persistence of viral replication after anti-hbe seroconversion during antiviral therapy for chronic...
TRANSCRIPT

Journal of Hepatology 2000; 32: 307-316 Printed in Denmark . All rights raewed Mmksgaard . Copenhagen
Copyright Q European Association for the Study of the Liver 2000
Journal of Hepatology ISSN 0168-8278
Persistence of viral repletion after anti43Be seroconversion during antiviral therapy for chronic hepatitis B
Christian Pichoud’, Franqoise Berby’, Lieven Stuyver3, Marie-Anne Petit4, Christian Trepo172 and
Fabien Zoulim’>2 ‘~NSERM Unit 271, and 2Liver Unit, H&e1 Dieu, Lyon, Frame, 3~~noge~etics, Ghent, Belgium, and 4Centre Htipato-Biliaire Paul Browse,
CR INSERM 98-04, Villejuif; France
Background/Aims: Hepatitis B virus genome mutants may be selected during the ~rnun~rn~iat~ clear- ance of infection or during long-term nucleoside ana- log administration and may escape both antiviral pressures. The pattern of anti-HBe seroconversion was analyzed in patients receiving new nucleoside ana- logs, l~i~dine or famciclovir, in comparison with patients treated with interferon alpha. M&-M&: Eighteen consecutive patients who serocon- verted to anti-HBe were included in the study. Serial serllll;l samples were studied with the quantitative de- termination of HBV DNA by the branched DNA as- say (Chiron) and by a quantitative PCR assay (Roche diagnostics), determination of pre-Sl Ag, the genetic analysis of the viral genome with the determination of pre-core promoter or pre-core region mutations with a line probe assay (Innogenetics) and, in selected sampks of polymerase gene mutations Results: The quantitative PCR assay was found to be
HRONIC C hepatitis B remains a major health prob- lem worldwide, due to a high prevalence (300 mil-
lion) of chronic carriers of hepatitis B virus (HBV) and the clinical consequences of the disease including liver cirrhosis and hepatocellular carcinoma (1). HBV is not a cytopathogenic virus and i~une-mediated viral clearance is frequently associated with a flare of hepa- titis, reflecting lysis of infected hepatocytes ac- companied by a pronounced decrease of replication
Received 16 April; revised 22 June; accepted 27 June 1999
Correspondence: Fabien Zoulim, INSERM Unit 271, 151 cours Albert Thomas, 69003 Lyon, France. Tel: 33 4 72 68 19 70. Fax: 33 4 72 68 19 71. e-mail: zoulim@lyonl5l .inserm.fr
more sensitive than the bDNA assay, allowing a 2-5- log decrease in viral DNA levels to be demonstrated after anti-HBe seroconversion. Viral persistence after anti-HBe seroconversion induced by interferon, lami- vudine or famciclovir, was often associated with circu- lating HBV genomes harboring mutations in the pre- core promoter. The clinical significance of these find- ings was demonstrated by the observation of reversion to HBeAg in two patients treated with interferon and one with lamivndine. Conclusion: Persistence of significant levels of vi- remia that are not detected by the branched DNA as- say may be observed after anti-HBe seroconversion. A precise monitoring of viremia levels with more sen- sitive assays and HBV mutant strains is warranted in patients undergoing antiviral therapy.
Key words: Antiviral therpay; Hepatitis B virus; Im- mune response; Pre-core mutants; Viral resistance.
levels followed by anti-HBe seroconversion and sus- tained normalization of ALT levels (2). The rate of spontaneous anti-HBe seroconversion is estimated to be approximately 5% per year and to be significantly increased by interferon alpha therapy (3). However, under the pressure of spontaneous or interferon-in- duced anti-HBe immunity, HBV genomes that harbor nonsense, frameshift, or initiation codon mutations in the viral pre-core region that arrest the expression of HBe Ag without altering the replication capacity of the virus, may be selected (4). In HBe Ag negative carriers, the most frequently detected mutation is a nucleotide transition at the pre-core codon 28 which converts a UGG into a UAG stop codon (M2 mutant) which may also be associated with another mutation at codon 29
307

C. Pichoud et al.
that converts GGC to GAC (M4 mutant) (508). Other mutations in the pre-core promoter at nucleotide posi- tion 1762 and 1764 that decrease the promoter activity and the expression of HBeAg (9) have been described in both HBeAg positive and negative patients, but are thought to be selected at the time of anti-HBe serocon- version (10,ll). The course of viral infection after the emergence of HBe-minus variants remains a matter of controversy. Some studies showed the progression of chronic hepatitis and resistance of the mutated strains to interferon alpha therapy (12-15), while the results of other studies suggest a link with HBeAg clearance and remission of liver disease (16,17).
New hope in the treatment of chronic hepatitis B has been provided with the development of new antivirals which have shown a very potent antiviral effect in clin- ical trials. However, the kinetics of viral replication and the lack of anti-HBe response in the majority of the patients imply a prolonged administration of antivirals to eradicate or control viral infection (18,19). Such long-term antiviral treatment with a single nucleoside analog has been associated with the selection of poly- merase gene-resistant mutants that are resistant to the polymerase inhibitor in 23% of the patients after 12 months of therapy and in 38% after 24 months (18). La~vudine-~sistant mutants harbor mutations within the very conserved C domain in the YMDD motif of the reverse transcriptase (M552V or M5521) that con- fer a decreased sensitivity to therapy (20). These are very frequently associated with mutations in the B do- main of the reverse transcriptase L528M (21). Fam- ciclovir-resistant strains mainly harbor mutations in the B domain of the reverse transcriptase which may be cross resistant with lamivudine (22). The selection of such mutants is often associated with viral persist- ence and the progression of liver disease (23,24). In a group of patients who have the capacity to mount a vigorous antiviral immune response, anti-HBe serocon- version may be favored by antiviral therapy. This anti- HBV immune response may help to withdraw antiviral therapy prior to the emergence of viral polymerase gene-resistant mutants.
