ec letter template - european commission
TRANSCRIPT
EUROPEAN COMMISSION JOINT RESEARCH CENTRE
Directorate F – Health, Consumers and Reference Materials
INJURY AND ACCIDENT DATA COLLECTION IN SUPPORT OF CONSUMER PRODUCT SAFETY AND MARKET
SURVEILLANCE (CPS-IAData project)
Administrative Arrangement
(DG JUST No JUST/2015/CONS/AA/CO03/0123, JRC No 34217)
FINAL REPORT

2
3
INJURY AND ACCIDENT DATA COLLECTION IN SUPPORT OF CONSUMER PRODUCT SAFETY AND MARKET
SURVEILLANCE (CPS-IAData project)
Administrative arrangement
(DG JUST No JUST/2015/CONS/AA/CO03/0123, JRC No 34217)

4
5
TABLE OF CONTENTS
TABLE OF CONTENTS .................................................................................................................................... 5
EXECUTIVE SUMMARY ................................................................................................................................. 6
1. Background and objectives .......................................................................................................................... 5
2. Activities performed and achievements in the context of the AA ............................................................. 10
3. Conclusions ............................................................................................................................................... 33
4. Glossary ..................................................................................................................................................... 35
5. Annexes ..................................................................................................................................................... 36
6
EXECUTIVE SUMMARY In the context of the European Union Consumer Programme 2014–2020, the Directorate F-Health, Consumers and Reference Materials, of the Joint Research Centre (JRC) of the European Commission provided scientific and technical support to the Directorate General for Justice and Consumers (DG JUST), via the administrative arrangement (AA) entitled "Technical and Scientific Support in the area of injury and accident data collection for product safety and market surveillance" (DG JUST No JUST/2015/CONS/AA/CO03/0123, JRC No 34217) (CPS-IAData project).
The purpose of the AA was to explore the potential for increasing the availability of information on injuries caused by unsafe consumer products. The study was based on a review of existing data collection practices in EU and opportunities arising from the use of novel IT technologies.
A number of data sources of potential interest to the consumer product safety policy work were identified. These data sources present pros and cons in terms of: data richness, fragmentation, availability and accessibility, harmonised data collection and data coding methodologies, terminology, networking capacity and funding availability for data collection activities, willingness for data sharing, risk of data misinterpretation or misuse (e.g. fake news, information manipulation).
A possible solution to use such a variety of data and formats, was identified in setting up a centralised modular European Consumer Product Safety Platform (ECPSP). In this IT platform, data from the revitalised and improved IDB-FDS, together with data from online media monitoring systems (e.g. EMM) for the detection of emerging threats from products entering the market, information extracted from consumers’ reported injuries and data from other relevant data sources (fire-fighter or poison centres records) could be pooled together, taking advantage of novel IT paradigms to link different data sources containing structured, unstructured and semi-structured data. This could be complemented by information retrieved from deep investigations into mortality statistics (causes of death) in terms of consumer product involvement.
With respect to the sustainability and quality of data from the above listed potential data providers, some challenges have been identified, which may require coordinated and long-term actions as well as significant resources to be shared by various stakeholders (MS, EC, private sector). In addition, a more detailed analysis needs to be carried out to conclude on the feasibility, cost/benefit ratio and impact of the proposed options.
5
1. Background and objectives
1.1. Injury and accident data for consumer safety and market surveillance
The availability of data on accidents and injuries caused by unsafe products contributes to a proper functioning of product safety and market surveillance policy efforts. Detailed information on the circumstances of accidents leading to injuries can help to reveal the presence of dangerous products in the market, new products posing new risks, or help the setting of appropriate safety requirements by standardization. The support to product safety and market surveillance policy work could translate into larger societal benefits: information helpful for better product design and improved and more targeted prevention could lead in the future to more targeted allocation of resources in market surveillance and, more largely, reduced health related costs in treatment of injuries, hospitalisation or incapacity to work.
In Europe, the current data collection practices on injuries can be described as extremely diverse, involving different authorities and sectors. Injury surveillance carried out in hospitals’ emergency departments represents a systematic source of data about accidents and injuries in many countries. Yet, monitoring injuries in emergency departments is only one of the possible systems: for example, the information from national poison centres could be useful to identify dangerous substances in consumer products and relevant exposure channels. Likewise, databases maintained by fire brigades or other public bodies could deliver interesting information on specific categories of accidents. In addition, business operators' records on complaints, incidents or accidents, or studies undertaken by non-governmental organisations could also offer valuable data. Finally, also the reports and complaints of consumers to the public authorities themselves could contain useful input for a systematic collection of relevant information.
Whereas the amount of information available and potentially of use for market surveillance and product safety policy and enforcement at national level is considerable, its usability is difficult due to high fragmentation of the data sources and collection methods. Injury surveillance and injury information generated in the EU nowadays can be characterised as "operating on an incomplete puzzle of data sources"1. Data collection is often not comparable between countries, or between registers, due to the lack of a harmonised methodology and classification scheme.
This current situation therefore unveils a challenge: creating added value would be possible by identifying links, generating cross-sector and cross-border synergies and attempting higher centralisation of the data retrieval, analysis and reporting. The work towards the search for links and synergies may help achieving better and larger perspectives and trends of injuries and accidents and products involved, which in turn could fill in the gaps currently hampering an adequate use of data on injuries and accident in the area of product safety.
This would also allow a more accurate quantification of the burden of injuries on the citizens and health services. Currently available information on injuries tends to focus primarily on fatal injuries, which represent only one part of the total burden of injuries,
1 R. Kisser, J. Latarjet, R. Bauer and W. Rogmans (2009). Injury data needs and opportunities in Europe, International Journal of Injury Control and Safety Promotion, Vol. 16, No. 2, p103.

6
as mortality is usually connected with increase in morbidity. Both mortality and morbidity are not only important sources of human suffering, but also cause a heavy economic burden on national health related budgets.
The aim of ensuring inter-links among existing data sources on accidents and injuries would not only bring the benefits to the market surveillance and product safety activities. Injury and accident data serve already other sectors and policies such as health information, public security or road safety; therefore, although the policy domains outside product safety and market surveillance are not directly the focus of this project, there can be interesting and fruitful spill over effects.
Many safety policy actions in the field of road safety or safety at work have shown that injuries can be prevented, by making our living environment, as well as products and services safer. Targeted injury prevention must be based on evidence and requires data on consumers’ activities, accidents conditions, and injuries.
Not only information about victims, diagnoses and consequences of injuries is needed, but also about circumstances and risk factors like activities, products, services, and settings involved (external causes of injuries). Information on the external causes of injuries is a prerequisite to targeted preventive actions.
Consumer products are used extensively across a wide range of settings - homes, workplaces, day care centres and schools - and as external cause are involved in a significant proportion of injuries. Previous studies estimate that home and leisure injuries represent substantial part of all unintentional injuries and can contribute to high hospital cost burden.2,3 Accurate injury data which contain information on the involvement of the products in injuries, could therefore significantly contribute to the identification of trends, emerging hazards and for evidence based consumer safety policy in the EU.
1.2. Policy background and legal context
The need for proper injury surveillance systems has long been recognised by the World Health Organization (WHO). In 2011, the WHO report on “Injury Surveillance Guidelines”4 outlines the reasons for which injury surveillance systems are indispensable, namely: to estimate the community burden of injury; to monitor injury trends over time; to detect clusters of injury events by time, person and place; to prioritise and evaluate strategies for injury prevention; to set directions for injury-prevention research and to inform the development of injury prevention policies. Optimal injury surveillance systems provide information on what injuries occurred, to whom, where, when and why.
To tackle the growing problem of high fragmentation and incompleteness of data on injuries, the EU Council in 2007 issued a Recommendation on the prevention of injury and the promotion of safety5 that invites Member States to improve the usage of the
2 EuroSafe: Injuries in the European Union, Summary on injury statistics 2012-2014, Amsterdam 2016. http://www.eurosafe.eu.com/uploads/inline-files/EuropeSafe_Master_Web_02112016%20%282%29.pdf 3 C. Bonaldi, Cécile Ricard, J. Nicolau, M. Bouilly and B. Thélot. Estimates of home and leisure injuries treated in emergency departments in the adult population living in metropolitan France: a model-assisted approach. Population Health Metrics (2014) 12:2 4 WHO report on ‘Injuries Surveillance Guidelines’ http://apps.who.int/iris/bitstream/10665/42451/1/9241591331.pdf 5 COUNCIL RECOMMENDATION of 31 May 2007 on the prevention of injury and the promotion of safety. http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32007H0718%2801%29&from=EN
7
existing data on the national level, and engage in development of additional injury surveillance tools, in order to obtain comparable information. It also invited the European Commission to establish and support the community-wide injury prevention and surveillance activities. The Recommendation reported that on average, injuries6 account for about seven million hospital admissions, which represent 11% of all hospital admissions in the European Union. Injuries represent a huge financial burden on health and welfare systems, causing about 20% of sick leave and constituting a major factor for reduced productivity. In addition, every year, about 235 000 citizens of the EU die as a result of an accident or violence. Injuries are, after cardiovascular diseases, cancer and respiratory diseases, the fourth most common cause of death in the EU Member States. This document recommends EU Member States to:
Make better use of existing data and develop where appropriate injury surveillance and reporting tools to obtain comparable information, monitor trends and efficacy of preventive measures, assess the need for other actions.
Set up national action plans for preventing injuries, initiating interdepartmental and international coordination. Such plans should pay special attention to vulnerable groups, sports and leisure injuries, injuries caused by products and services, violence and self-harm.
Engage in activities for promotion of injury prevention and safety in schools, health institutions etc.
An evaluation of the outcomes of the '2007 Recommendation' has been carried out in 201110: it highlights the important role played by the Recommendation in intensifying the availability of data and setting up systems for data collection. However, the report suggests further harmonisation of surveillance and reporting, further investments in EU countries which have not yet developed systematic injury data collection systems, as well as adaptations in the classification of priority areas to improve comparability and reduce overlaps.
A reference to the importance of monitoring accidents and injuries, more widely, can be found in the Regulation (EC) No 765/2008 setting out the requirements for accreditation and market surveillance relating to the marketing of products11. Under Article 18, the Regulation requires Member States to “establish adequate procedures in order to […] monitor accidents and harm to health which are suspected to have been caused by those products; […]”.
Calls for accident data collection and injury surveillance have been recurring at both European and international level. The World Health Organisation (WHO) recognised the need for attention and investments in injury surveillance with an important resolution of the WHO Regional Committee for Europe in 2005 (WHO-EUR/RC55/R912). At European level, the Communication COM(2006)328 from the Commission to the Council
6 The Recommendation here refers to all injuries, unintentional and intentional, not specifically to injuries caused by the use of potentially unsafe consumer products. 10 IBF International Consulting "Evaluation Report on the Implementation of the 2007 Council Recommendation on the prevention of injury and the promotion of safety", Contract No. 17030600/11/605156. 11 http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2008:218:0030:0047:en:PDF 12 http://www.euro.who.int/en/about-us/governance/regional-committee-for-europe/past-sessions/fifty-fifth-session/resolutions/eurrc55r9
8
and the European Parliament on Actions for a Safer Europe13 recommended taking action on evidence-based injury surveillance in safety areas less explored, in particular on safety at home and during leisure time, as well as safety of vulnerable populations such as children and senior citizens.
The need for EU wide accident and injury data has been suggested by the 2011 European Parliament Report on the revision of the General Product Safety Directive and Market Surveillance14. The report calls for a consumer product safety information database which should include injury data and could derive information from existing data sources.
In the Communication COM(2013)76 from the Commission to the European Parliament, the Council and the Economic and Social Committee on a multi-annual plan for the surveillance of products in the EU15, 20 actions for safer and more compliant products are indicated. In one of the proposed actions, the European Commission commits to examine the costs and benefits of an EU accident/injury database containing a platform for both complaints and injuries. The Communication was adopted by the Commission as part of the proposed legislative package on Product Safety and Market Surveillance in February 2013.
The question of a Pan-European injury database, coordinated by the European Commission, has been posed in a joint call by a large group of stakeholders including business and consumers organisations16. This issue has also been raised in the framework of the negotiations on the Consumer Product Safety and Market Surveillance Regulations by European Parliament17. In this context, the European Parliament adopted amendments that would require the Commission to establish a "Pan-European injury database" covering injuries related to products used at home, and for leisure, transportation, and work activities.18
On the international scene, the OECD Working Party on Consumer Product Safety has also recognised the importance of improving injury data availability as a tool for protecting consumers and proposed the establishment of a platform for global pooling of injury data (Global Injury Data portal), among the ten recommendations, in a 2010 report on work to be undertaken by the newly chartered group.19
13http://www.europarl.europa.eu/meetdocs/2004_2009/documents/com/com_com%282006%290328_/com_com13%282006%290328_en.pdf 14 http://www.europarl.europa.eu/sides/getDoc.do?pubRef=-//EP//TEXT+REPORT+A7-2011-0033+0+DOC+XML+V0//EN 15 http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:52013DC0076&from=EN 16 The need for a pan-European accident and injury data system. Joint Call. http://www.anec.eu/attachments/Joint%20call%20for%20a%20pan-European%20accident%20&%20injury%20data%20system.pdf 17 COM(2013) 78 final, Proposal for a Regulation of the European Parliament and of the Council on consumer product safety and repealing Council Directive 87/357/EEC and Directive 2001/95/EC; COM(2013) 75 final, Proposal for Regulation of the European Parliament and of the Council on market surveillance of products 18 Amendment adopted by the European Parliament to Art 21a of the COM(2013) 75 final, Proposal for Regulation of the European Parliament and of the Council on market surveillance of products. http://www.europarl.europa.eu/meetdocs/2009_2014/documents/imco/dv/ca_msp_fin1_/ca_msp_fin1_en.pdf 19 OECD Woking Party on Consumer Safety. Global injury data portal: Project roadmap. http://search.oecd.org/officialdocuments/publicdisplaydocumentpdf/?cote=DSTI/CP/CPS%282014%2913&docLanguage=En
9
1.3. Objectives of the AA
Through the technical and scientific support provided by DG JRC to DG JUST via this AA, the main goal is to increase the potential value and the use of available injury and accident data across Europe in support of market surveillance and product safety policy work. Objectives of the AA were described in four Work Packages (WP):
1. To complete the map resulting from the survey among EU Member State authorities carried out in 2014, with a view of having a reliable picture on European sources of data on injuries/accidents of relevance for product safety and market surveillance policy work;
2. To explore feasible technical options to improve the interoperability of existing product-related databases and other data known or feasible pooling mechanisms and to develop a Data Policy framework to state the general principles of and provide guidance and rules about the data accessibility, sharing and use by the owners of those data collections systems, including specifying data protection issues;
3. To develop a method to organise/filter/extract/use the available data trends and to support the identification of possible priorities for actions to enhance consumer safety;
4. To identify possible gap filling actions and their associated costs which could “upgrade” existing data collected across Europe into valuable ones for product safety.
