psychological costs and benefits of predictive testing for huntington's disease
TRANSCRIPT
American Journal of Medical Genetics (Neuropsychiatric Genetics) 54174-184 (1994)
~ ~~
Psychological Costs and Benefits of Predictive Testing for Huntington’s Disease Ann-Marie Codori and Jason Brandt Department of Psychiatry and Behavioral Sciences, The Johns Hopkins University School of Medicine, Baltimore, Maryland
The impact of predictive genetic testing for Huntington’s disease (HD) was assessed in 68 persons at high (n = 17) or low risk (n = 51) for the disease at one to six years following dis- closure of test results. There was consensus in both groups that knowledge of HD genetic status was beneficial. A majority of persons felt relief from wondering and uncertainty. High-risk persons identified greater family closeness and financial security. For low-risk persons, the knowledge that their children were spared offered great consolation. Neg- ative effects in high-risk persons were psy- chological burden (worry, guilt). Even for low-risk subjects, there was a period of ad- justment and, in some, disappointment that low risk had not alleviated problems unre- lated to HD. Although the majority of mar- riages were unaffected by testing, some per- sons in both groups reported that their marriages sustained positive or negative im- pact. Despite mixed consequences, most did not regret being tested. The benefits of testing appear to outweigh its drawbacks, at least among this self-selected group of research participants. We also must conclude, however, that predictive genetic testing will result in negative as well as positive consequences, re- gardless of test outcome. o 1994 Wiley-Liss, Inc.
KEY WORDS Huntington’s disease, predic- tive testing, psycholopcal re- actions
INTRODUCTION In 1983, a genetic marker for Huntington’s disease
(HD) was discovered [Gusella et al., 19831. Since then,
Received for publication October 13, 1993; revision received December 17, 1993.
Address reprint requests to Ann-Marie Codori, Ph.D., De- partment of Psychiatry and Behavioral Sciences, Meyer 218, The Johns Hopkins Hospital, 600 N. Wolfe Street, Baltimore, MD
0 1994 Wiley-Liss, Inc.
21287-7218.
some people a t risk for HD have grappled with a new technological possibility: whether or not to be tested for the marker. HD is a currently incurable progressive disease of the brain that causes a choreiform movement disorder, dementia, and affective disturbances. It is in- herited by autosomal dominant transmission and, thus, occurs in roughly half of the offspring of affected per- sons. The gene is completely penetrant, so that all who inherit it develop the disease, assuming they survive to the time of symptom onset. After symptoms begin (usu- ally around age 401, death occurs within about 15 years [Folstein, 1989; Harper, 1991; Wexler, 19791. It is now known that a mutation on chromosome 4 [HD Collabora- tive Research Group, 19931, an “unstable trinucleotide repeat,” is responsible for virtually all cases of HD. From 1983 until early 1993, however, the locus ofthe HD gene had been isolated only to a 2 million base-pair segment of the tip of the short arm of chromosome-4 [Gusella et al., 19833. Nonetheless, DNA “markers” from this region allowed predictive genetic testing for at-risk persons.
The potential psychological costs and benefits of pre- dictive genetic testing for HD have been debated since the discovery of the first marker, years before any at-risk persons actually received test results. Ethicists, geneti- cists, and mental health professionals could foresee such problems as depression, suicide, family turmoil, divorce, and survivor guilt [Brandt, in press; Farrer, 1987; Kess- ler, 1987a, bl, as well as insurance and employment discrimination among those found to have the marker, On the positive sid.e, some argued that the genetic infor- mation would allow people to plan for the future and avoid passing on the gene for HD, and could decrease anxiety associated with being at risk [Bates, 1981; Craufurd and Harris, 19861. Although surveys showed that some at-risk persons said they might become de- pressed and have suicidal thoughts if they were found to have the marker [Kessler et al., 1987; Meissen and Ber- chek, 19871, the dominant viewpoint among those who actually were tested was that the test would be more beneficial than harmful [Codori et al., 1994; Tibben et al., 1993al.
Wexler [1979,19921 has argued that people who want to know their genetic status in order to plan for the future may be allowing the threat of HD to present a roadblock to a satisfying life. As an alternative to ge-
Impact of HD Testing 175
to benefit in some way from knowing their genetic sta- tus [Simpson et al., 1992; Tibbon et al., 1993al. Younger persons often want the information to help them in mak- ing decisions concerning careers, marriages, and fami- lies. Older persons often want testing so that they can inform their grown children about their own risk for HD. A common theme among all who are tested is that they want to be relieved of the worry and uncertainty that is associated with being at risk. A frequently heard com- ment is “Knowing will be better than not knowing.” Whether or not this prediction is verified by experience is the focus of the present study.
This study was conducted as part of the Presymptoma- tic Testing Program of the Baltimore Huntington’s Dis- ease Project at the Johns Hopkins University. Testing has been available to the offspring of affected persons in the context of a comprehensive research protocol since 1986 [Brandt et al., 19891. We report here on our sub- jects’ assessments of the costs and benefits from one to six years after testing. We have examined 1) perception of risk for HD, both before and after disclosure of test results, 2) confidence in test results, 3) perceived posi- tive and negative effects of testing, 4) unexpected out- comes, 5) effects of the test on family relationships, and 6) post-testing attitudes toward the predictive test.
METHOD Genetic Test
Several markers segregating with the HD gene have been identified and can be used for predictive testing [Allitto et al., 1991; Gusella et al., 1984; MacDonald et al., 1989; Pohl et al., 1988; Whaley et al., 19911. Recombination and other factors (e.g., inaccurately- reported paternity that goes undetected by linkage analysis) preclude complete accuracy in predicting the presence of the gene [Farrer et al., 19881. Risk estimates for the presence of the gene range usually from about 1%-10% in those without the linked-marker (low-risk) and from 90%-99% in those with the linked-marker (high-risk).
Procedures Our testing program includes extensive pre-test coun-
seling and eight in-person follow-up visits over a 3-year period. The protocol is described in detail elsewhere [Brandt et al., 19891. Exclusion criteria for the protocol are symptoms of HD and evidence of current serious psychological disorder (e.g., major depression, schizo- phrenia) or any condition that compromises subjects’ capacity to fully evaluate risks and benefits. Three peo- ple were not tested because of the presence of major depression at the time of the screening evaluation.
Persons who had known their genetic status for a t least a year as of June 30, 1993 were eligible for the present study. Twenty-three high-risk and 65 low-risk persons had received their test results a t least one year before this date. Six high-risk1 and nine low-risk per- sons2 were not included because they had discontinued
‘Three dropped out, 2 completed the program, 1 became af-
Two dropped out, 6 completed, 1 was killed in an auto accident. fected.
netic testing, she recommended that at-risk persons con- sider psychotherapy in order to remove potentially “illu- sory” obstacles that interfere with their lives. She also questioned whether people who ask for the test for the purpose of reducing anxiety may actually feel greater distress upon discovering they are going to get HD. The implication of her arguments is that some people may choose to undergo testing unnecessarily. It could be, she posits, that if they fully explored their motivations for being tested, some at-risk persons would realize that other solutions to their problems are more likely to pro- duce the desired results.
Since HD genetic testing began in research protocols in 1986, several studies have reported on the frequency and severity of depressive symptoms after testing. Meissen and coworkers reported that two of the four persons who had increased risk (86-94% probability of having gene) experienced “severe depression” when re- assessed three months after test-result disclosure. In 1989, Brandt and coauthors [19891 reported mean psy- chological distress scores on 12 persons at high-risk (295% probability of having gene) and 30 at low-risk ( 5 5 % probability of having gene, except one). Two years after testing, there was a slight increase over baseline scores on the Global Severity Index of the Symptom Checklist (SCL-9OR) [Derogatis, 19831 but scores re- mained within normal limits. The Canadian Collabora- tive Study of Predictive Testing reported case studies on four persons who were told they were likely HD gene- carriers [Bloch et al., 19921 as well as five who received low-risk test results [Huggins et al., 19921. Two of the four high-risk persons experienced some depression (measured with Beck Depression Inventory and the SCL-9OR) for several months following disclosure of the results; 10% of the low-risk persons had depressive symptoms for a period of time shortly after disclosure. The same research group presented psychological data on 37 likely gene-carriers collected at 1 week and 1 year after genetic testing [Wiggins et al., 19921. Average scores on the Beck Depression Inventory and the SCL-9OR were no greater than at baseline and tended to decrease over time, leading the authors to conclude that even high-risk test results can have beneficial effects for some persons. In summary, the findings concerning fre- quency of depressive symptoms are somewhat mixed and range from “severe” depression, to mild symptoms, to improvement in psychological state.
