outcomes in children who underwent transplantation for autoimmune hepatitis
TRANSCRIPT

Outcomes in Children Transplanted for Autoimmune Hepatitis
Steven R Martin1, Fernando Alvarez1, Ravinder Anand2, Changhong Song2, WanrongYin2, and the SPLIT Research Group1 Department of Pediatrics, Hôpital Sainte-Justine, University of Montreal2 The EMMES Corporation
AbstractThe outcomes of 113 children with autoimmune hepatitis (AIH), registered with Studies ofPediatric Liver Transplantation and transplanted between 1995 and 2006, were compared withthose transplanted for other diagnoses (non-AIH). 4.9% of liver transplants were for AIH. 81%had AIH type 1 and most were transplanted for complications of chronic disease (60%), themajority in females (72%). Transplantation for fulminant AIH was more common in males (52.5%vs. 47.5% chronic, p=0.042). AIH patients differed from non-AIH by: age (13.0±0.4 vs. 4.6±0.1years, p<0.0001), sex (64.6% female vs.52.9%, p=0.016), ethnicity (48.7% white vs. 58.2%,p<0.0001), initial immunosuppression (tacrolimus based: 72.6% vs. 62.6%, p=0.045; MMF use:31.0% vs. 21.6 %, p=0.02) and immunosuppression at two years post-transplant (monotherapy:51.9% vs.17.3%, p<0.0001). Late (>3 months), but not steroid-resistant or chronic rejection, wasmore common in AIH (log-rank p=0.0015). 5-year post-transplant survival for AIH was 86%(95%CI 73–93). Patient and graft survival, infectious and metabolic complications and re-transplantation rates did not differ between AIH and non-AIH groups. In conclusion, the higherrisk for late acute rejection and greater degree of immunosuppression does not compromiseoutcomes of liver transplantation for AIH. Children transplanted for AIH in North America aretypically female adolescents with complications of chronic AIH type 1 and include more childrenof African-American or Latino-American origin compared to the overall liver transplantpopulation. These observations may inform detection, treatment and surveillance strategiesdesigned to reduce the progression of autoimmune hepatitis and subsequently, the need fortransplantation.
KeywordsLiver transplantation; Pediatrics; Late rejection; Outcome
Many patients with autoimmune hepatitis (AIH) already have cirrhosis at the time ofdiagnosis, and despite appropriate treatment, about 10%–15% of cases develop end-stageliver disease and require transplantation. (1) Almost 20%–25% of children with AIH,considering those with acute and chronic liver failure, will die or require livertransplantation while they are still children. (2) In adults, AIH is the underlying disease in1.8–6% of those undergoing liver transplantation. (3–7) Adult patients transplanted for AIHexperience acute cellular rejection and steroid-resistant rejection more frequently in the firstyear post-transplant than those transplanted for non-immune disorders.(5–10) Despite thisincrease in immune-mediated liver injury post-transplant, the long-term graft and patientsurvival, with a few exceptions, does not appear to be compromised.
Corresponding author: Steven R Martin MD, Gastroenterology & Nutrition, Alberta Children’s Hospital, 2888 Shaganappi Trail NW,Calgary, Alberta, Canada, T3B 6A8, Phone: 403 955-7721, Fax: 403 955-2992, [email protected].
NIH Public AccessAuthor ManuscriptLiver Transpl. Author manuscript; available in PMC 2012 April 1.
Published in final edited form as:Liver Transpl. 2011 April 1; 17(4): 393–401. doi:10.1002/lt.22244.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

As a consequence of its rarity few large pediatric series of AIH have been published. (11–13) In the King’s College series, 52 patients were identified, of whom 10 (20%) requiredtransplantation. One died awaiting transplantation while five (62.5%) experienced long-termsurvival. (11) Fulminant liver failure was the indication for transplantation in 4/9. In theBicêtre series, 31 patients with type 1 AIH were followed. Two died of liver failure in theera prior to transplantation and 5 developed progressive liver failure, such that 7/31 (23%)could be considered to have required transplantation. (12) In contrast, in a recent pediatricseries of 51 AIH patients who were followed for a median of 8 years, 28 (55%) came totransplantation. (13)
The Studies in Pediatric Liver Transplantation (SPLIT) registry was started in September1995 and as of June 1st 2006, 44 participating centers in the United States and Canadaregistered 3161 children under the age of 18 years, of whom 2291 have received a first liver-only transplant. This represents approximately 56% of pediatric liver transplants in NorthAmerica and includes the largest accumulation of data on children transplanted for AIH. Thegoal of this study was to determine the outcome of liver transplantation for AIH in childrencompared to the overall transplant population and to determine whether this outcome isinfluenced by the type of AIH or the mode of presentation.
Patients & MethodsParticipation in the SPLIT registry was approved by each center’s institutional review board.Parents or legal guardians provided written informed consent and patient assent wasobtained where appropriate. Enrolled patients were followed every 6 months until transplant.Post-transplant follow-up forms were sent every 6 months for 2 years, then annually untilthe patient’s 18th birthday. The timely, accurate and complete submission of data from eachcenter was ensured by the Data Quality Committee, a subcommittee of the ScientificAdvisory Board. This process included periodic site visits to evaluate the accuracy of thedata; some data submissions were compared to that found in the UNOS database. In 2005–2006, 82.9% of post-transplant follow-up forms were submitted by the centers. In thefollow-up period of greater than 2 years, 79.4% of forms were submitted from activecenters.
