complement and autoimmunity
TRANSCRIPT

DIAGNOSIS OF AUTOIMMUNITY
Complement and autoimmunity
Eleonora Ballanti • Carlo Perricone • Elisabetta Greco •
Marta Ballanti • Gioia Di Muzio • Maria Sole Chimenti •
Roberto Perricone
Published online: 25 April 2013
� Springer Science+Business Media New York 2013
Abstract The complement system is a component of the innate immune system. Its main function was initially believed
to be limited to the recognition and elimination of pathogens through direct killing or stimulation of phagocytosis.
However, in recent years, the immunoregulatory functions of the complement system were demonstrated and it was
determined that the complement proteins play an important role in modulating adaptive immunity and in bridging innate
and adaptive responses. When the delicate mechanisms that regulate this sophisticated enzymatic system are unbalanced,
the complement system may cause damage, mediating tissue inflammation. Dysregulation of the complement system has
been involved in the pathogenesis and clinical manifestations of several autoimmune diseases, such as systemic lupus
erythematosus, vasculitides, Sjogren’s syndrome, antiphospholipid syndrome, systemic sclerosis, dermatomyositis, and
rheumatoid arthritis. Complement deficiencies have been associated with an increased risk to develop autoimmune dis-
orders. Because of its functions, the complement system is an attractive therapeutic target for a wide range of diseases. Up
to date, several compounds interfering with the complement cascade have been studied in experimental models for
autoimmune diseases. The main therapeutic strategies are inhibition of complement activation components, inhibition of
complement receptors, and inhibition of membrane attack complex. At present, none of the available agents was proven to
be both safe and effective for treatment of autoimmune diseases in humans. Nonetheless, data from preclinical studies and
initial clinical trials suggest that the modulation of the complement system could constitute a viable strategy for the
treatment of autoimmune conditions in the decades to come.
Keywords Complement system � Complement deficiency � Autoimmune disease � Anti-complement therapy
Introduction
The complement system is a component of the innate
immune system, which consists of physical, cellular, and
chemical elements. The immune system has evolved to
protect the human body against pathogens or other dan-
gerous elements, and its responses can be divided into
innate and adaptive immune responses. Traditionally, the
main function of the complement system was believed to
be limited to the recognition and elimination of pathogens
through direct killing and/or stimulation of phagocytosis
(innate responses) [1, 2]. In recent years, the immunoreg-
ulatory functions of the complement system were demon-
strated and it was determined that the complement proteins
play an important role in modulating adaptive immunity
and in bridging innate and adaptive responses [3]. The
contribution of complement to the development of humoral
immunity has been confirmed through a series of elegant
studies, and a body of data has accumulated demonstrating
E. Ballanti � E. Greco � M. Ballanti � G. Di Muzio �M. S. Chimenti � R. Perricone (&)
Rheumatology, Allergology and Clinical Immunology,
Department of Internal Medicine, Unit of Rheumatology,
University of Rome Tor Vergata, Via Montpellier 1,
00133 Rome, Italy
e-mail: [email protected]
C. Perricone
Reumatologia, Dipartimento di Medicina Interna e Specialita
Mediche, Sapienza Universita di Roma, Rome, Italy
Roberto Perricone
123
Immunol Res (2013) 56:477–491
DOI 10.1007/s12026-013-8422-y
that the activation of the complement system is also critical
to the development of T cell immunity [4].
The complement system comprises more than 30 plasma
and membrane-bound proteins [3, 5]. The activation of
these proteins occurs through three possible pathways: the
classical, the alternative, and the lectin pathways. All three
pathways are activated according to a cascade system, with
activation of one factor leading to the activation of the
next.
Pathways of complement system activation
The pathways of complement system activation constitute
enzyme cascades, analogous to the coagulation, fibrinoly-
sis, and kinin pathways. Several complement proteins are
cleaved during activation of the system, and the fragments
are generally designated with suffixes ‘‘a’’ and ‘‘b.’’ All
three pathways lead to the cleavage of C3 and finally
converge at the activation of C5 (Fig. 1). The activation of
the classical pathway is dependent on immunoglobulins
IgM or IgG, present in immune complexes (IC), and
binding to the C1 complex [6]. The binding of C1q to
antibody leads to activation of C4 and C2 inducing the
formation of the C4bC2a complex, also known as classical
pathway’s C3 convertase [7]. If the activation occurs
through the alternative pathway, factor D, a serine protease,
cleaves factor B, which is complexed with spontaneously
hydrolyzed iC3b, leading to formation of Ba and Bb. Bb
and C3b generate the C3 convertase of the alternative
pathway, C3bBb. Properdin increases the stability of this
enzyme [8]. The lectin pathway becomes activated, when
either mannose-binding lectin (MBL) or ficolins recognize
carbohydrate patterns on microbes and activate C2 and C4
through MBL-associated serine proteases (MASP), with
the formation of the same C3 convertase as the classical
pathway, C4bC2a [7]. Likewise, the classical and lectin
pathways generate the same C5 convertase (C3bC4bC2a),
whereas the alternative pathway generates a different C5
convertase (C3bBbC3b). The activation of C5 produces
C5a (a potent chemoattractant) and C5b which forms the
membrane attack complex (MAC) C5b-9, able to cause cell
lysis. In addition to cell lysis, effects of complement acti-
vation include activation of granulocytes and endothelia by
sublytic quantities of MAC; deposition of C3 fragments
(e.g., C3b, iC3b) on membranes and/or particles leading to
opsonization and enhanced phagocytosis; immune complex
clearance; clearance of apoptotic bodies; alterations in
immune cell signal transduction, adhesion activation and
cytokine production; anaphylatoxin-mediated effects [4].
Regulation of the complement system
To avoid excessive complement activation and thus protect
the host, the complement system is tightly controlled by
proteins present in the fluid phase and on cell membranes
[9]. Interestingly, evidence shows that many pathogenic
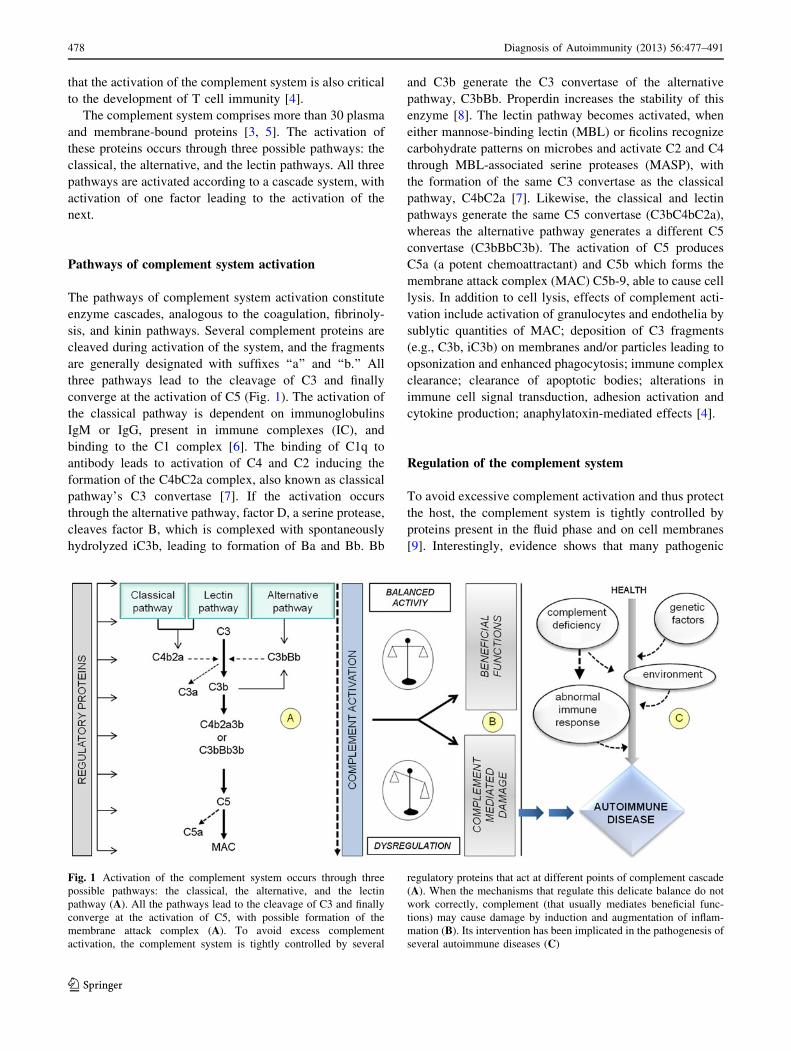
Fig. 1 Activation of the complement system occurs through three
possible pathways: the classical, the alternative, and the lectin
pathway (A). All the pathways lead to the cleavage of C3 and finally
converge at the activation of C5, with possible formation of the
membrane attack complex (A). To avoid excess complement
activation, the complement system is tightly controlled by several
regulatory proteins that act at different points of complement cascade
(A). When the mechanisms that regulate this delicate balance do not
work correctly, complement (that usually mediates beneficial func-
tions) may cause damage by induction and augmentation of inflam-
mation (B). Its intervention has been implicated in the pathogenesis of
several autoimmune diseases (C)
478 Diagnosis of Autoimmunity (2013) 56:477–491
123

microorganisms interact with these complement regulators
to elude the immune system [10].
Several proteins regulating the complement system
decrease the activity of C3 convertases in the classical and
alternative pathways, enzymes that catalyze key reactions
during the activation of the complement system. Moreover,
important control proteins are involved in the regulation of
C1 activity and of the MAC [9]. When the mechanisms that
regulate this delicate balance do not work properly or there
is an over-activation of the complement system exceeding
the capacity of the regulatory mechanisms, the complement
system may cause damage, by induction and amplification
of inflammation [3] (Fig. 1).
The importance of the regulatory mechanisms is evident
in hereditary angioedema (HAE). In this disease, the defi-
ciency of C1 inhibitor (C1INH), a multi-functional serine
protease inhibitor, causes inappropriate activation of the
complement system as well as of the other plasma enzy-
matic systems (contact system, coagulation system) that
results in recurrent episodes of angioedema involving the
skin and the mucosa [11].
