plasma annexin a5 level relates inversely to the severity of coronary stenosis
TRANSCRIPT
www.elsevier.com/locate/ybbrc
Biochemical and Biophysical Research Communications 356 (2007) 674–680
Plasma annexin A5 level relates inversely to the severityof coronary stenosis
Lambertus J.H. van Tits a,*, Waander L. van Heerde b, Gerly M. van der Vleuten a,Jacqueline de Graaf a, Diederick E. Grobbee c, Lucy P.L. van de Vijver d,
Anton F. Stalenhoef a, Hans M. Princen e
a Department of General Internal Medicine 441, Radboud University Nijmegen Medical Centre, Geert Grooteplein Zuid 8, 6525 GA Nijmegen,
P.O. Box 9101, 6500 HB Nijmegen, The Netherlandsb Central Laboratory for Hematology, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands
c Julius Center for Health Sciences and Primary Care, Utrecht University, Utrecht, The Netherlandsd Louis Bolk Institute, Driebergen, The Netherlands
e Gaubius Laboratory, TNO PG, Leiden, The Netherlands
Received 27 February 2007Available online 12 March 2007
Abstract
Exogenous radiolabeled annexin A5 is taken up by atherosclerotic tissue. We measured endogenous plasma annexin A5 and circu-lating oxidized low-density lipoprotein (oxLDL), a biochemical marker of atherosclerosis, in men with either severe angiographicallydetermined coronary stenosis (n = 90) or no or only minor stenosis (n = 96). Men without history of cardiac disease or treatmentand free of plaques in the carotid artery (by ultrasonography) were taken as controls (n = 87). Opposite to oxLDL, annexin A5 decreasedat increasing severity of stenosis. OxLDL was lowest and annexin A5 was highest in controls. Percentage differences between groups werehigher for annexin A5 than for oxLDL, and highest for oxLDL/annexin A5 ratio. The oxLDL/annexin A5 ratio is a better marker of theseverity of coronary stenosis than oxLDL alone, may reflect the presence and extent of the atherosclerotic cardiovascular disease, andmight prove useful for preclinical screening purposes.� 2007 Elsevier Inc. All rights reserved.
Keywords: Angiography; Annexin A5; Atherosclerosis; Cardiovascular diseases; Coronary disease; Coronary stenosis; Oxidized phospholipids; Oxidizedlow-density lipoprotein
Annexins comprise a group of evolutionary highly con-served proteins with calcium and membrane binding prop-erties. One of the 12 annexins found in vertebrates,classified as the annexin A subfamily, is annexin A5. It iswidely distributed intracellularly in human tissues [1] andreleased upon (traumatic) injury [2,3]. Because annexinA5 forms highly ordered two-dimensional crystals thatcoat the external leaflets of phospholipid bilayers, it canshield negatively charged phospholipids exposed by acti-vated and/or apoptotic cells from availability for critical
0006-291X/$ - see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.bbrc.2007.03.020
* Corresponding author. Fax: +31 24 3541346.E-mail address: [email protected] (L.J.H. van Tits).
phospholipid-dependent coagulation reactions [4]. Athero-sclerosis is a chronic inflammatory disease of the vesselwall, characterized by the local presence of increasedamounts of activated and apoptotic cells. In addition, ath-erosclerotic plaques contain high amounts of oxidized low-density lipoprotein (oxLDL) which, in contrast to nativeLDL, specifically binds annexin A5 [5]. OxLDL may beformed by oxidative processes during migration of theLDL particles in the vessel wall [6,7] and is a prerequisitefor atherogenesis. Whereas most of the oxLDL is retainedin the vessel walls, part of it may re-enter the circulationand the plasma level of oxLDL has been shown to be auseful marker for identifying patients with coronary artery

L.J.H. van Tits et al. / Biochemical and Biophysical Research Communications 356 (2007) 674–680 675
disease and persons at high cardiovascular risk [8–12]. Inagreement with an elevated inflammatory state and accu-mulation of oxLDL, high amounts of annexin A5 arefound in atherosclerotic plaques [1,13]. Moreover, recently,it was found that exogenous radiolabeled annexin A5 istaken up by aortic tissue and can be used for the non-inva-sive detection of apoptosis in animal models of human ath-erosclerosis [14,15] and for the identification of instabilityof atherosclerotic plaques in man [16]. The relation of sta-ble atherosclerotic cardiovascular disease with plasma lev-els of endogenous annexin A5, however, is essentiallyunexplored. It has been shown that acutely after myocar-dial infarction, plasma level of annexin A5 is elevateddue to release from cardiomyocytes [2]. In plasma of thehealthy population annexin A5 is present in low rangesof 0.6–28 lg/L [17]. We hypothesize that due to bindingof annexin A5 to components of the atherosclerotic plaque,the plasma level of endogenous annexin A5 is inverselyassociated with the presence and extent of atheroscleroticplaque formation and may have diagnostic value. Becausecoronary angiography is currently still the most usedmethod in every-day practice to diagnose coronary heartdisease, we investigated plasma levels of annexin A5 inrelation to angiographically determined coronary stenosis.