As of June 1, 2006, 169 patients were registered with the diagnosis code of ‘autoimmunehepatitis/cirrhosis’ or ‘fulminant autoimmune hepatitis.’ Each center registering one or moreof these patients was sent a supplemental form in order to confirm the diagnosis and obtaininformation on testing for the presence of serum auto-antibodies: nuclear (ANA), smoothmuscle (ASM), liver-kidney microsomes (LKM-1), or ‘other antibodies’ defined as anti-liver cytosol-1 (LC-1), anti-asialoglycoprotein receptor or anti-soluble liver antigen. Theform was completed for 132 patients of whom 2 were excluded (final diagnosis of primarysclerosing cholangitis; cirrhosis not considered to be of autoimmune origin). Of the 130registered patients with a completed form, 17 were not yet transplanted, while 113 receiveda first liver-only transplant and form the patient population for this study. The agedistribution of AIH patients compared with non-AIH patients (n=2178) is shown in figure 1.Certain outcomes in young infants differ from those in older children (14). Given that noAIH patient was under 1 year of age (compared to 35.2% of the whole SPLIT population),the AIH group was compared in this study to SPLIT patients that were older than one yearof age (non-AIH group, n=1411).
The pre-transplant diagnosis of AIH was in all cases accepted by pediatric hepatologists atSPLIT centers and reported to the SPLIT database. Although the definition of AIH, as withother primary diagnoses, is not operationalized in the SPLIT database, SPLIT centersconstitute tertiary care institutions with specific expertise in pediatric hepatology who are
Martin et al. Page 2
Liver Transpl. Author manuscript; available in PMC 2012 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
currently active in transplanting children for AIH and other liver diseases within NorthAmerica. Information was obtained from the registry on patient age, sex, ethnicity, bloodgroup, fulminant vs. chronic presentation; calculated Pediatric End Stage Liver Disease(PELD) score, hospitalization status (at home, hospitalized, ICU), height and weight Z-scores, type of donor organ (cadaveric whole, reduced, split; living donor).Immunosuppression was recorded as initial and long-term (one month, 12 months and 2years post-transplant). Outcomes included graft and patient survival; early acute rejection(<3 months), late acute rejection (>3 months), chronic and steroid resistant rejection. Thediagnosis of rejection was made according to each individual center’s practice.Complications included biliary, vascular and infectious complications, glucose intoleranceand re-transplantation AIH type 1 was defined by the presence of ANA and/or ASM whileAIH type 2 was defined by the presence of anti-LKM-1 or anti-LC-1. Occasional patientswith both ANA and LKM-1 were defined as AIH type 2. No data is available for studyingdisease recurrence and explant histology is not recorded in the database.
Statistical AnalysisData are presented as percentage or mean ± standard error. Wilcoxon tests were used fortesting the group differences of continuous variables. Large sample Chi-Square tests andFisher’s exact tests were used to test the group differences of categorical variables. TheKaplan-Meier method was used to estimate the probability of time to event. Log-rank testwas used for testing the group differences for the time to event data. Univariate Coxregression analysis was used to examine factors associated with patient and graft survival inAIH patients. Factors included liver disease presentation (fulminant vs. chronic); era oftransplantation (1995–1999 vs. 2000–2006); height and weight deficit ( < 2 z-scores vs. > 2z-scores); warm ischemia time; initial immunosuppression (cyclosporine A-based vs.tacrolimus-based); age at transplantation (1–5 years, 5–13 years, >13 years); organ type(living donor, cadaveric reduced, split, whole organ); donor age ( 0–6 months, 6–12 months,18–50 years, >50 years). For multilevel categorical factors, the “overall p-value” indicatesthat the risk factor has an effect on the outcome. A statistically significant “overall p-value”indicates that at least two levels of the risk factor differ with respect to the outcome.Pairwise comparisons between two levels of interest of a risk factor were indicated by the“p-value”. Factors significant at 0.10 level in the univariate analysis were entered into amultivariate model. In addition, outcomes in AIH and non-AIH patients were compared forpatient and graft survival and for rejection, adjusting for those factors of interest as definedin univariate analysis. All statistical analyses were implemented using the SAS System forWindows, version 9.1.3 (SAS Institute Inc., Cary, N.C.).
Resultsa) Patient Characteristics
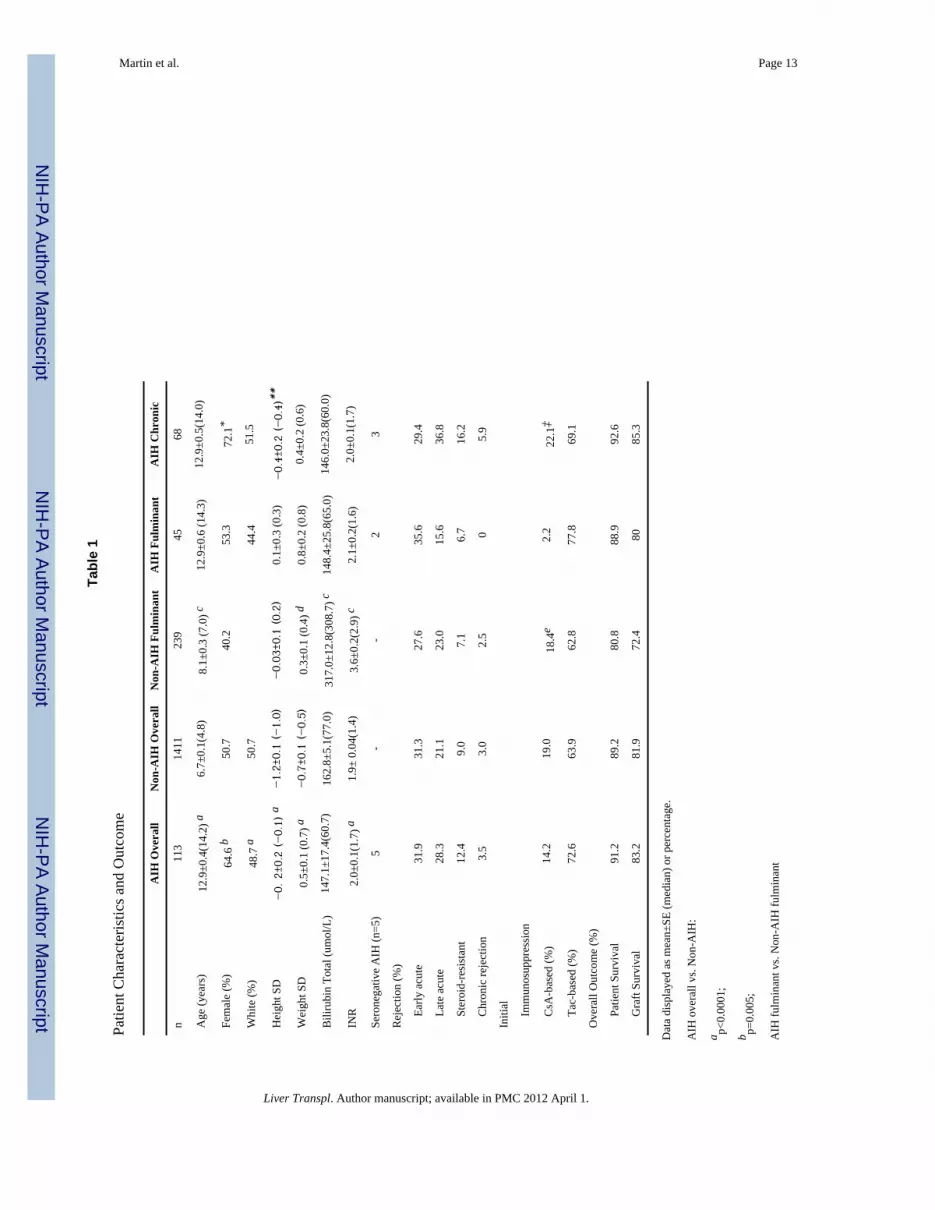
