huntington's disease: an update of therapeutic strategies
TRANSCRIPT

Gene 556 (2015) 91–97
Contents lists available at ScienceDirect
Gene
j ourna l homepage: www.e lsev ie r .com/ locate /gene
Review
Huntington's disease: An update of therapeutic strategies
Ashok Kumar a, Sandeep Kumar Singh b, Vijay Kumar b, Dinesh Kumar c, Sarita Agarwal a,⁎, Manoj Kumar Rana d
a Department of Genetics, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow 226014, Indiab Department of Neurology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow 226014, Indiac Department of Chemistry, Dr. Ram Manohar Lohia Avadh University, Faizabad 224001, Indiad Department of Microbiology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow-226014, India
Abbreviations: HD, Huntington's disease; htt gene, hudeacetylase inhibitors; RNAi, RNA interference; ASO, anttransglutaminase inhibitors.⁎ Corresponding author at: Department of Genetics,
Institute of Medical Sciences, Lucknow 226014, India.E-mail addresses: [email protected] (A. K
(S. Kumar Singh), [email protected] (V. Kumar),(D. Kumar), [email protected] (S. Agarwal), manojku(M.K. Rana).
http://dx.doi.org/10.1016/j.gene.2014.11.0220378-1119/© 2014 Elsevier B.V. All rights reserved.
a b s t r a c t
a r t i c l e i n f oArticle history:Received 9 September 2014Received in revised form 15 October 2014Accepted 11 November 2014Available online 12 November 2014
Keywords:Huntington's disease (HD)htt geneHistone deacetylase inhibitors (HDACi)RNA interference (RNAi)Antisense oligonucleotide (ASO)Transglutaminase inhibitors (Tgasei)
Huntington's disease (HD) is an autosomal dominant triplet repeat genetic disease, which results in progressiveneuronal degeneration in the neostriatum and neocortex, and associated functional impairments in motor, cog-nitive, and psychiatric domains. Although the genetic mutation caused by abnormal CAG expansion within thehtt gene on chromosome 4p16.3 is identified, the mechanism by which this leads to neuronal cell death andthe question of why striatal neurones are targeted both remain unknown. Patients manifest a typical phenotypeof sporadic, rapid, involuntary control of limb movement, stiffness of limbs, impaired cognition and severe psy-chiatric disturbances. There have been a number of therapeutic advances in the treatment of HD, such as fetalneural transplantation, RNA interference (RNAi) and transglutaminase inhibitors (Tgasei). Although there is in-tensive research into HD and recent findings seem promising, effective therapeutic strategies may not be devel-oped until the next few decades.
© 2014 Elsevier B.V. All rights reserved.
1. Introduction
Huntington's disease (HD) was first described by an Americanphysician, George Huntington, in 1872 after he studied several af-fected individuals and also noted observations made by his fatherand grandfather (Neylan, 2003). It is an adult-onset, chronic and pro-gressive neurodegenerative disease and clinically characterized byabnormal choreic involuntary movements and by psychiatric, psy-chological and intellectual disorders, and radiologically character-ized by striatal atrophy of variable degree. Pathologically, inatrophied striatum, the normally predominant small projecting neu-rons are specifically affected. Since these neurons are inhibitory infunction, their long axons terminate in the substantia nigra and useγ-aminobutyric acid (GABA) as a neurotransmitter and these GABAlevels in the substantia nigra of HD are markedly low (Perry et al.,1973). On the other hand, dopaminergic nigral neurons remain in-tact in HD and the dopamine level in the HD striatum is higherthan normal (Spokes, 1980). Therefore, HD is regarded as a relatively
ntingtin gene; HDACi, histoneisense oligonucleotide; Tgasei,
Sanjay Gandhi Post Graduate
umar), [email protected]@[email protected]
dopamine-predominant disease. In agreement with this finding,anti-dopaminergic drugs are clinically effective against choreicmovements.
2. Genetic insight and molecular biology of the disease
HD is a single gene disease with autosomal dominant inheritancepattern and prevalence is about 5 in 100,000 worldwide (Clarke,2005). Penetrance is almost 100% as individuals with the dominant al-lele eventually develop the disease. The average age of onset is 38years, though the timing ranges from 25 to 70 years. However, approx-imately 5% of HD cases have presented before 20 years of age(Turnpenny and Ellard, 2007). Although the disease locus of HD wasmapped to chromosome 4p16.3 by the G8 marker in the early 1980s,the HD gene was not cloned until 1993 (Gelehrter et al., 1998). HD iscaused by the mutation of the gene IT15, which contains 67 exons andencodes a 3144-amino-acid protein called “huntingtin (htt)” (Young,2005). The function of htt is unclear. It is essential for developmentand that absence of htt is lethal in mice (Nasir et al., 1995). HD gene isessential for post-implantation development and that it may play a sig-nificant role in the normal functioning of the basal ganglia. The wild-type htt up-regulates the expression of Brain DerivedNeurotrophic Fac-tor (BDNF) at the transcription level; however, the mechanism bywhich huntingtin regulates gene expression has not been determined(Zuccato et al., 2001).