Paroxysmal nocturnal hemoglobinuria is another
example of the consequences of the failure to regulate the
complement system. In such disease, a somatic mutation in
the phosphatidylinositol glycan class A gene causes a
deficiency of a protein required for the synthesis of gly-
cosylphosphatidylinositol, the lipid that anchors several
proteins to cell membranes [12]. As a result, two molecules
anchored by glycosylphosphatidylinositol, decay-acceler-
ating factor or CD55 (which regulates the formation of C3
convertase) and CD59 (which inhibits the formation of the
membrane attack complex), are lacking on cell membrane,
thus increasing susceptibility of erythrocytes to comple-
ment, leading to intravascular hemolysis [12].
Complement system as mediator of tissue damage
Several studies demonstrated that the complement system
is involved in inflammatory tissue damage. The activation
of the complement system in the tissues occurs through IC,
which trigger the classical complement pathway [5].
Moreover, in ischemic tissues, phospholipids and mito-
chondrial proteins, normally sequestrated in the cells, are
exposed and are able to activate the complement system
either directly by binding C1q or MBL or indirectly by
binding natural antibodies or C-reactive protein (CRP) [5].
CRP can activate the classical pathway by binding C1q.
Furthermore, necrotic cells and tissues lack the regulatory
molecules that normally prevent the binding of comple-
ment proteins [5].
Inappropriate activation of the complement system
causes the release of several pro-inflammatory mediators,
such as anaphylatoxins C3a and C5a that, in turn, are able
to stimulate the synthesis of other pro-inflammatory
mediators [13]. C5a is also a potent chemoattractant for
neutrophils, monocytes, and eosinophils [13]. In addition,
the MAC can contribute to inflammation and tissue dam-
age. Formation of the terminal complement complex C5b-9
can lead to cell death by necrosis or apoptosis [13].
The contribution of the complement system to tissue
damage is exemplified by necrosis following ischemia. In
fact, the activation of the complement system has been
demonstrated in areas of myocardial infarction and cerebral
stroke [5, 14].
Testing the complement system
Assays to test the complement levels in serum are one of
the standard measures used in the clinical management of
patients with autoimmune diseases. The complement sys-
tem is prone to in vitro artificial activation. Therefore, the
conditions of sample collection and storage are critical.
With some exceptions, samples for complement diagnosis
should be collected in ethylenediaminetetraacetic acid
(EDTA). Plasma should be separated soon after collection
and transferred immediately to the laboratory on ice or
frozen at -20 �C or preferably at -70 �C [15]. In the
majority of laboratories, measures are restricted to immu-
nochemical determinations of C3 and C4, and sometimes
C1q. The concentration of these proteins is usually asses-
sed by nephelometry or radial immunodiffusion by using
polyclonal antibodies, but more sensitive assays (sensitive
enzyme-linked immunosorbent assays—ELISA—or Wes-
tern blot) are available too.
A smaller number of laboratories routinely provide a
functional measurement of the activity of the whole com-
plement pathway from classical pathway activation
through to formation of the membrane attack complex,
such as the CH50 (complement hemolysis 50 %) test.
Although many variants have been described, hemolytic
assays are still based on protocols first described by Mayer
[16]. The test is very useful as it provides a profile of the
whole complement pathway. Tests for complexes or split
products formed during complement activation allow to
discriminate specific activation of the system from non-
specific [17]. Early tests to detect the cleavage of com-
plement proteins included counterimmunoelectrophoresis
or crossed immunoelectrophoresis. In the last decades,
ELISA tests using monoclonal antibodies have been
developed to specifically detect complement components,
such as alternative pathway proteins (native factor B, factor
D, and factor H, factor B split products Ba and Bb, C3-
fragments C3b/iC3b/C3dg) and anaphylatoxins (C3a and
C5a) in human blood plasma [18, 19]. Assays to measure
Diagnosis of Autoimmunity (2013) 56:477–491 479
123

these molecules are not widely available and require spe-
cial sample handling to a degree that makes routine clinical
use difficult. Complement components may represent a
target of autoantibody responses. Autoantibodies may
occur against individual components, convertase com-
plexes, complement regulating proteins, and complement
receptors. More clinically relevant autoantibodies are C3
nephritic factor, anti-C1q, and anti-C1INH that can be
detected through ELISA [20, 21].
In recent years, promising techniques to assess com-
plement activation within particular tissues have been
introduced. Non-invasive detection of complement activa-
tion through magnetic resonance imaging (MRI)-based
method has been proposed [22]. These results may open up
new avenues to develop tools for the monitoring of disease
progression in complement involving diseases.
Complement system and autoimmunity
The relation between the complement system and auto-
immunity is apparently paradoxical. If, on the one hand,
the complement system is activated and contributes to
tissue damage in autoimmune diseases, on the other hand,
deficiency of the complement proteins leads to autoim-
munity and it is challenging reconciling these two aspects.
The complement system is involved in the pathogenesis
and contributes to the clinical manifestations of several
autoimmune diseases (Fig. 1), such as systemic lupus
erythematosus (SLE), anti-glomerular basement membrane
disease, vasculitides, Sjogren’s syndrome (SS), anti-
phospholipid antibody syndrome (APS), systemic sclerosis
(SSc), dermatomyositis (DM), and rheumatoid arthritis
(RA) [23].
Paradoxically, complement system deficiencies are also
associated with autoimmune diseases. The prevalence of
complement system’s deficiencies in the population is
difficult to assess. Most heterozygotic complement-defi-
cient individuals are clinically normal. Generally, only C1-
INH (autosomal dominant), properdin (X-linked recessive),
and homozygotic complement-deficient individuals present
with clinical diseases. Deficiencies of components of the
complement system may result in a wide variety of clinical
presentations, including recurrent bacterial infections,
HAE, rheumatic disorders, leukocyte adhesion deficiency,
and hemolytic uremic syndrome [24].
Autoimmune disorders, mainly SLE, can be the com-
mon clinical manifestation of genetically determined dis-
orders of the complement system, and they are most
frequently observed in patients with deficiencies of the
early components of the classical pathway. Whereas over
30 % of patients with C2 deficiency and nearly 80 % of
patients with either C3 or C4 deficiency present
autoimmune manifestations, less than 10 % of the patients
with deficiencies of C5–9 develop similar clinical evi-
dences. The most common presentation is SLE, but discoid
lupus, dermatomyositis, scleroderma, and glomerulone-
phritis were also reported [25].
Several theories have been proposed to explain the
association between deficiencies of components of the
complement system and autoimmune diseases. The
majorities of these focus on the inadequate clearance of IC
in presence of reduced levels of complement system’s
components [26]. An excess of IC may deposit in the tis-
sues, resulting in inflammatory damage and release of
autoantigens that trigger an autoimmune response. Alter-
natively, the presence of high concentration of apoptotic
cells (AC) due to poor clearance may be sufficient to elicit
an autoimmune response [27].
In particular, among complement proteins, a primary
role in clearance activity is attributed to the first component
of the complement C1q. This can directly and indirectly
opsonize apoptotic cells for phagocytosis by macrophages.
It can directly bind AC and mediate AC phagocytosis
through CD91 or LRP-1 (low-density lipoprotein receptor–
related protein 1) on macrophages. It can also bind indi-
rectly, through CRP and IgM, to cause complement acti-
vation and C3 deposition [28, 29].
A third hypothesis suggests that the complement system
favors the development of tolerance against self [30].
The complement system is needed for the elimination of
self-reactive lymphocytes during maturation of the immune
system. Hence, deficiencies of the complement system
result in lack of normal B cell tolerance and production of
autoantibodies [31, 32].
Moreover, recent data seem to demonstrate that com-
plement system’s proteins, in particular C1q, act as a strong
signal for dendritic cells (DCs) [33]. Mature DCs are the
most powerful antigen-presenting cells (APCs) able to
induce and direct the differentiation of naive T cells.
Depending on the maturation signal and the cytokine
environment, DCs may stimulate CD4? helper, CD8?
cytotoxic or regulatory T cells, inducing tolerance. C1q
plays an important role in the initiation of DCs maturation
and induction of cytokine production, suggesting that, in
the absence of this complement system’s protein, DC
functions might be impaired. Therefore, C1q-containing IC
and C1q-opsonized apoptotic cells and pathogens most
probably play a role in both the induction and regulation of
immunity and autoimmunity [33]. Benoit et al. have
recently identified specific molecular pathways induced by
C1q. They demonstrated that C1q bounds to autologous
apoptotic lymphocytes modulating the expression of genes
associated with JAK/STAT signaling, chemotaxis, immu-
noregulation, and NLRP3 inflammasome activation in
LPS-stimulated human monocyte-derived macrophages.
480 Diagnosis of Autoimmunity (2013) 56:477–491
123

These results underline the role of C1q in suppressing
macrophage induced inflammation as well as providing
potential therapeutic targets to control macrophage polar-
ization and thus inflammation and autoimmune reactions
[34]. The protective role of the complement system from
autoimmune conditions is also expressed by the role of
complement receptors 1 (CR1) and 2 (CR2), the defect of
which has been associated with increased susceptibility to
autoimmune diseases [26]. These receptors, found on
erythrocytes, hematopoietic cells, follicular dendritic cells,
and B cells, are capable of binding C3 activation frag-
ments. CR2 binds C3d and iC3b. It has been demonstrated
that CR2 is able to amplify antigen-induced B cell acti-
vation through surface IgM (sIgM), to rescue peripheral B
cells from sIgM-mediated apoptosis, to promote antigen
processing and presentation of C3d-bound targets, to
modulate the expression of costimulatory molecules, to
stabilize the B cell receptor in lipid rafts, and to target IC to
germinal centers in secondary lymphoid organs [26]. Many
of these functions may occur via interactions of CR2 with
CD19 and CD81 on the B cell surface, where these
receptors form a multi-molecular signal transduction
complex.
Whereas the role as an activating receptor of CR2 is
better defined, the exact function of CR1 on B cells is yet to
be determined [35]. CR1 binds the C3b and with lower
affinity, iC3b and C4b, and it is capable of transmitting
both activating and inhibitory signals to human B cells.
Expression of CR2 and CR1 on human B cells has been
studied in some human autoimmune diseases. It was
observed that patients with SLE had abnormalities in the
expression of both CR2 and CR1 on B lymphocytes.
Peripheral B cells showed a marked decrease in both CR2
and CRl density when compared to control subjects [27,
36]. RA patients also had fewer CR1- and CR2-positive B
cells and decreased receptor expression compared to
healthy subjects [37, 38].
