facial nerve rehabilitation after radical parotidectomy
TRANSCRIPT
The Laryngoscope Lippincott Williams & Wilkins, Inc., Philadelphia 0 1999 The American Laryngological, Rhinoiogical and Otological Society, Inc.
Facial Nerve Rehabilitation After Radical Parotidectomy Pavan G. Reddy, MD; Richard L. Arden, MD; Robert H. Mathog, MD
Objective: E.namine functional outcomes in pa- tients undergoing radical parotidectomy and facial nerve grafting. Identify factors that may affect reha- bilitation in these patients. Study Design: Retrospec- tive chart review and photographic analyses of 12 patients undergoing radical parotidectomy with in- terposition nerve grafts for facial nerve reconstruc- tion. Methods: Data obtained for each patient regard- ing age, sex, histology of parotid neoplasm, cable graft source, administration of postoperative radiother- apy, and treatment for eye rehabilitation. Functional outcomes were assessed with the House-Brackmann grading system at 6 months, 1 year, and 2 years after surgery. Results: All nerve grafts were harvested from cervical plexus sensory nerves with microscopic epineural repair performed for all neurorrhaphies. Overall, 9 of 12 patients achieved a grade III 2 years after surgery. All patients under age 30 obtained a grade III. Of the seven patients receiving postopera- tive radiation, five achieved a grade III. Older pa- tients often required surgical procedures to facilitate eye closure. Conclusions: Facial nerve rehabilitation after radical parotidectomy can be successfully achieved with cervical plexus interposition nerve grafts. Postoperative radiotherapy did not appear to affect return of function, and younger patients con- sistently achieved good functional outcomes after nerve grafting. Older patients frequently require sur- gical procedures for eye rehabilitation after radical parotidectomy. Kiy Words: Radical parotidectomy, fa- cial nerve, facial nerve rehabilitation, interposition nerve grafts, functional outcome.
Laryngoscope, 109:894-899,1999
INTRODUCTION Radical parotidectomy, which entails total extirpa-
tion of the parotid gland in conjunction with resection of the facial nerve, is advocated for the surgical treatment of high-grade malignancies and recurrent benign tumors of the parotid that intimately involve the facial nerve.1,2 The
Presented a t the Meeting of the Middle Section of the American Laryngological, Rhinological and Otological Society, Inc., Milwaukee, Wis- consin, January 23, 1999.
From the Department of Otolaryngology-Head and Neck Surgery (P.G.R., R.L.A., R.H.M.), Wayne State University, Detroit, Michigan.
Send Correspondence to Pavan G. Reddy, MD, Wayne State Univer- sity, Department of Otolaryngology-Head and Neck Surgery, 5E UHC, 540 E. Canfield, Detroit, MI 48201, U.S.A.
aesthetic and functional deficits created by sacrifice of the facial nerve can be emotionally traumatizing to the pa- tient while presenting formidable challenges to the recon- structive surgeon. Among the many clinical modalities available for facial nerve rehabilitation, cable nerve graft- ing has been used successfully to rehabilitate the patient after radical parotidectomy.
In the past few decades much work has been dedicated to the study of nerve regenerati~n~.~ as well as to the refine- ment of microneural repair techniques.5 Still, many contro- versies regarding extratemporal facial nerve grafting exist. Some areas of debate include optimal source for cable nerve grafis, technical aspects of neurorrhaphy, and effects of ra- diation on hctional outcome. To elucidate the role of the above factors in facial nerve rehabilitation, the present study reviews a single surgeon’s experience with radical parotid- &my and cable nerve grafi reconstruction.
MATERIALSAND METHODS Twelve patients underwent radical parotidectomy with ca-
ble nerve grafting from 1979 to 1996. This group of patients consisted of seven females and five males with ages at the time of surgery ranging from 15 to 83. All patients, with the exception of one, were followed for a minimum of 2 years after surgery with photodocumentation performed at 6-month, l-year, and 2-year intervals. Retrospective chart review in conjunction with photo- graphic analysis was performed for each of the patients by three observers independently. However, the results of the photo- graphic analysis were not reported by an unbiased observer. Histology of resected parotid neoplasms and presence of perineu- ral invasion were obtained from pathology reports.
