choriocapillaris photodynamic therapy using indocyanine green
TRANSCRIPT

Choriocapillaris Photodynamic Therapy UsingIndocyanine Green
ROGERIO A. COSTA, MD, MICHEL E. FARAH, MD, EDNA FREYMULLER, MD,PAULO H. MORALES, MD, RICARDO SMITH, MD, AND JOSE A. CARDILLO, MD
● PURPOSE: To evaluate the potential of photodynamictherapy using indocyanine green for occlusion of choroi-dal neovascularization, the authors studied efficiency andcollateral damage of photodynamic therapy–induced pho-tothrombosis in the rabbit choriocapillary layer.● METHODS: Fundus photography, fluorescein angiogra-phy, and light and transmission electron microscopy wereused to study the efficiency of photodynamic therapy–induced photothrombosis using indocyanine green as thephotosensitizer, and to assess the resultant collateraldamage. The delivery system consisted of a modifiedinfrared diode laser tuned to 810 nm, near the maximumabsorption peak of indocyanine green.● RESULTS: Choriocapillary occlusion was achieved atindocyanine green doses of 10 and 20 mg/kg and a radiantas low as 6.3 J/cm2. When photodynamic therapy wasperformed with indocyanine green doses of 10 mg/kg,damage to the neural retina was minimal. Only innerphotoreceptor segments showed degeneration, probablysecondary to choroidal ischemia. Bruch membrane re-mained intact. Retinal pigment epithelium was invariablydamaged, as seen with other photosensitizers. Temporaryocclusion of large choroidal vessels occurred at both dyedoses.● CONCLUSIONS: In this experimental study, photody-namic therapy using indocyanine green and 810-nm lightirradiation produced endothelium-bound intraluminalphotothrombosis, with preservation of the retinal archi-tecture and minimal loss of visual cells. Membranetargetability, hydrophilic and fluorescent properties, andactivation at 805 nm suggest indocyanine green as apotential photosensitizer for choroidal neovasculariza-tion. These combined considerations point toward fur-
ther study of photodynamic therapy using indocyaninegreen for the treatment of choroidal vascular disease.(Am J Ophthalmol 2001;132:557–565. © 2001 byElsevier Science Inc. All rights reserved.)
P HOTODYNAMIC THERAPY IS A DEVELOPING TREAT-
ment modality. Interest in cytotoxic responses tophotosensitizing agents has been recorded as early as
1900.1 Reports from the 1970s of successful treatment ofanimal tumors using intravenous hematoporphyrin deriv-atives launched the modern photodynamic therapy era.2This technique involves intravenous injection of a photo-sensitizer that accumulates in the neovascular and tumortissue. This photosensitized tissue is then irradiated bylight at the absorption maximum of the dye leading tocytotoxicity.3,4 As a result of successful clinical trials, thebenzoporphyrin derivative monoacid photodynamic agent(verteporfin, Visudyne; CIBA Vision, Duluth) has recentlygained United States Food and Drug Administrationapproval for clinical use in age-related macular disease.5–7
Unfortunately, some patients with subfoveal choroidalneovascularization with age-related macular disease willnot be eligible for treatment because of clinical andangiographic features.8,9 Investigators have been seekingnew photosensitizers for photodynamic therapy that can bemore effectively used for treatment of choroidal neovascu-larization in patients with age-related macular disease andthat are able to improve the visual outcome of this disease.
Indocyanine green, an anionic tricarbocyanine dye thathas been used for imaging of the retinal and choroidalvasculature for over 30 years,10,11 was recently used todestroy colonic cancer cells in vitro. Cell death was theresult of the generation of singlet oxygen and the subse-quent formation of lipid peroxides after photoactivation bya diode laser emitting light at 805 nm.12 This relativelylarge, protein-bound, photosensitive molecule experiencesselective intravascular retention and peak absorption (805nm)13 close to the peak emission (810 nm) of the conven-tional diode laser, thus presenting an outstanding advan-tage because of deeper tissue penetration.14,15 In addition,indocyanine green dye, like other second-generationagents, is characterized by low skin phototoxicity, high
Accepted for publication Jun 21, 2001.From the Department of Ophthalmology (R.A.C., M.E.F., P.H.M.,
J.A.C.), Electron Microscopy Center (E.F.), and the Department ofMorphology (R.S.), Federal University of Sao Paulo, Paulista School ofMedicine, Sao Paulo, Brazil.
This study was presented in part at the annual meeting of theAssociation for Research in Vision and Ophthalmology, Fort Lauderdale,Florida, May 2001.
Reprint requests to Rogerio Alves Costa, MD, Av. Ibijau, 331, 4°andar, Sao Paulo, SP - Brazil 04524-020; fax: 55(11) 5579 7060; e-mail:[email protected]
© 2001 BY ELSEVIER SCIENCE INC. ALL RIGHTS RESERVED.0002-9394/01/$20.00 557PII S0002-9394(01)01138-2
tissue targetability, rapid biodistribution and clearance,and easy administration and monitoring, as required for aphotosensitizer for photodynamic therapy. We are unawareof previous reports of the potential of indocyanine green–mediated photodynamic therapy for choriocapillaris andcould find no reference to it in a computerized search usingMEDLINE.
The objective of this study was to evaluate the responseof the choriocapillaris to indocyanine green and 810-nmlight in pigmented rabbit eyes. Large choroidal vessels andextravascular ocular components, such as the neurosensoryretina and retinal pigment epithelium, were also evaluatedfor damage after photodynamic therapy with indocyaninegreen.
MATERIALS AND METHODS
INDOCYANINE GREEN DYE (ICG-PULSION, MUNCHEN, GER-
many) was obtained in dehydrated powder form. Indocya-nine green was reconstituted into solution form usingsterile distilled water at 5°C 1 hour before experimenta-tion. Light-protected status was maintained at all timesduring the handling of the indocyanine green to preventinadvertent activation.
The laser delivery system consisted of a modified infra-red diode laser and a slit-lamp biomicroscope. A diodelaser (TTT 1500; OPTO, Sao Carlos, Brazil) tuned to 810nm, near the maximum absorption peak of indocyaninegreen, was outfitted with an adjustable beam width (set-tings at 0.8, 1.0, 1.2, 1.5, 2.5, and 4.3 mm) and thencoupled to a slit-lamp biomicroscope (SL-3E; Topcon,Tokyo, Japan).
