serum osteoprotegerin is inversely associated with carotid plaque echogenicity in humans
TRANSCRIPT

A
cl
cs9ws
rc©
K
1
woisdca
0d
Atherosclerosis 191 (2007) 128–134
Serum osteoprotegerin is inversely associated with carotid plaqueechogenicity in humans
Anders Vik a,∗, Ellisiv B. Mathiesen b, Ann-Trude W. Notø a,Baldur Sveinbjørnsson c, Jan Brox d, John-Bjarne Hansen a
a Center for Atherothrombotic Research in Tromsø (CART), Department of Medicine, Institute of Clinical Medicine,Institute of Medical Biology, University of Tromsø, N-9037 Tromsø, Norway
b Institute of Community Medicine, Institute of Medical Biology, University of Tromsø, Tromsø, Norwayc Department of Experimental Pathology, Institute of Medical Biology, University of Tromsø, Tromsø, Norway
d Department of Medical Biochemistry, Institute of Medical Biology, University of Tromsø, Tromsø, Norway
Received 13 April 2005; received in revised form 5 March 2006; accepted 6 March 2006Available online 18 April 2006
bstract
Osteoprotegerin (OPG) is a member of the tumour necrosis factor superfamily involved in the regulation of bone metabolism and vascularalcification. High serum values of OPG are associated with cardiovascular disease in humans. The purpose was to investigate serum OPGevels in subclinical carotid atherosclerosis and the relation between OPG levels and plaque morphology.
OPG levels were compared in 29 persons with echogenic carotid plaques, 30 persons with echolucent plaques and 41 persons withoutarotid plaques, all recruited from a population health study. Computerized assessment of plaque echogenicity was done by use of the graycale median (GSM). Participants with echogenic carotid plaques had lower serum OPG level (1.23 ng/ml; 1.02–1.48) (geometric mean;5% CI) than persons with echolucent plaques (1.76 ng/ml; 1.46–2.14) and those without plaques (1.89 ng/ml; 1.60–2.21). OPG and PTHere independently related to GSM. A significant trend for decrease in GSM across quartiles of OPG was found (p = 0.003) which remained
ignificant even after adjustment for PTH and smoking.
The present study demonstrates lower serum OPG levels in persons with subclinical echogenic carotid plaques and identified an inverseelation between serum OPG and plaque echogenicity. The findings support the concept that OPG may play an important role in arterialalcification.
2006 Elsevier Ireland Ltd. All rights reserved.
scular d
cti[ipt
eywords: Osteoprotegerin; Carotid plaque; Plaque morphology; Cardiova
. Introduction
Osteoporosis in human populations has been associatedith a higher incidence of arterial calcification, a componentf many atherosclerotic lesions [1]. Vascular calcificationncreases with age and was long thought to be the finaltage of atherosclerosis. However, vascular calcification may
evelop at early stages of atherosclerosis. The process of vas-ular calcification is highly regulated, but why only sometherosclerotic plaques calcify is unknown [1]. Although vas-∗ Corresponding author. Tel.: +47 776 44378; fax: +47 776 26863.E-mail address: [email protected] (A. Vik).
td
sia
021-9150/$ – see front matter © 2006 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.atherosclerosis.2006.03.002
iseases; Arterial calcification
ular calcification seems to represent a more stable plaqueype and a lower chance for clinical events, previous stud-es are partly conflicting and its role remains controversial2–5]. Recently, Jørgensen et al. [6], reported a significantnverse correlation between the presence of echogenic carotidlaques and bone mineral density in a cross-sectional popula-ion based study. Osteoprotegerin (OPG) has been proposedo represent a link between osteoporosis and cardiovascularisease [7,8].
The glycoprotein OPG is a member of the tumour necro-is factor superfamily and has been highly conserved dur-ng evolution [9]. It is expressed at high concentrations by
variety of tissues and cell types including main compo-

lerosis
nsetaFitacuBaOT
srvibsfiscssgcvf
aicaerwfimaivtsth
2
2
u
icttsm(saoltpAvdadrtp9ptp(ButtIpc
2
mrpocosotictwns
A. Vik et al. / Atherosc
ents of the cardiovascular system [9–14] such as arterialmooth muscle cells and endothelial cells [14,15]. OPGxerts its function by serving as a decoy receptor for recep-or activator nuclear factor kappa B ligand (RANKL) [16]nd TNF-related apoptosis-inducing ligand (TRAIL) [16,17].unctionally, OPG binds to RANKL and TRAIL, thereby
nhibiting ligation of these mediators to their cognate recep-ors and subsequent activation of specific proinflammatorynd proapoptotic signalling pathways. RANKL activates itsognate receptor RANK which seems to be an important reg-lator of dendritic cells, T-cells and osteoclasts [16,18,19].oth OPG and RANKL are expressed in non-diseased aortasnd in atherosclerotic lesions in humans [12,20]. In vitro,PG prolongs endothelial cell survival [14] by inhibitingRAIL and thereby preventing apoptosis [15].
