mo1659 the pi3k/akt/mtor pathway in gastric cancer and its potential relationship with mir-125b,...
TRANSCRIPT

ORIGINAL ARTICLE
The PI3K/AKT/mTOR pathway is activated in gastric cancerwith potential prognostic and predictive significance
Oscar Tapia & Ismael Riquelme & Pamela Leal & Alejandra Sandoval & Susana Aedo &
Helga Weber & Pablo Letelier & Enrique Bellolio & Miguel Villaseca & Patricia Garcia &
Juan Carlos Roa
Received: 17 October 2013 /Revised: 31 March 2014 /Accepted: 28 April 2014 /Published online: 21 May 2014# Springer-Verlag Berlin Heidelberg 2014
Abstract Signaling pathway alterations are important in thedevelopment of gastric cancer (GC). Deregulation of thePI3K/AKT/mTOR pathway plays a crucial role in the regula-tion of multiple cellular functions including cell growth, prolif-eration, metabolism, and angiogenesis. Our goal was to assessexpression of proteins involved in the PI3K/AKT/mTOR path-way by immunohistochemistry (IHC) in tumor and nontumorgastric mucosa from patients with advanced GC. We evaluated71 tumor and 71 nontumor gastric mucosa samples from ad-vanced GC patients, selected from Hernán Henríquez AravenaHospital (Temuco, Chile). The targets studied were PI3K, AKT,p-AKT, PTEN, mTOR, p-mTOR, P70S6K1, p-P70S6K1, 4E-BP1, p-4E-BP1, eIF4E, and p-eIF4E. Expression data werecorrelated with clinicomorphological data. Descriptive and an-alytical statistics were used (95% confidence interval, p<0.05).For survival analyses, the Kaplan–Meier method and the log-rank test were used. PI3K, AKT, p-AKT, p-mTOR, p-4E-BP1,P70S6K1, p-P70S6K1, eIF-4E, and p-eIF-4E proteins weresignificantly overexpressed in tumor tissue. Conversely, PTEN
was underexpressed in tumor tissue, notably in pT3-pT4 tumors(p=0.02) and tumors with lymph node metastases (p<0.001).P70S6K1 expression was associated with pT3-pT4 tumors(p=0.03). Moreover, PI3K (p=0.004), AKT (p=0.01), p-AKT (p=0.01), P70S6K1 (p=0.04), p-P70S6K1 (p=0.001),and eIF-4E (p=0.004) were overexpressed in tumors withlymph node metastases. Low expression of 4E-BP1 was asso-ciated with poor overall survival (p=0.03). Our results suggestthat the PI3K/AKT/mTOR pathway is activated in GC, withoverexpression in tumor tissue of most of the studied proteins(total and phosphorylated). These might be considered as targetfor specific targeted therapy in GC.
Keywords AKT .mTOR . Immunohistochemistry . Gastriccancer
Introduction
Gastric cancer (GC) is the second cause of cancer mortalityworldwide. In Chile, GC is the main cause of death by cancer[1, 2]. Themainmorphological prognostic factors are the levelof infiltration of the tumor in the wall of the stomach (T stage)and lymph node involvement (N stage) [3–5].
Advances in molecular profiling and genomics have re-vealed that the phosphatidylinositol 3-kinases (PI3K)/AKT/mammalian target of the rapamycin (mTOR) signaling path-way plays a crucial role in mediating multiple cellular func-tions including cell growth, proliferation, metabolism, surviv-al, and angiogenesis (Fig. 1). Growth factor signaling medi-ated by the PI3K pathway through AKT, TSC1, and TSC2proteins activates mTOR. TSC1 and TSC2 form a dimer(TSC1/TSC2) to regulate mTOR activity indirectly. Whenupstream signals are activated, TSC1/TSC2 is inhibited byAKT, allowing mTOR (mTORC1) activation. Meanwhile,
Oscar Tapia and Ismael Riquelme are both first authors because theycontributed equally to the realization of this work.
Founded by FONDECYT Grant No 11110239.
O. Tapia : I. Riquelme : P. Leal :A. Sandoval : S. Aedo :H.Weber :P. Letelier : E. Bellolio :M. VillasecaDepartment of Pathology, Universidad de La Frontera,CEGIN-BIOREN, Temuco, Chile
P. LetelierSchool of Health Sciences, Universidad Católica de Temuco,Temuco, Chile
P. Garcia : J. C. Roa (*)Department of Pathology, School of Medicine, PontificiaUniversidad Católica de Chile, Marcoleta 377, 8330024 Santiago,Chilee-mail: [email protected]
Virchows Arch (2014) 465:25–33DOI 10.1007/s00428-014-1588-4

P70S6K1 and mTOR complex 2 (mTORC2) seem to act as anegative feedback mechanism to stop the activity of AKTandother proteins on mTORC1. Therefore, in cancer cells, PI3K-AKT increases its activity, which activates mTOR complex 1(mTORC1) by phosphorylation and decreases the feedbackactivity of P70S6K1-mTORC2. These changes result in un-controlled and increased mitochondrial processes, angiogene-sis, and ribosome biogenesis for greater protein synthesis, cellgrowth, proliferation, and autophagy [6–10].
