biodesign innovation
TRANSCRIPT

© 2016 Stanford Byers Center for Biodesign
Biodesign Program:Training approach and outcomes
NAE 2018 Annual MeetingPaul Yock

© 2016 Stanford Byers Center for Biodesign
The concept -- 2001
EDUCATION TRANSLATION
MED
TEC
H
Design Thinking
Entrepreneurship
Seed Funding
Mentoring, FacilitationO
ther
Ver
tical
s

© 2016 Stanford Byers Center for Biodesign
Innovation training philosophy…
Technology-push
0Technology 0Need
Need Pull
© 2016 Stanford Byers Center for Biodesign
Design thinking
empathize
define
ideate
prototype
testuser-centered
© 2016 Stanford Byers Center for Biodesign
What if your “user”is the 8-headed monstercalled healthcare?
Salon.com

© 2016 Stanford Byers Center for Biodesign© 2016 Stanford Byers Center for Biodesign
To deal with this complexity…
“The Biodesign Process”

© 2016 Stanford Byers Center for Biodesign
A well-characterized need is the DNA of a great invention!
Our mantra

Josh Makower
Todd Brinton Lyn Denend
Uday Kumar Jay Watkins Stefanos Zenios
Process & TrainingArchitects…

© 2016 Stanford Byers Center for Biodesign
Biodesign fellow teams
Identify >200 needs

© 2016 Stanford Byers Center for Biodesign
Need screening
Screen to the best few needs

© 2016 Stanford Byers Center for Biodesign© 2016 Stanford Byers Center for Biodesign
Need statement
A way to solve a specific problem…
in a well-characterized population…
in order to achieve a measurable outcome

© 2016 Stanford Byers Center for Biodesign© 2016 Stanford Byers Center for Biodesign
“A better way to detect potential rhythm disturbances
in non-hospitalized patients with suspected arrhythmias
to improve the patient experience and reduce the cost of diagnosis”
Need statement

© 2016 Stanford Byers Center for Biodesign
NOW it’s time to invent!
“Given enough time, sugar and caffeine, you will invent something!”

© 2016 Stanford Byers Center for Biodesign© 2016 Stanford Byers Center for Biodesign
Brainstorming the Zio patch…
© 2016 Stanford Byers Center for Biodesign© 2016 Stanford Byers Center for Biodesign
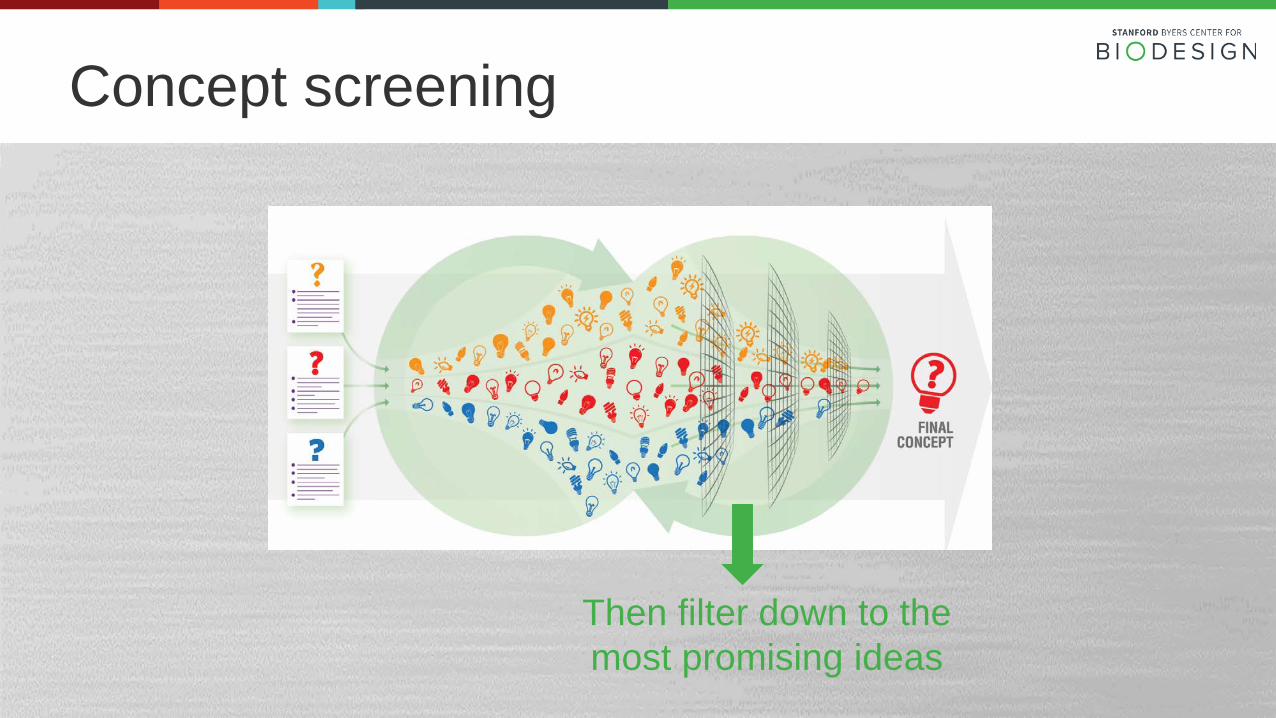
Concept screening
Then filter down to the most promising ideas