The normal and intermediate alleles have 10–26 and 27–35 CAG re-peat respectively. Individuals withmore than 39 CAG repeatwill almost
92 A. Kumar et al. / Gene 556 (2015) 91–97
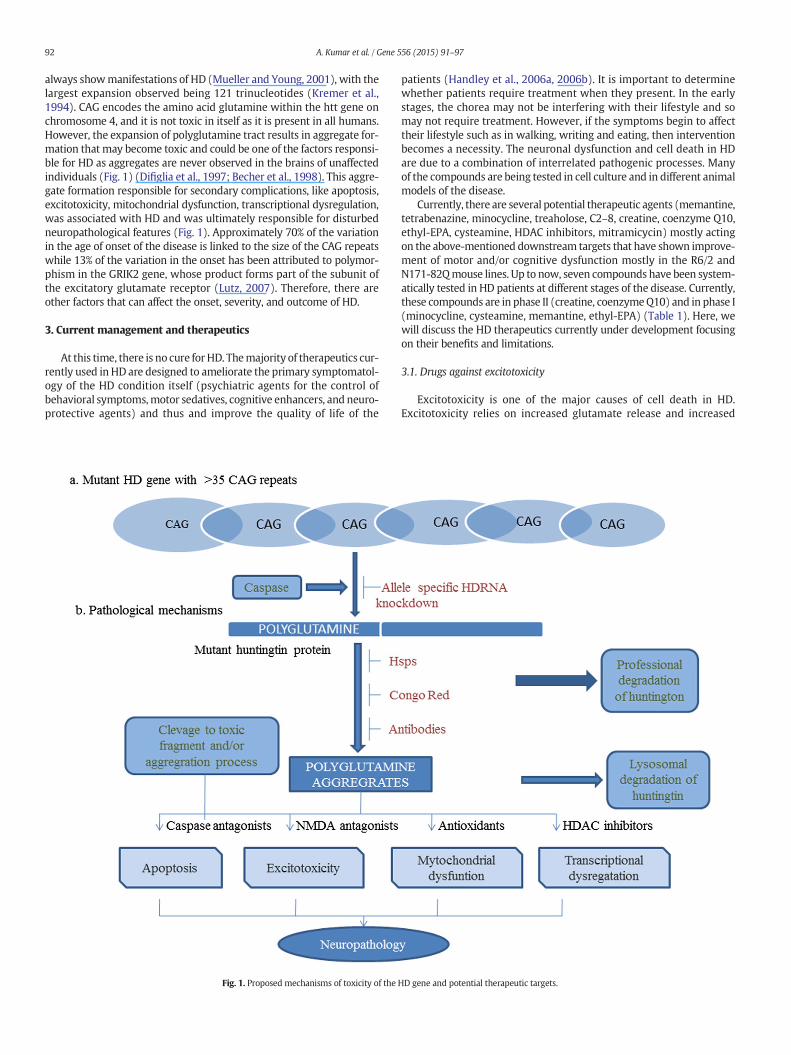
always showmanifestations of HD (Mueller and Young, 2001), with thelargest expansion observed being 121 trinucleotides (Kremer et al.,1994). CAG encodes the amino acid glutamine within the htt gene onchromosome 4, and it is not toxic in itself as it is present in all humans.However, the expansion of polyglutamine tract results in aggregate for-mation that may become toxic and could be one of the factors responsi-ble for HD as aggregates are never observed in the brains of unaffectedindividuals (Fig. 1) (Difiglia et al., 1997; Becher et al., 1998). This aggre-gate formation responsible for secondary complications, like apoptosis,excitotoxicity, mitochondrial dysfunction, transcriptional dysregulation,was associated with HD and was ultimately responsible for disturbedneuropathological features (Fig. 1). Approximately 70% of the variationin the age of onset of the disease is linked to the size of the CAG repeatswhile 13% of the variation in the onset has been attributed to polymor-phism in the GRIK2 gene, whose product forms part of the subunit ofthe excitatory glutamate receptor (Lutz, 2007). Therefore, there areother factors that can affect the onset, severity, and outcome of HD.
3. Current management and therapeutics
At this time, there is no cure forHD. Themajority of therapeutics cur-rently used in HD are designed to ameliorate the primary symptomatol-ogy of the HD condition itself (psychiatric agents for the control ofbehavioral symptoms,motor sedatives, cognitive enhancers, and neuro-protective agents) and thus and improve the quality of life of the
Fig. 1. Proposed mechanisms of toxicity of the
patients (Handley et al., 2006a, 2006b). It is important to determinewhether patients require treatment when they present. In the earlystages, the chorea may not be interfering with their lifestyle and somay not require treatment. However, if the symptoms begin to affecttheir lifestyle such as in walking, writing and eating, then interventionbecomes a necessity. The neuronal dysfunction and cell death in HDare due to a combination of interrelated pathogenic processes. Manyof the compounds are being tested in cell culture and in different animalmodels of the disease.
Currently, there are several potential therapeutic agents (memantine,tetrabenazine, minocycline, treaholose, C2–8, creatine, coenzyme Q10,ethyl-EPA, cysteamine, HDAC inhibitors, mitramicycin) mostly actingon the above-mentioned downstream targets that have shown improve-ment of motor and/or cognitive dysfunction mostly in the R6/2 andN171-82Qmouse lines. Up to now, seven compounds have been system-atically tested in HD patients at different stages of the disease. Currently,these compounds are in phase II (creatine, coenzymeQ10) and in phase I(minocycline, cysteamine, memantine, ethyl-EPA) (Table 1). Here, wewill discuss the HD therapeutics currently under development focusingon their benefits and limitations.
3.1. Drugs against excitotoxicity
Excitotoxicity is one of the major causes of cell death in HD.Excitotoxicity relies on increased glutamate release and increased
HD gene and potential therapeutic targets.