Because of the limited number of studies in GC address-ing more than three targets, we aimed to determine theexpression level of proteins in the PI3K/AKT/mTOR sig-naling pathway by immunohistochemistry (IHC). We in-cluded PI3K, PTEN, and total and phosphorylated fractionof AKT, mTOR, P70S6K1, 4E-BP1, and eIF4E, which
allowed us to identify potential new biomarkers and thera-peutic targets to treat patients with constitutive activation ofthese pathway components.
Materials and methods
Patients and tissue samples
We chose a case–control study design. We selected an adeno-carcinoma and a paired nontumor gastric mucosa sample from71 patients with advanced GC from the archives of the Pa-thology Unit at HernanHenriquez Aravena Hospital (Temuco,Chile). This study was approved by the ethics committee ofthe Faculty of Medicine at the Universidad de La Frontera
Fig. 1 The PI3K/AKT/mTORsignaling pathway
26 Virchows Arch (2014) 465:25–33

(Temuco, Chile). The clinicopathological data of the 71 pa-tients were obtained from medical records and are summa-rized in Table 1.
Briefly, the patient group consisted of 25 females and 46males with a median age of 62.3±11.2 years, 5 (7 %) ofMapuche ethnicity and 66 (93 %) Hispanic. Four cases wereclassified as pT2 (6 %), 38 as pT3 (53 %), and 29 as pT4(41 %) according to the TNM classification system (7th ed.).We classified 35 cases as well differentiated, 31 as moderatelydifferentiated, and 5 as poorly differentiated. Complete post-operative follow-up was available for 68 patients (96 %).
Immunohistochemistry
Tissue microarrays (TMAs) were constructed with 2 mmcores of 2 different representative areas of each tumor andnormal control mucosa. The IHC procedure was carried outaccording to García et al. [11]. Briefly, 4-μm thick sectionswere cut from each tissue microarray and de-waxed in xylene,rehydrated through graded concentrations of ethanol, andplaced in an antigen retrieval solution (citrate buffer, pH 6.0)for 15 min at 95 °C. After cooling for 30 min, the tissuesections were incubated in 3 % hydrogen peroxide for10 min to block endogenous peroxidase activity. The slideswere then washed thoroughly with phosphate-buffered salineand incubated (120 min, room temperature) with each anti-body (Table 2). Labeling was detected with the Liquid DABSubstrate-Chromogen System (Dako North America Inc,Carpinteria, CA, ISA) according to the manufacturer’s proto-col. Sections were counterstained with hematoxylin, thendehydrated, cleared, and mounted. Negative control was pre-pared by replacing the primary antibody with phosphate-buffered saline.
Evaluation of immunohistochemical staining
The expression of the PI3K/AKT/mTOR signaling pathwaycomponents was evaluated in nontumor and tumor issues. Theproteins studied in this work were PI3K, PTEN, AKT, p-AKT,mTOR, p-mTOR, P70S6K1, p-P70S6K1, 4E-BP1, p-4E-BP1, eIF4E, and p-eIF4E. The slides were examined indepen-dently by two pathologists (OTand JCR) who were blinded toboth the clinical and pathological data. IHC staining wasevaluated using a previously described semiquantitative scor-ing system [12]. Staining intensity was scored as 1 (negative),2 (weak), 3 (moderate), and 4 (intense). The percentage ofpositive cells was quantified as 0 (none), 1 (1–25 %), 2 (26–50 %), 3 (51–75 %), and 4 (76–100 %). For statistical analy-sis, the sum score of intensity and extent of staining wasgrouped into low (final score, 0 to 4) or high (final score, 5to 7; Table 3).
Statistical analyses
All statistical analyses were performed using GraphPad Prism5 (GraphPad Software, Inc.). The associations between IHCexpression and clinicopathological variables were examinedusing χ2 test and Fisher’s exact test for categorical variablesand the Student’s t test for continuous variables. Kaplan–Meier survival curves were plotted for cases with high versuslow expression of 4E-BP1. The difference between the sur-vival curves was analyzed using the log-rank test. A value ofp<0.05 was considered statistically significant.
Results
We examined IHC expression of proteins of the PI3K/AKT/mTOR signaling pathway and downstream effectors in tumorand nontumor tissue from patients with advanced gastriccancer in a TMA format. The proteins investigated werePI3K, PTEN, AKT, p-AKT, mTOR, p-mTOR, P70S6K1, p-P70S6K1, 4E-BP1, p-4E-BP1, eIF4E, and p-eIF4E. Examplesof staining intensity of upregulated and downregulated pro-teins are illustrated in Fig. 2. Statistically significant differ-ences were observed for 10 of the 12 proteins investigated.High expression in tumor tissue versus nontumor tissue wasfound for PI3K (p=0.001), AKT (p=0.01), P70S6K1(p=0.002), eIF4E (p<0.001) p-AKT (p=0.03), p-mTOR(p<0.001), p-4E-BP1 (p<0.001), p-P70S6K1 (p=0.01), andp-eIF4E (p<0.001). Conversely, PTEN was found to bedownregulated in tumor tissue (p<0.001; Figs. 2 and 3).
