orthopedic manual - prohealthsys
TRANSCRIPT
Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 121
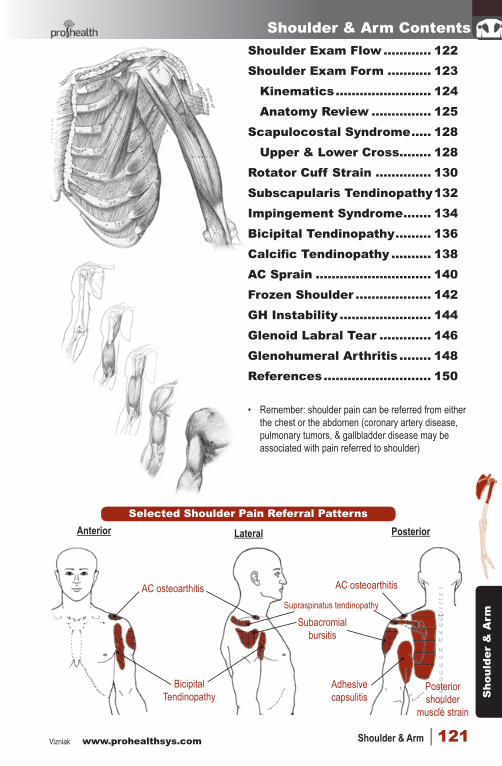
Shoulder & Arm Contents
BicipitalTendinopathy
Anterior
AC osteoarthitis
Lateral Posterior
AC osteoarthitis
Subacromial bursitis
Posterior shoulder
muscle strain
Adhesive capsulitis
Supraspinatus tendinopathy
Selected Shoulder Pain Referral Patterns
Shoulder Exam Flow ............ 122Shoulder Exam Form ........... 123
Kinematics ........................ 124Anatomy Review ............... 125
Scapulocostal Syndrome ..... 128Upper & Lower Cross ........ 128
Rotator Cuff Strain .............. 130Subscapularis Tendinopathy 132Impingement Syndrome ....... 134Bicipital Tendinopathy ......... 136Calcific Tendinopathy .......... 138AC Sprain ............................. 140Frozen Shoulder ................... 142GH Instability ....................... 144Glenoid Labral Tear ............. 146Glenohumeral Arthritis ........ 148References ........................... 150
• Remember: shoulder pain can be referred from either the chest or the abdomen (coronary artery disease, pulmonary tumors, & gallbladder disease may be associated with pain referred to shoulder)
4-shoulder NMS.indd 121 2014-01-14 11:05:12 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak122 | Orthopedic Conditions
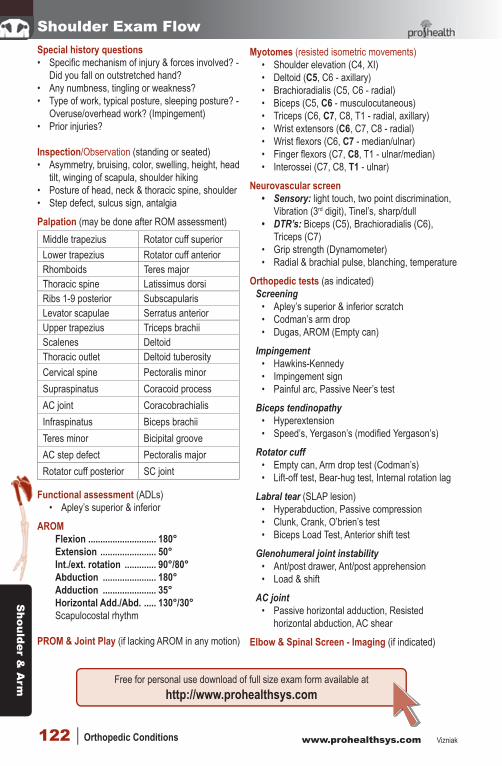
Shoulder Exam FlowSpecial history questions• Specific mechanism of injury & forces involved? -
Did you fall on outstretched hand? • Any numbness, tingling or weakness?• Type of work, typical posture, sleeping posture? -
Overuse/overhead work? (Impingement)• Prior injuries?
Inspection/Observation (standing or seated)• Asymmetry, bruising, color, swelling, height, head
tilt, winging of scapula, shoulder hiking• Posture of head, neck & thoracic spine, shoulder• Step defect, sulcus sign, antalgia
Palpation (may be done after ROM assessment)Middle trapezius Rotator cuff superiorLower trapezius Rotator cuff anteriorRhomboids Teres majorThoracic spine Latissimus dorsiRibs 1-9 posterior SubscapularisLevator scapulae Serratus anteriorUpper trapezius Triceps brachiiScalenes DeltoidThoracic outlet Deltoid tuberosityCervical spine Pectoralis minorSupraspinatus Coracoid processAC joint CoracobrachialisInfraspinatus Biceps brachiiTeres minor Bicipital grooveAC step defect Pectoralis majorRotator cuff posterior SC joint
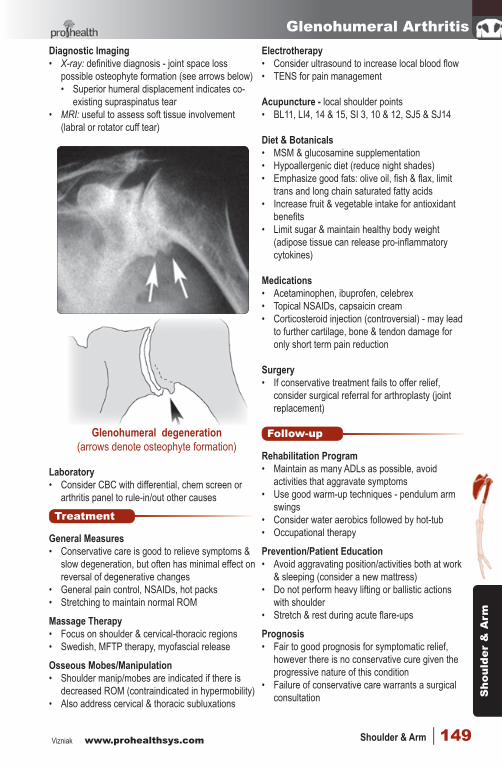
Functional assessment (ADLs)• Apley’s superior & inferior
AROM Flexion ............................ 180°Extension ....................... 50°Int./ext. rotation ............. 90°/80°Abduction ...................... 180°Adduction ...................... 35°Horizontal Add./Abd. ..... 130°/30°Scapulocostal rhythm
PROM & Joint Play (if lacking AROM in any motion)
Myotomes (resisted isometric movements)• Shoulder elevation (C4, XI)• Deltoid (C5, C6 - axillary)• Brachioradialis (C5, C6 - radial)• Biceps (C5, C6 - musculocutaneous)• Triceps (C6, C7, C8, T1 - radial, axillary)• Wrist extensors (C6, C7, C8 - radial) • Wrist flexors (C6, C7 - median/ulnar)• Finger flexors (C7, C8, T1 - ulnar/median)• Interossei (C7, C8, T1 - ulnar)
Neurovascular screen• Sensory: light touch, two point discrimination,
Vibration (3rd digit), Tinel’s, sharp/dull• DTR’s: Biceps (C5), Brachioradialis (C6),
Triceps (C7)• Grip strength (Dynamometer)• Radial & brachial pulse, blanching, temperature
Orthopedic tests (as indicated)Screening
• Apley’s superior & inferior scratch• Codman’s arm drop• Dugas, AROM (Empty can)
Impingement• Hawkins-Kennedy• Impingement sign• Painful arc, Passive Neer’s test
Biceps tendinopathy• Hyperextension• Speed’s, Yergason’s (modified Yergason’s)
Rotator cuff• Empty can, Arm drop test (Codman’s)• Lift-off test, Bear-hug test, Internal rotation lag
Labral tear (SLAP lesion)• Hyperabduction, Passive compression• Clunk, Crank, O’brien’s test• Biceps Load Test, Anterior shift test
Glenohumeral joint instability• Ant/post drawer, Ant/post apprehension• Load & shift
AC joint• Passive horizontal adduction, Resisted
horizontal abduction, AC shear
Elbow & Spinal Screen - Imaging (if indicated)
Free for personal use download of full size exam form available athttp://www.prohealthsys.com
4-shoulder NMS.indd 122 2014-01-14 11:05:12 AM
Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 123
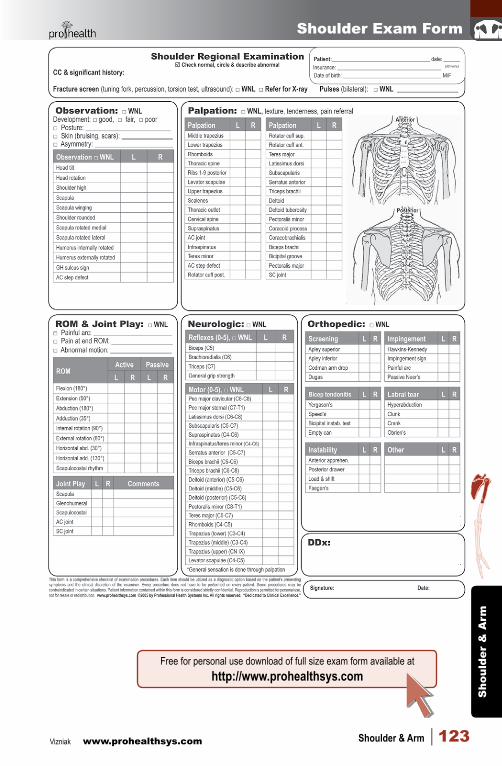
Shoulder Exam Form
Free for personal use download of full size exam form available athttp://www.prohealthsys.com
4-shoulder NMS.indd 123 2014-01-14 11:05:13 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak124 | Orthopedic Conditions
Shoulder KinematicsJoint type: synovial
Ball & socket (glenohumeral)Gliding (scapulothoracic - not a true joint)
Articular surfacesGlenohumeral: convex (head of humerus) on
concave (glenoid fossa)Scapulothoracic: concave (subscapular fossa)
on convex (posterior ribs)
Active range of motion (shoulder)Flexion .........................180°Extension ....................60°Int./ext. rotation ...........90°/80°Abduction ....................180°Adduction ....................35°Horizontal Add./Abd. ..130°/45°Scapulohumeral (humerus: scapula) 120°:60° (2:1)
Main muscle actionsFlexion: anterior deltoid, biceps brachii,
coracobrachialis, pectoralis majorExtension: posterior deltoid, latissimus dorsi,
triceps brachii, teres majorAbduction: middle deltoid, supraspinatusAdduction: latissimus dorsi, teres major,
pectoralis majorHorizontal adduction: pectoralis major,
coracobrachialis, anterior deltoidHorizontal abduction: posterior deltoid, teres
majorInternal rotation: subscapularis, pectoralis
major, latissimus dorsiExternal rotation: infraspinatus, teres minor
Resting positionGH: 55°-70° abduction, 30° horizontal abductionAcromioclavicular: arm at sideSternoclavicular: arm at side
Close packed positionGlenohumeral: maximal abduction & lateral rot.Acromioclavicular: 90° abductionSternoclavicular: full elevation
Normal end feelFlexion: elastic, firm capsularAbduction: elasticExtension: firmInternal/External : elastic / firmHorizontal adduction: soft tissueHorizontal abduction: firm/elastic
Abnormal end feelEmpty → severe instabilityHard capsular → frozen shoulderLate myospasm → instability
Capsular pattern of restrictionGlenohumeral: external rotation > abduction > internal rotation
Capsular pattern restrictions (detailed)Posterior capsule: ↓ horizontal adduction,
internal rotation & end range flexion, ↓ posterior glide
Posterior inferior capsule: ↓ elevation, internal rotation & horizontal adduction
Posterior superior capsule: ↓ internal rotationAnterior superior capsule: ↓ end range flexion
& extension, ↓ external rotation & horizontal abduction
Anterior capsule: ↓ abduction, extension, external rotation & horizontal adduction
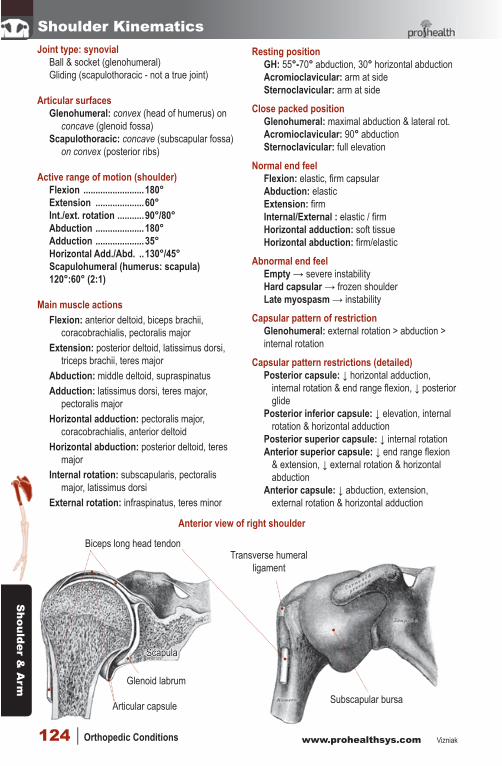
Anterior view of right shoulder
Subscapular bursa
Transverse humeral ligament
Articular capsule
Glenoid labrum
Biceps long head tendon
Scapula
4-shoulder NMS.indd 124 2014-01-14 11:05:13 AM
Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 125
54321
6
89
10
9
7
7
11
anterior view
lateral view
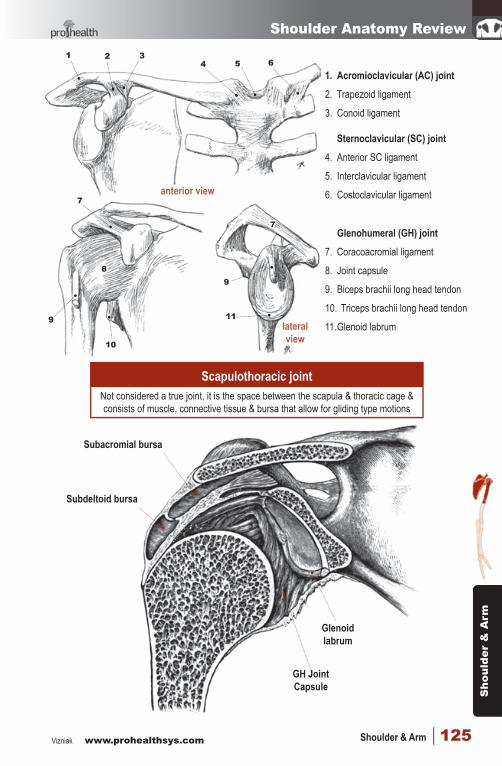
Scapulothoracic jointNot considered a true joint, it is the space between the scapula & thoracic cage & consists of muscle, connective tissue & bursa that allow for gliding type motions
1. Acromioclavicular (AC) joint2. Trapezoid ligament
3. Conoid ligament Sternoclavicular (SC) joint
4. Anterior SC ligament
5. Interclavicular ligament
6. Costoclavicular ligament Glenohumeral (GH) joint
7. Coracoacromial ligament
8. Joint capsule
9. Biceps brachii long head tendon
10. Triceps brachii long head tendon
11. Glenoid labrum
Shoulder Anatomy Review
Glenoid labrum
Subacromial bursa
Subdeltoid bursa
GH Joint Capsule