Methods
Subjects. We used plasma samples from a study that was conductedpreviously in several hospitals and clinical centers in Rotterdam andDordrecht in The Netherlands, to investigate coronary atherosclerosis inrelation to markers of LDL oxidation [18]. From 1993 to 1995, from 1489men undergoing a first coronary angiography, fasting venous blood hadbeen collected within 2 months after coronary angiography. Seven hun-dred and eighty nine of them met the inclusion criteria (45–80 years old,alive, no myocardial infarction in the year before the study, no diabetesmellitus type 1 or 2, no liver, kidney or thyroid disease, no alcohol or drugabuse, no use of HMG-CoA reductase inhibitors (statins), no psychiatriccomplaints and not a vegetarian) and were willing to participate. Subjectswere selected who had severe coronary stenosis (>85% stenosis in one and>50% stenosis in a second major coronary vessel, cases) and subjects withno or minor coronary stenosis (a maximum of 50% stenosis in no morethan two of the three major coronary vessels and less than 10% stenosis inthe third coronary vessel, hospital controls). This categorization was basedon a clinical rationale: subjects with severe coronary stenosis (according tothe criteria above) generally receive additional interventional treatment(bypass, angioplasty), but stenosis below 50% (in maximally two of thethree major coronary vessels) is mostly left without intervention, exceptfor treatment of cardiovascular risk factors. Two hundred and seventy-nine men fulfilled the stenosis criteria, but because only from 90 cases and96 hospital controls plasma samples were available that had not beenthawed since the time of blood collection, 186 patients entered the presentstudy.
Plasma samples from population control subjects were obtained fromThe Rotterdam Study, a population-based cohort study on chronic anddisabling diseases (conducted from 1991 to 1993) [19], and by additionalrecruitment (performed in 1994) of men between 45 and 55 years of age[18]. Thus, all population controls were recruited in the same region andthe same period as the hospital subjects. No angiographic data wereavailable, but the carotid artery vessel walls were examined by ultrasoundechography. The subjects who were selected had no plaques in the carotidartery and no history of cardiac disease or treatment. After exclusion ofsubjects who met one or more of the exclusion criteria of the present study(female, diabetes mellitus 1 or 2, liver, kidney or thyroid disease, use of
statins, vegetarian, and alcohol or drug abuse) and matching to hospitalsubjects with respect to smoking habits (smoking and non-smoking), weobtained 87 population control subjects of whom plasma samples had notbeen thawed in between.
All blood samples had been taken in EDTA Vacutainer tubes andplaced on ice immediately. Within 1 h after blood collection plasma wasprepared by centrifugation at 1750g for 15 min, frozen with saccharose(10%, w/v) in liquid nitrogen, and stored at �80 �C.
We obtained medical histories from medical files and through aquestionnaire administered at the time of blood sampling. Also informa-tion on smoking and drinking patterns, drug use and family history ofcardiovascular disease were available. Weight, height, and blood pressure(measured twice at one occasion in sitting position at the right upper armwith a random-zero sphygmomanometer) had been measured. Hyperten-sion was defined at that time as a systolic blood pressure of 160 mmHg ormore or a diastolic blood pressure of 95 mmHg or more, or use of anti-hypertensive drugs. An Ethics Committee on Human Research approvedthe study, and all participants gave informed consent.
Biochemical measurements. Plasma cholesterol and triglycerides weredetermined using commercially available reagents (Boehringer-Mann-heim, Mannheim, Germany). Hypercholesterolemia was defined as plasmatotal cholesterol >6.5 mmol/L or use of cholesterol lowering medication.HDL-cholesterol was determined with the phosphotungstate/Mg2+
method [20]. LDL-cholesterol was calculated with the Friedewald for-mula. Apolipoprotein B (apoB) was quantified by immunonephelometry[21]. Plasma lipoprotein(a) was measured by an in-house ELISA usingpurified IgG polyclonal antibodies to apolipoprotein(a) developed in arabbit [22]. Intra- and interassay coefficients of variation of the assayamounted 3.1% and 8%, respectively. For measurement of oxLDL acommercial non-competitive ELISA (Mercodia, Uppsala, Sweden) wasused. The assay uses monoclonal antibody 4E6 to specifically captureoxidized apoB from the sample, which is subsequently detected with anantibody to apoB. Intra- and interassay coefficients of variation of theassay amounted 6% and 7%, respectively. As shown previously by ourgroup [23] and confirmed recently by Holvoet et al. [24], oxLDL can bemeasured in EDTA plasma stored for longer periods (more than 15 years)at �80 �C, provided that the samples had been collected carefully and hadnot been thawed. Plasma annexin A5 and high-sensitivity C-reactiveprotein (hsCRP) were measured with commercial enzyme immunoassays(Hyphen BioMed, Neuville-sur-Oise, France, and Dako, Glastrup, Den-mark, respectively) according to the instructions of the manufacturers.Intra- and interassay coefficients of variation amounted 1.4% and 3.8% forannexin A5 assay and 6.0% and 9.7% for hsCRP assay, respectively.Because all samples had not been thawed since time of blood collection,hsCRP could be measured without reservation; annexin A5 is insensitiveto storage conditions.
Because we have previously shown that annexin A5 at physiologicalconcentrations binds to oxLDL, we examined whether this binding ofannexin A5 to oxLDL affects the measurement of oxLDL, and reversely,whether the presence of oxLDL influences the detection of annexin A5. Wefound that addition of annexin A5 (0.2–192 ng/ml, final concentration) didnot influence the detection of 6.5 mU/L oxLDL in plasma, and addition ofoxLDL (25–100 U/L, final concentration) did not influence the detectionof 5 ng/ml annexin A5 in plasma. This suggests that the measurement ofannexin A5 is not disturbed at increased plasma levels of oxLDL, and thatelevated levels of annexin A5 do not disturb the detection of oxLDL.
