glatiramer acetate immune system augmentation for peripheral nerve regeneration in rat crushed...
TRANSCRIPT
The PDF of the article you requested follows this cover page.
This is an enhanced PDF from The Journal of Bone and Joint Surgery
2010;92:396-403. doi:10.2106/JBJS.I.00109 J Bone Joint Surg Am.Sonnen, Leonid I. Katolik and Thomas E. Trumble Shai Luria, Thanapong Waitayawinyu, James Conniff, H. Josette Morton, Nicholas M. Nemechek, Joshua A.
Nerve Regeneration in Rat Crushed Sciatic Nerve ModelGlatiramer Acetate Immune System Augmentation for Peripheral
This information is current as of February 10, 2010
Supporting data http://www.ejbjs.org/cgi/content/full/92/2/396/DC1
Reprints and Permissions
Permissions] link. and click on the [Reprints andjbjs.orgarticle, or locate the article citation on
to use material from thisorder reprints or request permissionClick here to
Publisher Information
www.jbjs.org20 Pickering Street, Needham, MA 02492-3157The Journal of Bone and Joint Surgery
Glatiramer Acetate Immune System Augmentationfor Peripheral Nerve Regeneration in
Rat Crushed Sciatic Nerve ModelBy Shai Luria, MD, Thanapong Waitayawinyu, MD, James Conniff, BA, H. Josette Morton, Nicholas M. Nemechek,
Joshua A. Sonnen, MD, Leonid I. Katolik, MD, and Thomas E. Trumble, MD
Investigation performed at the University of Washington School of Medicine, Seattle, Washington
Background: Protective antiself response to nervous system injury has been reported to be mediated by a T-cellsubpopulation that can recognize self-antigens. Immune cells have been shown to play a role in the regulation of motorneuron survival after a peripheral nerve injury. The objective of the present study was to evaluate the effects of immunesystem augmentation with use of the antigen glatiramer acetate, which is known to affect T-cell immunity, on peripheralnerve regeneration.
Methods: Wild-type and nude-type (T-cell-deficient) rats underwent crush injury of the sciatic nerve. Three and six weeksafter the injury, the sciatic nerve was examined, both functionally (on the basis of footprint analysis and the tibialisanterior muscle response and weight) and histologically (on the basis of axon count).
Results: Significantly greater muscle responses were measured after three weeks in the group of wild-type rats thatwere treated with glatiramer acetate (control limb:injured limb ratio, 0.05 for the glatiramer acetate group [n = 9],compared with 0.51 for the saline solution group [n = 8]; p < 0.05). Higher axon counts were also found in this group(control limb:injured limb ratio, –0.07 for the glatiramer acetate group [n = 10], compared with 0.29 for the saline solutiongroup [n = 8]; p < 0.05). The nude-type rats showed no response to the intervention after three weeks but showed adelayed response after six weeks. A second dose of glatiramer acetate, delivered forty-eight hours after the injury, did notresult in an improved response as compared with the control groups.
Conclusions: We found that a single treatment with glatiramer acetate resulted in accelerated functional and histo-logical recovery after sciatic nerve crush injury. The role of T-cell immunity in the mechanism of glatiramer acetate wassuggested by the partial and late response found in the T-cell-deficient rats.
Clinical Relevance: Peripheral nerve injury may result in severe loss of sensation, weakness, and pain. The recovery isusually not complete with the limited treatment options. The recruitment of an endogenous mechanism, the immunesystem, to better coordinate the regeneration of nerves after injury is a different approach to this difficult clinical problem.
Peripheral nerve injury results in serious functional losswith paralysis, loss of sensation, and pain, with a pro-longed course of recovery and only partial return of
function. In recent years, there has been little improvement inthe microsurgical techniques of repair of injured nerves, andthe investigative efforts have focused on neurotrophic factors,peptides shown to be influential in the differentiation, func-tion, and survival of neurons1. Delivery of factors to the site ofinjury as well as their dosage regimen have been major prob-lems in this field of research.
In the study of central nervous system injury, it has beenshown that the immune system may recognize certain injury-associated self-compounds as potentially destructive and an-swer with a protective antiself response mediated by a T-cellsubpopulation that can recognize self-antigens2. This may beexplained by the production of neurotrophic factors by theimmune cells that support motor neuron survival before targetreconnection occurs3,4.
A study of facial nerve injury examining severe com-bined immunodeficient (SCID) mice demonstrated a decrease
Disclosure: In support of their research for or preparation of this work, one or more of the authors received, in any one year, outside funding or grants inexcess of $10,000 from the University of Washington Faculty Initiative Fund. Neither they nor a member of their immediate families received paymentsor other benefits or a commitment or agreement to provide such benefits from a commercial entity.
396
COPYRIGHT � 2010 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
J Bone Joint Surg Am. 2010;92:396-403 d doi:10.2106/JBJS.I.00109
in peripheral nerve survival in comparison with wild-typemice, and the investigators concluded that immune cells as-sociated with acquired immunity play a role in regulatingmotor neuron survival after a peripheral nerve injury, specif-ically the CD41 subgroup of T cells5,6. Reconstitution of SCIDmice with wild-type splenocytes containing T and B cells re-stored the survival of facial motor neurons in these mice to thelevel of the wild-type controls.
An endogenous system may better modulate the milieuof neurotrophic factors and may achieve better nerve regen-eration than any exogenous supply of specific factors.
Neuroprotective therapy is aimed at boosting the bene-ficial autoimmune response to injury-associated self-antigens.The development of neuroprotection has focused on antigensthat would not induce autoimmune disease. The syntheticcopolymer glatiramer acetate (Copolymer-1 or Copaxone; TEVANeuroscience, Kansas City, Missouri) has been a successfulexample of this effort.