4-shoulder NMS.indd 125 2014-01-14 11:05:13 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak126 | Orthopedic Conditions
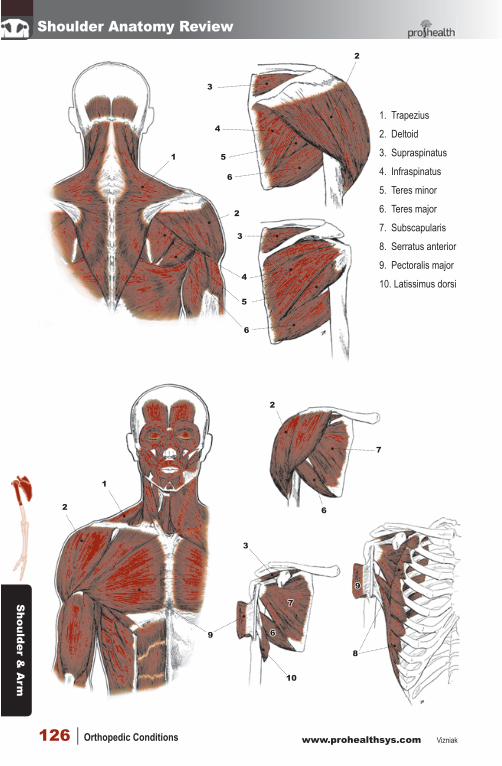
Shoulder Anatomy Review
1. Trapezius
2. Deltoid
3. Supraspinatus
4. Infraspinatus
5. Teres minor
6. Teres major
7. Subscapularis
8. Serratus anterior
9. Pectoralis major
10. Latissimus dorsi
1
6
5
4
3
6
5
4
3
2
2
2
2
7
6
7
6
10
9
9
8
3
1
4-shoulder NMS.indd 126 2014-01-14 11:05:15 AM
Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 127
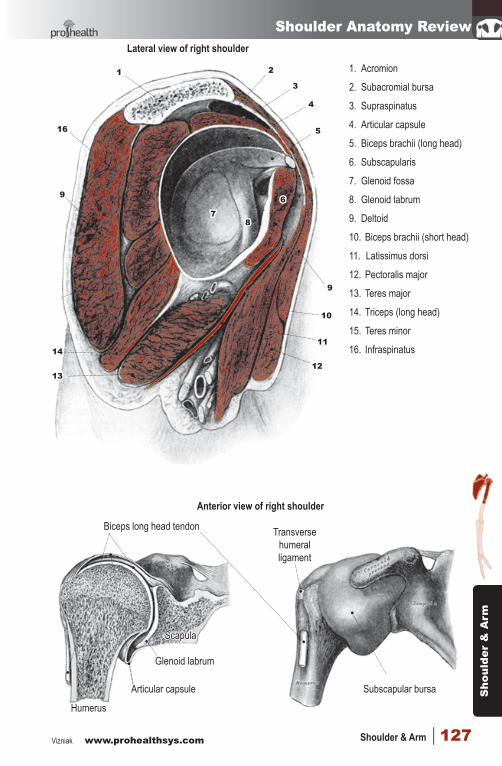
Shoulder Anatomy ReviewLateral view of right shoulder
1. Acromion
2. Subacromial bursa
3. Supraspinatus
4. Articular capsule
5. Biceps brachii (long head)
6. Subscapularis
7. Glenoid fossa
8. Glenoid labrum
9. Deltoid
10. Biceps brachii (short head)
11. Latissimus dorsi
12. Pectoralis major
13. Teres major
14. Triceps (long head)
15. Teres minor
16. Infraspinatus
16
9
14
13
11
10
9
87
6
5
4
3
21
12
Anterior view of right shoulder
Subscapular bursa
Transverse humeral ligament
Articular capsule
Glenoid labrum
Biceps long head tendon
Scapula
Humerus
4-shoulder NMS.indd 127 2014-01-14 11:05:15 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak128 | Orthopedic Conditions
Scapulocostal Syndrome
BasicsDefinition: common musculoskeletal, pain-producing
syndrome that affects the posterior shoulder area & may be associated with altered scapulothoracic motion, ‘snapping shoulder’ & bursitis
Pathophysiology: multiple potential pain generators due to abnormal relationship between scapula & ribs resulting in pain referral over region of posterior scapula, back & shoulder
Possible causes:• Poor posture (rounded shoulder, forward head
tilt, suboccipital extension & slouching)• MFTP in serratus anterior or subscapularis• Adhesions or scar tissue formation• Exostosis of ribs under scapula• Traumatic injury (whiplash, direct blow)
Demographics Incidence: very common (no specific data) Age: 25-50 Gender: female > male Risk factors: poor posture (desk jobs/students or
activities with arms extended in front of body for long periods of time)
Overuse during sports/work (swimming, gymnastics, laborers)
Diagnosis
History• Pain in scapular region, possible crepitus with
movement or dyskinesis• Possible history of prior injury: whiplash, repetitive
activity (swimming, throwing), poor ergonomic set-up of desk work station, hyperkyphosis
• Pain with shoulder activities or prolonged sitting
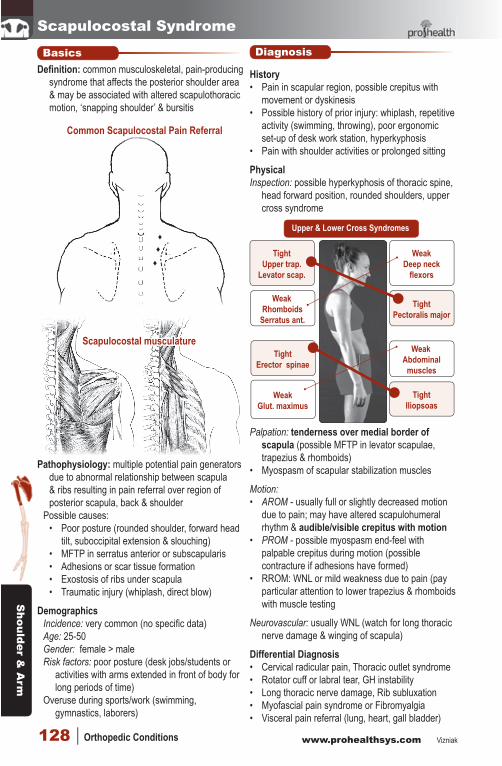
PhysicalInspection: possible hyperkyphosis of thoracic spine,
head forward position, rounded shoulders, upper cross syndrome
Upper & Lower Cross Syndromes
TightUpper trap.
Levator scap.
WeakRhomboids
Serratus ant.
WeakDeep neck
flexors
WeakAbdominal
muscles
WeakGlut. maximus
TightPectoralis major
TightIliopsoas
TightErector spinae
Palpation: tenderness over medial border of scapula (possible MFTP in levator scapulae, trapezius & rhomboids)
• Myospasm of scapular stabilization muscles
Motion: • AROM - usually full or slightly decreased motion
due to pain; may have altered scapulohumeral rhythm & audible/visible crepitus with motion
• PROM - possible myospasm end-feel with palpable crepitus during motion (possible contracture if adhesions have formed)
• RROM: WNL or mild weakness due to pain (pay particular attention to lower trapezius & rhomboids with muscle testing
Neurovascular: usually WNL (watch for long thoracic nerve damage & winging of scapula)
Differential Diagnosis • Cervical radicular pain, Thoracic outlet syndrome• Rotator cuff or labral tear, GH instability• Long thoracic nerve damage, Rib subluxation• Myofascial pain syndrome or Fibromyalgia• Visceral pain referral (lung, heart, gall bladder)
♦♦♦
Scapulocostal musculature
Common Scapulocostal Pain Referral
4-shoulder NMS.indd 128 2014-01-14 11:05:16 AM
Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 129
Scapulocostal SyndromeSpecial Test• Orthopedic tests are mainly used to rule out other
pathologies• Impingement - Hawkins-Kennedy, Impingement
sign, Painful arc, Passive Neer’s test• Rotator cuff - Empty can, Arm drop test, Lift-off
test, Bear-hug test, Trumpeter’s test• Glenohumeral joint stability - Ant/Post drawer, Ant/
Post apprehension, Load & shift, Fagean’s• C-cpine tests - Cervical compression/distraction
Diagnostic Imaging• Usually not indicated but may be used to rule out
other pathologies• Ultrasonography may show fluid collection in
scapulothoracic bursa indicating bursitis
Treatment
General Measures• Initial reduction of pain & discomfort (PRICE)• Correct postural faults, get patient up and moving!• Restore altered muscle activation or coordination
during shoulder motion (scapulohumeral rhythm)
Massage Therapy• Address tissue contracture, MFTP & myospasm• Myofascial release, MFTP therapy, Swedish• Heat & hydrotherapy
Osseous Mobes/Manipulation• Extremely effective in treating condition• Assess & treat costal dysfunctions• Also focus on extension restrictions/flexion
malpositions of thoracic sine• Address compensations in C-spine, shoulders &
lumbar spine (mobilize scapula)
Electrotherapy• Consider IFC & TENS for pain reduction• Ultrasound to improve healing (iontophoresis)• Diathermy to increase deep heat & blood flow
Acupuncture• Local shoulder points• LI15, 16, SJ5, 14, SI3, 10, 15, LI4,
Diet & Botanicals• Anti-inflammatory diet, ↑ Vit A,C, Zn, Mg, fish oils• Salix alba (analgesic, anti-inflammatory),
Boswellia serrata, Curcumine longa
Medications• NSAIDs, muscle relaxants• Some evidence to support scapulothoracic bursal
injections of Hyaluronic Acid & corticosteroids
• Hyaluronic Acid is thought to act as a lubricant & offer protective effects (maintain tissue structure & inhibit neovascularization)
Surgery (rarely required)• Arthroscopic or open methods are only indicated
in patients with a clearly identifiable osseous or soft tissue mass
Follow-up
Rehabilitation Program• Realize that scapula stabilization requires
coordinated muscle control of upper & lower trapezius & rhomboid muscles coupled with serratus anterior during activities - shoulder actions are further coupled to the scapula via the rotator cuff muscles & deltoid
• During acute stage focus on restore basic muscle control & balanced as well as basic stretches within the patients tolerance
• In recovery phase progress to more advanced activities (PNF, increased weight & endurance) paying particular attention to try & activate middle/lower trapezius & serratus anterior• Prone horizontal abduction with the shoulder at
90º & 120º abduction
Prevention/Education• Ergonomic evaluation
of work station & daily sitting habits are a must
• Educate patient on importance of proper posture
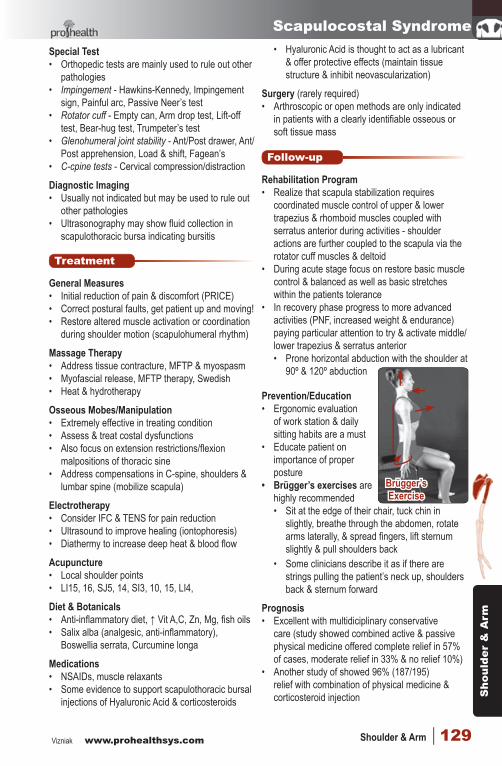
• Brügger’s exercises are highly recommended• Sit at the edge of their chair, tuck chin in
slightly, breathe through the abdomen, rotate arms laterally, & spread fingers, lift sternum slightly & pull shoulders back
• Some clinicians describe it as if there are strings pulling the patient’s neck up, shoulders back & sternum forward
Prognosis• Excellent with multidiciplinary conservative
care (study showed combined active & passive physical medicine offered complete relief in 57% of cases, moderate relief in 33% & no relief 10%)
• Another study of showed 96% (187/195) relief with combination of physical medicine & corticosteroid injection
Brügger’s Exercise
4-shoulder NMS.indd 129 2014-01-14 11:05:16 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak130 | Orthopedic Conditions
Rotator Cuff StrainBasics
Definition: stretch or tear of the rotator cuff tendon or muscle belly. Grade of strain depends on amount of fibers damaged, degree of pain & strength of muscle contraction
Give an exact diagnosis of tendons involved as it will change treatment - do NOT call an isolated subscapularis tear a rotator cuff strain!!!
