poster session 2: monday 4 may 2015, 08:00-18:00room: poster area
TRANSCRIPT

Poster Session 2
Monday 4 May 2015, 08:00–18:00
Room: Poster Area
P238Critical role of SPECT MPI in defining best therapeutic procedure in developingworld
S E. BouyoucefBab El Oued Universitary Hospital Centre, Algiers, Algeria
Cardiovascular diseases (CVDs) are the principal cause of death in the world, (WHO data-base). Among CVDs, coronary artery diseases (CAD) are the most common diseaseswhich are responsible for more than 38% of deaths. Also, CAD therapeutic strategy,patient based, may vary from basic useful with limited expenses to very complex nonusefuland veryexpensive. InDevelopingcountries, suchavoidableandnon usefulexpen-ditures are greatly needed to be saved in order to be allocated for other country priorities.Recently,CAD has started to decline in developed countries thanks to prevention. Nuclearcardiac imaging is an important tool and part of the prevention strategy as well as a dis-criminate imaging for choosing the appropriate therapy for each patient especiallywhen limited budget is a reality like in developing countries. Medical treatment, and thetwo primary modalities bypass grafting (CABG) and percutaneous coronary intervention(PCI) are the main pillars of therapeutic strategy of CAD. The local experience has showedthat when SPECT MPI is used extensively for CAD assessment, the reduction of the cost ofmanagement of CAD is palpable and real. A limited study targeting almost 5500 patientsreferred for SPECT MPI in order to assist for defining the best therapy for suspected or con-firmed CAD. This study has been conducted between 2010 and 2014. Patients with morethan 2 vessels diseases were excluded from the study. From 5560 patients, 1752 patientshave had a normal SPECT MPI and therefore declared not clearly eligible for revascular-ization approach. 2050 patients have had a minor to moderate abnormalities and revas-cularization was discussed but not systematically done. In the rest of 1645 patients withmoderate to severe abnormalities revascularization was done in most cases. In develop-ing world, SPECT MPI is an important tool not only for secondary prevention but also fordefining appropriate therapeutic strategy.
P239Computed tomography angiography derived risk score in the assessment of theprognosis of coronary artery disease
V. Uusitalo1, V. Kamperidis2, MA. De Graaf2, T. Maaniitty1, I. Stenstrom1, A. Broersen2,AJ. Scholte2, A. Saraste1, JJ. Bax2, J. Knuuti11Turku PET Centre, University of Turku & Turku University Hospital, Turku, Finland; 2LeidenUniversity Medical Center, Cardiology, Leiden, Netherlands
Purpose: Our objective was to evaluate the prognostic value of the integrated risk scorecombining the effects of coronary atherosclerosis burden, location and morphology asassessed by computed tomography angiography (CTA).Methods: 922 consecutive patients underwent CTA for the evaluation of suspected stablecoronary artery disease. Patients without visible atherosclerosis (n=261) and patients inwhom quantitative CTA analysis was not possible were excluded (n=153). The final studygroup consisted of 508 patients aged 63 + 9 years. Using novel automated CTA quanti-fication software coronary artery stenoses location, severity and coronary plaques com-position for each coronary segment were identified and integrated in a single CTAscore (0-42). Major adverse cardiac events (MACE) including death, myocardial infarction(MI) and unstable angina pectoris (UAP) were obtained from the national healthcarestatistics.Results: There were total of 20 (4%) MACE in median follow-up of 3.6 years. These con-sisted of 9 deaths, 5 MI and 6 UAP. CTA risk score was divided to tertiles with following cut-offs: 0–6.7, 6.7–14.8 and .14.8, respectively. All MI (n=5) and most of the MACE
occured in the highest risk score tertile (3 vs. 3 vs. 14, p=0.002). Total mortality was com-parable (1 vs. 2 vs. 5, p=0.09). Patients with UAP were evenly distributed within the tertiles(2 vs. 2 vs. 2). Most of the late revascularisations (.6 months from baseline) were done inthe third tertile (2 vs. 0 vs. 11, p,0.001). Total number of MACE and late revascularisationswere higher in the third tertile (3 vs. 3. vs. 21, p,0.001). After correction for age and genderthe CTA risk score remained independently associated with the occurrence of MACE.Conclusions: Comprehensive CTA risk score integrating the location, burden andmorphology of coronary atherosclerosis predicts future cardiac events in patientsassessed for the suspicion of coronary artery disease.
P240Usefulness of stress myocardial perfusion imaging and baseline clinical factorsfor predicting cardiovascular events in patients with peripheral artery disease
T. Furuhashi, M. Moroi, T. Awaya, H. Masai, M. Minakawa, T. Kunimasa, H. Fukuda, K. SugiDivision of Cardiovascular Medicine, Toho University Ohashi Medical Center, Tokyo, Japan
Purpose: Stress myocardial perfusion imaging (MPI) is a well-established diagnostic andprognostic tool for managing coronary artery disease (CAD). Certain clinical factors suchas peripheral artery disease (PAD) and chronic kidney disease (CKD) are well establishedrisk factors for poor cardiovascular prognosis. We assessed the usefulness of stress MPIand baseline clinical factors as independent predictors of cardiovascular events inpatients with PAD and suspected/known CAD who underwent stress MPI.Methods: Stress MPI was performed in 97 PAD patients, and the mean follow-up periodwas 30 months. PAD was characterised by an ankle-brachial index (ABI) of ,0.9 or ahistory of revascularisation for PAD. CKD was defined as an estimated glomerular filtrationrate (eGFR) of ,60 ml/min/1.73 m2 or persistent proteinuria for at least 3 months, andadvanced CKD was characterised by Stage IV to V CKD and haemodialysis. Patientswith summed stress score of ,4 were considered to be normal. Cardiovascular eventsincluded cardiac death, nonfatal myocardial infarction and Braunwald class III unstableangina requiring hospitalisation.Results: Cardiovascular events were observed in 28 patients (29%). Univariate Cox re-gression hazard analysis revealed that advanced CKD, haemodialysis, LVEF on echocar-diography and parameters of stress MPI (summed stress score, summed rest score andsummed difference score) were significant predictors of cardiovascular events. Multivari-ate Cox regression analysis revealed that advanced CKD (hazard ratio = 4.03; P , 0.001),left ventricular ejection fraction (hazard ratio =0.96; P=0.008) andsummed stress scoresof stress MPI (hazard ratio = 1.15; P = 0.013) were independent and significant predictorsof cardiovascular events. Moreover, the numbers of coexisting risk factors (advancedCKD, reduced left ventricular ejection fraction, and abnormal stress MPI) was identifiedas a significant predictor of cardiovascular events (hazard ratio = 2.32, P , 0.001).Conclusions: In PAD patients, advanced CKD, left ventricular systolic function, andsummed stress scores of stress MPI results can be significant and independent predictorsof cardiovascular events. For patients who have these cardiovascular risk factors, aggres-sive strategies (strengthened suboptimal therapies and careful observation) are neededas early as possible.
P241Apoptotic microparticles to mononuclear progenitor cells ratio as a novelbiomarker in advanced heart failure patients
A. Berezin, A. KremzerState Medical University, Zaporozhye, Ukraine
Background: Acutely decompensated chronic heart failure (ADHF) is considered a life-threatening event. Despite contemporary treatment strategies of ADHF, frequent recurrent
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2015. For permissions please email: [email protected].
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
doi:10.1093/ehjci/jev052
by guest on May 12, 2015
Dow
nloaded from

hospitalizations due to other cardiovascular reasons after discharge of patients from thehospital are occurred.The objective of the study was to examine prognostic value of circulating endothelial-derived apoptotic microparticles (EMPs) to mononuclear progenitor cells (MPCs) ratiofor post-discharged patients with clinical stabilization after ischemic ADHF.Methods:Wehave been consecutively enrolled 136 patients (62male) with CAD admittedwithaprimarydiagnosis ofADHF. All thepatients havegiven their written informed consentfor participation in the study. At baseline all enrolled patients were hemodynamicallystable and they had NYHA III/IV classes of ischemic CHF. Observation period started atdischarge from the hospital and was up to 3 years. Flowcytometry analysis for quantifyingthe number of EMPs and angiogenic MPCs was used.Results: Median follow-up was of 2.12 years. Twenty tree participants were died and CHF-related death was occurred in 18 (78.3%) patients. Three subjects (13.0%) died suddenlyand two patients (8.7%) died due to myocardial infarction. No other causes of death weredefined. Additionally, 86 subjects were hospitalized repetitively due to worsening CHF (17cases in diedcohort [73.9%] and68 cases [66.0%] in survivedcohort).Calculated EMPs toMPCs ratios in survived and died patient cohort were 8.4 (95% CI = 7.6–9.2) and 78.9(95% CI = 53.0–116.6) respectively (P=0.001). MPCs, EMPs, NYHA class, NT-proBNPand increased NT-proBNP . 30% within 24-48 hours of admission period remained stat-istically significant for all-cause mortality, CHF-related death, and CHF-related rehospita-lisation, whereas LVEF and hs-CRP for all variables did not. We found that the addition ofEPMs to MPCs ratio to the ABC model (NT-pro-BNP, increased NT-pro-BNP . 30%)improved the relative IDI by 19.6% for all-cause mortality, by 21.7% for CHF-relateddeath, and by 19.5% for CHF-related rehospitalisation.Conclusion: We demonstrated that EMPs to MPCs ratio is considered more tremendousindicator of an imbalance between angiogenic and apoptotic responses with possible re-lation to cardiovascular outcomes in post-discharged patients with clinical stabilizationafter ischemic ADHF.
P242Long-term prognostic value of prospectively ECG-triggered low-dose coronaryCTangiography
OF. Clerc, B. Kaufmann, M. Possner, R. Liga, J. Vontobel, F. Mikulicic, C. Graeni, DC. Benz,PA. Kaufmann, RB. BuechelUniversity Hospital Zurich, Zurich, Switzerland
Purpose: This study aims at assessing the long-term prognostic value of low-dose 64-slice coronary CT angiography (CCTA) using prospective ECG triggering in a patientpopulation with known or suspected coronary artery disease.Methods: We retrospectively included 434 patients undergoing low-dose CCTA with pro-spective triggering. Patients were stratified according to coronary lesions as documentedby CCTA: normal coronary arteries, non-obstructive lesions (luminal narrowing ,50%),obstructive stenosis (stenosis ≥50%) and revascularized patients (previous stenting orbypass). Follow-up was performed using hospital records and telephone interviewswith patients and physicians regarding major adverse cardiac events (MACE), definedas cardiac death, non-fatal myocardial infarction or the need for revascularization. Revas-cularization within 6 weeks after CCTA scanning was excluded from analysis. Kaplan-Meyer analysis and Cox regressions were performed.Results: Mean effective radiation dose from CCTA was 1.7+0.6 mSv. At baseline, 153(35%) patients had normal coronaries, 87 (20%) had non-obstructive lesions, 131(30%) showed obstructive stenosis, and 34 (8%) were previously revascularized.Twenty-nine (7%) patients were lost to follow-up. After a median follow-up of 6.1 years,MACE occurred in 0% of patients with normal coronaries, in 6% of patients with non-ob-structive lesions, in 30% of patients with obstructive stenosis, and in 39% of revascularizedpatients (Figure). Multivariate Cox regression identified non-obstructive (P=0.03) and ob-structive lesions (P,0.001) as independent predictors for MACE.Conclusions: Low-dose CCTA with prospective ECG triggering has an excellent prog-nostic performance and suggests a 6-year warranty period for patients with normal coron-aries.
P243Normal stress-only gated-SPECT myocardial perfusion imaging in women: is thisresult related with a good outcome?
MJV. Ferreira1, MJ. Cunha2, A. Albuquerque2, D. Ramos3, G. Costa2, J. Lima1, M. Pego3
1University of Coimbra, Faculty of Medicine, Coimbra, Portugal; 2Coimbra Hospital andUniversity Center, Nuclear Medicine, Coimbra, Portugal; 3Coimbra Hospital and UniversityCenter, Cardiology, Coimbra, Portugal
Women with ischemic symptoms, despite having a lower prevalence of non obstructivecoronary arterydisease, have ahigher riskof ischemic events than thegeneral population.Due to lower radiation exposure and lower costs it becomes common using the stress-restprotocol with Tc 99m-tetrafosmin in myocardial perfusion imaging because if stressimages are normal, rest images are avoided.This study aims to determine the risk of events in women with normal stress-only myocar-dial perfusion imaging.This was a retrospective, cohort study that included patients referred to myocardial perfu-sion imaging (gated-SPECT MPI) between January of 2007 and December of 2008 withnormal stress-only images regarding perfusion and left ventricular function. 412 women(64.9+11.7 years) were followed until January 31st of 2012 or until the occurrence of acardiac event: cardiac death, non-fatal myocardial infarction or revascularization. 84(20.4%) had a history of coronary artery disease (CAD) (myocardial infarction and/orrevascularization). During follow-up (43.7+12.9 months) 19 cardiac events occurred: 4deaths, 6 myocardial infarctions and 9 revascularizations (4.6%). In the first year of follow-up there were 4events (0.9%) UsingCox survival analysis, the presence ofa history ofCAD(HR 3.9; CI 1.6-9.6; p=0.003), the presence of diabetes (HR 4.2; CI 1.7-10.4; p=0.03) wererelated with the occurrence of events and when incorporated in a multivariate model cor-rected for age were both independent variables. Age (HR 1.0; CI 1.0-1.1; p=0.1) and theperformance of the test through exercise (HR 0.4; CI 0.1-1.3; p=0.1) were not significantlyrelated with events in this group.In spite of the characteristics of ischemic heart disease in women normal stress-onlyimages, according to our results, had a short and long term good prognosis. Womenwith diagnosed CAD and/or diabetes had a higher risk of events.
P244Prognostic value of gated-SPECT myocardial perfusion imaging in women withacute coronary syndrome
A. Peix, L. Cisneros, LO. Cabrera, K. Padron, L. Rodriguez, F. Heres, R. Carrillo, E. Mena,Y. FernandezInstitute of Cardiology, Havana, Cuba
Purpose: To assess the prognostic value of gated single photon emission computed tom-ography (SPECT) to predict the occurrence of cardiac events in women with acute coron-ary syndrome (ACS).Methods: Forty seven women (mean age: 57.5 years) admitted between April 2011 andApril 2012 with diagnosis of ACS were included in the study. They were divided in twogroups: those with STEMI (group 1, 18 patients) and those with NSTEMI (group 2, 29patients). All underwent gated-SPECT two-day myocardial perfusion imaging (MPI)with a physical stress - rest protocol, one month after the index event. A one year clinicalfollow-up was done to register the occurrence of adverse cardiac events (unstable angina,non-fatal myocardial infarction or death).Results: Both summed stress score (SSS) and rest score (SRS) were significantly greaterin STEMI patients (mean values: 10.35 vs. 4.85 for SSS, and 6.76 vs. 2.38 for SRS). Leftventricular ejection fraction (LVEF) was significantly higher in those with NSTEMI(post-stress LVEF: 70.33% vs. 57.76% in STEMI, as well as rest LVEF: 66.25% inNSTEMI vs. 57.65% in STEMI). Delta LVEF (LVEF post-stress minus LVEF at rest) was sig-nificantly higher in NSTEMI: 4.08% vs. 0.12% in STEMI, p=0.03. There were eight cardiacevents: six unstable angina, one non-fatal myocardial infarction and one cardiac death.From these, two appeared among patients with STEMI, while six among those withNSTEMI. SSS and SRS were associated with the occurrence of cardiac events inNSTEMI patients, but not in those with STEMI. By multivariate analysis, the SRS and thenumber of perfusion defects were the variables associated with the occurrence ofcardiac events (RR: 1.317, p,0.005 for the SRS, and RR: 1.791, p=0.012 for thenumber of defects).Conclusions: A gated-SPECT MPI is useful to risk stratify women with diagnosis of acutecoronary syndrome. SSR and perfusion defect extension were the best predictors ofadverse cardiac events.
P245Efficacy of oral pre-scan diazepam as an additional heart rate reducing agent toimprove image quality in CTCA
ED. Huizing1, JD. Van Dijk1, JA. Van Dalen1, JR. Timmer2, JP. Ottervanger2, CH. Slump3,PL. Jager11Isala Clinics, Nuclear Medicine, Zwolle, Netherlands; 2Isala Clinics, Cardiology, Zwolle,Netherlands; 3University of Twente, Enschede, Netherlands
Purpose: In Computed Tomography Coronary Angiography (CTCA) it is important toachieve a heart rate as low as possible during scanning to improve image quality.However, in clinical practice higher heart rates are observed, possibly due to anxiety. Di-azepam is an anxiolytic drug and the aim of this study was to assess the effectiveness oforal diazepam as a heart rate reducing agent for CTCA to improve image quality.Methods: A total of 101 patients underwent CTCA in two consecutive groups of patients.Both groups were administered metoprolol (beta-blocker) based on heart rate upon entry.Rate of MACE occurence during follow-up
Poster Session 2 i39
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from
In order to further reduce heart rate, the intervention group (n=56) received a dose of 5 mgdiazepam (oral) an hour prior to being scanned. The control group (n=45) did not receivediazepam. Image quality was assessed by scoring motion artefacts, step artefacts (boththree-point scale) and overall quality (a four-point scale). The relation between imagequality and heart rate was investigated for a correlation and heart rate reductionbetween groups was compared.Results: With increasing heart rate, motion artefacts and overall quality scores becamemore severe (p=0.03 and p=0.03, respectively). Step artefacts were not correlated withheart rate (p=0.75). The percentual reduction in heart rate in the diazepam and controlgroup was not different between groups (p=0.55) with 18.4% + 12.6% and 20.1% +14.8% reduction, respectively.Conclusions: Image quality as scored with motion artefacts and overall quality improveswith lower heart rate. Administration of diazepam in addition to metoprolol does not de-crease heart rate further and has no effect on image quality in the group investigated.
P246Image noise in non-contrast coronary artery calcium scan is predictive of anon-diagnostic CTcoronary angiogram in obese subjects
S. Venuraju1, A. Jeevarethinam1, A. Yerramasu2, S. Atwal1, VS. Mehta3, A. Lahiri11Wellington Hospital, London, United Kingdom; 2Royal Infirmary of Edinburgh, Edinburgh,United Kingdom; 3North Middlesex University Hospital NHS Trust, London, UnitedKingdom
Introduction: Performing CTcoronary angiography in obese subjects (BMI.35 kgs/m2)is extremely challenging due to increased photon scatter, resulting in significant imagenoise. Consequent degradation of image quality results in significantly higher percentageof non-diagnostic scans.Aim: The aim was to study the effect of factors affecting image quality and identify an ob-jective measure, predicting the occurrence of a non-diagnostic scan.Methods: Consecutive patients with a BMI . 35 Kgs/m2 referred to our centre for clinicallyindicated CTcoronary angiograms were included in the study (n=116). Image protocolswere optimized by two experienced physicians for every patient based on BMI, includingscanning with either 120 kVor 140 kV. Image quality was scored on a scale of 1–4 (1 beingexcellent and 4 being non-diagnostic). Objective measures of image quality, signal tonoise ratio and contrast to noise ratio were also measured. Image noise in CAC scanwas measured as standard deviation of the attenuation values (Hounsfield units, Hu)within a 2 cms2 region of interest drawn in the ascending aorta above the coronary ostia.Results: Mean age of patients in the study was 58.5+10.7 with 57% males. Median BMIwas 37.5 kgs/m2 (35.9 - 41.2 kgs/m2). BMI was significantly different in those scanned with120 kV thans those scanned with 140 kV (36.6 kgs/m2 vs 39.3 kgs/m2, p,0.001). A total of10 (8.6%) scans were non-diagnostic; 5 (8%) were scanned using 120 kVand 5 (10%) with140 kV. Subjective image quality score for the entire study population was 2.05+0.88.There was no difference in subjective image quality scores between those scannedwith 120 kV and 140kV (2.11+0.83 vs 1.98+0.93, p=0.44). The univariate predictors ofa non-diagnostic scan were average heart rate (p=0.01), BMI (p=0.006) and noise inCAC scan (p=0.001); in a multivariate analysis, only noise in the CAC scan was foundto be a significant predictor (p=0.005). Using ROC curve analysis, noise in CAC scan of22.85 Hu predicted a non-diagnostic scan with sensitivity of 70% and a specificity of67%. If only, those scanned with 120 kV are analysed, a noise in the CAC scan of 20 Hupredicts the occurrence of a non-diagnostic scan with a sensitivity of 80% and a specificityof 58%.Conclusions: Image noise in the non-contrast CAC scan of . 22.85 predicts the occur-rence of a non-diagnostic CTCAwith 70% sensitivity. Hence while scanning grossly obesepatients, this degree of image noise should prompt the discussion regarding feasibility ofproceeding with CTCA thereby preventing unnecessary radiation exposure.
P247New strategy in CT dose reduction in prospective coronary CT for minimizingcoverage
A. Arjonilla Lopez1, M J. Calero Rueda1, G. Gallardo2, J. Fernandez-Cuadrado1,D. Hernandez Aceituno2, J. Sanchez Hernandez2
1Hospital Rey Juan Carlos, Cardiac Imaging Unit, Mostoles, Spain; 2Universitary HospitalRey Juan Carlos, Radiology, Mostoles, Spain
Purpose: The purpose of this study is to show a strategy to more accurately select thecoverage area to include only the clinical region of interest with a subsequent dramaticdose reduction.Methods and Materials: 26 patients underwent prospective ECG-triggered coronary CTangiography using a 128-slice MDCT. A regular heart rate control of less than 60 bpm wasachieved through oral or intravenous administration of b-blockers, Nitroglycerine 0.4mg/sublingual tab was given if not contraindicated for coronary vessels dilatation. In 13patients the coverage was minimized to the extreme with the help of two low doseslices one at the bottom of the heart to make sure the most caudal portions of the posteriordescending and recurrent arteries were included in the study and the other one located 1cm below the charina which was also used for placing the tracker in order to use the leastnumber of steps possible for full heart coverage. Radiation dose in these patients wascompared to the one obtained in other 13 patients with standard coverage.Results: The scan length was reduced in a 14,5% in the minimizing group with a subse-quent dose reduction of approximately 30% (mean CDTI of 100, 3 mGy compare to thegroup with standard coverage where mean CTDI was 132 mGy).
Conclusion: Shorter scan length with the help of two low dose slices at the bottomand at the charina to more accurately select the coverage area do cut radiation dosesubstantially.
P248Evaluation of variable pitch helical CT scanning after CABG operation
H. Yoshida1, A. Mizukami2, A. Matsumura2
1Kameda Medical Center, Radiology Department, Kamogawa, Japan; 2Kameda MedicalCenter, Cardiology, Kamogawa, Japan
Purpose:Atour hospital, 64slice MDCTwith variable pitch helical scanning capability wasintroduced in July, 2009. With this system, variable helical pitch can be obtained with asingle scan, and ECG synchronization can be turned on and off. At our facility, this tech-nique is used in patients post CABG, and when scanning coronary arteries and theaorta concurrently. We evaluated the graphic resolution at the timing of helical pitchshift using phantom, and the quality of clinical image obtained in post CABG patientsusing this technique.Methods: CTused in this study was Aquilion 64 by Toshiba. Clinical image was obtainedusing clinically used helical pitch, and quality of image obtained around helical pitch shiftwas assessed using modality such as comb phantom. The image obtained with variablehelical pitch was compared with images acquired without it.Results/Discussion: Phantom image around the helical pitch shift was of good qualityeven in patients with history of CABG. The scan time and amount of contrast agentswere reduced compared to images obtained without variable helical pitch. The scantime and amount of irradiation decreased even in patients with arrhythmia, and this tech-nique showed to be useful.Conclusion: With this evaluation, the helical pitch shift did not interfere with image quality.In evaluation of post CABG patients, variable helical pitch was clinically useful. By evalu-ating other scanning techniques and improving the understanding of each technique, wewill be able to provide more images useful in clinical settings.
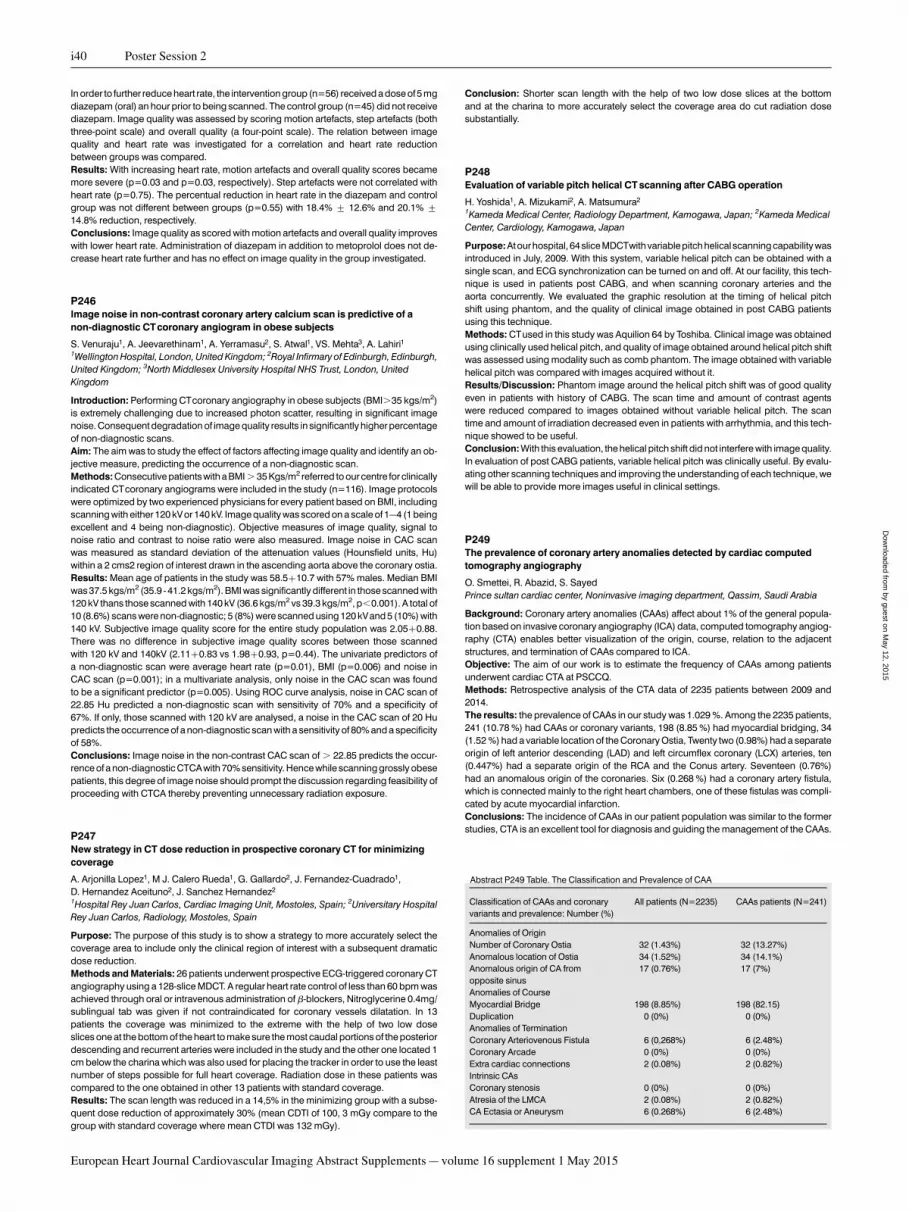
P249The prevalence of coronary artery anomalies detected by cardiac computedtomography angiography
O. Smettei, R. Abazid, S. SayedPrince sultan cardiac center, Noninvasive imaging department, Qassim, Saudi Arabia
Background: Coronary artery anomalies (CAAs) affect about 1% of the general popula-tion based on invasive coronary angiography (ICA) data, computed tomography angiog-raphy (CTA) enables better visualization of the origin, course, relation to the adjacentstructures, and termination of CAAs compared to ICA.Objective: The aim of our work is to estimate the frequency of CAAs among patientsunderwent cardiac CTA at PSCCQ.Methods: Retrospective analysis of the CTA data of 2235 patients between 2009 and2014.The results: the prevalence of CAAs in our study was 1.029 %. Among the 2235 patients,241 (10.78 %) had CAAs or coronary variants, 198 (8.85 %) had myocardial bridging, 34(1.52 %) had a variable location of the Coronary Ostia, Twenty two (0.98%) had a separateorigin of left anterior descending (LAD) and left circumflex coronary (LCX) arteries, ten(0.447%) had a separate origin of the RCA and the Conus artery. Seventeen (0.76%)had an anomalous origin of the coronaries. Six (0.268 %) had a coronary artery fistula,which is connected mainly to the right heart chambers, one of these fistulas was compli-cated by acute myocardial infarction.Conclusions: The incidence of CAAs in our patient population was similar to the formerstudies, CTA is an excellent tool for diagnosis and guiding the management of the CAAs.
Abstract P249 Table. The Classification and Prevalence of CAA
Classification of CAAs and coronaryvariants and prevalence: Number (%)
All patients (N=2235) CAAs patients (N=241)
Anomalies of OriginNumber of Coronary Ostia 32 (1.43%) 32 (13.27%)Anomalous location of Ostia 34 (1.52%) 34 (14.1%)Anomalous origin of CA fromopposite sinus
17 (0.76%) 17 (7%)
Anomalies of CourseMyocardial Bridge 198 (8.85%) 198 (82.15)Duplication 0 (0%) 0 (0%)Anomalies of TerminationCoronary Arteriovenous Fistula 6 (0,268%) 6 (2.48%)Coronary Arcade 0 (0%) 0 (0%)Extra cardiac connections 2 (0.08%) 2 (0.82%)Intrinsic CAsCoronary stenosis 0 (0%) 0 (0%)Atresia of the LMCA 2 (0.08%) 2 (0.82%)CA Ectasia or Aneurysm 6 (0.268%) 6 (2.48%)
i40 Poster Session 2
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from