All animals were treated in accordance with the Asso-ciation for Research in Vision and Ophthalmology Reso-lution on the Use of Animals in Research. Fifteenpigmented rabbits (weighing 2.0 to 2.5 kg) were examinedby indirect ophthalmoscopy and found to have normalfundi before entry into the study. Anesthesia consisted ofan intramuscular injection of ketamine hydrochloride (50mg/kg) plus xylazine hydrochloride (5 mg/kg) during allprocedures, with additional ketamine injections as needed.Pupillary dilation was obtained using topical tropicamide1% and phenylephrine hydrochloride 2.5%. Eyes wereenucleated under deep anesthesia, and the animals wereeuthanatized with an intravenous injection of pentobarbi-tal sodium (50 mg/kg).
Before any light application, a fundus contact lens(Mainster widefield; Ocular Instruments, Bellevue, WA)was placed on the rabbit’s cornea. To facilitate tissuesectioning for histologic examination, three intensemarker burns were produced in both eyes by photocoagu-lation in the inferior paramedullary zone. Three areas inthe left eye were exposed to the following light durationschedule (temporal to nasal): 20, 30, and 10 seconds. Thediameter of the laser beam at the retina (4000 �m) was
calculated in air and modified based on the contact lenssystem. The power density used was 230 mW/cm2 (groups1 and 2), 630 mW/cm2 (groups 3 and 4), or 950 mW/cm2
(group 5). The power densities chosen for this study werebased on the results of preliminary work in the same rabbitmodel indicating the amount of light necessary to inducethermal damage (2150 mW/cm2 and 129 J/cm2) (Costaand associates, unpublished data, 2000). These parametersresulted in total fluences of 2.3, 4.6, 6.3, 6.9, 9.5, 12.6,18.9, 19.0, and 28.5 J/cm2. Rabbits were injected through
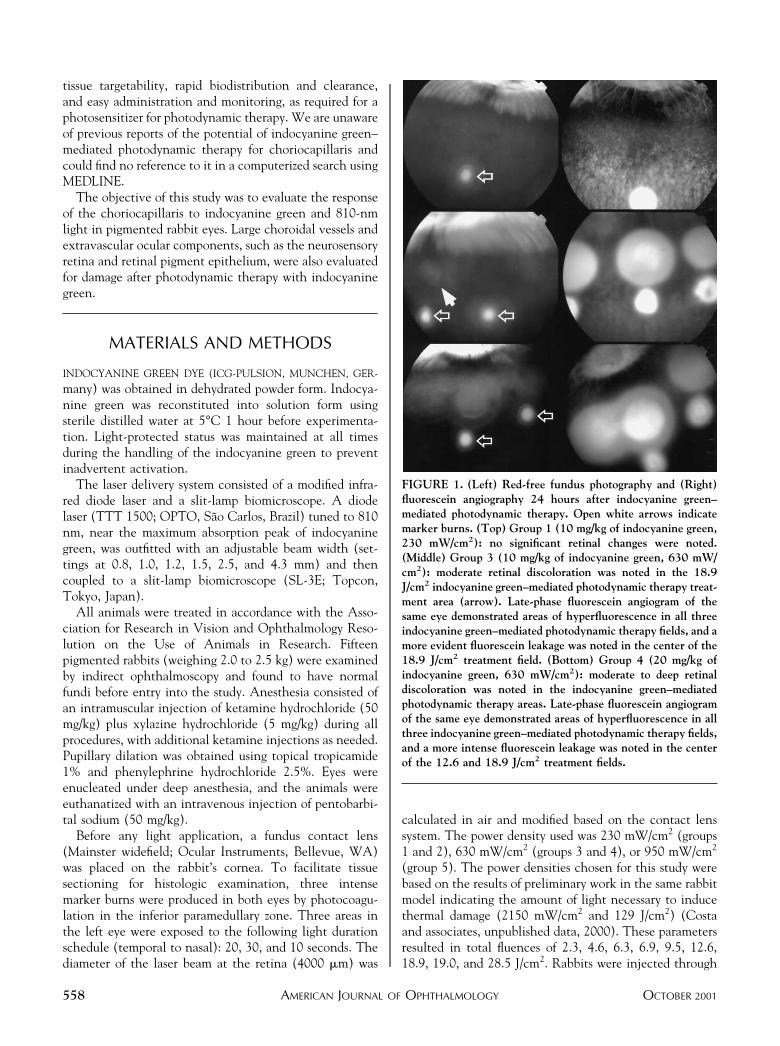
FIGURE 1. (Left) Red-free fundus photography and (Right)fluorescein angiography 24 hours after indocyanine green–mediated photodynamic therapy. Open white arrows indicatemarker burns. (Top) Group 1 (10 mg/kg of indocyanine green,230 mW/cm2): no significant retinal changes were noted.(Middle) Group 3 (10 mg/kg of indocyanine green, 630 mW/cm2): moderate retinal discoloration was noted in the 18.9J/cm2 indocyanine green–mediated photodynamic therapy treat-ment area (arrow). Late-phase fluorescein angiogram of thesame eye demonstrated areas of hyperfluorescence in all threeindocyanine green–mediated photodynamic therapy fields, and amore evident fluorescein leakage was noted in the center of the18.9 J/cm2 treatment field. (Bottom) Group 4 (20 mg/kg ofindocyanine green, 630 mW/cm2): moderate to deep retinaldiscoloration was noted in the indocyanine green–mediatedphotodynamic therapy areas. Late-phase fluorescein angiogramof the same eye demonstrated areas of hyperfluorescence in allthree indocyanine green–mediated photodynamic therapy fields,and a more intense fluorescein leakage was noted in the centerof the 12.6 and 18.9 J/cm2 treatment fields.
AMERICAN JOURNAL OF OPHTHALMOLOGY558 OCTOBER 2001
the marginal ear vein with a 1.5-ml intravenous bolus ofeither 10 mg/kg (groups 1 and 3) or 20 mg/kg (groups 2, 4,and 5) of indocyanine green followed by a saline flush.Control eyes consisted of fellow (right) eyes that werepreviously treated in the same manner, after injection ofan equivalent volume of sterile distilled water instead ofindocyanine green. Irradiation started 10 seconds afterintravenous injection of either distilled water or indocya-nine green. After treatment, animals were returned to theirhousing and raised under ordinary fluorescent lights (30lux) for 9 days.
