90 y radioembolization versus chemoembolization in the treatment of hepatocellular carcinoma: an...
TRANSCRIPT

part of
435ISSN 2042-630510.2217/CER.13.37 © 2013 Future Medicine Ltd 2(4), 435–444 (2013)
Locoregional catheter-based therapies for unresectable hepatocellular carcinoma (HCC) include conventional transarterial chemoembolization (cTACE), drug-eluting bead chemoembolization and yttrium-90 (90Y) radio-embolization. Although current guidelines recommend cTACE for inoperable HCC, comparative effectiveness of drug-eluting bead chemo embolization and 90Y radioembolization in the management of HCC remains undefined due to the lack of data evaluating safety and effectiveness among these therapies. A comprehensive search of the literature was carried out for studies examining comparative effectiveness of cTACE and 90Y based on objective tumor response and overall patient survival. Further data on efficacy, safety, toxicity and cost–effectiveness was also examined. The National Cancer Institute Levels of Evidence for Cancer Treatment Studies provided a useful framework for the critical understanding and stratification of current evidence on locoregional therapy for unresectable HCC. Based on current retrospective cohort studies, evidence for similar efficacy and safety between cTACE and 90Y radioembolization was demonstrated. Further prospective, randomized studies are required to validate these observations and to analyze cost–effectiveness of these interventions in unresectable HCC patients for definitive recommendations to be made.
KEYWORDS: carcinoma n chemoembolization n comparative effectiveness n drug-eluting bead chemoembolization n hepatocellular n radioembolization n yttrium-90
Hepatocellular carcinoma (HCC) is the third leading cause of cancer mortality world-wide, and a rapidly rising global disease burden with 748,300 new cases diagnosed yearly [1,2]. The incidence of HCC in the USA has doubled in recent decades [3] and this may be attributed to the increasing prevalence of chronic hepatitis C, alcoholic cirrhosis, nonalcoholic fatty liver disease (NAFLD) and metabolic syndrome [2,4].
In considering evidence-based HCC management, both US and European clinical guidelines endorse surgical resection for patients with solitary nodules and well-preserved liver function; liver transplantation for patients with tumors that meet the Milan criteria (single nodules ≤5 cm or up to three nodules <3 cm); and percutane-ous radiofrequency ablation (RFA) for appropriately sized and located inoperable tumors [5,6]. Unfortunately, the majority of HCCs are diagnosed beyond Barcelona Clinic Liver Cancer (BCLC) Stage A at the intermediate or advanced stages when ablation and curative surgery, including liver transplantation, are no longer feasible [7]. For such patients with BCLC Stage B (intermediate; multinodular asymptomatic tumors without vascular invasion or extrahepatic spread) or BCLC stage C tumors (advanced; solitary tumors invading segmental or lobar branch of the portal vein), locoregional therapies, such as transarterial chemoembolization (TACE) and/or sorafenib, have been shown to positively impact survival and have been cited as the standard of care [5,8,9].
90Y radioembolization versus chemoembolization in the treatment of hepatocellular carcinoma: an analysis of comparative effectiveness
Minzhi Xing1, Nima Kokabi1, Juan C Camacho1, David A Kooby2,3, Bassel F El-Rayes3,4 & Hyun S Kim*1,3,4
1Division of Interventional Radiology & Image Guided Medicine, Department of Radiology & Imaging Sciences, Emory University School of Medicine, GA, USA 2Division of Surgical Oncology, Department of Surgery, Emory University School of Medicine, GA, USA 3Winship Cancer Institute, Emory University, GA, USA 4Department of Hematology & Medical Oncology, Emory University School of Medicine, GA, USA *Author for correspondence: Tel.: +1 404 712 7033 Fax: +1 404 712 7970 [email protected]
REVIEWFor reprint orders, please contact: [email protected]

J. Compar. Effect. Res. (2013) 2(4) future science group436
review Xing, Kokabi, Camacho, Kooby, El-Rayes & Kim
In recent years, transarterial radioembolization using b-emitting yttrium-90 (90Y) integrated in glass matrix or resin microspheres has been devel-oped as an alternative to TACE for locoregional therapy [6]. Although current data support the use of 90Y radioembolization for intermediate and advanced HCC, uncertainty precludes its definitive recommendation as a standard of care [5]. The lack of prospective randomized studies comparing outcomes of HCC patients treated with chemoembolization versus radioemboli-zation contributes to this uncertainty [10]. The objective of this article is to critically review cur-rent evidence and compare the efficacy, safety and cost–effectiveness of TACE and 90Y radioem-bolization in HCC therapy in order to evaluate treatment strategies for regulatory purposes and potential applications in clinical practice.