P250Tortuosity of the coronary arteries in cardiac computed tomography
A. Mlynarska1, R. Mlynarski2, K. Golba1, M. Sosnowski11Medical University of Silesia, Katowice, Poland; 2Upper Silesian Cardiology Center,Katowice, Poland
Tortuosity of coronary arteries measures how sharply is the lumen bends in whole vesselor a segment and is expressed in degrees/cm, however clinical significance is lessacknowledged.Methods: In 55 pts. a 64 slice CT (Toshiba, Aquilion 64) was performed due to coronaryartery disease suspicion. Vessels (LAD, LCx, RCA, conus artery) and their tortuositywere analyzed by using the semi-automated vessel measurements by Vitrea 2 softwareby experienced researcher. Cardiac functional analysis (automatic with manual correc-tions) was performed in each - those data were correlated with tortuosity data.Results: Example of tortuosity measurements are presented in the figure below. Averagetortuosity for LAD was 1.42 + 0.2 for average vessel length 121.10 + 40.5; for LCx it was1.40 + 0.1 for average vessel length 94.70 + 29.4 and for RCA it was 1.99 + 0.4 foraverage vessel length 134.30 + 36.1. In selected cases tortuosity of conus artery (ifpresent) was 1.56 + 0.2. Significant differences were found between LAD and RCA tortu-osity (p,0.000) and LCx and RCA tortuosity (p,0.000). LAD tortuosity correlated signifi-cantly with function parameters: end diastolic volume (r=0.54; p,0.05), end systolicvolume (r=0.46; p,0.05) and stroke volume (r=0.57; p,0.05).Conclusions: Tortuosity is a small, sometimes significant, feature of coronary arteries thatcan be reliably evaluated in a cardiac computed tomography. Its magnitude depends onLV function, however clinical significance this observation needs further studies.
P251Impact of clinical risk factors and coronary calcium score on cardiovascularscreening strategies before kidney transplantation
S.Winther1,M.Svensson2,HS. Jorgensen2,K. Bouchelouche3,LC. Gormsen3,NR. Holm1,HE. Botker1, PR. Ivarsen2, M. Bottcher41Aarhus University Hospital, Department of Cardiology, Aarhus, Denmark; 2AarhusUniversity Hospital, Department of Nephrology, Aarhus, Denmark; 3Aarhus UniversityHospital, Department of Nuclear Medicine and PET-Center, Aarhus, Denmark; 4CardiacImaging Center, Hospital Unit West, Herning, Denmark
Background: While cardiac evaluation before kidney transplantation is recommended,no unequivocal strategy has been identified. Our aim was to investigate if coronarycalcium score (CACS) should replace risk factors for the selection of kidney transplant-ation candidates for cardiac evaluation and influence the choice of non-invasive modalityfor diagnostic of obstructive CAD.Method: We conducted a prospective study of 167 kidney transplantation candidates(age 54 [23–72] years and 43% treated with dialysis) referred for cardiac evaluation.Patients underwent risk factor assessment, CACS, coronary computed tomography angi-ography (CCTA), single-photon emission computed tomography (SPECT), and invasivecoronary angiography (ICA). We compared these modalities using ICA as reference.Results: The average number of risk factors and median CACS were significantlyincreased for the patients (22%) with obstructive CAD. The accuracy evaluated by receiveroperating characteristic curves was superior for CACS compared to risk factors, 0.85 vs.0.71 (p=0.01). Diagnostic accuracy of screening strategies before kidney transplantationis listed in the table.Conclusions: In kidney transplantation candidates, CACS was superior to risk factor as-sessment for predicting obstructive CAD and provides a better selection of patients andmodality for cardiac evaluation.
Abstract P251 Table.
Sensitivity Specificity PPV NPV
Diagnostic strategy with risk factors ≥3 as gatekeeperRisk factors ≥3 83 (CI: 65–94) 44 (CI: 34–72) 29 (CI: 20–40) 90 (CI: 79–97)Risk factors ≥3& CCTA
80 (CI: 61–92) 74 (CI: 65–82) 46 (CI: 32–61) 93 (CI: 85–97)
Risk factors ≥3& SPECT
47 (CI: 28–65) 94 (CI: 87–97) 67 (CI: 43–85) 86 (CI: 79–92)
Diagnostic strategy with coronary artery calcium score as gatekeeperCACS cut-off 234* 87 (CI: 69–96) 71 (CI: 62–80) 46 (CI: 32–59) 95 (CI: 88–99)CACS cut-off 400† 67 (CI: 47–83) 77 (CI: 68–84) 44 (CI: 30–60) 89 (CI: 81–95)Low coronary artery calcium score (n=93)
Continued
CACS ,400& CCTA
80 (CI: 44–98) 80 (CI: 69–88) 32 (CI: 15–54) 97 (CI: 90–100)
CACS ,400 &SPECT
60 (CI: 26–88) 80 (CI: 69–88) 26 (CI: 10–48) 94 (CI: 86–94)
High coronary artery calcium score (n=45)CACS ≥400 &CCTA
100 (CI: 83–100) 8 (CI: 1–26) 47 (CI: 31–62) 100 (CI: 16–100)
CACS ≥400 &SPECT
50 (CI: 27–73) 88 (CI: 69–98) 77 (CI: 46–95) 69 (CI: 50–84)
† The prespecified CACS threshold* The optimal CACS threshold.
P252Anatomic and functional discordance in coronary artery disease: role of SPECTand CTA fused images
C M. Cortes, EN. Aramayo G, M. Daicz, JF. Casuscelli, ED. Alaguibe, A. Neira Sepulveda,M. Cerda, GE. Ganum, M. EmbonHospital Universitario Fundacion Favaloro, buenos aires, Argentina
Purpose: To assess whether fused images of myocardial perfusion (SPECT) with cardiaccomputed tomography angiography (CTA) improve the interpretation of perfusiondefects and their correspondence to a vascular territory over side by side analysis.Methods: From 03/2009 to 08/2014 we studied 140 consecutive patients referred forSPECTand CTA on a separate scanner for evaluation of CAD. Both tests were performedwithin 1 + 16 days between each other. We selected subjects with abnormal perfusiondefined as SSS=0. The CTA stenosis .50 % were defined as abnormal in the followingvessels: left anterior descending, circumflex, diagonal, right coronary and marginal. Thecombined assessment of perfusion and anatomic images through side-by-side analysisand after fusion of both modalities were used to obtain three groups: perfusion/anatomymatch (normal or abnormal) and perfusion/anatomy unmatch territories.Results: Ninety-nine patients were included, 83 were men, age 58+9 years. Fifty six hadhigh blood pressure, 62 dyslipaemia, 13 diabetes. Thirty three patients had no history ofCAD. The side by side analysis showed 99 abnormal, 250 normal and 115 unmatched ter-ritories.Fusion imagesshowed128abnormal, 288normaland76unmatched territories (p0.03). Results in the unmatched groups are shown in table 1.Conclusion: In our population, fusion images of SPECTand CTA allowed to reduce thediscordance between coronary anatomy and functional images determined throughthe side by side analyis. This reduction was at the expense of the non-diagnostic tests.This could be a helpful tool for eventual invasive therapeutic decisions.
Unmatched groups Side by side analysis Fusion analysis p
Total 115 76 0,03Known CAD 82 48 0,001Diagnostic 33 28 NS
P253Prospective evaluation of early and delayed tolerance of regadenoson in patientssuspected of CAD ineligible for conventional stress testing
J. Vigne, B. Enilorac, A. Lebasnier, L. Valancogne, D. Peyronnet, A. Manrique, D. AgostiniUniversity Hospital of Caen, Caen, France
Purpose: Regadenoson (R) is a selective adenosine-2A receptor agonist approved as astressor agent in myocardial perfusion scintigraphy (MPS).Then R can beused inpatients(pts) with asthma or chronic obstructive pulmonary disease (COPD). Therefore the aim ofour study is to evaluate early and delayed side effects profile and hemodynamic responseof R in pts suspected of CAD ineligible for conventional stress testing.Methods: 206 consecutive pts, referred for clinically indicated MPS were included fromDecember 2013 to July 2014. Inclusion criteria were: asthma, COPD, severe obesity(BMI.35), caffeine intake and dipyridamole intolerance. R was administered over 20s.Heart rate (HR), systolic and diastolic blood pressure (SBP, DBP) were recorded and com-pared at different time points before and during pharmacological stress (baseline, 1 min, 3min). Early side effects were monitored in the department by a cardiologist and delayedside effects were assessed by phoning using a standardized questionnaire 96h atmaximum after MPS otherwise patients were considered lost to follow-up. Severe sideeffects were graded using MedDRA adverse event dictionary.Results: Patients distribution (121M / 85F, age : 64.4+ 10.9 YO)was :41% (n=84)severeobesity, 34% (n=70) asthma, 14% (n=29) COPD, 10% (n=21) caffeine intake and 1%(n=2) dipyridamole intolerance. There was a significant drop in SBP (mean: -3.25+16.3 mmHg, p,0.005) and DBP (mean: -2.5+9.34 mmHg, p,0.001) between base-line and 3min, and increase of HR (mean: +18+10.7 bpm, p,0.001) between baselineand 1min. Almost 82% (n=133) of followed up pts declared or presented at least 1 sideeffect (18% lost to follow-up, n=38). Early side effects occurred in 62% of patients(n=132), the most frequent was blockpnea (32%, n=66) followed by flushing (15%,n=30) and dyspnea (8%, n=17), and the most severe was grade 3 diarrhea (n=2)during MPS acquisition. The antidote, aminophylline, was required for 7.8% of patients(n=16). Delayed side effects were declared by 38% of followed up patients (n=79), themost frequent were: fatigue 19% (n=31), insomnia 7.4%(n=12)and dyspnea5.5% (n=9).
Abstract P250 Figure. Examples of tortuosity
Abstract 114 Table. Continued
Poster Session 2 i41
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from
Conclusion: R induces significant hemodynamic changes during MPS. Early anddelayed side effects are completely different, but benign and rapidly reversible,showing an optimal tolerance of R for pts with suspected CAD.
P254Stress testwithnuclear imaging is insufficient to ruleout ischemicheartdisease inpatients with left ventricular dysfunction of unknown etiology
D. Menendez, S. Rajpal, C. Kocherla, M. Acharya, P. ReddyLouisiana State University, Shreveport, United States of America
Introduction: In patients with left ventricular dysfunction (LVD) of unknown etiology, cor-onary angiography (CAG) is recommended and commonly performed to rule out ische-mic heart disease (IHD). Less commonly, cardiac stress test with myocardial perfusionimaging (MPI) is used for this purpose. However, the comparative efficacy of CAG andMPI in diagnosing IHD in pts with LVD of unknown etiology.Objective: Our study was designed to determine the value of MPI in correctly identifyingobstructive coronary artery disease (CAD) in patients who presented with left ventriculardysfunction (LVD).Methods: From a query of electronic records (EMR) of a tertiary care teaching hospitalover 2 years, 48 patients met our selection criteria of having a CAG done for left ventriculardysfunction (defined as ejection fraction,40%) and an available MPI and a 2D echocar-diogram. 9 patients were excluded from final analysis due to insufficient data on EMR. Ob-structive CAD was defined as .50% occlusion in a major epicardial coronary artery.Results: 39 patients (19 females and 20 males with mean age of 54 years) with LVD hadpositive MPI for ischemia. 24 of these 39 patients had obstructive CAD confirmed on CAG,resulting in a positive predictive value (PPV) of 62%. In the 24 patients with true obstructiveCAD based on CAG, including 10 with multivessel disease, MPI correctly identified thearea of ischemia 96% of the time.Conclusions: The results of our study show that in patients with LVD of unknown etiologywho underwent both MPI and CAG to rule out IHD: (a) MPI accurately identified IHD in only62% patients; (b) CAG is superior to MPI; (b) MPI correctly identified the area of ischemia innearly all patients with true obstructive CAD.
P255The utility of 99mTc-PYP-SPECT in diagnosis of latent myocarditis in patients withatrial fibrillation
I. Sazonova1, YUN. Ilushenkova1, RE. Batalov1, YV. Rogovskaya1, YB. Lishmanov1,SV. Popov1, NV. Varlamova2
1Research Institute of Cardiology, Tomsk Scientific Center, Tomsk, Russian Federation;2Tomsk Polytechnic University, Tomsk, Russian Federation
Aim: To compare results of myocardium SPECT with 99mTc-pyrophosphate (PYP) withMRI and histology data in patients with isolated persistent atrial fibrillation (AF)Materials and Methods: We examined 70 patients (pts) (32 males and 38 females, meanage 41.1 + 9.92) with isolated persistent AF. All patients underwent SPECT with99mTc-PYP at 3 and 18 hours post injection (delayed SPECT), following by SPECT with99mTc-MIBI at the rest condition. Both images were then combined. Accumulation of99mTc- PYP was accepted as pathological when focus localized in myocardium area,focus/background ratio exceeded 1,4. In 30 pts Cardiac Magnetic Resonance (MRI)with gadolinium was performed. Endomyocardial biopsy (EMB) samples were takenduring catheter ablation of AF. Scintigraphic results were compared with the EMB andimmunohistochemical findings.Results: According to histological data active lymphocytic myocarditis was verified in 9pts (13%), the remaining 61 pts had signs of cardioscleroses in combination with myoly-sis, histiolymphocytic infiltration or lipomatosis.The pathological uptake of 99mTc-PYP was found in 17 patients. The number of true-positive results was 7, true negative 51, false-positive–10, false negative 2. The sensitivitywas 77%, specificity 83%, accuracy 83%.Late gadolinium enhancement at MRI was marked at 18 of 30 pts, but neither of ptsmatched to «Lake Luise Criteria» of myocarditis. A direct correlation was found betweenMRI and 99mTc-PYP (R=0,64)/Conclusion: The results of our study have shown that in 13% of patients with isolated AFhad latent myocarditis. Cardiac SPECT with 99mTc-PYP has a potential as an effectivenoninvasive tool of diagnoses of latent myocarditis in pts with isolated AF and can serveas an additional criterion for EMB in a perspective.
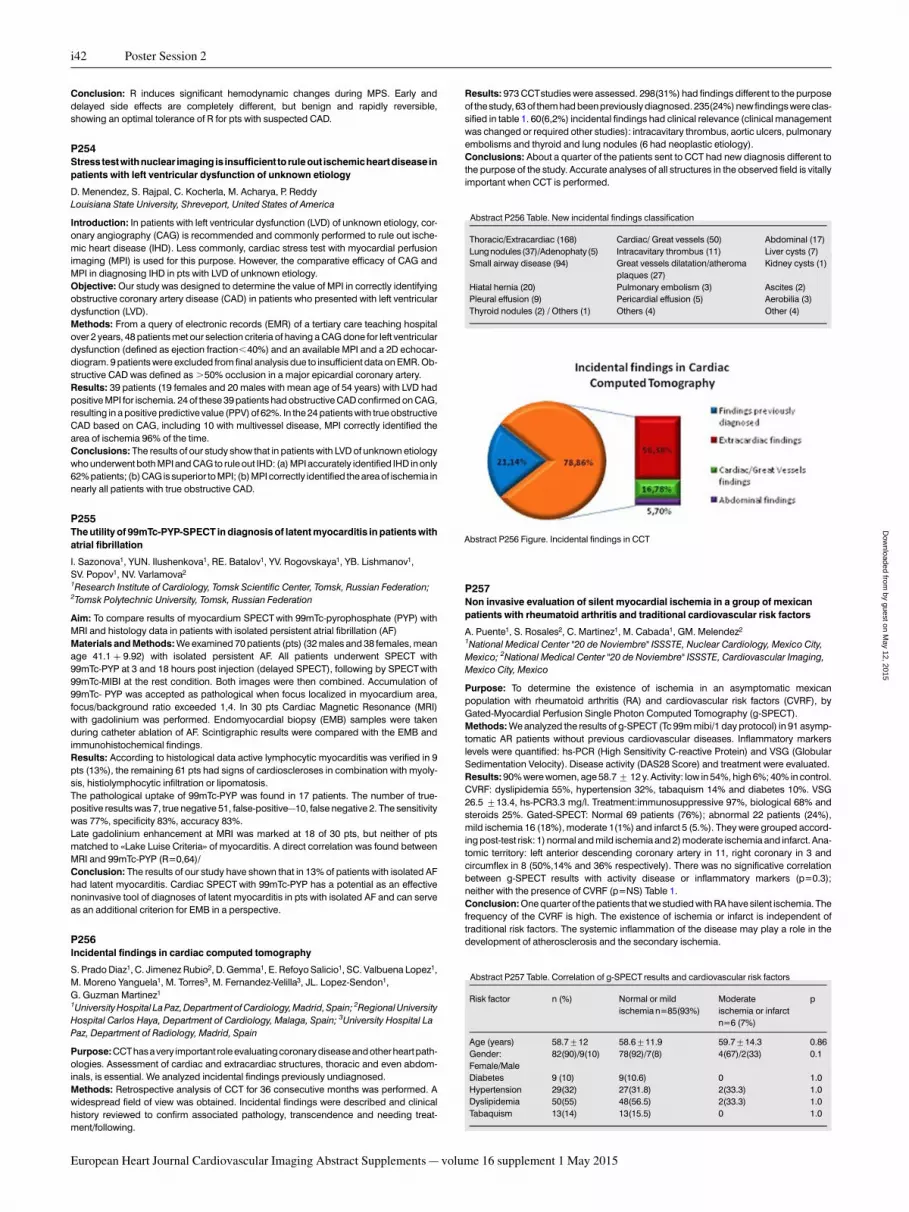
P256Incidental findings in cardiac computed tomography
S. Prado Diaz1, C. Jimenez Rubio2, D. Gemma1, E. Refoyo Salicio1, SC. Valbuena Lopez1,M. Moreno Yanguela1, M. Torres3, M. Fernandez-Velilla3, JL. Lopez-Sendon1,G. Guzman Martinez1
1University Hospital La Paz, Department of Cardiology, Madrid, Spain; 2Regional UniversityHospital Carlos Haya, Department of Cardiology, Malaga, Spain; 3University Hospital LaPaz, Department of Radiology, Madrid, Spain
Purpose:CCThasavery important role evaluating coronarydiseaseandother heartpath-ologies. Assessment of cardiac and extracardiac structures, thoracic and even abdom-inals, is essential. We analyzed incidental findings previously undiagnosed.Methods: Retrospective analysis of CCT for 36 consecutive months was performed. Awidespread field of view was obtained. Incidental findings were described and clinicalhistory reviewed to confirm associated pathology, transcendence and needing treat-ment/following.
Results: 973 CCTstudies were assessed. 298(31%) had findings different to the purposeof the study, 63 of them had been previously diagnosed. 235(24%) new findings were clas-sified in table 1. 60(6,2%) incidental findings had clinical relevance (clinical managementwas changed or required other studies): intracavitary thrombus, aortic ulcers, pulmonaryembolisms and thyroid and lung nodules (6 had neoplastic etiology).Conclusions: About a quarter of the patients sent to CCT had new diagnosis different tothe purpose of the study. Accurate analyses of all structures in the observed field is vitallyimportant when CCT is performed.
Abstract P256 Table. New incidental findings classification
Thoracic/Extracardiac (168) Cardiac/ Great vessels (50) Abdominal (17)Lungnodules(37)/Adenophaty(5) Intracavitary thrombus (11) Liver cysts (7)Small airway disease (94) Great vessels dilatation/atheroma
plaques (27)Kidney cysts (1)
Hiatal hernia (20) Pulmonary embolism (3) Ascites (2)Pleural effusion (9) Pericardial effusion (5) Aerobilia (3)Thyroid nodules (2) / Others (1) Others (4) Other (4)
P257Non invasive evaluation of silent myocardial ischemia in a group of mexicanpatients with rheumatoid arthritis and traditional cardiovascular risk factors
A. Puente1, S. Rosales2, C. Martinez1, M. Cabada1, GM. Melendez2
1National Medical Center "20 de Noviembre" ISSSTE, Nuclear Cardiology, Mexico City,Mexico; 2National Medical Center "20 de Noviembre" ISSSTE, Cardiovascular Imaging,Mexico City, Mexico
Purpose: To determine the existence of ischemia in an asymptomatic mexicanpopulation with rheumatoid arthritis (RA) and cardiovascular risk factors (CVRF), byGated-Myocardial Perfusion Single Photon Computed Tomography (g-SPECT).Methods: We analyzed the results of g-SPECT (Tc 99m mibi/1 day protocol) in 91 asymp-tomatic AR patients without previous cardiovascular diseases. Inflammatory markerslevels were quantified: hs-PCR (High Sensitivity C-reactive Protein) and VSG (GlobularSedimentation Velocity). Disease activity (DAS28 Score) and treatment were evaluated.Results: 90% were women, age 58.7 + 12 y. Activity: low in 54%, high 6%; 40% in control.CVRF: dyslipidemia 55%, hypertension 32%, tabaquism 14% and diabetes 10%. VSG26.5 +13.4, hs-PCR3.3 mg/l. Treatment:immunosuppressive 97%, biological 68% andsteroids 25%. Gated-SPECT: Normal 69 patients (76%); abnormal 22 patients (24%),mild ischemia 16 (18%), moderate 1(1%) and infarct 5 (5.%). They were grouped accord-ing post-test risk: 1) normal and mild ischemia and 2) moderate ischemia and infarct. Ana-tomic territory: left anterior descending coronary artery in 11, right coronary in 3 andcircumflex in 8 (50%,14% and 36% respectively). There was no significative correlationbetween g-SPECT results with activity disease or inflammatory markers (p=0.3);neither with the presence of CVRF (p=NS) Table 1.Conclusion: One quarter of the patients that we studied with RA have silent ischemia. Thefrequency of the CVRF is high. The existence of ischemia or infarct is independent oftraditional risk factors. The systemic inflammation of the disease may play a role in thedevelopment of atherosclerosis and the secondary ischemia.
Abstract P257 Table. Correlation of g-SPECT results and cardiovascular risk factors
Risk factor n (%) Normal or mildischemia n=85(93%)
Moderateischemia or infarctn=6 (7%)
p
Age (years) 58.7+12 58.6+11.9 59.7+14.3 0.86Gender:Female/Male
82(90)/9(10) 78(92)/7(8) 4(67)/2(33) 0.1
Diabetes 9 (10) 9(10.6) 0 1.0Hypertension 29(32) 27(31.8) 2(33.3) 1.0Dyslipidemia 50(55) 48(56.5) 2(33.3) 1.0Tabaquism 13(14) 13(15.5) 0 1.0
Abstract P256 Figure. Incidental findings in CCT
i42 Poster Session 2
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from

