novel therapeutic strategies
TRANSCRIPT

Agro
FOO
D In
dustr
y Hi
Tech
- M
arc
h/A
pril
201
3 - V
ol. 2
4(2)
Novel therapeutic strategies for celiac diseaseAARON LERNERCarmel medical Center,Pediatric gastroenterology and nutrition unit, B.Rappaport School of Medicine, Technion-Israel Institute of Technology7, Michal St. Haifa, 34362, Israel
Into
lera
nces
KEYWORDS: celiac disease; therapy; gluten; immunomodulation; propyl endopeptidase; tissue transglutaminase.
ABSTRACT: Celiac disease is an autoimmune condition affecting genetically susceptible individuals, following ingestion of wheat gluten, barley or-rye products. The only life long treatment is strict gluten free diet which is difficult personally and socially, affecting quality of life. Therefore, there is a need for alternative therapeutic modalities. New attractive potential therapies were starting to immerge: selecting, changing, degrading, manipulating or binding the dietary toxic environmental factors, decreasing intestinal permeability toward gluten or blocking the deamination of gluten by inhibiting tissue transglutaminase or the HLA-DQ presenting groove by carefully designed false peptide, shifting the typical Th1 to Th2 inflammatory reaction or antagonizing major proinflammatory cytokines, enhancing regulatory immune function or developing preventive vaccines, blocking adhesion molecule, inducing gluten oral or intranasal tolerance or applying epithelial repairing mitogens to oppose the mucosal destruction. The present alternative therapeutic strategies for celiac disease are reviewed.
INTRODUCTION
Celiac diseaseCeliac disease (CD) is a life-long autoimmune condition (1) of the gastrointestinal tract, affecting the small intestine and extra-intestinal sites of genetically susceptible individuals. The worldwide mean incidence is 1:100. Gluten is the storage protein of wheat and its alcohol soluble gliadins are the offending toxic molecules of the disease together with structurally related components found in barley and rye. Tissue transglutaminase (tTG) is the auto antigen (2) and three main auto antibodies: anti endomysium, anti tTG and anti deaminated gliadin peptide are the most useful serological markers to screen for the disease (3). The genetic repertoire is expending, containing more then 50 non-HLA genes but HLA-DQ2 and HLA-DQ8 molecules are the most important, predisposing genetic factors.
PathophysiologyThe pathogenesis of the disease is being unraveled. Following is a stepwise description of the sequential chain of events operating in CD. After ingestion of gluten it is degraded to multiple segments. A 33 amino acid peptide, corresponding to amino acid 57-89 that is resistant to luminal digestion by gastric, pancreatic, and intestinal brush border proteases, yet reactive to tTG, plays a pivotal role in disease induction. The repertoire of gluten peptides is wider and includes some native and non tTG deaminated gluten peptides capable of T cell immune stimulation (4). Interestly, those immune peptides are proline (15%) and glutamine (35%)-rich polypeptides that are at the base of two major steps in the celiac inflammatory cascade: 1. They confer resistance to enzymatic breakdown, since the human intestine lack prolyl endopeptidase who can readily cleave proline-rich immunostimulatory gluten peptides. 2. The glutamine-rich gluten peptides are an ideal substrate for deamination by the tTG. The deamination is crucial for the stability and avidity of the presented peptide in the HLA-DQ groove and
recognition of T-cell epitopes. Upon exposure to gluten peptides, intestinal epithelium undergoes immediate cytoskeletal rearrangement and functional barrier integrity is lost. A para -cellular leak and an inappropriate immune response to gluten develops. In parallel, the local innate immune system is activated. IL-15 is a key factor. Gluten 31-49 peptide induces epithelial cell damage and intraepithelial lymphocyte recruitment. IL-15 is produced, resulting in further epithelial injury, expansion of intraepithelial lymphocytes, cytotoxic IFNγ secretion and enhancement of the dendritic cells capacity to present antigens. The sub epithelial compartment is rich in tTG. Due to its increased avidity to the glutamine-rich gluten peptides, deamination occurs thus facilitating the high affinity binding of the resultant negatively charged glutamic acid residues, in key positions on gliadin peptide T-cell epitopes, to HLA-DQ2/8 molecules. The presentation of antigen to CD4 T lymphocytes, in the lamina propria results in Th1-cell type activation and subsequent release of IFNγ, macrophage activation and proinflammatory cytokines (IFNγ, IL-2, TNFα, TGFβ, IL-6) release (5). The activated humeral immunity is the origin of numerous specific and associated auto antibodies (6). Each pathogenetic step described: the toxic environmental gluten ingested, the enzyme resistant gluten peptides, their increased intestinal uptake, the increased IL-15 production, tTG gluten deamidation and Th1 cell and macrophage activation, are events selected for potential future therapeutic modality(4,7 -13). Unraveling the disease pathogenesis has fostered research and development in several nutritional, enzymatic, biochemical, immunological, biological and genetic avenues to treat the disorder.