OPG-deficient mice were reported to develop osteoporo-is and calcification of the renal arteries and aorta [21], andestoration of the gene from midgestation completely pre-ented the lesions [22]. Furthermore, in rats subcutaneousnjection of OPG prevented calcification of arteries inducedy administration of D-vitamin and warfarin [23]. Thus, OPGeems to play a crucial role for the regulation of arterial calci-cation in experimental animal models. In humans, elevatederum OPG levels have been reported in patients with stableoronary artery disease, and the OPG-level increased with theeverity of the disease [24,25]. Recently, prospective studieshowed that OPG was an independent risk factor for pro-ression of atherosclerosis in carotid arteries and incidentardiovascular disease [26], and for mortality and cardio-ascular events after acute myocardial infarction with heartailure [27].
Ultrasound imaging of arteries allows investigation oftherosclerosis in the early stages, and makes it possible todentify persons with subclinical atherosclerosis, i.e., beforelinical events have occurred. The carotid arteries are readilyccessible to ultrasound imaging and thereby non-invasivevaluation of morphological characteristics of atheroscle-otic plaques. Plaques that appear echolucent are lipid-rich,hereas echogenic plaques have higher content of densebrous tissue and calcification [28]. Computerized measure-ent of the gray scale median (GSM) of carotid plaques ismore objective method for evaluating plaque echogenic-
ty [29], and is reported to show good concordance withisual analysis of plaque echogenicity [30]. The purpose ofhe present study was to investigate serum OPG levels in per-ons with subclinical carotid atherosclerosis and to determinehe relation between serum OPG and plaque morphology inumans.
. Methods
.1. Study participants
The participants of the study were recruited from a pop-lation health study (the fifth survey of The Tromsø Study
s
bl
191 (2007) 128–134 129
n 2001), which included ultrasound examination of the rightarotid artery. Persons were eligible for the plaque group ifhey were aged 56–80 years and had one plaque or more inhe right carotid bifurcation or internal carotid artery at thecreening with a plaque thickness of ≥2.5 mm and plaqueorphology classified as echolucent (grade 1) or echogenic
grade 4) according to the Gray–Weale criteria [31]. Per-ons in the same age groups without plaques in their carotidrteries were used as controls. Exclusion criteria were anyf the following conditions: regular use of oral anticoagu-ants, cancer or other serious life-threatening medical condi-ions, hypothyroidism, creatinine ≥ 130 �mol/l, hepatic- orsychiatric disease, and current abuse of alcohol or drugs.
complete medical history with special focus on cardio-ascular events and smoking habits were obtained. Car-iovascular disease (CVD) was defined as prior or presentngina pectoris, myocardial infarction, peripheral vascularisease, transient ischemic attacks (TIA), stroke and amau-osis fugax. Hypertension was selfreported (in a health ques-ionnaire) use of antihypertensive medication or systolicressure above 160 mmHg and/or diastolic pressure above5 mmHg. Diabetes was selfreported or defined as fastinglasma glucose ≥ 7.0 mmol/l or nonfasting ≥ 11.1 mmol/l atwo occasions. Height and weight were measured with theatients in light clothing without shoes; body mass indexBMI) was calculated as weight per height squared (kg/m2).lood pressure was recorded in seated position by these of an automatic device (Dinamap Vital Signs Moni-or). Three recordings were made at 1-min intervals, andhe mean of the two last values is used in this report.nformed written consent was obtained from the partici-ants, and the study was approved by the regional ethicalommittee.
.2. Ultrasound examination
At the population health screening, high-resolution B-ode and color Doppler/pulsed-wave Doppler ultrasonog-
aphy of the right carotid artery was performed as describedreviously. A plaque was defined as a localized thickeningf the vessel wall of more than 50% compared to the adja-ent vessel wall thickness. To minimize measurement error,nly persons with a plaque thickness of ≥2.5 mm at thecreening and with uniform echolucent plaques (grade = 1)r uniform echogenic plaques (grade = 4) were eligible forhe present study. As only the right carotid artery was exam-ned at the screening, a new ultrasound examination of botharotid arteries was performed. These ultrasound examina-ions were performed by the same experienced examiner, andith the use of an Acuson Xp10 128 ART ultrasound scan-er equipped with a linear array 5–7 MHz transducer. Theubjects were examined in the supine position with the head
lightly tilted to the opposite side.Plaque morphology in terms of echogenicity was assessedy analysis of gray scale content of the plaques and calcu-ation of gray scale median (GSM). Assessment of plaque

1 lerosis
mateoto2gpittciloenttwtmpapwew[
arnpwtTowc
2
cuiitwN−aL
tachbtDmPfwDUsr(tScsTtfiaawtpd
2
tGbsgtatDarppfGsmGa
30 A. Vik et al. / Atherosc