P258Situs inversus and Pulmonary Embolism-case report
R. Ferreira, A. Gonzaga, J. SantosCentro Hospitalar do Baixo Vouga, Cardiology, Aveiro, Portugal
Situs inversus is a relatively rare condition, with an incidence of 1 in 4 000 to 10 000 people.It has noclinical significance per sebutmay affect surgical procedures. Pulmonary embol-ism (PE) is a major cause of mortality, morbidity, and hospitalization in Europe; it is acommon but still underdiagnosed condition. The authors present the case of a78-year-old female patient, with history of diabetes, dyslipidemia and obesity; admittedon our emergency room with dyspnea and chest pain. She was immobilized for aboutone month for venous ulcer on the left calcaneus. Physical examination was dominatedby signs of arterial hypotension and shock (tissue hypoperfusion and hypoxia, includingan altered level of consciousness). The complementary study with echocardiographyrevealed right ventricle pressure overload and dysfunction (TAPSE 12mm). Her emer-gency CT angiography revealed situs inversus, repletion defect in the two main rightand left pulmonary arteries, partial extension of the thrombus to the right lobar arteriesand on segmental branches of the left inferior pulmonary lobar artery. Intravenous antic-oagulation with UFH was initiated and thrombolysis was performed with a significanthemodynamic improvement. The authors wish to emphasize that the occurrence ofsudden dyspnea or chest pain, if not explained otherwise, should alert the clinicians toconsider PE in differential diagnosis.
P259Normal SPECT MPI predicts long term event free survival in younger patients-Results from a 10 year follow-up study
S. Vijayan, SMG. Smith, M. Smith, R. MuthusamyRotherham NHS Foundation Trust, Rotherham, United Kingdom
Aim: We set out to find out the age and gender specific differences in the long term prog-nostic value of a normal SPECT Myocardial perfusion scan (SPECT MPI) in the real world.Methods: All patients who had SPECT MPIs at our institution in the year 2000 were chosenand the normal scans were identified. We analysed the case notes for major adversecardiac events which included cardiac death, acute coronary syndromes and revascular-isation by PCI or CABG. We divided the patients into groups based on their age andgender and compared the results.Results: A total of 196 patients had SPECT MPI of which 96 were normal. The mean age(SD) was 58years (9). The mean follow-up period (SD) was 142 (4) months or11 years and10 months. There were 21 deaths, of which only six were attributable to cardiac causes.The total number of MACE was 15 which gave an annual MACE rate of 1.3%.The younger group (,65 years) had 73 patients and a mean age (SD) of 54 (7) years. Theolder group (.65 years) had 23 patients with a mean age (SD) of 70 (4) years. In theyounger age group the number of MACE over the total follow-up period was 7 (annualMACE rate = 0.8%) and in the older age group the number of MACE was 8 (annualMACE rate 2.9%) (Chi square, p=0.04)Thirty three patients were males who had a mean age (SD) of 55 (9) years and 63 patientswere females with a mean age (SD) of 60 (9) years. The number of MACE and annualMACE rate were 6 and 1.5% respectively in males and 9 and 1.2 % in females (p=0.61)Conclusions: The results suggest that a normal SPECT MPI predicts long term event freesurvival better in younger patients. There was no significant difference between male andfemale patients.
P260Epicardial adipose tissue assessed by cardiac CT reflects the presence ofcoronary artery disease: comparisons with abdominal visceral adipose tissue
Y. Takeishi, M. OikawaFukushima Medical University, Fukushima, Japan
Accumulation of visceral adipose tissue is associated with a risk of coronary arterydisease. The aim of this study was to examine whether different types of adipose tissuedepot may play differential roles in the progression of coronary artery disease. A consecu-tive 174patients whounderwent both computed tomography (CT)andechocardiographywere analyzed. Cardiac and abdominal CTscans were performed to measure epicardialadipose tissue and abdominal visceral adipose tissue. Out of 174 patients, 109 and 113
patients presented coronary calcification and coronary atheromatous plaque, respective-ly. The epicardial adipose tissue and abdominal visceral adipose tissue areas were signifi-cantly larger in patients with coronary atheromatous plaque compared to those without it(P , 0.01 and P , 0.05, respectively). Interestingly, the epicardial adipose tissue area wassignificantly larger in patients with coronary calcification compared to those without cor-onary calcification (P , 0.01), whereas no difference was observed in the abdominal vis-ceral adipose tissue area between patients with and without coronary calcification.Multivariable logistic regression analysis revealed that the epicardial adipose tissuewas an independent predictor of coronary atheromatous plaque (hazard ratio 2.844,95% confidence interval 1.100–7.351, P = 0.031) and coronary calcification (hazardratio 2.653, 95% confidence interval 1.064–6.618, P = 0.036), but the abdominal visceraladipose tissue area was not. These results suggest that epicardial adipose tissue and ab-dominal visceral adipose tissue may play differential pathological roles in coronary arterydisease. Given the importance of coronary calcification, epicardial adipose tissue may bea more useful parameter than abdominal visceral adipose tissue for cardiovascular riskstratification.
P261Psychosocial risk factors innon Diabetic patients, GatedSpect findings and silentischemia
J L. Goral1, J. Napoli1, OR. Montana2, AC. Damico3, MC. Quiroz2, AE. Damico3,PJ. Forcada4, JM. Schmidberg5, NE. Zucchiatti2, DB. Olivieri31Clinica DIM, Cardiologia Nuclear, Ramos Mejia, Buenos Aires, Argentina; 2Clinica DIM,Ecocardiografia, Ramos Mejia, Buenos Aires, Argentina, Argentina; 3Clinica DIM,Ergometria, Ramos Mejia, Buenos Aires, Argentina, Argentina; 4Clinica DIM, CardiologiaPreventiva, Ramos Mejia, Buenos Aires, Argentina, Argentina; 5Clinica DIM, Arritmias yElectrofisiologia, Ramos Mejia, Buenos Aires, Argentina, Argentina
Objectives: (1) Prevalence of Myocardial Perfusion defects (MPD) 99mTcGS in non DBTpatients with Stress or Depression. (2) Findings according to presence or absence of CADprior to each group. (3) Coronary Risk Factor and sex variables.Materials and Methods:Retrospective Study of 3756 non DBT patients (p), 375p withstress (S) GA, 141p with depression (D) GB; were listed: with or without CAD (AMI,CTA, MRC) GA1: 197p, GA2: 178p, GB1: 82p, GB2: 59p respectively. The incrementalvalue of ISQ(+) in GA2/GB2, was evaluated in addition of AMI, ATC-CRM. They were com-pared with Control group: 311p (CG). The extent and severity of MPD was measured by17-segment model;(S) and (D) were assessed with questionnaires: Rahe Stress Scaleand DSM-IV.Results: Prevalence in non DBT G: (S) 9.98% (ISQ: 30.6%), (D) 3.75% (ISQ: 25.5%), withISQ + (p0.05).GA1/GB1: ISQ: p0.05 for stress; When comparing (p) with ISQ (+) A1/B1:DSS: p0.07, ISQamount: p0.07 fordepression;GA2/GB2: ISQ: pNS;Whencomparing (p)with ISQ (+); DSS: p0.07, ISQ amount: p0.07 for depression. Rest-LVSD: GA1/GB1: 3.2/2.4%, GA2/GB2:11.2/12.0%; Dilated Cardiomiopathy: GA/GB: 7.7/9.2% (pNS).Silent MAIGA1/GB1: 4/3.7%. In CRF: (D) TBQ had greater prevalence p0.05; OBS p0.01; Age: S/D:60.9y/63.9y (p0.03), at greater age, greater ISQ load and ischemic amount for depres-sion.Sex Variable: stress: M/W: ISQ: p0.001, DSS: p0.001, ISQ amount: p0.001 for M; de-pression: M/W: ISQ: p0.001, DSS: p0.05, ISQ amount: p0.05 for W. Incremental value ofISQ+ were with AMI/ MRC in GA2, and AMI to GB2Conclusions: (1) ISQ(+)PrevalenceGA1 /B1: (S) 25.3%, (D)19.5%, GA2 /B2: (S) 36.5%,(D) 33.9%. (2) Although stress has greater ISQ + prevalence, when comparing ischemicgroups, it was revealed that Gs with depression had greater ISQ load and ISQ amount,meaning these were actually worse. (3) Stress and depression had greater impact onpopulations with prior CAD. (4) Compared to CG, stress and depression lead to greaterischemia.
P262Carotid plaque predicts severity of coronary artery calcification in asymptomaticdiabetics
A. Jeevarethinam1, S. Venuraju1, A. Dumo1, S. Ruano1, R. Rakhit2, J. Davar2, D. Nair2,M. Cohen3, D. Darko4, A. Lahiri11Wellington Hospital, Clinical Imaging and Research Centre, London, United Kingdom;2Royal Free Hospital, London, United Kingdom; 3Barnet General Hospital, London, UnitedKingdom; 4Central Middlesex Hospital, London, United Kingdom
Aims: We sought to prospectively evaluate the prevalence and significance of carotidplaque in asymptomatic diabetics with or without coronary atherosclerosis.Methods: As part of a ongoing trial (PROCEED-Progression of coronary atherosclerosisin diabetics: Evaluation of the role of CTcoronary angiography and novel biomarkers ofvascular inflammation and endothelial function) a cohort of 262 asymptomatic diabeticpatients were prospectively studied. They underwent both carotid Doppler to evaluateCIMTand carotid plaque and CTcoronary artery calcium (CAC) scan.Results: The average age was 61.3+9, BMI 29.6+7 and 154 (59%) were males. Carotidplaque prevalence was 124 (47%) and mean CIMT 0.75 +0.14 mm. 194 (74%) patientshad more than 0 (zero) CAC score, of which patients with .400 Au were 57 (22%). Theprevalence of carotid plaque in patients with severe calcium plaque burden (.400 Au)was 40 (70%).On univariate analysis, age (P ,0.001), hypertension (P 0.01), gender (P 0.003) and dur-ation of diabetes (P 0.004) were significantly associated with more than 0 CAC. Carotidplaque(P ,0.0001) and mean.CIMT(P 0.002) were also significantly associated with non zero CAC score. After adjustingfor traditional risk factors, carotid plaque still show significance (P 0.02) with non zeroCAC score, odds ratio 2.59(95% CI 1.17-5.74). On binary logistic regression analysis,
Abstract P259 Fig 1.
Poster Session 2 i43
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from

