poster session 4
TRANSCRIPT

POSTER SESSION 4
THE IMAGING EXAMINATION
P987An alternative method for epicardial adipose tissue thickness measurement byechocardiography
V. Parisi1; G. Ferro1; A. Bevilacqua1; A. Caruso2; G. Grimaldi2; G. Rengo1; D. Leosco1;N. Ferrara1
1University of Naples Federico II, Department of Translational Medical Sciences, Naples,Italy; 2Casa di cura San Michele, Maddaloni, Italy
Purpose: Epicardial adipose tissue (EAT) thickness, measured by echocardiography, isassociated to the presence of coronary artery disease (CAD) and severe aortic stenosis(AS). EAT thickness is commonly referred as the diameter of the echo-free spacebetween the right ventricular wall and the visceral layer of the pericardium in parasternallong axis view, using the aortic annulus as an anatomic landmark (EAT-1). We aimed todemonstrate that the direct measurement of the adipose tissue thickness visualized inthe space between the ascending aorta and the right ventricle (EAT-2) might be consid-ered an alternative method.Methods: We measured EAT-1 and EAT-2 in 130 pts with severe cardiac disease referredfor cardiac surgery: 53 pts with isolated AS, 49 pts with severe CAD, and 28 pts with bothsevere AS and CAD (AS+CAD); and in 50 control subjects matched for age, sex and BMI.The two measurements were obtained at end-systole in 3 cardiac cycles (figure). Results.Both EAT-1 and EAT-2 measurements had an excellent reproducibility. With respect tocontrols pts had significantly increased EAT-1 (2,4+0,5mm vs 6+2mm; p,0,05) andEAT-2 (3+1,2mm vs 12+3mm; p,0,05). EAT-1 and EAT-2 were not statistically differentin controls. EAT-2 was significantly higher than EAT-1 in CAD, AS, and AS+CAD pts(p,0,05). Interestingly, EAT-2, but not EAT-1, was significantly increased in AS+CADpts with respect to EAT-2 of pts with isolated AS and isolated CAD.Conclusions: Our data demonstrate that EAT-2, as well as EAT-1, is a valuable method tomeasure EAT thickness. Further,EAT-2 seems to better recognize EAT increase, in pts withAS+CAD. Comprehensively, EAT-2 is greater than EAT-1. The larger space betweenascending aorta and right ventricle, allowing EATexpansion, could justify our observation.
P988Utility of student-performed pocket-sized ultrasound echocardiography as a self-learning aid to improve physical examination skills in diagnosis of valvular heartdisease: a pilot study
B P Y. Yan; KH. Lai; MYT. Chan; DYY. Lam; KNY. Fong; C. Chau; MHL. Fok; K. Kam;GM. Tam; PW. LeeThe Chinese University of Hong Kong, Medicine & Therapeutics, Hong Kong, Hong KongSAR, People’s Republic of China
Purpose: We aim to evaluate the feasibility of using pocket-sized ultrasound (PUS) as alearning-aid to improve medical student physical examination (PE) skills in the diagnosisof valvular heart diseases.Methods: We recruited consecutive patients undergoing routine transthoracic echocar-diography (TTE) at our institution. Each patient underwent initial PE (iPE), limited PUSand repeat PE (rPE) by a pair of year 3 medical students blinded to TTE results after 6hours training in basic echocardiographic views (parasternal long and short axis, apical4-chamber and subcostal) in B-mode and color Doppler images to detect significant(moderate and severe) mitral, aortic and tricuspid valvular lesions. Diagnostic accuracyof iPE, PUS, rPE and student interpretation of technician performed TTE images (sTTE)was compared with TTE as reference. Kappa statistics was used to assess agreementbetween tests and students.
Results: Six students performed 116 PUS on 58 patients with mean age of 63.7+13.7years and 40% female. TTE detected 38 significant valvular lesions of which iPE identified15 lesions (k=0.24) compared to 24 lesions by PUS (k=0.48) and 23 lesions by rPE(k=0.46, p,0.01). PUS was superior to iPE in identifying significant mitral stenosis(k=0.55 vs. 019), aortic stenosis (k=0.47 vs. 0.17), aortic regurgitation (k=0.44 vs. 0.26)and tricuspid regurgitation (k=0.43 vs. 0.08, all p,0.01). Accuracy of sTTE (k=0.57) wassuperior to PUS (k=0.48). Overall diagnostic accuracy of iPE improved from k=0.22 to0.32 and PUS acquisition-time decreased from 9.4+3min to 6.6+2min between firstand second half of the 4-week study period. There was significant improvement in iPE diag-nosis ofmitral regurgitation (k=0.30 to0.40), aortic regurgitation (k=0.13 to 0.46) andaorticstenosis (k=0.04 to 0.25, all p,0.01). Inter-observer agreement of iPE, PUS, rPE and sTTEbetween students for each patient was similar (k=0.43 to 0.49).Conclusions: This study showed that teaching medical students to performand interpretalimited echocardiography using a PUS was feasible after a brief training period. Diagnosticaccuracy of student performed PUS was better than PE for significant valvular lesions. Sig-nificant improvement in PE accuracy was observed after a short period. Further studies arewarranted to determine the utility of incorporating PUS into mainstream medical training.
P989Transthoracic echocardiography and 64-MDCTcan identify a left atrial thrombuswith vague margins, connecting to a thrombus in the pulmonary vein
H. TakeuchiNagasaki-ken Tomie Hospital, Goto, Japan
Purpose: Cerebral infarction is clinically important problem. A left atrial thrombus isknown as a cause of cerebral infarction. The main location of cardiac thrombus isknown to be left atrial appendage. Since 2012, I have published several cases of pul-monary vein thrombosis (PVT) using 64-slice multidetector CT (64-MDCT), which is apossible cause of cerebral infarction. In 2014, I have published 35 patients (61%) inthe elderly 57 patients with chest pain had PVT, indicating that PVT is not uncommonin elderly patients. And I have published that 20 patients (35%) in the elderly 57 patientswith chest pain had left atrial thrombi, as assessed using 64-MDCT, indicating that leftatrial thrombi must be more common than we think presently. Transthoracic echocardi-ography (TTE) may not be able to depict appropriate images of left atrial thrombi. 64-MDCT can have the possibility to help to assess left atrial thrombi that are not alwaysdepicted clearly by TTE.Methods: TTE was exerted to those who had a left atrial thrombus with vague margins andclearmarginsasassessedusing64-MDCT,whichwasconnectedtoathrombusin thepulmon-ary vein.Results: There are two kinds of left atrial thrombi; one is a thrombus with clear margins,and another is a thrombus with vague margins as assessed using 64-MDCT. I presenttwo cases of left atrial thrombi connecting to pulmonary vein thrombi, as assessedusing 64-MDCT and transthoracic echocardiography (TTE), which thrombus weredemonstrated clearly. And I present a case of left atrial thrombi with vague margins con-necting to pulmonary vein thrombi, as assessed using 64-MDCTand TTE. The images ofthe thrombus with vague margins looked vaguely on both examinations. The images ofTTE examinations looked like artifacts or normal structure of left atrium, so the numberof the patients with left atrial thrombi is recognized to be small.Although a left atrial thrombus that is described clearly does not include blood flow, a leftatrial thrombus with vague margins includes blood flow, which characteristic may be dif-ferent from each other. More studies are required to elucidate the quality of the thrombi.Conclusions: When we suspect a left atrial thrombus as an artifact on TTE examinations,then it would be better to check it using 64-MDCT. The number of the patients with left atrialthrombi is larger than we think.
ANATOMY AND PHYSIOLOGY OF THE HEARTAND GREAT VESSELS
P990Pathology of the testosterone deficiency on cardiac performance documented byarterial-ventricular coupling and both central arterial stiffness and peripheralwave reflection analysis
A. Angelis; K. Aggeli; N. Ioakeimidis; I. Felekos; M. Abdelrasoul; K. Aznaouridis; K. Rokas;C. Vlachopoulos; D. TousoulisHippokration Hospital, University of Athens, 1st Department of Cardiology, Athens, Greece
Purpose: Our purpose is to investigate the influence of testosterone deficiency (TD) oncardiac performance an issue still debated. We focused on arterial-ventricular coupling,
Abstract P987 Figure.
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
doi:10.1093/ehjci/jev276
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2015. For permissions please email: [email protected]
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

a load independent portrayal of a net cardiac and vascular interaction, on pulse wave vel-ocity as a measure of central arterial stiffness and augmentation index as a determinant ofperipheral wave reflections.Methods: 132 men (55+9 years) underwent standard 2D echocardiography examin-ation followed by 3D echo estimation of LV end-diastolic (EDV) and end-systolicvolumes (ESV). Based on systolic blood pressure (SBP) end systolic blood pressurewascalculated (ESP=0,9XSBP).AssessmentofLVelastance (Elv=ESP/ESV), arterial ela-stance (Ea=ESP/SV) and ventricular-arterial coupling (Ea/Elv) was performed. The 2Decho E/E? ratio was measured to assess LV diastolic function. Vascular parameterswere estimated by carotid-femoral pulse wave velocity (PWVc-f) and augmentationindex (AIx) both important determinants of Ea. TD was defined when total testosterone(TT) levels were ≤ 3.4 ng/ml.Results: Compared to patients with normal TT levels, TD patients (n=32, 32%) hadhigher BMI, and a greater prevalence of diabetes and hypertension (all P,0.05). Theyalso had lower ejection fraction (EF), stroke volume (SV) and a higher Ea/Elv. TD wasalso associated with a higher mitral E/E?, increased PWVc-f and AIx (table). The associ-ation remained significant in multivariate analysis after adjustment for age and riskfactors.Conclusion: TD associates to an unfavorable cardiac performance by affecting centraland peripheral arterial stiffness parameters. This work reveals an underlying pathologymechanism of testosterone influence on hearts energetic adding further informationand clinical value on the androgen deficiency.
ASSESSMENT OF DIAMETERS, VOLUMES AND MASS
P991Left atrial transverse diameter: a useful alternative to indexed volume
R. Cano Carrizal; C. Casanova Rodriguez; E. Prieto Moriche; D. Iglesias Del Valle;R. Cadenas Chamorro; J. De Juan Baguda; A. Martin-Penato Molina;B. Paredes Gonzalez; A. Garcia Garcia; I. Plaza PerezHospital Infanta Sofia, San Sebastian de los Reyes, Spain
Purpose: the new EACVI/ASE guidelines recommend body surface indexed volumeas the most accurate measurement of left atrium (LA), however this is not always feas-ible in daily clinical practice. Our aim is to determine which LA diameter has a bettercorrelation with LA indexed volume (LAIV) and to establish the best cutoff value inorder to predict the presence of atrial enlargement, redefined as LA volume greaterthan 34 ml/m2.Methods: Prospective study including 223 consecutive ambulatory patients. Anteropos-terior (APD), superoinferior (SID), transverse diameters (TD) and LAIV were measured inmost studies (211, 95%).Results: Out of the 211 patients, 96 (45.50%) were female, 176 patients (83.41%) were insinus rhythm, significant valvular disease (moderate/severe) was present in 48 patients(22.75%) and impaired systolic function in 7 (3.32%). Average LAVI was 42+18ml/m2and average age was 65+15 years old. TD is the diameter that keeps a better correlationwith LAVI (r Pearson 0.86, p,0.0001), as well as a better relationship (R2 0,74; quadraticmodel). The values for APD and SID are r 0.75 (R2 quadratic 0.61) and r 0.77 (R2 quadratic0.62), respectively. TD has an excellent value to detect the presence of LA enlargementdetermined by LAVI (AUC 0.91, p,0.0001). The optimal cutoff value is 39mm (93% sen-sitivity, 78% specificity, 86% PPV, 88% NPV). A cutoff value of 35mm provides 100% NPV.Conclusions: TD is the atrial diameter that provides a better correlation with LAVI. The re-lationship between TD and LAVI keeps a quadratic model, with an optimal cutoff value of39mm to discriminate the presence of atrial enlargement determined by LAVI. ThereforeTD is a useful alternative when LAVI cannot be determined, over other diameters wide-spread used in daily practice.
P992Cardiac adaptation to deconditioning after 21-days of head-down bed-rest: anechocardiographic study
EG. Caiani1; P. Arbeille2; P. Massabuau3; F. Colombo1; G. Ferri1; C. Kasswat1;D. Medvedofsky4; RM. Lang4; P. Vaida5
1Politecnico di Milano, Electronics, Information and Bioengineering Dpt., Milan, Italy;2University F. Rabelais of Tours, Unite Medicine et Phisiologie Spatiales, Tours, France;3Toulouse Rangueil University Hospital (CHU), Toulouse, France; 4The University ofChicago, Chicago, United States of America; 5University of Bordeaux, Bordeaux, France
Prolonged immobilization generates cardiac deconditioning, that is a risk factor for car-diovascular disease. Our aim was to assess the effects of 21-days of strict head-down(-6 degrees) bed-rest (BR) on left ventricular dimensions and diastolic function, by trans-thoracic 2D echocardiography and Doppler.Methods: 12 healthy men (mean age 35+8) were enrolled; the experiment was con-ducted at MEDES (Toulouse, France) as part of the European Space Agency BRstudies. Examinations (Toshiba) were performed before (PRE) and towards the end ofBR (HDT17). Manual analysis of the acquired images was performed on3 to 5 consecutivebeats, and values averaged.Results: At HDT17, reductions in end-diastolic (13%), end-systolic (11%) and strokevolume (14%) were observed, while EF did not change. Also, a reduction in early diastolicfilling was present, with a 11% decrease in peak E, 10% in E/A, and 16% in E decelerationslope. These changes were accompanied by adecrease (17%) in plasma volume (by gas-rebreathing technique), and by a reduction (20%) in VO2max aerobic power (by gradedcycle ergometer test protocol to volitional fatigue atone dayafter the BRconclusion), whileexpiratory exchange ratio did not change.Conclusions: Deconditioning due to immobilization worsened aerobic power andaffected LV dimensions and diastolic function, as combined result of LV remodelingand fluids loss. This should be considered in patients when immobilized in bed, toproper adjust the therapy, or to define appropriate physical exercises when possible, inorder to avoid further complications.
Abstract P992 Table.
PRE HDT17 p
2D End-diastolic volume (ml) 149+34 129+37* 0.0032D End-systolic volume (ml) 64+27 57+28* 0.0282D Stroke volume (ml) 84+10 73+11* 0.001Ejection fraction (%) 58+9 58+9Mitral flow E velocity (cm/s) 72+11 62+14* 0.064Mitral flow A velocity (cm/s) 42+9 41+5E/A ratio 1.8+0.5 1.5+0.4* 0.076E dec. slope (cm/ s^2) 396+85 315+75* 0.055E dec.time (msec) 191+30 204+32Time-to-peak E (msec) 489+37 468+62
*: p,0.1 vs PRE (paired t-test)
P993Right ventricular dilatation in coronary artery disease patients with and withouthistory of myocardial infarction
VA. Kuznetsov; EI. Yaroslavskaya; DV. Krinochkin; GS. Pushkarev; EA. GorbatenkoTyumen Cardiology Center, Tyumen, Russian Federation
Background: Detection of right ventricle (RV) dilatation in patients with coronary arterydisease (CAD) is very important to identify subjects at high risk for adverse cardiovascularevents. However, the data about factors associated with RV dilatation in CAD patients areinsufficient.Purpose: To assess factors associated with RV dilatation in CAD patients with prior Q-wave myocardial infarction (MI) and without MI.Methods: Out of16839patients from coronary angiography databasewe selected patients(group I) with prior Q-wave MI: 1263 patients without RV dilatation and 99 patients with RVdilatation; and patients (group II) with stenosis ≥75% of at least one coronary artery withoutacute or prior MI: 1134 patients without RV dilatation and 75 patients with RV dilatation. RVwas considered as a normal if proximal end-diastolic RV outflow diameter measured byechocardiography in parasternal long-axis view was ≤26 mm and if RV outflow diameterwas ≥ 30 mm RV was considered as dilated. Patients with intermediate value of RVoutflow tract diameter and congenital or acquired valvular heart disease were not included.Results: of group I study: According to the multivariate analysis, RV dilatation was inde-pendently associated with male gender (OR 4.75; 95% CI 1.37-16.47; p=0.014), higherindex of LV mass (OR 2.80; 95% CI 1.37-5.74; p=0.005), significant mitral regurgitation(MR) (OR 2.67; 95% CI 1.72-4.16; p, 0.001), reduced left ventricular systolic function(OR 2.41; 95% CI 1.38-4.23; p=0.002), arrhythmias (OR 1.79; 95% CI 1.05-3.03;p=0.031), higher NYHA functional class (OR 1.70; 95% CI 1.15-2.51; p=0.008) andhigher body mass index (BMI) (OR 1.07; 95% CI 1.02-1.13; p=0.011).Results: of group II study: RV dilatation was independently associated with reduced leftventricular systolic function (OR 4.22; 95% CI 1.73-10.30; r=0.002), male gender (OR4.03; 95% CI 1.47-11.04; r=0.007), arrhythmias (OR 2.98; 95% CI 1.62-5.49; r,0.001),significant MR (OR 2.34; 95% CI 1.44-3.81; r=0.001), higher NYHA functional class(OR 1.87; 95% CI 1.05-3.32; r=0.034), higher BMI (OR 1.08; 95% CI 1.02-1.15;r=0.010), and lower CCS angina class (OR 0.42; 95% CI 0.25-0.71; r=0.001).Conclusions: RV dilatation in CAD patients was not associated with localization of coron-ary lesions or coronary dominance pattern but with male gender, parameters describing
Abstract P990 Figure.
Abstract P991 Figure.
Abstracts ii157
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

severity of left ventricular dysfunction and increased BMI. Most of variables related with RVdilatation were the same in both groups of CAD patients with and without history of MI.
P994Multi-site ultrasound assessment of arterial remodeling and distensibility inmarathon runners
RM. Bruno1; E. Bianchini1; N. Di Lascio1; F. Stea1; K. Ujka1; A. Marabotti1; GS. D’angelo1;L. Ghiadoni2; L. Pratali11Institute of Clinical Physiology of CNR, Pisa, Italy; 2University of Pisa, Pisa, Italy
Objective: to investigate features of arterial remodeling and distensibility in marathonrunners by a multi-site, non-invasive approach.Methods: 46 marathon runners (M) and 15 age-sex- and BMI matched sedentary (S) indi-viduals were recruited (age 44+7 vs 43+6 years, p=ns). The following measurementswere performed: brachial blood pressure (BP- oscillometric method), carotid and femoralBP, aortic BP (applanation tonometry+transfer function), carotid-femoral pulse wave vel-ocity (PWV), ultrasound assessment of abdominal aorta, common carotid, commonfemoral and brachial artery. For each arterial site mean diameter (MD) and distensionwere assessed by a contour-tracking algorithm applied to the ultrasound imagesequences, thus allowing calculation of local distensibility coefficient (DC).Results: M in comparison with S had increased Aortic MD (15.8+2.0 vs 13.1+1.1 mm,p=0.0001) and reduced DC (29.4+15.8 vs 37.1+7.1, p=0.05), with similar carotid andbrachial MD (7.16+0.59 vs 7.04+0.77mm and 4.05+0.56 vs 3.99+0.82mm, p=ns)and DC (37.3+9.0 vs 40.2+11.5 and 9.9+7.3 vs 9.3+5.7, p=ns) were similar. Further-more, femoral MD was increased (9.8+1.0 vs 8.8+1.4, p=0.01), whereas DC wassimilar (28.7+12.6 vs 33.1+16.0, p=ns). Carotid and femoral IMT, as well as carotid-femoral PWV, were similar. In M, aortic MD was related to carotid and femoral, but not tobrachial MD. Similar correlations were found for aortic DC (carotid DC r=0.47, p=0.03;femoral DC r=0.43, p=0.07; brachial DC r=0.11, p=0.65). In M, the number of years oftraining was an independent predictor of aortic DC (standardized coefficient 20.39,p=0.03) in a model adjusted for age, sex, BMI and heart rate (r2 full model 0.68). In con-trast, aortic MD was significantly associated only to age, body surface area and heart rate.Conclusions: Marathon runners present remodeling of aorta and femoral arteries andreduced abdominal aortic distensibility which is independently associated with longertraining. Multi-site assessment of local arterial distensibility might be more useful than as-sessment of regional arterial stiffness to identify specific patterns of vascular structure andfunction in athletes.
ASSESSMENTS OF HAEMODYNAMICS
P995Analysis of blood flow and left ventricle vortex formation in patients withHeartWare left ventricle assist device using Doppler-derived vector flow mapping
M. Zemedkun; Z. Wang; FM. AschWashington Hospital Center, Cardiology, Washington, United States of America
Purpose: To characterize left ventricular (LV) vortex formation and blood flow pattern inpatients with HeartWare left ventricle assist device (LVAD) by using a novel Doppler-derived vector flow mapping technology.Methods:Sevensubjectswithseverely reducedLVsystolic function withHeartWareLVADunderwent 2 dimensional and Doppler echocardiography using Prosound 75 (Hitachi-Aloka, Japan). The flow and vortex patterns were compared to a control group of 18 sub-jects with normal EF and no valvular disease. Image sector and 2D gain were adjusted,and Nyquist limit set between 40 and 60 cm/s to obtain a frame rate ≥30Hz. Three con-secutive beats in the apical 3 chamber view were acquired and analyzed offline usingDAS-RS1 software (Hitachi-Aloka, Japan) to obtain LV flow and vortex formation patterns.Results: Mean age was 67.4 years (range 61-74 years), 70% were male and LV ejectionfraction was 16.4%+/-2.4%. A characteristic continuous vortex formation around theinflow cannula was seen in all cases throughout the cardiac cycle, with the largestvortex area being formed in the early to mid systole (FIgure 1A). Direction of blood flowwas continuously directed towards the apex (Figure 1B). This characteristic pattern is dif-ferent from that of patients with normal LV, where vortices form around the mitral leafletsduring early diastole, then transition into the mid LV by late diastole (Figure 1C) and thelargest vortex area is seen during mid systole (Figure 1D).Conclusion: Analysis of blood flow patterns and vortex formation is feasible in patientswith HeartWareLVADusing Doppler-derived vector flow mapping. A pattern of continuousvortex around the inflow cannula is characteristic in these patients.
ASSESSMENT OF SYSTOLIC FUNCTION
P996Changes in effective arterial elastance early after cardiac resynchronizationtherapy predict left ventricular end-systolic volume reduction
K. Niki1; M. Sugawara2; S. Yauchi1; K. Inoue3; M. Yagawa3; I. Takamisawa3; J. Umemura3;T. Yoshikawa3; T. Sumiyoshi3; H. Tomoike3
1Tokyo CityUniversity,Tokyo,Japan; 2HimejiDokkyoUniversity,Himeji, Japan; 3SakakibaraHeart Institute, Tokyo, Japan
Purpose:Cardiac resynchronization therapy (CRT) is nowwidely used for the treatment ofheart failure and LVEF is used to discriminate responders from nonresponders to thetherapy. Since LV end-systolic volume (LVESV) is continuously affected by ventriculo-ar-terial interactions, afterload should be reduced as much as possible to obtain optimaleffect of CRT. Effective arterial elastance (Ea) is an afterload parameter integrating arterialresistance and stiffness. The purpose of this study was to evaluate the relationshipbetween Ea and volume reduction after CRT.Methods: Twenty-nine heart failure patients (age 62+12 years, 25 men, ischemic cardio-myopathy 14%, EF 22+6%), who underwent CRTwere studied. Ea (defined as LV end-systolic pressure divided by stroke volume) was noninvasively measured by ultrasonog-raphy before and early after CRT (after 1 week). Carotid arterial stiffness parameter b,which was defined as b=ln(Ps/Pd)/[(Ds-Dd)/Dd], where Ps and Pd were systolic and dia-stolicpressure, and Dsand Ddwere systolicanddiastolic diameter, andsystemic vascularresistance (SVR) were also measured. LVESV and EF were measured by echocardiog-raphy before and 6 months after CRT. Age matched healthy volunteers were enrolled asreference.Results: Before CRT, Ea (p,0.05) and b (p,0.05), but not SVR, were significantlyincreased in patients as compared with healthy subjects. Nine subjects were defined asnonresponders whose EF did not increase more than 5%. LVESV change rate after CRTwas significantly correlated with Ea change rate (r=0.49, p,0.05) but not with other mea-surements before CRT.Conclusions: Ea in heart failure patients was increased due to the increase in arterial stiff-ness even under conditions of normal SVR values. Ea change early after CRT predictsLVESV change occurring later.
Abstract P996 Table.
before CRT after CRT normal subjects
Ea [mmHg/ml] 1.81+0.57 1.69+0.49 1.51+0.48SVR [dyn s/cm5]
1465+328 1383+358 1447+281
b 18.7+7.5 17.2+5.4 15.1+0.9CO [l/mim] 3.40+0.66 3.55+0.80 4.68+0.78LVESV [ml] 201+76 191+82
P997Myocardial function long term after Kawasaki disease: conventional and globalmyocardial deformation imaging at rest
G. Christov1; J. Saundankar1; E. Perdreau1; T. Mukasa1; V. Shah2; N. Klein2; P. Brogan2;J. Marek2
1Great OrmondStreet Hospital for Children, Cardiothoracic unit, London, United Kingdom;2University College London, Infection, Inflammation and Rheumatology section, UCLInstitute of Child Health, London, United Kingdom
Purpose:Tostudyglobalmyocardial function longtermafterKawasakidisease(KD)at rest.Methods: Observational case-control study on 92 KD subjects; 51% male, aged 11.9years (4.3-32.2), 8.3 years (1.0 230.7) after the KD-diagnosis. Group I: without coronaryartery lesions (CAL-, N=54) at any point. Group II: with coronary artery lesions (CAL+,N=38) within first 2 months of KD or at any point of follow-up. Group III: sex/age-matched controls (N=51). Myocardial function was assessed by conventional techniquesincluding pulsed wave tissue Doppler imaging (TDI) as well as 2D speckle tracking myo-cardial deformation.Results: A total of 132/143 patients/echocardiograms at rest (50/54 CAL-, 34/38 CAL+,48/51 Controls) were available for conventional as well as 2D Longitudinal and Circumfer-ential Strain analysis. Mild systolic dysfunction did occur in one patient who required anearlier revascularization procedure. There was no statistically significant differencebetween the CAL+, CAL- and control groups on multivariate comparisons of the conven-tional and global myocardial strain measurements. There was also no statistically signifi-cant difference among all groups when assessing regional longitudinal andcircumferential strain. The subgroup of patients with current coronary abnormalities (17patients out of 38 from the CAL+ group) was also compared to each of the othergroups with no statistically significant difference.Conclusion: Resting conventional systolic and diastolic function parameters as wellas global myocardial longitudinal and circumferential strain long after KD remainwithout difference to normal controls, in patients with no significant perfusion abnor-malities.
Abstract P995 Figure. Formation of LV vortex in LVAD
ii158 Abstracts
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

Abstract P997 Table.
Parameter CAL - Mean+SD(Min-Max)
CAL+Mean+SD(Min-Max)
ControlMean+SD(Min-Max)
P-value,ANOVA
EFSimpson %
62.2+3.7 (55270) 62.3+5.5 (42270) 61.3+5.9 (50275) 0.6004
LVEDD Z 0.1+1.6 (23.9–2.5) 0.3+1.5 (20.7–4.6) 20.1+1.4 (23.3–2.6)
0.4193
E/A 1.9+0.5 (1.1–3.2) 2.0+0.5 (1.0–3.1) 2.0+0.6 (1.0–3.5) 0.5626E/E’ lateral 5.6+1.1 (2.9–8.0) 5.8+1.4 (3.5–9.8) 5.9+1.7(1.9–9.7) 0.3999E/E’ medial 7.1+1.3 (3.5–11.5) 7.3+1.7 (4.1–11.8) 7.3+1.6 (2.3–8.4) 0.2061Strain Long % 21.0+2.9 (15–30) 21.8+2.6 (16–29) 21.4+3.0 (16–30) 0.4336Strain Circ % 20.4+3.3 (14–29) 22.0+4.2 (13–31) 20.9+3.3 (11–29) 0.1193
Strain Long % - longitudinal global strain in negative values; Strain Circ % - circumferential globalstrain.
P998Stroke volume correlates with exercise capacity in HFpEF patients
A. Batalli1; P. Ibrahimi1; A. Ahmeti1; E. Haliti1; I. Bytyci1; A. Poniku1; MY. Henein2;G. Bajraktari11University Clinical Centre of Kosova, Clinic of Cardiology, Pristina, Kosovo, Republic of;2Heart Centre and Department of Public Health and Clinical Medicine, Umea University,Umea, Sweden
Background: and Aim: In patients with systolic heart failure (HF), several echo para-meters have been shown to correlate with functional capacity. These findings have notbeen thoroughly tested in patients with HF and preserved ejection fraction (HFpEF).The aim of this study was to prospectively examine echocardiographic parameters thatcorrelate and predict functional capacity assessed by 6 min walk test (6-MWT) in patientswith HFpEF.Methods: This study included 102 consecutive patients (age 60+10 years) withcongestive HFpEF. LV end-diastolic and end-systolic dimensions, ejection fraction (EF),mitral and tricuspid annuluspeak systolicexcursion (MAPSE andTAPSE), myocardial vel-ocities (s’, e’ and a’), left atrial (LA) dimensions, LA volume and LA emptying fraction wereall measured. Stroke volume (SV) was estimated by multiplying LV outflow tract velocitytime integral (VTI) by its cross sectional area. All patients underwent a 6-MWT, in thesame day, which divided them into two groups (Group I: tolerated ≤ 300 meter andGroup II: .300 m).Results: Group I had lower hemoglobin level (p = 0.006), TAPSE, septal MAPSE (p ,
0.001, for both) and LVSV (p = 0.004), compared with Group II. The 6-MWT distance cor-related with hemoglobin level (r = 0.31, p = 0.007), LVSV (r = 0.41, p , 0.001), TAPSE (r =0.40, p , 0.001) and septal MAPSE (r = 0.34, p = 0.001). None of the other echo para-meters correlated with 6-MWT distance. The linear regression analysis identified hemo-globin level (P=0.002) and LVSV (P=0.041) as independent predictors of 6-MWTdistance.Conclusions: Despite preserved EF, LV stroke volume is the only independent cardiacfunction predictor of limited exercise capacity in medically treated patients withchronic HFpEF. Regular assessment of stroke volume and identification of means for itsimprovement should help alleviating patients’ symptoms and improving their exercisecapacity.
P999Automated 2D quantification of left ventricular function with anatomicalintelligence: validated by cardiac magnetic resonance imaging
XX. Luo; F. Fang; SF. Gan; Z. Ma; CM. YuIVM, Div of Cardiology, Dept of M&T, PWH, The Chinese University of Hong Kong, HongKong, Hong Kong SAR, People’s Republic of China
Purpose:Rapidandaccurate assessmentof left ventricular (LV) function wouldbe import-ant in clinical practice. The newly developed Auto 2D Quantification (a2DQ) applicationprovides an option of automated quantification of LV volumes and ejection fraction (EF)with zero-click technology within a few seconds. We aimed to explore the feasibility andaccuracy of this most updated method comparing to cardiac magnetic resonanceimaging (MRI).Methods: Thirty-three patients (52+21 years, 58% males) with cardiac diseases whounderwent transthoracic echocardiography (iE33, Phillips) and cardiac MRI (1.5 T,Siemens, Germany) were enrolled. LV end-diastolic volumes (EDV), end-systolicvolumes (ESV), and EF measured by a2DQ method (Fig) and cardiac MRI was subse-quently obtained by the dedicated software. All these measurements of each patientwere obtained in the same day.Results: The LVEDV (125+51 vs 164+65 ml, P , 0.001) and ESV (65+41 vs 95+63ml, P , 0.001) were lower whereas the LVEF (52+13 vs 48+18 %, P = 0.014) was higheron a2DQ method than cardiac MRI. Bland Altman analysis showed good agreementbetween a2DQ and cardiac MRI, with bias and 95% limits of agreement of 39+27 ml,30+29 ml and 4+9% for EDV, ESV and LVEF, respectively. Furthermore, excellent cor-relation was found with the correlation coefficient of 0.91 for EDV, 0.94 for ESVand 0.87 forLVEF (all P ,0.001). In addition, the inter- and intra-observer variability of a2DQ for LV EDVwas 5.7% and 8.7%, 7.6 % and 14% for ESV, and 2.5 % and 4.8% for LVEF, respectively.
Conclusion: Automated quantification of LV volumes and LVEF with a2DQ is feasibleand accurate. This new tool allows automated, rapid and reproducible measurementsof LV volumes and EF, with good agreement compared to MRI.
P1000Early detection of anthracycline induced cardiotoxicity in adult lymphomapatients using bidimensional strain imaging and cardiac biomarkers: a singlecentre experience
A. Gonella1; E. Conte1; L. Morena1; L. Riva1; D. Civelli1; L. Losardo1; ME. Canepari2;C. Castellino2; M. Grasso2; F. Margaria1
1Santa Croce E Carle Hospital, Department of Cardiology, Cuneo, Italy; 2S.Croce e CarleHospital, Hematological, Cuneo, Italy
Introduction: Cardiotoxicity is a major threat in haematological patients treated withanthracyclines eventually evolving towards hypokinetic cardiomyopathy and heartfailure. 2D strain echocardiography (2DST) associated with biomarkers monitoring hasbeen developed for early detection of myocardial changes: a 10% to 15% early reductionin Global Longitudinal Strain (GLS) has been proposed as predictor of cardiotoxicity bothin oncological and pediatric haematological patients. Clear data on adult haematologicalpatients are missing. Methods: All adult lymphoma patients admitted at our institution toreceive an anthracycline containing regimen were prospectically included in the study.They underwent a baseline evaluation including cardiac biomarkers (NT-PROBNP, tropo-nin I) and 2DST. Biomarkers were tested before and after each course of chemotherapyand 2DST was repeated halfway (T1) and at the end of chemotherapy (T2).Results: From May to December 2014 14 patients were included: 13 Non-Hodgkin and 1Hodgkin Lymphoma (6 males, 8 females), aged 23-81 (median 60.5 yrs). The mediandose of antracycline administered was 204mg/mq (min 100mg/mq, max 304mg/mq).At baseline median left ventricular ejection fraction (LVEF) was 64% (min 51%- max 75%)and median GLS was 219% (min 215%, max 222%). No significant reduction in LVEFwas observed at T1 (median value 63%, min 44%, max 74%, p:0.99) and at T2 (medianvalue 64%, min 56%, max 69%, p: 0.34). Median GLS was 218% (min 11%, max 22%)at T1 and 218% at T2. Comparing GLS at baseline with GLS at T1 and T2 a downwardtend has been noticed. At T1 median GLS was 218%, (p: 0.15). At T2 median GLS was217.5%, (p: 0.05). Notably, only patients who received a total dose of anthracyclingreater than 150mg/mq developed a GLS reduction .10%. In our series no alterationsin troponin I was seen. Two/14 patients had elevated baseline NT PROBNP that remainedstable during treatment. None of the patients with normal baseline NT PROBNP had it ele-vated at the end of treatment, while it could be temporarily elevated between one courseand another.Conclusions:GLSseems to have highsensibility to recognizemyocardial damage,sinceit showed a downward trend during treatment without concomitant decrease in LVEF. Bio-markers did not prove to be helpful in our series. Hereafter is necessary to expand thestudied population and to evaluate longer in the follow up the evolution of cardiotoxicity,especially in patients with GLS reduction .10%.
P1001Feasibility and usefulness of cardiac magnetic resonance as a complement toechocardiography in the evaluation of heart failure with preserved left ventricularejection fraction in elderly patients
P L. Massoure1; O. Camus1; C. Gabaudan1; F. Desmots1; L. Fourcade1; A. Jacquier21Laveran Military Teaching Hospital (HIA), Department of Cardiology, Marseille, France;2Hospital La Timone of Marseille, Radiology, Marseille, France
Objectives: to evaluate the feasibility and usefulness of cardiovascular magnetic reson-ance (CMR) in the evaluation of heart failure with preserved left ventricular ejection fraction(HFpEF) as a complement to echocardiography in elderly patients.Methods: patients aged 65 and older hospitalized for symptomatic heart failure with a leftventricular ejection fraction (LVEF) . 40% underwent both CMR and 2D echocardio-graphic assessment of cardiac volumes, mass, and function within 3.9+1.2 days afterthe hospital admission.Results: among 14 patients (mean age 80.2+8.7 Y [66-91], median 79 Y), a good correl-ation was found between echocardiography and CMR for LVEF (56.7+8.1% vs 54.3+9.2%, r=0.8). Echocardiography mildly underestimated the LV end diastolic volume
Abstract P999 Figure. Auto 2D Quantification(a2DQ) application
Abstracts ii159
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