Pathophysiology• Degenerative strain - associated with minimal
trauma, often prior to chronic tendonitis or chronic impingement syndrome
• Acute traumatic strain – can present following a specific trauma (FOOSH, or a single violent blow or force to shoulder)• Prolonged or repetitive overuse of muscle/
tendon over a short period of time• Lifting or pulling• Pre-existing impingement syndrome
Demographics Incidence: ~30% of population Age: degenerative type is common in elderly Gender: male > female Risk factors: motions that require repeated overhead motions or forceful pulling motions
• Sports injuries or trauma• Athletes (esp those making repetitive motions):
• Baseball pitchers, swimmers• Quarterbacks, volleyball, boxers• Kayaking, tennis
• Poor nutrition, obesity & reduced strength or flexibility & previous injury
History• Pain over superior lateral shoulder• Pain aggravated by leaning on elbow & pushing
upwards on shoulder• Popping or tearing sensation at moment of injury,
followed by pain & weakness• Edema, erythema and/or hematoma of shoulder,
axilla, and/or upper arm (severe case)• Intolerance to overhead activity• Pain at night, especially when lying directly on
affected shoulder• Weakness may be reported, but is often masked
by pain and is usually found only through examination. With longer standing pain, the opposite shoulder is favored and gradually loss of motion and weakness may develop
• Loss of strength, possible crepitus with motion
DiagnosisPhysical• Inspection: normal bone and soft tissue outlines
• Protective shoulder hike may be seen• Possible wasting in the supraspinatus and
infraspinatus fossae (chronic cases)• Palpation: tenderness over rotator cuff muscles
• Myospasm & myofascial trigger points• Motion:
• AROM: weakness or pain during abduction, external rotation, internal rotation, or any combination of these actions - depends on which muscle(s) is specifically damaged
• PROM: pain if impingement occurs or pain at end-range if muscle is stretches
• RROM: pain and weakness during abduction, lateral &/or medial rotation
Differential Diagnosis • Supraspinatus rupture, Impingement syndrome• GH ligament laxity or Instability• Labral tear• Biceps strain/ tendinopathy• Remember: shoulder pain can be referred from
either the chest or abdomen (coronary artery disease, pulmonary tumors, & gallbladder disease)
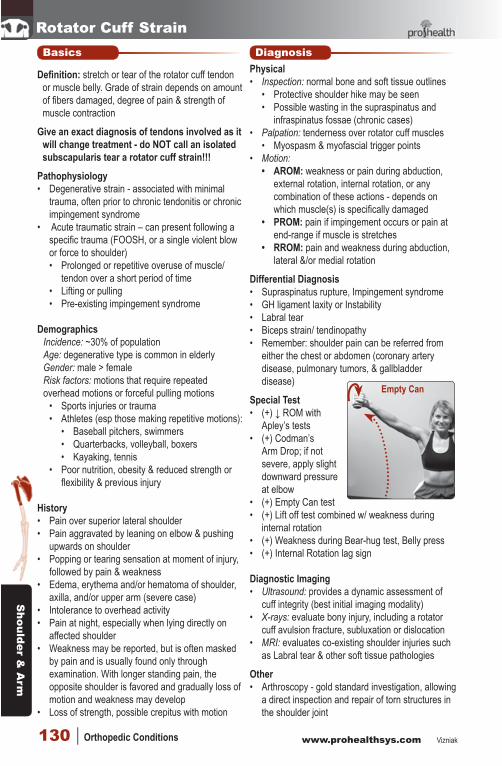
Special Test• (+) ↓ ROM with
Apley’s tests• (+) Codman’s
Arm Drop; if not severe, apply slight downward pressure at elbow
• (+) Empty Can test• (+) Lift off test combined w/ weakness during
internal rotation• (+) Weakness during Bear-hug test, Belly press• (+) Internal Rotation lag sign
Diagnostic Imaging• Ultrasound: provides a dynamic assessment of
cuff integrity (best initial imaging modality)• X-rays: evaluate bony injury, including a rotator
cuff avulsion fracture, subluxation or dislocation• MRI: evaluates co-existing shoulder injuries such
as Labral tear & other soft tissue pathologies
Other• Arthroscopy - gold standard investigation, allowing
a direct inspection and repair of torn structures in the shoulder joint
Empty Can
4-shoulder NMS.indd 130 2014-01-14 11:05:16 AM
Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 131
Rotator Cuff StrainTreatment
General Measures• PRICE - avoid prolong immobilization (increases
risk of Frozen shoulder)• Avoid actions that cause aggravation• Consider cold application if acute, switch to heat
in chronic cases• Avoid premature return to activity - can result in
chronic tendinopathy or impingement
Massage Therapy• Can be started 2 days to 2 weeks after the injury
depending on severity & patient tolerance• Myofascial trigger point therapy, myofascial
release & cross fiber, pin & stretch
Osseous Mobes/Manipulation• Do not perform on shoulder during acute phase• Initially focus on thoracic & cervical spine then
move to shoulder mobes & manip. as tolerated
Electrotherapy• Ultrasound - set at a level that produces a mild
feeling of warmth (increase local blood flow, help activate cells involved in healing process & speed repair of tissue)
• Interferential or microcurrent may offer benefit
Acupuncture• LI4, SI3, SJ4, 5 & 6; UB 17, 18, & 19• LV3, GB34, SP10, UB17
Diet & Botanicals• ↑ protein intake to help muscle/tendon heal• Vitamin C, E, selenium, fish oils, Ca, Mg• Anti-inflammatory: Curcuma longa, Boswellia• Analgesic: Salix alba, Filipendula ulmaris• Vulnerary: Arnica montana, Symphytum officinale
Medications• NSAIDs (Aspirin, Ibuprofen, Celebrex)• Injection of steroid medication directly into
injury site to help reduce any inflammation may be needed in chronic rotator cuff tear to allow rehabilitation to proceed
Surgery (last resort)• Arthroscpic, open or or mini-open repair• After surgical repair ~80% of patients achieve
a satisfactory result (adequate pain relief, restoration or improvement of function, improvement in range of motion)
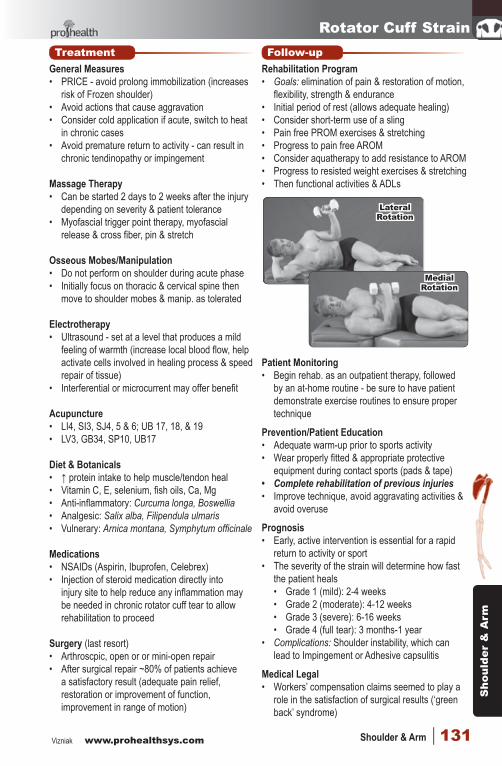
Follow-upRehabilitation Program• Goals: elimination of pain & restoration of motion,
flexibility, strength & endurance• Initial period of rest (allows adequate healing)• Consider short-term use of a sling• Pain free PROM exercises & stretching• Progress to pain free AROM• Consider aquatherapy to add resistance to AROM• Progress to resisted weight exercises & stretching• Then functional activities & ADLs
Patient Monitoring• Begin rehab. as an outpatient therapy, followed
by an at-home routine - be sure to have patient demonstrate exercise routines to ensure proper technique
Prevention/Patient Education• Adequate warm-up prior to sports activity • Wear properly fitted & appropriate protective
equipment during contact sports (pads & tape)• Complete rehabilitation of previous injuries• Improve technique, avoid aggravating activities &
avoid overuse
Prognosis• Early, active intervention is essential for a rapid
return to activity or sport• The severity of the strain will determine how fast
the patient heals • Grade 1 (mild): 2-4 weeks• Grade 2 (moderate): 4-12 weeks• Grade 3 (severe): 6-16 weeks• Grade 4 (full tear): 3 months-1 year
• Complications: Shoulder instability, which can lead to Impingement or Adhesive capsulitis
Medical Legal• Workers’ compensation claims seemed to play a
role in the satisfaction of surgical results (‘green back’ syndrome)
Lateral Rotation
Medial Rotation
4-shoulder NMS.indd 131 2014-01-14 11:05:16 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak132 | Orthopedic Conditions
Subscapularis Tendinopathy
BasicsDefinition: overuse or traumatic injury to the
subscapularis tendon resulting in pain, swelling & functional limitation
Pathophysiology: overuse or traumatic damage to the subscapularis tendon or muscle; actions or activities that may cause injury include:• Overuse with repeated
active internal rotation especially when combined with over head activities (throwing, swimming)
• Single traumatic event (rapid excessive stretch into external rotation, ballistic throw without warm-up)
Demographics Incidence: common (esp. athletic populations) Age: 20-40 (can happen at any age >20) Gender: male > female (usually sport/work related) Risk factors: may be predisposed to compensation
& improper biomechanics of shoulder action if there is co-existing Anterior instability, Hypermobility or Impingement
• Increased age & obesity Diagnosis
History• Usually gradual onset of shoulder pain felt in
anterior or posterior axillary fold• Pain is worse with internal rotation (esp. over
head) activities - giving a high five ☺• Pain may be “sharp” with activity but decreases
with warm-up, worse with excessive activity• Possible prior history of trauma or instability
PhysicalInspection: usually WNLPalpation: tenderness over subscapularis tendon or
lesser tubercle of humerus Motion:• AROM - external rotation may be painful at end-
range if subscapularis tendon is stretched• PROM painful or myospasm end-feel with ext. rot.• RROM - weakness on resisted internal rotationNeurovascular: usually WNL
Differential Diagnosis • Other Rotator cuff tear, Adhesive capsulitis• Labral tear, Impingement, Instability
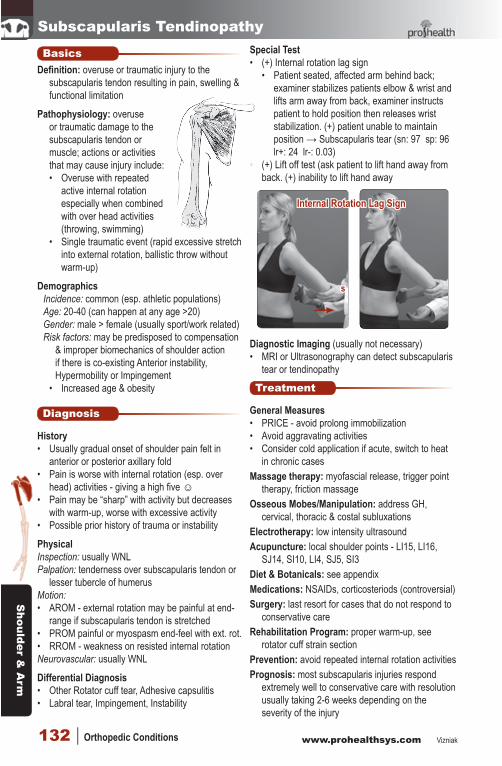
Special Test• (+) Internal rotation lag sign
• Patient seated, affected arm behind back; examiner stabilizes patients elbow & wrist and lifts arm away from back, examiner instructs patient to hold position then releases wrist stabilization. (+) patient unable to maintain position → Subscapularis tear (sn: 97 sp: 96 lr+: 24 lr-: 0.03)
• (+) Lift off test (ask patient to lift hand away from back. (+) inability to lift hand away
s
Diagnostic Imaging (usually not necessary)• MRI or Ultrasonography can detect subscapularis
tear or tendinopathy
Treatment
General Measures• PRICE - avoid prolong immobilization• Avoid aggravating activities• Consider cold application if acute, switch to heat
in chronic casesMassage therapy: myofascial release, trigger point
therapy, friction massageOsseous Mobes/Manipulation: address GH,
cervical, thoracic & costal subluxationsElectrotherapy: low intensity ultrasoundAcupuncture: local shoulder points - LI15, LI16,
SJ14, SI10, LI4, SJ5, SI3Diet & Botanicals: see appendixMedications: NSAIDs, corticosteriods (controversial)Surgery: last resort for cases that do not respond to
conservative careRehabilitation Program: proper warm-up, see
rotator cuff strain sectionPrevention: avoid repeated internal rotation activitiesPrognosis: most subscapularis injuries respond
extremely well to conservative care with resolution usually taking 2-6 weeks depending on the severity of the injury
Internal Rotation Lag Sign
••
4-shoulder NMS.indd 132 2014-01-14 11:05:16 AM
Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 133
Supraspinatus TendinopathyBasics
Definition: overuse or traumatic injury to the supraspinatis tendon &/or continuous soft tissues resulting in pain, swelling & functional limitation
Pathophysiology: overuse or traumatic damage to the supraspinatus tendon or muscle; actions or activities that may cause injury include:• Overuse with repeated
active internal rotation especially when combined with over head activities (throwing, swimming)
Demographics Incidence: ~50% of shoulder pain cases (common) Age: 20-40 (can happen at any age >20) Gender: male > female (usually sport/work related) Risk factors: direct trauma (shoulder tackle)
• Overhead activities (laborers, sports, swimming, basket ball, tennis)
Diagnosis
History• Usually gradual onset of dull, achy shoulder pain
directly below acromion that is worse following activity
• May affect ADLs (getting dressed or sleeping)• Pain is better with rest or ice• Possible prior history of trauma or instability
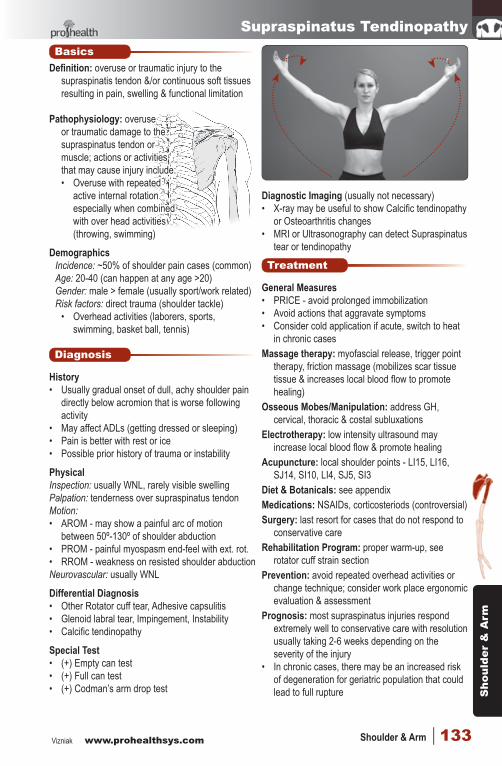
PhysicalInspection: usually WNL, rarely visible swellingPalpation: tenderness over supraspinatus tendon Motion:• AROM - may show a painful arc of motion
between 50º-130º of shoulder abduction• PROM - painful myospasm end-feel with ext. rot.• RROM - weakness on resisted shoulder abductionNeurovascular: usually WNL
Differential Diagnosis • Other Rotator cuff tear, Adhesive capsulitis• Glenoid labral tear, Impingement, Instability• Calcific tendinopathy
Special Test• (+) Empty can test• (+) Full can test• (+) Codman’s arm drop test
Diagnostic Imaging (usually not necessary)• X-ray may be useful to show Calcific tendinopathy
or Osteoarthritis changes• MRI or Ultrasonography can detect Supraspinatus
tear or tendinopathy
Treatment
General Measures• PRICE - avoid prolonged immobilization• Avoid actions that aggravate symptoms• Consider cold application if acute, switch to heat
in chronic casesMassage therapy: myofascial release, trigger point
therapy, friction massage (mobilizes scar tissue tissue & increases local blood flow to promote healing)
Osseous Mobes/Manipulation: address GH, cervical, thoracic & costal subluxations
Electrotherapy: low intensity ultrasound may increase local blood flow & promote healing
Acupuncture: local shoulder points - LI15, LI16, SJ14, SI10, LI4, SJ5, SI3
Diet & Botanicals: see appendixMedications: NSAIDs, corticosteriods (controversial)Surgery: last resort for cases that do not respond to
conservative careRehabilitation Program: proper warm-up, see
rotator cuff strain sectionPrevention: avoid repeated overhead activities or
change technique; consider work place ergonomic evaluation & assessment
Prognosis: most supraspinatus injuries respond extremely well to conservative care with resolution usually taking 2-6 weeks depending on the severity of the injury
• In chronic cases, there may be an increased risk of degeneration for geriatric population that could lead to full rupture
4-shoulder NMS.indd 133 2014-01-14 11:05:16 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak134 | Orthopedic Conditions
Impingement SyndromeBasics
Definition: narrowing of space between acromion & humeral that results in ‘pinching’ of the rotator cuff tendons (esp. supraspinatus) &/or biceps brachii long head