We therefore decided to study the molecular pat- terns of anti-HBe seroconversion in 18 consecutive pa- tients who seroconverted during lamivudine, famciclo- vir, or interferon therapy. We focused our attention on the determination of viremia levels with sensitive methods and on the determination of pre-core and polymerase genes sequences to survey the selection of pre-core and/or polymerase gene mutants that may es- cape both the anti-HBe immune response and the anti- viral pressure of drug therapy. Interestingly, the results of our investigation revealed new features of anti-HBe
sero~onversion in patients treated with nucleoside ana- logs. Indeed, pre-core promoter mutants were found to persist at low levels despite this combined antiviral pressure which may favor the emergence of polymerase mutants that are resistant to antiviral agents.
Patients and Methods Patients Eighteen consecutive patients who were followed in our liver depart- ment and seroconverted to anti-HBe were studied. All patients were positive for HBeAg in serum at the beginning of the study and suffer- ed from liver biopsy-proven chronic hepatitis B (12 with chronic active hepatitis, and six with active cirrhosis). The mode of transmission was sexual in two, professional in two, IV drug addiction in one, in- trafamilial or vertical in five, nosocomial or transfusion in three, and unknown in five. Patients were followed monthly for serum ALT levels (expressed in comparison with the upper limit of normal values (ULN)), and bi-monthly for HBeAg, anti-HBe, and HBV DNA in serum. Anti-HBe seroconversion was demonstrated by virological monitoring of the patients during follow-up. Among these 18 sero- converters, six patients received famciclovir in phase II and phase III clinical trials, five received lamivudine for compassionate use, five received interferon alpha, one patient received interferon alpha fol- lowed by Intone, and,one patient received no treatment and spon- taneously seroconverted to anti-HBe. Serum samples were prospect- ively stored at -20°C. Samples were then retrospectively selected for further virological studies at relevant time points, i.e., prior to ther- apy, at the time of anti-HBe seroconversion, after seroconversion and in some patients at the time of reversion to HBeAg. A total of 79 samples (mean of 4.4 samples per patient; range: 3 to 7 per patient) were submitted to detailed virological analysis including the quanti- tative determination of serum viral DNA and pre-SlAg, and the de- tection of pre-core mutants. Analysis of the viral polymerase gene sequence was performed on selected samples.
Viral markers in serum and assessment of response to therapy Viral markers including HBsAg, HBeAg and anti-HBe were deter- mined routinely in the serum of the patients by standard procedure (Monolisa, Pasteur, France and EBK, Sorin, Italy, respectively). Quantitative determination of viral DNA in serum was performed by the branched DNA assay (Quantiplex, Chiron, USA) according to manufacturer’s instructions. The limit of detection of this assay is 0.7 106 viral genomes equivalent per mL (25,26).
In parallel, in selected stored serum samples, HBV DNA levels were assessed with a quantitative PCR assay (~plicor~ HBV monitor test, Roche Diagnostics). Briefly, 50 ~1 of serum were pre- pared by p~trea~ent with pol~thylene glycol, alkaline lysis of the pelleted viral particles, and neutralization of the lysate. After adding a fixed amount of internal standard and a PCR mix, 30 cycles of PCR amplification were performed following the manufacturer’s in- structions. Biotinylat~ ampiicons were captured on streptavidine- coated microwells and hybridized with specific dinitrophenyl-labeled oiigonucl~tide probes. Following incubation with alkaline phospha- tase conjugated anti-DNP antibodies and a calorimetric substrate, a kinetic of 0.D. determination together with a calibration curve allowed a quantitative determination of HBV DNA levels. The limit of detection of this PCR assay is 400 copies of viral genome per ml, and quantitation is linear up to 4.107 copies per ml (27,28).
Pm-SlAg levels in serum were assessed with a previously published radioimmunoassay using a polyclonai anti-HBsAg for capture of HBV particles and either a monoclonal antibody against pre-SlAg or against HBsAg. A semi-quantitative determination of the pre- SlAg was allowed by the calculation of the pre-SlAg/HBsAg signals as described in detail elsewhere (29,30).
Analysis of HBV genome sequences Isolation of viral DNA for sequence analysis was performed with standard procedures. Two hundred microliter serum samples were in-
308

New patterns of anti-HBe seroncanversion
cubated for 4 h at 37°C in a buffer (50 mM Tris, 25 mM NaCI, 2.5 mM EDTA, 0.5% SDS) contai~ng 0.8 mglml Proteinase K, followed by phenol-chloroform extraction and precipitation with ethanol. The pellet was resuspended in 20 ~1 Hz0 and used for PCR amplification.
Defection of pre-core mutants and determination of viral genotypes In order to detect the variability of the viral genome at codon 28 and 29 of the pre-core region, a research line probe assay (LiPA) was designed with specific probes covering the following motifs: (i) 28W- 29G (wild type); (ii) 28X-29G (mutant M2); (iii) 28W-29D (mutant M4); and (iv) 28X-29D (double mutant M2-M4). In addition, two specific probes for the pre-core promoter region covering the import- ant variability at nucleotides 1762 and 1764 were also designed. Probes were applied on a nitrocellulose membrane as described (31). HBV pre-core region was amplified from a 10 pl aliquot of serum DNA extract, with biotinylated primers HBPr8: S-GAA GGA AAG AAG TCA GAA GGC-3’ (antisense) and HBPr69: 5’-ACA TAA GAG GAC TCT TGG AC-3’ (sense). Primer pair HBPr70: 5’- TAC TTC AAA GAC TGT GTG TTT A-3’ (sense), and HBPr7: S-CTC CAC AGT AGC TCC AAA TTC-3’ (antisense) was used in a set- ound round of amplification for nested PCR when required. LiPA test performance was identical as described for INNO-LiPA HCV II (31). Viral genotypes were also determined by LiPA after amplifi- cation of the S gene and hybridization of the PCR products on 18 specific probes allowing the determination of the 6 HBV genotypes {A to F) as described in detail elsewhere (32). In nine patients, genotype determination was confirmed by sequence analysis of the viral poly- merase gene.
