liver transplantation for chronic viral hepatitis
TRANSCRIPT

PROGRESS IN TRANSPLANTATION
Chronic Viral Hepatit is Teresa L. Wright * and Brian Pereiva t
epatotropic viruses, specifically hepatitis B vi- H rus (HBV), and hepatitis C virus (HCV) are common causes of end-stage liver disease, necessitat- ing liver transplantation, and important causes of morbidity and mortality in the posttransplantation period. Both viruses recur uniformly in patients with pretransplant infection, and therapeutic strategies aimed at preventing recurrence have, until recently, been largely ineffectual. Advancing methods for diag- nosis of these viruses, in particular, sensitive serologi- cal assays developed since identification of HCV in 1989. and accurate virological assays such as branched DNA assay @-DNA) and polymerase chain reaction (PCR) amplification of viral genome, have resulted in a rapid expansion of our knowledge of these impor- tant pathogens. Treatment is limited by the small number of effective drugs available, but new antiviral agents are under development. Finally, study of the host immune response has provided insight into pathogenesis of liver damage associated with viral infections. This review will examine the prevalence of hepatitis viruses in patients undergoing liver trans- plantation, consequences of posttransplantation re- currence, methods for diagnosis of disease, and strategies aimed at preventing and treating these infections.
Hepatitis B Infection Natural History
The largest experience evaluating the natural history of HBV infection in patients undergoing liver trans- plantation without preventative therapy comes from the University of Pittsburgh, Pittsburgh, PA (1). Outcome of 51 patients with chronic infection was compared with that of 38 patients with evidence of HBV immunity. Early posttransplantation survival
Liver Transplantation for
30 Liver Transphntution and Surgq, Vo[ 1, No 1 (January), 1995: pp 30-42
~~
From the Department of Veterans Aflairs Medical Center and the University of California, San Fruncisco, CA*, and the New England Medical Center, Boston, MAt
Address reprint request5 to Teresa L Wright, MD, Gartroenterol- ogy Unit I I I B , Veteran5 Adrnmctrahon Medical Center, 4150 Clement St, Sun Francisco, CA 94121
1074-3022/95/0101-000683 OOiO
was comparable in the hepatitus B surface antigen (HBsAg)-positive and HBsAg-negative groups, but survival after 60 days was significantly lower in HBV-infected than HBV-immune patients (45.1% and 63.2%, respectively). HBV infection (defined as HBsAg-positive in serum) recurred in 82% of patients surviving at least 60 days and was the leading cause of delayed death (73% of all deaths after 60 days).
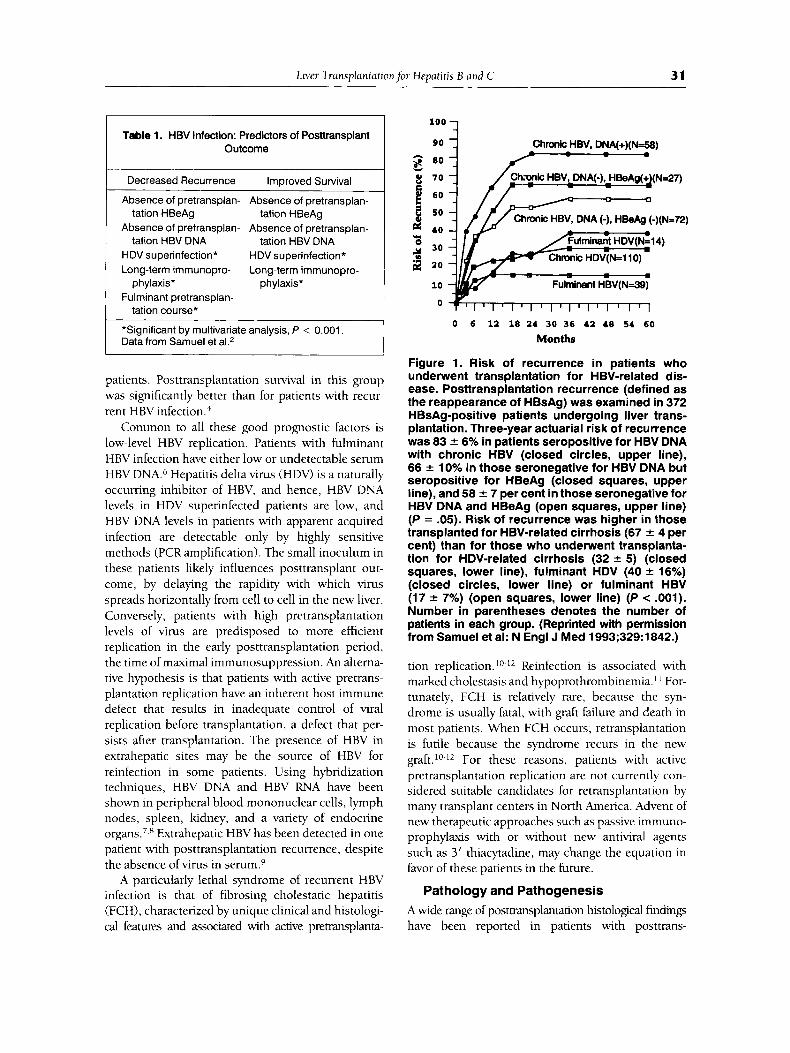
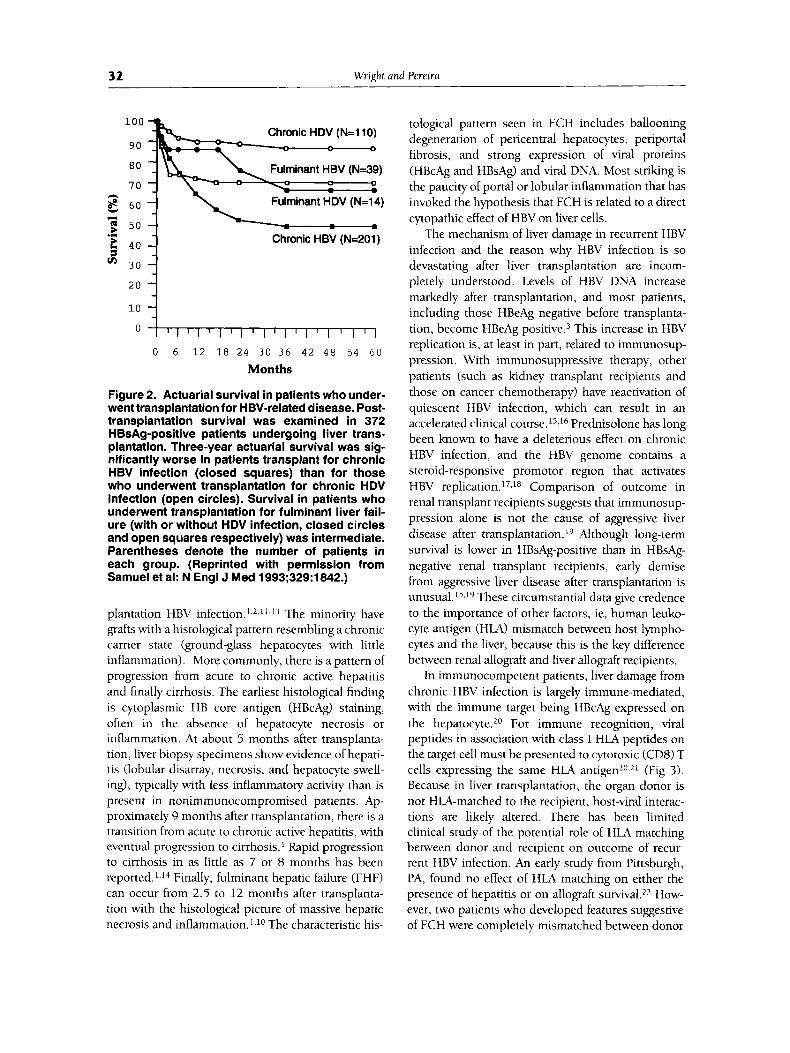
Information regarding pretransplantation vari- ables predictive of posttransplantation outcome comes from a variety of sources (Table 1),1-5 An initial small series, suggested, although did not prove, that pa- tients without active pretransplantation replication were at lower risk of HBV recurrence and graft loss than those with active replicati~n.~ A more recent large study from 17 European centers strongly sup- ported the prognostic importance of pretransplanta- tion replicative ~ t a t e . ~ In 372 patients who received transplants for acute or chronic HBV infection, the overall risk of recurrence was 40% and SO%, respec- tively, at 1 year and 3 years after transplantation. In those with HBV-related cirrhosis, recurrence was higher in those seropositive for HBV DNA at the time of transplantation (83%) than it was in those patients negative for both HBV DNA and hepatitis B e antigen (HBeAg) (58%) (Fig l).5 Risk of recurrence was lowest in patients who received transplants for fulminant hepatitis (with or without HDV coinfec- tion), and in patients with chropic HDV infection (Fig 1). Overall survival at 1 and 3 years after transplantation was 75% and 63%, respectively.5 The %year survival rate was significantly better in patients who received transplants for chronic HDV (83%) than for those who received transplants for chronic HBV infection (44%) (Fig 2 ) . The 3-year survival was worse in patients with HBV recurrence (54%) than those who remained HBsAg-negative (83%). The natural history of HBV infection apparently acquired with liver transplantation seems more benign than that of patients with overt pretransplantation HBV infection.' Of 207 HBsAg-negative patients before liver transplantation, 20 (10%) became HBsAg posi- tive. Using molecular techniques, occult pretransplan- tation infection was identified in 5 patients and occult infection from the donor was identified in 2
Liver Transplantationfor Hepatitis B and C 31
Table 1. HBV Infection: Predictors of Posttransplant Outcome
Decreased Recurrence Improved Survival
Absence of pretransplan- Absence of pretransplan-
Absence of pretransplan- Absence of pretransplan-
HDV superinfection* HDV superinfection* Long-term irnmunopro- Long-term imrnunopro-
tation HBeAg tation HBeAg
tation HBV DNA
phylaxis* phylaxis* I tation HBV DNA
Fulrninant pretransplan- tation course*
*Significant by multivariate analysis, P < 0.001. Data from Samuel et aL2
patients. Posttransplantation survival in this group was significantly better than for patients with recur- rent HBV infection.'