orphology was made in all plaques present in the nearnd far walls of the common carotid, the bifurcation, andhe internal carotid arteries on both sides (12 locations). Allxaminations and measurements of all plaques were recordedn videotapes. Stored B-mode images were subsequentlyransferred to a personal computer and digitized into framesf 768 × 576 pixels of 256 gray levels each (0 = black and56 = white) with the use of a commercially available videorabber card (meteor II/Matrox Intellicam). Measurements oflaque area were made with the use of the Adobe Photoshopmage-processing program (version 7.0.1), by tracing aroundhe perimeter of each plaque with a cursor. The gray-level dis-ribution and gray-scale median (GSM) of each plaque wasalculated. Normalization of GSM was performed accord-ng to the method by el-Barghouty [32]. A fixed area of theumen of the carotid artery (300 pixels), the brightest areaf the innermost adventitia adjacent to the plaque (150 pix-ls), and the plaque were marked. The plaque image wasormalized by adjusting linearly their gray tonal range sohat the lumen were assigned a GSM of 1 and the adventi-ia 200 [33]. After standardization, the GSM of the plaquesere re-calculated. In persons with more than one plaque,
he standardized GSM of the total plaque area was esti-ated as a weighted mean of the GSM value of each single
laque. The area of each plaque was divided by the totalrea of plaques in each person, and this fraction was multi-lied with each plaque’s normalized GSM value. All scoresere added to calculate the total normalized GSM score for
ach person. Reproducibility of the ultrasound examinationsas acceptable and has been reported in detail previously
34].A total of 58 persons with plaques in the right carotid artery
nd 47 without plaques at the screening examination wereecruited to the study. At the second ultrasound examination,o plaque could be detected in two of the 58 persons withlaques, and these were excluded from the study. Six personsith no plaques in the right carotid artery had plaques on
he left side and they were allocated to the plaque group.hree persons were excluded from the plaque group becausef serum creatinine concentration ≥ 130 �mol/l. Thus, thereere 59 persons in the plaque group and 41 persons in the
ontrol group.
.3. Blood collection and measurements
Blood was drawn in the morning at 7:45 a.m. from an ante-ubital vein on the right arm after 12 h of overnight fastingsing a 19-gauge needle in a vacutainer system with min-mal stasis. Serum was prepared by clotting whole bloodn a glass tube at room temperature for 1 h and then cen-rifuged at 2000 × g for 15 min at 22 ◦C. Aliquots of 1 mlere transferred into sterile cryovials (Greiner labortechnik,
urtringen, Germany), flushed with nitrogen, and frozen at70 ◦C until further analysis. Serum lipids were analysed onCobas Mira S (Roche Diagnostics, F. Hoffmann-La Rochetd., Basel, Switzerland) with reagents from ABX Diagnos-vfaw
191 (2007) 128–134
ics (Montpellier, France). Total cholesterol (CHOD-PAP)nd triglycerides (GPO-PAP) were measured with enzymaticolorimetric methods. Low density lipoprotein (LDL) andigh density lipoprotein (HDL) cholesterol were measuredy selective inhibition colorimetric assays (LDL choles-erol direct and HDL cholesterol direct, respectively, ABXiagnostics). Calorimetric determinations of serum albu-in and total calcium were conducted on Hitachi Modular(Roche Diagnostics, Mannheim, Germany) with reagents
rom Roche Diagnostics. Parathyroid hormone (Intact PTH)as measured by an immunometric assay (IMMULITE 2000,PC-Diagnostic Products Corporation, Los Angeles, CA,SA). High-sensitivity C-reactive protein (hsCRP) was mea-
ured by a particle-enhanced immunturbidimetric assay witheagents from Roche analysed in a Modular P autoanalyzerRoche Diagnostics, Mannheim, Germany). The concentra-ion of total OPG was analyzed by an ELISA assay (R&Dystems, Abingdon, UK) with mouse anti-human OPG asapture antibody. Biotinylated goat anti-human OPG andtreptavidin horseradish peroxydase were used for detection.he OPG assay was performed according to the instruc-
ions by the manufacturer. The intra- and interassay coef-cients of variation (CV) in our laboratory were 3.2%nd 6.8%, respectively. OPG levels between assays weredjusted for by use of an internal standard. The analysesere performed on coded samples without knowledge of sta-
us regarding atherosclerosis in the carotid arteries by theerson performing the assays. All samples were analyzed inuplicate.
.4. Statistical analysis
Subjects with plaques were divided in two groups,he echogenic group, defined as GSM above median,SM > 64.45, and the echolucent group, defined as GSMelow median, GSM ≤ 64.45. Continuous variables are pre-ented as mean (95% confidence interval (CI)), and cate-orical data as proportions (CI). Logarithmic transforma-ion was applied to the variables OPG, hsCRP, triglyceridesnd parathyroid hormone to approximate normal distribu-ion. Differences between proportions were tested by χ2-test.ifferences between means were tested for significance by
nalysis of variance. Linear trends were tested by multipleegression analysis. The mean levels of OPG in the threelaque groups were compared by analysis of variance (GLMrocedure), with adjustments for age, sex and possible con-ounding variables. The independent relationship betweenSM and OPG was also tested in multiple regression analy-
is, treating GSM as a continuous variable, and with adjust-ent for possible confounders. Controls (persons with noSM value) were excluded from this analysis. The statistical
nalysis was performed using SPSS software for Windows,
ersion 11.0 (SPSS, Inc., Chicago, IL). Confidence intervalsor proportions were calculated by the Epi Info software pack-ge (Epi Info, version 6.04d, 2001). Two sided P values < 0.05ere considered statistically significant.