The 113 AIH patients who received a first only liver transplant represented 4.9% of thosetransplanted within SPLIT. In examining the temporal distribution of AIH cases by year oflisting (<2000, 2000–2002, 2003–2006) no difference in the proportion of AIH cases wasobserved (p=0.37). Characteristics at the time of transplant of the total AIH population andof subgroups with a chronic or fulminant presentation were compared with non-AIH patients(table 1). AIH patients were significantly older than non-AIH, and received a greaterproportion of whole, deceased donor organ transplants (75.2% vs.59.3%, p=0.008),including few living donor organs (7.1% vs. 11.5%, p=0.008). AIH patients showed lessimpaired growth with a greater proportion of females and children of non-white ethnicity. Inparticular, a greater proportion of African-American and Latino-American patients weretransplanted for AIH than for other diagnoses (49.6% AIH vs. 29.7% non-AIH, p<0.0001).
Martin et al. Page 3
Liver Transpl. Author manuscript; available in PMC 2012 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

No differences were observed between the groups for hospitalization status, for blood typeor for median PELD score (9.6 vs.8.6).
b) ImmunosuppressionThe immunosuppressive regimen at transplant and throughout two years of follow-up isshown in table 2. At transplant, there were no differences between the groups in the use ofinduction therapy, corticosteroids, calcineurin inhibitors, azathioprine or sirolimus. By onemonth post-transplant, cyclosporine-based therapy was reduced in both groups in favor oftacrolimus and remained thereafter relatively unchanged until at least two years post-transplant. However, a greater reduction in the use of cyclosporine-basedimmunosuppression over time was observed in AIH patients (45.8% reduction, AIH vs.16.1% reduction, non-AIH). By one to two years after liver transplant, monotherapy wasmore common in non-AIH patients due principally to greater reductions in the use ofcorticosteroids and azathioprine. MMF was used in a greater proportion of AIH patients thannon-AIH from the time of transplantation; over time similar but small reductions in the useof MMF was reported in both groups. Sirolimus was introduced in a greater proportion ofAIH patients beginning at one year after transplantation.
c) OutcomeThe estimated probability of 5-year survival was 86% (95%CI 73–93). Univariate analysisdid not identify any factor that was significantly associated with patient and graft survival inthe AIH patients (table 3). Factors significant at a p-value of <0.1 in the univariate modelwere entered into a multivariate model. Variables selected for analysis of patient survivalwere liver disease presentation, weight deficit at transplant, and era of transplant; for graftsurvival analysis liver disease presentation and warm ischemia time were selected. Of thesefactors, only longer warm ischemia time was associated with a higher risk of graft loss(HR1.20; 95%CI 1.01–1.41, p=0.0374). When the AIH group was compared with the non-AIH group, no difference in patient or graft survival was observed (figure 2). Similarly,univariate analysis adjusting for various factors of interest revealed no significantdifferences between the AIH and non-AIH groups (table 4).
The time to first rejection is shown in figure 3, the curves remaining superimposed untilafter 6 months. No differences between AIH and non-AIH patients were observed for earlyacute rejection (31.9% vs. 31.3%), chronic rejection (3.5% vs. 3.0%) and steroid resistantrejection (12.4% vs. 9.0%). However, AIH patients were at greater risk of late acuterejection (28.3% vs. 21.1%, log-rank p=0.0056). In univariate analysis, there was nodifference in risk of rejection between AIH and non-AIH groups (table 4).
d) ComplicationsNo differences were observed between AIH and non-AIH patients within the first year pos-transplant for biliary tract complications (15.9% vs. 16.9%, p=0.783), for vascularcomplications (8.8% vs. 15.5 %, p=0.05), for glucose intolerance (12.4% vs. 10.5%,p=0.528) or for infection with cytomegalovirus (5.3 % vs. 8.6 %, p=0.218).Lymphoproliferative disease was rare in both groups (AIH n=0, non-AIH n=31 (2.2%)).This was associated with significantly fewer Epstein Barr virus (EBV) infections in AIHpatients (n=1) than non-AIH n=95 (6.7%) log rank p value= 0.0185). Within the first month,fungal infections were similar but bacterial infections were less frequent in AIH patients(16.8% vs. 28.5%, p=0.013). Re-transplantation was required in 11 (9.7%) AIH patients andin 9.9% of non-AIH (ns); none was for recurrent disease: primary graft dysfunction (2);biliary complications (1); hepatic artery thrombosis (2); acute cellular rejection (2); chronicrejection (1); not reported (3).