For resection of parotid neoplasms, a preauricular incision was made that curved underneath the ear lobule and extended along the anterior border of the sternocleidomastoid muscle. A skin-subcutaneous flap was raised over the parotid capsule with fine iris scissors until the distal branches of the facial nerve were seen exiting the gland. The temporal, zygomatic, buccal, and mandibular branches were incised and tagged for later grafting. The main trunk of the facial nerve was identified using the posterior belly of the digastric, the cartilaginous tragal pointer, and the tympanomastoid suture line as landmarks. Once the main trunk was identified, en bloc resection was performed to remove the neoplasm and all portions of the facial nerve that were encased with tumor. If the tumor was localized near the main trunk, a mastoidectomy with relaxation of the facial nerve in the facial canal was performed to provide adequate surgical
Laryngoscope 109: June 1999
894
Reddy et al.: Facial Nerve Rehabilitation

margins and to increase the length of the proximal facial nerve stump available for grafting.
The donor nerve graft was subsequently harvested from the cervical sensory plexus, which usually included the great auric- ular nerve, and occasionally the supraclavicular or lessor occipi- tal nerve. After freshening the cable nerve graft ends as well as the proximal and distal facial nerve stumps with a scalpel, mi- croscopic epineural repair was performed with interrupted 9-0 or 10-0 monofilament nylon sutures, with four to six sutures used at each anastomosis. Graft source and number of branches per graft were noted.
Patients receiving postoperative irradiation were identified with total radiation doses to the primary field recorded. The House-Brackmann facial nerve grading system6 was utilized to assess preoperative facial nerve function and postoperative func- tion at 6-month, 1-year, and 2-year intervals. Postoperative eye management included the use of topical moisturizing agents and various types of oculoplastic procedures including tarsorrhaphy, gold weight placement, or canthoplasty for selected patients.
RESULTS Five patients had impaired preoperative facial nerve
function (Table I). Of these five patients, four had histo- logical evidence of perineural invasion. One patient (pa- tient 8) had perineural invasion despite having normal preoperative nerve function. AU cable nerve grafts were harvested from the cervical sensory plexus. These cable grafts consisted of one to four distal branches that were anastornosed to named distal facial nerve branches (Table
I). Mastoidectomy and relaxation of the facial nerve was performed in 9 of 12 patients.
Postoperative evaluation of facial nerve function re- vealed that at 6 months after nerve grafting, no patient had better than a grade V level of function (Table 11). Two years after surgery, nine patients were classified as grade 111, one grade V, and one other a grade VI. Grade I11 was the highest grade achieved by any patient and all three patients under age 30 in this series achieved this grade.
Seven patients received postoperative external beam radiotherapy, with one patient receiving combined photon and neutron beam therapy. The external beam radiation dose to the primary field ranged from 4000 cGy to 5940 cGy, with a mean of 4987 cGy. Of the irradiated patients, two years after nerve grafting, five achieved good func- tional return (grade 1111, while two patients, of which one received neutron beam therapy, had poor functional re- turn. Postoperative eye care consisted of only topical mois- turizing agents in seven patients; five patients had surgi- cal procedures to facilitate eye closure in addition to topical therapy (Table 11).
DISCUSSION As shown in this series and in reports by Conley?
Lathrop,s and Fisch and Lanser,S cable nerve grafting is an effective technique to restore voluntary facial expres- sion and function after sacrifice of the facial nerve for
~~
TABLE I. Patients Undergoing Radical Parotidectomy.
Patient No.