Pathophysiology: (stages after Neer)• Stage 1: usually < 25 yrs old - edema &
hemorrhage resulting from excessive overhead activities; reversible with conservative treatment
• Stage 2: usually 25-40 yrs - tendinopathy resulting from repeated episodes of mechanically induced inflammation; shoulder functions satisfactorily during light activity but becomes symptomatic after vigorous overhead use, excessive repetitive use or heavy lifting; conservative treatment may offer benefit
• Stage 3: > 40 yrs - trophic changes in rotator cuff, biceps, & adjacent bone (osteophytes) leading to tendon ruptures & alterations of acromion & greater tuberosity; progressive disability often leads to surgical intervention
Demographics Incidence: higher in athletes & laborers Age: 25-40 yrsGender: male > female (2:1) Risk factors: prior injury or repeated overhead
activities (swimmers, baseball, volleyball, painters, racket sports), GH instability, enlarged acromion or coracoid process
Diagnosis
History• Dull achy shoulder pain that is worse with
shoulder abduction above 80º, overhead activity or excessive use
• Sudden onset of sharp pain in shoulder with tearing sensation suggests rotator cuff tear
• Gradual increase in shoulder pain with overhead activities suggests impingement
• Pain may be worse after sleep if arm was abducted over head or sleeping on a firm mattress (ask about sleeping position - very important)
PhysicalInspection: check muscle atrophy, asymmetry &
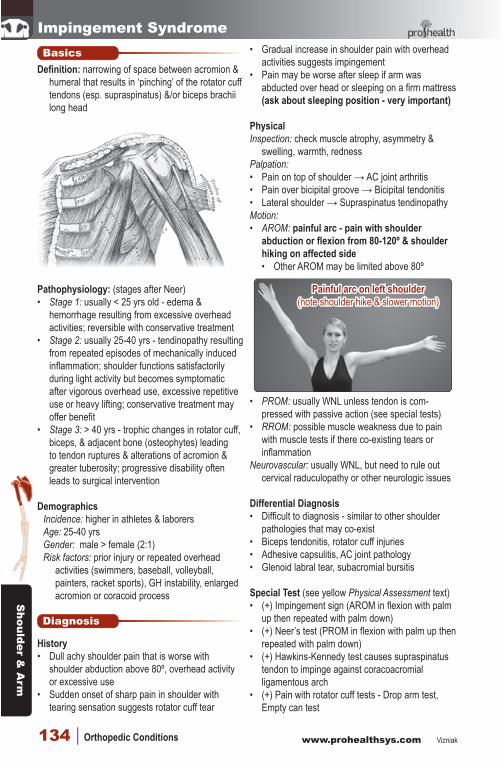
swelling, warmth, rednessPalpation: • Pain on top of shoulder → AC joint arthritis• Pain over bicipital groove → Bicipital tendonitis• Lateral shoulder → Supraspinatus tendinopathyMotion: • AROM: painful arc - pain with shoulder
abduction or flexion from 80-120º & shoulder hiking on affected side• Other AROM may be limited above 80º
• PROM: usually WNL unless tendon is com-pressed with passive action (see special tests)
• RROM: possible muscle weakness due to pain with muscle tests if there co-existing tears or inflammation
Neurovascular: usually WNL, but need to rule out cervical raduculopathy or other neurologic issues
Differential Diagnosis • Difficult to diagnosis - similar to other shoulder
pathologies that may co-exist • Biceps tendonitis, rotator cuff injuries• Adhesive capsulitis, AC joint pathology• Glenoid labral tear, subacromial bursitis
Special Test (see yellow Physical Assessment text)• (+) Impingement sign (AROM in flexion with palm
up then repeated with palm down)• (+) Neer’s test (PROM in flexion with palm up then
repeated with palm down)• (+) Hawkins-Kennedy test causes supraspinatus
tendon to impinge against coracoacromial ligamentous arch
• (+) Pain with rotator cuff tests - Drop arm test, Empty can test
Painful arc on left shoulder(note shoulder hike & slower motion)
4-shoulder NMS.indd 134 2014-01-14 11:05:16 AM

Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 135
Impingement Syndrome
Diagnostic Imaging: (usually not indicated)• X-rays: may be indicated to rule out arthritis or
other pathologies• MRI: best imaging to evaluate soft tissue changes
& rule in or out other shoulder pathologies
Other• Impingement test: injection 10 mL of 1% lidocaine
solution into subacromial space & repeat special impingement test - (+) = elimination or significant reduction of pain
Treatment
General Measures• Pain reduction & avoidance of aggravating activity• PRICE, NSAIDs• Ensure proper warm-up prior to activity
Massage Therapy• Myofascial release & trigger point therapy for
surrounding shoulder muscles• Cross fiber massage if not in acute stage• In subacute phase consider PNF stretching in
office (internal & external rotation; extension/flexion; add/abduction)
Osseous Mobes/Manipulation• Address subluxations of AC & SC joints & cervical
& thoracic spine
• Direct GH mobes & manip are indicated in cases that are not acute or hypermobile/unstable
Electrotherapy• TENS for pain reduction• Ultrasound therapy • Some studies show short term benefit with high-
intensity laser therapy (HILT)
Acupuncture• Local shoulder point & LI4, 15, 16, SI3, 10, SJ5, 14
Diet & Botanicals: see appendix
Medications• NSAIDs, Corticosteroid injection (controversial)• Glyceryl trinitrate/nitroglycerin
Surgery (last resort)• Depends on cause (open or arthroscopic)
resection of distal clavicle, excision of osteophytes, repair rotator cuff tear, acromioplasty, subacromial decompression
Follow-up
Rehabilitation Program• Ensure proper warm-up before activity• Acute goals - relieve pain & inflammation
• Ice & rest shoulder, avoid aggravation• PFROM, pendulum arm swings, AROM• Stretching as tolerated (esp. posterior capsule)
• Subacute goals - normalize ROM, perform symptom free ADLs, ↑ strength & flexibility• Progress to PFAROM then mild resistance
exercises (weights, tubing, aqua aerobics)• Eventually progress to more advanced
activities (increased resistance, activities that mimic sport or work activity, PNF)
Prevention/Patient Education• Evaluation of sport or work technique may be
needed to observe ergonimics• Avoid sleeping on a hard mattress with shoulder
abducted over head
Prognosis• Depends on coexisting factors (instability, arthritis,
labral or cuff tears, longer standing condition in older patient)
• 60-90% of simple case will usually resolve quick to pre-injury status (2-6 wks)
• Complicated cases can take much longer & should involve secondary consultation
Impingement Sign (palm up then palm down)
Neer’s Test
Hawkins Kennedy
4-shoulder NMS.indd 135 2014-01-14 11:05:17 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak136 | Orthopedic Conditions
Bicipital TendinopathyBasics
Definition: inflammation of biceps brachii long head tendon & surrounding sheath, biceps musculotendinous junction is particularly susceptible to overuse injuries; usually co-exists with other pathologies of the shoulder including rotator cuff tendinopathy & tears, GH instability & other muscle imbalances
Pathophysology (4 main theories): • Mechanical theory: repetitive loading of tendon
results in microscopic degeneration → fibroplasia within tendon → scar tissue
• Vascular theory: tendon degeneration occurs as a result of focal areas of vascular compromise
• Neural modulation: tendinopathy results from neurally mediated mast cell degranulation & release of substance P
• Subluxating tendon: tendon is held in place by transverse humeral ligament, rupture of ligament or shallow bicipital groove allows tendon to repeatedly shift out of place in bicipital groove
Demographics Incidence: very common Age: 20-30s most commonGender: male > female (2:1) Risk factors:
• Repetitive overhead activities• Prior injuries to shoulder• Sport specific - pitchers, swimmers, gymnasts,
racquet sports, rowing
History• History usually suggests diagnosis, but clinical
tests are needed to confirm• Pain over the anterior shoulder & bicipital groove• Pain is worst with activity especially with repeated
shoulder & elbow flexion &/or supination & overhead activities
• ↓ pain with rest, massage, heat• Possible repeatable ‘snapping’ or ‘clicking’ with
subluxation of tendon
PhysicalInspection: possible mild swelling & redness (rare)• Patient may have a tendency to want to hold or
rub shoulder to relieve painPalpation: hallmark sign is local tenderness to
palpation over the bicipital grooveMotion: possible repeated snapping if tendon is
subluxating out of bicipital groove
• PROM: usually WNL until end-play stretches bicipital tendon → pain
• AROM: possible aggravation of symptoms with shoulder & elbow flexion &/or supination
• RROM: pain with resisted shoulder & elbow flexion
Neurovascular screen: WNL
Diagnosis
Differential Diagnosis • Glenoid labral tear (often co-exist)• Impingement syndrome• Rotator cuff tear• GH instability• Inflam. arthropathy
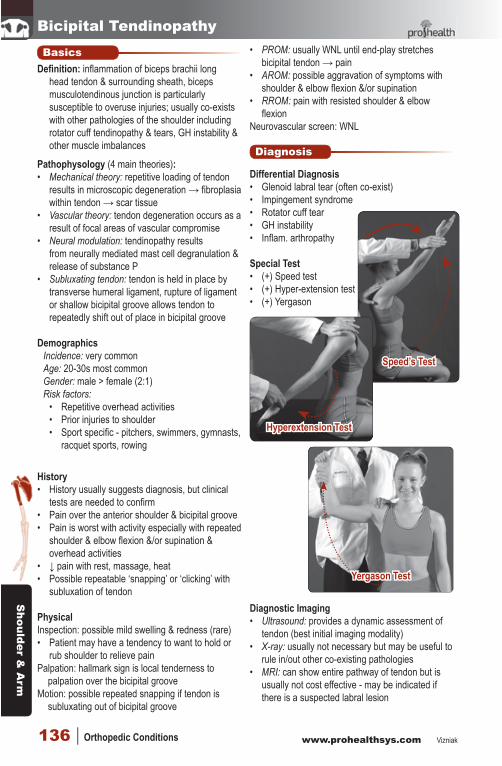
Special Test• (+) Speed test• (+) Hyper-extension test• (+) Yergason
Diagnostic Imaging• Ultrasound: provides a dynamic assessment of
tendon (best initial imaging modality) • X-ray: usually not necessary but may be useful to
rule in/out other co-existing pathologies • MRI: can show entire pathway of tendon but is
usually not cost effective - may be indicated if there is a suspected labral lesion
Speed’s Test
Hyperextension Test
Yergason Test
4-shoulder NMS.indd 136 2014-01-14 11:05:17 AM
Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 137
Bicipital TendinopathyTreatment
General Measures• PRICE to reduce pain & inflammation
• Ice area 10-15 min 2-3 x/day for first 48 hrs• Short term avoidance of aggravating motions
(above head activities)
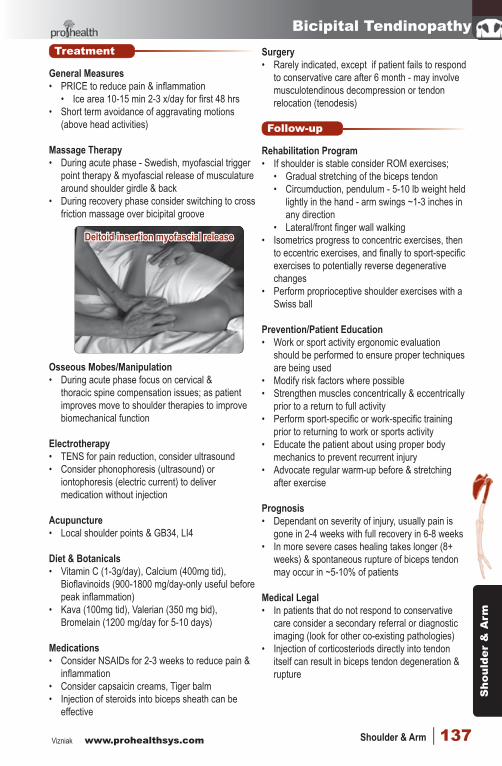
Massage Therapy• During acute phase - Swedish, myofascial trigger
point therapy & myofascial release of musculature around shoulder girdle & back
• During recovery phase consider switching to cross friction massage over bicipital groove
Osseous Mobes/Manipulation• During acute phase focus on cervical &
thoracic spine compensation issues; as patient improves move to shoulder therapies to improve biomechanical function
Electrotherapy• TENS for pain reduction, consider ultrasound• Consider phonophoresis (ultrasound) or
iontophoresis (electric current) to deliver medication without injection
Acupuncture• Local shoulder points & GB34, LI4
Diet & Botanicals• Vitamin C (1-3g/day), Calcium (400mg tid),
Bioflavinoids (900-1800 mg/day-only useful before peak inflammation)
• Kava (100mg tid), Valerian (350 mg bid), Bromelain (1200 mg/day for 5-10 days)
Medications• Consider NSAIDs for 2-3 weeks to reduce pain &
inflammation• Consider capsaicin creams, Tiger balm• Injection of steroids into biceps sheath can be
effective
Surgery• Rarely indicated, except if patient fails to respond
to conservative care after 6 month - may involve musculotendinous decompression or tendon relocation (tenodesis)
Follow-up
Rehabilitation Program• If shoulder is stable consider ROM exercises;
• Gradual stretching of the biceps tendon• Circumduction, pendulum - 5-10 lb weight held
lightly in the hand - arm swings ~1-3 inches in any direction
• Lateral/front finger wall walking• Isometrics progress to concentric exercises, then
to eccentric exercises, and finally to sport-specific exercises to potentially reverse degenerative changes
• Perform proprioceptive shoulder exercises with a Swiss ball
Prevention/Patient Education• Work or sport activity ergonomic evaluation
should be performed to ensure proper techniques are being used
• Modify risk factors where possible• Strengthen muscles concentrically & eccentrically
prior to a return to full activity• Perform sport-specific or work-specific training
prior to returning to work or sports activity• Educate the patient about using proper body
mechanics to prevent recurrent injury • Advocate regular warm-up before & stretching
after exercise
Prognosis• Dependant on severity of injury, usually pain is
gone in 2-4 weeks with full recovery in 6-8 weeks• In more severe cases healing takes longer (8+
weeks) & spontaneous rupture of biceps tendon may occur in ~5-10% of patients
Medical Legal• In patients that do not respond to conservative
care consider a secondary referral or diagnostic imaging (look for other co-existing pathologies)
• Injection of corticosteriods directly into tendon itself can result in biceps tendon degeneration & rupture
Deltoid insertion myofascial release
4-shoulder NMS.indd 137 2014-01-14 11:05:17 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak138 | Orthopedic Conditions
Demographics Incidence: 7% of painful shoulders (3-20% general population) Age: peak incidence 30-50 years Gender: female > male (2:1)Risk factors: exact cause is not known
• Chronic impingement, trauma• Wear & tear (repeated microtrauma)• Aging, genetic/metabolic factors
Diagnosis
History• Chronic, mild pain with occasional flare-up• Pain may be aggravated by overhead activity or
sleeping on the affected shoulder• Possible stiffness or weakness
PhysicalInspection: possible swelling or rednessPalpation: possible tenderness or warmth over
affected tendonMotion: possible intense pain with motion• Possible decreased ROM into shoulder abduction• Painful arc of motion from 70-120 º of flexion or
abduction
Differential Diagnosis • Frozen shoulder• Impingement syndrome• Rotator cuff tear (elderly)• Biceps tendinopathy
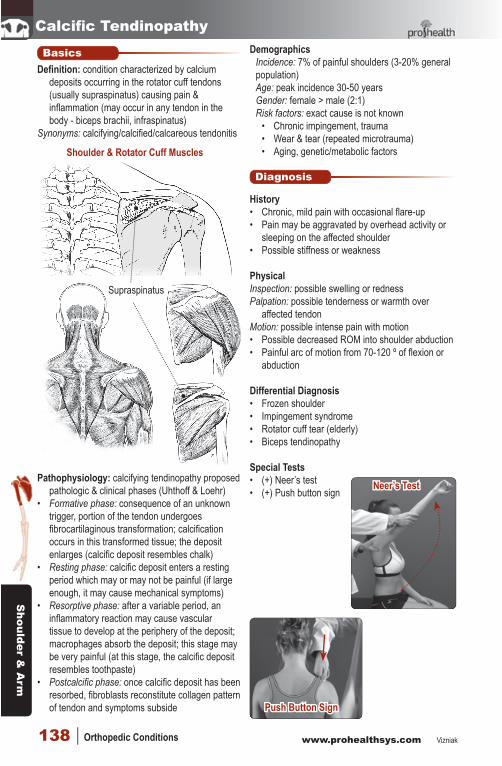
Special Tests• (+) Neer’s test• (+) Push button sign
Calcific Tendinopathy
Push Button Sign
BasicsDefinition: condition characterized by calcium
deposits occurring in the rotator cuff tendons (usually supraspinatus) causing pain & inflammation (may occur in any tendon in the body - biceps brachii, infraspinatus)
Synonyms: calcifying/calcified/calcareous tendonitis
Pathophysiology: calcifying tendinopathy proposed pathologic & clinical phases (Uhthoff & Loehr)
• Formative phase: consequence of an unknown trigger, portion of the tendon undergoes fibrocartilaginous transformation; calcification occurs in this transformed tissue; the deposit enlarges (calcific deposit resembles chalk)
