poster sessions - karger publishers
TRANSCRIPT
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 155
POSTER SESSIONS
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 156
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
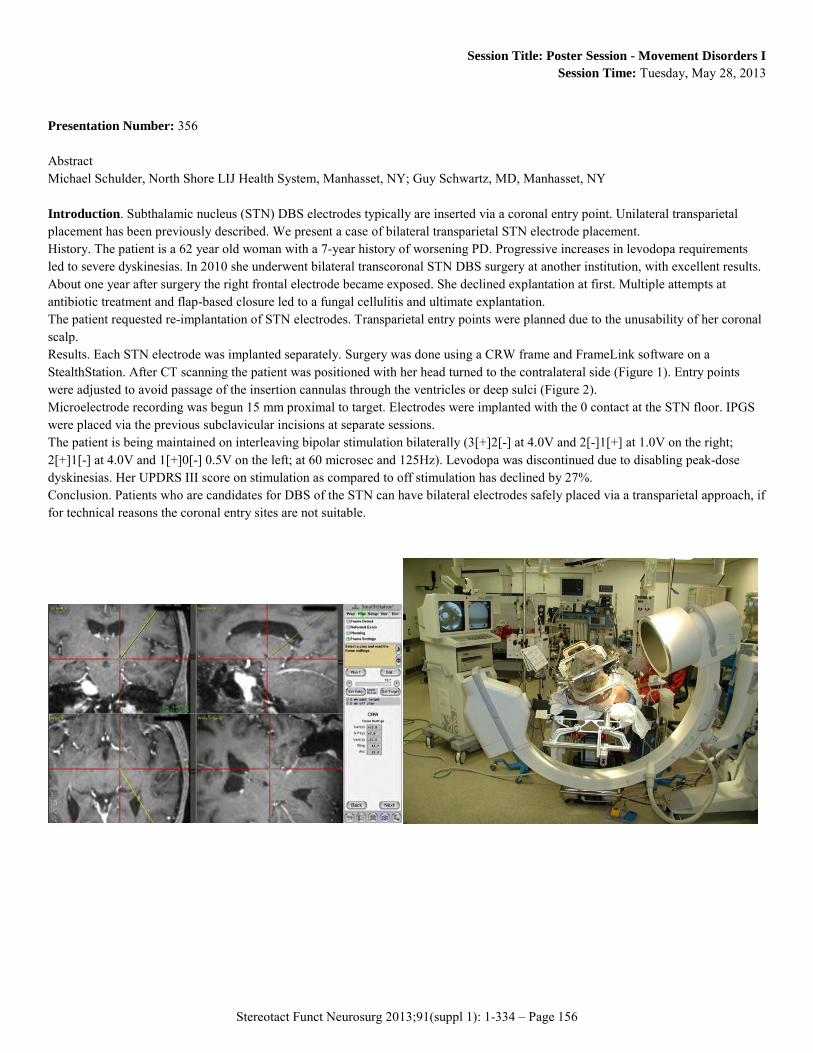
Presentation Number: 356 Abstract Michael Schulder, North Shore LIJ Health System, Manhasset, NY; Guy Schwartz, MD, Manhasset, NY Introduction. Subthalamic nucleus (STN) DBS electrodes typically are inserted via a coronal entry point. Unilateral transparietal placement has been previously described. We present a case of bilateral transparietal STN electrode placement. History. The patient is a 62 year old woman with a 7-year history of worsening PD. Progressive increases in levodopa requirements led to severe dyskinesias. In 2010 she underwent bilateral transcoronal STN DBS surgery at another institution, with excellent results. About one year after surgery the right frontal electrode became exposed. She declined explantation at first. Multiple attempts at antibiotic treatment and flap-based closure led to a fungal cellulitis and ultimate explantation. The patient requested re-implantation of STN electrodes. Transparietal entry points were planned due to the unusability of her coronal scalp. Results. Each STN electrode was implanted separately. Surgery was done using a CRW frame and FrameLink software on a StealthStation. After CT scanning the patient was positioned with her head turned to the contralateral side (Figure 1). Entry points were adjusted to avoid passage of the insertion cannulas through the ventricles or deep sulci (Figure 2). Microelectrode recording was begun 15 mm proximal to target. Electrodes were implanted with the 0 contact at the STN floor. IPGS were placed via the previous subclavicular incisions at separate sessions. The patient is being maintained on interleaving bipolar stimulation bilaterally (3[+]2[-] at 4.0V and 2[-]1[+] at 1.0V on the right; 2[+]1[-] at 4.0V and 1[+]0[-] 0.5V on the left; at 60 microsec and 125Hz). Levodopa was discontinued due to disabling peak-dose dyskinesias. Her UPDRS III score on stimulation as compared to off stimulation has declined by 27%. Conclusion. Patients who are candidates for DBS of the STN can have bilateral electrodes safely placed via a transparietal approach, if for technical reasons the coronal entry sites are not suitable.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 157
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
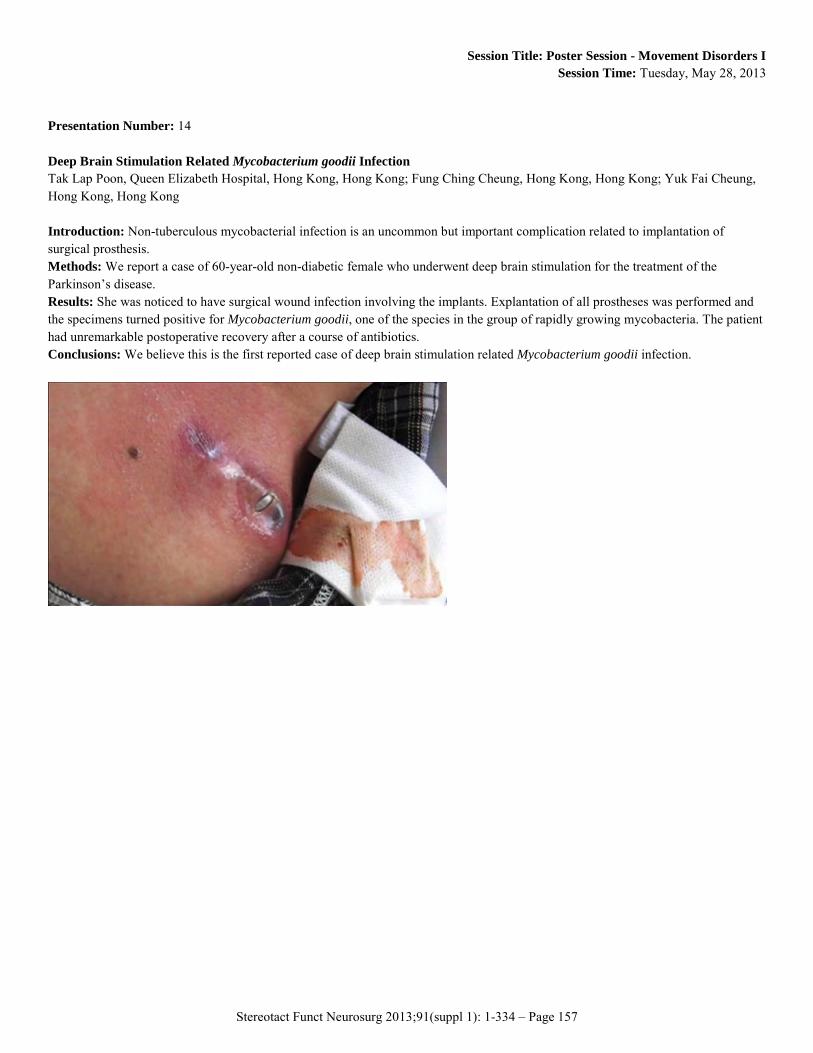
Presentation Number: 14 Deep Brain Stimulation Related Mycobacterium goodii Infection Tak Lap Poon, Queen Elizabeth Hospital, Hong Kong, Hong Kong; Fung Ching Cheung, Hong Kong, Hong Kong; Yuk Fai Cheung, Hong Kong, Hong Kong Introduction: Non-tuberculous mycobacterial infection is an uncommon but important complication related to implantation of surgical prosthesis. Methods: We report a case of 60-year-old non-diabetic female who underwent deep brain stimulation for the treatment of the Parkinson’s disease. Results: She was noticed to have surgical wound infection involving the implants. Explantation of all prostheses was performed and the specimens turned positive for Mycobacterium goodii, one of the species in the group of rapidly growing mycobacteria. The patient had unremarkable postoperative recovery after a course of antibiotics. Conclusions: We believe this is the first reported case of deep brain stimulation related Mycobacterium goodii infection.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 158
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 42 The first Implantation of Baclofen Pump for Treatment of Severe Spasticity in the Federal Center of Neurosurgery, state Tyumen, Russian Federation Artur Biktimirov, MD, Federal Center of Neurosurgery, Tyumen, Russian Federation; Albert Sufianov, MD, PhD, Tyumen, Russian Federation; Alexander Orlov, MD, Tyumen, Russian Federation Introduction: One of the leading Reasons of an Invalidation of the Patients after heavy Cerebral Injury, Stroke, Cerebral Spastic Infantile Paralysis, Multiple Sclerosis and many other Diseases that have a Trend to defeat to the Syndrome of Spasticity. At the Moment the Problem of Treatment of a heavy Syndrome of Spasticity is in the Russian Federation at an early Stage of Development. Methods: 15 Peoples took Part in our Researches that were operated during 2012. All Patients were made MRI, evaluated by means of the Ashworth Score, Spasm Frequency, Barthel Index, Rankin Scales and psychological Tests. Criteria for Implantation of a Pump became: a Tone of no less than 3 on a Scale Ashvort, Reduction of the Tone in 1 Point after the giving a Test Dose of Baclofen, and the most important Thing for the Russian Federation - to live near our Clinic. Results: Spasticity, Spasm Frequency and Quality of Life were clinically and statistically decreased by all Patients. We would like to note the Significant Improvement of Quality of Life at the Patient with a Myelopathy of the Spinal Cord. As a Result of Treatment is that she got rid of the Help in Movement in a Month and returned to a good State of Health. During the Treatment we had 2 Complications. First Case the Catheter tear from the Pump 2 times because of intensive physical Activity. Second Case took Place during the Flight by Plane. The Patient fell into a hypotonic Coma and then she was hospitalized. Next Day after Health Stabilization she was discharged from the Clinic. Conclusions: Chronic intrathecal Baclofen Therapy is really highly effective Method of Treatment for Spasticity that Promote to improve the Quality of Life and Demands Further Development on the Territory of the Russian Federation.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 159
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 408 Long-term Effectiveness of Bilateral Pallidal Deep Brain Stimulation in a 14-year-old Girl with Hallervorden-Spatz Disease Witold Libionka, M.D., Ph.D., Pomeranian Trauma Center in Gdansk, Gdansk, Poland; Wojciech Kloc, M.D., Ph.D., Gdansk, Poland Introduction: Neurodegeneration with brain iron accumulation (NBIA), formerly known as Hallervorden-Spatz disease, is a heterogenous group of progressive extrapyramidal disorders with radiographic evidence of focal iron accumulation in basal ganglia. Mutations in the PANK2 gene account for the majority of NBIA cases. Clinically the syndrome is characterized by dystonia and a pathognomonic pattern on brain MRI, called the eye-of-the-tiger sign. There have been only single case reports detailing pallidotomy or pallidal deep brain stimulation (DBS) for medically refractory Hallervorden-Spatz dystonia with long-term follow-up. Methods: 5-year follow-up of a 14-year-old girl with intractable generalized dystonia secondary to the PANK2 gene mutation treated with bilateral DBS of the globus pallidus internus performed under general anesthesia using microelectrode recording and macrostimulation. Before the operation she was dependent for activities of daily living because of continuous severe dystonic movements in the face, tongue, neck, upper and lower extremities with the Burke-Fahn-Marsden (BFM) Dystonia Rating Scale score of 90/120. Results: Treatment resulted in a still progressing improvement in motor functioning and dystonic symptoms with a reduction in disability (the BFM score improved to 60 points after 2 weeks of stimulation, 56 points after 3 months and 53 points after 6 months). The patient was able to continue normal education. Effect of stimulation was maintained over the period of 63 monts with only mild deterioration (BFM 56 points) presumably secondary to progression of the disease. Conclusions: Bilateral pallidal DBS is an effective and safe treatment option for intractable generalized dystonia in Hallervorden-Spatz syndrome with expected long-term improvement despite progresion of the disease.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 160
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 188 The First Experience Of Surgical Treatment Of Dystonia In Tyumen Region Albert A. Sufianov, Tyumen, Russian Federation; Vladimir A. Shabalov, Moscow, Russian Federation; Alexander S. Orlov, Federal center of neurosurgery, Tyumen, Tyumen, Russian Federation; Artur R. Biktimirov, Tyumen, Russian Federation; Tatyana F. Tubaeva, Tyumen, Russian Federation; Sergey V. Churkin, Tyumen, Russian Federation Introduction: Neurostimulation of deep brain structures is a recognized surgical treatment of primary dystonia. Currently, the greatest number of stereotactic implantation of neurostimulators in Russia carried out at the Institute of Neurosurgery in Moscow. At the same time there is a significant number of patients in other regions of Russia. There was built a new center of neurosurgery in Tyumen region where such operations are conducted with comparable volume of procedures. Methods: There were operated eight patients for treatment of dystonia in Federal Center of Neurosurgery in 2012. Pre-study and treatment planning was performed using MRI Siemens Avanto 1,5 T. Surgical intervention was carried out under endotracheal anesthesia with the standard technique using Leksell stereotactic apparatus and planning station. We performed stereotactic implantation of electrodes in GPi on both sides. The stimulation started usually on the 7 day after surgery. Results: We operated 8 patients, 7 of which suffered from generalized dystonia, one patient suffered from focal dystonia in here left hand. One patient developed dystonia secondary to prolonged use of neuroleptics. Male to female ratio was equal (4/4). The average age of the patients was 48.0 years and the average duration of disease before surgery was 12.3 years. All patients received preoperative medical therapy, including botulinum toxin. In 7 cases the electrodes for stimulation were implanted in the GPi on 2 sides. In case of patient with focal dystonia one electrode was implanted in the right Vop. None of complications after surgery were observed. Conclusions: Deep brain stimulation is an effective minimally invasive intervention in the treatment of generalized dystonia. It is necessary to improve the methods of MR imaging to get images high quality images for more precise planning and better result.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 161
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 308 Succesful Ventralis Intermedius Nucleus Stimulation for HolmesTremor Secondary to Thalamic Posttraumatic Lesions During Childhood Carlos Fernandez Carballal, H.G.U. Gregorio Marañón, Madrid, Spain; Francisco Grandas, Madrid, Spain; Olga Mateo, Madrid, Spain; José Manuel Garbizu Vidorreta, Madrid, Spain; Beatriz De la Casa, Madrid, Spain; Juan Guzmán de Villoria, Madrid, Spain Introduction: Holmes tremor is characterized by resting, postural, and intention tremor. Posttraumatic tremor has been treated with deep brain stimulation (DBS) in Vim with irregular results like other ethiologies of Holmes tremor. Methods: We present two patients with previous cranioencephalic traumas during childhood and posttraumatic thalamic lesions in MRI who had a good response after DBS. Results: Patient A: A 19-year-old woman had suffered a severe TCE with diffuse axonal injury seven years ago. The patient subsequently developed an incapacitating right-upper-extremity tremor refractory to medical treatment. Successive MRIshad showed hipointensal left posterior thalamic lesions in T2 sequences. Thepatient underwent implantation of a deep brain stimulator in the left VIM. A MRI revealed correct position of electrodes, just anterior and lateral to thalamic damage. The patient had a marked symptomatic and functional improvement of several components of tremor (intentional, postural and resting), that is sustained 32 months after surgery. Patient B: A 11-year-old woman had suffered a severe TCE when she was 5, requiring a decompressive craniectomy, with a good postoperative evolution. Gradually the patient developed a left-upper-extremity tremor. An MRI showed posttraumatic temporoocipital leucomalacia and loss of volume of right thalamus, due to axonal injury. No improvement was noted with medical treatment. The patient underwent implantation of a deep brain stimulator in the left VIM, with a marked improvement of tremor, sustained 18 months after the procedure Conclusions: Previous reports have demonstrated that medically resistant Holmes tremor related to a thalamic lesion can be successfully treated with thalamic deep brain stimulation. Partial preservation of Vim nucleus may allow DBS to be effective in cases of structural damage of thalamus, spetially when the traumatic lesions occur during pediatric age.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 162
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 99 Siberian Experience Of Stereotactic Microelectrode Guided Termodestruction Evstafiy Melidi, MD, Federal Neurosurgical Center of Ministry of Public Health, Novosibirsk, Russian Federation; Oxana Gavronina, MD, Novosibirsk, Russian Federation Introduction: The main tendency of modern functional neurosurgery is desire for minimally invasive treatment with destructive technology renaissance on new safety level with neurophysiological navigation monitoring. Methods: during the period 2011-2012 28 patients have undergone stereotactic deep brain structure lesioning. Patients were divided into two groups: first group included 22 patients (16 male, 6 female, age 47 to 74 years) with late stage Parkinson disease, second group included 6 patients (2 male, 4 female, age 36 to 68) with pharmacology resistant chronic pain syndromes of diverse etiology (VAS 9/10). All surgeries were done with Cosman-Roberts-Wells stereotactic frame and Radionics planning system. Definitive verification of targets was performed with intaoperative neurophysiological navigation monitoring and microelectrode recording data (MicroGuide Pro, AlphaOmega). Results: In group with Parkinson disease 15 patients underwent unilateral ventro-dorsal pallidotomy and 7 patients - ventro-intermediate thalamotomy. In all cases surgery allowed to improve the quality of live, average tremor and rigidity regression in contralateral limbs was 62% (UPDRS scale), dystonias and levodopa-induced diskinesias were 76% less common. All patients in the second group underwent bilateral anterior cingulotomy, which allowed to achieve statistically significant lowering of sensitivity to pain (VAS 3-4/10), improvement in daily activities and decrease in number of depressive disorders. Intake of narcotic analgesics, in the post-operative period, decrease by 74%, two patients were completely drug-free. There were no perioperative complications in both groups. Conclusion: intraoperative neurophysiological navigation allows conducting stereotactic destructive surgeries with submillimetric precision, achieving maximal individual clinical effect with lower risk of perioperative complications.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 163
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 61 Recovery Of Motor Function After Epidural Motor Cortex Stimulation sylvie raoul, MD, PhD, chu nantes, nantes, France Introduction: Chronic, drug-resistant neuropathic pain after stroke can be treated by surgically implanted motor cortex stimulation (MCS). Methods: We put MCS for a patient who had hemiplegia and pain of the left body. Pain was improved and she recover movement of the left body with syncinesia.The procedure was reproductible. When the stimulation was off the patient was enable to move her left body and 20 minutes after the stimulation on she can move her left hand and the foot. Results: We assess that MCS can be useful to recover motor function after stroke. We investigate which neurophysiologic pathway can be involved in this motor function improvement. Conclusions: And we conclude that cortical excitability is modified with the MCS and maybe the propriospinal pathway can be involved in this recovery.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 164
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 272 Idiopathic Parkinson´S Disease Complicated By Hydrocephalus, Evaluation Of Shunt Responsiveness. Luiz C. Pereira, PhD, Neurofuncional DF, Brasilia, Brazil; Valeria P. Araújo, neurofuncional DF, Brazil; Igor Campbell Borges, HBDF, Brazil Introduction: Long-term hydrocephalus (LTH) may coexist with idiopathic Parkinson’s disease (IPD) in a small subset of patients. The dilemma to treat by deep brain stimulation (DBS) or by Cerebro-Spinal (CSF) Shunt exists. Despite of concerns on the predictive value, the CSF tap test (CSF TT) remains a gold standard to select patients for Shunting. We report the results of 4 consecutive advanced IPD patients that presented concomitant LTH and were CSF TT positive. Methods: We reviewed all records of a private neurology/neurosurgery clinic in Brasilia. Pre end post-operative mental state exams, UPDRs, neuroradiological exams and video recordings were evaluated. Results: 4 male patients, mean age 62,0 years (range 52 to 74), mean history of IDP for 10,2 years (range 5 to 15) and mean neurosurgical follow up of 3,2 years were submitted to LTH treatment. Supposed etiologies were Idiopathic Normal Pressure Hydrocephalus in 3 patients and post chemical meningitis in one (multiple myelographies). CSF TT (3 days) were considered positive due to gain in posture and locomotion in all cases, better Minimental Scores in 2 cases, improvement in akinesia/bradikinesia in 3 cases and higher CSF pressure in one case. Shunts were programed slowly to the minimum pressure accepted. At last Follow up 1 patient sustained significant UPDRs III benefit (60% improvement), 1 could achieve significant motor benefit (50% improvement) but could not tolerate the lower pressure regime, 1 sustained mild motor benefit (20%) and 1 did not sustain any motor gain, also progressing to severe dementia. DBS surgery is now considered as the next option for 2 cases. Complications: Elective surgical drainage of large chronic subdural hematoma was required in 2 patients. Conclusions: Long-term hydrocephalus (LTH) associated to advanced idiopathic Parkinson’s disease (IPD) is a challenging matter. Shunting as a first procedure, for CSF TT positive patients seems secure.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 165
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 22 Clinical Multicenter Trial For The Treatment Of Cervical Dystonia Using The Hanger Reflex -Interim Report Takashi Asahi, University of Toyama, Toyama, Japan; Michi Sato, ME, Tokyo, Japan; Hiroyuki Kajimoto, PhD, Tokyo, Japan; Genko Oyama, PhD, Tokyo, Japan; Takaomi Taira, PhD, Tokyo, Japan; Akito Hayashi, PhD, Chiba, Japan; Masami Fujii, PhD, Yamaguchi, Japan; Shutaro Takashima, PhD, Toyama, Japan; Satoshi Kuroda, PhD, Toyama, Japan Introduction: When a wire clothes hanger is placed on the head so that it presses on the fronto-temporal region, the head rotates unexpectedly. As the mechanism underlying this reflex is not known, we have temporarily named this phenomenon the “hanger reflex”. We used this reflex to treat patients with cervical dystonia. Materials/Methods: First, we confirmed that the abnormal head positioning caused by cervical dystonia was reduced when a hanger was placed on the head of a patient with this condition. A portable device that induced the hanger reflex was then developed. After approval by the Ethical Committee of the University of Toyama, the device was used in two patients with cervical dystonia. Subsequently, a multicenter trial of this device was started in 2012, including eight centers. The subjects were adults with cervical dystonia who had an abnormally rotated head position. The portable device was used for at least 30 minutes per day for 3 months. Subjects were evaluated before and after treatment using a modified Tsui score and the Toronto Western Spasmodic Torticollis Rating Scale. If patients had been treated with botulinum toxin type A, they were enrolled in the trial after the effects of the botulinum treatment had worn off. Results: In the trial at the University of Toyama, improvement of abnormal head movement was observed in one of the two patients. Conclusions: This unique use of the hanger reflex has the potential to enable less invasive treatment of cervical dystonia. We expect positive results from the clinical multicenter trial. In this presentation, we would like to introduce the trial and show the interim report. This work was supported by (JSPS) KAKENHI (23791587)

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 166
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 409 Effectiveness of Deep Brain Stimulation in Previously Lesioned Pallidum for Generalized Primary Dystonia - Comparison to STN Target Witold Libionka, M.D., Ph.D., Pomeranian Trauma Center in Gdansk, Gdansk, Poland; Wojciech Kloc, M.D., Ph.D., Gdansk, Poland Introduction: Pallidotomy and thalomotomy were common treatments for dystonia before the neuromodulation era. Although initial response to lesioning may be satisfactory, in the long run results are less favourable. Nowadays, this group of patients looks for novel treatments. Methods: Two patients with generalized dystonia previously treated with bilateral thalamotomy and bilateral thalamotomy combined with monolateral pallidotomy presented with dystonic symptom progression. Pallidal deep brain stimulation (GPi DBS) was performed bilaterally in the first patient and contralaterally to the lesion in the second one. On the lesioned side STN was choosen as the target. Patients were evaluated with the Burke-Fahn-Marsden Dystonia Rating Scale (BFMDRS) before and 1, 3, 6 and 12 months after surgery. Results: First patient showed marked functional improvement (70% in BFMDRS after 3 months; maintained during further follow-up) while the second improved moderately (30% in BFMDRS after 3 months), primarily secondary to GPi stimulation. As STN DBS proved to be less effective, additional electrode was implanted into primarily lesioned GPi with satisfactory long-term effect (60% improvement in BFMDRS after 3, 6 and 12 months). Conclusions: Bilateral GPi DBS is an important treatment option for generalized dystonia patients who have undergone pallidotomy or thalamotomy and may be more effective than STN DBS.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 167
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 166 Status Dystonicus Due To Internal Pulse Generator Depletion In A Patient With Primary Generalized Dystonia. Michael R. Sobstyl, MD PhD, Postgraduate Medical Center, Warsaw, Poland; Mirosław Ząbek, MD PhD, Postgraduate Medical Center, Warsaw, Poland; Karol Budohoski, MD, Postgraduate Medical Center, Warsaw, Poland Introduction: To present a patient with primary generalized dystonia after bilateral pallidal stimulation surgery who developed severe status dystonicus (SD) due to the depletion of unilateral internal pulse generator (IPG). Status dystonicus refers to a severe, life threatening episode of generalized dystonia which necessities urgent hospital admission. Known precipitating factors triggering SD include: febrile infection and discontinuation or introduction of a new medication. Similarly to medication immediate withdrawal, abrupt discontinuation or change in stimulation may be regarded as a possible triggering factor for developing SD. Methods: We report on a case of severe SD as result of unilateral IPG depletion. The patient’s disease started at the age of 9 in the right foot and was followed by dystonic movements of the fingers of the right hand. Genetic testing revealed the presence of DYT-1 mutation. After obtaining written informed consent, the patient underwent bilateral pallidal implantation of deep brain stimulation electrodes under general anesthesia. Results: Over the follow-up period the patient experienced the rapid aggravation of dystonic spasms within the left hemibody and one day later was admitted to our emergency unit. On admission within 2 hours the patient developed complete respiratory failure with severe metabolic acidosis, requiring sedation with propofol and fentanyl, tracheal intubation, and mechanical ventilation. The diagnosis of severe SD due to depletion of one IPG was made. The depleted IPG was exchanged and bilateral stimulation was restored. At 12 months follow-up the patient remains under extensive rehabilitation, he is able to eat, but is wheelchair-bound, with improvements in muscle strength and bulk. Conclusions: DBS is widely used not only in Parkinson disease, but also in generalized and focal/segmental dystonia. This case demonstrates that any rapid discontinuation (even unilateral) in patients with generalized dystonia may trigger severe SD.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 168
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 88 Dopamine Agonist Withdrawal Syndrome (DAWS) following STN-DBS Genko Oyama, MD,PhD, Juntendo University School of Medicine, Tokyo, Japan; Atsushi Umemura, MD,PhD, Juntendo University School of Medicine, Japan; Takayuki Jo, MD, Juntendo University School of Medicine, Japan; Asuka Nakajima, MD, Juntendo University School of Medicine, Japan; Natsuko Nishikawa, MD, Juntendo University School of Medicine, Japan; Madoka Nakajima, MD,PhD, Juntendo University School of Medicine, Japan; Hisato Ishii, MD,PhD, Juntendo University School of Medicine, Japan; Yasushi Shimo, MD,PhD, Juntendo University School of Medicine, Japan; Hajime Arai, MD,PhD, Juntendo University School of Medicine, Japan; Nobutaka Hattori, MD,PhD, Juntendo University School of Medicine, Japan Introduction: Dopamine agonist withdrawal syndrome (DAWS) is rare complication of dopaminergic medication, which is defined as a withdrawal state with a severe, stereotyped cluster of physical and psychological symptoms that correlate with dopamine agonist withdrawal in a dose-dependent manner, levodopa-refractory and other medications for Parkinson's disease (PD). Methods: To report and characterize DAWS, we conducted a retrospective chart review of a case with PD who developed DAWS after reduction of pramipexole following bilateral implantation in the subthalamic nucleus (STN) of deep brain stimulation (DBS) devices. Results: The patient is a 69-year old right-handed woman with 16-year history of PD. As she suffered severe motor fluctuation despite multiple medications such as carbidopa/levodopa (10/100) 900mg, entacaopone 400mg, pramipexole 1.5mg, and amantadine 150mg, she underwent bilateral STN DBS. After surgery, carbidopa/levodopa and entacapone were reduced as she had some lesion effects on her motor symptoms. Afterwards she developed symptoms of depression and delusion, pramipexole was gradually reduced with the increase of STN stimulation and addition of quetiapine. Her psychiatric symptoms got worse, whereas her motor symptoms responded to STN stimulation and carbidopa/levodopa. Eventually, her psychiatric symptom improved after increasing pramipexole. Conclusions: As STN DBS has the potential to cause a subsequent reduction in dopamine agonist, DAWS may be encountered after STN DBS. Clinicians should consider the possibility of DAWS when treatment-refractory psychiatric/psychological complications prolong after the reduction of dopamine agonist, and should try to increase the dosage of dopamine agonist to baseline amounts. Additionally clinician should try to keep the dosage of dopaminergic agonists low to prevent the DAWS.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 169
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 175 Deep Brain Stimulation For Dstonia krzysztof szalecki, Institute of Psychiatry and Neurology, warsaw, Poland; Henryk Koziara, warsaw, Poland; Rafal Rola, warsaw, Poland; Pawal Nauman, warsaw, Poland; Wieslaw Bonicki, warsaw, Poland; Bartosz Krolicki, warsaw, Poland; Emilia Soltan, warsaw, Poland; Tomasz Tykocki, warsaw, Poland; Tomasz Mandat, warsaw, Poland Introduction: Deep brain stimulation (DBS) has become an approved method of treatment of various types of dystonia, however there are still plenty of questions regarding long term therapeutic effects. It was noticed that different types of dystonia respond differently to DBS treatment. Methods: Materials: 35 patients, 17 females and 18 males, aged 10-66 years old (mean 31) affected by different typed of dystonia were treated with DBS. 11 patients were diagnosed with PKAN, 3 patients were diagnosed with torticollis, one patient with oromandibural dystonia, and 20 patients with general dystonia. 24 patients underwent bilateral GPi DBS and 11 underwent subthalamic nucleus (STN) DBS. Direct and indirect methods were used to identify the target. Intraoperative microrecording and macrostimulation were conducted in each case. Clinical status of patients was evaluated before surgery and 6, 12 and 24 months after surgery with: Fahn-Marsden Scale(FMS), Unified Dystonia Rating Scale(UDRS ), Global Dystonia Scale(GDS) and Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS). The quality of life was evaluated with SF 36. Results: No serious morbidity or mortality were noticed in the group. Local chest hematoma was reported at the region, where internal pulse generator was implanted. The patient suffered from idiopathic thrombocytopenia. Best results were achieved among patients with with DYT-1 related general dystonia (mean 89%) and oromandibular dystonia (87%). The poorest results were noted at the PKAN group (mean 44%). Mean improvement of 73% was achieved. Conclusions: Deep brain stimulation is an effective and safe method of dystonia treatment. The degree of response to the treatment depends mainly on etiology of dystonia. The improvement lasts in 24 months follow-up.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 170
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 219 Pallidal Deep Brain Stimulation Ameliorate Chorea In A Patient With Antiphospholipid Antibody Syndrome Asssel Saryyeva, M.D., Hanover, Germany; Götz Lütjens, M.D., Medical School Hanover, Hanover, Germany; Christoph Schrader, M.D., Hanover, Germany; Joachim K. Krauss, Hanover, Germany Introduction: Antiphospholipid syndrome is an autoimmune disease which is associated with venous and arterial thrombosis, fetal abort and rarely with movement disorders such as chorea or dystonia. There are only few reports on deep brain stimulation for chorea related to huntington’s disease, choreaacanthozytosis or cerebral palsy. We report on a patient suffering from progressive choreo-athetotic movements due to antiphospholipid antibody syndrome treated with bilateral deep brain stimulation. Methods: A 38-year-old woman developed progressive choreo-athetotic movements of the limbs at 16. Later, she developed also orofacial dyskinesias which were considered as tardive dystonia after longtime medication with haloperidol. Antiphospholipid syndrome was diagnosed at age 24 when elevated titers of cardiolipin antibodies and an asymptomatic ischaemic lesion in the right frontal lobe were found. Therefore anticoagulation with coumarin was started. Symptomatic medication with tetrabenazin and tiaprid reduced chorea, but was limited because of side effects. Results: Bilateral implantation of quadripolar DBS electrodes in the globus pallidus internus and chronic stimulation led to marked improvement of chorea as well as of orofacial dyskinesias by about 80%. The medication with tetrabenazin was reduced from 150 to 25mg and tiaprid was cut off. The effect was sustained at 26 months postoperatively. Conclusions: Bilateral pallidal DBS is an effective treatment for chorea in antiphospholipid antibody syndrome. It may not only improve the choreatic movement disorder but also side effects induced by therapy such as tardive dyskinesia.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 171
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 68 DBS Lead Fracture In Post-DBS Patients Mooseong Kim, Inje University Busan Paik Hospital, Busan, Korea, Republic of Introduction: DBS is effective for movement disorders, pain, epilepsy, psychiatric disorder, severe obesity, etc. But, rarely lead fracture is happen. Methods: We operated over 300 DBS opeartion during last 10 years. One Parkinson's disease patient developed DBS lead fracture, 3 years later after DBS battery gone. Two patients( one parkinsonism, one dystonia patient) developed DBS lead fracture after operated other hospital. Results: Fracture site is DBS lead- extension line in parkinsonism, IPG extension line connecting site fracture in a dystonia patient. A 61-year-old female had operated both Gpi-DBS operations for dystonia in other hospital. Her symtom was improved immediately. But, 2 years later, symtom was aggavated, IPG voltage was increased until 9.0 volts. Symtom was more aggravated, her IPG was exhausted, so IPG was changed into new one under local anesthesia. Operation field, we found IPG extension line connecting site fracture. We operated under general anesthesia and changed into new IPG, new extension line. Conclusions: DBS is effective for movement disorder, but DBS lead fracture is rare complication of hardware-related. If patient's symtoms suddenly aggravated, radiological check and evaluation is needed.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 172
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 290 Persistent Parkinsonian Syndrome Induced By Radiotherapy And Chemotherapy Luiz C. Pereira, PhD, Neurofuncional DF, Brasilia, Brazil; Valeria P. Araújo, neurofuncional DF, Brazil; Igor Campbell Borges, HBDF, Brazil Introduction: Secondary parkinsonism may be related to many conditions such as toxic, traumatic, compressive, vascular, metabolic or post-infectious. Persistent Parkinsonism secondary to cancer treatment is rare and the exact prevalence still unknown. Methods: We reviewed all records of a private neurology/neurosurgery clinic in Brasilia, for a 10 year period. We present here 3 female patients who developed parkinsonism after oncological treatment: 1 systemic chemotherapy for Lymphoma, 1 whole brain radiotherapy for Glioma and 1 motor cortex radiosurgery for Pulmonary Adenocarcinoma Metastasis. Mental state exams, UPDRs, neuroradiological exams and motor performance video recordings were evaluated. Results: Ages were 40, 53 and 58 years and mean follow up 3,3 years (range 2 - 5 years). Symptoms started usually after 1 year of oncological therapy. All patients presented moderate bradikinesia and mild to moderate rigidity, while only one patient complained of moderate tremor. Axial symptoms such as posture, speech, and swallowing problems were mild. Before therapy all patients could carry on the activities of daily living, although spending great effort. The parkinsonian symptoms required persistent anticholinergic and dopamine therapy in all cases, with excellent results. No increase in dopamine requirement was observed but no remittion occurred. Conclusions: Parkinsonism after oncological treatment is an unusual complication but seem treatable and benign. Longer term follow up is required.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 173
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 128 Long-term Follow-up Results Of Unilateral Pallidal DBS And Contralateral Pallidotomy For Generalized Axial Dystonia NOBUHIKO TAKEDA, Tokyo womens university of medicine, Tokyo, Japan Introduction: Bilateral deep brain stimulation (DBS) of the globus pallidum interna (GPi)is well established as treatment of generalized axial dystonia. However, the long-term effect of unilateral pallidal DBS and contralateral pallidotomy is not known. We report two cases of generalized axial dystonia treated with unilateral pallidotomy and contralateral GPi DBS more than 10years ago. Methods: We followed up two cases. Case1: 40-year-old athletic school teacher who presented with severe retrocollis and back muscle dystonic movements. Case 2: 53-year-old teacher of drivingwho had retrocollis, that had been treated peripheral denervation with modest effects. Both patients were not able to work and had difficulty in daily life. Both of them underwent right pallidotomy and left GPi DBS simultaneously in 2000. They were followed up for 12 years. Results: Both cases showed remarkable improvement in dystonic symptoms immediately after the surgery. These benefits persisted for more than 12 years. They went back to the previous occupation and are still active.Every time IPG battery went flat, the dystonic symptoms returned. They underwent re-implantation of IPG 4 times. There were no pallidotomy-related adverse effects. Conclusion: Simultaneous unilateral pallidotomy and contralateral GPi DBS is effective for generalized axial dystonia for long time.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 174
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 138 Supramammillary Commissure as an Internal Landmark for Subthalamic Nucleus Targeting Faisal A. Al-Otaibi, King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia; Amal Mokeem, MD, Riyadh, Saudi Arabia; Thamer Al-Khairalla, MD, Riyadh, Saudi Arabia Introduction: Several internal landmarks to target the subthalamic nucleus (STN) have been used in practice. This study was conducted to identify the relationship between the supramammillary commissure (SMC) upper border and the upper border of the STN. Methods: Twelve consecutive patients who underwent 24 STN deep-brain stimulation (DBS) for Parkinson’s disease were analyzed. Red nucleus and anterior commissure-posterior commissure (AC-PC) distance-based targeting methods were used to target the STN. The co-ordinates (X, Y, and Z) for the STN and SMC upper border were calculated. The X, Y, and Z coordinates of the upper border of the STN identified during microelectrode recording (MER) were noted. The active DBS electrode contact coordinates were calculated based on fusion of postoperative CT with preoperative planning MRI. Results: On average, the SMC upper border was identified at 3.5 mm (± 0.6) below the mid-commissural point (MCP), whereas the top border of the STN was identified at 1.9 mm (± 0.8) below the MCP. The average location of the STN upper border was located 1.5 mm (± 0.7) above the top of the SMC. The average X, Y, Z co-ordinates for the location of the center of the DBS electrode active contact were 11.8, -2, and -1.7 from the MCP. The STN stereotactic coordinate based on SMC as a landmark is as follow: X = 12 mm lateral to SMC center, Y at the center of SMC, and Z at the level of SMC. Conclusion: SMC might be used as an internal landmark for indirect identification of the upper STN border location. However, the small number of patients, in addition to other factors such as image fusion error and brain shift, limits this study.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 175
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 214 Acute Pallidal Over-stimulation Due To Decreased Electrode Impedance Imitating Focal Status Epilepticus Cristian Blahak, M.D., Mannheim, Germany; Marc E. Wolf, M.D., Mannheim, Germany; Hans H. Capelle, M.D., Hanover, Germany; Götz Lütjens, M.D., Medical School Hanover, Hanover, Germany; Joachim K. Krauss, Prof., Hanover, Germany Introduction: Pallidal DBS has been established as an effective and safe therapy for dystonia. Stimulation-induced motor side effects can be caused by spread of current to the corticobulbar or corticospinal tract, resulting in dysarthria and tonic contraction of contralateral face and arm muscles, usually occurring gradually when increasing voltage. Methods: We report on an 80-year-old woman with tardive segmental dystonia. After insufficient medical treatment the patient underwent bilateral GPi-DBS surgery. She was regularly followed postoperatively every two or three months, the detailed stimulation settings including impedance and current drain were registered in a database. Results: The patient experienced a sustained clinical benefit from GPi-DBS, the mean Burke-Fahn-Marsden motor score decreased from 55 pre-OP to 16 at 47 months post-OP (bilateral monopolar stimulation with 4.1V, 130Hz and 210µs). In March 2010, the patient was admitted to another hospital with acute tonic spasms of right face and arm muscles, severe dysarthria and mild right sided hemiparesis. The symptoms were interpreted as a focal status epilepticus and treated with phenytoin and levetiracetam. Two weeks later the patient consulted our clinic, she still complained about severe dysarthria and motor disturbances of the right arm. When checking parameters of the left implantable pulse generator (IPG), a marked reduction of impedance by 45% with a resulting increase of current drain was found. We reduced voltage of the left IPG from 4.5V to 2.4V, subsequently motor disturbances and dysarthria resolved almost completely within minutes. Magnetic resonance imaging still showed correct position of both electrodes. The clear cause for the acute decrease of impedance could not be identified, we assume most likely an IPG malfunction. Conclusions: In GPi-DBS for dystonia, motor side effects due to capsular stimulation can occur as an acute event and without a simultaneous modification of stimulation settings, subsequently to a change in electrode impedance.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 176
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 411 A Critical Analysis Of Outcomes Of Deep Brain Stimulation Surgery For Parkinson's Disease Jeffrey W. Cozzens, MD, Southern Illinois University School of Medicine, Springfield, IL Introduction: Most papers that deal with outcomes for both pallidotomy and deep brain stimulation (DBS) for Parkinson's disease (PD), measure that outcome by comparing the average UPDRS score for a group of before the intervention with the average UPDRS score for the group after the intervention. When this is done most studies report an average 40 to 60% improvement in the off-medicine motor score for the surgical group and an average 50 to 90% improvement in dyskinesia disability for the surgical group. What these papers do not tell us is the percentage of patients who improve with DBS surgery. Only the package insert for the Activa DBS system contains this data. Methods: The methods and results of most of the significant published papers on bilateral subthalamic nucleus (STN) DBS surgery outcomes for Parkinson's disease are reviewed. The UPDRS data from 23 patients undergoing STN DBS surgery for PD at our institution are reviewed in terms of the percentage of patients achieving "good" outcome vs. "unchanged or worse" outcome. Results: The Activa package insert indicates that 91.8% of patients undergoing bilateral STN DBS surgery for PD have some improvement in UPDRS III scores (71.2% had major improvement) and 8.2% are unchanged or worse. This corresponds to the data from our institution. Conclusions: The extent of the benefit of bilateral STN DBS surgery for PD is greatly under reported. Clinical decisions about the management of advanced PD are flawed by the lack of information concerning the percentage of patients who achieve a "good" outcome with bilateral STN DBS surgery. This data is not available primarily because there is at present no widely accepted definition of "good" outcome. We propose further study of this issue and the establishment of criteria for outcomes in DBS surgery and a useful and validated outcome scale.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 177
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 54 Infections following Deep Brain Stimulation - a proposed classification system Raymond Cook, MBBS(Hons),FRACS, North Shore Private Hospital, Sydney, Australia; Lyndsey Jones, RN, Sydney, Australia; George Fracchia, BSc(Med),MBBS, Sydney, Australia; Nathan Anderson, B.Appl.Sc(MRS),M.Hlth.Sc.(MRS), Sydney, Australia; Jenny Miu, BMedSci(Hons),PhD, Sydney, Australia; Linton Meagher, BA,MBBS(Hons),M.Psychiatry,FRANZCP, Sydney, Australia; Peter Silburn, BSc(Hons),PhD,MBBS,FRACP, Brisbane, Australia; Paul Silberstein, BSc(Med),MBBS,MD,FRACP, Sydney, Australia Background: Infections are a well reported complication of DBS surgery, with early infections - those occurring within six months - the focus in the literature. In our experience late infections may be of equal or greater frequency than those seen in the early post operative period raising the possibility that the rate of late infection is under-reported in the literature. We report on seven incidences of infection from our surgical series, and propose a classification system for infections following DBS. Methods: Clinical notes on our consecutive series of 303 patients (624 electrodes) over an 11 year period were reviewed for infective complications. Results: There were seven incidences (six patients) of infection (2.3%). Infections were classified by latency from surgery (<6 months n=3; >6 months n=4) and site: lead infection (n=2), pocket infection (n=5) or systemic sepsis (n=0). There were 2 cases of erosion in the absence of infection: extracranial DBS lead (n=1) and stimulator pocket (n=1). There were no cases of intracranial infection. With one exception the causative organ was a skin commensal. Infections were treated with wash out of the IPG pouch and long term antibiotics (n=1), total (n=2) or partial (n=3) system explantation with reimplantation (n=5) at three months - all without reinfection. Conclusions: DBS infection may occur many months after initial implantation and patients must accept a long term infection risk. Most infections require further surgery for definitive management. A classification system based on infection site and latency from surgery is proposed.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 178
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 78 Stereotactic Deep Brain Surgery For Dystonia - Indian experience Milind Sankhe, P D HINDUJA NATIONAL HOSPITAL, MUMBAI, MUMBAI, India Objective: Generalised Dystonia, primary or secondary is disabling and refractory to medical line of management. Stereotactic surgery an option for these patients was introduced in India later than the rest of the world. We present the spectrum of our cases and share our initial experience with the results. Material & Methods: We analyze 28 patients having undergone surgery for dystonia. These include patients having generalized dystonia, focal and hemidystonia. The surgical spectrum includes pallidotomy, pallidal deep brain stimulation, thalamotomy and thalamic deep brain stimulation. The surgical techniques varied from the standard stereotaxy using thermocoagulation, gamma knife radiosurgery and the implantation of deep brain stimulation electrodes. Initial cases were performed without the use microelectrode recordings and efforts were made to localize the optic tracts anatomically and physiologically. We share the techniques used and the outcome in these patients. Results: Wide spectrum of patients including generalized and focal dystonia have been treated at our center. The number of patients with secondary dystonia is larger than the primary dystonia. The surgical technique is now standardized with good imaging quality and reliable microelectrode recordings. Patients with primary dystonia having undergone bilateral pallidal surgery had excellent outcome showing significant reduction in UDRS scores & allowing patients to return to near normal life. Patients with secondary dystonia who underwent pallidal surgery also showed some benefit improving their physical activities, but not allowing independence. Conclusions: Dystonia surgery is life changing to the individual and family. Pallidal surgery is beneficial for patients with generalized dystonia. Thalamic surgery has a role in patients with focal dystonia. Pallidal surgery for secondary dystonia is not as beneficial as primary dystonia however it makes it easier for the care givers.. Key words: Dystonia, Stereotactic surgery.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 179