Common to all these good prognostic factors is low-level HBV replication. Patients with fulminant HBV infection have either low or undetectable serum HBV DNA.6 Hepatitis delta virus (HDV) is a naturally occumng inhibitor of HBV, and hence, HBV DNA levels in HDV superinfected patients are low, and HBV DNA levels in patients with apparent acquired infection are detectable only by highly sensitive methods (PCR amplification). The small inoculum in these patients likely influences posttransplant out- come, by delaying the rapidity with which virus spreads horizontally from cell to cell in the new liver. Conversely, patients with high pretransplantation levels of virus are predisposed to more efficient replication in the early posttransplantation period, the time of maximal immunosuppression. An altema- tive hypothesis is that patients with active pretrans- plantation replication have an inherent host immune defect that results in inadequate control of viral replication before transplantation, a defect that per- sists after transplantation. The presence of HBV in extrahepatic sites may be the source of HBV for reinfection in some patients. Using hybridization techniques, HBV DNA and HBV RNA have been shown in peripheral blood mononuclear cells, lymph nodes, spleen, kidney, and a variety of endocrine
Extrahepatic HBV has been detected in one patient with posttransplantation recurrence, despite the absence of virus in serum.9
A particularly lethal syndrome of recurrent HBV infection is that of fibrosing cholestatic hepatitis (FCH), characterized by unique clinical and histologi- cal features and associated with active pretransplanta-
Chmk HBV, DNA(+)(N=58)
g 7 0
E 6o
$ 50 pc 40
30 Y * 2 ao
10
Q
0 6 11 18 24 30 36 42 48 54 60
Months
Figure 1. Risk of recurrence in patients who underwent transplantation for HBV-related dis- ease. Posttransplantation recurrence (defined as the reappearance of HBsAg) was examined in 372 HBsAg-positive patients undergoing liver trans- plantation. Three-year actuarial risk of recurrence was 83 f 6% in patients seropositive for HBV DNA with chronic HBV (closed circles, upper line), 66 f 10% in those seronegative for HBV DNA but seropositive for HBeAg (closed squares, upper line), and 58 f 7 per cent in those seronegative for HBV DNA and HBeAg (open squares, upper line) (P = .05). Risk of recurrence was higher in those transplanted for HBV-related cirrhosis (67 f 4 per cent) than for those who underwent transplanta- tion for HDV-related cirrhosis (32 f 5) (closed squares, lower line), fulminant HDV (40 f 16%) (closed circles, lower line) or fulminant HBV (17 f 7%) (open squares, lower line) (P < .001). Number in parentheses denotes the number of patients in each group. (Reprinted with permission from Samuel et al: N Engl J Med 1993;329:1842.)
tion replication. Reinfection is associated with marked cholestasis and hypoprothrombinemia." For- tunately, FCH is relatively rare, because the syn- drome is usually fatal, with graft failure and death in most patients. When FCH occurs, retransplantation is futile because the syndrome recurs in the new graft.10-12 For these reasons, patients with active pretransplantation replication are not currently con- sidered suitable candidates for retransplantation by many transplant centers in North America. Advent of new therapeutic approaches such as passive immuno- prophylaxis with or without new antiviral agents such as 3' thiacytadine, may change the equation in favor of these patients in the future.
Pathology and Pathogenesis A wide range of posttransplantation histological findings have been reported in patients with posttrans-
32 Wright and Pereira
100 Chronic HDV (N=llO)
9 0 - - - - - 0
Fulminant HBV (N=39)
Fulminant HDV (N=14) n
'E 40 4 1
\ Chronic HBV (N=201)
10 ::: 0 0 6 12 18 24 30 36 42 48 54 60
Months
Figure 2. Actuarial survival in patients who under- went transplantation for HBV-related disease. Post- transplantation survival was examined in 372 HBsAg-positive patients undergoing liver trans- plantation. Three-year actuarial survival was sig- nificantly worse in patients transplant for chronic HBV infection (closed squares) than for those who underwent transplantation for chronic HDV infection (open circles). Survival in patients who underwent transplantation for fulminant liver fail- ure (with or without HDV infection, closed circles and open squares respectively) was intermediate. Parentheses denote the number of patients in each group. (Reprinted with permission from Samuel et al: N Engl J Med 1993;329:1842.)
plantation HBV infection. L*J l- I3 The minority have grafts with a histological pattern resembling a chronic carrier state (ground-glass hepatocytes with little inflammation). More commonly, there is a pattern of progression from acute to chronic active hepatitis and finally cirrhosis. The earliest histological finding is cytoplasmic HB core antigen (HBcAg) staining, often in the absence of hepatocyte necrosis or inflammation. At about 5 months after transplanta- tion, liver biopsy specimens show evidence of hepati- tis (lobular disarray, necrosis, and hepatocyte swell- ing), typically with less inflammatory activity than is present in nonimmunocompromised patients. Ap- proximately 9 months after transplantation, there is a transition from acute to chronic active hepatitis, with eventual progression to cirrhosis. Rapid progression to cirrhosis in as little as 7 or 8 months has been reported. Finally, fulminant hepatic failure (FHF) can occur from 2.5 to 12 months after transplanta- tion with the histological picture of massive hepatic necrosis and inflammation. ] , lo The characteristic his-
tological pattern seen in FCH includes ballooning degeneration of pericentral hepatocytes, periportal fibrosis, and strong expression of viral proteins (HBcAg and HBsAg) and viral DNA. Most striking is the paucity of portal or lobular inflammation that has invoked the hypothesis that FCH is related to a direct cytopathic effect of HBV on liver cells.
The mechanism of liver damage in recurrent HBV infection and the reason why HBV infection is so devastating after liver transplantation are incom- pletely understood. Levels of HBV DNA increase markedly after transplantation, and most patients, including those HBeAg negative before transplanta- tion, become HBeAg p~s i t ive .~ This increase in HBV replication is, at least in part, related to immunosup- pression. With immunosuppressive therapy, other patients (such as kidney transplant recipients and those on cancer chemotherapy) have reactivation of quiescent HBV infection, which can result in an accelerated clinical course. I5.l6 Prednisolone has long been known to have a deleterious effect on chronic HBV infection, and the HBV genome contains a steroid-responsive promotor region that activates HBV replication. 17,18 Comparison of outcome in renal transplant recipients suggests that immunosup- pression alone is not the cause of aggressive liver disease after transplantation. l9 Although long-term survival is lower in HBsAg-positive than in HBsAg- negative renal transplant recipients, early demise from aggressive liver disease after transplantation is unusual. I5,l9 These circumstantial data give credence to the importance of other factors, ie, human leuko- cyte antigen (HLA) mismatch between host lympho- cytes and the liver, because this is the key difference between renal allograft and liver allograft recipients.
