diphosphate (t-mndp) as a radioactive drug - citeseerx
TRANSCRIPT
Br. J. Cancer (1974) 29, 373
INVESTIGATIONS OF TRITIATED MENADIOL SODIUMDIPHOSPHATE (T-MNDP) AS A RADIOACTIVE DRUG
J. S. MITCHELL
From the Radiotherapeutic Centre, Addenbrooke's Hospital, and Department of Radiotherapeutics,University of Cambridge, Hills Road, Cambridge, CB2 2 Q Q
Received 14 December 1973. Accepted 25 January 1974
Summary.-An attempt has been made to develop tritiated derivatives of Synkavit(menadiol sodium diphosphate, MNDP) of high specific activity as a radioactivedrug.
This paper summarizes the preliminary biological and physical studies, withemphasis on approximate radiation dosimetry and the necessary preliminarytesting, and then gives an account of the clinical investigations and the trials carriedout so far, which correspond essentially to Phases I and II trials for a chemothera-peutic agent.
In all, 214 patients with different sites and types of advanced and recurrent,inoperable, histologically verified malignant tumours including reticuloses havebeen treated with doses of at least 1 Ci of the various preparations. Among the 203evaluable treated cases, some form of response was observed in 23 out of 151 (15-2%)receiving the drug by intravenous injections and 13 out of 52 (25%) after intra-arterialinjections. For the sites and types of malignant diseases which showed responsesafter either intravenous or intra-arterial administration among the 55 patientssurviving at least 3 months after the first injection, some form of response wasobserved in 32 but only 5 of these showed either a " complete " or a " partial"response.
It is concluded that further investigation is desirable. It is suggested thatclinical trials with randomization should be carried out for inoperable cases ofcarcinoma of the colon and of the pancreas.
As A METHOD of improving the treat-ment of patients with cancer, I thought itwas important to try to develop radio-active drugs, i.e., compounds which areconcentrated selectively in the viablemalignant cells of tumours and carryincorporated radioactive atoms in suffi-ciently high specific activity to the rightplace, in order to produce the radiothera-peutic effect in situ, and without signifi-cant damage to normal tissues. Thepresent work arose from studies of chemi-cal radiosensitizers, which started in 1946with Synkavit (Roche Products Ltd,menadiol sodium diphosphate, MNDP).We noticed that a few minutes afterintravenous injection of doses of 100-150mg of MNDP some patients experienced
sensations or even local pain in the regionof the tumour. Following up this un-expected finding, investigations showedthat MNDP, or a major metabolite of it,concentrated to some extent selectivelyin the malignant cells of some experi-mental tumours in animals and certainhuman tumours.
For therapeutic applications, we havedeveloped tritiated derivatives of MNDP-abbreviated T-MNDP-incorporatingtritium, (3H) in very high specific activity.This is the work of a team in Cambridge,with the collaboration of the Radio-chemical Centre, Amersham, Bucks., andRoche Products Ltd, Welwyn GardenCity. It started in 1953 with the pre-paration of. derivatives of MNDP and
J. S. MITCHELL
some related compounds, labelled with14C, 82Br, 1311 and finally tritium, withprogressively increasing specific activity(Maxwell, 1954, 1955; Marrian and Max-well, 1956a, b; Marrian, 1957; Hor-witz et al. (1959); Andrews et al., 1962;Hodgson, 1968; Thomas, personal com-munication, 1970). The various aspectsof this investigation and published workon other radioactive drugs have beenreviewed (Mitchell, 1965, 1967, 1970,1971a, b).
Relevant properties of tritiurn andapproximate clinical dosimetry
Tritium (3H) appears to be very suit-able for incorporation into a radioactivedrug. Its radiobiological action is local-ized in single cells or cell constituents.It is a pure beta ray emitter with verysoft beta radiation which behaves biologic-ally like a low LET radiation. Thebeta particles are completely absorbed inabout 6 ,am in water and soft tissue ofunit density. The mean energy of thebeta particles is 5 73 ± 0 03 keV and thecorresponding range in unit density tissueis approximately 0 9 rim. The radio-active half-life is 12-4 years but almostinvariably the values of the biologicalhalf-life (BHL) observed for human tissuesand tumours with the radioactive drugsT-MNDP have been very much less,often between 7 and 14 days for the mainhalf-life, though sometimes less, and in sonecases greater for tumour than for normaltissues (Chipperfield, 1967a). Values ofthe main half-life found for carcinoma ofthe rectum were 9 and 13 days; a valueof 3-4 days was observed in a case ofsquamous carcinoma of the skin.
It is useful to introduce the conceptof the Differential Absorption Ratio(DAR) defined as the ratio of the specificactivity ofthe tumour or relevant normaltissue to the mean specific activity ofthe body as a whole. An important stepin the investigation of the individualpatient is the measurement of the specificactivity of tumour tissue, and also at
least one normal tissue, if possible. Thereare, of course, some cases where it is notpracticable to carry out such procedures.
The most important quantitative rela-tionship concerning the dosimetry is thatfor uniformly distributed tritium at astationary concentration, 1 mCi per g oftissue delivers a dose rate of 293 rad perday (24 h).
As a first approximation, calculationsof radiation dose based on the assumptionof uniform distribution of the tritium innormal tissues and tumours have proveduseful.
Assuming uniform distributionthroughout the body, 1 Ci of tritiumadministered in a single injection to a70 kg patient delivers a dose of 18-1 radfor a BHL of 3 days, 36-2 rad for BHL6 days, 54-4 rad for BHL 9 days, 72-5 radfor BHL 12 days and 78-5 rad for BHL13 days (Mitchell et al., 1963). Theapproximate values of the equivalentsingle doses, if the radiation were deliveredat a high dose rate, would be for thedifferent values of BHL, about 8, 14, 21,27 and 29 rad respectively.
For most of the patients treated byintravenous T-MNDP, repeated injectionshave been given at intervals, often of 3or 4 days, which in general are consider-ably less than the BHL in the tumour butare comparable with the BHL in the bodyas a whole, as shown by excretion studies.The approximate values of the dosesdelivered to normal tissues and tumourshave been calculated, usually by meansof a two-exponential model, with corres-ponding values of a short initial half-lifeand a longer main half-life (Chipperfield,1967a). It was found that in most casesa power law gave a good or even betterfit for the dependence of specific activityupon time but with this method calculationof the dose delivered was more difficult(White, 1973).
For doses calculated on the assump-tion of a uniform distribution of thetritium of T-MNDP in normal tissues andtumours, it appears that in most casesthe clinical results are not inconsistent
374
INVESTIGATIONS OF TRITIATED MENADIOL SODIUM DIPHOSPHATE (T-MNDP) :375
with experience of external radiotherapy,if the further assrumption is made that theRBE has the value of 15 in relation to60Co gamma radiation. Such a value isprobably not inconsistent with previousexperimental findings (see e.g., Hall,Oliver and Bedford, 1967, and our ownEM-autoradiographic studies, noting alsothe work of Cleaver, 1971.).
However, the basis for these calcula-tions can only be regarded as a crude firstapproximation. In general, in additionto macroscopic inhomogeneity there isinhomogeneity of the microscopic distri-bution of the tritium, which has beenstudied by morphometry and by auto-radiography including EM-autoradio-graphy, in addition to measurements ofthe specific activity of the tritium inmacroscopic specimens. With regard tothe human tumours studied (Chipperfield,1 967a), the initial uptake observed inbiopsy and surgical specimens taken 30min after intravenous or intra-arterialinjection was highest in cases of carcinomaof the gastrointestinal tract, with values of22*1 ± 8-4 1Cli per g wet weight per Ciinjected for TRK 219 and 27*4 i 2X2 ,uCiper g per Ci injected for TRA 119. Insome of these tumours and their metas-tases there was abundant stroma whichshowed low uptake, so that the meanspecific activity of the tumour cells maybe considerably higher than the averagevalue for the macroscopic specimen,e.g., in one case by a factor of 6 3. Thereis often wide variation among the tumourcells and in different parts of the tumour.Taking into account this distribution ofactivity, it is possible to calculate anapproximate value of the nmean tumourcell dose, but difficult to estimate theminimum tumour cell dose, even thoughthe uptake is limited to viable tumourcells. In a typical example of carcinomaof the colon, the specific activity of thegross specimen may be 20 ,uCi per g perCi injected, so that allowing for stromaand necrotic areas by means of a factorof 3*5, the mean specific activity of thetumour cells would be 70 /tCi per g per Ci
28
and for a single dose of 10 Ci injected0 70 mCi per g; the corresponding initialmean tumour cell dose would be 205 radper 24 h. For a typical value of thebiological half-life of 10 days and meanlife 14 4 days, the total mean cell dosedelivered would be 2950, say of the orderof 3000 rad. Assuming a value of theRBE of 1P5, the total mean tumour celldose would be equivalent biologically toabout 4500 rad of y radiation deliveredcontinuously over about 14 days.Examples of calculations for the repeatedsmall doses generally used in the treatmentof individual patients will be discussed inconsidering the results.
From the point of view of detaileddosimetry, as a further extension of theordinary (light microscopic) autoradio-graphy (Mitchell et al., 1963) quantitativeEM-autoradiographic studies have beencarried out on tumour cells in sectionsfrom patients treated with T-MNDP.Significant concentration, often by factorsof 3-5, was found in the nucleoli andnucleolus associated chromatin, mainlyin the mid and late S and early G2phases.