10
2. Activities performed and achievements in the context of the AA
The work was performed according to the technical annex of the AA DG JUST No JUST/2015/CONS/AA/CO03/0123, JRC No 34217; the achievements are summarised below.
Work Package 1: Complete the mapping of existing national databases on injuries and accidents of relevance for consumer product safety initiated by the 2014 survey
Sub-tasks:
Sub-task 1.1: Identify other potentially existing systems similar to the ones described in the 2014 survey in the EU Member States and possibly suggest/identify datasets not yet reflected in the outcome of the survey.
Sub-task 1.1 was carried out in three steps:
A systematic literature-review (following the PRISMA approach20) covering the period 2000 - 2016 (Science Direct, Scopus, PubMed) and Google search in the area of injury data collection.
A questionnaire survey was prepared covering alternative potential data sources on injuries that were not explored in DG JUST Survey 2014. The respective responsible authorities were contacted and interviewed, including: European and MS associations of firefighting and rescue services, poison centres, toy producers and insurances.
Selected EU experts in the field of injury data collection and consumer product safety were contacted and interviewed (by email, phone, in person).
A systematic literature review was conducted based on a simplified version of the PRISMA methodology (Preferred Reporting Items for Systematic Review and Meta-Analyses) that follows a transparent and traceable approach to identify, select and critically appraise relevant research. Selected publications provided the peer-reviewed information on the world wide status in the area of injury data collection. Over 1000 abstracts have been reviewed for relevance in each of the searched scientific database (Science Direct, Scopus, PubMed). Selected publications were ordered and consulted. This step provided the first list of existing databases/data sources on injuries and accidents of potential relevance for consumer product safety. This step also provided the names of the experts in the field of injury data collection, analyses and reporting. Identification through the PRISMA literature research methodology had the limitation that only data sources published in peer-reviewed journals and in English language were detected. In order to avoid that the institutions with a less academic/research are underrepresented, the literature review was complemented by a questionnaire survey. In consultation with the DG JUST coordinator a number of experts (over 80) have been contacted by JRC (via e-mail, phone, in person) and were asked to participate in the
20 Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009) Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med6(7): e1000097. https://doi.org/10.1371/journal.pmed.1000097
11
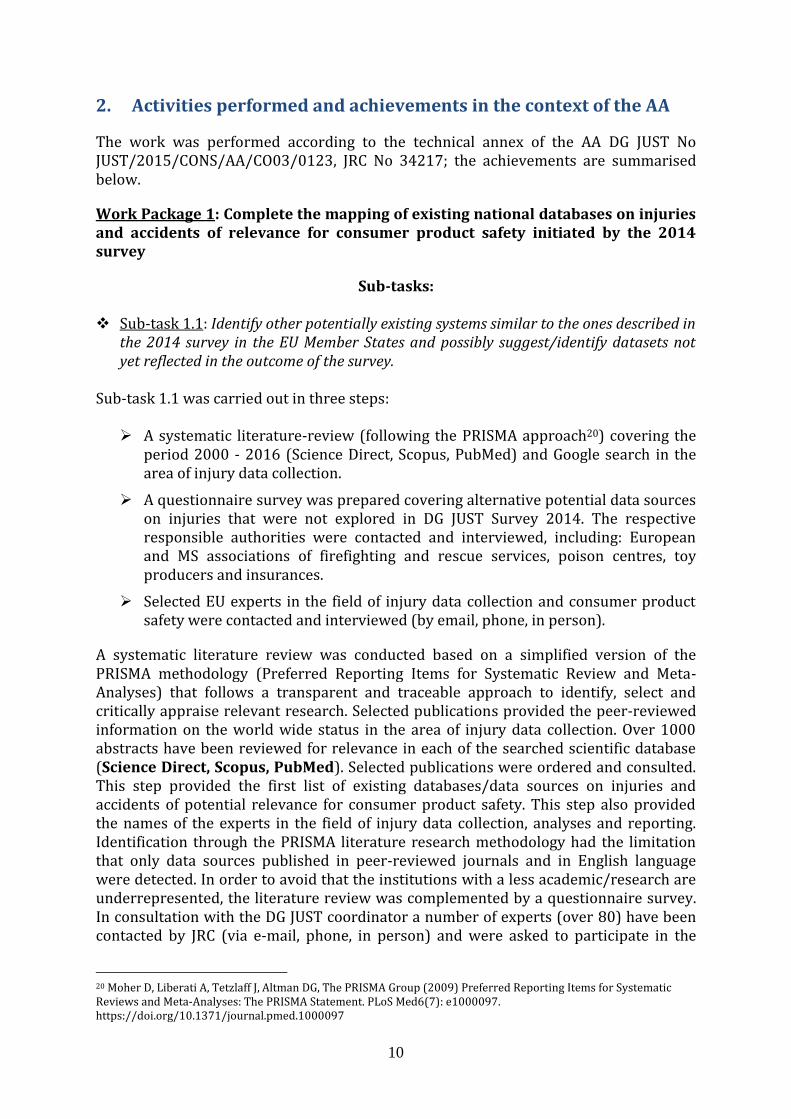
survey and provide information on existing injury data collection practices in their institutions, of potential relevance to consumer safety. This survey targeted institutions that were not interviewed in the 2014 survey, previously conducted by DG JUST, and in addition aimed at the identification of potential 'alternative' injury data sources, from the fire-brigade and rescue services, poison centres, toys associations/industry and insurance companies and their corresponding EU roof associations. The profile of sectors that were covered by the survey is visualised in Figure 1.
Figure 1. Sectors covered by questionnaire survey
While the initial response rate to the questionnaire was slow, finally it was turned out to be satisfactory (82% response rate).
The list of existing databases/data sources on injuries and accidents of potential relevance for consumer product safety is provided in Annex 1.
This list resulted from combining the information from DG JUST Survey 2014 and that from the work carried out in the WP1 of this AA (literature review, survey) in the period June-September 2016. It does not represent an exhaustive list of all Member States institutions collecting injury data; it contains only those of direct relevance to the AA project’s objectives that resulted from the literature review and from the institutions that provided response to the JRC survey questionnaire 2016. Yet, not all existing injury data collection systems are publicly available.
Sub-task 1.2: Refine the categorisation of the various injuries and accident databases
and assess the added value of each category for product safety and market surveillance Sub-task 1.2 required more detailed understanding of data sets that are collected in the context of each assessed category (fire-brigades association, poison centres etc.). This information has been collected to a good extent by contacting directly the responsible data providers/managers; however, this was not always possible, as some data collections are not publicly accessible. In addition, the institutions collecting injury data on the European level are not well interconnected, therefore DG JRC/F.2 organised a
12
one-day Workshop to understand better existing current practices on injury data collection efforts in EU and related challenges.
The specific activities that were carried out to complete sub-task 1.2 were:
Preparation of an inventory of categorised databases with potential relevance for product safety and market surveillance.
Organisation of one-day experts' Workshop at JRC (25 October 2016, Ispra).
The Workshop was a good opportunity to present the CPS-IAData project’s objectives to the selected panel of experts along with the survey outcomes and the inventory of injury databases produced in sub-task 1.1, and discuss current trends, challenges and future perspectives of injury data collection efforts in EU.
The participants shared their common understanding that currently the European Injury Database (IDB)21 is the only data source which was primarily designed for and dedicated to consumer safety. The IDB data, in particular its full data set (IDB-FDS22), are collected in a relevant number of hospitals in Member States, with a common methodology and could provide relevant information as support to standardisation work or product safety legislation and market surveillance efforts (although, at present, with some shortcomings, which may require substantial resources). A list of opportunities and challenges that should be faced for optimizing the IDB-FDS system is provided by SWOT analyses in Chapter 2.1.1 (Table 2). All other data sources identified in sub-task 1.1, including those managed by firefighter brigades, poison centres and insurance companies are tailored for purposes other than product safety. In many cases, in their current format, they do not include all required product related information directly and/or the information does not have the required 'quality' (e.g. data-set size, territorial coverage).
During the workshop, technical options for enabling interoperability of IDB with alternative data sources (i.e. poison centres data, fire-brigade data, online survey data, mortality data, and data pooled from media monitoring systems) were also discussed. The EC’s IPCHEM platform (Information Platform for Chemical Monitoring) that represents the reference platform in EU for retrieving, accessing and sharing chemical monitoring data collections from different data sources was proposed as the paradigm to follow for enabling interoperability among various data and information sources.
Overall, it was concluded that:
At present, the level of EU cooperation on collection of injury data is poor (except for mortality statistics, occupational and road accidents that are well defined and embedded in legislation), including the weak future prospects of IDB unless actions are taken to make it sustainable on a long-term basis.
Direct interoperability of most of the existing data sources using a common template, does not seem a feasible solution at present. The goal of trying to directly extract product-related injury data from data sources not created for this purpose (i.e. secondary data usage) is currently not promising and might be
21 https://ec.europa.eu/health/data_collection/databases/idb_en 22 IDB-FDS contains data on injuries caused by unintentional accidents, violence, suicide, road accidents and has extensive
methodology for coding of objects involved in the injury, places and mechanisms of injuries:
http://www.eurosafe.eu.com/uploads/inline-files/IDB%20JAMIE%20FDS%20Data%20Dictionary%20MAR14.pdf
13
too ambitious in terms of time and cost intensiveness and relevance of the data obtained.
Harmonising product categorisations across all data categories relevant to injuries/accidents seems not to be a viable solution, as most of the 'alternative' systems do not collect intentionally product related data.
The idea of creating a common IT platform for retrieving, accessing and sharing various data and information on injuries relevant for consumer product safety, looks appealing and promising. However, it could not deliver the expected benefits as long as all relevant databases/information systems to be interconnected will not provide the desired quality and type of information on the linkage of injuries/accidents to specific product(s) and with a wide coverage (i.e. from a significant number of countries and on a significant number of cases). The paradigm of the IPCHEM platform was considered premature to adopt and implement for many of the identified data-sources due to the highly fragmented and incomplete data sources related to product safety. Nevertheless, despite current drawbacks, data coming from some sectors (e.g. online media mining, fire-fighters records, poison centres records, consumer complaints) were seen as potential future drivers for spotting emerging issues in product safety.
Investigating on causes of death (mortality statistics) in terms of consumer product involvement was seen as an area with data gap in Europe: such investigations would provide information on emerging, long-term or seasonal trends in fatalities that could in future be prevented. Similar work is already being done by the US Consumer Product Safety Commission.
Options for bringing data from different sectors into one access point have been further investigated in the context of WP 2 and 3 of the AA (see next sections of this report).
Work Package 2: Feasibility study on technical options for linking existing product-related injury and accident databases and other data pooling mechanisms in EU Member States
Subtasks:
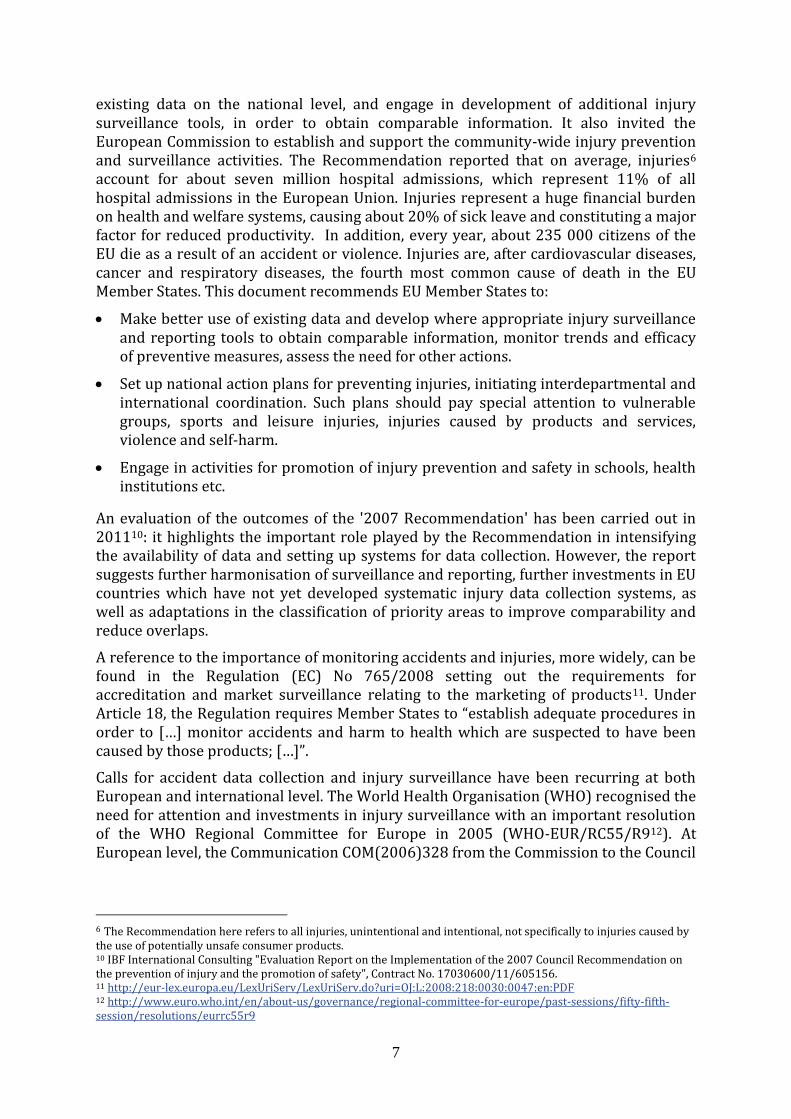
Sub-task 2.1: Analysis of methodological implications JRC explored technical options for building up a unique access point for retrieving information on potentially unsafe consumer products. Figure 2 shows potential data sources, providing structured, semi-structured and unstructured data to this platform, using existing data collection practices, but also taking advantage of the new technical and online media opportunities. The proposed integrated IT platform is provisionally named European Consumer Product Safety Platform (ECPSP).