Statistical analysis. The Mann–Whitney test was used to comparebetween group differences in proportions. Between group comparisons ofcontinuous variables were performed with Student’s t-test for unpairedsamples. For triglycerides and time of cardiac complaints natural log-transformed data were tested. For hsCRP, lipoprotein(a), oxLDL, andannexin A5 age-standardized ln-values were calculated and tested. Tostandardize for age, the predicted value of a variable was calculated bylinear regression and subtracted from the measured value to which theoverall mean value of the variable was added. For presentation, mean and95% CI of ln-values were converted to normal. A p-value < 0.05 wasconsidered statistically significant. Analyses were performed using SPSS12.01 for Windows.

676 L.J.H. van Tits et al. / Biochemical and Biophysical Research Communications 356 (2007) 674–680
Results
Table 1 shows the characteristics of the study groups.Cases were slightly but significantly older than hospitalcontrols. Duration of cardiac complaints was longer forcases than for hospital controls and significantly morecases than hospital controls had history of myocardialinfarction, family history of cardiovascular disease, hyper-cholesterolemia and hypertension, and had experiencedangina pectoris. Significantly more cases than hospital con-trols reported medication use (antihypertensives, anti-thrombotics, and analgetics). Plasma lipid profile of caseswas more atherogenic than that of hospital controls: caseshad higher levels of total cholesterol, triglycerides, LDL-cholesterol and apoB, and lower levels of HDL-cholesterol.After standardization for age, the same statistical outcomeswere obtained (data not shown). No significant differenceswere observed between cases and hospital controls withrespect to body mass index, blood pressure, and smokinghabits (smoking and non-smoking).
Mean age of the population controls was slightly higherthan that of the hospital controls but similar to that of thecases (Table 1). In contrast to hospital subjects and accord-ing to the inclusion criteria, population controls had nohistory of angina pectoris, myocardial infarction or othercardiac complaints. The lipid profile of the population con-trols was not significantly different from that of hospitalcontrols (also after standardization for age), and showssimilar differences with the lipid profile of cases like thelipid profile of hospital controls does. Body mass indexand smoking habits of population controls were compara-
Table 1Characteristics of the groups studied
Population controls (n = 8
Age (years) 61.5 ± 7.9Time of cardiac complaints (years) 0Past occurence of angina pectoris (%) 0History of MI (%) 0Family history of CVD (%) 11Hypercholesterolemia (%) 18Hypertension (%) 24Medication (%) 13Total cholesterol (mmol/L) 5.4 ± 1.1Triglycerides (mmol/L) 1.51 (1.01–2.02)HDL-cholesterol (mmol/L) 1.02 ± 0.25LDL-cholesterol (mmol/L) 3.66 ± 1.00Apolipoprotein B (mg/L) 849 ± 195BMI (kg/m2) 26.3 ± 3.5Systolic blood pressure (mmHg) 136 ± 18Diastolic blood pressure (mmHg) 85 ± 10Smokers (%) 20
Data are presented as means ± SD or median (interquartile range).Standardization for age did not lead to different significances between lipids aHypercholesterolemia is defined as plasma total cholesterol >6.5 mmol/L or ublood pressure >95 mmHg or systolic blood pressure >160 mmHg or use of aantithrombotics and analgetics.MI, myocardial infarction; CVD, cardiovascular disease; BMI, body mass ind
a Denotes significant difference compared with population controls.b Denotes significant difference between cases and hospital controls.
ble to the hospital groups. Compared to hospital subjects,mean diastolic blood pressure of population controls washigher and significantly fewer subjects reported medication(antihypertensives, antithrombotics, and analgetics) andfamily history of cardiovascular disease, and fewer subjectshad hypertension. Hypercholesterolemia in populationcontrols was as frequent as in hospital controls and less fre-quent compared to cases.
Altogether, the data from Table 1 show an increase inthe frequency of cardiovascular disease risk factors (hyper-tension, hypercholesterolemia, and family history of car-diovascular disease) and in history and duration ofcardiovascular disease (myocardial infarction and anginapectoris) from population controls having no carotid pla-ques to subjects with no or minor coronary stenosis andsubjects with severe coronary stenosis.
Table 2 shows plasma levels of the cardiovascular riskfactors hsCRP and lipoprotein(a) and plasma levels ofoxLDL and annexin A5, all standardized for age, of thegroups studied. For hsCRP a significant difference wasfound only when comparing plasma levels of populationcontrols and cases. No differences were observed betweenthe groups for lipoprotein(a). With respect to oxLDLand annexin A5 significant differences were observedbetween all groups studied. Plasma oxLDL was higher inhospital controls than in population controls and highestin cases. On contrary, annexin A5 was highest in popula-tion controls and lowest in cases. Thus, whereas hsCRPdid not show a significant difference between patients with-out and with severe coronary stenosis, plasma oxLDL, andannexin A5 did. Percentage differences between groups,
7) Hospital controls (n = 96) Cases (n = 90)
59.0 ± 8.8a 61.8 ± 9.3b
0.5 (0.3–1.5)a 0.8 (0.3–5.8)a,b
27a 67a,b
4a 33a,b
22a 35a,b
17 33a,b
69a 83a,b
74a 89a,b
5.6 ± 0.9 6.0 ± 1.2a,b
1.56 (1.17–2.03) 1.92 (1.45–2.36)a,b
1.00 ± 0.29 0.85 ± 0.20a,b
3.87 ± 0.93 4.22 ± 1.13 a,b
892 ± 181 990 ± 184a,b
26.0 ± 3.0 26.5 ± 2.5135 ± 17 133 ± 1882 ± 8a 82 ± 8a
22 14
nd lipoproteins.se of cholesterol lowering medication; hypertension is defined as diastolicntihypertensive medication; medication includes use of antihypertensives,
ex.