prevalence of carotid plaque was very significnat (P 0.000) in predicting severe CACburden(CAC.400 Au), odds ratio 3.3 (95% CI 1.7-6.3).Conclusion: Presence of carotid plaque was a strong predictor of higher coronary arterycalcium burden in asymptomatic diabetes. The early detection of carotid plaque will helpus to further risk stratify patients from traditionally available risk scoring algorithms in pre-dicting severity of CAD.
Abstract P262 Table. Multivariate analysis for CAC.0 Au
Variable Category Odds Ratio (95% CI) P value
Age 1.32(0.43, 4.06) 0.04Gender Female 1 0.002
Male 3.33 (1.56, 7.12)Duration of diabetes 1.33 (1.04, 1.71) 0.03Carotid plaque yes 2.59((1.17. 5.74) 0.02
Multivariate analysis for CAC.0 Au: carotid plaque has a good correlation with non zero CACscore.
P263Women with normal myocardial perfusion findings have less severe, but not lessintermediate coronary artery stenoses
S. Yokota1, JP. Ottervanger1, AHE. Maas2, M. Mouden1, JR. Timmer1, S. Knollema1,PL. Jager11Isala Hospital, Zwolle, Netherlands; 2Radboud University Nijmegen Medical Centre,Department of Cardiology, Nijmegen, Netherlands
Purpose: Although myocardial perfusion imaging (MPI) is frequently used as an initialdiagnostic procedure in suspected stable angina, intermediate stenoses can be easilymissed. Particularly in women, the diagnosis is more difficult partly because they havea less obstructive pattern of coronary atherosclerosis. However, also intermediate sten-oses are of prognostic importance. We evaluated the prevalence of normal findings,and intermediate and significant stenoses in both men and women with normal MPI.Methods: Between 2006 and 2010 a total of 256 patients had normal MPI but underwentinvasive coronary angiography within 6 months because of persistent or worseningangina symptoms. Based on angiography, patients were classified in 3 groups: normal(, 30% stenosis), intermediate stenoses (30-70%) and severe stenoses (.70%). Multi-variable analyses were performed to adjust for differences in baseline variables.Results: Mean age was 63 years, 47% were women. Women were older and had moreoften hypertension. Normal coronary arteries were observed in 18%, intermediate sten-oses in 46% and severe stenoses in 36%. Prevalence of normal coronary arteries werenot different between men and women. However, males had an increased risk of signifi-cant stenoses (OR 3.2 (95% CI 1.8–5.7), whereas females had a higher risk of intermedi-ate stenoses (OR 1.9, 95% CI 1.1–3.2).Conclusions: In selected patients with normal MPI, women have less severe coronarystenoses than men as shown by coronary angiography. Women have, however, moreoften intermediate stenoses. The different pattern of stenoses in women needs a betterdefined diagnostic and therapeutic approach in clinical practice.
P264The effects of athletic training and body composition on pulmonary function indifferent type of sports
SM. Sanja Mazic1, B. Lazovic2, MDJ. Marina Djelic1, JS. Jelena Suzic Lazic3,TA. Tijana Acimovic1, MD. Milica Deleva4
1Institute of medical physiology, School of Medicine, University of Belgrade, Serbia,physiology, belgrade, Serbia; 2Clinical Hospital Center Zemun, School of Medicine,University of Belgrade, Belgrade, Serbia; 3University Hospital Center (KBC) Dr DragisaMisovic-Dedinje, Belgrade, Serbia; 4Clinical Hospital Center Zvezdara, School ofMedicine, University of Belgrade, Belgrade, Serbia, belgrade, Serbia
Introduction: It is well known and investigated cardiovascular response to exercise. Like-wise, it is observed larger lung capacity in athletes, though with less consistency. Bothsystems are involved in oxygen transport and function only together.Objective: To compare lung volumes in a sample of top male athletes who belong to thesame sport’s group (moderate static and high dynamic) and to determine which para-meters of body composition affect respiratory function.Methods: A total sample of 1068 elite male athletes were involved in study. Followingsport’s discipline were included: basketball (n=493), handball (n=285), water polo(n=252) and swimming (n=38).Measurements of spirometric parameters included vital capacity, forced vital capacity andforced expiratory volume in one second, Tiffno index, peak expiratory flow, maximal volun-tary ventilation (VC, FVC, FEV1, FEV1/FVC, PEF, MVV, respectively) and anthropometry(bodyweightandheight,percentageofbodyfatandmuscles)wereevaluated inallsubjects.Results: Respiratory parameters statistically significantly differed in all investigated group.Thehighest lungvolumeswereobserved inswimmers.Bodyweightcorrelated with respira-tory function parameters in all groupsexcept inswimmers, where therewas nosignificance.Conclusions: Results of our study may suggest further investigation in respiratory adap-tation to exercise and influence of body weight on respiratory parameters. Further inves-tigations should show if there is necessity for additional respiratory classification in sport.
P265Dynamic renoscintigraphy in the evaluation of renal function in patients withchronic heart failure
ZH. VesninaResearch Institute for Cardiology, Tomsk, Russian Federation
Aim: Radionuclide estimation of renal functional activity in patients with coronary heartdisease (CHD) complicated by chronic heart failure (HF).Materials and Methods: The study included 235 patients (220 men and 15 women, meanage 56.24 + 1.17 years) with CHD 2-4 functional classes of angina complicated bychronicHF (NYHA I-III). All thepatients underwent dynamic radionuclide renoscintigraphywith 99mTc-DTPA. Filtration and excretory renal functions, including glomerular filtrationrate (GFR), blood clearance, parenchymal and collecting system clearance half-timewere estimated.Results: Functional renal activity disorders were not identified in only 44 (18.7%) pts.However, only 57 (24.3%) patients had chronic renal disease in anamnesis, including:chronic pyelonephritis - in 32 patients, urolithiasis - in 15 patients, polycystic kidneydisease–in 6 patients, chronic renal insufficiency - in 2 patients and 1 case of renalartery stenosis and nephropathy. Decreased GFR of one or both kidneys was found in177 (75.3%) pts studied. Only 52 (22.1%) of the patients had chronic renal disease in an-amnesis. The average value of the total GFR was 105.13 + 0.68 ml/ min, for left kidney–47.60 + 0.58 ml /min, for right kidney–57.52 + 0.46 ml/min. In 49 (20.9%) pts we foundpronounced renal dysfunction (the GFR decline in one or both kidneys by more than 30%of normal values). The majority of patients (101 (43 %)) had moderate changes in the fil-tration function and manifested GFR decline by 15-30% of normal values. Minor disorders(,15%) were identified in 27 (11.5%) pts. Evacuation disorders in parenchyma werefound in 93 pts (39.6%). The disorders were mostly moderate and minor (not more than15 minutes over the normal range) (57 (24.3%) and 18 (7.7%) pts, respectively). Theexceptions were 18 patients who had a significantly delayed indicator clearance (T1/2PAR was more than 35 min).The delay in indicator excretion from pelvicalyceal systemoccurred in 65 (27.7%) cases and mostly (45 patients) it was a small extent (no morethan 6 minutes over the upper limit of normal range). In 42 out of 65 patients had nourinary system pathology in anamnesis.Conclusion: Thus, the results of radionuclide renoscintigraphy suggest that renal dys-function progresses in not less than 75% of patients with CHD complicated with chronicheart failure. The data obtained show the extensive diagnostic possibilities of radionuclidemethod in renal dysfunction detection, even at the stage when there are no clinical andbiochemical manifestations of renal disease.
P266Right ventricular ejection fraction by first pass radionuclide angiography andgated SPECT myocardial perfusion imaging in patients with heart failure: Onecenter experience
N. Zafrir, T. Bental, I. Mats, A. Solodky, A. Gutstein, Y. Hasid, D. Belzer, R. KornowskiRabin Medical Center, Beilinson Hospital, Petah Tikva, Israel
Purpose: Right ventricular ejection fraction (RVEF) is a strong predictor of adverse out-comes in patients with heart failure and LV dysfunction. RVEF can be calculated by firstpass radionuclide ventriculography (FPRNA) as part of gated SPECT MPI, used for ische-mia, scar, as well as for viability assessment. The aim of this study was to perform compre-hensive assessment of LV and RV parameters, to examine the correlation of RVEF with LVperfusion and function variables and to predict cardiac death.Methods: Patients with heart failure who were referred for gated SPECT underwentFPRNA by Tc 99m sestamibi prior to gated SPECT MPI. FPRNA was done by a dedicatedcardiac system with a general purpose collimator while gated SPECTwas done with highresolution collimator. Of the 144 patients, 124 patients with LVEF, 40% were studied.RVEF was correlated to LV variables: LVEF, LVEDV, LVESV, scar size, location of scarand phase analysis parameters .The patients were followed for cardiac death.Results: Mean age was 67+ 10, 91% men. Mean LVEF was 26%+8, mean RVEF51%+12, infarct size (score 0-4), 3.0+1.8, NYHA class 2.4+0.7 and LV dyssynchronyby phase SD was 65+19. RV dysfunction (RVEF,40%) was demonstrated in 21 (17%)patients. RVEF demonstrated significant correlation with NYHA class, LVEF, LV EDV andESV but there was no correlation with infarct size, septum scar, and LV dyssynchrony.During 285+157 days of follow up, there were 12 (9.7%) cardiac deaths. NYHA classwas the only independent predictor of cardiac death (x2 14, p=0.003) while RVEFshowed borderline significance (-0.44, p=0.07).Conclusion: RVEF by FPRNAwith gated SPECT in patients with LV dysfunction is feasibleand can be done as one stop shop. RVEF was significantly correlated with LVEF, LVEDV,LVESV and might predict cardiac death in heart failure patients.
P267Dobutamine-atropine stress echocardiography versus dipyridamole sestamibiscintigraphy for the detection of myocardial ischemia
RIM. Ben Said, N. Ben Mansour, H. Ibn Haj Amor, C. Chourabi, A. Hagui, W. Fehri,H. Hawalamilitary Hospital, cardiology, Tunis, Tunisia
Background:DipyridamoleTechnetium 99-m (Tc-99m)sestamibi singlephoton emissioncomputed tomographic (SPECT) (DMIBI) and dobutamine-atropine stress echocardiog-raphy (DASE) are common tests for the evaluation of patients with known or suspectedcoronary artery disease (CAD).
i44 Poster Session 2
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from

Aim: The aim of this study is to take an interest in cases of discrepancy between DASE andDMIBI and explore them with coronary angiography.Methods and Results: To investigate this aim we enrolled, in a prospective study, 35 con-secutive patients with cardiovascular risk factors and clinical suspicion of CAD, whounderwent DMIBI, DASE and coronary angiography.the mean age of the population was 61 +/- 10 years with a male predominance (60%).65% of patients had hypertension, 55% had diabetes and 60% had dyslipidemiaBoth tests were concordant in 43% of cases (n = 15), scintigraphy was positive whiledobutamine echocardiography was negative in 54% of cases (n = 19). Dobutamine echo-cardiography was positive while the scan is negative in one case.Patients with a discrepancy between DASE and DMIBI (n=20) underwent coronary angi-ography. the result of coronary angiography was concordant with myocardial scintig-raphy in 70% of cases(n=14).Conclusions: DASE and DMIBI were comparable tests for the detection of CAD. Themainadvantage of DMIBI was a greater sensitivity. DASE may be advantageous in patients withlower probabilities of CAD.
P268Endovascular treatment of patients with postinfarction cardiosclerosis: is italways justified percutaneous coronary intervention?
Z. Shugushev1, A. Patrikeev2, D. Maximkin1, A. Chepurnoy2, V. Kallianpur1, A. Mambetov1,G. Dokshokov1
1Peoples Friendship University of Russia (RPFU), Moscow, Russian Federation; 2CentralClinical Hospital of Russian Railways, Endovascular Surgery, Moscow, Russian Federation
Objective: To define the practicality of carrying out endovascular procedures in postin-farct cardiosclerosis patients.Methods: 147 patients were selected for the study. Criterion of inclusion: ngina 1 ectorisII–III functional class according to CCS (Canadian Cardiovascular Society); to documentconfirmation of ischemia (according to stress test), occlusion or critical stenosis in one ormany coronary arteries according to the digital angiography: presence of lesion seg-ments affecting the contractibility of left ventricular myocardium; written acknowledge-ment from the patient about being given all information about this trial. In the followingstudy 131 patients have been included who were randomized into 2 groups. In 1thgroup (n=77) endovascular intervention was carried on occlused arteries without deter-mining the viability of the myocardium. In 2nd group (n=54), endovascular interventionwas carried in cases where viable myocardium in the affected zone was determined bystress- echocardiography using Dobutamine. The results were assessed according to fol-lowing criterion: survival, frequency of cardiovascular complications (death, M.I.,repeated interventions), frequency of restenosis and thrombosis of stent, changes inlocal kinetics of myocardium.Results: All patients were implanted drug eluting stents. Endovascular intervention wassuccessfully carried out on 91,6 and 96,2% of patients respectively in both groups.Later, only 123 patients were left - 71 patients in 1 st group and 52 patients in 2 ndgroup. During hospitalization, and during 12 months of observation, no cases of cardio-vascular complications were registered. The frequency of repeated intervention on astented vessel and the earlier stented segment of artery was 2,4% in both groups.During this the frequency of thrombosis of stent, not followed by fatal M.I., consisted1,6% amongst all patients included in the study. By the end of observation, the dynamicsof local kineticswasmuchbetter in2ndgroup,nearly50% incomparison with1stgroup (p, 0,0001). It was found that there is a strong positive correlation( r=0,054, p ,0,05) inbetween the period of reperfusion in the zone of viable myocardium and the continuityof it"s hibernation.Conclusions: In patients with viable myocardium in the zone of affected kinetics, endo-vascular intervention is effective, as it helps in prophylaxis against postinfarction remod-eling of heart and worsening of heats failure, and also has positive effect heart failure, andalso has positive effect on prognosis of disease.
P269Iodine-123 metaiodobenzylguanidine cardiac SPECT imaging in nondiabeticheart failure patients qualified for an implantable cardioverter defibrillator
A. Teresinska, O. Wozniak, A. Maciag, J. Wnuk, A. Dabrowski, A. Czerwiec, J. Jezierski,K. BiernackaInstitute of Cardiology, Warsaw, Poland
Purpose: The aim of this study was to determine the value of MIBG SPECT in pts with HFqualified for ICD.Methods: This is the first stage of a prospective study comprising consecutive patientswith post-infarction heart failure (IHF) qualified (on the basis of ESC Guidelines 2012)for undergoing implantation of ICD in the prevention of sudden cardiac death (SCD),i.e. pts with LVEF≤35%, NYHA class II–III, .40 d after myocardial infarction (MI).Another inclusion criteria are: age.50y, .3 mo after possible revascularization, signedinformed consent. Exclusion criteria: allergy to iodine, diabetes mellitus. The10-min-long planar studies were performed 15min and 3,5h after MIBG injection, andwere followed by 30-min-long SPECTstudies with LEHR collimators. The image variablesused in this analysis are: late planar H/M (HMR-late) and early and late SPECTsummar-ized defect scores (SDS-early and SDS-late). SDS was assessed in a standardized17-segment model of the LV in a 5-step scale: 0-normal uptake, 4–lack of uptake. Fourty-three nondiabetic subjects were included (41 M, 2 F): age 52-85 (68+/-9)y, weight 58-120(83+/-14)kg, NYHA class 2-3 (2,2+/-0,4), LVEF 15-35 (29+/-5)%; administered activity8,3-10,4 (9,5+/-0,4)mCi.
Results: HMR-late values were: 1,12-2,11 (av.1,62+/-0,21). SDS-early values: 9-50(av.28+/- 10) and correlation with HMR-late was moderate (-0,47, p,0,009). SDS-latevalues: 8-52 (av.33+/- 11) and correlation with HMR-late was moderate (-0,56,p,0,0006).In 6/43 pts (14%, ,6-28.) the assessment of SPECTstudies was impossible because ofextremely high lung uptake non-separating from ant, ant-lat or lat LV walls.In another 16/43 pts (37%, ,24-53.) the assessment of SPECT studies was equivocalbecause of high extracardiac uptake interferring with uptake in ant or ant-lat walls (in 9pts) or in inf or inf-sep walls (in 7 pts).Altogether, in 22/43 pts (51%, ,36-66.) the SPECT quality was unacceptable or low.Conclusions: In nondiabetic pts with post-infarction HF qualified for implantation of ICD,with LVEF≤35%, NYHA class II–III and age.50y, the good-quality SPECT studies areachieved only in approximately half of cases. MIBG scintigraphy should be performedwith planar technique. SPECTcan have an additional prognostic value for improving se-lection of patients for ICD, but its value is limited by frequent non-acceptable or very fre-quent borderline-quality results caused by high extracardiac MIBG uptake interferringwith anterior, lateral or inferior LV wall.
P270Assessment of the variability of Left Ventricular Ejection Fraction (LVEF) betweensoftware algorithms in Radionuclide Ventriculography (RNVG)
J. Robinson1, J. Prosser2, GSM. Cheung3, S. Allan1, G. Mcmaster1, S. Reid1, A. Tarbuck2,W. Martin1
1Glasgow Royal Infirmary, Glasgow, United Kingdom; 2NHS Highland, Inverness, UnitedKingdom; 3University of Aberdeen, Aberdeen, United Kingdom
Purpose: Herceptin therapy of HER2+ metastatic breast cancers expose patients to acardiotoxicity risk manifested as an asymptomatic decrease in left ventricular ejectionfraction (LVEF) and heart failure. This necessitates LV function is monitored using a reli-able, repeatable and robust method. Radionuclide ventriculography (RNVG) offerssuch a tool with national guidelines recommending the use of RNVG for pre-assessmentand monitoring based on LVEF. The repeatability and reproducibility of single (1ROI) anddual region-of-interest (2ROI) methods was first assessed. Raw data was then processedusing 5 different software packages to assess whether these applications can be usedinterchangeably or whether clinically significant differences exist.Method: 20 studies were performed with repeat acquisitions. Each dataset was pro-cessed by 2 experienced operators using 2ROI and 1ROI approaches.Bland-Altman ana-lysis was used to assess level of agreement between acquisitions, operators andmethods. A further 70 studies covering a wide range of LVEF were processed using 5 soft-ware packages with Bland-Altman analysis used to assess degree of agreement betweenall software pairings.Results: Operator variability was superior for 1ROI method with a standard deviation ofthe differences of ~2% compared to ~3.3% for 2ROI. Similarly, repeatability was 5% for1ROI compared to 4.4-7.2% for 2ROI. The 1ROI technique returns a systematicallylower LVEF due to overestimation of end-systolic counts.A strongly positive correlation (r=0.85-0.94) was observed between clinical LVEF(Odyssey) and the alternative software. However, Bland-Altman plots highlight pro-nounced variability in method differences despite this correlation, particularly with theOdyssey-Link, Link-Syngo and Link-Odyssey pairings. The latter gives a 95% confidenceinterval ranging from -22.6% to 19.4%.Conclusions: The 1ROI approach is a more reproducible and repeatable method for de-termination of LVEF compared to a 2ROI technique, at the expense of systematicallyunderestimating LVEF. 1ROI techniques should be used for monitoring LVEF. However,the reduced normal range requires application of a correction factor to ensure patientsare not precluded from Herceptin therapy due to an LVEF,55, as recommended by na-tional guidelines.The variability in LVEF between packages was marked with Bland-Altman analysisshowing wide confidence intervals for all pairwise differences which indicate that thesepackages are not interchangeable. It is therefore essential that the same analysis softwareis used for longitudinal monitoring of LVEF.
P271Are there any differences of left ventricle ejection fraction as assessed by either82-rubidium-PET imaging or 99m-Tc-SPECT?
RC. Queiroz, A. Falcao, MCP. Giorgi, R. Imada, SA. Nogueira, WA. Chalela, R. Kalil Filho,WA. MeneghettiHeart Institute(InCor) Hospital das Clınicas, Faculdade de Medicina da Universidade deSao Paulo, Sao Paulo, Brazil
Introduction: Left ventricle ejection fraction (LVEF) provides additional information to theresults of perfusion studies, and it has clinical relevance because of its diagnostic andprognostic value, especially in patients with coronary artery disease (CAD).Objective: the aim of this study was to compare LVEF assessed by myocardial perfusionscintigraphy (gated-SPECT) and Rubidium82-PET (82Rb-PET) imaging.Methods: Two hundred and six patients with suspected or established CAD were ana-lyzed. Median age was 65.8+10.6 years, 108 (52.4%) male, and 98 (47.6%) female. Allpatients underwent 82Rb-PET imaging and gated-SPECT with 99m-Tc-sestamibi asso-ciated with pharmacologic stress (dipyridamole). Rest and stress-LVEF were assessedfor both methods. For the statistical analysis, the nonparametric Friedman test was used.Results:Significantdifferences were observed when comparedLVEF. Rest-LVEFwassig-nificantly lower than stress-LVEF when assessed by 82Rb-PET (55.5 + 16.5% vs. 60.6 +16.1%, respectively; p, 0.05), and stress-LVEF was lower when assessed by
Poster Session 2 i45
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from