Glatiramer acetate is a synthetic amino acid polymerthat is an approved drug for the treatment of relapsingmultiple sclerosis and has been proved to be effective fordecreasing the frequency of relapses in patients with relapsingmultiple sclerosis7. It binds to the relevant major histocom-patibility complex proteins and leads to the activation of Tsuppressor cells8. The main mechanism that has been re-ported is of a phenotype switch of Th1 cells to Th2 cells,resulting in a change in the profile of cytokine expression9-11.In the rat model of partial optic nerve crush, adoptive ad-ministration of glatiramer acetate-reactive T cells or vacci-nation with glatiramer acetate on the day of central nervous
system injury had a marked preventive effect on the secondarydegeneration of nerve fibers12.
Our hypothesis was that glatiramer acetate will be neu-roprotective following peripheral nerve injury as well.
This hypothesis was examined in wild-type as well asnude-type rats. With the assumption that glatiramer acetateaugments nerve regeneration by recruiting T-cell immunity,our hypothesis was that in the nude (T-cell-deficient) rat, theeffect of glatiramer acetate will not be achieved or may bedecreased.
Materials and MethodsAnimals
Seventy-three female Harlan Sprague-Dawley rats (wild type;average weight, 225 g) (Harlan Laboratories, Madison,
Wisconsin) and seventy-one female nude rats (NIHRNU-M)(Taconic, Germantown, New York) were divided into groupsas depicted in Table I. This protocol was completed for a six-week period and for a three-week period following nerve in-jury. Each study period included two study groups and twocontrol groups for wild-type as well as nude-type rats (with atleast eight rats per group). The results were compared for eachstudy period separately and for wild-type and nude-type ratsseparately.
All rats were provided with autoclaved pellets and waterad libitum. The rats were permitted one week to acclimate totheir environment before being manipulated and used for theexperiments; all experiments were performed when the ratswere eight weeks of age. All rats were housed under a twelve-hour light/dark cycle in microisolator cages contained within a
TABLE I Study and Control Groups of Peripheral Nerve Regeneration in Rat Crushed Sciatic Nerve Model in Wild-Type and Nude-Type Rats*
Group Rat Type Intervention
A (study group) Wild One dose of glatiramer acetate (500 mg) 1 complete Freund’s adjuvantimmediately after nerve injury
B (study group) Wild Two doses of glatiramer acetate: (1) glatiramer acetate (500 mg) 1 completeFreund’s adjuvant immediately after nerve injury and (2) glatiramer acetate(500 mg) 1 incomplete Freund’s adjuvant forty-eight hours after nerve injury
C (control group) Wild One dose of complete Freund’s adjuvant with normal saline solution immediatelyafter nerve injury
D (control group) Wild One dose of normal saline solution immediately after nerve injury
E (study group) Nude One dose of glatiramer acetate (500 mg) 1 complete Freund’s adjuvantimmediately after nerve injury
F (study group) Nude Two doses of glatiramer acetate: (1) glatiramer acetate (500 mg) 1 completeFreund’s adjuvant immediately after nerve injury and (2) glatiramer acetate(500 mg) 1 incomplete Freund’s adjuvant forty-eight hours after nerve injury
G (control group) Nude One dose of complete Freund’s adjuvant with normal saline solution immediatelyafter nerve injury
H (control group) Nude One dose of normal saline solution immediately after nerve injury
*The study protocol was first completed for a period of six weeks after the injury. It was then repeated for a period of three weeks after the injury forboth wild and nude-type rats. Wild-type rats were Harlan Sprague-Dawley rats, and the nude-type rats were NIHRNU-M rats, deficient of T-celllymphocytes. The shaded areas represent control groups.
397
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 2 d F E B RUA RY 2010GL AT I R A M E R AC E TAT E IM M U N E SY S T E M AU G M E N TAT I O N F O R
PE R I P H E R A L NE RV E R E G E N E R AT I O N I N R AT M O D E L

laminar flow system to maintain a specific pathogen-free en-vironment. All experimental manipulations were performedunder aseptic conditions and were completed in accordancewith the National Institutes of Health guidelines on the careand use of laboratory animals for research purposes. The pres-ent study was approved by the institutional animal utilizationstudy committee.
Induction of Nerve InjuryAll rats were anesthetized with use of 56 mg/kg of Nembutal(sodium pentobarbital, 50 mg/mL), administered intraperi-toneally. The surgical site was shaved and was washed withantiseptic solution prior to positioning for surgery, and localanesthetic (0.5 mL of 1% lidocaine hydrochloride) was in-jected subcutaneously at the surgical site. The sciatic nerve onthe left side was approached with use of a semitendinosus-biceps femoris (long head) muscle-splitting incision. The nervewas dissected free of surrounding connective tissue. Withuse of a single pair of smooth microforceps, fully pressedfor thirty seconds, a consistent crush injury was created.The location of the crush was marked with a single stitch of9-0 nylon. The wound was closed with 4-0 sutures for theskin1.
ImmunizationAll injections were performed subcutaneously. The six-weekprotocol was performed first, and the emulsion, in a totalvolume of 0.2 mL, was injected into the animal’s two hindfootpads immediately after the crush injury. After review of theresults, it seemed that, because of the rapid regenerative ca-pability of the rat nerve, the six-week follow-up for the crush-injured nerves did not reveal the treatment effect. For thisreason, the three-week protocol was performed; during thisprotocol, the progress was evaluated weekly with use of anadditional measure, footprint analysis. In order to evaluate thefootprints, footpad injections were not used for the three-weekprotocol, and the emulsion was subcutaneously injected intothe base of the tail (resulting in the administration of the sametotal volume of 0.2 mL).
