retroviruses and autoimmunity - j-stage
TRANSCRIPT

REVIEW ARTICLE
Retroviruses and AutoimmunityIwao Sekigawa, Hitoshi Ogasawara*, Hiroshi Kaneko*, Takashi Hishikawa* and Hiroshi Hashimoto*
Abstract
The investigation of humanretroviruses has showndra-matic progress since the discovery of human immunodefi-ciency virus (HIV). These studies have also contributed tothe exploration of the role of retroviruses, including endog-enous retroviruses, in the induction of autoimmune diseasessuch as systemic lupus erythematosus (SLE). This reviewdescribes the potential role of retroviruses in autoimmu-nity, based on recent findings including our own results.(Internal Medicine 40: 80-86, 2001)
Key words: human immunodeficiency virus, human endog-enous retrovirus, systemic lupus erythematosus
Introduction
Retroviruses, including endogenous retroviruses, have re-peatedly been suggested as etiological factors for autoimmunerheumatic diseases such as SLE (1-4). Extensive studies per-formed during the last decade on the molecular biology of HIV-1 and human T cell leukemia virus (HTLV)-l have providedboth the intellectual framework and the molecular methods totest whether human retroviruses may be involved in the patho-genesis of a wide spectrum of autoimmune phenomena. In ad-dition, marked advances in our knowledge of human endog-enous retroviruses (HERV)have contributed to the investiga-tion of their role in the pathogenesis of humanautoimmunediseases. Onthe basis of recent results obtained at our labora-tory, we here review the virological and immunological prop-erties of human retroviruses that may be involved in the induc-tion of autoimmunity, especially the SLE- and HIV-relatedautoimmunephenomena.
Retroviruses and Autoimmunity
Retroviruses are plus strand RNAviruses with a modeofreplication in which the RNAgenome is transcribed into DNAby reverse transcriptase (RT) and is integrated into the hostgenome as a provirus. Twoidentical elements (the long termi-
nal repeats: LTRs) are reconstituted at the 5' and 3' ends of theprovirus, which contain the promoter, enhancer, and repressorsequences for tissue-specific expression. All genera ofretroviruses encode three basic genes, which are expressed andprocessed as polyproteins: gag encoding the core proteins, polencoding the RT, and env encoding the envelope proteins. Whileexogenous retroviruses such as HIVand HTLVcan reproduceviral RNAand viral particles from their proviral DNA, endog-enous retroviruses have generally lost the competence to repli-cate viral proteins because of several interrupters, includingtermination codons, deletions, frameshift mutations, or me-thylation sites. Endogenousretroviruses are knownto exist notonly in animals, but also in the genomic DNAof humans; ap-proximately 20 HERVfamilies have been reported to date, allof which are inherited in a Mendelian fashion (3, 5-8). Theprecise origin of HERVremains unclear, but certain HERV-related sequences can be traced back to the time of the diver-gence of Old and NewWorld monkeys (25-30 million yearsago) (7, 9). HERVare estimated to compose up to 0.1-0.6% ofhumanDNAand thus contribute substantially to the architec-ture of the human genome (10). Recent studies have revealedthat certain HERVcan undergo transcriptional and translationalactivation that results in HERVprotein expression and HERVparticle formation (3, 6, 1 1).The possibility that retroviruses may play an etiologic rolein various autoimmune diseases (such as rheumatoid arthritis,Sjogren's syndrome, mixed connective tissue diseases, inflam-matory neurologic diseases, and SLE) has long been discussed(3). A role for retroviruses as an etiologic factor in SLE is sup-ported by the following evidence: 1) the importance of endog-enous retroviruses in mouse models of SLE (12-14); 2) thedetection of antibodies, antigens, and sequences for animal andhumanretroviral components in the organs and serum of pa-tients with autoimmune diseases such as SLE (15-23); 3) elec-tron microscopic detection of unknownretroviral particles inthe organs of SLE patients (24); 4) the finding that viral com-ponents derived from endogenousor exogenousretrovirusescan induce the immune abnormalities observed in SLE (25-27); and 5) the similarity of autoimmune manifestations andimmune dysregulation between patients with SLEand thoseinfected with known human retroviruses such as HIV-1 (4, 28).