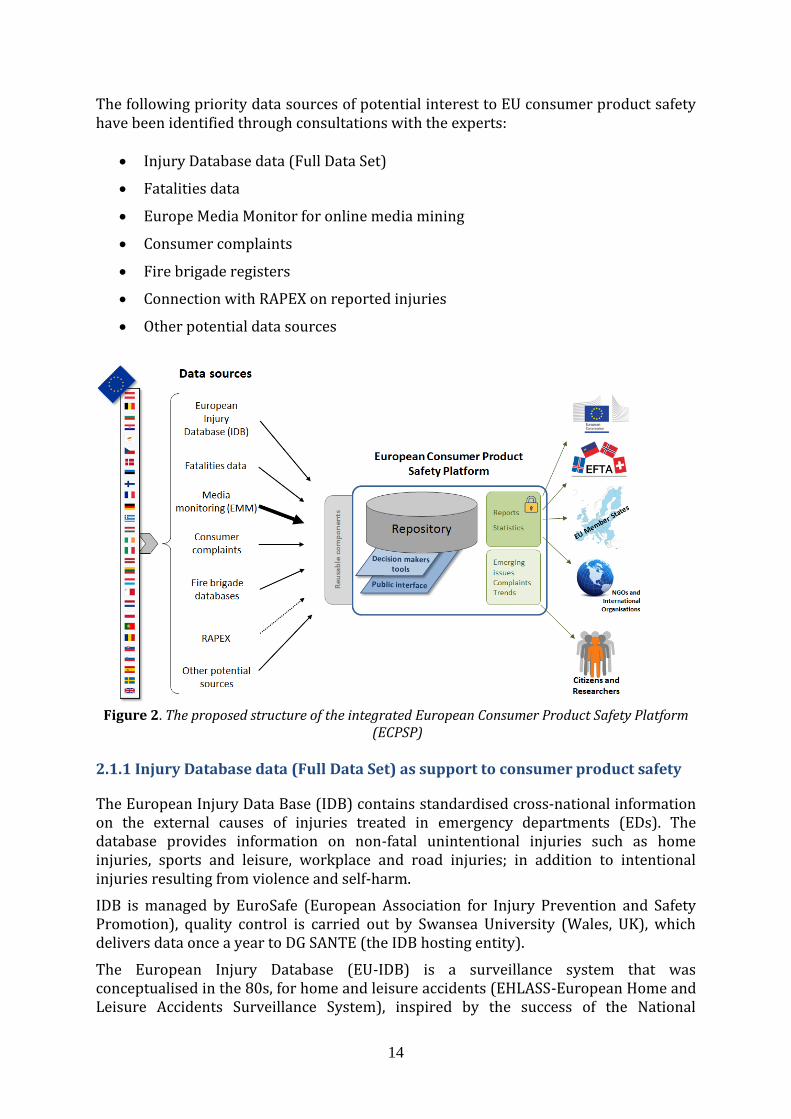
14
The following priority data sources of potential interest to EU consumer product safety have been identified through consultations with the experts:
Injury Database data (Full Data Set)
Fatalities data
Europe Media Monitor for online media mining
Consumer complaints
Fire brigade registers
Connection with RAPEX on reported injuries
Other potential data sources
Figure 2. The proposed structure of the integrated European Consumer Product Safety Platform
(ECPSP) 2.1.1 Injury Database data (Full Data Set) as support to consumer product safety
The European Injury Data Base (IDB) contains standardised cross-national information on the external causes of injuries treated in emergency departments (EDs). The database provides information on non-fatal unintentional injuries such as home injuries, sports and leisure, workplace and road injuries; in addition to intentional injuries resulting from violence and self-harm.
IDB is managed by EuroSafe (European Association for Injury Prevention and Safety Promotion), quality control is carried out by Swansea University (Wales, UK), which delivers data once a year to DG SANTE (the IDB hosting entity).
The European Injury Database (EU-IDB) is a surveillance system that was conceptualised in the 80s, for home and leisure accidents (EHLASS-European Home and Leisure Accidents Surveillance System), inspired by the success of the National
15
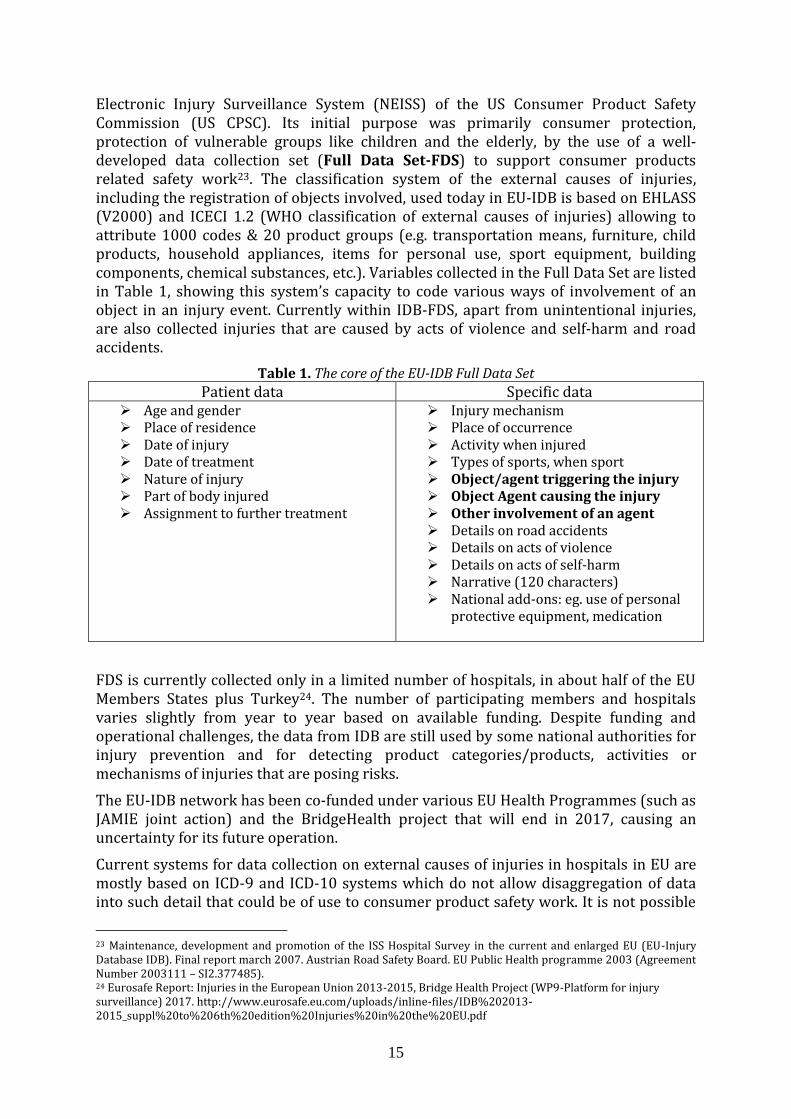
Electronic Injury Surveillance System (NEISS) of the US Consumer Product Safety Commission (US CPSC). Its initial purpose was primarily consumer protection, protection of vulnerable groups like children and the elderly, by the use of a well-developed data collection set (Full Data Set-FDS) to support consumer products related safety work23. The classification system of the external causes of injuries, including the registration of objects involved, used today in EU-IDB is based on EHLASS (V2000) and ICECI 1.2 (WHO classification of external causes of injuries) allowing to attribute 1000 codes & 20 product groups (e.g. transportation means, furniture, child products, household appliances, items for personal use, sport equipment, building components, chemical substances, etc.). Variables collected in the Full Data Set are listed in Table 1, showing this system’s capacity to code various ways of involvement of an object in an injury event. Currently within IDB-FDS, apart from unintentional injuries, are also collected injuries that are caused by acts of violence and self-harm and road accidents.
Table 1. The core of the EU-IDB Full Data Set
Patient data Specific data Age and gender Place of residence Date of injury Date of treatment Nature of injury Part of body injured Assignment to further treatment
Injury mechanism Place of occurrence Activity when injured Types of sports, when sport Object/agent triggering the injury Object Agent causing the injury Other involvement of an agent Details on road accidents Details on acts of violence Details on acts of self-harm Narrative (120 characters) National add-ons: eg. use of personal
protective equipment, medication
FDS is currently collected only in a limited number of hospitals, in about half of the EU Members States plus Turkey24. The number of participating members and hospitals varies slightly from year to year based on available funding. Despite funding and operational challenges, the data from IDB are still used by some national authorities for injury prevention and for detecting product categories/products, activities or mechanisms of injuries that are posing risks.
The EU-IDB network has been co-funded under various EU Health Programmes (such as JAMIE joint action) and the BridgeHealth project that will end in 2017, causing an uncertainty for its future operation.
Current systems for data collection on external causes of injuries in hospitals in EU are mostly based on ICD-9 and ICD-10 systems which do not allow disaggregation of data into such detail that could be of use to consumer product safety work. It is not possible
23 Maintenance, development and promotion of the ISS Hospital Survey in the current and enlarged EU (EU-Injury Database IDB). Final report march 2007. Austrian Road Safety Board. EU Public Health programme 2003 (Agreement Number 2003111 – SI2.377485). 24 Eurosafe Report: Injuries in the European Union 2013-2015, Bridge Health Project (WP9-Platform for injury surveillance) 2017. http://www.eurosafe.eu.com/uploads/inline-files/IDB%202013-2015_suppl%20to%206th%20edition%20Injuries%20in%20the%20EU.pdf

16
to identify specific products that are involved in an injury event. Therefore, a system that use ICECI classification, such as data from IDB-FDS can be used for the following tasks:
Identifying the product or the product category that presents the highest risk. Currently the system contains product categories (ICECI)25, but the information on the brand, product name or age of a specific product is not recorded.
Identifying the subject at risk: by gender, age, location or activity
Describing the hazard: by product involvement, mechanism of injury, narrative
Describing the severity of injury: by part of body injured, by days of hospital care, disability weights (only for non-fatal injuries)
Determining the probability of injury: in combination with additional exposure data.
Detailed product related information (e.g. brand name) could be obtained by the designated national authorities for consumer safety through follow-up studies in collaboration with hospitals. Such methodology of follow-up studies is frequently applied at US NEISS and some EU countries, since time constraints and the severity of incidents prevents the collection of detailed information on products in hospitals or emergency departments.
25 International Classification of External Causes of Injuries v1.2. Example of coding objects involved in
injuries see section C3/page 58: http://www.who-
fic.nl/dsresource?type=pdf&disposition=inline&objectid=rivmp:330718&versionid=&subobjectname=
17
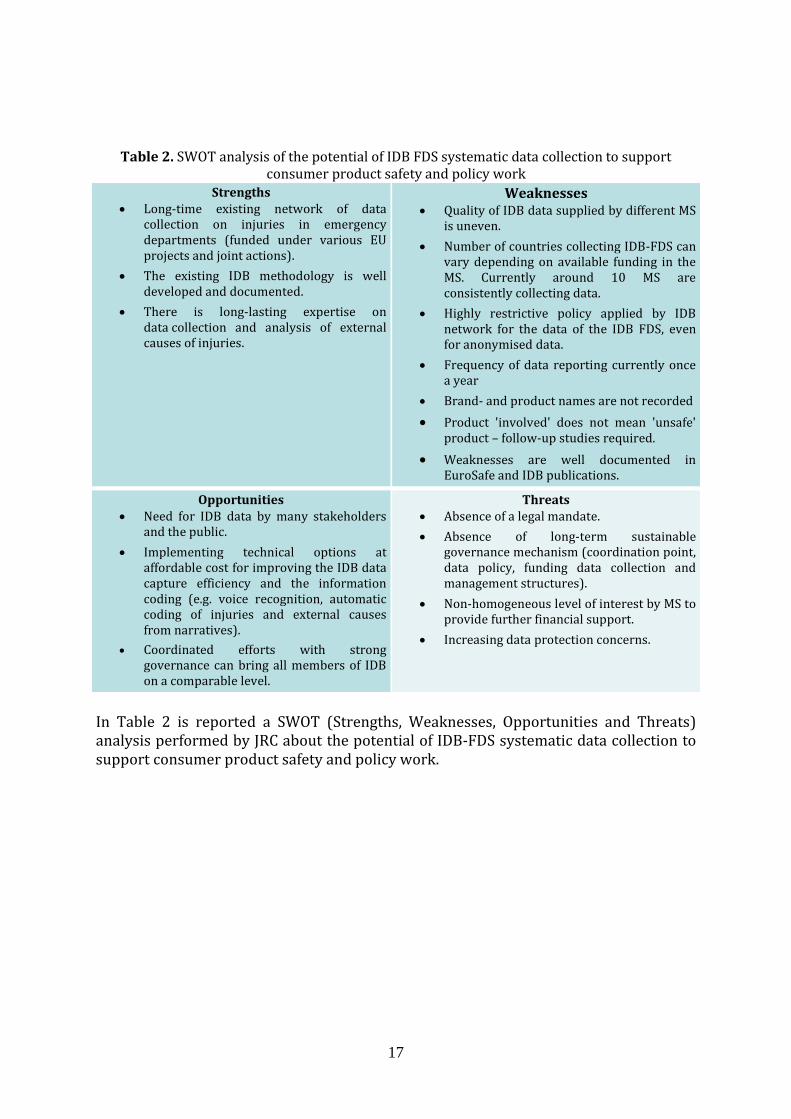
Table 2. SWOT analysis of the potential of IDB FDS systematic data collection to support consumer product safety and policy work
Strengths Long-time existing network of data
collection on injuries in emergency departments (funded under various EU projects and joint actions).
The existing IDB methodology is well developed and documented.
There is long-lasting expertise on data collection and analysis of external causes of injuries.
Weaknesses Quality of IDB data supplied by different MS
is uneven.
Number of countries collecting IDB-FDS can vary depending on available funding in the MS. Currently around 10 MS are consistently collecting data.
Highly restrictive policy applied by IDB network for the data of the IDB FDS, even for anonymised data.
Frequency of data reporting currently once a year
Brand- and product names are not recorded
Product 'involved' does not mean 'unsafe' product – follow-up studies required.
Weaknesses are well documented in EuroSafe and IDB publications.
Opportunities Need for IDB data by many stakeholders
and the public.
Implementing technical options at affordable cost for improving the IDB data capture efficiency and the information coding (e.g. voice recognition, automatic coding of injuries and external causes from narratives).
Coordinated efforts with strong governance can bring all members of IDB on a comparable level.
Threats Absence of a legal mandate.
Absence of long-term sustainable governance mechanism (coordination point, data policy, funding data collection and management structures).
Non-homogeneous level of interest by MS to provide further financial support.
Increasing data protection concerns.
In Table 2 is reported a SWOT (Strengths, Weaknesses, Opportunities and Threats) analysis performed by JRC about the potential of IDB-FDS systematic data collection to support consumer product safety and policy work.