(EDV) (55.6+25.8 vs 67+24.1 ml/m2, r=0.84) and the end systolic volume (24.9+15.8vs 31.3+13.9 ml/m2, r=0.66). Echocardiography overestimated the LV mass (87.4+23.5 vs 64+22.3 g/m2, r=0.5). Left atrial volume was increased (46.2+22.3 vs 52.8+24.9 ml/m2 assessed by CMR, r=0.9) and larger in patients with atrial fibrillation (AF)(71.5+26.9 vs 38.8+10.9 ml/m2, p=0.008). Right ventricular (RV) EDV and ESVassessed by CMR were normal (52.2+22. ml/m2 and 33.7+14.4 ml/m2). Mean RVEFwas 43.7+8.7%, whereas tricuspid annular plane systolic excursion was ≥ 15 mm inall cases (18.7+2.8 mm). RVEF was ,45% in 8 (57%) patients who had lower LVEF(p=0.005) and higher pulmonary artery systolic pressure (p=0.01). Late gadolinium en-hancement (LGE) was found in 8 cases, 4 with mid-wall LGE, 2 with subendocardial ortransmural LGE and 2 with subepicardial LGE. 2D LV global longitudinal strain (GLS)was impaired (mean 210.7+3.2%) but was not significantly different in patients withLGE, AF, LVEF , 50% or RVEF , 45%.Conclusion: CMR was feasible and safe in elderly patients hospitalized for HFpEF. In thispopulation, LVEF assessed by CMR and echocardiography were comparable. Echocar-diography underestimated volumes and overestimated LV mass. RV dysfunctionassessed by MRI and the presence of LGE were found in most of half of the cases, provid-ing additive diagnostic value.
P1002Short duration intermittent exercise increases cardiac troponin and induceschanges in parameters of right heart systolic function and hemodynamics
D. Divchev1; M. Weippert2; P. Schmidt3; H. Gettel2; A. Neugebauer2; K. Behrens2;K-M. Braumann2; B. Wolfarth3; CA. Nienaber11University Hospital Rostock, Rostock, Germany; 2University of Rostock, Rostock,Germany; 3Charite - Campus Mitte (CCM), Berlin, Germany
Introduction: Despite the high prevalence of high-intensity intermittent exercise in com-petitive and recreational sports, effects of short-duration high-intensity interval training(HIIT) on markers of myocardial necrosis are not fully investigated. The aim was toassess the effects of HIIT vs. moderate intensity continuous training (MICT) on cardiactroponin T (cTnT) and creatine kinase (CK) and their possible association with echocar-diographic parameters.Methods: Thirteen healthy males performed two different running sessions (randomizedcross-over design): 60 minutes MICTand HIIT (two times 12 × 30 sec running with 15 secrecovery between intervals and 3minutes recovery between the series) with at least 5dayswashout in between the training interventions. Venous blood samples for cardiac troponinT (cTnT), creatine kinase (CK) and the MB isoenzyme of creatine kinase (CK-MB) weretaken before (Pre), 1 hour (POST +1) and 4 hours (POST +4) following the cessationof the exercise session. A baseline transthoracic echocardiography (TTE) was carriedout at baseline and 30 minutes after cessation of HIITand MICT, respectively.Results: Average heart rate, serum lactate concentration, rating of perceived exertionafter HIIT were significantly higher compared to MICT; the training protocol had a signifi-cant effect on the release of cTnT. Four hours after HIIT 5 participants showed valuesabove normal. In contrast total CK and isoform CK-MB significantly increased regardlessof exercise protocols. Both training regimen significantly reduced TAPSE (24.8+1.6 atbaseline vs. 22.3+2.4 for HIIT (P = 0.0005) and 23.7+1.4 for MICT (P = 0.0007))while absolute reduction was more pronounced in HIIT. There was strong inverse correl-ation between right ventricular function assessed by TAPSE with absolute cTnTat POST4+ (Spearmans r = 0.771, p , 0.001).Conclusions: HIITshould be considered as a possible cause of releases of cTNTand CK.Because ECG and echocardiographic results indicated normal cardiac function after bothforms of exercise, this release seems to reflect a physiological rather than pathologicalphenomenon in healthy, exercising subjects probably attributable to changes in right ven-tricular function.
P1003Speckle tracking echocardiography: new pattern to identify patients with high riskright ventricular failure after implant left ventricular assistance device
E. Rodriguez Gonzalez; V. Monivas Palomero; S. Mingo Santos; MA. Restrepo Cordoba;J. Goirigolzarri Artaza; M. Gomez Bueno; E. Garcia Izquierdo; S. Serrano Fiz;A. Gonzalez Roman; J. Segovia CuberoUniversity Hospital Puerta de Hierro Majadahonda, Cardiology, Madrid, Spain
Right ventricular failure (RVF) after LVAD implantation is a major post-operative problemthat occurs in 20% to 30% of LVAD recipients. Previous studies identifed a TAPSE cutoff value of, 7.5mm and ,9.6 free wall longitudinal strain to predict RVF.Methods: Standard echocardiographic measurements of the RV were made, includingfractional area change (FAC) and TAPSE. Longitudinal strain of RV was measured infour apical view. RVF was defined prospectively as the post-operative need of intravenousinotrope support for 14 days or of inhaled nitrico oxide for 48 hours, or the need for right-sided circulatory support.Results: We included twenty consecutives patients (mean age 48.1+13.5, 88%males,80% with pre-operative inotropics) in whom LVAD were implanted between August2009 and February 2015 (2 Incor, 18 Excor). There were not differences in baseline char-actheristics in patients with RVF/ without RVF (age 44.8+14.4/54.5+12;p=0.57, LVEF23.5+7.4%/ 23 7.4%; p=0.9, inotropics 78%/100%). All patients had low risk RVFdefined by TAPSE.7.5mm. RVF was present only in 10% of patients with LVAD implant-ation. Alhough there were not significantly echocardiographic predictors of RVF, patienteswith RVF presented at baseline a relative preservation annulus desplacement measuredby classic parameters (TAPSE, S wave) with evident decreased medioapical strain valuesRV measured by speckle tracking.
Conclusions:Speckle tracking providesadditional information for evaluating RV functionand may become part of the echocardiographic examinations in patients with LVADtherapy to predict right ventricular failure during the follow up.
Abstract P1003 Table.
Without RVF (n=18) With RVF (n=2) P value
Michigan Score 3.9+1.9 6.2+3.2 0.13Transverse RV end-diastolic dimension 4.0+9.9 4.4+0.8 0.4Fraccional area change (%) 33.7+9.1 31.5+o.6 0.75TAPSE (mm) 15.8+3.6 17+2.8 0.67S wave by DTI (cm/sg) 9.9+2.7 10.9+1.4 0.68RV GLS (%) 212.2+4.8 29.2+1.3 0.4Free wall RVLS (%) 215.8+5–3 213.5+3.5 0.57Free wall Medioapicals segments RVLS (%) 215.2+5.7 29.7+1.0 0.23Septal RVLS (%) 28.6+5.5 24.9+0.8 0.38
GLS = Global longitudinal strain, LS = Longitudinal strain
P1004Immediate alteration of right ventricular systolic function after rv pacing inoverweight patient: subclinical RV dysfunction unmasked?
SASTRA. Pila-OnRamathibodi Hospital of Mahidol University, Bangkok, Thailand
Immediate Alteration of Right Ventricular Systolic Function after RV pacing in OverweightPatient: Subclinical RV dysfunction Unmasked?Sastra Pila-on, Teerapat Yingchoncharoen, Sirin Apinyasawat, Sukit Yamwong, PrinVathesatogkit, Oraporn SeeDepartment of Cardiology, Faculty of Medicine Ramathibodi Hospital, Mahidol UniversityBackground: Increasing body mass index (BMI) was known to be associated with in-creasing severity of RV systolic dysfunction in overweight patients without overt heartdisease. The effect of pacing on RV function in these population is unknown. Wesought to investigate the immediate effect of pacing on RV function and pulmonary circu-lation hemodynamics.Methods:Weprospectively enrolled 33patients (mean age69years, 51% men, 42% over-weight) who underwent cardiac device implantation (79% RV apical pacing) at Ramathi-bodi hospital during September 2014 to December 2014. Echocardiography wasperformed atbaseline (before the implantation) and 24hours after implantation. Meanpul-monary artery pressure (MPAP), systolic pulmonary artery pressure (SPAP), pulmonaryartery diastolic pressure (PADP), right atrial pressure (RAP), Tricuspid annular plane sys-tolic excursion(TAPSE), systolic excursion velocity (RV S’) and Tricuspid E/E’ wereobtained.Results: There is a significant correlation between BMI and change in RV S’ before andafter implantation (delta RV S’) (R=0.4, p=0.039) (Figure 1). Overweight subjects withBMI . 23 kg/m2 has significantly lower delta RV S’ when compared to the non-overweightsubject (2.1vs 20.6,p=0.002)(Figure2). There wasnosignificant difference in pulmonarypressure profile (SPAP, MPAP or PAEDP) between the overweight and non-overweight.The RV function and pulmonary pressure are not different in patients who received RVapical pacing when compared to those who received RV septal pacing.Conclusion: Overweight patients who underwent RV pacing has worse RV systolic func-tion when compared to the non-overweight subjects. This may indicate the subclinical RVsystolic dysfunction in overweight patients that was unmasked by RV pacing.
ASSESSMENT OF DIASTOLIC FUNCTION
P1005Acute effects of clove cigarette smoking on diastolic function in youngparticipants
C. Atmadikoesoemah; A. Soesanto; H. AndriantoroUniversity of Indonesia, Cardiology & Cardiovascular Medicine, Jakarta, Indonesia
Background: Smoking is one of the most modifiable risk factor in heart failure. In Indo-nesia, 88% of cigararette smoked is clove cigarette. To the best of our knowledge, therewere no studies published regarding this issue on left ventricular diastolic function. Thissudy is to describe the acute effects of clove cigarette smoking on diastolic function inyoung participants and comparing the effects caused by clove cigararette to regular cig-arette.Methods: This is an experimental study carried out in Department of Cardiology and Vas-cular Medicine Universitas Indonesia/ National Cardiavascular Center in March - April2013. Fifty participants divided into two groups: non daily smoker and daily smoker.Both groups were asked not to smoke for at least 2 hours prior to study. Echocardiographystudy was performed to before, right after and 60 minutes after smoking. Participants werethen asked to come back on the next day to perform the same procedure with another kindof cigarette.Result: After regular cigarette smoking, there was an increased septal E/e’ from baselinein the non daily smoker group right after and 60 minutes after smoking, mean value of7.63 + 1.63, 7.81 + 1.59 respectively, p = 0.000. In the daily smoker group, there wasalso an increase septal E/e profile, mean value of 7.76 + 1.31, 7.71 + 1.20), p = 0.000.After consumption of clove cigarette, a higher septal E/e’ was found in non daily
ii160 Abstracts
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

smoker group, which lasting to 60 minutes after smoking, mean value of 7.53 + 1.58,7.74 + 1.45), p = 0.000. Increased septal E/e’ was also showed in daily smoker group,mean value of 7.74 + 1.45, 7.78 + 1.40, p = 0.000Conclusion: Clove and regular cigarette smoking have acute effects on left ventriculardiastolic function in both non daily smokers and daily mokers. In comparison to regularcigarette, clove cigarette caused longer compromised diastolic function in non dailysmokers.
P1006Inter-studyreproducibilityof leftventricular torsionandtorsionratequantificationusing cardiovascular magnetic resonance myocardial feature tracking
J T. Kowallick1; G. Morton2; P. Lamata3; R. Jogiya3; S. Kutty4; J. Lotz1; G. Hasenfuss1;E. Nagel3; A. Chiribiri3; A. Schuster31University Medical Center Gottingen (UMG), Gottingen, Germany; 2Portsmouth HospitalsNHS Trust, Portsmouth, United Kingdom; 3King’s College London, London, UnitedKingdom; 4Children’s Hospital and Medical Center, Omaha, United States of America
Purpose: To determine the inter-study reproducibility of cardiovascular magnetic reson-ance feature tracking (CMR-FT) derived left ventricular (LV) torsion and torsion rates for acombined assessment of systolic and diastolic myocardial function.Methods: Steady-state free precession (SSFP) cine LV short-axis stacks were acquired at9:00 (Exam A), 9:30 (Exam B) and 14:00 (Exam C) in 16 healthy volunteers at 3 T. SSFPimages were analysed offline using CMR-FT (2D CPA MR, TomTec) to assess rotationaldisplacement in apical and basal slices. Global (average from subendocardial and sub-epicardial) peak torsion, peak systolic and peak diastolic torsion rates were calculatedusing the following definitions: 1.) twist (difference in apical and basal rotation), 2.)normal-ized twist (twist normalized to LV length) and 3.) circumferential-longitudinal (CL) shearangle (twist normalized to LV length and diameter). Exam A and B were compared toassess the inter-study reproducibility. Morning and afternoon scans were compared toaddress possible diurnal variation of LV rotational mechanics.Results: The different methods showed good inter-study reproducibility for global peaktorsion (intraclass correlation coefficient (ICC) 0.90-0.92; coefficient of variation (CoV)19.0-20.3%) and global peak systolic torsion rate (ICC 0.82-0.84; CoV 25.9-29.0%). Con-versely, global peak diastolic torsion rate showed little inter-study reproducibility (ICC0.34-0.47; CoV 40.8-45.5%). Global peak torsion as determined by the CL shear angleshowed the best inter-study reproducibility (ICC 0.90; CoV 19.0%). CMR-FT resultswere not measurably affected by diurnal variation between morning and afternoonscans (CL shear angle: 4.8+1.4 8, 4.8+1.5 8 and 4.1+1.6 8 for Exam A, B and C, re-spectively; p = 0.21).Conclusion: CMR-FT based derivation of myocardial peak torsion and peak systolictorsion rate has high inter-study reproducibility as opposed to peak diastolic torsionrate. The CL shear angle was the most reproducible parameter independently ofcardiac anatomy and may develop into a robust tool to quantify cardiac rotationalmechanics in longitudinal CMR-FT patient studies.
P1007Impact of diabetes mellitus on cardiovascular target organ damages in patientswith end-stage renal disease
IH. Jung1; JG. Moon2; YS. Byun1; TH. Kim3; SH. Park4; HS. Seo5
1Inje University, Seoul, Korea, Republic of; 2Gachon University, Incheon, Korea, Republicof; 3Sejong General Hospital, Bucheon, Korea, Republic of; 4Yonsei University College ofMedicine, Seoul, Korea, Republic of; 5Soonchunhyang University, Buchoen, Korea,Republic of
Background: Diabetes Mellitus (DM) is the most common cause of end-stage renaldisease (ESRD) and an important risk factor for cardiovascular (CV) disease. We investi-gated the impact of DM on CV target organ damage assessed with comprehensivescreening in ESRD patients.Methods: A total of 61 ESRD patients were enrolled and 24h-ambulatory blood pressuremonitoring (ABPM), central blood pressure with pulse wave velocity (PWV) measuremen-t,echocardiography, coronary computed tomography angiogram (CCTA) were per-formed. We compared the data between DM (n=23, 58+11 years, 13 men) and non-DM (n=38, 53+12 years, 24 men) group.
Abstract P1007 Table.
DM (n=23) Non-DM (n=38) p-value
LVEDD, mm 52+5 52+6 0.964LVESD, mm 34+4 34+5 0.687LV EF, % 65+8 64+9 0.717IVSd, mm 11+2 11+2 0.852PWd, mm 11+2 11+2 0.984E, cm/s 86+25 71+23 0.021A, cm/s 100+16 86+20 0.004LVMI, g/m2 134+35 136+38 0.901E’ 5+1 5+2 0.557A’ 8+2 9+2 0.781E/E’ 17+5 14+6 0.032
Results: 1) Clinical characteristics and ABPM results were similar between the 2 groupsexcept ESRD duration (5+5 vs. 11+8yrs, p=0.006); 2) Central aortic systolic pressure
(CASP [160+24 vs. 144+29 mm Hg]) and PWV (12+3 vs. 10+2 m/s) were higher inDM group (p,0.05 for all); 3) On echocardiography, early mitral inflow to early mitralannulus velocity ratio (E/E’), which reflect left-ventricular (LV) filling pressure, washigher in DM patients (17+5 vs. 14+6, p=0.032), despite similar LV ejection fraction(65+8 vs. 64+9%, p=0.717); 4) Although, prevalence of coronary artery disease(CAD) did not differ (13 [57%] vs. 28 [74%], p=0.166), severity of CAD (.50% stenosisand region number) was higher in DM group (p=0.031); 5) DM etiology was independentpredictor for E/E’, CASP and PWV (p,0.05 for all).
P1008Paired comparison of left atrial strain in patients with atrial fibrillation by twoblack-box algorithms
E. Wellnhofer1; C. Kriatselis1; JH. Gerds-Li1; M. Kropf2; B. Pieske2; M. Graefe1
1German Heart Center Berlin, Berlin, Germany; 2Charite - University Medicine Berlin,Berlin, Germany
We compared two black-box algorithms (Philips QLAB and TomTec 2D Cardiac Perform-ance Analysis) for left atrial (LA) strain analysis.Methods: We evaluated paired data sets from 99 consecutive patients (age 61+12years, 31 females, 54 paroxysmal AF) prior to pulmonary vein isiolation (PVI). The LAwas imaged from a transthoracic 4-chamber apical view. The longitudinal strain of theLA was determined offline by speckle tracking analysis with QLAB/TomTec software.We evaluated global (GS), mean (MS), median (MedS), minimal (MinS) and maximal(MaxS) strain and standard deviation (SD) of strain values for respective cycles. Compari-son was done by a paired t-test, Wilcoxon signed-rank test and correlation analysis. Clin-ical significance of differences was assessed by comparing group differences ofrecurrence of late (≥3 months after PVI) AF within a mean follow-up of 12 months (recAF).Results: Eighteen patients with paroxysmal AF (AFparox) and 23 patients with persistentAF (AFpers) experienced recAF. The difference D between QLAB and TomTec algorithmswas significant for all variables in AFparox and in the total sample for MS, MedS, MinS,MaxS and SD. Reduced D with exception of D MinS and D GS was found in AFpers.Results from both algorithms did not correlate significantly. Standard deviation of DMaxS and D GS was inacceptable.In the AFparox subgroup TomTec strain analysis values but not Philips strain analysisvalues were significantly lower in patients with recAF. In AFpers we found no predictivevalue of strain analysis.Conclusion: QLAB strain analysis may not be recommended for LA function analysis cur-rently. LA strain analysis may be helpful in patients with AFparox to stratify risk for recur-rence of AF after PVI. Dedicated software seems necessary, however. The value ofstrain analysis in AFpers appears to be limited right now.
Abstract P1008 Table. Comparison of strain values
TomTecTM QLABTM D D AFparox D AFpers
GS (%) 23.7+13.4 21.8+21.6 1.9+24.6 7.3+30.6 4.5+12.3MS (%) 9.6+6.6 6.9+7.3 2.1+9.1 4.9+10.1 20.2+6.8MedS (%) 8.8+6.8 6.5+7.4 2.3+9.1 4.7+9.4 20.7+7.9MinS (%) 21.7+1.9 23.1+3.1 1.4+3.6 0.3+2.6 2.7+4.2MaxS (%) 21.9+13.2 18.7+22.0 3.3+24.6 7.5+30.1 21.7+12.1SD (%) 7.6+4.0 6.3+4.4 1.3+5.9 3.1+6.5 20.9+4.1
P1009Effect of glycaemic status on left ventricular diastolic function detected by pulsedtissue doppler imaging in type 2 diabetes patients
M. Eldeep; K. Marghany; M. Mokarrab; M. AlbazAl-Azhar University, cardiology, Cairo, Egypt
Background: Diabetes mellitus is considering an important independent factor in devel-oping diastolic dysfunction. Diastolic dysfunction comprises about 30 to 50% of allpatients hospitalized for heart failure, The dramatic increase in hospitalization for heartfailure among the elderly can be largely attributed to this condition. The aim of thisstudy was to determine the effect of glycaemic status on left ventricular diastolic functionby pulsed tissue Doppler imaging in type 2 diabetic patientsMethods and Results: our study included (100) subjects,20 normal healthy subjects, 80known to be Diabetic patients presented in our diabetic outpatient clinic and Echocardio-graphic unit at Al-Hussein University Hospital between November 2010 and June2011.the patient were classified according glycaemic status in to three groups: Group (A)Normal healthy control subjects. Group (B)well controlled diabetes HbA1C less than 7,Group (C) uncontrolled diabetes HbA1C more than 7. There was no statistically significantdifference between the three groups as regard LVEDD,LVESD,LV EF% and LVFS%. Therewas statistically significant difference between the three groups as regard LA mean Ewave mean of A wave mean of E/A ratio diameter mean of DT mean of IVRT mean of Emwave mean of E/Em degree of diastolic dysfunction. There was statistically significant differ-ence in patient have LV diastolic dysfunction between the three groups as regard E wave, Awave,DT,andIVRT.but therewasnostatisticaldifferencebetweenpatienthavediastolicdys-function as regard mean of Em.There was negative correlation between HbA1c level andEwave, E/A, Em and positive correlation with LA, A wave, IVRT, DTand E/Em.Conclusions: The Glycemic status is well correlated with severity of diastolic dysfunctionin asymptomatic type 2 diabetic patients.Tissue Doppler imaging has been shown to bemore sensitive and more independent from various confounders, such as preload. for
Abstracts ii161
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