1 2
3
4
5
6
7
8
9
10
11
12
Age (Y)
29 75
76
34
70
~
16
83
49
65
15
63
47
Nerve Preoperative Sex Histology Invasion Facial Function Cable Graft Source Anastomotic Sites'
F M
F
M
M
F
F
F
F
F
M
M
Acinic cell Melanoma
Basaloid
SCC adenocarcinoma
SCC
Chondrosarcoma
High-grade
Adenoid cystic mucoepidermoid
Adenoid cystic
Recurrent pleomorphic adenoma
Moderate grade mucoepidermoid
Poorly differentiated carcinoma
N N
N
N
N
N
Y
Y
Y
N
Y
Y
Grade I Grade I
Grade I
Grade II
Grade I
Grade 1
Grade IV
Grade I
Grade VI
Grade I
Grade II
Grade 111
Great auricular Supraclavicular
Great auricular
Great auricular
Great auricular
Great auricular
Great auricular
Great auricular
Great auricular
Great auricular; lesser occipital
Great auricular
1 br. cable: upper main trunk to zygomatic 2 br. cable: main trunk to zygomatic and
buccal 2 br. cable: main trunk to zygomatic and
buccal 1 br. cable: mastoid segment to main
extratemporal trunk 2 br. cable: upper trunk to temporal and
zygomatic 2 br. cable: lower trunk to buccal and
mandibular 4 br. cable: main trunk to temporal,
zygomatic, buccal, and mandibular 3 br. cable: main trunk to zygomatic,
buccal, and mandibular 3 br. cable: upper trunk to temporal,
zygornatic, and buccal 3 br. cable: main trunk to temporal,
zygornatic, and buccal 4 br. cable: upper trunk to 2 buccal br.
and 2 zygomatic br. 1 br. cable: lower trunk to mandibular 1 br. cable: upper trunk to zygomatic
Great auricular 4 br. cable: main trunk to temporal, zygomatic, buccal, and mandibular
'Named distal branches. SCC = squamous cell carcinoma.
Laryngoscope 109: June 1999 Reddy et al.: Facial Nerve Rehabilitation
895
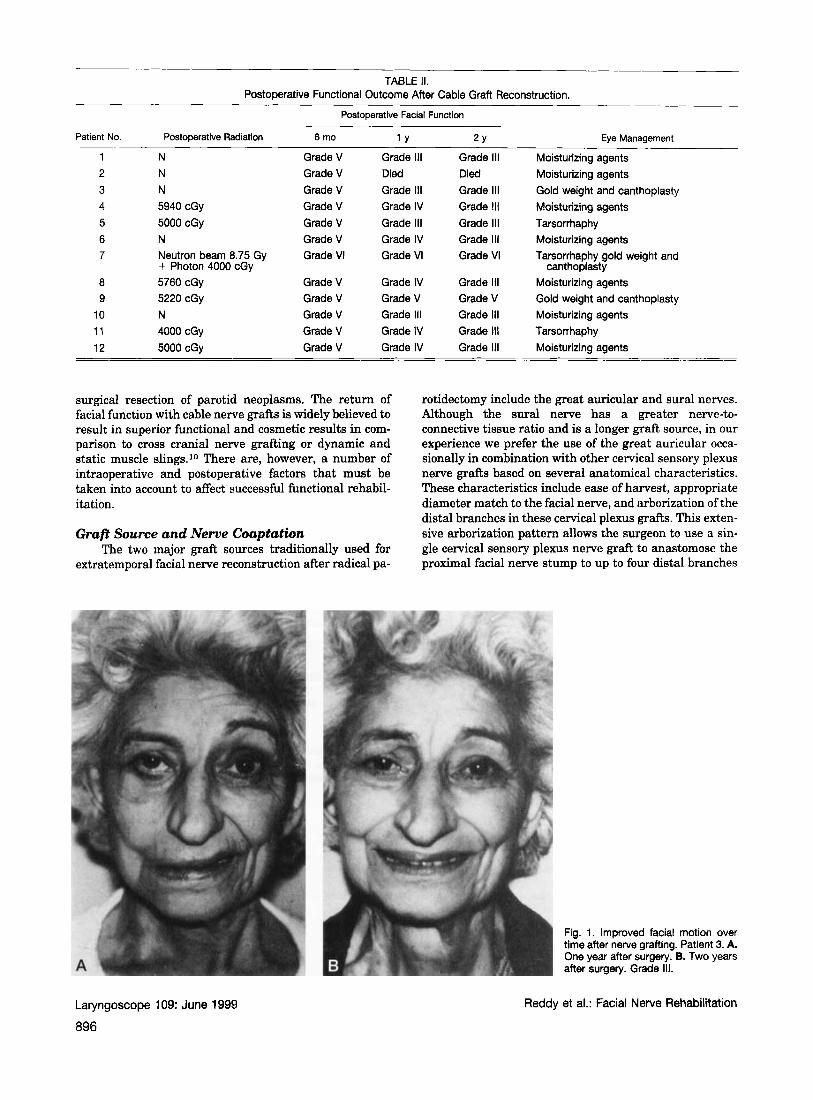
TABLE II. Postoperative Functional Outcome After Cable Graft Reconstruction.
Postoperative Facial Function
Patient No. Postoperative Radiation 6 mo 1 Y 2 Y Eye Management ~