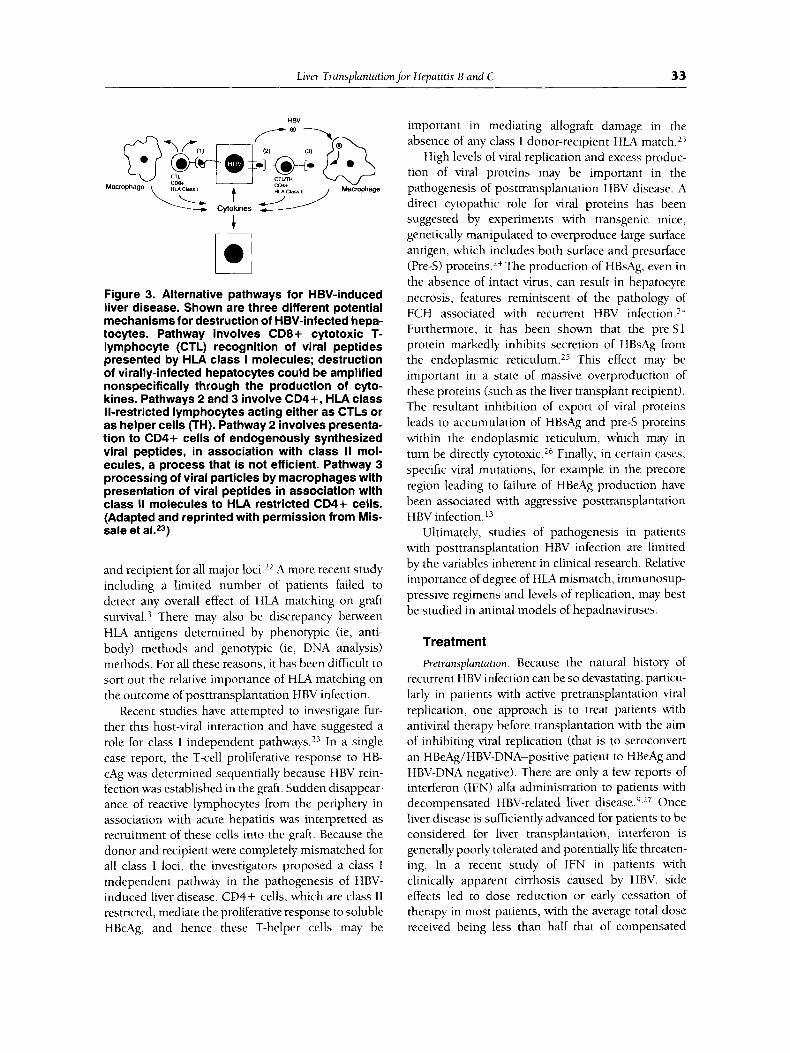
In immunocompetent patients, liver damage from chronic HBV infection is largely immune-mediated, with the immune target being HBcAg expressed on the hepatocyte.20 For immune recognition, viral peptides in association with class I HLA peptides on the target cell must be presented to cytotoxic (CD8) T cells expressing the same HLA antigen20,21 (Fig 3) . Because in liver transplantation, the organ donor is not HLA-matched to the recipient, host-viral interac- tions are likely altered. There has been limited clinical study of the potential role of HLA matching between donor and recipient on outcome of recur- rent HBV infection. An early study from Pittsburgh, PA, found no effect of HLA matching on either the presence of hepatitis or on allograft survival.22 How- ever, two patients who developed features suggestive of FCH were completely mismatched between donor
Liver Transplantationfor Hepatitis B and C 33
HBV -El ------
4
cil Figure 3. Alternative pathways for HBV-induced liver disease. Shown are three different potential mechanisms for destruction of HBV-infected hepa- tocytes. Pathway involves CD8+ cytotoxic T- lymphocyte (CTL) recognition of viral peptides presented by HLA class I molecules; destruction of virally-infected hepatocytes could be amplified nonspecifically through the production of cyto- kines. Pathways 2 and 3 involve CD4+, HLA class Il-restricted lymphocytes acting either as CTLs or as helper cells (TH). Pathway 2 involves presenta- tion to CD4+ cells of endogenously synthesized viral peptides, in association with class II mol- ecules, a process that is not efficient. Pathway 3 processing of viral particles by macrophages with presentation of viral peptides in association with class II molecules to HLA restricted CD4+ cells. (Adapted and reprinted with permission from Mis- sale et aLZ3)
and recipient for all major loci.L2 A more recent study including a limited number of patients failed to detect any overall effect of HLA matching on graft ~urvival.~ There may also be discrepancy between HLA antigens determined by phenotypic (ie, anti- body) methods and genotypic (ie, DNA analysis) methods. For all these reasons, it has been difficult to sort out the relative importance of HLA matching on the outcome of posttransplantation HBV infection.
Recent studies have attempted to investigate fur- ther this host-viral interaction and have suggested a role for class 1 independent pathways.13 In a single case report, the T-cell proliferative response to HB- cAg was determined sequentially because HBV rein- fection was established in the graft. Sudden disappear- ance of reactive lymphocytes from the periphery in association with acute hepatitis was interpretted as recruitment of these cells into the graft. Because the donor and recipient were completely mismatched for all class I loci, the investigators proposed a class I independent pathway in the pathogenesis of HBV- induced liver disease. CD4+ cells, which are class I1 restricted, mediate the proliferative response to soluble HBcAg, and hence these T-helper cells may be
important in mediating allograft damage in the absence of any class I donor-recipient HLA match.23
High levels of viral replication and excess produc- tion of viral proteins may be important in the pathogenesis of posttransplantation HBV disease. A direct cytopathic role for viral proteins has been suggested by experiments with transgenic mice, genetically manipulated to overproduce large surface antigen, which includes both surface and presurface (Pre-S) ~ r 0 t e i n s . l ~ The production of HBsAg, even in the absence of intact virus, can result in hepatocyte necrosis, features reminiscent of the pathology of FCH associated with recurrent HBV infection.24 Furthermore, it has been shown that the pre-S1 protein markedly inhibits secretion of HBsAg from the endoplasmic reticulum.25 This effect may be important in a state of massive overproduction of these proteins (such as the liver transplant recipient). The resultant inhibition of export of viral proteins leads to accumulation of HBsAg and pre-S proteins within the endoplasmic reticulum, which may in turn be directly cytotoxic.26 Finally, in certain cases, specific viral mutations, for example in the precore region leading to failure of HBeAg production have been associated with aggressive posttransplantation HBV infe~ti0n.l~
Ultimately, studies of pathogenesis in patients with posttransplantation HBV infection are limited by the variables inherent in clinical research. Relative importance of degree of HLA mismatch, immunosup- pressive regimens and levels of replication, may best be studied in animal models of hepadnaviruses.
Treatment Pretransplantation. Because the natural history of
recurrent HBV infection can be so devastating, particu- larly in patients with active pretransplantation viral replication, one approach is to treat patients with antiviral therapy before transplantation with the aim of inhibiting viral replication (that is to seroconvert an HBeAg/HBV-DNA-positive patient to HBeAg and HBV-DNA negative). There are only a few reports of interferon (IFN) alfa administration to patients with decompensated HBV-related liver di~ease.~J ' Once liver disease is sufficiently advanced for patients to be considered for liver transplantation, interferon is generally poorly tolerated and potentially life threaten- ing. In a recent study of IFN in patients with clinically apparent cirrhosis caused by HBV, side effects led to dose reduction or early cessation of therapy in most patients, with the average total dose received being less than half that of compensated
34 Wright and Pereira -
patients.28 Despite this limitation, a sustained loss of HBV DNA was seen in 33%, associated with improve- ment in synthetic function.28 A second study com- pared survival and reinfection rates of 22 patients with HBV infection treated with interferon awaiting liver transplantation, with survival and reinfection rates of 26 HBV-infected patients who received transplants without prior IFN therapy.19 Patients in both groups received prophylactic anti-HBslg therapy (see below). IFN effectively inhibited HBV replica- tion in the majority of treated patients (although most still had detectable HBV DNA by PCR).29 Absolute inhibition, ie, the absence of HBV DNA by PCR in serum, was associated with viral clearance. However, rate of posttransplantation HBV infection, time to reinfection, and survival rates were not significantly improved in IFN-pretreated patients.29 The number of patients in this study was small and the control group retrospective. Although prelimi- nary, treatment of patients with partially compen- sated HBV liver disease may result in inhibition of viral replication, which may in turn be critical to their candidacy for transplantation. IFN therapy should be undertaken with extreme caution in marginally com- pensated patients because of potentially life threaten- ing complications, eg, infections and exacerbations of liver disease).28 From these studies, absence of viral replication appears to be associated with post- transplantation viral clearance, and if this is attain- able (by IFN or any other antiviral therapy), reinfec- tion will likely be reduced.29 Partial inhibition (HBV DNA negative by dot-blot hybridization assays, but positive by PCR) is probably insufficient, because long-term clinical outcomes (survival, etc) are unaf- fected. Thus the goal of pretransplantation antiviral therapy should be complete eradication of HBV, a goal that is rarely attainable with current therapies.
Immunoprophylaxis. The most effective approach to prevent recurrent HBV has been the use of high dose anti-HBsIg in the penoperative and postoperative period^.^,^^ The goal of this passive immunoprophy- laxis is to neutralize circulating HBV particles and avoid reinfection of the graft. Early studies of low- dose anti-HBsIg used only in the immediate periop- erative period failed to show benefit.30 Results with higher doses, both penoperatively and for 6 months postoperatively, suggested that HBV recurrence was delayed, particularly in patients without active pre- transplantation viral rep l i~a t ion .~~ Standard protocol for HBV prevention is 10,000 IU intravenously during the anhepatic phase and then daily for the first 6 days after surgery. Dosing is repeated whenever
100
90
8 80
i! 50 d w 40
+j 30 0 i::l 2 20
No immunoprophylaxis (N=67)
Short-term therapy (N=83) h lo 0 -
0 6 12 18 24 30 36 42 48 54 60 Months
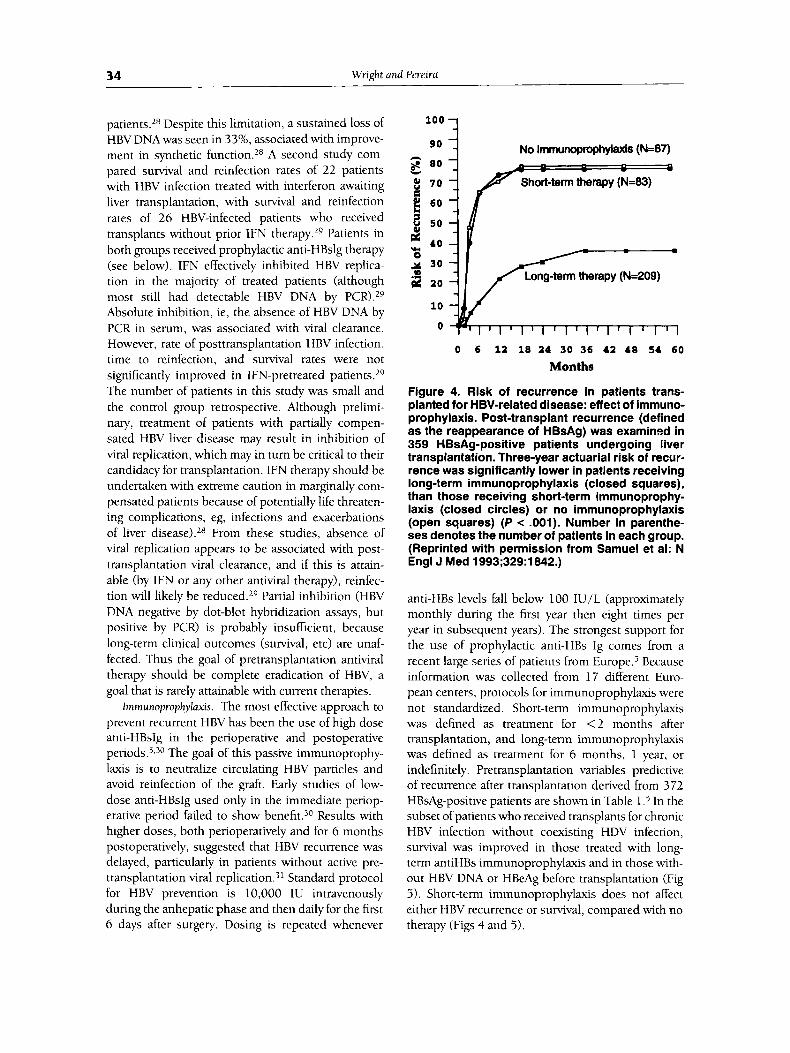
Figure 4. Risk of recurrence in patients trans- planted for HBV-related disease: effect of immuno- prophylaxis. Post-transplant recurrence (defined as the reappearance of HBsAg) was examined in 359 HBsAg-positive patients undergoing liver transplantation. Three-year actuarial risk of recur- rence was significantly lower in patients receiving long-term immunoprophylaxis (closed squares), than those receiving short-term immunoprophy- laxis (closed circles) or no immunoprophylaxis (open squares) (P < .001). Number in parenthe- ses denotes the number of patients in each group. (Reprinted with permission from Samuel et al: N Engl J Med 1993;329:1842.)