18
2.1.2. Fatalities statistics in support of consumer product safety
Mortality statistics is one of the most complete data collection practices in Europe. In all EU countries, the medical certification of death was made mandatory and data collection is regulated according to Commission Regulation (EU) No 328/2011 on Causes of Death (COD) statistics. Member States are required to provide the data specified in this Regulation to the Commission (Eurostat) within 24 months after the end of the reference year. Coding of the causes of death is performed by the use of a harmonised methodology and coding system (ICD-10, ICD-9).
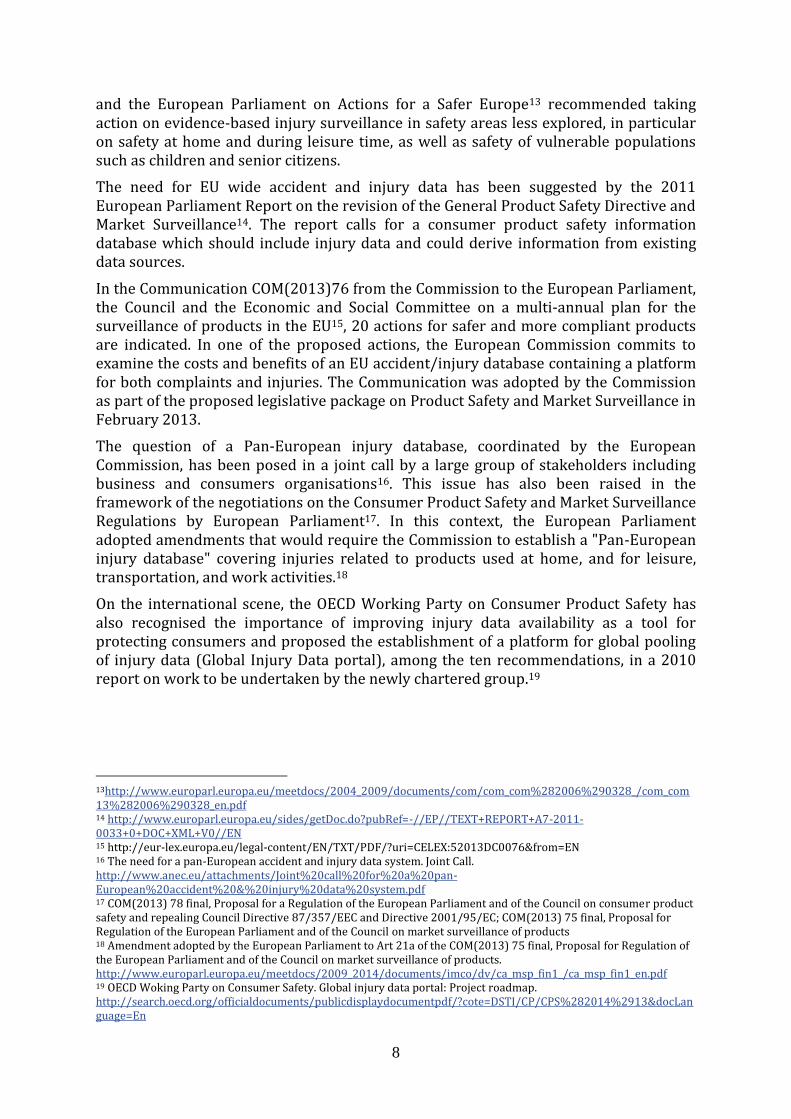
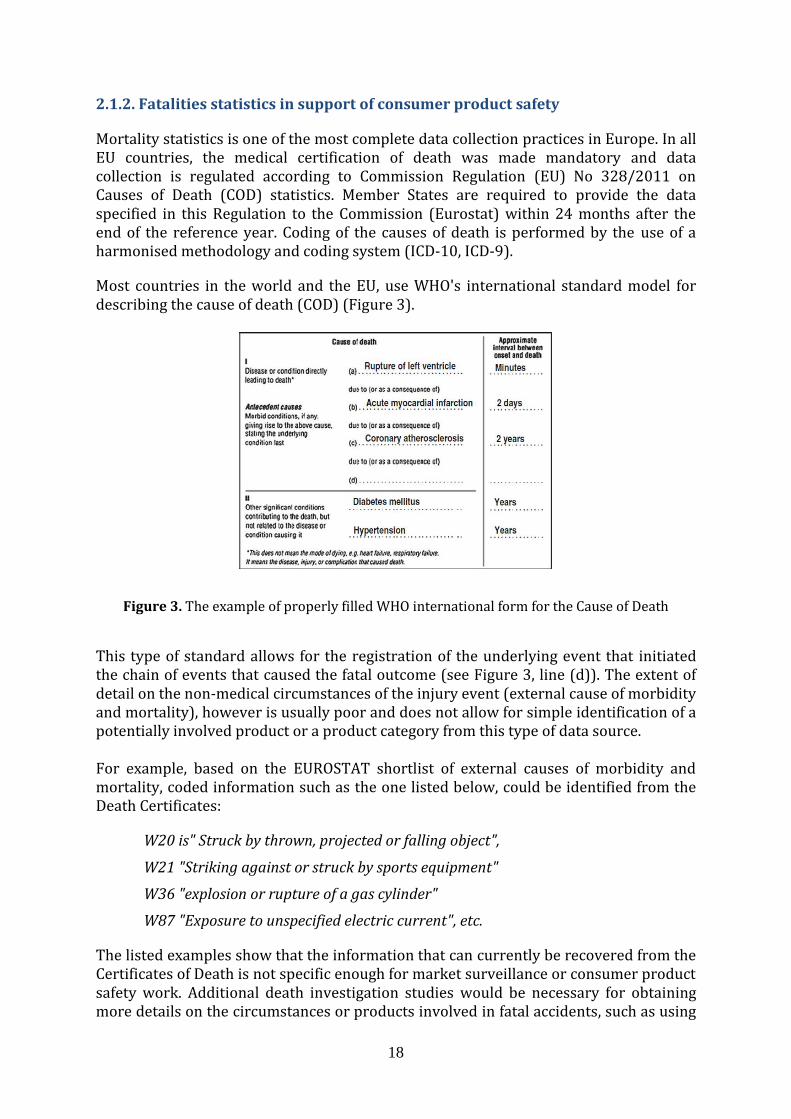
Most countries in the world and the EU, use WHO's international standard model for describing the cause of death (COD) (Figure 3).
Figure 3. The example of properly filled WHO international form for the Cause of Death
This type of standard allows for the registration of the underlying event that initiated the chain of events that caused the fatal outcome (see Figure 3, line (d)). The extent of detail on the non-medical circumstances of the injury event (external cause of morbidity and mortality), however is usually poor and does not allow for simple identification of a potentially involved product or a product category from this type of data source. For example, based on the EUROSTAT shortlist of external causes of morbidity and mortality, coded information such as the one listed below, could be identified from the Death Certificates:
W20 is" Struck by thrown, projected or falling object",
W21 "Striking against or struck by sports equipment"
W36 "explosion or rupture of a gas cylinder"
W87 "Exposure to unspecified electric current", etc.
The listed examples show that the information that can currently be recovered from the Certificates of Death is not specific enough for market surveillance or consumer product safety work. Additional death investigation studies would be necessary for obtaining more details on the circumstances or products involved in fatal accidents, such as using
19
medical records, exploring online news article clips or contacting the family of a deceased person. Similar work has already been carried out by the US Consumer Product Safety Commission 26,27. The use of Electronic Death Registration Systems may provide more opportunities for data usage in the future for consumer product safety purposes. Also the use of the new coding system ICD-11, that is being developed under the umbrella of WHO, may allow for more disaggregation of data on external causes of accidents in the future.
2.1.3. Media monitoring in support of consumer product safety
Thanks to the latest advancements in computing techniques, online news articles could represent a useful source for retrieving information on potentially unsafe products and emerging risks. On this assumption, in collaboration with the JRC’s ‘Text and Data Mining’ Unit (JRC I.3), a study has been carried out to find out how feasible is to use news articles for early identification of unsafe products. Europe Media Monitor (EMM) was used as a tool for monitoring online news and we utilised the EMM 'triggering keyword' based system to create and refine three working categories:
Unsafe Toys
Unsafe Consumer Products (extended list of products)
Unsafe Consumer Products (short list)
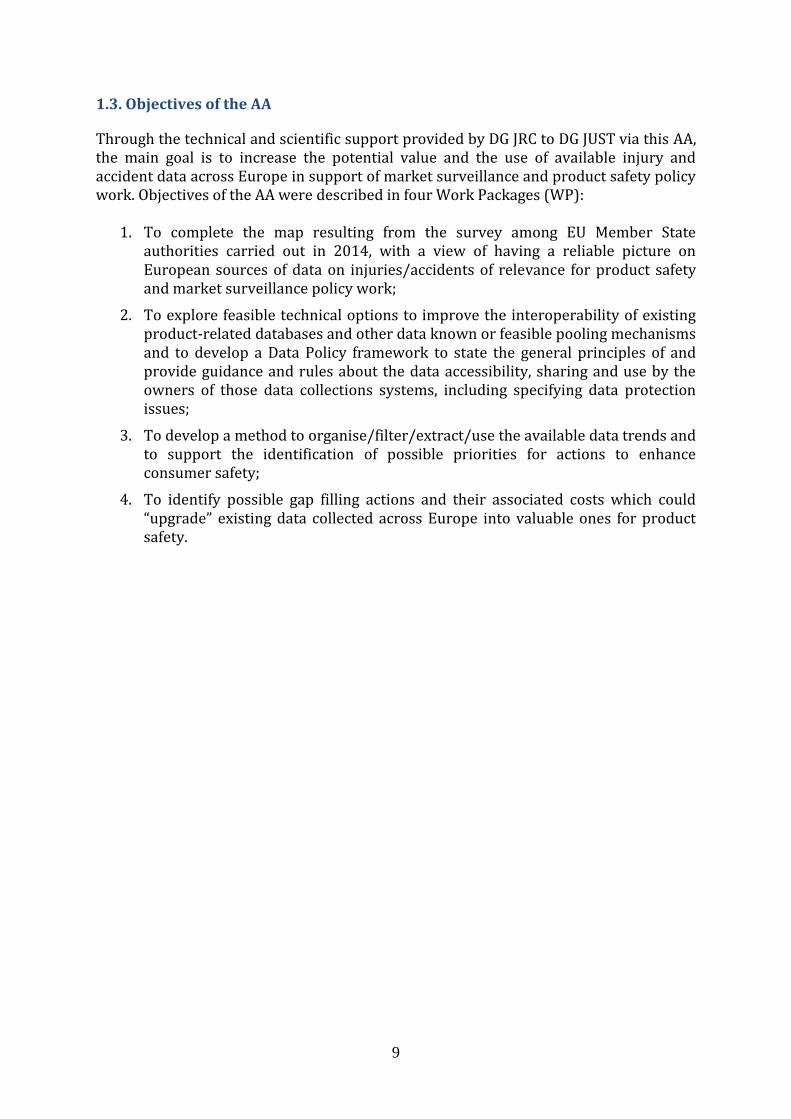
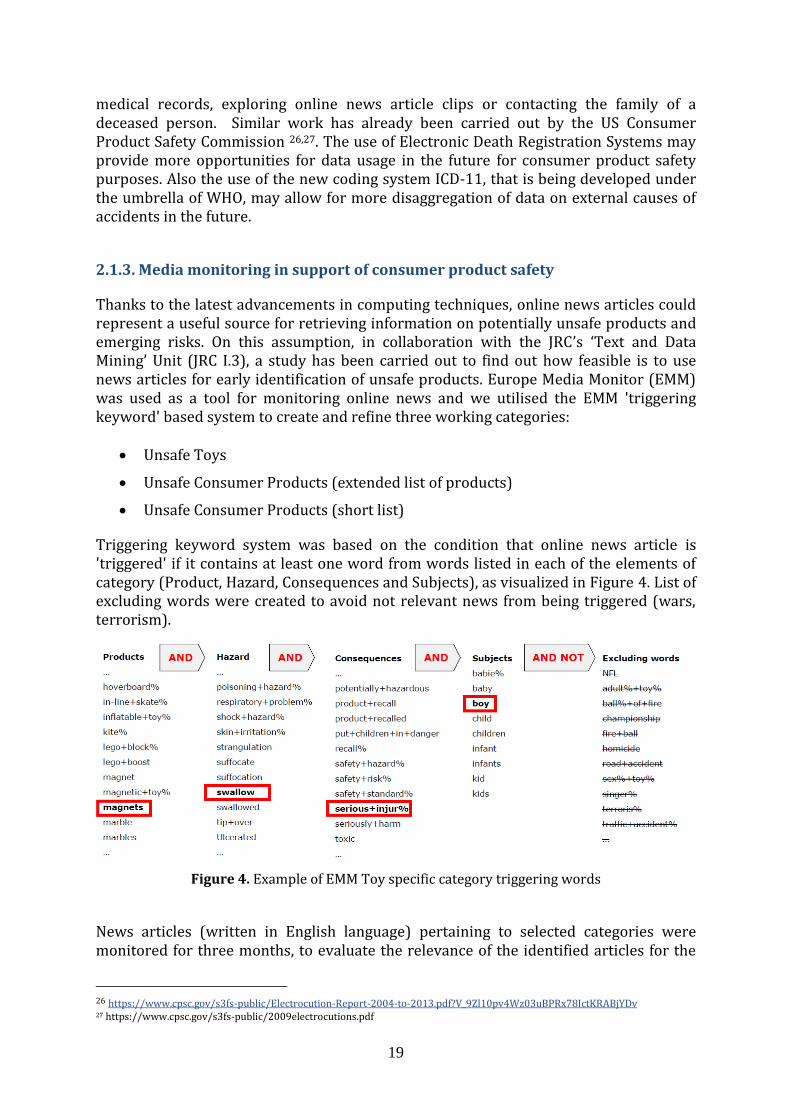
Triggering keyword system was based on the condition that online news article is 'triggered' if it contains at least one word from words listed in each of the elements of category (Product, Hazard, Consequences and Subjects), as visualized in Figure 4. List of excluding words were created to avoid not relevant news from being triggered (wars, terrorism).
Figure 4. Example of EMM Toy specific category triggering words
News articles (written in English language) pertaining to selected categories were monitored for three months, to evaluate the relevance of the identified articles for the
26 https://www.cpsc.gov/s3fs-public/Electrocution-Report-2004-to-2013.pdf?V_9Zl10pv4Wz03uBPRx78IctKRABjYDv 27 https://www.cpsc.gov/s3fs-public/2009electrocutions.pdf
20
purpose of our project. The 'captured' news articles were examined and flagged as ‘relevant’, or ‘false positive’ or ‘not relevant’.