1 N Grade V Grade 111 Grade 111 Moisturizing agents 2 N Grade V Died Died Moisturizing agents 3 N Grade V Grade 111 Grade Ill Gold weight and canthoplasty 4 5940 cGy Grade V Grade IV Grade 111 Moisturizing agents 5 5000 cGy Grade V Grade Ill Grade 111 6 N Grade V Grade IV Grade 111 Moisturizing agents 7 Neutron beam 8.75 Gy Grade VI Grade VI Grade VI Tarsorrhaphy gold weight and
8 5760 cGy Grade V Grade IV Grade 111 Moisturizing agents 9 5220 cGy Grade V Grade V Grade V Gold weight and canthoplasty
10 N Grade V Grade 111 Grade I l l Moisturizing agents 11 4000 cGy Grade V Grade IV Grade 111 Tarsorrhaphy 12 5000 cGy Grade V Grade IV Grade 111 Moisturizing agents
Tarsorrhaphy
+ Photon 4000 cGy canthoplasty
surgical resection of parotid neoplasms. The return of facial function with cable nerve grafts is widely believed to result in superior functional and cosmetic results in com- parison to cross cranial nerve grafting or dynamic and static muscle slings.10 There are, however, a number of intraoperative and postoperative factors that must be taken into account to affect successful functional rehabil- itation.
Graft Source and Nerve Coaptation The two major graft sources traditionally used for
extratemporal facial nerve reconstruction after radical pa-
rotidectomy include the great auricular and sural nerves. Although the sural nerve has a greater nerve-to- connective tissue ratio and is a longer graft source, in our experience we prefer the use of the great auricular occa- sionally in combination with other cervical sensory plexus nerve grafts based on several anatomical characteristics. These characteristics include ease of harvest, appropriate diameter match to the facial nerve, and arborization of the distal branches in these cervical plexus grafts. This exten- sive arborization pattern allows the surgeon to use a sin- gle cervical sensory plexus nerve graft to anastomose the proximal facial nerve stump to up to four distal branches
Fig. 1. Improved facial motion over time after nerve grafting. Patient 3. A. One year after surgery. B. Two years after surgery. Grade 111.