More recently, The Dutch program for HD testing published results of two follow-up studies conducted 6-months after test-result disclosure. Tibben and co- workers [1993b] described the characteristics of post- testing stress-responses among high- and low-risk persons and some of the baseline features that predict increased or decreased preoccupation with HD after testing. In the second paper, Tibben and coauthors [1993cl reported that the majority of high-risk persons rated their current life situations as “good” or better. In both papers, the authors’ primary argument is that the detrimental psychological effects of testing have been minimal because of denial and minimization of the im- pact of the test result.
People who choose HD genetic testing clearly expect
176 Codori and Brandt
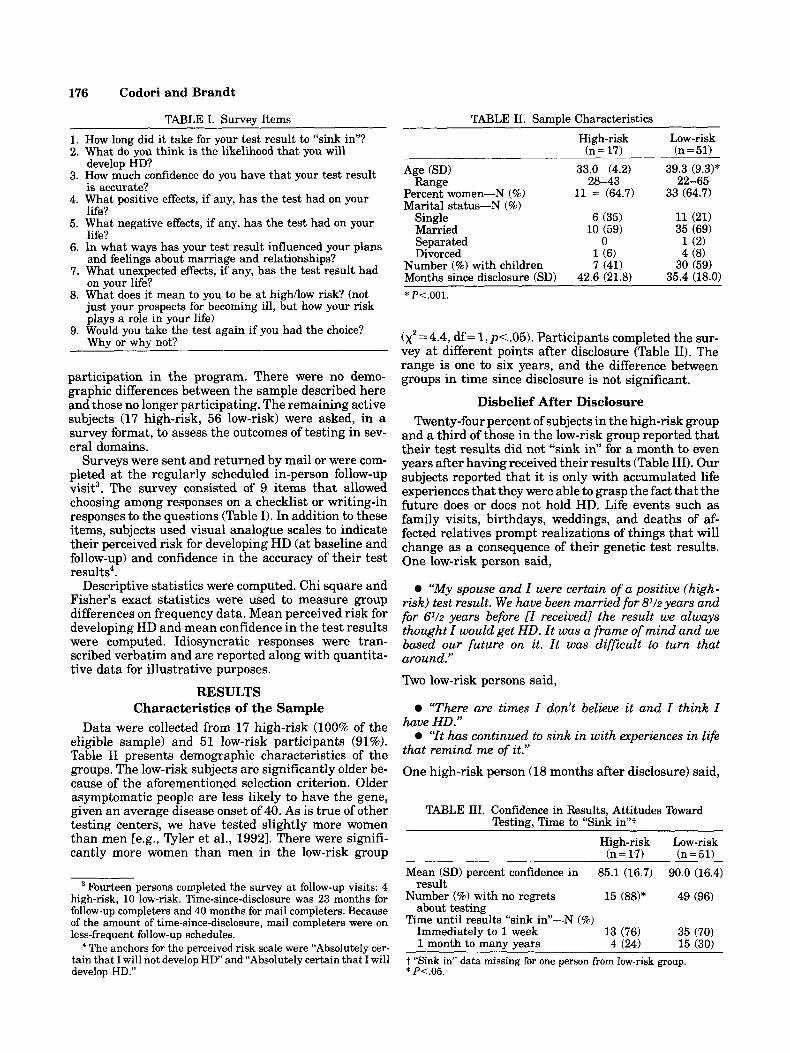
TABLE 11. SamDle Characteristics TABLE I. Survey Items
1. How long did it take for your test result t o “sink in”? 2. What do YOU think is the likelihood that you will
develop HD? 3. How much confidence do you have that your test result
is accurate?
life?
life?
and feelings about marriage and relationships?
on your life?
just your prospects for becoming ill, but how your risk plays a role in your life)
Why or why not?
4. What positive effects, if any, has the test had on your
5. What negative effects, if any, has the test had on your
6. In what ways has your test result influenced your plans
7. What unexpected effects, if any, has the test result had
8. What does it mean to you to be at highllow risk? (not
9. Would you take the test again if you had the choice?
participation in the program. There were no demo- graphic differences between the sample described here and those no longer participating. The remaining active subjects (17 high-risk, 56 low-risk) were asked, in a survey format, to assess the outcomes of testing in sev- eral domains.
Surveys were sent and returned by mail or were com- pleted at the regularly scheduled in-person follow-up visit3. The survey consisted of 9 items that allowed choosing among responses on a checklist or writing-in responses to the questions (Table I). In addition to these items, subjects used visual analogue scales to indicate their perceived risk for developing HD (at baseline and follow-up) and confidence in the accuracy of their test results4.
Descriptive statistics were computed. Chi square and Fisher’s exact statistics were used to measure group differences on frequency data. Mean perceived risk for developing HD and mean confidence in the test results were computed. Idiosyncratic responses were tran- scribed verbatim and are reported along with quantita- tive data for illustrative purposes.
RESULTS Characteristics of the Sample
Data were collected from 17 high-risk (100% of the eligible sample) and 51 low-risk participants (91%). Table I1 presents demographic characteristics of the groups. The low-risk subjects are significantly older be- cause of the aforementioned selection criterion. Older asymptomatic people are less likely to have the gene, given an average disease onset of 40. As is true of other testing centers, we have tested slightly more women than men [e.g., Qler et al., 19921. There were signifi- cantly more women than men in the low-risk group
Fourteen persons completed the survey at follow-up visits: 4 high-risk, 10 low-risk. Time-since-disclosure was 23 months for follow-up completers and 40 months for mail completers. Because of the amount of time-since-disclosure, mail completers were on less-frequent follow-up schedules.
The anchors for the perceived risk scale were “Absolutely cer- tain that I will not develop HD’ and “Absolutely certain that I will develop HD.”
~~ ~~
High-risk Low-risk (n = 51) (n = 17)
-~ ~
Age (SD) Range
Percent women-N (%) Marital status-N (%)
Single Married Separated Divorced
Number (%) with children Months since disclosure 1SD)
33.0 (4.2)
11 = (64.7)
6 (35) 10 (59)
0 1 (6) 7 (41)
42.6 (21.8)
28-43 39.3 (9.3)*
22-65 33 (64.7)
11 (21) 35 (69) 1 (2) 4 (8)
30 (59) 35.4 (18.0)
* P<.OOl.
(x2 = 4.4, df = 1, p<.05). Participants completed the sur- vey at different points after disclosure (Table 11). The range is one to six years, and the difference between groups in time since disclosure is not significant.
Disbelief After Disclosure Twenty-four percent of subjects in the high-risk group
and a third of those in the low-risk group reported that their test results did not “sink in” for a month to even years after having received their results (Table 111). Our subjects reported that it is only with accumulated life experiences that they were able to grasp the fact that the future does or does not hold HD. Life events such as family visits, birthdays, weddings, and deaths of af- fected relatives prompt realizations of things that will change as a consequence of their genetic test results. One low-risk person said,
“My spouse and I were certain of a positive (high- risk) test result. We have been married for P / 2 years and for 6l/2 years before [I received1 the result we always thought I would get HD. I t was a frame of mind and we based our future on it. I t was difficult to turn that around.” Two low-risk persons said,
“There are times Z don’t believe it and I think Z have HD.”