© 2016 Stanford Byers Center for Biodesign© 2016 Stanford Byers Center for Biodesign
Final phase: Implementation planning
© 2016 Stanford Byers Center for Biodesign
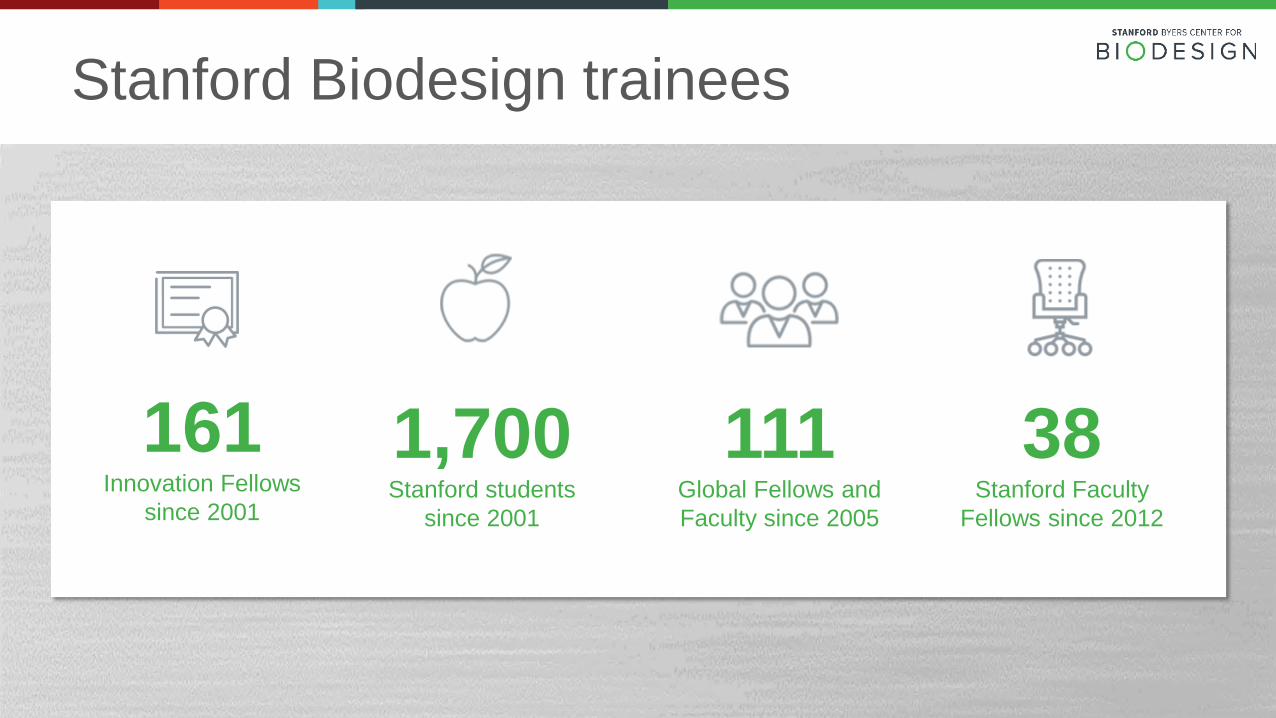
Stanford Biodesign trainees
161Innovation Fellows
since 2001
1,700Stanford students
since 2001
111Global Fellows and Faculty since 2005
38Stanford Faculty
Fellows since 2012