assessment of diastolic function in asymptomatic type 2 diabetic patients and its resultsare significant correlated with glycaemic state.
ISCHEMIC HEART DISEASE
P1010Increasedvalue ofcoronary calciumscore was associatedwith higherprevalenceof vulnerable plaques: study with cardiac tomography
P.Marcos-AlbercaMoreno; L.Perez-Isla; J.Palacios; JJ.GomezDeDiego; JA. De Agustin;M. Luaces; P. Mahia; J. Arrazola; MA. Garcia-Fernandez; C. MacayaHospital Clinic San Carlos, Madrid, Spain
Background: Increased valueofcoronarycalcium (Agatston score) isapredictorofmajorcoronary events in population at risk. Coronary angiography with multislice computedtomography (MDCT) allows the characterization of atherosclerotic plaque. Recent dataare conflicting concerning the prognosis of high values of calcium score (CS).Objective: To study the prevalence of different types of plaque (soft, calcified, or mixed)and its association with CSMethods: We studied 145 consecutive patients (P) with 64-MDCT. All P were pretreatedwith beta-blockers, unless contraindications to obtain sinus rhythm ,65 bpm and 0.4mg of sublingual nitroglycerin. Fixed phases at 75% and 40 of RR interval were used forstandardized retrospective reconstruction. Postprocessing accomplished with doublereading. Quantification of SC, the modified Agatston method was used. We excludedthe PP with SC = 0.Results: A total of 1907 segments corresponding to 126 P with CS. 0 were analyzed.Mean age was 66+11 year old, 79% were male and CS . 100 in 75%. In this group,75% of segments analyzed showed 78% of total plaques observed. The figure showshow in P with CS. 100, the prevalence of soft and mixed plaques was higher than Pwith CS ,100 (p ,0.001).Conclusion: Patients with more calcium in coronary arteries: 1) showed the greatest se-verity in number of affected segments and plaques observed 2) the prevalence of vulner-able plaques was significantly higher. Both data could drive statin and/or antiplatelettherapy improving outcomes in high CS.
P1011Comparison of fractional flow reserve and treadmill stress echocardiopgrahy:correlation and outcome in 51 patients
C H. Attenhofer Jost1; P. Mueller1; B. Naegeli1; P. Levis1; FW. Amann1; B. Seifert2;D. Maurer2; O. Bertel21Cardiovascular Center Zurich Klinik Im Park, Zurich, Switzerland; 2University of Zurich,Institute of Social and Preventive Medicine, Biostatistics Unit, Zurich, Switzerland
Background: Both, fractional flow reserve (FFR) and treadmill stress echocardiography(TSE), are used to predict provokable ischemia and outcome of coronary artery disease(CAD) with an accuracy of .90% (FFR) and 85% (TSE). There are no data on their com-parison in the literature.Method: In all patients (pt) who had both TSE and FFR (by coronary angiography) within90 days without intervening revascularization, findings were compared. If possible, long-term outcome was assessed. FFR was determined with intravenous adenosine (140mcg/kg/min); a value of ,0.8 was determined as pathological. Quantitative coronary angiog-raphy (QCA) was done as previously described. FFR was performed if needed to assesscoronary artery stenosis of uncertain significance.Results: Between 2008 and 2014, there were 51 patients (36 males) who fulfilled the inclu-sion criteria. 21 pt had history of prior revascularization by stenting/coronary artery bypassgrafting. Median time interval between TSE and coronary angiography was 26 days.Average age was 67+9 years, betablocker therapy was taken by 30pt. Any ischemia
in TSE was present in 43 pt (by echocardiography) respectively in 30 pt by ECG criteria.CAD ≥50% stenosis by QCA was present in 46 pt, single vessel disease in 22pt and multi-vessel disease in 24pt.FFR guided revascularization was performed in 25 pt. In those patients undergoing FFRguided revascularization, the number of ischemic segments by TSE und the ECG signsof ischemia were not significantly different from the patients without revascularization.Follow-upwasavailable in 40ptafter anaverageof2.9+1.9years. Later revascularizationwas necessary in 10 patients: in 4 pts in whom by FFR initially no revasularization was per-formed, and in 6 pt with initial FFR guided revascularization; only one oft the patientsneeding revascularization had a negative TSE. In no patient, an acute coronary syndromewas observed during follow-up.Conclusion: In intermediate/unclear coronary artery stenoses, FFR and TSE have an ac-ceptable concordance. However, differences do occur. Both methods can not predict orexclude the necessity of revascularizations in the future.
P1012Longitudinal 2D strain can efficiently diagnose CAD and localize the culprit lesionin patients with suspected NSTE-ACS but apparent normal global and regionalsystolic function
T. Caspar; H. Samet; L. Jesel; H. Petit-Eisenmann; A. Trinh; S. Talha; O. Morel; P. OhlmannUniversity Hospital of Strasbourg, Department of Cardiology, Strasbourg, France
Purpose: The clinical work-up of patients presenting with chest pain is a diagnostic chal-lenge. Conventional echocardiography is not informative in half of the cases. We investi-gated the diagnostic performance of global (GLS) and territorial (TLS) longitudinal strainto predict coronary artery disease (CAD) in patients presenting with suspected non-ST-segment elevation acute coronary syndrome (NSTE-ACS) but apparent normal globaland regional systolic function.Methods: 58 patients with suspected NSTE-ACS but normal LVEF (≥ 55%) and WMSI(=1) were prospectively enrolled. Speckle-tracking echocardiography was performedon admission and all the patients underwent angio-coronarography. CAD was definedas the presence of stenosis of . 50%.Results: CAD was present in 33 patients (57%). LVEF was 60.7+4.6% in group 1 (CAD)and 61.1+5.0% in group 2 (no CAD). Global longitudinal strain (GLS) was altered ingroup1 (-16.7+3.4%)as compared togroup2 (-22.4+2.9%, p,0.001). ROCcurveana-lysis showed a high diagnostic value of GLS for the prediction of CAD (AUC = 0.92 [0.84 -1.00], p=0.0001) with a sensitivity of 81% and a specificity of 88% at the optimal cut-off of219.7%. When the cut-off value of GLS was increased to ?21%, the sensitivity reached100%withaspecificityof68%. ThediagnosticvalueofGLS forCADin thestudypopulationwas significant whether troponin was positive (AUC=0.87 [0.74 - 1.00], p,0.001) or nega-tive (AUC=0.96[0.88 - 1.00],p,0.01).Diagnostic valuesof Troponin Ic (AUC=0.66),ECG(AUC=0.63), LVEF (AUC=0.52) and GRACE score (AUC=0.55) were significantly lowerthan for GLS (p,0.001). Territorial longitudinal strain (TLS) was able to discriminatebetween coronary stenosis in the LAD, LCX or RCA (AUC=0.93, 0.81 and 0.70 respective-ly, p,0.05).Conclusions:Longitudinal 2D strain has agood diagnostic valueand canefficiently local-ize the culprit lesion in patients presenting with NSTE-ACS but apparent normal globaland regional systolic function.
P1014Impaired right ventricle systolic function is associated with heart failure andmortality in ST-elevation myocardial infarction patients
S. Leao; F. Cordeiro; P. Magalhaes; M. Moz; J. Trigo; P. Mateus; P. Fontes; I. MoreiraHospital Center of Tras-os-Montes and Alto Douro, Cardiology, Vila Real, Portugal
Purpose: Right Ventricular dysfunction (RVD), assessed by fractional area change hasbeen reported as a strong predictor of major complications and in-hospital mortalityafter ST-elevation myocardial infarction (STEMI), although the understanding of itsimpact on long-term prognosis is scarce. Moreover, assessment of right ventricular frac-tional area change is challenging and time consuming. We intend to determine the long-term prognostic impact of RVD assessed by simple echocardiographic parameters(TAPSE or tricuspid s’ velocity).Methods: Retrospective study of 226 consecutive patients admitted for STEMI and under-going primary percutaneous intervention (PPCI), which have right ventricle assessmentduring index admission. Right ventricle dysfunction was defined as TAPSE , 1.7 cmand/or tricuspid s’ velocity , 9.5cm/s. Population was divided in two groups accordingto the presence of RVD. Primary endpoint was a composite of death and readmissionfor heart failure. Analysis of the time to first adverse clinical event was performed usinga Cox proportional hazards models.Results: RVD was present in 32 patients (14,2%). The two groups were not significantlydifferent in terms of gender, cardiovascular risk factors or infarct location. Those withRVD were significantly older (70+11 vs 64+13 years, p=0.021).Patients with RVDpresented worst clinical course during hospitalization, withkillip class ≥2 in 71.9% vs 32.1% (p,0.001) and cardiogenic shock in 18.8% vs 5.7% (p=0.02).After a mean follow-up of 15 months (Inter Quartile Range 10-25), RVD patients presented ahigher incidence of the composite endpoint of death or readmission for heart failure (HF)(Hazard Ratio (HR): 2.75, 95% Confidence Interval (CI): 1.46-5.18, p=0.002). In multivariateanalysis including age, left ventricle ejection fraction (LVEF) and culprit vessel, RVD provedto be an independent predictor of death or HF (HR: 2.10, 95% CI: 1.08-4.07, p=0.028).Conclusions: RVD, assessed by simple parameters such as TAPSE or s’ velocity, predictspoor outcome in STEMI patients undergoing PPCI. These measures are reliable, easy toacquire and improve identification ofpatientswith RVD even in the absence of clinical signs.It has additive prognostic value to LVEF, culprit vessel or age.
Abstract P1010 Figure. Vulnerable Plaque & Calcium Score
ii162 Abstracts
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022
P1015Prediction of recovery of left ventricular systolic function after primarypercutaneous coronary intervention in patients with acute STEMI by Dopplercoronary artery flow and myocardial stunning index
D. Sharif1; W. Matanis2; A. Sharif-Rasslan2; Y. Sharif2; U. Rosenschein1
1Bnai Zion Medical Center, Haifa, Israel; 2Technion, Haifa, Israel
Myocardial stunning is responsible for partially reversible left ventricular (LV) systolic dys-function after successful primary percutaneous coronary intervention in patients withacute ST-elevation myocardial infarction (STEMI).Aim: To test the hypothesis that early coronary blood flow (CBF) to LV systolic functionratios, as an equivalent to LV stunning index (SI), predict recovery of LV systolic functionPPCI in patients with acute STEMI.Methods: 24 patients with acute anterior STEMI who had successful PPCI were evalu-ated. Transthoracic echocardiography with measurement of LV ejection fraction (EF),LV and left anterior descending (LAD) coronary artery area wall motion score index(WMSI) as well as Doppler sampling of LAD blood velocities, early after PPCI and 5days later were performed. SI was evaluated as the earl ratio of CBF parameters in theLAD to LV systolic function parameters.Results: Early SI-LVEF well predicted late LVEF (r=0.51, p,0.01) and the change in LVEF(r=0.48, p,0.017). Early SI-LVMSI predicted well late LVEF (r=0.56, p,0.006) and thechange in LVEF (r=0.46, p,0.028). Early SI-LADWMSI predicted late LVEF (r=0.44,p,0.028). Other SI indices measured as other LAD-CBF to LV systolic function para-meters were not predictive of late LV systolic function.Conclusions: LV stunning indices measured as early LAD flow to LVEF, LVWMSI andLADWMSI ratios, well predicted late LVEF and the change in LVEF. Thus greater early cor-onary artery flow to LV systolic function parameter ratios, predict a better improvement inlate LV systolic function after PPCI.
P1016Global longitudinalstrainandcoronarymicrocirculationstatus inpredictionof leftventricle functional recovery after STelevation myocardium infarction
M. Faustino; S. Bravo Baptista; A. Freitas; J. Bicho Augusto; P. Leal; M. Nedio; C. Antunes;P. Farto E Abreu; V. Gil; C. MoraisHospital Prof. Dr. Fernando Fonseca, EPE, Amadora, Portugal
Purpose: The extent of microvascular dysfunction has been correlated with recovery ofleft ventricular (LV) function in patients with ST elevation myocardium infarction(STEMI), treated with primary angioplasty. Longitudinal myocardial strain after STEMI isalso a predictor of LV recovery, and a few studies demonstrated its relationship with micro-circulation function. The purpose of this study was to evaluate if the global longitudinalstrain can mediate the relationship between the state of coronary microcirculation evalu-ated invasively and the recovery of LV function.Methods: Coronary microcirculation was evaluated by the index of microcirculatory resist-ance (IMR) at the end of angioplasty. Echocardiograms were performed in the first 24 hours(Echo1) and after about 3 months (Echo2). Left ventricle ejection fraction (LVEF), wallmotion score index (WMSI), and global longitudinal strain (GLS) were measured.Results: 40 STEMI patients (mean age 59.3+/-12.7 years, 34 males) were included. GLSmedian was 213.9% (interquartile range 2.9). IMR median was 25.9 (interquartile range32.5) and patients were divided in two groups: Group1 (IMR ,26, with less microvasculardysfunction) and Group2 (IMR.=26, with more microvascular dysfunction).In Echo1 GLS was significantly better in Group1 patients than in Group2 (214.9 vs 212.9,p=0.005), however no other differences were found between groups in what concernsLVEF (0.48+0.06 vs 0.49+0.06, p=0.66) and WMSI (1.46+0.24 vs 1.52+0.22,p=0.38). IMR correlated positively and significantly with the GLS (R=0.6, p=0.001).Between Echo1 and Echo2, there were significant improvements in LVEF (0.48+0.06vs 0.55+0.06, p,0.0001) only in group 1, and WMSI improved significantly more inthis group (reduction of 217.1% vs 26.8% in Group 2, p = 0.015). The initial GLS corre-lated significantly with WMSI in Echo 2 (r=0.57, p=0.001), although no correlation withLVEF (r=0.17, p=0.359) was found. Patients were divided into two groups according tothe median GLS, verifying that the group with better strain also had the lower WMSI inecho 2 (1.218+0.04 VS 1.459+0.56, p=0.002), in spite of no differences in LVEF(0.53+0.02 vs0.52+0.01 p=0.352).Conclusion: Myocardial GLS early after infarction correlates with IMR evaluatedimmediately after primary angioplasty. IMR is associated with the recovery of cardiacfunction evaluated by the LVEF and WMSI and GLS also predicts cardiac recover evalu-ated by WMSI. This preliminary data suggest that strain could infer non-invasively theextent of microvascular integrity and predict ventricular recovery, deserving furtherinvestigation.
HEART VALVE DISEASES
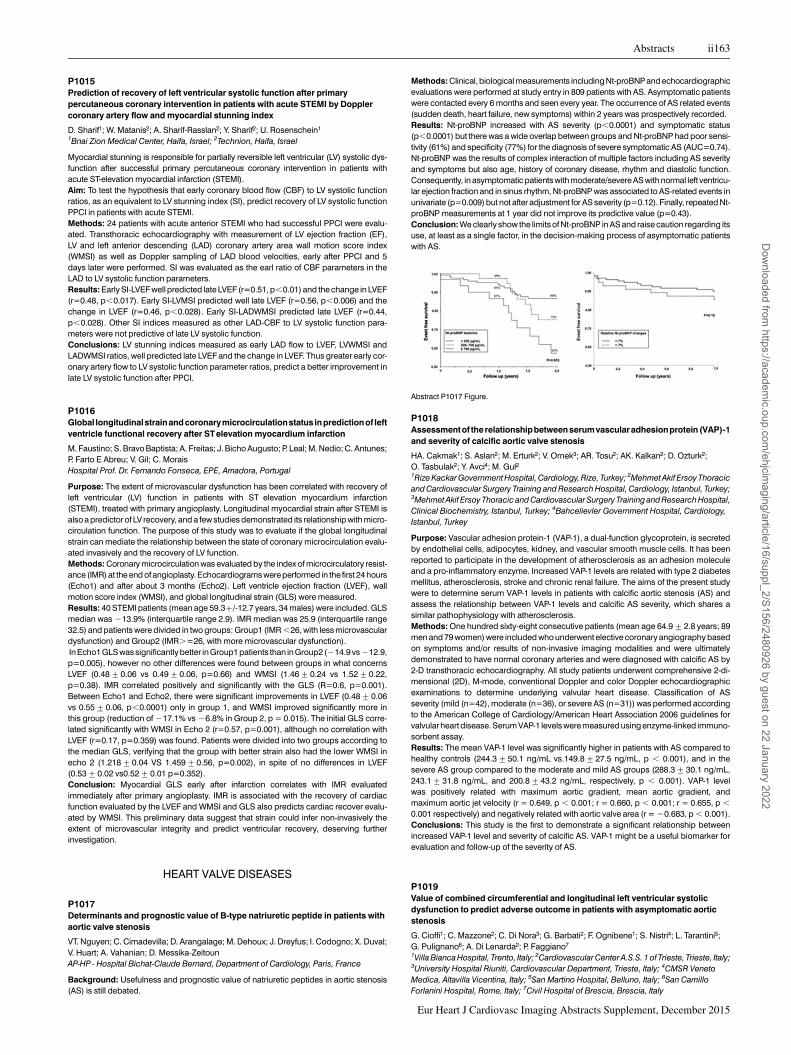
P1017Determinants and prognostic value of B-type natriuretic peptide in patients withaortic valve stenosis
VT. Nguyen; C. Cimadevilla; D. Arangalage; M. Dehoux; J. Dreyfus; I. Codogno; X. Duval;V. Huart; A. Vahanian; D. Messika-ZeitounAP-HP - Hospital Bichat-Claude Bernard, Department of Cardiology, Paris, France
Background: Usefulness and prognostic value of natriuretic peptides in aortic stenosis(AS) is still debated.
Methods: Clinical, biological measurements including Nt-proBNPand echocardiographicevaluations were performed at study entry in 809 patients with AS. Asymptomatic patientswere contacted every 6 months and seen every year. The occurrence of AS related events(sudden death, heart failure, new symptoms) within 2 years was prospectively recorded.Results: Nt-proBNP increased with AS severity (p,0.0001) and symptomatic status(p,0.0001) but there was a wide overlap between groups and Nt-proBNP had poor sensi-tivity (61%) and specificity (77%) for the diagnosis of severe symptomatic AS (AUC=0.74).Nt-proBNP was the results of complex interaction of multiple factors including AS severityand symptoms but also age, history of coronary disease, rhythm and diastolic function.Consequently, in asymptomatic patients with moderate/severe AS with normal left ventricu-lar ejection fraction and in sinus rhythm, Nt-proBNP was associated to AS-related events inunivariate (p=0.009) but not after adjustment for AS severity (p=0.12). Finally, repeated Nt-proBNP measurements at 1 year did not improve its predictive value (p=0.43).Conclusion: We clearly show the limits of Nt-proBNP in AS and raise caution regarding itsuse, at least as a single factor, in the decision-making process of asymptomatic patientswith AS.
P1018Assessmentof the relationshipbetweenserumvascularadhesionprotein (VAP)-1and severity of calcific aortic valve stenosis
HA. Cakmak1; S. Aslan2; M. Erturk2; V. Ornek3; AR. Tosu2; AK. Kalkan2; D. Ozturk2;O. Tasbulak2; Y. Avci4; M. Gul21Rize Kackar Government Hospital, Cardiology, Rize, Turkey; 2Mehmet Akif Ersoy Thoracicand Cardiovascular Surgery Training and Research Hospital, Cardiology, Istanbul, Turkey;3Mehmet Akif Ersoy Thoracic and Cardiovascular Surgery Training and Research Hospital,Clinical Biochemistry, Istanbul, Turkey; 4Bahcelievler Government Hospital, Cardiology,Istanbul, Turkey
Purpose: Vascular adhesion protein-1 (VAP-1), a dual-function glycoprotein, is secretedby endothelial cells, adipocytes, kidney, and vascular smooth muscle cells. It has beenreported to participate in the development of atherosclerosis as an adhesion moleculeand a pro-inflammatory enzyme. Increased VAP-1 levels are related with type 2 diabetesmellitus, atherosclerosis, stroke and chronic renal failure. The aims of the present studywere to determine serum VAP-1 levels in patients with calcific aortic stenosis (AS) andassess the relationship between VAP-1 levels and calcific AS severity, which shares asimilar pathophysiology with atherosclerosis.Methods: One hundred sixty-eight consecutive patients (mean age 64.9+2.8 years; 89men and 79 women) were included who underwent elective coronary angiography basedon symptoms and/or results of non-invasive imaging modalities and were ultimatelydemonstrated to have normal coronary arteries and were diagnosed with calcific AS by2-D transthoracic echocardiography. All study patients underwent comprehensive 2-di-mensional (2D), M-mode, conventional Doppler and color Doppler echocardiographicexaminations to determine underlying valvular heart disease. Classification of ASseverity (mild (n=42), moderate (n=36), or severe AS (n=31)) was performed accordingto the American College of Cardiology/American Heart Association 2006 guidelines forvalvular heart disease. Serum VAP-1 levels were measured using enzyme-linked immuno-sorbent assay.Results: The mean VAP-1 level was significantly higher in patients with AS compared tohealthy controls (244.3+50.1 ng/mL vs.149.8+27.5 ng/mL, p , 0.001), and in thesevere AS group compared to the moderate and mild AS groups (288.3+30.1 ng/mL,243.1+31.8 ng/mL, and 200.8+43.2 ng/mL, respectively, p , 0.001). VAP-1 levelwas positively related with maximum aortic gradient, mean aortic gradient, andmaximum aortic jet velocity (r = 0.649, p , 0.001; r = 0.660, p , 0.001; r = 0.655, p ,
0.001 respectively) and negatively related with aortic valve area (r = 20.683, p , 0.001).Conclusions: This study is the first to demonstrate a significant relationship betweenincreased VAP-1 level and severity of calcific AS. VAP-1 might be a useful biomarker forevaluation and follow-up of the severity of AS.
P1019Value of combined circumferential and longitudinal left ventricular systolicdysfunction to predict adverse outcome in patients with asymptomatic aorticstenosis
G. Cioffi1; C. Mazzone2; C. Di Nora3; G. Barbati2; F. Ognibene1; S. Nistri4; L. Tarantini5;G. Pulignano6; A. Di Lenarda2; P. Faggiano7
1Villa Bianca Hospital, Trento, Italy; 2Cardiovascular Center A.S.S. 1 of Trieste, Trieste, Italy;3University Hospital Riuniti, Cardiovascular Department, Trieste, Italy; 4CMSR VenetoMedica, Altavilla Vicentina, Italy; 5San Martino Hospital, Belluno, Italy; 6San CamilloForlanini Hospital, Rome, Italy; 7Civil Hospital of Brescia, Brescia, Italy
Abstract P1017 Figure.
Abstracts ii163
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022
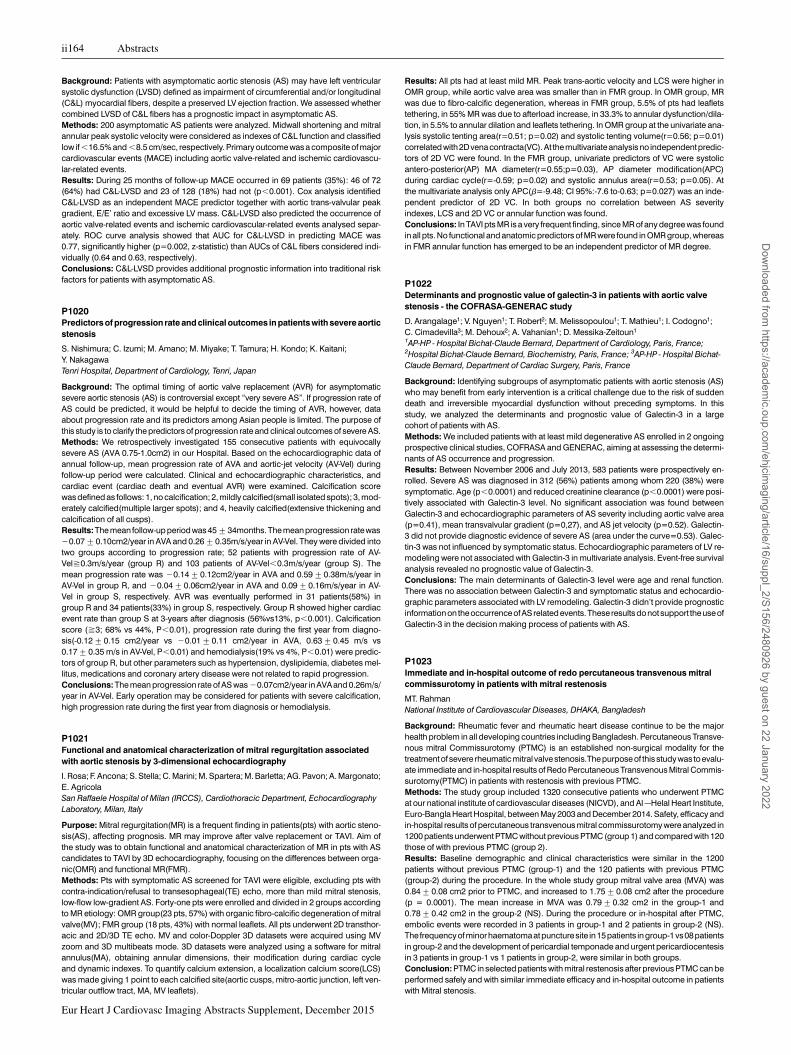
Background: Patients with asymptomatic aortic stenosis (AS) may have left ventricularsystolic dysfunction (LVSD) defined as impairment of circumferential and/or longitudinal(C&L) myocardial fibers, despite a preserved LV ejection fraction. We assessed whethercombined LVSD of C&L fibers has a prognostic impact in asymptomatic AS.Methods: 200 asymptomatic AS patients were analyzed. Midwall shortening and mitralannular peak systolic velocity were considered as indexes of C&L function and classifiedlow if ,16.5% and ,8.5 cm/sec, respectively. Primary outcome was a composite of majorcardiovascular events (MACE) including aortic valve-related and ischemic cardiovascu-lar-related events.Results: During 25 months of follow-up MACE occurred in 69 patients (35%): 46 of 72(64%) had C&L-LVSD and 23 of 128 (18%) had not (p,0.001). Cox analysis identifiedC&L-LVSD as an independent MACE predictor together with aortic trans-valvular peakgradient, E/E’ ratio and excessive LV mass. C&L-LVSD also predicted the occurrence ofaortic valve-related events and ischemic cardiovascular-related events analysed separ-ately. ROC curve analysis showed that AUC for C&L-LVSD in predicting MACE was0.77, significantly higher (p=0.002, z-statistic) than AUCs of C&L fibers considered indi-vidually (0.64 and 0.63, respectively).Conclusions: C&L-LVSD provides additional prognostic information into traditional riskfactors for patients with asymptomatic AS.
P1020Predictors of progression rate and clinical outcomes in patients with severe aorticstenosis
S. Nishimura; C. Izumi; M. Amano; M. Miyake; T. Tamura; H. Kondo; K. Kaitani;Y. NakagawaTenri Hospital, Department of Cardiology, Tenri, Japan
Background: The optimal timing of aortic valve replacement (AVR) for asymptomaticsevere aortic stenosis (AS) is controversial except “very severe AS”. If progression rate ofAS could be predicted, it would be helpful to decide the timing of AVR, however, dataabout progression rate and its predictors among Asian people is limited. The purpose ofthis study is to clarify the predictors of progression rate and clinical outcomes of severe AS.Methods: We retrospectively investigated 155 consecutive patients with equivocallysevere AS (AVA 0.75-1.0cm2) in our Hospital. Based on the echocardiographic data ofannual follow-up, mean progression rate of AVA and aortic-jet velocity (AV-Vel) duringfollow-up period were calculated. Clinical and echocardiographic characteristics, andcardiac event (cardiac death and eventual AVR) were examined. Calcification scorewas defined as follows: 1, no calcification; 2, mildly calcified(small isolated spots); 3, mod-erately calcified(multiple larger spots); and 4, heavily calcified(extensive thickening andcalcification of all cusps).Results: The mean follow-up period was 45+34months. The mean progression ratewas20.07+0.10cm2/year in AVA and 0.26+0.35m/s/year in AV-Vel. They were divided intotwo groups according to progression rate; 52 patients with progression rate of AV-Vel^0.3m/s/year (group R) and 103 patients of AV-Vel,0.3m/s/year (group S). Themean progression rate was 20.14+0.12cm2/year in AVA and 0.59+0.38m/s/year inAV-Vel in group R, and 20.04+0.06cm2/year in AVA and 0.09+0.16m/s/year in AV-Vel in group S, respectively. AVR was eventually performed in 31 patients(58%) ingroup R and 34 patients(33%) in group S, respectively. Group R showed higher cardiacevent rate than group S at 3-years after diagnosis (56%vs13%, p,0.001). Calcificationscore (^3; 68% vs 44%, P,0.01), progression rate during the first year from diagno-sis(-0.12+0.15 cm2/year vs 20.01+0.11 cm2/year in AVA, 0.63+0.45 m/s vs0.17+0.35 m/s in AV-Vel, P,0.01) and hemodialysis(19% vs 4%, P,0.01) were predic-tors of group R, but other parameters such as hypertension, dyslipidemia, diabetes mel-litus, medications and coronary artery disease were not related to rapid progression.Conclusions: The mean progression rate of AS was 20.07cm2/year in AVAand 0.26m/s/year in AV-Vel. Early operation may be considered for patients with severe calcification,high progression rate during the first year from diagnosis or hemodialysis.
P1021Functional and anatomical characterization of mitral regurgitation associatedwith aortic stenosis by 3-dimensional echocardiography
I. Rosa; F. Ancona; S. Stella; C. Marini; M. Spartera; M. Barletta; AG. Pavon; A. Margonato;E. AgricolaSan Raffaele Hospital of Milan (IRCCS), Cardiothoracic Department, EchocardiographyLaboratory, Milan, Italy
Purpose: Mitral regurgitation(MR) is a frequent finding in patients(pts) with aortic steno-sis(AS), affecting prognosis. MR may improve after valve replacement or TAVI. Aim ofthe study was to obtain functional and anatomical characterization of MR in pts with AScandidates to TAVI by 3D echocardiography, focusing on the differences between orga-nic(OMR) and functional MR(FMR).Methods: Pts with symptomatic AS screened for TAVI were eligible, excluding pts withcontra-indication/refusal to transesophageal(TE) echo, more than mild mitral stenosis,low-flow low-gradient AS. Forty-one pts were enrolled and divided in 2 groups accordingto MR etiology: OMR group(23 pts, 57%) with organic fibro-calcific degeneration of mitralvalve(MV); FMR group (18 pts, 43%) with normal leaflets. All pts underwent 2D transthor-acic and 2D/3D TE echo. MV and color-Doppler 3D datasets were acquired using MVzoom and 3D multibeats mode. 3D datasets were analyzed using a software for mitralannulus(MA), obtaining annular dimensions, their modification during cardiac cycleand dynamic indexes. To quantify calcium extension, a localization calcium score(LCS)was made giving 1 point to each calcified site(aortic cusps, mitro-aortic junction, left ven-tricular outflow tract, MA, MV leaflets).
Results: All pts had at least mild MR. Peak trans-aortic velocity and LCS were higher inOMR group, while aortic valve area was smaller than in FMR group. In OMR group, MRwas due to fibro-calcific degeneration, whereas in FMR group, 5.5% of pts had leafletstethering, in 55% MR was due to afterload increase, in 33.3% to annular dysfunction/dila-tion, in 5.5% to annular dilation and leaflets tethering. In OMR group at the univariate ana-lysis systolic tenting area(r=0.51; p=0.02) and systolic tenting volume(r=0.56; p=0.01)correlated with2Dvena contracta(VC). At the multivariateanalysis no independentpredic-tors of 2D VC were found. In the FMR group, univariate predictors of VC were systolicantero-posterior(AP) MA diameter(r=0.55;p=0.03), AP diameter modification(APC)during cardiac cycle(r=-0.59; p=0.02) and systolic annulus area(r=0.53; p=0.05). Atthe multivariate analysis only APC(b=-9.48; CI 95%:-7.6 to-0.63; p=0.027) was an inde-pendent predictor of 2D VC. In both groups no correlation between AS severityindexes, LCS and 2D VC or annular function was found.Conclusions: In TAVI pts MR is a very frequent finding, since MR of any degree was foundin all pts. No functional and anatomic predictors of MR were found in OMR group, whereasin FMR annular function has emerged to be an independent predictor of MR degree.
P1022Determinants and prognostic value of galectin-3 in patients with aortic valvestenosis - the COFRASA-GENERAC study
D. Arangalage1; V. Nguyen1; T. Robert2; M. Melissopoulou1; T. Mathieu1; I. Codogno1;C. Cimadevilla3; M. Dehoux2; A. Vahanian1; D. Messika-Zeitoun1
1AP-HP - Hospital Bichat-Claude Bernard, Department of Cardiology, Paris, France;2Hospital Bichat-Claude Bernard, Biochemistry, Paris, France; 3AP-HP - Hospital Bichat-Claude Bernard, Department of Cardiac Surgery, Paris, France
Background: Identifying subgroups of asymptomatic patients with aortic stenosis (AS)who may benefit from early intervention is a critical challenge due to the risk of suddendeath and irreversible myocardial dysfunction without preceding symptoms. In thisstudy, we analyzed the determinants and prognostic value of Galectin-3 in a largecohort of patients with AS.Methods: We included patients with at least mild degenerative AS enrolled in 2 ongoingprospective clinical studies, COFRASA and GENERAC, aiming at assessing the determi-nants of AS occurrence and progression.Results: Between November 2006 and July 2013, 583 patients were prospectively en-rolled. Severe AS was diagnosed in 312 (56%) patients among whom 220 (38%) weresymptomatic. Age (p,0.0001) and reduced creatinine clearance (p,0.0001) were posi-tively associated with Galectin-3 level. No significant association was found betweenGalectin-3 and echocardiographic parameters of AS severity including aortic valve area(p=0.41), mean transvalvular gradient (p=0,27), and AS jet velocity (p=0.52). Galectin-3 did not provide diagnostic evidence of severe AS (area under the curve=0.53). Galec-tin-3 was not influenced by symptomatic status. Echocardiographic parameters of LV re-modeling were not associated with Galectin-3 in multivariate analysis. Event-free survivalanalysis revealed no prognostic value of Galectin-3.Conclusions: The main determinants of Galectin-3 level were age and renal function.There was no association between Galectin-3 and symptomatic status and echocardio-graphic parameters associated with LV remodeling. Galectin-3 didn’t provide prognosticinformationon theoccurrence ofASrelated events.These results donotsupport theuse ofGalectin-3 in the decision making process of patients with AS.
P1023Immediate and in-hospital outcome of redo percutaneous transvenous mitralcommissurotomy in patients with mitral restenosis
MT. RahmanNational Institute of Cardiovascular Diseases, DHAKA, Bangladesh
Background: Rheumatic fever and rheumatic heart disease continue to be the majorhealth problem in all developing countries including Bangladesh. Percutaneous Transve-nous mitral Commissurotomy (PTMC) is an established non-surgical modality for thetreatment of severe rheumatic mitral valve stenosis.The purpose of this study was to evalu-ate immediate and in-hospital results of Redo Percutaneous Transvenous Mitral Commis-surotomy(PTMC) in patients with restenosis with previous PTMC.Methods: The study group included 1320 consecutive patients who underwent PTMCat our national institute of cardiovascular diseases (NICVD), and Al –Helal Heart Institute,Euro-Bangla Heart Hospital, between May 2003 and December 2014. Safety, efficacy andin-hospital results of percutaneous transvenous mitral commissurotomy were analyzed in1200 patients underwent PTMC without previous PTMC (group 1) and compared with 120those of with previous PTMC (group 2).Results: Baseline demographic and clinical characteristics were similar in the 1200patients without previous PTMC (group-1) and the 120 patients with previous PTMC(group-2) during the procedure. In the whole study group mitral valve area (MVA) was0.84+0.08 cm2 prior to PTMC, and increased to 1.75+0.08 cm2 after the procedure(p = 0.0001). The mean increase in MVA was 0.79+0.32 cm2 in the group-1 and0.78+0.42 cm2 in the group-2 (NS). During the procedure or in-hospital after PTMC,embolic events were recorded in 3 patients in group-1 and 2 patients in group-2 (NS).The frequencyofminor haematomaatpuncture site in15patients in group-1vs08patientsin group-2 and the development of pericardial temponade and urgent pericardiocentesisin 3 patients in group-1 vs 1 patients in group-2, were similar in both groups.Conclusion: PTMC in selected patients with mitral restenosis after previous PTMC can beperformed safely and with similar immediate efficacy and in-hospital outcome in patientswith Mitral stenosis.
ii164 Abstracts
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

P1024Speckle-tracking echocardiography for the aortopathy evaluation in bicuspidaortic valve
C. Zito1; L. Longobardo1; M. Cusma Piccione1; M. Zucco1; M. D’angelo1; L. Rivetti1;ML. Carerj1; I. Boretti1; MP. Calabro2; S. Carerj11University of Messina, Department of Cardiology, Messina, Italy; 2University of Messina,Pediatric Cardiology Division, Messina, Italy
Bicuspid aortic valve (BAV) is one of the most common congenital heart diseases, fre-quently associated with diffused alterations of aortic wall. The aim of this study is todetect whether increased aortic stiffness, very often found in these patients, and tradition-ally evaluated through echocardiography,has acorrelation with aortic strain, evaluated byspeckle tracking imaging (STI) technique.Methods: We enrolled 43 patients (mean age 36,5+16,2 years) with BAV and 13 normalsubjects (mean age 30,9+10,6 years), with comparable age and body surface area(BSA). We obtained all the measurements of aortic diameters (annulus, sinus of Valsalva(SV), sinu-tubular junction (STJ) and ascending aorta) by a parasternal long-axis view andindexed them for BSA. Aortic stiffness was calculated using the formula [ln(SBP/DBP)/[(AoS -AoD)/AoD], according to what already shown in literature, where AoS and AoDwere systolic and diastolic diameters respectively, and SBP and DBP, systolic and diastolicblood pressure, respectively. Longitudinal strain (LS) of ascending aorta has been estimatedas theaveragebetweenanteriorandposterioraorticwallsstrainvalues; thesemeasurementswere obtained off-line by a software for STI analysis (Echopac, GE Horten, Norway). Thesamesoftwareallows the calculation ofascending aorta circumferential strain (CS), obtainedby the parasternal short-axis view at the level of aortic root, just above the valve leaflets.Results: Ascending aorta was larger in BAV patients than in controls (17+7,7 mm/m2 vs.10,5+6,2 mm/m2; p=0,001). Aortic stiffness was increased in BAV patients compared tocontrols (8,63+7,39 vs 3,77+1,75; p = 0,003), whereas LS by STI was significantlyreduced (22,9+7,7 vs 48,8+13; p = 0,001). In overall population, aortic stiffness wasinversely related with left ventricle ejection fraction (r=-0,40, p=0.007) and aortic LS, esti-mated by STI (r = - 0,46; p = 0,014), whereas it was directly related with age (r=0,55,p,0.001) and aortic diameters (r=0,36, p=0,01; r=0,50, p=0,001; r= 0,42, p=0,005for SV, STJ and ascending aorta, respectively). An inverse relation has been found alsobetween CS, estimated by STI, and aortic diameters (r=-0,35, p = 0,019; r=-0,41, p =0,004; r=0,38, p = 0,009, for SV, STJ and ascending aorta, respectively).Conclusions: BAV is often associated with aortic elasticity impairment. Aortic LS and CSby STI well correlate with aortic dimensions and stiffness. STI allows a new evaluation ofaorthopathy that could be applyed in different BAV phenotypes which might cause differ-ent aortic walls strain changes.
P1025Vector flow mapping in aortic regurgitation: relationship between jet eccentricityand energy loss within the anterior component of the left ventricular vortex
VC. Lozano Granero; D. Rodriguez Munoz; A. Carbonell San Roman; JL. Moya Mur;R. Hinojar; A. Gonzalez; E. Casas; JJ. Jimenez Nacher; C. Fernandez-Golfin;JL. Zamorano GomezUniversity Hospital Ramon y Cajal de Madrid, Cardiology, Madrid, Spain
Purpose: Flow inside the left ventricle (LV) is organized in vortices following trans-mitralinflow. The anterior component of the vortex is thought to work as a preserver of thekinetic energy generated by blood inflow into LV, redirecting it into the outflow tract atend diastole. The aim of this study is to determine whether there are significant differencesin vortex behavior and energy management in individuals with aortic regurgitation (AR).Methods: Patients with moderate to severe chronic AR underwent examination withVector Flow Mapping, an advanced echocardiographic tool capable of depicting intracar-diac flow patterns. The AR jet was classified as been eccentric towards the anterior mitralleaflet (AML) or towards the interventricular septum (IVS). The predominant anterior com-ponent of the vortex ring visualized in apical 3-chamber view was studied.Results: 8 patients with AR were studied: 4 with an eccentric jet towards AML, all of whomhad a close to normal vortical pattern, and 4 towards IVS, all of whom showed a disruptionin the anterior component of the vortex caused by collision of the regurgitant jet. Bothgroups had similar energy loss (mW/m) during systole (4.77 in AML vs. 3.25 in IVS,p=0.21). However, IVS group showed a greater energy loss during diastole in theoutflow tract (15.36 in IVS vs. 7.01 in AML, p=0.047), with a higher ratio betweenenergy loss during diastole and systole in this region (2.31 in IVS vs. 0.71 in AML,p=0.006) and inside the vortex as a whole (2.12 in IVS vs. 1.05 in AML, p=0.02).Conclusions: AR jet direction seems to affect vortical behavior. Jets directed towards IVSshow greater energy loss in diastole, implying deficient energy preservation. The extentand clinical implications of these observations should be addressed in further studies.
P1026Effects of transapical off-pump mitral valve repair on annulus and leafletmorphology: intraprocedural 3D transoesophageal evaluation
P. Gripari; G. Tamborini; M. Muratori; S. Ghulam Ali; L. Fusini; F. Alamanni; M. PepiCentro Cardiologico Monzino, IRCCS, Milan, Italy
Purpose: Transapical off-pump mitral valve (MV) repair using the NeoChord device, thatdelivers artificial chordae tendinae, has been recently proposed as a minimally invasivetreatment option for degenerative MV regurgitation. We sought to investigate the immedi-ate effects of Neochord mitral valve repair (NMVR) on MV morphology.Methods:11patients (pts)with severedegenerativeMVregurgitation (8 isolatedposteriorleaflet prolapse, 3 bileaflet prolapse) underwent NMVR. Intraprocedural 3D transoeso-phageal datasets were acquired immediately before and after NMVR, and processedoffline using a dedicated software. Several parameters were measured at end systole, in-cluding the two main annular diameters, MV annular height and area, the leaflets coapta-tion height, the prolapse volume, the MV regurgitation orifice area.Results: All procedures were successful (residual regurgitation ≤2+) with 3 neochordaeimplanted in 1 case, 4 neochordae in 5 pts, 6 to 9 neochordae in 5 pts. Analysis was feas-ible in all cases (8+2 min). Mean volume rate was 32+13 Hz. In 5 arrhythmic cases, ana-lysis was performed on 3D live zoom dataset (6-11 Hz).NMVR led to a reduction of the MV regurgitation orifice area (pre=52+47 vs post=0+0mm2), increased leaflets coaptation height (3.21+0.69 vs 5.97+1.97 mm) and reducedprolapse volume (1.1+1.1 vs 0.41+0.7 mL). Conversely, NMVR did not affectsignificantly the MV annular diameters (intercommissural 47+9 vs 45+6 mm, antero-posterior 41+7 vs 39+5) height (9.0+1.97 vs 9.4+3.1 mm) and area (17.0+5.9 vs14.9+3.3 cm2)Conclusions: 3D TEE demonstrated significant modifications of MV morphology afterNMVR, associated with the restoration of MV competence without significant structuralchanges in MV annulus.
P1027Left heart remodeling in degenerative mitral regurgitation after percutaneous orsurgical intervention
K. Keramida1; M. Bellamy1; D. Dawson1; P. Nihoyannopoulos2
1Hammersmith Hospital, London, United Kingdom; 2Imperial College Healthcare NHSTrust, Hammersmith Hospital, London, United Kingdom
The goal of this study was to compare left ventricular (LV) and left atrial (LA) remodeling inpatients (pts) with degenerative, severe mitral valve regurgitation (MR) undergoing surgi-cal (SR) versus percutaneous mitral valve repair with the MItraClip system.Twenty three consecutive pts with severe degenerative MR were prospectively recruited.Thirteen underwent SR and10 MitraClip following amulti-disciplinary heart team decision.Pts underwent two dimensional (2D) TTE study before and 1 year after the intervention. LVglobal longitudinal (LVGLS) and circumferential strain both at the level of mitral valve(LVCS MV) and at the level of papillary muscles (LVCS PM) were calculated off line by2D speckle tracking echocardiography.In the MitraClip group 70% of the pts were male, with mean age 79+9 years, while in theSR group 69% were male, with mean age 52+20 years (p,0.001). At baseline MR wassevere in both groups, but after MitraClip MR was mild to moderate, while in SR, MR wasmild to trace. As is evident from Table 1, GLS before and after intervention was worse in theMitraClip group. MitraClip resulted in significant decrease in LVEDD and in LVCS MV, whileSR led to reduced LVEDD, LA diameter (LAD) and volume (LAV), LVGLS and CS MV. In SRgroup, LVGLS and LVCS PM were supranormal at baseline and 1 year after repair theywere reduced. Conversely, in the MitraClip group, those variables were impaired beforeclip implantation and deteriorated further after.Reverse LV and LA remodeling after SR of degenerative, severe MR is more pronouncedthan following MItraClip, indicating perhaps the most effective reduction of MR.
Abstract P1027 Table.
MITRACLIP SURGICAL REPAIR p valueVARIABLE BEFORE AFTER p value BEFORE AFTER p value
LVEDD (mm) 50.40+6.75 46.80+5.90 0.012 56.54+7.11 49.08+5.83 0.002 NSEF (%) 56.82+8.32 56.29+11.34 0.360 58.92+7.75 53.69+9.85 0.130 NSLAD(mm) 45.80+7.42 40.50+5.42 0.176 46.85+7.95 40.17+6.19 0.010 NSLAV(mm2) 87.86+32.33 97.56+43.91 0.228 99.54+41.75 68.08+24.89 0.021 0.008RVSP (mmHg) 51.17+14.82 42.63+13.89 0.250 39.38+13.75 25+4.38 0.281 NSLVGLS (%) 217.38+5.03 215.21+4.62 0.217 223.94+2.39 220.58+1.28 ,0.001 NSLVCS MV (%) 217.68+4.44 213.32+4.59 0.003 221.33+6.00 215.28+7.29 0.012 NSLVCS PM (%) 223.85+9.80 220.61+7.4 0.317 225.42+6.20 222.93+3.54 0.251 NS
Abstract P1025 Figure.
Abstract P1026 Figure.
Abstracts ii165
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