Fundus photography and fluorescein angiography wereperformed 24 hours after light treatments using a funduscamera (TRC-50IA/IMAGEnet; Topcon, Tokyo, Japan).Additional photography and angiography were performed6 hours after light treatments in group 5. Angiography wasperformed with sodium fluorescein 10% (0.1 ml/kg) bymeans of marginal ear vein injection.
All rabbits were euthanatized immediately after enucle-ation of both eyes 9 days after light irradiation, with theexception of one rabbit of group 5 in which histologicanalysis was performed 2 days after treatment. Immediatelyafter enucleation, the eye was incised at the equator andthe vitreous was removed. All specimens were fixed byimmersion in glutaraldehyde 2.5% in 0.1 mol/l cacodylatebuffer (pH 7.4) for 2 hours at 25°C. The tissue was thentransferred to 0.1 mol/l cacodylate buffer overnight. Eachlesion was individually resected and postfixed with osmiumtetroxide 2% in 0.1 mol/l cacodylate buffer for 1 hour at25°C. After several rinses in water, the specimen wasstained overnight in aqueous uranyl acetate 0.5% (w/v).The specimen was dehydrated in a series of graded alcoholsfollowed by propylene oxide. The tissue was embedded inepoxy resin and sectioned at 0.5 �m. For light microscopy,the sections were stained with 0.5% toluidine blue andviewed with a photomicroscope (Optiphot 2; Nikon,Tokyo, Japan). Areas of interest were ultra-thin–sectioned,stained with uranyl acetate/lead citrate, and examinedwith a transmission electron microscope (1200EXII: JEOL,Tokyo, Japan).
RESULTS
IN TOTAL, 90 TREATMENT AREAS WERE IRRADIATED IN THIS
study. There was no apparent color change in any treatedarea during or immediately following treatment. All con-trol eyes that were injected with distilled water andexposed to measured doses of light revealed no funduscopicor angiographic changes in the treatment areas, indicatingthat there was no detectable thermally induced alterationor other effect of the water alone on the pigment epithe-lium or on the integrity of the blood–retinal barrier.Because the water was chemically inert, there was also nophotochemical reaction noted in the 15 control eyes.
There was no demonstrable retinal change at the 24-
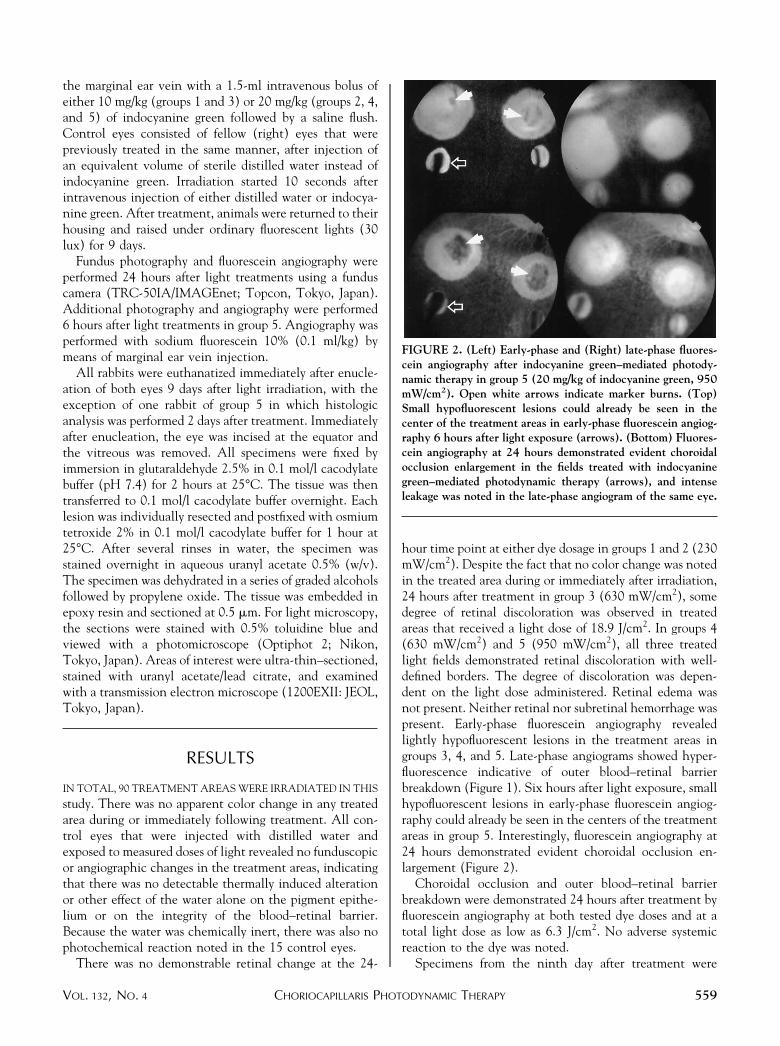
hour time point at either dye dosage in groups 1 and 2 (230mW/cm2). Despite the fact that no color change was notedin the treated area during or immediately after irradiation,24 hours after treatment in group 3 (630 mW/cm2), somedegree of retinal discoloration was observed in treatedareas that received a light dose of 18.9 J/cm2. In groups 4(630 mW/cm2) and 5 (950 mW/cm2), all three treatedlight fields demonstrated retinal discoloration with well-defined borders. The degree of discoloration was depen-dent on the light dose administered. Retinal edema wasnot present. Neither retinal nor subretinal hemorrhage waspresent. Early-phase fluorescein angiography revealedlightly hypofluorescent lesions in the treatment areas ingroups 3, 4, and 5. Late-phase angiograms showed hyper-fluorescence indicative of outer blood–retinal barrierbreakdown (Figure 1). Six hours after light exposure, smallhypofluorescent lesions in early-phase fluorescein angiog-raphy could already be seen in the centers of the treatmentareas in group 5. Interestingly, fluorescein angiography at24 hours demonstrated evident choroidal occlusion en-largement (Figure 2).
Choroidal occlusion and outer blood–retinal barrierbreakdown were demonstrated 24 hours after treatment byfluorescein angiography at both tested dye doses and at atotal light dose as low as 6.3 J/cm2. No adverse systemicreaction to the dye was noted.