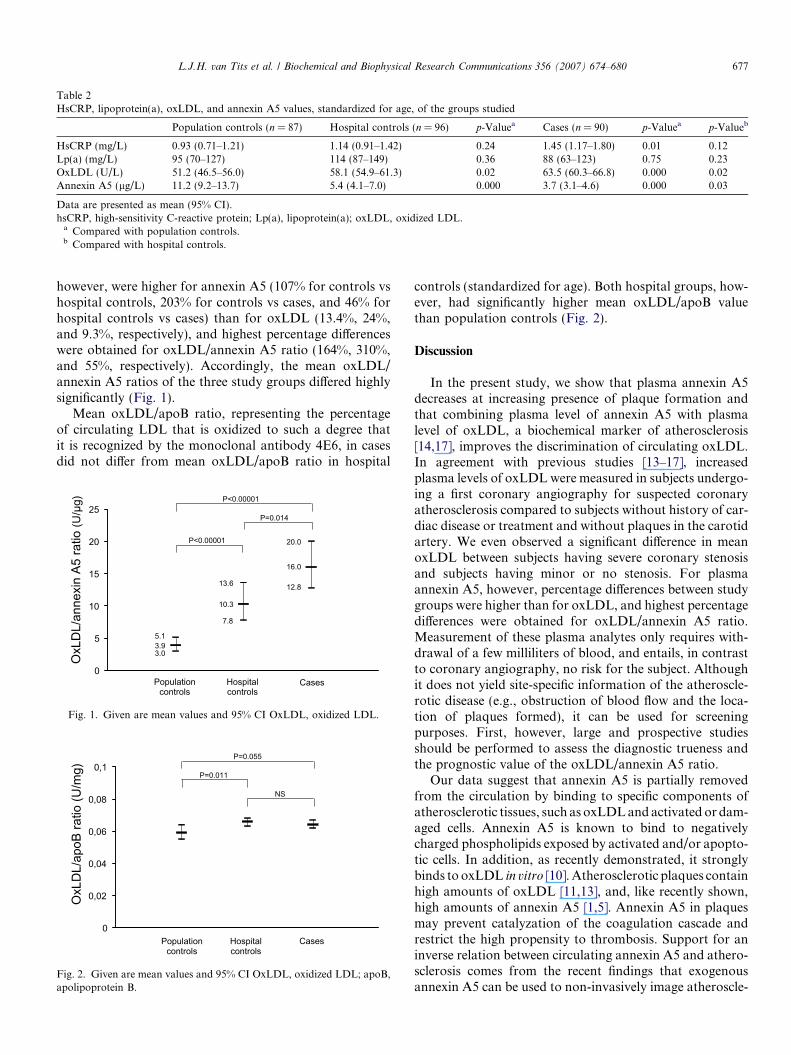
Table 2HsCRP, lipoprotein(a), oxLDL, and annexin A5 values, standardized for age, of the groups studied
Population controls (n = 87) Hospital controls (n = 96) p-Valuea Cases (n = 90) p-Valuea p-Valueb
HsCRP (mg/L) 0.93 (0.71–1.21) 1.14 (0.91–1.42) 0.24 1.45 (1.17–1.80) 0.01 0.12Lp(a) (mg/L) 95 (70–127) 114 (87–149) 0.36 88 (63–123) 0.75 0.23OxLDL (U/L) 51.2 (46.5–56.0) 58.1 (54.9–61.3) 0.02 63.5 (60.3–66.8) 0.000 0.02Annexin A5 (lg/L) 11.2 (9.2–13.7) 5.4 (4.1–7.0) 0.000 3.7 (3.1–4.6) 0.000 0.03
Data are presented as mean (95% CI).hsCRP, high-sensitivity C-reactive protein; Lp(a), lipoprotein(a); oxLDL, oxidized LDL.
a Compared with population controls.b Compared with hospital controls.