As example, for one of the working categories (Unsafe Toys), the system triggered approximately 250 articles and thanks to iterative keyword-lists adjustments we reached a stable percentage of around 50% of relevant results which is likely the best result that could be obtained with EMM for our scope according to the experience of the JRC.I.3 colleagues. In the same period the percentage of false positives dropped to a level of around 20% which is considered normal by the experienced users of EMM and the percentage of not relevant results continuously decreased with each keyword list refinement reaching 30% in the last evaluations. Relevant articles were dealing with news such as product recalls, injury incidents, near-miss events or warnings from consumers or authorities on emerging issues.
We also tested EMM to monitor targeted emerging issues in order to follow their evolution over time. For this purpose we created a category specific to a toy (fidget spinner) that became popular in summer 2017 and which caused several serious incidents worldwide. This test was concluded in October 2017 when the last article on this topic was detected and demonstrated the capacity of EMM to successfully automatically retrieve articles on a very specific subject, as well as to follow the dynamic evolution in time of that subject reoccurrence. All information retrieved by EMM can be visualised by frequency of reporting per country, geographic location of the captured article or as needed for a specific purpose.
EMM has the potential to detect emerging issues in product safety from online news articles, but some limitations and potential drawbacks need to be taken into account:
In order to obtain relevant results, EMM initially requires a significant level of effort for defining and refining the conditions for article 'triggering'.
To cover online news from all EU countries, EMM categories must be defined in multiple languages. Our study also showed that automatic translation of English triggering words into other languages may produce incorrect meanings, therefore the selection of triggering words and phrases has to be prepared and monitored manually for each EU language.
The web sources that EMM is using could be enriched with consumer product relevant sources (online stores, social media).
Even if the tool does most of the work automatically, results must be verified and analysed a posteriori, before they can be reliably used (i.e. to avoid data misinterpretation or information misuse).
Online articles may or may not provide correct information on the product involved. Information needs to be scrutinised with caution, on a case by case basis.
Only most serious accidents or sensationalist news will find their way to the online news. Online news articles could also be fake, so caution is needed.

21
2.1.4. Consumer complaints in support of consumer product safety
In 2001 the General Products Safety Directive (GPSD) required enforcement authorities in Member States to have a procedure in place for receiving safety complaints from consumers. From a survey conducted by JRC and DG JUST during this project, among the members of the Consumer Safety Network, it appeared that those authorities who responded to the survey allow for electronic submission of complaints in various forms (downloadable format, on line form, sending photos, videos), but also by phone and fax. However, most respondents to our survey reported different methodologies of collecting, keeping and analysing the data (e.g. categorisations of injuries and unsafe products). The availability of product related injury/accident data could be increased by harmonising the procedures/methodologies for receiving safety complaints from consumers among the EU Member States enforcement agencies and then potentially forwarding details of the incident and product concerned to an EU-wide consumer product safety platform. Such a harmonised procedure should profit from the use of novel technologies for submitting complaints such as mobile phone applications. 2.1.5. Firefighters and rescue service data registers as potential source of information relevant to consumer product safety
Firefighters and Rescue Services (FRS) have data collection and reporting systems in place that contain data on every emergency or fire accident attended by these services. These data systems have the potential for retrieval of very specific product details causing the fires/accidents, however are often limited to a certain range of products (e.g. candles, electrical appliances, etc.). The format in which the information is collected is not standardised throughout the European Union. Some countries collect more detailed information on accidents than others. The usefulness of these reports for accident prevention is currently limited, due to the lack of detailed information on the external causes and circumstances of the accident. In addition, the data are not always available/accessible due to confidentiality reasons. This could however change in case national or EU-authorities request for upgrading of FRS intervention reporting with more detailed and standardised data collection and encourage fire investigation on the scene and forensic science as part of the fire officers education. Additionally an EU-central contact point for near-misses could be envisaged and in case the fire is caused by a consumer product, the FRS-report (and therefore also the database) could be amended adding a field where a standardised product code could be selected and a brand name could be recorded. The Federation of the European Union Fire Officer Associations, expressed their willingness to undertake a potential pilot project with DG JUST, that could explore the potential of this sector to provide timely and product related information on specific high-risk products involved in fire incidents. 2.1.6. Other potential sources of data/information relevant to consumer product safety
Poison Centres’ Registries Poison centres collect accident data related to citizens' exposure to chemicals. The collected data typically include information on the substance or product category involved (e.g. home detergents and cleaning products, cosmetics) and its toxicological
22
ingredients/quantities. This potentially allows linking the accident with the product. Data are usually collected in the emergency departments of hospitals or specialised poison centres following a qualitative methodology based on internally standardised documentation of cases. However currently there is no harmonised case recording at EU level. Companies have the legal obligation (according to the CLP Regulation28, Article 45) to inform appointed bodies about the composition and the toxicological properties of mixtures classified as hazardous. The recent introduction of the Unique Formula Identifier (UFI) allows a precise and rapid identification of the product and its specific chemical formulation. The use and access of notified product information is limited due to confidentiality reasons (Article 45(2) of the CLP Regulation) and may only be used to meet medical demand by formulating preventative and curative measures and where requested by the Member State, to undertake statistical analysis to identify where improved risk management measures may be needed. Confidentiality issues as regards, individual cases recorded in poison centres, does also concern personal data as regulated by both national and European legislation.
In conclusion, data collected at poison centres contain valuable information on chemical mixtures or liquid consumer products. However, circumstances leading to the intoxication are typically not recorded, data are not collected in a harmonised way and data accessibility is difficult due to confidentiality reasons. Direct linking to the proposed Consumer Product Safety Platform is not feasible in the short term, without prior attempt for harmonisation among existing data collection methodologies and clarification about the conditions and boundaries of data accessibility limitations.
Data Records held by Insurance companies Insurance companies belong to a private sector which holds records that, in principle, could be a valid source of information on product related causes of injuries and/or death. Types of insurances which could possibly collect for this purpose relevant information are life insurances, personal accident insurances, medical and health insurances, workers compensation insurances and in particular product liability insurances. Product liability protects against claims of personal injury or property damage caused by products sold or supplied through the manufacturers’ business. However, it appeared that insurance claims are generally not recorded/analysed in a harmonised way neither at national level nor at European level and that product related causes are generally not registered. The interest of insurance associations to collaborate and share information was low in the course of this project’s execution. Accessibility to such data would anyhow be restricted due to data privacy and confidentiality reasons.
Sub-task 2.2: Analysis of technical options
Based on the priority data sources that have been selected, we propose two scenarios for a modular integrated IT platform that could serve as a support to consumer product safety work. In both cases, the systematically collected data on injuries would come from a revitalised IDB network of FDS data collections via dedicated
28 Regulation (EC) No 1272/2008 on classification, labelling and packaging of substances and mixtures
23
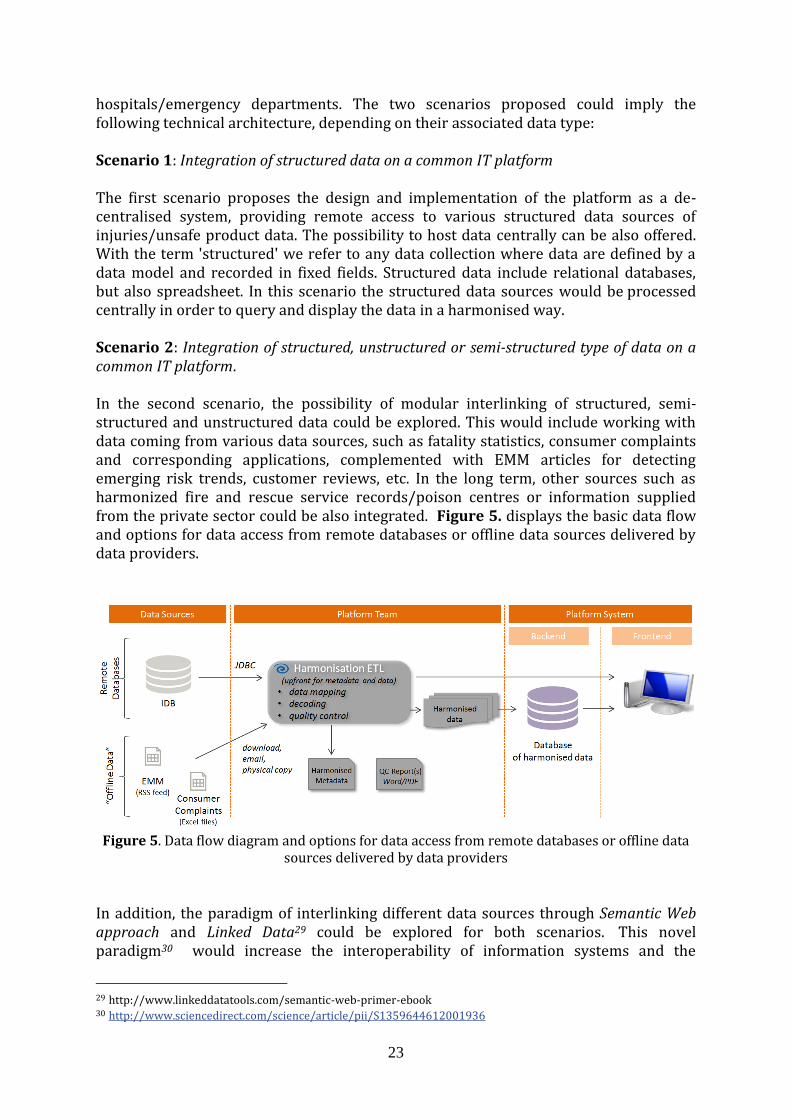
hospitals/emergency departments. The two scenarios proposed could imply the following technical architecture, depending on their associated data type: Scenario 1: Integration of structured data on a common IT platform The first scenario proposes the design and implementation of the platform as a de-centralised system, providing remote access to various structured data sources of injuries/unsafe product data. The possibility to host data centrally can be also offered. With the term 'structured' we refer to any data collection where data are defined by a data model and recorded in fixed fields. Structured data include relational databases, but also spreadsheet. In this scenario the structured data sources would be processed centrally in order to query and display the data in a harmonised way. Scenario 2: Integration of structured, unstructured or semi-structured type of data on a common IT platform. In the second scenario, the possibility of modular interlinking of structured, semi- structured and unstructured data could be explored. This would include working with data coming from various data sources, such as fatality statistics, consumer complaints and corresponding applications, complemented with EMM articles for detecting emerging risk trends, customer reviews, etc. In the long term, other sources such as harmonized fire and rescue service records/poison centres or information supplied from the private sector could be also integrated. Figure 5. displays the basic data flow and options for data access from remote databases or offline data sources delivered by data providers.
Figure 5. Data flow diagram and options for data access from remote databases or offline data
sources delivered by data providers
In addition, the paradigm of interlinking different data sources through Semantic Web approach and Linked Data29 could be explored for both scenarios. This novel paradigm30 would increase the interoperability of information systems and the
29 http://www.linkeddatatools.com/semantic-web-primer-ebook 30 http://www.sciencedirect.com/science/article/pii/S1359644612001936
24
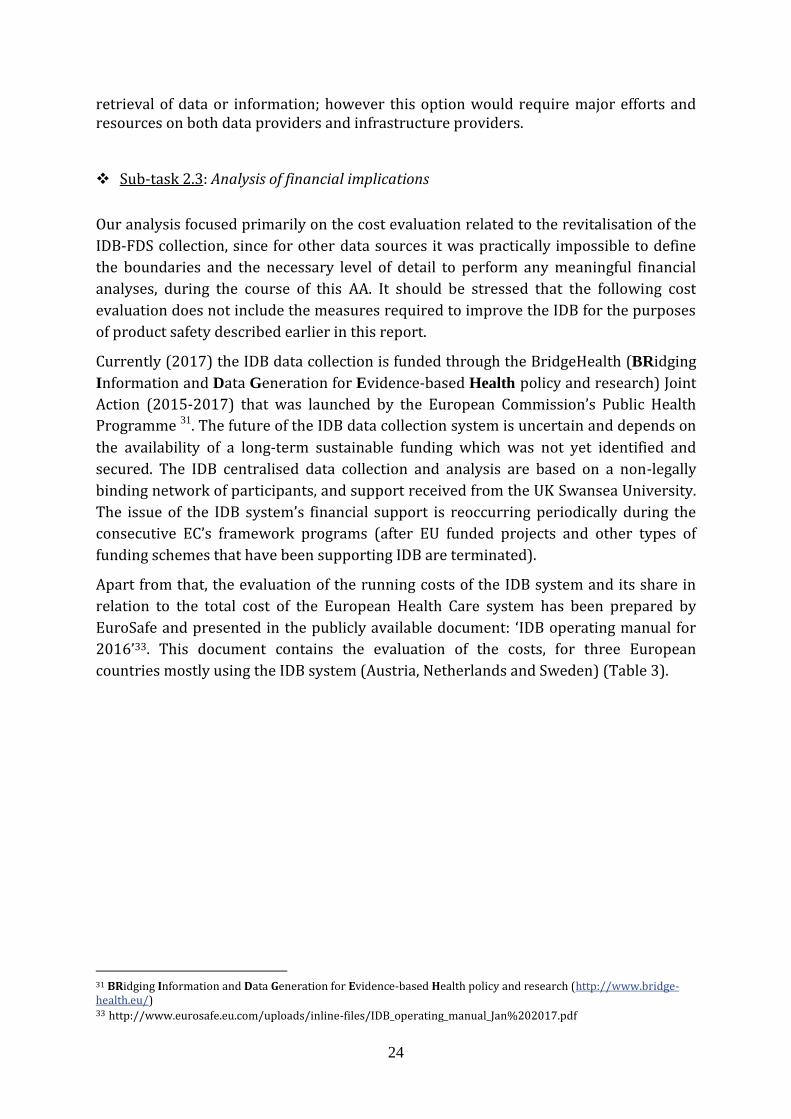
retrieval of data or information; however this option would require major efforts and resources on both data providers and infrastructure providers. Sub-task 2.3: Analysis of financial implications
Our analysis focused primarily on the cost evaluation related to the revitalisation of the
IDB-FDS collection, since for other data sources it was practically impossible to define
the boundaries and the necessary level of detail to perform any meaningful financial
analyses, during the course of this AA. It should be stressed that the following cost
evaluation does not include the measures required to improve the IDB for the purposes
of product safety described earlier in this report.
Currently (2017) the IDB data collection is funded through the BridgeHealth (BRidging
Information and Data Generation for Evidence-based Health policy and research) Joint
Action (2015-2017) that was launched by the European Commission’s Public Health
Programme 31. The future of the IDB data collection system is uncertain and depends on
the availability of a long-term sustainable funding which was not yet identified and
secured. The IDB centralised data collection and analysis are based on a non-legally
binding network of participants, and support received from the UK Swansea University.