Laryngoscope 109: June 1999
896
Reddy et al.: Facial Nerve Rehabilitation
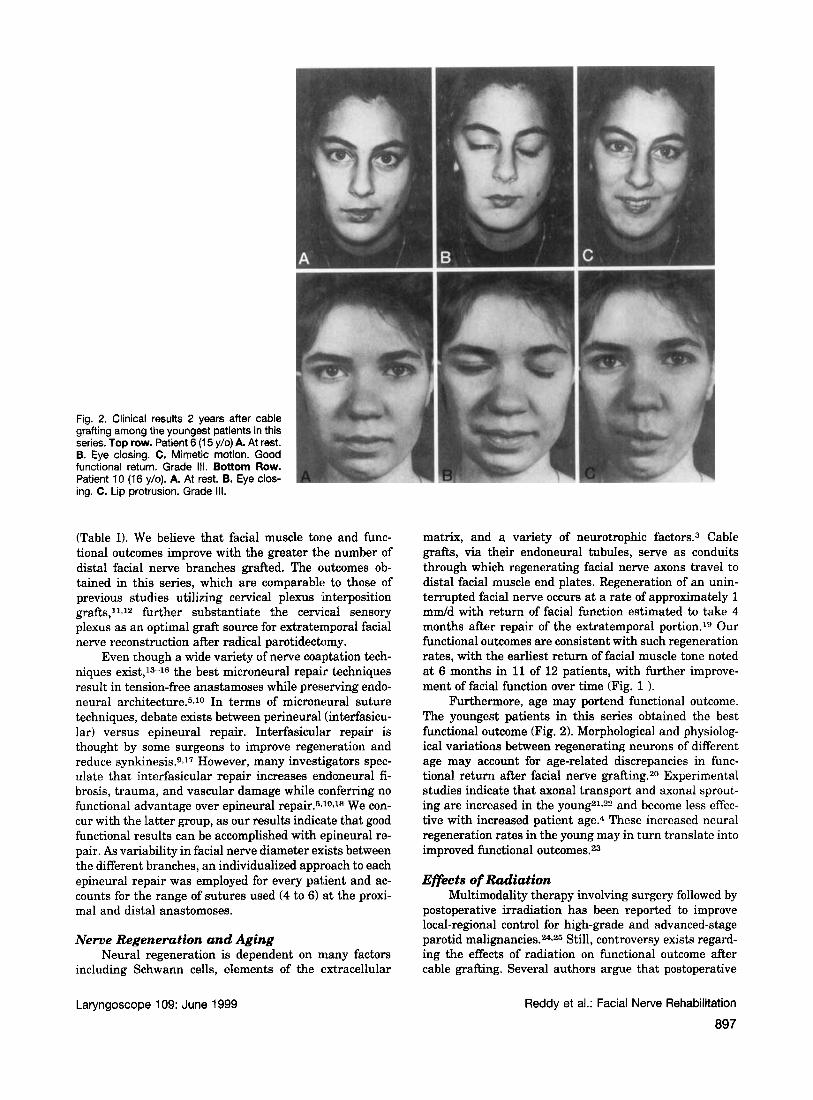
Fig. 2. Clinical results 2 years after cable grafting among the youngest patients in this series. Top row. Patient 6 (1 5 y/o) A. At rest. B. Eye closing. C. Mimetic motion. Good functional return. Grade 111. Bottom Row. Patient 10 (16 y/o). A. At rest. B. Eye clos- ing. C. Lip protrusion. Grade 111.
(Table I). We believe that facial muscle tone and fmc- tional outcomes improve with the greater the number of distal facial nerve branches grafted. "he outcomes ob- tained in this series, which are comparable to those of previous studies utilizing cervical plexus interposition grafts,l*J2 further substantiate the cervical sensory plexus as an optimal graft source for extratemporal facial nerve reconstruction after radical parotidectomy.
Even though a wide variety of nerve coaptation tech- niques exist,13-16 the best microneural repair techniques result in tension-free anastamoses while preserving endo- neural architecture.5.10 In terms of microneural suture techniques, debate exists between perineural (interfasicu- lar) versus epineural repair. Interfasicular repair is thought by some surgeons to improve regeneration and reduce synkinesis.gJ7 However, many investigators spec- ulate that interfasicular repair increases endoneural fi- brosis, trauma, and vascular damage while conferring no functional advantage over epineural repair.5JOJe We con- cur with the latter group, as our results indicate that good functional results can be accomplished with epineural re- pair. As variability in facial nerve diameter exists between the different branches, an individualized approach to each epineural repair was employed for every patient and ac- counts for the range of sutures used (4 to 6) at the proxi- mal and distal anastomoses.