From the Department of Medicine, Juntendo University Izu-Nagaoka Hospital, Shizuoka and *the Department of Internal Medicine and Rheumatology,Juntendo University School of Medicine, Tokyo
Reprint requests should be addressed to Dr. Iwao Sekigawa, the Department of Medicine, Juntendo University Izu-Nagaoka Hospital, 1 129 Nagaoka, Izu-Nagaoka-cho, Tagata-gun, Shizuoka 4 1 0-2295
80 Internal Medicine Vol. 40, No. 2 (February 2001)

Retroviruses and Autoimmunity
HIV and AutoimmunityThe mechanisms of autoimmunity in HIV- 1 infection havebeen aggressively debated. Several autoantibodies, includingantinuclear antibody, anti-cardiolipin antibody, anti-plateletantibody, and anti-lymphocyte antibody can be detected in theserum of HIV-infected patients. T cell and B cell dysfunctionassociated with HIV-1 infection is knownto be similar to thatobserved in SLE, including T cell activation (implied by theexpression of HLAclass II molecules), T cell anergy (indi-cated by a decrease of the mixed lymphocyte reaction (MLR)and by a decline of mitogen/antigen-mediated interleukin (IL)-2 production and cell proliferation), and polyclonal B cell acti-vation (PBA) involving cytokines such as IL-6 and tumor ne-crosis factor (TNF)-oc (4). CD4+T cell anergy (a weak responseor unresponsiveness to antigen specific or nonspecific stimuli)is known to be closely related to its activation in SLE patients(29). HIV-1 infection is initiated by binding between HIV-1envelope glycoprotein (gpl20) and CD4 molecules (Dl do-main) on T cells, although HIValso employs receptors forchemokines as co-receptors. HIV-1 gpl20 is known to play animportant role in the immunedysregulation associated withHIV- 1 infection, including the SLE-like phenomena describedabove, either directly or via the stimulation of cytokine pro-duction (30-41). The features of gp l20-mediated immune dys-function are summarized in Table 1, based upon reported re-sults including our own. As shownin this table, someaspectsof gpl20-mediated T and B cell dysfunction are enhanced bycytokines, especially TNF-oc, derived from gp l 20-stimulatedmacrophages. Various events affecting in CD4+T cells, such asloss of CD4molecules (due to down-modulation or apoptosis),T cell receptor (TCR) inactivation, and blocking of conjuga-tion between CD4and the major histocompatibility complex(MHC),as well as CD4+T cell anergy related to the activation
(Table 1), mayinfluence the antigen recognition process andmay be a significant factor in the decline of self-tolerance andthe resultant induction of autoimmunity by HIV infection inaddition to PBA.Interestingly, the changes of in vivo and/or invitro cytokine and chemokine productions with the progres-sion of HIV-1 infection are similar to those occurring in SLEwith an increase of disease activity, including an increase inthe production of T helper type 2 (Th2) cytokines and RANTES(regulated-upon activation, normal T expressed and secreted),as well as a decrease in the production ofT helper type 1 (Thl)cytokines and monocyte chemoattractant protein- 1 (MCP- 1)(42-45). Such changes of cytokine and chemokine productionare also regulated through stimulation by HIV envelope glyco-protein (46, 47). Furthermore, antibodies to CD4 moleculesare known to exist in 10-20% of HIV-1-infected patients andin 20-30% of SLE patients (48, 49). In SLE patients, theseantibodies can induce T cell anergy (49). Fluctuations in theproduction of cytokines, chemokines, and such autoantibodiesmaybe linked to the occurrence of SLE-like autoimmune phe-nomena in HIVinfection.In contrast, epidemiological studies have revealed that HIVinfection and SLE are rarely seen in the same patient. In fact,only 20 patients with a diagnosis of both SLE md HIV infec-tion,have been reported to date (50). Wepreviously reportedthat serum levels of IL-16 in SLE patients were significantlyhigher than in normal volunteers and that there wasa strongcorrelation between the IL- 16 level and the disease activity ofSLE (51). IL-16 is a CD8+T cell-derived cytokine that usesCD4 as its receptor (52) and can inhibit HIV-1 infection invitro (53). This cytokine also induces activation and anergy ofCD4+ T cells observed in SLE (52, 54, 55). Although severalpossibilities have been proposed, we think that IL-16 may havea protective effect against HIV infection in SLE patients andmaycontribute to the low incidence of the coexistence of bothdiseases (50).
Table 1. Immune Abnormalities Mediated by the Binding of HIV-1 gp!20 to CD4g p 1 2 0 -sti mu la te d ce ll I mm u n e a bn o r m al i t i e s ( r e f er e n c e s) T N F - c c d e p e n d e n c y