The issue of the IDB system’s financial support is reoccurring periodically during the
consecutive EC’s framework programs (after EU funded projects and other types of
funding schemes that have been supporting IDB are terminated).
Apart from that, the evaluation of the running costs of the IDB system and its share in
relation to the total cost of the European Health Care system has been prepared by
EuroSafe and presented in the publicly available document: ‘IDB operating manual for
2016’33. This document contains the evaluation of the costs, for three European
countries mostly using the IDB system (Austria, Netherlands and Sweden) (Table 3).
31 BRidging Information and Data Generation for Evidence-based Health policy and research (http://www.bridge-health.eu/) 33 http://www.eurosafe.eu.com/uploads/inline-files/IDB_operating_manual_Jan%202017.pdf
25
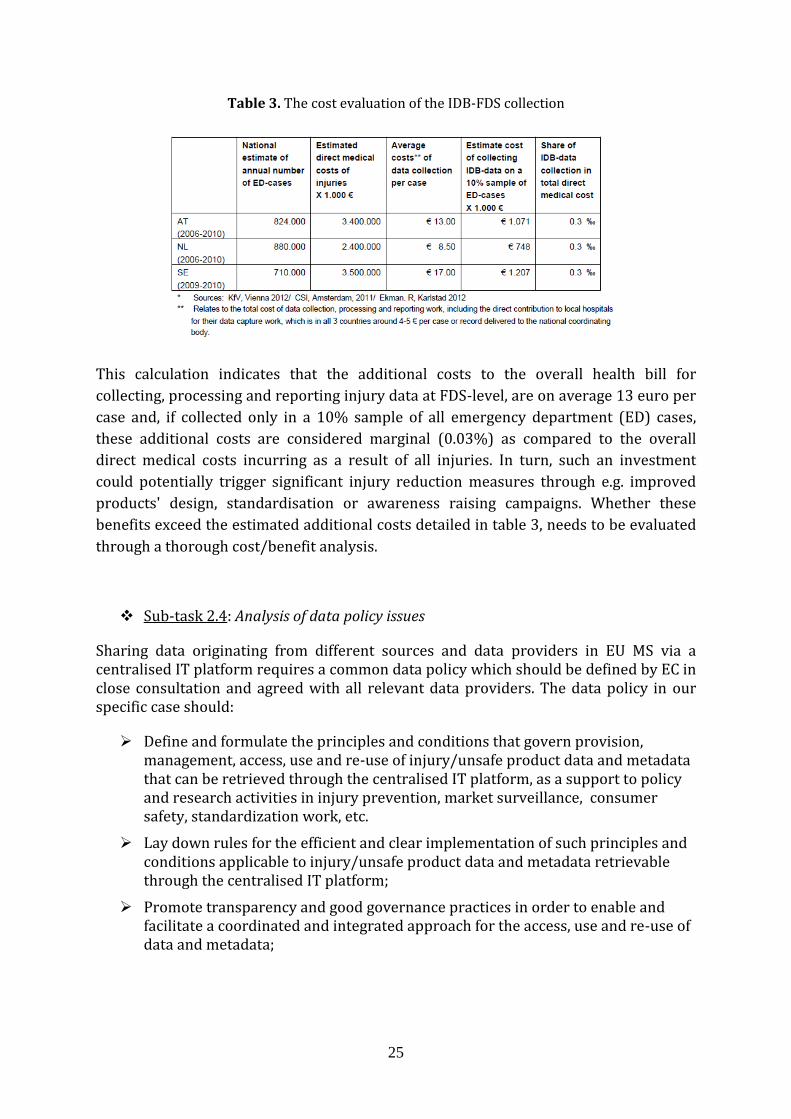
Table 3. The cost evaluation of the IDB-FDS collection
This calculation indicates that the additional costs to the overall health bill for
collecting, processing and reporting injury data at FDS-level, are on average 13 euro per
case and, if collected only in a 10% sample of all emergency department (ED) cases,
these additional costs are considered marginal (0.03%) as compared to the overall
direct medical costs incurring as a result of all injuries. In turn, such an investment
could potentially trigger significant injury reduction measures through e.g. improved
products' design, standardisation or awareness raising campaigns. Whether these
benefits exceed the estimated additional costs detailed in table 3, needs to be evaluated
through a thorough cost/benefit analysis.
Sub-task 2.4: Analysis of data policy issues
Sharing data originating from different sources and data providers in EU MS via a centralised IT platform requires a common data policy which should be defined by EC in close consultation and agreed with all relevant data providers. The data policy in our specific case should:
Define and formulate the principles and conditions that govern provision, management, access, use and re-use of injury/unsafe product data and metadata that can be retrieved through the centralised IT platform, as a support to policy and research activities in injury prevention, market surveillance, consumer safety, standardization work, etc.
Lay down rules for the efficient and clear implementation of such principles and conditions applicable to injury/unsafe product data and metadata retrievable through the centralised IT platform;
Promote transparency and good governance practices in order to enable and facilitate a coordinated and integrated approach for the access, use and re-use of data and metadata;
26
The EU Commission promotes the Open Data34 principles, as the default regime for making data retrievable through an IT platform and for their further use and re-use. However data owners/providers may impose exceptional accessibility regimes that restrict access to some of their data, for example in case of:
Protection of Personal Data
Protection of licencing conditions, commercial interests and intellectual property rights.
Protection of contractual obligations restricting access to data.
Currently the IDB, due to its data protection policy, is providing public access only to aggregated data from the minimum data set (IDB-MDS). The data policy applied by the IDB network and DG SANTE concerning the use of the IDB-FDS micro data is in line with the standards of the European Data Protection Directive 95/46/EC and Regulation 45/2001 on the processing of single case data by Community institutions. Single case data and the narratives which might allow the identification of the involved patient are only accessible to the EU institutions and on request to the research organisations for a limited time. This is very restrictive due to high level of data protection in EU, in particular when hospital data are involved. Therefore getting access is currently time consuming and narratives, which are important detail when analysing injury data, are currently not unconditionally available to all data users.
During the experts Workshop on 8-9 November 2017 in Ispra, it has also emerged that data, once retrieved from IDB, can currently not be handed to other institutions, for example standardisation bodies. For this reason, when defining a common data policy for the centralised IT platform the following aspects should be tackled upon:
Single or aggregated data related to injury/unsafe products which are retrievable through the centralised IT platform will be made available to all user groups under the conditions of Free, Full, Open and Timely access.
The injury/unsafe product data retrievable through the centralized IT platform shall be made available to all user groups as single data, unless otherwise decided by data providers.
If single data cannot be made available, the data should be made available to all user groups at the highest possible degree of detail (as distinct age groups, injury groups or product category groups).
The data shall be accompanied by a suitable explanation (metadata) to facilitate their interpretation by end-users.
Data policy for such centralised IT platforms has been previously created (e.g. IPCHEM Data Policy) and can be applied with necessary modifications to any new centralised IT platform operating with similar principles.
To overcome the challenges of data protection, different levels of data access can be provided to different data users. Any future activities on the improvement of the IDB network should also include revision of the current IDB data protection methods that
34 https://www.europeandataportal.eu/sites/default/files/goldbook.pdf

27
may involve a liaison of many stakeholders (e.g. hospitals' representatives, legal advisors, IT experts, EC DGs, data managers and data protection officers in EU MS, etc.).
The new General Data Protection Regulation (GDPR) 2016/679, entered into force on 25 May 2016. It will be applied starting from 25 May 2018. Once the GDPR will come into effect, it will replace the current Data Protection Directive 95/46, consolidating and innovating data protection rules. The Data Policy itself is not enough for the proper functioning of any system. It must be also accompanied by Data Policy Implementation Guidelines (meant as a living set of documents, procedures and templates). In addition, data quality and data management are essential elements for the proper use and re-use of data, therefore these should be incorporated into the Data Policy Implementation Guidelines.
Work Package 3: Methodology for data mining and analysis to support the identification of trends in product related injuries and accidents Tasks: Task 3.1: To develop a methodology to organise/filter/extract/analyse available data
to support the identification and comparison of temporal trends and associations between products, risks and accidents/injuries data and the setting of priorities for actions in relevant existing national systems in EU.
Concerns about the safety of products, underpinned by requests from consumers associations and governmental agencies appeared first in the 70s. Methodologies based on data collection from trauma centres and emergency department were established at the time, for routine registration of victims who had home or leisure injuries and where a consumer product was involved. The National Electronic Injury Surveillance System (NEISS) was the first system (launched in the USA since 1973) featuring a methodology that comprises codification of products by their own unique coding system, which however can be also transcribed into other systems. In 1976, the British Home Accident Surveillance System (HASS) was introduced, followed by similar systems in the Nordic countries and in the Netherlands. In the 1990s, after previous injury surveillance demonstration period, the Commission launched the first EHLASS programme (European Home and Leisure Accident Surveillance System)35 to collect data on accidents with a view to promote accident prevention, improve the safety of consumer products and educate consumers so that they make better use of products. From 2000 onwards, the European Commission has prioritised the further development of a standardised system for monitoring injuries in the European Union by establishing the Injury Data Base (IDB).
The IDB is partly a continuation of the EHLASS database and relies on the EHLASS (v2000) coding and the widely recognised International Classification of External Causes of Injuries (ICECI v1.2) coding system. Both the ICECI system and IDB-FDS methodology are well documented and fit for monitoring long term trends/seasonal trends on injuries involving consumer product categories.
35 http://cordis.europa.eu/news/rcn/2042_en.html

28
For the detection of emerging trends from new products on the market, a more timely information system is needed; therefore we suggest the use of online media (e.g. via use of the Europe Media Monitor), online customer reviews, and consumer complaints. Information on high risk products causing fire incidents could be technically obtained from the firefighters’ records, provided that this will become part of mandatory recording and that harmonisation efforts related to the recording format will be undertaken at EU level. Poison centres contain information on the product categories (detergents/washing liquids etc.) that caused the highest number of poisoning incidents, but this system still needs to undergo harmonisation both within MS and at EU level.
Work Package 4: Identification of future options and opportunities for data collection on injuries and accidents in support of product safety
Tasks:
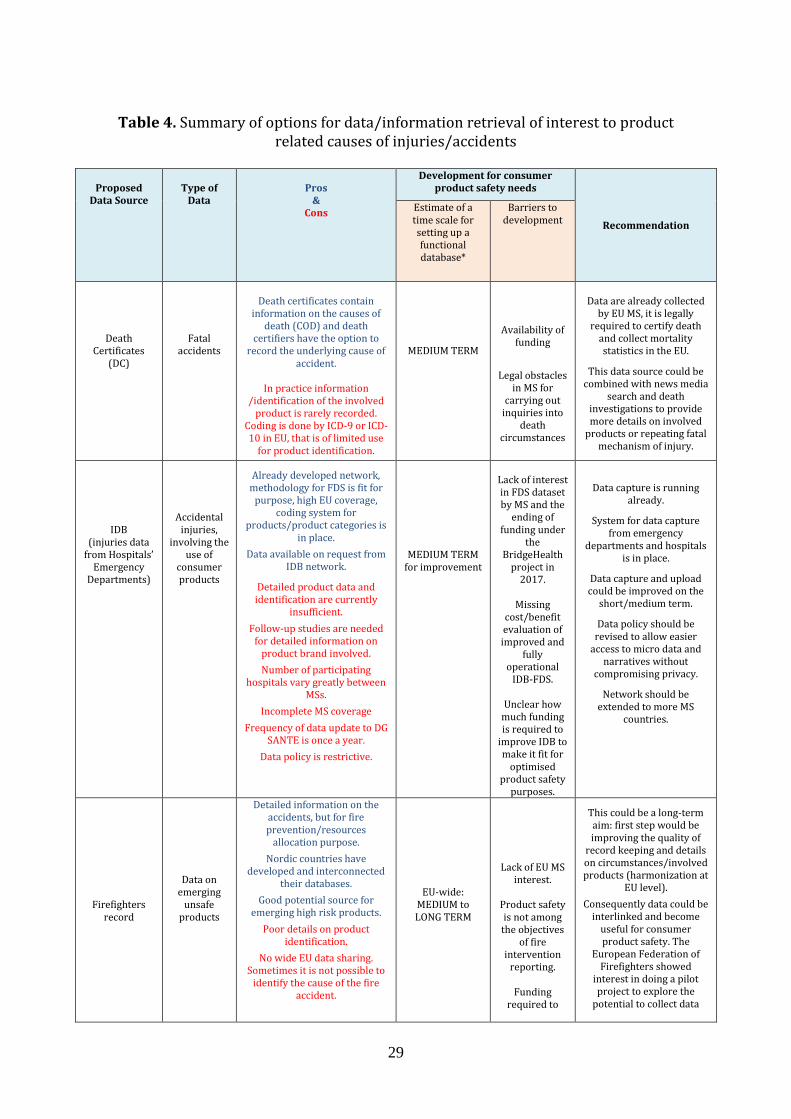
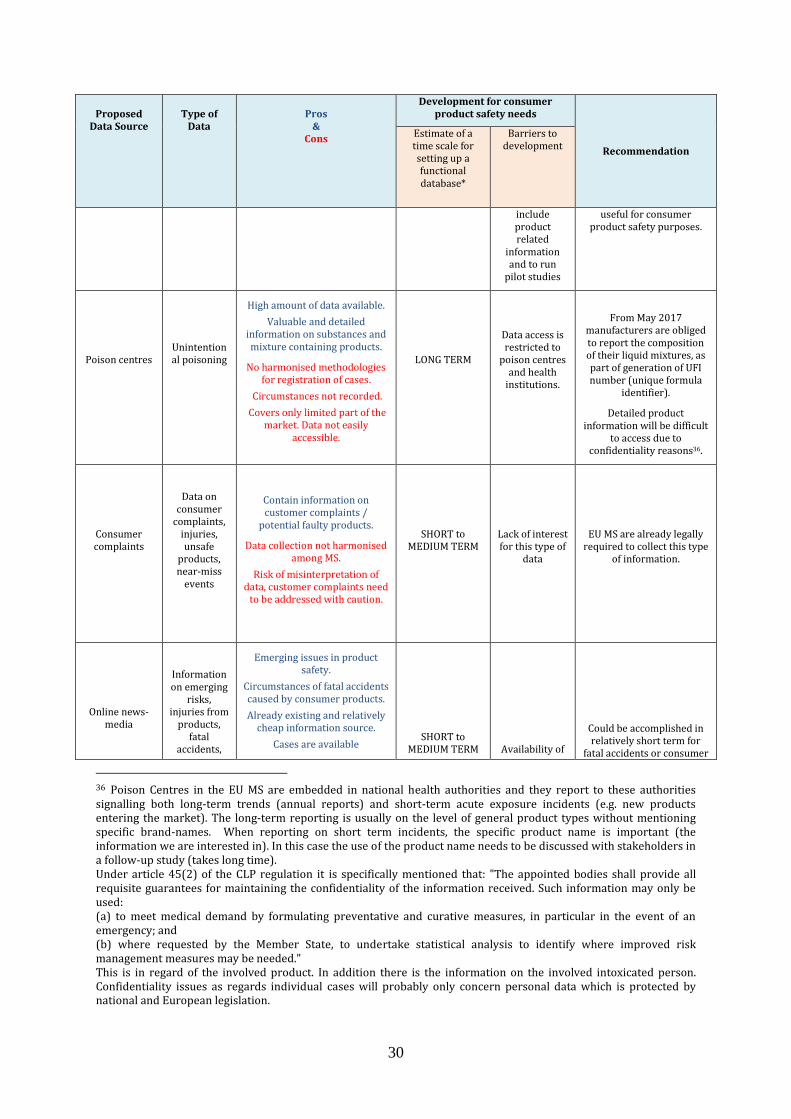
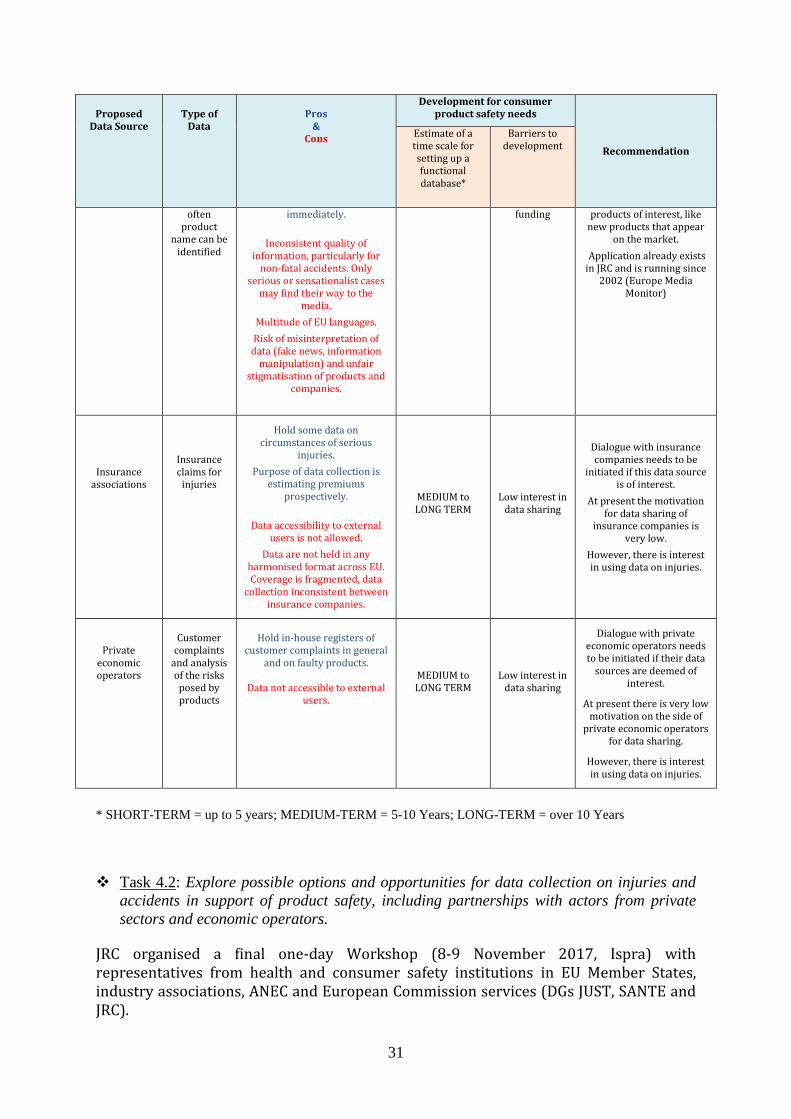
Task 4.1: Assess the possible costs and methods to improve some of the existing (categories of) databases in the direction of more accurate and usable information on the product related causes of injuries/accidents.