Complement system and autoimmune diseases
Systemic lupus erythematosus
SLE is the prototype of a multi-organ autoimmune disease.
As found in several other autoimmune disorders, SLE path-
ogenesis is multifactorial lying on genetic and environmental
factors and on abnormalities of both the innate and the
adaptive immune system [39]. The role of the complement
system in the pathogenesis of SLE is apparently paradoxical.
On the one hand, active SLE is accompanied by the activation
of the complement pathway, and there is evidence that the
complement system contributes to inflammatory tissue
damage. On the other hand, patients with hereditary
deficiencies of complement proteins of the classical pathway
are at increased risk for SLE, suggesting the protective role of
complement system’s proteins [5]. Hereditary homozygous
deficiencies of C1q, C1r and C1s (whose defect is usually
inherited together), and C4 are each strongly associated with
susceptibility to SLE, with frequencies of 93, 57, and 75 %,
respectively [5]. In contrast, 10 % of the subjects with C2
deficiency, the most frequent hereditary deficiency of the
complement system’s classical pathway, develop SLE [27].
The hypothesis invoked to explain the involvement of the
complement system in the pathogenesis of SLE is known as
the ‘‘waste-disposal’’ hypothesis [40]. According to this
hypothesis, complement system’s proteins play a role in
clearing IC and apoptotic cells from both tissues and circu-
lation. Failing this activity of the complement system, waste
material—consisting of partially degraded components of
the cytoplasm and nucleus—could accumulate and elicit an
autoimmune response. The ‘‘waste-disposal’’ hypothesis
envisages the following steps. The first step is the failure to
clear autoantigens [5]. The second step is the uptake of
autoantigen by immature dendritic cells in the presence of
inflammatory cytokines, which causes these cells to mature
into APCs, allowing the presentation of autoantigens to T
cells [5]. The third step is the provision of help by T cells to
autoreactive B cells, which have taken up autoantigen by
means of their immunoglobulin receptors. Such B cells
mature into plasma cells that secrete autoantibodies [2].
SLE-like disease associated with complement system’s
deficiencies clinically differs from SLE disease without
complement system’s deficiencies. In patients with SLE-
like disease and complement system’s deficiency, the onset
is at a younger age; renal, pulmonary, and pericardial
involvement are less conspicuous, but annular photosensi-
tive skin rashes are more prominent. Fulminant glomeru-
lonephritis, progressive nephritis, and renal failure are also
far less common in patients with SLE-like disease and
complement system’s deficiency. Antinuclear antibodies,
anti-DNA antibodies are usually relatively low or absent in
patients with SLE-like disease, whereas anti-Ro (SSA)
antibodies are often elevated [24].
The severity of SLE-like disease varies according to the
position of the missing component within the classical
pathway of activation (C1 [ C4 [ C2) [41]. Inherited
deficiencies of C1q and C4 are invariably associated with
the development of a severe SLE-like disease early in life,
while C2 deficiency is only weakly associated with a
milder form of SLE [41].
In the case of C3 deficiency, the clinical picture is rather
different [5]. It is characterized by recurrent pyogenic
infections, membranoproliferative glomerulonephritis,
rashes and it is rarely associated with SLE.
The initial cause of complement activation in SLE is
thought to be the formation of high levels of IC that
Diagnosis of Autoimmunity (2013) 56:477–491 481
123

activate complement via the classical pathway [40]. Key
mediators of tissue damage induced by the complement
system are the anaphylatoxins (C3a and C5a) and MAC.
Histologic data indicate that the activation of the comple-
ment system substantially contributes to tissues damages in
patients with SLE. Deposits of C3, C4, and associated
complement fragments are easily detected in biopsies of
inflamed tissues from patients with SLE [42]. In these
patients, the MAC is localized in the basement membrane
zone of cutaneous lesions and, compared with clinically
normal tissues, more prominent MAC deposits have been
observed in inflamed tissues [43].
Immunofluorescence studies in SLE patients have
shown deposits of immunoglobulins and complement in
renal glomeruli and vessels in spleen, heart, skin, and liver
[44, 45]. There is evidence that in SLE nephritis, the
activation of the complement system is triggered by the
deposition of IC in the glomerulus, either through the blood
flow or by in situ formation [44, 45].
In patients with active SLE, low complement concentra-
tions and activation of the complement system are charac-
teristic findings and are routinely evaluated for diagnostic
and disease monitoring purposes [17]. They can be consid-
ered conventional biomarkers for disease activity [46].
In vivo complement activation can be demonstrated by
tests for complexes or split products formed during the
activation of the complement system. Several studies have
shown that such measurements are more sensitive than
regular measurement of CH50 or complement native
components, such as C1q, C4, and C3, to verify comple-
ment activation and disease activity [17].
In addition to the previously mentioned reduced expres-
sion of complement receptors on B cells in SLE patients [47,
48], these are also reduced on erythrocytes. On red blood
cells, CR1 acts as a binding molecule for particles carrying
C3b clusters (for example parasites and bacteria) further
transporting them to the fixed mononuclear phagocytic
system in the liver, spleen, and bone marrow [47]. There is
evidence that reduction in CR1 levels on erythrocytes cor-
relates with disease activity in SLE [48].
Approximately a third of patients with SLE show ele-
vated levels of anti-C1q antibodies. Experimental models
seem to demonstrate that they are directed against a neo-
epitope of C1q not expressed in the intact C1q complex
[47]. These autoantibodies are associated with severe dis-
ease, with occurrence of glomerulonephritis and with
intense activation of classical pathway [47].
Rheumatoid arthritis
To date, the pathogenesis of RA is not fully understood but
there is increasing evidence of the role played by compo-
nents of the complement system’s cascade [49]. Animal
models suggest that the immunization with type II collagen
(CII), the major constituent protein of cartilage in diar-
throdial joints, induces autoimmune arthritis resembling
RA (collagen-induced arthritis or CIA) [50–53]. C3 or
factor B deficient mice immunized with bovine CII showed
reduction or complete remission of clinical or histologic
signs of arthritis [54]. Moreover, the systemic administra-
tion of anti-C5 monoclonal antibody (mAb) prevented the
onset of arthritis and improved established disease [55].
While increased complement system activation is plau-
sibly related to the onset and/or augmentation of inflam-
mation in RA, complement system’s deficiencies may also
induce RA. In particular, C1q and C2 deficiency are cor-
related with the development of RA [56, 57].
The plasma levels of most of the complement system’s
components are maintained by hepatic synthesis. We
evaluated plasma levels of complement system’s compo-
nents in 114 patients with active RA. Mean C3 and C4
plasma levels observed in patients with active RA were
significantly higher than in controls. This finding is con-
sistent with the presence of an underlining inflammatory
process [58] and confirms that complement system’s pro-
teins may act as acute phase proteins, with increased
hepatocyte synthesis occurring in response to inflammatory
cytokines [59–62].
However, it has to be noted that the synthesis of com-
plement system’s components also occurs in extrahepatic
sites and in chronically inflamed tissues such as the rheu-
matoid joint [63–66]. Synovial membrane cells which seem
to be responsible for the synthesis of complement system’s
components include lining cells, fibroblasts, mononuclear
phagocytes, and endothelial cells [67].
Evidence of complement system activation in the
synovial fluid is abundant. Levels of complement proteins
are generally depressed in the synovial fluid of patients
with RA, reflecting consumption of complement. More-
over, elevated levels of several complement cleavage
products, such as C3a, C3c, C5a, sC5b-9, Bb, C1-C1INH
complexes, have been observed in the synovial fluid [68–
71]. Some studies demonstrated low levels of MAC
inhibitors in synovial fluid and tissue of RA patients. This
observation might justify lytic or sublytic attacks on local
cells [70, 72].
Several mechanisms of complement system activation
have been proposed in RA patients. RA patients have
increased levels of circulating IC [73, 74], also including
rheumatoid factors (RFs), and they can activate the clas-
sical pathway of the complement system [75–78].
Although the activation of the classical pathway is pre-
dominant [79], the alternative pathway is also activated in
RA synovium as demonstrated by decreased levels of
factor B and properdin and increased levels of Ba in the
synovial fluid [80]. Increased complement activation via
482 Diagnosis of Autoimmunity (2013) 56:477–491
123

the lectin pathway could also play a role in RA. Changes in
IgG glycosylation cause an increase in binding of MBL
resulting in increased complement activation [81].
Trouw et al. [82], from in vitro observations, suggested
that anti-cyclic citrullinated peptide/protein antibodies
(anti-CCP) from RA patients may activate complement via
both the classical and the alternative pathways. Another
potential trigger for complement system activation in RA
patients could be CRP, since this acute phase protein can
activate the complement system both in vitro and in vivo
[83–87]. Furthermore, it appears that molecules present in
or released from cartilage, such as fibromodulin (FM), may
have a role in activating the complement system by inter-
acting with the globular head of C1q [88]. Several studies
failed to demonstrate a correlation between local and sys-
temic activation of the complement system in RA and
reported higher levels of complement cleavage products in
synovial fluid than in plasma [68, 89, 90]. These findings
are consistent with a prevalent local activation of the
complement system’s cascade. It has to be noted the pos-
sible association between the activation of the complement
system and disease activity. Some authors reported a cor-
relation between levels of complement system’s cleavage
products and disease activity in RA patients [68, 91].
Other inflammatory arthritides
There is limited availability of data in literature about role
of complement system’s proteins in other inflammatory
arthritides.
Studies conducted in psoriatic patients have shown
increased plasma concentrations of iC3b, C4d, and Bb
fragments, especially in patients with erythrodermic pus-
tular psoriasis and psoriatic arthritis (PsA) [92]. Partsch
et al. [93] have reported relatively low levels of the C3c
cleavage product in synovial fluid from PsA patients,
similar to that observed in patients with osteoarthritis.
A possible implication of complement activation in the
pathogenesis of PsA is supported by the finding of impaired
expression of complement regulators in these patients.
Triolo et al. [94] reported low expression of erythrocyte
membrane-anchored CD59, an important membrane
inhibitor of MAC. In keeping with this observation,
increased SC5b-9 plasma levels were detected in patients
with active disease and an inverse correlation was also
found between SC5b-9 plasma levels and CD59 expression
levels [94]. Rivas et al. found a statistically significant
decrease in CR1 density on erythrocyte membranes in PsA
patients with polyarthritis compared to controls. An inverse
correlation between CRl concentration and the articular
index of PsA patients has been reported, and this finding is
suggestive of a correlation between CRl levels and disease
severity in PsA patients [95].