T ce ll 1. A ct iv a ti on o fp 56 l ck ( 35 , 37 , 4 1) (- )
2 . D o w n - m o d u l a t i o n o f C D 4 ( 3 5 , 4 1 ) (+ )(in te rn aliz atio n )
3 . CD 4 + T c el l a ct iv a ti on (4 1) (+ )( H LA c la s s I I e x pr e ss i o n)
4. CD 4 + T ce l l a n er g y ( 3 0, 4 1)
( s up p re s si o n o f I L- 2 p r od uc t i on ) (+ )( i nh i b i ti o n of M L R) (- )
5. CD 4 + T c el l a p op t os i s ( 34 , 3 9 ) (+ )6. T CR i na c t iv a t io n (3 7 ) (- )7 . B lo c k i n g o f b i n d i n g b e t w e e n C D 4 a n d M H C ( 3 1 ) (- )
M a c ro p h ag e 1 . C yt ok i ne p r od uc t io n ( IL -6 , I L- 1 0, T N F- oc , e tc . ),wi th re la ted T c ell ( 38 , 3 9, 41 ) (+ )an d B ce l l a bn o rm a li t ie s ( P BA ) ( 3 2, 33 , 3 6 ) (+ )
2 . D e c r e a s e o f C D 4 e x p r e ss i o n o n m a c ro p h a g e s ( 4 0 ) (+ )
Internal Medicine Vol. 40, No. 2 (February 2001 ) 81
Sekigawa et al
HERV and SLE
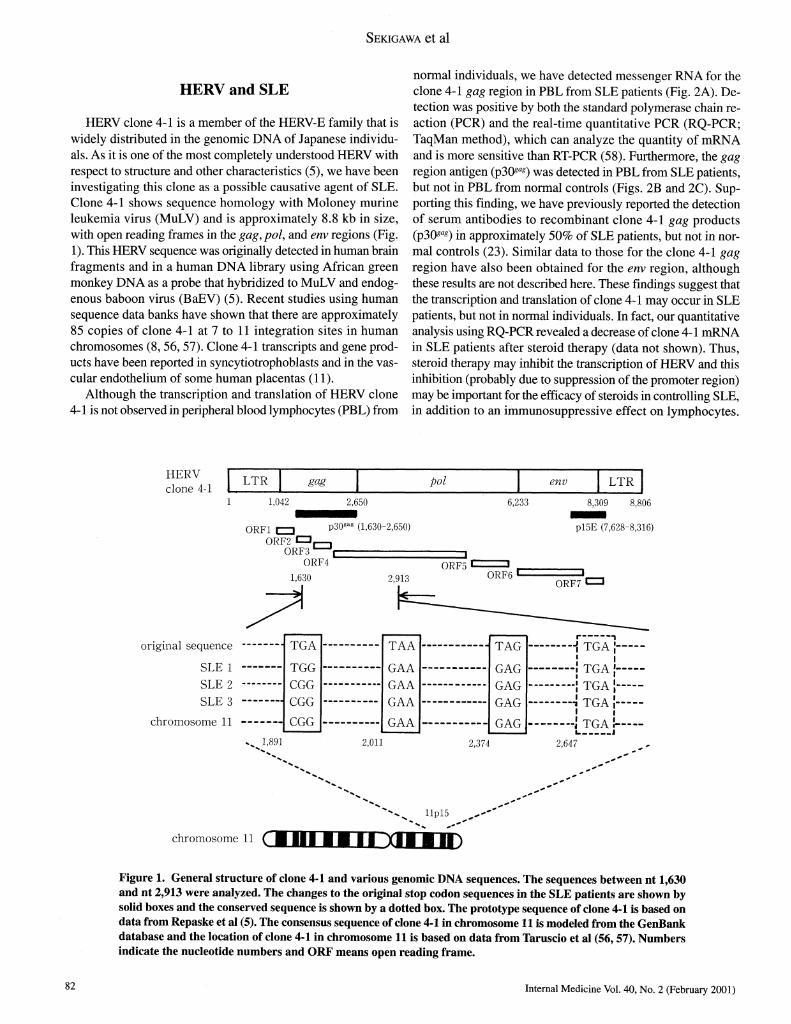
HERVclone 4-1 is a memberof the HERV-Efamily that iswidely distributed in the genomic DNAof Japanese individu-als. As it is one of the most completely understood HERVwithrespect to structure and other characteristics (5), we have beeninvestigating this clone as a possible causative agent of SLE.Clone 4-1 shows sequence homology with Moloney murineleukemia virus (MuLV) and is approximately 8.8 kb in size,with open reading frames in the gag, pol, and env regions (Fig.1). This HERVsequence was originally detected in human brainfragments and in a human DNAlibrary using African greenmonkey DNAas a probe that hybridized to MuLVand endog-enous baboon virus (BaEV) (5). Recent studies using humansequence data banks have shownthat there are approximately85 copies of clone 4-1 at 7 to ll integration sites in humanchromosomes (8, 56, 57). Clone 4-1 transcripts and gene prod-ucts have been reported in syncytiotrophoblasts and in the vas-cular endothelium of some human placentas (1 1).Although the transcription and translation of HERVclone
4- 1 is not observed in peripheral blood lymphocytes (PBL) from
normal individuals, we have detected messenger RNAfor theclone 4-1 gag region in PBL from SLE patients (Fig. 2A). De-tection was positive by both the standard polymerase chain re-action (PCR) and the real-time quantitative PCR (RQ-PCR;TaqManmethod), which can analyze the quantity of mRNAand is more sensitive than RT-PCR(58). Furthermore, the gagregion antigen (p3Oa*) was detected in PBL from SLE patients,but not in PBLfrom normal controls (Figs. 2B and 2C). Sup-porting this finding, we have previously reported the detectionof serum antibodies to recombinant clone 4-1 gag products(p3Oa*) in approximately 50% of SLE patients, but not in nor-mal controls (23). Similar data to those for the clone 4-1 gagregion have also been obtained for the env region, althoughthese results are not described here. These findings suggest thatthe transcription and translation of clone 4-1 may occur in SLEpatients, but not in normal individuals. In fact, our quantitativeanalysis using RQ-PCRrevealed a decrease of clone 4- 1 mRNAin SLE patients after steroid therapy (data not shown). Thus,steroid therapy may inhibit the transcription of HERVand thisinhibition (probably due to suppression of the promoter region)may be important for the efficacy of steroids in controlling SLE,in addition to an immunosuppressive effect on lymphocytes.
__I I I I I, ,. LTR gag pol env LTR
clone4-1 I I I 1_ I I
1 1,042 2,650 6,233 8,309 8,806
ORF1 CZD p3°gaS (i-630"2'650) P!5E (7,628-8,316)ORF2P,
ORF3' i 1
0RF4 ORF5 C=». .1630 ?Qis ORF6 à"------* .
i^u Z,yid QRF7 CZ3
original sequence TGA TAA - TAG -\ TGA |SLE1 TGG GAA GAG~ jTGAj
SLE 2 CGG GAA GAG | TGA |SLE 3 CGG GAA GAG -J TGA J
i ic hromosome ll CGG GAA GAG J TGA !I 1 I 1 I 1 i j
^1,891 2,011 2,374 2,647
"^-^ Hpl5 ^~'*~
chromosomell ( BUI H |B ^Cft B11^)
Figure 1. General structure of clone 4-1 and various genomic DNAsequences. The sequences between nt 1,630and nt 2,913 were analyzed. The changes to the original stop codon sequences in the SLEpatients are shown bysolid boxes and the conserved sequence is shown by a dotted box. The prototype sequence of clone 4-1 is based ondata from Repaske et al (5). The consensus sequence of clone 4-1 in chromosomell is modeled from the GenBankdatabase and the location of clone 4-1 in chromosome ll is based on data from Taruscio et al (56, 57). Numbersindicate the nucleotide numbersand ORFmeans open reading frame.