The rats in the study groups were injected with anemulsion containing glatiramer acetate with complete Freund’sadjuvant (CFA; Becton Dickinson, Franklin Lakes, New Jer-sey). Groups B and F (Table I) were treated with an additionalinjection of glatiramer acetate (with incomplete Freund’s ad-juvant [IFA; Becton Dickinson]) forty-eight hours after thenerve injury. These groups were evaluated for a longer-lastingeffect of glatiramer acetate. The dose of glatiramer acetate andcomplete Freund’s adjuvant was based on previous reports13.Freund’s adjuvant is an antigen solution emulsified in mineraloil, used as an immunopotentiator. It is composed of in-activated and dried mycobacteria. Incomplete Freund’s adju-vant is devoid of the mycobacteria and is less potent yet lesstoxic than complete Freund’s adjuvant.
The two control groups were injected with an emulsioncontaining complete Freund’s adjuvant with normal salinesolution or normal saline solution only.
Nerve-Regeneration MeasuresThree or six weeks after the surgery, according to the protocol,both functional and histological evaluations were performedand the contralateral legs were used as the nonoperativelytreated controls. The functional measurements that were ob-tained at three or six weeks included the tibialis anteriormuscle response to sciatic nerve stimulation and the tibialisanterior muscle weight. In the groups of rats that were killedafter three weeks, the functional evaluation included the ad-ditional measure of footprint analysis (specifically, toe spreadfactor, determined after seven, fourteen, and twenty-one days).The histological measurement at three or six weeks was anaxon count in the sciatic nerve.
Functional EvaluationQuantitative assessment of tibialis anterior muscle response tosciatic nerve stimulation: Isometric tetanic contractile forcemeasurements were made in situ with a technique adaptedfrom that previously described by Zhao et al.14. After the in-duction of anesthesia (56 mg/kg of Nembutal), the hindlimbwas immobilized on a frame and the foot was placed in asecure clamp to fix its position for the experimental analysisof muscle contraction force (response). An additional incisionwas made on the anterior aspect of the lower limb to exposethe target of sciatic innervation, the tibialis anterior muscle.The distal tendon of the tibialis anterior muscle was divided atits insertion and mobilized up to the level of its origin, withcare being taken to preserve the muscle’s neurovascular supply.The transected tendinous part of the tibialis anterior musclewas secured to a metal hook, which was connected to a forcetransducer (model FT03; Grass Instrument, West Warwick,Rhode Island). The force transducer signal was sent to anamplifier whose output was recorded with use of LabTechNotebook software (Laboratory Technologies, Andover, Mas-sachusetts) on a personal computer. The nerve was maintainedat approximately 37�C with warm saline solution. The segmentof the nerve proximal to the injury was dissected and wasisolated proximally in preparation for stimulation. A siliconesheet was placed beneath the exposed nerve to isolate it fromany conducting transudate on nearby tissues. An initial tensionof approximately 330 mN was applied by stretching the muscleon the force transducer. This tension, corresponding to thenormal length of the muscle, ensures that the contractions areisometric15. Platinum wire electrodes were used for electricalstimulation of the nerve proximal to the repair site. A stimu-lator (model S48; Grass Instrument) was used to deliver su-pramaximal stimuli (square wave impulses with a frequencyof 100 Hz and duration of 0.6 msec). The maximal force ofcontraction, the tetanic force expressed in mN, was then re-corded. A similar measurement was made for the nonopera-tively treated, contralateral (control) side. The first muscularresponse was used to compare the injured side with the con-trol side.
Tibialis anterior muscle weight: After the animal waskilled, both muscles were harvested and weighed and the dif-ference between the injured and control legs was recorded.
398
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 2 d F E B RUA RY 2010GL AT I R A M E R AC E TAT E IM M U N E SY S T E M AU G M E N TAT I O N F O R
PE R I P H E R A L NE RV E R E G E N E R AT I O N I N R AT M O D E L

Footprint analysis: toe spread factor: For the groups ofanimals that were killed after three weeks, footprints werecollected at three time points. Seven, fourteen, and twenty-onedays after the injury to the nerve, footprints were collectedand static toe spreading (for the first through fifth toes) wasmeasured. This measurement has been found to be a goodmeasure of functional recovery after sciatic nerve injury16. Theanalysis was performed by dipping the hind legs in ink andreleasing the rats to walk over a large sheet (1 m · 20 cm) ofwhite paper. The sheets were scanned, and measurements oftoe spreading were made for three consecutive prints, whichwere averaged. A ratio was calculated as previously described16,with the injured side being compared with the control side.
Histological Evaluation: Axon Count of Sciatic Nerve TissueFollowing nerve stimulation and after the animal was killed,sections measuring 0.5 cm in length were removed from thesciatic nerve, 0.5 cm proximal and 0.5 cm distal to the site ofinjury, and were immersed in Karnovsky fixative (for fourhours at 25�C), were washed in 0.2-M cacodylate buffer (pH7.4), were postfixed in 1.5% osmium tetroxide with 1.5%potassium ferricyanide followed by graded alcohol (30%,50%, 70%, 95%, and 100%), and were embedded in EM-Bed 812 (Electron Microscopy Sciences, Fort Washington,Pennsylvania) for axon counting. Sections measuring 1 mmin thickness were prepared with use of a Reichert-Jung Ul-tracut E with a diamond knife (Reichert-Jung, Weiss, Aus-tria). In all animals, the corresponding sections from thenonoperatively treated, contralateral (control) legs wereharvested and processed in a similar manner. All sectionswere stained with toluidine blue prior to analysis with lightmicroscopy.