It is to be noted that the introductionof tritium as a hydrogen isotope into anorganic molecule such as MNDP causes nochange in its chemical structure orpharmacological properties. Almost cer-tainly there is no significant isotope effect.Moreover, the properties of tritium andof T-MNDP and its metabolism are suchthat the handling of these preparationspresents no serious difficulties in thera-peutic applications. The health andsafety precautions described (Mitchell,1965) have been extended to the treatmentof outpatients with unit amounts of up to5 Ci but usually not more than 3 Ci bvintravenous injection.
MATERIALS AND METHODS
Preparations of T-MJIVDP used.-The firstpreparations of T-MINDP, called TI, weremade by the Wilzbach procedure but some ofthese appeared to contain tritiated water as
J. S. MITCHELL
an impurity, which was toxic to the bonemarrow. The specific activity of TI cor-responded to approximately one atom oftritium per molecule of MNDP. Thesepreparations were used from 4 February 1959to 17 August 1960 for the treatment of casesNos. 1-27.
Since September 1960 all the preparationsof T-MNDP have been made by chemicalsynthesis, the tritium being incorporated infirmly bound positions by means of catalyticdehydrogenation of the corresponding halogenderivatives (Andrews et al., 1962). Wedescribed these preparations following thecatalogue of the Radiochemical Centre:TRA 72, containing theoretically one atomof tritium in the 6-position, had maximumspecific activity 29-1 Ci/mmol, correspondingto 1 Ci in 14-64 mg of compound, and wasused from 21 September 1960 to 5 May 1961for the treatment of cases Nos. 28-48. TRA119 contained up to 3 atoms of tritium permolecule in the 5, 6 and 7 positions, withmaximum specific activity 87-3 Ci/mmol,corresponding to 1 Ci in 4-88 mg, and wasused from 7 March 1962 to 12 December 1963in the treatment of cases Nos. 49-99. Amore reliable preparation was the next one,TRK 219, wrhich contained 2 tritium atoms permolecule in the 6 and 7 positions withmaximum specific activity 58-2 Ci/mmol,corresponding to 1 Ci in 7 32 mg, and wasused from 24 September 1964 to 19 June 1970for cases Nos. 100-224. Attempts werethen made again to prepare the compoundwNith 4 tritium atoms per molecule in the 5, 6,7 and 8 positions (Hodgson, 1968; Thomas,personal communication, 1970). This pre-paration, TRK 397, varied in specific activityamong 8 batches from 83 Ci/mmol up to105 5 Ci/mmol, corresponding to 3-63 tritiumatoms per molecule and 4-03 mg per Ci, andwas used from 18 August 1970 to 12 Sep-tember 1972 for cases Nos. 225-260. Thepreparation, TRQ 347, of specific activity70 Ci/mmol was used from 6 February 1973to 20 March 1973 for cases Nos. 261, 262 and264. The preparation, TRQ 368, of specificactivity 85 Ci/mmol was used from 1 May1973 to 28 June 1973 for cases Nos. 263, 265and 266. The solutions are sterilized byfiltration into rubber capped bottles andfrozen; the bottles of solution are stored inthe gases above liquid nitrogen at about-196°C in a commercial liquid nitrogenrefrigerator " (Union Carbide Ltd). Storage
at this temperature reduces the rate ofdecomposition by a factor of at least 5(Evans, 1966).
With these radioactive drugs, one needsa high degree of radiopharmaceutical purity,as well as of radiochemical purity. Evennouw, the individual batches may differ inbiological properties. For this reason everybatch of T-MNDP is tested routinely ontissue cultures with autoradiography to becertain of a high degree of selective uptakein cells of a human tumour strain, Hep/2(derived from a nasopharyngeal carcinoma)with negligible uptake into cells of normalorigin, for which we now use mouse L cells.In earlier stages of the testing, other cellswere included, viz., HeLa cells and normalcells of human amniotic epithelium andembryonic skin, and lung epithelium, as wellas monkey kidney cells (Simon-Reuss, 1961;Dendy, 1969; Morley and Dendy, 1973). Abad " batch shows uptake into the cells of
normal origin. Quantitatively, ' good "
batches show from 30 up to even 100 timesthe uptake into the tumour cells comparedwith that in the normal cells. These testsalso provide a check for sterility. In addi-tion, every batch has been tested to excludeacute toxicity-which has never beenobserved after intravenous injection in rabbitsin doses corresponding to 11 Ci and 22 Ci/70kg body weight. These rabbits have beenkept for the rest of their life span for studiesof possible late radiation effects.
Pre-clinical testing.-In this investigation,using the preparations of T-MNDP of veryhigh specific activity, the chemical toxicityof MNDP is negligible (Mitchell, 1948, 1949).In addition to the tissue culture studies,many experiments have been carried out onmice, rats and rabbits; these have beencontinued throughout the years and includedhaematological studies on the rabbits. DiVita (1964, personal communication) showedthat in mice for a single intraperitonealinjection of TRA 72, the LD 50/30 days wasabout 20 mCi/g body weight, but only 1 1mCi/g for tritiated water, for which there isessentially uniform distribution of the radio-activity: a value of about 1 mCi/g had alsobeen found for tritiated water by Brues,Stroud and Rietz (1952). The results of ourdistribution studies with T-MNDP in ratswvith the Walker carcinosarcoma 256 wereconfirmed for mice with spontaneous mam-mary adenocarcinoma by Ganatraet al. (1969).
376
INVESTIGATIONS OF TRITIATED MENADIOL SODIUM DIPHOSPHATE (T-MNDP) 377
Information of great value from the pointof viewr of the clinical applications in man wAasobtained in studies of the treatment ofspontaneous malignant tumours and leukae-mias in cats and dogs by our veterinarycolleague, Dr I. A. Silver (Silver et al., 1962).For example, 5 out of 7 cases of carcinoma ofthe tongue and palate in cats respondedfavourably to initra-arterial injection ofquite small doses of T-MNDP and 2 of theselived longer than 2 years: tumours of thesesites did not respond satisfactorily to externalradiotherapy with 220 kVp x-rays. In
addition, in long-term studies in 4 normalpuppies aged 3 months (2 male and 2 female)injected wAith single doses of TRK 219equivalent to 22 Ci/70 kg body -weight, therewas no effect on bone growth or epiphysealclosure. No abnormalities of any sort couldbe detected in any of the 4 in life or at post-mortem examination at 1, 2, 3 and 4 years
respectively. The 2 longest surviving pup-
pies, one male and one female, wAere matedw,ith other dogs and fathered or producednormal litters. Subsequently they ere
mated together and also produced a normallitter. Measurements of the radioactivity oftissues taken at autopsy from other dogsshowed relatively high activities in the eye
(lens and retina), kidney, intestine andpancreas within a few hours of treatment.Nine months after treatment one case stillhad detectable activity in marrowx- andretina. No changes in the fundus of the eye
or defects of vision wA-ere observed (Professor1. A. Silver, personal communication, 1970).
Clinical trials a)?d relevaiat clinicalinvestigations
The design and analysis of the clinicalinvestigations of T-MNDP have followedthe general plan wTidely used for the examina-tion of new chemotherapeutic agents (Bruleet al., 1973). However, the problemsinvolved wAere not as fully understood whenthese trials wN-ere started in February 1959as at present and, moreover, there are essen-
tial differences betwTeen a radioactive drugsuch as T-MNDP and most chemotlhera-peutic agents. There is no serious problemof chemical toxicity because of the highspecific activity of the preparations ofT-MiNDP used. There wN-as already a sub-stantial body of knowledge concerning theeffects and hazards of internally administered
radioactive isotopes, and very considerableclinical experience of the uses of 1311 and 32pin inorganic form in therapy. The value andlimitations of approximate dosimetry forthese two isotopes had been emphasized inmany investigations, including our own(Phillips, 1954, 1957; Phillips and Saunders,1957; Phillips, Haybittle and Newberry,1960; Mitchell, 1955, 1971a, b). WithT-MNDP, the estimated radiation dosesproved to be a reliable starting point as afirst approximation, which enabled us tomake rapid progress. Partly because ofthis, and also because no other basis wouldhave been acceptable, wre set out to includeassessment of anti-tumnour action in theExploratory Phase, corresponding to Phase I,of our trials. Further, the investigationswhich can be regarded as within the scope ofclinical pharmacology as applied to a radio-active drug have continued throughout mostof Phase II; also the quality of the radioactivedrug has improved steadily over the years.
In Phase 1, we started the treatment ofpatients with advanced or refractorytumours" using intra-arterial (i.a.) injection,mainly with the Seldinger technique asdeveloped by Dr D. McC. Gregg (1958), andthen used intravenous (i.v.) injections inpatients with generalized metastases " (Hor-
wNitz et al., 1959). We noted that Gehan (1961)had shown that if a drug wAere effective in20% of patients, or more, there wNould be a950 chance of one or more successes in 14consecutive cases. Wre found 5 responseswhich were estimated on the modest basis
of reduction in size of the tumour, or of partof the tumour in the first 14 cases. Accord-ingly, w!e felt wre must continue the investiga-tion and wre were encouraged by the relief ofpain we observed in 5 of these patients.