82 Internal Medicine Vol. 40, No. 2 (February 2001)

Retroviruses and Autoimmunity
M l 2 3 4 5 6 7 8
bp1 QCQ - -** aJMIl^ML --à"å --̂ ^j^g^g^.
1,078 HH^^^^H^ ^^^å å W^g^ !
603 ^^^^^^^^H|310 HH^^^^^^^^^^^^^^^^lHfi ; A
Figure 2. Detection of clone 4-1 mRNAand p3&"s antigen in PBL. An approximately 600 bp fragment of the clone 4-1 gag regionwas amplified by RT-PCR using two gag primers (primer 1; nt 1,651-1,668, and primer 2; nt 2,238-2,250), (SLE patientswithout steroid treatment; lanes 1-5, normal individuals; lanes 6-8, Lane M; molecular weight marker) (A). PBL were stainedwith goat anti-MuLV pW*"* antibody, which reacted with recombinant clone 4-1 P308"8 as reported previously (23), and withfluorescein isothiocyanate (FITC)-labeled rabbit F(ab')2 anti-goat inimunoglobulin (Cappel Laboratories, West Chester, PA) asthe secondary antibody. A positive reaction was observed in SLE PBL(B), but not in normal PBL (C).
Interestingly, other immunosuppressants (cyclosporin A andFK506) have been shown to inhibit the promoter activity ofHIV provirus integrated into the human genome, thus suppress-
ing its transcription (59).Wehave found that 5-aza-deoxycytidine, a demethylating
agent, causes a quantitative increase of clone 4-1 gag mRNA
Internal Medicine Vol. 40, No. 2 (February 2001) 83

Sekigawa et al
(detected by RQ-PCR) in normal control lymphocytes (datanot shown). Thus, methylation of DNAmay be important forinhibiting clone 4- 1 gene transcription in normal individualsand preventing the production of its proteins, and this may alsobe true for other HERV(60). With reference to this point, somedrugs such as procainamide and hydralazine, which have ademethylating effect, are knownto occasionally trigger an SLE-like illness, especially in genetically predisposed individuals(6 1). These drugs maypromote the transcription of endogenousantigen-related genomic DNA, including HERVDNA, throughdemethylation and thus elicit autoimmunephenomena.Inter-estingly, however, the stimulation of mitogens such as li-popolysaccharide (LPS), concanavalin A (Con A), and phyto-hemagglutinin (PHA) does not induce a quantitative increaseof clone 4- 1 mRNAfrom normal PBLin vitro (data not shown).This indicates that clone 4-1 expression is not the consequenceof cell activations, though SLE-lymphocytes are known to beactivated in vivo (62).The prototype clone 4-1 gag region reported by Repaske etal has four stop codons between nt 1,630 and nt 2,650 (5). Ouranalysis using direct sequencing revealed that clone 4-1 DNAfrom several SLEpatients showedchanges at the same nucle-otides when compared with the original sequence (Fig. 1) (58).In all three SLE patients studied, adenine (A) at nt 1,893 waschanged to guanine (G), thymine (T) at nt 2,011 was changedto G, and T at nt 2,374 was also changed to G. As a result ofthese variations, three of the four stop codons in the gag regionof clone 4-1 were inactivated (Fig. 1). Our computer search ofcurrent entries in sequence libraries (GenBank database) re-vealed >90% sequence homology between genomic DNAfromthe SLEclone 4-1 gag region and the consensus sequence ofclone 4-1 located on chromosome ll of normal individuals,including inactivation of these stop codons, unlike clone 4-1located on the other chromosomes(Fig. 1). Wecannot com-pletely rule out the possibility that the virus detected by ourPCRprimers was not actually clone 4- 1 , because there are manymembers of the HERV-Efamily that are genetically similar tothis clone (6, 8). However, more precise information on theintegration sites of clone 4-1 in human chromosomes maybe-comeavailable as a result of the recent completionof the hu-man genomeproject. Despite this limitation, our findings raisethe possibility that the clone 4-1 transcribed in SLE patientsmay be derived from chromosome ll, and that inactivation ofstop codons maycontribute to the translation and productionof gag proteins. Chromosomell is known to contain a breakpoint, which is initiated by several activators including X-rays(56, 57). This is also interesting in view of the potential role ofenvironmental factors in the induction of SLE, because endog-enous retroviruses may be activated by various stimuli such asX-rays, ultraviolet light, chemical agents, bacteria and othermicroorganisms, hormones, and cytokines (3, 63, 64).Certain components derived from endogenous retroviruses,such as pl5E (which is a specific sequence of ^nv-encodedtransmembrane (TM) proteins and is conserved among virusesfrom several species, including murine, feline, and humanretroviruses), can induce the immuneabnormalities observed
in SLE lymphocytes, including the inhibition of IL-2 produc-tion and suppression of the lymphocyte proliferative response(25-27), although the mechanisminvolved is still unclear. TheTMenvelope proteins of clone 4-1 share amino acid sequencehomology with pl5E of the retroviruses from several species(25, 26). Our recent studies have indicated that synthetic clone4-1-derived pl5E peptides can induce CD4+ T cell activationand anergy, production of several cytokines (including IL- 1 6),and cytokine-related PBAin vitro (data not shown). Such CD4+T cell abnormalities may contribute to the loss of self-toler-ance and the induction of SLE-related autoimmune phenom-ena (including autoantibody production) in cooperation withPBA(62) and in addition to the role of molecular mimicry be-tween certain retroviral components and autoantibodies, whichis also reported to be important for autoantibody development(17, 18, 22).