Martin et al. Page 4
Liver Transpl. Author manuscript; available in PMC 2012 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

e) Chronic vs. fulminant presentation of AIHAIH patients were classified by transplant for complications of chronic disease (60%, n=68)or by fulminant presentation (40%, n=45). No significant differences were observed overallbetween chronic and fulminant presentation for age, ethnicity, weight, and blood type,degree of cholestasis, type of donor organ, hospitalization status or risk of for rejection. Thecalculated PELD of the chronic group was 10.8±1.7. A fulminant presentation was morecommon in males (52.5% vs. 47.5% chronic) than in females (32.8% vs. 67.2% chronic),p=0.042. Fulminant AIH patients had higher height z-scores. Cyclosporine appeared to beused less often for fulminant AIH but care is needed in interpreting these data as informationwas missing in 8/45 (17.8%) fulminant vs. 5/68 (7.4%) chronic. While no differences in 4year patient or graft survival were observed, all deaths in the fulminant group (5/45)occurred within the first year (log rank test p<0.05).
AIH and non-AIH patients with a fulminant presentation were also compared (table 1). Attransplant, fulminant non-AIH patients were younger and appeared more ill as suggested bya lower weight and a higher serum bilirubin and INR. Patient and graft survival in AIHfulminant patients was similar to the non-AIH fulminant and the chronic AIH group (table1).
f) AIH type 1 vs. AIH type 2Of the 113 AIH patients, 87 had serological data available; however for 13 of these cases theautoantibody data was incomplete (one or more antibody missing) thus preventing preciseclassification. Of the remaining 74 patients, 60 (81%) were AIH type 1, 9 (12%) were AIHtype 2 and 5 (6.8%) were negative for all markers. No patients were reported with anti-asialoglycoprotein receptor or anti-soluble liver antigen antibodies. Table 5 shows thecharacteristics of these two subgroups. Overall the age at transplantation was similar forboth AIH types. The two males with AIH type 2 were transplanted with a fulminantpresentation; they were younger (7.8±6.5 years) than other males presenting with eitherchronic or fulminant AIH type 1 (13.4±1.2 years and 15.4±0.6 years respectively). Allfemales were transplanted as adolescents, whether with a fulminant presentation (AIH type1: 15.3± 0.8 years vs. AIH type 2: 14.9±0.1 years), or with chronic disease (AIH type 1:12.3±0.8 vs. AIH type 2: 12.6±1.9 years). Due to the small numbers of AIH 2 patients,meaningful statistical comparisons could not be made.
DiscussionCurrent understanding of the course of patients who receive a liver transplant for AIH islargely based on the adult literature and on pediatric series from individual centers. Thepatients herein described represent the largest group of children with AIH followed afterliver transplantation. 4.9% of transplants within SPLIT were for AIH, a similar proportion tothat reported in adults (4% European Liver Transplant Registry, 2006; 3.6% The OrganProcurement and Transplantation Network database, 2007). Most children in this study cameto transplant with chronic disease. If one reasonably assumes that the 17 patients not yettransplanted of the 130 that were registered are likely to be listed with chronic disease, then85 children with AIH (75%) would come to transplant with complications of cirrhosis. Assuch, strategies to reduce the need for transplantation in AIH would seem best targeted toreducing the progression of the disease to cirrhosis, including early detection, aggressiveinitial treatment and, at least in pediatrics, a very close surveillance of patients in whomweaning of therapy is considered. Given the nature of a registry it is difficult to determinethe precise indications for listing these children for transplant (liver failure, complications ofportal hypertension) but the mean PELD scores for those with a chronic presentation were
Martin et al. Page 5
Liver Transpl. Author manuscript; available in PMC 2012 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

under 15, suggesting that the majority of patients were not in advanced liver failure at thetime of transplant.
Many of the demographic differences from the other children transplanted within SPLITreflect the nature of AIH as a disease that affects older children with a female preponderancecharacterized by preserved growth, greater use of whole organs and fewer living donors. Ofinterest is the higher proportion of non-white children transplanted for AIH compared toother diagnoses, potentially indicating a more aggressive disease in some ethnic groups, aswas previously suggested (15,16). Socioeconomic factors influencing access to timelyevaluation and therapy could be a confounding factor that would require further verification(17). Children transplanted for AIH have excellent outcomes that are not different fromchildren undergoing liver transplant for other conditions. Our results compare favorablywith the 5-year patient survival of 0.79 (95%CI 0.51–0.92) recently reported for pediatricAIH patients in the European Liver Transplant Registry (18). However, AIH patientsexperience greater levels of immunosuppression in the first two years after transplant andare at higher risk of late, acute rejection but not of steroid-resistant rejection or chronicrejection. A greater proportion of AIH patients received corticosteroids and was converted totacrolimus-based immunosuppression by the end of the first year post-transplant. We cannotreadily distinguish between the administration of higher degrees of immunosuppression as aconsequence of therapy for late rejection episodes (as suggested by the greater use ofsirolimus by the end of the first year) and an aggressive immunosuppressive approach fromthe time of transplantation to address a perceived greater risk for rejection (as suggested bythe greater use of MMF from the time of transplant).
Surprisingly, despite increased immunosuppression AIH patients experienced less infectiouscomplications than non-AIH patients, perhaps related to their older age (more likely alreadyexposed to CMV and EBV), lack of previous surgery and better nutritional status. AIHpatients are at greater risk for type 1 diabetes. Given the preference for tacrolimus-basedimmunosuppression and the prolonged use of corticosteroids, one might expect to observeglucose intolerance more frequently but this was not observed. The rate of re-transplantationin this study was only 9.7% and none was for recurrent disease. Clear criteria for recurrentAIH were not available at the inception of the SPLIT database and still remain somewhatcontroversial. We were, therefore, unable to study the risk of relapse of AIH post-transplantwhich has been estimated at approximately 22% (19).