© 2016 Stanford Byers Center for Biodesign
Learning resources…
ebiodesign.org

© 2016 Stanford Byers Center for Biodesign 19
Stanford-India Biodesign
© 2016 Stanford Byers Center for Biodesign
Singapore

© 2016 Stanford Byers Center for Biodesign
Japan
© 2016 Stanford Byers Center for Biodesign
Translational Outcomes
Kate Garrett (‘12)Founder, CEO, Ciel MedicalVP Airway Technologies, Vyaire Medical
© 2016 Stanford Byers Center for Biodesign 23
© 2016 Stanford Byers Center for Biodesign
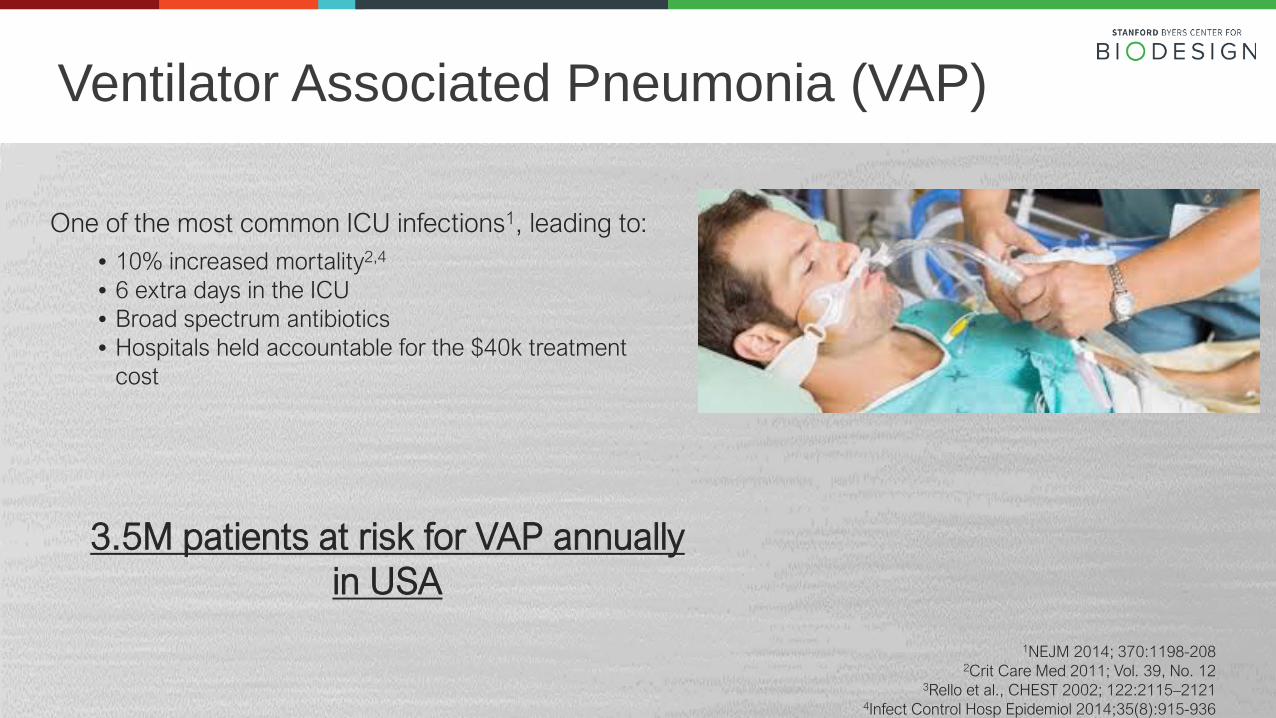
1NEJM 2014; 370:1198-2082Crit Care Med 2011; Vol. 39, No. 12
3Rello et al., CHEST 2002; 122:2115–21214Infect Control Hosp Epidemiol 2014;35(8):915-936
One of the most common ICU infections1, leading to:• 10% increased mortality2,4