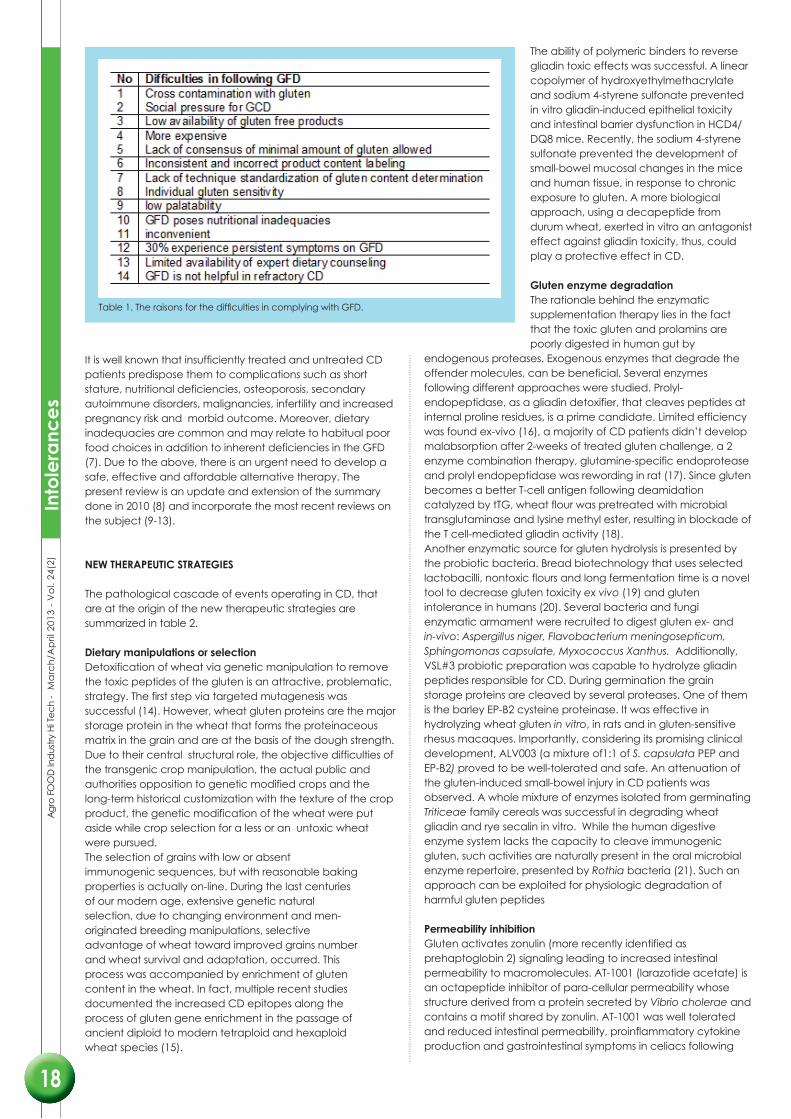
Need for alternative therapiesThe only treatment for CD is lifelong avoidance of gluten proteins. Those dietary restrictions in infancy and adulthood are a difficult experience for many patients. Complying with gluten free diet is difficult and decreases quality of life. Table 1 summarizes the difficulties in complying with gluten free diet.
AaronLerner
16
17
Intolerance
It is well known that insufficiently treated and untreated CD patients predispose them to complications such as short stature, nutritional deficiencies, osteoporosis, secondary autoimmune disorders, malignancies, infertility and increased pregnancy risk and morbid outcome. Moreover, dietary inadequacies are common and may relate to habitual poor food choices in addition to inherent deficiencies in the GFD (7). Due to the above, there is an urgent need to develop a safe, effective and affordable alternative therapy. The present review is an update and extension of the summary done in 2010 (8) and incorporate the most recent reviews on the subject (9-13).
NEW THERAPEUTIC STRATEGIES
The pathological cascade of events operating in CD, that are at the origin of the new therapeutic strategies are summarized in table 2.