Our group has recently conducted a study evaluating the
complement system in PsA treated with anti-tumor necro-
sis factor agents that demonstrated that moderate to severe
PsA disease is associated with higher C3 and C4 plasma
levels with respect to healthy subjects [96]. This finding is
compatible with the involvement of complement system’s
proteins during the acute phase response [97].
Systemic sclerosis
SSc is a chronic multi-system autoimmune disease that is
clinically highly heterogeneous. The two widely recog-
nized subsets of SSc are limited cutaneous and diffuse
cutaneous SSc. The disease affects the skin and multiple
internal organs leading, eventually, to fibrosis.
Although many studies have been conducted to inves-
tigate its pathogenesis, this is not fully understood and,
although the role of the complement system has been
investigated, no definitive conclusions can be drawn.
Reduced complement levels in SSc patients were first
observed in 1967 [98]. Senaldi et al. subsequently dem-
onstrated higher level of complement fragments in patients
with SSc, in particular those with diffuse cutaneous SSc,
with respect to controls. They postulated a direct correla-
tion between the complement system activation and clini-
cal severity [99]. In the light of these findings, low C3
levels were identified as candidate parameter for inclusion
in the American College of Rheumatology (ACR) classi-
fication criteria for SSc [100]. In 2001, hypocomplemen-
temia was included among the parameters used to assess
the disease activity score by the European Scleroderma
Study Group [101].
More recently Hudson et al. studied a cohort of 321
patients with SSc. It was observed that there was no dif-
ference in the clinical presentation of the disease between
patients with normal or low complement levels [102].
However, hypocomplementemia was associated with fea-
tures of overlap disease. In particular, inflammatory myo-
sitis and vasculitis were more frequent in patients with low
levels of complement system’s proteins compared to
patients with normal values [102]. Further studies are
needed to assess the role of the complement systems in the
pathogenesis of SSc.
Antiphospholipid antibodies syndrome
APS is characterized by thrombosis, recurrent miscarriage,
and pregnancy complications in the presence of anti-
phospholipid (aPL) antibodies. The pathogenic mecha-
nisms underlying aPL antibodies induced thrombosis are
not completely understood. It is well established that
activated complement fragments themselves have the
capacity to bind and activate inflammatory and endothelial
Diagnosis of Autoimmunity (2013) 56:477–491 483
123

cells as well as to induce a prothrombotic phenotype, either
through the MAC directly or through C5a receptor (CD88)-
mediated effects [103, 104].
To better understand these mechanisms, several murine
models have been developed. A study focused on APS
induced by passive transfer of human aPL-IgG antibodies has
demonstrated that complement blockade at the point of C3
activation prevents fetal loss and growth retardation [105].
Girardi et al. reported that, in a murine model, the
activation of the complement system’s cascade by the IC is
required for APS development. The model provided con-
vincing evidence that the activation of both classical and
alternative pathways is needed to generate sufficient C5
cleavage to cause fetal loss [106].
Recent experiments in mice have underscored the
importance of fetal regulation mechanisms to modulate
potentially damaging maternal immune responses derived
from the activation of the complement system. These
studies have focused on complement receptor 1–related
gene/protein y (Crry), a membrane-bound intrinsic com-
plement regulatory protein that blocks C3 and C4 activa-
tion on self-membranes in mice [107]. Adequate
complement system inhibition is essential for a normal
pregnancy, and this is demonstrated by the finding that
Crry deficiency in utero progressively leads to embryonic
death [108].
Moreover, studies performed in rats showed that CD59,
an inhibitor of C5b-9 assembly and insertion, protects
against thrombotic microangiopathy, demonstrating that
C5b-9 plays a critical role in the pathogenesis of throm-
bosis [109].
Interestingly, Pierangeli et al. found that mice deficient in
complement components C3 and C5 were resistant to
thrombosis and endothelial cell activation induced by aPL
antibodies. Furthermore, inhibition of C5 activation using
anti-C5 mAb prevented thrombophilia induced by aPL
antibodies. They showed that the activation of the comple-
ment system mediates two important effects of aPL anti-
bodies: induction of thrombosis and endothelial activation
[110]. Holers et al. [105] found that a C3 convertase inhibitor
can prevent fetal loss and growth restriction, and that mice
deficient in complement C3 are resistant to fetal injury
induced by aPL antibodies. Finally, Salmon and Girardi
explained pregnancy loss during APS as an inflammatory
disorder. They found that aPL antibodies targeted to decidual
tissues interfere with pregnancy by engaging the classical
pathway of complement system activation, followed by
amplification through the alternative pathway. Considering
the evidence that heparin inhibits the activation of the
complement system in vitro, it was postulated that heparin
may prevents pregnancy loss by inhibiting complement
activation on trophoblasts [111]. A recent study on humans
demonstrated that the activation of the complement system
also contributes to the development of APS in humans. It was
found that serum complement levels were significantly lower
in patients with primary APS than in patients with APS
secondary to non-SLE connective tissue diseases. Patients
with APS had significantly higher levels of C3a or C4a than
healthy controls, suggesting complement consumption
[112]. These studies highlight the importance of developing
and testing targeted complement inhibitory therapy for
patients with APS.
Inflammatory myopathies
Inflammatory myopathies can be differentiated into three
groups: dermatomyositis (DM), polymyositis, and inclu-
sion body myositis. There is increasing evidence that
complement-mediated microangiopathy plays a pathogenic
role in DM [113].
The primary antigenic target in DM is the endothelium
of the endomysial capillaries. Putative antibodies directed
against endothelial cells activate C3 [114]. In its turn,
activated C3 leads to formation of C3b and C4b fragments
and MAC, which can be detected early in the course of the
disease both in serum and in the capillaries before
inflammatory or structural changes are observed in the
muscular tissue [114]. Capillary complement deposits
induce swollen endothelial cells, vacuolization, capillary
necrosis, perivascular inflammation, ischemia, and
destruction of muscle fibers [114]. The characteristic
perifascicular atrophy reflects endofascicular hypoperfu-
sion, more prominent distally. In the later stage of the
diseases, a striking reduction in the number of capillaries
per muscle fiber associated with compensatory dilatation of
the lumen of the remaining capillaries is observed. Cyto-
kines and chemokines related to the activation of the
complement system are released. Cytokines and chemo-
kines upregulate vascular cell adhesion molecule (VCAM-
1) and intercellular adhesion molecule (ICAM-1) on the
endothelial cells and facilitate the egress of activated T
cells to the perimysial and endomysial spaces [114].
Muscle biopsy in DM reveals the deposition of the MAC
on endothelial cells [115]. Moreover, the deposition of
MAC was found in a high proportion of biopsies from skin
lesions of DM patients and was absent in unaffected skin,
suggesting that the complement system is also involved in
the pathogenesis of skin lesions [116]. The immunopath-
ologic mechanism associated with polymyositis and
inclusion body myositis is driven by CD8-positive cells and
to a lesser extent by the complement system.
Sjogren’s syndrome
SS is a chronic autoimmune disorder of the exocrine glands
with associated lymphocytic infiltrates of the affected
484 Diagnosis of Autoimmunity (2013) 56:477–491
123

glands. Dryness of the mouth and eyes results from the
involvement of the salivary and lacrimal glands [117].
SS occurs in a primary form not associated with other
diseases and in a secondary form that complicates other
rheumatic conditions.
In patients with primary SS, there is growing interest in
determining the negative prognostic significance of low
complement levels. The prevalence of hypocomplemente-
mia in SS patients has been evaluated in several studies.
Skopouli et al. [118] detected low C3 levels in 4 (2 %) and
low C4 levels in 44 (17 %) of 261 Greek patients, while Io-
annidis et al. [119] found low C3 in 17 (3 %) and low C4 in 122
(20 %) of 601 Greek patients in a multicenter study. Recently,
Theander et al. [120] reported low C3 levels in 98 (25 %) and
low C4 levels in 105 (27 %) of 386 Swedish patients. Ramos-
Casals et al. [121] observed low C3 values in 42 (12 %), low
C4 values in 39 (12 %), and low CH50 in 51 (15 %) of 336
Spanish patients. In the latter study, patients with SS and HCV
infection presented a higher frequency of hypocomplemente-
mia with respect to patients with primary SS, 76 and 24 %,
respectively. The proportion was even higher (78 %) in patient
with SS and HCV-related cryoglobulinemia.
Low complement levels seem to be associated with
systemic SS features, including extraglandular features
(fever, articular and cutaneous involvement, vasculitis and
peripheral neuropathy) and immunological markers (cryo-
globulinemia, RF) [121]. Hypocomplementemia is also a
marker of unfavorable outcomes in primary SS because it
is associated with lymphoma development and death. In
particular, low C4 levels showed the closest statistical
association with mortality and lymphoproliferation [119–
121]. These results support the inclusion of complement
level determination as a predictor of SS outcome both at
diagnosis and routinely during the clinical follow-up.
Vasculitides
Vasculitides are defined by the presence of leukocytes in
the vessel wall with reactive damage. Depending on the
specific vasculitic disorder, affected vessels vary in size,
type, and location. Many vasculitic disorders are caused by
IC, and the activation of the complement system is
involved in their pathogenesis. In particular, complement
involvement was demonstrated in small vessel vasculitides,
as described in the next paragraphs, but complement-
dependent cytotoxicity against endothelial cells has been
implicated in large vessel vasculitides too, such as Taka-
yasu’s arteritis [122].
ANCA-associated vasculitides
The anti-neutrophil cytoplasmic autoantibody (ANCA)-
associated vasculitides (AAVs) include Wegener’s
granulomatosis, microscopic polyangiitis, Churg–Strauss
syndrome, ‘‘renal-limited’’ vasculitis and certain drug-
induced vasculitis syndromes [123]. These small vessel
vasculitides are characterized by necrotizing inflammation
of the vessel wall, particularly of small arteries, arterioles,
capillaries, and venules, in conjunction with the presence
of ANCAs. In AAV, ANCAs are directed against pro-
teinase 3 (PR3) or to myeloperoxidase (MPO).
In AAVs, the adaptive immune response, expressed by
the ANCAs, interacts with innate immunity, in particular
with neutrophils and the complement system. Together
they target the endothelium, resulting in necrotizing vas-
culitis [124].