The clinicopathological features of the 71 tumor samples,including age, gender, ethnicity, histological grade, infiltrationlevel (pT), and lymph node involvement (pN), are summa-rized in Table 1. We found no correlation between expressionlevels and age or ethnic group. AKT was found to beoverexpressed in gastric cancer in male patients (p=0.02)and 4E-BP1 in female patients (p=0.02). PTEN wasunderexpressed in pT3 and pT4 tumors (p=0.02) whileP70S6K1 was overexpressed in pT3 and pT4 tumors(p=0.03). PI3K (p=0.004), AKT (p=0.01), p-AKT(p=0.01), P70S6K1 (p=0.04), p-P70S6K1 (p=0.001), andeIF4E (p=0.004) showed a high expression level in tumorswith lymph node metastases. In contrast, a low level of ex-pression of PTEN (p<0.001) was observed in tumors withlymph node metastases. Survival analysis showed a signifi-cant association between low expression of 4E-BP1 and pooroverall survival (p=0.03) (Fig. 4).
Discussion
Multiple risk factors for GC have been identified, includingtobacco smoking, salt consumption, smoked foods, meat and
Virchows Arch (2014) 465:25–33 27

Tab
le1
Clin
icalandpathologicalvariablesof
patientswith
gastriccancer
(n=71)
PI3K
PTEN
AKT
p-AKT
mTOR
p-mTOR
P70S
6Kp-70S6K
4EBP1
p-4E
BP1
eIF4
Ep-eIF4
E
Age
(mean±SD)
62.3±11.2
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
Gender%
(n)
N.S
N.S
0.02
N.S
N.S
N.S
N.S
N.S
0.02
N.S
N.S
N.S
Wom
en25
(35%)
11/25(44%)
15/25(60%)
Men
46(65%)
28/46(61%)
19/46(41%)
Ethnicgroup%
(n)
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
Mapuche
5(7
%)
Hispanic
66(93%)
Levelof
infiltration%
(n)
N.S
0.02
N.S
N.S
N.S
N.S
0.03
N.S
N.S
N.S
N.S
N.S
pT1
––
–
pT2
4(6
%)
3/4(75%)
1/4(25%)
pT3
38(53%)
15/38(39%)
22/38(58%)
g
pT4
29(41%)
11/29(38%)
18/29(62%)
Lym
phnodes%
(n)
0.004
<0.001
0.01
0.01
N.S
N.S
0.04
0.001
N.S
N.S
0.004
N.S
pN0
19(27%)
5/19
(26%)
14/19(74%)
7/19
(37%)
5/19
(26%)
8/19
(42%)
5/19
(26%)
4/19
(21%)
pN1
14(20%)
5/14
(36%)
9/14
(64%)
6/14
(43%)
6/14
(43%)
6/14
(43%)
6/14
(43%)
3/14
(21%)
pN2
11(15%)
8/11
(73%)
3/11
(27%)
7/11
(64%)
8/11
(73%)
8/11
(73%)
9/11
(81%)
8/11
(73%)
pN3
27(38%)
19/27(70%)
7/27
(26%)
17/27(63%)
19/27(70%)
17/27(63%)
21/27(78%)
17/27(63%)
pTNM
%(n)
0.01
0.002
N.S
N.S
N.S
N.S
0.02
0.008
N.S
N.S
0.02
N.S
IB4(6
%)
2/4(50%)
3/4(75%)
2/4(50%)
1/4(25%)
1/4(25%)
IIA
15(21%)
4/15
(27%)
12/15(80%)
5/15
(33%)
5/15
(33%)
5/15
(33%)
IIB
14(20%)
5/14
(36%)
9/14
(64%)
5/14
(36%)
4/14
(29%)
6/14
(43%)
IIIA
9(12%)
6/9(67%)
3/9(33%)
5/9(56%)
6/9(67%)
6/9(67%)
IIIB
2(3
%)
2/2(100
%)
0/2(0
%)
1/2(50%)
2/2(100
%)
2/2(100
%)
IIIC
27(38%)
19/27(70%)
6/27
(22%)
21/27(78%)
21/27(78%)
20/27(74%)
Degreeof
differentiation%
(n)
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
N.S
Poor
5(7
%)
Moderate
31(44%)
Well
35(49%)
The
fractio
nsandpercentagesrepresentthe
positiv
estaining
with
inthetotalnum
berofeachgroupofvariables.The
pvalues
refertothestatisticaldifferencesfoundwith
inthegroups
forv
ariables
analyzed
relatedto
each
target.F
isher’stestandStudent’s
ttestw
ereused
accordinglyto
calculatepvalues
28 Virchows Arch (2014) 465:25–33

nitrites in the diet, family history, male sex, blood group A,Ménétrier’s disease, history of partial gastrostomy for non-neoplastic conditions, and Helicobacter pylori infection. Thelatter risk factor has been closely linked to intestinal-typegastric cancer in the Lauren classification [13–18].