Table 4. provides a summary of potential sources of interest to the consumer product safety policy work and their associated pros and cons (in terms of data richness and availability, harmonised methodologies and networking capacity for data sharing, risk of data misinterpretation, etc.).
At this stage, more precise evaluation of costs was not possible. Hereafter we provide an estimate of the timeframe (short-term= up to 5 years; medium-term= 5-10 years, long-term= over 10 years) needed to reach functional use of data from these sources, task which would very much rely on available resources and motivation of the stakeholders involved. Potential barriers in sharing these data sources are also indicated.
29
Table 4. Summary of options for data/information retrieval of interest to product related causes of injuries/accidents
Proposed Data Source
Type of
Data
Pros
& Cons
Development for consumer product safety needs
Recommendation
Estimate of a time scale for setting up a functional database*
Barriers to development
Death Certificates
(DC)
Fatal accidents
Death certificates contain
information on the causes of death (COD) and death
certifiers have the option to record the underlying cause of
accident.
In practice information /identification of the involved
product is rarely recorded. Coding is done by ICD-9 or ICD-10 in EU, that is of limited use
for product identification.
MEDIUM TERM
Availability of funding
Legal obstacles in MS for
carrying out inquiries into
death circumstances
Data are already collected
by EU MS, it is legally required to certify death
and collect mortality statistics in the EU.
This data source could be combined with news media
search and death investigations to provide more details on involved
products or repeating fatal mechanism of injury.
IDB (injuries data
from Hospitals’ Emergency
Departments)
Accidental injuries,
involving the use of
consumer products
Already developed network, methodology for FDS is fit for
purpose, high EU coverage, coding system for
products/product categories is in place.
Data available on request from IDB network.
Detailed product data and identification are currently
insufficient.
Follow-up studies are needed for detailed information on
product brand involved.
Number of participating hospitals vary greatly between
MSs.
Incomplete MS coverage
Frequency of data update to DG SANTE is once a year.
Data policy is restrictive.
MEDIUM TERM for improvement
Lack of interest in FDS dataset by MS and the
ending of funding under
the BridgeHealth
project in 2017.
Missing
cost/benefit evaluation of improved and
fully operational
IDB-FDS.
Unclear how much funding is required to
improve IDB to make it fit for
optimised product safety
purposes.
Data capture is running already.
System for data capture from emergency
departments and hospitals is in place.
Data capture and upload could be improved on the
short/medium term.
Data policy should be revised to allow easier
access to micro data and narratives without
compromising privacy.
Network should be extended to more MS
countries.
Firefighters record
Data on emerging
unsafe products
Detailed information on the accidents, but for fire prevention/resources
allocation purpose.
Nordic countries have developed and interconnected
their databases.
Good potential source for emerging high risk products.
Poor details on product identification.
No wide EU data sharing. Sometimes it is not possible to
identify the cause of the fire accident.
EU-wide: MEDIUM to LONG TERM
Lack of EU MS interest.
Product safety is not among
the objectives of fire
intervention reporting.
Funding
required to
This could be a long-term aim: first step would be improving the quality of
record keeping and details on circumstances/involved products (harmonization at
EU level).
Consequently data could be interlinked and become
useful for consumer product safety. The
European Federation of Firefighters showed
interest in doing a pilot project to explore the
potential to collect data
30
Proposed
Data Source
Type of
Data
Pros
& Cons
Development for consumer product safety needs
Recommendation
Estimate of a time scale for setting up a functional database*
Barriers to development
include product related
information and to run
pilot studies
useful for consumer product safety purposes.
Poison centres
Unintentional poisoning
High amount of data available.
Valuable and detailed information on substances and mixture containing products.
No harmonised methodologies for registration of cases.
Circumstances not recorded.
Covers only limited part of the market. Data not easily
accessible.
LONG TERM
Data access is restricted to
poison centres and health
institutions.
From May 2017 manufacturers are obliged to report the composition of their liquid mixtures, as part of generation of UFI number (unique formula
identifier).
Detailed product information will be difficult
to access due to confidentiality reasons36.
Consumer complaints
Data on consumer
complaints, injuries, unsafe
products, near-miss
events
Contain information on customer complaints /
potential faulty products.
Data collection not harmonised among MS.
Risk of misinterpretation of data, customer complaints need
to be addressed with caution.
SHORT to MEDIUM TERM
Lack of interest for this type of
data
EU MS are already legally required to collect this type
of information.
Online news-media
Information on emerging
risks, injuries from
products, fatal
accidents,
Emerging issues in product safety.
Circumstances of fatal accidents caused by consumer products.
Already existing and relatively cheap information source.
Cases are available
SHORT to MEDIUM TERM
Availability of
Could be accomplished in relatively short term for
fatal accidents or consumer
36 Poison Centres in the EU MS are embedded in national health authorities and they report to these authorities signalling both long-term trends (annual reports) and short-term acute exposure incidents (e.g. new products entering the market). The long-term reporting is usually on the level of general product types without mentioning specific brand-names. When reporting on short term incidents, the specific product name is important (the information we are interested in). In this case the use of the product name needs to be discussed with stakeholders in a follow-up study (takes long time). Under article 45(2) of the CLP regulation it is specifically mentioned that: "The appointed bodies shall provide all requisite guarantees for maintaining the confidentiality of the information received. Such information may only be used: (a) to meet medical demand by formulating preventative and curative measures, in particular in the event of an emergency; and (b) where requested by the Member State, to undertake statistical analysis to identify where improved risk management measures may be needed." This is in regard of the involved product. In addition there is the information on the involved intoxicated person. Confidentiality issues as regards individual cases will probably only concern personal data which is protected by national and European legislation.
31
Proposed
Data Source
Type of
Data
Pros
& Cons
Development for consumer product safety needs
Recommendation
Estimate of a time scale for setting up a functional database*
Barriers to development
often product
name can be identified
immediately.
Inconsistent quality of
information, particularly for non-fatal accidents. Only
serious or sensationalist cases may find their way to the
media.
Multitude of EU languages.
Risk of misinterpretation of data (fake news, information
manipulation) and unfair stigmatisation of products and
companies.
funding products of interest, like new products that appear
on the market.
Application already exists in JRC and is running since
2002 (Europe Media Monitor)
Insurance associations
Insurance claims for
injuries
Hold some data on circumstances of serious
injuries.
Purpose of data collection is estimating premiums
prospectively.
Data accessibility to external
users is not allowed.
Data are not held in any harmonised format across EU. Coverage is fragmented, data
collection inconsistent between insurance companies.
MEDIUM to LONG TERM
Low interest in data sharing
Dialogue with insurance companies needs to be
initiated if this data source is of interest.
At present the motivation for data sharing of
insurance companies is very low.
However, there is interest in using data on injuries.
Private economic operators
Customer
complaints and analysis of the risks
posed by products
Hold in-house registers of
customer complaints in general and on faulty products.
Data not accessible to external
users.
MEDIUM to LONG TERM
Low interest in data sharing
Dialogue with private economic operators needs to be initiated if their data
sources are deemed of interest.
At present there is very low motivation on the side of
private economic operators for data sharing.
However, there is interest in using data on injuries.
* SHORT-TERM = up to 5 years; MEDIUM-TERM = 5-10 Years; LONG-TERM = over 10 Years
Task 4.2: Explore possible options and opportunities for data collection on injuries and
accidents in support of product safety, including partnerships with actors from private
sectors and economic operators.
JRC organised a final one-day Workshop (8-9 November 2017, Ispra) with representatives from health and consumer safety institutions in EU Member States, industry associations, ANEC and European Commission services (DGs JUST, SANTE and JRC).
32
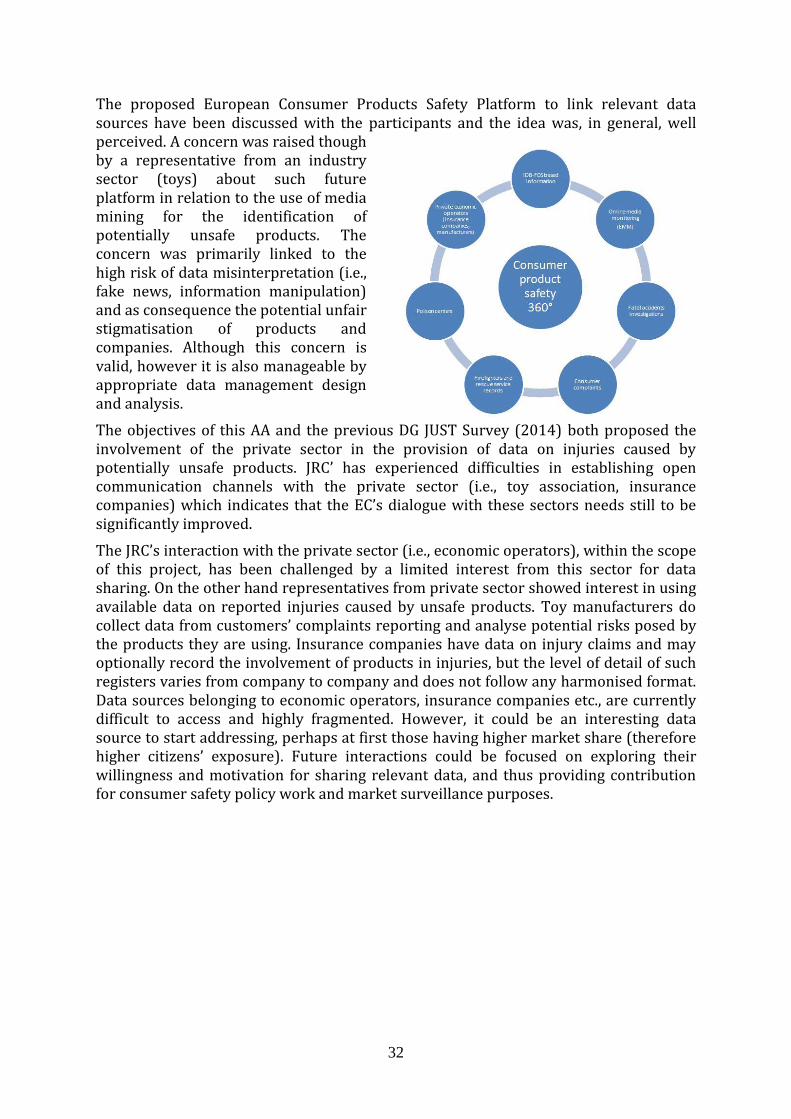
The proposed European Consumer Products Safety Platform to link relevant data sources have been discussed with the participants and the idea was, in general, well perceived. A concern was raised though by a representative from an industry sector (toys) about such future platform in relation to the use of media mining for the identification of potentially unsafe products. The concern was primarily linked to the high risk of data misinterpretation (i.e., fake news, information manipulation) and as consequence the potential unfair stigmatisation of products and companies. Although this concern is valid, however it is also manageable by appropriate data management design and analysis.