In vitro data demonstrate that in AAVs, the complement
system constitutes an amplification loop for ANCA-
induced neutrophil activation. Schreiber et al. [125]
showed that supernatants from ANCA-activated neutro-
phils activate the complement system via the alternative
pathway, resulting in the production, among others, of C5a.
C5a was able to prime neutrophils for ANCA-induced
activation, and blocking of the C5a receptor on neutrophils
abrogated this process.
Murine models have shown that complement depletion
prevented MPO-ANCA glomerulonephritis and mice defi-
cient in C5 or complement factor B did not develop pauci-
immune necrotizing crescentic glomerulonephritis
(NCGN) [126]. In agreement with these experimental data,
the complement components MAC, C3d, and factor B
could be detected in diseased glomeruli of patients with
AAVs. The alternative pathway component factor B
colocalized with MAC, but the classical pathway compo-
nent C4d could not be detected [127]. According to these
findings, compounds interfering with the complement
cascade should be explored as therapeutic options for
ANCA-associated vasculitides.
Cryoglobulinemia
Cryoglobulins (CG) are an abnormal group of serum pro-
teins that share the common property of reversible pre-
cipitation at low temperatures. It is widely accepted that the
majority of CG are either intact monoclonal immuno-
globulins or IC in which one component, usually IgM,
exhibits antibody activity to IgG. The latter are known as
mixed CG [128].
Monoclonal CG are usually associated with hemato-
logical disorders, whereas mixed CG are found in many
infectious and systemic disorders. Essential mixed cryo-
globulinemia shows a striking association with hepatitis C
virus infection ([90 %). It is a systemic vasculitis (leuk-
ocytoclastic vasculitis) affecting cutaneous vessels and
multiple visceral organs [129]. The classical pathway of the
complement system is usually activated in both essential
Diagnosis of Autoimmunity (2013) 56:477–491 485
123

and secondary cryoglobulinemia. Decreased C4 and C2
levels are observed together with slightly altered C3 levels.
Late complement components are also insignificantly
affected, although modest elevations have been reported.
Diminished serum levels of complement components may
reflect ongoing consumption by CG-containing IC [130,
131].
Henoch-Schonlein purpura/IgA nephropathy
Henoch-Schonlein purpura nephritis (HSPN) and IgA
nephropathy (IgAN) are currently considered related dis-
eases. Both diseases display similar histologic features and
IgA abnormalities. The common clinical pattern of IgAN is
an indolent progressive disease with slowly increasing
proteinuria and loss of the renal function associated with
episodes of macroscopic hematuria in half of the patients.
In the majority of patients, HSPN is characterized by acute
onset followed by full recovery [132]. The activation of the
complement pathway is likely to be involved in the path-
ophysiology of glomerular lesions. Glomerular deposition
of MBL, L-ficolin, MASP, C4d are reported in the vast
majority of patients with HSPN and IgAN. These findings,
together with the absence C1q, support the predominant
activation of the lectin pathways of the complement system
as pathophysiological mechanism [133]. The deposition of
complement fragments, derived from the activation of the
lectin pathway, has been shown to be associated with a
higher degree of proteinuria and hematuria as well as with
more severe histologic lesions in both HSPN and IgAN
patients [134, 135]. These findings emphasize the need for
further studies to assess the potential significance of the
measurement of blood and urinary complement splits
products and MAC to evaluate the disease activity.
Potential therapies targeting complement cascade
in autoimmune disease
The complement system is increasingly recognized to have
a causal link with tissue damage during ischemic, inflam-
matory, and autoimmune diseases. This makes the com-
plement system an attractive target for the treatment of a
wide range of diseases, such as connective tissue diseases,
glomerulonephritis, myocarditis, multiple sclerosis, type I
diabetes mellitus, asthma, myocardial infarction, paroxys-
mal nocturnal hemoglobinuria, vasculitis, and many others
[14, 15, 136–138].
An issue that deserves further consideration is the side
effects potentially associated with the modulation of
complement system’s activity in the long term. Prolonged
systemic suppression may, for instance, increase the sus-
ceptibility to bacterial infections [56].
Several compounds interfering with complement system
cascade have been studied in experimental models for
autoimmune diseases. The main therapeutic strategies are
inhibition of complement activation components, inhibition
of complement receptors, and inhibition of MAC [136].
Different molecules believed to have complement modu-
lation properties have been studied in several animal
models for arthritis. These include soluble CR1 [139] (that
suppresses complement system activation at the main
gathering point C3), C3a [140], and C5a [141] receptor
antagonists (that can be used to control the anaphylatoxins
C3a and C5a), recombinant CD59 [142] (that inhibits the
formation of MAC). Although PMX53, a C5a mimetic
compound that binds the C5a receptor, has shown
encouraging results in rats, where a significant improve-
ment of arthritis was observed with no side effect [141], its
use in RA patients did not fill the expectation [143].
The involvement of the complement system in the
pathogenesis of SLE was proven by the findings that an
inhibitory anti-C5 mAb blocks the development of glo-
merulonephritis in the (NZB 9 NZW)F1 animal model for
SLE [144], that fB_/_ MRL/lpr mice are protected from
renal disease [145], and that mice in which C3 activation
was blocked using transgenic expression of soluble Crry
[146] or recombinant Crry (a Fc fusion protein designated
Crry-Ig) [147] did not develop glomerulonephritis. Two
complement inhibitors, soluble complement receptor 1
(TP10), and a monoclonal anti-C5 antibody (Eculizumab),
have been shown to inhibit complement safely and promise
to be used therapeutically in lupus nephritis [148].
Additional animal models have assessed the comple-
ment system as potential therapeutic target for autoimmune
diseases, such as APS, PM/DM, autoimmune myocarditis,
multiple sclerosis, type 1 diabetes mellitus, asthma [136].
However, these did not translate into viable treatment
options for autoimmune diseases in humans.
Only two complement modulators have been approved
for use in human. Eculizumab binds to the complement
protein C5 inhibiting its cleavage and is indicated for the
treatment for paroxysmal nocturnal hemoglobinuria [149].
Plasma-derived C1 esterase inhibitor is indicated for the
treatment for hereditary angioedema [150].
An additional strategy to be considered is the replace-
ment of missing complement system’s proteins, to reverse
the effects of complement deficiencies. However, this
approach presents several potential drawbacks. Indeed,
purified or engineered complement proteins are not avail-
able for treatment purposes, and whole plasma preparations
would have to be used, with obvious complications of
plasma treatment. Secondly, the replacement of a missing
complement protein may be followed by complement
activation and tissue damage. Finally, exposure to a protein
that is genetically deficient may cause development of
486 Diagnosis of Autoimmunity (2013) 56:477–491
123

antibodies. At present, only anecdotal observations have
been reported [47]. The modulation of the complement
system is one of the benefits associated with the use of high
dose intravenous immunoglobulins (IVIg) in autoimmune
conditions. The complement systems modulating effect
exhibited by IVIg can be explained by several mechanisms.
First, activated C3 and C4 may bind to immunoglobulin
molecules, which then serve as scavengers, hence avoiding
in situ deposition of these fragments [151]. Furthermore,
C1q may bind to immunoglobulin leading to a deviation of
C1 binding from its target to the IVIg [151]. Third, IVIg
may enhance the inactivation of C3 in complex with
immunoglobulins and thus down-regulate the C3 conver-
tase activity [150]. Finally, IVIg are able to cause a mild
and controlled activation of the complement system. This
is not harmful per se, and it may reduce a pathological
activation observed in the pathogenesis of autoimmune
disease [151]. A broadly applicable anti-C therapeutic
agent, useful in acute and chronic conditions, should be
inexpensive, highly specific, either have a very long plasma
half-life or be active orally and be able to block the path-
ological activation of the complement system while caus-
ing minimal disruption of the systemic complement
function [152]. None of the currently available agents
satisfy these requirements, but data derived from preclini-
cal studies and initial clinical trials suggest that comple-
ment modulation could become an important therapeutic
strategy in autoimmune conditions in the next decades.
References
1. Moffitt MC, Frank MM. Complement resistance in microbes.
Springer Semin Immunopathol. 1994;15:327–44.
2. Morgan BP, Marchbank KJ, Longhi MP, Harris CL, Gallimore
AM. Complement: central to innate immunity and bridging to
adaptive responses. Immunol Lett. 2005;97:171–9.
3. Walport MJ. Complement. First of two parts. N Engl J Med.
2001;344:1058–66.
4. Hawlisch H, Kohl J. Complement and toll-like receptors: key
regulators of adaptive immune responses. Mol Immunol.
2006;43:13–21.
5. Walport MJ. Complement. Second of two parts. N Engl J Med.
2001;344:1140–4.
6. Nauta AJ, Castellano G, Xu W, Woltman AM, Borrias MC,
Daha MR, et al. Opsonization with C1q and mannose-binding
lectin targets apoptotic cells to dendritic cells. J Immunol.
2004;173:3044–50.
7. Gal P, Dobo J, Zavodszky P, Sim RB. Early complement pro-
teases: C1r, C1s and MASPs. A structural insight into activation
and functions. Mol Immunol. 2009;46:2745–52.
8. Rus H, Cudrici C, Niculescu F. The role of the complement
system in innate immunity. Immunol Res. 2005;33:103–12.
9. Liszewski MK, Farries TC, Lublin DM, Rooney IA, Atkinson
JP. Control of the complement system. Adv Immunol. 1996;61:
201–83.
10. Lindahl G, Sjobring U, Johnsson E. Human complement regu-
lators: a major target for pathogenic microorganisms. Curr Opin
Immunol. 2000;12:44–51.
11. Davis AE. The pathophysiology of hereditary angioedema. Clin
Immunol. 2005;114:3–9.
12. Boccuni P, Del Vecchio L, Di Noto R, Rotoli B. Glycosyl
phosphatidylinositol (GPI)-anchored molecules and the patho-
genesis of paroxysmal nocturnal hemoglobinuria. Crit Rev
Oncol Hematol. 2000;33:25–43.
13. Nauta AJ, Roos A, Daha MR. A regulatory role for complement
in innate immunity and autoimmunity. Int Arch Allergy
Immunol. 2004;134:310–23.
14. Theroux P, Martel C. Complement activity and pharmacological
inhibition in cardiovascular disease. Can J Cardiol. 2006;
22(Suppl B):18B–24B.