L.J.H. van Tits et al. / Biochemical and Biophysical Research Communications 356 (2007) 674–680 677
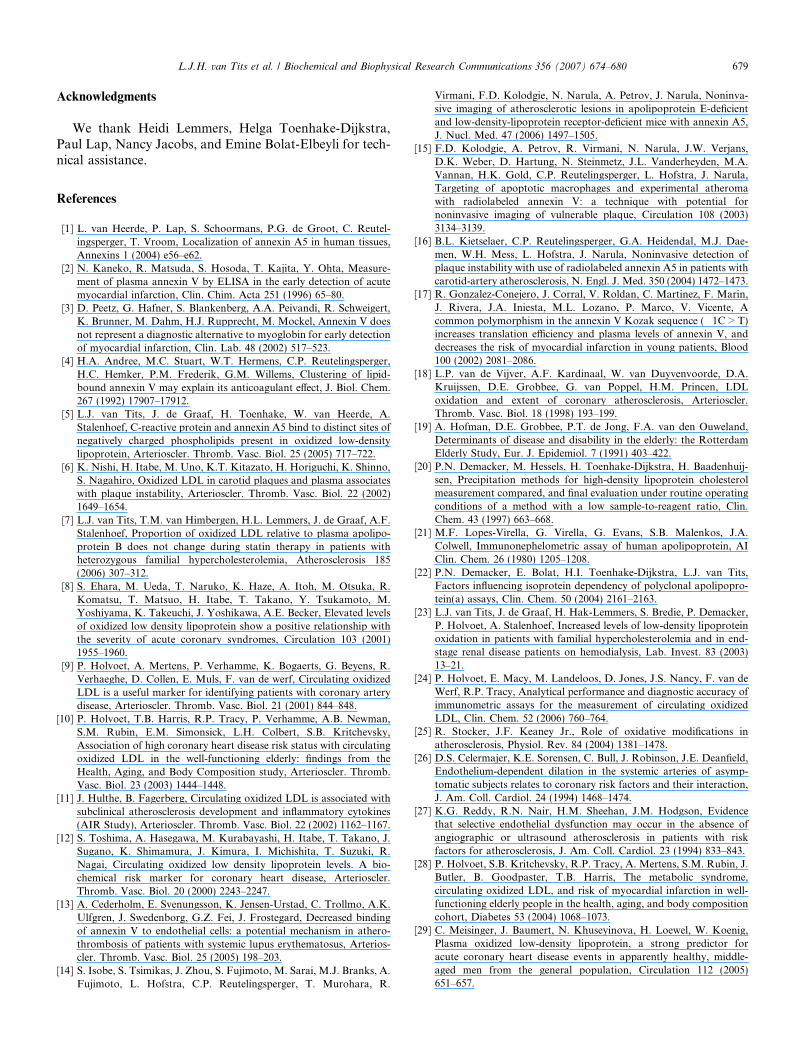
however, were higher for annexin A5 (107% for controls vshospital controls, 203% for controls vs cases, and 46% forhospital controls vs cases) than for oxLDL (13.4%, 24%,and 9.3%, respectively), and highest percentage differenceswere obtained for oxLDL/annexin A5 ratio (164%, 310%,and 55%, respectively). Accordingly, the mean oxLDL/annexin A5 ratios of the three study groups differed highlysignificantly (Fig. 1).
Mean oxLDL/apoB ratio, representing the percentageof circulating LDL that is oxidized to such a degree thatit is recognized by the monoclonal antibody 4E6, in casesdid not differ from mean oxLDL/apoB ratio in hospital
0
5
10
15
20
25
/LDLx
Oixenna
itar 5A n o
/U(
)gµ
Cases Population controls
Hospital controls
3.9 5.1
3.0
7.8
13.6
10.3
16.0
20.0
12.8
P=0.014
P<0.00001
P<0.00001
Fig. 1. Given are mean values and 95% CI OxLDL, oxidized LDL.
0
0,02
0,04
0,06
0,08
0,1
/LDLx
Oitar Bopa
/U( o
)gm
Population controls
Hospital controls
Cases
P=0.055
P=0.011
NS
Fig. 2. Given are mean values and 95% CI OxLDL, oxidized LDL; apoB,apolipoprotein B.
controls (standardized for age). Both hospital groups, how-ever, had significantly higher mean oxLDL/apoB valuethan population controls (Fig. 2).
Discussion
In the present study, we show that plasma annexin A5decreases at increasing presence of plaque formation andthat combining plasma level of annexin A5 with plasmalevel of oxLDL, a biochemical marker of atherosclerosis[14,17], improves the discrimination of circulating oxLDL.In agreement with previous studies [13–17], increasedplasma levels of oxLDL were measured in subjects undergo-ing a first coronary angiography for suspected coronaryatherosclerosis compared to subjects without history of car-diac disease or treatment and without plaques in the carotidartery. We even observed a significant difference in meanoxLDL between subjects having severe coronary stenosisand subjects having minor or no stenosis. For plasmaannexin A5, however, percentage differences between studygroups were higher than for oxLDL, and highest percentagedifferences were obtained for oxLDL/annexin A5 ratio.Measurement of these plasma analytes only requires with-drawal of a few milliliters of blood, and entails, in contrastto coronary angiography, no risk for the subject. Althoughit does not yield site-specific information of the atheroscle-rotic disease (e.g., obstruction of blood flow and the loca-tion of plaques formed), it can be used for screeningpurposes. First, however, large and prospective studiesshould be performed to assess the diagnostic trueness andthe prognostic value of the oxLDL/annexin A5 ratio.
Our data suggest that annexin A5 is partially removedfrom the circulation by binding to specific components ofatherosclerotic tissues, such as oxLDL and activated or dam-aged cells. Annexin A5 is known to bind to negativelycharged phospholipids exposed by activated and/or apopto-tic cells. In addition, as recently demonstrated, it stronglybinds to oxLDL in vitro [10]. Atherosclerotic plaques containhigh amounts of oxLDL [11,13], and, like recently shown,high amounts of annexin A5 [1,5]. Annexin A5 in plaquesmay prevent catalyzation of the coagulation cascade andrestrict the high propensity to thrombosis. Support for aninverse relation between circulating annexin A5 and athero-sclerosis comes from the recent findings that exogenousannexin A5 can be used to non-invasively image atheroscle-

678 L.J.H. van Tits et al. / Biochemical and Biophysical Research Communications 356 (2007) 674–680
rosis [7–9]. The uptake of radiolabeled annexin A5 by aortictissue correlated with both macrophage burden and theextent of apoptosis and it was proposed that radiolabeledannexin A5 marks vulnerable plaques. Thus, a decreasedplasma level of annexin A5, like found in the present studyin men undergoing coronary angiography, may indicatethe presence and extent of plaque formation. This may notapply to unstable cardiovascular conditions, however,because it has been reported that acutely after myocardialinfarction annexin A5 is released from cardiomyocytes [2].Furthermore, also traumatic injury and other diseases mayconfound the relation between plasma annexin A5 and ath-erosclerosis due to release of annexin A5 from cells [3,5].