Dietary manipulations or selectionDetoxification of wheat via genetic manipulation to remove the toxic peptides of the gluten is an attractive, problematic, strategy. The first step via targeted mutagenesis was successful (14). However, wheat gluten proteins are the major storage protein in the wheat that forms the proteinaceous matrix in the grain and are at the basis of the dough strength. Due to their central structural role, the objective difficulties of the transgenic crop manipulation, the actual public and authorities opposition to genetic modified crops and the long-term historical customization with the texture of the crop product, the genetic modification of the wheat were put aside while crop selection for a less or an untoxic wheat were pursued.The selection of grains with low or absent immunogenic sequences, but with reasonable baking properties is actually on-line. During the last centuries of our modern age, extensive genetic natural selection, due to changing environment and men-originated breeding manipulations, selective advantage of wheat toward improved grains number and wheat survival and adaptation, occurred. This process was accompanied by enrichment of gluten content in the wheat. In fact, multiple recent studies documented the increased CD epitopes along the process of gluten gene enrichment in the passage of ancient diploid to modern tetraploid and hexaploid wheat species (15).
The ability of polymeric binders to reverse gliadin toxic effects was successful. A linear copolymer of hydroxyethylmethacrylate and sodium 4-styrene sulfonate prevented in vitro gliadin-induced epithelial toxicity and intestinal barrier dysfunction in HCD4/DQ8 mice. Recently, the sodium 4-styrene sulfonate prevented the development of small-bowel mucosal changes in the mice and human tissue, in response to chronic exposure to gluten. A more biological approach, using a decapeptide from durum wheat, exerted in vitro an antagonist effect against gliadin toxicity, thus, could play a protective effect in CD.
Gluten enzyme degradation The rationale behind the enzymatic supplementation therapy lies in the fact that the toxic gluten and prolamins are poorly digested in human gut by
endogenous proteases. Exogenous enzymes that degrade the offender molecules, can be beneficial. Several enzymes following different approaches were studied. Prolyl-endopeptidase, as a gliadin detoxifier, that cleaves peptides at internal proline residues, is a prime candidate. Limited efficiency was found ex-vivo (16), a majority of CD patients didn’t develop malabsorption after 2-weeks of treated gluten challenge, a 2 enzyme combination therapy, glutamine-specific endoprotease and prolyl endopeptidase was rewording in rat (17). Since gluten becomes a better T-cell antigen following deamidation catalyzed by tTG, wheat flour was pretreated with microbial transglutaminase and lysine methyl ester, resulting in blockade of the T cell-mediated gliadin activity (18). Another enzymatic source for gluten hydrolysis is presented by the probiotic bacteria. Bread biotechnology that uses selected lactobacilli, nontoxic flours and long fermentation time is a novel tool to decrease gluten toxicity ex vivo (19) and gluten intolerance in humans (20). Several bacteria and fungi enzymatic armament were recruited to digest gluten ex- and in-vivo: Aspergillus niger, Flavobacterium meningosepticum, Sphingomonas capsulate, Myxococcus Xanthus. Additionally, VSL#3 probiotic preparation was capable to hydrolyze gliadin peptides responsible for CD. During germination the grain storage proteins are cleaved by several proteases. One of them is the barley EP-B2 cysteine proteinase. It was effective in hydrolyzing wheat gluten in vitro, in rats and in gluten-sensitive rhesus macaques. Importantly, considering its promising clinical development, ALV003 (a mixture of1:1 of S. capsulata PEP and EP-B2) proved to be well-tolerated and safe. An attenuation of the gluten-induced small-bowel injury in CD patients was observed. A whole mixture of enzymes isolated from germinating Triticeae family cereals was successful in degrading wheat gliadin and rye secalin in vitro. While the human digestive enzyme system lacks the capacity to cleave immunogenic gluten, such activities are naturally present in the oral microbial enzyme repertoire, presented by Rothia bacteria (21). Such an approach can be exploited for physiologic degradation of harmful gluten peptides
Permeability inhibitionGluten activates zonulin (more recently identified as prehaptoglobin 2) signaling leading to increased intestinal permeability to macromolecules. AT-1001 (larazotide acetate) is an octapeptide inhibitor of para-cellular permeability whose structure derived from a protein secreted by Vibrio cholerae and contains a motif shared by zonulin. AT-1001 was well tolerated and reduced intestinal permeability, proinflammatory cytokine production and gastrointestinal symptoms in celiacs following
Table 1. The raisons for the diffi culties in complying with GFD.