gated-SPECT than by 82Rb-PET (57.1 + 15.8% vs. 60.6 + 16.1%, respectively; p,0.05).No significant differences were found by comparing rest-LVEFassessed by gated-SPECTor by 82Rb-PET (56.6 + 15.3% vs. 55.5 + 16.5%, respectively; p.0.05), nor in rest andstress-LVEF assessed by gated-SPECT (56.6 + 15.3% vs. 57.1 + 15.8%, respectively;p.0.05).Conclusion: The study showed that the results of stress-LVEF by gated-SPECT and by82Rb-PETwere significantly different, probably because of the time that they areassessedduring the exam. While one is performed just during the stress, the other one is assessed30 minutes after. Thus, it could have some impact in clinical management of patients withheart disease. Studies investigating the prognostic value of this finding are needed.
P272The applicationof thecardiaccycle time indicators obtainedby planerequilibriumradionuclide ventriculography in the diagnostics of diastolic dysfunction inpatients with arterial hypertension
VV. Matveev, AS. Bubyenov, VI. PodzolkovI.M. Sechenov First Moscow State Medical University, Moscow, Russian Federation
Purpose: The application of the time parameters of a cardiac cycle measured by planerequilibrium radionuclide ventriculography (PERV) in the diagnostics of diastolic dysfunc-tion in patients with arterial hypertension (AH).Method: The survey was conducted on 142 patients divided into 3 groups. Group 1: 38patients with AH stage I; average age–20,7+6,2 years; group 2: 85 patients with AHstage II, average age–58,7+10,7 years; group 3: 19 healthy volunteers average age–29,4+10,8 years. The systolic blood pressure in group 1 was 141,8+10,1 mmHg; ingroup 2–163,7+11,2 mmHg; in group 3–122,6+8,9 mmHg; the diastolic–96,2+3,9mmHg, 105,9+9,7 mmHg and 65,3+4,3 mmHg respectively. The PERV survey was con-ducted by conventional methods with a gamma-camera MB9100. Surveyed: the end sys-tolic time (EST), the duration of maximum ejection velocity (dMEV), the duration ofmaximum filling velocity (dMFV), LV (RV)–left (right) ventricle. To balance the impact ofthe heart beat rate on the time parameters, their ratios to the duration of the RR intervalwere calculated, which is shown in the percentage index (In).Result: Systolic myocardial functions reflect as EST and dMEV; while comparing theseparameters in groups 1 and 2, no significant differences were found. ESTInLV39,0+5.5vs42,0+7,7 (p=0,10), dMEVInLV 24,7+4,1vs26,2+6,1 (p=0.29), ESTInRV38,1+6,2vs41,5+7,2 (p=0,07), dMEVInRV 23,9+4,54vs25,2+5,7 (p=0,34)–compar-ing group 1 and group 3–ESTInLV 43,7+5,2vs42,0+7,7 (p=0,25), dMEVInLV25,6+3,5vs26,2+6,1 (p=0,57), ESTInRV 42,3+6,0vs41,5+7,2 (p=0,61), dMEVInRV24,8+4,4vs25,2+5,7 (p=0,74)–comparing group 2 and group 3 respectively. The para-meters of diastolic function dMFVInLV and dMFVInRV of the patients with AH stages I andII changed significantly. Thus, in the AH patients compared to group 3 a reductionof dMFVInLV 57,3+7,1vs62,4+9,6 (p=0.03) was observed and dMFVInRV57,6+9,2vs63,8+11,6 respectively, whereas in the patients with AH stage I an increaseof the mentioned parameters were observed: dMFVInLV 68,9+13,1vs62,4+9,6(p=0,04) and dMFVInRV 71,7+15,7vs63,8+11,6 (p=0,04) respectively.Conclusion: The application of the cardiac cycle time parameters according to PERVdata, adjusted to the duration of the RR interval, revealed diastolic abnormalities in thepatients with AH: an early onset of the peak in the transmitral flow, indicating an increasingvelocity of the diastolic filling, both in the left and right ventricles of the young patients withAH stage I as opposed to a slowing of the onset of dMFV, indicating diastolic myocardialrelaxation of the patients with AH stage II.
P273Three-year results of stenting of bifurcation stenoses of the left main coronaryartery: data of intravascular ultrasound study
Z. Shugushev1, D. Maximkin1, A. Chepurnoy2, V. Baranovich1, A. Faibushevich1,Y. Kolzhecova1, O. Volkova1, V. Kallianpur11Peoples Friendship University of Russia (RPFU), Moscow, Russian Federation; 2CentralClinical Hospital of Russian Railways, Endovascular Surgery, Moscow, Russian Federation
Objective: Using objective methods of intravascular imaging to evaluate the results of bi-furcation stenting stenosis of the left main coronary artery.Methods: Three-year results of endovascular treatment of patients with true bifurcationstenosis of the left main coronary artery were evaluated in 94 patients, of whom 48 patientswere using one stent technology ‘provisional - T’, and while 46 were stented ‘two stent’techniques. All interventions were conduded by final dilation by ‘kissing- balloon’ highpressure balloons and under IVUS guidence. Long-term results were assessed by follow-ing criteria: frequency of cardiovascular complications (death, myocardial infarction,re-intervention), IVUS data (residual area of vessel lumen in the proximal segment ofleft main, zone of bifurcation, the ostia of anterior descending artery and circumflexartery). Decrease in diameter in remaining lumen . 70% coas considered as criteria forrestenosis.Results: Survival amongest patients in late period was 97,9%, 2 patients died from non-cardial causes.The frequencyof cardiac events in both groups was 8.3and 4.3%, respect-ively (p 0,05). Restenosis rateaccording to IVUS in thebody trunk of the left coronary arteryand anterior descending artery Stavila 0%. Restenosis of the circumflex artery to IVUS wasfound to be 14,5% and 4.3% of cases (p 0,001). Repeated revascularization was needed in4.2 % of patients from group 1 and 2.2% in patients of group 2 (p 0,05). Stent thrombosiswas not detected in either group. The average residual area of the lumen of the left coron-ary artery in the proximal part, after "T–provisional" wasstenting 7,89+0,03, and after a fullbifurcation stenting of 8.0+0.02 mm2 (p 0,05), at the ostia of the circumflex artery5,62+0,12 and 5,98+0,01 mm2 (p 0,05), at the ostia of the anterior descending artery
6,62+0,03 and 6.78+0,04 mm2. These results did not significantly differ compared tothe same 12 months of observation.Conclusion: The study demonstrates that the use of objective methods of visualization ofcoronary arteries in patients with bifurcation stenosis of left coronary artery as a method ofmonitoring the results of stenting, as well as adequate final dilation "kissing balloons" highpressure leads to low frequency of cardiovascular complications and restenosis in long-term period,that have a positive impact on the prognosis of such patients.
(W)274Impactofcoronaryarterycalcificationonpercutaneouscoronary interventionandpost-procedural complications
R. Abazid, O. Smettei, Y. Bashir, MO. Kattea, S. Sayed, H. Sakerprince sultan cardiac center, burydah, Saudi Arabia
Background and Purpose: Excessive coronary calcification can lead to adverse out-comes after percutaneous coronary intervention (PCI). We therefore evaluated theimpact of coronary calcium score (CCS) measured by multidetector computed tomog-raphy (MDCT) on immediate complications of PCI and rate of restenosis.Methods: We performed a single-center retrospective analysis of 84 patients with coron-ary stenosis diagnosed by MDCT who underwent PCI. Agatston method was used tomeasure total, target-vessel, and segmental (stent-deployment-site) CCS.Results: In108 PCI procedures, 32 lesions (29.5%)were American College of Cardiology/American Heart Association type A, 60 (55.5%) were type B, and 16 (15%) were typeC. ANOVA showed significantly higher segmental CCS in type C than in type A lesions(214 + 162 vs 29 + 51. ; P = 0.03) respectively. Eight patients (9.5%) had periproceduralcomplications and seven (8.3%) had in-stent restenosis and angina. Mean total, target-vessel, and segmental CCS was significantly higher in complicated than in successfulPCI (199 + 325 vs. 816 + 624 [P = 0.001], 92 + 207 vs. 337 + 157 [P = 0.001], and79 + 158 vs. 256 + 142 [P = 0.003], respectively), but there was no significant differencein CCS between successful PCI and PCI complicated by late restenosis.Summary: CCS measured by MDCT has an important role in predicting early, but not late,complications from PCI.
(W)275Multicenter study of the ability of nuclear technologists and automatedquantification to determine the need for rest imaging after stress-first myocardialperfusion imaging (MPI)
W. Chaudhry1, N. Hussain1, A. Ahlberg1, P. Slomka2, M. Henzlova3, L. Duvall11Hartford Hospital, Cardiology, Hartford, United States of America; 2Cedars-Sinai MedicalCenter, Los Angeles, United States of America; 3Mount Sinai Medical Center, cardiology,New York, United States of America
Background: Stress-first MPI protocols save time and decrease radiation dose. A limita-tion is the requirement for physician review of the stress images to determine the need forrest images. Thishurdle could beeliminated if an experienced nuclear technologist and/orautomated computer quantification could make this determination. In a multicenter studywe assessed technologists’ and computer generated total perfusion defect size’s (TPD)ability to correctly identify stress-first MPI studies requiring rest images.Methods: Technologists from two academic medical centers, blinded to clinical andstress test data, prospectively completed a data form on consecutive patients who under-went stress-first Tc-99m SPECT MPI. Stress images with attenuation correction (Gd-153line source or supine and prone imaging) underwent automated quantification of thestress TPD. The technologist’s decision on the need for rest imaging and the automatedTPD were compared with the gold standard of an assessment of perfusion images by aboard certified nuclear cardiologist which included the patient’s clinical and stress testdata.Results: Of a total of 250 patients (138 female, age 61 + 11 years), 83.2% did not requirerest images. The technologists correctly classified 91.2% of patient studies compared tothe clinical gold standard. Their sensitivity, specificity, and accuracy were 66.7%, 96.2%,and 91.2%, respectively. The positive predictive value (PPV) and negative predictive value(NPV) were 77.8% and 93.5%, respectively. ROC curve analysis demonstrated that anautomated stress TPD score ≥1.2 was associated with optimal sensitivity and specificity.The computer correctly classified 72.5% of patient studies using this cut-off value. It’s sen-sitivity, specificity, and accuracy were 73.2%, 72.4%, and 72.5% respectively. The PPVandNPV were 35.3% and 92.9%, respectively.Conclusion: Technologists had a high degree of agreement with the clinical gold stand-ard with a NPVof 93.5%. Automated quantification also had a high NPV, so that utilizing anexperienced technologist and automated systems to screen stress-first images wouldenhance the laboratory workflow as well as lower total tracer dose.
P276Early gated-SPECT perfusion imaging and intraventricular synchronism inpatients with coronary artery disease
A. Peix1, LO. Cabrera1, K. Padron1, L. Rodriguez1, J. Fernandez1, G. Lopez1, E. Mena1,Y. Fernandez1, M. Dondi2, D. Paez2
1Institute of Cardiology, Havana, Cuba; 2International Atomic Energy Agency, Vienna,Austria
Purpose: To assess the value of gated single photon emission computed tomography(SPECT) in patients with coronary artery disease (CAD) by increasing the detectabilityof transient ischemic-induced systolic dysfunction early after exercise, as well as to
Withdrawn
Withdrawn
i46 Poster Session 2
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from
investigate whether this earlier post-stress acquisition could improve the detection ofischemic-induced left ventricular (LV) dyssynchrony.Methods: Ninety four patients with suspected or known CAD were included in the study.All underwent gated-SPECT two-day myocardial perfusion imaging (MPI) with twopost-stress acquisitions: 15 minutes (early) and one hour (late) after injection.Results: Fifty-fourpatientshad ischemia onMPI (Group1) and40 didnot (Group 2).Therewas no difference between summed stress score (SSS) for early and late post-stressacquisitions in either group. The reduction of post-stress left ventricular ejection fraction(LVEF) more than 5% was significantly more frequent in early post-stress acquisition inboth groups (49% vs. 20%, Group 1, and 43% vs. 11%, Group 2). More than half of thepatients in both groups showed abnormal phase-derived standard deviation (PSD) andhistogram bandwidth (HB) post-stress, and in general were more frequent in earlypost-stress acquisition (for PSD: 63% vs. 56% and 56% vs. 50%, early vs. late post-stress,Groups 1 and 2, respectively. For HB: 62% vs. 62% and 61% vs. 51%, early vs. latepost-stress, Groups 1 and 2, respectively).Conclusions: A gated-SPECT protocol with early acquisition of post-stress imaging isfeasible and useful to analyze better left ventricular function in coronary artery diseasepatients. Furthermore, differences between post-stress and rest intraventricular syn-chronism can also be detected.
P277The addition of coronary calcium score to stress myocardial perfusionscintigraphy increases confidence in identifying normal perfusion in patientsreferred to a stable chest pain clinic
CJT. Butcher1, E. Reyes2, MB. Al-Housni1, R. Green1, H. Santiago1, F. Ghiotto1,S. Hinton-Taylor1, A. Pottle1, M. Mason1, SR. Underwood3
1Harefield Hospital, Cardiology, London, United Kingdom; 2Royal Brompton Hospital,London, United Kingdom; 3Imperial College London, London, United Kingdom
Purpose: Myocardial perfusion scintigraphy (MPS) is widely used for the diagnosis of ob-structive coronary artery disease (CAD) in patients with intermediate to high likelihood ofdisease. As with other techniques, artefact can confound interpretation. This is usually ap-parent from a comparison of stress and rest images but the resting image increases radi-ation exposure and the duration of the test. X-raycomputed tomography coronary calciumscore (CCS) can also aid diagnosis, especially in low likelihood patients by virtue of itshigh negative predictive value.We reviewed patients referred to a stable chest pain clinic to see if the addition of CCS tostress MPS increased confidence in reporting perfusion as normal, hence reducing theneed for a resting image. We also investigated if CCS alone was sufficient to exclude ab-normal MPS in the same cohort.Methods: Patients referred to a stable chest pain clinic between January 2012 andJanuary 2013 and who underwent both CCS and MPS were reviewed. The stress MPSstudy was viewed with the clinical history and categorised as "normal, no rest imagerequired", "likely normal but rest image required" and "abnormal, rest image required".On a separate occasion the same stress MPS was viewed with the clinical history andCCS.Results: There were 43 patients (17 male, mean age 66.8 SD 9.4 years). 82% had pre-testlikelihood of CAD 10-90% with none being ,10%. CCS ranged from 0-1380 (mean 201,SD 370). From stress MPS alone 13 patients did not require a rest image and with the add-ition of CCS this increased to 23 (P=0.03). Similarly, the number of patients thought likelyto be normal but requiring a rest scan reduced from 22 to 10 (P=0.007). Of the 19 patientswith CCS,10 21% had an abnormal stress MPS (p=0.03).Conclusions: In patients with .10% likelihood of CAD investigated for chest pain, theaddition of CCS to stress MPS increased confidence in identifying normal myocardial per-fusion and reduced the number of rest MPS studies required. However, CCS ,10 did notexclude abnormal MPS. CCS could therefore reduce the need for rest MPS, and reduceradiation burden, time and cost in this population.
P278Comparison of dyssynchrony parameters obtained by simultaneous acquisitionwith 8 and 16 frames/cycle in Gated SPECT myocardial perfusion (GSPECT)
I. Casans Tormo1, R. Diaz-Exposito1, E. Plancha-Burguera2
1Nuclear Medicine. Hospital Clınico Universitario., Valencia, Spain; 2Cardiology, HospitalFrancisco de Borja, Gandia, Spain
Purpose: To assess the influence of 8 and 16 frames/cycle acquisition in dysynchronyparameteres obtained by phase analysis of GSPECTand also the possible relation withleft ventricular ejection fraction (LVEF) value.Material and Methods: We have studied a group of 30 consecutive patients, mean age65+10 with known or suspected CAD, submitted to detect possible myocardial ischemia.GSPECTwere performed 1h after injection of a 99mTc-tracer (2 day-protocol, 20 mCi-70kg), obtaining 2 simultaneous acquisitions with 8 and 16 frames (64x64 matrix) in eachstudy (OSEM recontruction, no attenuation correction), with asessment of LVEFand para-meters of phase analysis (peak phase (PP), standard deviation (SD), histogram band-width (B), skewness (S) and kurtosis (K). We evaluated a total of 60 acquisitionsobtained at stress study in all patients by ECToolbox.Results: Mean values of LVEF (55.06+11.03, 24-79%), PP8 (134.16+18.02, 112-180),PP16 (144.9+18.9, 119-209), B8 (76.9+57.5, 27-262), B16 (56.5+35.0, 18-166), S8(4.14+0.87, 2.80-6.20), S16 (3.53+0.93, 1.47-5.34), K8 (20.09+10.42, 3.5-50.0), K16(14.0+7.29, 1.83-30.6). Considering all patients we found significative differencesbetween 8 and 16 frames acquisitions in PP (mean difference –10.7+11.8, p: .0001), B(20.3+43.6, p: .01), S (0.61+0.85, p: .001), K (6.09+11.43, p: .007). There were 17
patients with LVEF ≥ 55% (55-79, 61.8+7.2) and 13 with LVEF , 55% (24-54,46.2+8.7). Only PP (-10.4+8.4, p: .0001) showed significative differences between 8and 16 frames acquisitions in patients with LVEF ≥ 55%, while we found significative dif-ferences in PP (-11.1+15.5, p: .02), S (0.87+0.84, p: .003) and K (9.6+10.4, p: .006) inthe patients with LVEF,55%.Conclusion: In this study with simultaneous GSPECTacquisition in 8 and 16 frames/cyclein a group of coronary patients, we obtained significative differences in parameters ofphase analysis, especially in patients with LVEF ,55%, a factor that should be consideredin cardiac dyssynchrony evaluation by GSPECT with different acquisition modes.
P279Additional role of wall motion assessment by 99mTc-sestamibi gated SPECT inpatients with coronary artery disease. Comparison with restingechocardiography
K. Elsaban1, HIJJI. Alsakhri21al-hada armed force hospital, radiology, taif, Saudi Arabia; 2Al-Hada Military Hospital, Taif,Saudi Arabia
Background: (ECG)-gated SPECT is a currently well accepted technique in the evalu-ation of left ventricular function, particularly in the assessment of wall motion. Yet, weand other noticed some differences in WMS assessed by both resting echo. and stressgated SPECT in spite of being late.Aim of the Study: comparison of wall motion findings in both stress gated SPECT andresting echocardiography and studying the impact of perfusion changes on this wallmotion.Patients and Methods: 30 patients with well diagnosed CAD had been subjected to bothresting echocardiography (ECHO) and two-day stress-rest gated SPECT Sestamibi(GSPECT) and using 17 segment model and scoring 1 for normal and 5 for dyskinesiafor wall motion score and perfusion score (0 for normal, 1 for reversible perfusion defectand 2 for fixed perfusion defect).Results: Concerning detection of normal and abnormal wall motion (WM), there was highdegree ofagreement (84.1%),P,0.001 betweenboth techniques. However, to assess ac-curately degree of matching between both techniques using correspondence of wallmotion score, agreement was significantly decreased to 64.4%, &P,0.05 with corres-pondence of WMS 1 in echo to be 1.3+0.7 in GSPECT, 2 to be 2.9+0.8, 3 to be3.2+0.8 and 4 to be 3.9+0.8. This was explained by observation of :out of 361 segmentswith WMS 1 in echo 24 segments showed perfusion defects (reversible and fixed) whichcaused abnormal WM in GSPECT, in WMS (2) 46 perfusion defects caused higher scoresin GSPECT, in WMS(3) 24perfusion defects caused higher WMS in GSPECTwhile inWMS(4) (akinesia) no major difference in both perfusion and WMS in both techniques. Conclu-sions: Wall motion abnormality by gated SPECT is more informative in detection of loca-lized stunning caused by localized myocardial perfusion.
P280Comprehensive assessment of impaired coronary and peripheral artery vascularfunction in smokers using Oxygen-15 Labeled Water PETand Brachial ArteryUltrasound
K. Yoshinaga1, N. Ochi2, Y. Tomiyama1, C. Katoh3, M. Inoue2, M. Nishida2, E. Suzuki1,O. Manabe1, YM. Ito1, N. Tamaki11Hokkaido University Graduate School of Medicine, Sapporo, Japan; 2HokkaidoUniversity, Hospital, Sapporo, Japan; 3Hokkaido University, Faculty of Health Sciences,Sapporo, Japan
Background: Cigarette smoking has impact on vascular function. Comprehensive evalu-ation of endothelial dependent (End) and endothelium independent (Endind) vascularfunction in coronary artery and peripheral artery in smokers has never been studied.The purpose of the present study was to evaluate the relationship between the coronaryand peripheral vascular function in smokers using O-15 labeled water PETand brachialartery ultrasound.Methods: Eight active smokers (Brinkman index: 219.4+230.7) and 10 healthy indivi-duals underwent brachial artery ultrasound at rest, reactive hyperemia [250 mmHg cuffocclusion (FMD)], and sublingual nitroglycerin (NTG) administration. Delta arterial diam-eter and %change of arterial diameter were calculated. Myocardial blood flow (MBF) wasevaluated at rest, during adenosine triphosphate (ATP) administration, and cold pressortest (CPT) with O-15 water dynamic PET. Rest MBF and CPT MBF were corrected by ratepressure product (RPP).Results: Smokers significantly reduced End vasodilatation compared to control usingultrasound (delta FMD: 0.31+0.12 mm vs 0.44+0.11 mm, P=0.026, %FMD:6.62+2.28% vs 11.29+2.75%, P=0.0014) and using O-15 water PET (RPP correctedCPTresponse: -18.0+10.1%vs 1.4+20.3%,P=0.04).There wasnosignificant differencein NTG response (delta:0.73+0.30 mm vs 0.88+0.25 mm, P=0.27, %NTG: 15.9+6.8%vs 22.4+6.2%, P=0.055) and RPP corrected coronary flow reserve (3.19+1.22 vs3.77+1.14, P=0.32) between the two groups. On the other hand, there was no relation-ship between coronary and peripheral End function (R=0.40, P=0.1) and Endind vascu-lar function (R=0.24, P=0.3).Conclusions: Smokers exhibited impaired coronary endothelial function as well as per-ipheral endothelial function. In contrast, smokers did not show alteration in endothelial in-dependent vasodilation. Inaddition, therewasnocorrelation betweenPETandultrasoundmeasurements, possibly implying that while smokers may have systemic vascular endo-thelial dysfunction, the characteristics of that dysfunction may be different in coronary andperipheral arteries.
Poster Session 2 i47
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from

P281A rare report on exceptional case of massive pericardial effusion diagnosedincidentally on myocardial perfusion imaging
A. Tahilyani, FAHIM. Jafary, HH. Ho Hee HwaTan Tock Seng hospital, Cardiology, Singapore, Singapore
Background: We report a case of the incidental identification of pericardial effusion onmyocardial perfusion scan. There are various studies suggested to target the issues ofsensitivity and specificity of MIBI scans for the assessment of pericardial effusions bothqualitative and quantitative aspects.An echocardiogram was performed in patient with road traffic accident with atrial fibrillation,which demonstrated mid inferoseptal and apical hypokinesia and on further evaluation withperfusion scan it revealed a swinging type of motion with fluid collection around the heart.Method: Myocardial perfusion scan was done as outpatient to asses ischemic burden,given the hypokinetic segment on echocardiogram, which revealed unusual "swinging"type of motion and there is a lucent space around the heart suggestive of a fluid collection.A small mild area of perfusion defect is seen in the lateral wall, which corrects with proneimaging, suggestive of attenuation. No stress induced cavity dilatation is seen.Result: Diagnosis of pericardial effusion was thus confirmed on MIBI scan. Interestingpart is to see cardiac swinging image and pericardial effusion on perfusion scan.Discussion: There are very few case report and very little is known about the role of boththallium and technetium-99m-based myocardial perfusion imaging in diagnosis incidentalpericardial effusion and useful information can be provided in diagnosing this condition.The echocardiogram remains the gold standard for diagnosis of pericardial effusion.However computerized tomography and magnetic resonance imaging scan are com-monly performed procedure that could detect incidental pericardial effusion.
P282The evaluation of left ventricular dyssynchronization in patients withhypertension by phase analysis of myocardial perfusion gated spect
S. Ozdemir, B. Kirilmaz, A. Barutcu, YZ. Tan, F. Celik, S. SakgozCanakkale Onsekiz Mart University, Canakkale, Turkey
Purpose:Hypertension may lead left ventricularmechanical dyssynchrony characterizedby delayed activation of certain ventricular leading to uncoordinated contraction. The aimof this study was to evaluate the prognostic value of left ventricular dyssynchrony mea-sured by phase analysis of myocardial perfusion gated single photon emission computedtomography (SPECT) imaging in patients with hypertension.Methods: We retrospectively reviewed the records of patients who were referred to ourinstitution for myocardial perfusion scintigraphy with a diagnosis of coronary arterydisease. In total 147 patients (mean age of 57.97 + 10.80 years) with and without hyper-tension (91 and 56, respectively) were included in the present study.Results: There were statistically significant difference in histogram bandwidth para-meters of phase analysis between the patients with and without hypertension groups(p,0.001).Conclusion: Phase analysis can be considered as a reliable method for early detection ofleft ventricular dyssynchrony in hypertensive patients.
Phase Analysis Parameters Patients † p-value
Case group(with hypertension)(n=91)
Control group(without hypertension)(n=56)
Phase StandardDeviation(PSD)
Mean 14.23 12.12 0.012SD+ 6.04 4.40Median 13.02 11.44Minimum 4.70 5.90Maximum 46.37 28.86
Phase HistogramBandwidth(PHB)
Mean 41.70 35.03 p,0.001SD+ 10.49 7.75Median 41 34.50Minimum 26 23Maximum 67 52
Left VentricularMass Weight
Mean 119.37 111.16 p,0.001SD+ 14.19 9.46Median 119 113Minimum 94 88Maximum 170 137
Myocardial perfusion gated phase analysis parameters and electrocardiography parametersin patients with and without hypertension.
P283Gated-SPECT ischemia in left anterior descending coronary artery territorysecondary to myocardial muscular bridges
M. Cabada Gamboa1, A. Puente Barragan1, N. Morales Vitorino2, MA. Medina Servin2
1National Medical Center 20 de Noviembre, Nuclear Cardiology, Mexico City, Mexico;2National Medical Center 20 deNoviembre, Interventional Cardiology, Mexico City,Mexico
Purpose: To demonstrate that the presence of a muscular bridge Itself does not producesignificant ischemia measured by gated SPECT.
Methods: We analyzed myocardial perfusion ischemia detected by gated-SPECT(g-SPECT), one day protocol (Rest-Stress/Tc99m tetrofosmin) in 24 patients with muscu-lar bridges in the left descending coronary artery (LDCA), diagnosed by coronary angiog-raphy. Gated-SPECTwas acquired in a Ventri GE gamma camera, using Emory Toolboxprogram.Results: 87.5% were males. The patients were divided in 2 groups: 1) With muscularbridges and atherosclerosis coronary lesions .70% (n=7) and 2) With only muscularbridges (n=17). There were no comorbidity differences between both groups.Gated-SPECT evidenced moderated to severe myocardial ischemia predominantly ingroup 1 patients (p=0.03). Table 1.The risk to present myocardial ischemia was more in group 1 than in group 2 (OR 2.5, IC1.79-7.89 p= 0.03 vs. OR 2.0, IC 0.61-6.49, p= 0.17).Bivariate analysis demonstrated a significant correlation between the g-SPECT myocar-dial moderate to severe ischemia with the presence of significative atherosclerosis coron-ary lesions .70% (rs=0.47; p=0.01) and the bridge localization in the medial portion ofthe LDCA (rs=0.68; p=0.001); there were no correlation with the severity (.50%) of theLDCA muscular bridge occlusion (rs=0.29; p=0.16).Conclusion: The only presence of a muscular bridge doesn’t have correlation with signifi-cant myocardial ischemia (moderate/severe) regardless of their percentage of occlusion.The muscular bridge localization in the middle segment of LDCA and the existence ofsignificant atherosclerosis lesions were risks factors for the presence of significativeischemia.
Abstract P283 Table. LDCA lesions(.70%) and muscular bridge
Variable Muscular bridge +LDCA lesion
Muscular bridge p
Modarate -severe ischemia 4 (57.1%) 2 (11.7%) 0.03% of muscular bridge oclusion 48.5 + 16.7 49.1 + 20.3 0.60Muscular bridge oclusion ≥50% 4 (57.1%) 10 (58.8%) 0.64Proximal bridge localization* 4 (57.1%) 6 (35%) 0.29
P284Theabsolutemyocardialbloodflowdeterminedbydynamiccardiac13N-NH3PETis influenced by the partial volume effect
C. Hindorf1, S. Akil2, F. Hedeer2, J. Jogi2, H. Engblom2
1Skane University Hospital, Radiation Physics, Lund, Sweden; 2Lund University, Clinicalphysiology and nuclear medicine, Lund, Sweden
Aim: The absolute myocardial blood flow (MBF) is determined from dynamic cardiac PETstudies. The activity in blood as function of time is one of the input functions when the MBFis calculated. The quantification of the activity in blood is therefore crucial for the MBF as-sessment. The aim of this project was to investigate the impact of different positions of leftventricular (LV) blood pool volume of interest (VOI) on quantification of absolute MBF inpatients and by phantom experiments.Methods: Five patients previously diagnosed with coronary artery disease performedcardiac PET with 13N-NH3 at rest and in stress before and after PCI (20 cardiac PETstudies). An acquisition in dynamic mode was performed during the first four minutes(12 images of 10 s, 2 images of 30 s and 1 image of 60 s) after administration of 550MBq of 13N-NH3. The VOI to quantify the activity in the myocardial wall (epicardial andendocardial borders) from the dynamic studies was kept constant for each study whilstthe activity in the blood was quantified within three different VOIs drawn within the LVblood pool: 1) small basal VOI 2) small apical VOI and 3) large VOI extending from baseto apex of the LV. The absolute MBF was determined by the deGrado model within theCarimas software (Turku, Finland) for the three blood pool VOIs. The MBF as determinedwith the three VOIs (MBFbasalVOI, MBFapicalVOI, MBFLVVOI) was normalized to theMBFbasalVOI.The myocardial wall in a cardiac phantom was filled with 13N-NH3 to evaluate the influ-ence of the partial volume effect on the quantified activity in the ventricular lumen. The ac-tivity was determined with the three VOIs previously described.Results: The ratio MBFapicalVOI/MBFbasalVOI was 1.27 (median; range 1.0–1.72) andthe ratio MBFapicalVOI/MBFbasalVOI was 1.11 (median; range 0.97–1.36). Thephantomstudy showed that 16% of the activity in the myocardial wall is detected for a small apicalVOI, 14% for a LV VOI and 5% for a small basal VOI despite the absence of activity in theventricular lumen.Conclusions: The absolute myocardial blood flow determined with dynamic cardiac13N-NH3 PET is dependent on VOI position, probably due to partial volume effects,and should therefore be kept constant, preferably in the basal part of the LV blood pool,to enable accurate comparisons between examinations and patients.
P285Cold pressor test as stress test in myocardial perfusion studies evidences higheramount of ischemia in patients with intermediate coronary lesions
VD. Martire, ER. Pis Diez, MV. Martire, DO. PortilloCESALP. Fundacion Horacio Corrada, La Plata, Buenos Aires., Argentina
Background: There is no knowledge of the best stress test causing myocardial ischemiain patients (P) with intermediate coronary lesions (. 30 %–,70 %) (ICL) where multiple
i48 Poster Session 2
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from