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 20 Deep Brain Stimulation For Chorea-acanthocytosis Dong-Wan Kang, Pusan National University Hospital, Busan, Korea, Republic of; Jae-Hyuk Lee, Busan, Korea, Republic of Introduction: Chorea-acanthocytosis(ChAc) is a rare autosomal recessive neurodegenerative disorder characterized by progressive movement disorder that usually includes chorea and dystonia. Medical treatment is mostly ineffective. Deep brain stimulation (DBS) has been tried in ChAc, but the clinical outcomes have been inconsistent. We report here a genetically confirmed case of ChAc who showed significant improvement after bilateral deep brain stimulation (DBS) of the internal globus pallidum (GPi). Methods: A 36-year-old man without family history of movement disorders developed slurred speech, oro-facio-lingual dyskinesia, tongue and lip biting, intermittent fast bending forward and backward of neck and trunk, slow alternating lateral flexion of trunk when walking, and gait instability with frequent falls during the past 3 years. Chorea-acanthocytosis was eventually confirmed by the finding of bilateral striatal atrophy on brain MRI, acanthocytosis in the scanning electromicroscope, and finally homozygous nonsense mutation in the VPS13 gene. These symptoms did not respond to medications, such as tetrabenazine, haloperidol, olanzapine, and clonazepam. Results: After written consent was obtained, he underwent bilateral implantation of a quadripolar electrode into the GPi under generalized anaesthesia. Postoperatively, the benefit was rapidly evident with marked improvement in choreic movements. Tongue and lip biting almost disappeared. He was able to walk independently. However, alternating lateral dystonic flexion in trunk and dysarthria did not improved. In the postoperative evaluation, motor section of Unified Huntington’s Disease Rating Scale (UHDRS) scored 59 in the preoperative evaluation, and 36 (GPi DBS at 130 Hz) in the postoperative 1 year. Conclusions: The result of our patient suggests that DBS can be useful for symptomatic treatment in case of ChAc, although still few data exist about long term benefit. Chorea in particular was improved by GPi-DBS.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 180
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 81 Effects Of Deep Brain Stimulation On Tardive Dyskinesia Kazutaka Shimizu, Tokyo Metropolitan Neurological Hospital, Tokyo, Japan; Fusako Yokochi, Tokyo, Japan; Makoto Taniguchi, Tokyo, Japan; Ryoichi Okiyama, Tokyo, Japan; Ayako Isoo, Tokyo, Japan; Takashi Kawasaki, Tokyo, Japan; Koichi Hamada, Tokyo, Japan Introduction: Tardive dyskinesias (TD) is characterized by abnormal involuntary movements (AIMs) resulting from chronic treatment with agents that block dopamine receptors in the brain. It is difficult to treat TD with medicines. Deep brain stimulation (DBS) of the internal pallidum (GPi) may represent a therapeutic alternative for TD. In this report, we describe the cases of patients with TD successfully treated by GPi-DBS. Methods: GPi-DBS was performed on four patients using the Leksell frame and neural microrecording method. Tentative target was the dorsal surface of optic tract measured on MRI. Patients were evaluated before and after surgery using the Burke-Fahn-Mardsen Dystonia Rating Scale (BFMDS) and Dystonia Disability Scale (DDS). The background features of the patients are below.Pt1: A 45-year-old male with depression had been treated with neuroleptics. AIMs in the upper trunk and bilateral proximal upper limbs developed, which a year later AIMs extended to the face.Pt2: A 46-year-old male had depressive disorder for 10 years. He had been treated with multiple neuroleptics. He had AIMs in both the neck and face for 7 years.Pt3: A 25-year-old male had obsessive-compulsive disorder for 8 years treated with multiple neuroleptics. His AIMs first developed in his right upper arm and then face over 3 years.Pt 4: A 63-year-old female had been sufferig from oral dyskinesia for a year. Her history of taking medicines was not clear. Results: There were no adverse events in the intra- and postoperative periods. Postoperative BFMDS and DDS total scores of the patients improved in each follow-up assessment. But it was less effective on the cervical dorsiflexion. Conclusions: Clinical improvements of these patients, which correspond to previous studies, suggest that GPi-DBS provides a promising treatment option for TD. The effects of GPi-DBS on cervical dyskinesia remains unclear.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 181
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 170 Combined of Peripheral Denervation on SCM muscle and bilateral GPi Deep Brain Stimulation for Laterocollis Patients Jae Hyun Park, MD, Incheon St. Mary's Hospital, Incheon, Korea, Republic of; Ryoong Huh, MD,PhD, Incheon, Korea, Republic of Introduction: Laterocollis is hard to controlled by single procedure such as, Globus pallidus interna(GPi) deep brain stimulation(DBS) and selective peripheral denenervation. In case of selective peripheral denervation, it requires more invasive procedure for complete dennervation for levator scapulae muscle. In case of GPi DBS, especially tonic type laterocollis is not well controlled by itself. So, we tried combined simple peripheral denervation on sternocleidomastoid(SCM) muscle and bilateral GPi DBS for laterocollis. Methods: Between 2009 and 2012, 4 patients with laterocollis have been performed combined ipsilateral SCM muscle denervation with myomotomy and bilateral GPi DBS by staged operation. There are 2 males and 2 females and mean age was 51.8± 10 years old. The symptom duration was 24.8±10 months. Mean follow up duration was 11.3 ±months. Three patients were performed GPi DBS first and one patient performed SCM denervation first on other institute. The mean time interval of operations were 6.8 ± 2 months. Results: All of patients had excellent result in clinically. After fist operation, mean Toronto Western Spasmodic Torticollis Rating Scale(TWSTRS) reduction rate was 20.8% and after second operation, it was 92.4%. Though long-term follow up is needed, short-term outcome seems very excellent. There was no serious complication. Conclusions: In laterocollis, combined simple peripheral denervation of ipsilateral SCM muscle and bilateral GPi DBS can be a safe, successful treatment.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 182
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 218 Clinical Appearance Of Neuroacathocytosis Changes From Primary Hyperkinetic Choreatic To Secondary Parkinsonism In A Patient Treated With Pallidal Deep Brain Stimulation. Asssel Saryyeva, M.D., Hanover, Germany; Götz Lütjens, M.D., Medical School Hanover, Hanover, Germany; Christoph Schrader, M.D., Hanover, Germany; Georg Berding, Prof., Hanover, Germany; Mahmoud Abdallat, Hanover, Germany; Andreas Wloch, Hanover, Germany; Joachim K. Krauss, Prof., Hanover, Germany Introduction: The clinical picture of neuroacanthocytosis varies and may present most often with limp chorea but also dystonia and rarely parkinsonian symptoms. Despite the motor changes, alterations of behaviour and cognitive functions are observed. Methods: We report on a 46-year-old woman who underwent bilateral DBS in the globus pallidus internus (GPi) to treat genetically confirmed chorea-akanthocytosis. Two years after implantation, the clinical picture changed and primary hypokinetic parkinsonian symptoms became prevalent. To exclude that this change was due to stimulation, UPDRS motor subscale was assessed in “on” and “off” and positron emission tomography (PET) with fluordesoxyglycosis (FDG) was performed with stimulation “on” and “off”. Additionally levodopa testing was conducted. Results: UPDRS did not change in “on” and “off” stimulation and PDG-PET did not reveal differences within the basal ganglia between “on” stimulation and “off” stimulation. The levodopa test did not improve the clinical picture. Adjustment of the stimulation setting subjectively improved the clinical picture. Conclusions: The clinical picture of chorea-acanthocytosis may change overtime from primary hyperkinetic to secondary hypokinetic. Bilateral GPi stimulation could be excluded to be the primary cause of this change.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 183
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 220 Practical Use of a portable Auditory Device to improve Freezing of Gait in a patient with Parkinson’s Disease. William O. Contreras Lopez, University Freiburg Medical Center, Freiburg im Breisgau, Germany; Jairo Alberto Espinoza Martinez, MD, CIMAD, Colombia; Carlos Andres Escalante Higuera, Brainmee, Spain Objectives: To study the effect of rhythmic auditory cues on gait in a patient with Parkinson’s disease with severe freezing. Methods: A 65 years old volunteer patient with Parkinson’s disease (PD) for 7 years and with Deep brain stimulation (DBS) suffering from difficulty in walking, including: Difficulty of gait initiation, maintenance of the gait, dysfunctional turning, frequent freezing and a tendency to fall, who did not improve with pharmacological adjustments, physical therapy or changes in the electrical parameters of the DBS programming, was tested using auditory rhythmic cues matching step frequency through a new external portable device (Listenmee-Brainmee © Barcelona-Spain). The patient was analysed in a Gait Analysis Laboratory, using several cameras (video and infrared) placed around a walkway, which were linked to a computer. The systematic study of the patient motion, involved the analysis of the videos by a group of experts on gait (orthopaedics - neurologists) who were blinded towards the device being turned on or off. The results are reported in terms of change in object of analysis parameters (protocol laboratory MOVYSIS), and subjective quality of life. Results: The patient improved in the motion analysis. Rhythmical auditory cueing induced speed changes. Freezing of gait showed the same positive response. And the patient reported improvement in their quality of life and the desire to permanently continue the use of the device.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 184
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 366 The Effects on Autonomic Function after STN-DBS Surgery Kang-Du Liu, MD, Taipei Veterans General Hospital, Taipei, Taiwan Introduction: Dysfunctions of the autonomic nervous system (ANS) are common in Parkinson's disease (PD). The beneficial effects of STN stimulation on motor symptoms are well known, but little is known on autonomic function. Based on the fact that diffusion of current during stimulation of the STN may simultaneously involve the motor and non-motor, limbic and associative areas of the STN, the aims of this study were to examine whether STN stimulation has an influence on functions of the ANS and, if so, to correlate these effects with the active contacts of electrodes in the STN. Methods: Eight PD patients with good motor control and quality of sleep after STN-DBS surgery were recruited for the study. All patients had 2 days of recordings with portable polysomnography (PSG) (first night with stimulation “ON” and second night “OFF”). From the PSG data, the first sleep cycle of each recording night was defined. Heart rate variability (HRV) was analyzed between the same uninterrupted periods of the two sleep nights. In addition, the optimal electrode positions were defined from postoperative MRI studies and the coordinates of active contacts were confirmed. Results: The results of HRV spectral analysis showed that only low-frequency (LH)/high-frequency (HF) power was significantly activated in the stimulation “on” groups (P<0.001). Regarding the position of the electrode, in patients whose active contact of electrode was located more medial, the LF/HF power was much activated during stimulation (P=0.008). Conclusions: These results demonstrate that STN-DBS can enhance sympathetic regulation, and that the sympathetic response may be due to the activation of the limbic portion of the STN or descending sympathetic pathways in the zona incerta.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 185
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 302 Bilateral Globus Pallidus Internus Deep-Brain Stimulation for Woodhouse Sakati Syndrome Faisal A. Al-Otaibi, MD, King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia; Amal Mokeem, MD, Riyadh, Saudi Arabia; Thamer Al-Khairalla, MD, Riyadh, Saudi Arabia Introduction: Woodhouse Sakati syndrome (WSS) is a rare autosomal recessive neuroendocrine disorder. Extrapyramidal neurological manifestations are mainly characterized by dystonia and chorea. Here we report two cases of WSS that underwent bilateral globus pallidus internus deep-brain stimulation (GPi DBS). Methods: A retrospective analysis of two patients with WSS was conducted. Clinical, radiological, and biochemical features were analyzed. Both patients underwent bilateral GPi DBS. The follow-up period was 6 years for the first patient and one year for the second. Results: The first patient was a 40-year-old male who became bedridden due to generalized dystonia and suffered from diabetes mellitus. A magnetic resonance image (MRI) of the brain featured white matter abnormal signals at the centrum semiovale. Bilateral GPi DBS did not improve his dystonia. The second patient was a 19-year-old male who suffered from generalized dystonia with severe jaw dystonia that limited his oral intake. He developed weight loss secondary to jaw dystonia. An MRI of his brain was normal. Overall, he had a good response to GPi DBS. Jaw dystonia responded more than extremities. When the device was accidentally switched off, he developed locked jaw after 24 hours, but improved 10 hours after turning the device “on”. Conclusion: WSS is a rare syndrome that is associated with generalized dystonia. MRI abnormality may predict the response to DBS. Bilateral GPi DBS can improve dystonia in WSS. However, the degree of benefit is similar to that seen with other secondary dystonias.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 186
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 60 Electro-acunpuncture As Analgesia Technique For Dbs In Parkinson’S Disease sylvie raoul, MD, PhD, chu nantes, nantes, France Introduction: Deep brain stimulation in the subthalamic nucleus is common now to treat all symptoms of Parkinson’s disease. Usually this kind of surgery was done under local anaesthesia to evaluate the benefit of the surgery on rigidity, tremor and akinesia and to verify that there is no side-effect. Drugs which can modify rigidity are not indicated. So during the surgery morphinic drugs can not be used because of decreasing the rigidity. To decrease the pain and the discomfort of the surgery we used electro-acunpuncture. Methods: Ten patients were done under local anesthesia and electro-acunpuncture. Patients were prepared the day before surgery with a video of the surgery and explanations of the electro-acunpuncture technic and one electro-acupuncture was done to test the sensibility and the tolerance of the patient. The day of the surgery the patient is placed of the surgery table and the electro-acunpuncture begin before the surgeon put the frame on the head of the patient. Evaluation of VAS were done before the surgery and every painful phases of surgery and evaluation of the anxiety score. Results: Results were good with decreased of pain on Vas than more 50% compared to control subjects, anxiety was decreased too and patient’s satisfaction was evaluated with 80% of patients said that pain VAS was about 2/10 and decrease of anxiety score. Conclusions: electro-acupuncture can help patients to decrease pain and surgical discomfort.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 187
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 249 Planning Clinical Trial of Stem Cells in Patients with Parkinson's disease Inbo Han, MD, Seongnam, Korea, Republic of; Youngseok Park, MD, Seongnam, Korea, Republic of; Hyung-Min Chung, Seongnam, Korea, Republic of; Ji-Sook Moon, Seongnam, Korea, Republic of; Sangsup Chung, MD, PhD, CHA University, CHA Bundang Medical Center, Seongnam, Korea, Republic of Introduction: Parkinson's disease (PD) is a progressive neurodegenerative disease and fetal mesencephalic dopamine neuronal precursor cells (NPCs) have been considered to be the most suitable candidates for cell therapy. However, a drawback of this therapeutic approach is the ethical concerns of obtaining sufficient fetal tissue grafts to treat a large number of patients. We’re planning to explore the safety and tolerability after transplantation of fetal mesencephalic dopamine NPCs in patients with idiopathic PD. Methods: We will enroll fifteen patients and inclusion criteria are as follows: 1)patients with idiopathic PD, 2) Hoehn and Yare stage III or IV, 3) patients have shown improvement of Part III UPDRS (Unified Parkinson's Disease Rating Scale) score by at least 33% after levodopa dose in the morning, 4) less than 70 years. Results: We developed new techniques to provide a large amount of fetal NPCs for transplantation through in vitro expansion. All the patients will be transplanted bilaterally into the putamen and caudate nuclesus with fetal mesencephalic dopamine NPCs. We will evaluate symptoms in motor function part of UPDRS after transplantation of fetal NPCs, improvement of 18F-FP-CIT uptake in the putamen using 18F-FP-CIT PET Conclusion: We will develop and initiate a clinical trial that would use fetal mesencephalic dopamine NPCs for the treatment of PD.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 188
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 301 An Audit of patient satisfaction following Deep Brain Stimulation(DBS) Deb Roy, Queen Elizabeth Hospital, Birmingham, United Kingdom Introduction: In order to assess the care provided against the standard detailed within the Department of Health, United Kingdom (2005) National Services Framework for long term (neurological) conditions. It was agreed to survey patients attending for Deep Brain Stimulation (DBS) about their personal experience. Initial audit was conducted in October 2008 and then repeated in November 2009 and March 2012 Methods: Questions were based on standards set within the National Service framework for long term (neurological) conditions, which included discussion of treatment options, explanation of procedure and post operative support. The survey was split into 4 sections to include the experiences with different staff groups. This included the: 1) Appointment with Neurologists 2) Appointment with Neurosurgeons 3) The care received from anaesthetist 4) The care received from the hospital Parkinson’s disease nurse A total of 118 patients received a copy of the questionnaire through the post along with a self-addressed envelope. Patients were given four weeks to return the completed questionnaires after which a second and final reminder letter was sent. Patient anonymity was maintained throughout the process. 86 patients were audited from 1998 to 2008, 32 new patients repeated in March 2012. Results: 110 patients (93.2%) patients returned the questionnaire. P> Conclusions: The results suggest that the service for DBS patients does meet the standards set within the National Service Framework for long term (neurological) conditions: Patient centred service,,specialist rehabilitation and personal care and support. There is evidence that primary and secondary care are working together to provide a safe and effective service for the patients
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 189
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 292 Simultaneous Thalamic And Pallidal Stimulation In A Patient With Myoclonus Dystonia Syndrome Using A Novel Deep Brain Stimulation Device Wolfgang Hamel, MD, Universitätsklinikum Hamburg-Eppendorf, Hamburg, Germany; Carsten Buhmann, MD, Universitätsklinikum Hamburg-Eppendorf, Germany; Alexander Münchau, MD, Universitätsklinikum Hamburg-Eppendorf, Germany; Alessandro Gulberti, Dipl. Psych., Universitätsklinikum Hamburg-Eppendorf, Germany; Johannes Köppen, MD, Universitätsklinikum Hamburg-Eppendorf, Germany; Tobias Bäumer, MD, Universitätsklinikum Hamburg-Eppendorf, Germany; Simone Zittel, MD, Universitätsklinikum Hamburg-Eppendorf, Germany; Christian Gerloff, MD, Universitätsklinikum Hamburg-Eppendorf, Germany; Manfred Westphal, MD, Universitätsklinikum Hamburg-Eppendorf, Germany; Andreas Engel, MD, PhD, Universitätsklinikum Hamburg-Eppendorf, Germany; Christian Moll, MD, Universitätsklinikum Hamburg-Eppendorf, Germany Introduction Selected patients undergoing deep brain stimulation (DBS) may benefit from simultaneous utilisation of multiple targets. However, due to technical restrictions of currently available neurostimulators differential activation of multiple electrodes is limited (e.g. frequency), and optimal programming may require the implantation of two separate stimulation devices. We evaluated a novel DBS device (Synaptix, Niel, Belgium) that is based on 16 independent current sources and enables differential control of multiple leads. Methods: A 35 year-old male suffered from medically refractory myoclonus dystonia syndrome (MDS) associated with torticollis and irregular jerky movements of the head and both arms. Four quadrupolar DBS electrodes (diameter, 1.3 mm; electrode height, 1.25 mm; distance, 0.5mm) were implanted bilaterally into the ventrolateral thalamus (VIM) and globus pallidus internus (GPi) in a single session under local anaesthesia. Results: Stimulation was kept off until a microlesioning effect had resolved after four weeks. While thalamic stimulation led to an immediate and complete control of myoclonic head jerking, GPi electrodes had a rather moderate effect. Three months after the operation, 180Hz-stimulation (2.2mA, 90μs) of the VIM electrodes still resulted in a near-complete (>90%) resolution of jerky and tremulous head movements even in stressful situations during career re-entry. However, cervical dystonia was still present. Within the next 3 months, additional monopolar stimulation of the second most distal contacts of both pallidal electrodes (1.2mA, 60μs, 130Hz) completely resolved the remaining dystonia and occasionally occurring small-amplitude head movements. The effect is stable for >12 months. Conclusion: Symptom-specific programming of DBS required the use of different and high frequencies (up to 180 Hz). The new device represents a technological advance in the field of neurostimulation as simultaneous and independent stimulation could be performed without limitations.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 190
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 275 Long-term Outcome Of Bilateral Pallidal Deep Brain Stimulation In Patients With Primary Torsion Dystonia Fusako Yokochi, MD, PhD, Tokyo Metropolitan Neurological Hospital, Tokyo, Japan; Makoto Taniguchi, MD, PhD, Tokyo, Japan; Satoko Kumada, MD, PhD, Tokyo, Japan; Ryoichi Okiyama, MD, Tokyo, Japan; Koichi Hamada, MD, Tokyo, Japan; Takashi Kawasaki, MD, Tokyo, Japan; Ayako Isoo, MD, PhD, Tokyo, Japan; junichi yokosuka, MD, Tokyo, Japan Introduction: Primary torsion dystonia is also known as DYT1 and pallidal DBS (GPi-DBS) improves symptoms. Methods: Twelve patients with DYT1, (seven males and five female) were treated by bilateral GPi-DBS. The mean onset age, mean duration until the operation, and mean follow-up duration were 9.1 years, 13.3 years, and 6.1 years, respectively. The operation was performed using the Leksell frame and microrecording method under general anesthesia. The tentative target was the dorsal surface of the optic tract determined from MRI images. Clinical assessment was based on neurological findings and the Burke-Fahn-Marsden dystonia rating scale. Results: The symptoms of DYT1 varied. Ten patients had generalized dystonia (GD) and their initial symptom was limb dystonia. One of them had Charcot-Marie-Tooth disease (CMT)-like symptoms. GD of nine patients was satisfactorily improved, but the patient with CMT-like symptoms underwent orthopedic surgery to be able to stand or walk by himself. One patient had segmental dystonia and her initial symptom was cervical dystonia (CD), and she had botulinum toxin injection with DBS to improve her CD every months. One patient showed the symptom of truncal myoclonic-like movement and hand dystonia. The effects of GPi-DBS varied, but it was confirmed that their social activities improved. We tried to change the stimulation conditions in a few patients. The conditions were changed from a strong bipolar stimulation of an extensive area using to monopolar stimulation. Their symptoms were not changed. Conclusions: Previous reports showed that dystonia in DYT1 improved by GPi-DBS. Our findings are not in disagreement with such reports. The symptoms of DYT vary and the improvement depends on the symptoms. After a long-term follow-up, the condition of DBS stimulation might be changed to the maintenance mode.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 191
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 268 The Clinical Impact of Precise Electrode Positioning in STN DBS on Three-year Outcomes Jae Ha Hwang, Seoul National University Hospital, Seoul, Korea, Republic of; Ji Young Yun, Seoul, Korea, Republic of; Sang Woo Song, Seoul, Korea, Republic of; In Kyeong Kim, Seoul, Korea, Republic of; Jin Wook Kim, Seoul, Korea, Republic of; Han-Joon Kim, Seoul, Korea, Republic of; Hee Jin Kim, Seoul, Korea, Republic of; Young Eun Kim, Seoul, Korea, Republic of; Yong Hoon Lim, Seoul, Korea, Republic of; Mi-Ryoung Kim, Seoul, Korea, Republic of; Jae Hyuk Huh, Seoul, Korea, Republic of; Keyoung Min Lee, Seoul, Korea, Republic of; Sue K. Park, Seoul, Korea, Republic of; Cheolyoung Kim, Seoul, Korea, Republic of; Dong Gyu Kim, Seoul, Korea, Republic of; Beom Seok Jeon, Seoul, Korea, Republic of; Sun Ha Paek, Seoul, Korea, Republic of Introduction: Few studies have analyzed the clinical impact of subthalamic nucleus (STN) deep brain stimulation (DBS) as a function of the positioning of the inserted electrode. We investigated the three-year outcomes in Parkinson’s disease (PD) patients following bilateral STN DBS in terms of the electrode positions. Methods: Forty-one advanced PD patients were followed up for over three years following bilateral STN DBS. Patients were evaluated with the Unified Parkinson’s Disease Rating Scale (UPDRS), Hoehn and Yahr staging, Schwab and England Activities of Daily Living (ADL), and the Short Form-36 Health Survey (SF-36) before surgery and one, two, and three years after surgery. The patients were divided into two groups according to the electrode position based on the fused preoperative MRI and postoperative CT images: group I included patients who had both electrodes in the STN (n=30) while group II included patients who did not have both electrodes in the STN (n=11). Results: The UPDRS, the Hoehn & Yahr staging, the Schwab and England ADL, and the SF-36 scores showed significant improvements with decreased L-dopa equivalent daily doses (LEDDs) in both groups as well as in the group as a whole for up to three years following bilateral STN DBS. However, the off-medication UPDRS total and motor (part III) scores significantly deteriorated with increased LEDDs for patients in group II three years after STN DBS compared to that of the group I patients. Conclusions: We conclude that better electrode positioning leads to better long-term outcomes in advanced PD patients following STN DBS.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 192
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 84 High Cervical Spinal Cord And Bilateral Deep Brain Stimulation For Treatment Of Spasmodic Torticollis Michelle Kameda-Smith, MRCS, Dundee, United Kingdom; Suzanne sinclair, RCN, Dundee, United Kingdom; Robert Swingler, MD, FRCP, Dundee, United Kingdom; Sam Eljamel, MBBCh, MD, FRCSIre, FRCSEd, FRCS(SN), The University of Dundee, Dundee, United Kingdom Introduction: Spasmodic torticollis is the commonest form of adult-onset focal dystonia and medical treatments often renders limited benefit with significant side effects. Surgical treatment for spasmodic torticollis initially involved peripheral procedures; though, these procedures tended to lose benefit over time. However, stimulation of the high cervical spinal cord has been demonstrated to result in marked improvement in patients who have received continuous stimulation over several months. Failing this, recent studies have highlighted the efficacy of bilateral pallidal stimulation in the management of selected cases of intractable spasmodic torticollis. Methods and Results: A 61-year-old male, had previously undergone a C5/6 decompression and C4/5 interbody fusion, presented with intractable spasmodic torticollis since his mid-30’s. Botulinum toxin injection resulted in initial alleviation of symptoms, however the results were short lived and with successive injections, the treatment effect was markedly reduced. After failure of medical intervention, a high cervical spinal cord stimulator was sited. The significant alleviation of spasticity and neck pain lasted for 16 months prior to lead fracture. The lead was changed and repositioned with significant alleviation of symptoms for 15 months prior to treatment resistance from this modality. Bilateral deep brain stimulation of the globus pallidus internus (GPi) was successfully trialled and implanted. Significant alleviation of symptoms was noted for the first 5 years, but over the next 6 months thereafter, despite a combined botulinum injection and increase in DBS output, a reduction in treatment effect was experienced over time. The internal pulse generator was replaced and his symptoms markedly improved again. Conclusions: The treatment of spasmodic torticollis has been mostly described as beneficial for patients with longterm stimulation. However, the development of treatment resistance to both spinal cord stimulation and deep brain stimulation of the GPi in the same individual, to our knowledge, is the first to be described.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 193
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 36 Transaxillary Subpectoral Implantation of Implantable Pulse Generator for Deep Brain Stimulation Byung-chul Son, MD, PhD, St. Vincent's Hospital, The Catholic University of Korea, Suwon, Gyeonggi-do, Korea, Republic of; Yoon-suk Choi, MD, Suwon, Gyeonggi-do, Korea, Republic of; Sang-Won Lee, MD, PhD, Suwon, Gyeonggi-do, Korea, Republic of Introduction: Deep brain stimulation (DBS) is an effective modality of treating cardinal motor symptoms of several movement disorders such as Parkinson’s disease, essential tremor, and dystonia. Although hardware-related complications of DBS have been reported, the cosmetic satisfaction and discomfort associated with infraclavicular subcutaneous implantation of the pulse generator has not been described. The authors adopted a technique of transaxillary subpectoral IPG placement and investigated the difference in the discomfort, cosmetic satisfaction, mean operation time for IPG implantation, and severity of postoperative pain between infraclavicular subcutaneous placement and transaxillary subpectoral implantation of IPG. Methods: 25 patients who underwent bilateral, infraclavicular subcutaneous IPG placement for DBS and 15 patients who had bilateral, transaxillary subpectoral IPG placement were investigated. Results: The differences in cosmetic satisfaction and discomfort between the 2 groups were significant. The cosmetic satisfaction was higher and discomfort was less in the subpectoral IPG implantation group (p = 0.002 and p = 0.000). However, more time was needed for IPG implantation and the postoperative pain was more severe after subpectoral IPG implantation (p = 0.002 and p = 0.000). There was no difference in cosmetic satisfaction according to sex (p = 0.907). There was one transient intercostobrachial nerve injury in the subpectoral IPG implantation group and two infections which needed removal of one side of the DBS hardware in the infraclavicular IPG implantation group. Conclusions: These results demonstrated that subpectoral transaxillary IPG implantation can provide better cosmetic satisfaction in patients undergoing DBS, with less discomfort and morbidity related to erosion and infection.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 194
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 157 Thalamic Deep Brain Stiulation In Elderly Tremor Patients JiHee Kim, MD, Yonsei University College of Medicine, Seoul, Korea, Republic of; Young Cheol Na, MD, Seoul, Korea, Republic of; Won Hee Lee, MD, Seoul, Korea, Republic of; Eun Jeong Kweon, Seoul, Korea, Republic of; Won Seok Chang, MD, Seoul, Korea, Republic of; Hyun Ho Jung, MD, Seoul, Korea, Republic of; Jin Woo Chang, MD,PhD, Seoul, Korea, Republic of Introduction: Essential tremor (ET) is one of the most common movement disorders and can be disabling and refractory to optimal medical therapy. Although it can occur at any age, ET is more common with advancing age and has been estimated to affect up to 5 of every 100 persons over 65 years of age. Thalamic deep brain stimulation (DBS) is safe and effective in controlling tremor due to ET. To assess the role of age in the results of thalamic DBS, we carried out a study of two groups of patients regarding age at time of surgery. Methods: Between February 2000 and February 2010, twenty-seven patients diagnosed with ET underwent Vim DBS. The patients were divided into two groups for analyzing effects of age on outcome: Group I included twenty-one patients aged up to 70 and group II included six patients aged 70 or above. Improvement in tremor was graded as follows: Excellent, near improvement; good, more than 90% improvement; fair, more than 50% improvement. Results: Thirty-six DBS leads were implanted in these twenty-seven patients. Four patients were operated in the right hemisphere, thirteen in the left and ten bilaterally. Mean age at surgery was 59.6 years (range 33-79). The patients were followed for a mean time of 46.26 months (range 3-113 months). Of twenty-one patients in group I, six patients (28.6%) improved to excellent, thirteen patients (61.9%) improved to good, and three patients (14.3%) exhibited fair. Of six patients in group II, four patients (66.6%) improved to excellent and two patients (33.3%) improved to good. Conclusions: Thalamic DBS is clinically as effective in elderly patients as it is in younger ones. However, a more careful selection and follow-up of the elderly patients are required because elderly patients have a higher risk of surgery-related complications and a higher morbidity rate.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 195
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 154 Effects Of Subthalamic Nucleus Stimulation To Dynamic Postural Control In Parkinson’S Disease Yoshinori Higuchi, MD, PhD, Chiba University Graduate School of Medicine, Chiba, Japan; Osamu Nagano, MD, PhD, Chiba, Japan; Yumi Asano, MD, PhD, Chiba, Japan; Tatsuya Yamamoto, MD, PhD, Chiba, Japan; Tomoyuki Uchiyama, MD, PhD, Shimotsuga, Japan; Naokatsu Saeki, MD, PhD, Chiba, Japan; Ichiro Shimoyama, MD, PhD, Chiba, Japan Introduction: Postural stability is a crucial issue for patients’ activity and safety in their daily life. Subthalamic deep brain stimulation is a surgical intervention for advanced Parkinson’s disease with motor fluctuation and disabling dyskinesia. We assess the effects of subthalamic deep brain stimulation and medication on dynamic postural control of Parkinson’s disease using our measurement system. Methods: We included 14 patients with Parkinson’s disease were participated in this study. Mean age was 66 years old (56-76). Disease duration prior to surgery was 12.4 years (6-18). A force plate was used for evaluating the center of foot pressure (COP), and a wireless 3 axes accelerometer were set on the top of the head for detecting head motion. COP and head motion was recorded during repetitive alternative rotation of the head and thorax for 20 sec. We analyzed the deviation of COP and the head motion was analyzed on each medication and stimulation conditions (medication on/stimulation on; on/off; off/ on; off/off). Each data was transformed by fast Fourier transformation analysis. Total power of deviation of COP (DCOP) and peak power of head repetitive movement (PH) were analyzed. Results: Each medication/stimulation condition did not affected DCOP. However, DCOP/PH was significantly different between medication off/ stimulation off and the other conditions. Conclusions: Deviation of COP indicating fluctuation of posture stability was similar in any condition of medication/stimulation. Considering the degree of head movement, fluctuation of COP significantly increased on medication off/stimulation off. Both of stimulation and medication reduced fluctuation of COP during the head movement.
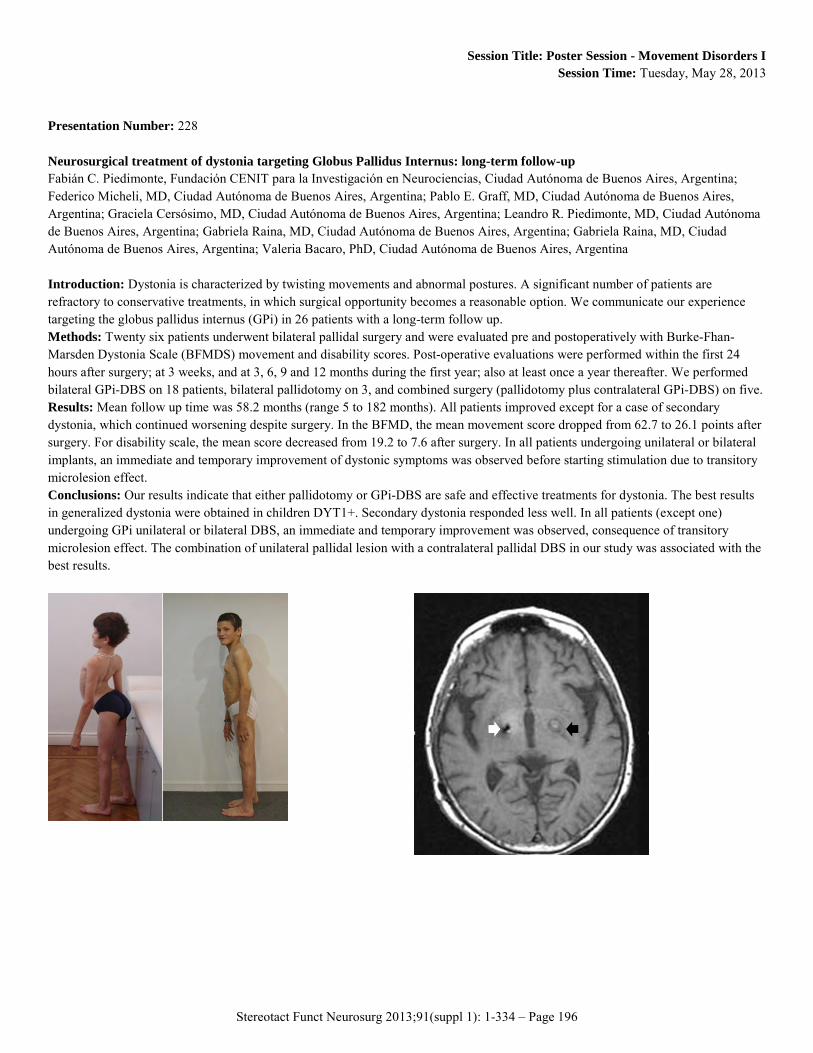
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 196
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 228 Neurosurgical treatment of dystonia targeting Globus Pallidus Internus: long-term follow-up Fabián C. Piedimonte, Fundación CENIT para la Investigación en Neurociencias, Ciudad Autónoma de Buenos Aires, Argentina; Federico Micheli, MD, Ciudad Autónoma de Buenos Aires, Argentina; Pablo E. Graff, MD, Ciudad Autónoma de Buenos Aires, Argentina; Graciela Cersósimo, MD, Ciudad Autónoma de Buenos Aires, Argentina; Leandro R. Piedimonte, MD, Ciudad Autónoma de Buenos Aires, Argentina; Gabriela Raina, MD, Ciudad Autónoma de Buenos Aires, Argentina; Gabriela Raina, MD, Ciudad Autónoma de Buenos Aires, Argentina; Valeria Bacaro, PhD, Ciudad Autónoma de Buenos Aires, Argentina Introduction: Dystonia is characterized by twisting movements and abnormal postures. A significant number of patients are refractory to conservative treatments, in which surgical opportunity becomes a reasonable option. We communicate our experience targeting the globus pallidus internus (GPi) in 26 patients with a long-term follow up. Methods: Twenty six patients underwent bilateral pallidal surgery and were evaluated pre and postoperatively with Burke-Fhan-Marsden Dystonia Scale (BFMDS) movement and disability scores. Post-operative evaluations were performed within the first 24 hours after surgery; at 3 weeks, and at 3, 6, 9 and 12 months during the first year; also at least once a year thereafter. We performed bilateral GPi-DBS on 18 patients, bilateral pallidotomy on 3, and combined surgery (pallidotomy plus contralateral GPi-DBS) on five. Results: Mean follow up time was 58.2 months (range 5 to 182 months). All patients improved except for a case of secondary dystonia, which continued worsening despite surgery. In the BFMD, the mean movement score dropped from 62.7 to 26.1 points after surgery. For disability scale, the mean score decreased from 19.2 to 7.6 after surgery. In all patients undergoing unilateral or bilateral implants, an immediate and temporary improvement of dystonic symptoms was observed before starting stimulation due to transitory microlesion effect. Conclusions: Our results indicate that either pallidotomy or GPi-DBS are safe and effective treatments for dystonia. The best results in generalized dystonia were obtained in children DYT1+. Secondary dystonia responded less well. In all patients (except one) undergoing GPi unilateral or bilateral DBS, an immediate and temporary improvement was observed, consequence of transitory microlesion effect. The combination of unilateral pallidal lesion with a contralateral pallidal DBS in our study was associated with the best results.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 197
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 209 Deep Brain Stimulation For Dystonia May Cause Body Weight Changes. Marc Wolf, M.D., Mannheim, Germany; Cristian Blahak, M.D., Mannheim, Germany; Götz Lütjens, Medical School Hanover, Hanover, Germany; Hans H. Capelle, Hanover, Germany; Michael Hennerici, Prof., Mannheim, Germany; Joachim K. Krauss, Prof., Hanover, Germany Introduction: In patients with Parkinson’s disease (PD) significant weight gain following DBS of the GPi or the subthalamic nucleus (STN) has been reported and attributed to multiple factors like the reduction of motor symptoms, changes in eating behaviour or metabolic alterations. In a recent study, severe body weight gain could be observed in some patients with primary cervical dystonia following STN-DBS, but no systematic analysis of body weight changes following pallidal or thalamic DBS in patients with dystonia has been reported so far. Methods: The body weight of 17 consecutive patients with segmental or generalized dystonia (mean age 54.6+/-16.1 years) who were treated with bilateral DBS of the GPi (n=14) or the VIM (n=3) was measured preoperatively (pre-OP) and at three follow-up (FU) time points post DBS surgery (post-OP). The median FU1 was 7 months, FU2 17 months and FU3 72 months post-OP. To evaluate outcome of DBS, the Burke-Fahn-Marsden motor (BFM) score was determined pre-OP and at all FU examinations. Results: Mean body weight pre-OP (SD) was 64.6kg (14.1kg) and increased stepwise to 68.7kg (13.1kg) at FU1, 69.9kg (13.4kg) at FU2 and 70.9kg (12.7kg) at FU3 (p<0.01 at all three FU compared to pre-OP). Relative body weight gain in percent at FU3 was correlated with the body mass index (BMI) at baseline (r=-0.53; p=0.035) and, for trend, with the BFM motor score at baseline (r=0.45; p=0.072), but not with improvement of BFM motor score at FU3, age, and disease duration at DBS. Conclusion: Chronic bilateral DBS in patients with segmental or generalized dystonia is associated with significant body weight gain, in particular during the first six months post-OP. This probably is a result of improvement of dystonic involuntary movements and changes of eating behaviour, possibly related to reduced orofacial dyskinesias.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 198
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 130 Pallidal Deep Brain Stimulation In Patients With Segmental And Cervical Dystonia Who Had Previous Radiofrequency Lesions Götz Lütjens, Medical School Hanover, Hanover, Germany; Hans Capelle, M.D, Hanover, Germany; Joachim K. Krauss, Prof., Hanover, Germany Introduction: In the past both pallidotomy and thalamotomy were used for treatment of dystonia. Little is known about the outcome of bilateral pallidal DBS in patients who underwent radiofrequency lesioning previously. Methods: We implanted DBS electrodes (3387) bilaterally in the posteroventral lateral globus pallidus internus (Gpi) and in the thalamic nucleus ventralis intermedius (Vim) in the first patient with segmental dystonia who previously underwent repeated bilateral pallidotomy. In the second patient with cervical dystonia who underwent unilateral thalamotomy previously DBS electrodes were bilaterally implanted in the Gpi. Stimulation parameters were chosen according to achieve the best improvement including bipolar and monopolar settings. Results: Follow-up time of the first patient was 52 months. The patient had a marked improvement of symptoms. The BfM score improved from 53 preoperatively to 9.5, and the disability scale improved from 13 to 4 during the follow-up. Follow-up time in the second patients was 13 months. Improvement was less pronounced, i. e. TWSTR-Scale A improved from 10 preoperatively to 7 and TWSTR-Scale B improved from 6 to 3 during follow-up. Conclusions: The results which were achieved in our patients indicate that Gpi DBS can yield substantial benefit in patients who had radiofrequency lesions earlier on.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 199
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 274 Pallidal Deep Brain Stimulation for Cervical Dystonia: Effect of Active Contact Location on Clinical Efficacy Harith Akram, MBChB FRCS (Neuro.Surg), The National Hospital for Neurology and Neurosurgery, Queen Square, London, United Kingdom; Anna Sadnicka, London, United Kingdom; Tom Foltynie, London, United Kingdom; Patricia Limousin, London, United Kingdom; Diane Ruge, London, United Kingdom; Marwan Hariz, PhD, London, United Kingdom; Ludvic Zrinzo, FRCS (Neuro.Surg), PhD, London, United Kingdom Introduction: The efficacy of GPi-DBS in primary generalized dystonia is significantly better when active contacts are located in the most posteroventral part of the GPi.(1) We aim to explore whether this is also the case in patients with cervical dystonia (CD). Methods: Ten consecutive patients (5M, mean age 56 years) with CD received bilateral GPi-DBS. They were assessed using the Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) before and 6-12m after surgery. The anatomical location of the active contacts were determined from the postoperative stereotactic MRI as previously described.(1) Results: Patients demonstrated a 60.8% mean improvement on the TWSTRS, and reported a subjective mean improvement of 79.2%. Four patients had a 100% improvement on the disability subsection of the TWSTRS. Seventeen out of 20 active contacts were in the posteroventral GPi. One contact was in the emergence of the Ansa Lenticularis and 2 in the mid segment of the GPi in the coronal plane. In the axial plane the contacts fell on average 76.2% posteriorly along the long axis of the GPi (Range 68%-86.6%). 16 were in the GPi pars lateralis (PME); 2 were in the accessory lamina, 1 in the GPi pars medialis (PMI) and 1 in the Ansa Lenticularis. There was a trend for patients with the highest objective improvement to have active contacts located more posteriorly and in the PME. Conclusions: GPi-DBS for CD is effective with contacts location in the posteroventral area, corresponding to the posterior third of the GPi. This mimics the position of most active contacts in patients who had DBS for primary generalised dystonia (1) 1. Tisch, S. et al. J Neurol Neurosurg Psychiatr 78, 1314-1319 (2007).