Determination of viral polymerase gene sequence The DNA sequence of the polymerase gene from selected patients, who received either famciclovir or lamivudine therapy and remained positive for serum HBV DNA after anti-HBe seroconversion by the quantitative PCR assay, was determined directly from PCR products. HBV polymerase sequence from a.a. 490 to 631 (nucleotide position 596 to 1016), which includes domains B and C of the viral reverse transcriptase, was analyzed as described elsewhere (33). One tenth of extracted DNA was amplified in a 50 ~1 reaction containing 50 mM KCl, 10 mM Tris-HCl, 1.5 mM MgClz, 0.2 mM of each dNTP 1 unit of Taq polymerase (Perkin Elmer), and 1 pM of each primer (gl: 5’- CCT GCT GGT GGC TCC AGT TC-3’ at nucleotide oosition 55- 76, and primer pR5: 5’-GGT TGC GTC AGC AAA dAC TTG-3’ at position 1197-l 178, were used for amplification of the conserved domains A to E of the viral polymerase gene. A nested PCR was performed on some samples, that did not give a successful amplifi- cation, using primers p4 5’-CTC ACA ATA CCC CAG AGT CTA GAC T-3’ at nucleotide position 23&254 and pR2: 5’-AAA GCC CAA AAG ACC CAC AAT’-3’ at position 1017-997. For each round of PCR, 30 cycles of amplification were performed with denaturation at 95°C for 1 min, annealing at 5O’C for 1 min, and extension at 72’C for 2 min. Viral DNA sequence analysis was performed directly on amplification products using primer p4 and automated sequence ana- lyzer.
Results Basefine characteristics of the seroconverters Virological findings at baseline are described in detail in Table 1. ALT levels were elevated in all cases (mean ALT levels: 4.76xULN; range: 1.429.8xULN) at baseline. HBeAg was positive in all patients while anti- HBe could be detected together with HBeAg in two. The pre-SlAg/HBsAg ratio was found to be higher than 7% in all but one patient who harbored a low level viremia at baseline (case #14). The mean serum viral DNA levels were 1071.28X lo6 equivalent ge-
names/ml (range: CO.7 to 5000X106 equivalent ge- name/ml) with the branched DNA assay Viral DNA levels ranged from 20844 to >40X106 copies/ml with the quantitative PCR assay. Distribution of viral geno- types was comparable to that of a large cohort of HBeAg positive patients followed in our liver depart- ment (unpublished results). Genotype A was more prevalent (nine patients), followed by genotype D (six patients), genotype C (two patients) and genotype B (one patient). The geographical origin of the patients was Asia in four (infected with genotype B in one, genotype C in two and genotype D in one), Mediter- anean Basin in one (genotype D) and France in 13 (genotype D in four and genotype A in nine). Determi- nation of pre-core mutant showed the presence of a pre-core promoter mutant (either pure or as a mixture) in nine patients, and of pre-core M2 mutant in two. The seven other patients were infected with “pure” wild-type sequences in the pre-core region.
Immure-mediated anti-HBe seroconversion Six seroconverters received interferon alpha therapy at a dose of 5 megaunits thrice weekly for 6 months (five patients) or 18 months (one patient); one patient sero- converted spontaneously. Anti-HBe seroconversion oc- curred after 2 (one patient), 4 (two patients), and 6 (one patient) months of interferon therapy while in two patients it occurred 4 and 12 months after cessation of therapy (Table 2 and Fig. 1). Anti-HBe seroconversion was associated with a return of ALT to normal values in all seven cases. A drop in viral DNA titers was ob- served in all cases, viral DNA became undetectable by the bDNA assay in each case, and decreased dramati- cally in the quantitative PCR assay by 2 to 5 logs. However, in all cases serum viral DNA remained posi- tive at relatively low titers ranging from 829 to 257 143 copies/ml in the PCR assay. In four patients initially infected with a pre-core promoter mutant, a progress- ive replacement of mutant virus populations by wild- type viruses occurred after anti-HBe seroconversion in 2 (cases #4 and 6) (Fig. 1), while in the two others mutant virus persisted after seroconversion (cases #5 and 7) (Table 2).
In patient #5, interferon therapy was followed by a maintenance therapy with lamivudine. Seven months after anti-HBe seroconversion, while the patient was still under lamivudine maintenance therapy, low levels of viremia were still detectable by the quantitative PCR assay. Analysis of the pre-core region showed a mixture of pre-core promoter mutant and wild-type genomes. Viral polymerase gene sequence by direct sequencing of PCR products, after seroconversion while the pa- tient was still under lamivudine treatment, showed 3
309

C. Pichoud et al.
TABLE 1
Baseline characteristics of the patients
Patient Treatment ALT HBeAglHBeAb Pre-SlIHBs bDNAa PCRa Genotype Promoter cd28-29 ratio
#I
#2 #3 #4 #5 #6 #I
#8 #9 #lO #I1 #12
#13 #14 #15
#16 #17 #18
NO 2.3 +I-
IFN 2.6 i-l- IFN 2.9 +I- IFN 2.0 -+-I-+ IFN-+LAM 29.8 +I- IFN 3.9 +I- IFN 1.7 +I-
LAM 2.4 +I- LAM 1.4 +I- LAM 3.6 +I+ LAM 5.2 +I- LAM 2.6 +I-
FAM 2.3 +I- FAM 2.3 +I- FAM 7.1 +I-
FAM 1.7 +I- FAM 2.4 +I- FAM 9.6 +I-
44% 22.8
58% 833.1 30% 19.4 ND 1.1 11% 3459 18% 1767.0 ND 1040.0
6 384 336 D
>40000000 A 1038655 C
237911 C 39272 851 D
>40000000 A >40000000 B
INDb WT+M2
WT WT MT MT MT MT
WT w-r w WT w-r WT
9% 313.7 4820860 D WT WT 29% 22.0 3 597948 A w-r WT
1% 119.0 >40000000 D WT WT+MZ 17% 5000 >40000000 D MT WT 23% 46.0 33 904460 A MT WT
28% 4960.0 3% co.7
28% 1188.0
26 796478 A 20844 D
>40 000 000 A
1225 198 A 337637 A
>40000000 A
WT+MT WT+MT WT
15% 15% 33%
co.1 co.7 490.0
WT WT MT
w w-r WT
WT wl- WI-
a Results of HBV DNA detection by the bDNA assay are expressed in lo6 equivalent genome per ml and those obtained with the quantitative PCR assay are expressed in genome copies per ml. b IND indicates an indeterminate reaction (no hybridization) on probes for the promoter region. Mutations in the pre-core region or promoter are indicated in italics.