From the beginning we started relevantinvestigations and first obtained evidence ofuptake of T-MNDP in tumours after i.a.injection. Detailed studies of tritium uptakeand distribution, half-lives and radiationdoses, and excretion and metabolism havecontinued (Horwitz et al., 1959; Marrian,Marshall and Mitchell, 1961: Marrian et al.,1965; Chipperfield, 1967a, b; see also White,1973). Summarizing our findings, includingthose on autopsies, after a single injection of10 Ci of T-MNDP/70 kg body weight, thetotal doses, wNith standard deviation, receivedby normal tissues were estimated as follows:kidney 222 ± 78 rad, testis 180 ± 29 rad,
J. S. MITCHELL
bone marrow 83 ± 65 rad, liver 145 ± 78rad, brain (long-lived component only)137 r 46 rad, skeletal muscle 54 f 26 radand small intestine 93 = 29 rad.
Phase 11, the main part of the trial so far,which is concei-ned with screening for clinicalactivity, has now been completed after thetreatment of a further 200 cases. Weselected the correct range of dosage from thebeginning, so that the patients in bothPhases I and 11 can be evaluated as a singlegr-oup. All patients have been re-assessed interms of present criteria. The selection ofpatients for treatment by means of T-MNDPwvas always discussed with colleagues. Iexamined all the patients myself, oftenthroughout the treatment and at least atsome stage of the treatment and follow-up;in most cases, I gave the intravenous injec-tions myself.
From 4 February 1959 to 13 July 1973 wehave treated, wvith doses of at least 1 Ci of thevarious preparations of T-MNDP, a total of214 patients wvith different types of advancedand recurrent, inoperable, histologically veri-fied malignant tumnours and reticuloses.These tritiated drugs wAere used only when allother therapeutic measures surgery, radio-therapy, chemotherapy and hormone therapyhad failed or wvere definitely contra-
indicated. Many of the patients were veryill and in poor' general condition.
Assess)nent of the results of treatment wvithT'-MNDP
The following criteria wvere used forassessment:
Curative. Well and free firom clinicalevidence of disease at 5 years or more afterfirst treatment with the radioactive drug,noting whether alive or dead.
Palliative.-Survival after first treatmentwith the radioactive drug, and
Clinical responses (Hill and Larsen, 1972;Gerner and Moore, 1973) were defined asfollows: C.R. cornplete response. Allineasurable signs and all symptoms of tumourdisappear; P.R.-partial response. At leasta 5000 decrease in the maximum crQss-sectional area of the tumour without simul-taneous progression of disease elsewhere:Iic.R. incomplete response (extension ofthe term ' lesser response' as defined byGerner and Moore, 1973) including: (a)reduiction of the size of the tumour with less
than a 5000 decrease in the maximumcross-sectional area, or (b) more than a 500odecrease in the maximum cross-sectionalarea of the tumour or of parts of the tumour,wzTith simultaneous progression of the diseaseelsewhere, or (c) significant improvement ofgeneral condition and increase in performancestatus (Karnofsky et al., 1951) or (d) usefulrelief of pain, if possible assessed in terms ofreduction of the amounts of analgesic drugsrequired, or (e) relief of intractable pruritus,or more than one of these criteria.
Responses were required to persist for atleast 4 weeks.
None. No significant clinical response.This includes: no change or stationarydisease, and progression, defined as a measur-able increase in the maximum cross-sectionalarea of the tumour greater than 250%, orappearance of new lesions, or definite worsen-ing of the patient's general condition.
N.E. Non-evaluable treatments werestudied, and classified as follows: Notevaluable because treatment was initiatedprophylactically for poor prognosis as adju-vant therapy following, or in associationwith, radiation therapy or surgery, includingpotentially curative measures, or not curableby standard means, but no lesions wereevaluable for measurement. Included werepatients who were treated with radiationtherapy and chemotherapy simultaneouslyor previously and in this case died within1 month of the complications of the previoustreatment.
RESULTS
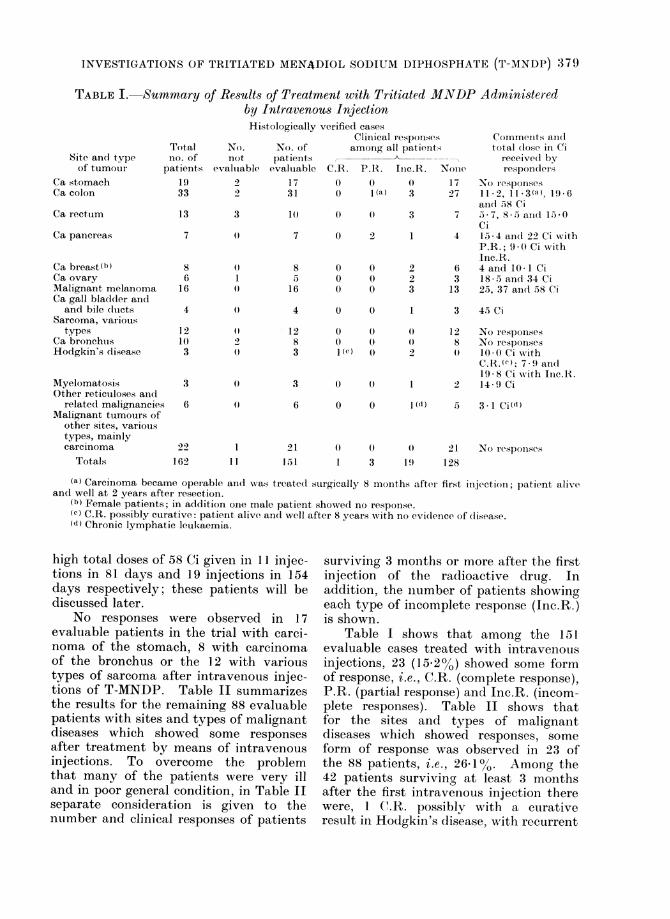
The results of treatment of the 162patients with the various preparationsof T-MNDP administered by intravenousinjection are sunmmarized in Table I. Ofthese patients, 151 were evaluable. Thenumbers of patients showing the differenttypes of clinical response are listed andthe footnotes give additional information.
Table I includes the total dose in Cireceived by patients showing some clinicalresponse. Except for single doses of upto 4 Ci, these total doses were deliveredin a series of repeated injections, often2-3 times weekly, each single injectionusually not exceeding 3 Ci. Mentionmust be made of 2 patients (Cases Nos.119 and 157) who received exceptionally
3'i-7
INVESTIGATIONS OF TRITIATED MENADIOL SODIUM DIPHOSPHATE (T-MNDP) 379
TABLE I. Summary of Ressults of Treatment with Tritiated MNDP Administeredby Intravenous InjectionHistologically verified cases
Site and typeof tumotur p
Ca stomachCa colon
Ca recttum
Ca pancreas
Ca breast(h)Ca ovaryMalignant melanomaCa gall bladder andand bile ducts
Sarcoma, varioustypes
Ca bronchusHodgkin's disease
MyelomatiosisOther reticuloses aiic
related malignanciesMIalignant tumours ofother sites, varioustypes, mainlycarcinoma
Totals
Totalno. ofatients
No.not
evalutable
No. ofpat ientsevaluable C.R.
Clinical respjonsesamong all patients
P.R. Inc.R. None
Comments an1(ltotal (lose in Ci
receive(l byrespond(ers
19 2 17 0 O ( 17 No responses33 2 31 0 1(a) 3 27 11-2, 11-3(a), 19-6
ain(i 58 Ci13 3 1 57 5 7, S ;, aI1(I 1 O0
ci7 (0 7 0 2 1 4 134 andl 22 Ciw ith
P.R.; 9 (0 Ci withInc.R.
8 0) 8 0 0 2 (6 4andO10-I Ci6 1 5 0 0 2 3 18-5annd34Ci
16 (0 16 0 0 3 13 25, 37and 5S8Ci
0} 4 0 0
12103
20
1283
0 00 01(c) 0
3 0 3 0 0
6 0
12162 11
3 45 Ci
12 No responises8 No responses
l010 Ci withC.R.(e): 7.) an(i19 8 Ci with Inc.R.
2 149 Ci
0 0 l (d) 5 3 -1 Ci(d)
21151
0) 0} 0 21)I1 3 1l) 128
No responses
(a) Carcinoma became operable and was treated surgically 8 inonths after first inijection; patient alivean(l well at 2 years after resection.
(b) Female patients; in addition one male patient show%ed no response.(c) C.R. possibly curative: patient alive and well after 8 years with no evi(delnce of disease.(d) Chronic lymphatic leukaemia.
high total doses of 58 Ci given in 11 injec-tions in 81 days and 19 injections in 154days respectively; these patients will bediscussed later.