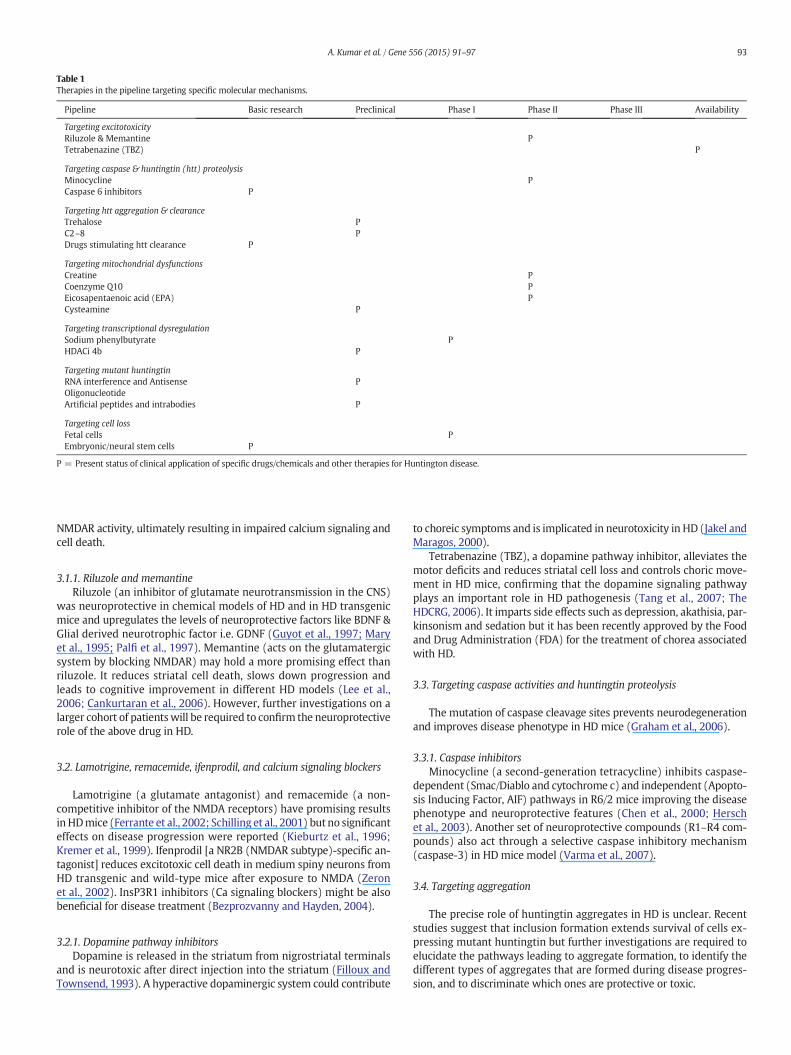
Table 1Therapies in the pipeline targeting specific molecular mechanisms.
Pipeline Basic research Preclinical Phase I Phase II Phase III Availability
Targeting excitotoxicityRiluzole & Memantine PTetrabenazine (TBZ) P
Targeting caspase & huntingtin (htt) proteolysisMinocycline PCaspase 6 inhibitors P
Targeting htt aggregation & clearanceTrehalose PC2–8 PDrugs stimulating htt clearance P
Targeting mitochondrial dysfunctionsCreatine PCoenzyme Q10 PEicosapentaenoic acid (EPA) PCysteamine P
Targeting transcriptional dysregulationSodium phenylbutyrate PHDACi 4b P
Targeting mutant huntingtinRNA interference and Antisense POligonucleotideArtificial peptides and intrabodies P
Targeting cell lossFetal cells PEmbryonic/neural stem cells P
P = Present status of clinical application of specific drugs/chemicals and other therapies for Huntington disease.
93A. Kumar et al. / Gene 556 (2015) 91–97
NMDAR activity, ultimately resulting in impaired calcium signaling andcell death.
3.1.1. Riluzole and memantineRiluzole (an inhibitor of glutamate neurotransmission in the CNS)
was neuroprotective in chemical models of HD and in HD transgenicmice and upregulates the levels of neuroprotective factors like BDNF &Glial derived neurotrophic factor i.e. GDNF (Guyot et al., 1997; Maryet al., 1995; Palfi et al., 1997). Memantine (acts on the glutamatergicsystem by blocking NMDAR) may hold a more promising effect thanriluzole. It reduces striatal cell death, slows down progression andleads to cognitive improvement in different HD models (Lee et al.,2006; Cankurtaran et al., 2006). However, further investigations on alarger cohort of patientswill be required to confirm the neuroprotectiverole of the above drug in HD.
3.2. Lamotrigine, remacemide, ifenprodil, and calcium signaling blockers
Lamotrigine (a glutamate antagonist) and remacemide (a non-competitive inhibitor of the NMDA receptors) have promising resultsin HDmice (Ferrante et al., 2002; Schilling et al., 2001) but no significanteffects on disease progression were reported (Kieburtz et al., 1996;Kremer et al., 1999). Ifenprodil [a NR2B (NMDAR subtype)-specific an-tagonist] reduces excitotoxic cell death in medium spiny neurons fromHD transgenic and wild-type mice after exposure to NMDA (Zeronet al., 2002). InsP3R1 inhibitors (Ca signaling blockers) might be alsobeneficial for disease treatment (Bezprozvanny and Hayden, 2004).
3.2.1. Dopamine pathway inhibitorsDopamine is released in the striatum from nigrostriatal terminals
and is neurotoxic after direct injection into the striatum (Filloux andTownsend, 1993). A hyperactive dopaminergic system could contribute
to choreic symptoms and is implicated in neurotoxicity in HD (Jakel andMaragos, 2000).
Tetrabenazine (TBZ), a dopamine pathway inhibitor, alleviates themotor deficits and reduces striatal cell loss and controls choric move-ment in HD mice, confirming that the dopamine signaling pathwayplays an important role in HD pathogenesis (Tang et al., 2007; TheHDCRG, 2006). It imparts side effects such as depression, akathisia, par-kinsonism and sedation but it has been recently approved by the Foodand Drug Administration (FDA) for the treatment of chorea associatedwith HD.
3.3. Targeting caspase activities and huntingtin proteolysis
The mutation of caspase cleavage sites prevents neurodegenerationand improves disease phenotype in HD mice (Graham et al., 2006).
3.3.1. Caspase inhibitorsMinocycline (a second-generation tetracycline) inhibits caspase-
dependent (Smac/Diablo and cytochrome c) and independent (Apopto-sis Inducing Factor, AIF) pathways in R6/2 mice improving the diseasephenotype and neuroprotective features (Chen et al., 2000; Herschet al., 2003). Another set of neuroprotective compounds (R1–R4 com-pounds) also act through a selective caspase inhibitory mechanism(caspase-3) in HD mice model (Varma et al., 2007).
3.4. Targeting aggregation
The precise role of huntingtin aggregates in HD is unclear. Recentstudies suggest that inclusion formation extends survival of cells ex-pressing mutant huntingtin but further investigations are required toelucidate the pathways leading to aggregate formation, to identify thedifferent types of aggregates that are formed during disease progres-sion, and to discriminate which ones are protective or toxic.