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 200
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 124 Intrathecal Baclofen Therapy For Spasticity And Secondary Dystonia Takuya Uchiyama, Kinki University Faculty of Medicine, Osaka, Japan Introduction: ITB therapy has garnered attention as a non-destructive, reversible, and programmable treatment method that induces neuromodulation. We report the surgical methods and therapeutic outcomes of 22 spastic and dystonic patients who underwent ITB therapy in our hospital, together with an investigation of the effects on metabolic and respiratory functions. Methods: Subjects comprised 22 patients who exhibited improvement in spasticity among 26 patients with hemiplegia, paraplegia, or tetraplegia presenting with severe spasticity and who underwent the baclofen screening test. Patients comprised 19 cases with spasticity and 3 cases with secondary generalized dystonia. The effect of ITB therapy was evaluated using the Ashworth scale. And also respiratory gas analyzer was used to measure resting metabolic rate before and 1 month after the procedure in the most recent 10 patients. Effects on respiratory function were also measured and evaluated in the same 10 patients using polysomnography before and 1 month after the procedure. Results: Lower limb spasticity improved markedly in all patients following ITB therapy. Catheter placement at the cervical level was effective for patients with upper limb and trunk spasticity and generalized dystonia. Some patients showed marked reductions in resting metabolism following ITB therapy, and this correlated with the degree of improvement in spasticity. Sleep apnea thus improved or remained unchanged in all cases, and did not worsen in any patient Conclusion: ITB therapy was effective for diffuse spasticity and secondary generalized dystonia. In addition, resting metabolism may be an indicator of treatment effectiveness. ITB therapy is non-destructive, versatile, and programmable, and may be further expected to serve as a neuromodulation treatment in neurosurgery.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 201
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 271 Proposal of International multi-center clinical trial with DBS Electrode Localization Analysis System (DELAS) Sun Ha Paek, Seoul National University Hospital, Seoul, Korea, Republic of; Jae Ha Hwang, Seoul, Korea, Republic of; Jin Wook Kim, Seoul, Korea, Republic of; Young Eun Kim, Seoul, Korea, Republic of; Han-Joon Kim, Seoul, Korea, Republic of; Yong Hoon Lim, Seoul, Korea, Republic of; Mi-Ryoung Kim, Seoul, Korea, Republic of; Cheolyoung Kim, Seoul, Korea, Republic of; Dong Gyu Kim, Seoul, Korea, Republic of; Beom Seok Jeon, Seoul, Korea, Republic of Introduction: The subthalamic nucleus (STN) stimulation has become the preferred treatment for the patients with advanced Parkinson’s disease (PD) who have intolerable drug-induced side effects or motor complications following the long-term use of dopaminergic drugs. The precise positioning of the electrodes into the STN is important for the good clinical outcome after surgery. Many approaches including image fusion of CT-MRI, MRI-MRI, and MRI-brain atlas as well as intraoperative microelectrode recording and stimulation have been practiced for the precise targeting of electrodes. However, not all the patients have their electrodes positioned exactly in the STN after surgery. Therefore clinical outcome may differ according to the electrode positions. Many unexpected factors such as possible brain shift due to CSF leakage, electrode artifacts in the MRI, error in the manipulation of the instruments, and possible migration of electrodes due to gravity after surgery make it difficult to precisely localize the center of the electrodes at a short-term period after surgery. Moreover little has been known in the literature on the issue of correlation between the clinical outcome and the electrode position after STN DBS. During the past seven years we have systematically approached on the analysis of clinical outcome in terms of the electrode position after STN DBS. Conclusions: I would like to briefly sketch out the result of our experience on these issues with the introduction of our DBS Electrode Localization Analysis System (DELAS), an on-line internet service in the web to estimate the location of the electrodes following STN DBS. I would like to propose the international multi-center clinical trial regarding the fusion-image-based programming as well as the reprogramming of the stimulator parameters using the visual information of the location of the electrode for the advanced PD patients treated with STN DBS.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 202
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 262 The Use of Propofol and Fentanyl in STN DBS for Patients with Advanced Parkinson’s Disease Jae Ha Hwang, Seoul National University Hospital, Seoul, Korea, Republic of; In Ho Song, Osong, Korea, Republic of; Yong Hoon Lim, Seoul, Korea, Republic of; Mi-Ryoung Kim, Seoul, Korea, Republic of; Young Eun Kim, Seoul, Korea, Republic of; In Keyoung Kim, Seoul, Korea, Republic of; Sang Woo Song, Seoul, Korea, Republic of; Jin Wook Kim, Seoul, Korea, Republic of; Han-Joon Kim, Seoul, Korea, Republic of; Cheolyoung Kim, Seoul, Korea, Republic of; Hee Chan Kim, Seoul, Korea, Republic of; In Young Kim, Seoul, Korea, Republic of; Dong Gyu Kim, Seoul, Korea, Republic of; Beom Seok Jeon, Seoul, Korea, Republic of; Sun Ha Paek, Seoul National University Hospital, Seoul, Korea, Republic of Introduction: Subthalamic nucleus (STN) deep brain stimulation (DBS) has become the preferred treatment for patients with advanced Parkinson’s disease (PD) and is typically performed while the patient is awake. However, anti-parkinsonian drugs must be stopped a day before surgery, which is difficult to endure for many patients. Propofol and fentanyl have occasionally been used to alleviate patients’ discomfort in these cases. We investigated the applicability of these drugs for routine administration during STN DBS. Methods: We analyzed microelectrode recordings form 8 patients with advanced Parkinson’s disease who had been treated with bilateral STN DBS. We first recorded from their left sides while awake and without anesthesia and then again from their right sides while patients were receiving continuous infusion of propofol (25 ug/kg/min) and fentanyl (25 ng/kg/min). Their microelectrode recording (MER) signals from each side were compared using mean firing rate (MFR) and discharge pattern analysis. Electrode positions were compared between both sides. Their clinical outcomes at 6 months after surgery were compared with previous reports. Results: There was no significant difference in the MFR of single unit activities between the left side MERs (38.7±16.8 spikes/sec, n=78) and right side MERs (35.5±17.2 spikes/sec, n=66). There was no significant difference in electrode positions between the right and left sides. Patents’ UPDRS total and UPDRS III scores at 6 months were comparable to previous reports. Conclusions: We suggest that continuous infusion of propofol and fentanyl can be routinely used during STN DBS surgery to alleviate the discomfort of advanced PD patients.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 203
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 156 Effects Of Relative Low-frequency Bilateral Globus Pallidus Internus Stimulation For Treatment Of Cervical Dystonia Young Cheol Na, MD, Yonsei University College of Medicine, Seoul, Korea, Republic of; Ji Hee Kim, MD, Seoul, Korea, Republic of; Won Hee Lee, MD, Seoul, Korea, Republic of; Eun Jeong Kweon, Seoul, Korea, Republic of; Won Seok Chang, MD, Seoul, Korea, Republic of; Hyun Ho Jung, MD, Seoul, Korea, Republic of; Jin Woo Chang, MD,PhD, Seoul, Korea, Republic of Introduction: To assess the effect of relative lower amplitude and frequency for globus pallidus internus (GPi) deep brain stimulation (DBS) of cervical dystonia (CD). Methods: Between February 2005 and October 2008, 14 patients diagnosed with CD underwent bilateral GPi DBS and all the patients received low-frequency stimulation and were followed for more than 2 years. We activated the implantable pulse generator 3-4 days postoperatively and initial amplitude, pulse width, and frequency were set at 1.5 V, 120 μs, and 70 Hz. The Toronto Western Spasmodic Torticolis Rating Scale (TWSTRS) was applied preoperatively and at 1, 6, 12 and 24 months postoperatively. Results: The overall TWSTRS scores improved 71.2% 2 years postoperatively (p=0.001). The mean improvement was 78.4% in severity subscores, 68.4% in disability, and 66.8% in pain scores for the 2-year follow-up period. The TWSTRS scores were significantly reduced (p<0.05), suggesting that the most significant improvement of the TWSTRS scores occurred within 1 month. The final amplitude was 2.9/2.7 V with the pulse width of 147.9/147.9 μs and the frequency of 101.1/100 Hz. Conclusions: According to our results, the initial settings of low amplitude and especially relatively low frequency are safe and effective for treatment of CD.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 204
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 89 Motor Cortex Stimulation for Freezing of Gait Mitsuhiro Ogura, MD, PhD, Wakayama Medical University, Wakayama, Japan; Hiroki Nishibayashi, MD, PhD, Wakayama, Japan; Koji Kakishita, MD, PhD, Wakayama, Japan; Naoyuki Nakao, MD, PhD, Wakayama, Japan Introduction: Freezing of gait (FOG) is commonly seen in Parkinson syndrome, including vascular Parkinsonism, pure akinesia, primary progressive freezing gait, et al. We treated three patients with levodopa-resistant gait disturbance with motor cortex stimulation (MCS), and obtained remarkable improvement of FOG in two of three cases. Methods: we underwent bilateral MCS on three patients, those who have gait disturbance as their chief symptom. Case 1 was a 67-year-old man affected by pure akinesia for seven years. The other two cases, 78 y.o. man (case 2) and 79 y.o. man (case 3), were diagnosed as primary progressive freezing gait, because of solitary feature of FOG without any clinical symptoms for three years (case 2) and five years (case3). Any medical therapy, including ledodopa, was not effective for their severe gait disturbance. Repetitive transcranial magnetic stimulation (rTMS) was applied before surgery to test if the rTMS improve the gait disturbance. Under general anesthesia, an epidural quadripolar electrode was implanted bilaterally on M1 parallel to the motor strip. Walking was evaluated by 7 meter up-and-go test before and after stimulation. Results: MCS improved FOG remarkably in two cases (case 1 and 2), who had responded well pre-operative rTMS. There was no effect of pre-operative rTMS and MCS in case 3, then the electrodes were removed. Stimulus parameter was 60-80 Hz, with 1-2 V pulses lasting 100-300 microsecond duration, anode in medial electrode and cathode in lateral one. The effect gradually decreased, but lasted more than three year (case 1) and one year (case 2). ECD-SPECT revealed that the cerebral perfusion increased in frontal lobe and basal ganglia post stimulation in all three cases. Conclusions: MCS may be an alternative therapy for a patient who has levodopa-resistant gait disturbance especially FOG. Pre-operative rTMS response would predict the effect of MCS.
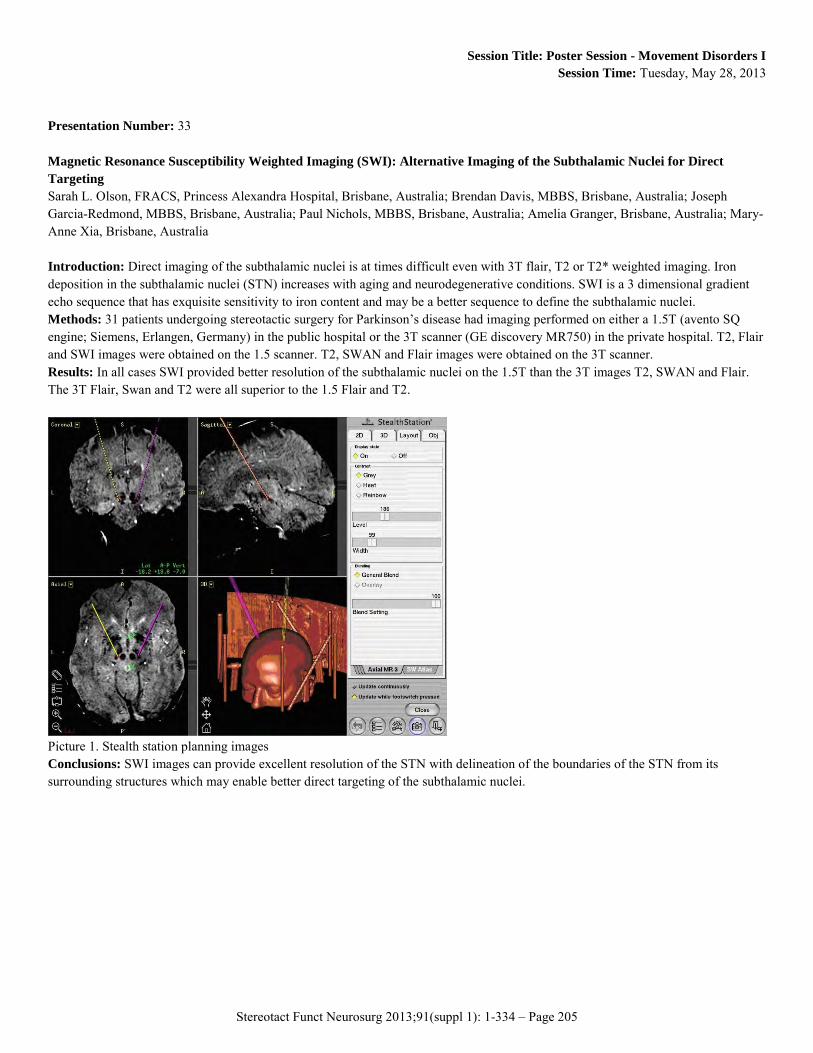
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 205
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 33 Magnetic Resonance Susceptibility Weighted Imaging (SWI): Alternative Imaging of the Subthalamic Nuclei for Direct Targeting Sarah L. Olson, FRACS, Princess Alexandra Hospital, Brisbane, Australia; Brendan Davis, MBBS, Brisbane, Australia; Joseph Garcia-Redmond, MBBS, Brisbane, Australia; Paul Nichols, MBBS, Brisbane, Australia; Amelia Granger, Brisbane, Australia; Mary-Anne Xia, Brisbane, Australia Introduction: Direct imaging of the subthalamic nuclei is at times difficult even with 3T flair, T2 or T2* weighted imaging. Iron deposition in the subthalamic nuclei (STN) increases with aging and neurodegenerative conditions. SWI is a 3 dimensional gradient echo sequence that has exquisite sensitivity to iron content and may be a better sequence to define the subthalamic nuclei. Methods: 31 patients undergoing stereotactic surgery for Parkinson’s disease had imaging performed on either a 1.5T (avento SQ engine; Siemens, Erlangen, Germany) in the public hospital or the 3T scanner (GE discovery MR750) in the private hospital. T2, Flair and SWI images were obtained on the 1.5 scanner. T2, SWAN and Flair images were obtained on the 3T scanner. Results: In all cases SWI provided better resolution of the subthalamic nuclei on the 1.5T than the 3T images T2, SWAN and Flair. The 3T Flair, Swan and T2 were all superior to the 1.5 Flair and T2.
Picture 1. Stealth station planning images Conclusions: SWI images can provide excellent resolution of the STN with delineation of the boundaries of the STN from its surrounding structures which may enable better direct targeting of the subthalamic nuclei.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 206
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 53 Deep Brain Stimulation for Multiple Sclerosis Associated Tremor: Objective and Patient Reported Outcome Measures Rasheed Zakaria, MA, The Walton Centre, Liverpool, United Kingdom; Giresh Vajramani, FRCS, Southampton, United Kingdom; Nicholas Fletcher, FRCP, Liverpool, United Kingdom; Paul Eldridge, FRCS, Liverpool, United Kingdom; Sundus Alusi, PhD, Liverpool, United Kingdom; Jibril Osman-Farah, MD, Liverpool, United Kingdom Introduction: Assess the outcomes of ventral intermediate (VIM) nucleus deep brain stimulation for the treatment of multiple sclerosis (MS) associated tremor. Methods: Sixteen patients with a mean age of 41.7 years (range 24 - 59) underwent surgery. The median duration of MS prior to surgery was 6.5 years and median duration of tremor prior to surgery was 4 years. Tremor was scored preoperatively and post operatively using Bain and/or Fahn-Tolosa-Marin systems. The Euro Qol 5D tool was used to assess quality of life before and after surgery. Results: Mean tremor reduction was 39% at 6 -12 months post operatively (range 0 - 87%). Five of 16 patients achieved at least 50% tremor reduction and 11 of 16 achieved at least 30% tremor reduction at last follow up, mean 11.6 months (range 3 - 80). Tremor was significantly reduced as rated by Bain scores (Wilcoxon matched pairs, Z=3.07, p=.002) and tended to significance as rated by Fahn scores (Wilcoxon matched pairs, Z=1.85, p=.06). Activities of daily living measures showed post operative improvement in feeding (statistically significant), hygiene, dressing, writing and working. Mean visual analogue scores (0-100) of patient reported wellbeing increased from 54.6 to 57.4 post operatively with a trend to significance (student t-test, t=1.26, p=.2). Euro-Qol 5D utility values as calculated by either the time trade off or visual analogue methodology increased following surgery with a trend to significance which was greater in the group with at least 50% tremor reduction. Conclusions: VIM DBS is an effective means of reducing disabling tremor in patients with MS. This tremor reduction tends to be associated with improved quality of life and function in those who respond. Patient reported outcome measures may not correlate with physician rated clinical outcome such as tremor scoring systems and more subtle assessment of these patients is required.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 207
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 37 Lesioning In Tremor - Is It Still Relevant? Dwarakanath Srinivas, MD, NATIONAL INSTITUTE OF MENTAL HEALTH AND NEUROSCIENCES, (NIMHANS), Bangalore, India; Pramod Pal, MD, Bangalore, India; Ravi Yadav, MD, Bangalore, India; Sampath Somanna, MD, Bangalore, India; Manish ranjan, MD, Bangalore, India; A. Arivazhagan, Bangalore, India Introduction: The introduction of DBS has heralded a sea change in the management of tremor (PD and non-PD) and dystonia and gradually supplanted Thalamotomy and Pallidotomy. Though DBS has many advantages, the cost involved puts it out of reach of a vast majority of Indian patients. In this presentation we explore the options available in such patients by presenting our experience using lesionings for tremor in a carefully selected cohort of patients. Material and Methods: A total of 15 patients underwent lesioning (14 thalamotomies, 1 subthalamotomy) for tremor of varying causes over a 4-year period at the NIMHANS, Bangalore. All underwent the lesion using the Leksell stereotactic frame using the Framelink Planning system. The lesioning was performed in the ventero-intermedius nucleus of the thalamus (Vim) under local anesthesia with detailed clinical monitoring. A detailed video presentation (pre and post op) will be done Results: There was an excellent response to the lesions with more than 90% of the tremor subsiding in all the patients. There was no mortality. 2 patients developed transient hemiparesis, which had improved to normal over a period of 3 months. One patient developed hemiballismus, which necessitated a Pallidotomy. Conclusions: Lesioning for tremor in a carefully selected cohort of patients has excellent results and is definitely a tool in the armamentarium of the functional neurosurgeon

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 208
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 406 Deep Brain Stimulation of the Subthalamic Nucleus Alters Prefrontal Activity Specific to Emotion Induction Sarah K. Bourne, BA, Vanderbilt Medical School, Nashville, TN; Bradley S. Folley, PhD, Nashville, TN; Jutta S. Mayer, PhD, Nashville, TN; Sohee Park, PhD, Nashville, TN; P David Charles, MD, Nashville, TN; Corrie R. Camalier, PhD, Nashville, TN; Srivatsan Pallavaram, PhD, Nashville, TN; Peter E. Konrad, MD, PhD, Nashville, TN; Joseph S. Neimat, MD, MS, Nashville, TN Introduction: Deep brain stimulation (DBS) of the subthalamic nucleus (STN) may alter emotional experience in patients with Parkinson’s disease (PD). STN DBS can impair ability to recognize emotions and may be associated with higher rates of depression. We previously showed that STN DBS altered prefrontal oxygenated hemoglobin concentration during an emotion induction task. In this study we investigated the effect of STN DBS on prefrontal oxygenated hemoglobin during stimuli with neutral emotional salience to determine whether STN DBS alteration of prefrontal hemodynamics is specific to emotional stimuli. Methods: PD patients with STN DBS were tested in stimulation on and off conditions. Subjects viewed a series of positive, negative, and neutral videos previously characterized for emotional qualities. Near infrared spectroscopy (NIRS) was used to monitor changes in prefrontal oxygenated hemoglobin during the task. Results: As previously reported, NIRS demonstrated STN stimulation associated decreased frontal polar oxygenated hemoglobin concentration during positive videos and decreased bilateral prefrontal oxygenated hemoglobin during negative videos. STN DBS did not have a significant effect on oxygenated hemoglobin concentration during neutral videos. Conclusions: STN DBS did not alter prefrontal activity during emotionally neutral stimuli. This suggests that the changes seen in prefrontal metabolism with STN DBS during positive and negative emotion induction are specific to emotional qualities. DBS stimulation does not appear to have a modulatory effect on frontal metabolism during emotionally neutral presentations.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 209
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 362 Does Survival Following Deep Brain Stimulation Of The Subthalamic Nucleus Depend On Patient Gender And Parkinson Disease Duration Prior To Surgery? Anwen White, Queen Elizabeth Hosptial, Birmingham, United Kingdom; Jamila Kausar, Queen Elizabeth Hospital, Birmingham, United Kingdom; Desire Ngoga, Queen Elizabeth Hospital, Birmingham, United Kingdom; Hardev Pall, Queen Elizabeth Hospital, Birmingham, United Kingdom; Rosalind Mitchell, Queen Elizabeth Hospital, Birmingham, United Kingdom Introduction: Bilateral subthalamic nucleus deep brain stimulation (STN DBS), is an effective surgical treatment for patients with advanced Parkinson’s disease, with improvements in motor function following surgery. Patients also reduce Parkinsonian medication and have improved health-related quality of life (HRQoL). Our aim was to examine patient survival following deep brain stimulation with respect to patient gender and duration of Parkinson’s disease prior to surgery. Methods: We performed a retrospective analysis on all patients offered STN DBS in our institution between January 2002 and November 2011. A comparison was made between patients whom were offered surgery but declined and those who proceeded with surgery. Excluded patients were those medically unfit for surgery and patients whom failed psychometric testing. Results: 147 patients were offered STN DBS at our institution between these dates. 106 patients (mean age 59) underwent surgery; 41 patients (mean age 61) declined surgery and proceeded with best medical management of their Parkinson’s disease. There was no significant difference in age, gender (predominance of men), ethnicity or duration of disease prior to the offer of surgery in both groups. Patients whom underwent STN DBS had a significantly longer survival than those whom did not undergo surgery (p=0.002) Females had a higher risk of mortality across both treatment groups (hazard ratio 3.03, 95% CI: 1.47-6.24, p=0.003) Patients whom had Parkinson’s disease for less than ten years prior to the offer of surgery had a improved survival (hazard ratio 2.3, 95%CI 1.0-5.2, p=0.042) Conclusion: Our study has shown that male patients have a lower mortality risk in comparison to female patients. Also, patients whom have Parkinson’s disease for greater than ten years prior to DBS have a higher mortality. Overall, patients whom underwent STN DBS had a longer survival than those treated with medicine alone.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 210
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 233 Dorsolateral Subthalamic Neuronal Activities Enhanced By Median Nerve Stimulation Facilitate Parkinson’S Disease During Deep Brain Stimulation In General Anesthesia Sheng-Tzung Tsai, MD, Tzu Chi General Hospital, Hualien, Taiwan; Wei-Yi Chung, National Chiao-Tung University, Hsinchu, Taiwan; Chung-Chih Kuo, Physiology, Tsu Chi University, Hualien, Taiwan; Shin-Yuan Chen, Tzu Chi General Hospital, Hualien, Taiwan Introduction: Deep brain stimulation (DBS) under general anaesthesia is an alternative option for Parkinson's disease (PD) patient, however, evidence of whether neuronal firing could be accurately recorded or not remains in paucity. The benefit of median nerve stimulation for localization of dorsolateral sub-territory of subthalamic nucleus (STN), which involves sensorimotor function, was explored. The aim of study is to characterize neuronal activities of dorsolateral STN and elucidate the influence of general anaesthetics and median nerve stimulation (MNS) on neurons during DBS surgery in patients. Methods: Eight PD patients were anaesthetized with desflurane and got the contralateral MNS at the wrist during microelectrode recording of STN. We analysed the spiking patterns and power spectrum density (PSD) of background activity along each penetration track and determined the spatial correlation with the target location estimated from standard neurophysiological procedures. Results: Dorsolateral STN spiking pattern showed more prominent bursting pattern without MNS and more oscillation with MNS. In terms of neural oscillation of background activity, beta band oscillation dominated within sensorimotor STN and showed significantly more PSD during MNS (p < 0.05). Conclusions: Neuronal firing within STN could be accurately identified and differentiated when PD patients received general anaesthetics. MNS can enhance the neural activities in beta-band oscillation, an index to ensure optimal electrode location via successfully tracked dorsolateral STN topography.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 211
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 327 Changes And Differences Of The Tremor Network In Tremor And Non-tremor Dominant Parkinson’s Disease Patients Revealed By Probabilistic Tractography David Kis, MD, University of Szeged, Department of Neurosurgery, Szeged, Hungary; Adrienn Máté, Szeged, Hungary; Tamas Kincses, MD, PhD, Szeged, Hungary; Péter Klivényi, MD, PhD, Szeged, Hungary; Pál Barzó, MD, PhD, DsC, Szeged, Hungary Introduction: Probabilistic tractography is a non-invasive method which is able to determine the probability of the projection of specific tracts, furthermore to segment cortical/subcortical brain regions by their cortical/subcortical connections. It has been proven that this method can be used to examine the basal ganglia’s connectivity in healthy subjects. Methods: Our aim was to examine if there is a demonstrable difference in the tremor network between two clinically different subgroups of Parkinson’s disease patients: 1, tremor-dominant; 2, non tremor-dominant. 8 patients were involved in the study: 3 had no tremor, 3 had bilateral minor tremor, 2 had prominent left-sided tremor. Diffusion tensor imaging, T1, T2 and susceptibility weighted imaging scans were acquired. We performed probabilistic tractography and connectivity based segmentation of the STN, 7 cortical masks (prefrontal, premotor, primary motor and sensory, dorsal parietal, temporal and occipital regions) and the thalamus. Results: Our results showed a prominent difference in the STN-thalamus connections between the two groups. In group 2 there was no remarkable difference between the left and right side but the probability of connection was very low (0-3%) in 5 patients and high (30-60%) in 1 patient. In group 1 the probability of connection was high (5-50%) ipsilateral to the tremor, but low (1-6%) on the contralateral side in both patients. The STN showed connections mainly to the motor and premotor area, the cerebellum and the ventralis oralis posterior nucleus of the thalamus. Conclusions: According to our results a structural difference appears during the development of tremor and non-tremor dominant Parkinson’s disease which is identifiable by probabilistic tractography. This method can be used for further examinations to clarify the underlying mechanism of the clinically different subgroups. It could be very helpful to find new therapeutic ways in the future.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 212
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 51 Neuroprotective Effects Of Ropinirole On 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine induced Parkinson's Animal Models Chul Bum Cho, Saint Mary's Hospital, Hallym University Sacred Heart hospital, Seoul, Korea, Republic of Introduction: Parkinson's disease (PD) is a neurodegenerative disorder, characterized by the selective loss of dopamninergic neurons in the substantia nigra pars compacta (SNpc). The effects of ropinirole, a nonergoline dopamine receptor agonist with a high affinity for dopamine D2 receptors, on Parkinsonism induced by 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP, 20mg/kg with 2h intervals, 4 times), were examined in behavioral test. Furthermore, the numbers of tyrosine hydroxylase (TH) immunostained cell were counted in the substantia nigra. Methods: The aim of the present study was to investigate the effects of ropinirole on MPTP-induced behavioral alteration and dopaminergic neuronal cell death in the substantia nigra. In this study, we confirmed the anti-Parkinsinian activity of ropinirole using MPTP-treated mice. We now investigate effect of oral administration with ropinirole on MPTP-lesioned mice on behavioral test and neuroprotective effects. Results: The behavioral results showed that treatment ropinirole (5×1mg/kg with interval 24h, 5 times) could improve the PD mice markedly. In addition, administration of ropinirole provides neuroprotection against the loss of dopaminergic neurons and behavioral impairment caused by MPTP. These results support the in vivo protection of ropinirole against MPTP and suggest that ropinirole treatment might represent a neuroprotective treatment of PD. Conclusions: In conclusion, the present study suggested that ropinirole could reverse MPTP-induced behavioral alteration and protective nigral neurons. Further studies will be carried out to evaluate ropinirole could benefit as a future preventive and therapeutic drug of PD.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 213
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 46 Atlas-base Coordinates Of Targets For Stereotactic Bilateral Neural Transplantation William O. Contreras Lopez, md, University Freiburg Medical Center, Freiburg im Breisgau, Germany; Michael Trippel, MD, Freiburg im Breisgau, Germany Introduction: The aim of this work is to provide an atlas-based coordinates method for identification of the six targets that are to be used in the planning of the neural transplantation treatment. Methods: <br /(a) analyse the feasibility and safety of the stereotactic surgical procedure in our center and (b) provide an original systematic Atlas-based targets coordinates method that can be adapted and used for HFST. The atlas allows identification of the six targets, and can be used in the planning of the transplantation treatment. The coordinates of putamen and caudate nucleus were identified in Three-Tesla Magnetic Resonance imaging and transformed into mid-commissural point (MCP) coordinates. From these data an electronic coordinate atlas was built up. For the second contra-lateral transplantation in the same patient, the coordinates were mirrored in order to determine contralateral targets and tracts. 22 patients with genetically confirmed HD underwent bilateral stereotactic human fetal striatal transplantation (HFST).Two caudate nucleus tracks were performed in all the 22 patients bilaterally; pre-commissural putamen tracks were performed in number of two bilaterally in 21 patients, with one patient that due to atrophy and vessel presence in the middle of the trajectory. One patient received 2 pre-commissural tracks on the right hemisphere and one on the left. 18 patients received two post-commissural tracks bilaterally; three patients received only one. Two of these were right and one left. One patient, (due to atrophy) received only one post-commissural track bilaterally. Conclusion: Stereotactic HFST is a safe, well tolerated stereotactic procedure in the treatment of Huntington’s disease. Atlas-based coordinates may shorten planning time for surgery. Tracts have to be adapted individually for anatomical differences, according to disease related brain atrophy, for the presence of blood vessels especially by selecting the best possible entry point. The analysis shows no complications.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 214
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 38 Simultaneous Bilateral Pallidotomy as a rescue procedure in Dystonic crisis secondary to PKAN in pediatric patients. Dwarakanath Srinivas, NATIONAL INSTITUTE OF MENTAL HEALTH AND NEUROSCIENCES, (NIMHANS), Bangalore, India; Pramod Pal, MD, Bangalore, India; Ravi Yadav, Bangalore, India Introduction: Pantothenate kinase-associated neurodegeneration (PKAN), formerly Hallerworden-Spatz syndrome (HSS) is a rare, autosomal, recessive neurodegenerative disorder with iron accumulation in the brain as a prominent finding. Dystonia is the predominant clinical finding with severe dystonic crisis occurring occasionally at presentation. We present our experience in four pediatric patients with HSS who presented with severe life threatening dystonic crisis and could not afford Deep Brain stimulation. Material and Methods: A total of 4 patients underwent surgery bilateral simultaneous pallidotomy for life threatening dystonic crisis secondary to HSS over a 4-year period at the NIMHANS, Bangalore. All underwent the lesioning using the Leksell stereotactic frame using the Framelink Planning system. The lesioning was performed in Globus pallidus internus under general anesthesia. A detailed video presentation (pre and post op) will be done Results: There was a good to satisfactory response to the lesions with significant improvement in the UDRS and FHM scores. There was no mortality. 2 patients developed transient dysphagia and dysarthria, which had improved to normal over a period of 3 months. Conclusions: Simultaneous Bilateral Pallidotomy as a rescue procedure in Dystonic crisis can be performed with satisfactory results in patients who cannot afford Deep brain stimulation
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 215
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 79 The Prevention of Post-operative Hallucination and Delusion after STN-DBS Surgery by Avoidance of SNr Injury. Kenji Sugiyama, MD, PhD, Hamamatsu University School of Medicine, Hamamatsu, Japan; Takao Naozaki, MD, Hamamatsu, Japan; Tetsuya Asakawa, PhD, Hamamatsu, Japan; Hiroki Namba, MD, PhD, Hamamatsu, Japan Introduction: STN-DBS has been world widely used for intractable Parkinson disease to alleviate all of its motor symptoms. However, some psychiatric complications, hallucination and delusion, have been reported immediately after STN-DBS surgery. Acute hallucination and delusion complications develop among or immediately after the surgery. We experienced 6 such cases in our 134 STN-DBS series. The etiology of these complications is still unclear, but there has been one literature, which indicated that hallucination and delusion can occur by disinhibition of thalamic VA nucleus caused by the SNr injury. In this paper we examined the feasibility of this hypothesis to prevent acute hallucination and delusion complications after STN-DBS by avoidance of SNr injury with electrode penetration. Methods: We examined the incidence rate of hallucination and delusion complications within two weeks after our consecutive STN-DBS surgery. From 1998 to 2003 in 61 surgeries, we inserted the searching semi-microelectrodes within the SNr through STN and sometimes set the tip of chronic stimulating electrodes into the SNr. From 2004 to 2012 in 73 surgeries we avoided to electrode penetration into the SNr by close observation of the unit recordings. We also took extreme care not to injure the SNr by positioning of the chronic stimulating electrodes. Results: From 1998 to 2003 we experienced 6 cases of hallucination and delusion complications among 61 STN-DBS surgeries. The incidence rate was 9.83 %. After 2004 we experienced none of these cases after changing the operation procedure to avoid SNr injury. There is strong statistically significant difference between two groups. Conclusions: It is possible to prevent acute hallucination and delusion complications after STN-DBS surgery by avoidance of the SNr injury with searching or chronic stimulating electrodes.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 216
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 92 Combination of GPi and Voa stimulation for Neuroacanthosis. Naoki Nakano, MD,PhD, Kinki. University, Osaka-sayama, Japan; Hiromasa Yoshioka, MD, Osaka-sayama, Japan; Saori Murakami, MD, Osaka-sayama, Japan; Takayuki Tasaki, MD, Osaka-sayama, Japan; Kinya Nakanishi, MD,PhD, Osaka-sayama, Japan; Takuya Uchiyama, MD,PhD, Osaka-sayama, Japan; Amami Kato, MD,PhD, Osaka-sayama, Japan Neuroacanthocytosis (NA) is the presence of severe involuntary movement disorders including chorea, dystonia and trunck spasms. Recent medicine is not effective, then the few reports result that deep brain stimulation (DBS) have been treated the patients with NA. However optimal DBS target is not yet clearly, some authors reported the successful improvement of NA with the internal globus pallidum (GPi) stimulation. While, other authors described that the trunk spasm is ameliorated by the thalamic (Voa) stimulation. We report two cases of NA treated by the combination of GPi stimulation and Voa stimulation. Patient 1 was 43-year-old man who developed trunk spasm at 35-year-old, followed by involuntary movement of tongue and extremities. Severe involuntary movement of tongue and lip biting could not take some foods orally, then he was placed percutaneous endoscopic gastromy for daily nutrition. He was placed DBS electrode at bilateral GPi and Voa for test stimulation. The several involuntary movements were improved by GPi and Voa stimulation during test stimulation. DBS system was placed at bilateral anterior chest and bilateral abdomen subcutaneously. The involuntary movement of tongue and sudden falling of body were improved with GPi stimulation. Trunk spasm and head shaking were improved with Vo stimulation. Patient 2 was 40-year-old man who developed trunk spasm at 35-year-old, followed by involuntary movement of extremities. The violent movement of upper extremity led the injury of eyeball unfortunately. He underwent placement of a DBS electrode in the bilateral GPi and Voa such as the patient 1. Trunk spasm, head shaking and violent movement of upper extremities were improved with Vo stimulation. Sudden falling of body was gradually improved with GPi stimulation. Bilateral DBS to the combination of GPi and Voa can improve several involuntary movements in two patients with NA.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 217
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 45 Surgical Neuromodulation For Nbia- Related Dystonia. Tomasz Mandat, MD PhD, COI, Warsaw, Poland; Henryk Koziara, Warsaw, Poland; Wieslaw Bonicki, Warsaw, Poland; Pawel Nauman, Warsaw, Poland; Tomasz Kmiec, Warsaw, Poland Introduction: Treatment of symptoms related to Neurodegeneration with Brain Iron Accumulation (NBIA) is difficult and frequently ineffective. The authors present a group of patients treated with deep brain stimulation for dystonia in NBIA. Materials and Methods: 12 patients with confirmed PANK2 mutation (NBIA-PKAN) were treated with deep brain stimulation in 2008 and 2012. Age of the patients varied from 7-27 years. The clinical condition of the patients was Global Dystonia Scale (GDS). At all cases the permanent electrodes were implanted to the subthalamic nuclei. The target was identified with direct and indirect method. Intrasurgical macrostimulation and microrecording were used for neurophysiological evaluation of the target. Postsurgical local field potentials were recorded in all cases. Results: Neither neurological deterioration nor surgical complication were reported among the group. Caregivers of the patients noted subjective improvement of the clinical state of the subjects that was confirmed with tailored scales. Conclusions: Subthalamic deep brain stimulation reduces dystonic movements among NBIA patients. The technique carries minimal surgical risk, and improves quality of life of the patients.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 218
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 414 Pronation/Supination for Objective Assessment of Bradykinesia Lauren Kumbier, Madison, WI; Mridu Sinha, Madison, WI; Alekhya Perugupalli, Madison, WI; Gurwattan S. Miranpuri, University of Wisconsin, Madison, WI; Karl Sillay, University of Wisconsin, Madison, WI Objective: We developed a system to analyze pronation/supination movement in patients with Parkinson’s disease (PD) using a gyroscope. The system can be conveniently deployed through an iPhone/iPod or any other smartphone device with similar dimensional and weight characteristics which has an inbuilt gyroscope. Methods: A smart phone application was developed to administer motor subsection 3.6 (pronation/supination) of the Unified PD Rating Scale (UPDRS) diagnostic test. The application acquired movement data for pronation/supination through the inbuilt gyroscope of the smartphone. Eight patients with and without deep brain stimulation (DBS) completed the clinical trial with the iPod strapped on to their forearms. Sessions were videotaped and presented for UPDRS rating. UPDRS sub-scores with and without the device were compared. Pronation/supination was analyzed for amplitude, frequency, angular velocity, and hesitations. Correlation of these parameters with the UPDRS sub-score was examined to identify the metrics that can be used to assess Bradykinesia severity. These quantitative measures will be used to assign ratings that represent the severity of PD. Results: Among the parameters analyzed, decrease in amplitude with respect to UPDRS 0 group and angular velocity showed significant correlation with UPDRS motor subsection 3.6 sub-scores ( amplitude: r= -0.7363, p <.01 ; angular velocity: r= -0.6184, p<.01 ). Frequency showed little correlation with r= 0.4733 p= 0.0473. Also, ratings with and without device matched in 80.3% cases. The blinded observer rated the UPDRS sub-score lower in two cases and higher in one case. Conclusion: This method can be used to assess the usefulness of DBS and other treatments for PD care. Confounders during the development of objective measures include the known interrater and intrarater variance of the UPDRS reference metric. Objective measures stand to reduce the number of patients required to complete clinical trials and move therapies from concept to applied treatment.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 219
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 328 Localization Of The Active Contacts And Beta Oscillations In The Subthalamic Nucleus Of Parkinsonian Patients David Garcia-Garcia, Universidad de Navarra. CIMA. CIBERNED, Pamplona, Spain; Jorge Guridi, MD, PhD, Clinica Universitaria de Navarra, Pamplona, Spain; Jon Lopez-Azcarate, PhD, Pamplona, Spain; Jon Toledo, MD, Pamplona, Spain; Manuel Alegre, MD, PhD, Pamplona, Spain; Jose A. Obeso, MD, PhD, Pamplona, Spain; Maria Cruz Rodriguez-Oroz, MD, PhD, San Sebastian, Spain Introduction: To study the localization of the beta activity in the subthalamic nucleus (STN) and of the contacts of the implanted electrodes for chronic stimulation providing the highest benefit (active contacts) in patients with Parkinson’s disease (PD). Methods: We recorded local field potentials in the STN through the surgically implanted electrodes in 30 PD patients during the "off" and "on" dopaminergic states. The position of the contacts of the electrodes was studied using the pre and post-operative MRI where the contacts were referenced to the midpoint of the intercommisural line. The anatomical position of each contact was obtained from a Morel’s based three-dimensional atlas for the STN (divided into functional regions) and the surrounded anatomical areas. Only electrodes programmed in monopolar where selected for the study being the catodes of these electrodes considered as the active contacts. The position of the contact of the electrode where the phase reversal of the recording of the beta activity was obtained was considered as the position where the beta band was generated. Results: All patients displayed a low beta activity (mean 15.33 Hz) in OFF and a high beta activity (mean 26.22 Hz) in OFF and ON. There were no differences between the topography of the active contacts (X: 10.86±1.62; Y: -1.01±1.92; Z: -1.63±1.44) and the position where the generators of the low and high beta activity were recorded: low beta OFF (X: 10.45±1.66; Y: -1.45±1.77; Z: -2.19±1.81); high beta OFF (X: 10.80±1.56; Y: -1.57±1.77; Z: -2.27±1.35); high beta ON (X: 10.81±1.51; Y: -1.53±1.86; Z: -2.44±1.32). Active contacts and oscillatory activity generators in the beta band were located in the rostral portion of the motor region of the STN. Conclusions: The rostral portion of the motor region of the STN is the region where DBS of the STN provides maximal antiparkinsonian benefit coinciding with the position where the beta activity is generated in the STN.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 220
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 231 Combinations of Subthalamic and Pedunculopontine nucleus-stimulation produce improvement in Saccadic Modulation in advanced Parkinson’s disease Mohammad J. Naushahi, BMedSci, MRCS, Imperial College Neuromodulation Group, London, United Kingdom; Amad N. Khan, MBBS, MSc, London, United Kingdom; Dipankar Nandi, DPhil, FRCS (SN), London, United Kingdom Introduction: Concomitant bilateral subthalamic nucleus (STN) and pedunculopontine nucleus (PPN)-stimulation has been proposed as a treatment option for advanced Parkinson’s disease (PD) patients who are not only refractory to medical therapy but also have prominent axial symptoms viz. gait disturbance and postural instability. This study explores the relative effects of bilateral STN and PPN-stimulation on both initiation and inhibition of saccades in advanced PD with a novel set of combinations, not previously reported, and with a view to gaining greater understanding of the pathophysiology of some of the axial motor symptoms of advanced PD and the possible mode of improvement with neurostimulation. Methods: Five patients with advanced PD performed two different oculomotor tasks whilst OFF-stimulation, ON bilateral STN-stimulation, ON bilateral PPN-stimulation, diagonal stimulation (unilateral STN-stimulation and contralateral PPN-stimulation) and unilateral STN and PPN-stimulation. The first task involved visually guided saccades (that are reflexive) and the second, antisaccades (that are volitional). Saccadic latency, accuracy and velocity were recorded for both the tasks, while prosaccades were measured for the antisaccade task only. Results: Bilateral STN-stimulation produced the greatest improvement in all parameters for visually guided saccades and antisaccades task as compared to OFF-stimulation (p < 0.001). The next best improvement was produced by diagonal stimulation, followed by unilateral STN and PPN-stimulation (p < 0.001). An improvement was also produced by PPN-stimulation alone, however, this was not statistically significant. Conclusions: This trend may be explained by the fact that stimulation causes improvement of saccades towards the opposite side, hence diagonal stimulation that had STN-stimulation on one side and PPN-stimulation on the other side was superior to unilateral STN and PPN-stimulation because it improves saccades for both right and left gaze, as opposed to unilateral stimulation that only improves saccades towards one side.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 221
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 260 A Subtle Change In MRI-verified Targeting Significantly Improves Long-term Speech Outcome After STN-DBS Elina Tripoliti, UCL, Institute of Neurology, London, United Kingdom; Harith Akram, London, United Kingdom; Etienne Holl, London, United Kingdom; Iciar Aviles-Olmos, London, United Kingdom; Joseph Candelario, London, United Kingdom; Jonathan Bose, London, United Kingdom; TOm Foltynie, London, United Kingdom; Patricia Limousin, London, United Kingdom; Marwan Hariz, London, United Kingdom; Ludvic Zrinzo, London, United Kingdom Introduction: Speech can be adversely affected by bilateral subthalamic nucleus deep brain stimulation (STN-DBS) with significant negative impact on quality of life. Previous work has implicated lead location in speech deterioration. As a result, our team introduced subtle changes when targeting the STN in order to minimise speech problems. Here we assess the effect of this change on speech and motor outcome. Methods: Patients were divided into two groups: patients before 2008 (group 1, N=32) and from 2008 till 2010 (group 2, N=22). Assessments were carried out at baseline and at one year, with and without medication, using a standard speech intelligibility scale and the UPDRS-III. Contact localisation was performed using pre- and post-implant stereotactic MRI as described previously. Results: At baseline, patient groups 1 and 2 did not differ in age (mean 58.8yrs), disease duration (mean 12.5yrs), UPDRS-III scores (off-medication 48.1 vs. 46.2; on-medication 12.4 vs. 16.3) or speech intelligibility (on-medication 70% vs. 78%). There was a small but clear difference in lead location between the two groups on post-implant stereotactic MRI. Electrode locations in group 1 lay more anteromedial and in group 2 more posterolateral in the STN. After one year of STN-DBS, group 1 experienced a significant deterioration in speech intelligibility (mean -15.8%, p=0.0054) but group 2 did not (mean -2.3%). UPDRS-III scores showed significant improvement in both groups after one year (UPDRS-III off-medication/ON-stimulation 23.3 vs. 27.4). Conclusion: Deterioration in speech is a late occurrence after STN-DBS and currently there is no way of reducing this by intraoperative testing. This study confirms that a subtle change in MRI-guided targeting, aiming at a more posterolateral location within the STN, can positively affect speech outcome. Speech however remains a variable and multifactorial side effect of stimulation for further investigation.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 222
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 207 The Rotenone-induced Rat Model Of Parkinson's Disease: Behavioral And Electrophysiological Features Mesbah Alam, PhD, Hannover Medical School, Hannover, Germany; Christof von Wrangel, Hannover, Germany; Kerstin Schwabe, PhD, Hannover, Germany; Joachim Kurt Krauss, MD,PhD, Hannover, Germany Introduction: The 6-hydroxydopamine (6-OHDA) Parkinson (PD) rat model is based on specific dopamine depletion in the nigrostriatal pathway, which leads to hyperactivity of the subthalamic nucleus (STN). Chronic rotenone injections similarly lead to loss of dopaminergic neurons in the nigrostriatal pathway but in addition also to loss of cholinergic neurons in the pedunculopontine nucleus (PPN), which has been thought to underly certain components of parkinsonian gait. We here evaluated the motor disability and the extra cellular neuronal firing activity of the STN in the rotenone rat model of PD. Methods: Male Sprague Dawley rats were treated with chronic rotenone injections (2.5 mg / kg bodyweight, i.p.) for 60 days. Control rats received vehicle injections. After the end of the treatment motor coordination was assessed by using the Rotarod test. Thereafter, single unit activities and local field potentials were recorded in the STN in urethane 1.2 g/kg anesthetized rats. Results: Rotenone injected rats spent significantly less time on the Rotarod as compared to vehicle treated rats. Further, electrophysiological data showed a higher firing rate and higher beta oscillatory activity in the STN. Conclusions: Similar as in 6-OHDA injection we found enhanced STN neuronal firing rates as well as increased beta oscillatory activity, key features of PD, in this model. The rotenone-induced rat model of PD should deserve further attention since it covers more aspects than just the dopamine depletion.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 223
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 403 Neurosurgical Treatment of X-linked Dystonia Parkinsonism Jose A. Aguilar, M.D., Philippine Movement Disorder Surgery Center, San Juan City, Philippines Introduction: X-Linked Dystonia Parkinsonism (DYT3, “Lubag”) is a progressive debilitating neurodegenerative disease affecting Filipino males with origins from Panay island, Philippines. We reviewed all the Philippine XDP patients who had undergone ablative neurosurgical procedures in the past as well as our recent pallidal DBS surgery case series. Methods: A retrospective review of XDP patients from the Philippine XDP registry was done to analyse the results of neurosurgical ablative treatments from 1960 to 1982, and bilateral pallidal Deep Brain Stimulation (DBS) surgeries from 2009 to 2012. The outcomes of the patients who had undergone staged bilateral pallidotomies or thalamotomies were reviewed for signs of clinical improvement and presence of postoperative morbidities. For the bilateral pallidal DBS, the preoperative and postoperative Burke-Marsden-Fahn Dystonia Scale scores and Unified Parkinson’s Disease Rating Scale Part III scores as well as the standardized video recordings were evaluated. Results: Data from the Philippine XDP registry showed that from 1960 to 1982, six patients underwent staged bilateral brain lesioning procedures (chemopallidotomies or thalamotomies). Half of the patients showed improvement after surgery but a significant number (83%) also developed postoperative morbidities, mainly speech impairment or hemiparesis. Starting 2009, we have treated four XDP patients with bilateral globus pallidus interna DBS surgeries. All four DBS patients showed immediate improvement of their Burke-Marsden-Fahn Dystonia Scale scores (mean = 67%, range = 56% to 83% improvement) and dramatic relief of their dystonic symptoms with no evident adverse effects. The follow-up period ranged from 2.5 months to 3 years. The beneficial effect of bilateral pallidal stimulation persists and had lasted up to 3 years in our longest follow-up period. Conclusion: Bilateral pallidal DBS surgery is a safe and effective procedure for immediately alleviating the disabling symptoms of XDP, in contrast to bilateral neuroablative procedures which might result to significant postoperative morbidities.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 224
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 98 Cenesthopathy-like Symptom After Subthalamic Stimulation For Parkinson Disease Chikashi Fukaya, Nihon University School of Medicine, Tokyo, Japan; Kentaro Shimoda, MD,PhD, Tokyo, Japan; Mitsuru Watanabe, MD,PhD, Tokyo, Japan; Koichiro Sumi, MD,PhD, Tokyo, Japan; Toshiki Obuchi, MD,PhD, Tokyo, Japan; Kazutaka Kobayashi, MD,PhD, Tokyo, Japan; Hideki Oshima, MD,PhD, Tokyo, Japan; Takamitsu Yamamoto, MD,PhD, Tokyo, Japan; Atsuo Yoshino, MD,PhD, Tokyo, Japan; Yoichi Katayama, MD,PhD, Tokyo, Japan Introduction: We sometimes encountered patients who complain about an uncomfortable feeling in their throat or abdomen after STN-DBS. These symptoms were not associated with any organic abnormality and sometimes severely affected to the patients. In the study, we analyzed the cause and factors related to these cenesthopathy-like symptom from the preoperative state. Methods: The subjects are 18 patients who complained of body discomfort such as cenesthopathy without any organic abnormality after STN-DBS at our institute (Group A) and 64 patients who underwent STN-DBS during the same period but did not complain of body discomfort (Group B). We analyzed the difference in the preoperative state between these two groups. Results: We did not detect a significant difference in preoperative scale of Schwab & England, Hamilton Depression Scale and Mini Mental State Examination. Regarding UPDRS, there was no significant difference except for part IV (p<0.01). In addition, levodopa equivalent dose (LED) and dose of l-dopa of Group A were also significantly higher than those of Group B (LED: p<0.01), (L-dopa: p<0.05). There was no significant difference in dose of agonist between Groups A and B. Conclusion: The incidence of cenesthopathy-like symptom was considered to be mainly related to the preoperative administration of l-dopa. Originally, cenesthopathy is noted as one of the Schizophrenia symptoms or withdrawal symptoms of narcotics. The mechanism of the pathology of Schizophrenia is sometimes explained on the basis of the hyperdopaminergic theory. The main action of narcotics is upregulation of dopaminergic emission in synaptic gap junctions. From these facts, we can postulate that the cenesthopathy-like symptoms may be associated with dopa dysregulation. Conclusion: High-dose administration of l-dopa is relevant to cenesthopathy-like symptom after STN-DBS for PD. Cenesthopathy might be a withdrawal symptom of l-dopa which can be related to dopa dysregulation.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 225
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 258 Prevention of Hemorrhagic Complication by Avoiding the Medullary Veins in Deep Brain Stimulation Surgery Makoto Dehara, Rinku General Medical Center, Izumisanoshi, Osaka, Japan; Takao Soda, Izumisanoshi, Osaka, Japan; Kimito Yamada, Izumisanoshi, Osaka, Japan; Yoshifumi Teramoto, Izumisanoshi, Osaka, Japan; Takeshi Shimizu, Izumisanoshi, Osaka, Japan; Shusuke Moriuchi, Izumisanoshi, Osaka, Japan Introduction: Several reports have revealed that the white matter around the lead of stimulating electrodes starts to swell after surgery and bleeds thereafter, although the cortical veins, sulci, and lateral ventricle wall are avoided during deep brain stimulation surgery (DBS). A possible reason for this bleeding may be injury to the medullary veins, which connect the ventricle and cortex. In certain cases, during the planning stage, the medullary veins are difficult to identify even on contrast-enhanced T1- or T2-weighted images. However, the medullary veins can be identified on images obtained by susceptibility-weighted imaging (SWI) or by applying 3D-time of flight spoiled gradient-recalled acquisition in the steady state (3D-TOF SPGR) method. Methods: To examine the effects of preoperative MRI used for visualizing the medullary veins, we used the images obtained by the 3D-TOF SPGR method for preoperative planning in four cases requiring subthalamic nucleus (STN)-DBS. As reported by us previously, in these four cases, we also adopted the Bone Wax Technique (BWT), which can eliminate subdural air invasion and CSF leakage. Results: We could change the trajectory to avoid the medullary veins in two cases by using images obtained by the 3D-TOF SPGR method. We performed STN-DBS by BWT without hemorrhagic complication in all the four cases. Conclusion: The images obtained by the 3D-TOF SPGR method can be useful for planning a trajectory that avoids the medullary veins. Furthermore, the trajectory avoiding the medullary veins may be helpful in reducing complications such as parenchymal hemorrhage. BWT may be effective in performing DBS avoiding the medullary veins.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 226
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 212 Medical Students` Knowledge About Deep Brain Stimulation Götz Lütjens, M.D., Medical School Hanover, Hanover, Germany; Andreas Wloch, Hanover, Germany; Hans Heissler, Hanover, Germany; Hans H. Capelle, M.D., Hanover, Germany; Christoph Schrader, M.D., Hanover, Germany; Joachim K. Krauss, Prof., Hanover, Germany Introduction: DBS is a well-established therapy for movement disorders such as dystonia, Parkinson´s disease (PD) and tremor and it is currently under investigation as a therapeutic option in neuropsychiatric disorders. Little is known about medical students´ knowledge about this powerful tool when they enter university and what they learn about it during their medical formation. Methods: A 10-item questionnaire with open and closed questions was designed. Questions addressed indications for DBS, its costs, impact on parkinsonian symptoms, complications, battery life, possible targets and percentage of PD patients who might profit from DBS. Students at Hannover Medical School were asked to complete the questionnaire in the preclinical study period and in the next to last year of the study. Results: The group of “beginners” included 204 students (duration of study: 3 months) and the “advanced” group implied 162 students (duration of study: 60 months). Of all students 63.6% were female and 36.4% were male. In the first group 22.7% had heard about DBS in medical lectures earlier. In comparison 98.76% had heard of DBS in medical lectures in the second group. In group one 63.4% of the students knew that DBS is routinely used in PD patients as compared to 83.3% in the second group. Knowledge about other movement disorders was much less common. In the first group 10.3% knew that DBS is used in patients with dystonia, whereas only one third knew about its use in dystonia (34%) in the second group. Outcome after DBS, its costs, the frequency of side effects, and established and future targets were nearly unknown. Conclusions: DBS is partly known among medical students in the preclinical phase with a moderate gain of knowledge during further study. We advocate to teach students appropriately and to expand clinical knowledge during the clinical phase of medical studies.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 227
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 320 Local Field Potentials Show Increased 6-10 Hz Activity Recorded From The Globus Pallidus Inernus And The Thalamus In Patients With Tourette-syndrome Wolf J. Neumann, Berlin, Germany; Julius Huebl, Berlin, Germany; Christof Brücke, Berlin, Germany; Götz Lütjens, Medical School Hanover, Hanover, Germany; Hans H. Capelle, Hanover, Germany; Joachim K. Krauss, Hanover, Germany; Andrea Kühn, Prof., Berlin, Germany Introduction: Tourette Syndrome (TS) is a disabling disease associated with motor tics, obsessive-compulsive behaviour and attention deficit hyperactivity disorder. Deep brain stimulation of the CMPf and GPi has been described to be effective to reduce tics in refractory TS. However, little is known about the functional significance of these targets in the pathophysiology of TS. We aimed to explore the disease specific pattern of oscillatory local field potential (LFP) activity of the centromedian-parafascicular nucleus (CMPf) and the dorsolateral globus pallidus internus (GPi). Methods: In five patients with severe TS DBS-electrodes were implanted in the dorsolateral GPi and CMPf. Bipolar LFP from four adjacent contacts (0: 1/1: 2/2: 3) at rest were recorded. Additionally an electromyography of motor tics was recorded in parallel to the LFPs in one patient. Results: A distinct peak in the 6-10 Hz frequency band occurred in both DBS targets with a mean peak frequency of about 7.2 Hz in the GPi and 8.3 Hz in the CMPf. 22 out of 23 individual recordings showed a distinct peak at 6-10 Hz with on average 20.1% in the GPi and 24.8% in the CMPf difference in max peak power compared to the remaining contact pairs. Additional power peaks were detected in the beta frequency band (13 -30 Hz) and high gamma frequency band (78-86 Hz). Tic-related EMG activity was associated with an increase in 6-10 Hz LFP activity. Conclusions: Our data extend previous findings of ~7 Hz activity in CMPf in TS suggesting that enhanced low frequency LFP activity is not restricted to thalamic nuclei but might be present in the cortex-basal ganglia-thalamic network in patients with TS. Furthermore, coherent low frequency activity was found between GPi and CMPf and the tic-related increase of 6-10 Hz activity may point to a potential pathophysiological role of enhanced low frequency activity in TS.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 228
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 129 Gait Changes In Patients With Segmental Dystonia Treated With Pallidal Deep Brain Stimulation Marc Wolf, M.D., Mannheim, Germany; Cristian Blahak, M.D., Mannheim, Germany; Götz Lütjens, Medical School Hanover, Hanover, Germany; Hans Capelle, M.D., Hanover, Germany; Michael G. Hennerici, Prof., Mannheim, Germany; Joachim K. Krauss, Prof., Hanover, Germany Introduction: Pallidal DBS has been established as an effective and safe therapy for dystonia. In general, side effects are rare, but there is increasing evidence that GPi DBS in dystonia can induce hypokinetic symptoms like micrographia or freezing of gait, sometimes even the full clinical picture of parkinsonism. Methods: We prospectively analyzed different parameters of normal gait in 10 consecutive patients (mean age 57.81/-14.3 years) with segmental dystonia but without involvement of lower trunk or legs who were treated with bilateral GPi DBS. Using a computerized gait analysis system with pressure sensitive insoles, walking distance (in 20s), cadence, step length and step duration were measured preoperatively (pre-OP) and at a median of 7 months post DBS surgery. None of the patients had typical capsular side effects, and only one patient reported mild gait disturbances with GPi DBS. Statistical analysis used Students t-test for paired variables. Results: While walking distances were comparable pre- and post-OP (mean1/-SD 21.21/-2.7 m vs. 20.21/-2.5 m; p 50.14), mean step length significantly decreased from 60.01/-6.9 cm pre-OP to 54.31/-6.4 cm with GPi-DBS (p<0.01). In consequence, cadence significantly increased from 105.61/-9.2 steps/min pre-OP to 111.31/-11.4 steps/min with GPi DBS (p<0.05), and step duration was slightly reduced post-OP (0.571/-0.05 s pre-OP vs. 0.541/-0.06 s with GPi-DBS; p<0.05). Conclusions: With chronic bilateral GPi DBS, patients with segmental dystonia showed a mild change in gait pattern with reduced step length and increased cadence. We postulate that this phenomenon reflects a disturbance of basal ganglia function in terms of a mild hypokinesia of gait. Given the other recently reported hypokinetic effects of GPi-DBS in dystonia like micrographia or freezing of gait, a general alteration of neuronal activity in striato-pallido-thalamo-cortical pathways following chronic stimulation of the posteroventral lateral GPi leading to hypokinesia of different aspects of motor function can be presumed.