P1028Potential of Multislice Computed Tomography in Assessment of FunctionalAnatomy of the Mitral Valve and Left Ventricle in Ischemic Mitral Regurgitation
N. Solowjowa1; L. Musayeva2; Y. Hrytsyna3; CH. Knosalla1; V. Falk1
1German Heart Center Berlin, Berlin, Germany; 2N.Tusa Clinic, Baku, Azerbaijan; 3Charite -Campus Virchow-Klinikum (CVK), Berlin, Germany
Purpose: Functional mitral regurgitation (FMR) remains an important prognostic deter-minant in patients with ischemic cardiomyopathy (ICMP). A differentiated surgical ap-proach based on parameters of left ventricular (LV) and mitral valve (MV) remodeling isessential. We evaluated volumetric and geometric parameters of the MV-LV complexwith multislice computed tomography (MSCT) in patients with ICMP, and their relationto moderate and severe FMR.Methods: Between 09/09 and 03/15, 121 patients (m:w=101:20, age 37-79, median 66.0years; mean NYHA class 2.97) with echocardiographic LV ejection fraction (LVEF) ,40%underwent cardiac MSCT for LV functional assessment. The following MSCT data wereanalyzed retrospectively: indexed left atrial and LV enddiastolic and endsystolicvolumes (LAVI, LVEDVI, LVESVI) and LV volumetric sphericity index (SI). LVEF, cardiacoutput (CO) and cardiac index (CI) were also calculated on the basis of MSCT data. Re-gional wall motion abnormalities were assessed semiquantitatively. MV apparatus wascharacterized by intercommissural and anteroposterior MV annulus diameter (ICD,AMD), MV annulus area and posterior circumference (MVAA, MVAPC), coaptation dis-tance, tenting area, anterior and posterior leaflet to annulus angle (CD, TA, ALA, PLA) insegments 1-3 and interpapillary muscle distance (IMD), measured in midsystole. Theseparameters were compared in patients (n=87) with moderate MR (,2.0) and patients(n=34) with severe (≥2.0) MR.Results: The differences in LVEDVI, LVESVI and LVEF between the two groups were notsignificant, whereas LAVI and SI were significantly higher in patient with severe FMR (LAVI73.3+24.8 vs. 56.3+17.1 ml/sqm, p=0.001; SI 0.48+0.1 vs. 0.42+0.09, p=0.009).Patients with severe FMR showed significantly longer CD (CD A2-P2 10.4+2.3vs.8.6+2.0 mm, p=0.000; CD A3-P3 8.7+2.3 vs.7.6+2.0 mm, p=0.011) and largerTA (TA A2-P2 2.26+0.9 vs. 1.64+0.6 sqcm, p=0.001), demonstrating more advancedMV remodeling. Motion abnormalities of posterior papillary muscle and posterior loadbearing LV wall were found significantly more often (p=0.004) in severe FMR. The differ-ences in MV diameter, circumference and area, IMD and segmental leaflet to annulusangles did not reach significance.Conclusions: MSCTrepresents an appropriate diagnostic tool for evaluation of FMR. Ourdata show more pronounced tethering of the mitral leaflets at the central and posterome-dial segments, higher prevalence of motion abnormalities of posterior papillary muscleand more advanced LA and LV remodeling in patients with severe FMR.
P1029Three-dimensional printing of normal and pathologic tricuspid valves fromtransthoracic three-dimensional echocardiographic data sets: feasibility andrelative accuracy
D. Muraru1; A. Maddalozzo1; C. Jenei2; D. Dequal3; F. Veronesi4; P. Aruta1; G. Romeo1;S. Iliceto1; L. Badano1
1University of Padua, Department of Cardiac, Thoracic and Vascular Sciences, Padua,Italy; 2University of Debrecen, Department of cardiology and cardiac surgery, Debrecen,Hungary; 3University of Padova, Department of Information Engineering, Padua, Italy;4University of Bologna, Department of Electrical, Electronic and Information Engineering,Bologna, Italy
Sizing the tricuspid valve (TV) annulus is inaccurate using conventional 2D. Recently, 3Dprinted models of the mitral valve have been obtained from 3D transoesophageal (TOE)volumetric data. However, TOE is unsuitable for routine assessment of the TVand the lackof dedicated software to quantitate the complex morphology of the TV has hampered thepossibility to print 3D modelsof the TV.Therefore, we explored the feasibility of using trans-thoracic 3D echocardiography (3DTTE) data to generate 3D patient-specific modelsof TV.Accordingly, multi-beat 3D dataset of the TV (32 vol/s) were acquired in 5 patients from theapical approach and were analyzed offline with custom-made software. Coordinatesrepresenting the annulus and the leaflets were imported into Mesh-Lab (Visual ComputingLab ISTI-CNR) to develop solid models to be converted to stereolithographic (STL) fileformat and 3D printed (Figure). Measurements of the antero-posterior (AP) and medio-lateral (ML) diameters, and TV annulus perimeters (P) obtained from slicing the 3Decho data set at the annulus level were compared with those performed on the 3D
models using a millimeter tape. AP (4.2+0.7 cm vs. 4.2+0.6 cm;; p= NS) and ML(3.7+0.6 cm vs. 3.6+0.7 cm; p= NS) diameters, as well as P (12.6+2.1 vs. 12.7+2.1 cm: p= NS) were similar when measured on the 2D slice and the 3D model. Thetwo sets of measurements were highly correlated, (r= 0.991). The mean absolute error(2D 2 3D) for AP, ML and P were 0.7+0.3 mm, indicating accuracy of the 3D model of,1 mm.Thus, 3D printing of the TV from 3DTTE data is feasible with highly conserved fidelity. Thistechnique has the potential for rapid integration into clinical practice to assist with deci-sion-making, surgical planning and teaching.
P1030Evaluation of aortic paravalvular leaks: A special reference for anatomicallocalization
MO. Gursoy1; M. Kalcik1; M. Ozkan2; MA. Astarcioglu1; T. Gokdeniz2; M. Yesin1;S. Karakoyun2; S. Gunduz1; MA. Tuncer3; C. Koksal31Kartal Kosuyolu Heart Education and Research Hospital, Department of Cardiology,Istanbul, Turkey; 2Kafkas University, Cardiology, Kars, Turkey; 3Kartal Kosuyolu Heart andResearch Hospital, Cardiovascular Surgery, Istanbul, Turkey
Purpose: We aimed to evaluate the echocardiographic, clinical, surgical and laboratorycharacteristics of the patients with aortic paravalvular leaks (PVLs).Methods: Seventy-seven aortic PVL patients underwent transthoracic and transesopha-geal echocardiographic (TEE) examination. Clinical, echocardiographical and surgicalfindings were recorded.Results: Of 77 patients, 21 (27.3%) had mild, 33 (42.8%) had moderate and 23 (29.9%)had severe aortic PVL. The patients with moderate-to severe PVLs had higher NYHAclass than those with mild PVLs (1.7+0.8 vs 1.2+0.4, respectively; p= 0.03). Therewas significant difference between mild and moderate-to-severe PVL groups in terms ofmean length of the defect (4.4+0.8 vs 6.1+2.2 mm, respectively; p=0.001) measuredby TEE. Seventeen patients (22.1%) had moderate-to-severe hemolysis and had higherincidenceof multiple PVLs compared to those with noor mildhemolysis. There wasaposi-tive strong correlation between lactate dehydrogenase levels and severity of PVL (r:0.84,p,0.001). Moderate-to-severe PVLs were more frequent between the noncoronary andthe left coronary sinus annuli, especially adjacent to the left main coronary artery(LMCA) ostium. Percutaneous closure was performed in 5 patients. Eleven patientsunderwent surgical repair and the localizations of PVLs were in accordance with echocar-diographic findings.Conclusions Aortic PVLs occur more frequently between noncoronary sinus and left cor-onary sinus annuli, especially adjacent to LMCA ostium. The difficulty to seat the pros-thesis due to steep angulation of the commisure and the annulus and avoidance ofdeep sutures, probably make this region prone to injury and leakage.
P1031Infective endocarditis complicated by perivalvular abscess or pseudoaneurysm:is surgery always mandatory?
A. Cresti1; M. Chiavarelli2; F. Guerrini1; N. D’aiello1; A. Albano1; F. De Sensi1; A. Picchi1;F. Cesareo1; S. Severi11Misericordia Hospital, ASL 9, Grosseto, Italy; 2Policlinico Le Scotte, CardiothoracicSurgery Department, Siena, Italy
Purpose: Perivalvular abscess and pseudoaneurysm are life-threatening complicationsof infective endocarditis (IE). Current guidelines recommend urgent surgical treatment.Natural history and surgical outcome, however, are not quite determined.Methods: All patients with definite diagnosis of IE, who were admitted to our Hospitalin Italy, between January 1998 and December 2014, were prospectively entered in adata base. Risk factors collected included preexistent heart disease and surgical proce-dures, heart failure, renal insufficiency, diabetes, embolic events, septic shock, chronicobstructive pulmonary disease, peripheral vasculopathy, intravenous drug abuse, theresults of transthoracic and transesophageal echocardiogram, blood cultures, antibiotictherapy and surgical treatment. In case of perivalvular abscess or pseudoaneurysm,urgent surgery was advised. One-year follow up was completed in all patients.Results: Among 170 consecutive patients with a definite diagnosis of IE according to theLi-Duke criteria, thirty-seven (21,7%) entered the present study: an abscess was evident in27 (15,8%), while a pseudoaneurysm in 10 (5,9%). Incidence rate of these perivalvularcomplications was 1/100.000/y. Mean age was 69+16 years; male/female ratio was1,6. Seventeen patients (46%) had native and twenty a prosthetic valve endocarditis.Twenty-three individuals (62%) underwent surgical treatment during IE hospitalizationwith a hospital mortality of 39% and a one-year survival of 50%. Among the medicallytreated patients, in-hospital mortality was 47%, one-year survival rate 29%. At 1 yearfollow-up, the cumulative death rate was 57% and survival rate did not statistically differamong medically and surgically treated patients (p:0,12). Patients with septic shockhad a prohibitive surgical risk and died in the hospital; the remaining medically treatedpatients had a hospital mortality of 43% and one-year survival was similar to the surgicalgroup (40%). Staphilococcus aureus was the most common microorganism (35%). At themultivariate analysis persistent bacteremia and septic shock were the only indipendentrisk factors for mortality.Interpretation: Patients with IE and perivalvular abscess or pseudoaneurysm had a highhospital and one-year mortality rate. Urgent surgery improved the chances of survival,with a high surgical risk. The prognosis of medically treated patients was poor, yet in29% it was successful alone and may be proposed in selected cases.Abstract P1029 Figure.
ii166 Abstracts
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

P1032A comparison between community-acquired and health care-associated infectiveendocarditis in a 3-year retrospective analysis
M. Braga; H. Nascimento; L. Flores; V. Ribeiro; F. Melao; P. Dias; MJ. Maciel; P. BettencourtSao Joao Hospital, Porto, Portugal
Introduction and purpose: Infective endocarditis (IE), an identity known since 1885,carries a poor prognosis and a high mortality. IE can be classified as community-acquiredIE or health care-associated IE. The aim of this study is to describe and to compare theclinical profile and in-hospital outcome between community-acquired IE (CA-IE) andhealth-care associated IE (HCA-IE).Methods: In a retrospective study, we included 169 cases of consecutive diagnosed IE ina tertiary center from July 2011 to July 2014. Data were collected from the electronic clin-ical process and registered in a uniform base. They were divided into two groups: CA-IE(60.7%) and HCA-IE (37.0%).Results: The mean age (CA-IE 60.7+17.2 vs. HCA-IE 65.4+ 17.7) and gender (malesex CA-IE 66.7% vs. HCA-IE 53.1%) were similar in both groups. Within the patientcomorbidities studied, left ventricular dysfunction (CA-IE 12.2% vs. HCA-IE 27.1%,p=0.018) and chronic pulmonary disease (CA-IE 7.6% vs. HCA-IE 21.9%, p=0.008)were more common in HCA-IE patients. No differences were found in prevalenceof diabetes mellitus and predisposing heart condition in the two clusters. Echocardio-graphic evidence of perforation or fistula (CA-IE 36.2% vs. HCA-IE 20.3%, p=0.029)and new valvular regurgitation (CA-IE 57.7% vs. HCA-IE 34.9%, p=0.004) weremore frequent in CA-IE. The main causative microorganisms in CA-IE group wereStaphylococcus spp. (28.4%, of which 15.3% were Staphylococcus methicillin-resistant), followed by Streptococcus spp. (24.5%) and Enterococcus spp. (15.7%).In the HCA-IE cases, Staphylococcus spp. (59.3%, of which 36.1% were Staphylococ-cus methicillin-resistant) and Enterococcus spp. (12.5%) were more ofteninvolved, while Streptococcus spp. was present in only 4.7% of the cases. Severalcomplications were studied and systemic embolism was more prevalent in CA-IEcases (CA-IE 28.4% vs. HCA-IE 12.7%, p=0.019). Surgery was performed in72.4% of CA-IE cases in contrast to 40.6% of HCA-IE sample (p,0.001). In-hospitalmortality was more frequent in the HCA-IE group (CA-IE 20.0% vs. HCA-IE 40.6%,p=0.004).Conclusion: Our results points out for some clinical, echocardiographic and microbiolo-gic differences between CA-IE and HCA-IE. The medical approach was different as wellsince the surgical treatment was more frequent in CA-IE. In addition, in-hospital mortalitywas higher in HCA-IE. Further studies are needed to find the inherent HCA-IE specificitiesin order to improve the clinical outcome.
P1033Impact of postprocedure aortic regurgitation after transaortic valve implantationin follow up in patients with moderate surgical risk. Is it always aortic regurgitationa risk predictor?
C. Ferreiro Quero; M. Delgado Ortega; M. Puentes Chiachio; M D. Mesa Rubio;M. Ruiz Ortiz; E. Duran Jimenez; J. Sanchez Fernandez; C. Morenate Navio; M. Pan;J. Suarez De LezoCardiology Department. University Hospital Reina Sofia, Cordoba, Spain
Background and Aim: Transcatheter aortic valve implantation (TAVI) has became aroutine procedure in patients with severe aortic stenosis and high risk for surgicalaortic valve replacement. Ongoing studies are evaluating applications of TAVI inexpanded populations of patients including those with lower risk profiles as well asthose with comorbidities that were excluded from early clinical trials. Postproceduralaortic regurgitation (AR) after TAVI is a relative common complication and has beendescribed as an independent risk factor for all cause and cardiovascular mortality.Our aim was to asses the influence of posprocedure AR in medium term follow up inpatients with moderate surgical risk who underwent TAVI with the Corevalve pros-thesis.Methods: From April/2008 to March/2014 a total of 189 patients (mean age 78+ 5years, 46% male, Logistic Euroscore 12+9%) who underwent TAVI with the Corevalveprosthesis in our departmen were included in our study. Clinical and echocardiograph-ic examination of patients were performed within 7 days before TAVI, at discharge, at 1,6 and 12 months, and annually thereafter. Prosthetic aortic valve regurgitation wasgraded by means of echocardiography into grades I, II, III and IV. Clinical eventswere defined as the occurrence of a stroke, hospitalization due to heart failure or allcause death.Results: Angina (52%) and functional class III-IV dyspnea (63%) were the most commonsymptoms. Basal echocardiographic study showed a normal ejection fraction (64%+14), an aortic valve area of 0.55 cm2+18 and a mean transvalvular gradient of 57+14 mmHg. In 92% of the series TAVI was succesfully implanted. At discharge, anydegree of AR was present in 79% of cases, and AR≥ grade II in 32% (paravalvular ARin 97% of them). After 2.5 years of mean follow up, event free survival in patients with post-procedural AR grade≥ II was 63%, while, patients with AR grade 0 or I showed an eventfree survival of 74% (p=0.14). Mortality rate in the whole series was 26.5% (49% cardio-vascular death).Conclusions: In our experience, postprocedural AR after TAVI was not related tocardiovascular events in the medium term follow up. The moderate surgical riskand event rate could be, at least partially, a possible explanation of this unexpectedfindings.
P1034Changes of mitral regurgitation in patients after transcatheter aortic valveimplantation: focus on valve type and etiology
R. Jansen1; P. Agostoni1; PR. Stella1; F. Nijhoff1; FZ. Ramjankhan2; WJ. Suyker2;SAJ. Chamuleau1
1University Medical Center Utrecht, Department of Cardiology, Utrecht, Netherlands;2University Medical Center Utrecht, Division Heart and Lungs, Department ofCardiothoracic Surgery, Utrecht, Netherlands
Purpose: Existing data on changes of mitral regurgitation (MR) following transcatheteraortic valve implantation (TAVI) remain contradictory, although there seems to be atrend towards MR reduction. Several factors have been associated, including theimplanted valve type and MR etiology. This study aimed to assess the change in MR se-verity after TAVI focused on valve type and MR etiology. In previous studies MR gradingis often insufficient, while data is mainly derived from analyses focused on specific out-comes, and color-flow mapping is used for MR quantification. Therefore, we determinedMR severity by a semiquantitative index.Methods: We retrospectively analysed 136 patients undergoing TAVI in a single centrebetween 2008 and 2014. For subgroup analyses patients were stratified into 1) twogroups according to valve type, and 2) two groups according to MR etiology. MR wasgraded 0-4 at baseline, 6 months and 1-year post-TAVI.Results: Echocardiograms were evaluated in 136 subjects: 94 (69%) after EdwardsSapien and 42 (31%) following Corevalve implantation. In 83 (61%) subjects the etiologiywas primary MR, in 51 (38%) secondary. At baseline MR was 1+ in 88 (65%), 2+ in 19(14%), 3+ in 6 (4%), and 4+ in 2 (2%). Twenty-one patients (15%) had no MR pre-TAVI.At 1-year follow-up MR was grade 0 in 24 (18%), 1+ in 88 (65%), 2+ in 16 (12%), 3+ in5 (4%) and 4+ in 3 (2%) of the subjects. Similar percentages were seen in both subgroups(figure 1). Differences in MR grade were not significant.Conclusions: Most patients referred for TAVI had some degree of MR, however severeMR was rarely seen. Overall, there was no significant change in MR severity at 6 monthsand 1 year after TAVI compared to baseline. This result was neither related to the typeof valve implanted nor to the cause of concomitant MR.
P1035Prosthetic valve endocarditis at patients after TAVI
P. Scislo; Z. Huczek; J. Kochman; B. Rymuza; J. Kochanowski; A. Scisbisz; R. Piatkowski;G. OpolskiMedical University of Warsaw, Warsaw, Poland
In this study we analyze series of 180 patients after all TAVI procedures performedbetween 03/2010 and 05/2015 in our department. At 62% of patients Medtronic Corevalvewas implanted, 35% - Edwards Sapien XT/3, 1% - Medtronic Engager and 2% - MedtronicEvolut R. In 76% cases transfemoral access was used, in 15% direct aorta, in 4% sub-clavian, 3% transcarotid and 3% apical.45% of patients have implanted 29 mm bioprosthesis, 35% - 26mm, 10% 223mm, 8% - 31mm and 2% - 27 mm.In one year follow up we found 4 patients who met the diagnostic criteria of valve endocar-ditis. The first patient had endocarditis on native mitral valve as a complication of severepneumonia but TAVI prosthesis was not infected. The second patient had endocarditison right atrium catheters during sepsis due to the liver transplantation (LTX) complica-tions, however had no signs on PVE. At third patient we observed typical PVE on due tourosepsis. Fourth patient develop PVE as a CDRiE complication.The first and fourt patient survived (50%), the second died because of non-cardiologicalcomplication of LTX, the third died due to procedure complications.Infective endocarditis after TAVI is rather rare complication (2,2%), and notalways the TAVIbioprosthesis is affected by PVE. However in cases of TAVI valve’s PVE we found 50% ofmortality.
P1036Patients with left-sided valve disease undergoing surveillance have an increasedprevalence of atrial fibrillation - results from a dedicated technician led valveclinic
R. Ray; K. Knott; D. Smith; A. Rodriguez; G. Finocchiaro; R. SharmaSt George’s Healthcare NHS Trust, Cardiology Department, London, United Kingdom
Purpose: The prevalence of atrial fibrillation (AF) in the general population is 2%. Dedi-cated valve clinics are advocated in the United Kingdom to monitor patients with valvularheart disease until the need for surgery. In such clinics it is important other comorbiditiesare not ignored. Our aim was to investigate the prevalence and predictors of AF in patientswith valve disease undergoing surveillance in a dedicated valve disease clinic.
Abstract P1034 Figure. Changes in MR after TAVI
Abstracts ii167
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

Methods: Consecutive patients who underwent surveillance in a cardiac technician-ledvalve clinic for native mitral and/or aortic valve disease at a tertiary cardiac centre overthe three year period 2010-2013 were included. Patients at the clinic have an assessmentof symptoms, medication, transthoracic echocardiogram and ECG. Patients with artificialvalve prostheses were excluded.Results: 244 patients were assessed. 127 (52%) were male and the mean age was 66.3+16.8 years. 34 patients (13.9%) had AF of which 30 patients were on warfarin. There was nosignificant difference in resting heart rate (73.9+2.6 bpm AF group vs.72.4+0.9 bpmsinus rhythm (SR) group). AF was more prevalent with increasing age (mean age 77.6+11.2 years AF group vs. 64.5+16.8 years SR group; P,0.001), in females (21 femalesvs. 13 males; p=NS) and with increasing severity of mitral regurgitation (MR) (10 out of72 patients (13.9%) with mild MR, 12 out of 42 patients (28.6%) with moderate MR and 3out of 6 patients (33.3%) with severe MR were in AF). The prevalence of AF was notrelated to the severity of aortic valve disease. In patients with mild and moderate mitral sten-osis, AFwas present in21.2%ofpatients. Those in AFhada significantly larger left atrial (LA)diameter (4.9+0.7 cm AF group vs. 4.0+0.8 cm SR group; P,0.001) and higher esti-mated pulmonary artery systolic pressure (40.6+14.1 mmHg AF group vs. 33.0+9.6mmHg SR group; p,0.01). Left ventricular (LV) systolic function was significantlyreduced in the AF group (57.9+5.9% AF group vs. 60.8+7% SR group; p,0.01).There was no significant difference in LVend systolic or LVend-diastolic diameter. Multivari-ate analysis identified LA diameter (HR: 6.11, 95% CI 3.09 to 12.09, p,0.001) and age (HR:1.062, 95% CI 1.02 to 1.11, p=0.005) as independent predictors of AF.Conclusions: Amongst patients undergoing surveillance for left-sided valve disease, AFis much more prevalent than in the general population. Independent predictors of thepresence of AF include LA diameter and age. Any dedicated valve clinic should includeAF as specific parameter to look for.
P1037A Simple Linear Iterative Clustering (SLIC) SuperPixels approach tomultidimensional segmentation of 3D Transesophagel echocardiographic (TEE)sequences
C. Veiga; F. Calvo Iglesias; DR. E Paredes-Galan Pablo Pazos Andres Iniguez RomoHospital of Meixoeiro, Cardiology, Vigo, Spain
Thiswork integrates Simple Linear Iterative Clustering (SLIC) segmentationwith a preproces-sing pipeline based on Shannon entropy and anisotropic diffusion techniques, to automatic-ally delineate and quantitatively describe the aortic valve geometry in 3D echocardiographicsequences.Achallengingtaskthathasbeenexploredonlytoa limitedextent.Theclinical rele-vance of the method is its ability to capture sinuses geometry in 3DE imagedata with minimaluser interaction while producing consistent measurements of 3D aortic valve geometry.Experiments show that our approach produces segmentations at a lower computationalcost while achieving a good quality segmentation.Results: of the proposed algorithm are provided on Table 1 and Figure 1.In this paper, an Aortic Valve segmentation algorithm based on SLIC, was presented. Thissystem attains very good results in terms of accuracy when compared with manualsystems. The system is characterized by its lower complexity in term of time computing.The system uses two dimensional superpixels. A further work will be analyze the perform-ance in volumetric supervoxels.
Abstract P1037 Table.
k Dmean STD D
3 2.06 1.11 0.8875 1.98 1.32 0.89610 1.12 0.86 0.915
Summary of the distance errors and clinical indices: mean surface Distance (Dmean) in pixelunits, Standard Deviation (STD), and Dice similarity index (D) measurements.
CARDIOMYOPATHIES
P1038Differencies in echocardiographic parameters evolution in males and femaleswith recent onset dilated cardiomyopathy
J. Krejci1; P. Hude1; E. Ozabalova1; V. Zampachova2; D. Mlejnek1; D. Sochorova2;L. Spinarova2
1St. Annes University Hospital - ICRC, Brno, Czech Republic; 2Masaryk University,St. Annes University Hospital, Brno, Czech Republic
Introduction: Improvement in left ventricular ejection fraction (LVEF) in patients withrecent onset dilated cardiomyopathy (RODCM) is less in males than in females. It hasnot been published whether and how the biopsy findings influence evolution of left ven-tricular function in both sexes.Objective: To compare the change in LVEF and other echocardiographic parameters inmen and women in groups with and without the evidence of myocardial inflammationdetected by endomyocardial biopsy (EMB).PatientsandMethods:44men and16 women with the presence of myocardial inflamma-tion (inflammatory cardiomyopathy - ICM) - i.e. with the presence of ≥14 CD45+ cells/mm2 and/or ≥7 CD3+ cells/mm2 in EMB. The echocardiographic findings at diagnosisand 6 months thereafter were assessed. The results were compared with a group of 74men and 16 women without the presence of inflammation (dilated cardiomyopathy -DCM - group).Results: In the ICM group, LVEF improved from 24+7% to 38+12% (p = 0.002) inmales, and from 25+8% to 45+12% (p = 0.018) in females. A difference in thechange between both groups (13+13% vs. 20+12%) was statistically significant (p =0.045). In the DCM group, LVEF increased from 24+7% to 30+9% (p ? 0.001) inmales, and from 23+8% to 32+12% (p = 0.021) in females. The difference betweenboth sexes was not statistically significant (5+9% vs 9+13%; p = 0.311).Conclusion: LVEF improvement in the group with biopsy-proven myocardial inflamma-tion is more pronounced in women than in men. In the group without evidence of inflam-mation is the change in LVEF similar in both sexes.
P1039Evaluation of echocardiographic and other parameters to predict sudden cardiacdeath in doberman pinschers with dilated cardiomyopathy
G. Wess1; L. Klueser1; PJ. Holler1; J. Simak1; H. Kuechenhoff21Ludwig-Maximilians University, Veterinary Cardiology, Munich, Germany; 2Ludwig-Maximilians University, Statistical Department, Munich, Germany
Purpose: Naturally occurring dilated cardiomyopathy (DCM) in Doberman Pinschers isan animal model resembling DCM in humans. DCM in in this dog breed is characterizedby ventricular arrhythmias and systolic dysfunction. About one third of the affected Dober-man Pinschers die from sudden cardiac death (SCD). So far it is unknown, which para-meters can best predicted SCD in dogs.Methods: a longitudinal prospective study was performed 106 client-owned DobermanPinschers with DCM. 52 dogs died within 6 months after the last examination time point(SCD group) and were compared to 54 Doberman Pinschers with DCM that were stillalive one year after inclusion (DCM control group). Holter-ECG, echocardiography, meas-urement of NT-proBNP and cTNI concentrations were performed in all dogs.Results: Using a regression analysis, left ventricular end-diastolic volume (LVEDV) wasfound to predict the occurrence of SCD within six months after measuring a heightenedlevel of LVEDV (LVEDV/BSA . 91.3 mL/m2; p = 0.00012). The probability of occurrenceincreases 9.9 (3.5 – 37.) fold for every 50 mL/m2 - unit increment in LVEDV normalized tobody surface area (BSA). Ejection fraction, LVESD/BSA and NT-proBNP showed a highcorrelation with LVEDV/BSA, but the computer model selected LVEDV/BSA as singlebest parameter to predict SCD. Other variables were not found to be significant in regres-sion analysis, but descriptive analysis of collected data showed that the concomitant pres-ence of ventricular tachycardia (VT), an increased concentration of cTNI, a velocity ofarrhythmias .260 beats per minute (bpm), and non-administration of antiarrhythmicmedication, further improve SCD risk assessment.Conclusion: and clinical importance: An increased cardiac size, documented as anincreased LVEDV qualifies best as prognostic parameter to predict the probability ofSCDofDoberman Pinscherssuffering fromDCM. It stoodoutas thesingle individualprog-nostic measure where a heightened level was apparent in 47 of 52 dogs that deceasedsuddenly within six months after the initial examination.
P1040Hypertrophic patterns in physiological hypertrophy and different forms ofhypertrophic cardiomyopathies determined with cardiac magnetic resonancetrabecula quantification
H. Vago1; CS. Czimbalmos1; A. Toth1; I. Csecs1; K. Kecskes1; F. Suhai1; O. Kiss1; T. Simor2;D. Becker1; B. Merkely1
1Heart and Vascular Center Senmelweis University, Budapest, Hungary; 2Heart Institute,Faculty of Medicine, University of Pecs, Pecs, Hungary
Distinguishing physiological cardiac hypertrophy from hypertrophic cardiomyopathy(HCM) is crucial in preventing sudden cardiac death in professional athletes. However,the hypertrophic pattern can be different in various types of HCM.The aim of our study was to compare with the help of CMR the left ventricular (LV) volumet-ric, mass and trabecular data and derived parameters of two groups: patients with apicalor non-apical hypertrophic cardiomyopathies and healthy professional athletes of bothgenders. Moreover, we compared the parameters of HCM adults with the parameters ofchildren under 16.We carried out CMR examinations on 159 adult HCM patients (male:95; male apical:15,female apical:4), 27 children with HCM (19 boys), 124 adult professional athletes(male:86) free of complaint, and 79 (male:41) healthy volunteers. We determined the fol-lowing parametersusing Medis QMass 7.6 software: LVejection fraction (EF), end-diastol-ic, end-systolic volume indices (LVEDVi, LVESVi), stroke volume index (LVSVi), massindex (LVMi) and trabecular mass index (TrMi). Derived parameters were calculated toevaluate the hypertrophic pattern [1.trabecular mass percent: TrM% (Trabecular
Abstract P1037 Figure. Evolution of SLIC segmentation
ii168 Abstracts
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