The difference in mean oxLDL between subjects havingsevere coronary stenosis and those with minor or no steno-sis appeared to be due to differences in the lipid profile (ormore specifically apoB) between these groups, because bothgroups showed no difference in mean oxLDL/apoB ratio.Remarkably, however, both hospital groups had elevatedmean oxLDL/apoB value compared to the healthy popula-tion controls having no history of cardiac disease. It ishypothesized that the plasma oxLDL/apoB ratio reflectsthe oxidative condition of the vessel wall [11,12]. Accord-ingly, our data suggest that most of the subjects undergo-ing a first coronary angiography for suspected coronaryatherosclerosis, are characterized by increased oxidativestress, irrespective of the severity of coronary stenosis. Thisindependency of the severity of stenosis is not surprising,because stenosis is a clinical symptom that is the result ofa chronic persisting diseased condition of which oxidativestress is one component. Oxidative stress has been shownto contribute to the development of endothelial dysfunc-tion [25], an abnormality which can be detected beforestructural changes to the vessel wall are apparent on angi-ography or ultrasound [26,27]. It is very likely that in ourstudy the hospital controls as well as the cases have endo-thelial dysfunction. Unfortunately, no assessment of endo-thelial function was performed on subjects of the presentstudy. It would be interesting to investigate whether theoxLDL/apoB ratio correlates with endothelial function inprospective studies. Plasma oxLDL and endothelial dys-function have been shown to be associated with a higherrisk of subsequent cardiac events in the general populationas well as in patients with stable coronary artery disease[28–35] and persistence of an increased level of plasmaoxLDL relative to apolipoprotein B after acute myocardialinfarction is a strong independent predictor of stent reste-nosis at 6-month follow-up [36]. Thus, our findings suggestthat all male subjects undergoing a first coronary angiogra-phy for suspected coronary atherosclerosis, irrespective ofthe severity of coronary stenosis, are biochemically at riskand should be adequately monitored.
Limitations
The study population gives cause for some limitations.First, only men were studied. Second, divergent methods
(coronary angiography vs carotid ultrasound) wereapplied for different study groups. Carotid ultrasound isan established technique to assess subclinical atherosclero-sis, which in addition can be performed on normalhealthy volunteers without any risk. On the other hand,coronary angiography is not accurate to assess atheroscle-rotic disease because plaques are often not visible due totheir small size and compensatory enlargement. Untiltoday, however, it is the most common method used inevery-day clinical practice to assess coronary heart dis-ease. Because we ascertained the absence of plaques inthe carotid arteries of the population controls by ultra-sound and observed more cardiovascular risk factors inhospital controls, it is justifiable to suppose that the aver-age value of plaque formation is higher in hospital con-trols than in population controls. Similarly, because ofthe increased presence of other cardiovascular disease riskfactors in addition to much higher level of coronary ste-nosis, we think that cases have more extensive atheroscle-rotic cardiovascular disease than hospital controls.Naturally, more sensitive intravascular or non-invasivetechniques (intravascular ultrasound, elastography, angi-oscopy, magnetic resonance, and multislice computedtomography) would have provided a more accurate char-acterization of the disease in the hospital subjects. Thepresent finding is that the plasma ratio of oxLDL/annexinA5 differs significantly between patients with severe coro-nary stenosis and those with no or only minor coronarystenosis, calls on to study this ratio in patients whose car-diovascular disease is characterized by such advancedtechniques.
Another limitation of the study concerns the age ofthe plasma samples. Although it has not yet been stud-ied whether levels of oxLDL are influenced by long-term storage, Holvoet et al. recently demonstrated thatoxLDL can be measured in samples that have beenstored for more than 15 years [24], provided that theyhad been collected carefully and had not been thawed.All of our samples fulfilled these criteria. Moreover,samples of controls and patients were stored for a sim-ilar period (justifying their mutual comparison) and lev-els of oxLDL measured in the population controls donot deviate from those found in fresh samples ofhealthy volunteers [24], suggesting that the levels ofoxLDL have not seriously changed due to storage.Annexin A5 is very stable and insensitive to storageconditions.
Conclusions
Plasma annexin A5 is decreased at severe coronarystenosis and the oxLDL/annexin A5 ratio is a bettermarker of the severity of coronary stenosis than oxLDLalone. The oxLDL/annexin A5 ratio may reflect the pres-ence and extent of the atherosclerotic cardiovascular dis-ease and might prove useful for preclinical screeningpurposes.
L.J.H. van Tits et al. / Biochemical and Biophysical Research Communications 356 (2007) 674–680 679
Acknowledgments
We thank Heidi Lemmers, Helga Toenhake-Dijkstra,Paul Lap, Nancy Jacobs, and Emine Bolat-Elbeyli for tech-nical assistance.
References
[1] L. van Heerde, P. Lap, S. Schoormans, P.G. de Groot, C. Reutel-ingsperger, T. Vroom, Localization of annexin A5 in human tissues,Annexins 1 (2004) e56–e62.
[2] N. Kaneko, R. Matsuda, S. Hosoda, T. Kajita, Y. Ohta, Measure-ment of plasma annexin V by ELISA in the early detection of acutemyocardial infarction, Clin. Chim. Acta 251 (1996) 65–80.
[3] D. Peetz, G. Hafner, S. Blankenberg, A.A. Peivandi, R. Schweigert,K. Brunner, M. Dahm, H.J. Rupprecht, M. Mockel, Annexin V doesnot represent a diagnostic alternative to myoglobin for early detectionof myocardial infarction, Clin. Lab. 48 (2002) 517–523.