MethodsStudies were identified using a PubMed and Cochrane Library Database search with the following keywords: ‘‘hepatocellular carci-noma’’ or ‘‘HCC’’ or ‘‘hepatic tumor’’ or ‘‘liver tumor’’ or ‘‘hepatic cancer’’ or ‘‘liver cancer’’ and ‘‘TACE’’ or “DEB-TACE” or “chemoem-bolization’’ or “90Y” or ‘‘radioembolization’’ and ‘‘clinical trials’’ in English. A manual search of general reviews on HCC and references from published clinical trials was also carried out. In total, 615 articles from 1988 to January 2013 were collected.
Articles were excluded if they dealt with liver metastases, recurrence of HCC after hepatec-tomy or sorafanib treatment, if they did not relate to therapeutic interventions (e.g., a com-parison of diagnostic methods), if they did not include intermediate or advanced disease (i.e., BCLC Stage B or C), or if they did not report sufficient data (listed below).
Following these exclusions we evaluated 40 articles. From each, the following informa-tion was extracted using a structured proforma:
■ Country of origin, duration of trial, number of patients;
■ Patient characteristics, etiology and severity of underlying liver disease, and tumor extent;
■ Transarterial treatment used: anticancer drugs and 90Y microspheres, dosage and delivery, embolization method, schedule and number of courses, selectivity of the procedure, hospital stay and periprocedural care;
■ Outcomes investigated included: overall sur-vival, tumor response and complications.
Objective tumor response (including com-plete response and partial response) was noted in each study using data based on the follow-ing standardized response criteria: The WHO, European Association for the Study of the Liver (EASL) guidelines, Response Evaluation Criteria in Solid Tumors (RECIST) guidelines, or modi-fied RECIST (mRECIST) guidelines. Child–Pugh scores were noted as a common indica-tor of severity of disease and for comparison of groups receiving differing treatment modalities. The majority of studies did not include definitive BCLC staging.
Among 40 articles, six directly compared 90Y radioembolization with conventional TACE, nine evaluated 90Y radioembolization alone and the remaining 25 evaluated conventional TACE or drug-eluting bead (DEB)-TACE. None of the articles directly compared the efficacy of DEB-TACE to 90Y radioembolization.
Evidence was stratified according to the Levels of Evidence for Pediatric and Adult Cancer Treatment Studies by the National Cancer Institute (NCI) Physician Data Query (PDQ®) in Table 1. This formal description of the lev-els of evidence is a uniform framework for data analysis in cancer therapy for therapeutic recom-mendations to be made. Evidence-based report-ing systems such as the Consolidated Standards for Reporting of Trials (CONSORT) and PICO were developed to facilitate authors’ presentation of trials in a structured and complete manner, while assessors use different tools for the deter-mination of trial quality. Key similarities such as evidence stratification based on study design exist between the NCI PDQ and other grad-ing systems such as the Dutch EBRO guidelines and Grading Recommendations Assessment, Development and Evaluation (GRADE). However, the NCI PDQ additionally evalu-ates evidence based on study end points such as overall survival and cause-specific mortality, allowing further stratification based on outcome measures studied, which is of particular interest for the evaluation of evidence in clinical inter-ventions for cancer therapy.