TABLE 2
Characteristics of the patients at the end of follow-up
Patient Treat- Time after ALT HBeAg/ Pre-Sll bDNA” PCRa Promoter cd28-29 Polymerase ment seroconversion HBeAb HBs ratio
#l
#2 #3 #4 #5
#6 #I
#8 #9 #lO #ll #12 #12
#13 #I4 #15
#16 #17 #18
NO 52 MO
IFN 12 MO IFN 19 MO IFN 15 MO IFN 26 MO -+LAM IFN 3 MO IFN 15 MO
LAM 10 MO LAM 5Mo LAM 12 MO LAM 13 MO LAM 5 MO LAM reversion
FAM 13 MO FAM 7Mo FAM 5Mo
FAM 10 MO FAM 9Mo FAM 6Mo
1.0 -1-k 12% co.7
1.0 -I+ 13% co.7 1.0 -I+ 8% <0.7 1.0 -/+ ND co.7 1.0 -1-k 3% <0.7
1.0 1.0
1.0 1.0 1.0 1.0 1 2.54
1.0 1.0 1.0
1.0 1.0 1.0
-1-k 7% +I+ ND
-Ii- 5% -I+ 0% -1-k 0% -I+ 21% -I+ 30% +-I- 18%
-1-k 18% -I+ 0% -I+ 11%
-1-k 7% -1-t 4% -I-+ 18%
co.7 17 568 WT WT
523.2 13272607 MT WT
co.7 co.7 co.7 co.7 co.7
8.6
CO.7 co.7 co.7
<0.7 CO.1 co.7
6523 WT+MT WT wild type <400 WI-+MT WT ND 2471 WI- WT+M2 wild type
888 WT+MT WT wild type 412 W’C+MT WT ND
4 192 671 MT WT L528MIM552 V
48 231 W+MT WT wild type <4Oo w WT wild type
922 WF+MT WT+MZ wild type
7899 w-r WT+M4 R471K 1694 WT+MT WT wild type
<400 w-r WT ND
<400 WT WT+M2
194 199 WT WT 8385 WT WT
829 WT WT 894 W-I-+-MT w-r S441CN483Dl
S565A
a Results of HBV DNA detection by the bDNA assay are expressed in lo6 equivalent genome per ml and those obtained with the quantitative PCR assay are expressed in genome copies per ml. ND: not determined. Mutations in the pre-core region or promoter as well as in the polymerase gene are indicated in italics.
amino acid changes S441C, Y4834 S565A by com- rus and stable seroconversion, no selection of pre-core
parison with the consensus sequence of genotype D. mutant was observed after anti-HBe seroconversion
In the two patients infected with pure wild-type vi- (cases #2 and 3). In the remaining patient infected with
310
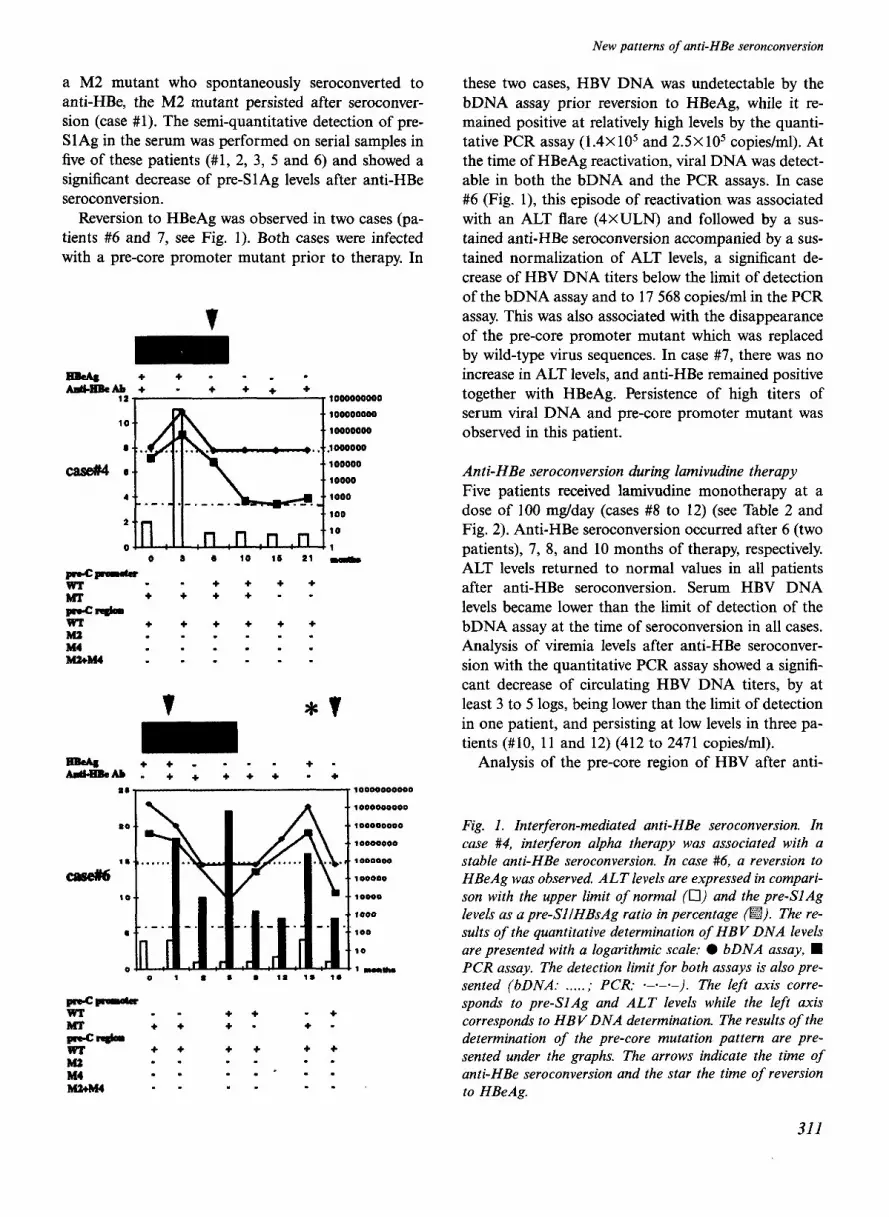
a M2 mutant who spontaneously seroconverted to anti-HBe, the M2 mutant persisted after seroconver- sion (case #l). The semi-quantitative detection of pre- Sl Ag in the serum was performed on serial samples in five of these patients (#l, 2, 3, 5 and 6) and showed a significant decrease of pre-Sl Ag levels after anti-HBe seroconversion.