anti-HBs levels fall below 100 IU/L (approximately monthly during the first year then eight times per year in subsequent years). The strongest support for the use of prophylactic anti-HBs Ig comes from a recent large series of patients from E ~ r o p e . ~ Because information was collected from 17 different Euro- pean centers, protocols for immunoprophylaxis were not standardized. Short-term immunoprophylaxis was defined as treatment for < 2 months after transplantation, and long-term immunoprophylaxis was defined as treatment for 6 months, 1 year, or indefinitely. Pretransplantation variables predictive of recurrence after transplantation derived from 372 HBsAg-positive patients are shown in Table 1 . 5 In the subset of patients who received transplants for chronic HBV infection without coexisting HDV infection, survival was improved in those treated with long- term antiHBs immunoprophylaxis and in those with- out HBV DNA or HBeAg before transplantation (Fig 5). Short-term immunoprophylaxis does not affect either HBV recurrence or survival, compared with no therapy (Figs 4 and 5).
Liver Transplantationfor Hepatitis 8 and C 35
1 0 0 n
8 0
No irnrnunoprophylaxis (N=67) .-( 6 50
'E 4 0 4 Short-term therapy (N=83)
~ : ~ 1 1 , 1 , 1 1 1 1 , 1 1 1 1 1 1 I 1 1 ,
0
0 6 1 2 18 2 4 3 0 3 6 4 2 4 8 5 4 60
Months
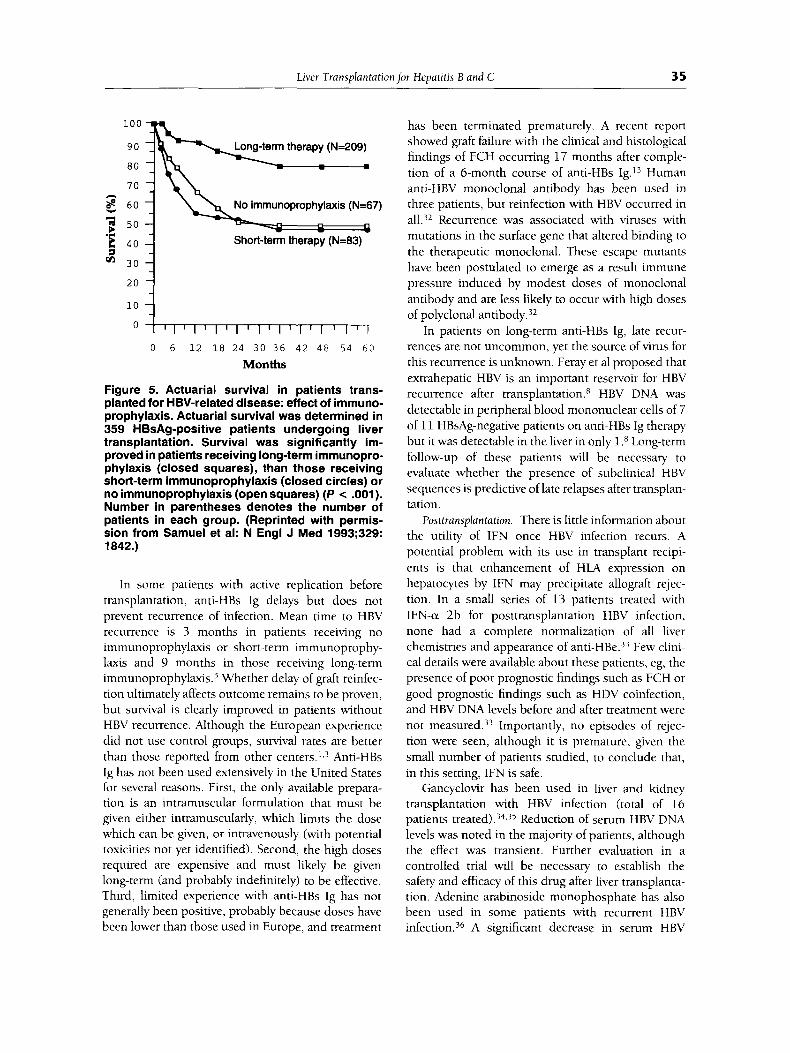
Figure 5. Actuarial survival in patients trans- planted for HBV-related disease: effect of immuno- prophylaxis. Actuarial survival was determined in 359 HBsAg-positive patients undergoing liver transplantation. Survival was significantly im- proved in patients receiving long-term immunopro- phylaxis (closed squares), than those receiving short-term immunoprophylaxis (closed circles) or no immunoprophylaxis (open squares) (P c .001). Number in parentheses denotes the number of patients in each group. (Reprinted with permis- sion from Samuel et al: N Engl J Med 1993;329: 1842.)
In some patients with active replication before transplantation, anti-HBs Ig delays but does not prevent recurrence of infection. Mean time to HBV recurrence is 3 months in patients receiving no immunoprophylaxis or short-term immunoprophy- laxis and 9 months in those receiving long-term immun~prophylaxis.~ Whether delay of graft reinfec- tion ultimately affects outcome remains to be proven, but survival is clearly improved in patients without HBV recurrence. Although the European experience did not use control groups, survival rates are better than those reported from other Anti-HBs Ig has not been used extensively in the United States for several reasons. First, the only available prepara- tion is an intramuscular formulation that must be given either intramuscularly, which limits the dose which can be given, or intravenously (with potential toxicities not yet identified). Second, the high doses required are expensive and must likely be given long-term (and probably indefinitely) to be effective. Third, limited experience with anti-HBs Ig has not generally been positive, probably because doses have been lower than those used in Europe, and treatment
has been terminated prematurely. A recent report showed graft failure with the clinical and histological findings of FCH occuning 17 months after comple- tion of a 6-month course of anti-HBs Ig.I3 Human anti-HBV monoclonal antibody has been used in three patients, but reinfection with HBV occurred in all.32 Recurrence was associated with viruses with mutations in the surface gene that altered binding to the therapeutic monoclonal. These escape mutants have been postulated to emerge as a result immune pressure induced by modest doses of monoclonal antibody and are less likely to occur with high doses of polyclonal antibody.32
In patients on long-term anti-HBs Ig, late recur- rences are not uncommon, yet the source of virus for this recurrence is unknown. Feray et a1 proposed that extrahepatic HBV is an important reservoir for HBV recurrence after transplantation.R HBV DNA was detectable in peripheral blood mononuclear cells of 7 of 11 HBsAg-negative patients on anti-HBs Ig therapy but it was detectable in the liver in only 1 .x Long-term follow-up of these patients will be necessary to evaluate whether the presence of subclinical HBV sequences is predictive of late relapses after transplan- tation.
Posttransplantation. There is little information about the utility of IFN once HBV infection recurs. A potential problem with its use in transplant recipi- ents is that enhancement of HLA expression on hepatocytes by IFN may precipitate allograft rejec- tion. In a small series of 13 patients treated with IFN-or 2b for posttransplantation HBV infection, none had a complete normalization of all liver chemistries and appearance of anti-HBe.33 Few clini- cal details were available about these patients, eg, the presence of poor prognostic findings such as FCH or good prognostic findings such as HDV coinfection, and HBV DNA levels before and after treatment were not mea~ured.)~ Importantly, no episodes of rejec- tion were seen, although it is premature, given the small number of patients studied, to conclude that, in this setting, IFN is safe.