94 A. Kumar et al. / Gene 556 (2015) 91–97
3.4.1. Screens for antiaggregation compoundsCongo red decreases neuronal aggregates and promotes pheno-
typic improvement in a mouse model of HD. It specifically inhibitspolyglutamine oligomerization by disrupting preformed oligomers,prevents ATP depletion and caspase activation, preserves normalcellular protein synthesis & degradation functions and promotesthe clearance of expanded polyglutamine repeats in vivo andin vitro (Sanchez et al., 2003). Similarly, disaccharide trehaloseprevented nuclear inclusion formation, improved motor dysfunctionand prolonged survival in R6/2 mice without any deleterious sideeffects (Tanaka et al., 2004).
Compound C2–8 improved motor performance and reduced bothneuronal atrophy and the size of huntingtin aggregates (Chopra et al.,2007). Epigallocatechin-3-gallate (EGCG), the most abundant polyphe-nol catechin in tea, is a potent inhibitor of mutant huntingtin exon 1protein aggregation (Ehrnhoefer et al., 2006). AGERA (agarose gel elec-trophoresis for resolving aggregates) is also used for resolving aggregatepools.
3.4.2. Drugs stimulating huntingtin clearanceThe mammalian target of rapamycin (mTOR) inhibitor rapamycin
resulted in a significant reduction in mutant htt aggregates, improvedneuronal survival in HDDrosophila andmotor performance and striatalneuropathology in HD mice with few side effects (Ravikumar et al.,2004). However, the combined inhibition of mTOR and inositolmonophosphatase (IMPase) by rapamycin and lithium respectively, re-sulted in additive clearance of mutant htt in vitro (Sarkar et al., 2008).While, trehalose induces autophagy of mutant htt and protect cellsagainst subsequent pro-apoptotic insults via the mitochondrial path-way (both reduce the formation and clearance of htt aggregates)(Sarkar et al., 2007).
3.5. Drugs against mitochondrial dysfunction
Mutant huntingtin binds directly tomitochondria (Choo et al., 2004;Orr et al., 2008), thereby altering their metabolic activity and motilitywithin the cells (Orr et al., 2008). IncreasedmtDNAmutations and dele-tions that can affect mitochondrial respiration have been detected inneurons of the cerebral cortex of HD patients (Cantuti-Castelvetriet al., 2005; Horton et al., 1995). Mutant huntingtin impairs mitochon-drial energy production and cellular respiration, leading to a reductionof the intracellular level of ATP, thus promoting apoptosis, oxidativestress, and susceptibility to excitotoxicity. Consequently, drugs that en-hancemitochondrial function or antioxidantsmay represent a potentialneuroprotective strategy in HD. However, to date, the majority of pre-clinical mouse trials designed to test the effects of different neuropro-tective agents demonstrated limited success, probably because of anunderestimation of the optimal therapeutic dose (Handley et al.,2006a, 2006b).
3.5.1. Creatine and coenzyme Q10Creatine stimulates mitochondrial respiration and has antioxidant
properties. It is neuroprotective in chemical and R6/2 models of HD(Ferrante et al., 2000). It reduced serum levels of 8-hydroxy-2-deoxyguanosine (8-OH-2′-dG), an indicator of oxidative injury in HD(Hersch et al., 2006). CoenzymeQ10 (lipid-soluble benzoquinone) is in-volved in ATP production, stimulation of mitochondrial activity andneuroprotection in R6/2 and N171-82Q mice (Ferrante et al., 2002).The combination of CoQ10 and creatineproduced additive neuroprotec-tive effects on improving motor performance and extending survival inR6/2 HD mice (Lichuan et al., 2009).
3.5.2. Eicosapentaenoic acid (EPA, n−3 fatty acid)EPA causes significant improvements in multiple motor and behav-
ioral abnormalities in different HD animal models (Raamsdonk et al.,2005).
3.5.3. Cystamine and 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine(MPTP) blockers
Cystamine andMPTP blockers inhibit oxidative damage and increasethe prosurvival effects of HD cell (Mao et al., 2006).
3.5.4. Meclizine drugIt silences oxidativemetabolism, suppresses apoptotic cell death and
acts as neuroprotective in a mouse model (Vishal et al., 2011).
3.6. Targeting gene transcription (transcription dysregulation)
Transcriptional dysregulation is an early event in HD pathology andis considered to significantly contribute to the molecular pathogenesisof the disease.
3.6.1. HDAC inhibitorsTranscriptional dysregulation in HD support the notion that treat-
ment with HDAC inhibitors may ameliorate mRNA abnormalities by adirect effect on histone acetylation. Therefore, the administration ofHDAC inhibitors became a good strategy to render the HD chromatinmore relaxed and prone to gene transcription.
SAHA (suberoylanilide hydroxamic acid) crosses the blood–brainbarrier, increases histone acetylation in the brain and reduces themotor impairment in R6/2 mice (Hockly et al., 2003). Similarly,HDACi4b efficiently prevents motor deficits and neurodegenerativeprocesses with a low toxicity profile in vitro (Thomas et al., 2008).Tubacin (selective HDAC6i) leads to rescue of the mutant htt aggrega-tion (Iwata et al., 2005). However, Sirtuins (class III of HDAC enzymes)shows neuroprotection in HD worms (Borra et al., 2005).
3.6.2. Compounds interacting with DNAIn addition to the compounds that directly interact with HDACs,
compounds interacting with DNA could have a potential therapeuticvalue in HD, by influencing transcriptional activity. Mithramycin andchromomycin (anthracycline antibiotics) inhibit neuronal apoptosis,bind DNA andmodulate epigenetic histonemodifications that influencetranscription (Chakrabarti et al., 2000). Furthermore, treatment withanthracycline compounds was able to rebalance epigenetic histonemodification in R6/2 and N171-82Q HD mouse lines, providing the ra-tionale for the design of clinical trials in HD patients (Ryu et al., 2006;Stack et al., 2007).
3.7. Targeting mutant huntingtin
Themutant huntingtin mRNAs are targeted by the use of RNA inter-ference (RNAi), while other strategies aim to block the protein productusing small synthetic peptides or antibodies that recognize mutanthuntingtin.