Reversion to HBeAg was observed in two cases (pa- tients #6 and 7, see Fig. 1). Both cases were infected with a pre-core promoter mutant prior to therapy. In
WEBe +- -* - !Ab, - + + + +
12- ~1002002000
. 100000000 .
.. 10000000
.’ 100000
.’ 10000
.’ 100
0 2 b 10 12 21
t *t
++. -.- + - =fi.+++++ -+
‘
New patterns of anti-HBe seronconversion
these two cases, HBV DNA was undetectable by the bDNA assay prior reversion to HBeAg, while it re- mained positive at relatively high levels by the quanti- tative PCR assay (1.4X lo5 and 2.5X lo5 copies/ml). At the time of HBeAg reactivation, viral DNA was detect- able in both the bDNA and the PCR assays. In case #6 (Fig. l), this episode of reactivation was associated with an ALT flare (4XULN) and followed by a sus- tained anti-HBe seroconversion accompanied by a sus- tained normalization of ALT levels, a significant de- crease of HBV DNA titers below the limit of detection of the bDNA assay and to 17 568 copies/ml in the PCR assay. This was also associated with the disappearance of the pre-core promoter mutant which was replaced by wild-type virus sequences. In case #7, there was no increase in ALT levels, and anti-HBe remained positive together with HBeAg. Persistence of high titers of serum viral DNA and pre-core promoter mutant was observed in this patient.
Anti-HBe seroconversion during lamivudine therapy Five patients received lamivudine monotherapy at a dose of 100 mg/day (cases #8 to 12) (see Table 2 and Fig. 2). Anti-HBe seroconversion occurred after 6 (two patients), 7, 8, and 10 months of therapy, respectively. ALT levels returned to normal values in all patients after anti-HBe seroconversion. Serum HBV DNA levels became lower than the limit of detection of the bDNA assay at the time of seroconversion in all cases. Analysis of viremia levels after anti-HBe seroconver- sion with the quantitative PCR assay showed a signifi- cant decrease of circulating HBV DNA titers, by at least 3 to 5 logs, being lower than the limit of detection in one patient, and persisting at low levels in three pa- tients (#lo, 11 and 12) (412 to 2471 copies/ml).
Analysis of the pre-core region of HBV after anti-
Fig. 1. Interferon-mediated anti-HBe seroconversion. In case #4, interferon alpha therapy was associated with a stable anti-HBe seroconversion. In case #6, a reversion to HBeAg was observed. ALT levels are expressed in compari- son with the upper limit of normal (0) and the pre-SlAg levels as a pre-SlIHBsAg ratio in percentage (m). The re- sults qf the quantitative determination of HBV DNA levels are presented with a logarithmic scale: l bDNA assay, n PCR assay. The detection limit for both assays is also pre- sented (bDNA: . . . . . ; PCR: *-*-a-). The left axis corre- sponds to pre-SlAg and ALT levels while the left axis corresponds to HBV DNA determination. The results of the determination of the pre-core mutation pattern are pre- sented under the graphs. The arrows indicate the time of anti-HBe seroconversion and the star the time of reversion to HBeAg.
311

C. Pichoud et al.
++++++... ._..-
-Ab . . . a . -+++ +++++
26
20
case#9 IS
t0 _._._._.
6
0 0 2 a 4 5 7 2 9 101112i31217
y-p-~ +
+ +
MI: + +
- P-cd= wr +
E M2+M4 :
+ + . .
.
+++++..- + - - -- ++++,,,,i_,
10000000
,.I 000000
100000
10000
1000
100
10
.l
+ M2 M4 M2+M4
+ + - . + +
+ + + . - _ . - .
- .
Fig. 2. Lamivudine-associated anti-HBe seroconversion. In case #9, lamivudine therapy was associated with a stable anti-HBe seroconversion. In case #12, a reversion to HBeAg was observed while the patient was still receiving lamivudine. The legend is the same as in Fig. 1. Results of polymerase gene sequencing at the time of viral break- through are also indicated.
HBe seroconversion showed: (i) the co-existence of wild-type and pre-core promoter mutant viruses, sug- gesting a progressive replacement of mutant virus by wild-type sequence genomes (patients #ll and 12); (ii) and the slow appearance of pre-core promoter mutant virus population together with wild-type virus in the
two patients initially infected with “pure wild type vi- rus” (cases #8 and 9). In patient #lo, wild-type pro- moter sequence and a mixture of wild type and M2 sequences in the pre-core region were found to be stable after anti-HBe seroconversion.
Determination of pre-Sl Ag levels in the serum of these five patients showed a significant decrease of pre- Sl Ag in cases #8, 9, and 10 after seroconversion and the persistence of stable levels in cases #l 1 and 12. The persistence of high levels of pre-SlAg was associated with the persistence of low levels viremia in case #ll and with a reversion to HBeAg in case #12.
One case of reversion to HBeAg was observed al- though lamivudine therapy was maintained (case #12, Fig. 2). In this patient reversion was observed 10 months after anti-HBe seroconversion. It was associ- ated with the persistence of pre-core promoter mutant viruses and a double mutation in the viral polymerase with a L528M and a M552V changes. These data indi- cate that viral strains harboring mutations in the pre- core promoter and the viral polymerase gene can be selected in the context of anti-HBe immune response and lamivudine therapy.
The viral polymerase gene sequence was also ana- lyzed in two other patients in whom viremia was still detectable after seroconversion (patients #lO and 11). Direct sequencing of PCR products showed a wild-type sequence in domains B and C of the viral polymerase, indicating the absence of selection of lamivudine resis- tant strains at the time of the study.
Anti-HBe seroconversion associated with famciclovir treatment Anti-HBe seroconversion was observed in six patients who received famciclovir therapy (Fig. 3 and Table 2). Seroconversion occurred after 4, 11 or 12 months of treatment during a 12.month administration of the antiviral in phase III clinical trials in three patients. In three other patients included in a phase II or III clin- ical trial, seroconversion was observed 2, 11 and 23 months after cessation of therapy.