Of concern was the finding that 23% of children transplanted for AIH appear not to havehad any search for confirmatory serum markers. While such markers are not pathognomonicfor AIH, the absence of a systematic search for serologic markers hinders the study of thecourse of AIH before and after transplantation. This should be addressed by the pediatrictransplant community.
Important research questions concerning children transplanted for AIH include theproportion of all AIH patients requiring transplant, the duration of disease before listing, thetype of pre-transplant therapy, its duration and its impact (non-response versus an initialresponse followed by long-term deterioration). Post-transplant issues include thedevelopment of co-morbidities such as ulcerative colitis, how to identify recurrent diseaseand the impact of medication adherence on outcomes. These questions are not wellanswered by a pediatric transplant registry such as SPLIT, or by individual centers, but willrequire the cooperation in the form of an international registry of AIH.
In conclusion, the majority of children receiving a liver transplant for autoimmune hepatitisin North America are female adolescents with AIH type 1 presenting as chronic disease,with an over representation of African-Americans and Latino-Americans compared with the
Martin et al. Page 6
Liver Transpl. Author manuscript; available in PMC 2012 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
overall transplant population. Despite a greater degree of immunosuppression, outcomes aresimilar to the overall population with no increase in infectious or metabolic complicationsand although the risk of late acute cellular rejection is higher this does not result in increasedchronic rejection, steroid-resistant rejection or need for re-transplantation.
AcknowledgmentsThe SPLIT Research Group are: S. Dunn, J. Menendez, L. Flynn (Alfred I Dupont Hospital for Children,Wilmington, DE); M. Jonas, D.. Healey. (Boston Children’s Hospital, Boston, MA); R. Kane, E. Phillips, H.Solomon(Cardinal Glennon Children’s Hospital, St. Louis University, St. Louis, MO); T. Heffron, S. Sekar, T.Pillen, L. Davis, J.DePaolo, G.Smallwood; (Children’s Healthcare of Atlanta, Atlanta, GA); J. Bucuvalas, F.Ryckman, A. Howkins, G. Arya, S. Krug, C. Tiao, K. Campbell.(Children’s Hospital Cincinnati, Cincinnati, OH);M. Narkewicz, R. Sokol, F. Karrer, K. Orban-Eller (Children’s Hospital Denver, University of Colorado School ofMedicine, Denver, CO); E. Rand, K. Anderer, B. Patel(Children’s Hospital of Philadelphia, Philadelphia, PA); G.Mazariegos, N. Chien, MA Karuna, K Haberman (Children’s Hospital of Pittsburgh, Thomas E StarzlTransplantation Institute Pittsburgh, PA); P. Atkinson (Children’s Hospital Western Ontario, London, ON,Canada); G. Telega, S. Lerrett, J Nebel (Children’s Hospital of Wisconsin, Milwaukee, WI); D. Desai, N. Mittal, L.Cutright, L. Arnott (Children’s Medical Center of Dallas, Dallas, TX); E. Alonso, J. Lokar, S. Kelly, K. Neighbors,R Superina, P Whitington, K Tuzinkiewicz (Children’s Memorial Medical Center, Transplant Center of Excellence,Chicago, IL); W. Andrews, J. Daniel, V. Fioravanti, A. Tendick (Children’s Mercy Hospital, Kansas City, MO); S.Jarvis (Duke University Medical Center, Durham, NC); A. Fecteau, V. Ng, W Drew (Hospital for Sick ChildrenToronto, Toronto, ON, Canada); J. Tector, J. Lim, J. Molleston, J. Pearson, S Hicks (Indiana University MedicalCollege, Indianapolis, IN); K. Schwarz, P. Colombani, M. Alford, C Bhave, L Wilson, R. Jurao (Johns HopkinsHospital, Baltimore, MD); J. Eason, J. Eshun, S. Powell, H Grewl (Le Bonheur Children’s Medical Center,Memphis, TN); D. Freese, M El-Yossef, J. Weckwerth, J. Greseth, L Pearson, L. Young (Mayo Medical School,Rochester, MN); R. Fisher, M. Akyeampong, M. Benka, A. Lassiter (Medical College of Virginia, Richmond, VA);N. Sekar, S. Parkar, R. Gagliardi (Mount Sinai Medical Center, New York, NY); S. Lobritto, J Cho (New YorkPresbyterian Hospital, New York, NY); L. Book, M. O’Gorman, C. Kawai, L. Bruschke, J. Kraus, R.Thorson(Primary Children’s Hospital Medical Center, Salt Lake City, UT); C. Viau (Sainte-Justine Hospital,Montreal, QC, Canada); R. Shepherd, J. Lowell, M. Nadler, S. Guelker (St. Louis Children’s Hospital, St. Louis,MO); W. Berquest, M. Castillo, A. Bula, R. Berquist (Stanford University Medical Center, Palo Alto, CA);
P. Karpen, J. Mayo, J. Goss, D. Ybarra, B. Carter, (Texas Children’s Hospital, Houston, TX); S. McDiarmid, S.Fiest (UCLA Medical Center, Los Angeles, CA); S. Gilmour, B. Dodd, N. Kneteman, A. Jones (University ofAlberta, Edmonton, AB, Canada); J. Lavine, A. Khanna, R. Clawson (University of California San Diego, SanDiego Medical Center, San Diego, CA); P. Rosenthal, D. Filipowski, J. Roberts (University of California SanFrancisco, San Francisco, CA); J. Millis, P. Boone (University of Chicago, Chicago, IL); R. González-Peralta, M.Langham, M. Hodik, (University of Florida-Shands Children’s Hospital, Gainesville, FL); A. Tzakis, T. Kato, D.Weppler, L. Cooper, M. Gonzalez, L. Smith, A. Santiago (University of Miami, Jackson Memorial Hospital,Miami, FL); J. Lopez, J. Magee, V. Shieck (University of Michigan, Ann Arbor, MI); A. Humar, B. Durand.(University of Minnesota, Minneapolis, MN); A. Langnas, D. Antonson, J. Botha, W. Grant, D. Sundan, D.Andersen, B. Fleckten, K. Seipel, C. Torres, B. Shaw. (University of Nebraska Med Center, Omaha, NE); J. Fair, P.McIver, J. Young, A. Raizada, J. Prinzhorn, . (University of North Carolina, Chapel Hill, NC); M. Orloff, T.Shisler, T. Rossi, C. Hill-Sober. (University of Rochester, Strong Memorial Hospital, Rochester, NY); G. Halff, J.Silva (University of Texas, HSC San Antonia, San Antonio, TX); S. Horslen, K. Wallace. (University ofWashington Seattle, Seattle, WA); M. Kalayoglu, A. D’Alessandro,, R. Judd, S. Knechtle, E. Spaith (University ofWisconsin, Madison, WI).