A. Vik et al. / Atherosclerosis 191 (2007) 128–134 131
Table 1Characteristics of persons with echogenic carotid plaques, echolucent carotid plaques, and without carotid plaques
Echogenic plaque (n = 30) Echolucent plaque (n = 29) Controls (n = 41) p
Age (years) 70.5 (68.4–72.7) 68.7 (66.2–71.3) 68.1 (66.3–70.0) 0.3Men (%) 46.7 (29.5–64.4) 58.6 (40.3–75.3) 51.2 (36.1–66.2) 0.7BMI (kg/m2) 26.2 (24.8–27.7) 25.6 (24.3–27.0) 27.5 (26.3–28.6) 0.1Smokers (%) 23.3 (10.8–40.8) 17.9 (6.9–35.2)a 24.4 (13.1–39.2) 0.8Systolic BP (mmHg) 132 (124–139) 127 (119–134) 130 (125–136) 0.6Diastolic BP (mmHg) 75 (72–78) 74 (69–79) 75 (72–78) 0.9Total cholesterol (mmol/l) 6.57 (6.07–7.09) 6.25 (5.77–6.73) 6.01 (5.64–6.39) 0.2LDL cholesterol (mmol/l) 4.25 (3.86–4.64) 4.01 (3.66–4.37) 3.70 (3.42–3.99) 0.1HDL cholesterol (mmol/l) 1.74 (1.54–1.94) 1.59 (1.36–1.82) 1.75 (1.61–1.89) 0.4Triglyceridesb (mmol/l) 1.01 (0.83–1.25) 1.04 (0.86–1.26) 1.05 (0.92–1.21) 0.9Calcium (mmol/l) 2.41 (2.38–2.44) 2.41 (2.39–2.43) 2.39 (2.36–2.41) 0.3PTHb (pmol/l) 5.32 (4.56–6.21) 4.00 (3.36–4.76) 4.96 (4.44–5.54) 0.02Creatinine (�mol/l) 86 (81–91) 86 (82–90) 83 (79–87) 0.4Hypertension (%) 33.3 (18.3–51.4) 17.2 (6.6–34.2) 34.1 (20.9–49.5) 0.3hsCRPb (mg/l) 1.28 (0.91–1.80) 1.35 (0.90–2.03) 1.36 (0.99–1.88) 1.0Cardiovascular disease (%) 20.0 (8.5–37.0) 20.7 (8.8–38.2) 22.0 (11.3–36.5) 1.0Diabetes (%) 3.3 (0.2–15.4) 3.4 (0.2–15.9) 4.9 (0.8–15.2) 0.9Statin users (%) 6.7 (1.1–20.3) 3.4 (0.2–15.9) 7.3 (1.9–18.6) 0.8AT II-antagonist users (%) 16.7 (6.4–33.1) 3.4 (0.2–15.9) 17.1 (7.8–30.9) 0.2
Vucent g
3
pawfpbgethci(
eorp
rftstas
rLBm
Ovbv
TT
P
1
2
≥
T
alues are means or percentages (95% CI).a Information on smoking was missing in 1 of the 29 persons in the echolb Values are geometric means (95% CI).
. Results
Characteristics of persons with echolucent carotidlaques, echogenic plaques and persons without carotidtherosclerotic plaques are shown in Table 1. Each participantith carotid plaques had from one to eight plaques. Twenty-
our (40.7%) persons had one plaque, 17 (28.8%) had twolaques, 18 (30.5%) had three or more plaques. The num-er of echogenic and echolucent plaques within each plaqueroup is shown in Table 2. There were no significant differ-nces between groups with regard to cerebrovascular risk fac-ors such as age, sex, BMI, smoking, diabetes, hypertension,sCRP, serum lipids and cardiovascular disease. Serum con-entration of parathyroid hormone was significantly highern the echogenic plaque group than in the echolucent groupp = 0.023), but not significantly different from controls.
Persons with echogenic plaques had lower OPG lev-
ls than persons with echolucent plaques and those with-ut carotid atherosclerotic plaques (Table 3). The differenceemained significant after adjustment for CVD risk factors,arathyroid hormone and the use of statins and angiotensin II-Opoi
able 2he number of echogenic and echolucent plaques within each plaque group shown
laques (n) Plaque group Echogenic plaques (n)
Echogenic 11Echolucent 0
Echogenic 15Echolucent 1
3 Echogenic 32Echolucent 5
he GSM value (mean, 95% CI) for each group is shown.
roup.
eceptor antagonists. When persons with CVD were excludedrom the analysis, the difference in OPG levels between thewo plaque groups was even more prominent (Table 3). Noignificant difference was found in serum OPG level betweenhe echolucent plaque group and the controls (Table 3),nd no sex-related differences were demonstrated (data nothown).