mass(g)/LVM(g)*100), 2.LV maximum diastolic wall thickness and end-diastolic volumeindex ratio (DWT/V), 3. LV mass and end-diastolic volume ratio (M/V)].The LVMi and TrMi were significantly higher in athletes and HCM patients compared tocontrol group in both genders (male athletes:114.9g/m2, 21.2g/m2; HCM:125.7g/m2,27.7g/m2; control:87.4g/m2, 18.3g/m2;p,0.001). However, the TrM% was lower inmale athletes compared to HCM patients and volunteers (athletes:18.6 vs HCM:45.8and control:20.9%;p,0.001). In both genders the M/V did not differ between athletesand controls, it was, however, higher in HCM patients compared to athletes (male:1.89vs 1.13g/ml;p,0.001). In male HCM patients the TrMi was significantly higher in non-apical form compared to apical form (p,0.05). LVMi and TrMi did not differ significantlybetween athletes and apical HCM patients, however the TrM%, M/V and DWT/V werehigher in apical form (p,0.001). In HCM patients TrM% was lower in children comparedto adults (male:19.0+5.4 vs 45.8+9.7%; female:16.6+2.6 vs 22.7+4.0%;p,0.001).In conclusion, HCM patients have more pronounced trabeculation compared to profes-sional athletes. The non-apical form is characterized by more remarkable trabeculationcompared to the apical form. A quantitative analysis of the myocardial trabeculae andthe derived CMR parameters seem to play an important role in distinguishing athlete’sheart from pathological hypertrophy.
P1041Potential role of quantitative contrast enhanced cardiovascular magneticresonance for the evaluation of sudden death risk in intermediate-risk patientswith hypertrophic cardiomyopathy
R. Hinojar1; C. Fernandez-Golfin1; JC. Portugal2; A. Esteban3; A. Megias1; S. Ruiz Leria1;LM. Rincon1; JJ. Jimenez-Nacher1; JL. Zamorano1
1University Hospital Ramon y Cajal de Madrid, Cardiology, Madrid, Spain; 2UniversityHospital Dr Negrin, Las Palmas DeGranCanaria, Spain; 3University Hospital Ramon y Cajalde Madrid, Radiology, Madrid, Spain
Background: Hypertrophic cardiomyopathy (HCM) remains the most common cause ofsudden cardiac death (SCD) in the young. Current strategies do not identify all HCMpatients at risk. A novel validated algorithm has recently been proposed by ESC guide-lines to guide implantable cardiac defibrillator (ICD) therapy based on the estimation of5-year risk of SCD. Recent evidence suggests that extensive myocardial fibrosis (.15%of LV mass) determined by late gadolinium enhancement (LGE) is independently asso-ciated with an increased risk of SCD events. Our aim is to establish the relation betweenLGE extension and the novel SCD risk-prediction model.Methods:Seventy patientswith HCM were prospectively recruited and underwent routineclinical evaluation and cardiac MRI protocol including assessment of function and scar(1.5 Tesla scanner). The probability of SCD at 5 years was calculated for every patientusing the proposed model. LGE imaging was acquired after the administration of 0.2mmol/kg of gadobutrol. Quantification of LGE was performed using the grayscale thresh-old method of ≥6 SDs. Extensive areas of LGE was defined by the presence of more than15% of LGE of the total LV mass. All CMR analysis was performed on commercially avail-able software (Circle CVI 42w, Calgary, Canada).Results:73% of the patientsshowedareas ofLGE(n=51).Theextensionof LGEwas posi-tively correlated with the SCD risk prediction (r=0.62, p,0.0001). Low, intermediate andhigh-risk groups according to the model showed significantly different extent of LGE(6.0+7 vs. 16+9 vs. 21+5 %, p,0.0001). 4 patients (7%) in low-risk group and 4(57%) in the intermediate-risk showed extensive areas of LGE. All high-risk patients(n=5) showed extensive areas of LGE.Conclusions: LGE extension is concordant with the model defining low and high-riskgroups? in intermediate-risk patients it seems to provide additional information andmay allow a better discrimination supporting ICD decision. LGE quantification holdspromise for SCD stratification in HCM.
P1042Overweight may aggravate early disease in hypertrophic cardiomyopathymutation positive family members
LA. Dejgaard1; T. Haland1; OH. Lie1; R. Massey2; T. Edvardsen1; KH. Haugaa1
1Oslo University Hospital, Deptof Cardiology andCenter for Cardiological Innovation,OsloUniversity Hospital, Rikshospitalet, Oslo, Norway; 2Oslo University Hospital, Dept ofCardiology, Oslo University Hospital, Rikshospitalet, Oslo, Norway
Purpose: Overweight has been associated with increased left ventricular (LV) mass andprogression of heart failure in hypertrophic cardiomyopathy (HCM). We aimed to explorecardiac changes in overweight HCM genotype positive (G+), phenotype negative (P-)family members.Methods: We recruited 134 HCM G+ family members by cascade genetic screening. Byechocardiography, we assessed LV ejection fraction (LVEF), maximum wall thickness(MWT), interventricular septal diameter (IVSd), LV mass (LVM), LVM index (LVMI) andleft atrial (LA) diameter. Diastolic parameters such as E/A ratio and e’ were assessed.Body mass index (BMI)≥25 kg/m2 was defined as overweight.Results: Of the 134 HCM G+ familymembers, 93 (69%) had MWT,13mm, defined asHCM G+/P-. The HCM G+/P- family members (age 36+14years, 63% female) hadBMI 23.9+3.9 kg/m2 and 24 (26%) had BMI≥25 kg/m2. Those with BMI≥25 kg/m2 hadthicker IVSd (9+1mm vs. 8+1mm, p,0.001) larger LA diameter (37+5mm vs. 32+7mm, p,0.001), greater LVM (155+33g vs. 123+29g, p,0.001) and LVMI (78+16g/m2 vs. 70+14g/m2, p= 0.03). E/A ratio (1.3+0.5 vs. 1.8+0.6, p=0.001) and e’(10+3cm/s vs. 13+3cm/s, p,0.001) were lower in the overweight subjects, whileLVEF did not differ (61% vs. 60%, p=0.47). BMI correlated with LA diameter (R=0.55,p,0.001), e’ (R=0.45, p,0.001) and LVM (R=0.45, p,0.001).
Conclusion: Overweight was related to thicker IVSd, larger LA diameter, greater LVM, andaltered diastolic parameters in HCM G+P- family members. Overweight may aggravateearly changes of disease in HCM.
P1043Longitudinal Strain/Strain Rate of papillary muscles in hypertrophiccardiomyopathy patients
EN. Pavlyukova1; VA. Evtushenko2; KA. Smushlyaev2; RS. Karpov2
1of cardiology and medical university, Tomsk, Russian Federation; 2Institute of Cardiology,Tomsk, Russian Federation
The aim of the study was to estimate Longitudinal Strain/Strain Rate (S/SR) of papillarymuscles (PM) and PM dyssynchrony in hypertrophic cardiomyopathy (HCMP) patients.Methods: The study was performed in 34 HCMP patients (aged 48.8+14.8 years, indexof left ventricular mass (ILVM) 203.5+79.6 g/m2, left ventricular (LV) outflow tract gradient82.3+13.4/49.7+10.5 mm Hg), 29 hypertensive patients with asymmetric LV hyper-trophy (aged 54.5+9.0 years, ILVM 173.6+54.4 g/m2) and 25 control subjects(47.2+10.9 years, ILVM 77.8+26.7 g/m2).All patients underwent coronary angiographyand they did not have coronary artery disease.The parameters of the degree of mitral regurgitation (MR) and deformation of mitral appar-atus were obtained using standard echocardiography. The longitudinal S/SR, time topeak Strain of anterolateral and posteromedial PM were calculated using Speckle Track-ing Imaging (Vivid E9 and EchoPac, GE Healthcare). The difference of 65 ms and more intime to peak strain between anterolateral and posteromedial PM was considered indica-tive of PM dyssynchrony.Results: Longitudinal S/SR of the anterolateral and posteromedial PM were reduced(p,0.01) in HCMP patients (anterolateral PM: Strain 21.39+2,14%; SR-0.15+0,15 s-1; posteromadial PM: Strain 28.00+6.21%; SR-0,81+0,21 s-1) in compared as hyper-tensive patients (anterolateral PM: Strain 220.17+5.13%; SR-1.31+0.12 s-1; postero-madial PM: Strain 212.21+2.59%; SR-0.94+0.21 s-1) and control group (anterolateralPM: Strain 224.06+10.12%; SR-1.66+0.12 s-1; posteromadial PM: Strain -21.38+6.56%; SR-1.16+0,21 s-1). Twelve patients with HCMP had positive Strain of the poster-omedial PM and 5 (15.6%) patients had positive strain of the anterolateral PM. Only one(3.4%) patient with hypertension had positive Strain of the posteromedial PM.Strain of the posteromedial PM correlated with parameters of degree of MR: vena con-tracta (r=0.72; p=0.02), ERO (r=0.43 p=0.03), volume (r=0.62; p=0.001) and leftatrial volume (r=0.56; p=0.03) in HCMP patients. We found correlates between time topeak Strain of the posteromedial PM and parameters of MR: volume (r=0.48; p=0.01)and vena contracta (r=0.49; p=0.003) in these patients.PM dyssynchonyhasbeen found in 18 (62.9%)HCMP patients and in 2 (8.0%) patients withhypertension. PM dyssynchrony did not reflect the degree of MR in patients with HCMP.Conclusion: Longitudinal S/SR of the anterolateral and posteromedial PM were reducedin HCMP patients. Strain of the posteromedial PM correlated with parameters of degree ofMR. PM dyssynchrony did not reflect the degree of MR in HCMP patients.
P1044Prognostic value of fibrosis on hypertrophic cardiomyopathy, atrial andventricular remodeling on echography and collagene markers
A. Zaroui; MONIA. Asmi; RYM. Ben Said; WIEM. Zidi; SANA. Wali; M. Feki; MS. Mourali;NEZIHZ. Kaabachi; RACHID. MechmecheLa Rabta Teaching Hospital, Tunis, Tunisia
Hypertrophic cardiomyopathy (HCM) is a disease characterized by cell disorganizationwith a matrix remodeling leading to fibrosis. Aim: to investigate biological markerswhich are the amino terminal pro peptide of type III collagen (PIIINP), a synthetic indicatorwhich may reflect the rate of myocardial fibrosis, a metalloproteinase (MMP3)involved inthe regulation of collagen and its specific tissue inhibitor TIPM2.we included 107 patientsand175 controls who beneficied of aclinical study. theserum level of thePIIINP,MMP3 andTIMP2 activities were determined in the peripheral vein by ELISA technique. We studiedthe association of serum levels of these markers with clinical, echocardiographic andprognostic parameters.Results: The meanagewas49years,60weremale,75%weresymptomatic (palpitations in38% of cases, chest pain in 28% of cases, syncope in 25% of cases) the rate of PIIINP wassignificantly higher in patients compared with controls (361.92+41.6 pg/ ml vs 242.80+
Abstract P1042 Figure.
Abstracts ii169
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022
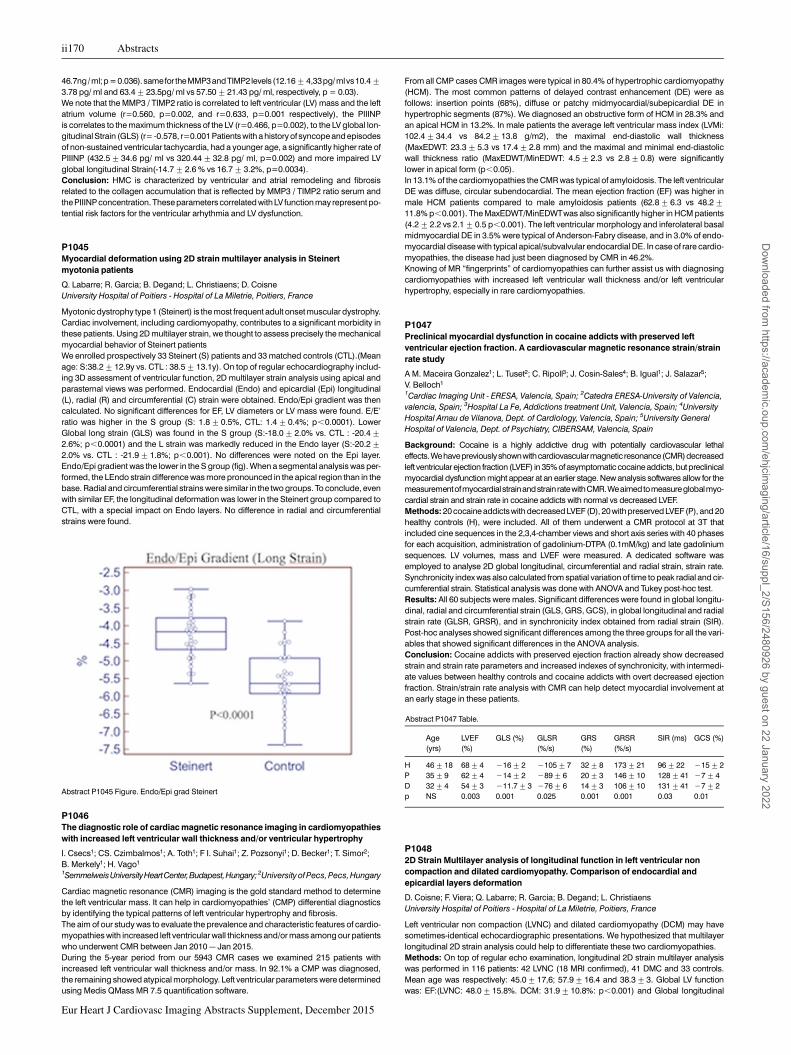
46.7ng/ml;p=0.036). samefor theMMP3andTIMP2 levels (12.16+4,33pg/mlvs10.4+3.78 pg/ ml and 63.4+23.5pg/ ml vs 57.50+21.43 pg/ ml, respectively, p = 0.03).We note that the MMP3 / TIMP2 ratio is correlated to left ventricular (LV) mass and the leftatrium volume (r=0.560, p=0.002, and r=0.633, p=0.001 respectively), the PIIINPis correlates to the maximum thickness of the LV (r=0.466, p=0.002), to the LV global lon-gitudinal Strain (GLS) (r= -0.578, r=0.001 Patients with a history of syncope and episodesof non-sustained ventricular tachycardia, had a younger age, a significantly higher rate ofPIIINP (432.5+34.6 pg/ ml vs 320.44+32.8 pg/ ml, p=0.002) and more impaired LVglobal longitudinal Strain(-14.7+2.6 % vs 16.7+3.2%, p=0.0034).Conclusion: HMC is characterized by ventricular and atrial remodeling and fibrosisrelated to the collagen accumulation that is reflected by MMP3 / TIMP2 ratio serum andthe PIIINP concentration. These parameters correlated with LV function may represent po-tential risk factors for the ventricular arhythmia and LV dysfunction.
P1045Myocardial deformation using 2D strain multilayer analysis in Steinertmyotonia patients
Q. Labarre; R. Garcia; B. Degand; L. Christiaens; D. CoisneUniversity Hospital of Poitiers - Hospital of La Miletrie, Poitiers, France
Myotonic dystrophy type 1 (Steinert) is the most frequent adult onset muscular dystrophy.Cardiac involvement, including cardiomyopathy, contributes to a significant morbidity inthese patients. Using 2D multilayer strain, we thought to assess precisely the mechanicalmyocardial behavior of Steinert patientsWe enrolled prospectively 33 Steinert (S) patients and 33 matched controls (CTL).(Meanage: S:38.2+12.9y vs. CTL : 38.5+13.1y). On top of regular echocardiography includ-ing 3D assessment of ventricular function, 2D multilayer strain analysis using apical andparasternal views was performed. Endocardial (Endo) and epicardial (Epi) longitudinal(L), radial (R) and circumferential (C) strain were obtained. Endo/Epi gradient was thencalculated. No significant differences for EF, LV diameters or LV mass were found. E/E’ratio was higher in the S group (S: 1.8+0.5%, CTL: 1.4+0.4%; p,0.0001). LowerGlobal long strain (GLS) was found in the S group (S:-18.0+2.0% vs. CTL : -20.4+2.6%; p,0.0001) and the L strain was markedly reduced in the Endo layer (S:-20.2+2.0% vs. CTL : -21.9+1.8%; p,0.001). No differences were noted on the Epi layer.Endo/Epi gradient was the lower in the S group (fig). When a segmental analysis was per-formed, the LEndo strain difference was more pronounced in the apical region than in thebase. Radial and circumferential strains were similar in the two groups. To conclude, evenwith similar EF, the longitudinal deformation was lower in the Steinert group compared toCTL, with a special impact on Endo layers. No difference in radial and circumferentialstrains were found.
P1046The diagnostic role of cardiac magnetic resonance imaging in cardiomyopathieswith increased left ventricular wall thickness and/or ventricular hypertrophy
I. Csecs1; CS. Czimbalmos1; A. Toth1; F I. Suhai1; Z. Pozsonyi1; D. Becker1; T. Simor2;B. Merkely1; H. Vago1
1SemmelweisUniversityHeartCenter,Budapest,Hungary;2University of Pecs, Pecs, Hungary
Cardiac magnetic resonance (CMR) imaging is the gold standard method to determinethe left ventricular mass. It can help in cardiomyopathies’ (CMP) differential diagnosticsby identifying the typical patterns of left ventricular hypertrophy and fibrosis.The aim of our study was to evaluate the prevalence and characteristic features of cardio-myopathies with increased left ventricular wall thickness and/or mass among our patientswho underwent CMR between Jan 2010 – Jan 2015.During the 5-year period from our 5943 CMR cases we examined 215 patients withincreased left ventricular wall thickness and/or mass. In 92.1% a CMP was diagnosed,the remaining showed atypical morphology. Left ventricular parameters were determinedusing Medis QMass MR 7.5 quantification software.
From all CMP cases CMR images were typical in 80.4% of hypertrophic cardiomyopathy(HCM). The most common patterns of delayed contrast enhancement (DE) were asfollows: insertion points (68%), diffuse or patchy midmyocardial/subepicardial DE inhypertrophic segments (87%). We diagnosed an obstructive form of HCM in 28.3% andan apical HCM in 13.2%. In male patients the average left ventricular mass index (LVMi:102.4+34.4 vs 84.2+13.8 g/m2), the maximal end-diastolic wall thickness(MaxEDWT: 23.3+5.3 vs 17.4+2.8 mm) and the maximal and minimal end-diastolicwall thickness ratio (MaxEDWT/MinEDWT: 4.5+2.3 vs 2.8+0.8) were significantlylower in apical form (p,0.05).In 13.1% of the cardiomyopathies the CMR was typical of amyloidosis. The left ventricularDE was diffuse, circular subendocardial. The mean ejection fraction (EF) was higher inmale HCM patients compared to male amyloidosis patients (62.8+6.3 vs 48.2+11.8% p,0.001). The MaxEDWT/MinEDWTwas also significantly higher in HCM patients(4.2+2.2 vs 2.1+0.5 p,0.001). The left ventricular morphology and inferolateral basalmidmyocardial DE in 3.5% were typical of Anderson-Fabry disease, and in 3.0% of endo-myocardial disease with typical apical/subvalvular endocardial DE. In case of rare cardio-myopathies, the disease had just been diagnosed by CMR in 46.2%.Knowing of MR “fingerprints” of cardiomyopathies can further assist us with diagnosingcardiomyopathies with increased left ventricular wall thickness and/or left ventricularhypertrophy, especially in rare cardiomyopathies.
P1047Preclinical myocardial dysfunction in cocaine addicts with preserved leftventricular ejection fraction. A cardiovascular magnetic resonance strain/strainrate study
A M. Maceira Gonzalez1; L. Tuset2; C. Ripoll3; J. Cosin-Sales4; B. Igual1; J. Salazar5;V. Belloch1
1Cardiac Imaging Unit - ERESA, Valencia, Spain; 2Catedra ERESA-University of Valencia,valencia, Spain; 3Hospital La Fe, Addictions treatment Unit, Valencia, Spain; 4UniversityHospital Arnau de Vilanova, Dept. of Cardiology, Valencia, Spain; 5University GeneralHospital of Valencia, Dept. of Psychiatry, CIBERSAM, Valencia, Spain
Background: Cocaine is a highly addictive drug with potentially cardiovascular lethaleffects.Wehavepreviouslyshownwithcardiovascularmagnetic resonance(CMR)decreasedleft ventricular ejection fraction (LVEF) in 35% of asymptomatic cocaine addicts, but preclinicalmyocardial dysfunction might appear at an earlier stage. New analysis softwares allow for themeasurementofmyocardialstrainandstrainratewithCMR.Weaimedtomeasureglobalmyo-cardial strain and strain rate in cocaine addicts with normal vs decreased LVEF.Methods: 20 cocaine addictswith decreased LVEF(D), 20 with preserved LVEF(P), and 20healthy controls (H), were included. All of them underwent a CMR protocol at 3T thatincluded cine sequences in the 2,3,4-chamber views and short axis series with 40 phasesfor each acquisition, administration of gadolinium-DTPA (0.1mM/kg) and late gadoliniumsequences. LV volumes, mass and LVEF were measured. A dedicated software wasemployed to analyse 2D global longitudinal, circumferential and radial strain, strain rate.Synchronicity index was also calculated from spatial variation of time to peak radial and cir-cumferential strain. Statistical analysis was done with ANOVA and Tukey post-hoc test.Results: All 60 subjects were males. Significant differences were found in global longitu-dinal, radial and circumferential strain (GLS, GRS, GCS), in global longitudinal and radialstrain rate (GLSR, GRSR), and in synchronicity index obtained from radial strain (SIR).Post-hoc analyses showed significant differences among the three groups for all the vari-ables that showed significant differences in the ANOVA analysis.Conclusion: Cocaine addicts with preserved ejection fraction already show decreasedstrain and strain rate parameters and increased indexes of synchronicity, with intermedi-ate values between healthy controls and cocaine addicts with overt decreased ejectionfraction. Strain/strain rate analysis with CMR can help detect myocardial involvement atan early stage in these patients.
Abstract P1047 Table.
Age(yrs)
LVEF(%)
GLS (%) GLSR(%/s)
GRS(%)
GRSR(%/s)
SIR (ms) GCS (%)
H 46+18 68+4 216+2 2105+7 32+8 173+21 96+22 215+2P 35+9 62+4 214+2 289+6 20+3 146+10 128+41 27+4D 32+4 54+3 211.7+3 276+6 14+3 106+10 131+41 27+2p NS 0.003 0.001 0.025 0.001 0.001 0.03 0.01
P10482D Strain Multilayer analysis of longitudinal function in left ventricular noncompaction and dilated cardiomyopathy. Comparison of endocardial andepicardial layers deformation
D. Coisne; F. Viera; Q. Labarre; R. Garcia; B. Degand; L. ChristiaensUniversity Hospital of Poitiers - Hospital of La Miletrie, Poitiers, France
Left ventricular non compaction (LVNC) and dilated cardiomyopathy (DCM) may havesometimes-identical echocardiographic presentations. We hypothesized that multilayerlongitudinal 2D strain analysis could help to differentiate these two cardiomyopathies.Methods: On top of regular echo examination, longitudinal 2D strain multilayer analysiswas performed in 116 patients: 42 LVNC (18 MRI confirmed), 41 DMC and 33 controls.Mean age was respectively: 45.0+17,6; 57.9+16.4 and 38.3+3. Global LV functionwas: EF:(LVNC: 48.0+15.8%. DCM: 31.9+10.8%: p,0.001) and Global longitudinal
Abstract P1045 Figure. Endo/Epi grad Steinert
ii170 Abstracts
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022
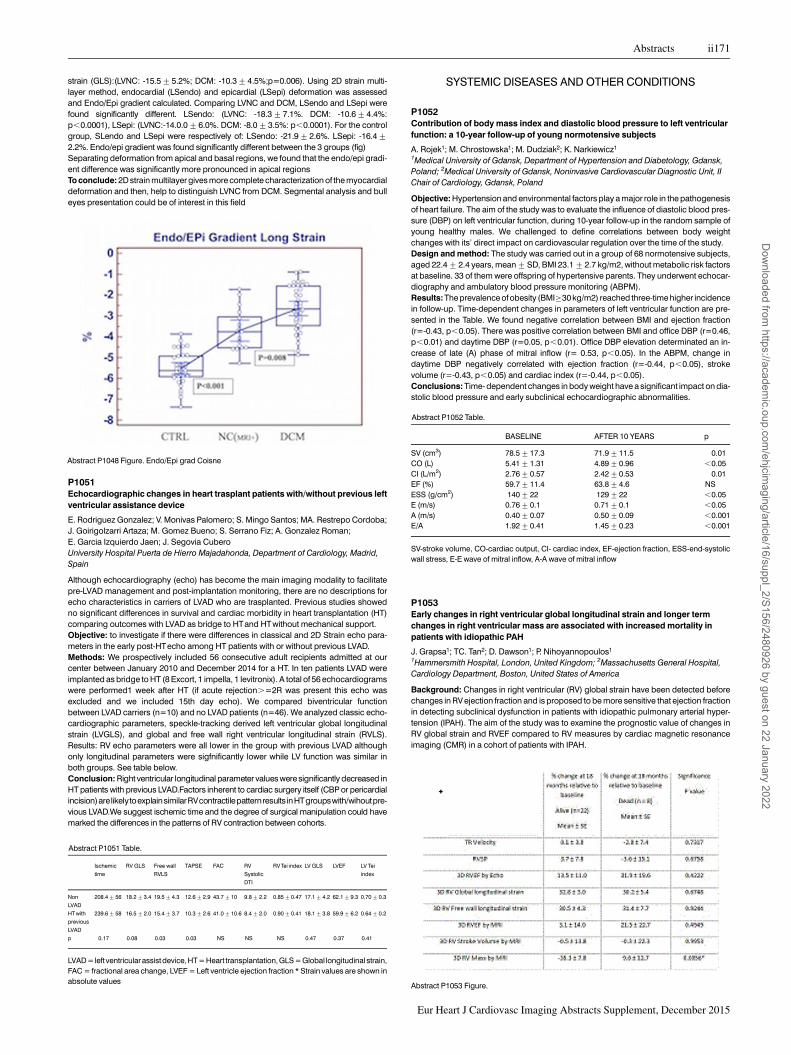
strain (GLS):(LVNC: -15.5+5.2%; DCM: -10.3+4.5%;p=0.006). Using 2D strain multi-layer method, endocardial (LSendo) and epicardial (LSepi) deformation was assessedand Endo/Epi gradient calculated. Comparing LVNC and DCM, LSendo and LSepi werefound significantly different. LSendo: (LVNC: -18.3+7.1%. DCM: -10.6+4.4%:p,0.0001), LSepi: (LVNC:-14.0.0+6.0%. DCM: -8.0+3.5%: p,0.0001). For the controlgroup, SLendo and LSepi were respectively of: LSendo: -21.9+2.6%. LSepi: -16.4+2.2%. Endo/epi gradient was found significantly different between the 3 groups (fig)Separating deformation from apical and basal regions, we found that the endo/epi gradi-ent difference was significantly more pronounced in apical regionsTo conclude: 2D strain multilayer gives more complete characterization of the myocardialdeformation and then, help to distinguish LVNC from DCM. Segmental analysis and bulleyes presentation could be of interest in this field
P1051Echocardiographic changes in heart trasplant patients with/without previous leftventricular assistance device
E. Rodriguez Gonzalez; V. Monivas Palomero; S. Mingo Santos; MA. Restrepo Cordoba;J. Goirigolzarri Artaza; M. Gomez Bueno; S. Serrano Fiz; A. Gonzalez Roman;E. Garcia Izquierdo Jaen; J. Segovia CuberoUniversity Hospital Puerta de Hierro Majadahonda, Department of Cardiology, Madrid,Spain
Although echocardiography (echo) has become the main imaging modality to facilitatepre-LVAD management and post-implantation monitoring, there are no descriptions forecho characteristics in carriers of LVAD who are trasplanted. Previous studies showedno significant differences in survival and cardiac morbidity in heart transplantation (HT)comparing outcomes with LVAD as bridge to HTand HTwithout mechanical support.Objective: to investigate if there were differences in classical and 2D Strain echo para-meters in the early post-HTecho among HT patients with or without previous LVAD.Methods: We prospectively included 56 consecutive adult recipients admitted at ourcenter between January 2010 and December 2014 for a HT. In ten patients LVAD wereimplanted as bridge to HT (8 Excort, 1 impella, 1 levitronix). A total of 56 echocardiogramswere performed1 week after HT (if acute rejection.=2R was present this echo wasexcluded and we included 15th day echo). We compared biventricular functionbetween LVAD carriers (n=10) and no LVAD patients (n=46). We analyzed classic echo-cardiographic parameters, speckle-tracking derived left ventricular global longitudinalstrain (LVGLS), and global and free wall right ventricular longitudinal strain (RVLS).Results: RV echo parameters were all lower in the group with previous LVAD althoughonly longitudinal parameters were sigfnificantly lower while LV function was similar inboth groups. See table below.Conclusion: Right ventricular longitudinal parameter values were significantly decreased inHT patients with previous LVAD.Factors inherent to cardiac surgery itself (CBP or pericardialincision)arelikelytoexplainsimilarRVcontractilepatternresults inHTgroupswith/wihoutpre-vious LVAD.We suggest ischemic time and the degree of surgical manipulation could havemarked the differences in the patterns of RV contraction between cohorts.
Abstract P1051 Table.
Ischemic
time
RV GLS Free wall
RVLS
TAPSE FAC RV
SystolicDTI
RV Tei index LV GLS LVEF LV Tei
index
NonLVAD
208.4+56 18.2+3.4 19.5+4.3 12.6+2.9 43.7+10 9.8+2.2 0.85+0.47 17.1+4.2 62.1+9.3 0.70+0.3
HT withpreviousLVAD
239.6+58 16.5+2.0 15.4+3.7 10.3+2.6 41.0+10.6 8.4+2.0 0.90+0.41 18.1+3.8 59.9+6.2 0.64+0.2
p 0.17 0.08 0.03 0.03 NS NS NS 0.47 0.37 0.41
LVAD=left ventricular assistdevice, HT= Heart transplantation, GLS =Global longitudinalstrain,FAC = fractional area change, LVEF = Left ventricle ejection fraction * Strain values are shown inabsolute values
SYSTEMIC DISEASES AND OTHER CONDITIONS
P1052Contribution of body mass index and diastolic blood pressure to left ventricularfunction: a 10-year follow-up of young normotensive subjects
A. Rojek1; M. Chrostowska1; M. Dudziak2; K. Narkiewicz1
1Medical University of Gdansk, Department of Hypertension and Diabetology, Gdansk,Poland; 2Medical University of Gdansk, Noninvasive Cardiovascular Diagnostic Unit, IIChair of Cardiology, Gdansk, Poland
Objective: Hypertension and environmental factors play a major role in the pathogenesisof heart failure. The aim of the study was to evaluate the influence of diastolic blood pres-sure (DBP) on left ventricular function, during 10-year follow-up in the random sample ofyoung healthy males. We challenged to define correlations between body weightchanges with its’ direct impact on cardiovascular regulation over the time of the study.Design and method: The study was carried out in a group of 68 normotensive subjects,aged 22.4+2.4 years, mean+SD, BMI 23.1+2.7 kg/m2, without metabolic risk factorsat baseline. 33 of them were offspring of hypertensive parents. They underwent echocar-diography and ambulatory blood pressure monitoring (ABPM).Results: The prevalence of obesity (BMI≥30 kg/m2) reached three-time higher incidencein follow-up. Time-dependent changes in parameters of left ventricular function are pre-sented in the Table. We found negative correlation between BMI and ejection fraction(r=-0.43, p,0.05). There was positive correlation between BMI and office DBP (r=0.46,p,0.01) and daytime DBP (r=0.05, p,0.01). Office DBP elevation determinated an in-crease of late (A) phase of mitral inflow (r= 0.53, p,0.05). In the ABPM, change indaytime DBP negatively correlated with ejection fraction (r=-0.44, p,0.05), strokevolume (r=-0.43, p,0.05) and cardiac index (r=-0.44, p,0.05).Conclusions: Time- dependent changes in body weight have a significant impact on dia-stolic blood pressure and early subclinical echocardiographic abnormalities.
Abstract P1052 Table.
BASELINE AFTER 10 YEARS p
SV (cm3) 78.5+17.3 71.9+11.5 0.01CO (L) 5.41+1.31 4.89+0.96 ,0.05CI (L/m2) 2.76+0.57 2.42+0.53 0.01EF (%) 59.7+11.4 63.8+4.6 NSESS (g/cm2) 140+22 129+22 ,0.05E (m/s) 0.76+0.1 0.71+0.1 ,0.05A (m/s) 0.40+0.07 0.50+0.09 ,0.001E/A 1.92+0.41 1.45+0.23 ,0.001
SV-stroke volume, CO-cardiac output, CI- cardiac index, EF-ejection fraction, ESS-end-systolicwall stress, E-E wave of mitral inflow, A-A wave of mitral inflow
P1053Early changes in right ventricular global longitudinal strain and longer termchanges in right ventricular mass are associated with increased mortality inpatients with idiopathic PAH
J. Grapsa1; TC. Tan2; D. Dawson1; P. Nihoyannopoulos1
1Hammersmith Hospital, London, United Kingdom; 2Massachusetts General Hospital,Cardiology Department, Boston, United States of America
Background: Changes in right ventricular (RV) global strain have been detected beforechanges in RV ejection fraction and is proposed to be more sensitive that ejection fractionin detecting subclinical dysfunction in patients with idiopathic pulmonary arterial hyper-tension (IPAH). The aim of the study was to examine the prognostic value of changes inRV global strain and RVEF compared to RV measures by cardiac magnetic resonanceimaging (CMR) in a cohort of patients with IPAH.
Abstract P1048 Figure. Endo/Epi grad Coisne
Abstract P1053 Figure.
Abstracts ii171
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