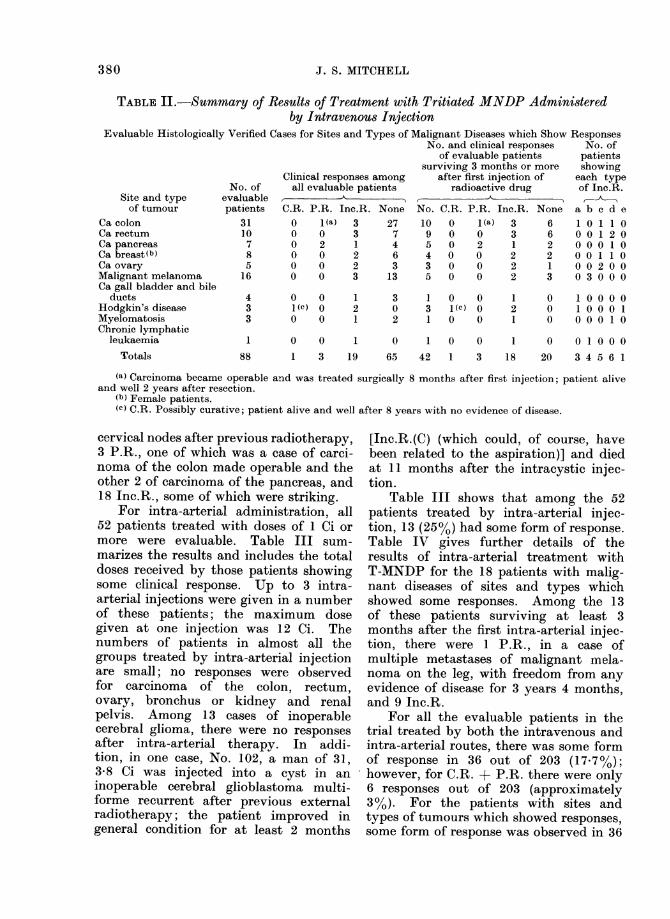
No responses were observed in 17evaluable patients in the trial with carci-noma of the stomach, 8 with carcinomaof the bronchus or the 12 with varioustypes of sarcoma after intravenous injec-tions of T-MNDP. Table II summarizesthe results for the remaining 88 evaluablepatients with sites and types of malignantdiseases which showed some responsesafter treatment by means of intravenousinjections. To overcome the problemthat many of the patients were very illand in poor general condition, in Table IIseparate consideration is given to thentimber and clinical responses of patients
surviving 3 months or more after the firstinjection of the radioactive drug. Inaddition, the number of patients showingeach type of incomplete response (Inc.R.)is shown.
Table I shows that among the 151evaluable cases treated with intravenousinjections, 23 (152%0) showed some formof response, i.e., C.R. (complete response),P.R. (partial response) and Inc.R. (incom-plete responses). Table II shows thatfor the sites and types of malignantdiseases which showed responses, someform of response was observed in 23 ofthe 88 patients, i.e., 26l1%. Among the42 patients surviving at least 3 monthsafter the first intravenous injection therewere, 1 C.R. possibly with a curativeresult in Hodgkin's disease, with recurrent
380 J. S. MITCHELL
TABLE II.-Summary of Result8 of Treatment with Tritiated MNDP Admini8teredby Intravenous Injection
Evaluable Histologically Verified Cases for Sites and Types of Malignant Diseases which Show ResponsesNo. and clinical responses No. of
of evaluable patients patientssurviving 3 months or more showing
Clinical responses among after first injection of each typeNo. of all evaluable patients radioactive drug of Inc.R.
Site and type evaluable , A_ _ A , _ _ _ _ _of tumour patients C.R. P.R. Inc.R. None No. C.R. P.R. Inc.R. None a b c d e
Ca colon 31 0 1(a) 3 27 10 0 1(a) 3 6 1 0 1 1 0Ca rectum 10 0 0 3 7 9 0 0 3 6 0 0 1 2 0Ca pancreas 7 0 2 1 4 5 0 2 1 2 0 0 0 1 0Ca breast(b) 8 0 0 2 6 4 0 0 2 2 0 0 1 1 0Ca ovary 5 0 0 2 3 3 0 0 2 1 0 0 2 0 0NMalignant melanoma 16 0 0 3 13 5 0 0 2 3 0 3 0 0 0Ca gall bladder and bile
ductsHodgkin's diseaseMyelomatosisChronic lymphatic
leukaemiaTotals
433
0 0 11(C) 0 20 0 1
302
131
0 01(c) 00 0
121
000
1 00001 0 0 0 1O O 0 1 0
1 0 0 1 0 1 0 0 1 0 0 1 0 0 088 1 3 19 65 42 1 3 18 20 3 4 5 6 1
(a) Carcinoma became operable and was treated surgically 8 months after first injection; patient aliveand well 2 years after resection.
(b) Female patients.(e) C.R. Possibly curative; patient alive and well after 8 years with no evidence of disease.
cervical nodes after previous radiotherapy,3 P.R., one of which was a case of carci-noma of the colon made operable and theother 2 of carcinoma of the pancreas, and18 Inc.R., some of which were striking.
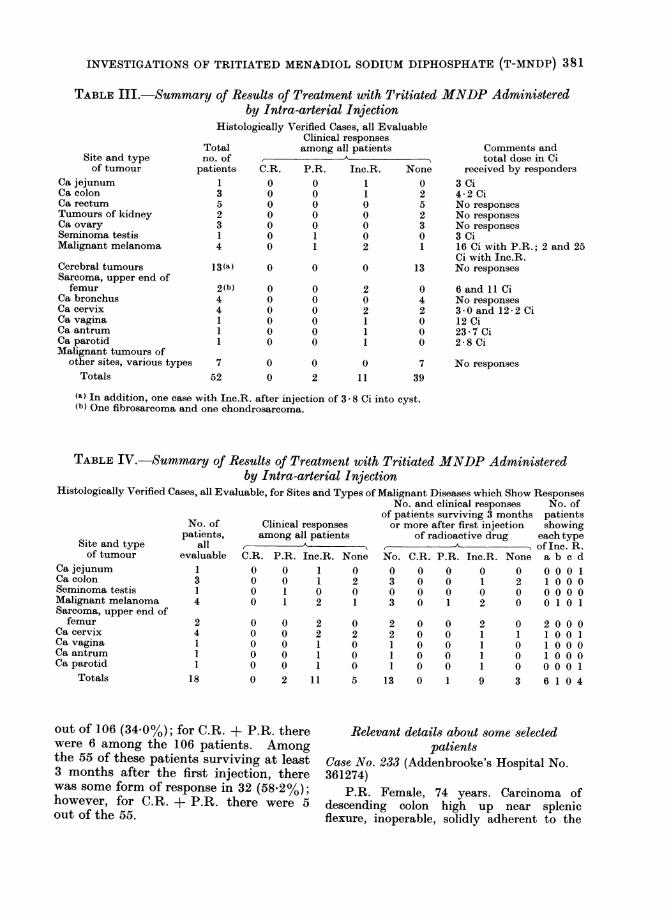
For intra-arterial administration, all52 patients treated with doses of 1 Ci ormore were evaluable. Table III sum-marizes the results and includes the totaldoses received by those patients showingsome clinical response. Up to 3 intra-arterial injections were given in a numberof these patients; the maximum dosegiven at one injection was 12 Ci. Thenumbers of patients in almost all thegroups treated by intra-arterial injectionare small; no responses were observedfor carcinoma of the colon, rectum,ovary, bronchus or kidney and renalpelvis. Among 13 cases of inoperablecerebral glioma, there were no responsesafter intra-arterial therapy. In addi-tion, in one case, No. 102, a man of 31,3.8 Ci was injected into a cyst in aninoperable cerebral glioblastoma multi-forme recurrent after previous externalradiotherapy; the patient improved ingeneral condition for at least 2 months
[Inc.R.(C) (which could, of course, havebeen related to the aspiration)] and diedat 11 months after the intracystic injec-tion.
Table III shows that among the 52patients treated by intra-arterial injec-tion, 13 (25%) had some form of response.Table IV gives further details of theresults of intra-arterial treatment withT-MNDP for the 18 patients with malig-nant diseases of sites and types whichshowed some responses. Among the 13of these patients surviving at least 3months after the first intra-arterial injec-tion, there were 1 P.R., in a case ofmultiple metastases of malignant n ela-noma on the leg, with freedom from anyevidence of disease for 3 years 4 months,and 9 Inc.R.
For all the evaluable patients in thetrial treated by both the intravenous andintra-arterial routes, there was some formof response in 36 out of 203 (17.7%);however, for C.R. + P.R. there were only6 responses out of 203 (approximately3%). For the patients with sites andtypes of tumours which showed responses,some form of response was observed in 36
C C%I
t
I
I
INVESTIGATIONS OF TRITIATED MENADIOL SODIUM DIPHOSPHATE (T-MNDP) 381
TABLE III.-Summary of Results of Treatment with Tritiated MNDP Administeredby Intra-arterial Injection
Histologically Verified Cases, all EvaluableClinical responses
Total among all patients Comments andLI', i 1- ,,I , .1Site and typeof tumour
Ca jejunumCa colonCa rectumTumours of kidneyCa ovarySeminoma testisMalignant melanoma
Cerebral tumoursSarcoma, upper end offemur
Ca bronchusCa cervixCa vaginaCa antrumCa parotidMalignant tumours of
other sites, various typesTotals
nppat
O. of total dose in Citients C.R. P.R. Inc.R. None received by responders
1 0 0 1 0 3 Ci3 0 0 1 2 4-2 Ci5 0 0 0 5 No responses2 0 0 0 2 No responses3 0 0 0 3 No responses1 0 1 0 0 3 Ci4 0 1 2 1 16 Ci with P.R.; 2 and 25
Ci with Inc.R.13(a) 0 0 0 13 No responses
2(b)441
1
000000
000000
202111
042000
7 0 0 0 752 0 2 11 39
6 and 11 CiNo responses3-0 and 12-2 Ci12 Ci23-7 Ci2-8 Ci
No responses
(a) In addition, one case with Inc.R. after injection of 3 - 8 Ci into cyst.(b) One fibrosarcoma and one chondrosarcoma.