• Resting phase: calcific deposit enters a resting period which may or may not be painful (if large enough, it may cause mechanical symptoms)
• Resorptive phase: after a variable period, an inflammatory reaction may cause vascular tissue to develop at the periphery of the deposit; macrophages absorb the deposit; this stage may be very painful (at this stage, the calcific deposit resembles toothpaste)
• Postcalcific phase: once calcific deposit has been resorbed, fibroblasts reconstitute collagen pattern of tendon and symptoms subside
Neer’s Test
Shoulder & Rotator Cuff Muscles
Supraspinatus
4-shoulder NMS.indd 138 2014-01-14 11:05:17 AM
Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 139
Calcific TendinopathyDiagnostic Imaging• Ultrasonography: with experienced operators,
ultrasound is more sensitive than plain x-rays & does not expose patient to radiation
• X-ray: common way to confirm diagnosis• Deposits range from a toothpaste to a chalky
consistency• Usually 1-2 cm in length• Sensitivity of x-rays for detecting calcific
deposits is 0.90 (compared to ultrasonography as standard)
• MRI (not indicated unless other co-existing pathology is suspected) may show • T1 - decreased signal intensity• T2 - increased signal intensity if edema is
present
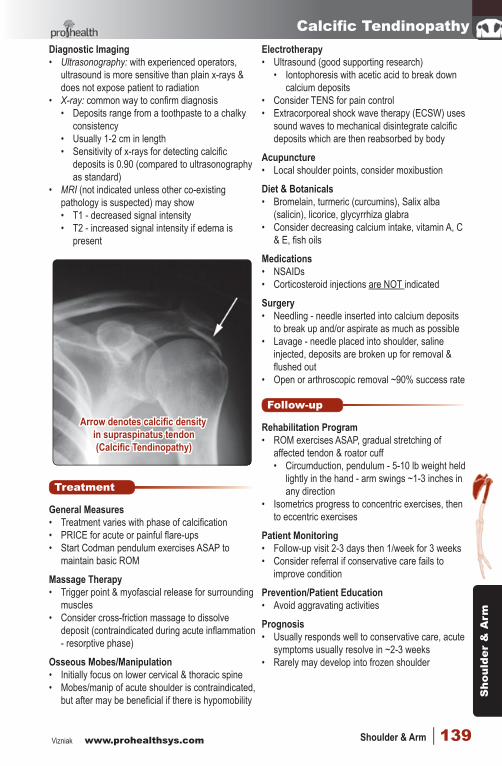
Arrow denotes calcific density in supraspinatus tendon(Calcific Tendinopathy)
Treatment
General Measures• Treatment varies with phase of calcification• PRICE for acute or painful flare-ups• Start Codman pendulum exercises ASAP to
maintain basic ROM
Massage Therapy• Trigger point & myofascial release for surrounding
muscles• Consider cross-friction massage to dissolve
deposit (contraindicated during acute inflammation - resorptive phase)
Osseous Mobes/Manipulation• Initially focus on lower cervical & thoracic spine• Mobes/manip of acute shoulder is contraindicated,
but after may be beneficial if there is hypomobility
Electrotherapy• Ultrasound (good supporting research)
• Iontophoresis with acetic acid to break down calcium deposits
• Consider TENS for pain control• Extracorporeal shock wave therapy (ECSW) uses
sound waves to mechanical disintegrate calcific deposits which are then reabsorbed by body
Acupuncture• Local shoulder points, consider moxibustion
Diet & Botanicals• Bromelain, turmeric (curcumins), Salix alba
(salicin), licorice, glycyrrhiza glabra• Consider decreasing calcium intake, vitamin A, C
& E, fish oils
Medications• NSAIDs• Corticosteroid injections are NOT indicated
Surgery• Needling - needle inserted into calcium deposits
to break up and/or aspirate as much as possible• Lavage - needle placed into shoulder, saline
injected, deposits are broken up for removal & flushed out
• Open or arthroscopic removal ~90% success rate
Follow-up
Rehabilitation Program• ROM exercises ASAP, gradual stretching of
affected tendon & roator cuff• Circumduction, pendulum - 5-10 lb weight held
lightly in the hand - arm swings ~1-3 inches in any direction
• Isometrics progress to concentric exercises, then to eccentric exercises
Patient Monitoring• Follow-up visit 2-3 days then 1/week for 3 weeks• Consider referral if conservative care fails to
improve condition
Prevention/Patient Education• Avoid aggravating activities
Prognosis• Usually responds well to conservative care, acute
symptoms usually resolve in ~2-3 weeks• Rarely may develop into frozen shoulder
4-shoulder NMS.indd 139 2014-01-14 11:05:18 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak140 | Orthopedic Conditions
AC SprainBasics
Definition: damage or tearing of the ligaments or joint capsule of the AC joint; AC separation is the displacement of the AC joint from its normal position
Cause of injury• Mechanism 1: direct force to the superior aspect
of the acromion, usually from a fall with arm in an adducted position → drives acromion inferiorly, spraining the intra-articular acromioclavicular ligaments
• Mechanism 2: FOOSH (fall on an outstretched hand) that can occur during collision sports → indirect force transmitted up arm, through humeral head to acromion, displacing it superiorly and stressing the AC ligaments
Demographics Age: 15-25 most commonGender: male > female (5:1) Risk factors: contact or extreme sports
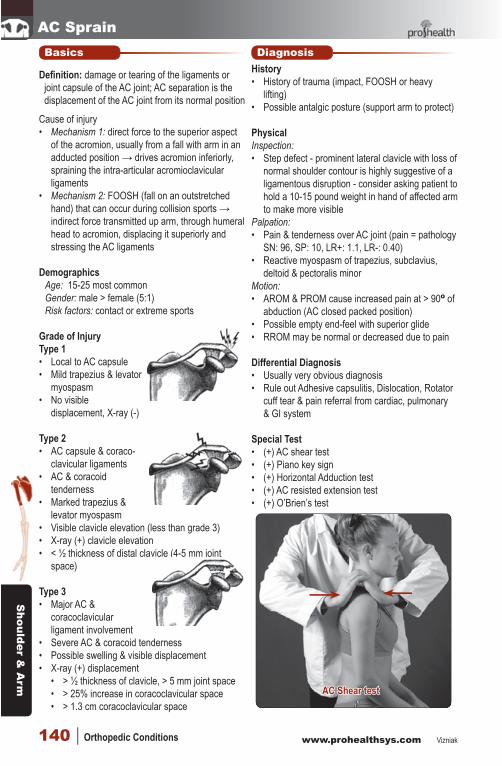
Grade of InjuryType 1• Local to AC capsule• Mild trapezius & levator
myospasm• No visible
displacement, X-ray (-)
Type 2• AC capsule & coraco-
clavicular ligaments• AC & coracoid
tenderness• Marked trapezius &
levator myospasm• Visible clavicle elevation (less than grade 3)• X-ray (+) clavicle elevation• < ½ thickness of distal clavicle (4-5 mm joint
space)
Type 3• Major AC &
coracoclavicular ligament involvement
• Severe AC & coracoid tenderness• Possible swelling & visible displacement• X-ray (+) displacement
• > ½ thickness of clavicle, > 5 mm joint space• > 25% increase in coracoclavicular space• > 1.3 cm coracoclavicular space
DiagnosisHistory• History of trauma (impact, FOOSH or heavy
lifting)• Possible antalgic posture (support arm to protect)
PhysicalInspection: • Step defect - prominent lateral clavicle with loss of
normal shoulder contour is highly suggestive of a ligamentous disruption - consider asking patient to hold a 10-15 pound weight in hand of affected arm to make more visible
Palpation:• Pain & tenderness over AC joint (pain = pathology
SN: 96, SP: 10, LR+: 1.1, LR-: 0.40)• Reactive myospasm of trapezius, subclavius,
deltoid & pectoralis minorMotion:• AROM & PROM cause increased pain at > 90º of
abduction (AC closed packed position)• Possible empty end-feel with superior glide• RROM may be normal or decreased due to pain
Differential Diagnosis • Usually very obvious diagnosis• Rule out Adhesive capsulitis, Dislocation, Rotator
cuff tear & pain referral from cardiac, pulmonary & GI system
Special Test• (+) AC shear test• (+) Piano key sign• (+) Horizontal Adduction test• (+) AC resisted extension test• (+) O’Brien’s test
AC Shear test
4-shoulder NMS.indd 140 2014-01-14 11:05:18 AM
Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 141
AC Sprain
TreatmentGeneral Measures• PRICE• Consider short-term use of arm sling• Sleep with injured side up
Massage Therapy• Initially focus on myofascial trigger point therapy,
myofascial release of shoulder muscles• After acute stage consider friction massage
Osseous Mobes/Manipulation• Do NOT work on AC joint directly (unstable)• Focus on T-spine, ribs & neck initially• Later consider mobes & manip in direction
opposite to force of injury
Electrotherapy• Consider pulsed ultrasound over shoulder• Microcurrent or IFC may offer benefit
Acupuncture• Local shoulder points LI4, SI3, SJ4 UB17 18 & 19
Follow-upRehabilitation Program• Depends on grade & stage of injury - go slow &
stay pain free - don’t re-injure• Type 1: activity modification may include the use
of a sling until symptoms subside and range of motion is reasonably comfortable• Cross arm in front of body to touch opposite
shoulder• Reach arm behind back• Slowly incorporate weights
• Type 2: sling for 2-4 weeks with PROM & AROM exercises - heavy lifting and contact sports should be avoided for 6-12 weeks to allow healing and prevent progression to a type 3 injury
• Type 3: consider surgical evaluation
Prevention/Patient Education• Avoid aggravating factors & causative activities
Prognosis• Type 1: conservative treatment result in resolution
in ~2 weeks• Type 2 & 3: usually responds well to conservative
care over 5-8 weeks • Increased risk of impingement symptoms, muscle-
fatigue discomfort & osteoarthrosis
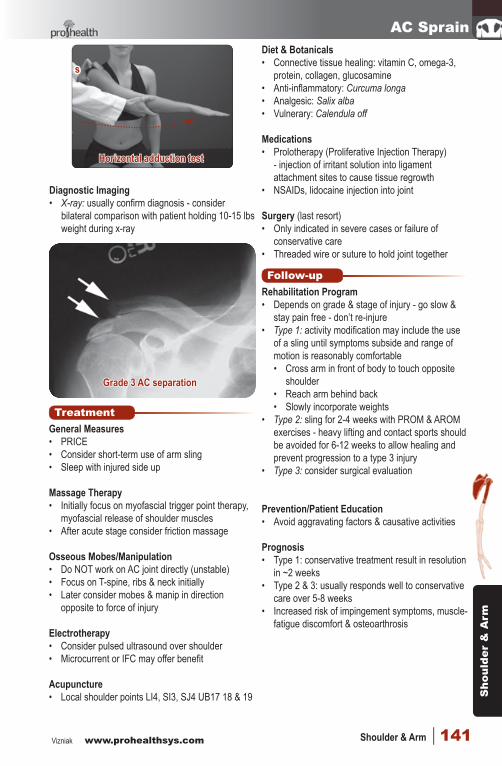
Grade 3 AC separation
Diagnostic Imaging• X-ray: usually confirm diagnosis - consider
bilateral comparison with patient holding 10-15 lbs weight during x-ray
Diet & Botanicals• Connective tissue healing: vitamin C, omega-3,
protein, collagen, glucosamine• Anti-inflammatory: Curcuma longa• Analgesic: Salix alba• Vulnerary: Calendula off
Medications• Prolotherapy (Proliferative Injection Therapy)
- injection of irritant solution into ligament attachment sites to cause tissue regrowth
• NSAIDs, lidocaine injection into joint
Surgery (last resort)• Only indicated in severe cases or failure of
conservative care• Threaded wire or suture to hold joint together
s
Horizontal adduction test
4-shoulder NMS.indd 141 2014-01-14 11:05:18 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak142 | Orthopedic Conditions
Frozen ShoulderBasics
Definition: frozen shoulder, or adhesive capsulitis, is an idiopathic condition of the shoulder associated with marked pain & contracture of the joint capsule
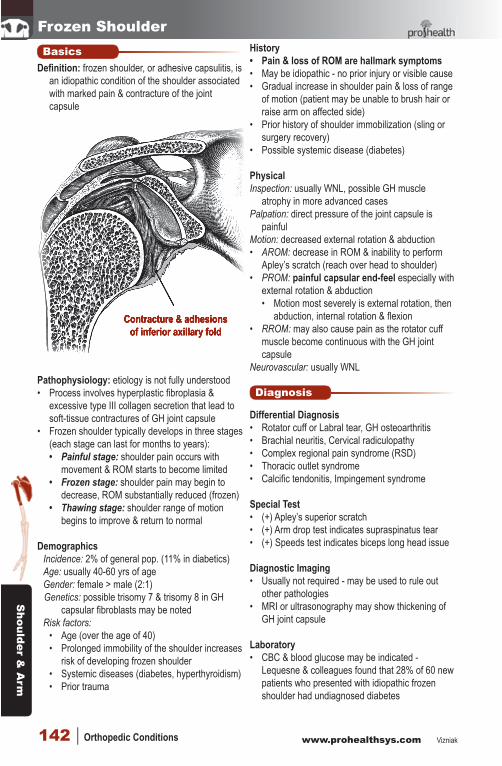
Contracture & adhesions Contracture & adhesions of inferior axillary foldof inferior axillary fold
Pathophysiology: etiology is not fully understood• Process involves hyperplastic fibroplasia &
excessive type III collagen secretion that lead to soft-tissue contractures of GH joint capsule
• Frozen shoulder typically develops in three stages (each stage can last for months to years): • Painful stage: shoulder pain occurs with
movement & ROM starts to become limited• Frozen stage: shoulder pain may begin to
decrease, ROM substantially reduced (frozen)• Thawing stage: shoulder range of motion
begins to improve & return to normal
Demographics Incidence: 2% of general pop. (11% in diabetics) Age: usually 40-60 yrs of age Gender: female > male (2:1) Genetics: possible trisomy 7 & trisomy 8 in GH
capsular fibroblasts may be notedRisk factors:
• Age (over the age of 40)• Prolonged immobility of the shoulder increases
risk of developing frozen shoulder• Systemic diseases (diabetes, hyperthyroidism)• Prior trauma
History• Pain & loss of ROM are hallmark symptoms• May be idiopathic - no prior injury or visible cause• Gradual increase in shoulder pain & loss of range
of motion (patient may be unable to brush hair or raise arm on affected side)
• Prior history of shoulder immobilization (sling or surgery recovery)
• Possible systemic disease (diabetes)
PhysicalInspection: usually WNL, possible GH muscle
atrophy in more advanced casesPalpation: direct pressure of the joint capsule is
painfulMotion: decreased external rotation & abduction• AROM: decrease in ROM & inability to perform
Apley’s scratch (reach over head to shoulder)• PROM: painful capsular end-feel especially with
external rotation & abduction• Motion most severely is external rotation, then
abduction, internal rotation & flexion• RROM: may also cause pain as the rotator cuff
muscle become continuous with the GH joint capsule
Neurovascular: usually WNL
Diagnosis
Differential Diagnosis • Rotator cuff or Labral tear, GH osteoarthritis• Brachial neuritis, Cervical radiculopathy• Complex regional pain syndrome (RSD)• Thoracic outlet syndrome• Calcific tendonitis, Impingement syndrome
Special Test• (+) Apley’s superior scratch• (+) Arm drop test indicates supraspinatus tear• (+) Speeds test indicates biceps long head issue
Diagnostic Imaging• Usually not required - may be used to rule out
other pathologies• MRI or ultrasonography may show thickening of
GH joint capsule
Laboratory• CBC & blood glucose may be indicated -
Lequesne & colleagues found that 28% of 60 new patients who presented with idiopathic frozen shoulder had undiagnosed diabetes
4-shoulder NMS.indd 142 2014-01-14 11:05:18 AM

Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 143
Frozen ShoulderTreatment
General Measures• Early ROM exercises & stretching are
fundamental to treatment • Consider NSAIDs & ice or heat to reduce pain• Continue with ADLs as much as pain will allow
Massage Therapy• Indicated during the “thawing” or recovery stage • Myofascial release (avoid during acute pain)• Myofascial trigger point therapy & Swedish • Heat therapy immediately before or after massage
Osseous Mobes/Manipulation• Shoulder mobilization as tolerated by patient
• Emphasis on anteroinferior capsular stretch• Inferior glide, anterior glide & axial distraction
• Also address thoracic & C-spine subluxations• Manipulation under anesthetic
• If conservative treatment fails, patient is given local anesthesia & shoulder is literally ‘ripped’ through normal ROM - the procedure is painless & ruptures chronic adhesions
Electrotherapy• Consider TENS to help modulate pain perception• Ultrasound to increase local blood flow
Acupuncture• Local points & GB34, LI15, 16, 11, SI9-10• Often used in conjunction with local massage
Diet & Botanicals• Anti-inflammatory diet (bromelain, valerian)• Consider vitamin B6, D supplementation
Medications• NSAIDs, Celebrex• Corticosteroid injection - “researchers at the
Manchester Rheumatology Service studied the accuracy of a variety of joint injections that were administered by using anatomic landmarks to the upper and lower extremities; their study demonstrated inaccurate placement of the drug in 65% of 108 joints injected!!!”