In the total study population there were no significant cor-elations between serum OPG levels and total cholesterol,DL cholesterol, HDL cholesterol, hsCRP, triglycerides, age,MI, systolic and diastolic blood pressure, parathyroid hor-one and calcium.When analysis was limited to persons with plaque only,
PG and PTH were significantly associated with GSM in uni-ariate linear regression analysis and a borderline associationetween smoking and GSM was found (p = 0.054). In multi-ariate analysis, adjusted for age, sex, PTH and smoking,
PG was independently associated with GSM (R2 = 0.24,= 0.04). Trend analysis for changes in GSM across quartilesf OPG was performed, and a significant trend for decreasen GSM with increasing OPG levels was found both in uni-in participants with one, two or ≥three plaques
Echolucent plaques (n) GSM (mean, 95% CI)
0 85.9 (72.6–99.1)13 37.9 (30.7–45.1)
5 86.6 (71.7–101.5)13 43.1 (32.1–54.1)
4 90.5 (79.9–101.1)29 42.2 (34.2–50.2)
132 A. Vik et al. / Atherosclerosis 191 (2007) 128–134
Table 3Relationship between OPG serum concentration and carotid plaque morphology in crude and adjusted analysis for participants with echogenic carotid plaques,echolucent carotid plaques, and participants without carotid plaques
Echogenic plaque Echolucent plaque Controls R2 p
OPG (ng/ml)a,† 1.23 (1.02–1.48) 1.76 (1.46–2.14) 1.89 (1.60–2.21) 0.12 0.002Model I OPG (ng/ml)a,‡ 1.23 (1.02–1.49) 1.74 (1.44–2.11) 1.90 (1.61–2.23) 0.15 0.003Model II OPG (ng/ml)a,§ 1.22 (1.00–1.48) 1.77 (1.45–2.17) 1.89 (1.60–2.23) 0.21 0.003Model III OPG (ng/ml)a,$ 1.11 (0.90–1.37) 1.86 (1.50–2.31) 1.91 (1.59–2.29) 0.19 <0.0001
Model I: adjusted for age and sex. Model II: adjusted for age, sex, BMI, HDL-cholesterol, hypertension, parathyroid hormone, use of statins and angiotensinII-receptor antagonists. Model III: participants with cardiovascular disease were excluded (remaining echogenic n = 24, echolucent n = 23, and controls n = 32).
a Osteoprotegerin, values are geometric means (95% CI).† Echogenic vs. controls; p = 0.003 echogenic vs. echolucent; p = 0.026 echolucent vs. controls p = 1.0 (post hoc tests, Bonferroni).‡ Echogenic vs. controls; p = 0.003 echogenic vs. echolucent; p = 0.036 echolucen§ Echogenic vs. controls; p = 0.003 echogenic vs. echolucent; p = 0.030 echolucen$ Echogenic vs. controls; p = 0.001 echogenic vs. echolucent; p = 0.003 echolucen
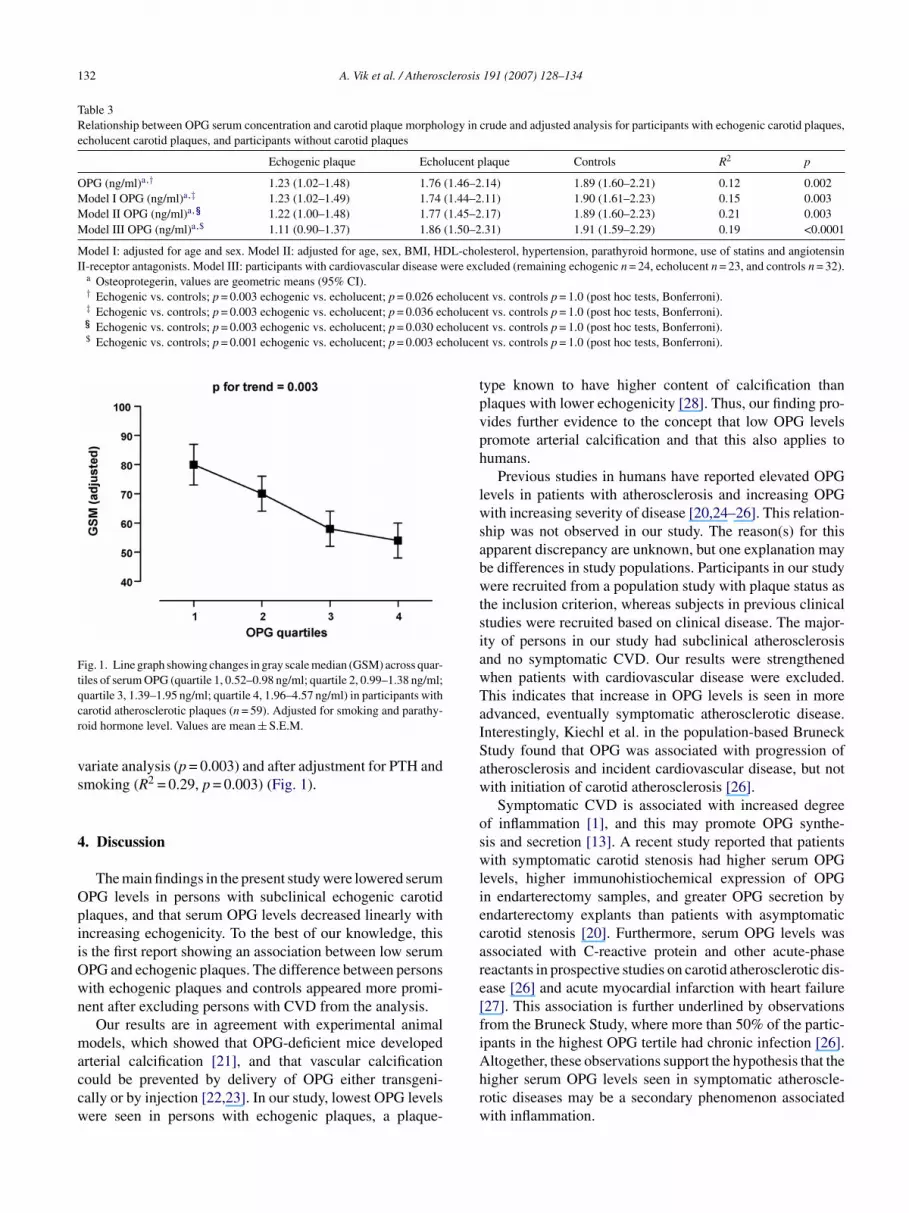
Fig. 1. Line graph showing changes in gray scale median (GSM) across quar-tiles of serum OPG (quartile 1, 0.52–0.98 ng/ml; quartile 2, 0.99–1.38 ng/ml;qcr
vs
4
OpiiOwn
maccw
tpvph
lwsabwtsiawTaISaw
oswliecare[fi
uartile 3, 1.39–1.95 ng/ml; quartile 4, 1.96–4.57 ng/ml) in participants witharotid atherosclerotic plaques (n = 59). Adjusted for smoking and parathy-oid hormone level. Values are mean ± S.E.M.
ariate analysis (p = 0.003) and after adjustment for PTH andmoking (R2 = 0.29, p = 0.003) (Fig. 1).
. Discussion
The main findings in the present study were lowered serumPG levels in persons with subclinical echogenic carotidlaques, and that serum OPG levels decreased linearly withncreasing echogenicity. To the best of our knowledge, thiss the first report showing an association between low serumPG and echogenic plaques. The difference between personsith echogenic plaques and controls appeared more promi-ent after excluding persons with CVD from the analysis.
Our results are in agreement with experimental animalodels, which showed that OPG-deficient mice developed