vascularmechanisms are involved and whicharedifferent fromthe classical flow limitationdiagnosed with the conventional treadmill test (ST) in severe lesions (.70%).Objective: To assess whether ST or the cold test (CT) is a better stress test to evidencemyocardial perfusion defects using gamma camera (SPECT) and the magnitude of theof them in this group of P.Method:Afollow-up studyhas been doneon96P,56 females and40males, aged59+8.4years old, all ICL-diagnosed (1.8+0.4 lesions/patient), 70/96 using digital CACG, 26/96using multi-slice CT, with indication of SPECT for risk stratification in ischemia. All Preceived the perfusion study with each of the stress tests under the same treatment andclinical conditions, with an interval shorter than 10 days between each. The following para-meters were analyzed for this sample: 1- ROC curve (comparison between two operatingcharacteristics) and 2- quantification and magnitude of induced ischemia by summed dif-ference score (SDS).Result: Both stress tests presented a ROC curve of similar diagnosis to evidence perfu-sion defects in coronary territories affected by ICL. In the SDS analysis the CTevidencedan amount of ischemia significantly higher for the same territory (Fig. 1).Conclusion: In P with intermediate lesions, with both stress tests ischemic perfusiondefect is diagnosed in the same way. However, the CT evidences higher magnitudethrough microvascular and endothelial dysfunction mechanisms, providing valuablephysiopathological information of significant clinical and therapeutic impact.
P286Quantitative perfusion parameters in a cohort of patients with no known ischemicheart disease and normal myocardial perfusion imaging studied by 82Rb-PET
CM. Hoff, A. Balche, J. Majgaard, LP. Tolbod, HJ. Harms, K. Bouchelouche, J. Soerensen,J. Froekiaer, LC. GormsenAarhus University Hospital, Dept. of Nuclear Medicine and PETcenter, Aarhus, Denmark
Purpose: 82Rb perfusion PET allows for visual as well as quantitative interpretation ofmyocardial function. Whereas visual interpretation relies on intra-individual redistributionof the tracer between rest and stress studies, quantitative interpretation of absolute flowvalues requires robust knowledge of reference values in the patient population. Onlyfew studies have reported normal ranges of myocardial perfusion obtained by 82RbPETand it was therefore our goal to establish these values.Methods: Three hundred and thirty patients with chest pain or dyspnea examined by82Rb-PET during a 6-month period were screened for eligibility. One hundred andeighty patients with no prior history of ischemic heart disease, a normal MPI scandefined by visual interpretation and no coronary events for a follow-up period of 6months were included as normal. Quantitative parameters were calculated using com-mercially available software (QPET, Cedars Sinai). Parameters included were regionaland global rest and stress myocardial blood flow (MBF) values, ejection fraction (EF)and total perfusion deficit (TPD).Results: Mean global MBF at stress was 2.92 mL/g/min (+SD 0.49), lower limit (LL) 1.94mL/g/min.Regional mean MBF at the apex was 2.83 mL/g/min (+SD 0.61), LL 1.61 mL/g/min, infer-ior wall 2.96 mL/g/min (+SD 0.56), LL 1.84 mL/g/min, lateral wall 3.10 mL/g/min (+SD0.62), LL 1.86 mL/g/min, anterior wall 2.83 mL/g/min (+SD 0.53), LL 1.77 mL/g/minand septal wall 2.88 mL/g/min (+SD 0.51 mL/g/min), LL 1.86 mL/g/min.Global coronary flow reserve (CFR) was 2.81 (+SD 0.71). EF at rest was 65.3% (+SD 10)and during stress 69% (+SD 12.3), yielding an EF reserve of 4.5%. TPD at rest and stresswas 6% (+SD 4).Conclusion: Based on a representative population of patients in which coronary arterydisease was ruled out, we propose the following lower cut-off points for MBF normalrange(mL/g/min):global2,apex1.6, septum1.8,anteriorwall1.8, lateralwall1.8and inferiorwall 1.8. CFR had a wide range reflecting large variability in resting flow rates indicating that
CFR should be interpreted with caution. In line with this, TPD calculated from software pro-vidednormalmaterialalsogenerateda toovariableparameter tobeusedinaclinicalsetting.
P287Prognostic impact of location and extent of vessel-related ischemia (VRI) atmyocardial perfusion scintigraphy in patients with or at risk for coronary arterydisease
F. Nudi1, G. Neri1, E. Procaccini1, A. Pinto1, M. Vetere1, G. Biondi-Zoccai21Madonna della Fiducia Clinic, Service of Nuclear Cardiology, Rome, Italy; 2SapienzaUniversity of Rome, Department of Medico-Surgical Sciences and Biotechnologies,Latina, Italy
Aim: We aimed at comparing the prognostic outlook of patients undergoing myocardialperfusion scintigraphy (MPS) according to the site of ischemia, with specific focus on leftanterior descending (LAD) involvement.Methods: Our institutional database was queried for subjects undergoing MPS, withoutmyocardial necrosis or recent revascularization. We focused on the prognostic impactof location of vessel-related ischemia (VRI) at MPS. The primary outcome was the long-term rate of cardiac death or myocardial infarction (CD/MI).Results: A total of 13,254 patients were included. Moderate or severe VRI occurred in2,627 (20%) patients, with 4 different and mutually exclusive types of VRI: LAD single-VRI,non-LAD single-VRI, LAD two- or three-VRI, and non-LAD two-VRI. Clinical outcomes at1-year and long-term (32+20 months) follow-up were significantly different among thegroups of patients with moderate or severe VRI, including death, cardiac death, non-fatalmyocardial infarction or their composites (p,0.001 for all comparisons). In most casespatients with LAD two- or three-VRI had the highest event rate, followed by subjects withLAD single-VRI, in comparison to those without LAD involvement. Such results were con-firmed at multivariable analysis. In addition, substantial concordance between VRI andangiographic evidence of significant disease was found in subjects undergoing coronaryangiography after MPS.Conclusions: Location and extent of myocardial ischemia at MPS according to the VRIconcept have a hierarchical prognostic impact, with LAD two- or three-VRI and LAD single-VRI proving worse than non-LAD two-VRI and non-LAD single-VRI.
P288Influence of left bundle branch block in assessment of coronary flow fromrubidium-82 PET imaging
A. Falcao, WA. Chalela, MCP. Giorgi, R. Imada, J. Soares Jr, R. Do Val, MA. Oliveira,R. Kalil Filho, JC. MeneghettiHeart Institute(InCor) Hospital das Clınicas,Faculdade de Medicina da Universidade deSao Paulo, Sao Paulo, Brazil
Background:Perfusion defects are frequent in myocardial scintigraphy in thepresence ofleft bundle branch block (LBBB). However, scarce studies show decreased coronary flowreserve (CFR) in the left anterior descending artery territory, regardless of the presence ofcoronary artery disease (CAD). We sought to investigate rubidium-82 positron emissiontomography myocardial perfusion imaging (Rb82-PET) in the assessment of myocardialblood flow (MBF) and CFR in LBBB patients.Methods: Forty one patients with LBBB, median age 63 years, 23 (56.1%) female wereanalyzed. CAD was defined as 1 50% luminal narrowing (LBBB-CAD; n=12); and no evi-dence or normal Rb82PETstudies was denominated LBBB-non CAD (n= 29). All of themunderwent rest and dipyridamole stress Rb82PET with absolute quantitative flow mea-surements in the anterior, septal, lateral, inferior and apical walls (mL/min/g). Rest andstress images were visually analyzed for relative myocardial perfusion according to thestandard 17 segment (AHA model), as well as left ventricle ejection fraction (LVEF).These parameters were compared to those obtained from 30 matched patients (controls)with normal studies and without LBBB.Results: Rest and stress MBF and CFR were significantly lower in LBBB patients than incontrols in all the walls (p,0.05). On the other hand, LBBB-CAD patients showed signifi-cantly lower CFR compared to LBBB non CAD (1.94 x 2.59mL/g/min; p=0.04). Compari-son of the anterior or the septal with the other walls revealed that stress flow weresignificantly lower in the anterior than in the septal wall, in both groups (p,0.05). Perfusionabnormalities in all but anterior and septal walls, were more prevalent in LBBB-CADpatients (30.70% x 3.80%; p,0.05), as well as LVEF , 45% (66.70% x 42.30%; p,0.05).Conclusion: LBBB patients showed decreased MBF and CFR, regardless of the pres-ence of CAD, probably due to the detrimental influence of LBBB over the ventricular dy-namics. In addition, the presence of CAD had a negative impact on CFR assessed byRb82PETand may be useful to identify CAD in LBBB patients.
Abstract P285 Figure.
Abstract P287 Table. Long-term events acccording to VRI
No VRI(N=5,340)
Minimal or mildVRI (N=4,604)
Moderate or severe VRI PSingle-VRI Two- or three-VRI
LAD involved (N=287) LAD not involved(N=560)
LAD involved (N=158) LAD not involved(N=286)
Death or myocardial infarction 93 (1.7%) 130 (2.8%) 24 (8.4%) 31 (5.5%) 26 (16.5%) 21 (7.3%) ,0.001Cardiac death or myocardial infarction 68 (1.3%) 78 (1.7%) 19 (6.6%) 23 (4.1%) 20 (12.7%) 16 (5.6%) ,0.001Death 41 (0.8%) 84 (1.8%) 13 (4.5%) 22 (3.9%) 20 (12.7%) 12 (4.2%) ,0.001Cardiac death 16 (0.3%) 32 (0.7%) 8 (2.8%) 14 (2.5%) 14 (8.9%) 7 (2.4%) ,0.001Non-fatal myocardial infarction 52 (1.0%) 46 (1.0%) 11 (3.8%) 9 (1.6%) 6 (3.8%) 9 (3.1%) ,0.001
Poster Session 2 i49
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from

P289Treatment with anti-RAGE antibody improves hind limb angiogenesis and bloodflow In diabetic mice with left femoral artery ligation
Y. Tekabe1, T. Anthony1, Q. Li1, AM. Schmidt2, L. Johnson1
1Columbia University Medical Center, New York, United States of America; 2New YorkUniversity, New York, United States of America
Purpose: Receptor for Advanced Glycation Endproducts (RAGE) plays an important rolein the development and progression of vascular disease and inhibits the angiogenic re-sponse to limb ischemia particularly in diabetics. We developed a murine monoclonalantibody to a unique peptide sequence on extracellular domain of RAGE which showedblocking properties. The purpose of this study was to investigate if treatment with this anti-body will improve the angiogenic response to hind limb ischemia following femoral arteryligation in diabetic mice compared to vehicle treated diabetics and that this difference canbe detected on in-vivo SPECT imaging.Methods: Twenty streptozotocin treated C57BL/6 mice (6 weeks of age) received eithermurine monoclonal anti-RAGE F(ab′)2 (100 mg thrice weekly) (n=10) or vehicle (n=10)for 9 weeks. Diabetic plus control nondiabetic C57BL/6 mice (n=10) underwent leftfemoral artery ligation and 5 days later angiogenesis imaging with 99mTc-Arg-Gly-Asp(RGD) (12.2+2.8 MBq) and nanoSPECT/CT. ROIs were drawn around uptake of radiotra-cer inbothhind limbsandquantifiedas %injected dose(ID).Twenty-fourdays later,an indexof hind limb blood flow was measured with ultrasound, mice euthanized, and muscles fromboth hind limbs were excised for histological and immunohistochemical characterization.Results: Radiotracer uptake in the ischemic limbs was visibly more in the antibody treatedcompared to vehicle treated and supported by the quantitative results for %ID: (3.1+1.4vs. 1.68+0.35; P=0.02) and at day 24 blood flow (pulsatility index) higher (1.49 + 0.5 vs.0.61+0.39, P=0.04). The mean blood glucose levels ranged from 275 to 375 mg/dL fortreatment and control groups (P=0.4). Quantitative immunohistological analysisshowed treatment with RAGE antibody significantly decreased RAGE expression andincreased capillary density in the ischemic hind limbs compared with vehicle treated dia-betic ischemic hind limbs (P=0.03 and 0.001, respectively).Conclusion: These results suggest a potential clinical strategy for treating PAD and mon-itoring therapeutic results.
P290Detection of increased myocardial integrin alphaVbeta3 expression in a pigmodel of inducible myocardial ischemia using [68Ga]-NODAGA-RGD PET
M. Groenman1, M. Tarkia1, M. Kakela1, P. Halonen2, T. Kiviniemi3, M. Pietila3,S. Yla-Herttuala2, J. Knuuti1, A. Roivainen1, A. Saraste3
1Turku PET Centre, Turku, Finland; 2A.I. Virtanen Institute for Molecular Sciences, Kuopio,Finland; 3Turku University Hospital, Heart Center, Turku, Finland
Purpose: Increased integrin avb3 expression can be detected by radiolabeledarginine-glycine-aspartic acid (RGD) peptides in the myocardium after an acute myocar-dial infarction (MI). However, RGD uptake in chronic myocardial ischemia is unknown.Therefore, we studied the feasibility of non-invasive imaging of integrin avb3 expressionwith the use of 68Ga-NODAGA-RGD PET in a pig model of chronic flow-limiting stenosisinduced by a bottleneck stent.Methods: A flow-limiting bottleneck stent was implanted under fluoroscopy guidance in theproximal left anterior descending (LAD) artery of 11 Finnish landrace pigs ageing 12 weeks.Antithrombotic therapy was used to prevent stent thrombosis. After 1 week, myocardial perfu-sion was evaluated by 15O-water PETat rest and during adenosine-induced stress. Ischemicarea-at-risk was defined as perfusion defect (,70% of maximum) during adenosine-inducedstress. A 60-min PET study was performed after injection of 300+31 MBq of 68Ga-NODAGA-RGD. Then, the heart was sliced and based on triphenyltetrazolium chloride(TTC) staining, tissue samples from the viable and non-viable myocardium at the ischemicarea-at-risk were obtained for ex vivo measurement of tracer uptake and autoradiography.Results: Eight pigs had ischemic area-at-risk (average area 19 % of the left ventricle) basedon PET perfusion imaging during adenosine-induced stress. In 5 of these, there was also aresting perfusion defect (average area 45% of the ischemic area-at-risk) where TTC showednon-viable myocardium. In PET imaging, myocardial 68Ga-NODAGA-RGD uptake washigher in the ischemic area-at-risk than in the remote myocardium (ischemic-to-remoteratio 1.45+0.26; p=0.004). ). To further asses the location and mechanism of the68Ga-NODAGA-RGD accumulation, ex vivo analyses were performed separately for theviable and non-viable myocardial regions inside the ischemic area-at-risk. The highest68Ga-NODAGA-RGD uptake was found in the damaged myocardial areas (non-viablemyocardium-to-remote ratio1.88+0.81;p=0.044)but itwasnot increased inviable regions.Conclusions: 68Ga-NODAGA-RGD PET demonstrates increased integrin avb3 expres-sion in the ischemic myocardium in a pig model of flow limiting stenosis. This increase,however, appears to be co-localized in the non-viable myocardial areas while no increasewas seen in regions with inducible ischemia but no scar. The results suggest thatincreased integrinavb3 expression and68Ga-NODAGA-RGD uptakearemarkers of myo-cardial ischemic injury.
P291Characterization of the 18F labeled tracer LMI1195 for cardiac innervationimaging: a feasibility study using a rodent model and a clinical PET/MR system
S. Nekolla1, S. Swirzek1, T. Higuchi1, S. Reder1, S. Schachoff1, M. Bschorner1, I. Laitinen1,S. Robinson2, B. Yousefi1, M. Schwaiger11Nuklearmedizinische Klinik der TU Munchen, Munchen, Germany; 2Departments ofDiscovery Chemistry and Discovery Biology, Lantheus Medical Imaging, North Billerica,United States of America
Objectives: Non-invasive imaging of the sympathetic innervation of the heart is a valuableaddition to the armamentarium of nuclear cardiology. SPECT tracers such as MIBG aresuccessfully used in the workup of heart failure patients; however, image quality is sub-optimal especially for estimation of local tracer distribution. LMI-1195 is a new, F-18 la-belled agent with a similar structure as MIGB which showed in initial animal studies apromising image quality. In this feasibility study, we sought to delineate in a time efficientapproach both functional and morphological information in a rabbit model using a fullyintegrated, clinical PET/MR device.Methods: We induced myocardial denervation after thoracotomy by phenol painting ontheepicardium of the left ventricle (LV).Twoanimals each weredenervated either in amod-erate (m) or more severe way (s) (m: 2x painting, 10% phenol, imagingDT=4h post inter-vention, s: 3x painting, 80%Phenol, DT=1 week). In both setups, an area of 20% LV wastargeted. In addition, two animals were sham operated (n). Using a clinical PET/MR thetracer distribution was assessed in static and dynamic data acquired over 90 minutes.In addition, images were measured post mortem. ECG gated studies were acquiredboth using PET and MRI. Image reconstruction was performed using OSEM3D (3i21s,matrix 344x344, no post-recon filtering). Regional tracer distributions were calculatedusing volumetric data analysis. Retention and normalized, static polar maps were gener-ated. Finally, in order to investigate partial volume effects, the uptake ratio between LVlumen and myocardium was assessed.Results: Using the dynamic data, tracer retention in the untreated areas was found to be10+2%/min. In the animals with denervation, the untreated areas showed homogeneousand a temporally constant signal (T:30min 80+9%, T:90min 82+8%) . Using the moder-ate denervation, no reduction of tracer uptake was measured. In the other setup, a clearsignal decline was found (15+8%). The myocardium/lumen ratio was 250+70% in thestatic data, 325+70% using diastolic images, and 280+78% in post mortem images.Conclusions: Integrated PET/MR tomographs allow the efficient assessment of multi-parametric cardiac functions in a rabbit model. LMI1195 showed excellent imagequality with high biologic specificity.
P292SUV is an accurate measure of cardiac 11C-PIB retention in amyloidosis
T. Kero, L. Lindsjo, G. Antoni, P. Westermark, K. Carlson, G. Wikstrom, J. Sorensen,M. LubberinkUppsala University, Uppsala, Sweden
Aim: To evaluate SUV as a measureof 11C-PIB retention in cardiac amyloidosis.Material and Methods: Patients with systemic amyloidosis and cardiac involvement(n=10) and healthy controls (n=5) were investigated with 25 minute dynamic PET-scanafter intravenous bolus injection of 6 MBq/kg 11C-PIB.The PET-studies were analyzed with Carimas software by two observers to calculate time-activity curves for plasma and left-ventricle tissue in 17 standardized segments and aglobal mean for the whole left ventricle.FUR(fractionaluptake rate) index model wasused to calculate the left ventricle retention of11C-PIB at 10-20 and 15-25 minutes after tracer injection. SUV (standardized uptakevalues) were calculated for the same timeframes after corrections for injected activitydose, bodyweight and decay.Difference in FUR and SUV between amyloidosis patients and controls was assessed withMann-Whitney U test. Agreement between FUR and SUV was assessed with linear regres-sion. Inter-reader reproducibility was assessed with intraclass correlation coefficient(ICC).Results: The mean FUR at 10-20 min was 0.073 min-1 (range, 0.043–0.188 min-1) inamyloidosis patients and 0.031 min-1 (range, 0.028–0.034 min-1) in healthy controls.The mean FUR at 15-25 min was 0.056 min-1 (range, 0.029–0.158 min-1) in amyloidosispatients and 0.024 min-1 (range, 0.022–0.026 min-1) in healthy controls.The mean SUV at 10-20 min was 3.05 g/ml (range, 1.87-8.22 g/ml) in amyloidosis patientsand 1.12 g/ml (range, 0.96-1.36 g/ml) in healthy controls. The mean SUVat 15-25 min was2.73 g/ml (range, 1.59-8.01 g/ml) in amyloidosis patients and 1.03 g/ml (range,0.89-1.24g/ml) in healthy controls.The mean FUR and SUV were higher in amyloidosis patients than in controls at both time-frames (p=0.001), although the difference was greater for both FUR and SUVat the earliertimeframe (p=0.005, Wilcoxon signed rank test).The correlation between FUR and SUV was excellent for both global and regional values(r.0.97). Inter-reader reproducibility was also excellent both for global and regional ana-lysis (ICC.0.98).Conclusion: SUV can be used as a measure of cardiac 11C-PIB retention in amyloidosisaffecting the heart. A ten minute static PET-scan and simple analysis could be sufficientinstead of dynamic scanning and more complex analysis.
P293Early detection of inflammation in experimental autoimmune myocardis using99mTc-fucoidan SPECT
F. Rouzet, T. Cognet, K. Guedj, M. Morvan, F. El Shoukr, L. Louedec, C. Choqueux,A. Nicoletti, D. Le GuludecInserm U1148 - LVTS, Paris, France
Purpose: Myocarditis, an inflammatory disease of the myocardium, is a major cause ofdeath and dilated cardiomyopathy. However its work-up is not standardized due to thelack of reliable marker of progression. Owing to variable physiological uptake, 18FDGcannot be regarded as an optimal marker of myocardial inflammation. Myocarditis is char-acterized by clusters of lymphoid and myeloid cell infiltrates, and endothelial activationwhich hallmark is the expression of adhesion molecules such as selectins. The aim of
i50 Poster Session 2
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from