Gancyclovir has been used in liver and kidney transplantation with HBV infection (total of 16 patients treated) .34,35 Reduction of serum HBV DNA levels was noted in the majority of patients, although the effect was transient. Further evaluation in a controlled trial will be necessary to establish the safety and efficacy of this drug after liver transplanta- tion. Adenine arabinoside monophosphate has also been used in some patients with recurrent HBV infe~tion.)~ A significant decrease in serum HBV

36 Wright and Pereiva
DNA and alanine transaminase (ALT) levels was observed, but the antiviral effect was incomplete or transient in seven of the eight treated patients.
In summary, the threat of recurrent infection and death from liver failure is ever present in patients undergoing liver transplantation for chronic HBV infection. Identification of pretransplantation predic- tors of outcome after transplantation will aid in selection of patients more likely to benefit from liver transplantation. This information, in conjunction with passive immunoprophylaxis, more effective anti- viral agents, and greater understanding of the effects of specific immunosuppressives on HBV replication, may result in improved survival in this patient population. Retransplantation has been performed in patients with graft failure from HBV recurrence, but in the absence of specific therapy to prevent reinfec- tion, HBV recurrence is the rule.' In a large European study, 19 patients underwent retransplantation for HBV disease, but two thirds of these patients died of either perioperative complications or further infec- tion.* However, little information is available with regard to rigorous use of immunoprophylaxis in this setting. Ethical issues regarding the use of limited donor organs in patients with reduced long-term survival need to be addressed but will be difficult to resolve.
Hepatitis D Infection Natural History
There is now convincing evidence that patients with chronic HDV infection are at lower risk for HBV recurrence after liver transplantation, and that if reinfection does occur, the disease is less devastating than it is in patients with HBV infection alone.3.5J2,37.38 One of the earliest reports came from Italy, where HDV is endemic.37 Of seven patients with chronic HDV, two patients cleared their infection, whereas in five, HDV recurred, three with hepatitis. A subse- quent report from the same group described the outcome in 27 patients with HDV cirrhosis.37 Anti- HBs Ig prophylaxis was not used consistently. Only 2 patients died of HBV HDV coinfection after transplan- tation. Overall survival was 78%, and both HBV and HDV were cleared in 18%. Of 21 patients who survived the early posttransplantation period, HDV infection recurred in 76%, the majority with simuta- neous HBV infection. Interestingly, HDV infection recurred before any signs of HBV reactivation in many patients, and histological hepatitis was present only in patients with recurrent HBV infection but not
in patients with HDV infection alone. The largest reported experience of HDV infection and liver transplantation again comes from Europe.5 One hundred ten patients underwent transplantation for chronic infection and 14 for fulminant infection, with and without passive immunoprophylaxis (see above). Three-year actuarial risk of recurrence was 32% and 40% in patients with HDV-related cirrhosis and fulminant HDV, respectively (Fig 1).
The reported experience from centers in the United States has been limited. Lucey et a1 described the outcome of 15 patients who underwent liver transplantation for HBV infection with or without simultaneous HDV infection. l2 Graft reinfection oc- curred in 8 of 10 patients with HBV infection alone, and in 4 of 5 with both HBV and HDV. Five patients in the former group died of liver failure related to recurrent infection, although all five patients with both HBV and HDV infection were alive, despite recurrence in four. Decreased recurrence rates and improved survival in HDV-cirrhosis are likely second- ary to inhibitory effects of HDV on HBV repl i~a t ion .~~ Low pretransplantation HBV DNA levels result in decreased risk of recurrence, and low posttransplan- tation levels result in attenuated posttransplantation d i ~ e a s e . ~ , ' ~
Pathology and Pathogenesis
Two distinct pathological findings have been de- scribed in posttransplantation HDV infection40: (1) typical findings of recurrence, with inflammatory changes on liver biopsy specimen and active HBV replication (HBV DNA in serum and HBcAg expres- sion in hepatocytes); and (2) Atypical histological findings with hepatocyte necrosis in the absence of inflammation on liver biopsy, without evidence of active replication. Subclinical HDV recurrence is common, suggesting that HDV alone is not cyto- pathic to liver cells and that disease only becomes apparent when HBV infection recurs.38 These studies provide clinical support for in vitro findings of HDV replication but not production of infectious particles in the absence of HBV infection.39
Treatment The best information about decreased recurrence rates and improved survival with long-term immuno- prophylaxis comes from Samuel et a1 (Figs 1 and 2).5 In patients with chronic HDV infection, the 3-year risk of recurrence was significantly reduced in pa- tients receiving long-term immunoprophylaxis (1 7%) as compared with the risk of those receiving short-

Liver Transplantation for Hepatitis B and C 37
term immunoprophylaxis (56%) and those receiving no therapy (70%). HDV superinfection is only one of three independent risk factors (Table 1) (relative risk 3.92). Deaths from recurrence of HBV were rare in patients transplanted for chronic HDV infection (2 of 110, or 2.7%). Of those who remained HBsAg negative, serum HDV RNA and/or liver HDAg were no longer detectable at 4 years after tran~plantation.~~ There is little known about the use of IFN once HDV infection recurs. In nonimmunocompromised pa- tients, IFN-a 2a at doses of 9 million units three times weekly, can normalize serum ALT levels and inhibit HDV replication in 50% of patients.42 How- ever, the benefit is transient in most patients, and relapse is common when treatment is stopped. Preliminary data suggest that IFN can reduce HDV replication in reinfected liver grafts.43
Hepatitis C Infection Hepatitis C virus (HCV) is important to the liver transplant recipient for several reasons. Chronic HCV infection is a frequent cause of end-stage liver disease in North America and Europe and is present in 25% to 40% of patients undergoing liver transplantation. Recurrence of HCV after liver transplantation is almost universal, and thus, many liver transplant recipients with and without overt hepatitis are vire- mi^.^^ HCV infection in the organ donor and/or present in the blood transfused in the peritransplant period make acquisition of HCV a possibility. Diag- nostic tests developed within the past few years have enabled the clinician to study the natural history of HCV before transplantation, assess the prevalence of disease in patients undergoing transplantation, and examine the consequences of HCV infection in the period after transplantation.
Natural History Pretransplantation. After transfusion of HCV-in-
fected blood or after acute, community-acquired HCV infection, infection persists in approximately 80% of recipient^.^^ Commonly, the initial disease is subclinical, and the consequences of infection are not apparent for many years. Although the natural history of chronic HCV infection is not well defined, evaluation of blood transfusion recipients suggested that those who develop hepatitis after transfusion have only a slightly increased long-term risk of liver-related deaths (mean follow-up of 17 years) and no overall increased mortality compared with control cohorts who did not develop hepatitis after transfu-
~ i o n . ~ ~ The slowly progressive nature of this disease is apparent from a retrospective study of HCV patients who had a prior parenteral exposure (blood transfu- sion) in which mean time to development of chronic hepatitis, cirrhosis, and hepatocellular carcinoma was 10, 21, and 29 years, re~pectively.~’ Unfortu- nately, the natural history of HCV infection and predictors of poor prognosis are not as well defined as those for other causes of liver disease, eg, primary biliary cirrhosis, so that the timing of liver transplan- tation in these patients is more problematic. Trans- plantation should be considered in patients with cirrhosis and biochemical evidence of deteriorating synthetic function and/or complications of portal hypertension.
Posttransplantation. As in patients with chronic HBV infection undergoing liver transplantation, the major- ity of patients with HCV infection are viremic, and hence susceptible to recurrent disease. The first report of recurrence of HCV after transplantation was in six anti-HCV-positive patients, five of whom remained positive at 1 year after transplantation and two of whom developed clinical and histological evidence of hepatitis.48 In one of these two patients, HCV infection resulted in graft failure and retransplan- tation. Subsequent clinical and virological studies have elucidated the issue of recurrent disease. Essen- tial to these studies has been the development of accurate methods of diagnosis of both pretransplanta- tion and posttransplantation infection. Because sero- logical assays underestimate HCV infection in this immunosuppressed population, it is important to distinguish studies in which infection is identified by antibody tests from those in which RNA assays are used. Using first-generation anti-HCV tests, an appar- ent acquisition rate of HCV infection with liver transplantation was surprisingly high (35%) ,44 but the rate fell to 16% when pretransplantation samples were tested by second-generation anti-HCV assays and HCV PCR, because first-generation tests errone- ously ascribed patients to a group of “acquired” infection who had instead reactivated infection. Rate of acquisition by patients who received transplants subsequent to routine screening of blood products for HCV is very low (2.5°h).49 A recent study has shown that antibody titers to the HCV core region fall relative to other antibody titers, eg, anti-rotavims antibodies, in patients on immunosuppression follow- ing liver tran~plantation.~~ Fall in antibody titer to certain viral antigens (C1003 and C33C) or complete loss of reactivity has been noted in other immunosup- pressed patients (kidney and bone marrow trans-

38 Wright and Pereira
plant recipients), whereas reactivity to other anti- bodies (C25, N e l and e2) are less affected.51 Incorporation of these antigens into new HCV assays would improve diagnosis of HCV infection in these patient groups.71 There is currently no gold standard for diagnosis. Accurate detection of HCV nucleic acid sequences by amplification with PCR is limited by false-positive and false-negative results as well as by restricted availability of this test. Currently, PCR detection of HCV is performed only on a research basis, is labor-intensive, and is subject to variation among different laboratories. There is considerable interest in developing new methods for detection of HCV RNA in serum. A new assay, the branched-chain DNA assay or b-DNA assay, (Chiron Corporation, Emeryville, CA) is a hybridization assay.52 HCV RNA in the unknown sample is quantified by comparison of the amount of chemiluminescence to that of known RNA standards. Values are expressed as viral equivalents per mL.