• 6 extra days in the ICU• Broad spectrum antibiotics • Hospitals held accountable for the $40k treatment
cost
Ventilator Associated Pneumonia (VAP)
3.5M patients at risk for VAP annually in USA
© 2016 Stanford Byers Center for Biodesign
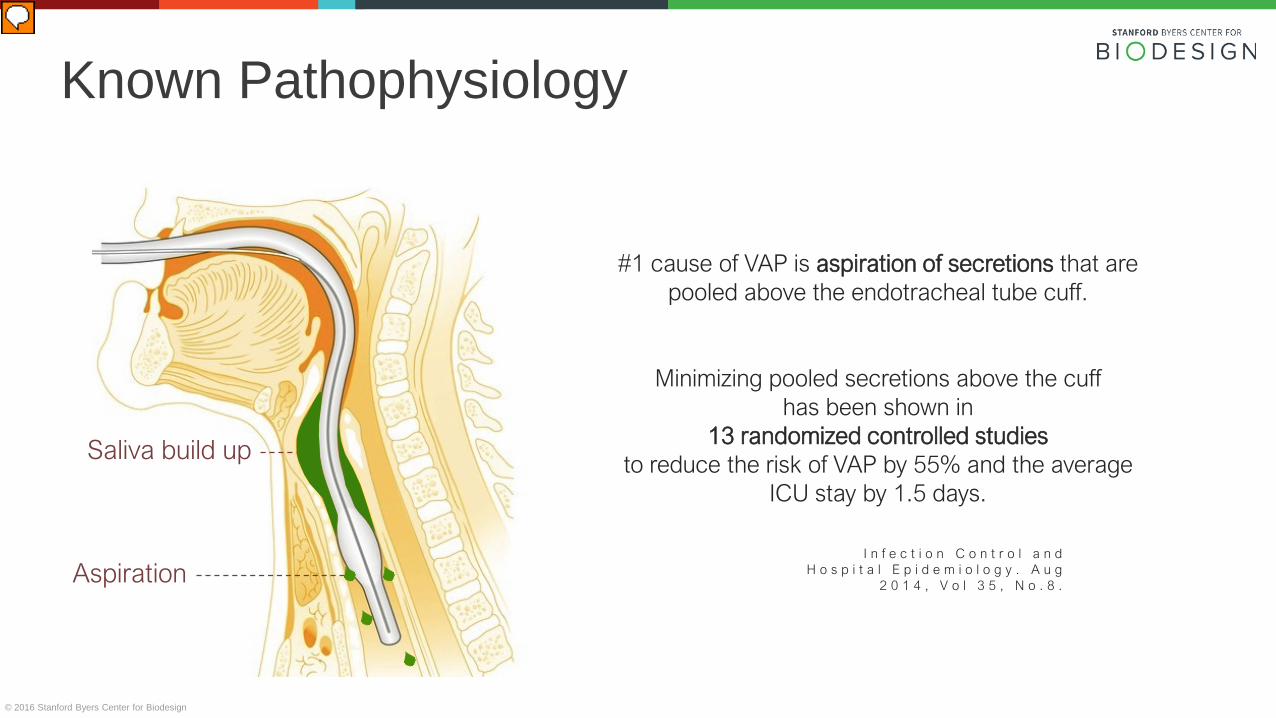
Saliva build up
Aspiration
#1 cause of VAP is aspiration of secretions that are pooled above the endotracheal tube cuff.
Minimizing pooled secretions above the cuff has been shown in
13 randomized controlled studiesto reduce the risk of VAP by 55% and the average
ICU stay by 1.5 days.
I n f e c t i o n C o n t r o l a n d H o s p i t a l E p i d e m i o l o g y . A u g
2 0 1 4 , V o l 3 5 , N o . 8 .
Known Pathophysiology