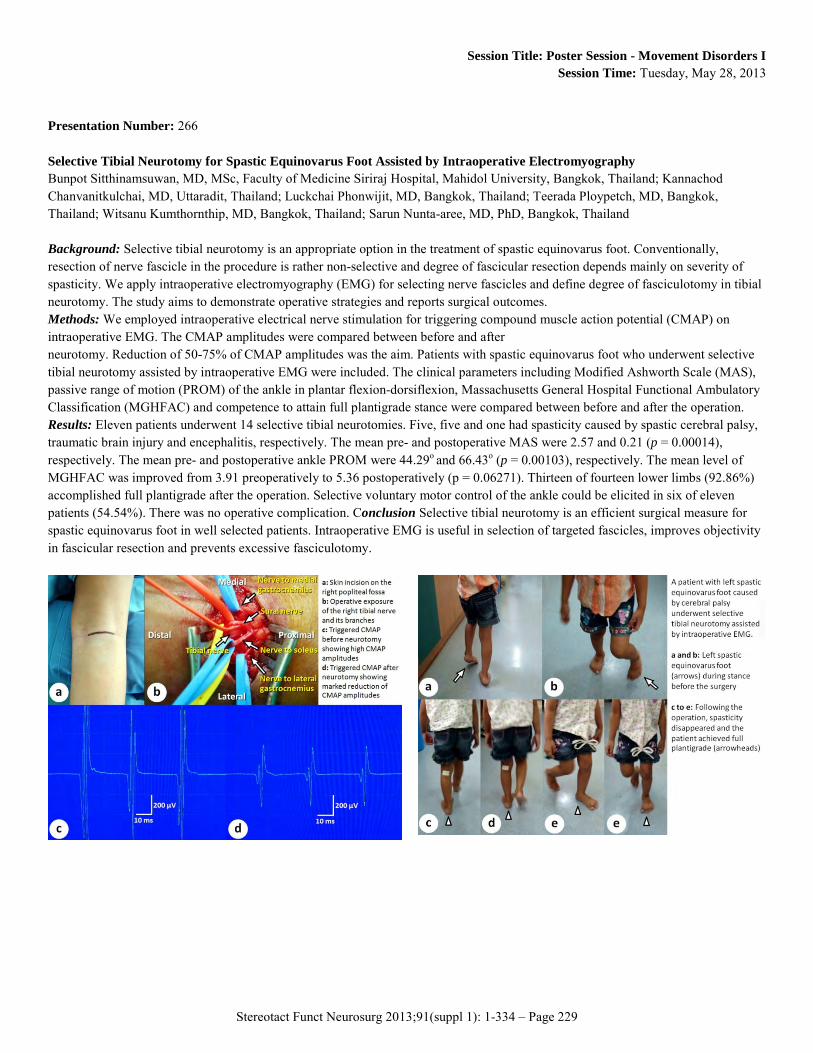
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 229
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 266 Selective Tibial Neurotomy for Spastic Equinovarus Foot Assisted by Intraoperative Electromyography Bunpot Sitthinamsuwan, MD, MSc, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; Kannachod Chanvanitkulchai, MD, Uttaradit, Thailand; Luckchai Phonwijit, MD, Bangkok, Thailand; Teerada Ploypetch, MD, Bangkok, Thailand; Witsanu Kumthornthip, MD, Bangkok, Thailand; Sarun Nunta-aree, MD, PhD, Bangkok, Thailand Background: Selective tibial neurotomy is an appropriate option in the treatment of spastic equinovarus foot. Conventionally, resection of nerve fascicle in the procedure is rather non-selective and degree of fascicular resection depends mainly on severity of spasticity. We apply intraoperative electromyography (EMG) for selecting nerve fascicles and define degree of fasciculotomy in tibial neurotomy. The study aims to demonstrate operative strategies and reports surgical outcomes. Methods: We employed intraoperative electrical nerve stimulation for triggering compound muscle action potential (CMAP) on intraoperative EMG. The CMAP amplitudes were compared between before and after neurotomy. Reduction of 50-75% of CMAP amplitudes was the aim. Patients with spastic equinovarus foot who underwent selective tibial neurotomy assisted by intraoperative EMG were included. The clinical parameters including Modified Ashworth Scale (MAS), passive range of motion (PROM) of the ankle in plantar flexion-dorsiflexion, Massachusetts General Hospital Functional Ambulatory Classification (MGHFAC) and competence to attain full plantigrade stance were compared between before and after the operation. Results: Eleven patients underwent 14 selective tibial neurotomies. Five, five and one had spasticity caused by spastic cerebral palsy, traumatic brain injury and encephalitis, respectively. The mean pre- and postoperative MAS were 2.57 and 0.21 (p = 0.00014), respectively. The mean pre- and postoperative ankle PROM were 44.29o and 66.43o (p = 0.00103), respectively. The mean level of MGHFAC was improved from 3.91 preoperatively to 5.36 postoperatively (p = 0.06271). Thirteen of fourteen lower limbs (92.86%) accomplished full plantigrade after the operation. Selective voluntary motor control of the ankle could be elicited in six of eleven patients (54.54%). There was no operative complication. Conclusion Selective tibial neurotomy is an efficient surgical measure for spastic equinovarus foot in well selected patients. Intraoperative EMG is useful in selection of targeted fascicles, improves objectivity in fascicular resection and prevents excessive fasciculotomy.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 230
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 155 Subthalamic Neuron Activity In Patients With Parkinson Disease: Neurophysiological Criteria For Deep Brain Stimulation Electrode Implantation. Yasukazu Kajita, Nagoya University, Nagoya, Japan; Yoshiki Kaneoke, MD.PhD, Wakayama, Japan; Toshiya Nagai, Nagoya, Japan; Takahiro Nakura, MD.PhD, Nagakute, Japan; Daisuke Nakatsubo, MD, Obu, Japan; Toshihiko Wakabayashi, MD, Nagoya, Japan (Introduction) Deep brain stimulation (DBS) of the subthalamic nucleus (STN) for the patients with Parkinson disease (PD) is performed using intraoperative microelectrode recording (MER) to define the optimal site. Microelectrode criteria for DBS implantation is, however, various, including length of STN recorded, the presence of movement-related neurons and distance from the border of adjacent structures. The electrode location affects the surgical outcome in the patients with unilateral STN-DBS stronger than with bilateral stimulation. The correlation between microelectrode criteria and surgical outcome was respectively examined in the patients with unilateral STN DBS. (Methods) 1) We retrospectively collected MER data obtained in 14 patients with unilateral STN-DBS to examine the distribution of movement-related neurons in STN. 2) In one hundred patients with unilateral STN DBS, the correlation between the data of MER including the length of STN recorded, the number of total thalamic and STN neurons, orofacial, upper and lower extremity movement-related neurons in STN, and surgical outcome was examined. Surgical outcome assessment included the Unified PD Rating Scale (UPDRS). (Results) 1) One hundred forty seven movement-related cells in STN were observed in 31 tracks. One hundred thirty cells (88.0%) were located in the dorsal two-thirds of the nucleus. Upper extremity-related cells were localized in lateral and dorsal to the lower extremity-related cells. 2) The number of total STN neurons, movement-related neurons and the length of STN recorded were significantly correlated with improvement of the surgical outcome and the number of movement-related neurons was most strongly related with the surgical outcome. (Conclusion) In the patients with unilateral STN-DBS, electrophysiological mapping with MER modify the DBS target and improves the clinical efficacy of DBS electrodes. Furthermore, the presence of movement-related neurons in STN is the most important neurophysiological criteria necessary for successful DBS lead placement.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 231
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 372 Bilateral Vim-DBS Improved for Involuntary Movement due to Chronic Inflammatory Demyelinating Polyneuropathy. A Case Report Takamizawa Sachiko, Saitama Medical University Hospital, Iruma-gunn, Japan; Masahito Kobayashi, Iruma-gunn, Japan; Takamitsu Fujimaki, PhD, Iruma-gunn, Japan Introduction: Chronic inflammatory demyelinating polyneuropathy (CIDP) is an uncommon disease, causing various symptoms. We have experienced a CIDP patient whose medication-resistant, complicated involuntary movement improved by bilateral Vim deep brain stimulation (DBS). Case presentation: We present a 66-year-old woman suffering from severe 2-4Hz involuntary movements of both hands. The movement was observed both at rest and during intentional movements. When she pinched a piece of paper, she could not stop her hand movement and squeezed it up. She didn’t show other neurological abnormal findings such as sensory disturbance and cerebellar ataxia. Medication such as L-DOPA and β-blocker was not effective. Referred by neurologists, she was admitted in our neurosurgical department and bilateral Vim DBS was performed and her symptoms were dramatically improved. One month after DBS surgery, she developed ataxic gait and sensory disturbance. She was referred back to neurological departments and diagnosed as chronic inflammatory demyelinating polyneuropathy (CIDP) based on clinical presentation, electromyogram, and biopsy. Administration of immunoglobulin and corticosteroid improved most of her symptoms but not involuntary movements, which resolved by DBS. She has been treated by medication and DBS for two years. Discussion: CIDP is an immune-mediated disorder of the peripheral nervous system. Many patients improve by medical treatment but some of them will be suffering from relapsing or residual symptoms such as numbness or tremors. Bilateral Vim deep brain stimulation was effective for severe involuntary movements caused by CIDP.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 232
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 167 Long-term Follow-up Study For Patients With Primary Generalized Dystonia Treated By Bilateral Pallidal Stimulation Michael R. Sobstyl, MD PhD, Postgraduate Medical Center, Warsaw, Poland; Mirosław Ząbek, MD PhD, Postgraduate Medical Center, Warsaw, Poland; Zbigniew Mossakowski, MD, Bródno Regional Hospital, Warsaw, Poland Introduction: The aim of this study is to present our experience of bilateral pallidal stimulation in patients with primary generalized dystonia (PGD) in the long-term follow-up. Bilateral pallidal stimulation is the preferred surgical therapy for patients with PGD. Methods: The study population is composed of 10 patients with the diagnosis of PGD (6 patients with DYT-1 positive PGD and 4 patients with DYT-1 negative PGD). The patients were operated on in general anesthesia. The posteroventrolateral pallidum was calculated according to the midcommissural point derived from fusion of stereotactic computer tomography images with magnetic resonance images. The DBS leads (Type 3387) were implanted without intraoperative electrophysiological guidance. The formal objective assessment included the Burke-Fahn-Marsden Dystonia Rating Scale (BFMDRS). The BFMDRS assessment was performed before surgery and 1,2, 3 and 4 years during follow-up period. Results: At the last follow-up visit in 6 patients with DYT-1 positive PGD the functional and motor parts of the BFMDRS improved by 52 % and 58 % respectively when compared to the preoperative scores. In 4 patients with DYT-1 negative PGD the functional and motor parts of the BFMDRS improved by 43 % and 49 % respectively. The hardware-related complications occurred in 4 patients (4 breakages of DBS leads). All hardware-related complications were successfully managed. Conclusions: Bilateral pallidal stimulation remains an effective and safe treatment for patients with PGD.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 233
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 360 Bilateral Pallidal Deep Brain Stimulation for Treatment of Meige Syndrome Raghuram Gopalakrishnan, MD, Columbia Asia Hospital, Bangalore, India; Takaomi Taira, MD, PhD, Tokyo Women's Medical University, Japan Introduction: Primary Meige syndrome is an idiopathic movement disorder characterized by blepharospam, oromandibular and cervical dystonia. Bilateral deep brain stimulation of the Globus pallidus internus (GpI) has been found to be an effective treatment in medically refractory cases. Our experience with treating eight patients with Meige syndrome was analysed. Methods: Eight patients with Meige syndrome who were treated with bilateral deep brain stimulation of GpI were analysed retrospectively. The mean follow up period was 36.12 ± 26.75 months. The mean age at surgery was 55.25 ± 10.18 years.The average duration of illness was 5.5 ± 4.2 years. All patients were assessed using the Burke-Fahn-Marsden dystonia rating scale (BFMDRS). Bilateral deep brain stimulation of the GpI was done under local anesthesia using two quadripolar leads (Model 3387, Medtronic) on each side. A total of four electrodes were implanted. Patients underwent trial stimulation with various combinations and the two electrodes (one on each side) with best response were connected to the Internal Pulse Generators (Soletra, Medtronic) after one to two weeks of electrode implantation. The patients were assessed pre op and on follow up. The pre op scores and the scores on the last follow up were compared to assess the percentage of improvement. Results: At the last follow up the percentage of improvement in the BFMRDS was 83.45 % ± 8.8%. The improvement was independent of sex, age and the duration of symptoms. The extent of improvement was maximum in blepharospam and oromandibular dystonia. There was no major side effect of the procedure. The procedure of implanting two electrodes on either side provided us with multiple options for programming. Conclusion: Bilateral deep brain stimulation of the Globus pallidus internus is an effective treatment for Meige syndrome.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 234
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 97 Long-term Outcomes Of Bilateral Subthalamic Nucleus Stimulation In Japanese Patients With Parkinson Disease Atsushi Umemura, MD, Juntendo University, Tokyo, Japan; Yuichi Oka, MD, Nagoya, Japan; Kenji Okita, MD, Nagoya, Japan; Genko Oyama, MD, Tokyo, Japan; Yasushi Shimo, MD, Tokyo, Japan; Nobutaka Hattori, MD, Tokyo, Japan Introduction: We studied long-term outcomes of subthalamic nucleus stimulation (STN DBS) in Japanese patients with Parkinson disease (PD). Methods: Fifty-five consecutive patients treated with bilateral STN DBS were followed up until 5 years after surgery. Each patient underwent an assessment of UPDRS preoperatively and then 1 month, 1 year and 5 years after surgery. Twelve patients were lost to follow up within 5 years. Among them, 5 patients became a bed-ridden status because of deterioration of axial symptoms of PD and 7 patients died of other diseases or accident. Results: In 43 patients with 5-year follow up, improvements in medication-off UPDRS III motor score, dyskinesia, motor fluctuation, and reduced need for dopaminergic medication were maintained over 5 years compared to the preoperative status. Long-term outcome was particularly favorable for the symptoms of tremor and rigidity. On the other hand, axial symptoms concerning speech, gait and postural stability gradually deteriorated. Persisting adverse effects included apraxia of eyelid opening and dysarthria. Conclusions: STN DBS produces significant improvement in motor function over 5 years in most cases of advanced PD. These results are almost consistent with the results in Western countries. However, considering the dropout patients, long-term outcomes of STN DBS seem to be worse than expected. Some patients showed rapid deterioration of refractory axial symptoms even after STN DBS. Other treatment strategy toward axial symptoms is the next subject in long-term treatment of PD.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 235
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 299 Thalamic Deep Brain Stimulation for Essential Tremor: Long-Term Therapeutic Efficacy and Changes of Electrical Parameters Settings during Follow-up Carlos Fernandez Carballal, MD, H.G.U. Gregorio Marañón, Madrid, Spain; Antonio Vargas López, H.G.U. Gregorio Marañón, Madrid, Spain; José Manuel Garbizu Vidorreta, H.G.U. Gregorio Marañón, Madrid, Spain; Beatriz De la Casa, H.g.u. Gregorio Marañón. Madrid, Spain; Pedro María Rodríguez Cruz, HGU Gregorio Marañón, Madrid, Spain; Grandas Francisco, HGU Gregorio Marañón, Madrid, Spain Introduction: Deep brain stimulation (DBS) of the ventral intermediate nucleus of the thalamus (Vim) has proven to be efficacious in the treatment of essential tremor (ET), and has replaced Vim thalamotomy as first surgical choice in most centers. We report on long-term follow-up of a series of patients treated in our institution Methods: Patients with ET who received unilateral or bilateral Vim BBS were collected. The tremor and handwriting components of the Fahn-Tolosa-Marin clinical tremor rating scale were assessed pre- and postoperatively. Stimulation parameters at different intervals after surgery were also recorded. Results: Twenty three patients with ET received unilateral or bilateral Vim DBS. In two patients the hardware was removed due to infection and were lost of follow-up. The average follow-up period was 76,8 months in the remaining twenty-one patients. One patient required a new procedure due to suboptimal localization. The average tremor score improved from 2,94 preoperatively to 0.89 postoperatively (on stimulation; p < 0.001) and the average handwriting score improved from 3.22 to 1.22 at one year (p < 0.001) and 1.33 in the last evaluation (p < 0.001). The hardware-related complication rate including mentioned infections was 21%. Comparison of stimulation parameters showed significant differences (p< 0,05), with a gradual increase in all stimulation parameters (voltage, frequency and TEED-total electrical energy delivered) during follow-up. Conclusions: Deep brain stimulation of the Vim is an efficient and safe treatment for essential tremor. Tremor and handwriting improvements are stable. However, tolerance may develop in some patients during follow-up requiring changes in stimulation parameters to keep the clinical improvements.
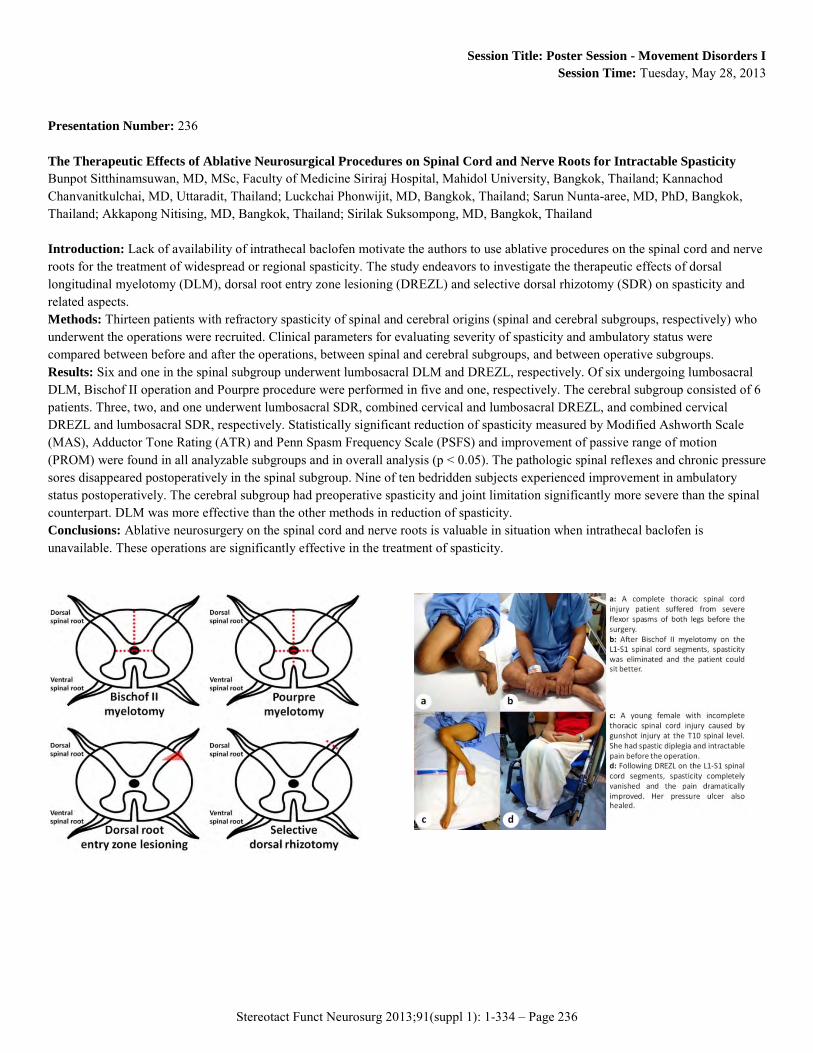
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 236
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 236 The Therapeutic Effects of Ablative Neurosurgical Procedures on Spinal Cord and Nerve Roots for Intractable Spasticity Bunpot Sitthinamsuwan, MD, MSc, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; Kannachod Chanvanitkulchai, MD, Uttaradit, Thailand; Luckchai Phonwijit, MD, Bangkok, Thailand; Sarun Nunta-aree, MD, PhD, Bangkok, Thailand; Akkapong Nitising, MD, Bangkok, Thailand; Sirilak Suksompong, MD, Bangkok, Thailand Introduction: Lack of availability of intrathecal baclofen motivate the authors to use ablative procedures on the spinal cord and nerve roots for the treatment of widespread or regional spasticity. The study endeavors to investigate the therapeutic effects of dorsal longitudinal myelotomy (DLM), dorsal root entry zone lesioning (DREZL) and selective dorsal rhizotomy (SDR) on spasticity and related aspects. Methods: Thirteen patients with refractory spasticity of spinal and cerebral origins (spinal and cerebral subgroups, respectively) who underwent the operations were recruited. Clinical parameters for evaluating severity of spasticity and ambulatory status were compared between before and after the operations, between spinal and cerebral subgroups, and between operative subgroups. Results: Six and one in the spinal subgroup underwent lumbosacral DLM and DREZL, respectively. Of six undergoing lumbosacral DLM, Bischof II operation and Pourpre procedure were performed in five and one, respectively. The cerebral subgroup consisted of 6 patients. Three, two, and one underwent lumbosacral SDR, combined cervical and lumbosacral DREZL, and combined cervical DREZL and lumbosacral SDR, respectively. Statistically significant reduction of spasticity measured by Modified Ashworth Scale (MAS), Adductor Tone Rating (ATR) and Penn Spasm Frequency Scale (PSFS) and improvement of passive range of motion (PROM) were found in all analyzable subgroups and in overall analysis (p < 0.05). The pathologic spinal reflexes and chronic pressure sores disappeared postoperatively in the spinal subgroup. Nine of ten bedridden subjects experienced improvement in ambulatory status postoperatively. The cerebral subgroup had preoperative spasticity and joint limitation significantly more severe than the spinal counterpart. DLM was more effective than the other methods in reduction of spasticity. Conclusions: Ablative neurosurgery on the spinal cord and nerve roots is valuable in situation when intrathecal baclofen is unavailable. These operations are significantly effective in the treatment of spasticity.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 237
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 169 Neuronal Activity In The Internal Pallidum Recorded In A Patient With X-linked Dystonia-parkinsonism (DTY3) Koichi Hamada, MD, Tokyo Metropolitan Neurological Hospital, Tokyo, Japan; Fusako Yokochi, MD, Tokyo, Japan; Makoto Taniguchi, MD, Tokyo, Japan; Takashi Kawasaki, MD, Tokyo, Japan; Ayako Isoo, MD, Tokyo, Japan; Ryoichi Okiyama, MD, Tokyo, Japan Introduction: X-linked dystonia-parkinsonism (DYT3) occurs frequently in the Philippines. The symptoms are dystonia with parkinsonism and are intractable. The pathological changes are limited to the striatum. We treated a patient with DYT3 by deep brain stimulation(DBS) of the internal pallidum(GPi) and analyzed the neuronal activity recorded during the operation. Methods: A 49-years-old Japanese man born in the Philippines was diagnosed as having DYT3 ay a genetic study. His symptoms were facial and segmental dystonia with bradykinesia. GPi-DBS was performed under general anesthesia for dystonia using the Leksell frame, Ben-gun and microelectrode recording(MER). The tentative target was the dorsal surface of optic tracts determined by magnetic resonance imaging(MRI). MER was carried out using a Medtronic FC1003 electrode and an RD-130TES data logger (TEAC Corporation) through Leadpoint, and units were analyzed offline. Results: The two tracks of MER were recorded in each GPi. First we recorded along the track of the Ben-Gun center. However meaningful neuronal activity was not recorded. The next tracks were placed 2mm lateral to GPis in both hemisphares. Along the next tracks, the neuronac activity was very high-amplitude units were recorded. The amplitudes of units were more than 1.5V. The discharges showed burst patterns with supression or phasic pattern. At and below the tentative targets, the photic responsive units were recorded in each track. Finally, the DBS electrode was implanted in the second lateral track in each GPi, and the DBS was successful. Conclusion: The distribution of high amplitude units in the GPi recorded in DYT3 was characteristic of DYT3 and quite different from that in Parkinson's disease or DYT1. The units in DYT3 should be related to the pathological changes of the striatum and the projection from the striatum.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 238
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 340 Stimulation Of Electrode Contacts Within Zona Incerta Directly Blocks Levodopa-induced Dyskinesias In Pd Patients Erich T. Fonoff, MD, PhD, University of Sao Paulo, Sao Paulo, Brazil; Carolina Souza, MD, PhD, Sao Paulo, Brazil; Maria Gabriela Ghilardi, MD, Sao Paulo, Brazil; Rubens Cury, MD, Sao Paulo, Brazil; Rachael Rodrigues, MD, Sao Paulo, Brazil; Egberto Barbosa, MD, Sao Paulo, Brazil; Manoel J. Teixeira, MD, PhD, Sao Paulo, Brazil Introduction: Sustained levodopa-induced dyskinesias remain a problem despite the benefits achieved with the control of other PD symptoms in STN DBS. To assess the possibility to obtain direct control of L-dopa-induced dyskinesias in PD patients by using stimulating electrode contacts located in the area right above STN stimulating contacts, namely zona incerta. Methods: Six out of 72 operated patients still experienced sustained disabling dyskinesias. PD patients (age 61±9.18y/H&Y 2.66±0.75) had been treated by STN-DBS (Medtronic - model 3387) for 4.9±1.3 years with remarkable improvement in other PD symptoms. Electrode trajectory was calculated in order to permit additional stimulation of the zona incerta between reticular thalamic nucleus and STN. Patients were evaluated by an experienced neurologist using clinical rating scales (UPDRS and UDysRS) in two conditions, either under usual stimulation of distal contacts (STN - eliciting dyskinesias) or the new protocol with stimulation of the upper contacts (in zona incerta - blocking dyskinesias. The later condition was kept for 4 to 6 weeks followed by reevaluation. Medication doses were kept still during the study. Results: Patients showed a tendency of improvement of UDPRS total scores, from 41.83±11.05 to 30.5±10.25 after 6 weeks (p=0,95), as well as for the UPDRSIII scores from 18±6.38 to 13.83±5.41 (p=0.25). However, the scores for UPDRS IV showed a reduction of 57%, from 6.66±1.86 to 3.16±2.71 (p=0,026) and 56% reduction in the UDysRS (total score), from 45.5±6.53 to 20.0±11.9 (p=0.001). 64% decrease in UDysRS part 3 was observed (encodes functional impairment), from 10.83±1.72 to 3.83±2.56 (p<0.001), while UDysRS part 4 decreased 60%, from 9.0 ±2.09 to 3.66±1.86 (p<0.001). Conclusions: The present results suggest that stimulation of zona incerta, just above and anterior to STN stimulation target, may produce direct control of levodopa-induced dyskinesias in PD patients.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 239
Session Title: Poster Session - Movement Disorders I Session Time: Tuesday, May 28, 2013
Presentation Number: 151 Multimodal and Multifocal Surgical Treatment of Generalized Dystonia Emilia W. Sołtan, MD, Institute of Psychiatry and Neurology, Warszawa (Warsaw), Poland; Henryk Koziara, MD,PhD, Warszawa (Warsaw), Poland; Rafal Rola, MD,PhD, Warszawa (Warsaw), Poland; Slawomir Barszcz, MD,PhD, Warszawa (Warsaw), Poland; Bartosz Krolicki, MD, Warszawa (Warsaw), Poland; Krzysztof Szalecki, MD, Warszawa (Warsaw), Poland; Tomasz Tykocki, MD,PhD, Warszawa (Warsaw), Poland; Pawel Nauman, MD,PhD, Warszawa (Warsaw), Poland; Wieslaw Bonicki, MD,PhD, Warszawa (Warsaw), Poland; Tomasz Mandat, MD,PhD, Warszawa (Warsaw), Poland Introduction: The objective of our research is to evaluate of effectiveness and safety of multimodal stereotactic procedures (MSP), lesioning and deep brain stimulation (DBS)) and multifocal stimulation (globus pallidus pars interna (GPi) and subthalamic nucleus (STN)) treatment of generalized dystonia (GD). Lesioning including thalamotomy and pallidotomy are historical stereotactic methods of GD treatment. DBS is a surgical method of choice for various movement disorders treatment that includes GD. MSP and multifocal DBS were involved in movement disorders treatment to achieve better results, but no analysis has been conducted yet. Methods: Five GD patients underwent bilateral GPi DBS or thalamotomy or pallidotomy in past. All of them demonstrated significant improvement that vanished after few years after surgery. Three of them, who underwent lesioning in the past were qualified for DBS: GPi (2 patients) and STN (1 patient). Two patients, who underwent GPi stimulation in past were qualified for multifocal stimulation- additional STN DBS. Results: MSP and multifocal DBS have showed sustained improvement in dystonic movement that lasted in two to three years follow-up. No surgical or stimulation related complications were reported. Conclusions: MSP: lesioning and DBS and combined, multifocal GPi and STN DBS might and should be considered when dystonic symptoms aggravate over time.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 240
Session Title: Poster Session - Movement Disorders II Session Time: Wednesday, May 29, 2013
Presentation Number: 179 Medial Associative-limbic And Lateral Motorpart Of Rat Subthalamic Nucleus And Effect Of 6-hydroxydopamine Lesions In Dorsolateral Striatum Mesbah Alam, PhD, Hannover Medical School, Hannover, Germany; Christoph Lindemann, PhD, Hannover, Germany; Joachim Kurt Krauss, MD,PhD, Hannover, Germany; Kerstin Schwabe, PhD, Hannover, Germany Introduction: Lesions of the rat nigrostriatal dopamine system by injection of 6-hydroxydopamine (6-OHDA) lead to abnormal neuronal activity in the basal ganglia (BG) motor loop similar to that found in Parkinson’s disease (PD). In the BG motor loop the subthalamic nucleus (STN) represents an important structure, which, however, also comprises areas of the BG associative and limbic loops. We tested interested whether neuronal activity would differ between the STN medial associative-limbic and lateral motor part, and whether selective 6-OHDA-induced lesions of the dorsolateral striatum, the entrance region of the BG motor loop, would differently affect these subregions. Methods: In male Sprague Dawley rats 6-OHDA (n=12) or vehicle (n=10) was bilaterally injected in the dorsolateral striatum. Four weeks later extracellular single-unit activity and local field potentials were recorded in medial and lateral STN neurons of urethane anaesthetized rats. Results: In sham-lesioned rats discharge rate and burst activity were higher in the lateral compared to the medial STN. Similar differences were found for other neuronal activity measures (coefficient of variation of inter spike interval, skewness, kurtosis, approximate entropy). After 6-OHDA injection neuronal burst activity and low frequency oscillatory activity (0.3-2.5 Hz) was enhanced, while the discharge rate was not affected. In addition, in 6-OHDA-lesioned rats β-band oscillatory activity was enhanced, with no difference between STN subregions. Conclusions: We found important differences of neuronal activity between STN subregions, indicating functional segregation. However, selective 6-OHDA lesions of the dorsolateral striatum also had a pronounced effect on the medial STN subregion, indicating interaction between BG loops.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 241
Session Title: Poster Session - Movement Disorders II Session Time: Wednesday, May 29, 2013
Presentation Number: 196 Coherence Of Striatal And Entopeduncular Nucleus Neuronal Activity With Motor- Cortex In 6-ohda Rat-model Of Parkinson Mesbah Alam, Hannover Medical School, Hannover, Germany; Xingxing Jin, MD, Hannover, Germany; Kerstin Schwabe, PhD, Hannover, Germany; Joachim Kurt Krauss, MD,PhD, Hannover, Germany Introduction: The nigrostriatal loss of dopamine leads to hypokinesia together with excessive oscillatory beta band activity within the basal ganglia-cortical loop, while enhanced theta band activity is related to levodopa-induced dyskinesia (LID). This study investigates the neuronal firing characteristics of the striatum and entopeduncular nucleus (EPN) and the coherence of oscillatory activities of these regions with the motor cortex in the 6-OHDA rat model of Parkinson’s disease (PD) with and without LID. Methods: Twelve 6-OHDA lesioned hemiparkinsonian (HP) rats, eight of which were rendered dyskinetic by repeated injection of L-DOPA (HP-LID) were used. Single unit activity and local field potentials were measured in urethane (1.2 g/kg, i.p) anesthesia in the dorsolateral striatum and the EPN by platinum-tungsten microelectrodes “off” and after L-DOPA injection “on”. Motorcortex activity was measured by an electrocorticogram. Results: Firing activity in the striatum and EPN was similar in HP-LID and HP rats. Injection of L-DOPA decreased the firing rate in both groups in the EPN, without affecting the striatal firing rate. Striatal oscillatory activity in the theta band (4-8 Hz) was higher in HP-LID rats in both, “on” and “off” state as compared to HP rats. In the EPN theta activity did not differ between groups, but decreased in the “on” state in both groups. In both regions the beta activity (12-30 Hz) was higher in HP rats as compared to HP-LID rats in the “off” state, L-DOPA injection, however, reduced beta activity to a larger extent in HP-LID rats as compared to HP rats. The striato-cortical coherence of theta activity was stronger and beta activity was lower in HP-LID rats as compared to HP rats only in the “on” state. Conclusions: The findings of this study indicate that LID is associated with increased theta oscillatory activity in the strito-cortical loop of basal ganglia.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 242
Session Title: Poster Session - Movement Disorders II Session Time: Wednesday, May 29, 2013
Presentation Number: 43 Early Stim Study And Its Possible Influence On Clinical Practice In Patient Selection Hubertus M. Mehdorn, M.D.,Ph.D., University of Kiel, Kiel, Germany; Daniela Falk, M.D., Kiel, Germany Deep Brain Stimulation (DBS) as any surgical treatment carries age related surgical risks e.g. intracranial hematoma and infection. Furthermore it is evident that DBS is no cure for Parkinson’s Disease (PD) but may help to delay the clinical and social decline of PD patients. In order to clarify whether patients affected by Parkinson’s disease (PD) would benefit from DBS,early“ in their career, a binational multicenter study was conducted with french and german neurologists and neurosurgeons involved. In 20 centers a total of 251 patients were included who were randomized for early DBS to STN resp. best medical therapy when presenting with mild motor complications. They were followed for 2 years and prospectively assessed using the standards for detailed evaluation of quality of life (QoL). Results disclosure is not yet possible at time of abstract submission (but data will be available at time of congress), however, on the basis of previous well-conducted multicenter studies and the new relevant data, it will be speculated how the inclusion criteria of patients for DBS will be altered in the near future.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 243
Session Title: Poster Session - Movement Disorders II Session Time: Wednesday, May 29, 2013
Presentation Number: 306 Deep Brain Stimulation in Hyperkinetic Movement Disorders Marta Del Álamo, Ramón y Cajal Hospital, Madrid, Spain; Lidia Cabañes, Madrid, Spain; Ignacio Regidor, Madrid, Spain Introduction: Movement disorders have been grossly categorized into either hypokinetic (e.g. PD, and related disorders) where there is a paucity of movement, or hyperkinetic (dystonia, tremor, choreas, etc.) where there is excessive movement. We analyze the efficacy and safety of Deep Brain Simulation in hyperkinetic Movement disorders. Methods: 127 Hyperkinetic Movement disorder patients were operated with DBS since 1995. Retrospective analysis of our DBS treated patients' database was done. Demographic and clinical features, aetiology, and adverse events were recorded. Efficacy was measured by the change in the specific movement disorder scale (e.g. severity of Dystonia one year after DBS (Burke Fahn Marsden scale, BFM) and clinical global impression (CGI 1-7). Surgery was performed with Leksell stereotactic frame and Microrrecording and intraoperative stimulation. Results: Most frequent Hyperkinetic movement disorder was tremor with 84 patients (29 Essential tremor, 35 Parkinson disease patients with tremor as predominant symptom, 9 patients with Multiple Sclerosis, 1 orthostatic tremor, 3 patients with neuropathy tremor, 5 patients with post-traumatic tremor, 2 patients with Holmes tremor) in this group we used Vim target. Second most frequent Hyperkinetic movement disorder was Dystonia with 32 patients operated (16 patients with Generalized dystonia DYT1 (-), 2 patients with Generalized dystonia DYT1 (+), 3 patients with cerebral palsy, 3 patients with Mioclonus Dystonia, 2 patients with Tardive Dystonia, 1 Cervical Dystonia case, 2 patients with Hemidystonia, 1 PKAN, 1 Mitochondrial Encephalopathy, 1 Complex regional pain syndrome and 1 case secondary to encephalitis). Target stimulated in this group was GPi. Chorea patients (8) were operated also using GPi (2 Huntington`s disease and 6 Parkinson Disease patients with chorea discinesias as predominant symptom). Others were: Tourette syndrome, Hemibalysm-hemidystonia, and schizophrenia with complex stereotypes. Target stimulated in all of them was Gpi. Conclusions: DBS is effective and safety for medical resistant hyperkinetic movement disorders.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 244
Session Title: Poster Session - Movement Disorders II Session Time: Wednesday, May 29, 2013
Presentation Number: 382 Middle To Long-term Outcome Of Intrathecal Baclofen Therapy For The Patients With Intractable Spasticity Teppei Matsubara, University of Tsukuba, Tsukuba, Japan; Satoshi Ayuzawa, Tsukuba, Japan; Tsukasa Aoki, Tsukuba, Japan; Satoshi Ihara, Tsukuba, Japan; Akira Matsumura, Tsukuba, Japan Introduction: We assess middle to long-term effect of ITB therapy and its clinical characteristics. Methods: There are 25 patients, at least 6 months after the ITB therapy in our hospital between March 2007 and August 2012. Results: Nine of 25 patients are cerebral palsy with diffuse spasticity. The catheter tips are placed on upper thoracic levels to affect both lower and upper extremities. Mean Ashworth score remarkably decreases from 3.1 to 1.2 in the lower ones, and from 2.8 to 1.5 in the upper ones, with the mean baclofen dose of 126 μg/day. Five patients with hypoxic brain damage need high dose (347 μg/day) to control their severe spasticity. Three patients of spastic paraplegia use lower dose (55 μg/day) due to the weakness of their lower limbs. There are 28% of complications including 2 cases of device removal, and one case of erectile dysfunction. This case needs further treatment including selective peripheral neurotomy after ITB therapy. Conclusions: In terms of middle to long-term management of spasticity, we should be aware that comprehensive therapy is needed other than ITB therapy because of its complication.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 245
Session Title: Poster Session - Movement Disorders II Session Time: Wednesday, May 29, 2013
Presentation Number: 417 Tardive Dystonia: Promising Experience Of Pallidal Deep Brain Stimulation Anna Gamaleya, Burdenko Neurosurgical Institute RAMS, Moscow, Russian Federation; Alexey Tomskiy, Moscow, Russian Federation; Vladimir Shabalov, Moscow, Russian Federation Introduction: Tardive dystonia (TD) occurs due to use of dopamine-blocking agents (DBA), mainly neuroleptics. None of the drugs are consistently beneficial for TD, remission rate is low even when DBA are completely discontinued. Botulinum toxin could provide some symptomatic relief. In severe cases, treatment options remain disappointing. Methods: We report the experience of GPi-DBS in two patients with resistant TD. The first patient is a 29-year-old woman. She received prolonged psychiatric treatment including different DBA because of persistent depression from the age of 19 years. TD manifested following risperidon therapy 7 years ago with dystonia of the left arm and was triggered by infection. Further, dystonia spread gradually to generalized form with severe axial retroflexion (motor BFMDRS 49.5). The other patient is a 26-year-old man, who suffered schizophrenia with prominent obsessive-compulsive symptoms. Complex antipsychotic regimens were prescribed since 13 years. Three years ago, oromandibular and laryngopharyngeal dystonia developed. Directly incriminated drug was risperidon. TD rapidly progressed impairing all daily life activities and ambulation (BFMDRS 65). In both patients, discontinuation of DBA was ineffective; botulinum toxin injections did not provide satisfactory result. Considering disabling dystonia, electrodes for DBS were implanted under general anesthesia in posteroventrolateral GPi. Results: Following GPi-DBS, amelioration of dystonia was gradual reflecting reduction in disability. At follow-up of 3 months, clinical improvement was 39.4 and 63.1%, respectively; at 6 month - 65.6 and 83.1%, at 1 year - 77.8 and 90.8%, at the last follow-up 91.0 and 90.8% (3 and 1.5 years, respectively). No significant worsening of psychiatric symptoms occurred; however, both patients still needed neuroleptics to control underlying condition. Conclusions: In TD, GPi-DBS seems to be safe and even more effective than in primary dystonia. Patients experience stable profit by ongoing neuroleptic therapy. Although, GPi-DBS is promising for recovery of motor impairment, persistent psychiatric disorder might remain a challenge.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 246
Session Title: Poster Session - Psychiatric Neurosurgery Session Time: Wednesday, May 29, 2013
Presentation Number: 208 Comparative Characterization Of Single Cell Activity In Globus-pallidus-internus Of Patients With Dystonia And Tourette Syndrome Mesbah Alam, PhD, Hannover Medical School, Hannover, Germany; Kerstin Schwabe, PhD, Hannover, Germany; Mihai Manu, MD, Hannover, Germany; Goetz Luetjens, MD, Hannover, Germany; Hans E. Heissler, Hannover, Germany; Joachim Kurt Krauss, MD,PhD, Hannover, Germany Introduction: In both, dystonia and Tourette’s syndrome (TS), altered processing in the basal ganglia has been described. Deep brain stimulation of the globus pallidus internus (GPi) is a standard treatment for dystonia, and has been also successfully used to alleviate symptoms in TS. The aim of this study was to evaluate possible differences of neuronal discharge rates and patterns in the GPi of patients with dystonia and TS. Methods: Nine patients with dystonia (6 men and 3 women, mean age 52 years; primary dystonia) and six patients with TS (2 men and 4 women, mean age 30 years) were studied during functional stereotactic neurosurgical operations for implantation of DBS electrodes. All surgery was performed under general anaesthesia. Single-unit activity recordings in the GPi was obtained during routine microelectrode recording and mapping to delineate nuclear borders and to identify the sensorimotor subregions. Results: Based on the comparison of mean inter spike intervals from neurons recorded in the GPi, dystonia patients showed higher mean firing rates. The parameters of bursts and discharge patterns were similar in both dystonia and TS patients. The non-linear time series analysis of Lempel-Ziv complexity showed high entropy in TS as compared to dystonia. The spectral analysis of neuronal spike trains showed decreased gamma oscillatory activity in TS compared to dystonia patients, while low frequency activities in the delta and theta oscillatory range were similar in both groups. Conclusions: Our data provides evidence that the neuronal dynamic complexity, randomness and gamma oscillatory modulation of spike trains in the GPi differ to some extent between dystonia and TS.