TABLE IV.-Summary of Results of Treatment with Tritiatedby Intra-arterial Injection
MNDP Administered
Histologically Verified Cases, all Evaluable, for Sites and Types of Malignant Diseases which Show ResponsesNo. and clinical responses No. of
of patients surviving 3 months patientsNo. of Clinical responses or more after first injection showing
patients, among all patients of radioactive drug each typeSite and type all A,A_ , of Inc. R.of tumour evaluable C.R. P.R. Inc.R. None No. C.R. P.R. Inc.R. None a b c d
Ca jejunum 1 0 0 1 0 0 0 0 0 0 0 0 0 1Ca colon 3 0 0 1 2 3 0 0 1 2 1 0 0 0Seminoma testis 1 0 1 0 0 0 0 0 0 0 0 0 0 0Malignant melanoma 4 0 1 2 1 3 0 1 2 0 0 1 0 1Sarcoma, upper end offemur
Ca cervixCa vaginaCa antrumCa parotid
Totals
24111
18
0 0 2 0 2 00 0 2 2 2 00 0 1 0 1 00 0 1 0 1 00 0 1 0 1 00 2 11 5 13 0
out of 106 (34.0%); for C.R. + P.R. therewere 6 among the 106 patients. Amongthe 55 of these patients surviving at least3 months after the first injection, therewas some form of response in 32 (58.2%);however, for C.R. + P.R. there were 5out of the 55.
000001
211119
010003
2001001001 00000610
010U14
Relevant details about some selectedpatients
Case No. 233 (Addenbrooke's Hospital No.361274)
P.R. Female, 74 years. Carcinoma ofdescending colon high up near splenicflexure, inoperable, solidly adherent to the
I-
J. S. MITCHELL
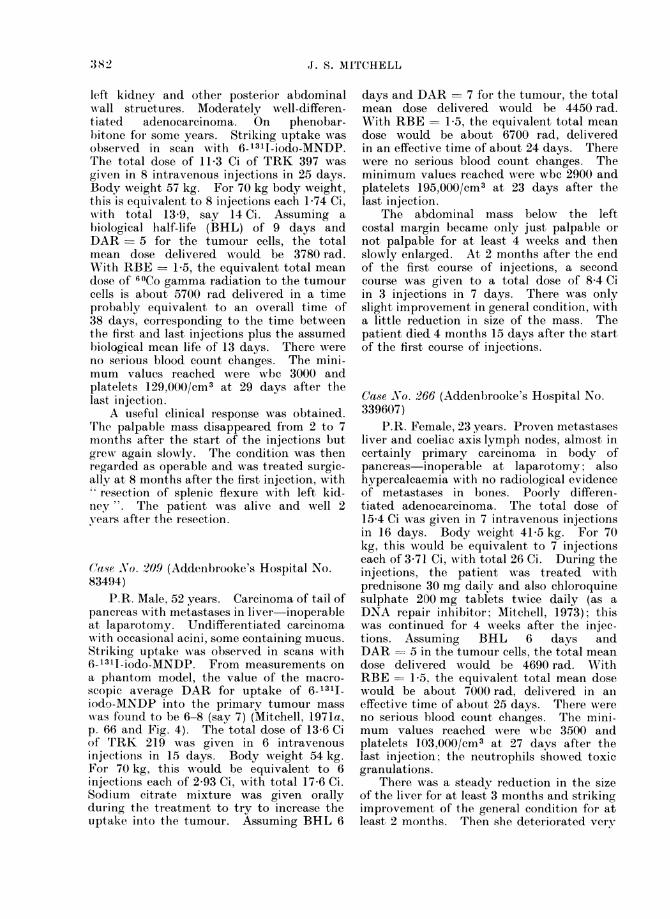
left kidney and other posterior abdominalwall structures. Moderately well-differen-t iated adenocarcinoma. On phenobar-bitone for some years. Striking uptake wNasobserved in scan with 6-1311-iodo-MNDP.'I'he total dose of 11-3 Ci of TRK 397 wasgiven in 8 intravenous injections in 25 days.Body weight 57 kg. For 70 kg body weight,this is equivalent to 8 injections each 1P74 Ci,with total 13-9, say 14 Ci. Assuming abiological half-life (BHL) of 9 days andDAR = 5 for the tumour cells, the totalmean dose delivered would be 3780 rad.With RBE _ 1-5, the equivalent total meandose of _iCo gamma radiation to the tumourcells is about 5700 rad delivered in a timeprobably equivalent to an overall time of38 days, corresponding to the time betweenthe first and last injections plus the assumedbiological mean life of 13 days. There wereno serious blood count changes. The mini-mum values reached were wbc 3000 andplatelets 129,000/cm3 at 29 days after thelast injection.
A useful clinical response was obtained.Trhe palpable mass disappeared from 2 to 7moniths after the start of the injections butgreN again slowly. The condition was thenregarded as operable and was treated surgic-ally at 8 months after the first injection, withresection of splenic flexure with left kid-
ney". The patient was alive and well 2years after the resection.
Ca,-se No. 209 (Addenbrooke's Hospital No.83494)
P.R. Male, 52 years. Carcinoma of tail ofpancreas wAith metastases in liver inoperableat laparotomy. Undifferentiated carcinomawNith occasional acini, some containing mucus.Striking uptake was observed in scans with6-1311-iodo-MNDP. From measurements ona phantom model, the value of the macro-scopic average DAR for uptake of 6-131I1iodo-MNDP into the primary tumour masswas found to be 6-8 (say 7) (Mitchell, 1971a,p. 66 and Fig. 4). The total dose of 13-6 Ciof TRK 219 was given in 6 intravenousinjections in 15 days. Body wreight 54 kg.For 70 kg, this would be equivalent to 6injections each of 2-93 Ci, w\ith total 17-6 Ci.Sodium citrate mixture was given orallyduring the treatment to try to increase theu]ptake into the tumour. Assuming BHL 6
days and DAR = 7 for the tumour, the totalmean dose delivered would be 4450 rad.With RBE = 1-5, the equivalent total meandose would be about 6700 rad, deliveredin an effective time of about 24 days. Therewere no serious blood count changes. Theminimum values reached were wbc 2900 andplatelets 195,000/Cm3 at 23 days after thelast injection.
The abdominal mass below the leftcostal margin became only just palpable ornot palpable for at least 4 weeks and thenslowly enlarged. At 2 months after the endof the first course of injections, a secondcourse was given to a total dose of 8-4 Ciin 3 injections in 7 days. There was onlyslight improvement in general condition, witha little reduction in size of the mass. Thepatient died 4 months 15 days after the startof the first course of injections.
Case .No. 266 (Addenbrooke's Hospital No.339607)
P.R. Female, 23 years. Proven metastasesliver and coeliae axis lymph nodes, almost incertainly primary carcinoma in body ofpancreas-inoperable at laparotomy; alsohypercaleaemia with no radiological evidenceof metastases in bones. Poorly differen-tiated adenocarcinoma. The total dose of15-4 Ci was given in 7 intravenous injectionsin 16 days. Body weight 41-5 kg. For 70kg, this would be equivalent to 7 injectionseach of 3-71 Ci, with total 26 Ci. During theinjections, the patient w\as treated withprednisone 30 mg daily and also chloroquinesulphate 200 mg tablets twice daily (as aDNA repair inhibitor; Mitchell, 1973); thiswas continued for 4 weeks after the injec-tions. Assuming BHL 6 days andDAR = 5 in the tumour cells, the total meandose delivered would be 4690 rad. WithRBE= 1-5 the equivalent total mean dosewould be about 7000 rad, delivered in aneffective time of about 25 days. There wereno serious blood count changes. The mini-mum values reached wNere wbc 3500 andplatelets 103,000/cm3 at 27 days after thelast injection; the neutrophils showed toxicgranulations.