Recent studies have suggested that the PI3K/AKT/mTORpathway and its main effector, mTORC1, are activated in GC,deregulating key cell processes such as angiogenesis, metab-olism, cell growth, and proliferation [19–27] (Fig. 1). Phos-phorylation of Ser2448 through the PI3K/AKT pathway acti-vates mTORC1, resulting in activation of the eukaryotic ini-tiation factor 4E (elF4E) and the ribosomal S6 kinase p70(p70S6 kinase 1) and inactivation of the eIF4E inhibitor 4E-BP1. Activation of mTORC1 increases expression of media-tors involved in cell growth and division (e.g., cyclin D1) anddecreases expression of negative regulators of cell cycle pro-gression. In addition, mTORC1 modulates cell metabolism,stimulating the expression of the nutrient transporters on thecell surface, which increases the nutrient supply to achieve themetabolic and energy requirements of cells in proliferation[27–29]. In the same way, mTORC1 increases HIF-1α trans-lation, triggering the expression of proangiogenic factors likeVEGF [30].
This pathway has also been reported as active in CNS,endocrine, gynecological, gastrointestinal, and urological
and hematological malignancies. Statistically significant asso-ciations between the state of the PI3K/AKT/mTOR pathwayand various prognostic clinicopathological parameters, suchas the stage of the disease, the degree of tumor differentiation,nodal and distant metastasis, tumor size, and chemosensitivityhave been reported [10, 31–36]. Recognition of the impor-tance of mTOR as attractive target for anticancer therapyhas lead to the development of new drugs (temsirolimus,everolimus, and deforolimus) with tumor growth inhibitingand antiangiogenic properties and promising results in ex-perimental studies.
Previous studies on GC by other authors have shown thatexpression of PI3K, AKT, p-AKT, mTOR, p-mTOR,P70S6K1, and p-P70S6K32 is increased in tumor tissue,indicating that the PI3K/AKT/mTOR pathway is activated.Activation has been associated with metastasis (PI3K), lowersurvival (p-AKT), pathogenesis, and progression (mTOR andp-P70S6K1) [38–42].
In GC, PI3K and p-AKT have been previously reported asstrongly expressed in 80 and 82 % of cases, respectively [43],which is similar to the results we obtained. Cinti et al. detected p-AKT immunostaining in 34 (68 %) of 50 cases without anycorrelation between p-AKT expression and gender, age, tumorlocation, or Lauren histotype. This is similar to our data, al-though we found overexpression associated with male gender(p=0.02). Cinti et al. also found p-AKTexpression to be signif-icantly correlated with depth of infiltration (pT) and lymph nodemetastases. We found no association with T stage but confirmthe correlation with lymph node metastases (p=0.01) [39].Another study reported low expression of AKT and p-AKT ingastric cancer (32.9 and 28.9 %, respectively) without anycorrelation with clinicopathological factors [37].
PTEN plays a fundamental role in the regulation of thispathway. Without PTEN upstream regulators of thePI3K/AKT/mTOR (PI3K-AKT) pathway, which inhibit apo-ptosis and increase cell proliferation and are shared by other
Table 2 Standardized conditions for each of the antibodies used. Antibodies used and standardized staining conditions
Antibody Brand Control (+) Dilution Retrieval Incubation Buffer dilution Staining
PI3K CellSignaling Lung Ca 1:200 Citrate pH 6.0 O.N 4 °C 8112 Membrane
PTEN CellSignaling Colon 1:25 Citrate pH 6.0 O.N 4 °C 8112 Cytoplasm
AKT CellSignaling Lung Ca 1:25 Citrate pH 6.0 O.N 4 °C 8112 Cytoplasm
p-AKT CellSignaling Lung Ca 1:25 Citrate pH 6.0 O.N 4 °C 8112 Cytoplasm
mTOR CellSignaling Breast Ca 1:25 Citrate pH 6.0 O.N 4 °C 8112 Cytoplasm
p-mTOR CellSignaling Breast Ca 1:25 Citrate pH 6.0 O.N 4 °C TBST Cytoplasm
eIF4E CellSignaling Colon 1:200 Citrate pH 6.0 O.N 4 °C 8112 Cytoplasm/nucleus
p-eIF4E Epitomics Breast Ca 1:100 Citrate pH 6.0 O.N 4 °C 8112 Membrane
4E-BP1 CellSignaling Lung Ca 1:400 Citrate pH 6.0 O.N 4 °C 8112 Cytoplasm
p-4E-BP1 CellSignaling Colon Ca 1:400 Citrate pH 6.0 O.N 4 °C 8112 Cytoplasm
p70S6K1 CellSignaling Breast Ca 1:60 Citrate pH 6.0 O.N 4 °C 8112 Cytoplasm
p-P70S6K1 SantaCruz Breast Ca 1:50 Citrate pH 6.0 O.N 4 °C 8112 Membrane
Table 3 Parameters used to evaluate expression level according toimmunohistochemistry staining
Intensity of staining % Cells Final score
0 Negative 0 0 0–2 0
1 Weak 1 1–25 % 3–4 1
2 Moderate 2 26–50 % 5 2
3 Intense 3 51–75 % 6–7 3
4 76–100 %
Virchows Arch (2014) 465:25–33 29
signaling networks activated in GC, such as Wnt and NF-κB,are no longer inhibited [44, 45]. Our finding of low or absentexpression of PTEN suggests that this protein loses its regu-latory capacity in advanced GC, with results similar to thosereported by Wen et al. [44] and Kang et al. [46].