3.7.1. Targeting mutant huntingtin RNA: antisense oligonucleotide (ASO)and RNAi
Successful delivery of ASO into NT2 cells leads to the down regula-tion of mutant huntingtin and reduction of aggregate formation(Nellemann et al., 2000). The ASO and RNAi perform their knockdown function by nonallele-selective and allele selective manner foran e.g. modified ASO (peptide nucleic acid, PNA) enable the selectiverecognition of the mutant allele and the determination of the selectiveinhibition of mutant protein expression in human fibroblasts (Huet al., 2009), and short hairpin RNA (shRNA) reducesmutant huntingtinmRNA and protein level in the striatumofN171-82Qmice (Harper et al.,2005).
3.7.2. Targeting the mutant protein: artificial peptides and intrabodiesIntrabodies (recombinant antibodies (Abs) or Ab fragments having
high specificity and high affinity to the target site) recognize theproline-rich domain of htt, improve body weight, and ameliorate

95A. Kumar et al. / Gene 556 (2015) 91–97
motor, cognitive, and neuropathological symptoms in multiple mousemodels of HD (R6/2, N171-82Q, YAC128, and BACHD) (Southwellet al., 2009).
3.8. Other therapeutics
3.8.1. Fetal neural transplantationAs the striatum commonly degenerates in HD resulting in the loss of
motor and cognitive functions, efforts have been made to restore thesefunctions by transplanting fetal striatal neuroblasts into the striata ofHD patients. However, this therapy has not been very successful in thelong term. In a study by Bachoud-Lévi and colleagues in which five pa-tients were graftedwith human fetal neuroblasts, there was an increasein metabolic activity in various subnuclei of the striatum in three of thefive patients, although there was a progressive deterioration in the twoother patients 2 years after surgery (Bachoud-Lévi et al., 2000). Howev-er, 4 to 6 years after surgery, clinical improvement initially observed inthe three patients began to decline and dystonia deteriorated consis-tently, while the two patients who did not benefit from the transplanta-tion continued to deteriorate in a comparable way to non-grafted HDpatients. Therefore, although neuronal transplantationmay provide im-provement and stability initially, it is not a permanent cure for HD(Bachoud-Lévi et al., 2006).
3.8.2. Transglutaminase inhibitor (Tgasei)Transglutaminases (as cysteamine, Q10) are a family of enzymes
that catalyze the formation of a covalent bond between a free aminogroup and the gamma-carboxamid group of protein- or peptide-bound glutamine. They form extensively cross-linked, generally insolu-ble protein polymers and have been implicated in a number of medicalconditions such as celiac disease, Parkinson disease (PD) and HD(Griffin et al., 2002; Verme et al., 2004; Karpuj et al., 2002a, 2002b).Karpuj and colleagues demonstrated that inhibition of transglutaminase(TGase) could provide a new treatment approach to HD (Karpuj et al.,2002a, 2002b). Crosslinking is the formation of bonds to link one poly-mer chain to another. It is thought that this promotes the formation ofthe protein aggregates that cause HD.
3.8.3. UbiquilinAs expanded polyglutamine (PolyQ) tracts have been implicated
in protein aggregation and cytotoxicity in HD, ubiquilin has been dis-covered to reduce protein aggregation and toxicity induced by PolyQin cells and animal models of HD. Ubiquilin is an ubiquitin-like (UBL)protein and has an N terminal UBL domain and a C-terminalubiquitin-associated (UBA) domain. Ubiquitin is a highly conserved76 amino acid protein (Glitz, 2011) and ubiquilin-1 is one of thefour members of the ubiquilin protein family. Wang and associatesstate that overexpression of ubiquilin decreases the aggregationand toxicity of green fluorescent protein (GFP)–huntingtin fusionprotein containing 74 polyQ repeats, while a decrease in the levelof ubiquilin resulted in increased aggregation and cytotoxicity(Wang et al., 2006).
3.8.4. Embroynic stem (ES) cells and germ (EG) cellsES cells are isolated and expanded from the inner cell mass of the
blastocyst stage embryo. In the case of human ES cells, most current-ly available lines have been generated from surplus embryos follow-ing in vitro fertilization. As might be expected, these very primitivecells have the capacity to produce every cell type of the body andare capable of substantial expansion in culture, while remaining rel-atively stable in terms of the cell population characteristics and alsohaving a substantial neurogenic potential (Reubinoff et al., 2000;Zhang et al., 2001). Human ES cells can be directed neurally using avariety of methods, including exposure to retinoic acid, placementof cells in serum-free mediumwith the mitogen FGF-2, and selectionusing cell-sorting methods. Studies on mouse ES cells have shown
that specific neural progenitor subtypes can be derived by manipu-lating culture conditions to expose cells to a program of extrinsic sig-nals that recapitulate the developmental events of neural patterning(Kim et al., 2002; Wichterle et al., 2002).
EG cells, like ES cells, spontaneously form embryoid bodies (EBs),spherical structures in which cells begin to differentiate and whichcan form cell types from all three lineages of embryonic develop-ment. When dissociated, EB-derived cells can be vigorously and reli-ably expanded and efficiently cloned. The resulting cell linespredominantly express markers of the neural lineage, althoughmarkers of other lineages are also found. Their gene expression pro-files appear to be relatively stable over multiple passages, althoughheterogeneous between individual lines (Shamblott et al., 1998).So far, EB-derived cells have been insufficiently characterized toproperly assess their potential usefulness for neural transplantation.Although they appear to contain neural progenitors capable of ro-bust, long-term expansion, it is not clear whether these are similarto the neural progenitors that can be derived from ES cells andwhose subsequent differentiation can be controlled.