15. Rother KO, Till GO, Hansch GM. The complement system. 2nd
ed. Berlin: Springer; 1998.
16. Kabat EA, Mayer MM. Experimental Immunochemistry. 2nd
ed. Springfield, IL: Thomas; 1961.
17. Sturfelt G, Truedsson L. Complement and its breakdown prod-
ucts in SLE. Rheumatology. 2005;44:1227–32.
18. Oppermann M, Baumgarten H, Brandt E, Gottsleben W, Kurts
C, Gotze O. Quantitation of components of the alternative
pathway of complement (APC) by enzyme-linked immunosor-
bent assays. J Immunol Methods. 1990;133:181–90.
19. Klos A, Ihrig V, Messner M, Grabbe J, Bitter-Suermann D.
Detection of native human complement components C3 and C5
and their primary activation peptides C3a and C5a (anaphyla-
toxic peptides) by ELISAs with monoclonal antibodies.
J Immunol Methods. 1988;111:241–52.
20. Seino J, Warmold A, Wall Bake Lvd, van Es LA, Daha MR. A
novel ELISA assay for the detection of C3 nephritic factor.
J Immunol Methods. 1993;159:221–7.
21. Shoenfeld Y, Gershwin ME, Meroni PL. Autoantibodies. 2nd
ed. Amsterdam: Elsevier; 2007.
22. Thurman JM, Rohrer B. Noninvasive detection of complement
activation through radiologic imaging. Adv Exp Med Biol.
2013;734:271–82.
23. Chen M, Daha MR, Kallenberg CG. The complement system in
systemic autoimmune disease. J Autoimmun. 2010;34:J276–86.
24. Pettigrew HD, Teuber SS, Gershwin ME. Clinical significance
of complement deficiencies. Ann N Y Acad Sci. 2009;
1173:108–23.
25. Etzioni A. Immune deficiency and autoimmunity. Autoimmun
Rev. 2003;2:364–9.
26. Boackle SA. Complement and autoimmunity. Biomed Phar-
macother. 2003;57:269–73.
27. Bussone G, Mouthon L. Autoimmune manifestations in primary
immune deficiencies. Autoimmun Rev. 2009;8:332–6.
28. Pittoni V, Valesini G. The clearance of apoptotic cells: impli-
cations for autoimmunity. Autoimmun Rev. 2002;1:154–61.
29. Lu JH, Teh BK, Wang L, Wang YN, Tan YS, Lai MC, et al. The
classical and regulatory functions of C1q in immunity and
autoimmunity. Cell Mol Immunol. 2008;5:9–21.
30. Carroll MC. The role of complement in B cell activation and
tolerance. Adv Immunol. 2000;74:61–88.
31. Truedsson L, Bengtsson AA, Sturfelt G. Complement deficien-
cies and systemic lupus erythematosus. Autoimmunity. 2007;40:
560–6.
32. Munoz LE, Janko C, Schulze C, Schorn C, Sarter K, Schett G,
et al. Autoimmunity and chronic inflammation—two clearance-
related steps in the etiopathogenesis of SLE. Autoimmun Rev.
2010;10:38–42.
33. Csomor E, Bajtay Z, Sandor N, Kristof K, Arlaud GJ, Thiel S,
et al. Complement protein C1q induces maturation of human
dendritic cells. Mol Immunol. 2007;44:3389–97.
Diagnosis of Autoimmunity (2013) 56:477–491 487
123

34. Benoit ME, Clarke EV, Morgado P, Fraser DA, Tenner AJ.
Complement protein C1q directs macrophage polarization and
limits inflammasome activity during the uptake of apoptotic
cells. J Immunol. 2012;188:5682–93.
35. Erdei A, Isaak A, Torok K, Sandor N, Kremlitzka M, Prechl J,
et al. Expression and role of CR1 and CR2 on B and T lym-
phocytes under physiological and autoimmune conditions. Mol
Immunol. 2009;46:2767–73.
36. Marquart HV, Svendsen A, Rasmussen JM, Nielsen CH, Junker
P, Svehag SE, et al. Complement receptor expression and acti-
vation of the complement cascade on B lymphocytes from
patients with systemic lupus erythematosus (SLE). Clin Exp
Immunol. 1995;101:60–5.
37. Wilson JG, Ratnoff WD, Schur PH, Fearon DT. Decreased
expression of the C3b/C4b receptor (CR1) and the C3d receptor
(CR2) on B lymphocytes and of CR1 on neutrophils of patients
with systemic lupus erythematosus. Arthritis Rheum. 1986;29:
739–47.
38. Prokopec KE, Rhodiner M, Matt P, Lindqvist U, Kleinau S.
Down regulation of Fc and complement receptors on B cells in
rheumatoid arthritis. Clin Immunol. 2010;137:322–9.
39. Gualtierotti R, Biggioggero M, Penatti AE, Meroni PL. Updat-
ing on the pathogenesis of systemic lupus erythematosus.
Autoimmun Rev. 2010;10:3–7.
40. Manderson AP, Botto M, Walport MJ. The role of complement
in the development of systemic lupus erythematosus. Annu Rev
Immunol. 2004;22:431–56.
41. Pickering MC, Botto M, Taylor PR, Lachmann PJ, Walport MJ.
Systemic lupus erythematosus, complement deficiency and
apoptosis. Adv Immunol. 2000;76:227–324.
42. Biesecker G, Lavin L, Ziskind M, Koffler D. Cutaneous local-
ization of the membrane attack complex in discoid and systemic
lupus erythematosus. N Engl J Med. 1982;306:264–70.
43. Helm KF, Peters MS. Deposition of membrane attack complex
in cutaneous lesions of lupus erythematosus. J Am Acad Der-
matol. 1993;28:687–91.
44. Paronetto F, Koffler D. Immunofluorescent localization of
immunoglobulins, complement, and fibrinogen in human dis-
eases. I. Systemic lupus erythematosus. J Clin Invest. 1965;44:
1657–64.
45. Lachmann PJ, Muller-Eberhard HJ, Kunkel HG, Paronetto F.
The localization of in vivo bound complement in tissue section.
J Exp Med. 1962;115:63–82.
46. Sciascia S, Ceberio L, Garcia-Fernandez C, Roccatello D,
Karim Y, Cuadrado MJ. Systemic lupus erythematosus and
infections: clinical importance of conventional and upcoming
biomarkers. Autoimmun Rev. 2012;12:157–63.
47. Walport MJ. Complement and systemic lupus erythematosus.
Arthritis Res. 2002;4(Suppl 3):S279–93.
48. Ross GD, Yount WJ, Walport MJ, Winfield JB, Parker CJ,
Fuller CR, et al. Disease-associated loss of erythrocyte com-
plement receptors (CR1, C3b receptors) in patients with sys-
temic lupus erythematosus and other diseases involving
autoantibodies and/or complement activation. J Immunol. 1985;
135:2005–14.
49. Ballanti E, Perricone C, Di Muzio G, Kroegler B, Chimenti MS,
Graceffa D, et al. Role of the complement system in rheumatoid
arthritis and psoriatic arthritis: relationship with anti-TNF
inhibitors. Autoimmun Rev. 2011;10:617–23.
50. Trentham DE, Townes AS, Kang AH. Autoimmunity to type II
collagen an experimental model of arthritis. J Exp Med.
1977;146:857–68.
51. Courtenay JS, Dallman MJ, Dayan AD, Martin A, Mosedale B.
Immunisation against heterologous type II collagen induces
arthritis in mice. Nature. 1980;283:666–8.
52. Cathcart ES, Hayes KC, Gonnerman WA, Lazzari AA, Fran-
zblau C. Experimental arthritis in a nonhuman primate.
I. Induction by bovine type II collagen. Lab Invest. 1986;54:
26–31.
53. Yoo TJ, Kim SY, Stuart JM, Floyd RA, Olson GA, Cremer MA,
et al. Induction of arthritis in monkeys by immunization with
type II collagen. J Exp Med. 1988;168:777–82.
54. Hietala MA, Jonsson IM, Tarkowski A, Kleinau S, Pekna M.
Complement deficiency ameliorates collagen-induced arthritis in
mice. J Immunol. 2002;169:454–9.
55. Wang Y, Rollins SA, Madri JA, Matis LA. Anti-C5 monoclonal
antibody therapy prevents collagen-induced arthritis and ame-
liorates established disease. Proc Natl Acad Sci USA. 1995;92:
8955–9.
56. Mizuno M. A review of current knowledge of the complement
system and the therapeutic opportunities in inflammatory
arthritis. Curr Med Chem. 2006;13:1707–17.
57. D’Cruz D, Taylor J, Ahmed T, Asherson R, Khamashta M,
Hughes GR. Complement factor 2 deficiency: a clinical and
serological family study. Ann Rheum Dis. 1992;51:1254–6.
58. Di Muzio G, Perricone C, Ballanti E, Kroegler B, Greco E,
Novelli L, et al. Complement system and rheumatoid arthritis:
relationships with autoantibodies, serological, clinical features,
and anti-TNF treatment. Int J Immunopathol Pharmacol. 2011;
24:357–66.
59. Miura N, Prentice HL, Scheider PM, Perlmutter DH. Synthesis
and regulation of the two human complement C4 genes in stable
transfected mouse fibroblasts. J Biol Chem. 1987;262:7298–305.
60. Andus T, Heinrich PC, Bauer J, Trau-Thi TA, Decker K,
Manuel D, et al. Discrimination of hepatocyte stimulating
activity from human recombinant tumour necrosis factor a. Eur J
lmmunol. 1988;17:1193–7.
61. Anthony R, EL-Omar E, Lappin DF, MacSween RNM, Whaley
K. Regulation of hepatic synthesis of C3 and C4 during acute-
phase response in the rat. Eur J Immunol. 1989;19:1405–12.
62. Ramadori G, Van Daume J, Riedert H, Mayer Zum Buschen-
felde KH. Interleukin-6, the third mediator of acute-phase
reaction, modulates hepatic protein synthesis in human and
mouse comparison as with interleukin-1b and tumour necrosis
faclor-a. Eur J Immunol. 1988;18:1259–64.
63. Moffat GJ, Lappin D, Birnie GD, Whaley K. Complement
biosynthesis in human synovial tissue. Clin Exp Immunol. 1989;
78:54–60.