Xiao et al. found no difference in total mTOR expressionbetween tumor tissue and normal tissue. Their multivariateanalysis showed that age, depth of invasion, lymphatic inva-sion, lymph node metastasis, Lauren’s classification, andmTOR expression are independent prognostic factors for gas-tric carcinoma (p<0.05) [42]. Corresponding with our results,Lang et al. reported strong expression of p-mTOR both inintestinal- and diffuse-type gastric adenocarcinoma (60 and
64 %, respectively) and in early and advanced tumor stages[47]. Increased p-mTOR expression was also reported by Sunet al. [48]. Murayama et al. found associations between p-mTOR and GC stage and clinicopathological features [41].Altogether, we conclude that in GCmTOR is activated mainlyby phosphorylation (p-mTOR) rather than overexpression,indicating its importance for cell growth, proliferation, anddifferentiation in GC and emphasizing its interest as a possiblemarker for this disease.
P70S6K1 and p-P70S6K1 have been reported asoverexpressed in several tumor types but few reports onP70S6K1 and p-P70S6K1 in gastric cancer have been pub-lished. Xiao et al. found high cytoplasmic expression of p-
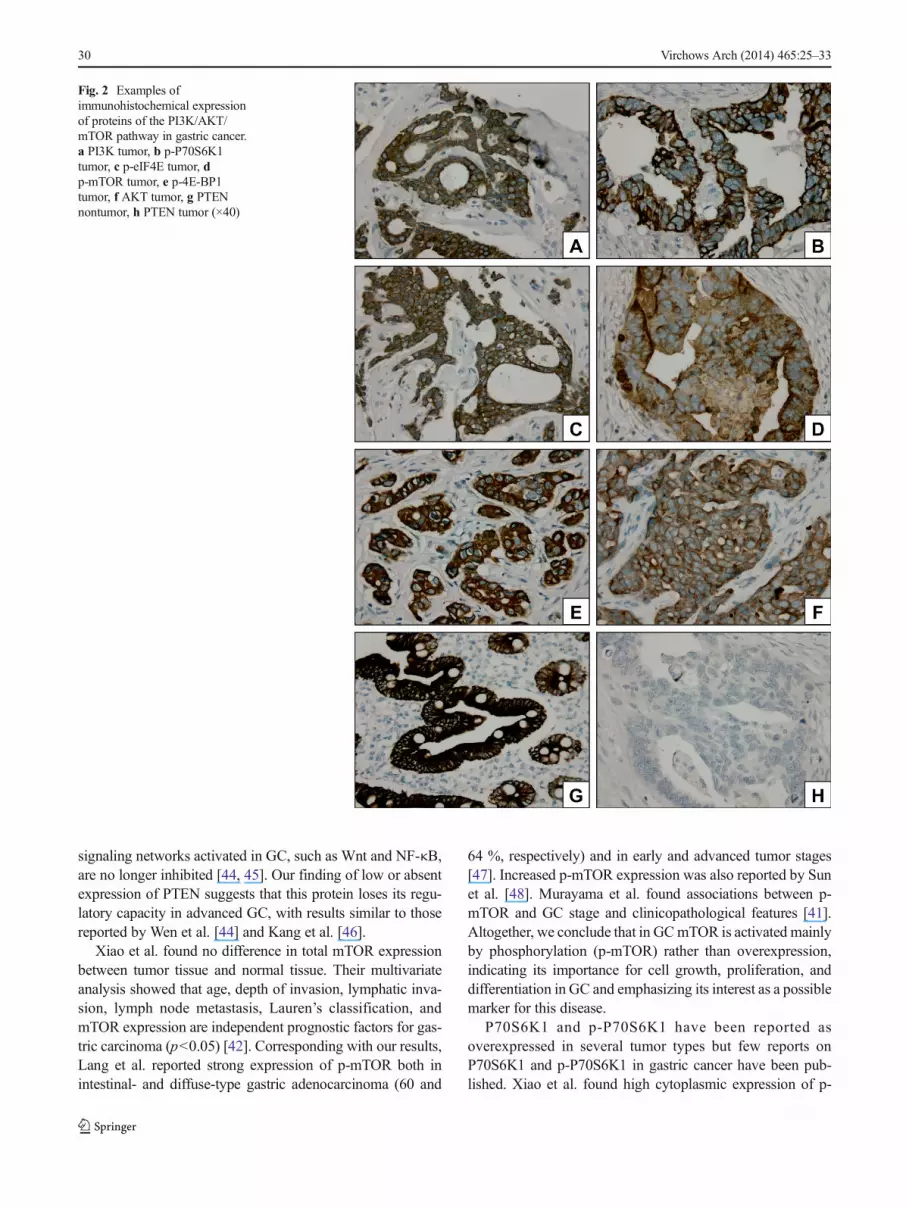
Fig. 2 Examples ofimmunohistochemical expressionof proteins of the PI3K/AKT/mTOR pathway in gastric cancer.a PI3K tumor, b p-P70S6K1tumor, c p-eIF4E tumor, dp-mTOR tumor, e p-4E-BP1tumor, f AKT tumor, g PTENnontumor, h PTEN tumor (×40)
30 Virchows Arch (2014) 465:25–33

P706SK1 in gastric adenoma in comparison with non-neoplastic mucosa (p<0.05) with prognostic significance[42]. We found overexpression of p-4E-BP1 in tumor tissuebut not of 4E-BP1. Yang et al. found decreased expression of4E-BP1 in gastric cardiac adenocarcinoma compared withnormal tissues, but a marked increase in the expression of p-4E-BP1 [49], the latter in agreement with our results. Also,Sun et al. reported overexpression of p-4E-BP1 in 68.4 % ofGC tissue samples tested, significantly higher than inparacancerous (57.9 %) and normal tissue samples (29 %)[48].
Overexpression of eIF4E and p-eIF4E has been reported inGC [50]. Chen et al. found overexpression of eIF4E to becorrelated with tumor vascular invasion and with lower sur-vival but no correlation with tumor invasion depth, lymphnode metastasis, or Lauren’s classification [51]. Liang et al.found that eIF4E and p-eIF4E are overexpressed in GC incomparison with adjacent noncancerous tissue (78.57 and76.19 %, respectively) with a significant correlation betweeneIF4E overexpression and distant metastasis [52]. We found a
strong correlation between high expression of eIF4E andTNM stage (p=0.02) and lymph node metastasis (p=0.004).Altogether, these results indicate that eIF4Emight be involvedin gastric carcinogenesis and might be used as an independentprognosis marker in GC patients.
Our results show that the PI3K/AKT/mTOR pathwaymight provide prognostic markers in GC, with potential im-pact on the choice of therapy in the case of inhibitors of PI3K,AKT and mTOR combined with other antineoplastic agents,as has been reported for other malignancies [53, 54]. Ourresults are substantiated by the simultaneous analysis of the12 most important target proteins of the PI3K/AKT/mTORsignaling pathway.