In all three patients (cases #13 to 15) who serocon- verted during therapy, ALT levels returned to normal values after anti-HBe seroconversion, while HBV DNA titers were below the limit of detection of the bDNA assay and decreased by 3 to 5 logs with the PCR assay (HBV DNA range: <400 to 48 231 copies/ ml). At the end of follow-up two patients were infected with a mixture of wild-type and pre-core promoter mu- tants, and a mixture of M2 and wild-type strains at pre-core codon 28 was found in patient #15. Since low- level viremia persisted despite anti-HBe seroconversion and antiviral treatment in all three patients, sequence
312

New patterns of anti-HBe seronconversion
++++ --- - - - - +++
ai 1o(uIooooOb
lODOOO8OM $I
wooooooO
16 moo8oob
case#15 ao toooon
100000 16 WOO0
IO low
100 6
10
0 I
e_,oIza4y:)
+
$- . + +
+ + * M2 * . +
. . _ I
q t + ++++---- - Aatl.liUeAb * - * * * ++*+ +
58 mowwoa
wawooo 16
lwwoa
20 woeoo
caseM7 ‘5 toma faoB
10
100
6 10
+ + * M2 I .
M4 w I m MkM4 * . .
Fig. 3. F~c~c~ovir therapy and anti-HBe seroconversion. Patient #15 seroconverted to anti-HBe during antiviral therapy. Patient #17 seroconverted after cessation of treat- ment. The legend is the same as in Fig. 1. Results of poly- merase gene sequencing at the time of viral breakthrough are also indicated.
analysis of the viral polymerase gene was performed but did not reveal any mutation in the conserved do- mains of the reverse transcriptase.
Among the three patients (#16 to 18) who serocon- verted 2, 11 and 23 months after cessation of therapy, no ALT flare was observed during clinical monitoring
in 2 (cases #16 and 17). HBV DNA levels were below the limit of detection of the bDNA assay post-treat- ment. With the PCR assay the levels of viremia were 1225 198 and 337637 copies/ml. Both patients were in- fected with wild-type pre-core viruses. After anti-HBe seroconversion a significant decline in HBV DNA levels by 2 to 3 logs was observed with the PCR assay. In both cases a selection of a pre-core promoter mutant (case #17) or a M4 mutant (case #16) was observed alter anti-HBe seroconversion. In case #18, high levels of viremia were observed after cessation of famciclovir therapy associated with elevated ALT (9.6xULN). Anti-HBe seroconversion was observed 2 months after cessation of therapy and accompanied by a rapid de- cline of viral DNA levels, by more than 5 logs, below the limit of detection of the bDNA and the PCR as- says. Pre-core promoter mutants that were present prior to seroconversion were replaced by wild-type se- quences after anti-HBe seroconversion. Analysis of the evolution of pre-SlAg in these six patients showed a significant decrease of the pre-Sl AglHBsAg ratio after seroconversion.
Discussion In patients with chronic hepatitis B, anti-HBe serocon- version usually reflects an immune-mediated clearance of infected hepatocytes that actively replicate HBV and is associated with the control of viral replication and a remission of liver disease. The rate of spontaneous anti-HBe seroconversion is approximately 5% each year, and is significantly increased by interferon ther- apy (34) as well as therapy with new nucleoside analogs such as lamivudine (18) or famciclovir (35). However, the selection of viral pre-core promoter and/or pre-core region mutants may allow the persistence of viral repli- cation after anti-HBe seroconversion (4,6,17).
In our study of 18 consecutive seroconverters, using new quantitative methods for the detection of HBV DNA and the molecular characterization of circulating HBV genomes, we have observed new molecular fea- tures of anti-HBe seroconversion. Using a quantitative PCR assay (27,28), we could confirm that viral DNA titers not only drop after anti-HBe seroconversion by more than 2 logs but more ~portantly may persist below the detection limit of the bDNA assay at sig- nificant levels. Indeed, persistence of circulating viral DNA titers higher than 400 copies/ml was observed in 7/7 patients treated with interferon, in 4/5 treated with lamivudine, and 4/6 patients treated with famciclovir, while the bDNA assay could detect HBV genomes in only two patients after anti-HBe seroconversion. The discrepancy observed between the quantitative data in
313

C. Pichoud et al.
the bDNA and the PCR assays is due to the absence of a universal standard for the detection and quantifi- cation of HBV DNA (36). Since the linearity of the PCR assay is observed in samples containing HBV DNA levels below 100 000 copies/ml (27,28), its clinical value depends mainly on the detection of low levels of viremia (Pawlotsky et al., submitted manuscript). The clinical relevance of the detection of relatively low levels of viral replication was emphasized by the de- scription of reversion to HBeAg in two patients who received interferon therapy and one patient receiving lamivudine treatment. Interestingly, the significant de- crease of viral DNA titers after seroconversion was also associated with a relative decline in pre-SlAg levels in serum in patients with sustained anti-HBe seroconversion and control of viral replication, consist- ent with our previous observations (29,30,37). This in- dicates that the detection of pre-SlAg after anti-HBe seroconversion may be a marker of the persistence of a pool of infected hepatocytes that still harbor viral CCC DNA. In agreement with this hypothesis was the finding that pre-Sl Ag persisted at relatively high levels in two patients who reverted to HBeAg (#6 and 12), in one patient who experienced an increase in viral DNA titers together with the persistence of anti-HBe (#13), and in one patient whose viral DNA levels remained detectable after seroconversion despite lamivudine therapy (#ll).