The Studies of Pediatric Liver Transplantation (SPLIT) research group thanks the following people at the datacoordinating center (EMMES Corporation): A. Lindblad PhD, K. Martz, D. Falleroni, J. He, G. Fraser, J. Mitchell,L.Covington, N. Hornbeak, N. Patel.
Abbreviations
SPLIT Studies of Pediatric Liver Transplantation
AIH Autoimmune Hepatitis
PELD Pediatric end stage liver disease
UNOS United Network for Organ Sharing
ANA anti-nuclear antibody
Martin et al. Page 7
Liver Transpl. Author manuscript; available in PMC 2012 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

ASM anti-smooth muscle antibody
LKM-1 anti-liver kidney microsomal type 1 antibody
LC1 anti-liver cytosol antibody
MMF mycophenolate mofetil
References1. Manns MP, Strassburg CP. Autoimmune hepatitis: Clinical challenges. Gastroenterology. 2001;
120:1502–1517. [PubMed: 11313321]2. Alvarez, F. Autoimmune Hepatitis. In: Suchy, R.; Balistreri, WF., editors. Liver Disease in
Children. Lippincott, Williams and Wilkins; Philadelphia: 2001. p. 429-441.3. Prados E, Cuervas-Mons V, de la Mata M, et al. Outcome of autoimmune hepatitis after liver
transplantation. Transplantation. 1998; 66:1645–1650. [PubMed: 9884253]4. Cattan P, Berney T, Conti F, Calmus Y, Homberg JC, Houssin D, Soubrane O. Outcome of
orthotopic liver transplantation in autoimmune hepatitis according to subtypes. Transpl Int. 2002;15:34–38. [PubMed: 11875611]
5. Hayashi M, Keeffe EB, Krams SM, Martinez OM, Ojogho ON, So SK, et al. Allograft rejectionafter liver transplantation for autoimmune liver diseases. Liver Transpl Surg. 1998 May; 4(3):208–14. [PubMed: 9563959]
6. Ratziu V, Samuel D, Sebagh M, Farges O, Saliba F, Ichai P, et al. Long-term follow-up after livertransplantation for autoimmune hepatitis: evidence of recurrence of primary disease. J Hepatol.1999; 30:131–41. [PubMed: 9927160]
7. Reich Reich DJ, Fiel I, Guarrera JV, Emre S, Guy SR, Schwartz ME, et al. Liver transplantation forautoimmune hepatitis. Hepatology. 2000; 32:693–700. [PubMed: 11003612]
8. Molmenti EP, Netto GJ, Murray NG, Smith DM, Molmenti H, Crippin JS, et al. Incidence andrecurrence of autoimmune/alloimmune hepatitis in liver transplant recipients. Liver Transpl. 2002Jun; 8(6):519–26. [PubMed: 12037782]
9. Vogel A, Heinrich E, Bahr MJ, Rifai K, Flemming P, Melter M, et al. Long-term outcome of livertransplantation for autoimmune hepatitis. Clin Transplant. 2004; 18:62–69. [PubMed: 15108772]
10. Wright HL, Bou-Abboud CF, Hassanein T, Block GD, Demetris AJ, Starzl TE, et al. Diseaserecurrence and rejection following liver transplantation for autoimmune chronic active liverdisease. Transplantation. 1992; 53:136–9. [PubMed: 1733061]
11. Gregorio GV, Portmann B, Reid F, Donaldson PT, Doherty DG, McCartney M, et al. Autoimmunehepatitis in Childhood: A 20 year experience. Hepatology. 1997; 25:541–547. [PubMed: 9049195]
12. Maggiore G, Veber F, Bernard O, Hadchouel M, Homberg JC, Alvarez F, et al. Autoimmunehepatitis associated with anti-actin antibodies in children and adoloscents. J Pediatr GastroenterolNutr. 1993; 17:376–381. [PubMed: 8145091]
13. Bahar RJ, Yanni GS, Martin MG, McDiarmid SV, Vargas JH, Gershman GB, et al. Orthotopicliver transplantation for autoimmune hepatitis and cryptogenic chronic cirrhosis in children.Transplantation. 2001; 72 (5):829–833. [PubMed: 11571445]
14. Sundaram SS, Alonso EM, Anand R. Study of Pediatric Liver Transplantation Research Group.Outcomes after liver transplantation in young infants. J Pediatr Gastroenterol Nutr. 2008 Oct;47(4):486–92. [PubMed: 18852642]
15. Verma S, Torbenson M, Thuluvath PJ. The impact of ethnicity on the natural history ofautoimmune hepatitis. Hepatology. 2007; 46:1828–1835. [PubMed: 17705297]
16. Smith A, Gentile J. Autoimmune hepatitis is a more common indication for orthotopic livertransplantation among African American patients than among non-African American patients[abstract]. Transplantation. 2006; 82(suppl 2):981.
