroeger, A. (1994) The socioeconomic impact of malaria in Columbia and Ecuador. Health Pol. Plann. 9, 2, 144-154.
Sawyer, D. (1993) Economic and social consequences of malaria in new colonization projects in Brazil. Soc. Sci. Med. 37, 9, 1131 1136.
Sevilla-Casas, E. (1993) Human mobility and malaria risk in the Naya river basin of Colombia. Soc. Sci. Med. 37, 9, 1155 1167.
Singer, B. (1989) Social science and the improvement of tropical disease control programs. In Bloom, B.R. and Carami, A. (Eds), Biomedical Science and the Third World: Under the Volcano. Annals of the New York Academy of Sciences 569, New York, N.Y., pp. 275 287.
Singhanetra-Renard, A. (1993) Malaria and mobility in Thailand. Soc. Sci. Med. 37, 9, 1147-1154. Snow, R.W. (1988) A trial of bed nets (mosquito nets) as a malaria control strategy within a primary
health care programme in a rural area of The Gambia, West Africa. Trans. R.Soc. Trop. Med. Hyg. 82, 212-215.
Sornmani, S., Butraporn, P., Fungladda, W., Okanurak, K. and Dissapongsa, S. (1983) Migration and disease problems: A study of patterns of migration in an endemic area of malaria in Thailand. Southeast Asian J. Trop. Med. Pub. Health 14, 64-68.
Sornmani, S. and Manderson, L. (Guest Eds.) (1992) Social and behavioural aspects of malaria control. Special issue of Southeast Asian J. Trop. Med. Pub. Health 23, Supp. 1.
Tang, L., Deng, D. and Liu, C. (1990) Microepidemiological study on socio-economic factors contributing to malaria epidemic potential in Guangba area of Hainan Province, China. Bull. Soc. Fr. Parasitol.8 (Suppl.2), 823.
Vlassoff, C. ( 1991 ) Social and economic research in TDR: future directions. Parasitol. Today 7, 2, 37-39. Wu, K., Chen, W., Lin, M., Pang, X., Cai, X., Liu, Z., Chen, S., Lan, X., Hang, M., Chen, X., Yang,
K., Tao, Z., Deng, J. and Deng, D. (1992) An investigation of the present malaria condition in a renowned endemic area - Nanqiao district of Hainan Province. Hainan J. Med.4: 3-6.