Specimens from the ninth day after treatment were
FIGURE 2. (Left) Early-phase and (Right) late-phase fluores-cein angiography after indocyanine green–mediated photody-namic therapy in group 5 (20 mg/kg of indocyanine green, 950mW/cm2). Open white arrows indicate marker burns. (Top)Small hypofluorescent lesions could already be seen in thecenter of the treatment areas in early-phase fluorescein angiog-raphy 6 hours after light exposure (arrows). (Bottom) Fluores-cein angiography at 24 hours demonstrated evident choroidalocclusion enlargement in the fields treated with indocyaninegreen–mediated photodynamic therapy (arrows), and intenseleakage was noted in the late-phase angiogram of the same eye.
CHORIOCAPILLARIS PHOTODYNAMIC THERAPYVOL. 132, NO. 4 559

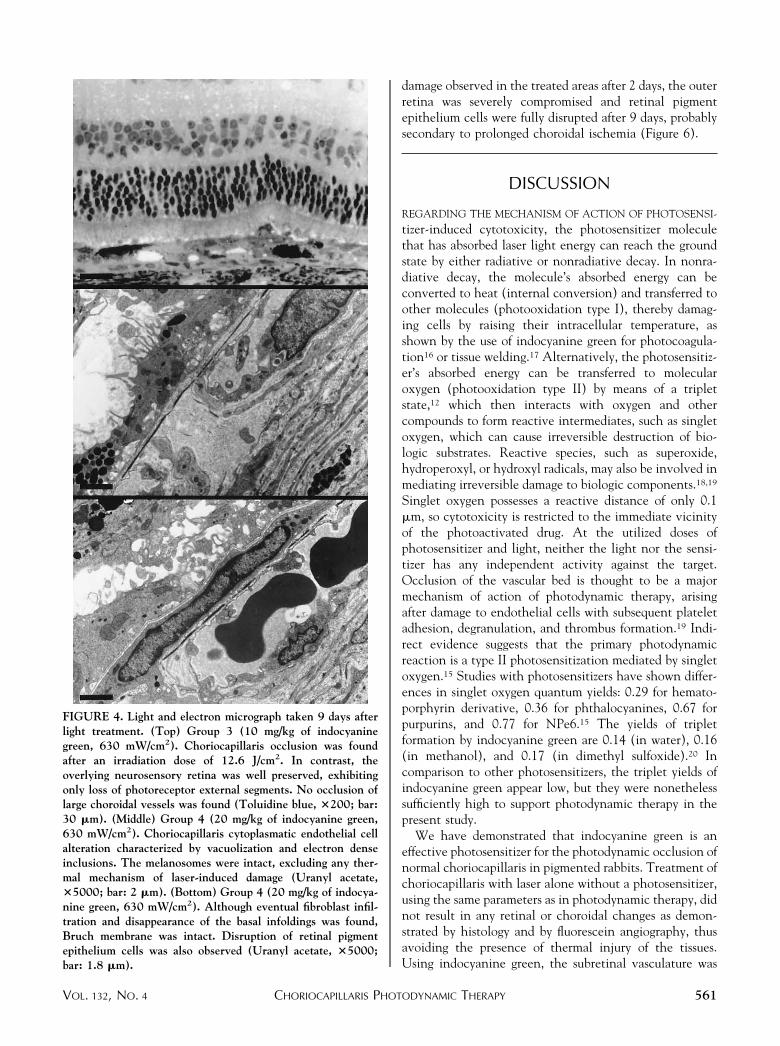
obtained from two left eyes of each group and from oneright eye of the respective controls. The control eyes thatreceived laser and distilled water, as well as the lesions ingroup 1 and 2 eyes, showed no obvious alteration in retinaland choroidal architecture (Figure 3). Lesions of group 3(6.3 and 12.6 J/cm2) and group 4 (6.3 J/cm2) revealedchoriocapillaris occlusion and endothelial cell cytoplas-matic alteration characterized by vacuolization and elec-tron dense inclusions. No occlusion of large choroidalvessels was observed after 9 days. Bruch membrane wasintact, although eventually fibroblast infiltration and dis-appearance of the basal infoldings were noted. Disruptionof retinal pigment epithelium cells was observed, withmelanosomes remaining intact. The overlying neurosen-sory retina was well preserved, exhibiting loss only ofphotoreceptor external segments (Figure 4).
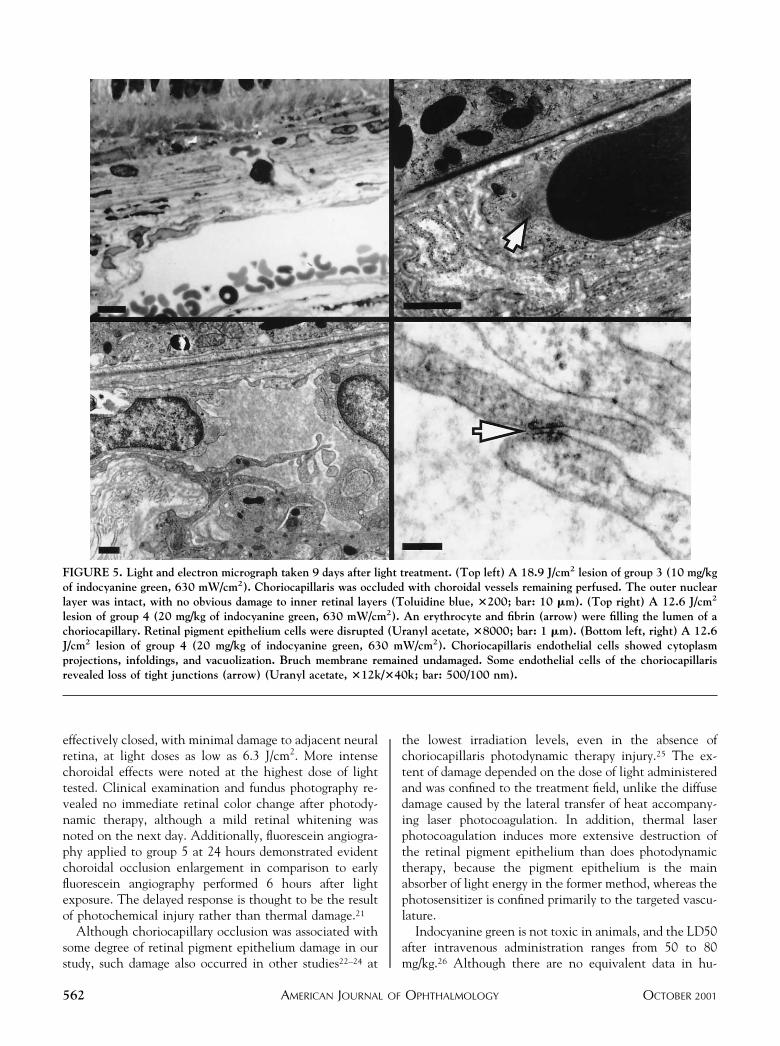
Lesions of group 3 (18.9 J/cm2), group 4 (12.6 J/cm2),and group 5 (9.5 J/cm2) revealed similar features onhistologic examination. The choriocapillaris was filledwith a combination of red blood cells and fibrin, withchoroidal vessels remaining perfused. Choriocapillarisendothelial cells showed cytoplasm projections, infold-ings, and vacuolization. Some endothelial cells of thechoriocapillaris exhibited loss of tight junctions. Bruch
membrane remained undamaged. Retinal pigment epi-thelium cells were disrupted. The outer nuclear layerwas intact, with no obvious damage to inner retinallayers (Figure 5).