“It has continued to sink in with experiences in life that remind me of it.” One high-risk person (18 months after disclosure) said,
TABLE 111. Confidence in Results, Attitudes Toward Testing, Time to “Sink in”?
High-risk Low-risk (n = 51) (n = 17)
Mean (SD) percent confidence in 85.1 (16.7) 90.0 (16.4) result
Number (%) with no regrets 15 (88)* 49 (96) about testing
Time until results “sink in”-N (%) Immediately to 1 week 13 (76) 35 (70) 1 month to many years 4 124) 15 130)
~
T “Sink in” data missing for one person from low-risk group. * P<.05.
Impact of HD Testing 177
who described thoughts suggestive of denial or excessive hope. In fact, two in this group described at length the processes by which they were coming to accept their future losses.
There were no significant differences in age, sex, or marital status between the eleven high-risk persons who underestimated their risk for HD and the remain- ing six who had risk perceptions of 90% or greater. These subgroups also did not differ on the frequency of positive or negative effects of testing (to be discussed later). However, the difference between their baseline risk per- ceptions approached significance ( p = .07). Mean base- line risk perception among the under-estimators was 38.2%, versus 59.7% in the rest of the high-risk group.
In summary, the majority of high-risk people signifi- cantly underestimated their risk for HD even after they were told their results. It appears that they are less than fully convinced that they are going to get HD.
Confidence in Test Result Accuracy It could be argued that perceptions of risk will be
influenced by confidence in the accuracy of the linkage test results. The accuracy and error rate of the genetic test are discussed at length during the baseline counsel- ing sessions, and subjects understand the various factors that can lead to errors in prediction. Following dis- closure, subjects can either be comforted or distressed by the margin of error in the test. In the case of high-risk test results, subjects may be especially inclined to hope or assume that their results are among the false-positive group-
At follow-up, both groups had high levels of confidence in the accuracy of their test results (85% in high-risk and 90% in low-risk). There was no significant differ- ence between the groups (Table 111). However, the eleven high-risk persons who underestimated their risk for HD were significantly less confident in their test results than the remainder of the high-risk group (79.8% versus 94.8%, respectively) (t = - 2.59, df = 11, p = .025). There was no correlation between confidence and time since disclosure among high risk persons.
In summary, a subset of the high-risk group (those who underestimated their risk for HD) had significantly lower confidence than those who correctly assessed their HD risk. Confidence was unrelated to risk perception in the low-risk group.
Positive Effects of Testing Everyone surveyed believed that being tested pro-
duced some favorable outcomes. As noted in Table IV, a majority in both groups reported that they benefitted by knowing what the future holds and by spending less time worrying about developing HD. Five high-risk peo- ple offered these comments about relief from uncer- tainty.
“Knowingahead[oftime thatI willgetHDlmahs it easier to plan [our] financial future.”
“I understand that there is no cure, but when there is one, I want to be able to receive it. If not in time for me, then in time for my children, i f they have it.”
“I would rather have the answer (i.e., results of ge- netic test), negative or positive . . . than uncertainty.”
8 80
‘‘It’s still hard to believe it (the test result), because 1 show no signs of it (HD).” Thus, after a lifetime of thinking that one’s future might hold HD, some people need time to fully comprehend and accept the greater certainty afforded by genetic testing.
Perceptions of Risk for HD Before and After Disclosure
The costs and benefits of having genetic information may depend on perceptions of the information. Offspring of affected persons are not new to the notion of genetic risk, since most of them grow up aware of the approx- imately 50/50 chance that HD lies ahead. By the time they have genetic testing, at-risk persons have usually given much consideration to whether or not they will develop the disease.
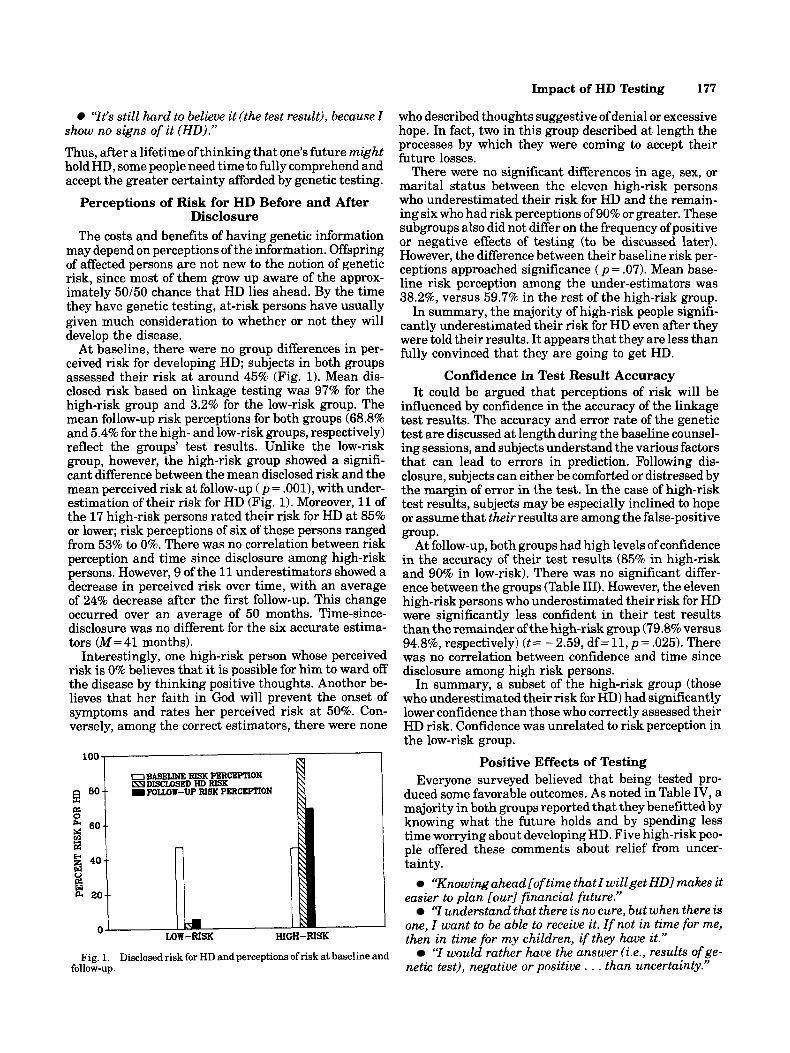
At baseline, there were no group differences in per- ceived risk for developing HD; subjects in both groups assessed their risk at around 45% (Fig. 1). Mean dis- closed risk based on linkage testing was 97% for the high-risk group and 3.2% for the low-risk group. The mean follow-up risk perceptions for both groups (68.8% and 5.4% for the high- and low-risk groups, respectively) reflect the g-roups’ test results. Unlike the low-risk group, however, the high-risk group showed a signifi- cant difference between the mean disclosed risk and the mean perceived risk at follow-up ( p = .001), with under- estimation of their risk for HD (Fig. 1). Moreover, 11 of the 17 high-risk persons rated their risk for HD at 85% or lower; risk perceptions of six of these persons ranged from 53% to 0%. There was no correlation between risk perception and time since disclosure among high-risk persons. However, 9 of the 11 underestimators showed a decrease in perceived risk over time, with an average of 24% decrease after the first follow-up. This change occurred over an average of 50 months. Time-since- disclosure was no different for the six accurate estima- tors (M=41 months).
Interestingly, one high-risk person whose perceived risk is 0% believes that it is possible for him to ward off the disease by thinking positive thoughts. Another be- lieves that her faith in God will prevent the onset of symptoms and rates her perceived risk at 50%. Con- versely, among the correct estimators, there were none
I U BASEN?, REX PERCEPTION EYDISCLOSEDWRISK -- I FOWW-Up RISK PERCEPTION
Fig. 1. Disclosed risk for HD and perceptions of risk at baseline and follow-up.