Methods: Thirty consecutive patients (24 women, mean age 46.8+5.3 years) with newlydiagnosed IPAH were prospectively recruited and followed with serial transthoracic echo-cardiograms (TTE) and CMR 6 monthly for 18 months. A range of 2D and 3D echocardio-graphic measures of right ventricular dimensions and systolic function, were assessed ateach time point by CMR and by echo. 2D global longitudianal strain (GLS) and 3D RVEFwas assessed using vendor independent software. Statistical analyses were performedusing JMP statistical package.Results: Eight patients (27%) died. At 6 months, changes in 2D RV global longitudinalstrain but not 3D RVEF or RV mass was significant in patients who died compared topatients who were alive. However at 18 months only changes relative to baseline in RVmass by CMR and not RV strain or LVEF was significant in patients who died.Conclusion: Early changes (within the first 6 months of commencing treatment) in RVglobal longitudinal strain may have prognostic value in patients with IPAH. Howeverafter 18 months of treatment, only changes in RV mass, may have prognostic value andnot changes in RV dimensions and function.
P1054Echocardiographic and hemodynamic features of PAH and PH - PID in systemicsclerosis
N. MethiaCHU Mustapha, Cardiology, Algiers, Algeria
Aims: The distinction between pulmonary arterial hypertension (PAH) and pulmonaryhypertension (PH) secondary to severe diffuse interstitial lung disease (PH - PID) in sys-temic sclerosis (SSc) is important, before the introduction of a specific therapy for PAH.We compared echocardiographic and hemodynamic characteristics of PAH and PH -PID in scleroderma Algerian patients.Materials and Methods: Our study is transversal, descriptive. From December 2010 toJune 2013, 205 women and 29 men with SSc were included.We based on the velocity of tricuspid regurgitation (VTR) to select patients at high risk ofPH (VTR . 3m/s) to benefit from a right heart catheterization to confirm PH (mPAP≥25mmHg).All patients underwent ahigh resolution chest CTand functional respiratory investigations.Tests suitable for small samples were used.Results: We have detected and confirmed 12 PAH and 3 PID-HTP in this series.All patients with PH-PID had severe lung disease with CVF,35%)Pulmonary hypertension was more severe with a larger repercussion on the right cavitiesin the PAH group than in the HTP-PID group with respectively a mean velocity of VTR of4,24m / s vs 3,73m / s (p = 0.012), an RA surface 25.5 cm2 vs 14.66 cm2 (p = 0.006), aRV 33.5 vs 23.3 cm (p = 0.001), a TEI value of 0, 75 vs 0.53 (p = 0.05).This was confirmed at right heart catheterization with mean PAP:48mmHg vs 31.66(p =0.009), pulmonary vascular resistance (PVR): 10.39 vs 5.70uw (p = 0.002) and RAP 11,83 mm Hg vs 5 (p = 0.017)Conclusion: PH-PID is generally moderate with less severe impact on the right cavitiescompared to the PAH
P1055Combined circumferential and longitudinal left ventricular systolic dysfunction inpatients with rheumatoid arthritis without overt cardiac disease
G. Cioffi1; O. Viapiana2; F. Ognibeni2; A. Dalbeni2; D. Gatti2; C. Di Nora3; C. Mazzone4;G. Faganello4; A. Di Lenarda4; M. Rossini21Villa Bianca Hospital, Trento, Italy; 2University of Verona, Department of Medicine, Verona,Italy; 3University Hospital Riuniti, Cardiovascular Department, Trieste, Italy;4Cardiovascular Center A.S.S. 1 of Trieste, Trieste, Italy
Aim: Patients with rheumatoid arthritis (RA) have an increased risk for CV disease. Due toaccelerated atherosclerosis and changes in left ventricular (LV) geometry, LV circumferen-tial and longitudinal (C&L) shortening may be impaired in these patients despite pre-served LV ejection fraction. We focused on prevalence and factors associated withcombined C&L dysfunction in RA patients.Methods and Results: 198 outpatients with RA without overt cardiac disease wereanalyzed during January-June 2014 and compared with 198 matched controls.C&L function were evaluated by stress-corrected midwall shortening (sc-MS) andTissue Doppler mitral annular peak systolic velocity (S’). Combined C&L dysfunctionwas defined if sc-MS ,86.5% and S’ ,9.0 cm/sec, (10th percentiles of sc-MS and S’derived by 132 healthy people, respectively). Combined C&L dysfunction wasdetected in 56 patients (28%), and was associated with LV mass (OR 1.03 [CI1.01-1.06], p=0.04) and concentric LV geometry (OR 2.76 [CI 1.07-7.15], p=0.03).By multiple logistic regression analysis, RA emerged as independent factor asso-ciated with combined C&L dysfunction (OR 2.57 [CI 1.06 – 6.25]). The relationshipbetween sc-MS and S’ was statistically significant in the subgroup of 142 patientswithout combined C&L dysfunction (r=0.40, F statistic ,0.001), having the bestfitting by a linear function (sc-MS=58.1+3.34*peak S’; r2=0.19, p,0.0001), absentin patients with combined C&L dysfunction.Conclusions: Combined LV C&L dysfunction is detectable in about one-fourth of asymp-tomatic RA patients and is associated with LVconcentric remodeling/hypertrophy.RA pre-dicts this worrisome condition, which may explain the increased risk for CVevents in thesepatients.
P1056Echocardiographic parameters correlation with abnormal liver tests in patientswith exacerbated chronic heart failure
G. Styczynski; A. Milewska; M. Marczewska; P. Sobieraj; M. Sobczynska; M. Dabrowski;A. Kuch-Wocial; C A. SzmigielskiMedical University of Warsaw, Department of Internal Medicine, Hypertension & VascularDiseases, Warsaw, Poland
Purpose: Elevated total bilirubin (TB) and transaminases are frequently reported inpatients with chronic heart failure (CHF) and those parameters are related to thesepatients’ worse prognosis. We decided to evaluate echocardiographic parameters correl-ation with elevated TB and transaminases in patients with exacerbated CHF.Methods: In 146 consecutive patients (mean age 75 years, 58% males) we analyzed fol-lowing echocardiographic parameters: right ventricular diameter (RVEDD), right atrialarea (RAA), tricuspid regurgitation (TR), right ventricular systolic pressure (RVSP), tricus-pid annular plane systolic excursion (TAPSE), tricuspid lateral annulus systolic velocity(RVVTI), estimated right atrial pressure (RAP), portal vein pulsatility index (PVPI), left ven-tricular diameter (LVEDD), left ventricular ejection fraction (LVEF), cardiac output (CO) andcardiac index (CI).Results: Elevated TB was found in 59 patients (40%), and transaminases in 43 patients(29%). In univariate logistic regression analysis RVEDD, RAA, TR, RAP, TAPSE, RVVTI,PVPI, LVEF, CO and CI were significant predictors of elevated TB, and LVEDD indexedfor body surface area was significant predictor of elevated transaminases (all p,0.05).However, in multivariate regression model, only PVPI remained a significant predictor ofelevated TB. Sensitivity, specificity, positive and negative predictive values of PVPI.0.5in the prediction of elevated TB were: 80%, 86%, 80% and 86% respectively.Conclusions: Several echocardiographic indices of right heart dysfunction and low cardiacoutput are related to increased TB in patients with exacerbated chronic heart failure. Anincreased portal vein pulsatility index (PVPI) has the best predictive value in these patients.
P1057Male and female athlete’s left ventricular magnetic resonance parametersdetermined by trabecula quantification in different sport activities
C. Czimbalmos1; H. Vago1; I. Csecs1; A. Toth1; F I. Suhai1; O. Kiss1; N. Sydo1; D. Becker1;T. Simor2; B. Merkely1
1Semmelweis University Heart Center, Budapest, Hungary; 2University of Pecs HeartInstitute, Pecs, Hungary
Introduction: Cardiac magnetic resonance (CMR) imaging is the gold standard methodof evaluation left ventricular volumes, ejection fraction and mass. A new CMR softwareoption enables semi-automatic quantification of myocardial trabeculation.Purpose: Our goal was to evaluate left ventricular magnetic resonance parameters forathletes and to examine how these parameters change with quantitative analysis of leftventricular trabeculation.Methods andMaterials: CMR examination was performed on 159 top athletes (121 male,38 female; 25+7y) and on 68 healthy volunteers (41 male, 27 female, 27+6y). The fol-lowing types of sports were examined: canoe and kayak paddlers (n=40), water-poloplayers (n=29), rowers (n=17), cyclists (n=9), kick-boxers (n=9), football players(n=6) and ultra-marathon runners (n=5). Left ventricular parameters were determinedusing Medis QMass MR 7.6 quantification software. Left ventricular trabeculae mass(TrM) was also analyzed quantitatively.Results:Left ventricular volumes andmass (LVMi) were significantly higher in the athlete’sgroup both with and without quantifying the TrM (p,0.001). When TrM was included in themeasurement, myocardial mass indices were higher, volumes were lower both in the ath-letes and in the control group (p,0.001). Compared to the malevolunteers, TrM index washigher both in male and female athletes (male: 20.8 g/m2+4.3 vs 18.3 g/m2+3.1;female: 16.9 g/m2+3.5 vs 13.6 g/m2+4.1). However, TrM% (TrM(g)/LVM(g)*100) washigher in the control group (male: 20.9%+2.5 vs 19.2%+3.9; female: 22.2%+5.8 vs19.7%+4). This suggests a more pronounced hypertrophy in the compact myocardiumdue to extensive physical training. LVMi corrected with TrM was significantly higher incanoe and kayak paddlers (121.5g/m2+16.6) compared to water-polo players (108.2g/m2+16.9), cyclists (101.2 g/m2+13.1), ultra-marathon runners (100.3 g/m2+9.8)and kick-boxers (88 g/m2+12.3). Moreover, kick-boxers had lower left ventricular end-diastolic (87.8 ml/m2+12.4 vs 103.9 ml/m2+12.3) and stroke volume index (58.1 ml/m2+6.5 vs 68.3 ml/m2+7.7) compared to canoe and kayak paddlers, and lower LVMicompared to rowers (110.8 g/m2+11.6) and water-polo players. This suggests a lessintense cardiac adaptation in kick-boxers, probably due to the technical components spe-cific to this sport.Conclusion: Quantitative analysis of myocardial trabeculation could fundamentally alternormal left ventricular parameters. Different sports activities were found to result in differ-ent cardiac adaptations.
P1058Strenuous effort is associated with the right ventricle functional changes in thegroup of master-level rowers
M. Konopka1; K. Burkhard-Jagodzinska2; W. Krol1; A. Jakubiak1; K. Aniol-Strzyzewska2;D. Sitkowski2; M. Dluzniewski1; W. Braksator11Medical University of Warsaw, Department of Cardiology, Hypertension and InternalDiseases, Warsaw, Poland; 2Institute of Sport, Department of Physiology, Warsaw, Poland
Purpose: The data on the right ventricle (RV) function changes in professional athletescaused by adaptation to high endurance training are the subject of active research. The
ii172 Abstracts
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

main purpose of this study was to determine RV free wall functional changes, expressedby 2-D speckle tracking echocardiography (2-D STE) derived strain and DTI-derived vel-ocities of the tricuspid annulus, according to the response to strenuous exercise.Methods: 32 master-level rowers (National Rowing Team) at the beginning of new rowingseason; 22 (69%) men; mean age 24,9+3,5 years; mean training period 11,1+3,6years; training time per week 21,5+5,6 hours. All subjects underwent cardiopulmonarytest (mean duration – 18,9+1,5 min) with the evaluation of peak oxygen consumption(VO2max – 62,8+4,9 ml/kg/min). 2-D STE with evaluation of longitudinal strain ineach segment of the right ventricle free-wall (basal – RVLS-B; mid – RVLS-M, apicalRVLS-A) and DTI-derived velocities of the tricuspid annulus (TV S’, TV E’, TV A) was per-formed twice: (1) at rest before exercise test (2) within 10 minutes after maximal exercisetest.Results: Compared with initial values, after maximal effort, a significant strain reductionwas observed in the basal (RVLS-B: -26,8+3,6 vs -23,8+3,7; p=0,001) and medial(RVLS-M: -29,7+2,9 vs -27,1+3,7; p=0,001) segments with no change in the apical(RVLS-A: -26,8+3,3 vs -26,7+3,6; p=0,09). We also observed post-exercise DTI-derived TV S’ reduction (15,5+2,9 vs 13,7+2,5; p=0,01). In contrast, diastolic functionexpressed by TV E’ and TV A’ was augmented: (E’: 17,0+3,4 vs 21,4+4,6; p,0,001),(A’: 11,5+2,9 vs 16,3+5,3; p,0,001).Conclusions: 1. Short period of time after strenuous effort in the group of top-level endur-ance athletes is associated with depression of RV systolic and augmentation of diastolicfunction.2. Reduction of 2D-STE derived strain is observed in the basal and mid RV segments(highest in the basal). It may explain the nature of physiological adaptation to significantlyincreased cardiac flow in endurance (IIIC) athletes.3. Significant changes are observed even after a relatively short but intense effort.
P1059Echocardiography predictors for recurrence after catheter ablation of atrialfibrillation
T. Sturmberger; V. Eder; C. Ebner; S. Winter; M. Martinek; H. Puererfellner; J. AichingerPublic Hospital Elisabethinen, Linz, Austria
Background: Catheter ablation (CA) is an effective and potentially curative treatment inpatients with atrial fibrillation (AF) to restore sinus rhythm (SR). However, the recurrencerateafter CAremains unsatisfactory andCA isanexpensive procedure withpotentially crit-ical complications. Thus, it is crucial to identify those patients who are most likely to benefitfrom AF ablation with respect to restoration of SR. The reported predictors of recurrenceafter CAare the presence of hypertension, long duration of AF, prolonged procedural time,enlarged LA diameter, or increased LA volume and decreased left atrial (LA) function ordecreased left atrial appendage (LAA) emptying velocity (LAV). However echocardio-graphic parameters for assessing SR maintenance after CA are not accurately defined.The aim of this study was to assess the echocardiographic predictors for the recurrenceof AF after CA.Methods and Results: A total of 138 patients (74% males, mean age 59,1years) with per-sistent or paroxysmal nonvalvular AF who had undergone CA in our institution betweenJanuary 2013 and March 2014 were included. In our cohort 89 patients (65%) underwentCA for the first time, 49 patients(35%) underwent multiple procedures, the last in the periodbetween January 2013 and March 2014. Transthoracic echocardiography was performedin all patients before the procedure. Left ventricular diastolic function was evaluatedaccording to current guidelines. The LAA velocity profiles were obtained by pulsed-waveDoppler interrogation 1 cm within the orifice of the LAA.The follow-up strategy after CA included clinical follow up, 12-lead electrocardiography(ECG) and 24-h ECG 3 and 6 months after CA.Results: During the follow up period 92 (67%) patients remained in SR after the finalprocedure. AF recurred in 46 (33%) patients. We observed that the presence of leftventricular diastolic dysfunction was the best predictor of AF recurrence. The presenceof LVDD was increasingly more likely in patients who required repeated ablations.Depressed left ventricular ejection fraction was not associated with AF relapse. In ourrestrospective study patients with decreased LAV (,40cm/sec) were more likely tohave AF recurrence.Conclusion: Our results indicate that elevated left ventricular filling pressure estimated byraised E/Eratio and decreased LAV is associated with increased risk of AF relapse afterCA. Patients with normal left ventricular diastolic function had the lowest recurrencerate. We did not find a correlation between left ventriclur systolic dysfunction and AFrecurrence.
P1060Echocardiographic evaluation of cardiac involvement in Hodgkin andnon-Hodgkin lymphomas
P. Sormani1; C. Rusconi2; M. Zancanella2; A. Peritore1; B. De Chiara3; F. Spano’3;P. Vallerio3; R. Cairoli2; C. Giannattasio1; A. Moreo3
1University of Milan-Bicocca, Milan, Italy; 2Niguarda Ca’ Granda Hospital, Division ofHematology, Milan, Italy; 3Dpt of Cardiology, Niguarda Hospital Milan, Milano, Italy
Purpose: To determine the rate of pericardial and myocardial abnormalities in patientsaffected by Hodgkin lymphoma (HL) and non-Hodgkin lymphoma (NHL) using cardiacultrasound at the time of diagnosis.Methods: We retrospectively analyzed echocardiographic findings in 558 patients withnewly diagnosed lymphoma (49% male, mean age 50+19 years) between 2006 and2014. We evaluate cardiac involvement as pericardial effusion and masses localized inmyocardium and pericardium separately of 213 HL and 345 NHL. These findings were
compared with computed tomography (CT)-scan and positron emission tomography(PET) imaging.Results: Among HL patients 13 (6.1%) had pericardial effusion at first echocardiog-raphy: in 8 (3.8%) cases pericardial effusion was mild, in 4 (1.9%) cases moderateand in 1 (0.4%) severe, requiring therapeutic pericardiocentesis. In 2 (0.9%) patientswith mediastinal bulky HL the mass was detected at ultrasound evaluation shifting theheart, without compression of cardiac structures. Among NHL patients 19 (5.5%) hadpericardial effusion: in 13 (3.7%) patients was mild, in 4 (1.2%) patients moderate andin 2 (0.6%) cases severe. Pericardiocentesis was performed in 3 cases. Patients withprimary mediastinal NHL had a grater incidence of pericardial effusion compared withremaining NHL patients (45% vs. 4.2%, p , 0.01). In 10 (2.9%) patients mediastinalmass was detected at cardiac ultrasound. No HL patients had myocardial localizationwhile 6 (1.7%) patients had a cardiac localization of the tumor; 3 (0.9% of NHL) patientshad a primary cardiac diffuse large B cell lymphoma (PCL) with right ventricular localiza-tion and infiltration causing dysfunction. All these echocadiographic findings (pericar-dial effusion and masses) were confirmed at CT scan, while PET did not show cardiacinvolvement except for the 3 PCL.Conclusions: Cardiac involvement in patients affected by lymphomas is a rare butserious condition that must be carefully monitored since it could have dramatic conse-quences. In these patients transthoracic echocardiography is a useful initial diagnostictool to evaluate myocardial and pericardial abnormalities. It is also an excellent techniqueto monitor patients during and after treatment. CTscan is routinely used for initial stagingand can provide additional cardiac information, while PET, probably due to physiologic-ally high myocardial up-take, proved to be a less sensitive tools for lymphoma relatedcardiac alterations and seems to be more useful in disease staging and response totherapy.
P1061Relation between red cell distribution width and left ventricular function indecompensated chronic heart failure
RN. Siliste1; A. Chitroceanu2; R. Ianula1; D. Spataru1; D. Isacoff11Coltea Clinical Hospital, Bucharest, Romania; 2University of Medicine and PharmacyCarol Davila, Bucharest, Romania
Background:andaim: Studieshave already shown that an increase in red celldistributionwidth (RDW) is associated with a poor prognosis in patients with heart failure (HF). Ourstudy aims to correlate RDW to biohumoral and echocardiographic parameters provedto be associated with a negative outcome in HF.Method: 100 patients with acute decompensated chronic heart failure admitted in Cardi-ology Unit during the period January 2013-December 2013 were included; mean age ofthe cohort 73.94+10.63 years, 60% female. Age- and sex-matched 30 control subjectswere also evaluated. Patients with cancer, moderate to severe anemia, COPD, infectiousdiseases or autoimmune disorders were excluded from both groups.Results: RDW was significantly higher in NYHA class IV patients vs. NYHA class III andclass II patients (14.26+3.37 % vs. 12.65+1.01% vs. 12.6+0.97%, p=0.03, respective-ly p= 0.41), but also in HF group compared to control group (13.06+2.26% vs. 12.0%+0.82, p=0.003). RDW correlates with serum NTproBNP (r=0.42, p=0.01) and E/A ratio(r=0.475, p=0.007), but not with left atrial volume index (r=-0.145), E/e ratio (r=0.07),LV ejection fraction (r=0.103), LV end-diastolic diameter (r=-0.05) or right ventricle diam-eter (r=0.172).Conclusions: RDW correlates with the severity of the symptoms (NYHA class), serumNTproBNP level and E/A ratio, but does not correlate with other echocardiographic markers(left atrial volume index, LV ejection fraction and LV or RV dilatation). RDW may be associatedwith severe disease by reflecting subtle metabolic and proinflammatory abnormalities in HF.
P1062Three dimensional transesophageal echocardiographic evaluation of aorticplaque after cerebrovascular event
AC. Rodrigues; C. Monaco; L. Guimaraes; R. Cordovil; R. Piveta; L. Franca; CH. Fischer;M. Vieira; E. Lira; S. MorhyHospital Israelita Albert Einstein, Sao Paulo, Brazil
Background: The presence of plaque in thoracic aorta has been associated with emboliccerebrovascular events. Three dimensional transesophageal echocardiography (3DTEE) is used to assess cardiac and vascular anatomy and function; however, data onaortic anatomy with this technique is scarce. We sought to evaluate whether additional in-formation of atherosclerotic aortic plaque morphology could be obtained by 3D TEE inpatients after a ischemic cerebrovascular accident (CVA).Methods: we studied patients . 18 years old after an acute (, 1 week) CVA confirmed bycomputed tomography or magnetic resonance. TEE was undertaken all patients con-secutively within one week of the index event to compare 3D with two dimensional (2D)findings such as plaque location, number, dimension and area, the presence of mobiledebris and ulcerations (defined as a crater on the plaque ≥2.0 mm in depth). The exam-ination was completed with assessment for intracavitary thrombi and interatrial septum forpatency of foramen ovale (PFO). Patients were followed for one year to assess for the pres-ence later events (cardiovascular death or new CVA).Results: We studied 64 patients, 33 (52%) female, aged 61+11 years old, 90 % in sinusrhythm. Aortic plaque was found mainly in the descending aorta (50%), followed byascending aorta (2%) and aortic arch (2%), with multiple plaques seen in descendingaorta. Similar measurements were obtained for plaque diameters (0.29+0,03cmwith 2D TEE and 0,29+0.04cm with 3D TEE), whereas measurements of plaque areawas found to be slightly increased for 3D measurements (0.24+0.02 cm2 versus
Abstracts ii173
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

0.37+0.03 cm2 for 2D and 3D TEE respectively, p , 0.05. Correlation for aortic plaquedimensions was excellent (r = 0.96), however, for aortic plaque area measurements cor-relations were less adequate(r = 0.70). Aortic debris were similarly seen both from 2Dand 3D TEE (3 versus 4 patients, p = NS), however, regarding the presence of ulcera-tions, 3D TEE was more accurate (6 ulcerations from 3D TEE compared to 2 for 2DTEE, p = 0.03). A PFO was found in 22 % of the patients, whereas none of the patientshad intracavitary thrombi. During follow-up only one patient had a new CVA, and onepatient died.Conclusion: Except for the presence of atherosclerotic ulcerated plaques, 3D TEE doesnot seem to provide important additional information over 2D TEE in patients with ische-mic stroke.
P1063Absence of left atrial stunning after cardioversion of recent-onset atrial fibrillationin patients at low stroke risk
E. Antonielli1; A. Pizzuti2; S. Dogliani3; B. Mabritto2; A. Bassignana3; D. Pancaldo3;B. Doronzo3
1Casa di Cura Citta di Bra, Bra, Italy; 2Mauriziano Hospital, Cardiology, Torino, Italy; 3SS.Annunziata Hospital, Cardiology, Savigliano, Italy
Purpose: To evaluate the presence and degree of spontaneous echo contrast (SEC) inthe left atrium and of left atrial appendage (LAA) contractility before and after CV in patientswith recent-onset AF.Methods: We studied 57 patients. Group 1 consisted of 33 clinically stable patients(without hemodynamic instability, chest pain consistent with angina, NYHA4 congestiveheart failure, diabetes, active medical problems requiring urgent evaluation) presentedto the Emergency Department with recent-onset AF (,48 hours duration). They under-went transesophageal echocardiography (TEE) guided CV. Control group (group 2) con-sisted of 24 patients admitted to the Cardiological Department for elective TEE guided CVof longer duration (.2 days) AF. All patients repeated TEE within 1 hour after successfulCV. Patients characteristics are listed in the table.Results: Patients with recent-onset AF (group 1) showed no thrombogenic milieu at base-line without any evidence of atrial stunning after successful CV. SEC mean grade (0-3grading) was 0.09+0.3 vs 0.12+0.4 after CV (p = 0.98) and LAA outflow velocity was60.7+19.4 vs56.7+20.5cm/sec after CV(p=0.07).Group 2patientsshowed significant-ly higher degree of SEC compared to group 1 (0.09+0.3 vs 0.66+0.7, p =0.0093) andsignificantly lowerLAA flowvelocities (60.7+19.4vs32.5+12.4, p,0.0001),with a signifi-cant worsening after successful CV (SEC degree 0.66+0.9 vs 1.37+0.9, p=0.0093; LAAoutflow velocity 32.5+12.4 vs 20.4+12.7 cm/sec, p,0.0001).Conclusions: The absence of thrombogenic milieu and of left atrial stunning after CV inpatients with recent-onset AF favours early CV without anticoagulation, at least in patientswith low thromboembolic risk profile. These patients could be soon discharged from theurgent centre.
Abstract P1063 Table.
Total (n=57) Group1(n=33)
Group2(n=24)
p value
Age (years) 63.4+11.8 60.3+12.3 67.5+10 0.018Male sex 38 (67%) 23 (70%) 15 (62%) NSAtrial Fibrillation duration (days) 10.5+20.3 1.4 22.8 ,0.0001CHADsVASc score 2.3+1.4 1.9+1.24 2.8+1.5 0.016Electrical Cardioversion 21 (37%) 4 (12%) 17 (71%) ,0.0001Left Ventricular ejection fraction (%) 55.8+9.0 56.8+7.3 54.6+11.1 NS
P1064Cardiac tumors: the significance of contrast enhancement using the technique ofbolus injection of contrast
C. Evdoridis; D. Papasaikas; E. Sergi; D. Papadimitriou; P. Tolios; G. Papagiannis;V. Tzamou; A. TrikasElpis General Hospital, Athens, Greece
Contrast hyperenhancement of cardiac tumors using the technique of continuous injec-tion of contrast, suggests a highly vascular or malignant tumor. Conversely, benigntumors have usually a poor blood supply and appear hypoenhanced.Methods: We used the technique of bolus injection of contrast (visual assessment, four-chamber view) to study 5 malignant and 4 benign cardiac tumors.Results: Our study showed as expected hyperenhancement of malignant tumors com-pared to the surrounding myocardium (Myocardial contrast enhancement-MCE-) whilebenign tumors showed hypoenhancement. Mass contrast enhancement –MaCE- inthe case of malignant tumors persisted several minutes after the disappearance ofMCE (Figure 1, panels 1-3). On the contrary in the case of benign tumors, MaCE disap-peared before MCE.Conclusion: With the bolus injection of contrast there is a transit time of tissue contrastenhancement which is proportional to tissue vascularity (blood volume-BV-) and inverselyproportional to blood flow –BF- (Figure 2). As a consequence, highly vascular tumors asopposed to tumors with poor blood supply display persistence of contrast enhancement.This help in the differential diagnosis between malignant and other tumors of the heart.
STRESS ECHOCARDIOGRAPHY
P1065End-systolic volume and end-diastolic volume reserve predict cardiac events inpatients with negative stress echocardiography
MC. Scali1; T. Bombardini1; E. Picano2
1University Hospital of Pisa, Cardio-Thoracic Department, Pisa, Italy; 2Institute of ClinicalPhysiology, CNR, Pisa, Italy
Background: The potentially prognostically relevant information on left ventricular end-diastolic volume (LVEDV) and left ventricular end-systolic volume (LVESV) changes inpatients with negative SE for heart-failure-related events is unsettled. Aim of this studywas to assess the prognostic value of stress-induced variation in LVEDV and LVESVchanges in patients with negative SE.Methods: We enrolled 890 patients (593 males, age 63+12 years, ejection fraction 47+12 %), with negative (exercise 172, dipyridamole 481, and dobutamine 237) SE result.Cardiac index (CI) was evaluated at rest and peak stress from raw measurement ofheart rate by EKG, LVEDV and LVESV by biplane Simpson rule from 2D-echo. Changesfrom rest to peak stress (reserve) were tested as predictors of combined death andheart failure hospitalization.Results: For the overall population, CI increased from 2.05 to 3.33 L/min/m2. At peakstress, 181 patients decreased the LVESV and increased the LVEDV (Group I) with ahigher CI increase (+1.89 L/min/m2 vs. rest); 573 patients decreased the LVESV andthe LVEDV (Group II, increased systolic function and decreased relaxation; CI +1.17 L/min/m2 vs.rest); 136 patients increased the LVESV during stress (Group III, decreasedsystolic function and decreased relaxation; CI +0.90 L/min/m2); p,0.05 betweenGroups (Figure). During a median follow-up of 19 months (interquartile range 8-36), 50deaths and 84 hospitalization occurred. The overall event-free survival for the Group I sub-jects was 89%, compared with 86% (Group II) and 76% (Group III) patients, p,0.02.Conclusion: Patients with negative stress echocardiography may experience an adverseoutcome, which can be identified by assessment of systolic function reserve and diastolicrelaxation reserve during SE.
P1066Pressure-volume relationship in the stress-echo lab:does (left ventricularend-diastolic) size matter?
MC. Scali1; T. Bombardini1; S. Salvadori2; MF. Costantino3; E. Picano2
1University Hospital of Pisa, Cardio-Thoracic Department, Pisa, Italy; 2Institute of ClinicalPhysiology, CNR, Pisa, Italy; 3Hospital of Potenza, Cardiology Department, Potenza, Italy
Background: The DESPVR is calculated as the variation between rest and peak stressEnd-Systolic Pressure-Volume Relation (ESPVR). DESPVR is an afterload independentindex of left ventricular (LV) contractility which allows a more accurate prognostic stratifi-cation than ejection fraction in patients without inducible wall motion abnormalities.Whether and to what extent it depends upon LV end-diastolic volume (EDV) remainsunclear.Aim: To assess the dependence of ESPVR upon LVEDV during physical or pharmaco-logical stress in patients with negative stress echo (SE) and all ranges of resting LVfunction.
Abstract P1064 Figure.
Abstract P1065 Figure.
ii174 Abstracts
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

Methods: We analyzed interpretable data obtained in 891 patients, (593 men, age 63+12 years) with ejection fraction 47+12%: 338 normal or near-normal or hypertensive; 229were coronary artery disease; 324 were ischemic or non-ischemic dilated cardiomyop-athy. They were studied with SE during exercise (n=172), dipyridamole (n=482) or dobu-tamine(n=237). TheESPVRwasevaluatedat restandpeak stress fromraw measurementof systolic arterial pressure by cuff sphygmomanometer and EDV and ESV by biplaneSimpson rule from 2D-echo.Results: In the overall population, the relationship between ESPVR and LVEDV waspresent at rest (r2=0.5, p=0.00; Fig. left panel) and peak stress (r2=0.4, p=0.00; Fig.middle panel), but absent if only the DESPVR (Delta rest-stress ESPVR) was considered(r2=0.1, p=ns; Fig. right panel). The DESPVR value was highest for normals or near-normals and hypertensive, and lowest for ischemic or non-ischemic dilated cardiomyop-athy patients.Conclusion: LV end-diastolic volume does not affect the rest-stress changes in ESPVR ineither normal or abnormal left ventricles, during physical or pharmacological stress. TheDESPVR is independent from EDV.
P1067Blunted stress upregulation of stroke volume index is related to impairedend-diastolic volume recruitment
MC. Scali1; T. Bombardini1; S. Salvadori2; E. Picano2
1University Hospital of Pisa, Cardio-Thoracic Department, Pisa, Italy; 2Institute of ClinicalPhysiology, CNR, Pisa, Italy
Background: In the normal heart, when exercise is performed, left ventricular (LV) end-diastolic volume increases slightly, whereas end-systolic volume (ESV) decreases signifi-cantly. Little is known of end-diastolic volume (EDV) recruitment during exercise, dipyrid-amole and dobutamine stress echo (SE).Aim: Toassess thedependence of strokevolume(SV)uponLVEDVchangesduring physicalor pharmacological stress in patients with negative SE and all ranges of resting LV function.Methods: We analyzed interpretable data obtained in 891 patients: 593 men; age 63+12years, ejection fraction 47+12% (338 normal or hypertensive; 229 coronary arterydisease; 324 dilated cardiomyopathy).Patients underwent SE during exercise (n=172), dipyridamole (n=482) or dobutamine(n=237). By selection, all patients had negative SE by wall motion criteria. Strokevolume was evaluated at rest and peak stress from raw measurement of LV EDV andESV by biplane Simpson rule, 2D-echo.Results: For the overall population, SV index increased from 29+10 to 32+11 mL/m2. Asignificant positive linear relationship between SV changes and EDV changes (R=0.63,p=0.00; Fig. Left panel) but not with ESV changes (R=0.24, p=ns; Fig. Middle panel)was present. The SV recruitment was maximal in patients with ESV decrease and EDV in-crease at peak stress (Fig. Right panel -B). Conversely, the worst hemodynamic responsewas an ESV increase with an EDV decrease during stress (Fig. Right panel -A).Conclusion: LV EDV affects the rest-stress changes in SV in both normal and abnormalleft ventricles, during either physical or pharmacological stress. An increase in EDV po-tently contributes to the frequency-dependent upregulation of cardiac output during SE.
P1068Study of right ventricular to pulmonary circulation uncoupling at peak exercise inheart failure by gas exchange analysis combined to echocardiography
G. Generati; F. Bandera; M. Pellegrino; V. Labate; F. Carbone; E. Alfonzetti; M. GuazziIRCCS, Policlinico San Donato, Heart Failure Unit, San Donato Milanese, Italy
Background: Right ventricular (RV) dysfunction and pulmonary hypertension (PH)impact on clinical status and have a prognostic value in heart (HF) patients. There is inter-est in assessment the RV to pulmonary circulation (PC) uncoupling during exerciseeven though much needs to be defined on the functional phenotypes. Aim: todefine how the degrees of RV-PC uncoupling may engender specific functional pheno-types. Methods: 94 HFrEF patients (mean age 66+11 y, male 70%, ischemic etiology71%, mean LVEF 34+9%) underwent a maximal CPET (incremental ramp protocol)combined with exercise-echo. Results: Population was divided into 4 groups usingthe 4 quadrant approach (Figure) based on TAPSE vs systolic PAP (PASP) relationshipas a length vs developed force of the RV during exercise (cutoff based on medianvalues of 20 mm and 57 mmHg). At peak exercise patients with more favorableTAPSE vs PASP relationship (group A) showed the better functional CPET response
(higher peak VO2; lower VE/VCO2 slope and prevalence of exercise oscillatory venti-lation (EOV), p= 0.000, 0.005 and 0.000). Group B and C showed similar peak VO2and the occurrence of dynamic PH (group C) was related to dynamic mitral regurgita-tion (MR) and high rate of EOV (B vs C p=0.001 and 0.000). Interestingly, for similarexercise tolerance and LV function parameters, group D patients had more severelyimpaired ventilatory efficiency associated with very high prevalence of rest severe(MR) and EOV (p=0.005, 0.002). Conclusions: This proposed non-invasive RV func-tional evaluation approach at peak exercise seems appealing for stageing HF syn-drome severity based on the degree of the right heart dysfunction. It appears alsouseful to unmask different ventilatory phenotypes irrespective of a similar impairmentin functional capacity and peak VO2.
P1069Assessment of ventricular-vascular coupling during exercise in hypertensivepatients
L. Rivetti; M. Cusma Piccione; C. Zito; M. D’angelo; R. Manganaro; F. Pizzino; A. Terrizzi;S. Quattrocchi; A. Ioppolo; S. CarerjUniversity of Messina, Department of Cardiology, Messina, Italy
Background: The ability of the heart to adequately respond to the increase of metabolicdemandduringexertion reliesonseveral adaptivechanges leading toaugmentedcardiacoutput without any rise of filling pressures. The impairment of these compensatorymechanisms, as found in various heart diseases including systemic hypertension, cantranslate to reduced functional capacity. In this study, we sought to investigate the cardio-vascularadaptation to exertion in acohort ofasymptomatic hypertensive patients,with theaim to identify early cardiac abnormalities.Methods: We enrolled 54 subjects including 30 patients (45.1+11.9 years, 19 males)and 24 age-matched healthy controls (44.4+9.6 years, 14 males). A comprehensiveechocardiographic and vascular evaluation, implemented by speckle-tracking imaging(STI) and echo-tracking analysis to assess, respectively, myocardial deformation and ar-terial stiffness, has been performed at rest and during exertion.Results There was a greater increase of E/E’ from rest to peak exercise in patients thanin controls (p = 0.014 and p = 0.087, respectively). Global longitudinal strain (GLS) ofthe left ventricle (LV) significantly increased from rest to peak stage in healthy subjects(p=0.011) whereas it remained unchanged in hypertensive patients (p = 0.777). In add-ition, LV untwist increased in both groups (p = 0.031 and 0.015 in patients and controls,respectively), with a minor increase in patients than in controls (p = 0.029 betweengroups, at peak stage). Left atrial (LA) reservoir was significantly increased, throughoutthe exercise, only in controls (p = 0.001) whereas it was almost unchanged in patients(p = 0.293. LA stiffness, calculated as the ratio between E/E’ and LA reservoir, was sig-nificantly higher in patients than in controls both at rest (p=0.023) and during exercise(p , 0.001). Concerning vascular parameters, beta index and pulse wave velocity(PWV) by echo-tracking, increased during exercise in both groups, showinghigher values in hypertensive patients in each step (p = 0.658 for beta index and p =0.010 for PWV at peak stage; p = 0.004 for beta index and p , 0.001 for PWV duringrecovery.Conclusions: Exercise echocardiography implemented by STE and echo-tracking maybe valuable in the early detection of cardiovascular abnormalities in asymptomatic hyper-tensive patients.
Abstract P1066 Figure. LVEDV does not affect ESPVR changes
Abstract P1067 Figure. Stroke volume, LVEDV and LVESV changes
Abstract P1068 Figure.
Abstracts ii175
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