Results & discussion ■ Transarterial chemoembolization
The initial description of conventional TACE (cTACE) was made by Yamada et al. in 1980

90Y radioembolization versus chemoembolization in the treatment of hepatocellular carcinoma review
future science group www.futuremedicine.com 437
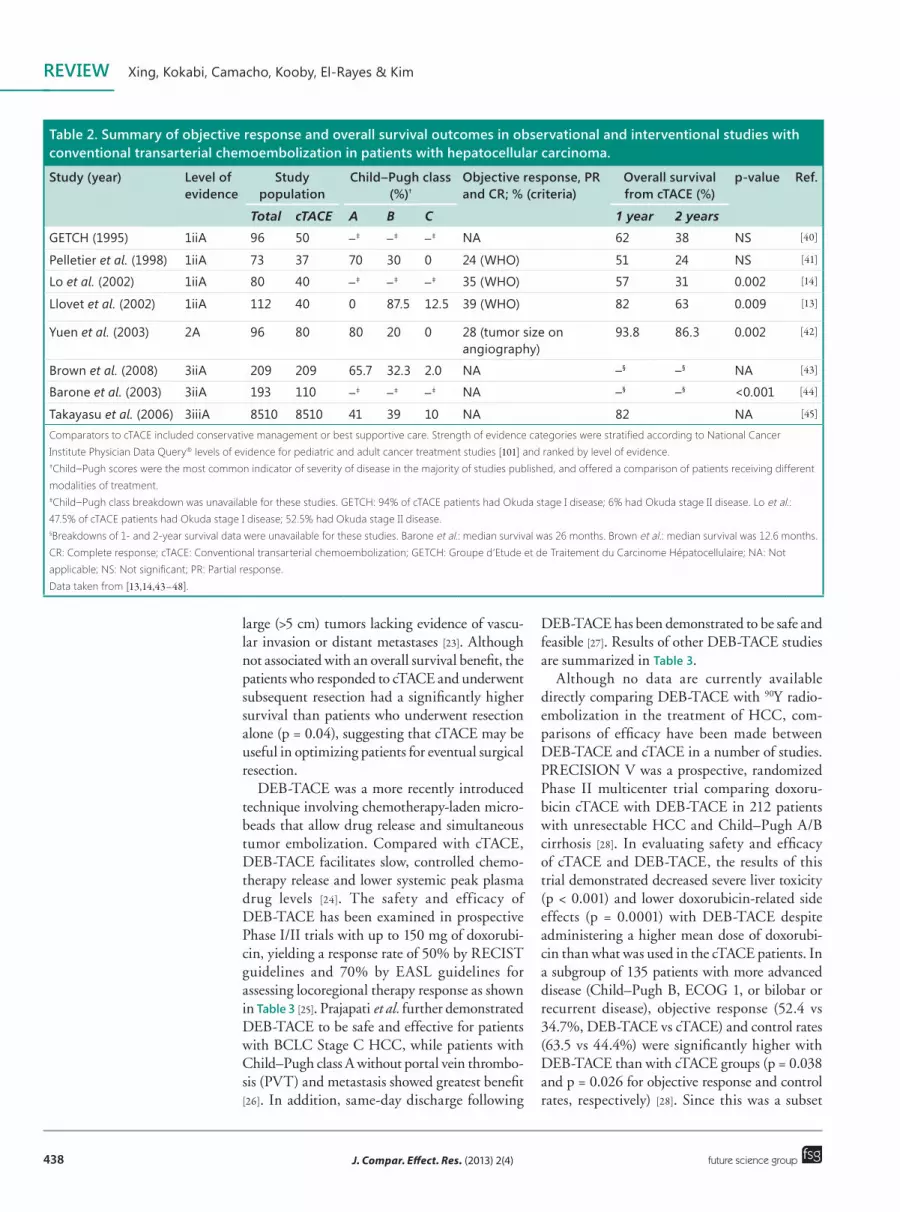
involving transcatheter administration of che-motherapy and concurrent embolization via the hepatic artery [11]. In addition to minimizing vascular washout of chemotherapy, emboliza-tion-induced hypoxia potentially reduces the tumor cell’s ability to eliminate intracellular drugs. This prolongs cancer contact with che-motherapy and induces high levels of local che-motherapy while minimizing systemic exposure [12]. Recent data for studies examining cTACE as a treatment for HCC are found in Table 2, with the comparator being best supportive care or conservative management of HCC.