The axon counts were performed blinded by a group ofthree investigators (J.C., N.M.N., S.L.) with use of an EclipseE600 microscope (Nikon, Melville, New York) with a RetigaEX CCD camera (QImaging, Burnaby, British Columbia,Canada) and QCapture software (QImaging). Analysis wasperformed on a Macintosh personal computer (Apple, Cu-pertino, California) with use of the public-domain NIH Imageprogram (developed at the United States National Institutes ofHealth and available on the Internet at http://rsb.info.nih.gov/nih-image/) for the calculation of area and point counting inorder to express the results as a ratio of the density (axons/mm2) of the fibers of the experimental side to the control side.The ratio of axon density provides information relative to thecontralateral, control nerve and thus is an animal-specificmeasure of regeneration valuable for between-group andamong-group comparisons1.
Statistical AnalysisStandard two-sided tests with a significance level of a and apower of 1 2 b were used for power analysis using the vali-dation data of previous studies1,17. The population sizes werecomputed with use of the following two-sided test, assumingequal sizes in both study populations: n = (s1
2 1 s22) (Z1-a/2 1
Z1-b)2 (1/D2), where D = m2 2 m1, a = 0.05, b = 0.2 (for 80%
power with 95% confidence), Z12a/2 = 1.96, and Z1-b = 0.84.For axon counting, s1 (variance 1) = 0.448, s2 (variance 2) =0.237, m2 2 m1 = 0.56, and n = 6.4 for each study group. Formuscle weights, s1 (variance 1) = 0.372, s2 (variance 2) =0.186, m2 2 m1 = 0.45, and n = 6.7 for each study group.
The differences in means were based on previous stud-ies1,17. To provide an extra margin of safety, we elected to use aminimum of eight animals per group.
The hypothesis was tested for each dependent variablewith use of analysis of variance, followed by a series of pairwiseunivariate comparisons using the Student t test to detect sig-nificant differences between groups. Multiple comparisonswere accounted for with use of the Scheffe post hoc test for mus-cle contracture, weight, and axon count and the Fisher pro-tected least significant difference test for the footprint analysis.
Source of FundingThere was no external funding source for the study.
Results
One hundred and forty-six rats were included in the study.Two rats were killed because of malocclusion and con-
sequent malnourishment (one rat) or because of autophagia ofmore than one toe proximal to the distal interphalangeal jointof the injured limb (one rat) according to the criteria of theinstitutional ethical committee.