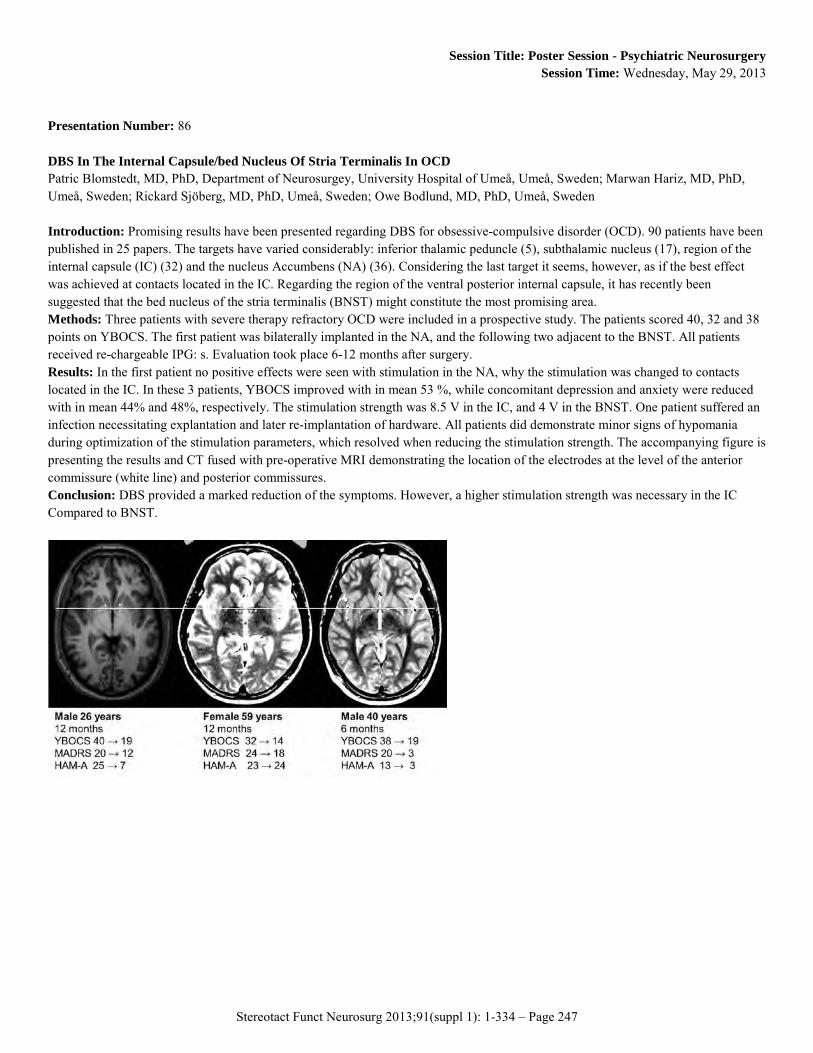
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 247
Session Title: Poster Session - Psychiatric Neurosurgery Session Time: Wednesday, May 29, 2013
Presentation Number: 86 DBS In The Internal Capsule/bed Nucleus Of Stria Terminalis In OCD Patric Blomstedt, MD, PhD, Department of Neurosurgey, University Hospital of Umeå, Umeå, Sweden; Marwan Hariz, MD, PhD, Umeå, Sweden; Rickard Sjöberg, MD, PhD, Umeå, Sweden; Owe Bodlund, MD, PhD, Umeå, Sweden Introduction: Promising results have been presented regarding DBS for obsessive-compulsive disorder (OCD). 90 patients have been published in 25 papers. The targets have varied considerably: inferior thalamic peduncle (5), subthalamic nucleus (17), region of the internal capsule (IC) (32) and the nucleus Accumbens (NA) (36). Considering the last target it seems, however, as if the best effect was achieved at contacts located in the IC. Regarding the region of the ventral posterior internal capsule, it has recently been suggested that the bed nucleus of the stria terminalis (BNST) might constitute the most promising area. Methods: Three patients with severe therapy refractory OCD were included in a prospective study. The patients scored 40, 32 and 38 points on YBOCS. The first patient was bilaterally implanted in the NA, and the following two adjacent to the BNST. All patients received re-chargeable IPG: s. Evaluation took place 6-12 months after surgery. Results: In the first patient no positive effects were seen with stimulation in the NA, why the stimulation was changed to contacts located in the IC. In these 3 patients, YBOCS improved with in mean 53 %, while concomitant depression and anxiety were reduced with in mean 44% and 48%, respectively. The stimulation strength was 8.5 V in the IC, and 4 V in the BNST. One patient suffered an infection necessitating explantation and later re-implantation of hardware. All patients did demonstrate minor signs of hypomania during optimization of the stimulation parameters, which resolved when reducing the stimulation strength. The accompanying figure is presenting the results and CT fused with pre-operative MRI demonstrating the location of the electrodes at the level of the anterior commissure (white line) and posterior commissures. Conclusion: DBS provided a marked reduction of the symptoms. However, a higher stimulation strength was necessary in the IC Compared to BNST.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 248
Session Title: Poster Session - Psychiatric Neurosurgery Session Time: Wednesday, May 29, 2013
Presentation Number: 131 Acute Effects Of Stimulation In The Bed Nucleus Of The Stria Terminalis/ Ventral Striatum-internal Capsule In Patients With Treatment-resistant Obsessive Compulsive Disorder. Götz Lütjens, M.D., Medical School Hanover, Hanover, Germany; Lotta Winter, Hanover, Germany; Kerstin Schwabe, Prof., Hanover, Germany; Asssel Saryyeva, M.D., Hanover, Germany; Hans Heissler, Hanover, Germany; Mesbah Alam, Hanover, Germany; Kai Kahl, M.D., Hanover, Germany; Joachim K. Krauss, Prof., Hanover, Germany Introduction: Deep brain stimulation (DBS) in different targets emerges as a promising therapeutic option for patients with treatment-resistant obsessive compulsive disorder (trOCD). We here describe the acute stimulation effects of different stimulation settings on OCD symptoms and mood states in 2 patients with trOCD after implantation of DBS electrodes in the bed nucleus of the stria terminalis/ ventral striatum-internal capsule (BNST/VS-IC). Methods: Quadripolar DBS electrodes (Medtronic 3387) were implanted bilaterally with stereotactic guidance and microelectrode recordings in the BNST/VS-IC. Electrode location was confirmed via postoperative stereotactic CT. On the following day, the target was stimulated using different amplitudes (1V, 2V, 3.5V) and different contacts (0-/1+, 0-/3+, 2-/3+) with a constant pulse width of 210 µsec and a frequency of 130 Hz for 5 minutes, respectively. Obsessive-compulsive symptoms and mood states were assessed by an independent rater using visual analogue scales. Results: Subjective intensity of obsessive-compulsive thoughts was reduced most by acute stimulation with 2V but, however, deteriorated with higher amplitudes. Subjective feelings of pleasure and spontaneous smiling were induced also at low voltage. Stimulation of different contact pairs located either in the BNST (0-/1+) or in the IC (2-/3+), and combined stimulation (0-/3+) produced differential and particularly specific effects. Conclusions: We here show acute effects on core symptoms of OCD after stimulation in the BNST/VS-IC. The induction of positive feelings accompanied symptom reduction.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 249
Session Title: Poster Session - Psychiatric Neurosurgery Session Time: Wednesday, May 29, 2013
Presentation Number: 24 Anterior Capsulotomy For The Treatment Of Obsessive Compulsive Disorder - A Review Of Old And New Literature Joshua Pepper, BSc MBBS, UCL, London, United Kingdom; Marwan Hariz, MD PhD, London, United Kingdom Introduction: Obsessive compulsive disorder (OCD) is a chronic and debilitating psychiatric condition that affects 2% of the population. Anterior Capsulotomy has been an effective and established procedure for treatment refractory OCD patients over the last half century. The unrestricted use of frontal lobotomy/leucotomy in the 1950’s generated significant public and professional fear around the use of ablative psychosurgery. This stigma is still preventing patients with the severest forms of OCD from accessing this treatment option. Here, we evaluate the published literature on anterior capsulotomy. Methods: Publications on anterior capsulotomy for OCD were obtained from the PubMed database, proceedings of neurosurgical meetings, and references from relevant papers. Duplicate patients were identified and removed. To be included, the studies needed to report on baseline characteristics (age; duration and severity of OCD) and outcome (length to follow up; clinical state at follow up). Patients with a Yale-Brown Obsessive Compulsive Score (YBOCS) were grouped according to improvement in this scale (Excellent >75%, Good 50-74%, Response 33-49%, No response/worse <33%). Patients without a YBOCS score were grouped according to the clinical description provided (Excellent: symptom free, Good: Live independently/back to work with some help, Response: level of social functioning meaningfully improved, or No response/worse). Results: In total 15 studies were identified reporting on outcomes of 300 patients. In the YBOCS group 23% had an excellent response and over half had a good outcome. In the group without YBOCS 65% of patients were living independently or back to work and 90% of patients had a meaningfully improved level of social function after surgery. Common complications noted include weight gain and personality change. Conclusion: Anterior capsulotomy is an effective procedure for medical refractory OCD. The current stigma and fear surrounding the use of ablative stereotactic neurosurgery in OCD is based more on history than facts.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 250
Session Title: Poster Session - Psychiatric Neurosurgery Session Time: Wednesday, May 29, 2013
Presentation Number: 72 Clinical Results of Stereotactic Surgery for Refractory OCD Peng Li, MD, west china hospital, sichuan university, chengdu, China; Wei Wang, MD, west china hospital, sichuan university, chengdu, China Introduction: The study is to understand the short-term and long-term advantages and disadvantages of bilateral capsulotomy. Methods: Nineteen patients of refractory OCD, who had undergone bilateral capsulotomy under the guidance of Leksell multifunctional stereotactic operation system, were followed up for three years. The pre and postoperative scores of the Y-BOCS, HAMA, HAMD and the changes of cerebral metabolism were analyzed. Results: Complete remission of the OCD symptoms was reported in one patient. And no obvious improvement was reported by one patient. The other 17 patients reported obvious improvement. The scores of the Y-BOCS, the HAMA, the HAMD showed significant improvements after the surgery(p<0.05). The scores at 1 week, 1 months, 3 months and 6 months varied significantly. But no significant changes of the scores could be observed from six months to 3 years after the surgery. Diffusion tensor imagination(DTI)showed that transverse fibers of anterior limb of internal capsule were cut. Brain 18FDG-PET showed that metabolism decrease in orbital frontal cortex, motor area, premotor area, basal ganglia, thalamus and limbic system after surgery. Nine patients appear emotional indifference the second day after surgery. One patient reported executive dysfunction, 3 patients with juvenile behavior and 2 cases with urinary incontinence. In 6 months after surgery, these symptoms disappeared. Conclusions: Stereotactic operation maybe an effective treatment in mental disorders. Long-term follow up should be carried out for such patients.
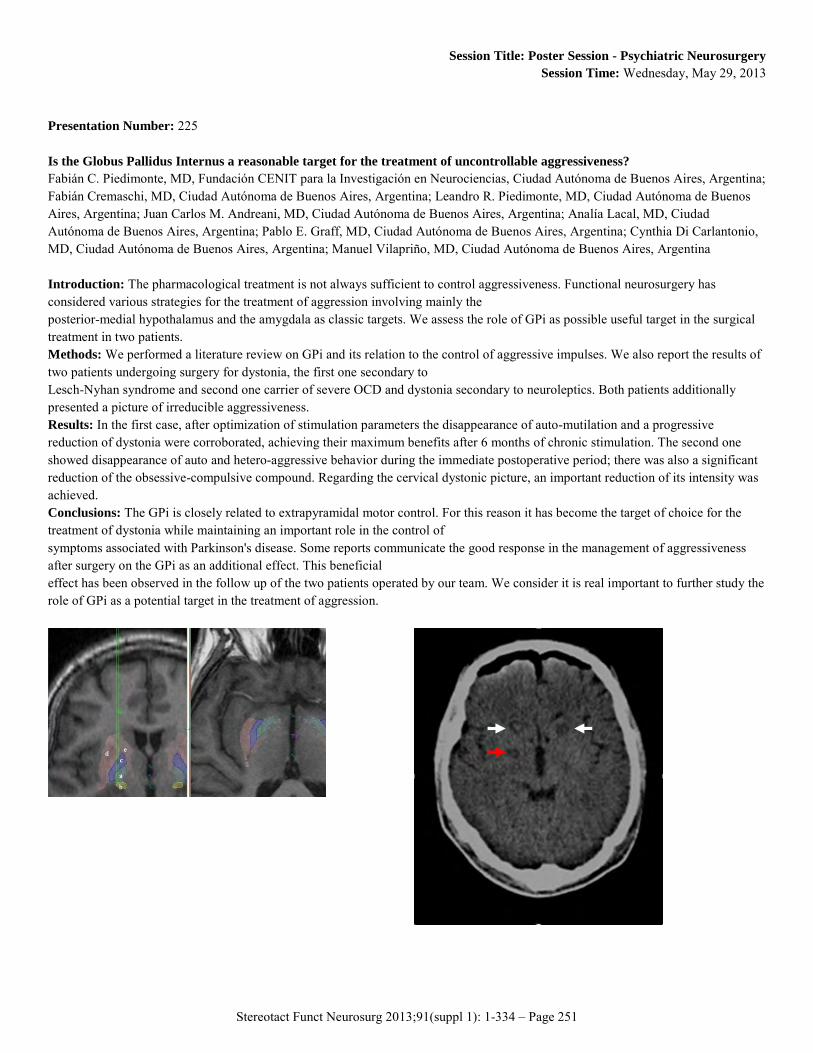
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 251
Session Title: Poster Session - Psychiatric Neurosurgery Session Time: Wednesday, May 29, 2013
Presentation Number: 225 Is the Globus Pallidus Internus a reasonable target for the treatment of uncontrollable aggressiveness? Fabián C. Piedimonte, MD, Fundación CENIT para la Investigación en Neurociencias, Ciudad Autónoma de Buenos Aires, Argentina; Fabián Cremaschi, MD, Ciudad Autónoma de Buenos Aires, Argentina; Leandro R. Piedimonte, MD, Ciudad Autónoma de Buenos Aires, Argentina; Juan Carlos M. Andreani, MD, Ciudad Autónoma de Buenos Aires, Argentina; Analía Lacal, MD, Ciudad Autónoma de Buenos Aires, Argentina; Pablo E. Graff, MD, Ciudad Autónoma de Buenos Aires, Argentina; Cynthia Di Carlantonio, MD, Ciudad Autónoma de Buenos Aires, Argentina; Manuel Vilapriño, MD, Ciudad Autónoma de Buenos Aires, Argentina Introduction: The pharmacological treatment is not always sufficient to control aggressiveness. Functional neurosurgery has considered various strategies for the treatment of aggression involving mainly the posterior-medial hypothalamus and the amygdala as classic targets. We assess the role of GPi as possible useful target in the surgical treatment in two patients. Methods: We performed a literature review on GPi and its relation to the control of aggressive impulses. We also report the results of two patients undergoing surgery for dystonia, the first one secondary to Lesch-Nyhan syndrome and second one carrier of severe OCD and dystonia secondary to neuroleptics. Both patients additionally presented a picture of irreducible aggressiveness. Results: In the first case, after optimization of stimulation parameters the disappearance of auto-mutilation and a progressive reduction of dystonia were corroborated, achieving their maximum benefits after 6 months of chronic stimulation. The second one showed disappearance of auto and hetero-aggressive behavior during the immediate postoperative period; there was also a significant reduction of the obsessive-compulsive compound. Regarding the cervical dystonic picture, an important reduction of its intensity was achieved. Conclusions: The GPi is closely related to extrapyramidal motor control. For this reason it has become the target of choice for the treatment of dystonia while maintaining an important role in the control of symptoms associated with Parkinson's disease. Some reports communicate the good response in the management of aggressiveness after surgery on the GPi as an additional effect. This beneficial effect has been observed in the follow up of the two patients operated by our team. We consider it is real important to further study the role of GPi as a potential target in the treatment of aggression.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 252
Session Title: Poster Session - Psychiatric Neurosurgery Session Time: Wednesday, May 29, 2013
Presentation Number: 264 DBS for Refractory Cocaine Dependence Antonio Gonçalves-Ferreira, MD.PhD, University Hospital Santa Maria, Lisbon, Portugal; Frederico Simões Couto, MD, Lisbon, Portugal; Alexandre Rainha Campos, MD, Lisbon, Portugal; Lia Lucas Neto, MD, Lisbon, Portugal; Diogo Gonçalves-Ferreira, MD, Lisbon, Portugal; Lucilia Salgado, MD, Lisbon, Portugal; Joao Teixeira, MD, Lisbon, Portugal; Maria Ceu Rueff, PhD, Lisbon, Portugal; Martin Lauterbach, MD, Lisbon, Portugal; Helena Raposo, MD, Lisbon, Portugal; Rui Sequeira, MD, Lisbon, Portugal Introduction: Drug dependence involves motivational and behavioral disturbances such as compulsive drug intake and episodes of intense craving often refractory to all kinds of therapy. Preliminary data from others showed some clinical efficacy of DBS for alcohol and heroin dependence, but it was never shown for cocaine. The main objective of this study is to evaluate the clinical efficacy of DBS to treat refractory cocaine dependence. Methods: A 36 year old man with a long history of refractory cocaine dependence (DSM IV 304.20) was the first patient admitted for surgery of a larger study approved by the local Ethics Committee. The surgical indication was approved by independent psychiatrists of the National Council for Mental Health, after an appropriate informed consent was signed. Bilateral electrodes (3387 Medtronic®) were implanted under local anesthesia to reach, with the same intraparenchimous trajectory on each side, the posterior nucleus accumbens (Acc), bed nucleus of stria terminalis (NST) and middle forebrain bundle (MFB). Intraoperative monopolar stimulation was performed at each contact with 130hz, 150µs pulse width and 1-6 volts amplitude. The electrodes were connected subcutaneously to an Activa PC® pulse generator. No operative morbidity was registered. The post-operative DBS started 5 days after the operation and was kept continuously for 6 months with adjustments of the DBS parameters. It was followed by another 6 months period of randomized DBS. Results: A marked increase of weeks free of consumption (80% versus 40%) with a high percentage of negative analysis (73% versus 17%) for cocaine (primary variables) after surgery was registered. A general reduction in most secondary efficacy variables was also observed (cocaine craving, YBOCS, DDQ, ASIX, and the CGI); no significant adverse events were observed. Conclusions: The preliminary conclusion is that a positive and safe result is achieved with this DBS treatment for refractory cocaine dependence.
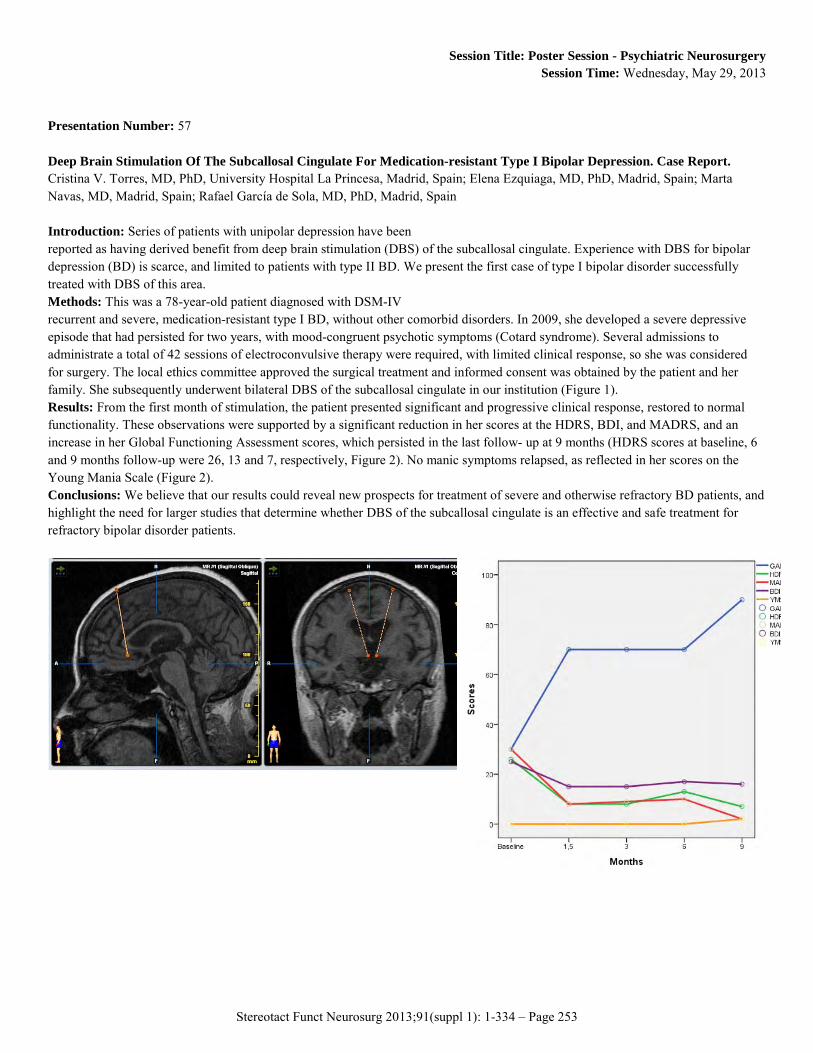
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 253
Session Title: Poster Session - Psychiatric Neurosurgery Session Time: Wednesday, May 29, 2013
Presentation Number: 57 Deep Brain Stimulation Of The Subcallosal Cingulate For Medication-resistant Type I Bipolar Depression. Case Report. Cristina V. Torres, MD, PhD, University Hospital La Princesa, Madrid, Spain; Elena Ezquiaga, MD, PhD, Madrid, Spain; Marta Navas, MD, Madrid, Spain; Rafael García de Sola, MD, PhD, Madrid, Spain Introduction: Series of patients with unipolar depression have been reported as having derived benefit from deep brain stimulation (DBS) of the subcallosal cingulate. Experience with DBS for bipolar depression (BD) is scarce, and limited to patients with type II BD. We present the first case of type I bipolar disorder successfully treated with DBS of this area. Methods: This was a 78-year-old patient diagnosed with DSM-IV recurrent and severe, medication-resistant type I BD, without other comorbid disorders. In 2009, she developed a severe depressive episode that had persisted for two years, with mood-congruent psychotic symptoms (Cotard syndrome). Several admissions to administrate a total of 42 sessions of electroconvulsive therapy were required, with limited clinical response, so she was considered for surgery. The local ethics committee approved the surgical treatment and informed consent was obtained by the patient and her family. She subsequently underwent bilateral DBS of the subcallosal cingulate in our institution (Figure 1). Results: From the first month of stimulation, the patient presented significant and progressive clinical response, restored to normal functionality. These observations were supported by a significant reduction in her scores at the HDRS, BDI, and MADRS, and an increase in her Global Functioning Assessment scores, which persisted in the last follow- up at 9 months (HDRS scores at baseline, 6 and 9 months follow-up were 26, 13 and 7, respectively, Figure 2). No manic symptoms relapsed, as reflected in her scores on the Young Mania Scale (Figure 2). Conclusions: We believe that our results could reveal new prospects for treatment of severe and otherwise refractory BD patients, and highlight the need for larger studies that determine whether DBS of the subcallosal cingulate is an effective and safe treatment for refractory bipolar disorder patients.
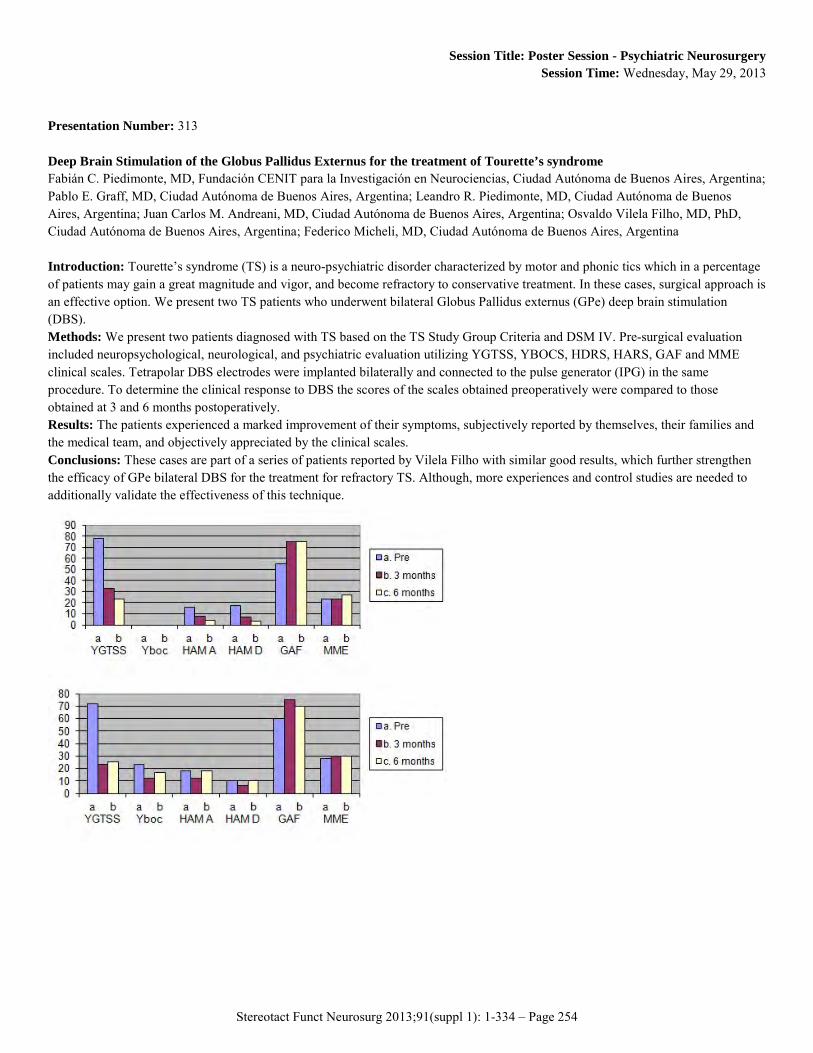
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 254
Session Title: Poster Session - Psychiatric Neurosurgery Session Time: Wednesday, May 29, 2013
Presentation Number: 313 Deep Brain Stimulation of the Globus Pallidus Externus for the treatment of Tourette’s syndrome Fabián C. Piedimonte, MD, Fundación CENIT para la Investigación en Neurociencias, Ciudad Autónoma de Buenos Aires, Argentina; Pablo E. Graff, MD, Ciudad Autónoma de Buenos Aires, Argentina; Leandro R. Piedimonte, MD, Ciudad Autónoma de Buenos Aires, Argentina; Juan Carlos M. Andreani, MD, Ciudad Autónoma de Buenos Aires, Argentina; Osvaldo Vilela Filho, MD, PhD, Ciudad Autónoma de Buenos Aires, Argentina; Federico Micheli, MD, Ciudad Autónoma de Buenos Aires, Argentina Introduction: Tourette’s syndrome (TS) is a neuro-psychiatric disorder characterized by motor and phonic tics which in a percentage of patients may gain a great magnitude and vigor, and become refractory to conservative treatment. In these cases, surgical approach is an effective option. We present two TS patients who underwent bilateral Globus Pallidus externus (GPe) deep brain stimulation (DBS). Methods: We present two patients diagnosed with TS based on the TS Study Group Criteria and DSM IV. Pre-surgical evaluation included neuropsychological, neurological, and psychiatric evaluation utilizing YGTSS, YBOCS, HDRS, HARS, GAF and MME clinical scales. Tetrapolar DBS electrodes were implanted bilaterally and connected to the pulse generator (IPG) in the same procedure. To determine the clinical response to DBS the scores of the scales obtained preoperatively were compared to those obtained at 3 and 6 months postoperatively. Results: The patients experienced a marked improvement of their symptoms, subjectively reported by themselves, their families and the medical team, and objectively appreciated by the clinical scales. Conclusions: These cases are part of a series of patients reported by Vilela Filho with similar good results, which further strengthen the efficacy of GPe bilateral DBS for the treatment for refractory TS. Although, more experiences and control studies are needed to additionally validate the effectiveness of this technique.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 255
Session Title: Poster Session - Psychiatric Neurosurgery Session Time: Wednesday, May 29, 2013
Presentation Number: 342 Nucleus Accumbens Stimulation in Pathological Obesity - Case Report Marek Harat, PhD, Military Clinical Hospital, Bydgoszcz, Poland; Pawel Sokal, MD, Military Clinical Hospital, Bydgoszcz, Poland; Marcin Rudas, MD, Bydgoszcz, Poland; Piotr Zieliński, MD, Bydgoszcz, Poland; Julita Gryz, MD, Bydgoszcz, Poland Background: Obesity is posing great social and health problem in western societies. No behavioral, pharmacological nor surgical treatment as yet is satisfactorily effective. Therefore there is ongoing research on modulation of deep brain activity to diminish the need for food intake. One of the potential treatment methods is deep brain stimulation (DBS). Objectives: One of the targets of DBS in obesity treatment is nucleus accumbens. Methods: We describe the case of 19 years old woman with hypothalamic obesity. She steadily gained weight afer craniopharyngioma tumor surgery. She weighted 151,4 kg before DBS and all of the current non-surgical methods proved to be inneficient. She was treated with implantation of DBS electrode to nucleus accumbens bilaterally. Results were measured with body mass, body mass index, Beck Depression Scale, Wisconsin Card Sorting Test, Trail Making Test and Stroop Color- Word Interference Test. Results: Three months after surgery weight was 132 kg, BMI was 46.2. Neuropsychological test results are intact. Conclusion: The presented case supports the results of other authors as to the succesful treatment of obesity with nucleus accumbens stimulation.
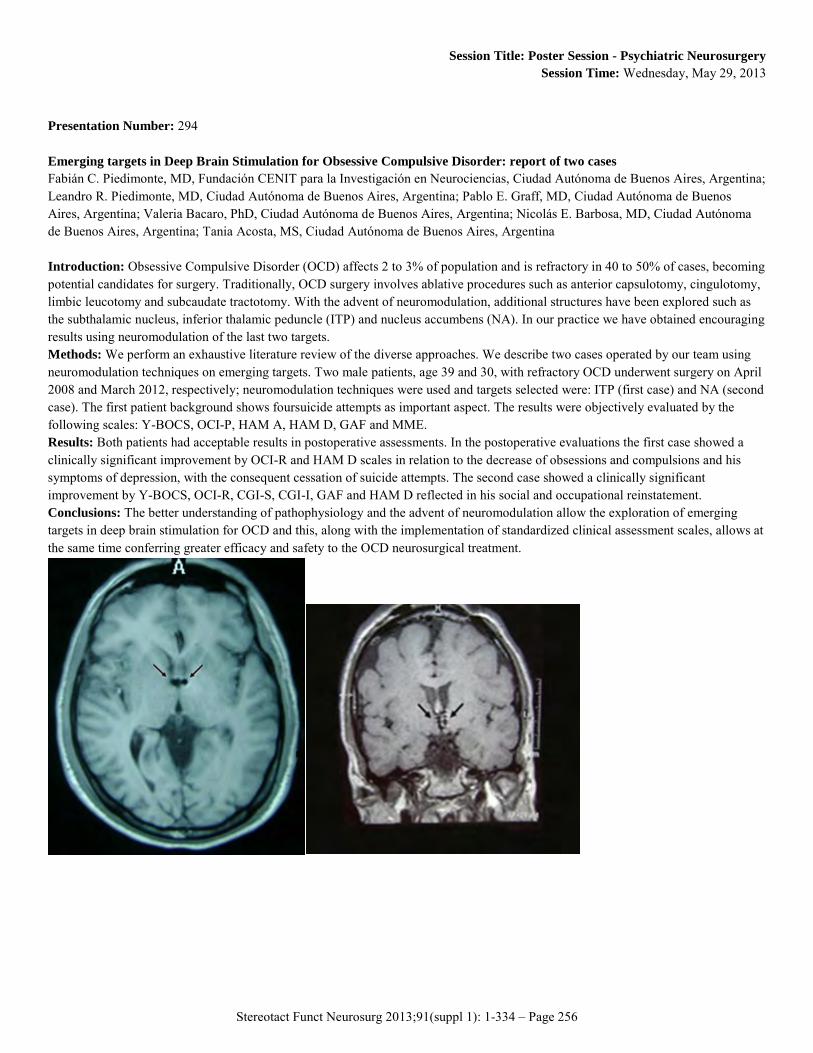
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 256
Session Title: Poster Session - Psychiatric Neurosurgery Session Time: Wednesday, May 29, 2013
Presentation Number: 294 Emerging targets in Deep Brain Stimulation for Obsessive Compulsive Disorder: report of two cases Fabián C. Piedimonte, MD, Fundación CENIT para la Investigación en Neurociencias, Ciudad Autónoma de Buenos Aires, Argentina; Leandro R. Piedimonte, MD, Ciudad Autónoma de Buenos Aires, Argentina; Pablo E. Graff, MD, Ciudad Autónoma de Buenos Aires, Argentina; Valeria Bacaro, PhD, Ciudad Autónoma de Buenos Aires, Argentina; Nicolás E. Barbosa, MD, Ciudad Autónoma de Buenos Aires, Argentina; Tania Acosta, MS, Ciudad Autónoma de Buenos Aires, Argentina Introduction: Obsessive Compulsive Disorder (OCD) affects 2 to 3% of population and is refractory in 40 to 50% of cases, becoming potential candidates for surgery. Traditionally, OCD surgery involves ablative procedures such as anterior capsulotomy, cingulotomy, limbic leucotomy and subcaudate tractotomy. With the advent of neuromodulation, additional structures have been explored such as the subthalamic nucleus, inferior thalamic peduncle (ITP) and nucleus accumbens (NA). In our practice we have obtained encouraging results using neuromodulation of the last two targets. Methods: We perform an exhaustive literature review of the diverse approaches. We describe two cases operated by our team using neuromodulation techniques on emerging targets. Two male patients, age 39 and 30, with refractory OCD underwent surgery on April 2008 and March 2012, respectively; neuromodulation techniques were used and targets selected were: ITP (first case) and NA (second case). The first patient background shows foursuicide attempts as important aspect. The results were objectively evaluated by the following scales: Y-BOCS, OCI-P, HAM A, HAM D, GAF and MME. Results: Both patients had acceptable results in postoperative assessments. In the postoperative evaluations the first case showed a clinically significant improvement by OCI-R and HAM D scales in relation to the decrease of obsessions and compulsions and his symptoms of depression, with the consequent cessation of suicide attempts. The second case showed a clinically significant improvement by Y-BOCS, OCI-R, CGI-S, CGI-I, GAF and HAM D reflected in his social and occupational reinstatement. Conclusions: The better understanding of pathophysiology and the advent of neuromodulation allow the exploration of emerging targets in deep brain stimulation for OCD and this, along with the implementation of standardized clinical assessment scales, allows at the same time conferring greater efficacy and safety to the OCD neurosurgical treatment.