178 Codori and Brandt
‘ I t (getting genetic test result) put my mind at ease.” ‘7 feel a tremendous sense of relief knowing the re-
sult (of the genetic test).” Low-risk subjects reported the following:
“I can’t live with uncertainty and indecision; taking the test allowed me to maintain control over my life and arrange my future without a sword hanging over my head!”
‘ I t is wonderful to not question and wonder about whether or not I a m showing symptoms of HD or over- reacting to rwrmal responses to life’s stress.”
Equivalent proportions in both groups returned to school as a consequence oftheir DNA tests (Table IV). As one person put it, “Being at low risk now frees me to pursue my dream of going to college to obtain a de- gree . . . where before I didn’t want to spend money on my education. I was preparing for having HD.”
Despite some convergence on the benefits of testing, the groups differed in their assessments of the other positive effects (Table IV). These differences are de- scribed below.
High-risk group. About half of the high-risk per- sons (53%) said that the test had helped them to de- termine what is most important in life (Table IV). They said,
T v e realized that I have to make the best of each day; there is no time to waste . . . I probably take a few more risks-pushing myself at times and just trying to see what I’m truly capable of accomplishing.” * “Knowing that the risk is high gives you a chance to
assess priorities and re-prioritize some of them. Instead of presuming something could be done in the future. . . some things can be [done] sooner. It’s probably like being told you have a terminal illness. I t heightens your aware- ness and teaches you to appreciate things around you.”
Y a m trying to live my life to the fullest and spend as much quality time that I can with my family knowing that I probably will not be able to make up the time at a later date. I a m taking advantage of what I have now.”
Significantly more of the high-risk subjects said they benefitted from testing in that they had made financial preparations for the future, obtained insurance, and were doing more traveling (Table IV). Their comments:
TABLE IV. Positive Effects of Testing: N (%)
High-risk Low-risk (n = 17) (n=51) P
Spend less time worrying about getting HD
Told my children their risk for HD
Returned to school Realize what is
important in life Made financial plans Travel more Obtained more insurance Engage in less symptom
searching
40 (78)
24130 (80)
9 (18) 12 (24)
1(2) 2 (4) 3 (6)
36 (71)
ns
.002
ns .02
.01
.009 ns NA
‘We increased our disability insurance amount a n d . . . IRA funds. [We] also increased death benefits to care for my son’s college education.”
‘We built a new house and made it more easy to get in and out. [We] bought more life insurance.”
“Knowing that my risk forHD is high has prompted me toget on with life and do the thingsl’ve always wanted to d o . . . [like] travel in Europe. . .”
Low-risk group. The majority of low-risk persons (71%) reported that they engaged in less “symptom- searching.” The comments of one subject reflect the sen- timents of all who endorsed this item: “It (being at low risk) means that I can almost guarantee a life without worrying that every dropped dish, every missed step or mental lapse could be a sign of HD.” Significantly more of the low-risk group said that one benefit of testing was being able to tell their children about their own risk for HD (Table IV).
“I spared my kids [ f rom HD] and that means the world to me. They can have children without worrying like I have all my life.”
“There is a little more peace of mind and less worry knowing my children will not suffer from the disease.” The notion of having a future, at all, was new for some low-risk subjects:
‘TI am] making plans for the future that I never would have allowed myself to hope for-let alone plan for. I’ve become much more independent.”
In summary, all subjects believed that they had de- rived something positive from testing which, in the ma- jority, was a diminished preoccupation with developing HD. The groups differed in their assessments of the other benefits of testing. Persons at high risk valued having had the chance to reassess their priorities as well as the chance to make practical preparations for the future. Significantly more high-risk persons were trav- eling “sooner rather than later”-a common pre-testing plan. The low-risk group appreciated the alleviation of symptom-searching and the knowledge that their chil- dren were spared HD.
- put it.
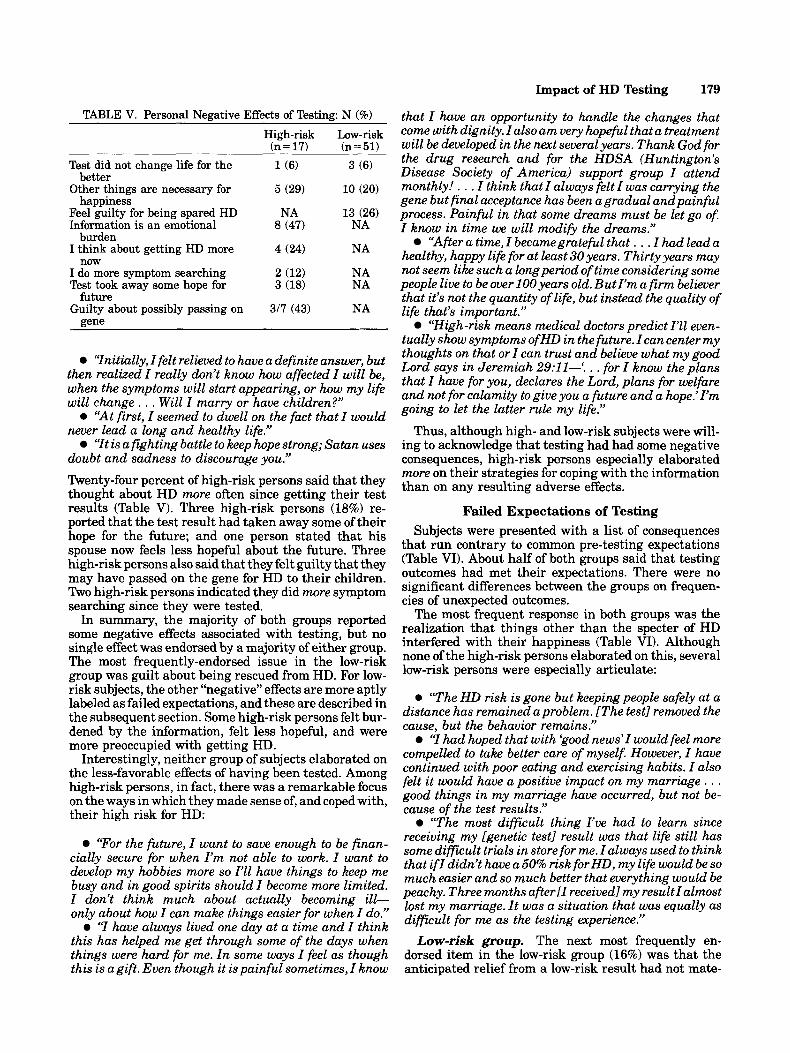
Personal Negative Effects of Testing The majority of both groups acknowledged that they
had experienced one or more negative consequence of predictive testing (Table V). However, 16 of the low-risk group (3 1%) and two from the high-risk group (12%) said that they had experienced nothing negative. The differ- ence in frequencies was not significant.
Twenty-six percent of low-risk persons reported feel- ing guilty for having been “spared” HD. Two persons elaborated on this: “My feelings ofguilt have beengrow- ing stronger since my sister was diagnosed as having HD” and ‘TI havelguilt about my brother[who has HDI.”
Among high-risk persons, the most frequently- endorsed negative effect of testing (47%) was that the test results were an emotional burden (Table V). As they
Impact of HD Testing 179
that I have a n opportunity to handle the changes that come with dignity. I also a m very hopeful that a treatment will be developed in the next several years. Thank God for the drug research and for the HDSA (Huntington’s Disease Society of America) support group I attend monthly! . . . I think that I always felt I was carrying the gene but final acceptance has been agradual and painful process. Painful in that some dreams must be let go of. I know in time we will modify the dreams.”
“After a time, I becamegratefid that . . . I had lead a healthy, happy life for at least 30 years. Thirty years may not seem like such a long period of time considering some people live to be over 100 years old. Butl’m a firm believer that it’s not the quantity of life, but instead the quality of life that’s important.”
“High-risk means medical doctors predict I71 even- tually show symptoms ofHD in the future. I can center my thoughts on that or I can trust and believe what my good Lord says in Jeremiah 29:11-‘. . . for I know the plans that I have for you, declares the Lord, plans for welfare and not for calamity to give you a future and a h0pe.j l’m going to let the latter rule my life.”