P1070Long term prognostic value of negative stress electrocardiography and stressechocardiography in patients with pretest probability for coronary artery diseaseof 15-65%
V. Giga; N. Boskovic; J. Stepanovic; B. Beleslin; I. Nedeljkovic; M. Dobric;A. Djordjevic-DikicInstitute for cardiovascular diseases, Clinical Center of Serbia, Belgrade, Serbia
Background: Current guidelines recommend the use of stress with addition of imaging aspreferable for the detection of coronary artery disease. However, stress electrocardiog-raphy could be used in patients with pretest probability for coronary artery disease(CAD) of 15-65%.The aim of our study was to compare long term prognostic value of negative stress elec-trocardiography (SECG) and stress echocardiography (SECHO) in patients with chestpain and pretest probability of CAD of 15-65%.Methods: We included in the study 676 patients (58+10 years, 56% females, 13% withdiabetes) without known CAD and pretest probability of 15-65% who were referred to ex-ercise testing for the evaluation of chest pain. All the patients had interpretable ECG. Themodality of test (SECG or SECHO) was used according to the decision of referring phys-ician. Patients were followed for mean of 94+2 months for the occurrence of cardiovas-cular death, myocardial infarction and clinically indicated revascularization.Results: Out of 676 patiens 57 patients (8.4%) had positive test and were excluded fromfurther analysis. Of the remaining 619 patients with negative finding, 418 (67%) underwentSECG, whreas 201 patients (33%) underwent SECHO. There was no difference in base-line characteristics between the groups. During the follow up period 42 patients (6.7%)had an adverse event (6 deaths, 11 myocardial infarction, 25 clinically indicated revascu-larization). There was no difference in events between groups (27/418, 6.4%) in SECG and(15/201, 7.5%) in SECHO group (p=NS). Multivariate predictors of adverse events werepresence of diabetes and male gender (p,0.0001, for both).Conclusion: Patients with pretest probability for CAD of 15-65% and negative exercisetesting have excellent long term prognosis irrespective of the modality of test (stress elec-trocardiography or stress echocardiography) used for the detection of myocardial ische-mia. Male patients and patients with diabetes have more pronounced risk for theoccurrence of adverse events.
P1071Comparisonof cardiopulmonary exercise testing and stress echocardiography inprediction and quantification of coronary artery disease
D. Popovic1; I. Petrovic1; M. Banovic1; R. Lasica1; V. Pesic2; B. Plecas - Solarovic2;D. Vidojevic2; T. Djordjevic2; M. Orovic2; B. Vujisic - Tesic2
1Clinical Center of Serbia, Clinic for Cardiology, Belgrade, Serbia; 2University of Belgrade,Faculty of Pharmacy, Belgrade, Serbia
Cardiopulmonary exercise test (CPET) on upright bicycle is superior to ECG-exercise testin detection of myocardial ishaemia. The aim of this study was to examine the utility ofCPET recumbent bicycle in relation to stress echocardiography testing in prediction ofcoronary artery disease severity. We studied 30 Caucasian males, mean age 63.10+8.55, with significant lesions of coronary arteries (≥50%), quantified by Syntax score.CPETwas performed within two months of coronary angiography. The protocol involvedramp-pattern increase in work rate (WR). Tests were symptom limited, or were stoppedwhen ≥2 mm ST depression occurred in at least two adjacent leads. Myocardial wallmotion was recorded by echocardiography at rest and maximal phase of the test, andreported using conventional 16-segment model. The ishaemia was quantified by wallmotion score index (WMSI). Basal spirometric parameters were normal. Mean ejectionfraction was 59.3+7.63%. Examiners exhibited mean 1.56+0.88 number of stenoticcoronary arteries (NSCA) and Syntax score 10.39+7.56. PeakWMSI was 1.18+0.1,and DWMSI peak/rest 0.12+0.07. Following CPET data were obtained: peak oxygenuptake (peakVO2; 1.21+0.23 ml/min/kg), peak minute ventilation (peakVE; 37.35+13.14 ml/min), peak O2pulse (11.36+2.61 ml) and DVO2/DHR (20.03+9.47 l), VE/VCO2 slope (28.99+3.11) and end-tidal pressures of O2 (PETO2) and CO2 (PETCO2)in all phases. Our results revealed significant correlations of peakWMSI; DWMSI peak/rest; peakVE; peak and rest PETCO2 and PETO2; as well as the change of HR,O2pulse and VO2 in recovery with Syntax score (p,0.01). The best independent predict-or of Syntax score was peakPETCO2 (R2=0.86, r=0.93, p,0.0001). NSCA correlatedwith restWMSI; DWMSI peak/rest; peakVO2; O2pulse and PETO2 et peak exercise andin recovery; the change of VO2 and O2pulse in recovery; and VE/VCO2slope (p,0.01).The best predictor of NSCA was peak O2pulse (R2=0.86, r=0.93, p,0.0001). Our datasuggest that CPET parameters have better predictive value for coronary artery diseasequantification scores then WMSI.
P1072Use of Tissue Synchronization Imaging (TSI) in stressed patients after coronaryrevascularization
V. Bordonaro; S. Buccheri; VE. Bottari; C. Romano; FA. Atanasio; C. Tamburino; I P. MonteUniversity of Catania, Catania, Italy
Tissue Synchronization Imaging (TSI) is a new and non-invasive imaging technique,applied to which can automatically measure time to peak of myocardial left ventricle(LV) velocities, applied to identify regional wall delay and reverse remodelling after resyn-chronization therapy. Recent advances have been confirmed the relationship betweenasynchronous motion of ischemic segments and LV function in patients with coronaryartery disease (CAD).
Aim of the study was investigated the application of the TSI to the exercise stress echocar-diography (ESE) in patients with revascularized CAD.Between April 2012 and July 2014, all consecutive subjects were enrolled. We selected for theCADGroup30patientspreviously treatedwithPTCA,andfortheNormalGroup20healthysub-jects with no history of ischemic heart disease, matched for anthropometric characteristics.ESE was conducted using a semi-supine bicycle ergometer with 25 W incrementalloading every 3 minutes. ECG and blood pressure were monitored at resting and eachminute throughout the stress. ECHO examination was made before, during, at the peakof exercise and after 5 min of recovery, using Vivid 7 ultrasound system, equipped withprobe matrix for multiplane acquisitions. The ECHO protocol included biplane acquisi-tions (parasternal long-axis and short-axis views) and triplane acquisitions (apical 4, 3and 2 chamber views). All views were evaluated at baseline and peak stress.At baseline, compared with the Normal, CAD had significantly higher LV dimension (LVIDdp=0.024 e LVIDs p=0.001), higher A velocity (p,0.001) and lower E/A ratio (p,0.001) oftransmitral flow, lower E’ and A’ (p,0.001 and 0.024 respectively) of mitral annular tissuevelocities, and increased E/E’ ratio (p=0.001).At peak CAD had significantly lower values of E (p=0.001), E/A (p=0.004), S’ (p,0.001) eE’ (p,0.001) and a lower increase of E (p=0.005), A (p=0.006), S’ (p,0.001) and E’(p=0.006) velocities compared to Normal.TSI analysis showed that the CAD group had a significantly increased LV dyssynchrony, atbaseline and at peak (p,0.01 for each parameter). However, the rest-peak variations didnot showed significant differences. The most delayed segment corresponded to therevascularized areas in 63% of patients. The maximum activation delay showed a signifi-cant correlation negative with the LVEF (r=0.217, p=0.031) and the S’ (r=-0.393,p,0.001) and positive with the E/E’ratio (r=0.376, p,0.001)TSI is non-invasive method for assessing regional myocardial disease and provides avisual detection of abnormal myocardial motion.
P1073Automated left ventricular function during stress echocardiography
F. Korchi1; A. Kassongo1; P. Meimoun2; D. De Zuttere3; HERVE. Lardoux1
1Institut Mutualiste Montsouris, Paris, France; 2University Hospital of Compiegne,Compiegne, France; 3Institut Franco Britannique, LEVALLOIS PERRET, France
Background: Diagnostic accuracy of Stress Echocardiography (SE) is limited by the sub-jectivity of visual assessment of regional contractile left ventricular function (LVEF). Thus,methods increasing observer agreement and providing quantitative analysis of globaland segmental LVEF systolic function should be a significant improvement for SE analysisMethods: Over a 4 month period, all patients underwent SE (Dobutamine DOB or Exer-cise EX) using a VIVID 9 2D probe (without contrast agent), were prospectively included.A systematic record of 3 apical views, at baseline (BAS), peak (PK) and early recovery(REC) ,110/mn, was performed. We evaluate during (SE) the feasibility of automatedLVEF at all levels and of global longitudinal strain (GLS) at BAS and REC. Patients wereexcluded if GLS analysis was not accurate foranalysis of two consecutive segments, inany apical view.Results: 94 patients were prospectively studied: 17 patients (7.5%) were excludedbecause of poor image quality. Finally, 77 patients, 68.15(9.15) years– 39 male and 38female met all criteria.Among 40EX (51.9%)and 37DOB, SEwas negative (n=67),positive(n= 6) and doubtful (n=4).. Intra and inter observer agreement was assessed among 18randomly patients: , 5% (LVEF and SE); for intra; 5.7% (LVEF) and 7% (SE) for inter obser-ver agreement. Results are presented as M (SD) at respectively BAS, PK and REC steps:Heart rate (Bpm): 73,8(14,3), 141(12,6)*¥; 96,8(20,4). LVEF(%)58,34(7,7); 61,9(8)*¥;59,(7,5). LVEF End Systolic Volume (ml) 77,8(23,4); 75,7(22) * ¥;78,6(21,6). GLS %:-19.4(3,6)BAS; -19,5(3,7) REC ns – (* p , 0.05 vs. baseline; ¥ p , 0.05 vs. recovery)Conclusions: Despite image quality limitations, automated left ventricular function isfeasible during SE, in most patients, at all stages. GLS is also feasible at rest and recovery.Both methods should be considered as a first step towards a quantitative assessment ofLEVF during SE.
CONTRAST ECHOCARDIOGRAPHY
P1074Simultaneous assessment of myocardial perfusion, wall motion and deformationduring myocardial contrast echocardiography. A feasibility study
G. Zoppellaro; L. Venneri; RS. Khattar; W. Li; R. SeniorRoyal Brompton Hospital, Department of Echocardiography, London, United Kingdom
Purpose: Ultrasound contrast agents may be used for the assessment of regional wallmotion and myocardial perfusion, but is generally considered not suitable for deformationanalysis. The aim of our study was to assess the feasibility of deformation imaging oncontrast-enhanced images using a novel methodology.Methods: We prospectively enrolled 40 patients who underwent stress echocardiog-raphy with continuous intravenous infusion of Sonovue contrast agent for the assessmentof myocardial perfusion imaging with flash-replenishment technique. We compared lon-gitudinal strain (Le) values, assessed with a vendor-independent software on 68 restingcontrast-enhanced and 68 resting non-contrast recordings. Strain analysis on contrastrecordings was evaluated in the first cardiac cycles after the flash.Results: Tracking of contrast images was deemed feasible in all subjects and in all views.Contrast administration improved image quality and increased the number of segmentsused for deformation analysis. Le of non-contrast and contrast-enhanced images werestatistically different (-18.8+4.5% and -22.8+5.4%, respectively; p,0.001) but their
ii176 Abstracts
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022
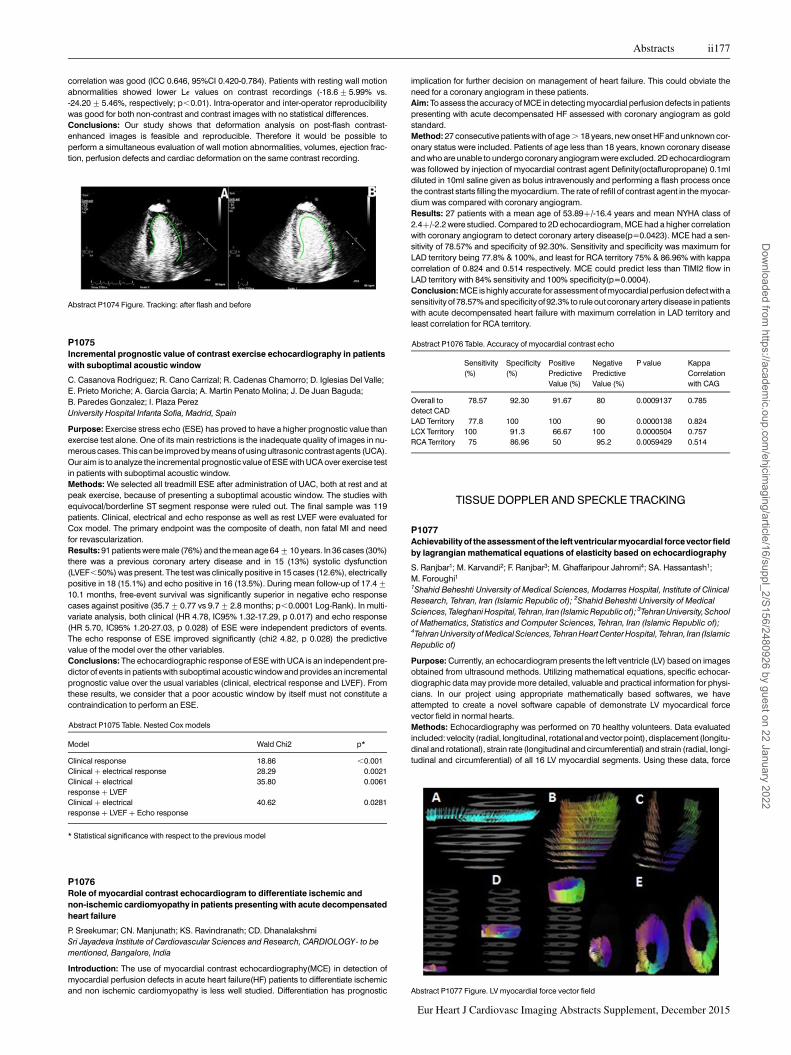
correlation was good (ICC 0.646, 95%CI 0.420-0.784). Patients with resting wall motionabnormalities showed lower Le values on contrast recordings (-18.6+5.99% vs.-24.20+5.46%, respectively; p,0.01). Intra-operator and inter-operator reproducibilitywas good for both non-contrast and contrast images with no statistical differences.Conclusions: Our study shows that deformation analysis on post-flash contrast-enhanced images is feasible and reproducible. Therefore it would be possible toperform a simultaneous evaluation of wall motion abnormalities, volumes, ejection frac-tion, perfusion defects and cardiac deformation on the same contrast recording.
P1075Incremental prognostic value of contrast exercise echocardiography in patientswith suboptimal acoustic window
C. Casanova Rodriguez; R. Cano Carrizal; R. Cadenas Chamorro; D. Iglesias Del Valle;E. Prieto Moriche; A. Garcia Garcia; A. Martin Penato Molina; J. De Juan Baguda;B. Paredes Gonzalez; I. Plaza PerezUniversity Hospital Infanta Sofia, Madrid, Spain
Purpose: Exercise stress echo (ESE) has proved to have a higher prognostic value thanexercise test alone. One of its main restrictions is the inadequate quality of images in nu-merous cases. This can be improved by means of using ultrasonic contrast agents (UCA).Our aim is to analyze the incremental prognostic value of ESE with UCA over exercise testin patients with suboptimal acoustic window.Methods: We selected all treadmill ESE after administration of UAC, both at rest and atpeak exercise, because of presenting a suboptimal acoustic window. The studies withequivocal/borderline ST segment response were ruled out. The final sample was 119patients. Clinical, electrical and echo response as well as rest LVEF were evaluated forCox model. The primary endpoint was the composite of death, non fatal MI and needfor revascularization.Results: 91 patients were male (76%) and the mean age 64+10 years. In 36 cases (30%)there was a previous coronary artery disease and in 15 (13%) systolic dysfunction(LVEF,50%) was present. The test was clinically positive in 15 cases (12.6%), electricallypositive in 18 (15.1%) and echo positive in 16 (13.5%). During mean follow-up of 17.4+10.1 months, free-event survival was significantly superior in negative echo responsecases against positive (35.7+0.77 vs 9.7+2.8 months; p,0.0001 Log-Rank). In multi-variate analysis, both clinical (HR 4.78, IC95% 1.32-17.29, p 0.017) and echo response(HR 5.70, IC95% 1.20-27.03, p 0.028) of ESE were independent predictors of events.The echo response of ESE improved significantly (chi2 4.82, p 0.028) the predictivevalue of the model over the other variables.Conclusions: The echocardiographic response of ESE with UCA is an independent pre-dictor of events in patients with suboptimal acoustic window and provides an incrementalprognostic value over the usual variables (clinical, electrical response and LVEF). Fromthese results, we consider that a poor acoustic window by itself must not constitute acontraindication to perform an ESE.
Abstract P1075 Table. Nested Cox models
Model Wald Chi2 p*
Clinical response 18.86 ,0.001Clinical + electrical response 28.29 0.0021Clinical + electricalresponse + LVEF
35.80 0.0061
Clinical + electricalresponse + LVEF + Echo response
40.62 0.0281
* Statistical significance with respect to the previous model
P1076Role of myocardial contrast echocardiogram to differentiate ischemic andnon-ischemic cardiomyopathy in patients presenting with acute decompensatedheart failure
P. Sreekumar; CN. Manjunath; KS. Ravindranath; CD. DhanalakshmiSri Jayadeva Institute of Cardiovascular Sciences and Research, CARDIOLOGY- to bementioned, Bangalore, India
Introduction: The use of myocardial contrast echocardiography(MCE) in detection ofmyocardial perfusion defects in acute heart failure(HF) patients to differentiate ischemicand non ischemic cardiomyopathy is less well studied. Differentiation has prognostic
implication for further decision on management of heart failure. This could obviate theneed for a coronary angiogram in these patients.Aim: To assess the accuracy of MCE in detecting myocardial perfusion defects in patientspresenting with acute decompensated HF assessed with coronary angiogram as goldstandard.Method: 27 consecutive patients with of age . 18 years, new onset HF and unknown cor-onary status were included. Patients of age less than 18 years, known coronary diseaseand who are unable to undergo coronary angiogram were excluded. 2D echocardiogramwas followed by injection of myocardial contrast agent Definity(octafluropropane) 0.1mldiluted in 10ml saline given as bolus intravenously and performing a flash process oncethe contrast starts filling the myocardium. The rate of refill of contrast agent in the myocar-dium was compared with coronary angiogram.Results: 27 patients with a mean age of 53.89+/-16.4 years and mean NYHA class of2.4+/-2.2 were studied. Compared to 2D echocardiogram, MCE had a higher correlationwith coronary angiogram to detect coronary artery disease(p=0.0423). MCE had a sen-sitivity of 78.57% and specificity of 92.30%. Sensitivity and specificity was maximum forLAD territory being 77.8% & 100%, and least for RCA territory 75% & 86.96% with kappacorrelation of 0.824 and 0.514 respectively. MCE could predict less than TIMI2 flow inLAD territory with 84% sensitivity and 100% specificity(p=0.0004).Conclusion: MCE is highly accurate for assessment of myocardial perfusion defect with asensitivity of 78.57% and specificity of 92.3% to rule out coronary artery disease in patientswith acute decompensated heart failure with maximum correlation in LAD territory andleast correlation for RCA territory.
Abstract P1076 Table. Accuracy of myocardial contrast echo
Sensitivity(%)
Specificity(%)
PositivePredictiveValue (%)
NegativePredictiveValue (%)
P value KappaCorrelationwith CAG
Overall todetect CAD
78.57 92.30 91.67 80 0.0009137 0.785
LAD Territory 77.8 100 100 90 0.0000138 0.824LCX Territory 100 91.3 66.67 100 0.0000504 0.757RCA Territory 75 86.96 50 95.2 0.0059429 0.514
TISSUE DOPPLER AND SPECKLE TRACKING
P1077Achievability of the assessmentof the left ventricularmyocardial force vector fieldby lagrangian mathematical equations of elasticity based on echocardiography
S. Ranjbar1; M. Karvandi2; F. Ranjbar3; M. Ghaffaripour Jahromi4; SA. Hassantash1;M. Foroughi11Shahid Beheshti University of Medical Sciences, Modarres Hospital, Institute of ClinicalResearch, Tehran, Iran (Islamic Republic of); 2Shahid Beheshti University of MedicalSciences,TaleghaniHospital, Tehran, Iran (Islamic Republicof); 3TehranUniversity,Schoolof Mathematics, Statistics and Computer Sciences, Tehran, Iran (Islamic Republic of);4Tehran University of Medical Sciences, Tehran Heart Center Hospital, Tehran, Iran (IslamicRepublic of)
Purpose: Currently, an echocardiogram presents the left ventricle (LV) based on imagesobtained from ultrasound methods. Utilizing mathematical equations, specific echocar-diographic data may provide more detailed, valuable and practical information for physi-cians. In our project using appropriate mathematically based softwares, we haveattempted to create a novel software capable of demonstrate LV myocardical forcevector field in normal hearts.Methods: Echocardiography was performed on 70 healthy volunteers. Data evaluatedincluded: velocity (radial, longitudinal, rotational and vector point), displacement (longitu-dinal and rotational), strain rate (longitudinal and circumferential) and strain (radial, longi-tudinal and circumferential) of all 16 LV myocardial segments. Using these data, force
Abstract P1074 Figure. Tracking: after flash and before
Abstract P1077 Figure. LV myocardial force vector field
Abstracts ii177
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

vectors of myocardial samples were estimated by MATLAB software, interfaced in theechocardiograph system.Results: LV Myocardial force vector field is rendered in MATLAB software by the followingsteps: 10 short-axis slices are shown at the end systole. For 1 slice, the force vector fieldfrom end diastole to end systole was shown by red arrows (Figure A). Color-codedforce vector field illustration of all 10 slices (Figure B). Force vector field on a long-axisview was depicted here (Figure C). The force vector field for 3 slices during the contractionspanning from end diastole to end systole (Figure D). The force vector field for 3 slicesduring the contraction spanning from end diastole to end systole (Figure E).Conclusion: We were able to define the whole LV myocardial force vector field mathem-atically, for the first time, by MATLAB software in normal subjects. This will enable physi-cians to diagnose and follow-up many cardiac diseases.
P1078Trastuzumab cardiomyopathy is prevented by the administration of Ranolazine atthe end of antineoplastic treatment: in vitro and echocardiographic study
N. Maurea1; C. Coppola1; G. Piscopo1; F. Galletta1; C. Maurea1; E. Esposito2; A. Barbieri3;G. Riccio4; M. De Laurentiis5; C. De Lorenzo4
1Istituto Nazionale per loStudio e la Curadei Tumori Fondazione Giovanni Pascale - IRCCS,Division of Cardiology, Naples, Italy; 2stituto Nazionale per lo Studio e la Cura dei TumoriFondazione Giovanni Pascale - IRCCS, Department of Breast Surgery and CancerPrevention, Naples, Italy; 3Istituto Nazionale per lo Studio e la Cura dei Tumori FondazioneGiovanni Pascale - IRCCS, Animal Facility, Naples, Italy; 4University ‘Federico II’,Department of Molecular Medicine and Medical Biotechnology, Naples, Italy; 5IstitutoNazionale per lo Studio e la Cura dei Tumori Fondazione Giovanni Pascale - IRCCS, BreastOncology Unit, Naples, Italy
Purpose: The anti-cancer anti-ErbB2 Trastuzumab (T) is used to treat HER2 positivebreast cancer, but can produce cardiac dysfunction. The mechanisms of such cardiotoxi-city have not been elucidated, but oxidative stress may play an important role. The late INainhibitor Ranolazine (R) protects from doxorubicin-induced oxidative stress and cardiacdysfunction as we have demonstrated. We aim at assessing whether R, administeredafter T treatment, reduces Tcardiotoxicity in vivo and in vitro.Methods: In vitro, rat H9C2 cardiomyoblasts and human fetal cardiomyocytes weretreated with T for 3 days and then treated in the absence or presence of R for 3 days.Cell viability was determined by cell counts and MTTassays. In vivo, fractional shortening(FS) and ejection fraction (EF) were measured by M-mode echocardiography and radialand longitudinal strain (RS and LS) were measured using 2D speckle-tracking, in C57/BL6mice, at 0, 2 and after 7 days of daily administration of T. These measurements wererepeated after 5 days of R treatment initiated at the end of T treatment. We have dividedmice in 4 groups. The first group (G1) was treated with T for 7 days. The second group(G2) was treated with T for 7 days and then treated with R for 5 days. The other 2 werecontrol groups: CG1 (sham) and CG2 (no R). We have evaluated tissue expression ofBNP (brain natriuretic peptide) by PCR analysis on heart tissue. Moreover, apoptoticpathway was assessed by western blotting, in lysates from murine hearts.Results: R reduced T toxicity in H9C2 cardiomyoblasts and human fetal cardiomyocytesas evidenced by higher percentage of viable cells treated with T+ R with respect to cellstreated with Talone (p,0.01). In vivo, after 7 days with T, FS decreased to 48.7+4.1%,p,0.01 vs 62.3+0.8% (sham), EF to 81.8+3.5%, p,0.01 vs 91.7+0.5% (sham), RSto 21+8.1%, p,0.01 vs 43.2+4% (sham), and LS to -11+3.7%, p,0.01 vs -38.8+6% (sham). In mice treated with R for 5 days after T treatment, the indices of cardiac func-tion recovered: FS was 61+1.2%, EF was 91+0.7%, p,0.01; RS was 35+1.8%,p,0.05 vs T. However the alteration of LS persisted after treatment with R (-15.4+5.1%, p=0.3 vs T). R prevents the increased expression of BNP (p,0.05) on hearttissue. In lysates from murine hearts, R reduced apoptosis as evidenced by decreasedlevels of cleaved caspase 3.Conclusions: R post-treatment reduces cardiotoxic effects due to Tas demonstrated invitro by higher percentage of viable cells and in vivo by the normalization of the valuesof FS, EF and RS and by the reduction of apoptosis on heart tissue.
P1079Detection and quantification of shear waves using a clinical cardiac ultrasoundsystem, a phantom study
M. Strachinaru1; N. De Jong2; ML. Geleijnse1; BM. Van Dalen1; HJ. Vos2
1Erasmus Medical Center, Cardiology, Rotterdam, Netherlands; 2Erasmus Medical Center,Biomedical Engineering, Rotterdam, Netherlands
Purpose: The propagation velocity of shear waves relates to stiffness. We aimed to provethat a clinical ultrasound system can effectively track this wave velocity in cardiac mode.Methods: A research scanner (Vantage, Verasonics Inc), with a ATL L7-4 probe, was usedas shear wave inducer through acoustical radiation force into an ultrasound phantom(040GSE, CIRS Inc). An ultrasound push was produced with a 4 MHz frequency, 1.4 mspulse. The expected shear wave velocity is 2.8m/s for this phantom. The shear wavewas detected with the research scanner at 5000Hz frame rate, as reference. Simultan-eously, a clinical scanner (Philips IE33; Philips, Best, The Netherlands), equipped with aS5-1 probe, was set up to detect the same phenomenon, using a clinical tissue Dopplerapplication, at frame rates between 460-645Hz. A manufacturer designed software(Philips Qlab 9) was used to measure the slope of the front wave along an M-mode line.The speed was averaged over 10 acquisitions.Results: The primary shear wave, as well as secondary and reflected waves, were welldetected by both scanners (Figure). The research scanner calculated a speed of 2,5+0,2m/s and the clinical one 2,7+0,2m/s.
Conclusion: Clinical cardiac ultrasound scanners can be used to successfully track andquantify shear waves in an experimental setting.
P1080Functional reverse remodeling of myocardium after coronary artery bypasssurgery
K. Keramida1; N. Kouris2; D. Dawson1; CD. Olympios2; P. Nihoyannopoulos3
1Hammersmith Hospital, London, United Kingdom; 2Thriassio General Hospital, Athens,Greece; 3Imperial College Healthcare NHS Trust, Hammersmith Hospital, London, UnitedKingdom
Myocardial reperfusion by coronary artery bypass graft surgery (CABG) improves prog-nosis and reduces mortality. Traditional echocardiographic indices, such as left ventricu-lar ejection fraction (LVEF), left ventricular dimensions and stroke volume are notimproved in such a way that would justify the outcome of these patients. We hypothesizedthat LV function improves following CABG and 2D speckle tracking echocardiographymay possibly prove it by longitudinal (GLS) and circumferential strain (GCS).This is a pilot study and so far we have included 50 patients (81% male, with mean age64+10 years) with coronary artery disease who successfully underwent CABG.Routine echocardiography and GLS and GCS measurements were performed 1 weekbefore and 1 year after CABG.The baseline echocardiographic study revealed that 47,6% of our patients had regionalwall motion abnormalities (RWMAs) before CABG. After CABG left ventricular dimensionsdecreased, while LVEF and GLS increased but not significantly. On the other hand, GCSdecreased in a statistically significant degree (p=0.014) and multiple regression analysisshowed that the change GCS is correlated strongly with GLS change (t=-2.378,p=0.037), independently of LVEF, LV dimensions, the presence of RWMAs and thenumber of critically stenosed coronary arteries. It is evident that GLS before CABG wasreduced and as a compensatory mechanism GCS was supranormal, while after CABGLVEF and consequently GLS tend to improve, so GCS decreased, proving once againthe established knowledge that longitudinal and circumferential strains are complemen-tary.Strain analysis may provide a new insight in “functional” reverse remodeling of ischemicmyocardium following CABG. The compensatory reduction of GCS in parallel with the in-crease of GLS indicate the overall improvement of LV mechanics after CABG.
Abstract P1080 Table.
Variable Before CABG After CABG p value
LVEF (%) 54.75+13.44 56.90+12.62 0.517LVEDD (mm 47.45+7.01 45.90+5.74 0.123LVESD (mm) 33.66+8.92 31.84+7.02 0.172GLS (%) 217.12+4.71 218.18+4.34 0.271GCS (%) 224.86+6.60 219.53+7.02 0.014
P1081Intraventricular flow to guide optimization of atrio-ventricular delay inresynchronization therapy
D. Rodriguez Munoz; A. Carbonell San Roman; C. Lozano Granero; JL. Moya Mur;C. Fernandez-Golfin; J. Moreno Planas; E. Casas Rojo; S. Fernandez Santos;A. Hernandez-Madrid; JL. Zamorano GomezUniversity Hospital Ramon y Cajal, Department of Cardiology, Madrid, Spain
Introduction: Atrio-ventricular delay (AVD) optimization is commonly guided by trans-mitral Doppler flow. Despite evidence showing its beneficial clinical impact for patientsunder cardiac resynchronization therapy (CRT), its use is rare due to the prolonged exam-inations and experienced staff required. Vector Flow Mapping (VFM) enables visualizationand measurement of full-chamber intracardiac flow, providing inflow and outflow curves inthe same heartbeat.Methods: Patients with CRT in sinus rhythm underwent echo-guided AVD optimizationwith analysis of trans-mitral flow and VFM automatic time-flow curves. AV intervalsranging from 80 to 280 were programmed. Optimal AVD was calculated by the twomethods, selecting the shortest interval without A-wave truncation. Results obtainedwith the two methods were compared using intraclass correlation coefficient (ICC).
Abstract P1079 Figure.
ii178 Abstracts
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