rterial calcification [21], and that vascular calcificationould be prevented by delivery of OPG either transgeni-ally or by injection [22,23]. In our study, lowest OPG levelsere seen in persons with echogenic plaques, a plaque-
Ahrw
t vs. controls p = 1.0 (post hoc tests, Bonferroni).t vs. controls p = 1.0 (post hoc tests, Bonferroni).t vs. controls p = 1.0 (post hoc tests, Bonferroni).
ype known to have higher content of calcification thanlaques with lower echogenicity [28]. Thus, our finding pro-ides further evidence to the concept that low OPG levelsromote arterial calcification and that this also applies toumans.
Previous studies in humans have reported elevated OPGevels in patients with atherosclerosis and increasing OPGith increasing severity of disease [20,24–26]. This relation-
hip was not observed in our study. The reason(s) for thispparent discrepancy are unknown, but one explanation maye differences in study populations. Participants in our studyere recruited from a population study with plaque status as
he inclusion criterion, whereas subjects in previous clinicaltudies were recruited based on clinical disease. The major-ty of persons in our study had subclinical atherosclerosisnd no symptomatic CVD. Our results were strengthenedhen patients with cardiovascular disease were excluded.his indicates that increase in OPG levels is seen in moredvanced, eventually symptomatic atherosclerotic disease.nterestingly, Kiechl et al. in the population-based Brunecktudy found that OPG was associated with progression oftherosclerosis and incident cardiovascular disease, but notith initiation of carotid atherosclerosis [26].Symptomatic CVD is associated with increased degree
f inflammation [1], and this may promote OPG synthe-is and secretion [13]. A recent study reported that patientsith symptomatic carotid stenosis had higher serum OPG
evels, higher immunohistiochemical expression of OPGn endarterectomy samples, and greater OPG secretion byndarterectomy explants than patients with asymptomaticarotid stenosis [20]. Furthermore, serum OPG levels wasssociated with C-reactive protein and other acute-phaseeactants in prospective studies on carotid atherosclerotic dis-ase [26] and acute myocardial infarction with heart failure27]. This association is further underlined by observationsrom the Bruneck Study, where more than 50% of the partic-pants in the highest OPG tertile had chronic infection [26].
ltogether, these observations support the hypothesis that theigher serum OPG levels seen in symptomatic atheroscle-otic diseases may be a secondary phenomenon associatedith inflammation.
lerosis
vaacakiaP�icpi
ewtatadlnoa
bprttccSCod
scstctm
A
ANHu
R
[
[
[
[
[
[
[
[
[
A. Vik et al. / Atherosc
Although studies suggest an important role for OPG inascular pathophysiology, it is not evident whether OPG iscausal risk factor or represents a counterregulatory mech-
nism. OPG has been proposed to be a compensatory vas-ular defense system that is up regulated in atherosclerosisnd conditions that confer a high vascular risk in order toeep excessive activation of inflammation pathways and othernjurious stimuli under control [7,35]. Several experimentalnd clinical studies support the counterregulatory hypothesis.roinflammatory cytokines such as interleukin-1beta, TNF-and growth factors such as platelet-derived growth factor
nduce OPG expression in human vascular smooth muscleells [13]. OPG is shown to promote endothelial cell survivalossibly by preventing TRAIL interaction with death induc-ng TRAIL receptors on endothelial cells [15].