4. Conclusion and future directions
The genetics and some therapeutic advances in the management ofHD have been discussed. Most of these therapies focus on the develop-ment of neuroprotective strategies, with the aim of delaying the onsetand slowing the progression of HD. As the onset of neurodegenerativeprocesses begin long before the clinical manifestations of HD, it is alsoimportant to develop laboratory methods of monitoring disease pro-gression before the onset of clinical symptoms. Most of the advancesdiscussed are still ongoing; therefore, it is hoped that the final outcomewould becomemore apparent in the very near future. Up to now, sevencompounds have been systematically tested in HD patients at differentstages of the disease. Currently, these compounds are in phase II(creatine, coenzyme Q10) and in phase I (minocycline, cysteamine,memantine, ethyl-EPA). Only one is now available in several countries(tetrabenazine). Unfortunately, only a few drugs, all belonging to old-generation drugs, have been tested in HD patients with some benefits.One possible explanation can be found in the discrepancies existing be-tween mouse and human trials. These discrepancies highlight the diffi-culty in predicting the efficacy of new drugs in humans based on animalmodels of HD. All of the existing transgenic HDmousemodels share fea-tures with the human pathology, but not unexpectedly, none of themindividually seems to recapitulate the entire spectrum of phenotypesof human HD. Although there is intensive research into Huntington'sdisease and recent findings seem promising, effective therapeutic strat-egies may not be developed until the next few decades. This is becausemany of the laboratory breakthroughs prove to be unsuccessful inhumans for a variety of unknown reasons. It is difficult, at this stage,to suggest that one potential treatment is better than the other asmost of them have not been tried in humans so as to evaluate their ef-fect, hence the reason why all therapeutic options should be exploredby researchers.
Conflicts of interest
The authors have no financial conflicts of interest.
Acknowledgments
The authors are thankful to Sanjay Gandhi Post Graduate institute ofMedical Sciences (SGPGIMS), Lucknow for providing infrastructure fa-cility. Ashok Kumar is thankful to DBT-New Delhi (DBT-JRF 2009-10/515) for his fellowship.
96 A. Kumar et al. / Gene 556 (2015) 91–97
References
Bachoud-Lévi, A.C., Rémy, P., Nguyen, J.P., et al., 2000. Motor and cognitive improvementsin patients with Huntington's disease after neural, transplantation. Lancet 356(9246), 1975–1979.
Bachoud-Lévi, A.C., Gaura, V., Brugières, P., et al., 2006. Effect of fetal neural transplants inpatients with Huntington's disease 6 years after surgery: a long-term follow-upstudy. Lancet Neurol. 5 (4), 303–309.
Becher, M.W., Kotzuk, J.A., Sharp, A.H., et al., 1998. Intranuclear neuronal inclusions inHuntington's disease and dentatorubral and pallidoluysian atrophy: correlation be-tween the density of inclusions and IT15 CAG triplet repeat length. Neurobiol. Dis.4 (6), 387–397.
Bezprozvanny, I., Hayden,M.R., 2004. Deranged neuronal calcium signalling and Hunting-ton disease. Biochem. Biophys. Res. Commun. 322, 1310–1317.
Borra, M.T., Smith, B.C., Denu, J.M., 2005. Mechanism of human SIRT1 activation by resver-atrol. J. Biol. Chem. 280, 17187–17195.
Cankurtaran, E.S., Ozalp, E., Soygur, H., et al., 2006. Clinical experience with risperidoneand memantine in the treatment of Huntington's disease. J. Natl. Med. Assoc. 98,1353–1355.
Cantuti-Castelvetri, I., Lin, M.T., Zheng, K., Keller-McGandy, C.E., Betensky, R.A., Johns, D.R.,2005. Somatic mitochondrial DNA mutations in single neurons and glia. Neurobiol.Aging 26, 1343–1355.
Chakrabarti, S., Bhattacharyya, D., Dasgupta, D., 2000. Structural basis of DNA recognitionby anticancer antibiotics, chromomycin A(3), mithramycin: roles of minor groovewidth and ligand flexibility. Biopolymers 56, 85–95.
Chen, M., Ona, V.O., Li, M., et al., 2000. Minocycline inhibits caspase-1 and caspase-3 ex-pression and delays mortality in a transgenic mouse model of Huntington disease.Nat. Med. 6, 797–801.
Choo, Y.S., Johnson, G.V., MacDonald, M., Detloff, P.J., Lesort, M., 2004. Mutant huntingtindirectly increases susceptibility of mitochondria to the calcium-induced permeabilitytransition and cytochrome c release. Hum. Mol. Genet. 13, 1407–1420.
Chopra, V., Fox, J.H., Lieberman, G., et al., 2007. A small-molecule therapeutic lead forHuntington's disease: preclinical pharmacology and efficacy of C2–8 in the R6/2transgenic mouse. Proc. Natl. Acad. Sci. U. S. A. 104, 16685–16689.
Clarke, C.R.A., 2005. Neurological disease, In: Kumar, P., Clark, M. (Eds.), Kumar and ClarkClinical Medicine, 6th ed. W.B. Saunders, Edinburgh and New York, pp. 1173–1271.
DiFiglia, M., Sapp, E., Chase, K.O., et al., 1997. Aggregation of huntingtin in neuronalintranuclear inclusions and dystrophic neuritis in brain. Science 277, 1990–1993.
Ehrnhoefer, D.E., Duennwald, M., Markovic, P., et al., 2006. Green tea (−)-epigallocate-chin-gallate modulates early events in huntingtin misfolding and reduces toxicityin Huntington's disease models. Hum. Mol. Genet. 15, 2743–2751.
Ferrante, R.J., Andreassen, O.A., Jenkins, B.G., et al., 2000. Neuroprotective effects of crea-tine in a transgenic mouse model of Huntington's disease. J. Neurosci. 20, 4389–4397.
Ferrante, R.J., Andreassen, O.A., Dedeoglu, A., et al., 2002. Therapeutic effects of coenzymeQ10 and remacemide in transgenic mouse models of Huntington's disease. J.Neurosci. 22, 1592–1599.
Filloux, F., Townsend, J.J., 1993. Pre- and postsynaptic neurotoxic effects of dopaminedemonstrated by intrastriatal injection. Exp. Neurol. 119, 79–88.
Gelehrter, T.D., Collins, F.S., Ginsburg, D., 1998. Principles of Medical Genetics, 2nd ed.Williams & Wilkins, Baltimore.
Glitz, D., 2011. Protein synthesis: translation and posttranslational modifications, In:Devlin, T.M. (Ed.), Textbook of Biochemistry: With Clinical Correlations, 7th ed.John Wiley & Sons, Inc., Hoboken NJ, pp. 209–254.
Graham, R.K., Deng, Y., Slow, E.J., et al., 2006. Cleavage at the caspase-6 site is required forneuronal dysfunction and degeneration due to mutant huntingtin. Cell 125,1179–1191.