64. Ruddy S, Colten HR. Rheumatoid arthritis. Biosynthesis of
complement proteins by synovial tissues. N Engl J Med. 1974;
290:1284–8.
65. Neumann E, Barnum SR, Tarner IH, Echols J, Fleck M, Judex
M, et al. Local production of complement proteins in rheuma-
toid arthritis synovium. Arthritis Rheum. 2002;46:934–45.
66. Guc D, Gulati P, Lemercier C, Lappin D, Birnie GD, Whaley K.
Expression of the components and regulatory proteins of the
alternative complement pathway and the membrane attack
complex in normal and diseased synovium. Rheumatol Int.
1993;13:139–46.
67. Whaley K, Guc D, Gulati P, Lappin D. Synthesis of complement
components by synovial membrane. Immunopharmacology.
1992;24:83–9.
68. Doherty M, Richards N, Hornby J, Powell R. Relation between
synovial fluid C3 degradation products and local joint inflam-
mation in rheumatoid arthritis, osteoarthritis, and crystal asso-
ciated arthropathy. Ann Rheum Dis. 1988;47:190–7.
69. Oleesky DA, Daniels RH, Williams BD, Amos N, Morgan BP.
Terminal complement complexes and C1/C1 inhibitor com-
plexes in rheumatoid arthritis and other arthritic conditions. Clin
Exp Immunol. 1991;84:250–5.
488 Diagnosis of Autoimmunity (2013) 56:477–491
123

70. Konttinen YT, Ceponis A, Meri S, Vuorikoski A, Kortekangas
P, Sorsa T, et al. Complement in acute and chronic arthritides:
assessment of C3c, C9, and protectin (CD59) in synovial
membrane. Ann Rheum Dis. 1996;55:888–94.
71. Jose PJ, Moss IK, Maini RN, Williams TJ. Measurement of the
chemotactic complement fragment C5a in rheumatoid synovial
fluids by radioimmunoassay: role of C5a in the acute inflam-
matory phase. Ann Rheum Dis. 1990;49:747–52.
72. Høgasen K, Mollnes TE, Harboe M, Gotze O, Hammer HB,
Oppermann M. Terminal complement pathway activation and
low lysis inhibitors in rheumatoid arthritis synovial fluid.
J Rheumatol. 1995;22:24–8.
73. Zubler RH, Nydegger U, Perrin LH, Fehr K, McCormick J,
Lambert PH, et al. Circulating and intra-articular immune
complexes in patients with rheumatoid arthritis: correlation of
125IClq binding activity with clinical and biological features of
the disease. J Clin Invest. 1976;57:1308–19.
74. Hay FC, Nineham LJ, Perumal R, Roitt IM. Intra-articular and
circulating immune complexes and antiglobulins (IgG and IgM)
in rheumatoid arthritis: correlation with clinical features. Ann
Rheum Dis. 1979;38:1–7.
75. Robbins DL, Fiegal DW Jr, Leek JC, Shapiro R, Wiesner K.
Complement activation by 19S IgM rheumatoid factor: rela-
tionship to disease activity in rheumatoid arthritis. J Rheumatol.
1986;13:33–8.
76. Sato Y, Sato R, Watanabe H, Kogure A, Watanabe K, Nishimaki
T, et al. Complement activating properties of monoreactive and
polyreactive IgM rheumatoid factors. Ann Rheum Dis. 1993;52:
795–800.
77. Sato Y, Watanabe H, Kogure A, Miyata M, Watanabe K,
Nishimaki T, et al. Complement-activating properties of IgM
rheumatoid factors reacting with IgG subclasses. Clin Rheu-
matol. 1995;14:425–8.
78. Tanimoto K, Cooper NR, Johnson JS, Vaughan JH. Comple-
ment fixation by rheumatoid factor. J Clin Invest. 1975;55:
437–45.
79. Ruddy S, Austen KF. Activation of the complement and pro-
perdin systems in rheumatoid arthritis. Ann N Y Acad Sci.
1975;256:96–104.
80. El-Ghobarey A, Whaley K. Alternative pathway complement
activation in rheumatoid arthritis. J Rheumatol. 1980;7:453–60.
81. Malhotra R, Wormald MR, Rudd PM, Fischer PB, Dwek RA,
Sim RB. Glycosylation changes of IgG associated with rheu-
matoid arthritis can activate complement via the mannose-
binding protein. Nat Med. 1995;1:237–43.
82. Trouw LA, Haisma EM, Levarht EW, van der Woude D, Ioan-
Facsinay A, Daha MR, et al. Anti-cyclic citrullinated peptide
antibodies from rheumatoid arthritis patients activate comple-
ment via both the classical and alternative pathways. Arthritis
Rheum. 2009;60:1923–31.
83. Volonakis JE. Complement activation by C-reactive protein
complexes. Ann N Y Acad Sci. 1982;389:235–49.
84. Wolbink GJ, Brouwer MC, Buysman S, ten Berge IJM, Hack
CE. CRP-mediated activation of complement in vivo: assess-
ment by measuring circulating complement-C-reactive protein
complexes. J Immunol. 1996;157:473–9.
85. Wolbink GJ, Bossink AWJ, Groeneveld ABJ, de Groot MCM,
Thijs LG, Hack CE. Complement activation in patients with
sepsis is in part mediated by C-reactive protein. J Infect Dis.
1998;177:81–7.
86. Molenaar ET, Voskuyl AE, Familian A, van Mierlo GJ, Dijk-
mans BA, Hack CE. Complement activation in patients with
rheumatoid arthritis mediated in part by C-reactive protein.
Arthritis Rheum. 2001;44:997–1002.
87. Lagrand WK, Niessen HWM, Wolbink GJ, Jaspers LH, Visser
CA, Verheugt FWA, et al. C-reactive protein co-localizes with
complement in human hearts during acute myocardial infarction.
Circulation. 1997;95:97–103.
88. Sjoberg A, Onnerfjord P, Morgelin M, Heinegard D, Blom AM.
The extracellular matrix and inflammation: fibromodulin acti-
vates the classical pathway of complement by directly binding
C1q. J Biol Chem. 2005;280:32301–8.
89. Mollnes TE, Lea T, Mellbye OJ, Pahle J, Grand O, Harboe M.
Complement activation in rheumatoid arthritis evaluated by
C3dg and the terminal complement complex. Arthritis Rheum.
1986;29:715–21.
90. Olmez U, Garred P, Mollnes TE, Harboe M, Berntzen HB,
Munthe E. C3 activation products, C3 containing immune
complexes, the terminal complement complex and native C9 in
patients with rheumatoid arthritis. Scand J Rheumatol. 1991;20:
183–9.
91. Wouters D, Voskuyl AE, Molenaar ET, Dijkmans BA, Hack CE.
Evaluation of classical complement pathway activation in
rheumatoid arthritis: measurement of C1q–C4 complexes as
novel activation products. Arthritis Rheum. 2006;54:1143–50.
92. Rosenberg EW, Noah PW, Wyatt RJ, Jones RM, Kolb WP.
Complement activation in psoriasis. Clin Exp Dermatol. 1990;
15:16–20.
93. Partsch G, Bauer K, Broll H, Petera P, Dunky A, Meretey K.
Complement C3 cleavage product in synovial fluids detected by
immunofixation. Z Rheumatol. 1991;50:82–5.
94. Triolo G, Accardo-Palumbo A, Sallı L, Ciccia F, Ferrante A,
Tedesco L, et al. Impaired expression of erythrocyte glycosyl-
phosphatidylinositol-anchored membrane CD59 in patients with
psoriatic arthritis. Relation to terminal complement pathway
activation. Clin Exp Rheumatol. 2003;21:225–8.
95. Rivas D, Riestra-Noriega JL, Torre-Alonso JC, Rodriguez A,
Gutierrez C. Decrease in detectable complement receptor type 1
levels on erythrocytes from patients with psoriatic polyarthritis.
Br J Rheumatol. 1994;33:626–30.
96. Chimenti MS, Perricone C, Graceffa D, Di Muzio G, Ballanti E,
Guarino MD, et al. Complement system in psoriatic arthritis: a
useful marker in response prediction and monitoring of anti-
TNF treatment. Clin Exp Rheumatol. 2012;30:23–30.
97. Chimenti MS, Ballanti E, Perricone C, Cipriani P, Giacomelli R,
Perricone R. Immunomodulation in psoriatic arthritis: focus on
cellular and molecular pathways. Autoimmun Rev. 2012;. doi:
10.1016/j.autrev.2012.10.002.
98. Townes AS. Topics in clinical medicine. Complement’s levels
in disease. Johns Hopkins Med J. 1967;120:337–9.
99. Senaldi G, Lupoli S, Vergani D, Black CM. Activation of the
complement system in systemic sclerosis. Relationship to clin-
ical severity. Arthritis Rheum. 1989;32:1262–7.
100. Subcommittee for Scleroderma Criteria of the American Rheu-
matism Association Diagnostic and Therapeutic Criteria Com-
mittee. Preliminary criteria for the classification of systemic
sclerosis (scleroderma). Arthritis Rheum. 1980;23:581–90.
101. Valentini G, Della Rossa A, Bombardieri S, Bencivelli W, Sil-
man AJ, D’Angelo S, et al. European multicentre study to define
disease activity criteria for systemic sclerosis. II. Identification
of disease activity variables and development of preliminary
activity indexes. Ann Rheum Dis. 2001;60:592–8.
102. Hudson M, Walker JG, Fritzler M, Taillefer S, Canadian
Scleroderma Research Group, Baron M. Hypocomplementemia
in systemic sclerosis, clinical and serological correlations.
J Rheumatol. 2007;34:1–6.
103. Wetsel RA. Structure, function and cellular expression of
complement anaphylatoxin receptors. Curr Opin Immunol.
1995;7:48–53.
104. Shin ML, Rus HG, Nicolescu FI. Membrane attack by com-
plement: assembly and biology of terminal complement com-
plexes. Biomembranes. 1996;4:123–49.
Diagnosis of Autoimmunity (2013) 56:477–491 489
123

105. Holers VM, Girardi G, Mo L, Guthridge JM, Molina H, Pier-
angeli SS, et al. Complement C3 activation is required for an-
tiphospholipid antibody-induced fetal loss. J Exp Med. 2002;
195:211–20.
106. Girardi G, et al. Complement C5a receptors and neutrophils
mediate fetal injury in the antiphospholipid syndrome. J Clin
Invest. 2003;112:1644–54.