The results are summarized in tables in the Appendix.
Functional EvaluationTibialis Anterior Muscle Response to Sciatic Nerve StimulationSignificantly greater muscle responses were measured afterthree weeks in the group of wild-type rats treated with gla-tiramer acetate in comparison with all other groups, includingthe double dose of glatiramer acetate, complete Freund’s ad-juvant, and normal saline solution (control:injured limb ratio,0.05 mN compared with 0.52, 0.53, and 0.51, respectively; p <0.05). No differences were found between the groups of wild-type rats after six weeks or nude-type rats after three or sixweeks (at the 95% confidence level).
Tibialis Anterior Muscle WeightNo difference was found in muscle weights between the groupsof wild or nude-type rats (at the 95% confidence level).
Footprint Analysis: Toe Spread FactorA significant decrease in toe spread was found after twenty-onedays in the wild-type group treated with two doses of glatirameracetate in comparison with the complete Freund’s adjuvantgroup (ratio, 20.083 compared with 0.044; p < 0.01). Althoughthe differences were not significant, the group that receivedtwo doses of glatiramer acetate was found to have decreasedtoe spread after twenty-one days in comparison with thegroup that received one dose of glatiramer acetate group andthe group that received normal saline solution. No differenceswere found between the groups of nude-type rats (at the 95%confidence level).
399
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 2 d F E B RUA RY 2010GL AT I R A M E R AC E TAT E IM M U N E SY S T E M AU G M E N TAT I O N F O R
PE R I P H E R A L NE RV E R E G E N E R AT I O N I N R AT M O D E L
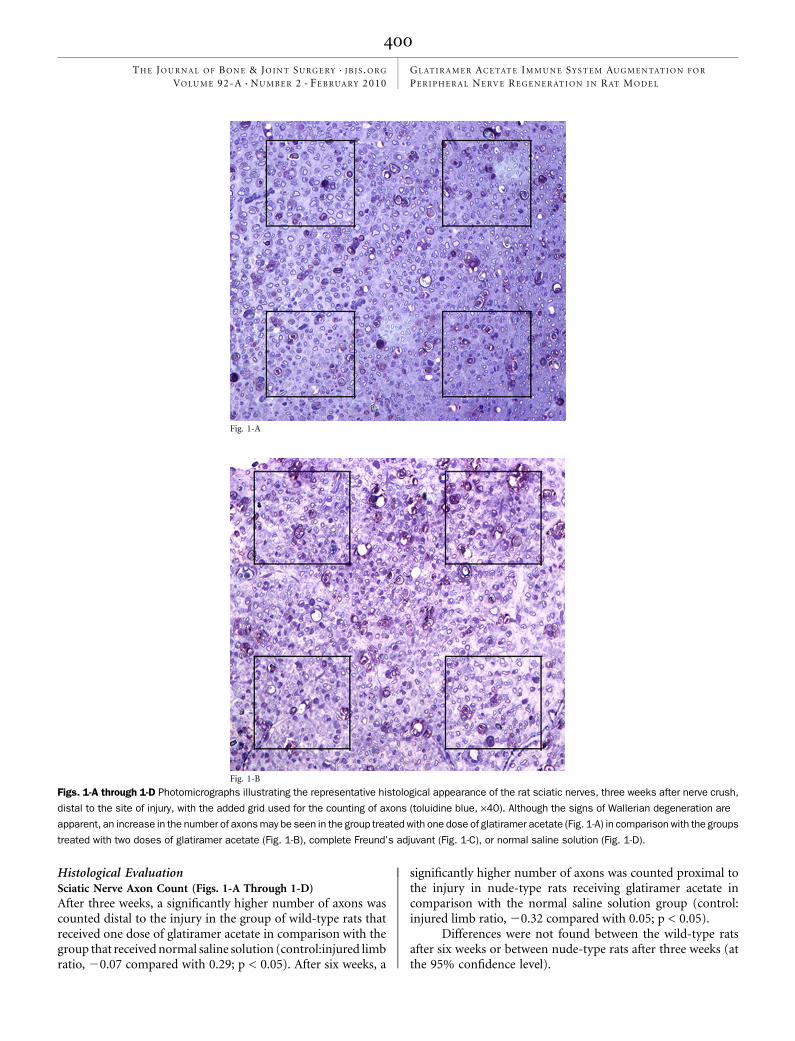
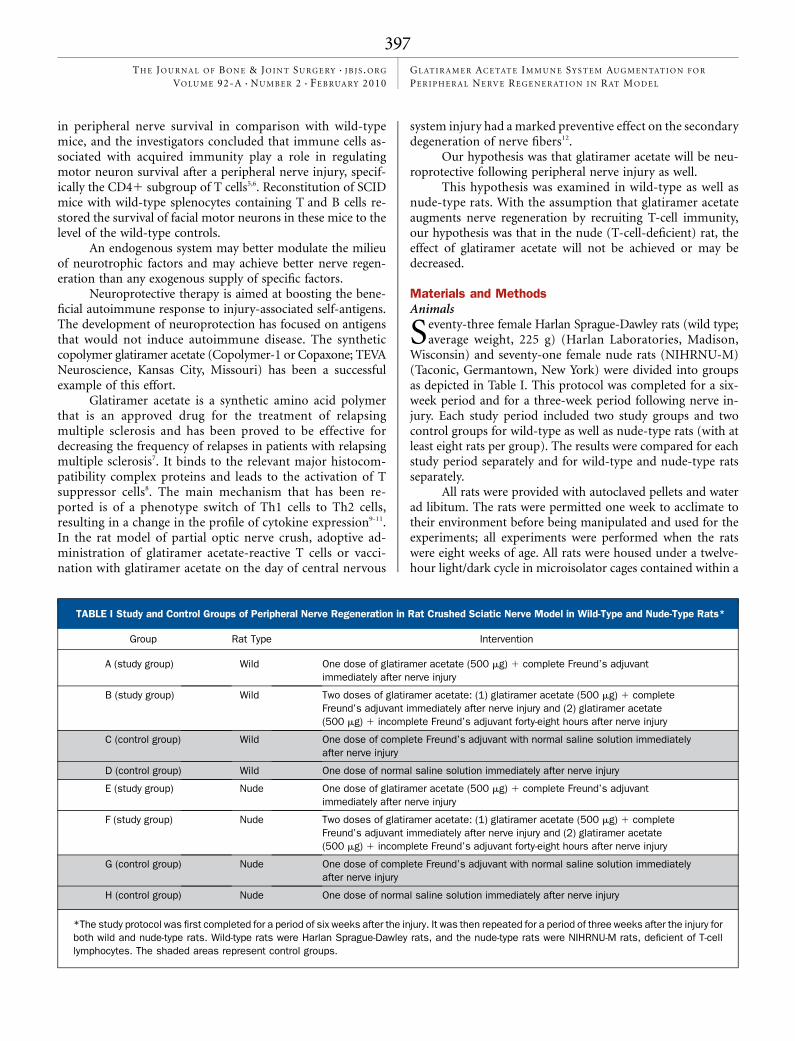
Histological EvaluationSciatic Nerve Axon Count (Figs. 1-A Through 1-D)After three weeks, a significantly higher number of axons wascounted distal to the injury in the group of wild-type rats thatreceived one dose of glatiramer acetate in comparison with thegroup that received normal saline solution (control:injured limbratio, 20.07 compared with 0.29; p < 0.05). After six weeks, a
significantly higher number of axons was counted proximal tothe injury in nude-type rats receiving glatiramer acetate incomparison with the normal saline solution group (control:injured limb ratio, 20.32 compared with 0.05; p < 0.05).
Differences were not found between the wild-type ratsafter six weeks or between nude-type rats after three weeks (atthe 95% confidence level).