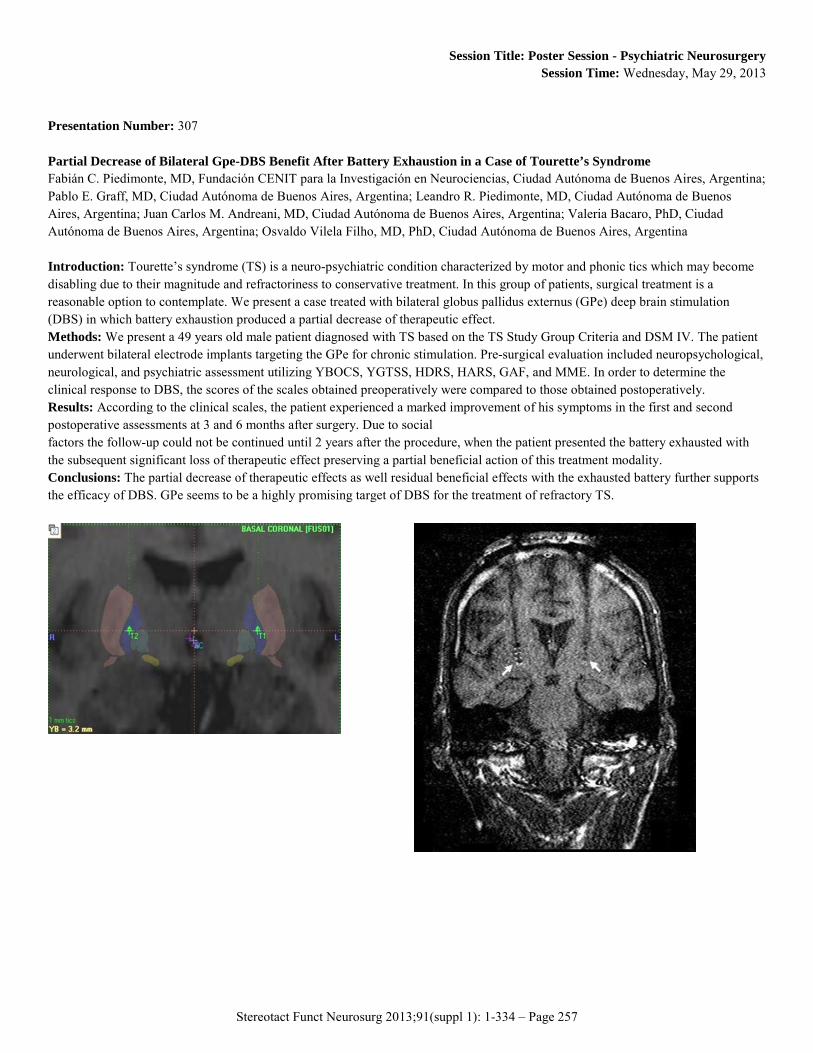
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 257
Session Title: Poster Session - Psychiatric Neurosurgery Session Time: Wednesday, May 29, 2013
Presentation Number: 307 Partial Decrease of Bilateral Gpe-DBS Benefit After Battery Exhaustion in a Case of Tourette’s Syndrome Fabián C. Piedimonte, MD, Fundación CENIT para la Investigación en Neurociencias, Ciudad Autónoma de Buenos Aires, Argentina; Pablo E. Graff, MD, Ciudad Autónoma de Buenos Aires, Argentina; Leandro R. Piedimonte, MD, Ciudad Autónoma de Buenos Aires, Argentina; Juan Carlos M. Andreani, MD, Ciudad Autónoma de Buenos Aires, Argentina; Valeria Bacaro, PhD, Ciudad Autónoma de Buenos Aires, Argentina; Osvaldo Vilela Filho, MD, PhD, Ciudad Autónoma de Buenos Aires, Argentina Introduction: Tourette’s syndrome (TS) is a neuro-psychiatric condition characterized by motor and phonic tics which may become disabling due to their magnitude and refractoriness to conservative treatment. In this group of patients, surgical treatment is a reasonable option to contemplate. We present a case treated with bilateral globus pallidus externus (GPe) deep brain stimulation (DBS) in which battery exhaustion produced a partial decrease of therapeutic effect. Methods: We present a 49 years old male patient diagnosed with TS based on the TS Study Group Criteria and DSM IV. The patient underwent bilateral electrode implants targeting the GPe for chronic stimulation. Pre-surgical evaluation included neuropsychological, neurological, and psychiatric assessment utilizing YBOCS, YGTSS, HDRS, HARS, GAF, and MME. In order to determine the clinical response to DBS, the scores of the scales obtained preoperatively were compared to those obtained postoperatively. Results: According to the clinical scales, the patient experienced a marked improvement of his symptoms in the first and second postoperative assessments at 3 and 6 months after surgery. Due to social factors the follow-up could not be continued until 2 years after the procedure, when the patient presented the battery exhausted with the subsequent significant loss of therapeutic effect preserving a partial beneficial action of this treatment modality. Conclusions: The partial decrease of therapeutic effects as well residual beneficial effects with the exhausted battery further supports the efficacy of DBS. GPe seems to be a highly promising target of DBS for the treatment of refractory TS.
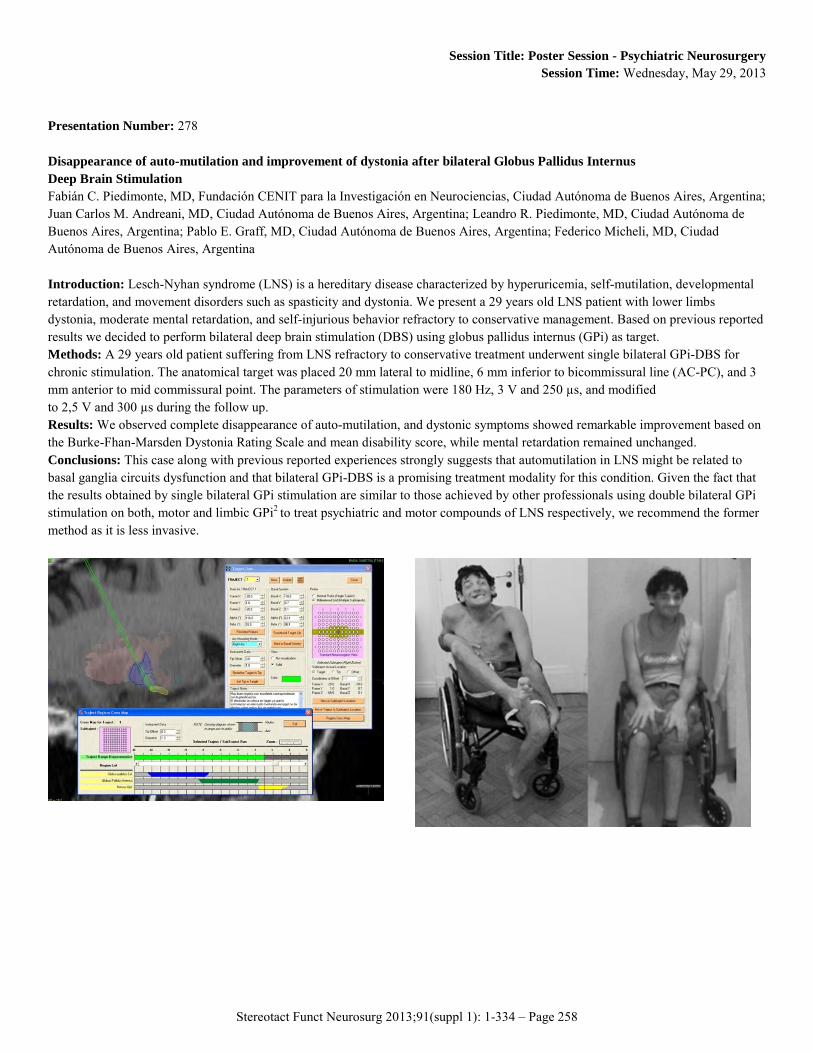
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 258
Session Title: Poster Session - Psychiatric Neurosurgery Session Time: Wednesday, May 29, 2013
Presentation Number: 278 Disappearance of auto-mutilation and improvement of dystonia after bilateral Globus Pallidus Internus Deep Brain Stimulation Fabián C. Piedimonte, MD, Fundación CENIT para la Investigación en Neurociencias, Ciudad Autónoma de Buenos Aires, Argentina; Juan Carlos M. Andreani, MD, Ciudad Autónoma de Buenos Aires, Argentina; Leandro R. Piedimonte, MD, Ciudad Autónoma de Buenos Aires, Argentina; Pablo E. Graff, MD, Ciudad Autónoma de Buenos Aires, Argentina; Federico Micheli, MD, Ciudad Autónoma de Buenos Aires, Argentina Introduction: Lesch-Nyhan syndrome (LNS) is a hereditary disease characterized by hyperuricemia, self-mutilation, developmental retardation, and movement disorders such as spasticity and dystonia. We present a 29 years old LNS patient with lower limbs dystonia, moderate mental retardation, and self-injurious behavior refractory to conservative management. Based on previous reported results we decided to perform bilateral deep brain stimulation (DBS) using globus pallidus internus (GPi) as target. Methods: A 29 years old patient suffering from LNS refractory to conservative treatment underwent single bilateral GPi-DBS for chronic stimulation. The anatomical target was placed 20 mm lateral to midline, 6 mm inferior to bicommissural line (AC-PC), and 3 mm anterior to mid commissural point. The parameters of stimulation were 180 Hz, 3 V and 250 µs, and modified to 2,5 V and 300 µs during the follow up. Results: We observed complete disappearance of auto-mutilation, and dystonic symptoms showed remarkable improvement based on the Burke-Fhan-Marsden Dystonia Rating Scale and mean disability score, while mental retardation remained unchanged. Conclusions: This case along with previous reported experiences strongly suggests that automutilation in LNS might be related to basal ganglia circuits dysfunction and that bilateral GPi-DBS is a promising treatment modality for this condition. Given the fact that the results obtained by single bilateral GPi stimulation are similar to those achieved by other professionals using double bilateral GPi stimulation on both, motor and limbic GPi2 to treat psychiatric and motor compounds of LNS respectively, we recommend the former method as it is less invasive.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 259
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 288 New Insights in the Role of Descending Inhibition in Effects of Spinal Cord Stimulation on Neuropathic Pain: Involvement of Serotonergic Circuitry Bengt Linderoth, MD PhD, Dept Clin Neurosci,Karolinska Institutet, Stockholm, Sweden; Zhiyang Song, MD PhD, Dept Clin Neurosci. Karolinska Institutet Sthlm, Sweden; Antti Perttovaara, MD PhD, Dept Physiology, Univ Helsinki., Helsinki, Finland; Nayef Saade, MD PhD, Dept. Anatomy, Cell Biol. & Physiol., AUB, Beirut, Lebanon; Björn A. Meyerson, MD PhD, Dept Clin Neurosci., Karolinska InstituteStockholm, Sweden Introduction: During the last decades research on the mechanisms of spinal cord stimulation (SCS) has mainly focused on segmental spinal mechanisms activated antidromically by current applied to the dorsal columns (DCs). Several segmental inhibitory circuits have been described; GABAergic, cholinergic, adenosinergic etc. Lately, however, studies of the supraspinal circuitry activated by SCS have progressed considerably. Methods: These studies have been carried out on various animal models of neuropathic pain. The modifications of responses after the application of SCS via chronically implanted miniature electrodes have been studied in animals with with single or dual stimulation systems located at the DC nuclei and on the lumbar cord, in rats with DC lesions or intact. Microelectrode recordings from different brain stem areas have been performed as well as the manipulation of the activity in these regions by administration of different drugs i.p., to the spinal i.t.space, or via indwelling chronic brain stem cannulas. Results: The studies illustrate that there is a participation of both the rostroventromedial medulla via descending serotonergic axons to the spinal cord and the locus coeruleus area. These areas display different local activation patterns during SCS and the analyses demonstrate a complex participation of both the spinal and brainstem circuitries in the effects of SCS. Recent studies suggest that the activation of the 5-HT2, 5-HT3 and 5-HT4 receptors plays an important role in SCS-induced relief of neuropathic pain. The activation of 5-HT3 receptors appears to operate via a spinal GABAergic link. Conclusions: SCS activates both segmental and suprasegmental mechanisms, as well, and the activated circuitry in the brain stem interacts with the segmental interneurons to exert inhibitory effects on hyperexcited secondary cells in the dorsal horns. The supraspinal activation seems in fact to be equally important for the effect as the spinal segmental.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 260
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 368 Supraspinal Mechanisms in the Mode of Action of Spinal Cord Stimulation - Possible Involvement of Locus Coeruleus Bjorn A. Meyerson, MD, PhD, Karolinska Institutet, Stockholm, Sweden; Zhiyang Song, MD,PhD, Stockholm, Sweden; Antti Pertovaara, MD, PhD, Helsinki, Finland; Bengt Linderoth, MD, PhD, Stockholm, Sweden Introduction: The neurobiological mechanisms of spinal cord stimulation (SCS) when applied for neuropathic pain are still incompletely known. Experimental studies performed on animal models (rat) of such pain have focused on spinal circuitries but there is mounting evidence that also supraspinal mechanisms play an important role. The present study aims at exploring the possible role of the locus coeruleus (LC) and its spinal descending pain controlling system. Methods: The activation of a miniature SCS implanted in spared nerve injury (SNI) rats often results in an attenuation of the signs of neuropathy, i.e. hypersensitivity to mechanical and thermal stimuli. Microrecordings were performed in the LC during SCS in both SCS responding and non-responding animals, and the content of noradrenaline in the spinal cord was analyzed (ELISA). In awake SCS responding rats lidocaine was microinjected in the LC via an implanted cannula animals, and the possible effect on the SCS antihypersensitivity action was assessed following intrathecal administration of α1 and 2 receptor antagonists. Results: SCS produced a prominent increase in the neuronal discharge in the LC but only in SCS responding animals. In the responding animals, SCS was associated also with increased c-fos cell expression in the LC. The noradrenaline content assessed in the dorsal quadrant of the spinal cord ipsilateral to the nerve injury was unchanged immediately following a period of SCS in all three groups, responding, non-responding and intact animals. In awake animals, lidocaine block of the LC or block of descending noradrenergic system by intrathecal administration of α1 and 2 receptor antagonists had no influence on the SCS hypersensitivity suppressive effect. Conclusions: Our experimental data indicate that activation of the LC is associated with the pain relieving effect of SCS but provide no support for the direct involvement of the spinally projecting noradrenergic pain controlling system.
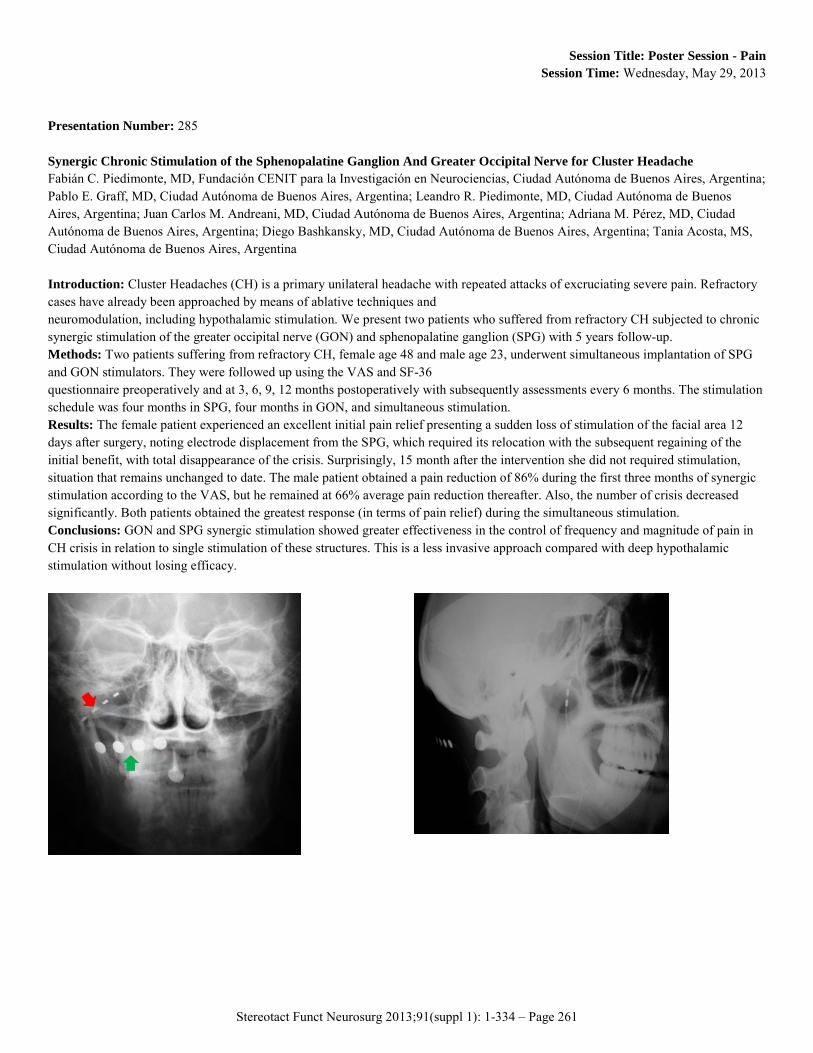
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 261
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 285 Synergic Chronic Stimulation of the Sphenopalatine Ganglion And Greater Occipital Nerve for Cluster Headache Fabián C. Piedimonte, MD, Fundación CENIT para la Investigación en Neurociencias, Ciudad Autónoma de Buenos Aires, Argentina; Pablo E. Graff, MD, Ciudad Autónoma de Buenos Aires, Argentina; Leandro R. Piedimonte, MD, Ciudad Autónoma de Buenos Aires, Argentina; Juan Carlos M. Andreani, MD, Ciudad Autónoma de Buenos Aires, Argentina; Adriana M. Pérez, MD, Ciudad Autónoma de Buenos Aires, Argentina; Diego Bashkansky, MD, Ciudad Autónoma de Buenos Aires, Argentina; Tania Acosta, MS, Ciudad Autónoma de Buenos Aires, Argentina Introduction: Cluster Headaches (CH) is a primary unilateral headache with repeated attacks of excruciating severe pain. Refractory cases have already been approached by means of ablative techniques and neuromodulation, including hypothalamic stimulation. We present two patients who suffered from refractory CH subjected to chronic synergic stimulation of the greater occipital nerve (GON) and sphenopalatine ganglion (SPG) with 5 years follow-up. Methods: Two patients suffering from refractory CH, female age 48 and male age 23, underwent simultaneous implantation of SPG and GON stimulators. They were followed up using the VAS and SF-36 questionnaire preoperatively and at 3, 6, 9, 12 months postoperatively with subsequently assessments every 6 months. The stimulation schedule was four months in SPG, four months in GON, and simultaneous stimulation. Results: The female patient experienced an excellent initial pain relief presenting a sudden loss of stimulation of the facial area 12 days after surgery, noting electrode displacement from the SPG, which required its relocation with the subsequent regaining of the initial benefit, with total disappearance of the crisis. Surprisingly, 15 month after the intervention she did not required stimulation, situation that remains unchanged to date. The male patient obtained a pain reduction of 86% during the first three months of synergic stimulation according to the VAS, but he remained at 66% average pain reduction thereafter. Also, the number of crisis decreased significantly. Both patients obtained the greatest response (in terms of pain relief) during the simultaneous stimulation. Conclusions: GON and SPG synergic stimulation showed greater effectiveness in the control of frequency and magnitude of pain in CH crisis in relation to single stimulation of these structures. This is a less invasive approach compared with deep hypothalamic stimulation without losing efficacy.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 262
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 159 Delayed Recurrence Of Hemifacial Spasm After Successful Microvascular Decompression: Follow-up Results At Least 5 Years After Surgery Won Seok Chang, MD, Yonsei University College of Medicine, Seoul, Korea, Republic of; Young Cheol Na, MD, Seoul, Korea, Republic of; Ji Hee Kim, MD, Seoul, Korea, Republic of; Won Hee Lee, MD, Seoul, Korea, Republic of; Eun Jeong Kweon, Seoul, Korea, Republic of; Hyun Ho Jung, MD, Seoul, Korea, Republic of; Jin Woo Chang, MD,PhD, Seoul, Korea, Republic of Introduction: Microvascular decompression (MVD) for hemifacial spasm (HFS) is regarded as the gold-standard treatment due to its efficacy and durability. However, some patients still suffer from delayed recurrence after initially successful MVD. In this study, we describe our clinical experience in a single institute following up initially successful MVD for HFS 5 or more years after surgery. We analyzed the probability of, risk/predisposing factors for, and timing of delayed recurrence. Methods: We retrospectively reviewed data from 587 patients meeting our inclusion criteria who underwent MVD for HFS from March, 1999, to June 2006. We evaluated the time-dependent probability of recurrence and factors affecting delayed recurrence and time of recurrence. Results: The probability of delayed recurrence was 1.0, 1.7, and 2.9% at 1 year, 2 years, and 5 years after surgery, respectively. Mean time to recurrence was 153.1 months (95% confidence interval [151.4-154.9]). The probability of late recurrence was increased in patients with co-morbid arterial hypertension (p=0.036). However, there was a trend towards an association of delayed recurrence with co-existence of young age, male gender, vein or VA offender, and experience of transient facial weakness. Conclusions: Delayed recurrence of HFS after initially successful MVD is rare; however, there are patients who experience delayed recurrence more than 2 years after MVD, even until 5 years after MVD. Our results suggest that arterial hypertension contributes to late recurrence. We did not find a statistically significant relationship between recurrence and other putative risk/predisposing factors.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 263
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 158 Microneurovascular Decompression In Patients With Hemifacial Spasm Caused By Vascular Compression Of Facial Nerve At Cisternal Portion Young Goo Kim, MD, Yonsei University College of Medicine, Seoul, Korea, Republic of; Ji Hee Kim, MD, Seoul, Korea, Republic of; Young Cheol Na, MD, Seoul, Korea, Republic of; Won Hee Lee, MD, Seoul, Korea, Republic of; Sang Keum Park, Seoul, Korea, Republic of; Won Seok Chang, MD, Seoul, Korea, Republic of; Hyun Ho Jung, MD, Seoul, Korea, Republic of; Jin Woo Chang, MD,PhD, Seoul, Korea, Republic of Introduction: Hemifacial spasm is commonly caused by arterial compression of the facial nerve. Although vascular compression usually occurs at the facial nerve exit zone, in some cases, the facial nerve is compressed more distally. We analyzed the clinical outcome of microneurovascular decompression in patients with hemifacial spasm caused by either distal or proximal compression. Methods: From September 1978 to March 2009, 2137 patients underwent microneurovascular decompression for hemifacial spasm due to vascular compression of the facial nerve, including 2022 patients (94.6%) with proximal compression, 101 patients (4.7%) with both proximal and distal (mixed) compression, and 14 patients (0.7%) with only distal compression. Results: Complete remission of facial spasm occurred in 10 of 14 patients (71.4%) with compression of the cisternal portion, compared with 1773 of 2022 patient (87.7%) with proximal compression (p=0.08) and 87 of 101 patients (86.1%) with mixed compression (p=0.23). Permanent facial weakness occurred in one patient (7.1%) with compression of the cisternal portion, 18 patients (0.9%) with proximal compression, and one patient (1.0%) with mixed compression. Permanent hearing loss occurred in no patients with compression of the cisternal portion, 29 patients (1.4%) with proximal compression, and three patients (3.0%) with mixed compression. Conclusions: Outcomes after microneurovascular decompression for hemifacial spasm with compression of the cisternal portion were not statistically different than with proximal compression of the facial nerve. When the clinical diagnosis of hemifacial spasm is confirmed and vascular compression is seen only in the cisternal portion of the facial nerve, microneurovascular decompression for these patients provides outcomes similar to those with proximal compression of the facial nerve.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 264
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 318 Two birds, One stone: Single Electrode Dual Target Stimulation for the Treatment of Phantom Limb Pain Hugh P. Sims-Williams, MBChB MRCS, North Bristol NHS Trust (Frenchay), Bristol, United Kingdom; Wissam R. Selbi, PhD MRCS, Bristol, United Kingdom; Shazia Javed, MBBS MRCS, Bristol, United Kingdom; Anthony E. Pickering, PhD FRCA, Bristol, United Kingdom; Nik K. Patel, MD FRCS(SN), Bristol, United Kingdom Introduction: Phantom Limb Pain (PLP) occurs in 55-85% of amputees, producing significant morbidity and societal cost. DBS can offer long term success (>50% improvement) in the majority of patients with PLP(1). Low frequency stimulation of Peri-Ventricular Gray / Peri-Aqueductal Gray (PVG/PAG) may modulate descending opioidergic pain pathways, and high frequency inhibitory stimulation of Parafascicular (Pf) complex may interrupt the affective pain pathways to anterior cingulate cortex via paleospinothalamic tract(2). Previously using two generators to stimulate PVG/PAG and Pf at respective frequencies we have observed a synergistic analgesic effect. We describe successful DBS treatment of a young woman with PLP using a single electrode and generator. Methods: DBS was performed using our MRI directed method with implantable guide tubes under general anaesthesia(3). The trajectory and entry point were chosen so that the electrode contacts passed through Pf proximally and PVG/PAG distally. The DBS Vercise generator (Boston Scientific) enables duel frequency: PVG/PAG was optimally stimulated with 10Hz at contacts 3- and 4-, while Pf with 132Hz at contact 8-. Results: PVG/PAG stimulation produced warmth in the phantom limb resulting in complete resolution of her cold pain. Pf stimulation resulted in telescoping of the phantom limb from its previously flexed contracted position, and pain and amputation stump allodynia improved by 50%. Battery reserve was 95% after 1-week usage, requiring 10 minutes to recharge. Conclusions: Combined use of PVG/PAG and Pf provided a superior result to either individual target alone. Technological advancement allows for dual frequency current generation within a single electrode saving time, cost and reducing risk of complications. 1. Bittar et al. DBS for pain relief: a meta-analysis. J Clin Neurosci. 2005;12(5): 515-9. 2. Weigel et al. Centre Median-Parafascicular Complex and Pain Control. Stereotact Funct Neurosurg. 2004;82: 115-126 3. Patel et al. Magnetic resonance imaging-directed method for functional neurosurgery using implantable guide tubes. Neurosurgery. 2007;61(5Suppl2): 358-65.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 265
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 254 Peripheral Nerve Stimulation For Neuropathic Pain Caused By Leprosy Tiago S. Freitas, Brasília University Hospital, Brasília, Brazil; Oswaldo Neto, Brasília, Brazil; Iruena Kessler, Brasília, Brazil Introduction: Leprosy is an infectious disease that affects mainly the skin and peripheral nervous system. Associated chronic painful neuritis causes considerable functional limitation, and its treatment may involve surgical decompression in cases resistant to conservative treatment. Although considered an excellent option, some patients persist with neuropathic pain after surgery. This study focuses on the use of peripheral nerve stimulation in management of patients previously submitted to all available treatments for chronic leprous neuropathy. Methods: 15 leprosy patients with chronic neuropathic pain irresponsive to medication and surgical decompression were selected for a trial implant. All patients underwent prior testing for 7 days and were assessed with Visual Analogic Scale (VAS) and neuropathic pain scale (NPS). Those with at least 50% scale improvement received a permanent device. Follow-up evaluated VAS and NPS at 7 days, 1 month, 3 months and 6 months post-procedure. Results: 8 patients received a permanent device. Among these, 6 patients (75%) showed at least a 50% improvement in VAS and NPS while 2 patients showed a 30% scale improvement. All improvements maintained during 6 months follow-up. There were 2 lead migration and no infection Conclusion: Leprosy remains a public health problem in developing countries and is a major cause of peripheral neuropathy worldwide. Furthermore, it is responsible for serious limitations to patients despite treatment exhaustion. Peripheral nerve stimulation is an important additional tool in management of chronic neuropathic pain secondary to leprosy. Longer follow-up and a greater number of patients are necessary to confirm its potential benefit
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 266
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 230 Characteristics And Responsiveness Of Patients With Post-traumatic Stress Disorder And Chronic Pain. Is Neuroaugmentation Response Adequate? Luiz C. Pereira, PhD, Neurofuncional DF, Brasilia, Brazil; Valeria Patricia Araújo, Neurofuncional DF, Brazil; Igor Campbell Borges, HBDF, Brazil Introduction: Many studies report high comorbidity for Chronic Pain (CP) and posttraumatic stress disorder(PTSD), but research devoted to the efficacy of neuromodulatory treatment is minimal. This study aims to evaluate the characteristics of those patients and the responsiveness to surgical interventions. Methods: We reviewed all records of a private neurology/neurosurgery clinic in Brasilia, for a 10 year period. Results: Among 8780 patients 3933 reported pain as a major symptom,682(17,3%) as disabling,231(5,8%) as intolerable, but only 42 (1%) needed neuromodulatory devices. PTSD was reported to be associated to CP in 29 patients(0,7%), 13 resulting from significant sexual abuse(SA), 5 from severe non-sexual psychological trauma(NSPT) and 11 after significant life-threatening trauma(LTT). The distribution of reported worst pain sites for SA, NSPT and LTT were respectively: 4, 2 and 3 as facial or head pain; 3, 5 and 4 as spinal pain; 7, 2 and 7 as segmental pain. The CP PTSD association set comprised of a clinical group (14 cases) and an intervention group (15 cases). For the clinical group(3 men) mean age was 38,6 years, time from pain to first consultation 6,4 years. As a result pain control was not achieved for the vast majority. For the intervention group(4 men) mean age was 46,7 years, time from pain to first consultation 4,9 years. Neuromodulation was the preferred therapy for this group: 8 spinal cord stimulators(SCS), 3 temporary SCS, 1 intrathecal morphine pump, 2 spinal blocks versus one radiofrequency lesion. All implanted patients referred at least 50% relief of pain (2 reported > 80% relief). All surgical cases were followed to this date. Surgical complications: 2 electrode breakages and 1 generator failure. Clinical complications: 1 suicide. Conclusion: Neuromodulation seems suitable as a pain therapy for selected CP PTSD patients. The responsiveness seams equal to other pain groups. Uninterrupted psychiatric treatment is obligatory.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 267
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 216 Possible Reason For The Loss Of Effectivity Of Motor Cortex Stimulation Wilhelm E. Eisner, Prof.,MD, Medical University Innsbruck, Austria, Innsbruck, Austria; Thomas Fiegele, PhD, Innsbruck, Austria Introduction: Over 300 cases reported in the medical literature since 1991 indicate that Motor Cortex Stimulation (MCS) using 4 or more contact electrode paddles is effective for the treatment of neuropathic pain, in particular for central post-stroke pain (CPSP) and trigeminal neuropathic pain (TGN) /facial pain. Methods: We experienced in 8 patients a reduction in effectivity of treatment after two years of treatment. Some patient could life with that because they had a stable amount of pain reduction after two years of treatment and some therapeutic effect but reduced in all possible settings. The therapeutic effect got reduced slowly following a stable period of effectvity of 18 months. In two patients the therapeutic effect was reduced tramatically. We offered both patients DBS for neuropathic pain therapy. One patient wanted the stimulator which was almost empty to be removed and for the moment no further therapy. Two patients had such a worsened situation that they were willing to suicide. We offered DBS of the thalamus and the capsula interna. For performing a stereotactic planning MRI for DBS we had to remove the electrode. Results: We removed the system by recraniotomy the patient. After removing the resume round electrode we found scare tissue between dura and electrode. After removing the scare tissue we discovered a calcified plate. Now we knew why we had no stimulation anymore despite of full integrety of the stimulation system. Conclusions: In the seventies we used electric therapy for not good healing fractures with some effectivity. In a few patients with surgical spinal chord electrodes we discovered spinal stenosis in the area of the electrode? We did not have these findings in the percutaneous electrodes at all?!
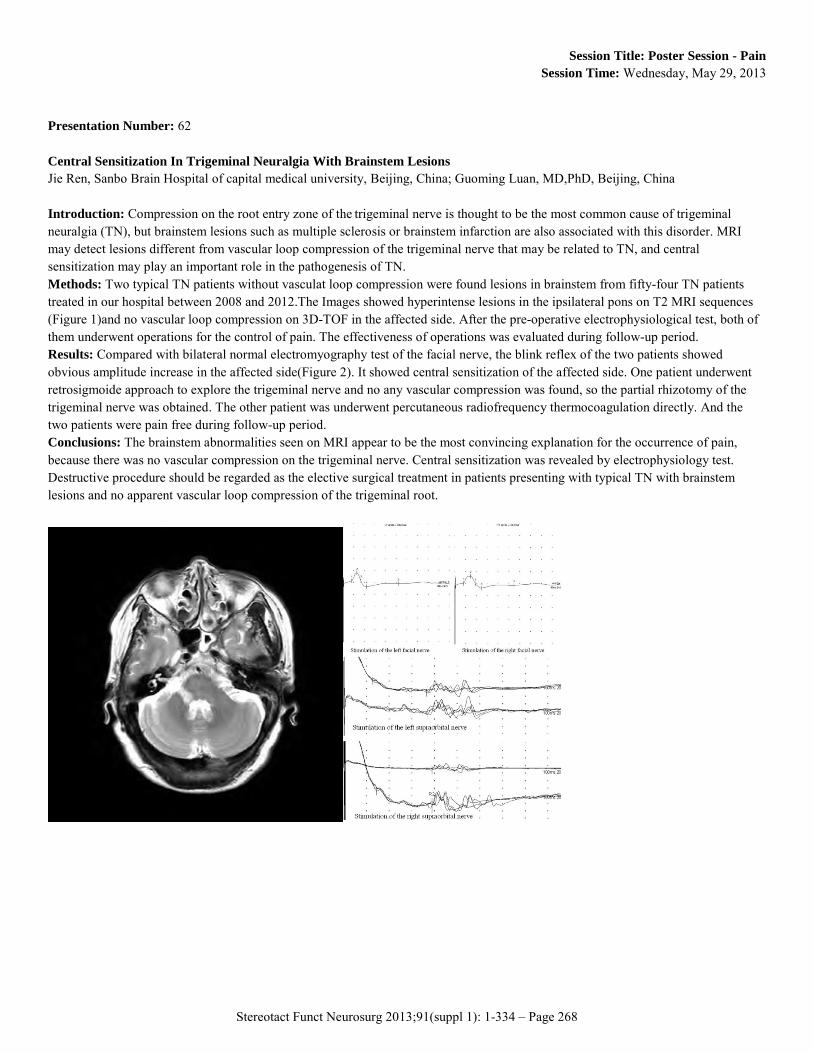
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 268
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 62 Central Sensitization In Trigeminal Neuralgia With Brainstem Lesions Jie Ren, Sanbo Brain Hospital of capital medical university, Beijing, China; Guoming Luan, MD,PhD, Beijing, China Introduction: Compression on the root entry zone of the trigeminal nerve is thought to be the most common cause of trigeminal neuralgia (TN), but brainstem lesions such as multiple sclerosis or brainstem infarction are also associated with this disorder. MRI may detect lesions different from vascular loop compression of the trigeminal nerve that may be related to TN, and central sensitization may play an important role in the pathogenesis of TN. Methods: Two typical TN patients without vasculat loop compression were found lesions in brainstem from fifty-four TN patients treated in our hospital between 2008 and 2012.The Images showed hyperintense lesions in the ipsilateral pons on T2 MRI sequences (Figure 1)and no vascular loop compression on 3D-TOF in the affected side. After the pre-operative electrophysiological test, both of them underwent operations for the control of pain. The effectiveness of operations was evaluated during follow-up period. Results: Compared with bilateral normal electromyography test of the facial nerve, the blink reflex of the two patients showed obvious amplitude increase in the affected side(Figure 2). It showed central sensitization of the affected side. One patient underwent retrosigmoide approach to explore the trigeminal nerve and no any vascular compression was found, so the partial rhizotomy of the trigeminal nerve was obtained. The other patient was underwent percutaneous radiofrequency thermocoagulation directly. And the two patients were pain free during follow-up period. Conclusions: The brainstem abnormalities seen on MRI appear to be the most convincing explanation for the occurrence of pain, because there was no vascular compression on the trigeminal nerve. Central sensitization was revealed by electrophysiology test. Destructive procedure should be regarded as the elective surgical treatment in patients presenting with typical TN with brainstem lesions and no apparent vascular loop compression of the trigeminal root.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 269
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 310 Severe And Disabling Nonspecific Low Back Pain Treated By Concomitant Spinal Cord Stimulation And PVG PAG Deep Brain Stimulation, A Case Report. Valeria P. Araújo, Neurofuncional DF, Brasilia, Brazil; Luiz C M Pereira, PhD, Neurofuncional DF, Brazil; Igor Campbell Borges, HBDF, Brazil; Introduction: Chronic Low Back Pain (CLBP) remains an important health problem. Nonspecific Low Back Pain (NSLBP) comprises a subgroup in which history and physical examination does not correlate to significant radiological abnormalities. Disabling NSLBP may occur and become a major issue. Patients may be considered as psychosomatic or psychogenic. Fortunately refractory NSLBP is rare and, in those cases, well-established anatomical targets for chronic stimulation may be applied. Regarding CLBP, stimulation of the dorsal columns and central gray matter areas has been reported for decades, as treatment options. Methods: This is the first literature report of chronic stimulation of the periventricular gray matter (PVG) and periaquedutal gray matter (PAG), simultaneous to a T10 Spinal Cord Stimulation, for the treatment of NSLBP. Results: a female patient, 34 years old, sleeked neurosurgical advice after unsuccessful 9 year treatment for NSLBP, by pain clinics and pain doctors. She had been submitted to adequate prolonged multidisciplinary treatments including physiotherapy and various rehabilitation methods, psychotherapy and psychiatric treatment, rational pain pharmacotherapy ( and opioid use), prolonged acupuncture, multiple spinal and myofascial blocks. Reduced quality of life and independence were major issues. For the last 8 years multidisciplinary treatments were maintained and various neurosurgical interventions tested: Lumbar radicular blocks and facet rhizotomies did not help; intermittent, transitory ant prolonged epidural morphine injections helped less than 40%, transitorily and caused significant side effects; Spinal cord stimulation decreased 30 % of pain; Bilateral deep Brain Stimulation (DBS) of PVG and PAG decreased 30 to 40% of pain. Only the association of DBS and SCS decreased pain by 70%. The reported satisfaction was very high, the patient returned to School and social activities, but no medications or therapies could be reduced. Conclusions: This is the first reported case of concomitant DBS and SCS for NSLBP.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 270
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 393 Prevention Of Cerebrospinal Fluid Leakage After Microsurgical DREZotomy Without Use Of Fibrin Glue Toshiyuki SASAKI, MD, PhD, Tokyo Woman's Medical University, Tokyo, Japan Introduction: Cerebrospinal fluid (CSF) leakage is a common complication after intradural spinal surgery. Becausepersistent CSF leakage puts patients under significant risk of poor wound healing, meningitis and arachnoiditis, meticulous wound closure is important. Spinal surgery has a higher incidence of CSF leakage because of the high intradural hydrostatic pressure. Numerous methods have been developed to prevent CSF leakage after spinal surgery including use of fibrin glue, polyglycolic acid mesh and vicryl mesh. Our experience to prevent CSF leakage with 375 patients who underwent intradural spinal surgery is reported here. There was significant advantage in the incidence of CSF leaks comparing previous reports. Methods: Three hundred and seventy-five patients underwent intradural spinal surgery between 2001 and 2012 in Tokyo Woman’s Medical University. One hundred and ten patients underwent selective dorsal rhizotomy, 99 underwent selective peripheral denervation, 89 underwent removal of intradural spinal tumor, 55 underwent Microsurgical DREZotomy, 5 were treated for tethered cord syndrome, 15 for arteriovenous fisturas and two were treated for adhesive arachnoiditis. Dural closure was performed by 4-0 nonabsorbable continuous suture. We performed 4 or 5 layers closure and we sew each layer on underneath structure. Meticulous closure is important at both ends of the incision. Each stitch was left until we finish closing the layer to confirm the gap of suture. We didn’t use fibrin glue or polyglycolic acid mesh. Results: No symptomatic CSF leakage and no infection were marked in any case. Several cases showed postoperative pseudomeningocele but all cases have no symptoms. Conclusions: There was no CSF leakage in our series of 375 intradural spinal surgery. Watertight dural closure is not essential if muscles and subcutaneous tissues are closed meticulously. Fibrin glue is not indispensable to prevent CSF leakage. Extradural CSF collection does not cause of persistent complications.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 271
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 314 Electrical Stimulation of Periventricular/Periaqueductal Gray And Posterolateral Thalamic Region In Patient With Post Stroke Chronic Central Pain. Katarzyna Obszanska, Neurosurgery and Pediatric Neurisurgery Department of the Medical University in Lublin, Lublin, Poland; Marcin Tutaj, MD, Jagiellonian University in Krakow, Poland; Agnieszka Cegiełkowska-Bednarczyk, MD, Neurosurgery Department Medical University Lublin, Poland; Tomasz Trojanowski, MD, Neurosurgery Department Medical University Lublin, Poland Introduction: In the study we present reduction of pain and thalamic tremor with stimulation of periventricular/ periaqueductal (PVG/PAG) and posterolateral (VPL) for pain in the patient with post stroke chronic central pain. PVG/PAG can modulate pain perception via the descending pathway to the spinal dorsal horn and via ascending pathway to the thalamus. Tremor rarely occurs as a consequence of thalamic lesion. Posterolateral thalamic region may be responsible for delayed tremor. Methods: We present a patient who experienced ischemic stroke within the posterolateral part of the left hypothalamus with subsequent severe burning pain localized in right upper limb, predominantly within the hand and the thalamic tremor both postural and present at rest which occurred 4 months after stroke. The patient was offered the implantation of electrodes to (PVG/PAG)/as well as implantation an electrode to (VPL). Microelectrode recording and macrostimulation were all used in the process of target localization, apart from defining the exact target for stimulation by the stereotactic MRI. Correct target localization in the PVG/PAG and VPL was conformed when a 50Hz stimulation elicited paresthesia in the contralateral limb. Results: We achieved reduction of pain after surgery when we switch on electrode in PVG/PAG and VPL. Pain intensity was assessed using the McGill-Melzack visual analogue scale for 7,9 points before the stimulation and 4.9 points during stimulation. Additionally when we switch on PVL's electrode, the next day we observed significant alleviation of the patient’s thalamic tremor in the hand. Conclusions: Stimulation of PVG/PAG can modulate pain perception by inhibition of the sensory thalamus. Since PVL and VIM are located in close vicinity, stimulation in the PVL could either spread to the VIM.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 272
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 177 Spinal Cord Stimulation for Refractory Angina Pectoris Vladimir Shabalov, Scientific Research Institute of Neurosurgery (Burdenko), Moscow, Russian Federation; Vladimir Murtazin, Novosibirsk scientific research institute of circulation pathology n.a. academician E.N. Meshalkin, Novosibirsk, Russian Federation; Andrei Ashurkov, Novosibirsk, Russian Federation; Abdirakman Duishobaev, Novosibirsk, Russian Federation; Alexei Krivoshapkin, Novosibirsk, Russian Federation Introduction: Refractory angina pectoris is a chronic condition with the severe chest pain, caused by coronary artery disease, that cannot be relieved by the coronary intervention, coronary artery bypass grafting, and best medical treatment. Spinal cord stimulation (SCS) is an electrical neuromodulation therapy that appears to be an effective and safe treatment option for this specific group of patients. This is the first report of SCS to treat angina pectoris in Russia. Methods: We had applied SCS in 4 patients with refractory angina pectoris. The first procedure was a trial neurostimulation to reveal the efficacy of pain relief before the second one to implant the permanent neurostimulation system. Prone position and local anesthesia were used. A 14-gauge Tuohy needle was inserted in the Th7-Th8 interlaminar space under fluoroscopic guidance. The epidural space was identified using a loss-of-resistance technique. The Octrode lead 3086 (St. Jude Medical Inc., Minnesota, USA) was inserted in the epidural space at the C7-Th1 level. The pulse generator Eon С was implanted into the subcutaneous space of the left upper external quadrant of the buttock. Myocardium perfusion scintigraphy (MPS) was performed on admission and the 7th day after procedure. The visual analogue scale (VAS) was used to assess the degree of pain both in rest and physical activity. Results: The patients showed 7,25±0,48 points according VAS before the procedure. After surgery they described angina pectoris relief down to 0,75±0,48 points (p<0,05). All the patients demonstrated the rise of tolerance to the physical activity. MPS detected the increase in coronary reserve from 9 to 3 prearranged units. There were no any procedural complications. Conclusions: Our experience demonstrates that SCS is a minimally invasive technique to reduce the pain and improve quality of life with coronary reserve enhancement in the patients with refractory angina pectoris.