107. Kim YU, Kinoshita H, Molina H, Hourcade D, Esya L, Wagner
M, et al. Mouse complement regulatory protein Crry/p65 utilizes
the specific mechanisms of both decay-accelerating factor and
membrane cofactor protein. J Exp Med. 1995;181:151–9.
108. Xu C, Mao D, Holers VM, Palanca B, Cheng A, Molina H. A
critical role for the murine complement regulator Crry in feto-
maternal tolerance. Science. 2000;287:498–501.
109. Nangaku M, Alpers CE, Pippin J, Shankland SJ, Kurokawa K,
Adler S, et al. CD59 protects glomerular endothelial cells from
immune-mediated thrombotic microangiopathy in rats. J Am
Soc Nephrol. 1998;9:590–7.
110. Pierangeli SS, Girardi G, Vega-Ostertag M, Liu X, Espinola RG,
Salmon J. Requirement of activation of complement C3 and C5
for antiphospholipid antibody-mediated thrombophilia. Arthritis
Rheum. 2005;52:2120–4.
111. Salmon JE, Girardi G. Antiphospholipid antibodies and preg-
nancy loss: a disorder of inflammation. J Reprod Immunol.
2008;77:51–6.
112. Oku K, Atsumi T, Bohgaki M, Amengual O, Kataoka H, Horita
T, et al. Complement activation in patients with primary anti-
phospholipid syndrome. Ann Rheum Dis. 2009;68:1030–5.
113. Dalakas MC. Pathogenesis and therapies of immune-mediated
myopathies. Autoimmun Rev. 2012;11:203–6.
114. Dalakas MC, Hohlfeld R. Polymyositis and dermatomyositis.
Lancet. 2003;362:971–82.
115. Kissel JT, Mendell JR, Rammohan KW. Microvascular depo-
sition of complement membrane attack complex in dermato-
myositis. N Engl J Med. 1986;314:329–34.
116. Mascaro JM Jr, Hausmann G, Herrero C, Grau JM, Cid MC,
Palou J, et al. Membrane attack complex deposits in cutaneous
lesions of dermatomyositis. Arch Dermatol. 1995;131:1386–92.
117. Fox RI. Sjogren’s syndrome. Lancet. 2005;366:321–31.
118. Skopouli FN, Dafni U, Ioannidis JP, Moutsopoulos HM. Clinical
evolution, and morbidity and mortality of primary Sjogren’s
syndrome. Semin Arthritis Rheum. 2000;29:296–304.
119. Ioannidis JP, Vassiliou VA, Moutsopoulos HM. Long-term risk
of mortality and lymphoproliferative disease and predictive
classification of primary Sjogren’s syndrome. Arthritis Rheum.
2002;46:741–7.
120. Theander E, Manthorpe R, Jacobsson LT. Mortality and causes
of death in primary Sjogren’s syndrome: a prospective cohort
study. Arthritis Rheum. 2004;50:1262–9.
121. Ramos-Casals M, Brito-Zeron P, Yague J, Akasbi M, Bautista
R, Ruano M, et al. Hypocomplementaemia as an immunological
marker of morbidity and mortality in patients with primary
Sjogren’s syndrome. Rheumatology (Oxford). 2005;44:89–94.
122. Arnaud L, Haroche J, Mathian A, Gorochov G, Amoura Z.
Pathogenesis of Takayasu’s arteritis: a 2011 update. Autoimmun
Rev. 2011;11:61–7.
123. Seo P, Stone JH. The antineutrophil cytoplasmic antibody-
associated vasculitides. Am J Med. 2004;117:39–50.
124. Kallenberg CGM. Pathophysiology of ANCA-associated small
vessel vasculitis. Curr Rheumatol Rep. 2010;12:399–405.
125. Schreiber A, Xiao H, Jennette JC, Schneider W, Luft FC,
Kettritz R. C5a receptor mediates neutrophil activation and
ANCA-induced glomerulonephritis. J Am Soc Nephrol.
2009;20:289–98.
126. Xiao H, Schreiber A, Heeringa P, Falk RJ, Jennette JC. Alter-
native complement pathway in the pathogenesis of disease
mediated by anti-neutrophil cytoplasmic autoantibodies. Am J
Pathol. 2007;170:52–64.
127. Xing GQ, Chen M, Liu G, Heeringa P, Zhang JJ, Zheng X, et al.
Complement activation is involved in renal damage in human
antineutrophil cytoplasmic autoantibody associated pauci-
immune vasculitis. J Clin Immunol. 2009;29:282–91.
128. Lospalluto J, Dorward B, Miller W Jr, Ziff M. Cryoglobulinemia
based on interaction between a gamma macroglobulin and 7S
gamma globulin. Am J Med. 1962;32:142–5.
129. Ferri C, Zignego AL, Pileri SA. Cryoglobulins. J Clin Pathol.
2002;55:4–13.
130. Monti G, Galli M, Invernizzi F, Pioltelli P, Saccardo F,
Monteverde A, et al. Cryoglobulinaemias: a multi-centre study
of the early clinical and laboratory manifestations of primary
and secondary disease. GISC. Italian Group for the Study of
Cryoglobulinaemias. QJM. 1995;88:115–26.
131. Tarantino A, Anelli A, Costantino A, De Vecchi A, Monti G,
Massaro L. Serum complement pattern in essential mixed
cryoglobulinaemia. Clin Exp Immunol. 1978;32:77–85.
132. Davin JC. Henoch-Schonlein purpura nephritis: pathophysiol-
ogy, treatment, and future strategy. Clin J Am Soc Nephrol.
2011;6:679–89.
133. Hisano S, Matsushita M, Fujita T, Iwasaki H. Activation of the
lectin complement pathway in Henoch-Schonlein purpura
nephritis. Am J Kidney Dis. 2005;45:295–302.
134. Roos A, Rastaldi MP, Calvaresi N, Oortwijn BD, Schlagwein N,
van Gijlswijk-Janssen DJ, et al. Glomerular activation of the lectin
pathway of complement in IgA nephropathy is associated with
more severe renal disease. J Am Soc Nephrol. 2006;17:1724–34.
135. Espinosa M, Ortega R, Gomez-Carrasco JM, Lopez-Rubio F,
Lopez-Andreu M, Lopez-Oliva MO, et al. Mesangial C4d
deposition: a new prognostic factor in IgA nephropathy. Nephrol
Dial Transplant. 2009;24:886–91.
136. Holers VM. The complement system as a therapeutic target in
autoimmunity. Clin Immunol. 2003;107:140–51.
137. Makrides SC. Therapeutic inhibition of the complement system.
Pharmacol Rev. 1998;50:59–87.
138. Asghar SS, Pasch MC. Therapeutic inhibition of the comple-
ment system. Y2K update. Front Biosci. 2000;5:E63–81.
139. Goodfellow RM, Williams AS, Levin JL, Williams BD, Morgan
BP. Soluble complement receptor one (sCR1) inhibits the
development and progression of rat collagen-induced arthritis.
Clin Exp Immunol. 2000;119:210–6.
140. Ames RS, Lee D, Foley JJ, Jurewicz AJ, Tornetta MA, Bautsch
W, et al. Identification of a selective nonpeptide antagonist of
the anaphylatoxin C3a receptor that demonstrates antiinflam-
matory activity in animal models. J Immunol. 2001;166:6341–8.
141. Woodruff TM, Strachan AJ, Dryburgh N, Shiels IA, Reid RC,
Fairlie DP, et al. Antiarthritic activity of an orally active C5a
receptor antagonist against antigen-induced monarticular
arthritis in the rat. Arthritis Rheum. 2002;46:2476–85.
142. Fraser DA, Harris CL, Williams AS, Mizuno M, Gallagher S,
Smith RA, et al. Generation of a recombinant, membrane-tar-
geted form of the complement regulator CD59: activity in vitro
and in vivo. J Biol Chem. 2003;278:48921–7.
143. Vergunst CE, Gerlag DM, Dinant H, Schulz L, Vinkenoog M,
Smeets TJ, et al. Blocking the receptor for C5a in patients with
rheumatoid arthritis does not reduce synovial inflammation.
Rheumatology (Oxford). 2007;46:1773–8.
144. Wang Y, Hu Q, Madri JA, Rollins SA, Chodera A, Matis LA.
Amelioration of lupus-like autoimmune disease in NZB/W F1
mice after treatment with a blocking monoclonal antibody spe-
cific for complement component C5. Proc Natl Acad Sci USA.
1996;93:8563–8.
145. Watanabe H, Garnier G, Circolo A, Wetsel RA, Ruiz P, Holers
VM, et al. Modulation of renal disease in MRL/lpr mice
490 Diagnosis of Autoimmunity (2013) 56:477–491
123

genetically deficient in the alternative complement pathway
factor B. J Immunol. 2000;164:786–94.
146. Bao L, Haas M, Boackle SA, Kraus DM, Cunningham PN, Park
P, et al. Transgenic expression of a soluble complement inhib-
itor protects against renal disease and promotes survival in
MRL/lpr mice. J Immunol. 2002;168:3601–7.
147. Bao L, Haas M, Kraus DM, Hack BK, Rakstang JK, Holers VM,
et al. Administration of a soluble recombinant complement C3
inhibitor protects against renal disease in MRL/lpr mice. J Am
Soc Nephrol. 2003;14:670–9.
148. Murdaca G, Colombo BM, Puppo F. Emerging biological drugs:
a new therapeutic approach for Systemic Lupus Erythematosus.
An update upon efficacy and adverse events. Autoimmun Rev.
2011;11:56–60.
149. Parker CJ. Management of paroxysmal nocturnal hemoglobin-
uria in the era of complement inhibitory therapy. Hematology
Am Soc Hematol Educ Program. 2011;2011:21–9.
150. Cicardi M, Zanichelli A. Replacement therapy with C1 esterase
inhibitors for hereditary angioedema. Drugs Today. 2010;46:
867–74.
151. Mollnes TE, Høgasen K, De Carolis C, Vaquero E, Nielsen EW,
Fontana L, et al. High-dose intravenous immunoglobulin treat-
ment activates complement in vivo. Scand J Immunol. 1998;48:
312–7.
152. Morgan BP, Harris CL. Complement therapeutics; history and
current progress. Mol Immunol. 2003;40:159–70.
Diagnosis of Autoimmunity (2013) 56:477–491 491
123