[4] H.A. Andree, M.C. Stuart, W.T. Hermens, C.P. Reutelingsperger,H.C. Hemker, P.M. Frederik, G.M. Willems, Clustering of lipid-bound annexin V may explain its anticoagulant effect, J. Biol. Chem.267 (1992) 17907–17912.
[5] L.J. van Tits, J. de Graaf, H. Toenhake, W. van Heerde, A.Stalenhoef, C-reactive protein and annexin A5 bind to distinct sites ofnegatively charged phospholipids present in oxidized low-densitylipoprotein, Arterioscler. Thromb. Vasc. Biol. 25 (2005) 717–722.
[6] K. Nishi, H. Itabe, M. Uno, K.T. Kitazato, H. Horiguchi, K. Shinno,S. Nagahiro, Oxidized LDL in carotid plaques and plasma associateswith plaque instability, Arterioscler. Thromb. Vasc. Biol. 22 (2002)1649–1654.
[7] L.J. van Tits, T.M. van Himbergen, H.L. Lemmers, J. de Graaf, A.F.Stalenhoef, Proportion of oxidized LDL relative to plasma apolipo-protein B does not change during statin therapy in patients withheterozygous familial hypercholesterolemia, Atherosclerosis 185(2006) 307–312.
[8] S. Ehara, M. Ueda, T. Naruko, K. Haze, A. Itoh, M. Otsuka, R.Komatsu, T. Matsuo, H. Itabe, T. Takano, Y. Tsukamoto, M.Yoshiyama, K. Takeuchi, J. Yoshikawa, A.E. Becker, Elevated levelsof oxidized low density lipoprotein show a positive relationship withthe severity of acute coronary syndromes, Circulation 103 (2001)1955–1960.
[9] P. Holvoet, A. Mertens, P. Verhamme, K. Bogaerts, G. Beyens, R.Verhaeghe, D. Collen, E. Muls, F. van de werf, Circulating oxidizedLDL is a useful marker for identifying patients with coronary arterydisease, Arterioscler. Thromb. Vasc. Biol. 21 (2001) 844–848.
[10] P. Holvoet, T.B. Harris, R.P. Tracy, P. Verhamme, A.B. Newman,S.M. Rubin, E.M. Simonsick, L.H. Colbert, S.B. Kritchevsky,Association of high coronary heart disease risk status with circulatingoxidized LDL in the well-functioning elderly: findings from theHealth, Aging, and Body Composition study, Arterioscler. Thromb.Vasc. Biol. 23 (2003) 1444–1448.
[11] J. Hulthe, B. Fagerberg, Circulating oxidized LDL is associated withsubclinical atherosclerosis development and inflammatory cytokines(AIR Study), Arterioscler. Thromb. Vasc. Biol. 22 (2002) 1162–1167.
[12] S. Toshima, A. Hasegawa, M. Kurabayashi, H. Itabe, T. Takano, J.Sugano, K. Shimamura, J. Kimura, I. Michishita, T. Suzuki, R.Nagai, Circulating oxidized low density lipoprotein levels. A bio-chemical risk marker for coronary heart disease, Arterioscler.Thromb. Vasc. Biol. 20 (2000) 2243–2247.
[13] A. Cederholm, E. Svenungsson, K. Jensen-Urstad, C. Trollmo, A.K.Ulfgren, J. Swedenborg, G.Z. Fei, J. Frostegard, Decreased bindingof annexin V to endothelial cells: a potential mechanism in athero-thrombosis of patients with systemic lupus erythematosus, Arterios-cler. Thromb. Vasc. Biol. 25 (2005) 198–203.
[14] S. Isobe, S. Tsimikas, J. Zhou, S. Fujimoto, M. Sarai, M.J. Branks, A.Fujimoto, L. Hofstra, C.P. Reutelingsperger, T. Murohara, R.
Virmani, F.D. Kolodgie, N. Narula, A. Petrov, J. Narula, Noninva-sive imaging of atherosclerotic lesions in apolipoprotein E-deficientand low-density-lipoprotein receptor-deficient mice with annexin A5,J. Nucl. Med. 47 (2006) 1497–1505.
[15] F.D. Kolodgie, A. Petrov, R. Virmani, N. Narula, J.W. Verjans,D.K. Weber, D. Hartung, N. Steinmetz, J.L. Vanderheyden, M.A.Vannan, H.K. Gold, C.P. Reutelingsperger, L. Hofstra, J. Narula,Targeting of apoptotic macrophages and experimental atheromawith radiolabeled annexin V: a technique with potential fornoninvasive imaging of vulnerable plaque, Circulation 108 (2003)3134–3139.
[16] B.L. Kietselaer, C.P. Reutelingsperger, G.A. Heidendal, M.J. Dae-men, W.H. Mess, L. Hofstra, J. Narula, Noninvasive detection ofplaque instability with use of radiolabeled annexin A5 in patients withcarotid-artery atherosclerosis, N. Engl. J. Med. 350 (2004) 1472–1473.
[17] R. Gonzalez-Conejero, J. Corral, V. Roldan, C. Martinez, F. Marin,J. Rivera, J.A. Iniesta, M.L. Lozano, P. Marco, V. Vicente, Acommon polymorphism in the annexin V Kozak sequence (�1C > T)increases translation efficiency and plasma levels of annexin V, anddecreases the risk of myocardial infarction in young patients, Blood100 (2002) 2081–2086.