Agro
FOO
D In
dustr
y Hi
Tech
- M
arc
h/A
pril
201
3 - V
ol. 2
4(2)
Into
lera
nces
18
Into
lera
nce
gluten exposure. The product is currently the subject of phase IIb clinical trail and its efficacy awaits verification. It should be noted that gliadin peptides also have a transcellular intestinal epithelium entry, involving secretory IgA and its receptor, which logically is not blocked by larazotide acetate.
tTG blockadetTG is a promising target for therapeutic intervention in CD aimed at blocking its activity for 2 reasons: 1. Gluten deamination by tTG enhances the immune response to gluten in celiacs while blocking deamination will curtail it.2. It will control the proinflammatory activity of tTG. Multiple peptides and non-peptides, competitive and or active site irreversible inhibitors were suggested, however, they are all in the discovery phase (10). Since tTG2 is involved in major biological pathways like apoptosis, cell adhesion, signal transduction, collagen assembly and wound repair mechanism, its systemic inhibition can be harmful. The potential inhibitor should be safe, has limited activity to the gut and effective. The suicide inhibitor, L-682777 was suggested and abandoned since it is a specific inhibitor of factor XІІІa. On the contrary, KCC009 inhibits intestinal tTG2 when given orally, well tolerated by rodents, has short serum half-life and looks promising for further evaluation. An alternative way to explore the subject is by a mouse model with activated intestinal tTG and application of tTG inhibitors (22). However, tTG inhibitors do not block ex vivo gliadin-induced infiltration of CD8+ intraepithelial lymphocytes nor enhanced epithelial apoptosis and IgA-mediated transcellular transport of intact toxic gliadin peptide to the lamina propria. It appears that the present strategy is operative in preventing gliadin-induced adaptive but not the innate immune response.
HLA-DQ groove blockadeBlocking the binding of gliadin peptides to celiac specific HLA-DQ is also an attractive future therapeutic strategy. An amino acid substitution of a gliadin T-cell stimulatory sequence can convert the epitope to an agonist or antagonist inducing anergy and abolishing the inflammatory cascade (23). Alanine single amino acid substitution in position from 3 troughs 8 and 10 of an immunodominant peptide of wheat α-gliadin, abolished its immunogenicity. On the same line, single amino acid substitution in the sequence of T-cell stimulant gliadin peptide 57-73, prevented INF-γ secretion by peripheral blood lymphocytes. Substituting residues in positions 64-67, corresponded to the peptide’s anchor in the HLA-DQ cleft. Substitution of proline residues by azidoprolines inhibited gluten-induced T-cell activation but actually, more potent HLA-DQ blockers were identified (23). In future studies the efficacy of those compounds to completely abolish the immune response in CD patients remains to be established.
Th1 to Th2 shiftThe same decapeptide, originated from durum wheat, mentioned before shifted the mucosal T-cell immune response from a Th1 phenotype to Th2
phenotype, dominated by IL-10 production instead of INF-γ secretion, thus inhibiting the inflammatory cascade (24). An additional approach, based on the hygiene hypothesis, uses infections with enteric parasites to push the balance toward Th2. In celiac patients, inoculated by Necator americanus, the production of IFN-γ was reduced but mucosal histology and inflammatory changes occurred similarly to the control group. In another study, from the same Australian group, hookworm infection suppressed the inflammatory immune responses in the CD patients.
Anti-inflammatory cytokinesThe potential cytokine therapy for CD was summarized in several recent reviews (8-13). Only human recombinant IL-10 was tried and showed suppression of gluten-dependent T-cell activation in CD cultured intestinal mucosa (25). Antibodies neutralizing INF-γ, CD3, CD20, CD40L, TNF and humanized anti-IL-15 are additional logical candidates. Most recently, a protocol using humanized Mik-beta-1 monoclonal antibody to IL-2/15Rβ (CD122) is in a clinical trial in leukemia. Refractory celiac disease where IL-15 and his receptor are playing a critical role is a prime candidate for such a therapy (26). The biological against adhesion are mentioned in the paragraph "Inhibitors of T- cell migration".