© 2016 Stanford Byers Center for Biodesign 26
Catheter coils in mouth
Aspiration risk persists.

© 2016 Stanford Byers Center for Biodesign
An improved endotracheal tube to reduce the risk of aspiration in ventilated patients
Need statement
© 2016 Stanford Byers Center for Biodesign
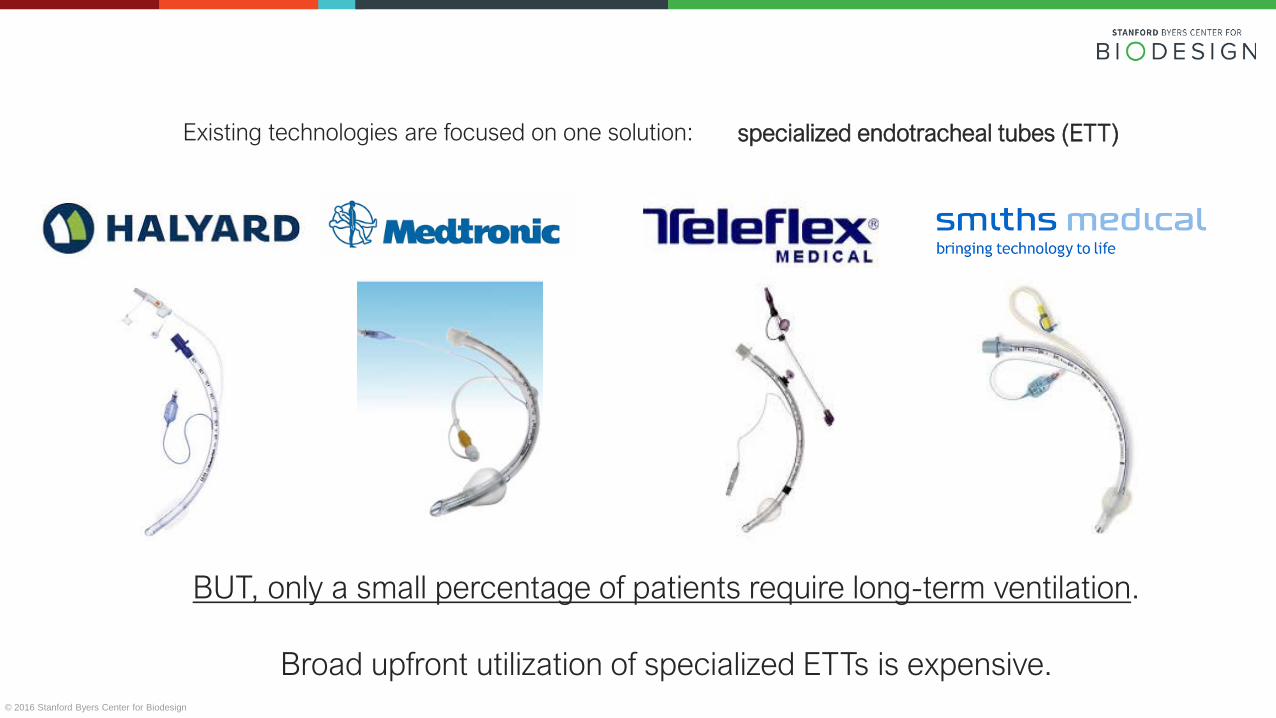
BUT, only a small percentage of patients require long-term ventilation.
Broad upfront utilization of specialized ETTs is expensive.
Existing technologies are focused on one solution: specialized endotracheal tubes (ETT)
© 2016 Stanford Byers Center for Biodesign
A way to reduce the risk of aspiration in long-term intubated patients that can be applied post-intubation.
An improved endotracheal tube to reduce the risk of aspiration in ventilated patients.
Need statement

© 2016 Stanford Byers Center for Biodesign
Sherpa Suction SystemTM

© 2016 Stanford Byers Center for Biodesign
Clinical Studies / Early Customer Adoption
R&D / Manufacturing FDA
Animal studies
30+ cadavers
Injection mold tooling
Commercial Launch
V&V
Biocompatibility
Sterility
Documentation
Product evaluations
Poster presentations
Value analysis assessments
Multi-center trials
Acquisition by Vyaire Medical
April 2017

© 2016 Stanford Byers Center for Biodesign 32
© 2016 Stanford Byers Center for Biodesign 33
The best measure of translational impact:
premiermhc.com; ahrq.gov; consultqd.clevelandclinic.org
Patients Reached!