Griffin, M., Casadio, R., Bergamini, C.M., 2002. Transglutaminases: nature's biologicalglues. Biochem. J. 368 (2), 377–396.
Guyot, M.C., Palfi, S., Stutzmann, J.M., et al., 1997. Riluzole protects from motor deficitsand striatal degeneration produced by systemic 3-nitropropionic acid intoxicationin rats. Neuroscience 81, 141–149.
Handley, O.J., Naji, J.J., Dunnett, S.B., et al., 2006a. Pharmaceutical, cellular and genetictherapies for Huntington's disease. Clin. Sci. 110, 73–88.
Handley, O.J., Naji, J.J., Dunnett, S.B., Rosser, A.E., 2006b. Pharmaceutical, cellular and ge-netic therapies for Huntington's disease. Clin. Sci. 110, 73–88.
Harper, S.Q., Staber, P.D., He, X., et al., 2005. RNA interference improves motor and neuro-pathological abnormalities in a Huntington's disease mouse model. Proc. Natl. Acad.Sci. U. S. A. 102, 5820–5825.
Hersch, S., Fink, K., Vonsattel, J.P., et al., 2003. Minocycline is protective in a mouse modelof Huntington's disease. Ann. Neurol. 54, 841–843.
Hersch, S.M., Gevorkian, S., Marder, K., et al., 2006. Creatine in Huntington disease is safe,tolerable, and bioavailable in brain and reduces serum 8OH2'dG. Neurology 66,250–252.
Hockly, E., Richon, V.M., Woodman, B., et al., 2003. Suberoylanilide hydroxamic acid, a his-tone deacetylase inhibitor, ameliorates motor deficits in a mouse model ofHuntington's disease. Proc. Natl. Acad. Sci. U. S. A. 100, 2041–2046.
Horton, T.M., Graham, B.H., Corral-Debrinski, M., Shoffner, J.M., Kaufman, A.E., Beal, M.F.,1995. Marked increase in mitochondrial DNA deletion levels in the cerebral cortexof Huntington's disease patients. Neurology 45, 1879–1883.
Hu, J., Matsui, M., Corey, D.R., 2009. Allele-selective inhibition of mutant huntingtin bypeptide nucleic acid–peptide conjugates, locked nucleic acid, and small interferingRNA. Ann. N. Y. Acad. Sci. 1175, 24–31.
Iwata, A., Riley, B.E., Johnston, J.A., et al., 2005. HDAC6 and microtubules are required forautophagic degradation of aggregated huntingtin. J. Biol. Chem. 280, 40282–40292.
Jakel, R.J., Maragos, W.F., 2000. Neuronal cell death in Huntington's disease: a potentialrole for dopamine. Trends Neurosci. 23, 239–245.
Karpuj, M.V., Becher, M.W., Springer, J.E., et al., 2002a. Prolonged survival and decreasedabnormal movements in transgenic model of Huntington disease, with administra-tion of the transglutaminase inhibitor cystamine. Nat. Med. 8, 143–149.
Karpuj, M.V., Becher, M.W., Steinman, L., 2002b. Evidence for a role for transglutaminasein Huntington's disease and the potential therapeutic implications. Neurochem. Int.40 (1), 31–36.
Kieburtz, K., Feigin, A., McDermott, M., et al., 1996. A controlled trial of remacemide hy-drochloride in Huntington's disease. Mov. Disord. 11, 273–277.
Kim, J.H., Auerbach, J.M., Rodriguez-Gomez, J.A., et al., 2002. Dopamine neurons derivedfrom embryonic stem cells function in an animal model of Parkinson's disease. Nature418, 50–56.
Kremer, B., Goldberg, P., Andrew, S.E., et al., 1994. A worldwide study of the Huntington'sdisease mutation. The sensitivity and specificity of measuring CAG repeats. N. Engl. J.Med. 330, 1401–1406.
Kremer, B., Clark, C.M., Almqvist, E.W., et al., 1999. Influence of lamotrigine on pro-gression of early Huntington disease: a randomized clinical trial. Neurology 53,1000–1011.
Lee, S.T., Chu, K., Park, J.E., et al., 2006. Memantine reduces striatal cell deathwith decreas-ing calpain level in 3-nitropropionic model of Huntington's disease. Brain Res. 1118,199–207.
Lutz, R.E., 2007. Trinucleotide repeat disorders. Semin. Pediatr. Neurol. 14 (1), 26–33.Mao, Z., Choo, Y.S., Lesort, M., 2006. Cystamine and cysteamine prevent 3-NP-inducedmi-
tochondrial depolarization of Huntington's disease knock-in striatal cells. Eur. J.Neurosci. 23, 1701–1710.
Mary, V., Wahl, F., Stutzmann, J.M., 1995. Effect of riluzole on quinolinate induced neuro-nal damage in rats: comparison with blockers of glutamatergic neurotransmission.Neurosci. Lett. 201, 92–96.
Mueller, R.F., Young, I.D., 2001. Emery's Elements of Medical Genetics, 11th ed. ChurchillLivingstone, Edinburgh.
Nasir, J., Floresco, S.B., O'Kusky, J.R., et al., 1995. Targeted disruption of the Huntington'sdisease gene results in embryonic lethality and behavioural and morphologicalchanges in heterozygotes. Cell 81 (5), 811–823.
Nellemann, C., Abell, K., Norremolle, A., et al., 2000. Inhibition of Huntington synthesis byantisense oligodeoxynucleotides. Mol. Cell. Neurosci. 16, 313–323.
Neylan, T.C., 2003. Neurodegenerative disorders: George Huntington's description of he-reditary chorea. J. Neuropsychiatry Clin. Neurosci. 15 (1), 108.
Orr, A.L., Li, S., Wang, C.E., Li, H., Wang, J., Rong, J., 2008. NH2-terminal mutant huntingtinassociates with mitochondria and impairs mitochondrial trafficking. J. Neurosci. 28,2783–2792.
Palfi, S., Riche, D., Brouillet, E., et al., 1997. Hantraye P. Riluzole reduces incidence of ab-normal movements but not striatal cell death in a primate model of progressivestriatal degeneration. Exp. Neurol. 146, 135–141.