Gluten peptide vaccine and tolerance inductionAny human autoimmune disease with known causative antigen can be amenable to peptide-based, antigen-specific therapy. The potential of the vaccines to suppress gluten-selected T cells and to induce Tregs could abolish the pathogenic T cells operating in CD. Phase І clinical trails investigating nexvax2, a vaccine containing three 15-16 mer DQ2 immunoactive peptides to induce tolerance to gluten have been conducted. Vaccine-specific T-cells responses were shown with some gastrointestinal symptoms. No DQ8-specific vaccine was investigated in CD. Tolerance induction by oral antigen administration is successfully used to prevent experimental autoimmune diseases. A large European study of gluten introduction to high risk babies, between the ages 4-7 month is on its way in order to explore gluten tolerance induction early in life. Intranasal administration, however, of a recombinant α-gliadin down-regulated the immune response to wheat gliadin in DQ8 transgenic mice (27).
Agro FOO
D Industry Hi Tech - M
arch/A
pril 2013 - V
ol. 24(2)Intolerances
19
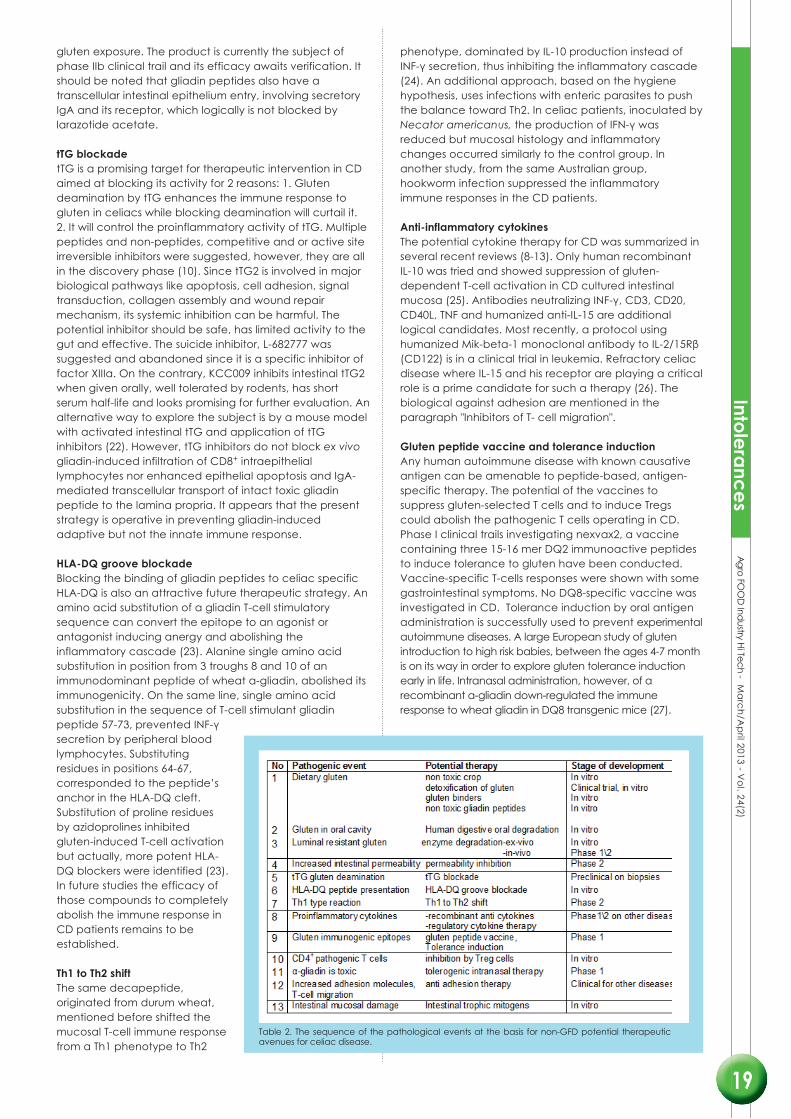
Table 2. The sequence of the pathological events at the basis for non-GFD potential therapeutic avenues for celiac disease.

Inhibition by Tr1 cellsDietary Ag-specific Tr1 cells are present in the human intestinal mucosa and strategies to boost their numbers and/or function may offer new therapeutic opportunities to restore gut homeostasis. Recently, gliadin-specific type1 regulatory T cells from the intestinal mucosa of treated celiac patients were shown to inhibit pathogenic T cells (28). Additionally, since anti-CD3 is a potential inducer of Tregs, it may be relevant in CD.
Inhibitors of T-cell migrationSelective inhibition of leukocyte adhesion to suppress inflammatory disease wastried in multiple sclerosis and inflammatory bowel disease. Antibodies targeting CCR9 and CCL25 were shown to suppress animal induced intestinal inflammation. CCX282-B is a selective human CCR9 antagonist that was shown to reduce the inflammation in Crohn’s disease mouse model. Integrin-α4 antagonist and more so, humanized anti integrin-α4β7 are potential candidates for CD inflammatory modulation.