17. Zeni MB, Sappenfield W, Thompson D, Chen H. Factors associated with not having a personalhealth care provider for children in Florida. Pediatrics. 2007; 119 (Suppl 1):S61–7. [PubMed:17272587]
Martin et al. Page 8
Liver Transpl. Author manuscript; available in PMC 2012 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

18. Schramm C, Bubenheim M, Adam R, Karam V, Buckels J, O’Grady JG, et al. Primary livertransplantation for autoimmune hepatitis: a comparative analysis of the European TransplantRegistry Liver Transplantation. 2010; 16:461–469.
19. Gautam M, Cheruvattath R, Balan V. Recurrence of autoimmune liver disease after livertransplantation: a systematic review. Liver Transplantation. 2006; 12:1813–1824. [PubMed:17031826]
Martin et al. Page 9
Liver Transpl. Author manuscript; available in PMC 2012 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.Age distribution of AIH patients (n=113) and the total non-AIH population (n=2178), allrecipients of a first liver-only transplant in SPLIT. Non-AIH patients >1 year were includedin the study (n=1411) Non-AIH; AIH.
Martin et al. Page 10
Liver Transpl. Author manuscript; available in PMC 2012 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 2.Kaplan-Meier curves for patient (A) and graft (B) survival in AIH and in Non-AIH patients> 1year of age.
Martin et al. Page 11
Liver Transpl. Author manuscript; available in PMC 2012 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 3.Kaplan-Meier curves for first rejection in AIH and in Non- AIH patients > 1year of age.
Martin et al. Page 12
Liver Transpl. Author manuscript; available in PMC 2012 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Martin et al. Page 13
Tabl
e 1
Patie
nt C
hara
cter
istic
s and
Out
com
e
AIH
Ove
rall
Non
-AIH
Ove
rall
Non
-AIH
Ful
min
ant
AIH
Ful
min
ant
AIH
Chr
onic
n11
314
1123
945
68
Age
(yea
rs)
12.9
±0.4
(14.
2) a
6.7±
0.1(
4.8)
8.1±
0.3
(7.0
) c12
.9±0
.6 (1
4.3)
12.9
±0.5
(14.
0)
Fem
ale
(%)
64.6
b50
.740
.253
.372
.1*
Whi
te (%
)48
.7 a
50.7
44.4
51.5
Hei
ght S
D−0.
2±0
.2 (−0.
1) a
−1.
2±0.
1 (−
1.0)
−0.
03±0
.1 (0.
2)0.
1±0.
3 (0
.3)
−0.
4±0.
2 (−
0.4)
**
Wei
ght S
D0.
5±0.
1 (0
.7) a
−0.
7±0.
1 (−
0.5)
0.3±
0.1
(0.4
) d0.
8±0.
2 (0
.8)
0.4±
0.2
(0.6
)
Bili
rubi
n To
tal (
umol
/L)
147.
1±17
.4(6
0.7)
162.
8±5.
1(77
.0)
317.
0±12
.8(3
08.7
) c14
8.4±
25.8
(65.
0)14
6.0±
23.8
(60.
0)
INR
2.0±
0.1(
1.7)
a1.
9± 0
.04(
1.4)
3.6±
0.2(
2.9)
c2.
1±0.
2(1.
6)2.
0±0.
1(1.
7)
Sero
nega
tive
AIH
(n=5
)5
--
23
Rej
ectio
n (%
)
Ea
rly a
cute
31.9
31.3
27.6
35.6
29.4
La
te a
cute
28.3
21.1
23.0
15.6
36.8
St
eroi
d-re
sist
ant
12.4
9.0
7.1
6.7
16.2
C
hron
ic re
ject
ion
3.5
3.0
2.5
05.
9
Initi
al
Im
mun
osup
pres
sion
C
sA-b
ased
(%)
14.2
19.0
18.4
e2.
222
.1‡
Ta
c-ba
sed
(%)
72.6
63.9
62.8
77.8
69.1
Ove
rall
Out
com
e (%
)
Pa
tient
Sur
viva
l91
.289
.280
.888
.992
.6
G
raft
Surv
ival
83.2
81.9
72.4
8085
.3
Dat
a di
spla
yed
as m
ean±
SE (m
edia
n) o
r per
cent
age.
AIH
ove
rall
vs. N
on-A
IH:
a p<0.
0001
;
b p=0.
005;
AIH
fulm
inan
t vs.
Non
-AIH
fulm
inan
t
Liver Transpl. Author manuscript; available in PMC 2012 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Martin et al. Page 14c p<
0.00
01;
d p=0.
01
e p=0.
002.
AIH
chr
onic
vs.
AIH
fulm
inan
t:
* p=0.
042;
**p=
0.04
7;
‡ p=0.
0047
; mis
sing
dat
a: 5
chr
onic
, 8 fu
lmin
ant.
Liver Transpl. Author manuscript; available in PMC 2012 April 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Martin et al. Page 15
Tabl
e 2
Type
of I
mm
unos
uppr
essi
on in
AIH
and
Non
-AIH
Gro
up
Initi
al1
mon
th1
year
2 ye
ars
AIH
Non
-AIH
AIH
Non
-AIH
AIH
Non
-AIH
AIH
Non
-AIH
N=1
13N
=141
1N
=106
N=1
299
N=7
3N
=962
N=5
2N
=745
Indu
ctio
n17
.719
.0-
--
--
-
CyA
-bas
ed14
.219
.27.
5 a
15.3
9.6
14.9
7.7
16.1
Tac
ro-b
ased
72.6
63.9
79.2
73.1
83.6
80.4
88.5
79.5
Ster
oids
86.7
88.2
82.1
84.0
65.8
b53
.559
.6f
33.6
MM
F31
.0d
21.6
31.1
22.9
28.8
d18
.125
.016
.2
Aza
thio
prin
e15
.016
.410
.411
.511
.06.