Fig. 1-A
Fig. 1-B
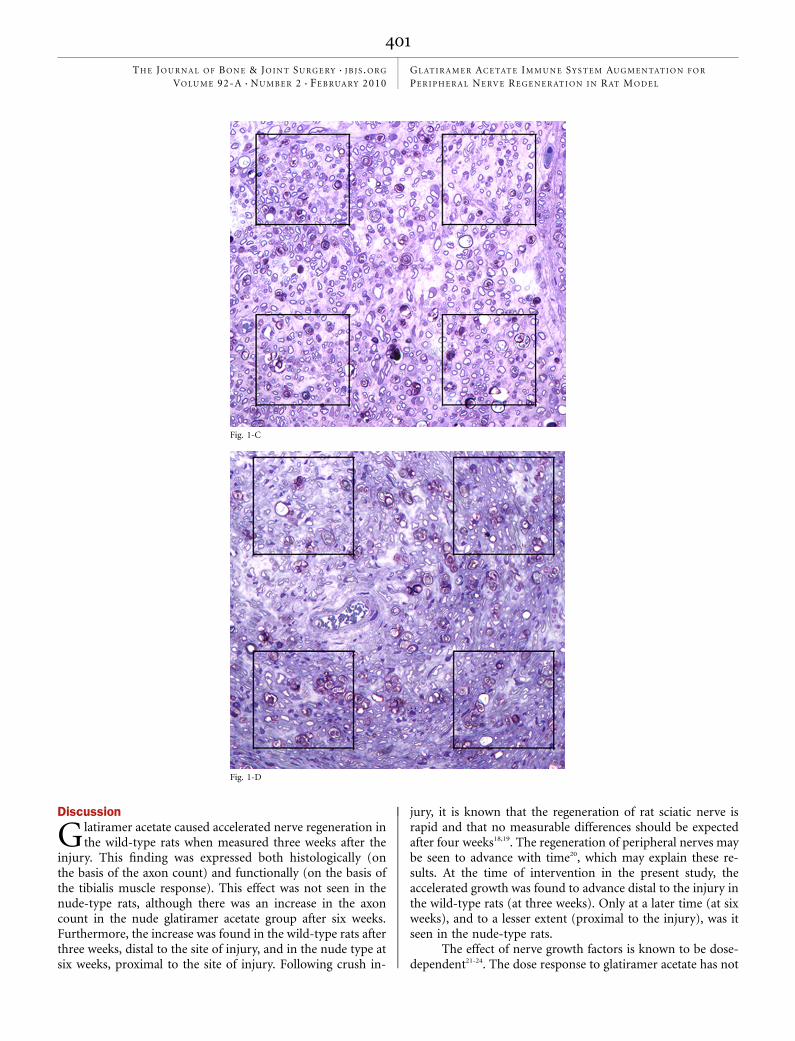
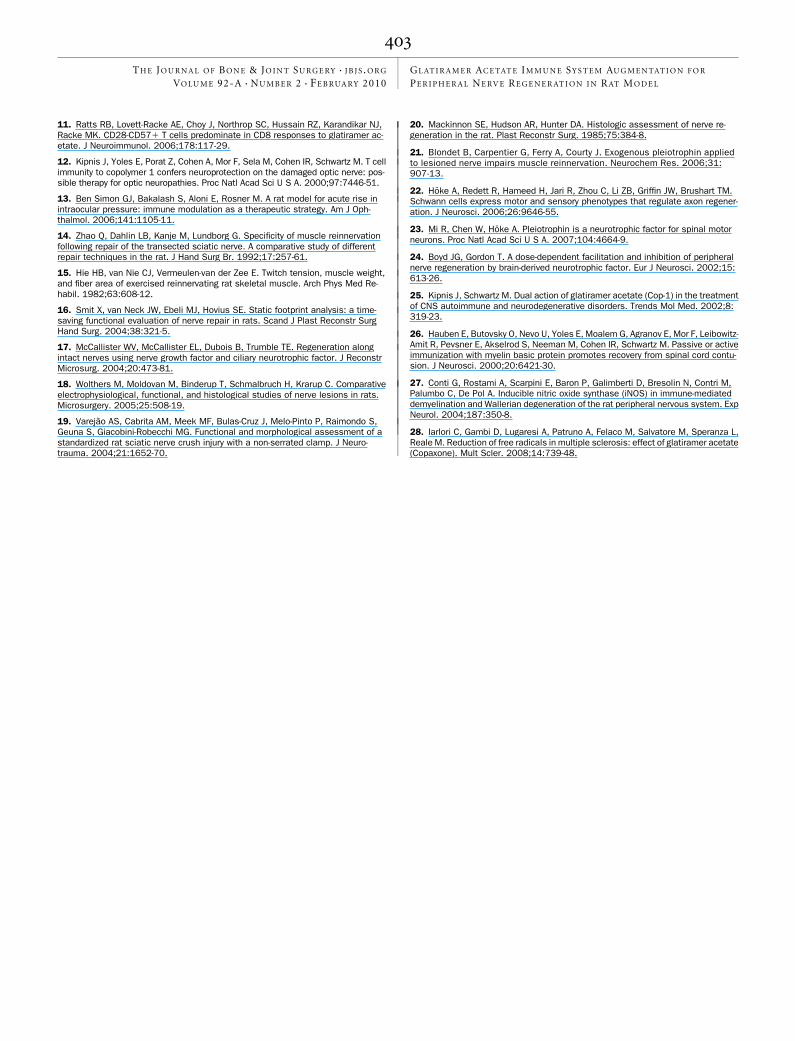
Figs. 1-A through 1-D Photomicrographs illustrating the representative histological appearance of the rat sciatic nerves, three weeks after nerve crush,
distal to the site of injury, with the added grid used for the counting of axons (toluidine blue, ·40). Although the signs of Wallerian degeneration are
apparent, an increase in the number of axons may be seen in the group treated with one dose of glatiramer acetate (Fig. 1-A) in comparison with the groups
treated with two doses of glatiramer acetate (Fig. 1-B), complete Freund’s adjuvant (Fig. 1-C), or normal saline solution (Fig. 1-D).
400
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 2 d F E B RUA RY 2010GL AT I R A M E R AC E TAT E IM M U N E SY S T E M AU G M E N TAT I O N F O R
PE R I P H E R A L NE RV E R E G E N E R AT I O N I N R AT M O D E L
Discussion
Glatiramer acetate caused accelerated nerve regeneration inthe wild-type rats when measured three weeks after the
injury. This finding was expressed both histologically (onthe basis of the axon count) and functionally (on the basis ofthe tibialis muscle response). This effect was not seen in thenude-type rats, although there was an increase in the axoncount in the nude glatiramer acetate group after six weeks.Furthermore, the increase was found in the wild-type rats afterthree weeks, distal to the site of injury, and in the nude type atsix weeks, proximal to the site of injury. Following crush in-
jury, it is known that the regeneration of rat sciatic nerve israpid and that no measurable differences should be expectedafter four weeks18,19. The regeneration of peripheral nerves maybe seen to advance with time20, which may explain these re-sults. At the time of intervention in the present study, theaccelerated growth was found to advance distal to the injury inthe wild-type rats (at three weeks). Only at a later time (at sixweeks), and to a lesser extent (proximal to the injury), was itseen in the nude-type rats.