Several reports have shownan important role for activatedCD8+ T cells in the induction of SLE, in addition to CD4+ Tcells. The number of CD4+T cells is generally decreased inSLE patients when compared with that of normal individualsand this phenomenon is inversely correlated with the increaseof activated CD8+ T cells (implied by HLA-DRexpression)and with the rise in the serum level ofIL-16 (55, 65). Also, theremoval of activated CD8+T cells and the loss of factors pro-duced by these cells normalizes CD4+T cell abnormalities suchas decreased in vitro IL-2 production in SLE (66, 67). Thus,activated CD8+T cells and/or the cytokines derived from thesecells seem to influence both the decrease of CD4+T cell num-bers and the impairment of CD4+T cell function in SLE (55).In general, endogenous antigens such as HERVare presentedwith HLAclass I molecules and are recognized by CD8+Tcells (68). Therefore, CD8+ T cells may be activated in SLEthrough the recognition of translated HERVproducts expressedon the cell surface and these activated CD8+T cells may thenproduce various cytokines, including IL- 16. This mechanismmay also be important in HERV-related autoimmunity, in ad-dition to the immune abnormalities promoted by the incuba-tion of cultured lymphocytes with clone 4-1 pl5E peptide, asdescribed above.Virus-infected cells are eliminated by CD8+cytotoxic T lym-phocytes (CTL) and/or natural killer (NK) cells. Recent evi-dence has indicated that the binding of killer cell inhibitoryreceptor (KIR) on CD8+cells with E antigen of HLAclass Imolecules on virus-infected cells can inhibit the cytolytic ac-tivity of CD8+cells against infected cells (69). Cytomegalovi-rus (CMV)infection is reported to occasionally promote theexacerbation of SLE (70), and a glycoprotein homologous withHLAclass I antigens is encoded by CMVand is known to be aligand of KIR (71). This mechanism may be related to the in-hibition of the killing of CMVby CTL and/or NK cells. Ourcomputer search using the GenBankdatabase revealed an ex-tremely high level of sequence homology between the clone 4-1 gag region and the E antigen (-91% homology) (72), whichmay contribute to the escape of clone 4-1 from killing by CTLand/or NKcells and to the production of clone 4-1 viral pro-teins in vivo.
84 Internal Medicine Vol. 40, No. 2 (February 2001)

Retroviruses and Autoimmunity
Conclusion
Retroviruses seemto be one of the most plausible causativeagents for various autoimmune diseases like SLE based onexperimental data from humans and animals, although therehave also been negative reports regarding their role in suchdiseases (73). HTLV-1 can induce several autoimmune mani-festations as does HIV-1 (74), though these findings are notdescribed here. In addition to autoimmune disorders, the po-tential role of HERVas a causative factor of other humandis-eases such as cancer and diabetes has been postulated, althoughthis is still controversial (3, 6). More accurate information onHERVwill soon be revealed by the ongoing human genomeproject. Investigation of the role of clone 4-1 in other autoim-mune diseases besides SLE, such as rheumatoid arthritis (75),as well as studies on the pathogenic influence of other HERVin SLE, should be performed to clarify the etiology of thesediseases and to develop new therapeutic strategies.
Acknowledgements: We wish to thank Dr. T. Naito, Dr. S. Lee, Dr. H.Akimoto (Juntendo University), Dr. N. Maruyama (Tokyo Metropolitan Insti-tute of Gerontology), Prof. N. Yamamoto(Tokyo Medical and Dental Univer-sity), and Dr. Y. Kaneko (Ajinomoto Co., Inc.) for helpful discussion of themanuscript.
References
1) Herrmann M, Hagenhofer M, Kalden JR. Retroviruses and systemic lu-pus erythematosus. Immunol Rev 152: 145-156, 1996.
2) Nakagawa K, Harrison LC. The potential roles of endogenous retrovirusesin autoimmunity. Immunol Rev 152: 193-236, 1996.
3) Urnovitz HB, Murphy WH.Human endogenous retroviruses: nature, oc-currence, and clinical implications in human disease. Clin Microbiol Rev9. 72-99, 1996.
4) Sekigawa I, Kaneko H, Hishikawa T, et al. HIV infection and SLE: theirpathogenic relationship. Clin Exp Rheumatol 16: 175-180, 1998.
5) Repaske R, Steele PE, O'Neill RR, Rabson AB, Martin MA. Nucleotidesequence of a full-length humanendogenous retroviral segment. J Virol54: 764-772, 1985.
6) Lower R. The pathogenic potential of endogenous retroviruses: facts andfantasies. Trends Microbiol 7: 350-356, 1999.