Intestinal trophic mitogenA potential therapeutical avenue is the discovery of novel epithelial mitogens that stimulates mucosal growth in both the small and large intestine. Recently, R-spondin1, such an intestinal mitogen, was shown to stimulate crypt cell growth, accelerate mucosal regeneration and restore intestinal architecture in experimental colitis in mice (29).
SUMMARY
CD is a prevalent and curable condition affecting 1% of the population. Strict gluten free diet is the only life-long therapy but it is difficult to sustain and affects quality of life. Due to the low dietary compliance and the predisposition for complications, there is an urgent need for an alternative therapy. Recent publications documented the enthusiasm of the celiac patients toward the potential pharmaceutical therapies. Based on the increased knowledge on the disease pathophysiology and the steps of the inflammatory cascade progress, attractive therapeutical targets were selected: selecting, changing, degrading, manipulating or binding the dietary toxic environmental factors, decreasing intestinal permeability toward gluten or blocking the deamination of gluten or the HLA-DQ groove, shifting to Th2 inflammatory reaction or antagonizing proinflammatory cytokines, enhancing regulatory immune function or developing preventive vaccines, blocking adhesion molecule, inducing gluten tolerance or applying novel epithelial repairing mitogens. Time will tell which of those therapeutical avenues will come forward with a safe, effective and affordable profile for the benefit of CD patients. The in vitro models developed for gluten toxicity (30), will become important to verify the efficacy of the future therapeutic strategies, before proceeding to clinical trials.
REFERENCES
1. Lerner A, Blank M, Shoenfeld Y., Isr J Med Sci, 32:33-6 (1996). 2. Reif S, Lerner A., Autoimmun Rev, 3:40-45 (2004).3. Rozenberg O, Lerner A, et al., Crit Rev allerg Immunol. 42:331-341 (2012).4. Lerner A., Harefuah, 151:358-361 (2012).5. Lahat N, Shapiro S, et al., Scand J Immunol 49:441-446 (1999).6. Shaoul R. Lerner A., Autoimmun. Rev. 6:559- 65 (2007).7. Shepherd SJ, Gibson PR., J Hum Nutr Diet Nov 30; Epub ahead of print.(2012)8. Lerner A,. Autoimmun. Rev. 9:144-147 (2010).9. Donnelly SC, Ellis HJ, Ciclitira PJ., Expert Opin Pharmacother 12:1731-44 (2011).10. Sollid LM, Khosla C., J Inter Med 269:604-13 (2011).11. McAllister CS, Kagnoff MF., Semin Immunopathol 34:581-600 (2012).12. Lindfors K, Lahdeaho ML, et al., Expert Opin Ther Targets 16:665-75 (2012).13. Lahdeaho ML, Lindfors K, et al., Expert Opin Biol Ther 12:1589-600 (2012).14. Vader LW, Stepniak DT, et al., Gastroenterol. 125:1105-13 (2003).15. Lerner A., Med Hypotheses. 77;773-6 (2011).16. Matysiak-Budnik T, Candalh C, et al., Gastroenterology. 129:786-96 (2005).17. Gass J, Bethune MT, Gastroenterol. 133:472-80 (2007).18. Gianfrani C, Siciliano RA, et al., Gastroenterol. 133:780-9 (2007).19. Di Cagno R, Rizzello CG, et al., J Food Prot. 71:1491-5 (2008).20. Di Cagno R, De Angelis M, et al., Appl Environ Microbiol. 70:1088-96 (2004).21. Zamakhchari M, Wei G, et al., Plos One 6:e24455 (2011).22. Dafik L, Alberelli M, et al., Plos one 7:e30642 (2012).23. Juse U, van de Wal et al., Hum Immunol 71:475-81 (2012).24. Silano M, Di benedetto R, et al., Am J Clin Nutr. 87:415-23 (2008).25. Salvati VM, Mazzarella G, et al., Gut. 54:46-53 (2005).26. Waldmann TA, Conlon KC, et al., Blood. 121:476-84(2012).27. Senger S, Luongo D, et al., Immunol Lett. 88:127-34 (2003).28. Gianfrani C, Levings MK, et al., J Immunol. 177:4178-86 (2006).29. Zhao J, de Vera J, et al., Gastroenterol. 132:1331-43 (2007).30. Lindfors K, Rauhavira T, et al., Exp Biol Med 237:119-25 (2012).