the study was to evaluate the ability of 99mTc-fucoidan, an imaging agent specific of selec-tins, in the early assessment of inflammation in a model of experimental autoimmune myo-carditis (EAM).Methods: EAM has been induced in male Lewis rats with purified rat cardiomyosinand compared with controls. The experiments were performed in the very early phaseof myocarditis (10, 15 and 21 days after immunization) and included (1) quantificationof 99mTc-fucoidan myocardial/lung ratio using SPECT/CT; (2) qualitatively: comparativeanalysis on adjacent slices of tracer uptake on autoradiography and selectins onimmuno-histochemistry (CD62p, CD62e); and (3) quantitatively: relationship between99mTc-fucoidan uptake by well counting (expressed as %ID/g of myocardium) and myo-cardial content of inflammatory cells (CD45; CD11b) using flow cytometry.Results: myocardial uptake of 99mTc-fucoidan was significantly increased in EAM com-pared to controls (SPECTuptake ratio: 1.6+0.1 vs. 1.2+0.4, p=0.04 at D10; 2.3+0.2 vs.1.3+0.8, p,0.0001 at D15 and 1.9+0.2 vs. 1.3+0.3; p=0.015 at D21). Areas of99mTc-fucoidan uptake co-localized with endothelial expression of P- and E-selectins.There was a close relationship between uptake of the tracer and myocardial content inCD45+/CD11b+ cells.Conclusions:99mTc-fucoidan allowsdetecting early steps of endothelial activation asso-ciatedwithEAM, and itsuptake iscorrelated withmyocardial content in inflammatory cells.Further study is required to determine whether it may allow monitoring chronic diseaseand/or therapy efficacy.
P294Diagnosis of cardiac involvement in Andrade type familial amyloidpolyneuropathy with 99mTc-DPD
A. Jimenez-Heffernan1, F. Munoz-Beamud2, E. Sanchez De Mora1, C. Borrachero2,C. Salgado1, C. Ramos-Font1, J. Lopez-Martin1, ML. Hidalgo3, R. Lopez-Aguilar3,E. Soriano1
1Hospital Juan Ramon Jimeez. Department of Diagnostic Imaging., Huelva, Spain;2Hospital Juan Ramon Jimenez, Internal Medicine, Huelva, Spain; 3Hospital Juan RamonJimenez. Department of Cardiology, Huelva, Spain
Purpose: The degree of cardiac involvement is the major prognostic determinant in sys-temic amyloidoses but cardiomyopathy may not be diagnosed if neuropathy is theleading clinical manifestation and echocardiography is not performed. Furthermorethere is awidespectrum of echocardiographic findings none in itself specific and althoughdiastolic dysfunction is thehallmarkof amyloidheartdisease severe impairment ispresentonly in advanced stages of myocardial infiltration. We aim to assess the role of99mTc-diphosphono-propano-dicarboxylic acid (DPD) cardiac imaging in a transthyretin(TTR) related form of amyloidosis.Methods: We studied 24 patients with Andrade type familial amyoid polyneuropathy(FAP) (18 men, 6 women, age: 50 + 14.6 years) for assessment of myocardial uptake.Mean time from diagnosis was 5.3+ 4.8 years. Fifteen patients had undergone orthotopicliver transplantation between 10 and 1 years before. Whole body scans were acquiredthree hours after injection of 740 MBq of 99mTc-DPD in a dual head gamma camera fol-lowed by SPECT acquisition in patients showing heart uptake. Visual scoring of uptakewas 0 absent, 1-3 mild to intense uptake. All patients underwent complete clinical exam-ination, ECG and echocardiographic studies.Results: Five patients showed biventricular cardiac uptake, with scores 2 and 3 in two andthree patients respectively. Bone uptake was attenuated in the score 2 patients and mild orabsent in the score 3 patients. Echocardiography showed increased left ventricular wallthickness predominantly in the septum in three patients one of whom had diastolic dys-function. Moderate diastolic dysfunction without hypetrophy was present in the othertwo patients. Six of the 19 patients without DPD heart uptake showed mild diastolic impair-ment three of whom had mild ventricular hypetrophy.Conclusions:99mTc-DPD issensitiveandspecific in the depictionof cardiac involvementin Andrade’s disease and may provide an early diagnosis when compared to echocardi-ography. Increasing cardiac uptake of 99mTc-DPD is associated with decreasing boneuptake.
P295An investigation of the estimation of photon attenuation and scatter correctionsfor the myocardial uptake of myocardial I-123 MIBG SPECT in a patient with HCMusing a CT-SPECTcombined system
A. Okizaki, M. Nakayama, S. Ishitoya, J. Sato, K. TakahashiAsahikawa Medical University, Department of Radiology, Asahikawa, Japan
Purpose: Some authors reported that the uptake of the inferior wall in myocardial I-123MIBG SPECT is underestimated because of photon attenuation and scatter. CT-SPECTcombined system might be useful for attenuation and scatter corrections with myocardialSPECT. The purpose of this study was to investigate these corrections for the myocardialuptake of myocardial I-123 MIBG SPECT in a patient with HCM using a CT-SPECTsystem.Additionally, a comparison between FBP and OSEM reconstruction algorithms were per-formed, to estimate the effect from adjacent activity in the liver.Methods: Twelve patients with HCM were studied. After an injection of I-123 MIBG(111MBq), SPECT acquisition was performed on a dual-headed digital gamma camerasystem. After that, CT-SPECT was performed immediately on the same device forphoton attenuation and scatter corrections. The data were reconstructed with FBP andOSEM. Polar maps were obtained in each patient with two algorithms that were withand without the corrections based on CT-SPECT data. The left ventricular myocardiumwas divided into 7 segments on the polar map. The uptake was evaluated by quantitative
perfusion SPECTsoftware, and inferior to anterior wall ratio (IAR) was calculated. Finally,paired t-tests were performed in these data.Results: Results were summarized in the table. There is no significant difference in uptakeof the inferior wall, anterior wall and IAR between the two reconstruction algorithms. On theother hand, the corrections with CT-SPECT could statistically increase the uptake of theinferior wall (p ,0.01) and decrease it of the anterior wall (p,0.01), increase IAR(p,0.005). These change of the I-123 MIBG distribution could be derived from the correc-tions, not depend on the reconstruction algorithms.Conclusions: Photon attenuation and scatter corrections based on the CT-SPECTdata could be useful to evaluate the myocardial sympathetic nerve activity in a patientwith HCM.
Abstract P295 Table. I-123 MIBG Uptake
FBP OSEM without correction OSEM with correction
Anterior Wall 108.5 109.3 103.0*Inferior Wall 84.7 84.3 92.7*Inferior-Anterior Ratio 0.80 0.81 0.93**
*p,0.01; **p,0.005, compared with OSEM without attenuation and scatter corrections
P296CZT-Camera vs dual-headed Anger camera with resolution recovery: Acomparison of semiquantitative myocardial perfusion and functional parameters
I. Burchert, F. Caobelli, T. Wollenweber, M. Nierada, J. Fulsche, C. Dieckmann, FM. BengelHannover Medical School, Nuclear Medicine, Hannover, Germany
Aim: Providing high sensitivity and resolution, the cadmium-zinc-telluride (CZT) -Camerarepresents a new standard for myocardial perfusion imaging (MPI). However, modernAnger cameras using resolution recovery reconstruction algorithms also provide an im-provement in image quality. The aim of our study was an intraindividual comparison ofboth techniques.Methods:Standard dose ofTc99m-Sestamibi stress (Regadenoson) and restMPISPECTscans were sequentially performed on 30 consecutive patients using a CZT-Camera (Dis-covery NM 530c; 3 and 7 min acquisition time) and a dual-headed Anger camera (Discov-ery NM/CT 670; 20 min acquisition time). Images acquired on CZT camera werereconstructed with and without CT-based attenuation correction (AC). Those acquiredon Anger Camera were reconstructed 1)with FBP and 2) with OSEM algorithm, with andwithout AC, applying scatter correction and resolution recovery (RR). Myocardialcounts (measured by ROI-analysis), summed stress-(SSS), rest-(SRS) and difference-scores (SDS) and LVEF were compared.Results: All acquired parameters correlated significantly between camera systems. Thecoefficients of correlation were consistently higher for the non-corrected image data (NC)than for the data including AC and RR for the Anger camera (e.g.: SSS for NC–R2=0.74 vsAC-RR - R2=0.54). The coefficients of correlation between the Anger camera and the 3min CZT-acquisitions were consistently lower than those with the 7 min acquisitions.Conclusion: Semiquantitative MPI SPECT results of conventional Anger cameras andCZT-cameras are significantly correlated. Nevertheless, new resolution recovery recon-struction algorithmsmay amplifyartifacts. Individualproperties of the imaging procedureshave to be taken into account for the interpretation of the results.
P297Comparison of measurements of left ventricular wall thickness and cavity size onSPECT MPI to those obtained with transthoracic echocardiography
S. Shuaib, D. Mahlum, S. PortAurora Sinai/Aurora St. Luke’s Medical Centers, Aurora Cardiovascular Services,Milwaukee, United States of America
Purpose: Left ventricular wall thickness (LVWT) frequently appears increased on singlephoton emission computed tomography (SPECT) myocardial perfusion imaging (MPI)but the accuracy of SPECT MPI for the qualitative or quantitative assessment of LVWT isnot well established. This study tried to determine the accuracy of a quantitative measure-ment of LVWT on SPECT MPI data by comparing it to similar measurements made bytransthoracic echocardiography (TTE).Methods: We retrospectively studied 139 consecutive patients (mean age 69 years, 53%men) who underwent SPECT MPI from December 2012 to January 2013 and had TTEwithin one year prior to SPECT MPI. Gated, stress SPECT MPI was performed using adual head gamma camera. Non-attenuation corrected data were used. A software rulertool was used manually to measure the septal and lateral LVWT and LV end diastolicdiameter (LVEDD) from the horizontal, long axis view using the contour display of thewalls generated by the automated edge detection program. The measurements were per-pendicular to the long axis of the cavity. Measurements of the same variables on TTE wereobtained from the recorded final report. A paired t-test and a Bland-Altman analysis wereused to analyze the data.Results: Septal (S) and lateral (L) LVWTon SPECT MPI are significantly greater than onTTE. LVEDD on SPECT MPI is significantly smaller than on TTE. The ratio of wall thicknessto LVEDD on SPECT MPI is significantly greater than on TTE. Bland-Altman analysisshowedoverestimation by SPECT MPIof TTEwall thickness throughout the rangeof thick-nesses in the study.
Poster Session 2 i51
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from

Conclusion: Both the absolute LVWT and the LVWT/LVEDD ratio are overestimated bySPECT MPI in comparison to TTE. It is wall thickness to cavity ratio that the reader appreci-ates visually on SPECT MPI and would therefore result in the tendency to misdiagnose thepresence of LV hypertrophy.
Abstract 221 Table.
SPECT MPI TTE
Measurements Mean SD Mean SD P
S-LVWT 1.38 0.18 1.06 0.19 ,0.0001L-LVWT 1.61 0.16 1.00 0.18 ,0.0001LVEDD 4.08 0.78 4.89 0.73 ,0.0001S-LVWT/LVEDD 0.35 0.08 0.22 0.05 ,0.0001L-LVWT/LVEDD 0.41 0.08 0.21 0.05 ,0.0001
P298Potential usefulness of multidetector computed tomography (MDCT) in thequantification of mitral calcium
D. Gemma, E. Refoyo, E. Cuesta, G. Guzman, T. Lopez, S. Valbuena, M. Fernandez-Velilla,S. Del Prado, M. Moreno, JL. Lopez-SendonUniversity Hospital La Paz, Madrid, Spain
Introduction: Mitral valve repair (MVR) is the surgical treatment of choice for severemitral re-gurgitation (MR) in patients with echocardiographic favorable anatomy. Classical criteria donot include the calcium scoring (CS), however the likelihood of repair is reduced in calcifiedvalves. Multidetector computed tomography (MDCT) is the technique of choice for assessingCS. OBJECTIVES: determine the degree of agreement between mitral valve CS obtained byMDCTand by transesophageal echocardiography (TEE) in MR preoperative studies.Materials and Methods: Retrospective observational study involving patients with MRwho underwent valve surgery at our instiutution between January 2010 and April 2013and who had preoperative assessment with TEE and MDCT. The degree of calcificationof the mitral annulus and its corners were assessed using the two techniques, assigninga value of CS 0-2 by TEE (0=without calico; 1=mild calcification; 2= moderate/severe cal-cification), and performing an Agatston score in the case of MDCT: score 0=0 HounsfieldUnits (HU); score 1=1-4000 HU; score 2=. 4000HU.Results: 19 patients were included (52,6% men), mean age 68 +/- 10 years old. MVR wasperformed in 11 patients (57,9%), while valve replacement was executed in the remaining8 patients (42,1%). 3 patients had previously implanted mitral annulus, which were notincluded in the analysis. Although statistically significant, the degree of agreementbetween the 2 tests was not excellent (p=0,002; kappa=0,51). The correlation betweenthe two techniques was 100% in patients without mitral calcification and in those with mod-erate/severe calcification (scores de 0 y 2), while there was greater discrepancy in the 9patients with mild calcification.Conclusions: Qualitative assessment of mitral calcification by TEE presents a goodagreement with MDCT CS. However in patients with mild calcification in TEE, the MDCToptimize the quantification of mitral calcium.
Score CT
No calcificationScore 0
Mild calcificationScore 1-4000
Moderate/severecalcification Score.4000
ScoreTEE
No clacification(Score 0)
6 0 0
Mild calcification(Score 1)
3 4 2
Moderate/severecalcification(Score 2)
0 0 1
Grade of agreement Kappa 0,59 p=0,002
P299Comparison between stress-rest 99mTc-Sestamibi SPECTand rest 2Dechocardiography for measurement of left ventricular ejection fraction
M. Harbinson1, L. Donnelly2
1Queen’s University, Belfast, United Kingdom; 2University of Aberdeen, Aberdeen, UnitedKingdom
Background: Left ventricular end-diastolic and end-systolic volume (EDV, ESV) and ejec-tion fraction(LVEF)aremostcommonlycalculatedusingrestechocardiography.99Techne-tium gated SPECT imaging can also provide these measurements. It is of clinical interest tocompare these values as estimatedby each technique. For stress only SPECT imaging, therelationship between the gated volumesand function,andrestechodataestimated cardiacfunction, are less researched and are important for stress only SPECT protocols.Aims: To compare EDV, ESV and LVEF obtained by:
– rest SPECTand echocardiography (correlation target (r) of 0.75)– restSPECTandstress SPECTwith normal perfusion data (correlation target (r) of 0.75)– stress SPECTand echocardiography in those with normal perfusion
Methods: 132 patients (75 males, 57 females, age range 31-89 years) with both a99mTc-Sestamibi SPECT scan and 2D rest echocardiography scan within 12 months ofeach other were selected. SPECT was carried out on a dual headed gamma camera(GE Infinia) with 60 steps at 30 seconds/step with 16 time gating bins. Quantitative datawas provided by automated quantitative gated SPECT (QGS) software (Cedar-Sinai).For echocardiography, Simpson’s Biplane was the method of choice for estimatingLVEF, though many of the scans included used Teicholz method. For this reason the echo-cardiographers’ report on the overall category of LV function was used instead. LVEFvalues were compared by category (normal, mild, moderate, severe) or as continuousvariables.Results: Objective One- Rest SPECT vs. echocardiography produced a correlation coef-ficient (r) of 0.80 for LVEF which exceeded the audit standard of 0.75. This was when the LVcategory method was used.Objective Two- There was 97% LV category agreement between the rest and stressSPECT. There was only a moderate correlation of r= 0.66 for LVEF, which did not meetthe audit standard. Correlation coefficients for EDV and ESV were excellent at r=0.93and 0.90, respectively.Objective Three- Continuous variable correlation was not possible but there was 100% LVcategory agreement between stress SPECTand echocardiography.Conclusion: There is good evidence that cardiac volumes and LVEF obtained by gatedSPECT agree well with echocardiographers’ assessments of LV function. Future auditsshould be carried out and include a larger patient population. The agreement betweenrest echo and stress SPECT values for cardiac volumes and function in patients withnormal perfusion is important when moving to a ‘stress only’ SPECT protocol for suchpatients.
P300Ultra-low dose stress-first Tc-99m tetrofosmin myocardial perfusion SPECT inpatients with chest pain using a high-efficiency camera: prognosis, duration, andradiation doses
A J. Einstein, L L. Johnson, A J. Deluca, A C. Kontak, D W. Groves, J. Stant, T. Pozniakoff,B. Cheng, L E. Rabbani, S. BokhariColumbia University Medical Center, New York, United States of America
Purpose: While SPECT MPI provides clinically useful information about patients withchest pain (CP), there is growing concern regarding its radiation burden and thestudy’s duration. Use of a high-efficiency (HE) camera offers the potential to markedlyreduce radiation dose, as does use of a stress-first (SF) protocol. No previous studyhas assessed outcomes and radiation doses of patients undergoing MPI on aHE-SPECTcamera using an ultra-low-dose stress-first protocol.Methods: 100 patients presenting to the emergency department with CP and candidatesfor SF MPI received ~185MBq (5 mCi) of Tc-99m tetrofosmin at peak stress, followed byHE-SPECTsupine and prone imaging. Rest imaging was performed only on patients withany abnormality on stress imaging, after review by a nuclear cardiologist. Patients werecontacted 3 months subsequent to discharge and electronic medical records and theSocial Security Death Index reviewed to evaluate cardiac events, additional imaging, orthe need for repeat CP evaluation.Results: 69 patients underwent stress-only and 31 underwent stress-rest imaging. Radi-ation dose averaged 2.22 mSv over all patients (standard deviation 1.9, range 0.42 to 6.56mSv). Median study duration was 128 minutes (IQR 106-209). 96 patients met the primaryoutcome criteria of being free at 3 months of major adverse cardiac events, repeat hospitalchest pain evaluation, and repeat imaging or stress testing. For the 4 patients not meetingthe primary outcome criteria, one had a completely normal MPI result but nonethelessunderwent an outpatient stress CMR study, while three re-presented to the emergency de-partment with similar symptoms, were discharged from the emergency departmentwithout hospital admission or repeat cardiac imaging, and were alive one year later withno evidence of a repeat event. One year after MPI and hospital discharge, all patientswere living and without acute coronary syndrome.Conclusions: HE-SPECT SF imaging can be performed in CP patients without high prob-ability of a perfusion defect, with excellent 1 year prognosis, radiation dose averaging 2.2mSv, and test duration typically ~2 hours.
P301Simultaneous myocardial Tc-99m / I-123 imaging using Cadmium Zinc Telluride(CZT) SPECT: A feasibility phantom study
F. Caobelli1, C. Schuetze2, M. Nierada1, J. Fulsche1, C. Dieckmann1, FM. Bengel11Hannover Medical School, Nuclear Medicine, Hannover, Germany; 2Hannover MedicalSchool, Medical Physics, Hannover, Germany
Background: CZT detectors have superior energy resolution which facilitates multi-isotope simultaneous imaging. This may enable integrated studies of myocardial perfu-sion (Tc-99m agent) and innervation (I-123 MIBG), but the proximity of energy peaks(140 and 159 keV) may remain a challenge. We evaluated the feasibility in a phantommodel.Methods: An anthropomorphic thorax phantom with a cardiac insert (110mL) and a smalltransmural defect insert in lateral wall (TD, 4.7mL, 4.3%) was employed to simulate an invivo distribution of 400 MBq Tc-99m perfusion agent and/or 150 MBq I-123 MIBG. In singleisotope studies, TD was filled either with water or the same radioisotope concentration. Indual-isotope studies, remote myocardium was filled with both isotopes and TD was filledwith: 1) water, 2) Tc-99m only 3) I-123 only or 4) both isotopes. Images were acquired in listmode over 7 minutes, and reconstructed using 2, 5 and 8% energy window setting. Polarmaps were generated to evaluate defect sizes.
i52 Poster Session 2
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from