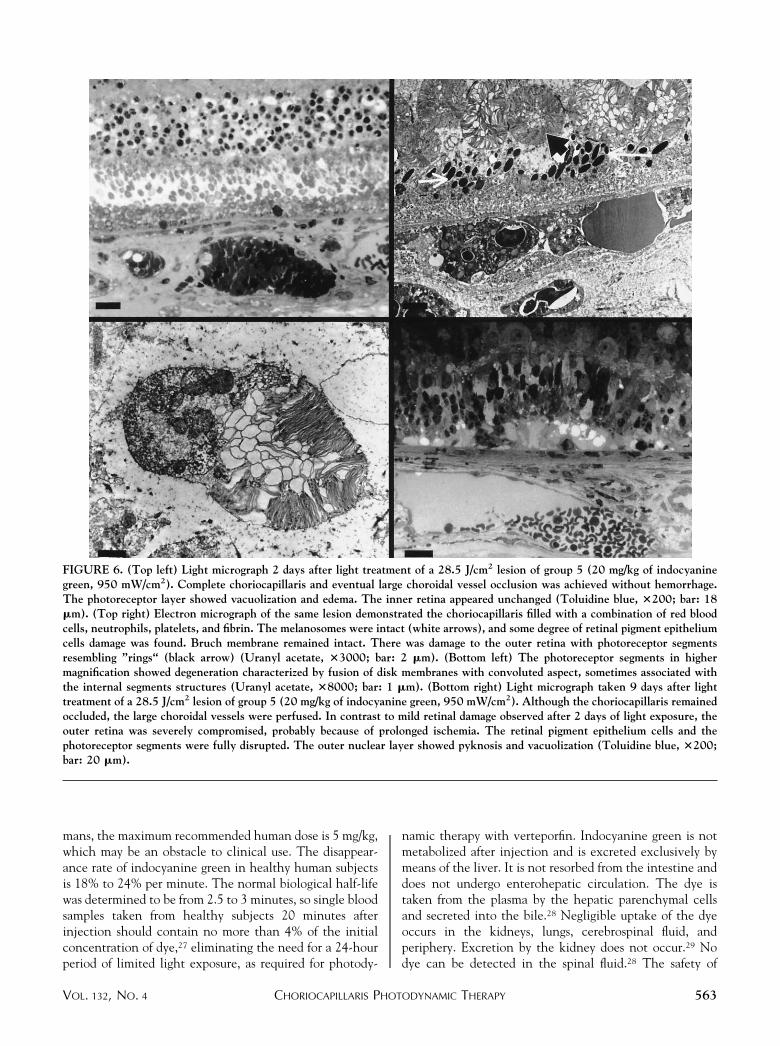
Choriocapillaris occlusion was also achieved in lesionsof group 4 (18.9 J/cm2) and group 5 (19.0 and 28.5 J/cm2).The choriocapillaris was filled with a combination of redblood cells, neutrophils, platelets, and fibrin. The retinalpigment epithelium was fully disrupted in some treatedareas. There was damage to the outer retina, and the outernuclear layer showed pyknosis and vacuolization. Theinner retina appeared unchanged. Occlusion of large cho-roidal vessels in any degree was found after 9 days. Therewere significant differences in histologic appearance whenanalysis was realized 2 days after light exposure in lesions ofgroup 5. Complete choriocapillaris and eventual largechoroidal vessel occlusion was achieved. Bruch membraneremained intact. A mild degree of retinal pigment epithe-lium cell damage was observed, with melanosomes remain-ing intact. The photoreceptor segments were disruptedresembling “rings” and condensed in the apical region ofthe retinal pigment epithelium. The outer nuclear layerwas swollen, and the inner retina appeared unchanged. Incontrast to mild retinal and retinal pigment epithelium
FIGURE 3. Light micrograph taken 9 days after light treatment. Group 5 control eye (distilled water, 950 mW/cm2). Areas ofchoroid and retina, including photoreceptors, appear unchanged at an irradiation of 28.5 J/cm2 (Toluidine blue, �200; bar: 20 �m).(Insert) Group 1 (10 mg/kg of indocyanine green, 230 mW/cm2). At an irradiation dose of 4.6 J/cm2, no obvious alteration in retinalor choroidal architecture was noted (Toluidine blue, �500; bar: 10 �m).
AMERICAN JOURNAL OF OPHTHALMOLOGY560 OCTOBER 2001
damage observed in the treated areas after 2 days, the outerretina was severely compromised and retinal pigmentepithelium cells were fully disrupted after 9 days, probablysecondary to prolonged choroidal ischemia (Figure 6).