Thus, although high- and low-risk subjects were will- ing to acknowledge that testing had had some negative consequences, high-risk persons especially elaborated more on their strategies for coping with the information than on any resulting adverse effects.
Failed Expectations of Testing Subjects were presented with a list of consequences
that run contrary to common pre-testing expectations (Table VI). About half of both groups said that testing outcomes had met their expectations. There were no significant differences between the groups on frequen- cies of unexpected outcomes.
The most frequent response in both groups was the realization that things other than the specter of HD interfered with their happiness (Table VI). Although none of the high-risk persons elaborated on this, several low-risk persons were especially articulate:
TABLE V. Personal Negative Effects of Testing: N (%)
High-risk Low-risk (n = 17) (n = 51)
Test did not change life for the
Other things are necessary for better
happiness Feel guilty for being spared HD Information is an emotional
burden I think about getting HD more
now I do more symptom searching Test took away some hope for
Guilty about possibly passing on future
gene
3 (6)
10 (20)
13 (26) NA
NA
NA NA
NA
‘Initially, I felt relieved to have a definite answer, but then realized I really don’t know how affected I will be, when the symptoms will start appearing, or how my life will change. . . Will I marry or have children?”
0 “At first, I seemed to dwell on the fact that I would never lead a long and healthy life.”
‘It is a fighting battle to keep hope strong; Satan uses doubt and sadness to discourage you.” Twenty- four percent of high-risk persons said that they thought about HD m r e often since getting their test results (Table V). Three high-risk persons (18%) re- ported that the test result had taken away some of their hope for the future; and one person stated that his spouse now feels less hopeful about the future. Three high-risk persons also said that they felt guilty that they may have passed on the gene for HD to their children. Two high-risk persons indicated they did more symptom searching since they were tested.
In summary, the majority of both groups reported some negative effects associated with testing, but no single effect was endorsed by a majority of either group. The most frequently-endorsed issue in the low-risk group was guilt about being rescued from HD. For low- risk subjects, the other “negative” effects are more aptly labeled as failed expectations, and these are described in the subsequent section. Some high-risk persons felt bur- dened by the information, felt less hopeful, and were more preoccupied with getting HD.
Interestingly, neither group of subjects elaborated on the less-favorable effects of having been tested. Among high-risk persons, in fact, there was a remarkable focus on the ways in which they made sense of, and coped with, their high risk for HD:
0 ‘The HD risk is gone but keeping people safely at a distance has remained a problem. [The test] removed the cause, but the behavior remains.”
Y had hoped that with ‘good news’I would feel more compelled to take better care of myself. However, I have continued with poor eating and exercising habits. I also felt it would have a positive impact on my marriage . . . good things in my marriage have occurred, but not be- cause of the test results.”
‘The most difficult thing I’ve had to learn since receiving my [ g e n k c test] reiult was that life still has some di f f iul t trials in store for me. I always used to think ‘‘For the future’ I want to enough to be finan-
Cia2lY secure for when not to work. I want to me
I become more limited. that i f 1 didn’t have a 50% risk forHD, my life would be SO much easier and so much better that everything would be peachy. Three months after[I received] my resultIalmost
hobbies more so l’.h? have things to busy and in good spirits I don’t think much about becoming d?- only about how I can make things easier for when I do.”
<I have alwavs lived one dav at a time and I think lost my marriage. I t was a situation that was equally as dificult for me as the testing aperience.,j
this has helped me get throughsome of the days when things were hard for me. I n some ways I feel as though this is agift. Even though it is painful sometimes, I know
Low-risk group. The next most frequently en- dorsed item in the low-risk group (16%) was that the anticipated relief from a low-risk result had not mate-

180 Codori and Brandt
TABLE VI. UnexDected Effects of Testing: N (%) “I had to readjust my thinking to not being an HD
In my heart I now know that I thought that I would get the opposite test result, and adjusting to the result has been difficult
Although I know my risk for HD, I still feel the uncertainty that prompted me to have the test in the first place
I used to think that I wanted my test result so I could plan for the future, but I now realize that I could have planned for the future without my test result
Although I thought I could cope with knowing my test result, it has been harder than I anticipated
Before I received my test result I thought that I would make many changes in my life, but I have not made any changes
I have not experienced the sense of relief that I always had thought I would from a low- risk result
I am surprised that the prospect of living life without developing HD is distressing to me
unexDected I have experienced nothing
High-risk Low-risk (n = 17) (n = 51)
rialized (Table VI). As one person put it, “There has been no euphoria.” Another said, “Z have not experienced the sense of relief that I always thought I would, as quickly as I expected.”
A small minority (8%) had come to realize that they could have planned for the future without their HD test. Three people still felt the sense of uncertainty that had prompted them to be tested in the first place. Four sub- jects indicated that they had always thought they would have gotten the opposite test result. As one person put it, ‘When Z came in to have the test . . . I was just going to confirm my belieflthat] I had HD. I was notprepared for my result to be low-risk. I t was the most wonderful sur- prise . . . I feel free.”
A few people reported that they had not made the life changes they had talked about making prior to testing. They said,
“I thoughtl wouldpursue college, but that isn’t what Z want.”
“It’s more frustrating now because there are more choices. I a m torn between having children OR a career, or changing careers.”
The transition from 50% risk to low-risk was marked by some emotional and cognitive readjustment:
“Making decisions about my future [is hard1 be- cause I’ve never allowed myself to want a future too much.”
patient.” “Immediately after the results and for some weeks I
felt very detached from the world. . .” High-risk group. As was the case in the low-risk
group, a minority of this group reported that some of their expectations were unfulfilled (Table VI). The high- risk people elaborated less on their checklist responses than did the low-risk group. Three people (18%) said that they had expected to get the opposite test result, and two of them commented: “I didn’t think my results would be positive” and ‘7 was only going to confirm in my own mind, the absence of the genetic marker.” Three high-risk persons also reported that they have contin- ued to feel “uncertainty” since they received their test results. Two said that they now realized they could have planned for the future without their HD test results. Two reported that coping with the information was harder than they had expected, and others didn’t en- dorse this item, but made comments that suggest that coping was an issue:
“The first couple of months were very difficult for me. I didn’t expect this from me.”
Y a m surprised at how long it took me to accept and to realize that Z needed more help dealing with my in- creased risk. Z have been seeing a therapist for about a year and a half now. I wish I would have done so sooner. I kept telling myself that I was fine. This (seeing a thera- pist) would have saved some time and much stress.”
“I wish I could be an ordinary person who wasn’t plagued with these concerns for myself and family. Why did it have to be me?” In summary, a minority of both groups acknowledged that predictive testing had not had the effects they had anticipated. Contrary to their expectations, and produc- ing disappointment, were the realizations by both groups that knowing their risk for HD would not, by itself, lead to happiness and would not provide solutions to all problems. A counter-intuitive finding for a few low-risk persons was that “letting go” of their risk for HD was not as easy as anticipated. A few high-risk persons also were surprised at the difficulty they had in coping with their test results, reinforcing our clinical impressions of the tendency for persons not to expect much distress from high-risk results.