7) Lower R, Lower J, Kurth R. The viruses in all of us: characteristic andbiological significance of humanendogenousretrovirus sequences. ProcNatlAcad Sci USA93: 5177-5184, 1996.
8) Tristem M. Identification and characterization of novel human endog-enous retrovirus families by phylogenetic screening of the human ge-nome mapping project database. J Virol 74: 3715-3730, 2000.
9) Fanning T, Alves G. A family of repetitive DNAsequences in old worldprimates. Gene 199: 279-282, 1997.
10) Leib-Mosch C, Bachmann M, Brack-Werner R, Werner T, Erfle V,Hehlmann R. Expression and biological significance of human endog-enous retroviral sequences. Leukemia 6 Suppl 3: 72s-75s, 1992.
1 1) Kitamura M, MaruyamaN, Shirasawa T, et al. Expression of an endog-enous retroviral gene product in human placenta. Int J Cancer 58: 836-
840,1994.12) Yoshiki T, Mellors RC, Strand M, August JT. The viral envelope glyco-protein of murine leukemia virus and the pathogenesis of immunecom-plex glomerulonephritis of NewZealand mice. J Exp Med 140: 1011-
1027, 1974.
13) Shirai T, Ohta K, Kohno A, et al. Naturally occurring antibody responseto DNAis associated with the response to retroviral gp70 in autoimmune
New Zealand mice. Arthritis Rheum 29: 242-250, 1986.14) Wu J, Zhou T, He J, Mountz JD. Autoimmune disease in mice due tointegration of an endogenous retrovirus in an apoptosis gene. J Exp Med
178: 461-468, 1993.
15) Mellors RC, Mellors JW. Antigen related to mammaliantype-C RNAviral p30 proteins is located in renal glomeruli in human systemic lupuserythematosus. Proc Natl Acad Sci USA 73: 233-237, 1976.
16) Rucheton M, Graafland H, Fanton H, Ursule L, Ferrier P, Larsen CJ. Pres-ence of circulating antibodies against gag-gene MuLVproteins in pa-tients with autoimmune connective tissue disorders. Virology 144: 468-
480,1985.17) Query CC, Keene JD. A human autoimmune protein associated with UlRNAcontains a region of homology that is cross-reactive with retroviralp30 gag antigen. Cell 51: 211-220, 1987.
1 8) Talal N, Garry RF, Schur PH, et al. A conserved idiotype and antibodiesto retroviral proteins in systemic lupus erythematosus. J Clin Invest 85:
1866-1871, 1990.
19) Brookes SM, Pandolfino YA, Mitchell TJ, et al. The immune response toand expression of cross-reactive retroviral gag sequences in autoimmune
disease. Br J Rheumatol 31: 735-742, 1992.20) Blomberg J, Nived O, Pipkorn R, Bengtsson A, Erlinge D, Sturfelt G.Increased antiretroviral antibody reactivity in sera from a defined popula-tion of patients with systemic lupus erythematosus: correlation with au-toantibodies and clinical manifestations. Arthritis Rheum37: 57-66, 1994.
21) Herrmann M, Kalden JR. PCRand reverse dot hybridization for the de-tection of endogenous retroviral transcripts. J Virol Methods 46: 333-
348, 1994.
22) Koshino K, Tokano Y, Hishikawa T, Sekigawa I, Takasaki Y, HashimotoH. Detection of antibodies to HIV- 1 gp41 and HLAclass II antigen-derived peptides in SLE patients. Scand J Rheumatol 24: 288-292, 1995.
23) Hishikawa T, Ogasawara H, Kaneko H, et al. Detection of antibodies to arecombinant gag protein derived from humanendogenous retrovirus likesequence, clone 4-1, in autoimmune diseases. Viral Immunol 10: 137-
147, 1997.
24) Tamura N, Sekigawa I, Hashimoto H, Yamamoto N, Kira S. Syncytialcell formation in vivo by type C retroviral particles in the systemic lupuserythematosus (SLE) lung. Clin Exp Immunol 107: 474-479, 1997.
25) Cianciolo GJ, Copeland TD, Oroszlan S, Synderman R. Inhibition of lym-phocyte proliferation by a synthetic peptide homologous to retroviral en-velope proteins. Science 230: 453-^55, 1985.
26) Ruegg CL, Monell CR, Strand M. Inhibition of lymphoproliferation by asynthetic peptide with sequence identity to gp41 of human immunodefi-ciency virus type 1. J Virol 63: 3257-3260, 1989.
27) Haraguchi S, Good RA, Cianciolo GJ, Engelman RW, Day NK. Immu-nosuppressive retroviral peptides: immunopathological implications forimmunosuppressive influences of retroviral infections. J Leukoc Biol 61 :
654-666, 1997.
28) Kaye BR. Rheumatologic manifestations of infection with human immu-nodeficiency virus (HIV). Ann Intern Med 111: 158-167, 1989.
29) Hishikawa T, Tokano Y, Sekigawa I, et al. HLA-DF T cells and deficientinterleukin-2 production in patients with systemic lupus erythematosus.Clin Immunol Immunopathol 55: 285-296, 1990.
30) Diamond DC, Sleckman BP, Gregory T, Lasky LA, Greenstein JL,Burakoff SJ. Inhibition of CD4+T cell function by the HIV envelopeprotein gpl20. J Immunol 141: 3715-3717, 1988.