DISCUSSION
REGARDING THE MECHANISM OF ACTION OF PHOTOSENSI-
tizer-induced cytotoxicity, the photosensitizer moleculethat has absorbed laser light energy can reach the groundstate by either radiative or nonradiative decay. In nonra-diative decay, the molecule’s absorbed energy can beconverted to heat (internal conversion) and transferred toother molecules (photooxidation type I), thereby damag-ing cells by raising their intracellular temperature, asshown by the use of indocyanine green for photocoagula-tion16 or tissue welding.17 Alternatively, the photosensitiz-er’s absorbed energy can be transferred to molecularoxygen (photooxidation type II) by means of a tripletstate,12 which then interacts with oxygen and othercompounds to form reactive intermediates, such as singletoxygen, which can cause irreversible destruction of bio-logic substrates. Reactive species, such as superoxide,hydroperoxyl, or hydroxyl radicals, may also be involved inmediating irreversible damage to biologic components.18,19
Singlet oxygen possesses a reactive distance of only 0.1�m, so cytotoxicity is restricted to the immediate vicinityof the photoactivated drug. At the utilized doses ofphotosensitizer and light, neither the light nor the sensi-tizer has any independent activity against the target.Occlusion of the vascular bed is thought to be a majormechanism of action of photodynamic therapy, arisingafter damage to endothelial cells with subsequent plateletadhesion, degranulation, and thrombus formation.19 Indi-rect evidence suggests that the primary photodynamicreaction is a type II photosensitization mediated by singletoxygen.15 Studies with photosensitizers have shown differ-ences in singlet oxygen quantum yields: 0.29 for hemato-porphyrin derivative, 0.36 for phthalocyanines, 0.67 forpurpurins, and 0.77 for NPe6.15 The yields of tripletformation by indocyanine green are 0.14 (in water), 0.16(in methanol), and 0.17 (in dimethyl sulfoxide).20 Incomparison to other photosensitizers, the triplet yields ofindocyanine green appear low, but they were nonethelesssufficiently high to support photodynamic therapy in thepresent study.
We have demonstrated that indocyanine green is aneffective photosensitizer for the photodynamic occlusion ofnormal choriocapillaris in pigmented rabbits. Treatment ofchoriocapillaris with laser alone without a photosensitizer,using the same parameters as in photodynamic therapy, didnot result in any retinal or choroidal changes as demon-strated by histology and by fluorescein angiography, thusavoiding the presence of thermal injury of the tissues.Using indocyanine green, the subretinal vasculature was
FIGURE 4. Light and electron micrograph taken 9 days afterlight treatment. (Top) Group 3 (10 mg/kg of indocyaninegreen, 630 mW/cm2). Choriocapillaris occlusion was foundafter an irradiation dose of 12.6 J/cm2. In contrast, theoverlying neurosensory retina was well preserved, exhibitingonly loss of photoreceptor external segments. No occlusion oflarge choroidal vessels was found (Toluidine blue, �200; bar:30 �m). (Middle) Group 4 (20 mg/kg of indocyanine green,630 mW/cm2). Choriocapillaris cytoplasmatic endothelial cellalteration characterized by vacuolization and electron denseinclusions. The melanosomes were intact, excluding any ther-mal mechanism of laser-induced damage (Uranyl acetate,�5000; bar: 2 �m). (Bottom) Group 4 (20 mg/kg of indocya-nine green, 630 mW/cm2). Although eventual fibroblast infil-tration and disappearance of the basal infoldings was found,Bruch membrane was intact. Disruption of retinal pigmentepithelium cells was also observed (Uranyl acetate, �5000;bar: 1.8 �m).
CHORIOCAPILLARIS PHOTODYNAMIC THERAPYVOL. 132, NO. 4 561
effectively closed, with minimal damage to adjacent neuralretina, at light doses as low as 6.3 J/cm2. More intensechoroidal effects were noted at the highest dose of lighttested. Clinical examination and fundus photography re-vealed no immediate retinal color change after photody-namic therapy, although a mild retinal whitening wasnoted on the next day. Additionally, fluorescein angiogra-phy applied to group 5 at 24 hours demonstrated evidentchoroidal occlusion enlargement in comparison to earlyfluorescein angiography performed 6 hours after lightexposure. The delayed response is thought to be the resultof photochemical injury rather than thermal damage.21
Although choriocapillary occlusion was associated withsome degree of retinal pigment epithelium damage in ourstudy, such damage also occurred in other studies22–24 at
the lowest irradiation levels, even in the absence ofchoriocapillaris photodynamic therapy injury.25 The ex-tent of damage depended on the dose of light administeredand was confined to the treatment field, unlike the diffusedamage caused by the lateral transfer of heat accompany-ing laser photocoagulation. In addition, thermal laserphotocoagulation induces more extensive destruction ofthe retinal pigment epithelium than does photodynamictherapy, because the pigment epithelium is the mainabsorber of light energy in the former method, whereas thephotosensitizer is confined primarily to the targeted vascu-lature.
Indocyanine green is not toxic in animals, and the LD50after intravenous administration ranges from 50 to 80mg/kg.26 Although there are no equivalent data in hu-
FIGURE 5. Light and electron micrograph taken 9 days after light treatment. (Top left) A 18.9 J/cm2 lesion of group 3 (10 mg/kgof indocyanine green, 630 mW/cm2). Choriocapillaris was occluded with choroidal vessels remaining perfused. The outer nuclearlayer was intact, with no obvious damage to inner retinal layers (Toluidine blue, �200; bar: 10 �m). (Top right) A 12.6 J/cm2
lesion of group 4 (20 mg/kg of indocyanine green, 630 mW/cm2). An erythrocyte and fibrin (arrow) were filling the lumen of achoriocapillary. Retinal pigment epithelium cells were disrupted (Uranyl acetate, �8000; bar: 1 �m). (Bottom left, right) A 12.6J/cm2 lesion of group 4 (20 mg/kg of indocyanine green, 630 mW/cm2). Choriocapillaris endothelial cells showed cytoplasmprojections, infoldings, and vacuolization. Bruch membrane remained undamaged. Some endothelial cells of the choriocapillarisrevealed loss of tight junctions (arrow) (Uranyl acetate, �12k/�40k; bar: 500/100 nm).