Results: 15 patients (33% male, aged 66.5+10.8, LVEF 41.7+9.3) were studied. ICCshowed excellent concordance between the two techniques (0.94, CI [0.84 – 0.98],p,0.0001). VFM time-flow based measurements showed better inter-observer agree-ment (0.97, CI [0.89 – 0.98], p,0.0001) than trans-mitral flow measurements (0.89, CI[0.74 – 0.95], p,0.001).Conclusions: Atrio-ventricular delayoptimization guided byfull-ventricular flow characteriza-tion is feasible and accurate. The possibility to obtain information on flow behaviour in thewhole ventricle may reduce inter-observer variability and make the process easier and faster.
P1082Speckle tracking to assess the initial improvement of myocardial activity aftercoronary artery bypass grafting
F. D’auria1; R. Leone2; F. Itri2; G. Del Negro2; M. Colombino2; P. Masiello2; A. Longobardi2;F. Rosapepe2; S. Iesu2; G. Di Benedetto2
1University Campus Bio-Medico of Rome, Cardiac Surgery, Rome, Italy; 2AOU S. Giovannie Ruggi, Cardiac Surgery, Salerno, Italy
Purpose: SPAIN IMA study investigates the changes in myocardial function afteroff-pump coronary artery bypass grafting (OPCABG)using longitudinal strain on speckle-tracking imaging (LST).Methods:40patients (12 f-28m), mean(m)age 66y,with cardiovascular major risk factors(40% diabetes type II, 100% hypertension, 70% smoke, 40% BPCO, 64% obesity), LVEF50% or greater, mNYHA II, mCCS 3, mEuroscore II 4.38, mSyntax score 29 (10% previous-ly PCI),were enrolled andunderwent to complete OPCABG.Routine 2D TTEand LSTwereperformed 1 week before OPCABG and 3, and 6 months after OPCABG.Results: 3 and 6 months follow up 100% completed. Longitudinal strain (LS) increased at3 and 6 months after OPCABG (P ,. 05). However, the LVEF, left ventricular end-diastolicdimension, and stroke volume measured by TTE were not significantly changedafter OPCABG treatment during the 6 months of follow-up. Strong correlationbetween coronary lesion in angiography imaging and the corresponding heart zonewith a reduction in global and segmental LS.Conclusion: LST is more effective than LVEF, LVD, and LVV for monitoring improvement inmyocardial function after OPCABG. LST could guide the revascularization strategybecause it correlates with the coronary lesions.
P1083Three-dimensional speckle tracking echocardiographic assessment of rightventricular function in chronic obstructive pulmonary disease with and withoutpulmonary hypertension
L. Capotosto; S. D’orazio; R. Ashurov; G. Continanza; E. Mangieri; C. Terzano; A. VitarelliSapienza University, Rome, Italy
Background: The purpose of this study was to assess right ventricular (RV) function inpatients with chronic obstructive pulmonary disease (COPD) with and without pulmonaryhypertension (PH) using three-dimensional speckle tracking echocardiography (3DSTE)and compare 3DSTE parameters with conventional RV function indexes.
Methods: Thirty-two patients with COPD and thirty-two healthy subjects were studied.Twelve patients had PH confirmed by right heart catheterization (mean pulmonaryartery pressure .25mmHg). Twenty patients had normal pulmonary artery pressures.Standard 2D measurements (tricuspid annulus excursion -TAPSE-, fractional areachange -RVFAC-) and mitral and tricuspid tissue-Doppler annular velocities wereobtained. RV 3D volumes, and RV global and regional ejection fraction (3DRVEF) weredetermined. Peak systolic velocities and strain were measured in the LV and RV free-wallsegments. Respiratory function tests were performed (FEV1/VC = forced expiratoryvolume in one second / vital capacity; DLCO/VA = carbon monoxide diffusion lung cap-acity per unit of alveolar volume).Results: Global free-wall RV longitudinal strain (GFW-RVLS) and 3DRVEF were signifi-cantly lower compared to controls both in patients with PH (p,0.0001 and p=0.0003 re-spectively) and without PH (p,0.001 and p,0.005 respectively). Both GFW-RVLS and3DRVEF correlated similarly with mean pulmonary artery pressure (r=0.62 and r=0.64;p=0.004 for both) and with pulmonary vascular resistance (r=0.65 and r=0.67;p=0.003 for both). No correlation was observed between RV and LV strain parameters.A significant relationship was shown between GFW-RVLS and DLCO/VA (r=0.72,p,0.005), and GFW-RVLS and FEV1/VC (r=0.75, p,0.001).Conclusions: RV 3D and 3DSTE parameters were abnormal in COPD patients comparedto normals and had a higher association with COPD severity compared to standard RVfunction measurements. RV deformation changes did not appear to be a consequenceof LV dysfunction. Detection of RV systolic impairment, even in the absence of pulmonaryhypertension, suggests that RV myocardial damage in COPD cannot be blamed solely topressure overload.
P1084Left ventricular apical rotation at rest and with exercise: association with centralhemodynamics and left ventricular diastolic functional reserve
J. Seo; IJ. Cho; HJ. Chang; GR. Hong; JW. Ha; NS. Chung; CY. ShimYonsei Cardiovascular Center, Seoul, Korea, Republic of
Background: Augmented apical rotation (AR) has been suggested as a compensatorymechanism for reduced myocardial relaxation. Central arterial stiffening is an importantcontributor for impaired myocardial relaxation. We hypothesized that 1) central hemo-dynamic characteristics would be related to left ventricular (LV) AR parameters at restand after exercise, 2) LV AR parameters at rest would predict LV diastolic functionalreserve and, 3) there would be gender-related difference in LV AR characteristics.Methods: In 106 consecutive subjects (51 men, age 57+9 years) who were referred fortreadmill exercise echocardiography, radial artery tonometry was performed simultan-eously to assess central hemodynamics including augmentation index (AIx) and pulsepressure amplification (PPA). Subjects who had structural heart disease, atrial fibrillation,or inducible myocardial ischemia during exercise were excluded. LV longitudinal diastolicfunction and reserve were assessed by tissue Doppler imaging and the degree of AR andtime to peak AR (T-AR) were evaluated by speckle tracking imaging at rest and after peakexercise.Results: Resting T-AR but not AR degree was correlated with resting AIx (r=0.29,p=0.003) and resting PPA (r=-0.30, p=0.003). T-AR at peak exercise showed better cor-relations with peak AIx (r=0.34, p=0.001) and peak PPA (r=-0.50, p,0.001) than peakAR degree. In multivariate analysis, resting PPA was an independent determinant ofT-AR at rest (b=-0.26, p=0.005) and peak PPA was that of T-AR at peak exercise(b=-0.31, p=0.004), even after adjusting for confounding factors. Resting T-ARrevealed independent correlations with the changes of e’ (b=-0.26, p=0.005) with exer-cise and diastolic functional reserve (b=-0.30, p=0.004). In subgroup analyses bygender, women showed significantly prolonged T-AR at rest (383+32 vs. 360+37,p=0.004) and after exercise (210+49 vs. 238+38, p=0.006) than men. The predictivevalue of T-AR at rest for LV diastolic functional reserve with exercise was greater inwomen than in men.Conclusions Characteristics of LV AR might be affected by central hemodynamics notonly at rest but also after peak exercise. T-AR at rest is a good indicator for impaired LV dia-stolic functional reserve during exercise, especially in women.
P1085Intraventricular flow analysis during apical right ventricular stimulation
F. Bianco1; V. Cicchitti1; F. Radico1; M. Conti1; V. Bucciarelli1; M. Marchetti2; G. Tonti1;R. De Caterina1; E. Di Girolamo3; S. Gallina1
1G. d’Annunzio University, Department of Cardiology, Chieti, Italy; 2SS. AnnunziataHospital, Cardiology, Chieti, Italy; 3SS. Annunziata Hospital, Arrhythmology, Chieti, Italy
Purpose: a high percentage of ventricular pacing, in patients with a chronic apical rightventricular (ARV) stimulation, is known to be associated with an increased risk ofchronic heart failure (CHF). The left ventricular (LV) flow vortex formation is the result ofa proper synergy of wall dynamic forces that minimize kinetic energy dissipation andfacilitate redirection of blood towards the outflow tract. A dysfunctional LV vortex forma-tion might justify the onset of CHF. Echocardiographic particle-image-velocimetry(Echo-PIV) is a new imaging-technology able to detect and differentiate physiologicaland altered cardiac intracavitary flow patterns. The aim of our study was to assess differ-ent left cardiac intracavitary flow patterns during spontaneous rhythm and during ARV-pacing.Methods: we evaluated all patients afferent for periodic pacemaker (PMK) controls for sixmonths.The inclusion criteriawere:patientsover 18yearold, notPMKdependent, insinusrhythm, with a spontaneous ECG narrow-QRS, with preserved ejection fraction and a lowpercentage of right ventricular stimulation. All patients enrolled, first, underwent a
Abstract P1082 Figure. A-C preoperative, B-D 6 months follow up
Abstract P1081 Figure.
Abstracts ii179
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

standard echocardiographic evaluation. Then, after a 2 mL intravenous injection of sono-graphiccontrastagent, wereacquired aseriesof three-chambers-viewcine-loops forbothpacing models, each lasting 3 beats. All images acquired were studied with the Echo-PIV,off-line.Results: according to sample size, we enrolled 7 consecutive patients with a mean per-centage of pacing , 20% (mean age: 77.2+9.8 years, mean LVEF: 65,9+1,9%).During ARV-pacing, diastolic kinetic energy (KE) dissipation increased up-to 21,47%,compared to spontaneous rhythm, with a vortex formation time (VFT) decreased of14,7 % (P=0,05). Moreover, pressure vectors changed from -11,42 [+22,48, SD] to-30,98 [+37,21], P=0,016. At last, a negative correlation between TAPSE and systolicKE dissipation (r=0,94; P,0,001) was assessed.Conclusions: The present study describes, for the first time, the modifications ofintraventricular flow energetic properties induced by ARV-pacing. Further data areneeded to assess the role of these parameters in the development and maintenance ofLV dysfunction resulting in CHF.
P1086Age-related changes in the biomechanics of left ventricular and association withNT-proBNP
EV. Plokhova; D. Akasheva; O. Tkacheva; I. Strazhesko; E. Dudinskaya; I. Pokshubina;V. Pykhtina; A. Kruglikova; N. Brailova; S. BoytsovNational Center of Preventive Medicine, Moscow, Russian Federation
Purpose: The proportion of older people in the population increases. Therefore, the studyof cardiovascular aging process becomes more important for therapeutic intervention.This study sought to investigate age-related changes of the biomechanics of left ventricu-lar (LV) by determining different parameters in older people, using speckle tracking echo-cardiography (STE). N-terminal pro-brain natriuretic peptide (NT-proBNP) is a markersubclinical myocardial dysfunction which increases with advancing age. We examinedthe relationship NT-proBNP with the parameters of STE.Methods: 2-D speckle tracking analysis was performed on 151 healthy nonobese volun-teers aged 60 to 87 years without history of cardiovascular disease or regular use of medi-cation and significant deviations by 12-lead electrocardiogram. LV myocardialdeformations were obtained using off-line analysis program QLAB (Advanced UltrasoundQuantification Software Release 8.1.2 (Philips). Longitudinal LV strain was measured inthe 3 apical views; circumferential and radial strains in parasternal short-axis images atthe LV basal and apical level. LV peak systolic twist is defined as the value of apical LV sys-tolic rotation–basal LVsystolic rotation. Values aremean+SD. We assessed the intraob-server and interobserver variability for all parameters.The plasma concentration ofNT-proBNP was measured with ELISA method.Results: In 23 subjects (15%), image quality was insufficient for STE analysis. The sub-jects were 66.05+7.07 years old, 42% were men. Global longitudinal LV strain wasreduced in older people (-16.36+1.26%). Radial strain of LV basal (42.95+5.06%)and LV systolic twist (8.76+1.568) were increased. Age was significantly related to longi-tudinal LV strain (b=0.120, p=0.01), radial strain basal (b=0.202, p=0.01) and LV systolictwist (b=0.225, p=0.003). Plasma level of NT-proBNP were associated with age (r=0.56,p=0.002), longitudinal LV strain (r=0.42, p,0.001) and LV systolic twist (r=0.49,p,0.001).Conclusions: LV longitudinal strain decreases in older people. Radial strain and LV twistincreases with aging in order to compensate for the disturbance of the longitudinal de-formation or diastolic dysfunction in the elderly. Changes in these parameters are asso-ciated with the level of NT-proBNP indicating age-related disorders of myocardialcontractility.
P1087Ventricular interaction in asymptomatic patients late after repaired tetralogy ofFallot: a combined two-dimensional speckle tracking and three-dimensionalechocardiography study
K-P. Weng; CC. LinKaohsiung Veterans General Hospital, Kaohsiung, Taiwan, ROC
Purpose: LV dysfunction in repaired TOF patients have been demonstrated in previousstudies, but there are still some controversial issues about interventricular interactionlate after repaired TOF. The aim of the present prospective study was to assess ventricularinteraction in adolescent patients with repaired TOF using 2D speckle tracking and realtime 3D echocardiography simultaneously.Methods: We studied 31 patients with repaired TOF (M/F: 22/9, age: 16.1+6.1 yrs) whohad history of cardiac surgery with mean follow-up duration of 12.8 years, and 32 age- andsex-matched normal individuals (M/F: 23/9, age: 16.6+5.1yrs). All subjects underwentspeckle tracking and 3D echocardiography, EKG, treadmill, and blood sampling formeasurement of BNP.Results: Compared to the control group, the TOF group had higher BNP level (31.8+21.4 vs 14.1+12.4 pg/ml, p= 0.0016), lower peak oxygen uptake (VO2) (8.4+1.7 vs9.9+1.6 ml/kg/min, p=0.015), and longer QRS duration (126+30 vs 82+9 ms,p=0.001). Patientswith repaired TOFhad significantly impairedRVglobal andsix regionallongitudinal strain and strain rate than normal controls. Likewise, LV global and some nearapical regional longitudinal strain and strain rate were reduced in patients with repairedTOF. Compared to the normal controls, patients with repaired TOF had significantlylonger time to peak longitudinal strain in terms of basal to apical segments in RV. Therewas a significant correlation of longitudinal global strain (r=0.456, p=0.01) and time topeak longitudinal strain (r=0.484, p=0.006) between LV and RV in patients with repairedTOF. In terms of 3D echocardiography, patients with repaired TOF had lower LV stroke
volume, higher end diastolic volume, end systolic volume, stroke volume in RV, lowerRVEF, and higher pulmonary regurgitation fraction.Conclusions: Our results suggest patients with repaired TOF had abnormal biventricularmyocardial performance, as demonstrated by combined 2D speckle-tracking and 3Dechocardiography. The implications of these findings for management of patients lateafter repaired TOF remain to be determined.
P1088Effects of isolated significant mitral stenosis and isolated significant mitralregurgitation on left atrial deformation and electromechanical delay assessed byspeckle tracking echocardiography
M. Wahba Hassanein; Z A. Ashour; S W G. Bakhoum; A M A. Abdel WahabCairo University Hospitals, Cardiology, Cairo, Egypt
Purpose: To compare the effects of mitral stenosis (MS) and mitral regurgitation(MR)onLA deformation using two-dimensional speckle tracking echocardiography (STE).Methods: Thirty patients with isolated moderate to severe MS, 30 patients with isolatedmoderate to severe MR 30 healthy controls were included in the studyb. Using Speckletracking technique, peak atrial longitudinal strain (PALS), left atrial(LA) reservoir strainrate (RSR), LA conduit SR (CdSR), and LA contractile SR(CtSR) were calculated asthe average of LA 6 equidistant segments in the four-chamber view. The time to peaksystolic longitudinal strain (TTP SS), peak RSR (TTPRSR), peak CdSR (TTPCdSR)and peak CtSR(TTPCtSR) were also measured. PA-interval was measured from thevelocity curve of the left atrial basal lateral segment generated by speckle trackingtechnique.Results: The LA average PALS, RSR, CdSR and CtSR were significantly lower in MSpatients and in MR patients (all p=0.000) compared to controls. LA average PALS was sig-nificantly higher in MR compared to MS patients(p=0.02). The PA-interval was significant-ly shorter in the MS group compared to controls(p=0.000) and MR group(p=0.02).Significant inverse correlations were noted between the LA volume index (LAVI) andaverage PALS (r= -0.47, P=0.01), RSR (r= -0.45, P=0.01), CdSR (r= -0.59, P=0.001)and CtSR (r= -0.4, P=0.03) in MR patients and between LAVI and average RSR (r=-0.51, P=0.004) in MS patients.Conclusion: Isolated significant mitral stenosis and isolated significant mitral regurgita-tion have different negetive effects on left atrial deformation and electromechanicaldelay when assessed by PALS, TTP SS, TTP CdSR and PA-interval, which seems to bemore pronounced in isolated mitral stenosis.
P1089Left ventricular postsystolic shortening (PSS) by spectral tissue doppler imagingas a predictor for the presence of significant coronary artery disease
EKHLAS. Hussein1; ZIZI. Saad1; RAUOOF. Malik2; ADEL. Almasswary3; M. Elrawy1
1Zagazig University, cardiology department, Zagazig, Egypt; 2King Khalid university,cardiology department, abha, Saudi Arabia; 3Aseer central hospital, Abha, Saudi Arabia
Purpose: We investigated the diagnostic utility of post systolic shortening (PSS) by spec-tral tissue Doppler imaging (TDI) in the detection of coronary artery disease (CAD) amongpatients with chest pain.Methods: Eighty consecutive patients (51% females) with typical ischemic chest pain butwithout prior myocardial infarction,coronary revascularization,arrhythmia or heart failure,-who had no regional wall motion abnormalities on resting echocardiography and whowere scheduled to undergo coronary angiography, were selected. TDI was performedin each patient before coronary angiography to detect PSS at two levels (basal and midleft ventricle (LV)). in each of the four LV walls (anterior, inferior, lateral, septal). Coronaryangiography was performed and interpreted per standard clinical protocols.Results: Among the 60 patients who proved to have angiographic CAD, PSS in at least 1of the 8 examined LV points was found in all the patients versus none among patientswithout angiographic CAD (P , 0.001). Sensitivity of detecting CAD was 0.97 for PSS intheanteriorand lateral territories,0.93 inseptal territory, and0.90 in inferior territory.Thepres-enceofPSSineachsegmentshowedexcellentagreementwithangiography inthedetectionof CAD (K 0.80-0.93) and its presence was positively associated with conventional CAD riskfactors.Conclusion:Amongpatients withchest pain andnormal left ventricularcontraction on2Dechocardiography, the demonstration of PSS by spectral TDI can be used to predict thepresence of significant CAD.
Abstract P1088 Figure. PA-interval by speckle tracking
ii180 Abstracts
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022

P1090Reduction of longitudinal function is an early marker of left ventricular damage inCushing syndrome
F. Lo Iudice; M. Lembo; R. Muscariello; F. Carlomagno; R. Pivonello; A. Colao; B. Trimarco;M. GalderisiUniversity Hospital Federico II, Naples, Italy
Purpose: Cushing syndrome (CS) has been associated with structural and functionalalterations involving left ventricle, such as left ventricular (LV) concentric hypertrophyand diastolic dysfunction. Aim of our study was to evaluate LV longitudinal function inCS patients in comparison with normal subjects and hypertensive patients.Methods: At the time of diagnosis, 18 patients affected by CS (mean age 48+13 years, 2males) underwent a complete Doppler-echocardiographic examination including LVglobal longitudinal strain (GLS) determination by Speckle Tracking Echocardiography.CS patients were compared with 18 age and sex matched normal controls (NC) and 18age and sex matched never treated hypertensive patients (HTN).Results: CS patients showed higher LV mass (40.4+13.1 vs 33.3+5.7 vs33.0+9.4 g/ m2 2,7; p,0.05) and relative wall thickness (RWT) (0.37+0.06 vs 0.31+0.05 vs 0.31+0.07; p,0.05) compared with both NC and HTN. Transmitral E/A ratiowas lower in CS patients compared to NC but not to HTN (0.99+0.30 vs 1.37+0.57vs 1.10+0.37; p,0.05) while Simpson-derived biplane ejection fraction, left atrialvolume index and E/e’ ratio did not differ significantly among the three groups. GLSwas significantly reduced in CS patients in comparison to both NC and HTN (218.5+1.4 vs 221.8+2.0 vs 220.4+2.6 %; p,0.001). After excluding subjects with LV hyper-trophy (LV mass index , 45 in women and , 49 g/m2 2.7 in men), GLS remained signifi-cantly lower (218.1+0.9 vs 221.8+2.0 vs 220.5+2.7 %; p,0.0001) in CS patients incomparison with NC and HTN.Conclusion: CS is associated with LV concentric hypertrophy and with a reduction of LVlongitudinal function in comparison to both normal subjects and hypertensive patients.GLS reduction is evident even before the development of LV hypertrophy, and may re-present therefore an early marker of LV involvement in CS.
P1091The improvement of longitudinal intrinsic function of left ventricle before and afterexercise training in heart failure with preserved ejection fraction patients
S L. Purwowiyoto; A. Santoso; A M. SoesantoUniversity of Indonesia, Department of Cardiology and Vascular Medicine, NCCHK,Jakarta, Indonesia
Purpose: to know if there is any improvement in intrinsic longitudinal left ventricular func-tion using apical 4 chamber longitudinal strain before and after exercise training in HFPEFpatients.Methods: This is a quasi-experimental study. Thirty consecutive HFPEF patients joinedsupervised exercise training in the division of prevention and rehabilitation of cardiovas-cular center Harapan Kita. Exercise training program was conducted for a month withtotal of 20 times exercise training and evaluated every 2 weeks. Echocardiography wasperformed before the program started, week 2 and week 4 of exercise training. The6MWT, MLWHF and WHO5 questionnaire was evaluated before and after exercise trainig.Results: there was no significant difference in EF before, week 2 and week 4 of exercise.There was decrease inE/e’ and LAVI,also increase in longitudinal strain showing improve-ment of systolic and diastolic function after exercise. There was significant differences inthe 6MWT, the value of MLWHF and WHO5 score before and after exercise. Apical 4chamber longitudinal strain values obtained by 216.20% (210.70% to 217.81%).Apical 4 chamber longitudinal strain was improved at weeks 2 and 4 of exercise (beforeexercise A4ChLS = 216.20% [210.70% to 217.81%]; week 2 of exercise A4ChLS =218.00%+2.69% and week 4 exercise A4ChLS = 221.86%+1.79%) and there weresignificant differences (p , 0.001)Conclusions: There was an improvement in the longitudinal intrinsic left ventricular func-tion before and after exercise training in HFPEF patients
P1092Right atrial global systolic strain has higher prognostic value than right atrialdimensions
T. Segura De La Cal; JL. Moya Mur; A. Garcia Martin; S. Carbonell; C. Fraile Sanz;LM. Rincon; DA. Rodriguez Munoz; JJ. Jimenez Nacher; C. Fernandez-Golfin;JL. ZamoranoUniversity Hospital Ramon y Cajal de Madrid, Cardiology, Madrid, Spain
Aims:: Right atrium(RA) is seldom assessed in patients affected by left-heartcardiopathies. We aimed to determine, whether RA function(evaluated by global longitu-dinal strain[GLS] and strain rate[SR])or dimensions, better correlate with outcomes insuch patients.Methods: 103 outpatients were selected according to different degrees of right-heart over-load secondary to left-heart disease (65:sinus rhythm[SRhyt];35:atrial fibrillation[AF]). -Anatomical parameters evaluated: RAvolume(RAv), systolic and diastolic RA area(RAAs,RAAd). - RA deformation was determined(4C view). QRS established its onset. Toreflect its reservoir function, we evaluated RA positive GLS(S-wave)and SR(RASRs); andnegative SR at early-diastole(RASRe). If SRhyt, for contractile function, GLS and SR atECG-Pwave(A-wave and RASRa).- A composite end-point of cardiac death, heart failure hospitalization and cardiac surgerywas considered.Results: During a 20.9+13.0 month’s follow-up period, 29 SRhyt and 14 AF patients pre-sented events.- If SRhyt, univariate analysis(Cox)showed significant association between events and allstrain parameters(picture1). In a multivariate analysis(Cox), S-wave is the single param-eter significantly associated with outcomes. Best S-wave cutoff-value for event predictionwas 37.2%(AUC= 0.786), with both sensitivity and specificity of 76%. Kaplan-Meier ana-lysis showed significantly lower event-free survival rate for patients with S,32.7%(picture1). - If AF, none of the mentioned parameters demonstrated significant as-sociation with outcomes.Conclusions: If SRhyt, all RA strain-derived parameters correlate better to cardiac prog-nosis than RA dimensions. RA-GLS during ventricular contraction(S-wave), showed thebest correlation to patients’ prognosis. This predictive value is lost in AF.
P1093Left ventricular systolic functions in patients with non-dipper and dipperhypertension via two-dimensional longitudinal strain
A. Ongun; U. Habibova; DM. Gerede; I. Dincer; M. Kilickap; C. ErolAnkara University School of Medicine, Ankara, Turkey
Purpose: “Non-dipper” HTcases has higher rates of target organ damage that increasesthe cardiovascular morbidity and mortality. Two-dimensional (2D) deformation analysiscan detect subclinical left ventricular (LV) systolic dysfunction at an early stage whichcan’t be determined by conventional echocardiography (ECHO). The aim of the studywas to assess the role of 2D speckle tracking on detecting subclinical LV systolic dysfunc-tion in recently diagnosed “non-dipper” and “dipper” hypertensive patients whose LV sys-tolic functions were normal by conventional ECHO.Methods: Patients newly diagnosed essential hypertension were enrolled in the study.According to the ABPM results patients were divided into two groups as “dippers” and“non-dippers”. If LV systolic functions and regional wall motions were determined asnormal by conventional ECHO, 2D global and segmental longitudinal strain analysiswas conducted by speckle tracking method. Global and segmental systolic strain andstrain rates were measured. Global longitudinal strain (GLS) and global longitudinalstrain rates (GLSR) were calculated as arithmetic average of all segmental longitudinalstrain and strain rates. The study included 40 patients.Results: According to the ABPM, 32 patients were classified as “non-dippers”. Theaverage age of the patients in both of the groups was similar (49.5+ 12.4 years vs.52.0+ 13.5 years, p=0.85). 70% of the cases were men. No meaningful statistical dif-ference was determined between the groups’ demographical features and laboratorydata. The patients were on similar cardiovascular drugs. There was no statistically dif-ference between the “non-dippers” and “dippers” in the left ventricular diameters,mass, mass index, and EF. 2D speckle tracking analysis showed that mean GLS andGLSR were similar between the groups (Table 1). LV segmental analyses, also,showed that regional strain and strain rates were not different between the observedgroups.
Abstract P1089 Table. PSS Data in different LV territory
predictor variable Anterior Anterior Inferior Inferior Lateral Lateral Septal Septalb+SE P b+SE P b+SE P b+SE p
Age,years 3.04+0.85 0.001 3.23+1.00 0.002 2.63+0.91 0.005 1.34+0.99 0.99Female sex 3.23+11.49 0.78 7.93+13.50 0.56 213.66+12.25 0.27 221.75+13.38 0.11Diabetes 9.89+11.49 0.36 10.60+12.59 0.40 29.12+11.43 0.43 22.22+12.48 0.86Hypertension 24.84+12.32 0.048 19.33+14.47 0.19 13.06+13.14 0.32 30.94+14.35 0.034Smoking 22.36+10.84 0.043 12.53+12.73 0.33 9.20+11.55 0.43 8.69+12.61 0.49Dyslipidemia 23.10+10.77 0.035 49.53+12.65 /0.001 33.44+11.48 0.005 56.84+12.54 0.001Family History 45.54+10.99 /0.001 44.25+12.91 0.001 38.01+11.72 0.002 36.11+12.79 0.006SBP mmhg 0.12+0.36 0.74 20.60+0.43 0.16 0.24+0.39 0.55 20.37+0.42 0.38
PPS: postsystolic shortining. SBP:systolic blood presure.
Abstract P1092 Figure.
Abstracts ii181
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022
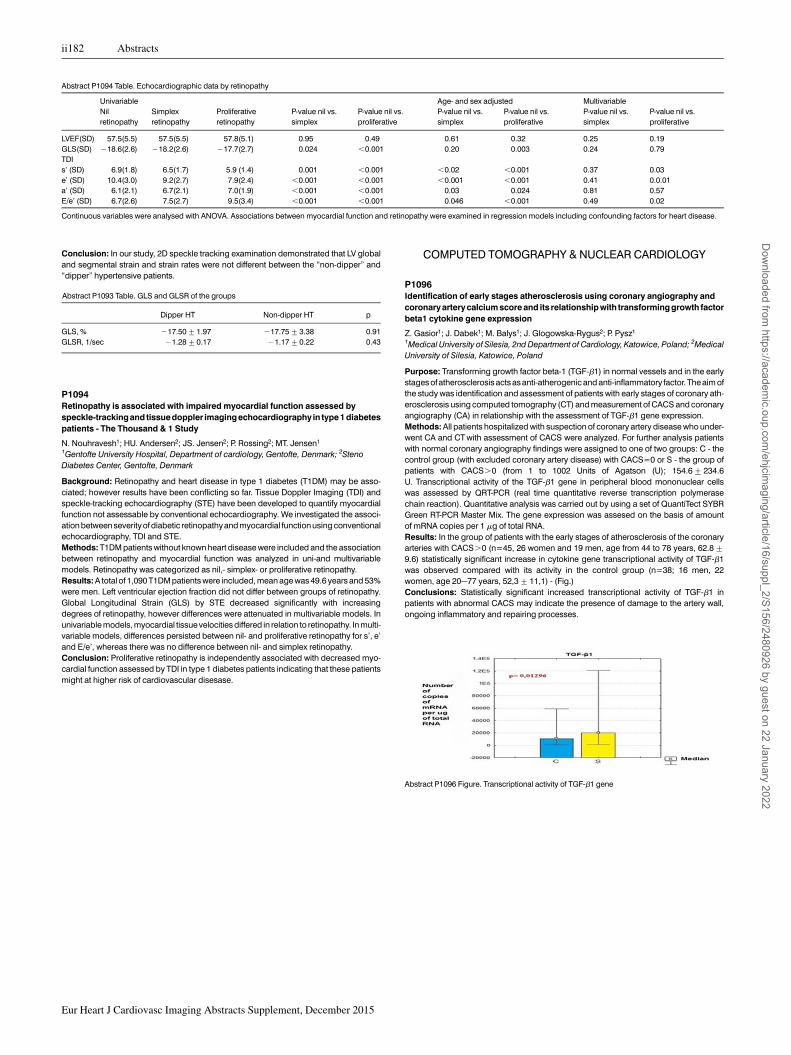
Conclusion: In our study, 2D speckle tracking examination demonstrated that LV globaland segmental strain and strain rates were not different between the “non-dipper” and“dipper” hypertensive patients.
Abstract P1093 Table. GLS and GLSR of the groups
Dipper HT Non-dipper HT p
GLS, % 217.50+1.97 217.75+3.38 0.91GLSR, 1/sec 21.28+0.17 21.17+0.22 0.43
P1094Retinopathy is associated with impaired myocardial function assessed byspeckle-trackingand tissuedoppler imagingechocardiography in type1diabetespatients - The Thousand & 1 Study
N. Nouhravesh1; HU. Andersen2; JS. Jensen2; P. Rossing2; MT. Jensen1
1Gentofte University Hospital, Department of cardiology, Gentofte, Denmark; 2StenoDiabetes Center, Gentofte, Denmark
Background: Retinopathy and heart disease in type 1 diabetes (T1DM) may be asso-ciated; however results have been conflicting so far. Tissue Doppler Imaging (TDI) andspeckle-tracking echocardiography (STE) have been developed to quantify myocardialfunction not assessable by conventional echocardiography. We investigated the associ-ation between severityof diabetic retinopathyand myocardial function using conventionalechocardiography, TDI and STE.Methods: T1DM patients without known heart disease were included and the associationbetween retinopathy and myocardial function was analyzed in uni-and multivariablemodels. Retinopathy was categorized as nil,- simplex- or proliferative retinopathy.Results: A total of 1,090 T1DM patients were included, mean age was 49.6 years and 53%were men. Left ventricular ejection fraction did not differ between groups of retinopathy.Global Longitudinal Strain (GLS) by STE decreased significantly with increasingdegrees of retinopathy, however differences were attenuated in multivariable models. Inunivariable models, myocardial tissue velocities differed in relation to retinopathy. In multi-variable models, differences persisted between nil- and proliferative retinopathy for s’, e’and E/e’, whereas there was no difference between nil- and simplex retinopathy.Conclusion: Proliferative retinopathy is independently associated with decreased myo-cardial function assessed by TDI in type 1 diabetes patients indicating that these patientsmight at higher risk of cardiovascular disesase.
COMPUTED TOMOGRAPHY & NUCLEAR CARDIOLOGY
P1096Identification of early stages atherosclerosis using coronary angiography andcoronary artery calcium score and its relationship with transforming growth factorbeta1 cytokine gene expression
Z. Gasior1; J. Dabek1; M. Balys1; J. Glogowska-Rygus2; P. Pysz1
1Medical University of Silesia, 2nd Department of Cardiology, Katowice, Poland; 2MedicalUniversity of Silesia, Katowice, Poland
Purpose: Transforming growth factor beta-1 (TGF-b1) in normal vessels and in the earlystages of atherosclerosis acts as anti-atherogenic and anti-inflammatory factor. The aim ofthe study was identification and assessment of patients with early stages of coronary ath-erosclerosis using computed tomography (CT) and measurement of CACS and coronaryangiography (CA) in relationship with the assessment of TGF-b1 gene expression.Methods: All patients hospitalized with suspection of coronary artery disease who under-went CA and CT with assessment of CACS were analyzed. For further analysis patientswith normal coronary angiography findings were assigned to one of two groups: C - thecontrol group (with excluded coronary artery disease) with CACS=0 or S - the group ofpatients with CACS.0 (from 1 to 1002 Units of Agatson (U); 154.6+234.6U. Transcriptional activity of the TGF-b1 gene in peripheral blood mononuclear cellswas assessed by QRT-PCR (real time quantitative reverse transcription polymerasechain reaction). Quantitative analysis was carried out by using a set of QuantiTect SYBRGreen RT-PCR Master Mix. The gene expression was assesed on the basis of amountof mRNA copies per 1 mg of total RNA.Results: In the group of patients with the early stages of atherosclerosis of the coronaryarteries with CACS.0 (n=45, 26 women and 19 men, age from 44 to 78 years, 62.8+9.6) statistically significant increase in cytokine gene transcriptional activity of TGF-b1was observed compared with its activity in the control group (n=38; 16 men, 22women, age 20–77 years, 52,3+11,1) - (Fig.)Conclusions: Statistically significant increased transcriptional activity of TGF-b1 inpatients with abnormal CACS may indicate the presence of damage to the artery wall,ongoing inflammatory and repairing processes.
Abstract P1094 Table. Echocardiographic data by retinopathy
Univariable Age- and sex adjusted MultivariableNilretinopathy
Simplexretinopathy
Proliferativeretinopathy
P-value nil vs.simplex
P-value nil vs.proliferative
P-value nil vs.simplex
P-value nil vs.proliferative
P-value nil vs.simplex
P-value nil vs.proliferative
LVEF(SD) 57.5(5.5) 57.5(5.5) 57.8(5.1) 0.95 0.49 0.61 0.32 0.25 0.19GLS(SD) 218.6(2.6) 218.2(2.6) 217.7(2.7) 0.024 ,0.001 0.20 0.003 0.24 0.79TDIs’ (SD) 6.9(1.8) 6.5(1.7) 5.9 (1.4) 0.001 ,0.001 ,0.02 ,0.001 0.37 0.03e’ (SD) 10.4(3.0) 9.2(2.7) 7.9(2.4) ,0.001 ,0.001 ,0.001 ,0.001 0.41 0.0.01a’ (SD) 6.1(2.1) 6.7(2.1) 7.0(1.9) ,0.001 ,0.001 0.03 0.024 0.81 0.57E/e’ (SD) 6.7(2.6) 7.5(2.7) 9.5(3.4) ,0.001 ,0.001 0.046 ,0.001 0.49 0.02
Continuous variables were analysed with ANOVA. Associations between myocardial function and retinopathy were examined in regression models including confounding factors for heart disease.
Abstract P1096 Figure. Transcriptional activity of TGF-b1 gene
ii182 Abstracts
Eur Heart J Cardiovasc Imaging Abstracts Supplement, December 2015
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/16/suppl_2/S156/2480926 by guest on 22 January 2022