Surgery (not usually required)• Arthroscopic release• Suprascapular nerve block
Follow-up
Rehabilitation Program• Should be used in conjunction with other
modalities (manip., ultrasound, acupuncture)• Follow rehab program with massage & ice• Start with basic PFROM exercises, then pin &
stretch, then progress to PNF patterns & contract relax methods
Patient Monitoring• Give home care program & have patient
demonstrate exercises with each office visit• Warm-up with pendulum arm swings• Stretch with towel pulls & finger wall walking &
door stretches• Progress to aquatic therapy (pool/hot tub)• Then elastic tubing exercises that focus on
shoulder external rotation & abduction• Add resistance weight training as tolerated• Always stretch after activity
Prognosis• With good patient compliance, recovery with
conservative care is usually excellent• Inform the patient that the healing process for
frozen shoulder will be slow (6 -24 months), but they will get better!
• Realize frozen shoulder spontaneously resolves ~2 years after initial onset in ~60% of cases
External rotation mobilization
Anterior mobilization at 90º
Door stretch Towel stretch
4-shoulder NMS.indd 143 2014-01-14 11:05:18 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak144 | Orthopedic Conditions
GH InstabilityBasics
Definition: inability to maintain the humeral head centered in the glenoid fossa due to laxity of the shoulder capsule, ligaments &/or rotator cuff muscle imbalances or congenital joint anomalies
Degrees of instability• Apprehension - fear that shoulder will subluxate
or dislocate• Subluxation - transient partial separation of
articular surfaces - humeral head usually spontaneously returns to normal position
• Dislocation - complete separation of articular surfaces
Types of glenohumeral instability• Anterior inferior (80% of cases) - humeral head
slides anterior & inferior• Posterior (~10%) - humeral head slides posteriorly• Multidirectional (~10%) - usually congenital
Grades of instability
Grade DescriptionWNL 0-25% translation
1 25-50% translation, humeral head riding up on glenoid labrum
2 50-75% translation, humeral head rides up & over glenoid labrum, immediately reduces
3 > 75% translation & humeral head remains dislocated
WNL = within normal limits
Pathophysiology: • Traumatic: instability secondary to damage of the
rotator cuff, glenoid labrum &/or GH ligaments• Can be single events or recurrent injury• Direct trauma - tackle
from behind with shoulder in abduction & external rotation or long axis traction force applied to arm
• Overuse trauma - repeated overhead activities (boxers, swimmers, racket sports, throwers)
• Intentional subluxation or dislocation - patient can voluntarily demonstrate instability
• Atraumatic: congenital local anomalies may have familial tendencies & are more likely bilateral• Generalized joint laxity - these patients have
less cross-linked collagen fibers in their capsule = increase flexibility
• Glenoind dysplasia - shallow glenoid fossa, anterior of posterior tilt of glenoid
Demographics Incidence: ~2-3% of population Age: 15-30 (young athletes) Gender: female > male (2:1)Genetics: specifics unknown but does tend to run
in families Risk factors: prior injury, rotator cuff damage,
repeated overhead activities, nerve damage
History• General shoulder pain, worse with activity or
certain arm positions (overhead activity, carrying objects at side, overuse, prior injury)
• Pain is better with rest or heat• Patient may note a history of catching or locking
with motion or prior athletic injury (dislocation)• Often associated with impingement symptoms
(painful arc of motion)
PhysicalInspection: possible sulcus sign or rednessPalpation: possible tenderness over joint if it is
inflamed or there are damaged fibers present• Trigger points & myospasm of rotator cuff
Motion: AROM & PROM may show repeatable clunk or apprehension with abduction & external rotation• Pain/impingement with 80-120º shoulder
abduction & altered scapulohumeral rhythm • RROM - usually WNL (may be weak due to
pain or coexisting damage)Neurovascular screen: WNL - be sure to check
axillary & suprascapular nerve function as well as radial pulse
Diagnosis
Differential Diagnosis • Glenoid labral tear or GH osteoarthritis • Biceps tendinopathy• Rotator cuff tendinopathy or strain• Shoulder impingement • Subacromial bursitis• Any of above may co-
exist with GH instability
Special Test (see yellow physical assessment text)• (+) Load & shift (anterior
& posterior instability)
©VIZNIAK
Load & Shift
4-shoulder NMS.indd 144 2014-01-14 11:05:19 AM
Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 145
GH InstabilityInferior instability tests• (+) Sulcus test (arm dependant & pull down)• (+) Faegin’s test (arm abducted 90°)
Anterior instability (best done supine)• (+) Anterior apprehension test• (+) Relocation test• (+) Release maneuver
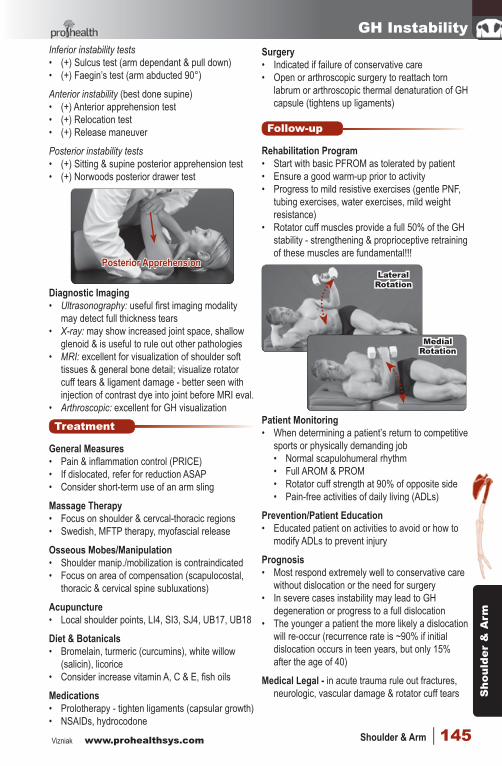
Posterior instability tests• (+) Sitting & supine posterior apprehension test• (+) Norwoods posterior drawer test
Posterior Apprehension
Diagnostic Imaging• Ultrasonography: useful first imaging modality
may detect full thickness tears• X-ray: may show increased joint space, shallow
glenoid & is useful to rule out other pathologies• MRI: excellent for visualization of shoulder soft
tissues & general bone detail; visualize rotator cuff tears & ligament damage - better seen with injection of contrast dye into joint before MRI eval.
• Arthroscopic: excellent for GH visualization
Treatment
General Measures• Pain & inflammation control (PRICE)• If dislocated, refer for reduction ASAP• Consider short-term use of an arm sling
Massage Therapy• Focus on shoulder & cervcal-thoracic regions• Swedish, MFTP therapy, myofascial release
Osseous Mobes/Manipulation• Shoulder manip./mobilization is contraindicated• Focus on area of compensation (scapulocostal,
thoracic & cervical spine subluxations)
Acupuncture• Local shoulder points, LI4, SI3, SJ4, UB17, UB18
Diet & Botanicals• Bromelain, turmeric (curcumins), white willow
(salicin), licorice• Consider increase vitamin A, C & E, fish oils
Medications• Prolotherapy - tighten ligaments (capsular growth)• NSAIDs, hydrocodone
Surgery• Indicated if failure of conservative care• Open or arthroscopic surgery to reattach torn
labrum or arthroscopic thermal denaturation of GH capsule (tightens up ligaments)
Follow-up
Rehabilitation Program• Start with basic PFROM as tolerated by patient• Ensure a good warm-up prior to activity• Progress to mild resistive exercises (gentle PNF,
tubing exercises, water exercises, mild weight resistance)
• Rotator cuff muscles provide a full 50% of the GH stability - strengthening & proprioceptive retraining of these muscles are fundamental!!!
Lateral Rotation
Medial Rotation
Patient Monitoring• When determining a patient’s return to competitive
sports or physically demanding job• Normal scapulohumeral rhythm• Full AROM & PROM• Rotator cuff strength at 90% of opposite side• Pain-free activities of daily living (ADLs)
Prevention/Patient Education• Educated patient on activities to avoid or how to
modify ADLs to prevent injury
Prognosis• Most respond extremely well to conservative care
without dislocation or the need for surgery• In severe cases instability may lead to GH
degeneration or progress to a full dislocation• The younger a patient the more likely a dislocation
will re-occur (recurrence rate is ~90% if initial dislocation occurs in teen years, but only 15% after the age of 40)
Medical Legal - in acute trauma rule out fractures, neurologic, vascular damage & rotator cuff tears
4-shoulder NMS.indd 145 2014-01-14 11:05:19 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak146 | Orthopedic Conditions
Glenoid Labral TearBasics
Definition: often overlooked cause of chronic shoulder pain due to tearing or detachment of the fibrocartilagenous glenoid labrum & insertion point of the biceps brachii long head
Labral lesions can occur in isolation or in combination with rotator cuff tears, GH instability, impingement, dislocation & other shoulder injuries
Pathophysiology: types of glenoid labrum lesions:• SLAP lesion (more common) - tearing superior
labrum anterior posterior - see classification below
Type SLAP clinical description
1 Fraying of the labrum, but the biceps anchor is intact
2 Tear of superior labrum that results in instability of biceps anchor (most common)
3 Bucket-handle tear of the superior labrum
4 Bucket-handle tear that expands into biceps tendon
• Bankhart lesion (less common) - tear of lower half of labrum & inferior glenohumeral ligament - seen with shoulder dislocations
• Bennett lesion (least common) - posterior labral tear associated with posterior rotator cuff damage
Demographics Incidence: ~10-20% of patients with shoulder pain,
higher in athletes & on dominant armAge: usually 20-40, but can occur at any age Gender: male > female (5:1) Risk factors: trauma & instability
• Repetitive stress (throwing, swimming)• Direct trauma (dislocation, subluxation, direct
blow to shoulder, FOOSH, overhead activity)• Instability can result in labral tear
Diagnosis
History• Pain with overhead or cross body activities• Snapping, popping, catching with motion• Occasional night pain or pain with ADLs • A sense of instability in the shoulder • ↓ range of motion & strength • Prior history of overuse or direct trauma
(dislocation, subluxation or instability)• Patient may have seen a number of other
healthcare providers with a history of failed conservative care treatments
PhysicalInspection: patient maybe protective & have
shoulder/arm in a sling positionPalpation: tenderness around bicipital tendon,
anterior deltoid & supraspinatus insertion• Possibly slight edema & warmthMotion: • AROM: pain, crepitus, ↓ ROM above head• PROM: crepitus (rule out AC crepitus - very
common), ↓ ROM with myospasm end-feel & muscle guarding or apprehension
• RROM: weakness due to pain of bicepsNeurovascular: usually WNL (check pulse & DTRs)
Differential Diagnosis • Similar to other shoulder pathologies that may
co-exist - difficult to diagnosis • Biceps tendonitis• Rotator cuff injuries (occur in 40% of labral tears)• Adhesive capsulitis• Shoulder impingement or sprain• AC joint pathology• Subacromial bursitis
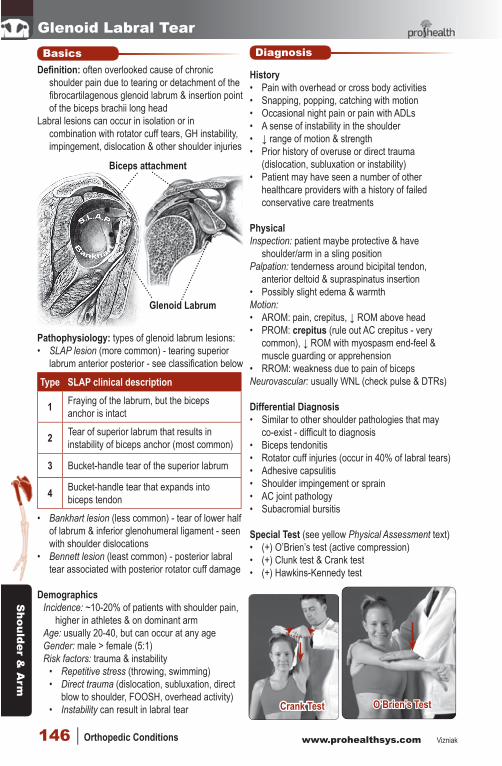
Special Test (see yellow Physical Assessment text)• (+) O’Brien’s test (active compression)• (+) Clunk test & Crank test• (+) Hawkins-Kennedy test
Crank Test O’Brien’s Test
Glenoid Labrum
Biceps attachment
4-shoulder NMS.indd 146 2014-01-14 11:05:19 AM
Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 147
Glenoid Labral Tear(+) Biceps Load Test IIProcedure: patient supine, shoulder abducted ~120°
& elbow flexed ~90°; examiner fully externally rotates shoulder then asks patient to flex elbow while resisting action
Interpretation: ant. shoulder pain → SLAP lesionClinical notes: This test is very reliable (valid) for
the diagnosis SLAP lesions (R: 0.82 SN: 90 SP: 97 LR+: 26.4 LR-: 0.11)
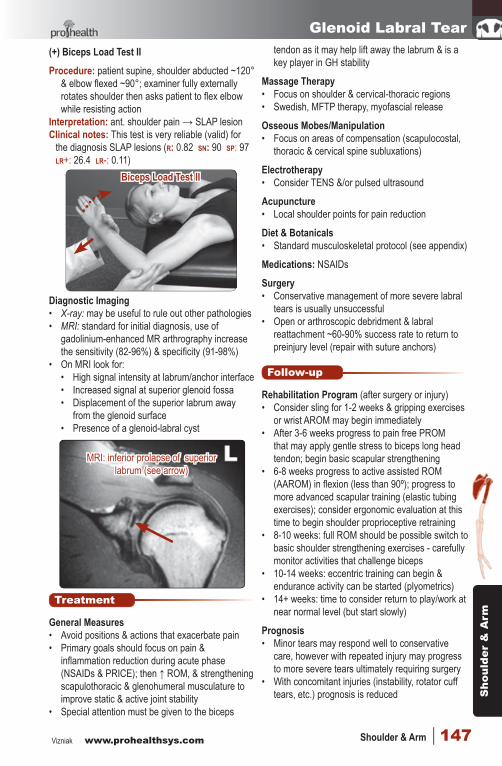
Diagnostic Imaging• X-ray: may be useful to rule out other pathologies• MRI: standard for initial diagnosis, use of
gadolinium-enhanced MR arthrography increase the sensitivity (82-96%) & specificity (91-98%)