31) Rosenstein Y, Burakoff SJ, Herrmann SH. HIV-gpl20 can block CD4-class II MHC-mediated adhesion. J Immunol 144: 526-531, 1990.
32) Breen EC, Rezai AR, Nakajima K, et al. Infection with HIV is associatedwith elevated IL-6 levels and production. J Immunol 15: 480-484, 1990.
33) Oyaizu N, Chirmule N, Ohnishi Y, Kalyanaraman VS, Pahwa S. Humanimmunodeficiency virus type 1 envelope glycoproteins gpl20 and gpl60induce interleukin-6 production in CD4+ T-cell clones. J Virol 65: 6277-6282, 1991.
34) Banda NK, Bernier J, Kurahara DK, et al. Crosslinking CD4 by humanimmunodeficiency virus gpl20 primers T cells for activation-inducedapoptosis. J Exp Med 176: 1099-1106, 1992.
35) Hivroz C, Mazerolles F, Soula M, et al. Humanimmunodeficiency virus
Internal Medicine Vol. 40, No. 2 (February 2001) 85

Sekigawa et al
gpl20 and derived peptides activate protein tyrosine kinase p56lck in hu-man CD4 lymphocytes. Eur J Immunol 23: 600-607, 1993.
36) Macchia D, Almerigogna F, Parronchi P, Ravina A, Maggi E, RomagnaniS. Membranetumor necrosis factor-a is involved in the polyclonal B-cellactivation induced by HIV-infected human T cells. Nature 363: 464-466,
1993.
37) Goldman F, Jensen WA, Johnson GL, Heasley L, Cambier JC. gpl20ligation of CD4 induces p56lck activation and TCRdesensitization inde-pendent of TCR tyrosine phosphorylation. J Immunol 153: 2905-2917,
1994.
38) Ameglio F, Capobianchi MR, Castilletti C, et al. Recombinant gpl20 in-duces IL- 10 in resting peripheral blood mononuclear cells: correlationwith the induction of other cytokines. Clin Exp Immunol 95: 455-458,
1994.
39) Sekigawa I, Koshino K, Hishikawa T, et al. Inhibitory effect of the immu-nosuppressant FK506 on apoptotic cell death induced by HIV-1 gpl20. J
Clin Immunol 15: 312-317, 1995.40) Karsten V, Gordon S, Kirn A, Herbein G. HIV-1 envelope glycoproteingpl20 down-regulates CD4 expression in primary human macrophagesthrough induction of endogenoustumor necrosis factor-a. Immunology
88:55-60,1996.41) Kaneko H, Hishikawa T, Sekigawa I, Hashimoto H, Okumura K, KanekoY. Role of tumor necrosis factor (TNF)-a in the induction of HIV- 1 gpl20-mediated CD4+ T cell anergy. Clin Exp Immunol 109: 41-46, 1997.
42) Romagnani S, Del Prete G, Manetti R, et al. Role ofTH1/TH2 cytokinesin HIV infection. Immunol Rev 140: 73-92, 1994.
43) Barcellini W, Rizzardi GP, Borghi MO, et al. In vitro type-1 and type-2cytokine production in systemic lupus erythematosus: lack of relation-ship with clinical disease activity. Lupus 5: 139-145, 1996.
44) Bisset LR, Rothen M, Joller-Jemelka HI, Dubs RW, Grob PJ, Opravil M.Change in circulating levels of the chemokines macrophage inflamma-tory proteins la and 1 (3, RANTES,monocyte chemotactic protein-1 andinterleukin- 16 following treatment of severely immunodeficient HIV-infected individuals with indinavir. AIDS ll: 485-491, 1997.
45) Kaneko H, Ogasawara H, Naito T, et al. Circulating levels of (3-chemokinesin systemic lupus erythematosus. J Rheumatol 26: 568-573, 1999.
46) Neoh LP, Akimoto H, Kaneko H, et al. The production of (3-chemokinesinduced by HIV-2 envelope glycoprotein. AIDS ll: 1062-1063, 1997.
47) Sekigawa I, Kaneko H, Neoh L-P, et al. Differences of HIV envelopeprotein between HIV- 1 and HIV-2: possible relationship to the lower viru-
lence ofHIV-2. Viral Immunol ll: 1-8, 1998.48) Sekigawa I, Groopman JE, Allan JD, et al. Characterization of autoanti-bodies to the CD4 molecule in human immunodeficiency virus infection.Clin Immunol Immunopathol 58: 145-153, 1991.
49) Lenert G, Lenert P. CD4-reactive antibodies from SLE patients inducedreversible inhibition of polyclonal T lymphocyte proliferation. HumImmunol 49: 113-121, 1996.
50) Sekigawa 1, Lee S, Kaneko H, et al. The possible role ofinterleukin-16 inthe low incidence of HIV infection in patients with systemic lupus erythe-matosus. Lupus 9: 155-156, 2000.
51) Lee S, Kaneko H, Sekigawa I, Tokano Y, Takasaki Y, Hashimoto H. Cir-culating IL-16 in systemic lupus erythematosus. Br J Rheumatol 37: 1334-
1337, 1998.
52) Center DM, Kornfeld H, Cruikshank WW.Interleukin 16 and its functionas a CD4 ligand. Immunol Today 17: 476-481, 1996.
53) Maciaszek JW, Parada NA, Cruikshank WW,Center DM, Kornfeld H,Viglianti GA. IL-16 represses HIV-1 promoter activity. J Immunol 158:
5-8, 1997.