In summary, we provide immunohistochemical evidencethat the PI3K/AKT/mTOR pathway is activated in GC, withoverexpression of the majority of the proteins (total and phos-phorylated) involved in this pathway. The level of expressionof PI3K, AKT, p-AKT, PTEN, P70S6K1, p-P70S6K1, andeIF-4E is correlated with the depth of tumor infiltration andthe presence of lymph node metastases, which points towardstheir potential role as prognostic marker.
Conflict of interest The authors declare that they have no conflict ofinterest.
References
1. Jemal A, Bray F, Center M, Ferlay J, Ward E, Forman D (2011)Global cancer statistics. CA Cancer J Clin 61:69–90
2. Heise K, Bertran E, Andia ME, Ferreccio C (2009) Incidence andsurvival of stomach cancer in a high-risk population of Chile.World JGastroenterol 15:1854–1862
3. Recommendations for clinical practice: 2004 Standards, Options andRecommendations for management of patients with adenocarci-nomas of the stomach (excluding cardial and other histological forms
Fig. 3 Frequency of cases with high staining scores of proteins of the PI3K/AKT/mTOR pathway in nontumor and tumor tissues (*<0.05, **<0.01,***<0.001). Each bar indicates the percentage of high scoring cases per tissue type
Fig. 4 Kaplan–Meier curves for cumulative survival rate of patients withadvanced gastric cancer according to 4E-BP1 expression. The red lineindicates patients whose tumors expressed low levels of 4E-BP1 and theblue line indicates patients with high 4E-BP1 expression (p=0.03, log-rank test)
Virchows Arch (2014) 465:25–33 31

of cancer) Federation nationale des centres de lutte contre le cancer].(2005) Gastroenterol Clin Biol 29: 41–55
4. AllumWH, Griffin SM,Watson A, Colin-Jones D (2002) Guidelinesfor the management of oesophageal and gastric cancer. Gut 50(Suppl5):v1–v23
5. Nakajima T (2002) Gastric cancer treatment guidelines in Japan.Gastric Cancer 5:1–5
6. Al-Batran SE, Ducreux M, Ohtsu A (2012) mTOR as a therapeutictarget in patients with gastric cancer. Int J Cancer 130:491–496
7. Easton JB, Houghton PJ (2006) mTOR and cancer therapy.Oncogene 25:6436–6446
8. Fresno Vara JA, Casado E, de Castro J, Cejas P, Belda-Iniesta C,Gonzalez-Baron M (2004) PI3K/Akt signalling pathway and cancer.Cancer Treat Rev 30:193–204
9. Rosen N, She QB (2006) AKT and cancer—is it all mTOR? CancerCell 10:254–256
10. Bellacosa A, Kumar CC, Di CristofanoA, Testa JR (2005)Activationof AKT kinases in cancer: implications for therapeutic targeting. AdvCancer Res 94:29–86
11. Garcia P, Leal P, Alvarez H, Brebi P, Ili C, Tapia O et al (2013)Connective tissue growth factor immunohistochemical expression isassociated with gallbladder cancer progression. Arch Pathol LabMed137:245–250
12. Xiao L, Wang YC, Li WS, Du Y (2009) The role of mTOR andphospho-p70S6K in pathogenesis and progression of gastric carcino-mas: an immunohistochemical study on tissue microarray. J Exp ClinCancer Res 28:152
13. Van den Brandt PA, Botterweck AA, Goldbohm RA (2003) Saltintake, cured meat consumption, refrigerator use and stomach cancerincidence: a prospective cohort study (Netherlands). Cancer CausesControl 14:427–438
14. Mayne ST, Risch HA, Dubrow R, Chow WH, Gammon MD,Vaughan TL et al (2001) Nutrient intake and risk of subtypes ofesophageal and gastric cancer. Cancer Epidemiol Biomarkers Prev10:1055–1062