Another particular finding came from the character- ization of viral genomes after anti-HBe seroconversion with a line probe assay for the study of the pre-core region and by sequencing of the viral polymerase gene in patients receiving nucleoside analog therapy In pa- tients receiving interferon alpha, the persistence of a pre-core promoter mutant was associated with a rever- sion to HBeAg in two cases, which may suggest that these mutants may escape the anti-HBe immune re- sponse (10) by modulating the level of HBeAg express- ion (9) and may re-emerge with an HBeAg positive phenotype (4). In patients who seroconverted during lamivudine therapy the persistence of pre-core pro- moter mutants in four out of five patients may suggest that these mutants do not only escape the anti-HBe immune response but may also be recalcitrant to nucle- oside analog therapy. In the three patients who sero- converted during famciclovir therapy, the same obser- vation of the persistence of pre-core promoter mutants was made, confirming the previous hypothesis. With regard to pre-core stop codon mutants (M2), no mu- tant was selected after seroconversion in this small series of interferon seroconverters, while M2 mutants persisted or were selected by the anti-HBe immune re- sponse in one case of lamivudine treatment and one
case of famciclovir treatment. Another interesting finding was the possibility of anti-HBe seroconversion after cessation of famciclovir therapy which was not associated with ALT flare in two of these three pa- tients. It remains to determine whether this phenom- enon of delayed anti-HBe seroconversion is indeed a specific feature of famciclovir treatment. Furthermore, in an additional group of 32 HBeAg positive patients who did not seroconvert to anti-HBe, no change in the pre-core sequence and pre-Sl Ag detection was ob- served (data not shown) (38), confirming the clinical relevance of our findings.
Reversion to HBeAg positivity was observed in three cases among this group of 18 consecutive seroconvert- ers, which underlines the need for careful monitoring of patients, even after anti-HBe seroconversion. HBV reactivation with the loss of anti-HBe and a reversion to HBeAg has been described in patients without im- mune suppression (39) and has been observed in clin- ical trials after cessation of lamivudine therapy (40,41). In our series, this serological event was observed in one patient during interferon treatment, and in one patient after cessation of interferon. More interestingly, we de- scribed the first case of HBeAg reversion in a patient who was still undergoing lamivudine therapy. In two of these cases HBV DNA was still detectable by the quantitative PCR assay, in two of two tested cases pre- SlAg levels remained at significant levels suggesting the persistence of a pool of infected hepatocytes de- spite anti-HBe immune response, and in the three cases a persistence of pre-core promoter mutants was ob- served suggesting that these mutants can escape the anti-HBe immune response. In the case treated with lamivudine, analysis of HBV polymerase gene showed a selection of a double mutant L528M + M552V (20). These findings may indicate a progressive and sequen- tial selection of a pre-core promoter mutant after anti- HBe seroconversion followed by the selection of poly- merase mutant resistant to lamivudine.
Altogether our findings emphasize the need to moni- tor viral replication after anti-HBe seroconversion with more sensitive and quantitative assays. Furthermore, during nucleoside analog therapy, not only sensitive as- says to measure the level of viremia but assays to detect viral mutants are required to predict the selection of viral strains that may escape both the immune response and the inhibition by antiviral therapy. These assays will be important to tailor antiviral strategies to the virological status of the patients.
Acknowledgements We are grateful to Dr Frederic Eberle (Roche Dia- gnostics, France) for providing the quantitative PCR
314

assays. This work was supported by grants from IN- SERM, the “Hospices Civils de Lyon”, and Smith Kline Beecham Pharmaceuticals.
References 1. Lee WM. Hepatitis B virus infection. N Engl J Med 1997; 337:
173345. 2. Hoofnagle JH, Shafritz DA, Popper H. Chronic type B hepatitis
and the healthy HBs Ag carrier state. Hepatology 1987; 7: 758- 63.
3. Hoofnagle JH, Di Bisceglie AM. The treatment of chronic viral hepatitis. N Engl J Med 1997; 336: 347-56.
4. Gunther S, Fischer L, Pult I, Sterneck M, Will H. Naturally oc- curing variants of hepatitis B virus. Adv Virus Res 1999; 52: 25- 137.
5. Carman W, Hadziyannis S, MC Garvey MJ, Jacyna M, Karayi- annis P, Makris A, et al. Mutation preventing formation of hepa- titis B e antigen in patients with chronic hepatitis B infection. Lancet 1989; ii: 588-91.
6. Okamoto H, Yotsumoto S, Akahane Y, Yamanaka T, Miyazaki Y, Sugai Y, et al. Hepatitis B viruses with precore region defects prevail in persistently infected hosts along with seroconversion to the antibody against e antigen. J Virol 1990; 64: 1298-303.
7. Tong S, Li J, Vivitski L, Trepo C. Active hepatitis B virus repli- cation in the presence of anti-HBe is associated with viral vari- ants containing an inactive pre-C region. Virology 1990; 176: 596603.
8. Lok A, Akarca U, Greene S. Mutations in the pre-core region of hepatitis B virus serve to enhance the stability of the secondary structure of the pregenome encapsidation signal. Proc Nat1 Acad Sci USA 1994; 91: 4077-81.
9. Buckwold VE, Xu Z, Chen M, Yen TSB, Ou J-H. Effects of a naturally occurring mutation in the hepatitis B virus basal core promoter on precore gene expression and viral replication. J Virol 1996; 70: 5845-51.
10. Okamoto H. Tsuda F. Akahane Y. Suaai Y. Yoshiba M. Moriva- , a
ma K, et al. Hepatitis B virus with mutations in the core pro- moter for an e antigen-negative phenotype in carriers with anti- body to e antigen. J Virol 1994; 68: 8102-10.
11 Gunther S, Piwon N, Iwanska A, Schilling R, Meisel H, Will H. Type, prevalence, and significance of core promoter/enhancer II mutations in hepatitis B viruses from immunosuppressed patients with severe liver disease. J Virol 1996; 70: 8318-31.
12. Gunther S, Paulij W, Meisel H, Will H. Analysis of hepatitis B virus populations in an interferon-alpha-treated patient reveals predominant mutations in the C-gene and changing e-anti- genicity. Virology 1998; 244: 14660.
13. Fattovich G, Brollo L, Alberti A, Ponisso P Giustina G, Realdi G. Long-term follow-up of anti-HBe-positive chronic active hepatitis B. Hepatology 1988; 8: 16514.
14. Brunetto M, Giarin M, Oliveri F, Chiaberge E, Baldi M, Alfar- ano A, et al. Wild-type and e antigen-minus hepatitis B viruses and course of chronic hepatitis. Proc Nat1 Acad Sci USA 1991; 88: 418690.
15. Zhang X, Zoulim F, Habersetzer F, Xiong S, Trepo C. Analysis of hepatitis B virus genotypes and pre-core region variability during interferon treatment of HBe antigen negative chronic hepatitis B. J Med Virol 1996; 48: 8-16.
16. Lok ASF, Akarca US, Greene S. Predictive value of precore hepa- titis B virus mutations in spontaneous and interferon-induced hepatitis B e antigen clearance. Hepatology 1995; 21: 19-24.