Nerve Regeneration and Aging Neural regeneration is dependent on many factors
including Schwann cells, elements of the extracellular
matrix, and a variety of neurotrophic factor^.^ Cable grafts, via their endoneural tubules, serve as conduits through which regenerating facial nerve axons travel to distal facial muscle end plates. Regeneration of an unin- terrupted facial nerve occurs at a rate of approximately 1 m d d with return of facial function estimated to take 4 months after repair of the extratemporal portion.19 Our functional outcomes are consistent with such regeneration rates, with the earliest return of facial muscle tone noted at 6 months in 11 of 12 patients, with further improve- ment of facial function over time (Fig. 1 ).
Furthermore, age may portend functional outcome. The youngest patients in this series obtained the best functional outcome (Fig. 2). Morphological and physiolog- ical variations between regenerating neurons of different age may account for age-related discrepancies in func- tional return after facial nerve grafting.20 Experimental studies indicate that axonal transport and axonal sprout- ing are increased in the young21,22 and become less effec- tive with increased patient age.4 These increased neural regeneration rates in the young may in turn translate into improved functional outcomes.23
Eficts of Radiation Multimodality therapy involving surgery followed by
postoperative irradiation has been reported to improve local-regional control for high-grade and advanced-stage parotid malignancies.24.26 Still, controversy exists regard- ing the effects of radiation on functional outcome after cable grafting. Several authors argue that postoperative
Laryngoscope 109: June 1999 Reddy et al.: Facial Nerve Rehabilitation
897
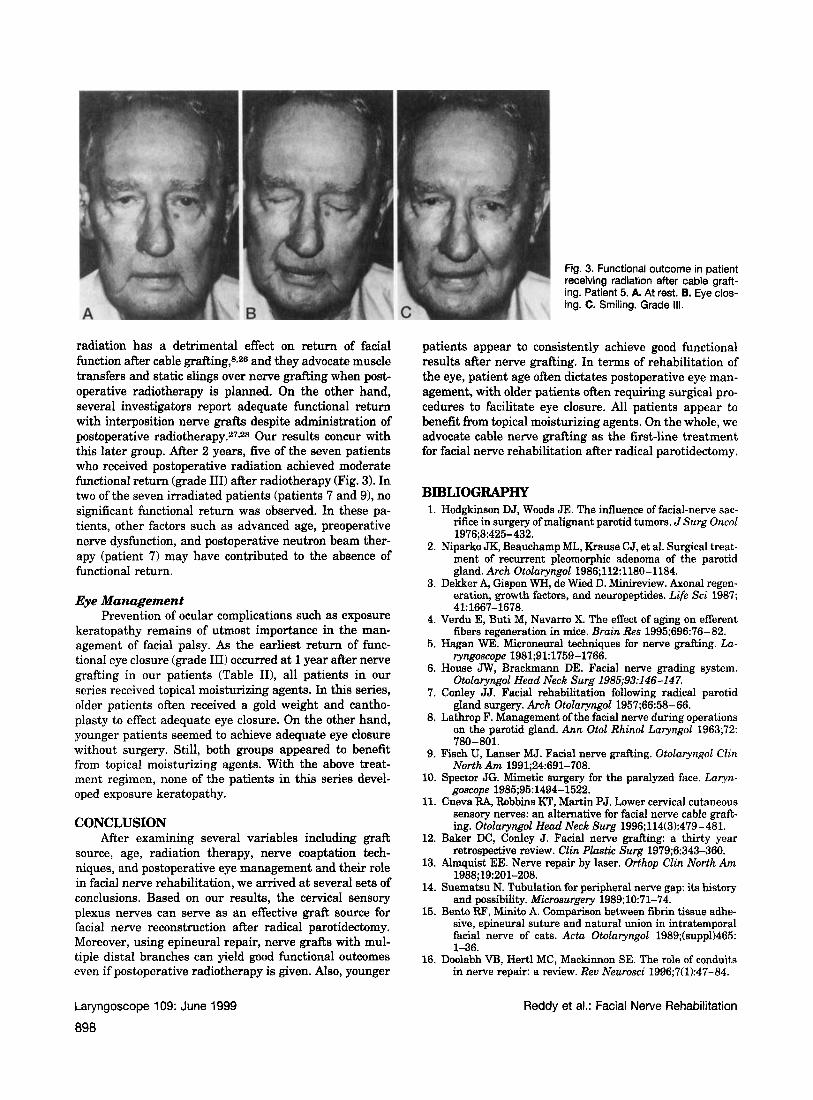
Fig. 3. Functional outcome in patient receiving radiation alter cable graft- ing. Patient 5. A. At rest. B. Eye clos- ing. C. Smiling. Grade I l l .