© 2016 Stanford Byers Center for Biodesign 34

© 2016 Stanford Byers Center for Biodesign
Lymph/Axis
BRÜNSo Far…

© 2016 Stanford Byers Center for Biodesign© 2016 Stanford Byers Center for Biodesign
Our “product”

BRYANT LINInternal Med, Stanford
VENITA CHANDRAClinical Associate Professor
Vascular Surgery
ROSS VENOOKLecturer,
Bioengineering
TODD BRINTONClinical Professor,
Cardiovascular Medicine
RYAN VAN WERTClinical Assistant Professor
Pulmonology
DAN AZAGURYAssistant Professor,
Surgery
DAVID CAMARILLOAssistant Professor,
Bioengineering
SID SINHAAssistant Professor,
Gastrointestinal Medicine
JAMES WALLAssistant Professor,
Surgery
Biodesign fellow alums now on Stanford faculty
JANENE FUERCHClinical Assistant Professor,
Neonatology
Bryant LinClinical Assistant Professor,
Medicine

© 2016 Stanford Byers Center for Biodesign
DukeNandan Lad
Cornell Akhilesh Sista
OregonJonathan Steinberger
MinnesotaMarie Johnson
NorthwesternS Gnanashanmugam
UC San DiegoGarrett Smith
Cleveland ClinicShubhayu Basu
Alums who have started & lednew Biodesign-like programs

Alumni pool includes 30 current start-up CEO’s…

© 2016 Stanford Byers Center for Biodesign
Challengesahead…
© 2016 Stanford Byers Center for Biodesign© 2016 Stanford Byers Center for Biodesign
• new technology is driving healthcare expense!
• diminished venture funding
• weak pipeline of technologies for patient care
A perfect storm for medtechinnovation…
© 2016 Stanford Byers Center for Biodesign© 2016 Stanford Byers Center for Biodesign
Value-Based Innovation
Can we develop a discipline of inventing biomedical technologies with a focus on maximizing value (health benefit:cost?)

© 2016 Stanford Byers Center for Biodesign© 2016 Stanford Byers Center for Biodesign
Adjusting the process…
Value Proposition

© 2016 Stanford Byers Center for Biodesign© 2016 Stanford Byers Center for Biodesign
Adjusting the process…
Value exploration!
© 2016 Stanford Byers Center for Biodesign© 2016 Stanford Byers Center for Biodesign
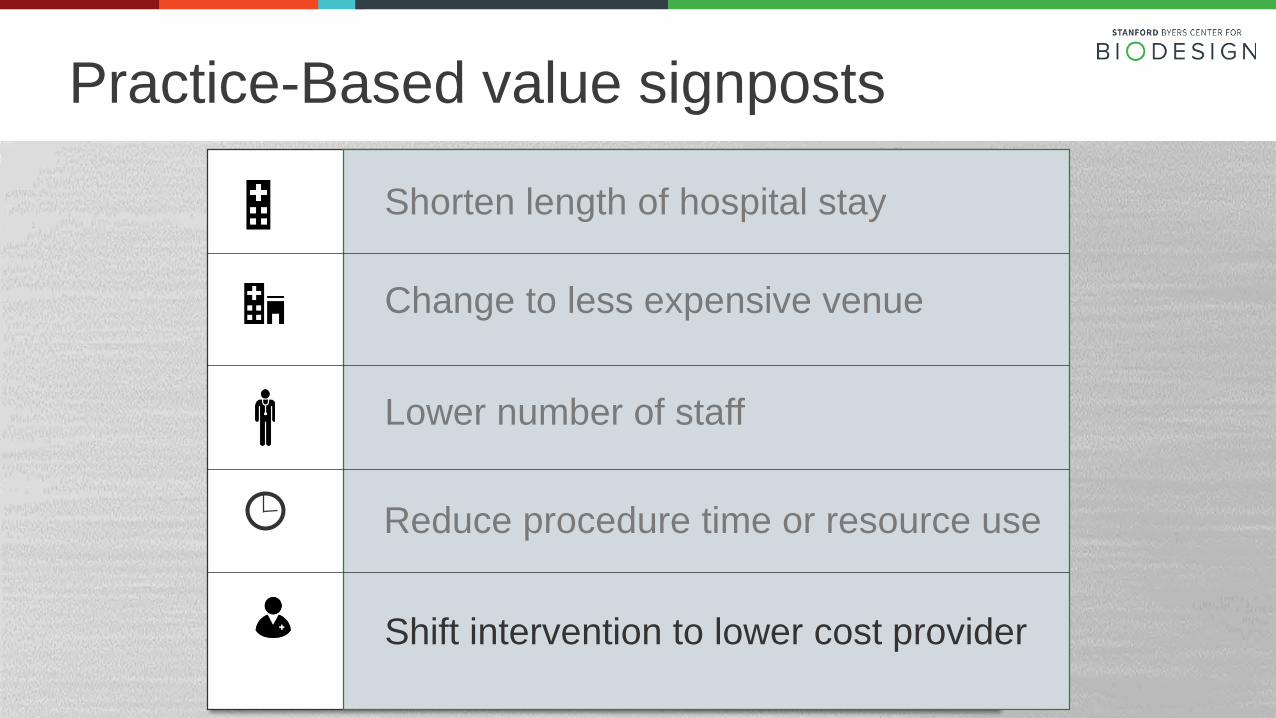
Practice-Based value signposts
Shorten length of hospital stay
Change to less expensive venue
Lower number of staff
Reduce procedure time or resource use
Shift intervention to lower cost provider