Positive and Negative Effects on Marriage and Family
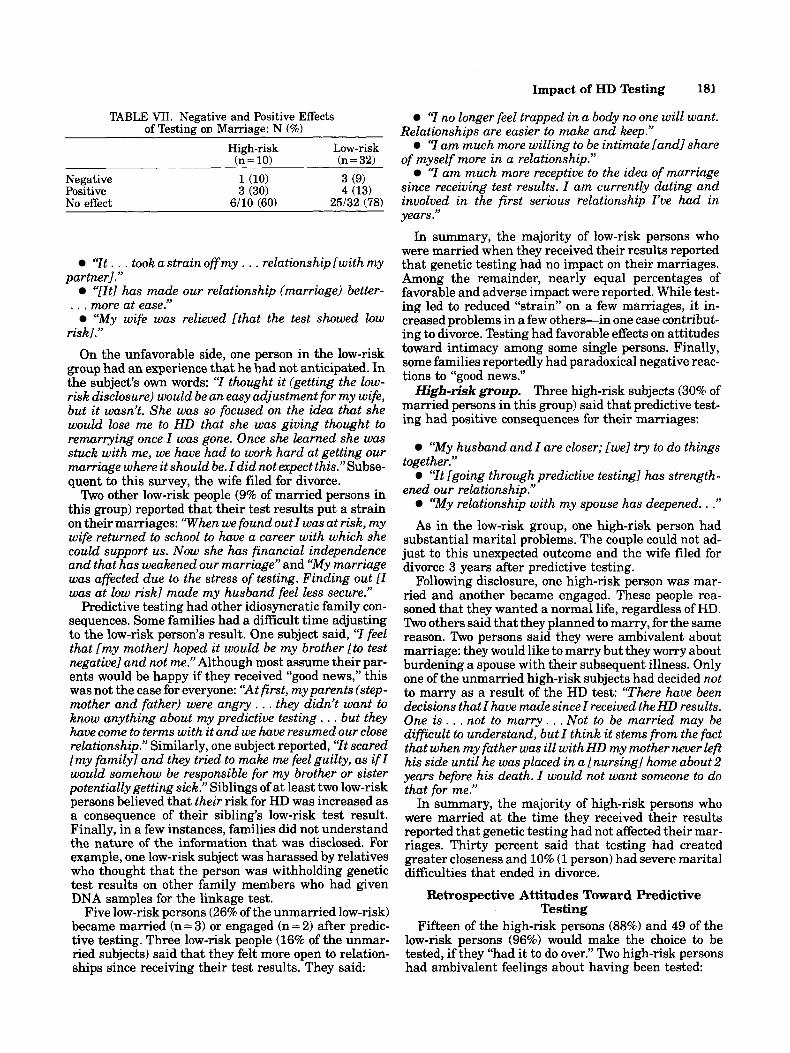
Sixty percent of the high-risk persons (6/10) and 78% of the low-risk people (25132) who were married at the time they received their test results said that predictive testing had no impact on their marital relationships. Among the remainder, there were both positive and negative effects on marriages (Table VII) .
Low-risk group. Four low-risk people (13% of mar- ried persons in this group) reported that predictive test- ing had had positive effects on their marriages:
so much.” “[My] marriage improved because I’m not worrying
Impact of HD Testing 181
“I no longer feel trapped in a body no one will want. Relationships are easier to make and keep.”
“I a m much more willing to be intimate [andl share of myself more in a relationship.”
“I a m much more receptive to the idea of marriage since receiving test results. I a m currently dating and involved in the first serious relationship rue had in years.”
In summary, the majority of low-risk persons who were married when they received their results reported that genetic testing had no impact on their marriages. Among the remainder, nearly equal percentages of favorable and adverse impact were reported. While test- ing led to reduced “strain” on a few marriages, it in- creased problems in a few others-in one case contribut- ing to divorce. Testing had favorable effects on attitudes toward intimacy among some single persons. Finally, some families reportedly had paradoxical negative reac- tions to “good news.’’ High-risk group. Three high-risk subjects (30% of
married persons in this group) said that predictive test- ing had positive consequences for their marriages:
“My husband and I are closer; [we] try to do things
“It [going through predictive testing1 has strength-
“My relationship with my spouse has deepened. . .” As in the low-risk group, one high-risk person had
substantial marital problems. The couple could not ad- just to this unexpected outcome and the wife filed for divorce 3 years after predictive testing.
Following disclosure, one high-risk person was mar- ried and another became engaged. These people rea- soned that they wanted a normal life, regardless of HD. Two others said that they planned to marry, for the same reason. Two persons said they were ambivalent about marriage: they would like to marry but they worry about burdening a spouse with their subsequent illness. Only one of the unmarried high-risk subjects had decided not to marry as a result of the HD test: “There have been decisions that I have made since I received the HD results. One is. . . not to marry. . . Not to be married may be difficult to understand, but I think it stems from the fact that when my father was ill with HD my mother never left his side until he wasplaced in a [nursing1 home about2 years before his death. I would not want someone to do that for me.”
In summary, the majority of high-risk persons who were married at the time they received their results reported that genetic testing had not affected their mar- riages. Thirty percent said that testing had created greater closeness and 10% (1 person) had severe marital difficulties that ended in divorce.
Retrospective Attitudes Toward Predictive Testing
Fifteen of the high-risk persons (88%) and 49 of the low-risk persons (96%) would make the choice to be tested, if they “had it to do over.” Two high-risk persons had ambivalent feelings about having been tested:
together.”
ened our relationship.’’
TABLE VII. Negative and Positive Effects of Testing on Marriage: N (%)
High - r i s k (n = 10)
Low-risk (n = 32)
Negative 1(10) 3 (9) Positive 3 (30) 4 (13) No effect 6/10 (60) 25/32 (78)
“It . . . took a strain off my . . . relationship [with my
‘Tit] has made our relationship (marriage) better- . . . more at ease.”
“My wife was relieved [that the test showed low ri~kl.”
On the unfavorable side, one person in the low-risk group had an experience that he had not anticipated. In the subject’s own words: “I thought it (getting the low- risk disclosure) would be a n easy adjustment for my wife, but it wasn’t. She was so focused on the idea that she would lose me to HD that she was giving thought to remarrying once I was gone. Once she learned she was stuck with me, we have had to work hard at getting our marriage where it should be. I did not expect this.”Subse- quent to this survey, the wife filed for divorce.
Two other low-risk people (9% of married persons in this group) reported that their test results put a strain on their marriages: ‘When we found out I was at risk, my wife returned to school to have a career with which she could support us. Now she has financial independence and that has weakened our marriage” and “My marriage was affected due to the stress of testing. Finding out [I was at low risk] made my husband feel less secure.”
Predictive testing had other idiosyncratic family con- sequences. Some families had a difficult time adjusting to the low-risk person’s result. One subject said, “I feel that [my mother1 hoped it would be my brother [to test negative] and not me.” Although most assume their par- ents would be happy if they received “good news,” this was not the case for everyone: “At first, my parents (step- mother and father) were angry. . . they didn’t want to know anything about my predictive testing . . . but they have come to terms with it and we have resumed our close relationship.” Similarly, one subject reported, “It scared [my family1 and they tried to make me feel guilty, as i f I would somehow be responsible for my brother or sister potentially getting sick.” Siblings of at least two low-risk persons believed that their risk for HD was increased as a consequence of their sibling’s low-risk test result. Finally, in a few instances, families did not understand the nature of the information that was disclosed. For example, one low-risk subject was harassed by relatives who thought that the person was withholding genetic test results on other family members who had given DNA samples for the linkage test.
Five low-risk persons (26% of the unmarried low-risk) became married (n = 3) or engaged (n = 2) after predic- tive testing. Three low-risk people (16% of the unmar- ried subjects) said that they felt more open to relation- ships since receiving their test results. They said:
partner].”

182 Codori and Brandt
“Maybe [I would be tested again]. The test had both positive and negative consequences.’’
‘Yes [I would be tested] i f I were preoccupied with HD; no, i f I were not preoccupied with HD.” Two low-risk persons said they would not choose to be tested, one arguing that the whole testing process was too “emotionally traumatic” because of the lengthy counseling period before disclosure of the test results. The other person reported that testing caused too much conflict among the family members who were asked to give DNA samples. Thus, a minority of high-risk per- sons were ambivalent about being tested because of the consequences ofthe news. A minority of low-risk persons would not be tested because of perceived hardships for themselves or their relatives imposed by the require- ments of the testing protocol.
DISCUSSION A discussion of our findings must be preceded by an
acknowledgment that our data were obtained from a highly selected group. First, our subjects are chosen for the absence of significant psychological disorder. Sec- ond, there is some evidence that those persons who choose genetic testing perceive themselves to be more psychologically adept a t handling “bad news” than those who choose not to be tested [Codori et al., 1994; Tibben et al., 1993al. Consequently, it is important that our findings be generalized only with caution.