There was a steady reduction in the sizeof the liver for at least 3 months and strikingimprovement of the general condition for atleast 2 months. Then she deteriorated very
38 2
INVESTIGATIONS OF TRITIATED MENADIOL SODIUM DIPHOSPHATE (T-MNDP) 383
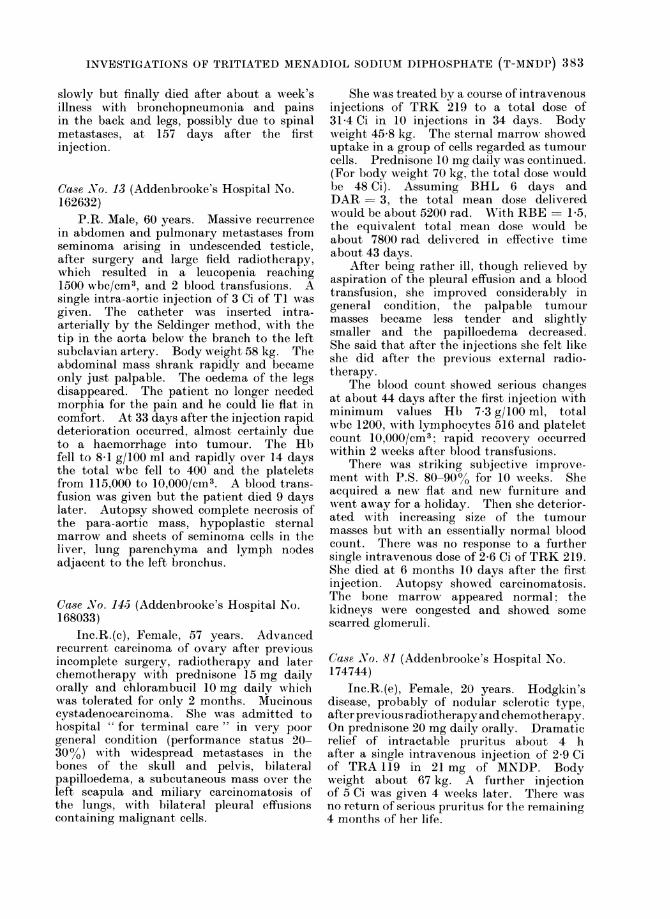
slowly but finally died after about a week'sillness with bronchopneumonia and painsin the back and legs, possibly due to spinalmetastases, at 157 days after the firstinjection.
Case No. 13 (Addenbrooke's Hospital No.162632)
P.R. Male, 60 years. Massive recurrencein abdomen and pulmonary metastases fromseminoma arising in undeseended testicle,after surgery and large field radiotherapy,which resulted in a leueopenia reaching1500 wbe/Cm3, and 2 blood transfusionls. Asingle intra-aortic injection of 3 Ci of TI wasgiven. The catheter was inserted intra-arterially by the Seldinger method, Nith thetip in the aorta below the branch to the leftsubelavian artery. Body weight 58 kg. Theabdominal mass shrank rapidly and becameonly just palpable. The oedema of the legsdisappeared. The patient no longer neededmorphia for the pain and he could lie flat incomfort. At 33 days after the injection rapiddeterioration occurred, almost certainly dueto a haemorrhage into tumour. The Hbfell to 8-1 g/100 ml and rapidly over 14 daysthe total wbc fell to 400 and the plateletsfrom 115,000 to 10,000/cIn3. A blood trans-fusion was given but the patient died 9 dayslater. Autopsy showed complete necrosis ofthe para-aortic mass, hypoplastic sternalmarrow and sheets of seminoma cells in theliver, lung parenchyma and lymph nodesadjacent to the left bronchus.
Case No. 14,5 (Addenbrooke's Hospital No.168033)
Inc.R.(c), Female, 57 years. Advancedrecurrent cai-cinoma of ovary after previousincomplete surgery, radiotherapy and laterchemotlherapy with prednisone 15 mg dailyorally and chlorambucil 10 mg daily whichwas tolerated for only 2 months. Mucinouscystadenocarcinoma. Slhe was admitted tohospital ' for terminal care " in very poorgeneral condition (performance status 20-300o) with widespread metastases in thebones of the skull and pelvis, bilateralpapilloedema, a subcutaneous mass over theleft scapula and miliary carcinomatosis ofthe lungs, w%ith bilateral pleural effusionscontaining malignant cells.
She was treated by a course of intravenousinjections of TRK 219 to a total dose of31-4 Ci in 10 injections in 34 days. Bodyweight 45-8 kg. The sternal marrow showeduptake in a group of cells regarded as tumourcells. Prednisone 10 mg daily wAas continued.(For body weight 70 kg, the total dose wouldbe 48 Ci). Assuming BHL 6 days andDAR = 3, the total mean dose deliveredwould be about 5200 rad. WAith RBE = 1 5,the equivalent total mean dose would beabout 7800 rad delivered in effective timeabout 43 days.
After being rather ill, though relieved byaspiration of the pleural effusion and a bloodtransfusion, she improved considerably ingeneral condition, the palpable tumourmasses became less tender and slightlysmaller and the papilloedema decreased.She said that after the injections she felt likeshe did after the previous external radio-therapy.
The blood count shoNed serious changesat about 44 days after the first injection withminimum values Hb 7-3 g/100 ml, totalwbc 1200, with lymphocytes 516 and plateletcount 10,000/cm3; rapid recovery occurredwithin 2 weeks after blood transfusions.
There was striking subjective improve-ment with P.S. 80-90% for 10 weeks. Sheacquired a new- flat and new furniture andwent away for a holiday. Then she deterior-ated with increasing size of the tumourmasses but with an essentially normal bloodcount. There was no response to a furthersingle intravenous dose of 2-6 Ci of TRK 219.She died at 6 months 10 days after the firstinjection. Autopsy showed carcinomatosis.The bone marrow appeared normal, thekidneys were congested and showed somescarred glomeruli.
Case Vo. 81 (Addenbrooke's Hospital No.174744)
Inc.R.(e), Female, 20 years. Hodgkin'sdisease, probably of nodular sclerotic type,after previous radiotherapy and chemotherapy.On prednisone 20 mg daily orally. Dramaticrelief of intractable pruritus about 4 hafter a single intravenous injection of 2-9 Ciof TRA 119 in 21 mg of MNDP. Bodyweight about 67 kg. A further injectionof 5 Ci was given 4 weeks later. There wasno return of serious pruritus for the remaining4 months of her life.
J. S. MITCHELL
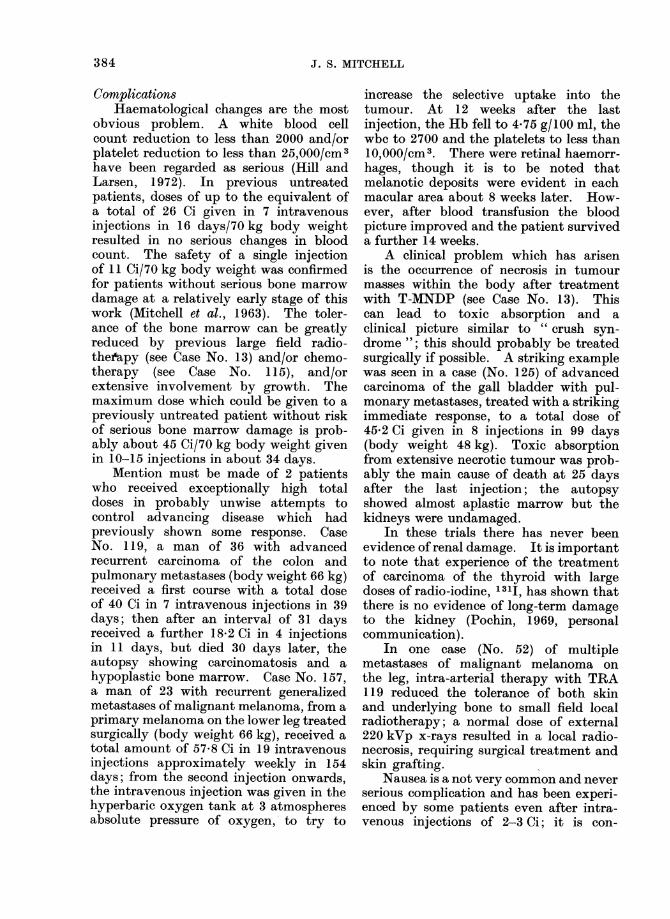
ComnplicationsHaematological changes are the most
obvious problem. A white blood cellcount reduction to less than 2000 and/orplatelet reduction to less than 25,000/cm3have been regarded as serious (Hill andLarsen, 1972). In previous untreatedpatients, doses of up to the equivalent ofa total of 26 Ci given in 7 intravenousinjections in 16 days/70 kg body weightresulted in no serious changes in bloodcount. The safety of a single injectionof 11 Ci/70 kg body weight was confirmedfor patients without serious bone marrowdamage at a relatively early stage of thiswork (Mitchell et al., 1963). The toler-ance of the bone marrow can be greatlyreduced by previous large field radio-theiapy (see Case No. 13) and/or chemo-therapy (see Case No. 115), and/orextensive involvement by growth. Themaximum dose which could be given to apreviously untreated patient without riskof serious bone marrow damage is prob-ably about 45 Ci/70 kg body weight givenin 10-15 injections in about 34 days.
Mention must be made of 2 patientswho received exceptionally high totaldoses in probably unwise attempts tocontrol advancing disease which hadpreviously shown some response. CaseNo. 119, a man of 36 with advancedrecurrent carcinoma of the colon andpulmonary metastases (body weight 66 kg)received a first course with a total doseof 40 Ci in 7 intravenous injections in 39days; then after an interval of 31 daysreceived a further 18-2 Ci in 4 injectionsin 11 days, but died 30 days later, theautopsy showing carcinomatosis and ahypoplastic bone marrow. Case No. 157,a man of 23 with recurrent generalizedmetastases of malignant melanoma, from aprimary melanoma on the lower leg treatedsurgically (body weight 66 kg), received atotal amount of 57-8 Ci in 19 intravenousinjections approximately weekly in 154days; from the second injection onwards,the intravenous injection was given in thehyperbaric oxygen tank at 3 atmospheresabsolute pressure of oxygen, to try to
increase the selective uptake into thetumour. At 12 weeks after the lastinjection, the Hb fell to 4-75 g/100 ml, thewbc to 2700 and the platelets to less than10,000/cm3. There were retinal haemorr-hages, though it is to be noted thatmelanotic deposits were evident in eachmacular area about 8 weeks later. How-ever, after blood transfusion the bloodpicture improved and the patient surviveda further 14 weeks.