• On MRI look for:• High signal intensity at labrum/anchor interface• Increased signal at superior glenoid fossa• Displacement of the superior labrum away
from the glenoid surface• Presence of a glenoid-labral cyst
Treatment
General Measures• Avoid positions & actions that exacerbate pain• Primary goals should focus on pain &
inflammation reduction during acute phase (NSAIDs & PRICE); then ↑ ROM, & strengthening scapulothoracic & glenohumeral musculature to improve static & active joint stability
• Special attention must be given to the biceps
tendon as it may help lift away the labrum & is a key player in GH stability
Massage Therapy• Focus on shoulder & cervical-thoracic regions• Swedish, MFTP therapy, myofascial release
Osseous Mobes/Manipulation• Focus on areas of compensation (scapulocostal,
thoracic & cervical spine subluxations)
Electrotherapy• Consider TENS &/or pulsed ultrasound
Acupuncture• Local shoulder points for pain reduction
Diet & Botanicals• Standard musculoskeletal protocol (see appendix)
Medications: NSAIDs
Surgery• Conservative management of more severe labral
tears is usually unsuccessful• Open or arthroscopic debridment & labral
reattachment ~60-90% success rate to return to preinjury level (repair with suture anchors)
Follow-up
Rehabilitation Program (after surgery or injury)• Consider sling for 1-2 weeks & gripping exercises
or wrist AROM may begin immediately • After 3-6 weeks progress to pain free PROM
that may apply gentle stress to biceps long head tendon; begin basic scapular strengthening
• 6-8 weeks progress to active assisted ROM (AAROM) in flexion (less than 90º); progress to more advanced scapular training (elastic tubing exercises); consider ergonomic evaluation at this time to begin shoulder proprioceptive retraining
• 8-10 weeks: full ROM should be possible switch to basic shoulder strengthening exercises - carefully monitor activities that challenge biceps
• 10-14 weeks: eccentric training can begin & endurance activity can be started (plyometrics)
• 14+ weeks: time to consider return to play/work at near normal level (but start slowly)
Prognosis• Minor tears may respond well to conservative
care, however with repeated injury may progress to more severe tears ultimately requiring surgery
• With concomitant injuries (instability, rotator cuff tears, etc.) prognosis is reduced
Biceps Load Test II
MRI: inferior prolapse of superior labrum (see arrow)
4-shoulder NMS.indd 147 2014-01-14 11:05:19 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak148 | Orthopedic Conditions
Glenohumeral Arthritis
BasicsDefinition: progressive degradation & damage to the
glenohumeral joint articular surfaces that can lead to inflammation and painArthrosis = degeneration in jointArthritis = inflammation of joint
Pathophysiology:• Progressive wear & tear damage to the GH
joint articular surfaces result in asymmetric narrowing of the joint space which progresses to subchondral sclerosis & osteophyte formation; later with complete loss of articular cartilage & finally bone destruction
Demographics Incidence: ~20% of elderly population (common) Age: usually > 65 yrs (possible 40+ yrs) Gender: male > female (2:1)Genetics: unclear but there is familial predisposition Risk factors:
• Prior injury or repetitive stress use of shoulder• Joint infection, Rheumatoid arthritis• Ligament or Rotator cuff tear (GH instability)• Paget’s disease, Lyme disease• Osteonecrosis (stages by Ficat System below)
Stage Clinical description
1 X-ray shows mottling of trabeculae with resorption & normal shape of the head
2 X-ray shows a crescent sign (ie, meniscus-shaped area of sclerosis)
3 Collapse of the articular surface (loss of joint space)
4 Arthritic changes in the GH joint occur secondary to collapse of articular surface
Diagnosis
History• Insidious onset of shoulder pain & discomfort -
often ‘stiff’ in the morning, better with mild activity then worse with excessive activity
• Pain is better with rest or heat, pain may change with variation in barometric pressure
• Crepitus with motion (snapping & popping)• Possible loss of ROM & affected ADLs
PhysicalInspection: look for signs of wasting & asymmetry
over shoulder & upper back/neck
Palpation: possible tenderness over GH capsule• MFTP & myospasm of upper back neck &
shoulder musculatureMotion: general ↓ in AROM with possible pain• PROM - may reveal clicking or popping (crepitus)
with limited or firm abnormal end-feels• RROM - muscle weakness due to painNeurovascular: usually WNL
Differential Diagnosis • Frozen shoulder (Adhesive capsulitis)• GH instability, Supraspinatus tear• Labral tear or Rotator cuff tendinopathy• Cervical radiculopathy
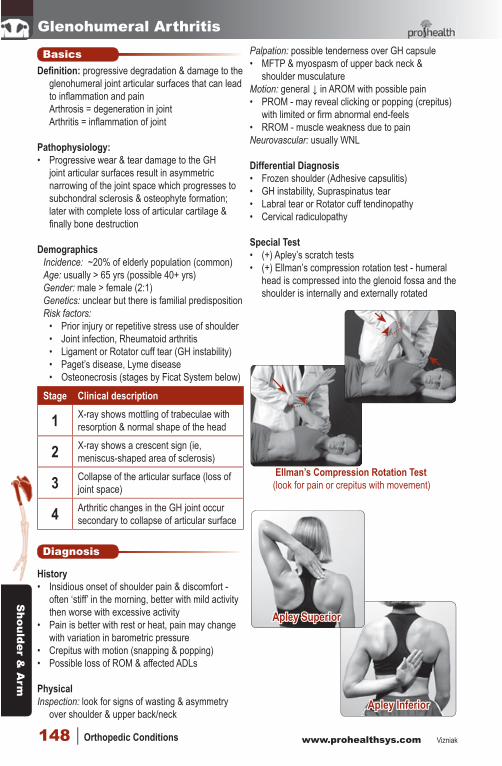
Special Test• (+) Apley’s scratch tests• (+) Ellman’s compression rotation test - humeral
head is compressed into the glenoid fossa and the shoulder is internally and externally rotated
Ellman’s Compression Rotation Test(look for pain or crepitus with movement)
Apley Inferior
Apley Superior
4-shoulder NMS.indd 148 2014-01-14 11:05:19 AM
Sho
ulde
r &
Arm
Vizniak www.prohealthsys.com Shoulder & Arm | 149
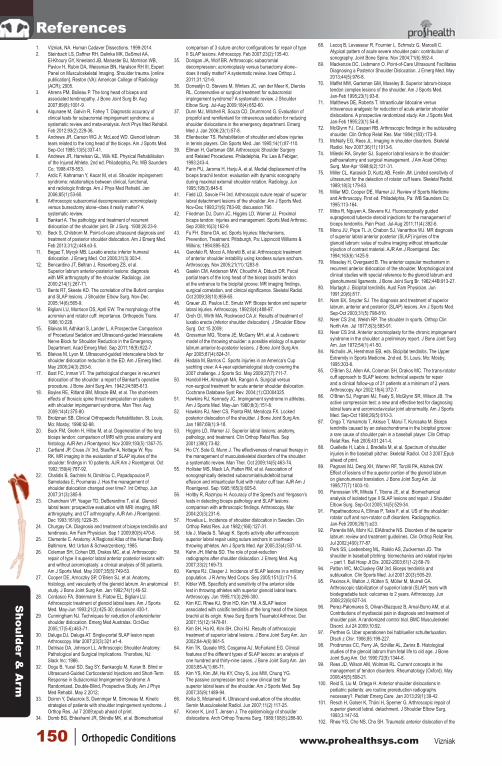
Glenohumeral ArthritisDiagnostic Imaging• X-ray: definitive diagnosis - joint space loss
possible osteophyte formation (see arrows below) • Superior humeral displacement indicates co-
existing supraspinatus tear• MRI: useful to assess soft tissue involvement
(labral or rotator cuff tear)
Laboratory• Consider CBC with differential, chem screen or
arthritis panel to rule-in/out other causes
Treatment
General Measures• Conservative care is good to relieve symptoms &
slow degeneration, but often has minimal effect on reversal of degenerative changes
• General pain control, NSAIDs, hot packs• Stretching to maintain normal ROM
Massage Therapy• Focus on shoulder & cervical-thoracic regions• Swedish, MFTP therapy, myofascial release
Osseous Mobes/Manipulation• Shoulder manip/mobes are indicated if there is
decreased ROM (contraindicated in hypermobility)• Also address cervical & thoracic subluxations
Electrotherapy• Consider ultrasound to increase local blood flow• TENS for pain management
Acupuncture - local shoulder points• BL11, LI4, 14 & 15, SI 3, 10 & 12, SJ5 & SJ14
Diet & Botanicals• MSM & glucosamine supplementation• Hypoallergenic diet (reduce night shades)• Emphasize good fats: olive oil, fish & flax, limit
trans and long chain saturated fatty acids• Increase fruit & vegetable intake for antioxidant
benefits• Limit sugar & maintain healthy body weight
(adipose tissue can release pro-inflammatory cytokines)
Medications• Acetaminophen, ibuprofen, celebrex• Topical NSAIDs, capsaicin cream• Corticosteroid injection (controversial) - may lead
to further cartilage, bone & tendon damage for only short term pain reduction
Surgery• If conservative treatment fails to offer relief,
consider surgical referral for arthroplasty (joint replacement)
Follow-up
Rehabilitation Program• Maintain as many ADLs as possible, avoid
activities that aggravate symptoms• Use good warm-up techniques - pendulum arm
swings• Consider water aerobics followed by hot-tub• Occupational therapy
Prevention/Patient Education• Avoid aggravating position/activities both at work
& sleeping (consider a new mattress)• Do not perform heavy lifting or ballistic actions
with shoulder• Stretch & rest during acute flare-ups
Prognosis• Fair to good prognosis for symptomatic relief,
however there is no conservative cure given the progressive nature of this condition
• Failure of conservative care warrants a surgical consultation
Glenohumeral degeneration (arrows denote osteophyte formation)
4-shoulder NMS.indd 149 2014-01-14 11:05:19 AM
Shoulder &
Arm
www.prohealthsys.com Vizniak150 | Orthopedic Conditions
1. Vizniak, NA. Human Cadaver Dissections. 1999-2014.2. Steinbach LS, Daffner RH, Dalinka MK, DeSmet AA,
El-Khoury GY, Kneeland JB, Manaster BJ, Morrison WB, Pavlov H, Rubin DA, Weissman BN, Haralson RH III, Expert Panel on Musculoskeletal Imaging. Shoulder trauma. [online publication]. Reston (VA): American College of Radiology (ACR); 2005.
3. Ahrens PM, Boileau P. The long head of biceps and associated tendinopathy. J Bone Joint Surg Br. Aug 2007;89(8):1001-9.
4. Alqunaee M, Galvin R, Fahey T. Diagnostic accuracy of clinical tests for subacromial impingement syndrome: a systematic review and meta-analysis. Arch Phys Med Rehabil. Feb 2012;93(2):229-36.
5. Andrews JR, Carson WG Jr, McLeod WD. Glenoid labrum tears related to the long head of the biceps. Am J Sports Med. Sep-Oct 1985;13(5):337-41.
6. Andrews JR, Harrelson GL, Wilk KE. Physical Rehabilitation of the Injured Athlete. 2nd ed. Philadelphia, Pa: WB Saunders Co; 1998:478-553.
7. Ardic F, Kahraman Y, Kacar M, et al. Shoulder impingement syndrome: relationships between clinical, functional, and radiologic findings. Am J Phys Med Rehabil. Jan 2006;85(1):53-60.
8. Arthroscopic subacromial decompression: acromioplasty versus bursectomy alone--does it really matter? A systematic review.
9. Bankart A. The pathology and treatment of recurrent dislocation of the shoulder joint. Br J Surg. 1938;26:23-9.
10. Beck S, Chilstrom M. Point-of-care ultrasound diagnosis and treatment of posterior shoulder dislocation. Am J Emerg Med. Feb 2013;31(2):449.e3-5.
11. Begaz T, Mycyk MB. Luxatio erecta: inferior humeral dislocation. J Emerg Med. Oct 2006;31(3):303-4.
12. Bencardino JT, Beltran J, Rosenberg ZS, et al. Superior labrum anterior-posterior lesions: diagnosis with MR arthrography of the shoulder. Radiology. Jan 2000;214(1):267-71.
13. Bents RT, Skeete KD. The correlation of the Buford complex and SLAP lesions. J Shoulder Elbow Surg. Nov-Dec 2005;14(6):565-9.
14. Bigliani LU, Morrison DS, April EW. The morphology of the acromion and rotator cuff: importance. Orthopedic Trans. 1986;10:228.
15. Blaivas M, Adhikari S, Lander L. A Prospective Comparison of Procedural Sedation and Ultrasound-guided Interscalene Nerve Block for Shoulder Reduction in the Emergency Department. Acad Emerg Med. Sep 2011;18(9):922-7.
16. Blaivas M, Lyon M. Ultrasound-guided interscalene block for shoulder dislocation reduction in the ED. Am J Emerg Med. May 2006;24(3):293-6.
17. Bost FC, Inman VT. The pathological changes in recurrent dislocation of the shoulder: a report of Bankart’s operative procedure. J Bone Joint Surg Am. 1942;24:595-613.
18. Boyles RE, Ritland BM, Miracle BM, et al. The short-term effects of thoracic spine thrust manipulation on patients with shoulder impingement syndrome. Man Ther. Aug 2009;14(4):375-80.
19. Brotzman SB. Clinical Orthopaedic Rehabilitation. St. Louis, Mo: Mosby; 1996:92-98.
20. Buck FM, Grehn H, Hilbe M, et al. Degeneration of the long biceps tendon: comparison of MRI with gross anatomy and histology. AJR Am J Roentgenol. Nov 2009;193(5):1367-75.
21. Cartland JP, Crues JV 3rd, Stauffer A, Nottage W, Ryu RK. MR imaging in the evaluation of SLAP injuries of the shoulder: findings in 10 patients. AJR Am J Roentgenol. Oct 1992;159(4):787-92.
22. Chalidis B, Sachinis N, Dimitriou C, Papadopoulos P, Samoladas E, Pournaras J. Has the management of shoulder dislocation changed over time?. Int Orthop. Jun 2007;31(3):385-9.
23. Chandnani VP, Yeager TD, DeBerardino T, et al. Glenoid labral tears: prospective evaluation with MRI imaging, MR arthrography, and CT arthrography. AJR Am J Roentgenol. Dec 1993;161(6):1229-35.