AMERICAN JOURNAL OF OPHTHALMOLOGY562 OCTOBER 2001
mans, the maximum recommended human dose is 5 mg/kg,which may be an obstacle to clinical use. The disappear-ance rate of indocyanine green in healthy human subjectsis 18% to 24% per minute. The normal biological half-lifewas determined to be from 2.5 to 3 minutes, so single bloodsamples taken from healthy subjects 20 minutes afterinjection should contain no more than 4% of the initialconcentration of dye,27 eliminating the need for a 24-hourperiod of limited light exposure, as required for photody-
namic therapy with verteporfin. Indocyanine green is notmetabolized after injection and is excreted exclusively bymeans of the liver. It is not resorbed from the intestine anddoes not undergo enterohepatic circulation. The dye istaken from the plasma by the hepatic parenchymal cellsand secreted into the bile.28 Negligible uptake of the dyeoccurs in the kidneys, lungs, cerebrospinal fluid, andperiphery. Excretion by the kidney does not occur.29 Nodye can be detected in the spinal fluid.28 The safety of
FIGURE 6. (Top left) Light micrograph 2 days after light treatment of a 28.5 J/cm2 lesion of group 5 (20 mg/kg of indocyaninegreen, 950 mW/cm2). Complete choriocapillaris and eventual large choroidal vessel occlusion was achieved without hemorrhage.The photoreceptor layer showed vacuolization and edema. The inner retina appeared unchanged (Toluidine blue, �200; bar: 18�m). (Top right) Electron micrograph of the same lesion demonstrated the choriocapillaris filled with a combination of red bloodcells, neutrophils, platelets, and fibrin. The melanosomes were intact (white arrows), and some degree of retinal pigment epitheliumcells damage was found. Bruch membrane remained intact. There was damage to the outer retina with photoreceptor segmentsresembling ”rings“ (black arrow) (Uranyl acetate, �3000; bar: 2 �m). (Bottom left) The photoreceptor segments in highermagnification showed degeneration characterized by fusion of disk membranes with convoluted aspect, sometimes associated withthe internal segments structures (Uranyl acetate, �8000; bar: 1 �m). (Bottom right) Light micrograph taken 9 days after lighttreatment of a 28.5 J/cm2 lesion of group 5 (20 mg/kg of indocyanine green, 950 mW/cm2). Although the choriocapillaris remainedoccluded, the large choroidal vessels were perfused. In contrast to mild retinal damage observed after 2 days of light exposure, theouter retina was severely compromised, probably because of prolonged ischemia. The retinal pigment epithelium cells and thephotoreceptor segments were fully disrupted. The outer nuclear layer showed pyknosis and vacuolization (Toluidine blue, �200;bar: 20 �m).
CHORIOCAPILLARIS PHOTODYNAMIC THERAPYVOL. 132, NO. 4 563

intravenous indocyanine green in humans is well docu-mented, with severe adverse reactions occurring in only0.05% of recipients.30
Although peak concentration levels for the second-generation photodynamic agents (benzoporphyrins, pur-purins, phthalocyanines, mono-L-aspartyl-chlorine-6)were determined in an experimental study,15 the distribu-tion and retention of these drugs in human neovasculartissue is currently extrapolated from pretreatment fluores-cein angiography data that may not accurately reflect thebiodistribution of the sensitizer in the eye or its associatedtarget field. On an individual patient basis, it is theoreti-cally possible to couple the phototherapeutic properties ofindocyanine green with concomitant fundus imaging tooptimize disease treatment.
Therapy with some photodynamic ophthalmic agentsmay be limited by poor aqueous solubility, necessitatingliposomal or intralipid formulation and consequent intra-venous administration by slow infusion. In contrast, indo-cyanine green is a water-soluble tricarbocyanine dye thatcan be rapidly administered intravenously, thereby avoid-ing the long interval (10 minutes or more) required forslow infusion of a suspension preparation. This propertyalso enhances treatment practicality, by increasing patientcompliance and comfort.
In addition to having a high molecular weight (775 kD),indocyanine green is bound rapidly and almost completely(98%) to plasma proteins. Albumin was thought to be themajor carrier; however, in human serum, 80% of indocya-nine green has been demonstrated to be bound to globu-lins, probably �-1 lipoproteins,28,31 which enable vascularretention and minimal leakage from abnormal vessels.32
Like choroidal neovascularization, tumor neovasculature ishighly proliferative.33 The hyperproliferative neovascularendothelium exhibits enhanced permeability and elevatedlevels of specific albumin and scavenger receptors,34 as wellas low-density–lipoprotein receptors,35 leading to in-creased low-density–lipoprotein transport across endothe-lial junctions.36
To act as a photodynamic agent, the photosensitizermust be irradiated at the targeted tissue by nonthermallight at an absorption peak of the photosensitizer. Indo-cyanine green exhibits a high absorption cross-section inthe infrared region around 805 nm. Infrared light pene-trates deeper into tissue than red light,14 thereby confer-ring the advantage of enhanced membrane selectivity.
Taking into consideration that the model used does nothave vascularization equivalent to the human eye, partic-ularly on account of the avascular nature of the rabbitretina, this experimental study demonstrates the ability ofindocyanine green to effectively close the choriocapillariswith minimal damage to the neurosensory retina of pig-mented rabbits. Even with doses as high as 20 mg/kg,histopathologic examination revealed preservation of theneurosensory retinal architecture, with minimal loss ofvisual cells. Damage was largely confined to choriocapil-
laris endothelial cells and retinal pigment epithelium cells.With an increase of the indocyanine green dose from 10mg/kg to 20 mg/kg at appropriate light fluences, chorio-capillaris occlusion and outer blood–retinal barrier break-down in rabbits became more evident in fluoresceinangiograms. In this animal model, optimal lesions withminimal retinal damage could be achieved for both dyedoses with a light flux as low as 6.3 J/cm2. Membranetargetability, hydrophilic and fluorescent properties, andactivation at 805 nm suggest indocyanine green as apotential photosensitizer for choroidal neovascularization.Taken together, considering that experimental results willnot mimic the real and actual situation that occurred inhumans, these facts point toward further study of indocya-nine green–mediated photodynamic therapy for the treat-ment of choroidal vascular disease.
REFERENCES
1. Raab O. Uber die wirkung fluoreszierenden stoffen. InfusuriaZeitschrift Biologic 1900:524–546.
2. Dougherty TJ, Grindey GB, Fiel R, Weishaupt KR, BoyleDG. Photoradiation therapy II: cure of animals tumors withhematoporphyrin and light. J Natl Cancer Inst 1975;55:115–121.
3. Manyac MJ, Russo A, Smith PD, Glatstein E. Photodynamictherapy. J Clin Oncol 1988;6:380–391.
4. Gomer C. Photodynamic therapy in the treatment of malig-nancies. Semin Hematol 1989;26:27–31.
5. Miller JW, Schmidt-Erfurth U, Sickenberg M, et al. Photo-dynamic therapy with verteporfin for choroidal neovascular-ization caused by age-related macular degeneration. Resultsof a single treatment in a phase 1 and 2 study. ArchOphthalmol 1999;117:1161–1173.