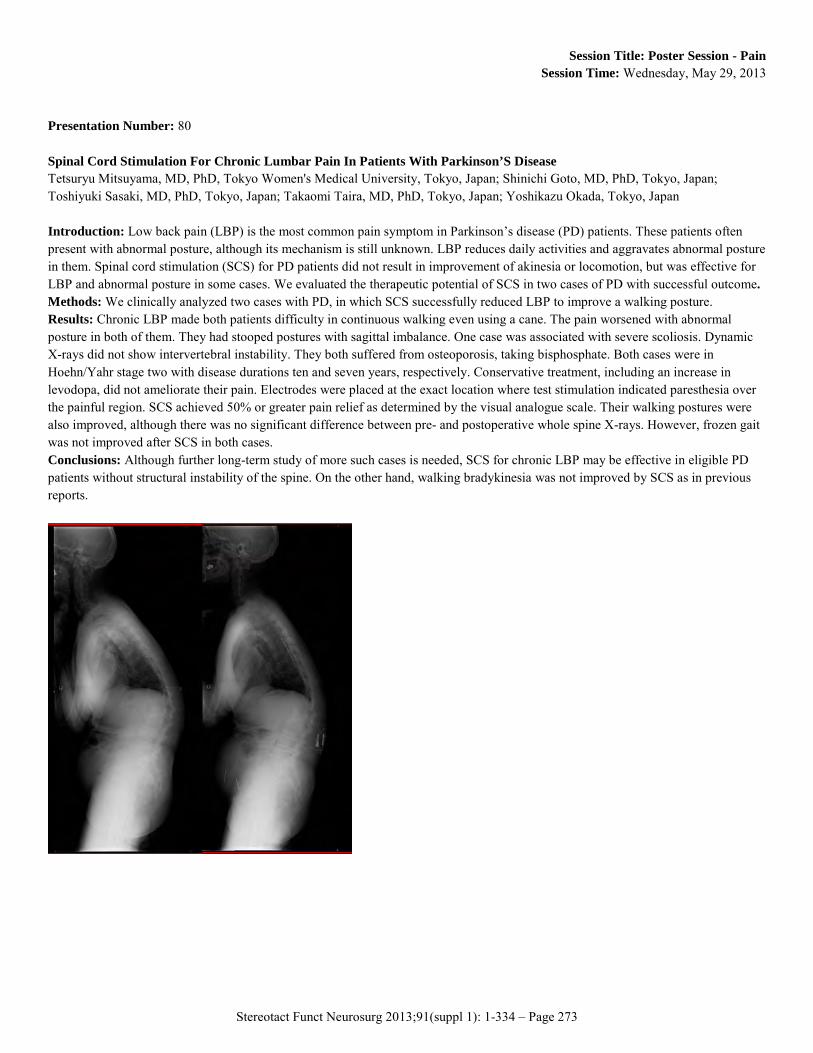
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 273
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 80 Spinal Cord Stimulation For Chronic Lumbar Pain In Patients With Parkinson’S Disease Tetsuryu Mitsuyama, MD, PhD, Tokyo Women's Medical University, Tokyo, Japan; Shinichi Goto, MD, PhD, Tokyo, Japan; Toshiyuki Sasaki, MD, PhD, Tokyo, Japan; Takaomi Taira, MD, PhD, Tokyo, Japan; Yoshikazu Okada, Tokyo, Japan Introduction: Low back pain (LBP) is the most common pain symptom in Parkinson’s disease (PD) patients. These patients often present with abnormal posture, although its mechanism is still unknown. LBP reduces daily activities and aggravates abnormal posture in them. Spinal cord stimulation (SCS) for PD patients did not result in improvement of akinesia or locomotion, but was effective for LBP and abnormal posture in some cases. We evaluated the therapeutic potential of SCS in two cases of PD with successful outcome. Methods: We clinically analyzed two cases with PD, in which SCS successfully reduced LBP to improve a walking posture. Results: Chronic LBP made both patients difficulty in continuous walking even using a cane. The pain worsened with abnormal posture in both of them. They had stooped postures with sagittal imbalance. One case was associated with severe scoliosis. Dynamic X-rays did not show intervertebral instability. They both suffered from osteoporosis, taking bisphosphate. Both cases were in Hoehn/Yahr stage two with disease durations ten and seven years, respectively. Conservative treatment, including an increase in levodopa, did not ameliorate their pain. Electrodes were placed at the exact location where test stimulation indicated paresthesia over the painful region. SCS achieved 50% or greater pain relief as determined by the visual analogue scale. Their walking postures were also improved, although there was no significant difference between pre- and postoperative whole spine X-rays. However, frozen gait was not improved after SCS in both cases. Conclusions: Although further long-term study of more such cases is needed, SCS for chronic LBP may be effective in eligible PD patients without structural instability of the spine. On the other hand, walking bradykinesia was not improved by SCS as in previous reports.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 274
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 248 Microsurgical DREZ Lesioning - How Wide and How Deep Should It Be? Makoto TANIGUCHI, Tokyo Metropolitan Neurological Hospital, Fucyu/Tokyo, Japan Introduction: Although not yet be supported by high-powered evidence, DREZ lesioning is known as one of the most effective alternatives for alleviating severe arm pain following brachial plexus avulsion injury. However, little technical modification has been added so far to its original method introduced about 40 years ago mainly because of limited number of cases. Our latest case of DREZ lesioning will be reported in order to emphasize remaining unsolved technical issue of this maneuver. Methods: A 57 year old man suffering from severe C7-8 area pain following motor cycle accident 20 years ago underwent microsurgical DREZ lesioning. In this particular case, both anterior and dorsal roots were damaged. The upper and lower border of DREZ lesion was set to C6 and T1, considering multi-leveled inputs of Lissauer's tract to dorsal horn neurons. The dorsolaterall fascicles are already destroyed and seen as a groove. Fibers of dorsal root were followed, dissecting groove between dorsal and lateral column. When the gray matter of dorsal horn were visualized, dorsal horn cells were destroyed mechanically using micro forceps up to 4 mm deep from gray mater surface intending total destruction of the layers I to V of Rexed. Results: Following the operation, the pre-existed pain of the patient was vanished without any additional motor sequela, which lasted up to 3 post-operative years. However, the patient developed new moderate pain at C6 level and conra-lateral C8 incomplete analgesia both of which did not exist preoperatively. Conclusions: Microsurgical DREZ lesion is an acceptable method of choice when the all other non-destructive treatment modalities have failed to alleviate arm pain following brachial plexus injury. However, its technique demands modification taking modern concept of pathophysiology of central neuropathic pain into account. Especially, the inquiry of 'how deep and how wide' remains to be worked out.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 275
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 389 Frameless Stereotactic Anterior Cingulotomy For Intractable Pain Tzu-Tsao Chung, Tri-Service General Hospital, Taipei, Taiwan; Cheng-Fu Chang, Ph.D., Taipei Medical University Hospital, Taipei, Taiwan Introduction: Medically refractory chronic pain constitutes a major indication for pain surgery. Anterior cingulotomy is considered a valid neurosurgical option for these patients. Anterior cingulotomy involves the placement of bilateral lesions in the anterior cingulate under stereotactic guidance. Methods: We reported a case of a MRI-based frameless stereotactic anterior cingulotomy for treating intractable pain, in a 51-year-old male. Coronal MRI was performed using 3 mm-thick sections without a gap. A single lesion on each side was created. The target slice was that 24 mm posterior to the anterior tip of the lateral ventricles. Thermal lesioning was accomplished using a temperature of 80 ℃for 90 seconds. Results: The patient achieved fair pain relief (visual analog scale [VAS] score reduction of 2-5 points) following the cingulotomy procedure. No affected neurocognitive functions, including language, memory, motor, and intellectual functions, were noted. But a decline in focused attention performance was identified at the early post-operative assessment. Conclusions: Frameless stereotactic anterior cingulotomy may be helpful for treating intractable pain in patients. Among this patient, the neurocognitive domains remained unchanged, and the pain relief achieved was modest. But the possible neurocognitive deficits must be weighed against the potential benefits of pain relief.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 276
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 396 Glossopharyngeal Neuralgia Caused by a Lipoma. Case Report Young Hwan Ahn, MD,PhD, Ajou University School of Medicine, Suwon, Korea, Republic of Introduction: The cerebello-pontine angle lipomas causing trigeminal neuralgia or hemifacial spasm are rare. A lipoma causing glossopharyngeal neuralgia is also very rare. Methods: A 46-year-old woman complained of 2-year history of severe right throat pain, ipsilateral episodic otalgic pain. The throat pain was described as an episodic lancinating character confined to the throat. Computed tomography and magnetic resonance imaging revealed a suspicious offending posterior inferior cerebellar artery (PICA) compressing lower cranial nerves incluing glossopharyngeal nerve. Results: At surgery, a soft, yellowish mass (2x3x3 mm in size) was found incorporating the lateral aspect of proximal portion of 9th and 10th cranial nerves. The proximal portion of 9th nerve was displaced medially. The distal portion of glossopharyngeal nerve was pushed laterally by pulsatory compression of PICA. Only microvascular decompression of the offending PICA was performed. Additional procedure was not performed. Her severe lancinating pain remained unchanged, immediate post-operatively. The neuralgic pain disappeared over a period of several weeks. Conclusions: In a patient with a fatty neurovascular lump causing glossopharyngeal neuralgia, microvascular decompression of offending vessel was enough to treat the neuralgic pain.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 277
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 56 The Prettey Rare Sudden Death After Implantation Of Spinal Cord Stimulation JungHee Kim, M.D., Seoul Medical Center, Seoul, Korea, Republic of; JaeHong Kim, M.D., Seoul, Korea, Republic of Introduction: we report the case that the rare sudden death of unknown origin associated with SCS implantation. but most reports overlook the complications, this is not clearly identified as yet. Methods: a 46-year-old man presented with low back pain, radiating pain combined weakness owing to spinal lipomatosis. his current diagnoses were spinal lipomatosis, DM, particularly FBSS(failed back surgery syndrome). we should scheduled SCS implantation, checked symptom during 7 days testing periods, located T8-9 16 polar channel device. After testing periods, his satisfaction was very high, dwindled away VAS score reached 3. 3 months later, sudden abnormal unknown symptoms started developing. we couldn't find causes so treated with conservative methods. not increasing inflammatory lab(CRP, ESR, WBC counts), fever, wouldn't search the problem. his vital sign was changed to nearly septic condition, but neurologic exam normal state. we doubted the cardiac problem, performed an coronary angiogram, was not found the evidence of patient situation. the patient's blood pressure continuously unchecked till he died from cardiac arrest. Results: our case was completely different. Although life-threatening complications with SCS are very rare, other adverse occurrences are frequent. Not finding the cause of death, but would be presumed in the presence of proof to the SCS procedure. Conclusions: this difference that analysed the infection rates was not statistically significant form that of the diabetics. we reported abnormal sudden death complication couldn't explained the causes, but estimated concerned with SCS implantation.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 278
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 326 Motor Threshold is Influenced by Head Position and Muscle Activation during Motor Cortex Stimulation Chris Honey, MD, D.Phil., University of British Columbia, Vancouver, BC, Canada; Manish Ranjan, MBBS, MCh., Vancouver, BC, Canada Introduction: Motor Cortex Stimulation (MCS) was introduced by Tsubokawa in 1991 to help treat deafferentation pain. Despite two decades of use, little information is available concerning the ideal stimulation parameters. Too little stimulation risks lack of efficacy, while too much risks seizure. This study prospectively evaluated the effect of i) head position and ii) voluntary muscle activation on the motor threshold of patients undergoing MCS. Methods: Patients with successful MCS (more than 50% pain reduction after 1 year of stimulation) were evaluated to determine their motor threshold (MT). MT was defined as the voltage required to produce a motor contraction in the painful area (with contact, pulse width and frequency held constant). The MT was then tested with the patient 1. sitting at rest, 2. sitting with voluntary activation of the painful area, 3. supine at rest and 4. supine with activation. Values were then compared within subjects using paired t-test with a level of significance set at 0.05. Results: The MT was significantly lower when the muscle was voluntarily active both in the supine (p<0.001) and sitting position (p<0.001). The MT was significantly lower in the upright position both when the affected area was at rest (p<000.1) or active (p=0.002). Conclusions: The knowledge that motor threshold (MT) is lower when a patient is sitting and activating the affected muscle is crucial for the clinician adjusting MCS parameters. For example, if the MT is tested while the muscle is at rest (which would be common in most clinics) and found to be 5.0V, the MCS might be set at 60% of this: 3.0V. Once the patient leaves the clinic and activates the muscle, the MT could drop to 4.0V - therefore the MCS would actually be 75% of MT. This phenomenon could partially explain the complication of delayed seizure.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 279
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 330 Balloon Compression For Trigeminal Neuralgia Rafid Al-Mahfoudh, Walton centre for Neurology and Neurosurgery, liverpool, United Kingdom; G. Sivakumar, liverpool, United Kingdom; M. Stovell, liverpool, United Kingdom; J. Osman-Farah, liverpool, United Kingdom; P R Eldridge, liverpool, United Kingdom Methods: Analysis of prospectively collected data of patients undergoing balloon compression for trigeminal neuralgia. Results: A total of 105 patients had 186 balloon compression for trigeminal neuralgia over a ten year period. There were 63 males and 42 females. The age range was 37 years to 92 years with a median of 74 years. Follow up ranged between 6 months to 10 years. The neuralgia was right sided in 65 patients and left sided in 36. Bilateral pain was reported in 4 patients. The description was typical in 84 (80%) and atypical in 13 (12.4%). The distribution of the facial pain was most common in V2/V3 39 (37.1%) followed by V1/V2 16 (15.2%). The duration of TGN prior to the procedure ranged from 3 months to 30 years (mean 7.86 years, median 6 years, SD 6.802). MRTA was performed in 74 patients, 43 (58.1%) had a vascular contact. The mean pain relief period was 15.17 months. Complications included diminished corneal reflex (6, 5.7%), chemosis (1), superficial transient conjunctival infection (1), bradycardia leading to incompletion of the procedure (1), anaesthetic dolorosa (1), bleeding (1) and subarachnoid haemorrhage (1). Conclusions: Balloon compression is an important modality of treatment especially in the elderly, patients with co-morbidities and where other modalities have failed. The procedure is safe, effective and can be repeated.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 280
Session Title: Poster Session - Pain Session Time: Wednesday, May 29, 2013
Presentation Number: 420 Common Infectious Agents in Children With Ventriculoperitoneal Shunt Infections in a Kenyan Population Naomi Ochieng, Bethany Kids Hospital at Kijabe, Nairobi, Kenya Introduction: Ventriculoperitoneal shunt infections are a major cause of morbidity and mortality. Most data on these infections is in Western literature. Limited data is available on the infecting organisms in our setup. Knowledge of the common infecting organisms would arm clinicians on appropriate antibiotics for prophylaxis. Methods: This is a retrospective descriptive study conducted at Bethany Kids at Kijabe hospital (BKKH)a paediatric neurosurgical referral center serving a wide population mainly from central Kenya. It also handles referrals from all over the country.The BKKH database was used to select charts of all the patients who had developed a shunt infection post ventriculoperitoneal insertion. The charts were then retrieved and data on age, sex, cultured organism, csf cell count, sensitivity, time post vps insertion and outcome were recorded. The data was coded and analysed with spss statistics 17.0. We excluded all those which had negative cultures and missing data. Results: There were a total of 53 patients with csf infections that met the inclusion criteria; 25 males and 28 females. 68% were below 6 months of age. The most common infecting organisms were gram negative cocci at 40% followed by coagulase negetive Staphylococci and Staphylococcus aureus respectively. 68% of the patients cleared the infection and 41% went ahead to have another VPS placed. 79% of infections occurred within 2 months of shunt placement. Gram negative infections were associated with worse outcomes. 13/13 of Staph Aureus infections were sensitive to cefazolin. However, only 1/21 of the gram negative organisms was sensitive to cefazolin. 17/21 of the gram negative organisms were sensitive to meropenem. Conclusions: The spectrum of organisms causing infections in our set up is different from that noted in the West and hence we need to develop different antibiotic protocols to reflect this.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 281
Session Title: Poster Session - Epilepsy Session Time: Wednesday, May 29, 2013
Presentation Number: 93 Seizure Outcome After Vagus Nerve Stimulation In Patients With Refractory Epilepsy. Arthurt Cukiert, Clinica de Epilepsia de Sao Paulo, Sao Paulo, Brazil; Jose Burattini, Sao Paulo, Brazil; Cristine Cukiert, Sao Paulo, Brazil Introduction: We report the results regarding seizures obtained in our VNS series. Methods: Ninety-seven patients were studied (mean age = 18.6 years). Forty-seven had secondary generalized epilepsy (SGE; Lennox and Lennox-like syndromes), 11 were temporal lobe resection failures, 11 had frontal lobe epilepsy, 10 had posterior quadrant epilepsy and 21 had non-localized epileptic foci. Final standard parameters were 2.5-3.5 mA, 500usec and 30Hz (30 sec “on”, 5 minutes “off. Mean follow-up time was 4.7years. Results: Three patients had to be explanted due to infection. Ninety-percent of the patients with SGE got at least 50% seizure frequency reduction. Only 1 patient who failed temporal lobe surgery benefit from the procedure; 50% of the patients with frontal or posterior quadrant epilepsy did so. Attention level and cognitive improvement was noted in 60% of the patients but did not strictly correlate with seizure outcome. There was an immediately postoperative period (generator “off”) of seizure frequency reduction (“honeymoon phase”) in 50% percent of the pediatric patients (not noted in adults). Sixteen percent of the kids presented seizure frequency worsening when stimulation current was set higher than 2.5 mA. Conclusions: VNS was effective in both adults and kids. The pediatric population appeared to represent a set of patients with better seizure and cognitive outcome after VNS. Children might be at higher risk for seizure frequency worsening at higher stimulation currents when compared to adults. Patients who failed temporal lobe resection did not benefit from the procedure.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 282
Session Title: Poster Session - Epilepsy Session Time: Wednesday, May 29, 2013
Presentation Number: 106 Outcome after functional hemispherectomy. Arthurt Cukiert, Clinica de Epilepsia de Sao Paulo, Sao Paulo, Brazil; Jose Burattini, Sao Paulo, Brazil; Cristine Cukiert, Sao Paulo, Brazil Introduction: Hemispherectomy is the largest neurosurgical procedure available; the results regarding seizures and development are among the best considering all cortical resection. We describe our series of patients submitted to functional hemispherectomy. Methods: Ninety-two patients were submitted to functional hemispherectomy from 1996-2012. Fourteen were adults and 78 were kids. Twenty-six patients had Rasmussen’s syndrome, 47 patients had hemiplegic syndrome (HHE), 5 patients had Sturge-Weber syndrome and 14 had cortical dysplasia. Age ranged from 2 months to 42 years (45 males). Mean post-operative follow-up was 7.2 years. All patients were submitted to functional hemispherectomy, which included temporal lobe resection, resection of the fronto parietal convexity and complete callosal section. The disconnected frontal and occipital poles remained in place. Results: Eighty-eight percent of the patients with Rasmussen syndrome remained seizure-free. This was also true for 87% of the patients with HHE, all patients with Sturge-Weber and 65% of the patients with cortical dysplasia. There was no worsening of motor function in patients who were previously hemiplegic; all patients with residual motor function became hemiplegic after the procedure. Gait actually improved in most of the patients who were previously hemiplegic. Cognitive improvement was noted in all patients with Surge-Weber, in all but one patient with HHE, and all but 2 patients with Rasmussen’s syndrome and in 8 out of 14 patients with cortical dysplasia. Seventy-eight patients presented with a transient (mean duration = 9 days) post-operative febrile syndrome (aseptic meningitis). Conclusions: Hemispherectomy is a very effective and highly underused procedure, especially in kids with HHE syndrome. It can be performed safely in specialized centers. A very high rate of seizure-free patients and a high number patients with some degree of cognitive and motor improvement might be expected.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 283
Session Title: Poster Session - Epilepsy Session Time: Wednesday, May 29, 2013
Presentation Number: 105 DBS For Refractory Temporal Lobe Epilepsy. Arthurt Cukiert, Clinica de Epilepsia de Sao Paulo, Sao Paulo, Brazil; Jose Burattini, Sao Paulo, Brazil; Cristine Cukiert, Sao Paulo, Brazil Introduction: We present our experience with Hip-DBS, a non-resective technique, in patients with temporal lobe epilepsy. Methods: Nine patients with temporal lobe epilepsy were studied. Three had normal MRI, 4 had bilateral MTS and 2 had unilateral MTS. Seven patients were implanted bilaterally in the hippocampus, and 2 unilaterally, using a Kinetra device. The electrodes were inserted along the axis of the hippocampus through a posterior approach; the most anterior contact was positioned in the head of the hippocampus. Pre-, intra- and post-stimulation scalp EEG recordings were obtained in all patients intra-operatively. Continuous stimulation was carried out using 300usec, 130Hz,2-4V pulses. Results: In 6 patients, an increase in temporal lobe spiking was noticed unilaterally at the time of electrode insertion. In all patients an ipsolateral temporal lobe recruiting response was noted during low frequency acute stimulation. In 6 patients, high frequency intraoperative hippocampal stimulation reduced or abolished interictal spiking. Seven patients received unilateral and 2 bilateral stimulation (1 with normal MRI and 1 with bilateral MTS) so far. Two patients with unilateral stimulation are seizure free and the other five had at least 90% reduction in seizure frequency. The 2 patients with bilateral hippocampal stimulation were non-responders. There was no memory decline in patients submitted to bilateral hippocampal stimulation. Mean follow-up time was 30 months. Conclusions: Hippocampal stimulation seems to be an effective and safe non-resective technique in this patient population. Memory decline did not occur with bilateral hippocampal stimulation suggesting that Hip-DBS did not lead to complete inactivation of the hippocampus.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 284
Session Title: Poster Session - Epilepsy Session Time: Wednesday, May 29, 2013
Presentation Number: 277 Stimulation of the Anterior Nucleus of Thalamus for the Treatment of Epilepsy, Inicial Experience at University Hospital Santa Maria, Lisbon, Portugal Antonio Gonçalves-Ferreira, MD, PhD, University Hospital Santa Maria, Lisbon, Portugal; Alexandre Rainha Campos, MD, Lisbon, Portugal; Carlos Morgado, Lisbon, Portugal; Carla Bentes, MD, Lisbon, Portugal; Ana-Rita Peralta, MD, Lisbon, Portugal; Joao Reis, MD, Lisbon, Portugal; Ana Catarina Santos, Psyc, Lisbon, Portugal; Jose Pimentel, MD,PhD, Lisbon, Portugal Introduction: Deep brain Stimulation (DBS) is a new therapeutic modality for refractory Epilepsy. The main target is the Anterior Nucleus of Thalamus (ANT), a key structure of the limbic system, and ANT-DBS is supposed to relieve mainly limbic seizures, as shown in SANTE study. The present study was aimed to evaluate the outcome of this procedure in our patients treated between 2011 and 2013. Methods: Seven adult (5 female, 2 male) patients were bilaterally implanted with DBS electrodes in the ANT (model 3387, Medtronic®) and Activa PC® pulse generator. The ages were 23-47 years (mean: 34y). All patients had temporal lobe epilepsy (4 bilateral, 1 multicentric). Three had already been operated: one vagal nerve stimulation, two amygdalo-hippocampectomy (one plus temporal dysplasia resection). All 7 patients were submitted to our surgical protocol under general anesthesia. The approach trajectories were transventricular in 4 patients, extraventricular In 2 and both (trans on right, extra on left) in 1. No operative morbidity was registered. DBS parameters: amplitude - 5V, pulse width - 90 µs, frequency – 145 pulses/min, 1 min ON, 5 min OFF. The post-operative time was 1 to 24 months; follow-up evaluations (4-24 months) included 6 patients. Results: Four patients experienced a moderate reduction of seizure frequency, one a marked reduction. Five patients have lower seizures intensity and duration. Two patients have no more drop attacks and one no more secondary generalized tonic-clonic seizures. All patients fell improved concerning epilepsy and quality of life. Conclusions: Our series of ANT-DBS for Epilepsy shows positive results essentially on seizures severityand quality of life.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 285
Session Title: Poster Session - Epilepsy Session Time: Wednesday, May 29, 2013
Presentation Number: 283 Modification of Temporal Lobectomy Surgical Techniques: Analysis of Surgical Exposure Faisal A. Al-Otaibi, MD, king Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia Introduction: Standard temporal lobectomy is a well-established surgical procedure for the treatment of temporal lobe epilepsy. Here we report a modification of the surgical techniques for temporal lobectomy and analyses of the required surgical exposure for temporal surgical resection. Methods: Modified surgical exposure of the temporal lobe was performed via a linear skin incision instead of a question-mark opening. Neuronavigation-guided exposure. The craniotomy is limited to less than 4 cm. No retractor was used to expose fimbria and medial hippocampus in any procedure. Sixteen consecutive patients who underwent this modified surgical approach were compared with 14 patients who underwent the traditional temporal lobectomy in the context of extent of resection, operative time, surgical complications, cosmetic effect, and patient satisfaction. Results: The posterior resection of the hippocampus was at the level of the quadrigeminal plate. Neocortical resection involved 3 to 7 cm from the temporal tip based on the gyrus levels and temporal side. The surgical exposure was adequate for posterior resection. Neuronavigation was accurate in localization during the exposure stage and found to overestimate the posterior resection by an average of 2 cm. In the modified surgical approach group, no complications were encountered, but one patient developed intermittent pain at the lower end of the surgical wound. Visual field postoperative assessment was not included in this study. All patients who underwent the modified surgical approach had an excellent cosmetic effect. In contrast, 8 patients of the 14 who underwent the traditional surgical approach showed significant depression in the temporal area due to significant bone removal at the temporal and lateral sphenoid wing bones. Conclusion: A modified surgical approach is considered a less invasive surgical exposure with excellent cosmetic effect and patient satisfaction. More patients are needed for further evaluation of this modified surgical technique.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 286
Session Title: Poster Session - Epilepsy Session Time: Wednesday, May 29, 2013
Presentation Number: 101 Targetting In Deep Brain Stimulation For Epilepsy Arthurt Cukiert, Clinica de Epilepsia de Sao Paulo, Sao Paulo, Brazil; Jose Burattini, Sao Paulo, Brazil; Cristine Cukiert, Sao Paulo, Brazil Introduction: We had been using centro-median (CM), anterior nucleus (AN) and hippocampal (Hip) DBS over the last 6 years; this paper discusses technical aspects related to the procedures. Methods: Twenty-three patients with refractory epilepsy were submitted to DBS: 7 in CM, 7 in AN and 9 in Hip. Patients submitted to CM had generalized epilepsy, those submitted to AN had fronto-temporal epilepsy or failed prior temporal lobe resection, and those submitted to Hip-DBS had temporal lobe epilepsy. Results: The hippocampus was targeted using intra-operative CT/MRI fusion with direct visibilization. The more distal electrode was aimed at the the head of the hippocampus, and oriented at the axis of the hippocampus itself with an occipital entry point. Thalamic nuclei were targeted initially based on the proportional coordinates. During AN, the visualization of the mammilo-thalamic tract was also a useful landmark. In CM, the more distal electrode was aimed at the level of the posterior commissure point. During thalamic low-frequency stimulation recruiting responses after unilateral stimulation were always bilateral and diffuse, prevailing over the stimulated side. Low frequency stimulation of the hippocampus generated localized recruiting responses. High frequency stimulation led to DC-shifts after thalamic stimulation, without modification of the cortical epileptic discharges. High frequency hipocampal stimulation led to spike frequency reduction in two thirds of the patients; no DC shift was noted. Conclusions: As DBS is used in an increasing frequency to treat epilepsy, targeting definition and intra-operative technique should be standardize. Biomarkers for adequate electrode positioning and their relationship to outcome need to be further studied and refined.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 287
Session Title: Poster Session - Epilepsy Session Time: Wednesday, May 29, 2013
Presentation Number: 104 Epileptic Syndrome And Outcome In Kids With Posterior Fossa Lesions. Arthurt Cukiert, Clinica de Epilepsia de Sao Paulo, Sao Paulo, Brazil; Jose Burattini, Sao Paulo, Brazil; Cristine Cukiert, Sao Paulo, Brazil Introduction: An increasing (though very small) number of kids with posterior fossa lesions and seizures have been reported in the literature. Their epileptic syndrome has not been clearly defined and the pathological substrate was heterogeneous, although hamarthomatous lesions prevailed. We report 2 such kids submitted to surgery. Methods: One kid was 5 (Patient 1) and the other 6 year-old (Patient 2)_by the time of surgery. Both had daily, frequent seizures, beginning in the first days of life. Patient 1 had bilateral symmetric tonic seizures prevailing during sleep (but not exclusively). Ictal video-EEG monitoring showed bilateral diffuse recruiting rhythms. MRI showed a discrete, rounded lesion above the left facial colliculus. Patient 2 had motor simple and complex partial seizures that sometimes resemble facial tics. MRI showed a 3 cm lesion occupying the middle cerebellar peduncle. Ictal video-EEG showed a bilateral slow spike-and-wave pattern. Results: Patient 1 was submitted to complete removal of the lesion; pathological examination showed hamarthoma. He has been seizure-free since surgery; a post-operative EEG was normal. Patient 2 was submitted to partial removal of the lesion; pathological examination showed ganglioglioma. There was 90% improvement in seizure frequency. Post-operative EEG showed rare spiking, with the same morphology as preoperatively. Conclusions: As seen in patients with hypothalamic hamarthoma, surface EEG was false-positive and epileptogenesis is very likely related to the posterior fossa lesion. Although focal, these lesions led to generalized epileptic syndromes. Complete resection of the lesion might lead to seizure freedom; partial removal would very unlikely be successful regarding seizure control.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 288
Session Title: Poster Session - Stereotactic Technology Session Time: Wednesday, May 29, 2013
Presentation Number: 65 Deep Brain Stimulation (DBS) at the Crossroad Between Common Sense and Nonsense Marwan Hariz, UCL Institute of Neurology, London, United Kingdom Introduction: Modern DBS has been around for a quarter of a century. The purpose of this study is to review the achievements of DBS so far, and to discuss future trends in clinical applications of this technique. Methods: A survey of PuBMed publications was conducted to examine the various clinical DBS applications as well as proposals and suggestions for its use in the future. Results: The literature confirms that DBS is solidly established in the neurosurgical treatment of Parkinson´s disease (PD), dystonia, and tremors. Improved understanding of brain circuitries and their involvement in various neurological and psychiatric states, coupled with the fact that DBS is a safe procedure and an exquisite tool for ethical and safe study of the human brain, have opened completely new avenues for this technology, both for future therapies and in research. Serendipitous discoveries and advances in structural and functional imaging are providing an increasing number of ‘‘new’’ brain targets for an increasing number of pathologies, leading to investigations of DBS in a variety of neurological, psychiatric, behavioural, and cognitive conditions. Trials and proof of concept of DBS have been conducted, are underway, or are planned in several fields: in pain, epilepsy, OCD, depression, Tourette, tinnitus, minimally conscious states, as well as in eating disorders, addiction, cognitive decline, and autonomic states. However, in the last couple of years, there have been alarming reports indicating that in the future, DBS may be proposed for enhancement of memory in healthy people, and even as a tool for “treatment” of “antisocial behavior” and for improving “morality”. Conclusion: The future of DBS as a tool to study and to treat brain disorders is promising. Those who consider this tool for dubious experiments, and promote it for even more dubious indications, will risk to jeopardize the whole concept of DBS.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 289
Session Title: Poster Session - Stereotactic Technology Session Time: Wednesday, May 29, 2013
Presentation Number: 363 The intraventricular Infusion Treatment Of subacute sclerosing panencephalitis(SSPE) masahiro ichikawa, Fukushima medical university, Fukushima, Japan Introduction: SSPE(subacute sclerosing panencephalitis) is a progressive and fatal central nervous system disorder that results from a persistent SSPE virus infection and frequentry characterized by a slow periodic movement often called myoclonus.Compound which inhibits the replication of SSPE virus might be a candidate for the specific drug for SSPE. Out of several compounds which had been tried for the treatment of SSPE, two drugs, i.e., inosiplex and interferon-alpha, were reported to be effective. Those drugs, however, could not cure the disease. Recently, ribavirin therapy has been proposed as novel antiviral chemotherapy for SSPE. Methods: Ribavirin is a anti-virus drug for C type chronic viral hepatitis.By intraventricular administration, ribavirin level in CSF reaches a concentration at which ribavirin could completely inhibit the replication of SSPE virus. Results: Three patient were treated with the intrathecal ribavirin and interferon by useing continous drug infusion pomp. We could not observe complete cure effect for SSPE prognosis. But during intraventriclular treatment, we observed the decrease of myoclonus and biomaker. Conclusions: The intraventricular continuous infusion therapy of ribabin and interferon seemed to have a certain effect on clinical courses of patients with SSPE. To reach the conclusion that ribavirin therapy is clinically effective, clinical trials on many cases will be required.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 290
Session Title: Poster Session - Stereotactic Technology Session Time: Wednesday, May 29, 2013
Presentation Number: 238 MRI Sequences and Surgical Technique For Safe and Less Invasive Stereotactic Neurosurgery Masahito Kobayashi, MD, PhD, Saitama Medical University Hospital, Iruma-gun, Saitama, Japan; Takayuki Ohira, MD, PhD, Tokyo, Japan; Takamitsu Fujimaki, MD, PhD, Iruma-gun, Saitama, Japan Introduction: For deep brain stimulation (DBS) of STN or other targets, MRI and semi-microrecording of neuronal activities has been used to identify targets anatomically and neurophysiologically. Recently, a multi-channel parallel probe system has developed for more detailed targeting while risk of bleeding and brain damages may increase. With more precise and clear anatomical images, a single-channel probe would be sufficient for DBS surgery. We have developed parameters for definite Proton and T2 weighted images (WI) and other surgical techniques to prevent brain shift and insert stimulating electrodes precisely, which is also useful for other stereotactic surgery such as biopsy. Methods: Subjects are two normal volunteers for MRI evaluation, 12 patients for STN-DBS, and 17 patients for stereotactic biopsy. In T2 and Proton WI sequences for DBS, a 1.5T-MRI apparatus was used with FOV of 300mm, matrix 512X512, slice thickness of 2mm. Two normal volunteers underwent MR scans without stereotactic frame, changing TR (3500, 7000, 10000msec) and numbers of acquisition (1,2 and 3). Surgical procedures are performed with several techniques, such as putting bone wax and dripping artificial cerebrospinal fluid after perforation of skull, positioning probe-tracks away from ventricles and sulci, and avoiding excessive elevation of patients’ heads. Results: In normal volunteers, most clear and precise T2 and Proton WIs for basal ganglions were acquired with TR of 7000 msec and twice of acquisitions. In all STN-DBS surgeries using these paremeters, STNs were defined clearly in planning MRI and also identified electrophysiologically with more than 5.5 mm length. Successful diagnosis was achieved in all 17 patients for biopsy. There was no bleeding, brain damage or other adverse effects in any patients. Conclusion: Our MR sequences and some surgical techniques provide quite safe and successful surgical results without multi-track surgical system.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 291
Session Title: Poster Session - Stereotactic Technology Session Time: Wednesday, May 29, 2013
Presentation Number: 391 STN-DBS with Semi-micro Recording and 3T-MRI Images Masayuki Nakano, MD, Southern TOHOKU Fukushima Hospital, Fukushima, Japan; Takaomi Taira, MD, Tokyo, Japan; Masahiro Oinuma, MD, Fukushima, Japan; Mitsuo Sato, MD, Fukushima, Japan; Jun Asari, MD, Fukushima, Japan; Kazuo Watanabe, MD, Koriyama, Japan Introduction: In performing STN (subthalamic nucleus) -DBS, targeting is essentially important. But with semi-micro recording, sometimes we need repeated recording when the target was not identified in the first tracking. We analyzed the usefulness of 3T (tesla)-MRI in STN-DBS. Methods: The materials are 8 patients who suffered Parkinson’s disease and underwent STN-DBS in our hospital with 3T-MRI information ( 3T-guided group), and 20 patients without 3T-MRI ( Non 3T-guided group). 3T-guided group patients were studied with 3T-MRI before surgery, and those data was fused with 1.5T MRI images in operation. We analyzed 1) Number of slices detected STN, 2) The difference of 3T-guided targets and tentative target in non 3T-guided ordinary targets. 3) Number of recordings in the surgery between 3T-guided group and non 3T-guided group. Equipment is Signa HDxt(3T), and parameter is as follows, TR: 4400 ms, TE: 111.3 ms, Slice Thickness: 2mm, 1mm, Slice plane: axial, Matrix: 512, Number of slices: 69. Results: The results are as follows. 1) The number of slices detected STN were 2.0 slices in 2mm scan, 3.57 slices in 1mm scan. 2) Modification of the tentative targets before tracking was performed in 5 cases out of 8 cases. 3) Number of recording was one time in 3T-guided group, in the other hand, 1.13 times in non 3T-guided serial recent 20 cases. Conclusions: In conclusion, we think 3T-guided STN-DBS with semi-micro recording is reasonable method and less invasive procedure.
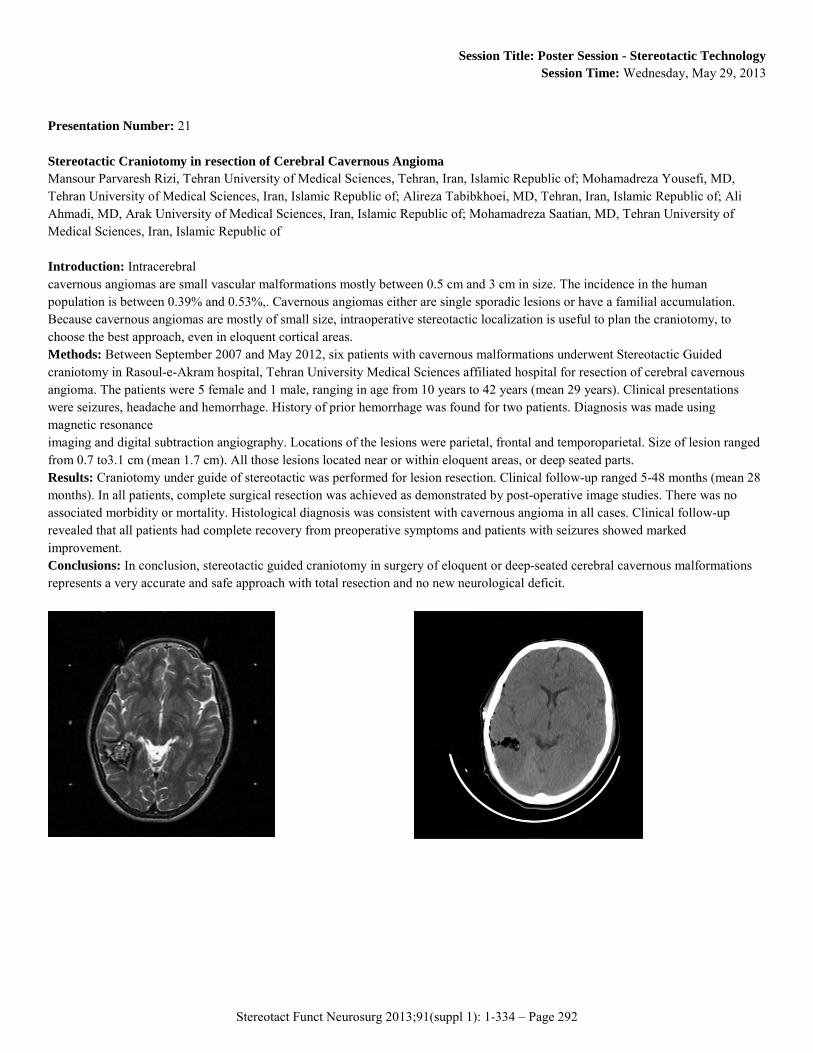
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 292
Session Title: Poster Session - Stereotactic Technology Session Time: Wednesday, May 29, 2013
Presentation Number: 21 Stereotactic Craniotomy in resection of Cerebral Cavernous Angioma Mansour Parvaresh Rizi, Tehran University of Medical Sciences, Tehran, Iran, Islamic Republic of; Mohamadreza Yousefi, MD, Tehran University of Medical Sciences, Iran, Islamic Republic of; Alireza Tabibkhoei, MD, Tehran, Iran, Islamic Republic of; Ali Ahmadi, MD, Arak University of Medical Sciences, Iran, Islamic Republic of; Mohamadreza Saatian, MD, Tehran University of Medical Sciences, Iran, Islamic Republic of Introduction: Intracerebral cavernous angiomas are small vascular malformations mostly between 0.5 cm and 3 cm in size. The incidence in the human population is between 0.39% and 0.53%,. Cavernous angiomas either are single sporadic lesions or have a familial accumulation. Because cavernous angiomas are mostly of small size, intraoperative stereotactic localization is useful to plan the craniotomy, to choose the best approach, even in eloquent cortical areas. Methods: Between September 2007 and May 2012, six patients with cavernous malformations underwent Stereotactic Guided craniotomy in Rasoul-e-Akram hospital, Tehran University Medical Sciences affiliated hospital for resection of cerebral cavernous angioma. The patients were 5 female and 1 male, ranging in age from 10 years to 42 years (mean 29 years). Clinical presentations were seizures, headache and hemorrhage. History of prior hemorrhage was found for two patients. Diagnosis was made using magnetic resonance imaging and digital subtraction angiography. Locations of the lesions were parietal, frontal and temporoparietal. Size of lesion ranged from 0.7 to3.1 cm (mean 1.7 cm). All those lesions located near or within eloquent areas, or deep seated parts. Results: Craniotomy under guide of stereotactic was performed for lesion resection. Clinical follow-up ranged 5-48 months (mean 28 months). In all patients, complete surgical resection was achieved as demonstrated by post-operative image studies. There was no associated morbidity or mortality. Histological diagnosis was consistent with cavernous angioma in all cases. Clinical follow-up revealed that all patients had complete recovery from preoperative symptoms and patients with seizures showed marked improvement. Conclusions: In conclusion, stereotactic guided craniotomy in surgery of eloquent or deep-seated cerebral cavernous malformations represents a very accurate and safe approach with total resection and no new neurological deficit.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 293
Session Title: Poster Session - Stereotactic Technology Session Time: Wednesday, May 29, 2013
Presentation Number: 127 Tips and Verification of Stereotactic Accuracy for DBS lead positioning Takanobu Kaido, National Center of Neurology and Psychiatry, Kodaira, Tokyo, Japan; Akio Takahashi, Kodaira, Tokyo, Japan; Yuu Kaneko, Kodaira, Tokyo, Japan; Taisuke Otsuki, Kodaira, Tokyo, Japan Introduction: More accurate lead implantation would be effective and safe at deep brain stimulation (DBS). We here show our tips to improve accuracy and results of verification. Methods: We retrospectively studied surgical cases who had undergone DBS lead implantation between May 2011 and October 2012. Cases with different fixation of lead or with changed location of lead based on intraoperative findings were excluded from this study. Sixteen cases (20-70 years old, 8 men) were included. Targeted diseases were Parkinson disease in 7, essential tremor in 1, dystonia in 4, and Tourette syndrome in 4. Implanted electrodes were 29 (16 in left). Anatomical targets were the STN in 1,GPi in 19, Vim in 2, CM-Pf of thamalus in 4. Stereotactic instrument was mechanically checked its accuracy with TargetSimulator before every sterilization. Operation was planned on preoperative MRI with SurgiPlan. At the operation, CT after fixation of stereotactic frame was obtained and merged on preplanning. Skull was perforated along the trajectory of lead implantation. Fibrin glue was administered to avoid leakage of cerebrospinal fluid. Microrecording was performed. Stereo-X-ray was used to confirm the location of electrodes. DBS lead was changed under X-ray fluoroscopy not to be off the point. Burr hole cover was available to fix the DBS lead. After surgery, all patients showed clinical improvement. Coordinates of tip of implanted DBS lead was checked on postoperative CT merged on intraoperative framed CT. Errors of coordinates were shown as average +/- error of means. Results: Errors (mm) were 0.5±0.1 in X, 0.4±0.1 in Y, 0.5±0.1 in Z. Vector error, length of preplanned target and tip of implanted lead, was 1.0±0.1 mm. Conclusions: Our tips was useful to control appropriate positioning of DBS lead.