A clinical problem which has arisenis the occurrence of necrosis in tumourmasses within the body after treatmentwith T-MNDP (see Case No. 13). Thiscan lead to toxic absorption and aclinical picture similar to " crush syn-drome "; this should probably be treatedsurgically if possible. A striking examplewas seen in a case (No. 125) of advancedcarcinoma of the gall bladder with pul-monary metastases, treated with a strikingimmediate response, to a total dose of45-2 Ci given in 8 injections in 99 days(body weight 48 kg). Toxic absorptionfrom extensive necrotic tumour was prob-ably the main cause of death at 25 daysafter the last injection; the autopsyshowed almost aplastic marrow but thekidneys were undamaged.
In these trials there has never beenevidence of renal damage. It is importantto note that experience of the treatmentof carcinoma of the thyroid with largedoses of radio-iodine, 1311, has shown thatthere is no evidence of long-term damageto the kidney (Pochin, 1969, personalcommunication).
In one case (No. 52) of multiplemetastases of malignant melanoma onthe leg, intra-arterial therapy with TRA119 reduced the tolerance of both skinand underlying bone to small field localradiotherapy; a normal dose of external220 kVp x-rays resulted in a local radio-necrosis, requiring surgical treatment andskin grafting.
Nausea is a not very common and neverserious complication and has been experi-enced by some patients even after intra-venous injections of 2-3 Ci; it is con-
384
INVESTIGATIONS OF TRITIATED MENADIOL SODIUM DIPHOSPHATE (T-MNDP) 385
trolled almost invariably by oral perphen-azine (Fentazin) 4 mg tablets; usuallyone tablet is taken about half an hourbefore the injection and another 2 hafterwards.
Three patients appeared to be madeworse by intravenous injections ofT-MNDP, one case (No. 97) with multiplerecurrent secondary skin nodules of malig-nant melanoma, another (No. 68) alsowith multiple metastases of malignantmelanoma and shortly afterwards develop-ing cerebral metastases, and a case (No.211) of advanced carcinoma of the colonwhich obstructed after the intravenousinjection of 2-9 Ci, presumably due tolocal oedema. Another patient (CaseNo. 244) with an inoperable carcinoma ofthe colon, which had previously perforatedand been treated surgically by palliativesigmoid colectomy, experienced abdominalpain even after single intravenous doses of0 5 Ci of TRK 397; it was only possible togive a total dose of 2-5 Ci.
After intra-arterial injection, one case
(No. 5) developed a femoral arterial myco-tic aneurysm, 3-4 cm diameter, 3 monthsafter catheterization as a result of woundsepsis.
Ancillary proceduresMany laboratory and clinical studies
have been made to try to increase theselective uptake of T-MNDP into tumours.The most encouraging ancillary agent isprednisone, which appears to increase thealkaline phosphatase on the tumour cellsurface in some cases; the effects on normalcells must be studied further. The possi-bilities of the use of phenobarbitone as an
enzyme inducer should also be con-
sidered. Fasting appears to be of prac-
tical value (White, 1973). In in vitroexperiments with Ehrlich ascites tumourcells it had been found that lack of glucosein the medium increased the dephos-phorylation of MNDP but not of ATP(Fisher, 1968, personal communication;see Mitchell, 1971a, p. 46). This findingmay explain the striking response,
Inc.R.(b) in a patient (No. 103) withrecurrent multiple metastases of malig-nant melanoma who also had diabetes,controlled on tolbutamide. The use ofpotassium citrate mixture to try toreduce the acidosis in tumours did notappear to be effective. Hyperbaric oxy-gen seemed to have some effect but it isdoubtful whether this procedure is ofsufficient practical value to justify itsfurther study. Acetylcholine did notincrease the uptake, as studied by scanningwith 6-1311-iodo-MNDP but producedlocal pain in the region of the tumour. Itmust be noted that tolazoline (Priscol)was used as a vasodilator with many of theintra-arterial injections. Recently, inter-esting results have been obtained by theuse of chloroquine as a DNA repairinhibitor to try to increase the effects ofthe radiation delivered by the radioactivedrug, perhaps selectively in the tumourcells (Mitchell, 1973).
We have made many attempts toselect patients for treatment on the basisof measurements of the uptake of MNDPinto the tumour, using the followinginvestigations:
(i) Measurements of the specificactivity of tritium in samples oftumour and normal tissue if pos-sible. (It may be noted that avalue of the DAR of 14 was foundfor a biopsy specimen of recurrentmelanoma of the skin taken 35 miiiafter intravenous injection of 0 5 Ciof TRK 397, but there was noclinical response to treatment.)
(ii) Autoradiographic studies on sec-tions fronm operation and biopsyspecimens in conjunction withmeasurements of the specificactivity.
(iii) Autoradiographic studies of in vitrouptake by primary cultures ofmalignant cells freshly grown fromspecimens of tumour or asciticfluid. Many of the cases for whichthe cells in culture showed uptakehad been treated with prednisone.
386 J. S. MITCHELL
(iv) Radioisotope scanning using theradioiodine labelled derivative,6 - 1311 - iodo - 2 - methyl - 1,4 -naphthaquinol - bis(di - ammoniumphosphate), abbreviated 6-1311-iodo MNDP. (Details of this workwill be published elsewhere.) SeeMarrian et (al. (I 969).
CONCL-USIONS
The results of the trials of T-MNDPas a radioactive drug in the treatment ofselected patients with advanced malignantdiseases of various types and sites are ingeneral modest. The clinical results insome patients have been useful. It islikely that no responses can be expectedfor certain types and sites of tumour,e.g., inoperable carcinoma of the stomachfor treatment by intravenous injections,inoperable cerebral glioma for treatmentby intra-arterial injections. It is con-cluded that much further investigation isdesirable.
It is suggested that Phase III shouldbe started, with controlled clinical trials,with proper design and random alloca-tion of patients-perhaps with chemo-therapy in the control groups for thetreatment of inoperable cases of carcinomaof the colon and of carcinoma of thepancreas.
Further studies of ancillary agents andprocedures to improve the selection ofpatients appear to be necessary.
The possibilities of T-MNDP in thetreatment of selected patients withadvanced carcinoma of the rectum, breastand ovary and with advanced Hodgkin'sdisease and testicular seminoma haveprobably not been fully explored andappear to justify further investigation.Studies of rare tumours, such as primaryhepatoma, should also be envisaged.
This work provides further evidencethat tritium, when incorporated into asuitable compound, can produce thera-peutic effects in patients with malignantdiseases of certain sites and types. Thescope and limitations of the effectiveness
of T-MNDP as a radioactive drug appearto depend not only on the nature andproperties of the carrier molecule, whichare obviously of essential importance, butalso on the biochemistry and patho-logical physiology of the tumour, especiallyon the blood supply and size of the tumourmasses and the interrelationships of thetumour and the host.
I wish to acknowledge with gratefulthanks the most helpful collaboration ofthe staff of the Radiochemical Centre,Amersham, and of Roche Products Ltd,Welwyn Garden City.
These investigations are the work of ateam in Cambridge over many years. Iwish to thank the many collaborators towhose work reference has been made, andmany colleagues on the staff of the Radio-therapeutic Centre and the United Cam-bridge Hospitals. In addition, I wish tothank Mr E. A. King, Miss J. Young, MissE. J. Porter and Dr J. L. Haybittle.
I wish to express my grateful thanksfor financial assistance to the Inter-national Atomic Energy Agency, theMedical Research Council, the BritishEmpire Cancer Campaign-now the Can-cer Research Campaign and my ownCancer Research Fund.
REFERENCESANDREWS, K. J. M., BULTITULDE, F., EVANS, E. A.,GRONOW, M., LAMIBERT, R. W. & MARRIAN, D. H.(1962) A Radioactive Drug: 2-AMethyl-6-Tritio-1 ,4-Napht,haquinol. Bis (Disodium Phosphate)and 2-Methyl-5,6,7-Tritritio-1 ,4-NaphthaquinolBis (Disodium Phosphate). J. chem. Soc.,3440.
BRUES, A. M., STROUD, A. N. & RIETZ, L. (1952)Toxicity of Tritium Oxide to Mice. Proc. Soc.exp. Biol. Med., 79, 174.
BRULIE, G., ECKHARDT, S. J., HALL, T. C. & WINK-LER, A. (1973) Drug Therapy of Cancer. Geneva:World Health Organization.
CHIPPERFIELD, B. (1967a) Tritium Uptake, Half-Lives and Radiation Doses in Tissues of CancerPatients Treated with Tritiated 2-Methyl-1,4-Naphthaquinol Diphosphate. Int. J. Cancer, 2,381.