Previously, arterial calcification was assumed to be anntirely passive shift of calcium from the bone to the vascularall, but increasing evidence recognize an underlying regula-
ion by calcification inhibitors [12]. OPG is considered to becandidate calcification inhibitor due to its capacity to coun-
eract calcification [22,23,36]. In the present study, both OPGnd PTH were significant predictors for plaque echogenicityetermined by GSM. The linear relation between serum OPGevels and plaque echogenicity in our study remained sig-ificant even after adjustment for serum PTH levels. Thesebservations may indicate an independent role for OPG inrterial calcification in humans.
The main limitation of this study is a relatively small num-er of participants and therefore caution is needed when inter-reting the results. However, both cases and controls wereecruited from a population health study, which increaseshe chances for obtaining a representative sample. Secondly,he proportions that were smokers, had hypertension and/orardiovascular disease, were not significantly higher in ourontrol group than in the general population of the Tromsøurvey. Thus, it is unlikely that a selection bias has occurred.alcification was not measured directly, but several previ-us validation studies have shown that calcified plaques andense fibrotic plaques appear echogenic [28].
In conclusion, the present study demonstrates lowerederum OPG levels in persons with subclinical echogenicarotid plaques and identified an inverse relation betweenerum OPG and plaque echogenicity. The findings supporthe concept that OPG plays a crucial role in arterial calcifi-ation. Further experimental and clinical studies are neededo settle the role for OPG in early atherogenesis and plaque
orphology in humans.
cknowledgements
CART is sponsored by an independent grant from Pfizer
S. Ellisiv B. Mathiesen was financed by a grant from theorwegian Research Council. We are indebted to Dr. Steinarald Johnsen and Dr. Einar Fosse, who did the carotidltrasound screening at the fifth survey of the Tromsø Study.[
191 (2007) 128–134 133
eferences
[1] Doherty TM, Asotra K, Fitzpatrick LA, et al. Calcification in atheroscle-rosis: bone biology and chronic inflammation at the arterial crossroads.PNAS 2003;100:11201–6.
[2] Richardson P, Davies M, Born G. Influence of plaque configurationand stress distribution on fissuring of coronary atherosclerotic plaques.Lancet 1989;2:941–4.
[3] Lee RT, Grodzinsky AJ, Frank EH, et al. Structure-dependent dynamicmechanical behavior of fibrous caps from human atheroscleroticplaques. Circulation 1991;83:1764–70.
[4] Huang H, Virmani R, Younis H, et al. The impact of calcificationon the biomechanical stability of atherosclerotic plaques. Circulation2001;103:1051–6.
[5] Mathiesen EB, Bonaa KH, Joakimsen O. Echolucent plaquesare associated with high risk of ischemic cerebrovascular eventsin carotid stenosis: The Tromso Study. Circulation 2001;103:2171–5.
[6] Jorgensen L, Joakimsen O, Berntsen GR, et al. Low bone mineral den-sity is related to echogenic artery plaques. A population based study.Am J Epidemiol 2004;160:549–56.
[7] Browner WS, Lui L-Y, Cummings SR. Associations of serum osteo-protegerin levels with diabetes, stroke, bone density, fractures, andmortality in elderly women. J Clin Endocrinol Metab 2001;86:631–7.
[8] Hofbauer LC, Schoppet M. Osteoprotegerin: a link betweenosteoporosis and arterial calcification? The Lancet 2001;358:257–9.
[9] Simonet WS, Lacey DL, Dunstan CR, et al. Osteoprotegerin: a novelsecreted protein involved in the regulation of bone density. Cell1997;89:309–19.
10] Tan KB, Harrop J, Reddy M, et al. Characterization of a novelTNF-like ligand and recently described TNF ligand and TNF recep-tor superfamily genes and their constitutive and inducible expressionin hematopoietic and non-hematopoietic cells1. Gene 1997;204:35–46.
11] Yun TJ, Chaudhary PM, Shu GL, et al. OPG/FDCR-1, a TNF receptorfamily member. Is expressed in lymphoid cells and is up-regulated byligating CD40. J Immunol 1998;161:6113–21.
12] Dhore CR, Cleutjens JPM, Lutgens E, et al. Differential expressionof bone matrix regulatory proteins in human atherosclerotic plaques.Arterioscler Thromb Vasc Biol 2001;21:1998–2003.
13] Zhang J, Fu M, Myles D, et al. PDGF induces osteoprotegerin expres-sion in vascular smooth muscle cells by multiple signal pathways. FEBSLett 2002;521:180–4.