The effect of nerve growth factors is known to be dose-dependent21-24. The dose response to glatiramer acetate has not
Fig. 1-C
Fig. 1-D
401
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 2 d F E B RUA RY 2010GL AT I R A M E R AC E TAT E IM M U N E SY S T E M AU G M E N TAT I O N F O R
PE R I P H E R A L NE RV E R E G E N E R AT I O N I N R AT M O D E L

been described in the past, although it has been suggested thatits effect should be limited for optimum neuroprotection25. Inthe present study, we found that the additional dose of gla-tiramer acetate, forty-eight hours after the injury, did not re-sult in improved regeneration compared with the controlgroups. This finding may have been due either to the dose ofglatiramer acetate or to the timing of its administration13,26. It ispossible that the additional late effect (at forty-eight hours) ofglatiramer acetate or its elevated dose had a negative effect onthe dynamics of the immune response, or the growth factormilieu, at the site of injury (as seen with the footprint analysis).Specifically, brain-derived neurotrophic factor (BDNF) has beenknown to have a bimodal effect on peripheral nerve regenera-tion24. Several explanations have been suggested: (1) differentialactivity of BDNF motor-neuronal receptors (trkB facilitatoryreceptor as compared with p75 inhibitory receptor), (2) down-regulation of trkB activity with prolonged exposure to BDNF,(3) generation of free radicals with higher levels of BDNF, and(4) p75 receptor-mediated decrease in supportive Schwann cellactivity24. BDNF has been implicated as having a major role inthe mechanism of action of glatiramer acetate9, which may ex-plain the results of the present study.
Although we saw a positive effect on nerve regenerationwith glatiramer acetate both histologically and functionally,other functional measures failed to demonstrate improvementin the recovery from injury. Several factors may explain thisfinding. Some measures may be less sensitive than others, theregeneration may have been too rapid to evaluate differences inthis model, or the dose or treatment regimen may not havebeen the optimum one. It is also known that there is limitedcorrelation between the different outcome measures, whichdepict different aspects of the recovery process18. Finally, itshould be noted that the crush injury model is a more difficulttest of therapeutic benefit in comparison with the nervetransection injury. The crush injury requires a shorter evalu-ation period, and the recovery is more complete and lessvariable than is the case with transection18.
An increase in axon count in comparison with thecontrol limb was noted at six weeks in most groups. Thisincrease represents the robust capability of the rat peripheralnerve to regenerate18. This increase was significantly higher in
the nude-type rats treated with glatiramer acetate after sixweeks. This finding can not be explained by the proposedmechanism of T-cell manipulation by glatiramer acetate. Itmay be explained by other mechanisms of glatiramer acetateaction described in the literature. The late and less pronouncedregeneration may be explained by the minor role of two othersuggested mechanisms: (1) production of neurotrophic factorsby cells other than T cells9,25; or (2) regulation of free radicalproduction as shown in multiple sclerosis models27,28.
We found a beneficial effect of the antigen glatirameracetate on the regeneration of the injured peripheral nerve. Thiswas limited by the addition of another, later dose of glatirameracetate and was significantly decreased in nude-type rats un-dergoing similar intervention. Additional investigation is neededto evaluate the relationship between dosage and regimen.
AppendixTables showing the details of all experiments are availablewith the electronic version of this article on our web site
at jbjs.org (go to the article citation and click on ‘‘SupportingData’’). n
Shai Luria, MDThanapong Waitayawinyu, MDJames Conniff, BAH. Josette MortonNicholas M. NemechekLeonid I. Katolik, MDThomas E. Trumble, MDDepartment of Orthopaedics and Sports Medicine,University Medical Center,University of Washington School of Medicine,Box 356500, 1959 Pacific Street,Seattle, WA 98195-6500.E-mail address for S. Luria: [email protected]
Joshua A. Sonnen, MDDepartment of Pathology, Harborview Medical Center,University of Washington School of Medicine, Box 359791,325 9th Avenue, Seattle, WA 98104-2499
References
1. McCallister WV, Tang P, Smith J, Trumble TE. Axonal regeneration stimulated bythe combination of nerve growth factor and ciliary neurotrophic factor in an end-to-side model. J Hand Surg Am. 2001;26:478-88.
2. Schwartz M. Harnessing the immune system for neuroprotection: therapeuticvaccines for acute and chronic neurodegenerative disorders. Cell Mol Neurobiol.2001;21:617-27.
3. Hohlfeld R, Kerschensteiner M, Stadelmann C, Lassmann H, Wekerle H. Theneuroprotective effect of inflammation: implications for the therapy of multiplesclerosis. J Neuroimmunol. 2000;107:161-6.
4. Serpe CJ, Sanders VM, Jones KJ. Kinetics of facial motoneuron loss followingfacial nerve transection in severe combined immunodeficient mice. J Neurosci Res.2000;62:273-8.
5. Jones KJ, Serpe CJ, Byram SC, Deboy CA, Sanders VM. Role of the immunesystem in the maintenance of mouse facial motoneuron viability after nerve injury.Brain Behav Immun. 2005;19:12-9.
6. Serpe CJ, Coers S, Sanders VM, Jones KJ. CD41 T, but not CD81 or B, lym-phocytes mediate facial motoneuron survival after facial nerve transection. BrainBehav Immun. 2003;17:393-402.