Full comprehension of the genetic testing information occurs, for some persons, with repeated realizations that the future does, or does not, hold HD. For them, an assessment of the complete impact of predictive testing will likely evolve over time, as the awareness of gains or losses becomes clearer. They may experience both posi- tive and negative emotions, depending on what aspect of the information is the current focus of attention. For example, we learned from a low-risk person that an early sense of “freedom” can be followed by the realiza- tion that an unlimited future creates its own form of uncertainty and challenges. The psychological effects of the knowledge may vary over time and are not indica- tive of a simple “all good” or “all b a d experience.
The high-risk group was clearly split in their percep- tion of risk for HD and confidence in the accuracy of the test results. The majority of high-risk subjects signifi- cantly underestimated their HD risk and had signifi- cantly lower confidence in their test results than the rest of the group. This combination of findings suggests that some of these persons may believe that their results could be among the small number of expected false posi- tives. Beyond the differences in risk perceptions, the subsets of the high-risk group could not be distinguished on the basis of their reported costs or benefits of testing. Consequently, we cannot conclude that either level of perceptual accuracy is associated with more favorable outcomes. It is tempting to speculate further about rela- tionships between coping strategies and risk perception. For example persons who make plans for the future or try to grow from the experience might have more accu- rate risk perceptions that those who cope by distracting themselves with competing activities [Carver et al., 19891.
Without exception, every subject in the present study reported that there had been psychological benefits as- sociated with predictive testing. Likewise, the majority acknowledged that there had been some associated costs. But for a few common experiences, the costs and benefits of testing were quite individualized. One favor- able outcome that cut across groups was decreased pre- occupation with HD. This is an important finding, given that most persons who request testing are distressed by the uncertainty about whether HD lies ahead and engage in symptom-seeking behaviors, wondering whether any observed or imagined change is “the begin- ning.” Thus, predictive testing can bring some relief from worries about HD.
Other authors have suggested that decreased preoc- cupation with HD reflects denial [Tibben et al., 1993133. Whether our subjects are denying distress is not clear from the present data. However, other evidence suggests that this may not be the case. In a separate study (un- published data), we found that 95% of high-risk persons chose testing because of their preoccupation with HD and because greater certainty about their risk (even high risk) is preferable to uncertainty. Persons at risk for HD are not the only ones shown to have information preferences. There are individual differences in prefer- ences for the amount of disease-related information that people desire when facing potentially life-threatening illnesses. Research involving patients preparing to un- dergo a diagnostic evaluation for cervical cancer showed that levels of stress (as measured by physiological arousal) were lower when the amount of preparatory information was consistent with coping style [Miller and Mangan, 19831. “Information-seekers” were less aroused with more preparatory information; “information- avoiders” were less around with less preparatory infor- mation. Thus, it is premature to conclude that, in all cases, decreased preoccupation with HD after disclosure of results reflects denial. It may be that lessened preoc- cupation with HD is due to relief afforded by greater certainty among a group of persons selected for a strong desire for information.
There were no adverse outcomes that were experi- enced by even close to a majority of either group. But, common to a minority of both groups was the realization that knowing their genetic status would not, in and of itself, make for a happy life. Several people in the low- risk group described troubles that they thought would have been alleviated by freedom from high risk for HD. From losing weight to being able to choose a career, some people expected the genetic test to affect areas of their lives that, we must presume, they thought were prob- lematic because of their HD risk. As Wexler hypothe- sized [1979, 19921, for some people, the risk for HD serves as a ready explanation for decisions that don’t get made or challenges that are not faced.
The disclosure of genetic information uncovered or created family and marital problems in both groups. In all four cases of marital distress after testing, the cou- ples had anticipated receiving the opposite news and had organized their lives around this expectation. Whether it was the tested person or hisher spouse who felt the unsettling effects of information, it appears that

Impact of HD Testing 183
lay in expectations that the genetic information would have had favorable consequences for areas of subjects’ lives that are unrelated to HD. Common expectations were that being relieved of uncertainty and worry about developing a fatal illness would make decisions easier, improve relationships, or simplify difficult tasks. There- fore, as in the Tibben study [1993b], we found that a few people erroneously attributed some of life’s problems to their at-risk status. When these problems are not re- solved with predictive testing, there can be surprise and disappointment.
Attitudes Toward the Predictive Test Most subjects in both groups had no regrets about
being tested and, if they “had it to do over,” would make the same choice. The two low-risk persons who would forego testing attributed their new perspective to the difficulties they associated with the testing process (i.e., lengthy counseling, family reactions to giving DNA samples). Conversely, the two high-risk persons who were ambivalent about their previous decisions to be tested were influenced by the distress they had experi- enced as a result of their increased risk (e.g., in one case, divorce). Thus, although the majority of our sample had no regrets about testing, a minority in both groups had “second thoughts” and their reasons varied according to their test results.
Summary and Conclusions For professionals involved in genetic testing for HD we
offer the following recommendations: 1) At-risk persons should understand that genetic information will almost certainly result in undesirable as well as desirable con- sequences, regardless of test outcome. These conse- quences can be trivial or severe, including the pos- sibility that marriages can be undermined. 2) The primary benefits of testing occur in the realm of HD- related issues, and less often in other areas. 3) Most people will worry less about HD after testing. However, persons found to be at high risk may, in fact, worry more about HD after testing. 4) Persons undergoing testing should be honest with themselves about their expecta- tions for the benefits of testing. They should be helped to develop reasonable goals for testing or be encouraged to consider alternative solutions to problems that will not be resolved by genetic testing. 5 ) Finally, it is our experi- ence that these issues, which sometimes seem abstract and irrelevant before disclosure, can be made more com- pelling if counselors describe the experiences of “real people” who have been through testing already.
Persons at risk for HD will ultimately make their own decisions about testing and live with the consequences of these decisions. Predictive testing programs owe them a full description of the likely costs and benefits as they confront this very important choice.
ACKNOWLEDGMENTS This work was supported in part by National Insti-
tutes of Mental Health grant MH46034 and National Institute of Neurological Disease and Stroke grant NS 16375.
The authors acknowledge the contributions of Drs.
the news disrupted some balance in their relationships. For example, in one case the wife’s greater earning po- tential was acceptable if its purpose was to support the family once the husband became disabled. When no longer necessary, the wife’s financial independence was disconcerting to the at-risk person. As hypothesized by Tibben and coauthors [1993bl and reported by the Cana- dian Collaborative Study [Huggins et al., 19921, we found that test results contrary to expectations may put couples at risk for conflict and divorce.
High-Risk Group On the positive side, there was relief from wondering
and uncertainty. Families reportedly benefitted from improvements in the amount and quality of time spent together and from greater financial security. Moreover, unmarried persons were not deterred from marriage because of their genetic test results. Adverse effects came primarily in the form of psychological burden (e.g., worry, guilt), as found in the Tibben study [1993bl. This finding clearly indicates that at-risk persons should be cautioned that testing can create, rather than alleviate, problems.
Perhaps most striking about the high-risk group was what they didn’t say about the psychological cost of predictive testing. Although subjects readily endorsed a variety of negative effects, the form of their responses was confined primarily to marks on the checklist. This style contrasts with their more-lengthy elaborations on the benefits of testing and on their strategies for coping with their increased genetic risk. The explanation for this phenomenon may lie in what one of the high-risk persons said: that there is a choice about where to focus attention. It could be that many of our high-risk subjects chose to focus attention on what they had gained and how they could cope with whatever negative emotions emerged. This selective focusing of attention could be an adaptive response to what can be overwhelming knowl- edge.