HCV infection recurs after transplantation in almost all patients with pretransplantation infec- tion.44,49,52 Absolute proof of recurrence was pro- vided by demonstration of high-sequence homology in the hypervariable domain of the E2/NS1 region in paired pretransplantation and posttransplantation serum samples.53 By using the newly developed HCV RNA quantitative assay from Chiron, HCV EWA levels have been shown to increase 16-fold after transplantation in patients with recurrent infection.j2 Although the long-term consequences of posttrans- plantation HCV remain to be defined, infection is generally much less devastating than that of posttrans- plantation HBV infection. Interestingly, only half of all patients with detectable viremia at 1 year after transplantation have histological hepatitis.44 A more recent study confirmed and extended these findings, with hepatitis in 65% of patients with hepatitis C, despite normal ALT in half.j4 Although the disease course in many patients is benign, aggressive post- transplantation HCV infection leading to liver failure is well-do~umented.~~ The presence of HCV infection in blood donors with normal liver enzymes suggests the existence of a healthy carrier state, and it is likely that such a camer state also exists in some immuno- suppressed transplant recipients. Indeed, presence of high HCV RNA levels in the absence of liver damage and, more generally, lack of strong correlation be- tween levels of HCV RNA and histological damage have been shown in this settings2
Histological evidence of hepatitis not ascribable to HBV or cytomegalovirus (CMV) is present after transplantation in 14% to 35% of all liver allo-
g r a f t ~ . ~ ~ , ~ ~ , ~ ~ The first study showing that HCV infec- tion causes the majority of cases of hepatitis occur- ring after transplantation was conducted at the Mayo Clinic,57 and this has been confirmed.44 In three studies in which other viral infections were excluded, HCV infection accounted for 60%, 92%, and 96% of cases of hepatitis occumng after transplantation, r e s p e ~ t i v e l y . ~ ~ ~ ~ ~ ~ ~ ~
HCV infection, either before transplantation in the recipient or in the donor, is clearly linked to liver disease after transplantation. In recipients of organs from first-generation anti-HCV-positive donors, the prevalence of liver disease is seven times greater than it is in recipients of organs from untested donors.58 However, there is a wide spectrum of HCV liver disease that occurs after transplantation, both histo- logically and clinically, ranging from viremia without apparent consequences to hepatic f a i l ~ r e . ~ ~ , ~ ~ Al- though most HCV infection after transplantation is caused by prior infection in the recipient, acquisition from the donor organ or transfused blood products also O C C U ~ S . ~ ~ . ~ ~ A large study of 3,078 cadaveric organ donors from eight organ procurement agencies in the United States found a prevalence of anti-HCV (by EIA2) and HCV RNA (by PCR) of 4.2% and 2.4%, re~pective1y.j~ Recipients of anti-HCV-positive do- nors with detectable viremia were more likely to develop liver disease after transplantation and be HCV RNA positive, than were recipientsof anti-HCV- positive, HCV-RNA-negative donors.59 Thus, the presence of HCV RNA in the donor was highly associated with HCV transmission. The reduced risk of HCV acquisition from HCV-RNA-negative donors, may enable selective use of these organs in certain circumstances.
Given the preliminary information available about the natural history of HCV infection after liver transplantation, review of the natural history in other immunosuppressed patients, those undergoing renal transplantation, may be important. The range of biochemical abnormalities in renal transplant recipi- ents has been shown to vary widely (with elevations of serum aminotransferases from 9% to 75%).60,61 Anti-HCV seropositivity after transplantation is asso- ciated with chronically elevated aminotransferases (87% versus 57% in patients with and without HCV infection, respectively) and cirrhosis, defined by ultrasound criteria (21% versus lo%, respectively).61 However, these investigators employed EL41 for diagnosis, did not examine histological changes, and tracked patients for a relatively short period (mean duration of follow-up of 50 months, range 3 to 114 months). Pretransplantation HCV infection does ap-

Liver Transplantationfor Hepatitis B and C -
39
pear to influence adversely outcome of renal trans- plant recipients.b2 Sixty four anti-HCV-positive and 534 anti-HCV-negative recipients were tracked after transplantation. Serum aminotransferases were higher at the time of transplantation in previously infected patients, but follow-up values did not differ between infected and uninfected patients. Moreover, there were no differences in patient survival or graft survival between the two groups.62 HCV infection may on occasion contribute to liver failure after transplantation. In a study of 28 patients with HCV viremia tracked for 3 years after transplantation, infection was clinically silent in most patients.63 Only 5 patients had clinically significant liver disease, and one patient died of complications of cirrhosis. As in liver transplant recipients, kidney transplant recipi- ents have an increase in HCV replication on immuno- suppressive therapy.b3
Pathology and Pathogenesis
Histopathological findings in patients with HCV infection after transplantation have been addressed in a recent Of 43 viremic patients and at least one year of follow-up, 18 developed a mild form of chronic hepatitis, and 4 had progressive liver damage with chronic active hepatitis and bridging fibrosis or cirrhosis. Hepatitis developed an average of 4 months after transplantation. Mononuclear cell infiltrates in bile ducts from some patients suggest overlap in features of recurrent HCV and rejection. These find- ings contrast with the experience from Pittsburgh, PA, in which chronic active hepatitis was seen in only 5 of 317 transplanted patients (1.6%), and no patient progressed to cirrhosis.5b In the latter study, because antibody tests alone were used for diagnosis, the prevalence of HCV infection was likely underesti- mated. Histological findings typical of HCV infection after transplantation include fatty infiltration, portal and parenchymal mononuclear infiltrates, and swol- len hepatocytes with necrosis. Other common find- ings include bile duct damage associated with mono- nuclear cell infiltrates and lymphoid aggregates. Less frequent findings include centrilobular or diffuse cell swelling and parenchymal or piecemeal necrosis without significant inflammation (not observed in patients not receiving transplants) and bile duct damage and mixed lymphocytic and polymorpho- nuclear portal infiltrate. These latter findings may make the histological distinction between hepatitis and ischemia and/or rejection difficult. The lower prevalence of hepatitis after transplantation in some studies may be explained in part by overlapping histopathological features, resulting in diagnostic
uncertainties among HCV after transplantation and other entities common in the liver allograft.56 In a large series of HCV infection occurring after transplan- tation, severity of liver damage assessed histologically was not different in patients with recurrent and acquired infection. 52
Factors that determine why some patients are more susceptible to liver damage than others are currently under study. Many interrelated variables likely involved, including the level of viremia before transplantation, genotype of the virus, degree of immunosuppression after transplantation, and the ability of the host immune system to recognize and mount an immune response. The mechanisms by which this virus causes liver damage are poorly understood. An initial study of nonimmunosup- pressed patients suggested that high-level HCV repli- cation, as reflected by HCV viremia, may damage liver cells both by an immune-mediated mechanism and by a direct cytopathic effect.65 Immunosuppres- sion is likely to play a major role in the dramatic increase after transplantation of HCV RNA levels.j2 Whether immunosuppression augments HCV repli- cation by general effects on host-viral interaction or by a specific effect on viral replication remains to be investigated. In animal models of HCV, immunosup- pression results in decreased hepatic inflammation.b6 In some patients, despite very high levels of HCV RNA, there is no histological evidence of liver dam- age, arguing against a direct cytopathic effect of HCV.52 However, progressive hepatic failure with profound cholestasis has recently been described in a heart transplant recipient with organ-transmitted HCV infe~tion.~’ In situ PCR showed HCV RNA in more than 80% of hepatocytes, associated with very high levels of HCV RNA. The investigators propose that in this setting, HCV may be directly cytopathic to liver cells.67 Lastly, genotype of HCV may play a role, and it has been suggested that infection by HCV type 11 (according to Okamoto’s classification) has a more aggressive course after transplantation.68 It is likely that, as in patients with HBV infection, both immune- mediated and direct virally mediated mechanisms are important for development of liver damage after transplantation.
Treatment Management of the nontransplant patient with chronic HCV infection is hampered by lack of both definitive information as to the natural history of disease and direct proof that therapy alters histological progres- sion or patient survival. There is even less informa- tion in the transplant population.

40 Wriaht and Pereiru
There is only preliminary information about the efficacy of IFN-a in the treatment of hepatitis occur- ring after tran~plantation.33,~~ Of 11 patients with HCV and six with non-A, non-B hepatitis (the majority of whom presumably had HCV) treated with 3 million U three times weekly for 6 months, only 1 in each group had complete normalization of liver enzymes with therapy.33 The second pilot studied evaluated the safety and efficacy of IFN-a 2b for treatment of HCV infection in liver transplant recipi- e n t ~ . ~ ~ HCV RNA levels were monitored before and after treatment, and pretreatment parameters predic- tive of a complete response were determined. Eigh- teen post-liver-transplantation patients with detect- able HCV RNA in serum and biopsy-proven hepatitis received 3 million units of interferon three times weekly for at least 4 months. Pretreatment serum AST and ALT levels were at least 1.5 times the upper limit of normal. Complete response was seen in 5 patients (28%). At the end of therapy, HCV RNA levels were reduced in both responders and nonresponders. After cessation of treatment, alanine transaminase remained normal in four of five responders, but serum HCV RNA levels returned to pretreatment levels in both responders and nonresponders. There was no significant change in histology with therapy. Responders were more likely than were nonre- sponders to have low pretreatment HCV RNA levels and low serum bilirubin. Side effects resulted in early cessation of therapy in two patients and dose reduc- tion in six. Therefore, normalization of liver enzymes can be seen in patients with HCV infection after transplantation on interferon therapy, and treatment is associated with fall in HCV RNA levels regardless of biochemical response. However, virological im- provement is transient. Controlled clinical trials in this patient population are currently underway in the United States.