CHIPPERFIELD, B. (1967b) Excretion of Tritiumafter Therapeutic Injections of Tritiated 2-Methyl-I,4-Naphthaquinol Diphosphate in CancerPatients. Int. J. Cancer, 2, 396.
INVESTIGATIONS OF TRITIATED MENADIOL SODIUM DIPHOSPHATE (T-MNDP) 387
CLEAVER, J. E. (1971) Haematological Consequencesof Radio-Isotope Incorporation, with particularreference to Tritium, Phosphorus and Strontium.In Manual on Radiation Haematology. Vienna:International Atomic Energy Agency.
DENDY, P. P. (1969) Selective Uptake of a Radio-active Drug into Human Tumour Cells Growingin Tissue Culture. Acta radiol. ther. phys. biol.,8, 514.
EVANS, E. A. (1966) Stability of a RadioactiveDrug-Tetrasodium 2-Methyl-I ,4-NaphthaquinolDiphosphate Labelled with Tritium. Nature,Lond., 209, 196.
GANATRA, R. D., RAMANATHAN, P., PATEL, M. C.,MEHTA, M. N., SHAHANI, S. N., SHARMA, S. M.,MANI, R. S., NORONHA, 0. P. D. & BLAU, M.(1969) Radio-Iodinated Synkol as a Tumour-Localizing Agent. In Medical Radioisotope Scin-tigraphy, Vol. II. Vienna: International AtomicEnergy Agency.
GEHAN, E. A. (1961) The Determination of theNumber of Patients Required in a Preliminaryand a Follow-up Trial of a New ChemotherapeuticAgent. J. chron. Dis., 13, 346.
GERNER, R. E. & MOORE, G. E. (1973) Multiple-Drug Therapy for Malignant Solid Tumors inAdults. Cancer Chemother. Rep., Pt 1, 57, 237.
GREGG, D. McC. (1958) Renal Aortography andSelective Renal Arteriography. Postgrad. mned.J., 34, 149.
HALL, E. J., OLIVER, R. & BEDFORD, J. S. (1967)The Relative Biological Effectiveness of TritiumBeta Particles Compared to Gamma Radiation-Its Dependence on Dose-rate. Br. J. Radiol.,40, 704.
HILL, G. J. & LARSEN, R. R. (1972) Cancer Chemo-therapy. I. Methods, Agents and OverallResults in 400 Patients. Oncology, 26, 206.
HoDGsoN, A. (1968) Studies Related to the Synthesisof a Tritiated Derivative of 2-Methyl-1,4-Naph-thoquinone. Ph.D. Dissertation, University ofCambridge.
HORWITZ, H., GREGG, D. McC., MARRIAN, D. H.,MARSHALL, B. & MITCHELL, J. S. (1959) Clinicaland Laboratory Studies of the TherapeuticPossibilities of Tritiated Synkavit, Mainly byIntra-arterial Administration. Acta rad. Suppl.,188, 111.
KARNOFSKY, D. A., BURCHENAL, J. H., ARMISTEAD,G. C., SOUTHAM, C. M., BERNSTEIN, J. L., CRAVER,L. F. & RHOADS, C. P. (1951) Triethylene Mela-mine in the Treatment of Neoplastic Disease.A.M.A. Archs internal Med., 87, 477.
MARRIAN, D. H. & MAXWELL, D. R. (1956a) TracerStudies of Potential Radiosensitising Agents:Tetrasodium 2-14C-Methyl- 1,4-Naphthohydroqui-none Diphosphate. Br. J. Cancer, 10, 575.
MARRIAN, D. H. & MAXWELL, D. R. (1956b) TracerStudies of Potential Radiosensitising Agents:Tetrasodium 2-Methyl-382Br-1,4-Naphthohydro-quinone Diphosphate and Tetrasodium 2,3-Dimethyl - 5,6 - di - l311 - iodo - 1,4 - benzohydro-quinone Diphosphate. Br. J. Cancer, 10, 739.
MARRIAN, D. H. (1957) Tritium-labelled 2-Methyl-1,4-Naphthoquinone and Confirmation of theStructure of its Adduct with Sodium HydrogenSulphite. J. chemn. Soc., 499.
MARRIAN, D. H., MARSHALL, B. & MITCHELL, J. S.(1961) Laboratory and Clinical Studies ofSome Quinol Diphosphates and Related
Compounds as Chemical Radiosensitizers and theDevelopment of a Radioactive Drug. Chemo-therapia, 3, 225.
MARRIAN, D. H., MARSHALL, B., MITCHELL, J. S. &SIMoN-REuss, I. (1965) An Attempt to Developa Radioactive Drug for Cancer Chemotherapy.In The Trcatment of Cancer. Ed. J. S. Mitchell.Cambridge: University Press. p. 98.
MARRIAN, D. H., MITCHELL, J. S., BULL, C. H.,King, E. A. & SZAZ, K. F. (1969) Labelled Com-pound Related to Synkavit and Its Uptake inCertain Human Tumours Studied by Radio-Isotope Scanning. Acta radiol., 8, 221.
MAXWELL, D. R. (1954) Some Experiments withLabelled Compounds Related to 2-Methyl-1,4-Naphthohydroquione Diphosphate (Synkavit).In 2nd Radioisotope Conference, Oxford. London:Butterworth.
MAXWELL, D. R. (1955) Studies of ChemotherapeuticAgents, which Incorporate Radioactive Atomsand May Concentrate in Malignant Tumour Cells.Ph.D. Dissertation, University of Cambridge.
MITCHELL, J. S. (1948) Clinical Trials of Tetra-sodium 2-Methyl-1,4-Naphthohydroquinone Di-phosphate, in Conjunction with X-ray Therapy.Br. J. Cancer, 2, 351.
MITCHELL, J. S. (1949) Histological ChangesProduced by Large Doses of Tetra-sodium2-Methyl-1,4-Naphthohydroquinone Diphosphatein Some Human Tumours. Experienta, 5, 293.
MITCHELL, J. S. (1955) Isotopes. In British Prac-tice in Radiotherapy. Ed.: E. Rock Carling, B.Windeyer and D. W. Smithers. London: Butter-worths. p. 97.
MITCHELL, J. S., KINa, E. A., AMARRIAN, D. H. &CHIPPERFIELD, B. (1963) Investigation of a Radio-active Drug (TRA 119) With Special Reference toAutoradiographic and Related Studies. Actaradiol. B. ther. phys. biol., 1, 321.
MITCHELL, J. S. (1965) An Attempt to Develop aRadioactive Drug. Clin. Radiol., 16, 305.
MITCHELL, J. S. (1967) The Use of Tritium-LabelledCompounds. Chapter from Modern Trends inRadiotherapy. Ed.: T. J. Deeley and C. A. P.Wood. London: Butterworths.
MITCHELL, J. S. (1970) Uber die Moglichkeit derEntwicklung radioaktiver Pharmaka. Fortschr.Strahlensch. Strahlenschutz in Forschung undPraxis, 10. Stuttgart: Georg Thieme.
MITCHELL, J. S. (1971a) Cancer. If Curable, whynot Cured? Cambridge: W. Heffer and Sons.
MITCHELL, J. S. (1971b) Neuere Untersuchungenzur Frage der Therapeutischen Anwendungenvon Tritium-Markierten Organischen Substanzen.Atomlkernenergie, 18, 109.
MITCHELL, J. S. (1973) Clinical Trials of Radio-sensitizers and Fractionation. Br. J. Radiol., 46,481.
MORLEY, T. G. & DENDY, P. P. (1973) Mechanismsof Selective Uptake of 2-Methyl-1,4-Naphtho-quinol Bis Disodium Phosphate Into SomeMammalian Cells in Tissue Culture. Br. J.Cancer, 28, 55.
PHILLIPS, A. F. (1954) The Gamma-ray Dose inCarcinoma of the Thyroid Treated by Radio-iodine. Acta radiol., 41, 533.
PHILLIPS, A. F. (1957) Choice of a RadioactiveIsotope for the Treatment of Carcinoma of theThyroid. Br. J. Radiol., 30, 247.

388 J. S. MITCHELL
PHILLIPS, A. F. & SAUNDERS, R. D. (1957) Auto-radiography and Radioactivity Measurementswith Human Neoplasms Containing Radiophos-phorus. Acta radiol., 48, 101.
PHILLIPS, A. F., HAYBITTLE, J. L. & NEWBERY, G.R. (1960) Use of Iodine-124 for the Treatment ofCarcinoma of the Thyroid. Acta Un. int. Cancr.,16, 1434.
SILVER, I. A., CATER, D. B., MARRIAN, D. H. &MARSHALL, B. (1962) Tritiated Tetra-sodium2-Methyl-1,4-Naphthaquinol Diphosphate for
Treatment of Spontaneous Tumours in Animals.Acta radiol., 58, 281.
SIMON-REUSS, I. (1961) 3H Incorporation intoAscites Tumour and Tissue Culture Cells Exposedto Svnkavit and its Tritiated Analogue. Actaradiol., 56, 49.
WHITE, C. (1973) Laboratory Studies of a Radio-active Drug Used in the Treatment of Patientswith Cancer. Ph.D. Dissertation, University ofCambridge.