15. Knekt P, Jarvinen R, Dich J, Hakulinen T (1999) Risk of colorectaland other gastro-intestinal cancers after exposure to nitrate, nitrite andN-nitroso compounds: a follow-up study. Int J Cancer 80:852–856
16. La Vecchia C, Negri E, Franceschi S, Gentile A (1992) Familyhistory and the risk of stomach and colorectal cancer. Cancer 70:50–55
17. Palli D, Russo A, Ottini L, Masala G, Saieva C, Amorosi A et al(2001) Red meat, family history, and increased risk of gastric cancerwith microsatellite instability. Cancer Res 61:5415–5419
18. Huang JQ, Zheng GF, Sumanac K, Irvine EJ, Hunt RH (2003) Meta-analysis of the relationship between cagA seropositivity and gastriccancer. Gastroenterology 125:1636–1644
19. Sayed D, Abdellatif M (2010) AKT-ing via microRNA. Cell Cycle 9:3213–3217
20. Ambros V (2004) The functions of animal micro-RNAs. Nature 431:350–355
21. Calin GA, Croce CM (2006) MicroRNA signatures in human can-cers. Nat Rev Cancer 6:857–866
22. Filipowicz W, Bhattacharyya SN, Sonenberg N (2008) Mechanismsof post-transcriptional regulation by microRNAs: are the answers insight? Nat Rev Genet 9:102–114
23. Kozomara A, Griffiths-Jones S (2011) miRBase: integratingmicroRNA annotation and deepsequencing data. Nucleic AcidsRes 39:D152–D157
24. He L, Hannon GJ (2004) MicroRNAs: small RNAs with a big role ingene regulation. Nat Rev Genet 5:522–531
25. Edinger AL, Thompson CB (2002) Akt maintains cell size andsurvival by increasing mTOR-dependent nutrient uptake. Mol BiolCell 13:2276–2288
26. Wullschleger S, Loewith R, Hall MN (2006) TOR signaling ingrowth and metabolism. Cell 124:471–484
27. Hay N, Sonenberg N (2004) Upstream and downstream of mTOR.Genes Dev 18:1926–1945
28. Caron E, Ghosh S, Matsuoka Y, Ashton-Beaucage D, Therrien M,Lemieux S et al (2010) A comprehensivemap of the mTOR signalingnetwork. Mol Syst Biol 6:453
29. Foster KG, Fingar DC (2010) Mammalian target of rapamycin(mTOR): conducting the cellular signaling symphony. J Biol Chem285:14071–14077
30. Yang Q, Guan KL (2007) Expanding mTOR signaling. Cell Res 17:666–681
31. Altomare DA, Testa JR (2005) Perturbations of the AKT signalingpathway in human cancer. Oncogene 24:7455–7464
32. Bellacosa A, de Feo D, Godwin AK, Bell DW, Cheng JQ, AltomareDA et al (1995) Molecular alterations of the AKT2 oncogene inovarian and breast carcinomas. Int J Cancer 64:280–285
33. Altomare DA, You H, Xiao GH, Ramos-Nino ME, Skele KL, DeRienzo A et al (2005) Human and mouse mesotheliomas exhibitelevated AKT/PKB activity, which can be targeted pharmacological-ly to inhibit tumor cell growth. Oncogene 24:6080–6089
34. Altomare DA, Wang HQ, Skele KL, De Rienzo A, Klein-Szanto AJ,Godwin AK et al (2004) AKT and mTOR phosphorylation is fre-quently detected in ovarian cancer and can be targeted to disruptovarian tumor cell growth. Oncogene 23:5853–5857
35. Altomare DA, Tanno S, De Rienzo A, Klein-Szanto AJ, Tanno S,Skele KL et al (2002) Frequent activation of AKT2 kinase in humanpancreatic carcinomas. J Cell Biochem 87:470–476
36. Robertson GP (2005) Functional and therapeutic significance of Aktderegulation in malignant melanoma. Cancer Metastasis Rev 24:273–285