6. Schmidt-Erfurth U, Miller JW, Sickenberg M, et al. Photo-dynamic therapy with verteporfin for choroidal neovascular-ization caused by age-related macular degeneration. Resultsof a retreatments in a phase 1 and 2 study. Arch Ophthalmol1999;117:1177–1187.
7. TAP Study Group. Photodynamic therapy of subfovealchoroidal neovascularization in age-related macular degen-eration with verteporfin. One-year results 2 randomizedtrials—report 1. Arch Ophthalmol 1999;117:1329–1345.
8. Marguerio RR, Marguerio AR, DeSantis ME. Laser treat-ments with verteporfin therapy and its potential impact onretinal practices. Retina 2000;20:325–330.
9. VIP Study Group. Verteporfin therapy of subfoveal choroidalneovascularization in age-related macular degeneration: two-year results of a randomized clinical trial including lesionswith occult with no classic choroidal neovascularization—verteporfin in photodynamic therapy report 2. Am J Oph-thalmol 2001;131:541–560.
10. Fox I, Brooker G, Heseltine D, Essex H, Wood E. New dyesfor continuous recording of dilution curves in whole bloodindependent of variations in blood oxygen saturation. Am JPhysiol 1956;187:599–606.
11. Flower R, Hochheimer B. Indocyanine green dye fluores-cence and infrared absorption choroidal angiography per-formed simultaneously with fluorescein angiography. JohnsHopkins Med J 1976;138:33–42.
12. Baumler W, Abels C, Karrer S, et al. Photo-oxidative killing
AMERICAN JOURNAL OF OPHTHALMOLOGY564 OCTOBER 2001
of human colonic cancer cells using indocyanine green andinfrared light. Br J Cancer 1999;80:360–363.
13. Paumgartner G, Probst P, Kraines R, Leevy C. Kinetics ofindocyanine green removal from the blood. NY Acad Sci1970;170:134–170.
14. Anderson R, Hu J, Parrish J. Optical radiation transfer intohuman skin. In: Marks R, Payne P, editors. Bioengeneeringand the skin. Boston: Lancaster MTP, 1981:253–265.
15. Grossweiner LI. The science of phototherapy. Boca Raton,FL.: CRC Press, 1994.
16. Reichel E, Puliafito C, Duker J, Guyer D. Indocyanine greendye enhanced diode photocoagulation of poorly definedsubfoveal choroidal neovascularization. Ophthalmic Surg1994;25:195–201.
17. Decoste S, Farinelli W, Flotte T, Anderson R. Dye-enhancedlaser welding for skin closure. Laser Surg Med 1992;12:25–32.
18. Henderson BW, Dougherty TJ. How does photodynamictherapy work? Photochem Photobiol 1992;55:145–157.
19. Roberts W, Hasan T. Role of neovasculature and vascularpermeability on the tumor retention of photodynamicagents. Cancer Res 1992;52:924–930.
20. Reindl S, Penzkofer A, Gong S-H, et al. Quantum yield oftriplet formation for indocyanine green. J Photochem Pho-tobiol A 1997;105:65–68.
21. Miller JW, Walsh AW, Kramer M, et al. Photodynamictherapy of experimental choroidal neovascularization usinglipoprotein-delivered benzoporphyrin. Arch Ophthalmol1995;113:810–818.
22. Wilson CA, Royster AJ, Tiedeman JS, Hatchell DL. Exuda-tive retinal detachment after photodynamic injury. ArchOphthalmol 1991;109:125–134.
23. Schmidt UE, Hasan T, Gragoudas E, et al. Vascular targetingin photodynamic occlusion of subretinal vessels. Ophthal-mology 1994;101:1953–1961.
24. Peyman GA, Moshfeghi DM, Moshfeghi A, et al. Photody-
namic therapy for choriocapillaris using tin ethyl etiopur-purin (SnET2). Ophthalmic Surg Lasers 1997;28:409–417.
25. Yao X-Y, Marmor MF. Induction of serous retinal detach-ment in rabbit eyes by pigment epithelial and choriocapillaryinjury. Arch Ophthalmol 1992;110:541–546.
26. Lutty GA. The acute intravenous toxicity of biologicalstains, dyes, and other fluorescent substances. Toxicol ApplPharmacol 1978;44:225–249.
27. Villeneuve JP, Huot R, Marleau D, Huet PM. Estimation ofhepatic blood flow with indocyanine green: comparisonbetween the continuous infusion and single injections meth-ods. Am J Gastroenterol 1982;77:233–237.
28. Paumgartner G. The handling of indocyanine green by theliver. Schweiz Med Wochensch 1975;105(suppl 17):1–30.
29. Cherrick GR, Stein SW, Leevy CM, Davidson CS. Indocya-nine green: observations on its physical properties, plasmadecay and hepatic extraction. J C1in Invest 1960;39:592–600.
30. Hope-Ross M, Yannuzzi LA, Gragoudas ES, et al. Adversereactions due to indocyanine green. Ophthalmology 1994;101:529–533.
31. Baker KJ. Binding of sulfobromophtalein (BSP) sodium andindocyanine green (ICG) by plasma alpha-1 lipoproteins.Proc Soc Exp Biol Med 1966;122:957–963.
32. Ham W, Sliney D. Retinal sensitivity to damage from shortwavelength light. Nature 1976;260:153–155.
33. Denekamp J. Vascular attack as a therapeutic strategy forcancer. Cancer Metastasis Rev 1990;9:267–282.
34. Schmidt U, Birngruber R, Hasan T. Seletive occlusion ofocular neovascularization by photodynamic therapy. Oph-thalmology 1992;89:391–394.
35. Rutledge J, Curry F, Blanche P, Krauss R. Solvent drag ofLDL across mammalian endothelial barriers with increasedpermeability. Am J Physiol 1995;268:H1982–H1991.
36. Schnitzer J, Carley W, Palade G. Albumin interacts with a60-kDa microvascular endothelial glycoprotein. Proc NatlAcad Sci 1988;85:6773–6777.
The full-text of AJO is now available online at www.ajo.com. AuthorsInteractive�, currently available in limited form, is undergoing an upgrade.
CHORIOCAPILLARIS PHOTODYNAMIC THERAPYVOL. 132, NO. 4 565