© 2016 Stanford Byers Center for Biodesign© 2016 Stanford Byers Center for Biodesign
patient withpalpitations
internist
cardiologist
electrophysiologist
Holter
The economic need
© 2016 Stanford Byers Center for Biodesign
Saving $620 perAF patient per year

© 2016 Stanford Byers Center for Biodesign
Challenges, continued
Team dynamics…including diversity issues

© 2016 Stanford Byers Center for Biodesign
The Biodesign “Shrink”Doug Rait, PhDDirector, Team Learning & Design
Team dynamics

© 2016 Stanford Byers Center for Biodesign
Mix of engineers and physicians
• Different perceptions of risk (medical, technical)
• Different approaches to decision making
• Stress is compounded by flat team structure

© 2016 Stanford Byers Center for Biodesign
Mix of academic and industry culture
• Learning a process… or inventing a product?
• Exploring openly… or delivering on milestones?
• Sharing discoveries… or protecting I.P.?

© 2016 Stanford Byers Center for Biodesign
Gender-based issues
22% of fellows experienced (and 41% observed) problematic workplace issues – largely gender based—during the year.
Anonymous survey of alumni fellows, 2017:
Biodesign Diversity Task ForceKate Garrett, Chair
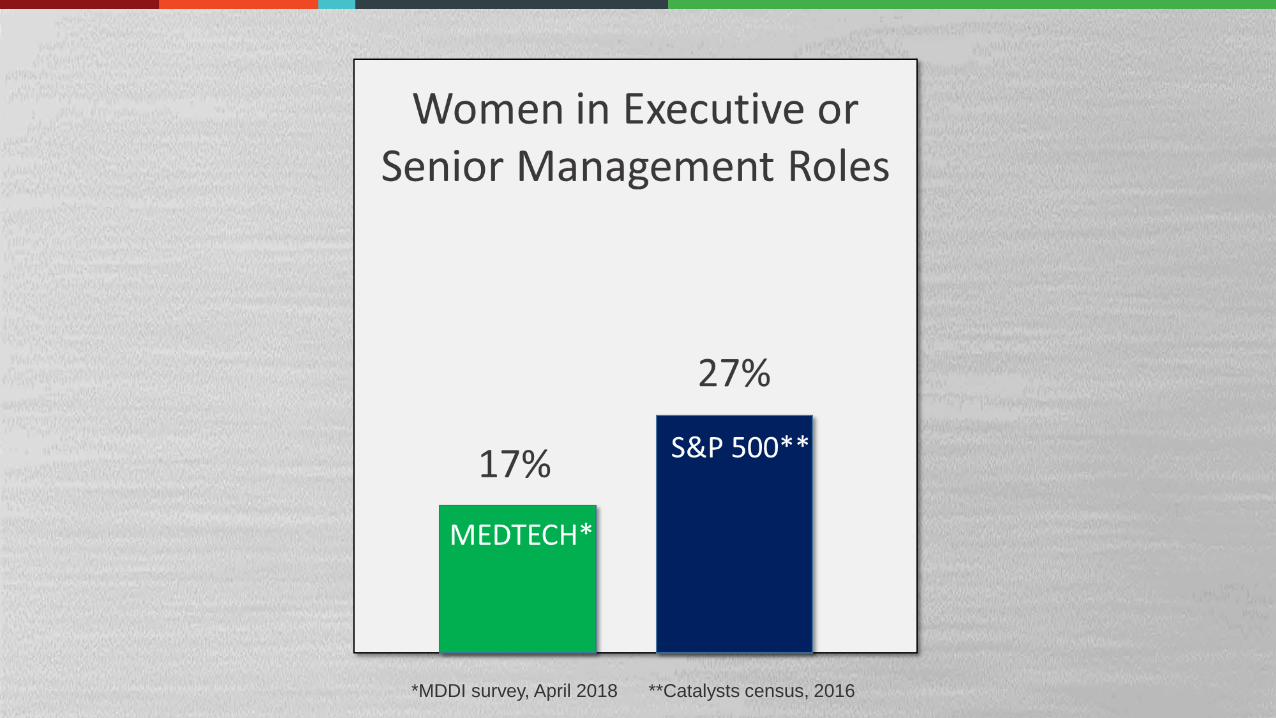
© 2016 Stanford Byers Center for Biodesign*MDDI survey, April 2018 **Catalysts census, 2016
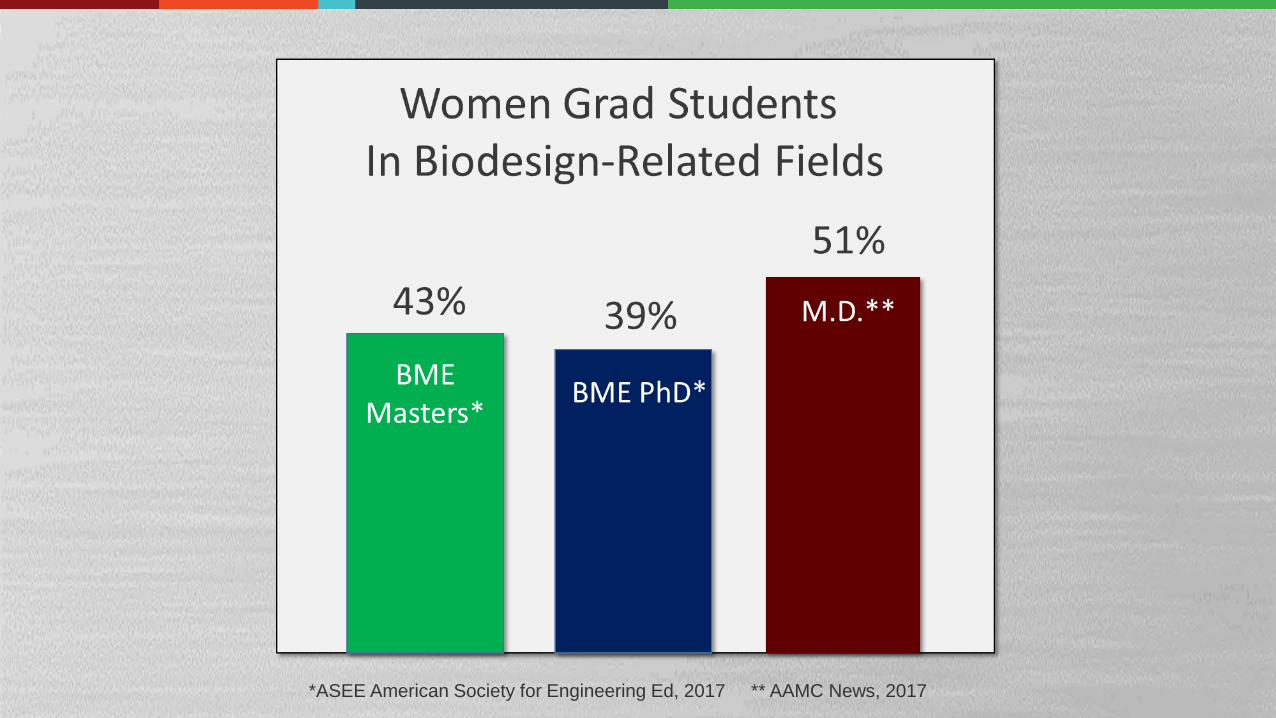
© 2016 Stanford Byers Center for Biodesign*ASEE American Society for Engineering Ed, 2017 ** AAMC News, 2017

© 2016 Stanford Byers Center for Biodesign
The opportunity for Biodesign…

© 2016 Stanford Byers Center for Biodesign
2018-19 Innovation fellows

© 2016 Stanford Byers Center for Biodesign
Questions…comments?