radiation has a detrimental effect on return of facial function after cable grafting,8926 and they advocate muscle transfers and static slings over nerve grafting when post- operative radiotherapy is planned. On the other hand, several investigators report adequate functional return with interposition nerve grafts despite administration of postoperative radiotherapy.27.28 Our results concur with this later group. After 2 years, five of the seven patients who received postoperative radiation achieved moderate functional return (grade 111) after radiotherapy (Fig. 3). In two of the seven irradiated patients (patients 7 and 91, no significant functional return was observed. In these pa- tients, other factors such as advanced age, preoperative nerve dysfunction, and postoperative neutron beam ther- apy (patient 7) may have contributed to the absence of functional return.
Eye Management Prevention of ocular complications such as exposure
keratopathy remains of utmost importance in the man- agement of facial palsy. As the earliest return of func- tional eye closure (grade 111) occurred at 1 year after nerve grafting in our patients (Table II), all patients in our series received topical moisturizing agents. In this series, older patients often received a gold weight and cantho- plasty to effect adequate eye closure. On the other hand, younger patients seemed to achieve adequate eye closure without surgery. Still, both groups appeared to benefit from topical moisturizing agents. With the above treat- ment regimen, none of the patients in this series devel- oped exposure keratopathy.
CONCLUSION After examining several variables including graft
source, age, radiation therapy, nerve coaptation tech- niques, and postoperative eye management and their role in facial nerve rehabilitation, we arrived at several sets of conclusions. Based on our results, the cervical sensory plexus nerves can serve as an effective graft source for facial nerve reconstruction after radical parotidectomy. Moreover, using epineural repair, nerve grafts with mul- tiple distal branches can yield good functional outcomes even if postoperative radiotherapy is given. Also, younger
patients appear to consistently achieve good functional results after nerve grafting. In terms of rehabilitation of the eye, patient age often dictates postoperative eye man- agement, with older patients often requiring surgical pro- cedures to facilitate eye closure. All patients appear to benefit from topical moisturizing agents. On the whole, we advocate cable nerve pafling as the first-line treatment for facial nerve rehabilitation after radical parotidectomy.
BIBLIOGRAPHY 1. Hodgkinson DJ, Woods JE. The influence of facial-nerve sac-
rifice in surgery of malignant parotid tumors. JSurg Oncol
2. Niparko JK, Beauchamp ML, Krause CJ, et al. Surgical treat- ment of recurrent pleomorphic adenoma of the parotid gland. Arch Otolaryngol 1986112:1180-1184.