54) Ogasawara H, Takeda-Hirokawa N, Sekigawa I, Hashimoto H, Kaneko Y,Hirose S. Inhibitory effect of interleukin- 1 6 on interleukin-2 productionby CD4+ T cells. Immunology 96: 215-219, 1999.
55) Sekigawa I, Matsushita M, Lee S, et al. A possible pathogenic role ofCD8+ T cells and their derived cytokine, IL-16, in SLE. Autoimmunity2000 (in press).
56) Taruscio D, Manuelidis L. Integration site preferences of endogenousretroviruses. Chromosoma101: 141-156, 1991.
57) Taruscio D, Mantovani A. Eleven chromosomal integration sites of a hu-man endogenous retrovirus (HERV4-1 ) map close to known loci of thir-teen hereditary malformation syndromes. Teratology 54: 108-1 10, 1996.
58) Ogasawara H, Hishikawa T, Sekigawa I, Hashimoto H, Yamamoto N,MaruyamaN. Sequenceanalysis of humanendogenousretrovirus clone4-1 in systemic lupus erythematosus. Autoimmunity 2000 (in press).
59) Karpas A, Lowdell M, Jacobson SK, Hill F. Inhibition of human immu-nodeficiency virus and growth of infected T cells by the immunosuppres-sive drugs cyclosporin A and FK506. Proc Natl Acad Sci USA 89: 8351-
8355, 1992.
60) Groudine M, Eisenman R, Weintraub H. Chromatin structure of endog-enous retroviral genes and activation by an inhibitor of DNAmethyla-
tion. Nature 292: 311-317, 1981.61) Yung RL, Quddus J, Chrisp CE, Johnson KJ, Richardson BC. Mecha-
nisms of drug-induced lupus. I. cloned Th2 cells modified with DNAmethylation inhibitors in vitro cause autoimmunity in vivo. J Immunol
154: 3025-3035, 1995.
62) Horwitz DA, Stohl W, Gray JD. T lymphocyte, natural killer cells,cytokines, and immune regulation, in: Dubois' Lupus Erythematosus. 5thed. Wallance DJ, Harn BH, Eds. Williams & Wilkins, Baltimore, 1997:
155-194.
63) Perron H, Garson JA, Bedin F, et al. Molecular identification of a novelretrovirus repeatedly isolated from patients with multiple sclerosis. Thecollaborative research group on multiple sclerosis. Proc Natl Acad SciUSA 94: 7583-7588, 1997.
64) Rigby SP, Griffiths DJ, Weiss RA, Venables PJ. Human retrovirus-5 provi-ral DNAis rarely detected in salivary gland biopsy tissues from patientswith Sjogren's syndrome. Arthritis Rheum 40: 2016-2021 , 1997.
65) Maeda N, Sekigawa I, Iida N, Matsumoto M, Hashimoto H, Hirose S.Relationship between CD47CD8+T cell ratio and T cell activation insystemic lupus erythematosus. Scand J Rheumatol 28: 166-170, 1999.
66) Linker-Israeli M, Gray JD, Quismorio FP Jr, Horwitz DA. Characteriza-tion of lymphocytes that suppress IL-2 production in systemic lupus erythe-matosus. Clin Exp Immunol 73: 236-241, 1988.
67) Linker-Israeli M, Quismorio FP Jr, Horwitz DA. Further characterizationof interleukin-2 production by lymphocytes of patients with systemic lu-pus erythematosus. J Rheumatol 15: 1216-1222, 1988.
68) Suh WK, Cohen-Doyle MF, Fruh K, Wang K, Peterson PA, Williams DB.Interaction of MHCclass I molecules with the transporter associated withantigen processing. Science 264: 1322-1326, 1994.
69) Mingari MC, Moretta A, Moretta L. Regulation of KIR expression inhuman T cells: a safety mechanism that may impair protective T-cell re-sponses. Immunol Today 19: 153-157, 1998.
70) Hayashi T, Lee S, Ogasawara H, et al. Exacerbation of systemic lupuserythematosus related to cytomegalovirus infection. Lupus 7: 561-564,
1998.
71) Farrell HE, Vally H, Lynch DM, et al. Inhibition of natural killer cells bya cytomegalovirus MHCclass I homologue in vivo. Nature 386: 510-
514,1997.72) Ogasawara H, Kaneko H, Hishikawa T, et al. Molecular mimicry betweenhumanendogenous retrovirus clone 4-1 and HLAclass I antigen: withreference to the pathogenesis of systemic lupus erythematosus. Rheuma-tology 38: 1163-1164, 1999.
73) Fujinami RS, Libbey JE. Endogenous retroviruses: are they the cause ofmultiple sclerosis? Trends Microbiol 7: 263-264, 1999.
74) Iwakura Y, Tosu M, Yoshida E, et al. Induction of inflammatory arthropa-thy resembling rheumatoid arthritis in mice transgenic for HTLV-1. Sci-
ence 253: 1026-1028, 1991.75) Takeuchi K, Katsumata K, Ikeda H, Minami M, Wakisaka A, Yoshiki T.
Expression of endogenous retroviruses, ERV3and A4-1 , in synovial tis-sues from patients with rheumatoid arthritis. Clin Exp Immunol 99: 338-
344,1995.86 Internal Medicine Vol. 40, No. 2 (February 2001)