The objectives of this AA and the previous DG JUST Survey (2014) both proposed the involvement of the private sector in the provision of data on injuries caused by potentially unsafe products. JRC’ has experienced difficulties in establishing open communication channels with the private sector (i.e., toy association, insurance companies) which indicates that the EC’s dialogue with these sectors needs still to be significantly improved.
The JRC’s interaction with the private sector (i.e., economic operators), within the scope of this project, has been challenged by a limited interest from this sector for data sharing. On the other hand representatives from private sector showed interest in using available data on reported injuries caused by unsafe products. Toy manufacturers do collect data from customers’ complaints reporting and analyse potential risks posed by the products they are using. Insurance companies have data on injury claims and may optionally record the involvement of products in injuries, but the level of detail of such registers varies from company to company and does not follow any harmonised format. Data sources belonging to economic operators, insurance companies etc., are currently difficult to access and highly fragmented. However, it could be an interesting data source to start addressing, perhaps at first those having higher market share (therefore higher citizens’ exposure). Future interactions could be focused on exploring their willingness and motivation for sharing relevant data, and thus providing contribution for consumer safety policy work and market surveillance purposes.
33
3. Conclusions
The CPS-IAData project (AA between DGs JUST and JRC) explored the potential for increasing the availability of information on injuries caused by unsafe consumer products. The research was based on the analysis of existing data collection practices in EU and opportunities arising from the use of novel IT technologies. This report summarises the outcomes related to the execution of the tasks foreseen in the context of the administrative arrangement, carried out from March 2016 – November 2017.
There are a number of data sources of potential interest to the consumer product safety policy work, such as injuries data from hospitals’ emergency departments (e.g. sourced through IDB network), death certificates, firefighter’s records, poison centres, consumer complaints, online news media, insurance associations and private economic sectors. These data sources present pros and cons in terms of: data richness, fragmentation, availability and accessibility, harmonised methodologies, terminology, networking capacity and funding availability for data collection activities, willingness for data sharing, risk of data misinterpretation or misuse (e.g. fake news, information manipulation).
A possible solution to use such a variety of data and formats, would be to put in place a centralised modular European Consumer Product Safety Platform (ECPSP). In this new IT platform, data from the revitalised and improved IDB-FDS, together with data from online media monitoring systems (e.g. EMM) for the detection of emerging threats from products entering the market, information extracted from consumers’ reported injuries and data from other relevant data sources (fire-fighter or poison centres records) could be pooled together, taking advantage of novel IT paradigms to link different data sources containing structured, unstructured and semi-structured data. This could be complemented by information retrieved from deep investigations into mortality statistics (causes of death) in terms of consumer product involvement.
With respect to the sustainability and quality of data from potential data providers, some challenges have been identified, which may require coordinated and long-term actions as well as significant resources to be shared by various stakeholders (MS, EC, private sector).
The European Injury Database (IDB), coordinated by EUROSAFE and hosted by DG SANTE, is currently the largest injury data-collection in EU based on hospital emergency department data, which within its Full Data Set (IDB-FDS) contains information on the consumer products involved. However, the absence of a legal mandate for a systematic collection of IDB-FDS data, along with the lack of sustainable funding, the increasing data protection concerns and the uncertain amount of required funding to improve the current setting of the IDB to optimise its capacity for product safety purposes (cost/benefit), are among the main weaknesses. These might prevail over existing strengths and opportunities, thus diminishing the potential of an IDB-FDS systematic data collection to support consumer products safety and policy work (details in Table 2).
To ensure long-term IDB-FDS operation a long-term sustainable governance mechanism (coordination point, data policy, funding mechanism, data collection and management structures) would be needed to be developed by MS, European Commission and other relevant stakeholders (private sector, industry, economic operators). This would ensure a long-term IDB-FDS collection effort by EU Member States. However, the willingness

34
and readiness of all relevant stakeholders to develop such long-term sustainable governance mechanism has to be further explored.
The other relevant data sources identified in this report, such as fire-fighters records or poison centres information could be progressively linked to the ECPSP platform. However, as these latter data sources are tailored for different purposes (and therefore their respective data collections follow different methodologies, that are not intentionally focused on recording the involvement of the consumer product in the incident), at present, their data (in terms of both type and quality of information on the linkage of injures/accidents to specific products) are not ready to be directly integrated into such IT platform and deliver the expected benefits. These data collections should be first standardised, harmonised and brought on the level of content and compatibility as required by the IDB-FDS methodology and with a wide geographical and statistically significant coverage (i.e. coming from a wide number of countries and a significant number of cases). Such task would require substantial coordinated efforts and resources over an extended timeframe.
Last but not least, it should be stressed that the expected policy and societal benefits of the aforementioned proposed solution can only be reached provided that better prospects are envisaged for long-term sustainable data collection efforts in EU Member States. Setting up a win-win data sharing landscape could motivate stakeholders from the private sector to provide data (e.g. industry sectors, insurance companies, economic operators). Such type of data providers already own or are capable of recording data useful for consumer product safety policy work and market surveillance purposes, but are currently showing low interest in sharing this information, for various reasons (including data privacy and confidentiality reasons), notwithstanding they are interested in using such data when available.
A more detailed analysis needs to be carried out to conclude on the feasibility, cost/benefit ratio and impact of the proposed options.
35
4. Glossary
AA Administrative Arrangement ANEC European Association for the Co-ordination of Consumer Representation
in Standardisation AISBL BridgeHealth BRidging Information and Data Generation for Evidence-based Health
policy and research CLP Classification, Labelling and Packaging COD Causes of Death CPS-IAData Consumer Product Safety - Injury and Accident Data collection in
support of consumer product safety and market surveillance CPSD Consumer Products Safety Data DC Death Certificates DG Directorate General DG JUST Directorate General for Justice and Consumers DG SANTE Direction Générale de la Santé et de la sécurité alimentaire EC European Commission ECPSP European Consumer Product Safety Platform ED Emergency Department EFTA European Free Trade Association EHLASS European Home and Leisure Accidents Surveillance System EMM Europe Media Monitor EU European Union EUR Regional Committee for Europe EUROSTAT Statistical Office of the European Communities EU-IDB European Injury Database ECPSP European Consumer Product Safety Platform EuroSafe European Association for Injury Prevention and Safety Promotion FDS Full Data Set FRS Firefighters and Rescue Services GPSD General Products Safety Directive HASS Home Accident Surveillance System ICECI International Classification of External Causes of Injury ICD International Classification of Diseases IDB European Injury Database IPCHEM Information Platform for Chemical Monitoring IT Information Technology JAMIE Joint action on monitoring injuries in Europe JRC Joint Research Centre MDS Minimum Data Set MS Member State NEISS National Electronic Injury Surveillance System OECD Organisation for Economic Co-operation and Development PRISMA Preferred Reporting Items for Systematic Review and Meta-Analyses RAPEX Rapid Alert System for dangerous non-food products SWOT Strengths, Weaknesses Opportunities, Threats UFI Unique Formula Identifier US CPSC US Consumer Product Safety Commission WHO World Health Organization WP Work Package
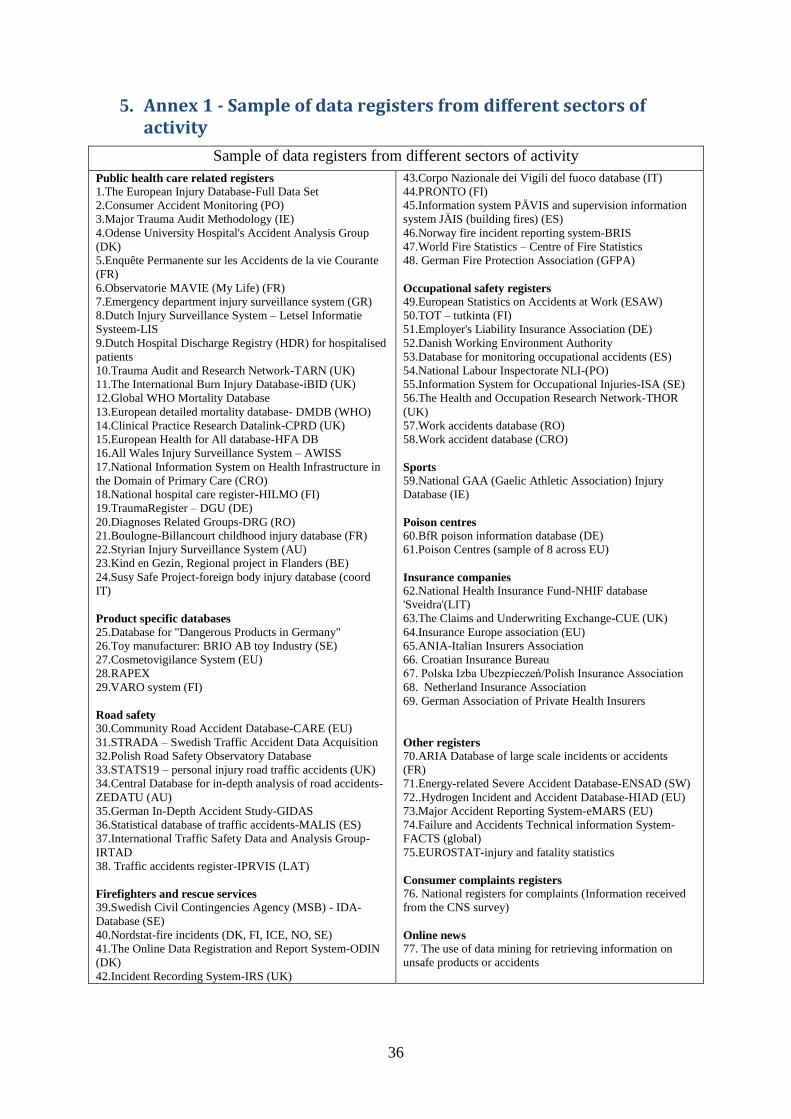
36
5. Annex 1 - Sample of data registers from different sectors of activity
Sample of data registers from different sectors of activity
Public health care related registers
1.The European Injury Database-Full Data Set
2.Consumer Accident Monitoring (PO)
3.Major Trauma Audit Methodology (IE)
4.Odense University Hospital's Accident Analysis Group
(DK)
5.Enquête Permanente sur les Accidents de la vie Courante
(FR)
6.Observatorie MAVIE (My Life) (FR)
7.Emergency department injury surveillance system (GR)
8.Dutch Injury Surveillance System – Letsel Informatie
Systeem-LIS
9.Dutch Hospital Discharge Registry (HDR) for hospitalised
patients
10.Trauma Audit and Research Network-TARN (UK)
11.The International Burn Injury Database-iBID (UK)
12.Global WHO Mortality Database
13.European detailed mortality database- DMDB (WHO)
14.Clinical Practice Research Datalink-CPRD (UK)
15.European Health for All database-HFA DB
16.All Wales Injury Surveillance System – AWISS
17.National Information System on Health Infrastructure in
the Domain of Primary Care (CRO)
18.National hospital care register-HILMO (FI)
19.TraumaRegister – DGU (DE)
20.Diagnoses Related Groups-DRG (RO)
21.Boulogne-Billancourt childhood injury database (FR)
22.Styrian Injury Surveillance System (AU)
23.Kind en Gezin, Regional project in Flanders (BE)
24.Susy Safe Project-foreign body injury database (coord
IT)
Product specific databases
25.Database for "Dangerous Products in Germany"
26.Toy manufacturer: BRIO AB toy Industry (SE)
27.Cosmetovigilance System (EU)
28.RAPEX
29.VARO system (FI)
Road safety
30.Community Road Accident Database-CARE (EU)
31.STRADA – Swedish Traffic Accident Data Acquisition
32.Polish Road Safety Observatory Database
33.STATS19 – personal injury road traffic accidents (UK)
34.Central Database for in-depth analysis of road accidents-
ZEDATU (AU)
35.German In-Depth Accident Study-GIDAS
36.Statistical database of traffic accidents-MALIS (ES)
37.International Traffic Safety Data and Analysis Group-
IRTAD
38. Traffic accidents register-IPRVIS (LAT)
Firefighters and rescue services
39.Swedish Civil Contingencies Agency (MSB) - IDA-
Database (SE)
40.Nordstat-fire incidents (DK, FI, ICE, NO, SE)
41.The Online Data Registration and Report System-ODIN
(DK)
42.Incident Recording System-IRS (UK)
43.Corpo Nazionale dei Vigili del fuoco database (IT)
44.PRONTO (FI)
45.Information system PÄVIS and supervision information
system JÄIS (building fires) (ES)
46.Norway fire incident reporting system-BRIS
47.World Fire Statistics – Centre of Fire Statistics
48. German Fire Protection Association (GFPA)
Occupational safety registers
49.European Statistics on Accidents at Work (ESAW)
50.TOT – tutkinta (FI)
51.Employer's Liability Insurance Association (DE)
52.Danish Working Environment Authority
53.Database for monitoring occupational accidents (ES)
54.National Labour Inspectorate NLI-(PO)
55.Information System for Occupational Injuries-ISA (SE)
56.The Health and Occupation Research Network-THOR
(UK)
57.Work accidents database (RO)
58.Work accident database (CRO)
Sports
59.National GAA (Gaelic Athletic Association) Injury
Database (IE)
Poison centres
60.BfR poison information database (DE)
61.Poison Centres (sample of 8 across EU)
Insurance companies
62.National Health Insurance Fund-NHIF database
'Sveidra'(LIT)
63.The Claims and Underwriting Exchange-CUE (UK)
64.Insurance Europe association (EU)
65.ANIA-Italian Insurers Association
66. Croatian Insurance Bureau
67. Polska Izba Ubezpieczeń/Polish Insurance Association
68. Netherland Insurance Association
69. German Association of Private Health Insurers
Other registers
70.ARIA Database of large scale incidents or accidents
(FR)
71.Energy-related Severe Accident Database-ENSAD (SW)
72..Hydrogen Incident and Accident Database-HIAD (EU)
73.Major Accident Reporting System-eMARS (EU)
74.Failure and Accidents Technical information System-
FACTS (global)
75.EUROSTAT-injury and fatality statistics
Consumer complaints registers
76. National registers for complaints (Information received
from the CNS survey)
Online news
77. The use of data mining for retrieving information on
unsafe products or accidents

37

38