37. Oki E, Baba H, Tokunaga E, Nakamura T, Ueda N, Futatsugi M et al(2005) AKT phosphorylation associates with LOH of PTEN andleads to chemoresistance for gastric cancer. Int J Cancer 117:376–380
38. Liu JF, Zhou XK, Chen JH, Yi G, Chen HG, BaMC et al (2010) Up-regulation of PIK3CA promotes metastasis in gastric carcinoma.World J Gastroenterol 16:4986–4991
39. Cinti C, Vindigni C, Zamparelli A, La Sala D, Epistolato MC,Marrelli D et al (2008) Activated Akt as an indicator of prognosisin gastric cancer. Virchows Arch 453:449–455
40. Morgensztern D, McLeod HL (2005) PI3K/Akt/mTOR pathway as atarget for cancer therapy. Anticancer Drugs 16:797–803
41. Murayama T, Inokuchi M, Takagi Y, Yamada H, Kojima K,Kumagai J et al (2009) Relation between outcomes andlocalisation of p-mTOR expression in gastric cancer. Br J Cancer100:782–788
42. Xiao L, Wang YC, Li WS, Du Y (2009) The role of mTOR andphospho-p70S6K in pathogenesis and progression of gastric carcino-mas: an immunohistochemical study on tissue microarray. J Exp ClinCancer Res 28:152
43. Ye B, Jiang LL, Xu HT, Zhou DW, Li ZS (2012) Expression ofPI3K/AKT pathway in gastric cancer and its blockade suppressestumor growth and metastasis. Int J Immunopathol Pharmacol 25(3):627–636
44. Wen YG, Wang Q, Zhou CZ, Qiu GQ, Peng ZH, Tang HM (2010)Mutation analysis of tumor suppressor gene PTEN in patients withgastric carcinomas and its impact on PI3K/AKT pathway. Oncol Rep24:89–95
45. Dreesen O, Brivanlou AH (2007) Signaling pathways in cancer andembryonic stem cells. Stem Cell Rev 3:7–17
46. Kang YH, Lee HS, Kim WH (2002) Promoter methylation andsilencing of PTEN in gastric carcinoma. Lab Invest 82:285–291
47. Lang SA, Gaumann A, Koehl GR, Seidel U, Bataille F, Klein D, EllisLM, Bolder U, Hofstaedter F et al (2007) Mammalian target ofrapamycin is activated in human gastric cancer and serves as a targetfor therapy in an experimental model. Int J Cancer 120:1803–1810
48. Sun DF, Zhang YJ, Tian XQ, Chen YX, Fang JY (2013) Inhibition ofmTOR signalling potentiates the effects of trichostatin A in human
32 Virchows Arch (2014) 465:25–33

gastric cancer cell lines by promoting histone acetylation. Cell BiolInt. doi:10.1002/cbin.10179
49. Yang HY, Xue LY, Xing LX, Wang J, Wang JL (2013) Putative roleof the mTOR/4E-BP1 signaling pathway in the carcinogenesis andprogression of gastric cardiac adenocarcinoma. Mol Med Rep 7(2):537–542
50. Fan S, Ramalingam SS, Kauh J, Xu Z, Khuri FR, Sun SY (2009)Phosphorylated eukaryotic translation initiation factor 4 (eIF4E) iselevated in human cancer tissues. Cancer Biol Ther 8(15):1463–1469
51. Chen CN, Hsieh FJ, Cheng YM, Lee PH, Chang KJ (2004)Expression of eukaryotic initiation factor 4E in gastric
adenocarcinoma and its association with clinical outcome. J SurgOncol 86:22–27
52. Liang S, Guo R, Zhang Z, Liu D, Xu H, Xu Z, Wang X, Yang L(2013) Upregulation of the eIF4E signaling pathway contributes tothe progression of gastric cancer, and targeting eIF4E by perifosineinhibits cell growth. Oncol Rep 29(6):2422–2430
53. Yap TA, Garrett MD, Walton MI, Florence Raynaud F, de Bono FS,Workman P (2008) Targeting the PI3K–AKT–mTOR pathway: prog-ress, pitfalls, and promises. Curr Opin Pharmacol 8:393–412
54. Fruman DA, Rommel CR (2014) PI3K and cancer: lessons, chal-lenges and opportunities. Nat Rev Drug Discov 13:140–156
Virchows Arch (2014) 465:25–33 33