[18] L.P. van de Vijver, A.F. Kardinaal, W. van Duyvenvoorde, D.A.Kruijssen, D.E. Grobbee, G. van Poppel, H.M. Princen, LDLoxidation and extent of coronary atherosclerosis, Arterioscler.Thromb. Vasc. Biol. 18 (1998) 193–199.
[19] A. Hofman, D.E. Grobbee, P.T. de Jong, F.A. van den Ouweland,Determinants of disease and disability in the elderly: the RotterdamElderly Study, Eur. J. Epidemiol. 7 (1991) 403–422.
[20] P.N. Demacker, M. Hessels, H. Toenhake-Dijkstra, H. Baadenhuij-sen, Precipitation methods for high-density lipoprotein cholesterolmeasurement compared, and final evaluation under routine operatingconditions of a method with a low sample-to-reagent ratio, Clin.Chem. 43 (1997) 663–668.
[21] M.F. Lopes-Virella, G. Virella, G. Evans, S.B. Malenkos, J.A.Colwell, Immunonephelometric assay of human apolipoprotein, AIClin. Chem. 26 (1980) 1205–1208.
[22] P.N. Demacker, E. Bolat, H.I. Toenhake-Dijkstra, L.J. van Tits,Factors influencing isoprotein dependency of polyclonal apolipopro-tein(a) assays, Clin. Chem. 50 (2004) 2161–2163.
[23] L.J. van Tits, J. de Graaf, H. Hak-Lemmers, S. Bredie, P. Demacker,P. Holvoet, A. Stalenhoef, Increased levels of low-density lipoproteinoxidation in patients with familial hypercholesterolemia and in end-stage renal disease patients on hemodialysis, Lab. Invest. 83 (2003)13–21.
[24] P. Holvoet, E. Macy, M. Landeloos, D. Jones, J.S. Nancy, F. van deWerf, R.P. Tracy, Analytical performance and diagnostic accuracy ofimmunometric assays for the measurement of circulating oxidizedLDL, Clin. Chem. 52 (2006) 760–764.
[25] R. Stocker, J.F. Keaney Jr., Role of oxidative modifications inatherosclerosis, Physiol. Rev. 84 (2004) 1381–1478.
[26] D.S. Celermajer, K.E. Sorensen, C. Bull, J. Robinson, J.E. Deanfield,Endothelium-dependent dilation in the systemic arteries of asymp-tomatic subjects relates to coronary risk factors and their interaction,J. Am. Coll. Cardiol. 24 (1994) 1468–1474.
[27] K.G. Reddy, R.N. Nair, H.M. Sheehan, J.M. Hodgson, Evidencethat selective endothelial dysfunction may occur in the absence ofangiographic or ultrasound atherosclerosis in patients with riskfactors for atherosclerosis, J. Am. Coll. Cardiol. 23 (1994) 833–843.
[28] P. Holvoet, S.B. Kritchevsky, R.P. Tracy, A. Mertens, S.M. Rubin, J.Butler, B. Goodpaster, T.B. Harris, The metabolic syndrome,circulating oxidized LDL, and risk of myocardial infarction in well-functioning elderly people in the health, aging, and body compositioncohort, Diabetes 53 (2004) 1068–1073.
[29] C. Meisinger, J. Baumert, N. Khuseyinova, H. Loewel, W. Koenig,Plasma oxidized low-density lipoprotein, a strong predictor foracute coronary heart disease events in apparently healthy, middle-aged men from the general population, Circulation 112 (2005)651–657.

680 L.J.H. van Tits et al. / Biochemical and Biophysical Research Communications 356 (2007) 674–680
[30] F.G. Nordin, B. Hedblad, G. Berglund, J. Nilsson, Plasma oxidizedLDL: a predictor for acute myocardial infarction? J. Intern. Med. 253(2003) 425–429.
[31] K. Shimada, H. Mokuno, E. Matsunaga, T. Miyazaki, K. Sumiyoshi,K. Miyauchi, H. Daida, Circulating oxidized low-density lipoproteinis an independent predictor for cardiac event in patients withcoronary artery disease, Atherosclerosis 174 (2004) 343–347.
[32] J.P. Halcox, W.H. Schenke, G. Zalos, R. Mincemoyer, A. Prasad, M.A.Waclawiw, K.R. Nour, A.A. Quyyumi, Prognostic value of coronaryvascular endothelial dysfunction, Circulation 106 (2002) 653–658.
[33] T. Neunteufl, S. Heher, R. Katzenschlager, G. Wolfl, K. Kostner, G.Maurer, F. Weidinger, Late prognostic value of flow-mediateddilation in the brachial artery of patients with chest pain, Am. J.Cardiol. 86 (2000) 207–210.
[34] V. Schachinger, M.B. Britten, A.M. Zeiher, Prognostic impactof coronary vasodilator dysfunction on adverse long-termoutcome of coronary heart disease, Circulation 101 (2000)1899–1906.
[35] J.A. Suwaidi, S. Hamasaki, S.T. Higano, R.A. Nishimura, D.R.Holmes Jr., A. Lerman, Long-term follow-up of patients with mildcoronary artery disease and endothelial dysfunction, Circulation 101(2000) 948–954.
[36] T. Naruko, M. Ueda, S. Ehara, A. Itoh, K. Haze, N. Shirai, Y.Ikura, M. Ohsawa, H. Itabe, Y. Kobayashi, H. Yamagishi, M.Yoshiyama, J. Yoshikawa, E.A. Becker, Persistent high levels ofplasma oxidized low-density lipoprotein after acute myocardialinfarction predict stent restenosis, Arterioscler. Thromb. Vasc. Biol.26 (2006) 877–883.