The greatest concern about the use of IFN-a in liver transplantation patients after surgery has been the possibility of precipitating allograft rejection. IFNs increase expression of HLA class I and I1 antigens that are involved in the cellular immune response in allograft rejection, and thus there is a theoretical risk of precipitating rejection with therapy.1° The results of two studies in renal trans- plant recipients given prophylactic interferon to reduce CMV infection are confli~ting.’~,’~ In one study, there was a beneficial effect of 3 million U daily in decreasing shedding of CMV without an adverse effect on graft function.70 In the second, there was no virological benefit in the treatment group, and there was an increase in graft loss because of
r e j e ~ t i o n . ~ ~ Given the histological overlap between hepatitis and rejection, allograft rejection may be underestimated in patients with ongoing hepatitis. A controlled trial in which treatment with IFN-a is compared with no treatment will be required to show both the safety and efficacy of this drug.
With this review, we hope that we have shown, not only the importance of hepatotrophic viruses as pathogens leading to liver transplantation but also their importance as causes of morbidity and mortality after transplantation. Study of these viruses can provide important clues with regard to the pathogen- esis of viral-associated liver disease. New approaches to treating disease are under development and pro- vide exciting opportunities for clinical research. How- ever, we caution that guidelines for transplantation used in the past should not be seen as inviolate in the future. The patient with liver failure from active hepatitis B infection (HBV-DNA-positive) is cur- rently not considered a candidate in many centers. Only by keeping an open mind about potential benefits of specific therapies will we have positive impact on this disease. With carefully controlled clinical trials, we will overcome one of the major problems in organ transplantation.
References 1.
2.
3.
4.
5.
6.
7.
8.
Todo S, Demetris AJ, Van Thiel DH, Teperman L, Fung JJ, Starzl TE. Orthotopic liver transplantation for pa- tients with hepatitis B virus-related liver disease. Hepa-
Samuel D, Bismuth A, Mathieu D, Arulnaden J-L, Reynes M, Benhamou J-P, et al. Passive immunopro- phylaxis after liver transplantation in HBsAg-positive patients. Lancet 1991 ;337:813-815. O’Grady JG, Smith HM, Davies S, Daniels HM, Donald- son PT, Tan KC, et al. Hepatitis B virus reinfection after orthotopic liver transplantation. J Hepatol 1992;14:104- 111. Chazouilleres 0, Mamish D, Kim M, Carey K, Ferrell L, Roberts J, et al. ”Occult” hepatitis B viral infection: An important source of transmission to the liver transplant recipient. Lancet 1994;343:142-146. Samuel D, Muller R, Alexander G, Fassati L, Ducot B, Benhamou JP, et al. Liver transplantation in European patients with the hepatitis B surface antigen. N Engl J Med 1993;329:1842-1847. Lugassy C, Bernuau J, Thiers V, Kroyaand K, Degott C, Wantzin P, et al. Sequences of hepatitis B virus DNA in the serum and liver of patients with acute benign and fulminant hepatitis. J Infect Dis 1987;155:64-71. Yoffe B, Burns DK, Bhatt HS, Combes B. Extrahepatic hepatitis B virus DNA sequences in patients with acute hepatitis B infection. Hepatology 1990;12:187-192. Feray C, Zignegno AL, Samuel D, Bismuth A, Reynes M, Tiollais P, et al. Persistent hepatitis B virus infection of mononuclear blood cells without concomitant liver
tology 1991 ;13:619-626.
Liver Trunsplantationfor Hepatitis B und C 41
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
infection. The liver transplantation model. Transplanta- tion 1990;49:1 155-1 158. Lavine JE, Lake JR, Ascher NL, Ferrell LD, Ganem D, Wright TL. Persistent hepatitis B virus following inter- feron alfa therapy and liver transplantation. Gastroenter-
Davies SE, Portmann BC, O'Grady JG, Aldis PM, Chaggar K, Alexander GJM, et al. Hepatic histological findings after transplantation for chronic hepatitis B virus infection, including a unique pattern of fibrosing cholestatic hepatitis. Hepatology 1991 ;13:150-157. Benner K, Lee RG, Keeffe EB, Lopez RR, Sasaki AW, Pinson CW. Fibrosing cytolytic liver failure secondary to recurrent hepatitis B after liver transplantation. Gastro- enterology 1992;103:1307-1312. Lucey MR, Graham DM, Martin P, Di Bisceglie A, Rosenthal S, Waggoner JG, et al. Recurrence of hepati- tis B and delta hepatitis after orthotopic liver transplan- tation. Gut 1992;33:1390-1396. Fang JWS, Tung FYT, Davis GL, Dolson DJ, Van Thiel DH, Lau JYN. Fibrosing cholestatic hepatitis in a trans- plant recipient with hepatitis B virus pre-core mutant. Gastroenterology 1993; 105:901-904. Muller R, Gubernatis G, Farle M, Niehoff G, Klein H, Wittekind C, et al. Liver transplantation in HBs antigen (HBsAg) carriers. Prevention of hepatitis B virus (HBV) recurrence by passive immunization. J Hepatol 1991 ;13:
Parfrey PS, Forbes RDC, Hutchinson TA, et al. The impact of renal transplantation on the course of hepati- tis B liver disease. Transplantation 1985;39:610-615. Lok ASF, Liang RHS, Chiu EKW, Wong K-L, Chan T-K, Todd D. Reactivation of hepatitis B virus replication in patients receiving cytotoxic therapy. Gastroenterology
Lam KC, Lai CL, Ng RP, Trepo C, Wu PC. Deleterious effect of prednisolone in HBsAg-positive chronic active hepatitis. N Engl J Med 1981 ;304:380-386. Tur-Kapsa R, Burk RD, Shaul Y, Shafritz DA. Hepatitis B virus contains a glucocorticoid-responsive element. Proc Natl Acad Sci USA 1986;83:1627-1631. Pirson Y, Alexandre GPJ, van Ypersele de Strihou C. Long-term effect of HBs antigenemia on patient survival after renal transplantation. N Engl J Med 1977;296:194- 196. Peters M, Vierling J, Gershwin ME, Milich D, Chisari FV, Hoofnagle JH. Immunology and the liver. Hepatology 1991 ; 13:977-994. Wright TL. Cytomegaloviral infection and vanishing bile duct syndrome. Culprit or innocent bystander? Hepatol-
Demetris AJ, Todo S, Van Thiel DH, Fung JJ, lwaki Y, Sysyn G, et al. Evolution of hepatitis B virus liver disease after hepatic replacement: practical and theo- retical considerations. Am J Pathol 1991 ;137:667-676. Missale G, Brems JJ, Takiff H, Pockros PJ, Chisari FV. Human leukocyte antigen class I-independent path- ways may contribute to hepatitis B virus-induced liver disease after transplantation. Hepatology 1993;18:491- 496. Chisari FV, Klopchin K, Moriyama T, Pasquinelli C, Dunsford HA, Sell S, et al. Molecular pathogenesis of hepatocellular carcinoma in hepatitis B virus transgenic mice. Cell 1989;59:1145-1156.
ology 1991 ;100:263-267.
90-96.
1991;100:182-188.
Ogy 1992;16:494-496.
25. Persing DH, Varmus HE, Ganem D. Inhibition of secre- tion of hepatitis B surface antigen by a related presur- face polypeptide. Science 1986;234: 1388-1 391 .
26. Lau JYN, Bain VG, Davies SE, O'Grady JG, Alberti A, Alexander GJM, et al. High-level expression of hepatitis B viral antigens in fibrosing cholestatic hepatitis. Gastro- enterology 1992;102:956-962.
27. Rakela J, Wooten RS, Batts KP, Perkins JD, Taswell HF, Krom RA. Failure of interferon to prevent recurrent hepatitis B infection in hepatic allograft. Mayo Clin Proc
28. Hoofnagle JH, Di Bisceglie AM, Waggoner JG, Park Y. Interferon alfa for patients with clinically apparent cirrho- sis due to chronic HBV. Gastroenterology 1993;104:
29. Marcellin P, Samuel D, Areias J, Loriot M-A, Arulnaden J-L, Gigou M, et al. Pretransplantation interferon treat- ment and recurrence of hepatitis B virus infection after liver transplantation for hepatitis B-related end-stage liver disease. Hepatology 1994;19:6-12.
30. Lauchart W, Muller R, Pichlmayr R. lmmunoprophylaxis of hepatitis B virus reinfection in recipients of human liver allografts. Transplant Proc 1987;19:2387-2389.
31. Lauchart W, Muller R, Pichlmayr R. Long-term immuno- prophylaxis of hepatitis B virus reinfection in recipients of human liver allografts. Transplant Proc 1987;19:4051- 4053.