Tibben and coauthors [1993a, bl labeled similar ob- servations “denial,” suggesting that denial can lead to psychopathology. Whatever label is assigned, there is evidence that a limited focus on the potentially dire consequences of an unfavorable medical diagnosis can be adaptive. For example, research with myocardial in- farction patients [Havik and Maeland, 1988; Levenson et al., 1984; Levine et al., 19871 indicates that high levels of “denial” (measured in a variety of ways) in the early stages of recovery is associated with more favor- able psychological and physical outcome. Persistent de- nial of illness can be maladaptive when specific health behaviors are required. It could be argued that denial of illness is appropriate in asymptomatic persons at high risk for HD: they are not yet ill, and there are no health- related actions required. Long-term follow-up as persons become symptomatic will be necessary to show the po- tentially detrimental effects of denial.
Low-Risk Group Among low-risk subjects there was relief from the
psychological burdens of HD risk for themselves and their children. Many of the “negative” effects of testing
184 Codori and Brandt
Gary A. Chase, Susan Folstein, Haig Kazazian, De- borah Meyers, and Phillip R. Slavney. Also acknowl- edged are Mrs. Margaret Abbott and Mss. Mary Louise F’ranz, Laura Kasch, Laura Krafft, and Rachel Gross.
This work was presented in part at the 43rd annual meeting of the American Society of Human Genetics, 1993.
REFERENCES Allitto B, MacDonald M, Bucan M, Richards J, Romano D, Whaley W,
et al. (1991): Increased recombination adjacent to the Huntington disease-linked D4S10 marker. Genomics 9:104-112.
Bates M (1981): Ethics of provocative test for Huntington’s disease. N Engl J Med 304:175-176.
Bloch M, Adam S, Wiggins S, Huggins M, Hayden M (1992): Predictive testing for Huntington disease in Canada: The experience of those receiving an increased risk. Am J Med Genet 42:499-507.
Brandt J (in press): Ethical considerations in genetic testing: An empir- ical study of presymptomatic diagnosis of Huntington’s disease. In Fulford KWM (ed): “Medicine and Moral Reasoning.”
Brandt J, Quaid K, Folstein S, Garber P, Maestri N, Abbott M, et al. (1989): Presymptomatic diagnosis of delayed-onset disease with linked DNA markers: The experience of Huntington’s disease. JAMA 261:3108-3114.
Carver C, Scheier M, Weintraub J (1989): Assessing coping strategies: A theoretically based approach. J Pers SOC Psychol 56:267-283.
Codori AM, Hanson R, Brandt J (1994): Self-selection in predictive testing for Huntington’s disease. Am J Med Genet 54:167-173.
Craufurd D, Harris R (1986): Ethics of predictive testing for Hun- tington’s chorea: The need for more information. Br Med J 293: 249-251.
Derogatis L (1983): “SCL-9OR Manual-11.” Towson, MD: Clinical Psychometric Research.
Farrer L, Myers R, Cupples L, Conneally P (1988): Considerations in using linkage analysis as a presymptomatic test for Huntington’s disease. J Med Genet 25577-588.
Farrer L (1987): Suicide and presymptomatic testing in Huntington disease. Am J Med Genet 26319-320.
Folstein SE (1989): “Huntington’s Disease: A Disorder of Families.” Baltimore, MD. The Johns Hopkins University Press.
Gusella J , Tanzi R, Anderson M, Hobbs W, Gibbons K, Raschtchian R, et al. (1984): DNA markers for nervous system diseases. Science
Gusella J, Wexler N, Conneally P, Naylor S, Anderson M, Tanzi R, et al. (1983): A polymorphic DNA marker linked to Huntington’s disease. Nature 306:234-238.
Harper P (ed) (1991): “Huntington’s Disease.” Philadelphia: Saunders. Havik 0, Maeland J (1988): Verbal denial and outcome in myocardial
infarction patients. J Psychosom Res 32145-157. Huggins M, Bloch M, Wiggins S, Adam S, Suchowersky 0, Trew M,
et al. (1992): Predictive testing for Huntington disease in Canada: Adverse effects and unexpected results in those receiving a de- creased risk. Am J Med Genet 42:508-515.
The Huntington’s Disease Collaborative Research Group (1993): A novel gene containing a trinucleotide repeat that is expanded and unstable on Huntington’s disease chromosomes. Cell 72:971-983.
225~1390-1326.
Kessler S (1987a): Psychiatric implications of presymptomatic testing for Huntington’s disease. Am J Orthopsychiatry 57:212-219.
Kessler S (1987b): The dilemma of suicide and Huntington disease. Am J Med Genet 26:315-317.
Kessler S, FieldT, Worth L, Mosbarger H (1987): Attitudes ofpersons at risk for Huntington disease toward predictive testing. Am J Med Genet 26:259-270.
Levenson J, Kay R, Monteferrante J, Herman M (1984): Denial predicts favorable outcome in unstable angina pectoris. Psychosom Med 4625-32.
Levine J, Warrenburg S, Kerns R, Schwartz G, Delaney R, Fontana A, et al. (1987): The role of denial in recovery from coronary heart disease. Psychosom Med 49:109-117.
MacDonald M, Cheng S, Zimmer M, Haines J , Poustka A, Allitto B, et al. (1989): Clustering of multi-allele DNA markers near the Huntington’s disease gene. J Clin Invest 84:1013-1016.
Meissen G, Berchek R (1987): Intended use of predictive testing by those at risk for Huntington disease. Am J Med Genet 26:283-293.
Meissen G, Myers R, Mastromauro C, Koroshetz W, Klinger K, Farrer L, et al. (1988): Predictive testingfor Huntington’s disease with use of a linked DNA marker. N Engl J Med 318:535-542.
Miller S, Mangan C (1983): Interacting effects of information and coping style in adapting to gynecologic stress: Should the doctor tell all? J Pers SOC Psychol 45223-236.
Pohl T, Zimmer M, MacDonald M, Smith B, Bucan M, Poustka A, (1988): Construction of a Not1 linking library and isolation of new markers close to the Huntington’s disease gene. Nucleic Acids Res
Simpson B, Besson J, Alexander D, Allan K, Johnston A (1992): One hundred requests for predictive testing for Huntington’s disease. Clin Genet 41:326-330.
Tibben A, Frets P, vandeKamp J, Niermeijer M, Vegter-vandervlis M, Fbos R, et al. (1993a): Presymptomatic DNA-testing for Huntington disease: Pretest attitudes and expectations of applicants and their partners in the Dutch program. Am J Med Genet (Neuropsychiatric Genet) 48:lO-16.
Tibben A, Duivenvoorden H, Vegter-vandervlis M, Niermeijer M, Frets P, vandeKamp J, et al. (199313): Presymptomatic DNA testing for Huntington disease: Identifying the need for psychological inter- vention. Am J Med Genet (Neuropsychiatric Genet) 48:137-144.
Tibben A, Frets P, vandeKamp J, Niermeijer M, Vegter-vandermis M, Roos R, et al. (199313: On attitudes and appreciation 6 months after predictive DNA testing for Huntington disease in the Dutch pro- gram. Am J Med Genet (Neuropsychiatric Genet) 48:103-111.
Qler A, Ball D, Craufurd D (1992): Presymptomatic testing for Hun- tington’s disease in the United Kingdom. Br Med J 304:1593-1596.
Wexler N (1979): Genetic “Russian Roulette”: The experience of being at risk for Huntington’s disease. In Kessler S (ed): “Genetic Coun- seling: Psychological Dimensions.” New York: Academic Press.
Wexler N (1992): The Tiresias Complex: Huntington’s disease as a paradigm of testing for late-onset disorders. FASEB J 6:2820-2825.
Wiggins S, Whyte P, Huggins M, Adam S, Theilmann J , Bloch M, et al. (1992): The psychological consequences of predictive testing for Huntington’s disease. N Engl J Med 327:1401-1405.
Whaley W, Bates G, Novelleto A, Sedlacek 2, Cheng S, Romano D, et a1 (1991): Mapping of cosmid clones in the Huntington’s disease region of chromosome 4. Somat Cell Mol Genet 17:83-91.
169185-9198.