3. Dekker A, Gispen WH, de Wied D. Minireview. Axonal regen- eration, growth factors, and neuropeptides. Life Sci 1987;
4. Verdu E, Buti M, Navarro X. The effect of aging on efferent fibers regeneration in mice. Brain Res 1995;696:76-82.
5. Hagan WE. Microneural techniques for nerve grafting. La- ryngoscope 1981;91:1759-1766.
6. House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck Surg 1985;93:146-147.
7. Conley JJ. Facial rehabilitation following radical parotid gland surgery. Arch Otolaryngol 1957;66:58-66.
8. Lathrop F. Management of the facial nerve during operations on the parotid gland. Ann Otol Rhino1 Laryngol 1963;72:
9. Fisch U, Lanser MJ. Facial nerve grafting. Otolaryngol CZin North Am 1991;24:691-708.
10. Spector JG. Mimetic surgery for the paralyzed face. Laryn- goscope 1985;95: 1494-1522.
11. Cueva RA, Robbins KT, Martin PJ. Lower cervical cutaneous sensory nerves: an alternative for facial nerve cable graft- ing. Otolaryngol Head Neck Surg 1996;114(3):479-481.
12. Baker DC, Conley J. Facial nerve grafting: a thirty year retrospective review. Clin Plastic Surg 1979;6:343-360.
13. Almquist EE. Nerve repair by laser. Orthop Clin North Am
14. Suematsu N. Tubulation for peripheral nerve gap: its history and possibility. Microsurgery 1989; 10:71-74.
15. Bento RF, Minito A. Comparison between fibrin tissue adhe- sive, epineural suture and natural union in intratemporal facial nerve of cats. Actu Otolaryngol 1989;(suppl)465: 1-36.
16. Doolabh VB, Hertl MC, Mackinnon SE. The role of conduits in nerve repair: a review. Rev Neurosci 1996;7(1):47-84.
1976;8:425-432.
41~1667-1678.
780-801.
1988;19:201-208.
Laryngoscope 109: June 1999
898
Reddy et al.: Facial Nerve Rehabilitation
17. Crumley RL. Interfasicular nerve repair. Is it applicable in facial nerve injuries? Arch Otolaryngol 1980;106:313-316.
18. Nine DG, Hudson AFt, Bratton BR. Experimental study of the fasicular nerve repair with and without epineural clo- sure. J Neurosurg 1981;54:513-520.
19. Adkins WY, Osguthorpe JD. Management of trauma of the facial nerve. Otolaryngol Clin North Am 1991;24:587-611.
20. Salimbeni-Ughi G. Evaluation of results in 36 cases of facial palsy treated with nerve grafts. Ann Plast Surg 1982;9(1):
21. Robbins N, Nakashiro S. Connections among plasticity, re- generation, and aging at the neuromuscular junction. Adu Neurol 1993;59:47-52.
22. Vaughan DW. Effects of advancing age on peripheral nerve regeneration. J Comp Neurol 1992;323:219-237.
23. Belin BM, Ball DJ, Langer JC, Bridge PM, Hagberg PK, Mackinnon SE. The effect of age on peripheral motor nerve
36-41.
Laryngoscope 109: June 1999
function after crush injury in the rat. J Trauma 1996;40(5):
24. Matsuba HM, Thawley SE, Devineni VR, et al. High-grade malignancies of the parotid gland: effective use of planned combined surgery and irradiation. Laryngoscope 1985;95:
25. Armstrong JC, Harrison LB, Spiro RH, et al. Malignant tu- mors of major salivary gland origin. A matched-pair anal- ysis of the role of combined surgery and postoperative radiotherapy. Arch Otolayngol 1990; 116:290 -293
26. Pillsbury HC, Fisch U. Extratemporal facial nerve grafting and radiotherapy. Arch Otolaryngol 1979; 105:441-446.
27. Conley JJ . Facial nerve grafting. Arch Otolaryngol 1961;73:
28. McGuirt WF, Welling B, McCabe BF. Facial nerve function following irradiated cable grafts. Laryngoscope 1989;99: 27-34.
775-777.
1059-1063.
322-327.
Reddy et al.: Facial Nerve Rehabilitation
a99