17. Chan HL, Hussain M, Lok AS. Different hepatitis B virus geno- types are associated with different mutations in the core promoter and precore regions during hepatitis B e antigen seroconversion. Hepatology 1999; 29: 97684.
18. Lai CL, Chine RW, Leung NWY, Chang TT, Guan R, Tai DI, et al. A one year trial of lamivudine for chronic hepatitis B. N Engl J Med 1998; 339: 61-8.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
New patterns of anti-HBe seronconversion
Nowak M, Bonhoeffer S, Hill A, Boehme R, Thomas H, McDa- de H. Viral dynamics in hepatitis B virus infection. Proc Nat1 Acad Sci USA 1996; 93: 4398402. Zoulim F, Trepo C. Drug therapy for chronic hepatitis B: anti- viral efficacy and influence of hepatitis B virus polymerase muta- tions on the outcome of therapy. J Hepatol 1998; 29: 15168. Allen MI, Deslauriers M, Andrews CW, Tipples GA, Walters KA, Tyrell DLJ, et al. Identitication and characterization of mutations in hepatitis B virus resistant to Lamivudine. Hep- atology 1998; 27: 167(r7. Aye TT, Bartholomeusz A, Shaw T, Bowden S, Breschkin A, McMillan J, et al. Hepatitis B virus polymerase mutations during antiviral therapy in a patient following liver transplantation. J Hepatol 1997: 1148-53. Locarnini SA, Aye TT, Shaw T, De Man R, Angus PW, McCaughan GW, et al. The emergence of famciclovir resistant mutations in the hepatitis B virus polymerase during therapy fol- lowing liver transplantation. Hepatology 1997; 26(NO4 Pt2): ab- stract 958. de Man RA, Bartholomeusz AI, Niesters HGM, Zondervan PE, Locarnini SA. The sequential occurrence of viral mutations in a liver transplant recipient re-infected with hepatitis B: hepatitis B immune globulin escape, famciclovir non-response, followed by lamivudine resistance resulting in graft loss. J Hepatol 1998; 29: 669-75. Habersetzer F, Zoulim F, Jusot JF, Zhang X, Trabaud MA, Chev- allier P, et al. Clinical evaluation of the branched DNA assay for hepatitis B virus DNA detection in patients with chronic hepa- titis B lacking hepatitis B e antigen and treated with interferon alpha. J Viral Hepatitis 1998; 5: 407-14. Zaaijer H, ter Borg F, Cuypers H, Hermus M, Lelie P Compari- son of methods for detection of hepatitis B virus DNA. J Clin Microbial 1994; 32: 2088-91. Kessler HH, Pierer K, Dragon E, Lackner H, Santner B, Sttinzer D, et al. Evaluation of a new assay for HBV DNA quantitation in patients with chronic hepatitis B. Clin Diagn Virol 1998; 9: 37-43. Gerken G, Gomes J, Lampertico E Colombo M, Rothaar T, Trippler M, et al. Clinical evaluation and applications of the amplicor HBV monitorTM test, a quantitative HBV DNA PCR assay. J Virol Methods 1998; 74: 15565. Petit M, Zoulim F, Berthillon P, Cape.1 F, Li J, Dauguet C, et al. PreSl antigen/antibody patterns following interferon therapy in acute and chronic hepatitis B. J Hepatol 1994; 20: 47-56. Petit M, Zoulii F, Cape1 F, Dubanchet S, Dauguet C, Tmpo C. Variable expression of pre-Sl antigen in serum during chronic hepatitis B virus infection: an accurate marker for the level of hepatitis B virus replication. Hepatology 1990; 11: 809-14. Stuyver L, Wyseur L, van Arnhem W, Hernandez E Maertens G. A second generation line probe assay for hepatitis C virus. J Clin Microbial 1996; 34: 225966. Van Geyt C, De Gendt S, Rombout A, Wyseur A, Maertens G, Rossau R, et al. A line probe assay for hepatitis B virus geno- types. In: Schinazi RFS, Sommadossi J-P, Thomas HC, editors. Therapies for Viral Hepatitis. London: International Medical Press. p. 13945. Pichoud C, Seigntres B, Wang Z, Trepo C, Zoulii E Transient selection of a hepatitis B virus polymerase gene mutant associ- ated with a decreased replication capacity and famciclovir resis- tance. Hepatology 1999; 29: 230-7. Perillo R, Schiff E, Davis G, Bodenheimer HC, Lindsay K, Payne J, et al. A randomized, controlled trial of interferon alfa-2b alone and after prednisone withdrawal for the treatment of chronic hepatitis B. N Engl J Med 1990; 323: 295-301. Tmpo C, Jezek E Atkinson G, Boon R. Efficacy of famciclovir in chronic hepatitis B: results of a dose fmding study. Hepatology 1996; 24: 188A (abstract 247). Butterworth LA, Prior SL, Buda PJ, Faoagali JL, Cooksley WG. Comparison of four methods for quantitative measurement of hepatitis B viral DNA. J Hepatol 1996; 24: 68691.
315

C. Pichoud et al.
37. Zoulim F, Mimms L, Floreani M, Pichoud C, Chemin I, Kay A, et al. New assays for quantitative determination of viral markers in management of chronic hepatitis B virus infection. J Clin Microbial 1992; 30: 1111-9.
38. Grandjacques C, Pradat P Stuyver L, Chevallier M, Chevallier P, Pichoud C, et al. Rapid detection of mutations in the promoter and the pre-core region of HBV genome: correlation with viral persistence and disease activity. Hepatology 1998; 28(4 ($2)): ab- stract 294.
39. Davis GL, Hoofnagle JH, Waggoner JG. Spontaneous macti- vation of chronic hepatitis B virus infection. Gastroenterology. 1984; 86: 23&5.
40. Honkoop P De Man RA, Heijtink RA, Schahn SW. Hepatitis B reactivation after lamivudine. Lancet 1995; 346: 11567.
41. Nevens F, Main J, Honkoop P Tyrrell DL, Barber J, Sullivan MT, et al. Lamivudine therapy for chronic hepatitis B: a six month randomized dose-ranging study. Gastroenterology 1997; 113: 1258863.
316