14] Malyankar UM, Scatena M, Suchland KL, et al. Osteoprote-gerin Is an alpha vbeta 3-induced, NF-kappa B-dependent Sur-vival Factor for Endothelial Cells. J Biol Chem 2000;275:20959–62.
15] Pritzker LB, Scatena M, Giachelli CM. The role of osteoprote-gerin and tumor necrosis factor-related apoptosis-inducing ligandin human microvascular endothelial cell survival. Mol Biol Cell2004;15:2834–41.
16] Yasuda H, Shima N, Nakagawa N, et al. Osteoclast differentiationfactor is a ligand for osteoprotegerin/osteoclastogenesis-inhibitoryfactor and is identical to TRANCE/RANKL. PNAS 1998;95:3597–602.
17] Emery JG, McDonnell P, Burke MB, et al. Osteoprotegerin is a recep-tor for the cytotoxic ligand TRAIL. J Biol Chem 1998;273:14363–7.
18] Wong BR, Josien R, Lee SY, et al. TRANCE (tumor necrosis factor[TNF]-related activation-induced cytokine), a new TNF family member
predominantly expressed in T cells is a dendritic cell-specific survivalfactor. J Exp Med 1997;186:2075–80.19] Anderson DM, Maraskovsky E, Billingsley WL, et al. A homologue ofthe TNF receptor and its ligand enhance T-cell growth and dendritic-cellfunction. Nature 1997;390:175–9.

1 lerosis
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
34 A. Vik et al. / Atherosc
20] Golledge J, McCann M, Mangan S, et al. Osteoprotegerin and osteo-pontin are expressed at high concentrations within symptomatic carotidatherosclerosis. Stroke 2004;35:1636–41.
21] Bucay N, Sarosi I, Dunstan CR, et al. Osteoprotegerin-deficient micedevelop early onset osteoporosis and arterial calcification. Genes Dev1998;12:1260–8.
22] Min H, Morony S, Sarosi I, et al. Osteoprotegerin reverses osteoporosisby inhibiting endosteal osteoclasts and prevents vascular calcifica-tion by blocking a process resembling osteoclastogenesis. J Exp Med2000;192:463–74.
23] Price PA, June HH, Buckley JR, et al. Osteoprotegerin inhibits arterycalcification induced by warfarin and by Vitamin D. ArteriosclerThromb Vasc Biol 2001;21:1610–6.
24] Jono S, Ikari Y, Shioi A, et al. Serum osteoprotegerin levels are associ-ated with the presence and severity of coronary artery disease. Circu-lation 2002;106:1192–4.
25] Schoppet M, Sattler AM, Schaefer JR, et al. Increased osteoprotegerinserum levels in men with coronary artery disease. J Clin EndocrinolMetab 2003;88:1024–8.
26] Kiechl S, Schett G, Wenning G, et al. Osteoprotegerin is a risk factorfor progressive atherosclerosis and cardiovascular disease. Circulation2004;109:2175–80.
27] Ueland T, Jemtland R, Godang K, et al. Prognostic value of osteopro-
tegerin in heart failure after acute myocardial infarction. J Am CollCardiol 2004;44:1970–6.28] Gronholdt M-LM. Ultrasound and lipoproteins as predictors of lipid-rich. Rupture-prone plaques in the carotid artery. Arterioscler ThrombVasc Biol 1999;19:2–13.
[
191 (2007) 128–134
29] Sabetai MM, Tegos TJ, Nicolaides AN, et al. Reproducibility ofcomputer-quantified carotid plaque echogenicity: can we overcome thesubjectivity? Stroke 2000;31:2189–96.
30] Mayor I, Momjian S, Lalive P, et al. Carotid plaque: comparisonbetween visual and grey-scale median analysis. Ultrasound Med Biol2003;29:961–6.
31] Gray-Weale AC, Graham JC, Burnett JR, et al. Carotid artery atheroma:comparison of preoperative B-mode ultrasound appearance with carotidendarterectomy specimen pathology. J Cardiovasc Surg (Torino)1988;29:676–81.
32] el-Barghouty N, Geroulakos G, Nicolaides A, et al. Computer-assisted carotid plaque characterisation. Eur J Vasc Endovasc Surg1995;9:389–93.
33] Elatrozy T, Nicolaides A, Tegos T, et al. The objective characterisa-tion of ultrasonic carotid plaque features. Eur J Vasc Endovasc Surg1998;16:223–30.
34] Fosse E, Johnsen SH, Stensland-Bugge E, et al. Repeated visual andcomputer-assisted carotid plaque characterization in a longitudinalpopulation-based ultrasound study: The Tromso Study. Ultrasound MedBiol 2006;32:3–11.
35] Yano K, Tsuda E, Washida N, et al. Immunological characteriza-tion of circulating osteoprotegerin/osteoclastogenesis inhibitory factor:increased serum concentrations in postmenopausal women with osteo-
porosis. J Bone Miner Res 1999;14:518–27.36] Tyson KL, Reynolds JL, McNair R, et al. Osteo/chondrocytic tran-scription factors and their target genes exhibit distinct patterns ofexpression in human arterial calcification. Arterioscler Thromb VascBiol 2003;23:489–94.