24. Churgay CA. Diagnosis and treatment of biceps tendinitis and tendinosis. Am Fam Physician. Sep 1 2009;80(5):470-6.
25. Clemente C. Anatomy: A Regional Atlas of the Human Body. Baltimore, Md: Urban & Schwarzenberg; 1985.
26. Coleman SH, Cohen DB, Drakos MC, et al. Arthroscopic repair of type II superior labral anterior posterior lesions with and without acromioplasty: a clinical analysis of 50 patients. Am J Sports Med. May 2007;35(5):749-53.
27. Cooper DE, Arnoczky SP, O’Brien SJ, et al. Anatomy, histology, and vascularity of the glenoid labrum. An anatomical study. J Bone Joint Surg Am. Jan 1992;74(1):46-52.
28. Cordasco FA, Steinmann S, Flatow EL, Bigliani LU. Arthroscopic treatment of glenoid labral tears. Am J Sports Med. May-Jun 1993;21(3):425-30; discussion 430-1.
29. Cunningham NJ. Techniques for reduction of anteroinferior shoulder dislocation. Emerg Med Australas. Oct-Dec 2005;17(5-6):463-71.
30. Daluga DJ, Daluga AT. Single-portal SLAP lesion repair. Arthroscopy. Mar 2007;23(3):321.e1-4.
31. Detrisac DA, Johnson LL. Arthroscopic Shoulder Anatomy: Pathological and Surgical Implications. Thorofare, NJ: Slack Inc; 1986.
32. Dogu B, Yucel SD, Sag SY, Bankaoglu M, Kuran B. Blind or Ultrasound-Guided Corticosteroid Injections and Short-Term Response in Subacromial Impingement Syndrome: A Randomized, Double-Blind, Prospective Study. Am J Phys Med Rehabil. May 2 2012;
33. Doiron Y, Delacroix S, Denninger M, Simoneau M. Kinetic strategies of patients with shoulder impingement syndrome. J Orthop Res. Jul 7 2009;epub ahead of print.
34. Domb BG, Ehteshami JR, Shindle MK, et al. Biomechanical
comparison of 3 suture anchor configurations for repair of type II SLAP lesions. Arthroscopy. Feb 2007;23(2):135-40.
35. Donigan JA, Wolf BR. Arthroscopic subacromial decompression: acromioplasty versus bursectomy alone--does it really matter? A systematic review. Iowa Orthop J. 2011;31:121-6.
36. Dorrestijn O, Stevens M, Winters JC, van der Meer K, Diercks RL. Conservative or surgical treatment for subacromial impingement syndrome? A systematic review. J Shoulder Elbow Surg. Jul-Aug 2009;18(4):652-60.
37. Dunn MJ, Mitchell R, Souza CD, Drummond G. Evaluation of propofol and remifentanil for intravenous sedation for reducing shoulder dislocations in the emergency department. Emerg Med J. Jan 2006;23(1):57-8.
38. Ellenbecker TS. Rehabilitation of shoulder and elbow injuries in tennis players. Clin Sports Med. Jan 1995;14(1):87-110.
39. Ellman H, Gartsman GM. Arthroscopic Shoulder Surgery and Related Procedures. Philadelphia, Pa: Lea & Febiger; 1993:243-4.
40. Farin PU, Jaroma H, Harju A, et al. Medial displacement of the biceps brachii tendon: evaluation with dynamic sonography during maximal external shoulder rotation. Radiology. Jun 1995;195(3):845-8.
41. Field LD, Savoie FH 3rd. Arthroscopic suture repair of superior labral detachment lesions of the shoulder. Am J Sports Med. Nov-Dec 1993;21(6):783-90; discussion 790.
42. Friedman DJ, Dunn JC, Higgins LD, Warner JJ. Proximal biceps tendon: injuries and management. Sports Med Arthrosc. Sep 2008;16(3):162-9.
43. Fu FH. Stone DA, ed. Sports Injuries: Mechanisms, Prevention, Treatment. Pittsburgh, Pa: Lippincott Williams & Wilkins; 1994:895-923.
44. Garofalo R, Mocci A, Moretti B, et al. Arthroscopic treatment of anterior shoulder instability using knotless suture anchors. Arthroscopy. Nov 2005;21(11):1283-9.
45. Gaskin CM, Anderson MW, Choudhri A, Diduch DR. Focal partial tears of the long head of the biceps brachii tendon at the entrance to the bicipital groove: MR imaging findings, surgical correlation, and clinical significance. Skeletal Radiol. Oct 2009;38(10):959-65.
46. Grauer JD, Paulos LE, Smutz WP. Biceps tendon and superior labral injuries. Arthroscopy. 1992;8(4):488-97.
47. Groh GI, Wirth MA, Rockwood CA Jr. Results of treatment of luxatio erecta (inferior shoulder dislocation). J Shoulder Elbow Surg. Oct 15 2009;
48. Grossman MG, Tibone JE, McGarry MH, et al. A cadaveric model of the throwing shoulder: a possible etiology of superior labrum anterior-to-posterior lesions. J Bone Joint Surg Am. Apr 2005;87(4):824-31.
49. Hadala M, Barrios C. Sports injuries in an America’s Cup yachting crew: A 4-year epidemiological study covering the 2007 challenge. J Sports Sci. May 2009;27(7):711-7.
50. Handoll HH, Almaiyah MA, Rangan A. Surgical versus non-surgical treatment for acute anterior shoulder dislocation. Cochrane Database Syst Rev. 2004;(1):CD004325.
51. Hawkins RJ, Kennedy JC. Impingement syndrome in athletes. Am J Sports Med. May-Jun 1980;8(3):151-8.
52. Hawkins RJ, Neer CS, Pianta RM, Mendoza FX. Locked posterior dislocation of the shoulder. J Bone Joint Surg Am. Jan 1987;69(1):9-18.
53. Higgins LD, Warner JJ. Superior labral lesions: anatomy, pathology, and treatment. Clin Orthop Relat Res. Sep 2001;(390):73-82.
54. Ho CY, Sole G, Munn J. The effectiveness of manual therapy in the management of musculoskeletal disorders of the shoulder: a systematic review. Man Ther. Oct 2009;14(5):463-74.
55. Hollister MS, Mack LA, Patten RM, et al. Association of sonographically detected subacromial/subdeltoid bursal effusion and intraarticular fluid with rotator cuff tear. AJR Am J Roentgenol. Sep 1995;165(3):605-8.
56. Holtby R, Razmjou H. Accuracy of the Speed’s and Yergason’s tests in detecting biceps pathology and SLAP lesions: comparison with arthroscopic findings. Arthroscopy. Mar 2004;20(3):231-6.
57. Hovelius L. Incidence of shoulder dislocation in Sweden. Clin Orthop Relat Res. Jun 1982;(166):127-31.
58. Ide J, Maeda S, Takagi K. Sports activity after arthroscopic superior labral repair using suture anchors in overhead-throwing athletes. Am J Sports Med. Apr 2005;33(4):507-14.
59. Kahn JH, Mehta SD. The role of post-reduction radiographs after shoulder dislocation. J Emerg Med. Aug 2007;33(2):169-73.
60. Kampa RJ, Clasper J. Incidence of SLAP lesions in a military population. J R Army Med Corps. Sep 2005;151(3):171-5.
61. Kibler WB. Specificity and sensitivity of the anterior slide test in throwing athletes with superior glenoid labral tears. Arthroscopy. Jun 1995;11(3):296-300.
62. Kim KC, Rhee KJ, Shin HD, Kim YM. A SLAP lesion associated with calcific tendinitis of the long head of the biceps brachii at its origin. Knee Surg Sports Traumatol Arthrosc. Dec 2007;15(12):1478-81.
63. Kim SH, Ha KI, Kim SH, Choi HJ. Results of arthroscopic treatment of superior labral lesions. J Bone Joint Surg Am. Jun 2002;84-A(6):981-5.
64. Kim TK, Queale WS, Cosgarea AJ, McFarland EG. Clinical features of the different types of SLAP lesions: an analysis of one hundred and thirty-nine cases. J Bone Joint Surg Am. Jan 2003;85-A(1):66-71.
65. Kim YS, Kim JM, Ha KY, Choy S, Joo MW, Chung YG. The passive compression test: a new clinical test for superior labral tears of the shoulder. Am J Sports Med. Sep 2007;35(9):1489-94.
66. Kolla S, Motamedi K. Ultrasound evaluation of the shoulder. Semin Musculoskelet Radiol. Jun 2007;11(2):117-25.
67. Kroner K, Lind T, Jensen J. The epidemiology of shoulder dislocations. Arch Orthop Trauma Surg. 1989;108(5):288-90.
References68. Lecoq B, Levasseur R, Fournier L, Schmutz G, Marcelli C.
Atypical pattern of acute severe shoulder pain: contribution of sonography. Joint Bone Spine. Nov 2004;71(6):592-4.
69. Mackenzie DC, Liebmann O. Point-of-Care Ultrasound Facilitates Diagnosing a Posterior Shoulder Dislocation. J Emerg Med. May 2013;44(5):976-8.
70. Maffet MW, Gartsman GM, Moseley B. Superior labrum-biceps tendon complex lesions of the shoulder. Am J Sports Med. Jan-Feb 1995;23(1):93-8.
71. Matthews DE, Roberts T. Intraarticular lidocaine versus intravenous analgesic for reduction of acute anterior shoulder dislocations. A prospective randomized study. Am J Sports Med. Jan-Feb 1995;23(1):54-8.
72. McGlynn FJ, Caspari RB. Arthroscopic findings in the subluxating shoulder. Clin Orthop Relat Res. Mar 1984;(183):173-8.
73. McNally EG, Rees JL. Imaging in shoulder disorders. Skeletal Radiol. Nov 2007;36(11):1013-6.
74. Mileski RA, Snyder SJ. Superior labral lesions in the shoulder: pathoanatomy and surgical management. J Am Acad Orthop Surg. Mar-Apr 1998;6(2):121-31.
75. Miller CL, Karasick D, Kurtz AB, Fenlin JM. Limited sensitivity of ultrasound for the detection of rotator cuff tears. Skeletal Radiol. 1989;18(3):179-83.
76. Miller MD, Cooper DE, Warner JJ. Review of Sports Medicine and Arthroscopy. First ed. Philadelphia, Pa: WB Saunders Co; 1995:113-164.
77. Mitra R, Nguyen A, Stevens KJ. Fluoroscopically guided supraglenoid tubercle steroid injections for the management of biceps tendonitis. Pain Pract. Jul-Aug 2011;11(4):392-6.
78. Monu JU, Pope TL Jr, Chabon SJ, Vanarthos WJ. MR diagnosis of superior labral anterior posterior (SLAP) injuries of the glenoid labrum: value of routine imaging without intraarticular injection of contrast material. AJR Am J Roentgenol. Dec 1994;163(6):1425-9.
79. Moseley H, Overgaard B. The anterior capsular mechanism in recurrent anterior dislocation of the shoulder. Morphological and clinical studies with special reference to the glenoid labrum and glenohumeral ligaments. J Bone Joint Surg Br. 1962;44B:913-27.
80. Murtagh J. Bicipital tendinitis. Aust Fam Physician. Jun 1991;20(6):817.
81. Nam EK, Snyder SJ. The diagnosis and treatment of superior labrum, anterior and posterior (SLAP) lesions. Am J Sports Med. Sep-Oct 2003;31(5):798-810.
82. Neer CS 2nd, Welsh RP. The shoulder in sports. Orthop Clin North Am. Jul 1977;8(3):583-91.
83. Neer CS 2nd. Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am. Jan 1972;54(1):41-50.
84. Nicholis JA, Hershman EB, eds. Bicipital tendinitis. The Upper Extremity in Sports Medicine. 2nd ed. St. Louis, Mo: Mosby; 1995:303-6.
85. O’Brien SJ, Allen AA, Coleman SH, Drakos MC. The trans-rotator cuff approach to SLAP lesions: technical aspects for repair and a clinical follow-up of 31 patients at a minimum of 2 years. Arthroscopy. Apr 2002;18(4):372-7.
86. O’Brien SJ, Pagnani MJ, Fealy S, McGlynn SR, Wilson JB. The active compression test: a new and effective test for diagnosing labral tears and acromioclavicular joint abnormality. Am J Sports Med. Sep-Oct 1998;26(5):610-3.
87. Onga T, Yamamoto T, Akisue T, Marui T, Kurosaka M. Biceps tendinitis caused by an osteochondroma in the bicipital groove: a rare cause of shoulder pain in a baseball player. Clin Orthop Relat Res. Feb 2005;431:241-4.
88. Ouellette H, Labis J, Bredella M, et al. Spectrum of shoulder injuries in the baseball pitcher. Skeletal Radiol. Oct 3 2007;Epub ahead of print.
89. Pagnani MJ, Deng XH, Warren RF, Torzilli PA, Altchek DW. Effect of lesions of the superior portion of the glenoid labrum on glenohumeral translation. J Bone Joint Surg Am. Jul 1995;77(7):1003-10.
90. Panossian VR, Mihata T, Tibone JE, et al. Biomechanical analysis of isolated type II SLAP lesions and repair. J Shoulder Elbow Surg. Sep-Oct 2005;14(5):529-34.
91. Papatheodorou A, Ellinas P, Takis F, et al. US of the shoulder: rotator cuff and non-rotator cuff disorders. Radiographics. Jan-Feb 2006;26(1):e23.
92. Parentis MA, Mohr KJ, ElAttrache NS. Disorders of the superior labrum: review and treatment guidelines. Clin Orthop Relat Res. Jul 2002;(400):77-87.
93. Park SS, Loebenberg ML, Rokito AS, Zuckerman JD. The shoulder in baseball pitching: biomechanics and related injuries -- part 1. Bull Hosp Jt Dis. 2002-2003;61(1-2):68-79.
94. Patton WC, McCluskey GM 3rd. Biceps tendinitis and subluxation. Clin Sports Med. Jul 2001;20(3):505-29.
95. Paxinos A, Walton J, Rütten S, Müller M, Murrell GA. Arthroscopic stabilization of superior labral (SLAP) tears with biodegradable tack: outcomes to 2 years. Arthroscopy. Jun 2006;22(6):627-34.
96. Perez-Palomares S, Olivan-Blazquez B, Arnal-Burro AM, et al. Contributions of myofascial pain in diagnosis and treatment of shoulder pain. A randomized control trial. BMC Musculoskelet Disord. Jul 24 2009;10:92.
97. Perthes G. Uber operationen bei habitueller schulterluxation. Dtsch z Chir. 1906;85:199-227.
98. Prodromos CC, Ferry JA, Schiller AL, Zarins B. Histological studies of the glenoid labrum from fetal life to old age. J Bone Joint Surg Am. Oct 1990;72(9):1344-8.
99. Rees JD, Wilson AM, Wolman RL. Current concepts in the management of tendon disorders. Rheumatology (Oxford). May 2006;45(5):508-21.
100. Reid S, Liu M, Ortega H. Anterior shoulder dislocations in pediatric patients: are routine prereduction radiographs necessary?. Pediatr Emerg Care. Jan 2013;29(1):39-42.
101. Resch H, Golser K, Thöni H, Sperner G. Arthroscopic repair of superior glenoid labral. detachment. J Shoulder Elbow Surg. 1993;3:147-55.
102. Rhee YG, Cho NS, Cho SH. Traumatic anterior dislocation of the
4-shoulder NMS.indd 150 2014-01-14 11:05:20 AM