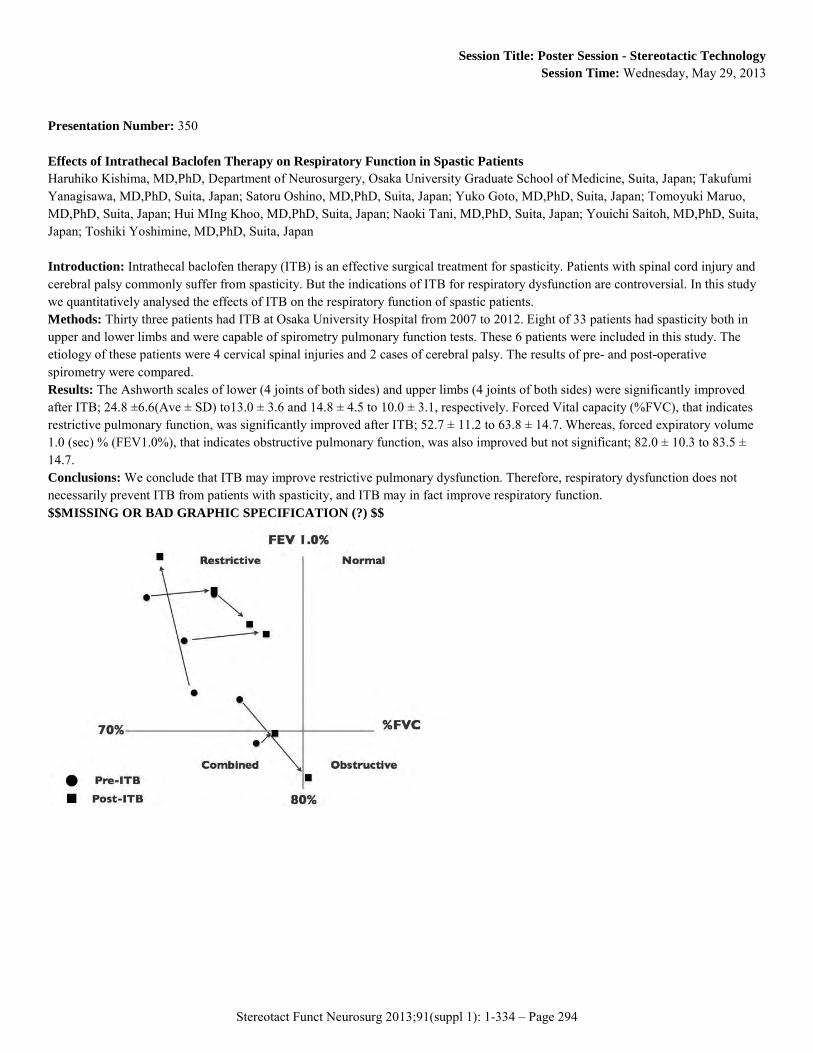
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 294
Session Title: Poster Session - Stereotactic Technology Session Time: Wednesday, May 29, 2013
Presentation Number: 350 Effects of Intrathecal Baclofen Therapy on Respiratory Function in Spastic Patients Haruhiko Kishima, MD,PhD, Department of Neurosurgery, Osaka University Graduate School of Medicine, Suita, Japan; Takufumi Yanagisawa, MD,PhD, Suita, Japan; Satoru Oshino, MD,PhD, Suita, Japan; Yuko Goto, MD,PhD, Suita, Japan; Tomoyuki Maruo, MD,PhD, Suita, Japan; Hui MIng Khoo, MD,PhD, Suita, Japan; Naoki Tani, MD,PhD, Suita, Japan; Youichi Saitoh, MD,PhD, Suita, Japan; Toshiki Yoshimine, MD,PhD, Suita, Japan Introduction: Intrathecal baclofen therapy (ITB) is an effective surgical treatment for spasticity. Patients with spinal cord injury and cerebral palsy commonly suffer from spasticity. But the indications of ITB for respiratory dysfunction are controversial. In this study we quantitatively analysed the effects of ITB on the respiratory function of spastic patients. Methods: Thirty three patients had ITB at Osaka University Hospital from 2007 to 2012. Eight of 33 patients had spasticity both in upper and lower limbs and were capable of spirometry pulmonary function tests. These 6 patients were included in this study. The etiology of these patients were 4 cervical spinal injuries and 2 cases of cerebral palsy. The results of pre- and post-operative spirometry were compared. Results: The Ashworth scales of lower (4 joints of both sides) and upper limbs (4 joints of both sides) were significantly improved after ITB; 24.8 ±6.6(Ave ± SD) to13.0 ± 3.6 and 14.8 ± 4.5 to 10.0 ± 3.1, respectively. Forced Vital capacity (%FVC), that indicates restrictive pulmonary function, was significantly improved after ITB; 52.7 ± 11.2 to 63.8 ± 14.7. Whereas, forced expiratory volume 1.0 (sec) % (FEV1.0%), that indicates obstructive pulmonary function, was also improved but not significant; 82.0 ± 10.3 to 83.5 ± 14.7. Conclusions: We conclude that ITB may improve restrictive pulmonary dysfunction. Therefore, respiratory dysfunction does not necessarily prevent ITB from patients with spasticity, and ITB may in fact improve respiratory function. $$MISSING OR BAD GRAPHIC SPECIFICATION (?) $$
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 295
Session Title: Poster Session - Stereotactic Technology Session Time: Wednesday, May 29, 2013
Presentation Number: 108 Development of an Implantable Catheter and Bone-anchored Port for Chronic Intermittent Convection-enhanced Drug Delivery to the Brain Neil Barua, BMBS, BMedSci, MRCS, Frenchay Hospital, Bristol, United Kingdom; Max Woolley, PhD, Renishaw, United Kingdom; Alison Bienemann, PhD, University of Bristol, United Kingdom; Dave Johnson, PhD, Renishaw, United Kingdom; Stephen O'Sullivan, Renishaw, United Kingdom; Gavin Murray, Renishaw, United Kingdom; Catriona Fennelly, Renishaw, United Kingdom; Owen Lewis, Renishaw, United Kingdom; Charlie Irving, Renishaw, United Kingdom; Marcella Wyatt, University of Bristol, United Kingdom; Paul Skinner, Renishaw, United Kingdom; Steven Gill, FRCS, MS, Frenchay Hospital, Bristol, United Kingdom Introduction: The translational potential of convection-enhanced drug delivery (CED) to the brain may be enhanced by the facility to perform chronic intermittent infusions. The aim of this study was to develop an implantable catheter and transcutaneous bone-anchored port (TBAP) which would facilitate chronic intermittent drug delivery to the brain. Methods: The TBAP was designed to promote robust osseocutaneous integration at the skin device interface. The port and catheter system was initially tested in 3 Large White/Landrace pigs for a one month period, allowing optimisation of the implantation method. The CED system was then implanted in 4 NIH miniature pigs for a period of 3 months. Intermittent infusions of 0.2% Gadolinium-DTPA were performed at one month intervals with real-time MRI tracking by attaching a needle administration set to the port. Results: The pilot study confirmed the feasibility of port implantation. By modelling the implantation method on the technique used for bone-anchored hearing aids, it was possible to achieve a stable skin/device interface which remained infection-free in all animals. Repeated infusions were successfully performed in 3 of the 4 NIH miniature pigs confirming patency of the system over the study period. In the fourth pig infusions were not successful at any re-access due to a manufacturing error which prevented insertion of the needle administration set. In one animal the port was inadvertently loosened at the one month infusion. This resulted in a failure of osseointegration and progressive tilting of the port. Despite the failure of bony integration, the skin/device interface remained intact with no evidence of infection. Conclusions: This study confirms the feasibility of performing intermittent CED through a transcutaneous bone-anchored port. The use of a transcutaneous port has the potential to facilitate clinical translation of CED of therapeutics requiring intermittent delivery to achieve optimum efficacy.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 296
Session Title: Poster Session - Stereotactic Technology Session Time: Wednesday, May 29, 2013
Presentation Number: 388 What African Neurosurgical Residents Think About Stereotactic And Functional Neurosurgery. - The Gap Within Mawuli K. Ametefe, MB ChB MGCS, Korle bu Teaching Hospital, Accra, Ghana Introduction: Over the last 100 years, stereotactic surgery has evolved from a laboratory method to a vibrant neurosurgical subspecialty. The effective use of this subspecialty in treating many disease conditions, movement disorders and pain control, seem to have left a large part of Africa behind. In assessing ways of getting the sub region involved and make the option available to our patients, we look at the opinion of neurosurgical residents on the field in relation to their training. The aim is to fill the deficit that will stimulate young neurosurgeons to pursue the field and bring the subspecialty closer to the sub region. Methods: Twelve basic questions designed to assess the knowledge and opinions of few (5) residents who have been exposed to some form of stereotactic procedure were administered. All residents took part willingly. Answers were discussed and inferences drawn. Results: All residents found the field of Stereotactic and functional neurosurgery to be very interesting. Only one of them knew about it prior to being exposed to it. Again all residents agreed that the current training program leaves them handicapped in considering and pursuing a sub specialization and sixty percent (60%) wouldn’t go into it. Conclusions: There is an exposure gap amongst residents and their training possibly worsens the situation. There is a need to bridge these gaps to get residents and probably young neurosurgeons interested in the ever evolving field of functional neurosurgery.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 297
Session Title: Poster Session - Stereotactic Technology Session Time: Wednesday, May 29, 2013
Presentation Number: 52 Spinal Cord Stimulation With Percutaneous Paddle Electrode For Peripheral Vascular Disease Under Anti-platelet Therapy Shinichi Goto, Tokyo Women's Medical University, Tokyo, Japan; Noritaka Shimizu, MD, PhD, Tachibanadai Hospital, Yokohama, Japan; Toshiyuki Tanaka, MD, Tachibanadai Hospital, Yokohama, Japan; Kazutoshi Narumiya, MD, Tachibanadai Hospital, Yokohama, Japan Introduction: Clinical benefits of spinal cord stimulation (SCS) in peripheral vascular disease (PVD) have been established (Claeys 1996, Spincemaille 2000, Amman (SCS-EPOS) 2003). In their majority advanced PVD patients receive anti-platelets or anti-coagulant therapy. Epidural spinal hematoma is a rare but serious possible complication of SCS. Epidural puncture and SCS lead insertion for the PVD patient under anti-platelets or anti-coagulant treatment requires careful attention for epidural bleeding by adequate pre-operative preparation and peri-operative observation with neurological evaluation. The shape of paddle electrodes offers improved stability reduced the risk of migration, and less electrical power consumption. However the new percutaneous paddle SCS system combined with one or two cylindrical lead seems bulky and gives cause for concern in haemostasis. We evaluated retrospectively our PVD patients having the potential risk factor for spinal epidural hemorrhage treated with new percutaneous paddle SCS. Methods: All patients (n=8) were on at least one anti- platelets drug until 1 week before the procedure. Six patients received two anti- platelets medication (aspirin and clopidogrel sulfate). Six patients with chronic renal failure, receiving 3 days a week dialysis using heparin, were planned the SCS operation between the dialysis sessions. They all underwent percutaneous paddle SCS with one or two additional cylindrical lead implantation. Results: Pre and post- operative platelet count were median 245×103/μL (range 82-305×103) and 175×103/μL (range 85-318×103). Except the first patient, 7 patients underwent SCS electrodes and IPG implantation in one stage after intra-operative confirmation of paresthesic sensation. No patient had a significant hemorrhage during the operation. No new neurological change was observed in all the patients. Conclusions: According to our initial experience, there was no evidence of neurological problems related to newly developed procedure using the perctaneous paddle SCS electrode via epidural sheath for PVD patients under anti-coagulation and anti-platelet aggregation therapy.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 298
Session Title: Poster Session - Stereotactic Technology Session Time: Wednesday, May 29, 2013
Presentation Number: 316 STN-DBS Surgery Under 1.5 MRI Guidance: Preliminary Experience In 2 PD Patients. stephan chabardès, MD,PHD, University hospital, GRENOBLE, France; Valerie Fraix, MD,PHD, GRENOBLE, France; Alexandre Krainik, MD,PHD, GRENOBLE, France; Anna Castriotto, MD,PHD, GRENOBLE, France; Peng Huan, MD, GRENOBLE, France; Manuella Oddoux, MD, GRENOBLE, France; Jean François Payen, MD,PHD, GRENOBLE, France; Emmanuel Gay, MD,PHD, GRENOBLE, France; Paul Larson, MD,PHD, San Francisco, CA; Paul Krack, MD,PHD, GRENOBLE, France; Jean François Le Bas, MD,PHD, GRENOBLE, France Nowadays, STN-DBS surgery requires multimodal resources in order to optimize the electrode placement within the target. Surgical strategies differ among teams, but the goal is usually to identify the STN on pre-op imaging and then to check that the target has been properly reached. Intraoperative stimulation in the awake patient allows to assess the benefit of stimulation on parkinsonism and absence of relevant stimulation-induced side effects. Microrecording can also be useful to identify the electrophysiological signature of the nucleus. Alternatively, MRI guidance performed during surgery has been proposed to facilitate optimal placement of the lead based on direct visualization of the target and monitoring of the insertion of the lead. Based on pioneer experience of the UCSF group, we started a pilot study to asses safety and feasibility of this technic. Material and methods. 2 PD patients suffering from disabling motor complications of dopamine were bilaterally implanted under general anesthesia and intraoperative MRI guidance. Surgery was performed in the regular MRI facility with a 1.5T scan. We used the ClearPoint Neuro-Intervention-System for planning and neuronavigation. Target coordinates were adapted according to direct and indirect definition of the STN on intra op T2-MRI sequences. Results: Surgery was safe and uneventfull. Vectorial errors of chronic lead placement were as follows: R-STN: 0.2; L-STN: 0.6 (patient#1) and R-STN: 0.2; L-STN: 0.4 (patient#2). At 3 months follow up, stimulation improved off-period UPDRS motor scores from 44 to 23/132(pat#1) and from 55 to 22/132(pat#2). Conclusion: Intra op MRI Guidance for STN-DBS surgery was safe and resulted in very good accuracy of lead position with clinical benefit in this small feasibility study. A randomized study comparing intraoperative MRI in general anesthesia versus our classical approach with microrecording and stimulation in the awake patient is planned with efficacy and patient satisfaction as primary outcomes.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 299
Session Title: Poster Session - Stereotactic Technology Session Time: Wednesday, May 29, 2013
Presentation Number: 331 Technical Considerations For The Peg Capping Method To Eliminate Csf Loss In The Supine Positioned Dbs Surgery Ichiro Takumi, MD, PhD, Nippon Medical School Musashi Kosugi Hospital, Kawasaki-shi, Kanagawa, Japan; Masahiro Mishina, MD, PhD, Tokyo, Japan; Kouhei Hironaka, Kawasaki-shi, Japan; Hirotomo Ten, Kawasaki-shi, Kanagawa, Japan; Koji Adachi, Kawasaki-shi, Kanagawa, Japan; Akira Teramoto, Tokyo, Japan; Akio Morita, Tokyo, Japan Introduction: The elimination of CSF loss in the DBS surgery is of vital importance to avoid possible brain shift and subsequent electrode displacement. We have previously advocated the usefulness of PEG Capping (Polyethylene Glycol Hydrogel Dural Sealant Capping) method for this solution. Here, we have analyzed our technique of this method. Methods: 10 cases of bilateral STN-DBS surgical cases are included in this study. PEG Capping was initially combined with the dual-floor method and converted into Stimulock™ method. Results; In both groups, postoperative air volume was eliminated by the PEG method but 2 exceptional cases of minor CSF leakage. One case was due to the dural laceration before the application on PEG Capping at the time of burr hole drilling. Another case was related to the insufficient dural incision, followed by the dural revision after the application of PEG Capping. Conclusions: We consider these are the technically important points for the PEG Capping method. PEG may expand and be absorbed after the installation, that Stimulock™ method may logically be advantageous in the electrode fixation. In our method of PEG capping with Stimulock™, burr hole is fully filled with PEGs, which will possibly decrease the occurrence of VAE (venous air embolism).

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 300
Session Title: Poster Session - Stereotactic Technology Session Time: Wednesday, May 29, 2013
Presentation Number: 300 Neuronavigation and Electrophysiology Guided Motor and Sensory Cortices Mapping Faisal A. Al-Otaibi, King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia; Tariq Abalkhail, MD, Riyadh, Saudi Arabia Introduction: Resective epilepsy surgery in eloquent cortical areas remains challenging in current practice. Neurophysiological monitoring under general anesthesia with direct cortical electrical stimulation and the use of median somatosensory evoked response (MSSEP) phase-reversal technique (N20-P20) is important to delineate motor and sensory cortices. Methods: A subset of 26 patients underwent motor cortex mapping under general anesthesia using MSSEP and direct cortical electrical stimulation mapping. The direct cortical stimulation was performed using monopolar technique with a frequency of 500 Hz, pulse width of 0.1 msec, and amplitude ranging between 1 and 20 mA for motor cortex mapping. Cortical and subcortical stimulation were performed. In 4 patients, this technique was used in an awake condition. Anatomical localization based on neuronavigation guidance was performed. A transcentral sulcus surgical approach was utilized on 3 patients for subcortical lesions. Postoperative magnetic resonance imaging (MRI) was correlated with preoperative images and postoperative neurological state. Results: Intraoperative MSSEP identified the motor cortex in 23 patients (88%). Direct cortical stimulation was successful in localizing the motor cortex in all patients. In 3 patients with large diffuse brain tumors the MSSEP was not successful in localizing the motor cortex. In those patients, subtotal tumor resection was done. Neuronavigation-based anatomical localization correlated well with neurophysiological mapping in 20 patients (76%). Nine patients developed new or additional transient motor and sensory deficits, and the remaining patients had a permanent new or additional deficit. Only 1 patient had a persistence moderate weakness affecting his functional state. The average time of electrophysiological mapping was approximately 50 minutes. Conclusion: Neurophysiological direct cortical stimulation is the most sensitive technique to map the motor cortex compared to MSSEP and neuronavigation. The presence of a large, diffuse tumor involving the primary somatosensory cortex affects MSSEP and neuronavigation localization.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 301
Session Title: Poster Session - Stereotactic Technology Session Time: Wednesday, May 29, 2013
Presentation Number: 386 Factors Related To Hydrocephalus After Aneurysmal Subarachnoid Hemorrhage Naoufel Ouerchefani, MD, Habib Bourguiba Hospital, Sfax, Tunisia Introduction: The aim of this study was to identify factors predictive of hydrocephalus among patients with spontaneous subarachnoid hemorrhage. The data can be used to predict which patients have a high probability of requiring permanent cerebrospinal fluid diversion. Methods: one hundred sixty one patients with spontaneous subarachnoid hemorrhage whatever the aetiology were retrospectively studied, to identify factors contributing to hydrocephalus. With these data, a stepwise logistic regression procedure was used to determine the effect of each variable on the development of hydrocephalus. Results: Overall, 32 of the 161 patients (20%) developped hydrocephalus. Ninety seven of the patients (60%) were female. Of the factors investigated, the following were associated with hydrocephalus, as determined with a variety of statistical Methods: 1) increasing age (P < 0.001),2) poor admission WFNS grade (P < 0.001), 3) Arterial Hypertension (p < 0,001), 4) thick subarachnoid hemorrhage on admission computed tomographic scans (P < 0.001), 5) intraventricular hemorrhage (P < 0.001). The sex, intracerebral hematomas, giant aneurysms, or multiple aneurysms did not influence the development of hydrocephalus. In addition, the risk of developing hydrocephalus increases twice with arterial hypertension and twelve times with intraventricular hemorrhage Conclusions: The results of this study can help identify patients with a high risk of developing hydrocephalus. This may help neurosurgeons expedite treatment, may decrease the cost and length of hospital stays, and may result in improved outcomes.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 302
Session Title: Poster Session - Radiosurgery and Brain Tumors Session Time: Wednesday, May 29, 2013
Presentation Number: 39 Validity of Recently-Proposed Prognostic Grading Indices for Brain Metastasis Patients Undergoing Repeat Radiosurgery Masaaki Yamamoto, MD, Ph.D., Katsuta Hospital, Hitachi-nala, Japan; Takuya Kawabe, MD, Department of Neurosurgery, Kyoto Prefectural Univ, Japan; Yoshinori Higuchi, MD, Ph.D., Department of Neurosurgery, Chiba University Gradu, Japan; Yasunori Sato, Ph.D., Clinical Research Center, Chiba University Graduat, Japan; Bierta E. Barfd, MD, Katsuta Hospital Mito GammaHouse, Hitachi-nak, Japan; Hidetoshi Kasuya, MD, Ph.D., Department of Neurosurgery, Tokyo Women’s Medical, Japan; Yoichi Urakawa, MD, Ph.D., Katsuta Hospital Mito GammaHouse, Hitachi-naka, Japan Introduction: We tested the validity of five prognostic indices, Recursive Partitioning Analysis (RPA), Score Index for Radiosurgery (SIR), Basic Score for Brain Metastases (BSBM), Graded Prognostic Assessment (GPA) and our recently proposed index, the Modified RPA system, mainly in patients with newly-developed or, uncommonly, recurrent brain metastasis (BM) treated with stereotactic radiosurgery (SRS). Methods: This was an institutional review board-approved, retrospective cohort study using our prospectively accumulated database including 746 patients who underwent re-SRS alone, without whole brain radiotherapy, during the 1998-2011 period. The Kaplan-Meier method was used to estimate the absolute risk of each event. Results: There were statistically significant survival differences among patients stratified into four or five groups based on the five systems (p; lower than 0.001). With RPA, SIR, BSBM and the Modified RPA, there were statistically significant median survival time (MST) differences among the three/four groups with no or minimal overlapping of 95% confidence intervals between any two pairs of groups. With the GPA system, however, the MST difference between the GPA 3.5-4.0 and GPA 3.0 groups did not reach statistical significance (p=.51). There were large patient number discrepancies among the three/four groups with the RPA, SIR, BSBM and GPA systems, while patient numbers were very similar among the three groups in the Modified RPA system. Our present results show the RPA and BSBM systems to reflect changes less well, with 83-95% of patients remaining in the same categories between the two procedures, than the other three systems. With SIR, GPA and the Modified RPA, 29-41% of patients were categorized into different subclasses, either better or worse. Conclusions: Among the five systems, as regards patient number proportions and MST separation among subgroups, and detailed reflection of patient status changes, the Modified RPA system was shown to be most applicable to patients undergoing re-SRS.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 303
Session Title: Poster Session - Radiosurgery and Brain Tumors Session Time: Wednesday, May 29, 2013
Presentation Number: 192 Awake Craniotomy and intraoperative MRI for Intrinsic Brain Tumor - Benefit or Burden for the Patient? Maximilian H. Mehdorn, MD PhD, University of Kiel, Kiel, Germany; Nils Warneke, MD, Kiel, Germany; Felix Schwartz, MD, Kiel, Germany; Simone Goebel, PhD, Kiel, Germany; Juliane Becker, Kiel, Germany Intraoperative high-field MRI is being applied worldwide with increasing frequency in brain tumor surgery in order to improve radicality of surgery and thereby enhance survival. Awake craniotomy has similarly been applied in order to prevent major neurological deficit incurring during removal of tumors in eloquent areas or extending deep into the white matter adjacent to tracts. Having started awake craniotomy in 1994 we additionally used intraoperative MRI since 2005 The personal series of the senior author comprises 79 patients who underwent awake tumor surgery between 1994 and 2005, using standard microsurgical equipment and neuronavigation, and 54 patients who were operated adding intraoperative MRI control. Patients tolerated both procedures as well as combination of both techniques well, and 4 patients have undergone repeat awake craniotomies without or within the MRI. Benefits and pitfalls have emerged from experiences with both techniques, and longterm data will be presented and compared to data obtained in the series of glioma patients from our dept from the same time periods.
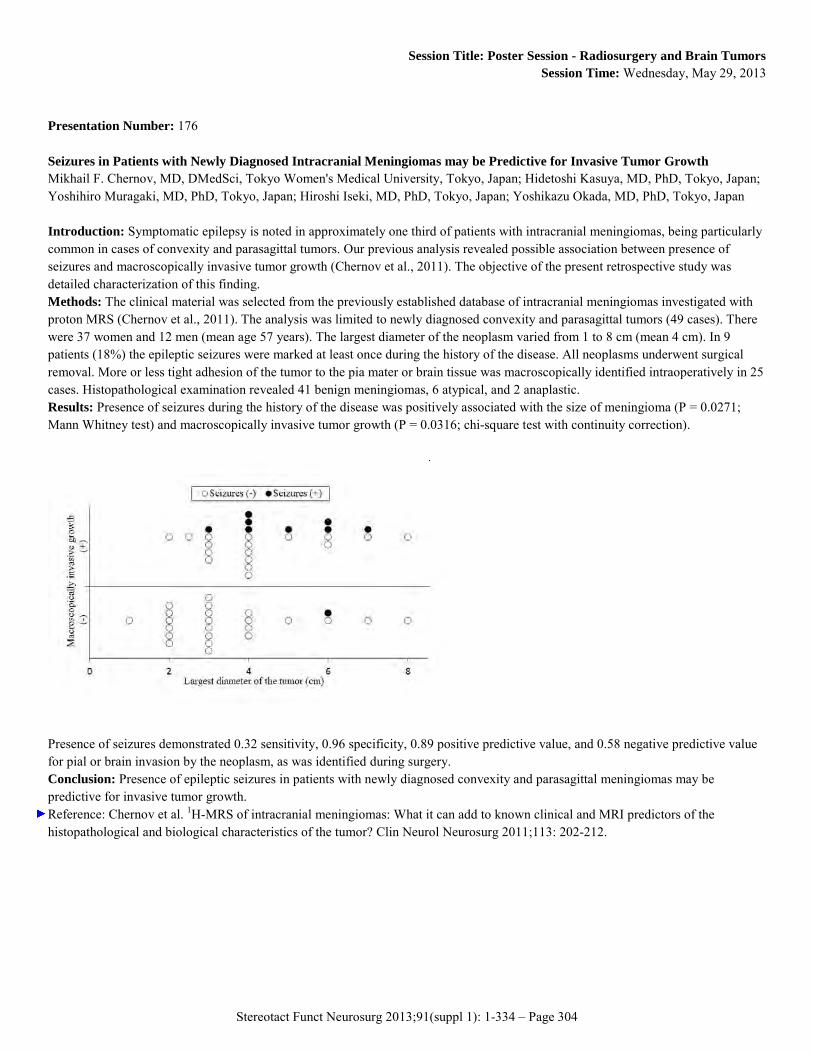
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 304
Session Title: Poster Session - Radiosurgery and Brain Tumors Session Time: Wednesday, May 29, 2013
Presentation Number: 176 Seizures in Patients with Newly Diagnosed Intracranial Meningiomas may be Predictive for Invasive Tumor Growth Mikhail F. Chernov, MD, DMedSci, Tokyo Women's Medical University, Tokyo, Japan; Hidetoshi Kasuya, MD, PhD, Tokyo, Japan; Yoshihiro Muragaki, MD, PhD, Tokyo, Japan; Hiroshi Iseki, MD, PhD, Tokyo, Japan; Yoshikazu Okada, MD, PhD, Tokyo, Japan Introduction: Symptomatic epilepsy is noted in approximately one third of patients with intracranial meningiomas, being particularly common in cases of convexity and parasagittal tumors. Our previous analysis revealed possible association between presence of seizures and macroscopically invasive tumor growth (Chernov et al., 2011). The objective of the present retrospective study was detailed characterization of this finding. Methods: The clinical material was selected from the previously established database of intracranial meningiomas investigated with proton MRS (Chernov et al., 2011). The analysis was limited to newly diagnosed convexity and parasagittal tumors (49 cases). There were 37 women and 12 men (mean age 57 years). The largest diameter of the neoplasm varied from 1 to 8 cm (mean 4 cm). In 9 patients (18%) the epileptic seizures were marked at least once during the history of the disease. All neoplasms underwent surgical removal. More or less tight adhesion of the tumor to the pia mater or brain tissue was macroscopically identified intraoperatively in 25 cases. Histopathological examination revealed 41 benign meningiomas, 6 atypical, and 2 anaplastic. Results: Presence of seizures during the history of the disease was positively associated with the size of meningioma (P = 0.0271; Mann Whitney test) and macroscopically invasive tumor growth (P = 0.0316; chi-square test with continuity correction).
Presence of seizures demonstrated 0.32 sensitivity, 0.96 specificity, 0.89 positive predictive value, and 0.58 negative predictive value for pial or brain invasion by the neoplasm, as was identified during surgery. Conclusion: Presence of epileptic seizures in patients with newly diagnosed convexity and parasagittal meningiomas may be predictive for invasive tumor growth. Reference: Chernov et al. 1H-MRS of intracranial meningiomas: What it can add to known clinical and MRI predictors of the histopathological and biological characteristics of the tumor? Clin Neurol Neurosurg 2011;113: 202-212.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 305
Session Title: Poster Session - Radiosurgery and Brain Tumors Session Time: Wednesday, May 29, 2013
Presentation Number: 152 Gamma Knife Surgery for Trigeminal Schwanommas Mehrnoush Gorjian, MD, International Neuroscience Institute, Hannover, Germany; Madjid Samii, MD,PhD, Hannover, Germany; Ladislau Steiner, MD,PhD, Hannover, Germany Introduction: Trigeminal schwannomas are of rare occurrence. In the reported literature, partial resection and post-surgery morbidity is still frequent. Methods: Steiner used the Gamma procedure between 1987 and 2005 to treat 26 patients (17 female and 9 male) with trigeminal schwannomas. Last follow up was done in 2007. The mean age of the patients was 50 years (range 19-76 years). Eight patients had undergone one or more tentative resection. Eighteen patients had upfront Gamma procedures. The patients without histological diagnosis presented with facial pain or numbness, the MRI secured the diagnosis. The median tumor volume was 4cc (range 0.63-8.5cc). The median prescription dose was 15 Gy (range 10.2-17 Gy). The mean maximum dose was 35 Gy 9range 26-50 Gy). Results: In 12 of 25 patients (48%), the tumor shrank. Ten (40%) tumors remained unchanged. Three tumors (12%) enlarged.In one patient the tumor remained unchanged on MRI 86 months after the Gamma procedure. Of 18 patients with initial Gamma surgery, follow up was available in 17 patients. Tumors shrank in 9 (53%), remained unchanged in 6 (35%), and there was tumor growth in 2 (12%). Of eight patients who had the Gamma surgery as secondary treatment, 3 decreased (37.5%), 4 (50%) remained unchanged and one enlarged. Improvement in pre-existing neurological deficits occurred in 18 (72%) of 25 patients. Four patients (16%) had no change in the initial symptoms. Three patients (12%) observed worsening of the facial pain. Two of these 3 patients had resection of the tumor, one was found to have a new prepontine portion. Conclusion: Microsurgery is the preferred treatment option for trigeminal schwannomas. In the patients that are poor surgical candidate due to somatic problems, in those unwilling open surgery or in the hands of less experienced neurosurgeons, Gamma Knife surgery is an alternative.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 306
Session Title: Poster Session - Radiosurgery and Brain Tumors Session Time: Wednesday, May 29, 2013
Presentation Number: 119 Effectiveness And Safety Of Gamma Knife Radiosurgery In The Brain Stem Metastases Won Ho Cho, MD, PhD, Pusan National University Hospital, Busan, Korea, Republic of Objective: Brain metastases have been one of major source of morbidity and mortality in systemic cancers. Especially Brainstem brain stem metastases still remain challengeable to overcome because of their poor responsiveness to conventional radiotherapy and inoperable nature. With the introduction of (Gamma Knife radiosurgery) GKRS, GKRS has been novel alternative modality in the brain stem metastases. However, GKRS has been applied to the limited cases due to the risk of radiation injury to adjacent brain stem. The authors retrospectively reviewed the efficacy and safety of GKRS in the brainstem metastases. Methods: This study enrolled 21 brain stem lesions in the 18 patients with brain stem metastases underwent GKRS between April 2004 and May 2012. 18 patients with brainstem We analyzed the tumor control rate and adverse effect related with radiation including clinical symptom and encephalomalatic change around irradiated brainstem. Results: Among the 18 patients, 17 patients harbored multiple metastatic lesions. The most common primary site was the lung (11 patients). Tumors were located in the midbrain (9 lesions), the pons (8 lesions) and the medulla oblongata (4 lesions). The mean tumor volume was 17.2 cm3 (range 0.05-64.9cm3), and the mean marginal radiation dose was 19.5 Gy (range 16.0-22.0 Gy). The median follow up time was 6.0 months. Tumor control was achieved in 19 of 21 lesions (90.5%). During following up, there was no significant adverse effect including neurologic deficit and radiation necorosis in MRI including 6 patients were followed up more than 1 year. Conclusions: GKRS achieved the excellent local tumor control rate without significant morbidity. The present results indicate that GKRS might be an effective and safe treatment modality in the brain stem metastasis.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 307
Session Title: Poster Session - Radiosurgery and Brain Tumors Session Time: Wednesday, May 29, 2013
Presentation Number: 222 Is It Possible To Remove Subcortically Located Space Occupaying Lesion In The Sensory Motor Strip With Motor Function Improvement? Wilhelm E. Eisner, Prof.,MD, Medical University Innsbruck, Austria, Innsbruck, Austria; Florian Sohm, MD, Innsbruck, Austria; Miriam Mulino, MD, Innsbruck, Austria; Thomas Fiegele, PhD, Innsbruck, Austria Introduction: Subcortical lesions in the sensorimotor strip are often considered to be inoperable. Functional magnet resonance tomography has proven to show motor function distribution but it is not able to exhibit particular motor function immediately above and around a circumscribed lesion. Electrophysiological methods like the phase reversal phenomenon of the primary cortical response following median nerve stimulation in the central sulcus is neither able to give neurosurgeons information of the local motor function distribution. The purpose of this study was to evaluate the practical value of a combined approach aided by frame based or frameless stereotactically guided surgery under electrophysiological control by direct cortical and subcortical stimulation. Methods: In a prospective study on 21 patients, space occupying lesions in the sensorimotor central area were removed using the Leksell stereotactic frame (11 patients) or Surgiscope® robotic navigation system (10 patients) and the Nicolet Viking IV® electrophysiological system utilizing direct cortical bipolar stimulation with cortical EEG recordings for identification of epileptic after-discharge. Results: Precise tumour localisation was achieved by both targeting systems and the information on the patient’s cortical motor distribution obtained by bipolar cortical stimulation led to postoperative improvement in motor function in all patients. One patient had preoperatively a hip bending weakness which resolved postoperatively but he exhibited postoperatively a new drop foot as the only deterioration in all patients. 15 of the patients had focal, defined pathologies (7 metastases; 2 cavernomas; 5 granulomas, 1 vascular malformation) which were removed radically. 11 patients out of 21 showed postoperatively motor improvement and 9 were equal to the preoperative neurological state. Conclusions: Due to the implementation of the two described technologies, surgery of lesions in the subcortical sensory-motor region can be performed with greater confidence and less motor deficits.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 308
Session Title: Poster Session - Radiosurgery and Brain Tumors Session Time: Wednesday, May 29, 2013
Presentation Number: 232 The Impact of Image Co-registration within Leksell Workstation For Glioma Surgery Management Manabu Tamura, MD, Institute of Advanced Biomedical Engineering and Science, Tokyo Women's Medical University, Tokyo, Japan; Takashi Maruyama, MD, Tokyo, Japan; Yoshiyuki Konishi, PhD, Tokyo, Japan; Motohiro Hayashi, MD, Tokyo, Japan; Jean Régis, MD, Marseille, France; Jean François Mangin, PhD, Gif sur Yvette, France; Takaomi Taira, MD, Tokyo, Japan; Yoshikazu Okada, MD, Tokyo, Japan; Yoshihiro Muragaki, MD, Tokyo, Japan; Hiroshi Iseki, MD, Tokyo, Japan Introduction: Leksell workstation including Leksell GammaPlan (LGP) and SurgiPlan, which offers us a useful treatment-planning application, helps plan tumor surgery in Gamma Knife procedures and stereotactic interventions, respectively. The practical computer-aided systems may be also effectively used for detailed evaluation of the neuroanatomy prior to open neurosurgical procedures. Our experiences in cerebral gliomas are reported. Methods: LGP version 8.3 was used before surgical resection of cerebral gliomas for: 1) delineation of subdural grid electrodes and detailed evaluation of their position relatively to cortical structures, and for: 2) fusion of the structural MRI and diffusion tensor imaging (DTI) for detailed visualization of the corticospinal tract and optic radiation, using image co-registration. Results: We evaluated of subdural grid positioning within LGP in two patients with seizures by left parietal glioma. Such detailed evaluation confirmed the electrode position relatively to cortical gyri and sulci and remarkably facilitated interpretation of the preparatory brain mapping before tumor resection. In addition, the evaluation of accuracy of the image fusion, as well as post-operative MRI, was demonstrated after the evaluation of brain function with these electrodes. In other glioma patients, simultaneous 3D visualization of the tumor and DTI with the use of LGP and SurgiPlan significantly facilitated tumor resection, permitted to avoid postoperative neurological deterioration and permitted precise planning of stereotactic biopsy. Conclusion: This evaluation helps neurosurgeons, as robust preparatory mapping can help confirm real-time mapping. Possibility for detailed evaluation of the regional neuroanatomy based on various images within Leksell planning workstations (LGP and SurgiPlan) may facilitate effective and safe resection of intracranial gliomas.

Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 309
Session Title: Poster Session - Radiosurgery and Brain Tumors Session Time: Wednesday, May 29, 2013
Presentation Number: 114 Robot-guided Convection-enhanced Delivery of Carboplatin for Advanced Diffuse Intrinsic Pontine Glioma Neil Barua, Frenchay Hospital, Bristol, United Kingdom; Max Woolley, PhD, Renishaw, United Kingdom; Stephen O'Sullivan, Renishaw, United Kingdom; Rob Harrison, Renishaw, United Kingdom; Steven Gill, FRCS, MS, Frenchay Hospital, Bristol, United Kingdom Introduction: Patients with diffuse intrinsic pontine glioma (DIPG) have a poor prognosis with median survival reported as 9 months. The failure of systemic chemotherapy to improve prognosis may be due to inadequate penetration of the blood-brain barrier (BBB). Convection-enhanced delivery (CED) has the potential to improve outcomes by facilitating bypass of the BBB. We describe the first use of carboplatin for the treatment of advanced DIPG using a robot-guided catheter implantation technique. Methods: A 5 year-old boy presented with a pontine mass lesion. The tumour continued to progress despite radiotherapy. Using an in-house modification to neuroinspire™ stereotactic planning software, the tumour volume was calculated as 43.6mL. A transfrontal trajectory for catheter implantation was planned facilitating the in-house manufacture of a recessed-step catheter. The catheter was implanted using a neuromate® robot. The initial infusion of carboplatin (0.09 mg/ml) was commenced with real-time T2-weighted MRI, facilitating estimation of the volume of infusate distribution. Infusions were repeated on a total of 5 days. Results: The catheter implantation and infusions were well tolerated. A total volume of 49.8mL was delivered over 5 days. T2-weighted MRI on completion of the final infusion demonstrated signal change through a total volume of 35.1mL, representing 95% of the targeted tumour volume. Follow-up at 4 weeks revealed clinical signs of improvement and increased T2 signal change, suggestive of early tumour necrosis. However, there was tumour progression in the regions outside the volume of distribution. The child died 2 months after treatment after developing aspiration pneumonia. Conclusions: This case demonstrates the feasibility of accurately and safely delivering small diameter catheters to the brainstem using a robot-guided implantation procedure, and performing high volume infusions at flow rates up to 10μl/min. We are hopeful that this treatment strategy could favourably impact the prognosis of patients treated at earlier stages of the disease.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 310
Session Title: Poster Session - Radiosurgery and Brain Tumors Session Time: Wednesday, May 29, 2013
Presentation Number: 405 CT Guided Stereotactic Biopsy In The Management Of Intracranial SOLs- A 3 Year Institutional Experience At Madras Institute Of Neurology sukirti chauhan, MBBS, MS, madras institute of neurology, chennai, tamilnadu, India; venkararaman sundar, MBBS, MCh in neurosurgery, chennai, tamilnadu, India; karthikeya pandian thirumaran, MBBS, MCh in neurosurgery, chennai, tamilnadu, India; siva subramanyam, chennai, tamilnadu, India Introduction: Stereotactic surgery at our institute- Madras Institute of Neurology is restricted mostly for diagnostic purposes. At a tertiary care centre like ours which caters to a large population, we encounter more than 1000 intracranial space occupying lesions per year. Methods: More than 1000 patients are seen by each of the 6 units of neurosurgery at Madras Institute of Neurology of which trauma cases form the majority. We analyzed the intracranial space occupying lesions in our unit in the past 3 years (January 2010 to December 2012). Of the 326 SOLs we had operated. 31 patients underwent stereotactic surgery- 30 cases done for diagnostic purpose and 1 case for aspiration of abscess. Results: 326 SOLs were operated which included 31 stereotactic surgeries. 30 of the cases were diagnostic stereotactic biopsy of which 9 were reported as Glioblastoma Multiforme, 17 were astrocytomas (including 14 low grade astrocytomas, 3 high grade astrocytoma), 3 were inconclusive. In 1 case abscess aspiration was done. Conclusions: With advances in modern diagnostic methodologies like MRI spectroscopy, CT imaging, RT-PCR for tuberculosis, the spectrum of cases requiring Stereotactic biopsy is limited. Since histopathology is the only definitive diagnostic method, we need to weigh the options of the patient load, indications, follow up and time constraints in a tertiary care set up like ours before defining the protocols which require Stereotactic biopsy. Though the indications include deep seated difficult to access lesions, suspicious highly malignant tumours, we mostly do it on cases which pose a diagnostic dilemma - infarct vs SOL, TB or malignancy/benign tumour. With improving economy and increasing trained neurosurgeons, we hope to widen the spectrum of the indications of Stereotactic Surgery in our set-up.
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 311
Session Title: Poster Session - Radiosurgery and Brain Tumors Session Time: Wednesday, May 29, 2013
Presentation Number: 31 Stereotactic Radiation Therapy of Patients With Brain Tumors: Khabarovsk Experience Evgeniy Sivov, Khabarovsk Clinical Oncology Centre, Khabarovsk, Russian Federation; A.V. Vitko, V.L. Kovalenko, A.A. Molokov, K.E. Poshataev, Kim Won Gi, M.V. Kosmachev, E.I. Ivanova., Introduction: Recently in our country for curing brain tumors stereotactic radiosurgery (SRS) is increasingly used, which combines a sufficient deleterious effect on the target with the maximum protection of the surrounding brain structures. We present our experience in the treatment on robotic system «Elekta AXESSE», UK. Materials and Methods: Since 2010 this method therapy is applied for treating patients with brain tumors in Khabarovsk Clinical Oncology Centre. During the period of May 2010 - December 2012, 43 patients were treated using SRT. 30 patients with meningioma; 4 - with recurrent astrocytoma; 3 - with metastasis; 3 - with hemispheric cavernous malformation; 2 case of intracanalicular vestibular schwannoma; 1 patient with adenoma. Patients’ age from 23 to 71 years old (mean, 52 Y). 10 men and 33 women. Formation of conformal dose distribution was obtained by multileaf (40-pair) collimator with a 0.25 mm accuracy of positioning. Frame fixation was standard. Dose distribution was calculated via XiO system. Patient positioning inaccuracy was measured by X-ray Volume Imaging (XVIm). The correction of patient’s position was preformed automatically with HexaPod system, resulting in 0.1 mm accuracy by linear coordinates and 0.1° by angular coordinates. Results: In the 6-months of postradiation period the stabilization of tumor and regression of symptoms was found in all patients. At the 12 months follow-up period tumor shrinking was found in 3 patients, in other cases the stabilization of tumor was observed. There were no severe adverse events. Conclusion: Our moderate experience of SRT of patients with brain tumors shows an effectiveness of the method. Moreover, in cases of tumor localization in eloquent areas and in patients with high operative risk, SRT implementation presents as the only accessible type of treatment.
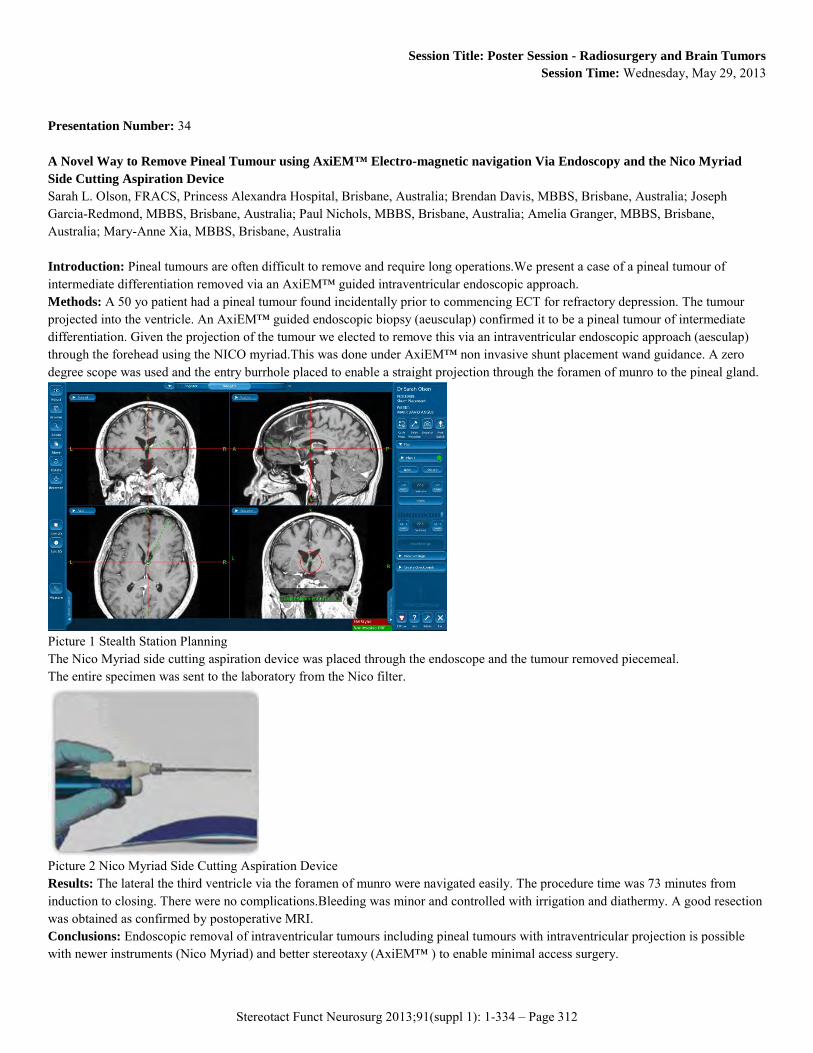
Stereotact Funct Neurosurg 2013;91(suppl 1): 1-334 – Page 312
Session Title: Poster Session - Radiosurgery and Brain Tumors Session Time: Wednesday, May 29, 2013
Presentation Number: 34 A Novel Way to Remove Pineal Tumour using AxiEM™ Electro-magnetic navigation Via Endoscopy and the Nico Myriad Side Cutting Aspiration Device Sarah L. Olson, FRACS, Princess Alexandra Hospital, Brisbane, Australia; Brendan Davis, MBBS, Brisbane, Australia; Joseph Garcia-Redmond, MBBS, Brisbane, Australia; Paul Nichols, MBBS, Brisbane, Australia; Amelia Granger, MBBS, Brisbane, Australia; Mary-Anne Xia, MBBS, Brisbane, Australia Introduction: Pineal tumours are often difficult to remove and require long operations.We present a case of a pineal tumour of intermediate differentiation removed via an AxiEM™ guided intraventricular endoscopic approach. Methods: A 50 yo patient had a pineal tumour found incidentally prior to commencing ECT for refractory depression. The tumour projected into the ventricle. An AxiEM™ guided endoscopic biopsy (aeusculap) confirmed it to be a pineal tumour of intermediate differentiation. Given the projection of the tumour we elected to remove this via an intraventricular endoscopic approach (aesculap) through the forehead using the NICO myriad.This was done under AxiEM™ non invasive shunt placement wand guidance. A zero degree scope was used and the entry burrhole placed to enable a straight projection through the foramen of munro to the pineal gland.
Picture 1 Stealth Station Planning The Nico Myriad side cutting aspiration device was placed through the endoscope and the tumour removed piecemeal. The entire specimen was sent to the laboratory from the Nico filter.
Picture 2 Nico Myriad Side Cutting Aspiration Device Results: The lateral the third ventricle via the foramen of munro were navigated easily. The procedure time was 73 minutes from induction to closing. There were no complications.Bleeding was minor and controlled with irrigation and diathermy. A good resection was obtained as confirmed by postoperative MRI. Conclusions: Endoscopic removal of intraventricular tumours including pineal tumours with intraventricular projection is possible with newer instruments (Nico Myriad) and better stereotaxy (AxiEM™ ) to enable minimal access surgery.