Perry, T.L., Hansen, S., Kloster, M., 1973. Huntington's chorea. Deficiency of gamma-aminobutyric acid in brain. N. Engl. J. Med. 288, 337–342.
Raamsdonk, V.J.M., Pearson, J., Rogers, D.A., et al., 2005. Ethyl-EPA treatment improvesmotor dysfunction, but not neurodegeneration in the YAC128 mouse model of Hun-tington disease. Exp. Neurol. 196, 266–272.
Ravikumar, B., Vacher, C., Berger, Z., et al., 2004. Inhibition of mTOR induces autophagyand reduces toxicity of polyglutamine expansions in fly and mouse models of Hun-tington disease. Nat. Genet. 36, 585–595.
Reubinoff, B.E., Pera, M.F., Fong, C.Y., et al., 2000. Embryonic stem cell lines from humanblastocysts: somatic differentiation in vitro. Nat. Biotechnol. 18, 399–404.
Ryu, H., Lee, J., Hagerty, S.W., Soh, B.Y., McAlpin, S.E., Cormier, K.A., 2006. ESET/SETDB1gene expression and histone H3 (K9) trimethylation in Huntington's disease. Proc.Natl. Acad. Sci. U. S. A. 103, 19176–19181.
Sanchez, I., Mahlke, C., Yuan, J., 2003. Pivotal role of oligomerization in expandedpolyglutamine neurodegenerative disorders. Nature 421, 373–379.
Sarkar, S., Davies, J.E., Huang, Z., et al., 2007. A novel mTOR-independent autophagy en-hancer, accelerates the clearance of mutant huntingtin and alpha-synuclein. J. Biol.Chem. 282, 5641–5652.
Sarkar, S., Krishna, G., Imarisio, S., et al., 2008. A rational mechanism for combinationtreatment of Huntington's disease using lithium and rapamycin. Hum. Mol. Genet.17, 170–178.
Schilling, G., Coonfield, M.L., Ross, C.A., et al., 2001. Coenzyme Q10 and remacemide hy-drochloride ameliorate motor deficits in a Huntington's disease transgenic mousemodel. Neurosci. Lett. 315, 149–153.
Shamblott, M.J., Axelman, J., Wang, S., et al., 1998. Derivation of pluripotent stem cellsfrom cultured human primordial germ cells. Proc. Natl. Acad. Sci. U. S. A. 95,13726–13731.
Southwell, A.L., Ko, J., Patterson, P.H., 2009. Intrabody gene therapy ameliorates motor,cognitive, and neuropathological symptoms in multiple mouse models ofHuntington's disease. J. Neurosci. 29, 13589–13602.
Spokes, E.G., 1980. Neurochemical alterations in Huntington's chorea: a study of post-mortem brain tissue. Brain 103, 179–210.
Stack, E.C., Del Signore, S.J., Luthi-Carter, R., Soh, B.Y., Goldstein, D.R., Matson, S., 2007.Modulation of nucleosome dynamics in Huntington's disease. Hum. Mol. Genet. 16,1164–1175.
Tanaka, M., Machida, Y., Niu, S., et al., 2004. Trehalose alleviates polyglutamine-mediatedpathology in a mouse model of Huntington disease. Nat. Med. 10, 148–154.
Tang, T.S., Chen, X., Liu, J., et al., 2007. Dopaminergic signalling and striatal neurodegener-ation in Huntington's disease. J. Neurosci. 27, 7899–7910.
The HDCRG, 2006. Tetrabenazine as antichorea therapy in Huntington disease: a random-ized controlled trial. Neurology 66, 366–372.
Thomas, E.A., Coppola, G., Desplats, P.A., et al., 2008. The HDAC inhibitor 4b amelioratesthe disease phenotype and transcriptional abnormalities in Huntington's diseasetransgenic mice. Proc. Natl. Acad. Sci. U. S. A. 105, 15564–15569.
97A. Kumar et al. / Gene 556 (2015) 91–97
Turnpenny, P., Ellard, S., 2007. Emery's Elements of Medical Genetics, 13th ed. ChurchillLivingstone Elsevier, Philadelphia.
Varma, H., Voisine, C., DeMarco, C.T., et al., 2007. Selective inhibitors of death in mutanthuntingtin cells. Nat. Chem. Biol. 3, 99–100.
Verme, I., Steur, E.N., Jirikowski, G.F., et al., 2004. Elevated concentration of cerebrospinalfluid tissue transglutaminase in Parkinson's disease indicating apoptosis. Mov. Disord.19 (10), 1252–1254.
Vishal, M.G., Nicolas, Offner, James, A., et al., 2011. MoothaMeclizine is neuroprotective inmodels of Huntington's disease. Hum. Mol. Genet. 20 (2), 294–300.
Wang, H., Lim, P.J., Yin, C., et al., 2006. Suppression of polyglutamine-induced toxicity incell and animal models of Huntington's disease by ubiquilin. Hum. Mol. Genet. 15(6), 1025–1041.
Wichterle, H., Lieberam, I., Porter, J.A., et al., 2002. Directed differentiation of embryonicstem cells into motor neurons. Cell 110, 385–397.
Lichuan, Yang, Calingasan, Noel Y., Wille, Elizabeth J., et al., 2009. Combination ther-apy with coenzyme Q10 and creatine produces additive neuroprotective effectsin models of Parkinson's and Huntington's diseases. J. Neurochem. 109 (5),1427–1439.
Young, I.D., 2005. Medical Genetics. Oxford University Press, Oxford.Zeron, M.M., Hansson, O., Chen, N., Wellington, C.L., et al., 2002. Increased sensitivity to N-
methyl-D-aspartate receptor-mediated excitotoxicity in a mouse model ofHuntington's disease. Neuron 33, 849–860.
Zhang, S.C., Wernig, M., Duncan, I.D., et al., 2001. In vitro differentiation of trans-plantable neural precursors from human embryonic stem cells. Nat. Biotechnol.19, 1129–1133.
Zuccato, C., Ciammola, A., Rigamonti, D., et al., 2001. Loss of huntingtin-mediatedBDNF gene transcription in Huntington's disease. Science 293 (5529),493–498.