015
.4c
5.4
Siro
limus
0.9
0.6
0.9
1.2
12.3
c4.
19.
64.
7
Mon
othe
rapy
0.9
d6.
26.
65.
49.
6e34
.717
.3e
51.9
Dat
a ar
e ex
pres
sed
as p
erce
ntag
es.
a p=0.
03;
b p=0.
04;
c p<0.
01;
d p=0.
02;
e p<0.
0001
;
f p=0.
0001
.
Liver Transpl. Author manuscript; available in PMC 2012 April 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Martin et al. Page 16
Tabl
e 3
Uni
varia
te A
naly
sis o
f Pat
ient
and
Gra
ft Su
rviv
al fo
r AIH
Sub
ject
s
Fact
ors
Patie
nt S
urvi
val
Gra
ft Su
rviv
al
Haz
ard
ratio
p- v
alue
Ove
rall
p-va
lue
Haz
ard
ratio
p- v
alue
Ove
rall
p-va
lue
Live
r Dis
ease
Pre
sent
atio
n3.
920.
0627
2.26
0.09
11
Era
of T
rans
plan
t4.
540.
1767
1.47
0.54
34
20
00–2
006
vs. 1
995–
1999
Ht.
defic
it at
Tra
nspl
ant
1.58
0.56
621.
370.
6145
Wt.
defic
it at
Tra
nspl
ant
5.58
0.10
892.
250.
4322
War
m is
chem
ia ti
me
1.09
0.46
871.
160.
0668
Imm
unos
uppr
essi
on
C
yclo
spor
ine
A v
s. Ta
crol
imus
0.34
0.31
430.
850.
8039
Age
at T
rans
plan
t0.
6622
0.98
57
5–
12 y
rs. v
s. 1–
4 yr
s.0.
520.
5548
1.11
0.92
12
≥
13 y
rs. v
s. 1–
4 yr
s.0.
370.
3778
1.03
0.97
76
Org
an ty
pe0.
6889
0.98
18
Li
ve v
s. C
ad. W
hole
--0.
9953
--0.
9922
C
ad. R
educ
ed v
s. C
ad. W
hole
2.71
0.22
511.
370.
6773
C
ad. S
plit
vs. C
ad. W
hole
0.00
0.99
570.
000.
9930
Don
or a
ge0.
7782
0.79
21
6–
11 m
onth
s vs.
1–17
yrs
.--
0.99
48--
0.99
25
18
–49
yrs.
vs. 1
–17
yrs.
0.98
0.98
190.
990.
9795
≥
50 y
rs. v
s. 1–
17 y
rs.
2.51
0.34
152.
150.
3299
All
patie
nts w
ere
at le
ast o
ne y
ear o
f age
at t
rans
plan
t. Fa
ctor
s as d
efin
ed in
met
hods
sect
ion.
(Cad
. = C
adav
eric
)
Liver Transpl. Author manuscript; available in PMC 2012 April 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Martin et al. Page 17
Tabl
e 4
Com
paris
on o
f Pat
ient
Sur
viva
l, G
raft
Surv
ival
and
Rej
ectio
n be
twee
n A
IH a
nd N
on-A
IH g
roup
s
Patie
nt S
urvi
val
Gra
ft Su
rviv
alR
ejec
tion
Haz
ard
Rat
iop-
valu
eH
azar
d R
atio
p-va
lue
Haz
ard
Rat
iop-
valu
e
AIH
vs.
Non
-AIH
Alo
ne0.
880.
6862
0.98
0.92
411.
140.
3307
Var
iabl
e A
djus
ted
for:
Live
r Dis
ease
Pre
sent
atio
n0.
740.
3573
0.87
0.54
951.
140.
3328
Era
of T
x0.
900.
7342
1.01
0.98
041.
200.
1952
Hei
ght D
efic
it at
Tx
1.16
0.64
951.
210.
4254
1.26
0.11
33
Wei
ght D
efic
it at
Tx
1.02
0.95
101.
120.
6283
1.19
0.21
52
War
m Is
chem
ia T
ime
0.76
0.44
630.
960.
8830
1.09
0.54
91
Age
At T
x0.
910.
7870
0.97
0.91
461.
130.
3823
Imm
unos
uppr
essi
on0.
880.
7017
1.10
0.69
381.
180.
2457
Org
an T
ype
0.91
0.79
371.
060.
8159
1.12
0.42
68
Don
or A
ge0.
770.
4409
0.88
0.59
871.
140.
3494
All
patie
nts >
1 y
ear o
f age
at t
rans
plan
t. V
aria
bles
as d
efin
ed in
met
hods
sect
ion
Liver Transpl. Author manuscript; available in PMC 2012 April 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Martin et al. Page 18
Table 5
Patient Characteristics and Outcome by AIH Subtype
AIH 1 AIH 2
n 60 9
Age (years) 13.4±0.5 (14.9) 11.1±1.9 (14.3)
Female (%) 63.3 77.8
Height SD 0.03±0.24(0.004) −0.2±0.6 (0.1)
Weight SD 0.5±0.2 (0.6) 0.6±0.5 (0.7)
Bilirubin Total (umol/L) 144.8±23.8(74.4) 237.7±83.1(109.4)
INR 2.0±0.1 (1.7) 2.5±0.6(1.6)
Fulminant presentation (%) 40 66.6
Chronic presentation (%) 60 33.3
PELD at transplant 11.8±1.6(10.6) 15.1±7.2 (11.3)
Early acute rejection (%) 36.7 33.3
Late acute rejection (%) 36.7 11.1
Steroid-resistant rejection (%) 16.7 22.2
Chronic rejection (%) 6.7 0
Data displayed as mean±SE (median) or percentage.
Liver Transpl. Author manuscript; available in PMC 2012 April 1.