7. Teitelbaum D, Fridkis-Hareli M, Arnon R, Sela M. Copolymer 1 inhibits chronicrelapsing experimental allergic encephalomyelitis induced by proteolipid protein(PLP) peptides in mice and interferes with PLP-specific T cell responses. J Neuro-immunol. 1996;64:209-17.
8. Teitelbaum D, Sela M, Arnon R. Copolymer 1 from the laboratory to FDA. Isr J MedSci. 1997;33:280-4.
9. Blanchette F, Neuhaus O. Glatiramer acetate: evidence for a dual mechanism ofaction. J Neurol. 2008;255 Suppl 1:26-36.
10. Qin Y, Zhang DQ, Prat A, Pouly S, Antel J. Characterization of T cell lines derivedfrom glatiramer-acetate-treated multiple sclerosis patients. J Neuroimmunol. 2000;108:201-6.
402
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 2 d F E B RUA RY 2010GL AT I R A M E R AC E TAT E IM M U N E SY S T E M AU G M E N TAT I O N F O R
PE R I P H E R A L NE RV E R E G E N E R AT I O N I N R AT M O D E L
11. Ratts RB, Lovett-Racke AE, Choy J, Northrop SC, Hussain RZ, Karandikar NJ,Racke MK. CD28-CD571 T cells predominate in CD8 responses to glatiramer ac-etate. J Neuroimmunol. 2006;178:117-29.
12. Kipnis J, Yoles E, Porat Z, Cohen A, Mor F, Sela M, Cohen IR, Schwartz M. T cellimmunity to copolymer 1 confers neuroprotection on the damaged optic nerve: pos-sible therapy for optic neuropathies. Proc Natl Acad Sci U S A. 2000;97:7446-51.
13. Ben Simon GJ, Bakalash S, Aloni E, Rosner M. A rat model for acute rise inintraocular pressure: immune modulation as a therapeutic strategy. Am J Oph-thalmol. 2006;141:1105-11.
14. Zhao Q, Dahlin LB, Kanje M, Lundborg G. Specificity of muscle reinnervationfollowing repair of the transected sciatic nerve. A comparative study of differentrepair techniques in the rat. J Hand Surg Br. 1992;17:257-61.
15. Hie HB, van Nie CJ, Vermeulen-van der Zee E. Twitch tension, muscle weight,and fiber area of exercised reinnervating rat skeletal muscle. Arch Phys Med Re-habil. 1982;63:608-12.
16. Smit X, van Neck JW, Ebeli MJ, Hovius SE. Static footprint analysis: a time-saving functional evaluation of nerve repair in rats. Scand J Plast Reconstr SurgHand Surg. 2004;38:321-5.
17. McCallister WV, McCallister EL, Dubois B, Trumble TE. Regeneration alongintact nerves using nerve growth factor and ciliary neurotrophic factor. J ReconstrMicrosurg. 2004;20:473-81.
18. Wolthers M, Moldovan M, Binderup T, Schmalbruch H, Krarup C. Comparativeelectrophysiological, functional, and histological studies of nerve lesions in rats.Microsurgery. 2005;25:508-19.
19. Varejao AS, Cabrita AM, Meek MF, Bulas-Cruz J, Melo-Pinto P, Raimondo S,Geuna S, Giacobini-Robecchi MG. Functional and morphological assessment of astandardized rat sciatic nerve crush injury with a non-serrated clamp. J Neuro-trauma. 2004;21:1652-70.
20. Mackinnon SE, Hudson AR, Hunter DA. Histologic assessment of nerve re-generation in the rat. Plast Reconstr Surg. 1985;75:384-8.
21. Blondet B, Carpentier G, Ferry A, Courty J. Exogenous pleiotrophin appliedto lesioned nerve impairs muscle reinnervation. Neurochem Res. 2006;31:907-13.
22. Hoke A, Redett R, Hameed H, Jari R, Zhou C, Li ZB, Griffin JW, Brushart TM.Schwann cells express motor and sensory phenotypes that regulate axon regener-ation. J Neurosci. 2006;26:9646-55.
23. Mi R, Chen W, Hoke A. Pleiotrophin is a neurotrophic factor for spinal motorneurons. Proc Natl Acad Sci U S A. 2007;104:4664-9.
24. Boyd JG, Gordon T. A dose-dependent facilitation and inhibition of peripheralnerve regeneration by brain-derived neurotrophic factor. Eur J Neurosci. 2002;15:613-26.
25. Kipnis J, Schwartz M. Dual action of glatiramer acetate (Cop-1) in the treatmentof CNS autoimmune and neurodegenerative disorders. Trends Mol Med. 2002;8:319-23.
26. Hauben E, Butovsky O, Nevo U, Yoles E, Moalem G, Agranov E, Mor F, Leibowitz-Amit R, Pevsner E, Akselrod S, Neeman M, Cohen IR, Schwartz M. Passive or activeimmunization with myelin basic protein promotes recovery from spinal cord contu-sion. J Neurosci. 2000;20:6421-30.
27. Conti G, Rostami A, Scarpini E, Baron P, Galimberti D, Bresolin N, Contri M,Palumbo C, De Pol A. Inducible nitric oxide synthase (iNOS) in immune-mediateddemyelination and Wallerian degeneration of the rat peripheral nervous system. ExpNeurol. 2004;187:350-8.
28. Iarlori C, Gambi D, Lugaresi A, Patruno A, Felaco M, Salvatore M, Speranza L,Reale M. Reduction of free radicals in multiple sclerosis: effect of glatiramer acetate(Copaxone). Mult Scler. 2008;14:739-48.
403
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 2 d F E B RUA RY 2010GL AT I R A M E R AC E TAT E IM M U N E SY S T E M AU G M E N TAT I O N F O R
PE R I P H E R A L NE RV E R E G E N E R AT I O N I N R AT M O D E L