32. McMahon G, Ehrlich PH, Moustafa ZA, McCarthy LA, Dottavio D, Tolpin MD, et al. Genetic alterations in the gene encoding the major HBsAg: DNA and immunologi- cal analysis of recurrent HBsAg derived from mono- clonal antibody-treated liver transplant patients. Hepa-
33. Wright HI, Gavaler JS, Van Thiel DH. Preliminary experi- ence with a-2binterferon therapy of viral hepatitis in liver allograft recipients. Transplantation 1992;53:121- 124.
34. Chossegros P, Pouteil-Noble C, Causse X, Pouyet M, Touraine JL, Trepo C. Gancylcovir is an effective antivi- ral agent for posttransplantation chronic HBV infections but maintenance therapy is required. J Hepatol 1992; 16[supplement 1]:S9.
35. Gish RG, Imperial JI, Esquivel CO, Keeffe EB. Ganciclo- vir treatment of severe hepatitis B virus (HBV) infection [abstract]. Gastroenterology 1993; 104:A908.
36. Marcellin P, Samuel D, Loriot MA, Areias J, Bismuth H, Benhamou JP. Anti-viral effect of adenine arabinoside monophosphate (ARA-AMP) in patients with recur- rence of hepatitis B virus (HBV) infection after liver transplantation [abstract]. Hepatology 1990; 12:966.
37. Rizzetto M, Macagno S, Chiaberge E, Verme G, Negro F, Marinucci G, et al. Liver transplantation in hepatitis delta virus disease. Lancet 1987;2:469-471.
38. Ottobrelli A, Marzano A, Smedile A, Recchia S, Saliz- zoni M, Cornu C, et al. Patterns of hepatitis delta virus reinfection and disease in liver transplantation. Gastro- enterology 1991 ;lo1 :1649-1655.
39. Mason WS, Taylor JM. Liver transplantation: A model for the transmission of hepatitis delta virus. Gastroenter-
40. David E, Rahier J, Pucci A, Camby P, Scevens M, Salizzoni M, et al. Recurrence of hepatitis D (delta) in liver transplants: histopathological aspects. Gastroen- terology 1993; 104: 1 122-1 128.
1 989;64:429-432.
11 16-1 121.
tology 1992;15:757-766.
ology 1991 ;lo1 11 741 -1 743.
42 Wright and Pereira
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
Samuel D, Zignego AL, Arulnaden JL, David MF, Gigou M, Feray C, et al. Liver transplantation for post hepatitis delta cirrhosis. Hepatology 19923 6:45A. Farci P, Mandas A, Coiana A, et al. Treatment of chronic hepatitis D with interferon alfa-2a. N Engl J Med
Hopf U, Neuhaus P, Lobeck H, Konig V, Kuther S, Bauditz J, et al. Follow-up of recurrent hepatitis B and delta infection in liver allograft recipients after treatment with recombinant interferon-a. J Hepatol 1991 ;13:339- 346. Wright TL, Donegan E, Hsu HH, Ferrell L, Lake JR, Kim M, et al. Recurrent and acquired hepatitis C viral infection in liver transplant recipients. Gastroenterology
Alter MJ, Margolis HS, Krawczynski K, Judson FN, Mares A, Alexander WJ, et al. Natural history of commu- nity-acquired hepatitis C in the United States. N Engl J Med 1992;327:1899-1905. Seeff LB, Buskell-Bales Z, Wright EC, Durako SJ, Alter HJ, lber FL, etal. N Engl J Med 1992;327:1906-1911. Kiyosawa K, Sodeyarna T, Tanaka E, Gibo Y, Yoshizawa K, Nakano Y, et al. Interrelationship of blood transfu- sion, non-A, non-B hepatitis and hepatocellular carci- noma: Analysis by detection of antibody to hepatitis C virus. Hepatology 1990;12:671-675. Martin P, Munoz SJ, Di Biscegie AM, Rubin R, Wag- goner JG, Armenti VT, Moritz MJ, Jarrell BE, Maddrey WC. Recurrence of hepatitis C virus infection after orthotopic liver transplantation. Hepatology 1991 ; 13:
Gretch DR, dela Rosa C, Perkins J, Corey L, Carrithers R. HCV infection in liver transplant recipients: chronic reinfection is universal, de novo acquisition rare. Hepa- tology 1992;16:45A [abstract]. Hsu HH, Wright TL, Tsao SC, Combs C, Donets M, Feinstone SM, Greenberg HB. Attenuated antibody response to hepatitis C virus after liver transplantation. Am J Gastroenterol 1994;89:1109-1174. Lok ASF, Chien D, Choo Q-L, et al. Antibody response to core, envelope and nonstructural hepatitis C virus antigens: comparison of imrnunocompetent and immu- nosuppressed patients. Hepatology 1993; 1 8:497-502. Chazouilleres 0, Kim M, Combs C, Ferrell L, Bacchetti P, Ascher NL, et al. Quantitation of Hepatitis C Virus RNA in Liver Transplant Recipients. Gastroenterology
Feray C, Samuel D, Thiers V, Gigou M, Pichon F, Bismuth A, et al. Reinfection of liver graft by hepatitis C virus after liver transplantation. J Clin Invest 1992;89:
Shiffman ML, Contos MJ, Luketic VA, Sonya1 AJ, Pur- dum PP, Mills S, et al. Biochemical and histological evaluation of recurrent hepatitis C following orthotopic liver transplantation. Transplantation 1994;57:526-532. Nakleh RE, Schwarzenberg SJ, Bloomer J, Payne W, Snover DC. The pathology of liver allografts surviving longer than one year. Hepatology 1989;11:465-470. Shah G, Demetris AJ, Gavaler JS, Lewis JH, Todo S, Starzl TE, et al. Incidence, prevalence, and clinical course of hepatitis C following liver transplantation. Gastroenterology 1992; 103:323-329.
1994;330:88-94.
1992;103:317-322.
71 9-721.
1994;106:994-999.
1361-1365.
57. Poterucha J, Rakela J, Lumeng L, Lee C-H, Taswell HF, Wiesner RH. Diagnosis of chronic hepatitis C after liver transplantation by the detection of viral sequences with polymerase chain reaction. Hepatology 19923 5:42-45.
58. Pereira BJG, Milford EL, Kirkman RL, Levey AS. Trans- mission of hepatitis C virus by organ transplantation. N Engl J Med 1991 ;325:454-460.
59. Pereira BJG, Wright TL, Schrnid CH, Bryan CF, Cheung RC, Cooper ES, et al. Screening and confirmatory testing of cadaver organ donors for hepatitis C virus infection: A US. national collaborative study. Kidney International, In Press.
60. Debure A, Degos F, Pol S, Degott C, Carnot F, Lugassy C, Lacombe M, Kreis H. Liver diseases and hepatic complications in renal transplant patients. Adv Nephro
61. Klauser R, Franz M, Traindi 0, Pidlich J, Hay U, Watschinger B, et al. Hepatitis C antibody in renal transplant patients. Transplant Proc 1992;24:286-288.
62. Pereira BJG, Wright TL, Schmid C, Lipkowitz GA, Shapiro ME, Milford E, et al. Comparative risk of post-transplantation liver disease, graft and patient survival in kidney recipients with and without pre- transplantation anti-HCV [abstract]. Am SOC Transplant Physicians 1994;A82.
63. Lau JYN, Davis GL, Brunson ME, Quian K-P, Lin H-J, Quan S, et al. Hepatitis C virus infection in kidney transplant recipients. Hepatology 1993;18:1027-1031.
64. Ferrell LD, Wright TL, Roberts J, Ascher N, Lake J. Pathology of hepatitis C viral infection in liver transplant recipients. Hepatology 1992;16:865-876.
65. Lau JYN, Davis GL, Kniffen J, Qian KP, Urdea MS, Chan CS, Mizokami M, Neuwald PD, Wilber JC. Significance of serum hepatitis C virus RNA levels in chronic hepati- tis c . Lancet 1991;341:1501-1504.
66. Krawczynski K, Beach M, Bradley DW, Meeks E, Spelbring JE. Immunosuppression and pathogenetic studies of acute hepatitis C virus (HCV) infection in chimpanzees. Hepatology 1992;16:345A [abstract].
67. Lim HL, Lau GKK, Davis GL, Dolson DJ, Lau JYN. Cholestatic hepatitis leading to hepatic failure in a patient with organ transmitted hepatitis C virus infec- tion. Gastroenterology 1991 ;106:248-251.
68. Feray C, Gigou M, Samuel D, Okamoto H, Reynes M, David MF, et al. Direct evidence for a more pathogenic effect of HCV type II: the model of liver transplantation. J Hepatol 1993;18(Suppl):S3.
69. Wright TL, Combs C, Kim M, Ferrell L, Bacchetti P, Ascher N, et al. Interferon alpha therapy for hepatitis C virus infection following liver transplantation. Hepatol-
70. Cheeseman SH, Rubin RH, Stewart JA, Tolkoff-Rubin NE, Cosimi AB, Cantell K, Gilbert J, Winkle S, Herrin JT, Black PH, Russell PS, Hirsch MS. Controlled clinical trial of prophylactic human-leukocyte interferon in renal transplantation. N Engl J Med 1979;300:1345-1349.
71. Kovarik J, Mayer G, Pohanka E, Schwarz M, Traindl 0, Graf H, et al. Adverse effect of low-dose prophylactic human recombinant leukocyte interferon-alpha treat- ment in renal transplant recipients. Transplantation
1988; 17:375-400.
Ogy 1994;20:773-779.
1988;45:402-405.