Results: Single isotope studiesyielded accuratedefect size across all energy window set-tings (4.23% for Tc-99m and 4.16% for I-123). In dual-isotope studies, defect size was ac-curately present/absent in both Tc-99m and I-123 images when TD was either cold or filledwith both isotopes. With Tc-99m only in TD, a false defect was detectable in Tc-99mimages, suggesting downscatter of I-123 into the Tc-99m window in remote myocardium.A similar, albeit less pronounced observation was present in I-123 images when TD con-tained I-123 only, suggesting upward crosstalk from Tc-99m in remote. Narrower recon-struction energy windows did not resolve false defects (%LV for 2% window: 2.97, for5%: 2.22; for 8%: 2.29% with I-123).Conclusion: Crosstalk and downscatter need to be considered even with CZT SPECTwhen Tc-99m/I-123 dual isotope studies are performed. Narrowing of energy windowsdoes not resolve this issue. Corrective algorithms need to be developed and implemented.
P302Effect of temporal resolution of 18F-FDG gated-PETover quantitative systolic anddiastolic values
S. Aguade-Bruix, MN. Pizzi, G. Romero-Farina, M. Terricabras, D. Villasboas,J. Castell-Conesa, J. Candell-RieraHospital Vall d’Hebron, Barcelona, Spain
From list mode gated-PETa reconstruction with more than 8 frames/cycle facilitates mostaccurated systole delimitation.Aim: To evaluate differences between quantitative systolic (EDV: End diastolic volume,ESV; End systolic volume, EF: Ejection fraction) and diastolic (PFR: Peak filling rate,TPFR: Time to peak filling rate) parameters obtained by gated-PET by mean of three dif-ferent temporal resolutions.Methods: 40 patients (mean age 57.2+17.1 years, 11 women) with indication of cardio-vascular PET(viability, dilated cardiomyopathy,endocarditis, vasculitis) were studied with18F-FDG gated PET. Cardiac bed acquisition was performed in Siemens mCT 64S PET/CTwith list mode(8minutes/bed). Three reconstruction series were created, with 8,16and24 frames/cycle, with exclusion of extrasystolic ECG cycles. Reconstruction parameteswere 3 iterations, 21 subsets, Gaussian filter order 5 and 128x128 matrix, with attenuation,TOF and PSF corrections.Results: The gated PET QGS values are: TableAn excel.lent correlation was obtained for systolic function parameters and for PFR, butsuboptimal correlation for TPFR. The trend from EF 8 to 16 and 24 images is incremental,but not for EDV. Student T test shows significant differences between the values of gatedPET 8, 16 and 24 except for EDV 8-16 (p = 0.167), EDV 16-24 (p = 0.280), and for any as-sociation of PFR and TPFR.Conclusion: A high temporal resolution improves the best systole definition, resulting inhigher EF and lower ESV. Significant changes in diastolic function parameters were notobserved.
Abstract P302 Table. Results
EF(%) EDV(ml) ESV(ml) PFR(VTD/s) TPFR(ms)
Gated PET8 39.2+14 141.4+63 91.3+57.5 1.35+0.55 222.8+90Gated PET16 42.5+14 145.2+64 89.7+57.7 1.38+0.66 219.1+82Gated PET24 44.0+15 143.9+63 87.2+56.7 1.46+0.70 232.1+95CorrelationGated PET 8-16 0.981 0.989 0.992 0.888 0.517Gated PET 8-24 0.988 0.994 0.993 0.855 0.665Gated PET16-24 0.988 0.993 0.997 0.829 0.818
Gated-PET values and correlation
P303In vivomonitoring ofdual stemcell therapyafter myocardial infarction inmice with[18F] fluorodeoxyglucose positron emission tomography
S. Brunner, L. Gross, A. Todica, S. LehnerUniversity Hospital Grosshadern, Munich, Germany
Recently, we established [18F]FDG positron emission tomography (PET) for measure-ment of cardiac function and myocardial vitality in murine models of cardiovasculardisease. We tested this technique for monitoring dual stem cell therapy (G-CSF + Sitglip-tin)–a novel promising therapeutic regime for ischemic diseases - in a murine model ofmyocardial infarction (MI).MI was induced in mice, and they were assigned to the saline or the dual stem cell therapy(G-CSF i.v. and Sitagliptin p.o. for 7 days) group. Mice had 2-deoxy-2-[18F]fluoro-d-glucose (FDG)-PET examinations on days 6 and 30 for calculation of the left ventricularejection fraction and infarct area. Further, we performed histology to assess infarct sizeand to visualize c-kit+ stem cells. Flow cytometry was performed to analyze intramyocar-dial c-kit+ stem cells.[18F]FDG-PET revealed a significant decrease in infarct size in the treatment group com-pared to control and an improvement of cardiac function. Results were confirmed by histo-logical analyses showing reduced infarct sizes 30 days after MI. Furthermore, theseresults were associated with increased intramyocardial numbers of c-kit+ stem cells inthe treatment group. Immunohistology visualized these c-kit+ cells mainly in the infarctborder zone.Our results show, that [18F]FDG-PET is a sufficient tool for monitoring novel treatmentregimes in preclinical models of myocardial infarction.
P304Comparison among different gated myocardial perfusion software andechocardiography in measuring the left ventricular ejection fraction
A. Di Palo, A. Niccoli Asabella, C. Magarelli, A. Notaristefano, C. Ferrari, G. RubiniUniversitary PolIclinic of Bari- Nuclear Medicine- D.I.M., Bari, Italy
Purpose: Gated myocardial perfusion imaging (G-MPI) allows the evaluation of left ven-tricular ejection fraction (LVEF) in patients with suspected coronary artery disease (CAD).The aim of this study was to obtain the LVEF quantitative results of four commercially avail-able software: quantitative gated single-photon emission computed tomography(SPECT) (QGS), Myovation, Emory Cardiac Tool Box (ECTb) and 4DM-SPECT, and tocompare these results with LVEF calculated by echocardiographyMethods: 76 patients with suspected or known CAD that underwent transthoracic echo-cardiography, were examined using rest G-MPI. The acquired and reconstructed datawere processed using QGS, Myovation, ECTb and 4DM-SPECT software. Furthermore,we analyzed a subgroup of 28/76 patients with myocardial hypertrophy. We evaluatedthe Pearson’s correlation between the LVEF calculated by the four software and by theechocardiography in the entire population and in subgroup. The Bland-Altman analysiswas used to evaluated the difference of LVEF values obtained by four different softwareand echocardiography in both groups.Results: In all study population LEVF values (mean + SD) calculated by QGS was55+18,2; Myovation 55+ 19,9; ECTb 63+18,2; 4DM-SPECT 61+18,1, by echocardi-ography was 51+11,5. 28 patients were affected by myocardial hypertrophy. In this sub-group LEVF values (mean + SD) calculated by QGS was 65+13,2; Myovation 66,8+12,5; ECTb 73,3+11,9; 4DM-SPECT 72,8+13, by echocardiography was 56,8+6,2.In all population, good correlation was observed between QGS, Myovation, ECTb,4DM-SPECT (r=0.83) and echocardiography. Using the Bland-Altman analysis the differ-ences within mean + 1.96 SD are not clinically important, so the four methods may beused interchangeably respect to echocardiography. In patients with myocardial hyper-trophy the correlation was lower between the four software and echocardiography (r=0.69). Using he Bland-Altman analysis the differences within mean + 1.96 SD are slightlymore relevant; the four methods in these patients overestimate the LVEF and a discrepan-cies were observed in patients with small ventricular volumes respect to echocardiog-raphy.Conclusions: The results of LVEF obtained by all software (QGS, Myovation, ECTb and4DM-SPECT) provides high correlation among them and with echocardiography even ifdifferent LVEF values were obtained and the four methods resulted substantially equiva-lent. In patients with myocardial hypertrophy there is slight LVEF overestimation by thenuclear medicine software, particularly in patients with small ventricular volume.
P305Comparisonof left ventricular functionalparametersobtained fromthreedifferentcommercial automated software cardiac quantification program packages
A. Sellem, S. Melki, W. Elajmi, H. HammamiMilitary Hospital of Tunis, Nuclear Medicine Department, Tunis, Tunisia
Objective: ECG-gated myocardial perfusion scintigraphy (MPS) can be used to deter-minate several cardiac functional parameters (e.g., left ventricular ejection fraction(LVEF), end-diastolic volume (EDV), and end-systolic volume (EDV)). In this study, weaimed to compare these cardiac functional parameters, in patients with normaland abnor-mal myocardial perfusion scintigraphy, calculated by the following cardiac quantificationprogram: Emory Cardiac Toolbox (ECTb), Quantitave gated spect (QGS), and Corri-dor4DM.Methods: One hundred thirty four patients (63 male and 71 female) from 2013 to 2014were included in this study. In all patients, (99m)Tc-MIBI ECG-Gated (16-bin framemode) myocardial perfusion scintigraphy were performed. By using 3 different cardiacquantification programs (ECTb, QGS, and Corridor4DM); LVEF, EDV, and ESV were cal-culated and were compared for interprogram variability assessment in patient withnormal and abnormal myocardial perfusion scintigraphy.Results: There were statistically significant differences between ECTb, QGS, and Corri-dor4DM programs (p,0.000). Correlation between the results of ECTb, QGS, and Corri-dor4DM were greater than 90% (p,0.001). In patients with no perfusion defect, LVEF, andESV using ECTb were significantly higher than QGS, and Corridor4DM. In patients withperfusion defect LVEF, and EDV using ECTb were significantly higher than QGS, and Cor-ridor4DM.Conclusion: Different MPS cardiac software programs give variable (but correlated)LVEF and left ventricular volumetric measures. Those obtained from different cardiac soft-ware cannot be used interchangeably.
P306Atrial septal defect and partial anomalous pulmonary venous return: role ofcomputed tomographic angiography
MC. Ziadi1, J. Montero1, JL. Ameriso2, RL. Villavicencio1
1Diagnostico Medico Orono, Rosario, Argentina; 2Cardiovascular Institute of Rosario(ICR), Cardiovascular Surgery, Rosario, Argentina
A 35-yo-F presents for a preoperative evaluation for a dermolipectomy. She has a previoushistory of palpitations but no significant abnormalities on a Holter monitor. On physicalexamination there is a loud P2 heard at the left upper sternal border. An echocardiogramshows normal left ventricular (LV) size with preserved LV systolic function. There is en-largement of the right cardiac chambers and an increased mean pulmonary systolicartery pressure of 47 mmHg. A CTA was arranged for further assessment. Coronary
Poster Session 2 i53
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from

arteries have normal take-off and distribution with absence of significant obstructivedisease. CT images depict a sinus venosus atrial septal defect (ASD) with a diameter of13 mm and a left to right shunt. The right superior pulmonary vein drains to the low superiorvena cava (SVC). The left atria and LV are normal in size. There is hypertrophy of the rightventricle (RV) wall with severe dilatation. Right atrium (RA) is also moderate to severelyincreased in size. Coronary sinus is dilated with a diameter of 13 mm. The pulmonarytrunk diameter is larger than the adjacent ascending aorta. Owing to these findings,patient was referred forsurgical repair of the ASD, with successful placement ofa syntheticpatch to redirect blood flow from the RSPV into the LA with no major complications.Sinus venosus ASD is responsible for 5-10% of all adults ASDs and may be associatedwith anomalous right pulmonary venous return. State-of-the-art CTA is ideally suited foraccurate depiction of complex cardiovascular anatomic features. This clinical case high-lights the role of CTA not only for the diagnosis of congenital cardiovascular anomalies butalso for the guidance of therapy and thus patient outcomes.
P307Giant coronary aneurism diagnosed after an acute coronary syndrome
T F. Benito Gonzalez, A. Mayorga Bajo, R. Gutierrez Caro, M. Rodriguez Santamarta,L. Alvarez Roy, E. Martinez Paz, C. Barinaga Martin, J. Martin Fernandez,D. Alonso Rodriguez, I. Iglesias GarrizHospital of Leon, Cardiology, Leon, Spain
We present the case of a 78-year-old male, former smoker, with a history of hypertensionand dyslipidemia under treatment, admitted to hospital with an inferior STsegment eleva-tionmyocardial infarction .He was taken to the cath lab forprimary percutaneouscoronaryintervention and the angiography showeddiffuse three-vessel coronary disease.The rightcoronary artery was ectatic and tortuous, with distal thrombotic occlusion. Aspirationthrombectomy was carried out and followed by balloon angioplasty, achieving success-fully artery recanalization (TIMI flow 3).An echocardiogram was performed that revealed the presence of a rounded anechoicmass at the right atrioventricular groove (23 x 23 mm), with slight enhancement afteradministration of ultrasound contrast medium, suggesting the diagnosis of a partiallythrombosed aneurysm of the right coronary. This suspicion was confirmed by a coronaryCT angiogram, that identified two partially thrombosed aneurysms in the right coronaryartery, located in the mid (12 mm dimeter) and distal segments (22 mm diameter)respectively.Giant coronary aneurysms (over 20mm diameter) represent an uncommon finding onangiography and are more frequent in the right coronary. The main aetiology is athero-sclerosis (like in this patient), responsible for 50% of the cases. Other causes include con-genital heart disease, connective disorders or Kawasaki disease. Coronary aneurysmsare usually diagnosed on angiography, but sometimes can go unnoticed (i.e. partially
thrombosed aneurysms). Cardiac CT scan can be very useful, while visualization ofthese lesions on echocardiography is exceptional.
P308A rare case of adult type alcapa syndrome: presentation, diagnosis andmanagement
D. Gemma, E. Refoyo, E. Cuesta, G. Guzman, S. Valbuena, S. Rosillo, S. Del Prado,M. Torres, M. Moreno, JL. Lopez-SendonUniversity Hospital La Paz, Madrid, Spain
A 67-year-old woman referred to our center due to atypical chest pain, no related to ex-ertion. No dyspnea was observed. The electrocardiogram was normal and echocardio-graphic study demonstrated mild left ventricular enlargement with normal systolicfunction, multiple dilated coronary branches through right ventricle free wall. Theorigin of the right coronary artery (RCA) was seen correctly, however the origin of theleft coronary artery (LCA) could not be visualized. An imaging study with 64-slice multi-detector computed tomography (MDCT) was performed, showing an anomalous originof the LCA from the main pulmonary artery (PA) (figure d), with a markedly dilated RCAwhich connect to the LCA through numerous dilated and tortuous intercoronary collat-eral arteries (figure a-b). It was also described severe dilatation of the main PA (42×37mm) and the main pulmonary branches (right 37 mm, left 35 mm), due to the retrogradeflow from de LCA to main PA with a well visualized jet of at least 2-3 mm wide (figure c).Anomalous LCA arising from the PA (ALCAPA syndrome) is a rare congenital abnormal-ity, very uncommon in adults since the mortality in untreated cases approaches 90% ininfancy, although the true incidence may be underestimated due to the absence of clearsymptoms in adults. Nowadays diagnosis is based on MDCT, while the management ofthe older patients is controversial and depends on the clinical manifestations. In ourcase, 6 months after the diagnosis the patient remain asymptomatic, the exercisestress echocardiography was negative for ischemia and a cardiac-MR was performed,not showing any pathological delayed gadolinium enhancement. No invasive proce-dures were perfomed and medical treatment was decided with beta-blockers and anti-agregation, and remains stable at the time to writing.
P309Assessment of myocardial viability by rest myocardial perfusiontomoscintigraphy in coronary heart disease
S. Taleb1, G. Cherkaoui Salhi1, Y. Regbaoui2, M. Ait Idir1, A. Guensi11Ibn Rochd University Hospital, Nuclear medecine department, Casablanca, Morocco;2Ibn Rochd University Hospital, Cardiology department, Casablanca, Morocco
Introduction: Rest Myocardial Perfusion Tomoscintigraphy (RMPT) has a mainstay role incoronary heart disease exploration thanks to its usefulness in diagnosis and prognosisassessments.Aim: To report the experience of in myocardium viability evaluation by RMPTMethod: Sixty-two myocardial viability assessments were performed by RMPTamong 125MPT during the period between January 2011 and December 2012. The technique usedwas Single-photon emission computed tomography acquisition gated to ECG. Informa-tion was taken from patients’ questionnaires and scanner reports.Results: Sex ratio (M/F) was 1,6. Mean age was 58 years (+/- 10), 84% of our patients’ agewas above 50 years. The exploration was performed after myocardial infarction (MI) in58,5 % of cases (27% of anterior MI, 22% inferior IM and 9,5% of extended MI),atypicalchest pain in 17,5 % , and in ischemic cardiomyopathy in 24%. The mean time betweenMI and RMPTwas 1,9 Month.RMPT studie showed no abnormal findings in 1,5%; limited necrosis to less than 3 seg-ments in 37%, extended necrosis (.3/17 segments) in 28,5% of cases. Hypoperfusionwith viability signs was found in 33% of cases leading to a quick revascularisation inpatients with low left ventricular systolic fraction.RMPTwas complemented with diagnostic and therapeutic angiography in 43% of casesshowing monovessel (16%) bi vessel (11%) and three-vessel disease (14,3%).
Abstract 87 Figure.
alcapa
Coronary aneurysms
i54 Poster Session 2
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from

Conclusion: RMPT provides supplementary prognosis element, it can be developed incoronary diseases’ screening to allow a better selection to revascularisation.
P310Myocardial infarction secondary to anomalous origin of the right coronary artery:non invasive cardiovascular imaging evaluation
A. Puente1, S. Rosales2, C. Martinez1, M. Cabada1
1National Medical Center "20 de Noviembre" ISSSTE, Nuclear Cardiology, Mexico City,Mexico; 2National Medical Center "20 de Noviembre" ISSSTE, Cardiovascular Imaging,Mexico City, Mexico
Introduction: Coronary anomalies incidence varies from 0.64-1.3%. Malignant are asso-ciated with myocardial infarction, syncope, sudden death. Non invasive cardiovascularimaging techniques are useful for their evaluation.Description:17yearold manwithoutcardiovascular history andrisk factors. Arrived to theemergency department complaining of three hours acute chest pain and dyspnea. ECG:inferior subepicardial ischemia. Laboratory: Trop I (1.16 ng/mL). Diagnosis: Non-STeleva-tion myocardial infarction. Treatment:conservatively. Echocardiogram:inferior hipoquine-sia. Gated-SPECT (Tc99m mibi/one day): inferior and inferolateral non transmuralinfarction with moderate ischemia, normal left ventricular function (Fig 1-a). CoronaryComputed Tomography Angiography (CCTA): Right coronary artery (RCA) arise fromLeft Coronary Sinus(LCS), upper situation, posterior path between pulmonary trunkand aorta; non atherosclerosis lesions (Fig 1-b). Actually, asymptomatic with medicaltreatment (B-blockers, IECA and calcium antagonist).Discussion: In this case, ischemic complication can be produced by: 1) Anatomic com-pression of anomalous RCA by great vessels which courses between aorta and pulmon-ary to return to the normal position 2) an oblique angle (.458) at the junction of LCS and 3)spasm of the proximal portion.Conclutions: High risk malignant anomalous RCA in young patients like this one, isfrequently cause of myocardial infarction. Anatomical and functional non invasive evalu-ation can be used to diagnose and identify high risk patients, avoiding further invasiveevaluation.
P311An unusual case of severe hypertension in a young man
T F. Benito Gonzalez1, A. Mayorga Bajo1, R. Gutierrez Caro1, M. Rodriguez Santamarta1,L. Alvarez Roy1, E. Martinez Paz1, C E. Martin Lopez2, M. Castano Ruiz2,J. Martin Fernandez1, I. Iglesias Garriz1
1Hospital of Leon, Cardiology, Leon, Spain; 2Hospital of Leon, Cardiovascular Surgery,Leon, Spain
We report the case of a 29-year-old man, current smoker, with hypertension and dyslipide-mia, both untreated. He was referred to the cardiology outpatient clinic complaining of fre-quent dizziness and headaches in the recent months, and slight dyspnea on moderateexertion. The physical examination revealed an aortic systolic murmur and low amplitudepulses in lower extremities. Blood pressure was 170/110 mmHg and 115/90 mmHg inupper and lower limbs respectively. The echocardiogram showed left ventricular hyper-trophy, with a bicuspid aortic valve causing mild aortic stenosis and an ascendingaortic aneurysm (52 mm). A chest CT scan confirmed the dilatation of the ascendingaorta and exposed the presence of an interrupted aortic arch beyond the origin of theleft subclavian artery (IAA type A) with an important development of collateral circulationthrough mammary and intercostal arteries. Surgical correction was performed in twostages. First interrupted aortic arch was solved through a bypass between the distalaortic arch and the left subclavian artery and the descending aorta. Later the aortic rootand ascending aorta were replaced by a valved tube graft (Bentall-Bono procedure). Inthe follow up, the patient remained asymptomatic, with normal blood pressure andwithout any complication. Hypertension in young patients may be the presentation cluefor the diagnosis of some systemic or congenital heart diseases, and a rigorous physicalexamination can play a key role for the detection of these underlying secondary causes.The IAA is a fairly rare malformation and it is often associated with other abnormalities suchas VSD or bicuspid aortic valve. The definitive treatment is surgical correction, than can beaccomplished in a single or two-stage approach depending on the associated anomalies.
Fig.1-a:g-SPECT, 1-b:CCTA IAA
Poster Session 2 i55
European Heart Journal Cardiovascular Imaging Abstract Supplements – volume 16 supplement 1 May 2015
by guest on May 12, 2015
Dow
nloaded from