Several prospective randomized trials have established that locoregional therapy using cTACE confers a survival advantage over best supportive care for patients with intermediate stage HCC. Llovet et al. compared doxorubi-cin cTACE or transarterial embolization (TAE) with best supportive care in 112 patients with unresectable HCC and well-preserved liver func-tion and found increased survival with cTACE (29% with cTACE vs 17% with symptomatic treatment) [13]. Lo et al. examined 80 patients receiving cisplatin cTACE versus best support-ive care and demonstrated a survival benefit of 26% with cTACE compared to 3% with best supportive care at 3 years. Although these tri-als represent the best data for cTACE, limita-tions included highly selected patients and low
power [14]. Nonetheless, cTACE remains the most well-examined and commonly used locore-gional therapy for unresectable HCC [10]. It is now the accepted standard-of-care for regional therapy in HCC patients with preserved liver function whose disease is not amenable to surgi-cal resection or transplantation [15].
cTACE has also shown favorable results for downstaging of patients prior to liver transplant. Patients who are downstaged successfully with cTACE protocols demonstrate a similar post-transplant survival time as those who initially meet the Milan criteria [16–18]. This has estab-lished cTACE as an accepted method of con-ferring eligibility for transplant in patients with HCC exceeding the Milan criteria [19].
Given existing prolonged wait times (median: 13 months) for scheduled transplants [20], cTACE has been used as a bridge to liver transplantation to prevent disease progression beyond the Milan criteria [21]. Although pretransplant cTACE is performed extensively, there is a lack of prospec-tive randomized trials characterizing survival [19]. Bridging cTACE may also allow the identification of patients with more aggressive tumors who prog-ress despite therapy and are therefore unlikely to benefit from transplant [22]. In a nonrandomized, prospective analysis of 168 consecutive patients, Luo et al. compared cTACE and hepatic resection as two options for treating patients with multiple
Table 1. Levels of evidence for pediatric and adult cancer treatment studies.
Types of study design and relevant end points Strength of evidence
Study design (decreasing order of strength)
Randomized controlled trial: ■ Double-blinded ■ Nonblinded treatment delivery
1i1ii
Nonrandomized controlled trial 2
Case series: ■ Population-based ■ Consecutive, nonpopulation-based ■ Nonconsecutive, nonpopulation-based
3i3ii3iii
End points (decreasing order of strength)
Total mortality (or overall survival from a defined time) A
Cause-specific mortality (or cause-specific mortality from a defined time) B
Carefully assessed quality of life C
Indirect surrogates: ■ Event-free survival ■ Disease-free survival ■ Progression-free survival ■ Tumor response rate
DiDiiDiiiDiv
Adapted from [101].
J. Compar. Effect. Res. (2013) 2(4) future science group438
review Xing, Kokabi, Camacho, Kooby, El-Rayes & Kim
large (>5 cm) tumors lacking evidence of vascu-lar invasion or distant metastases [23]. Although not associated with an overall survival benefit, the patients who responded to cTACE and underwent subsequent resection had a significantly higher survival than patients who underwent resection alone (p = 0.04), suggesting that cTACE may be useful in optimizing patients for eventual surgical resection.
DEB-TACE was a more recently introduced technique involving chemotherapy-laden micro-beads that allow drug release and simultaneous tumor embolization. Compared with cTACE, DEB-TACE facilitates slow, controlled chemo-therapy release and lower systemic peak plasma drug levels [24]. The safety and efficacy of DEB-TACE has been examined in prospective Phase I/II trials with up to 150 mg of doxorubi-cin, yielding a response rate of 50% by RECIST guidelines and 70% by EASL guidelines for assessing locoregional therapy response as shown in Table 3 [25]. Prajapati et al. further demonstrated DEB-TACE to be safe and effective for patients with BCLC Stage C HCC, while patients with Child–Pugh class A without portal vein thrombo-sis (PVT) and metastasis showed greatest benefit [26]. In addition, same-day discharge following
DEB-TACE has been demonstrated to be safe and feasible [27]. Results of other DEB-TACE studies are summarized in Table 3.
Although no data are currently available directly comparing DEB-TACE with 90Y radio-embolization in the treatment of HCC, com-parisons of efficacy have been made between DEB-TACE and cTACE in a number of studies. PRECISION V was a prospective, randomized Phase II multicenter trial comparing doxoru-bicin cTACE with DEB-TACE in 212 patients with unresectable HCC and Child–Pugh A/B cirrhosis [28]. In evaluating safety and efficacy of cTACE and DEB-TACE, the results of this trial demonstrated decreased severe liver toxicity (p < 0.001) and lower doxorubicin-related side effects (p = 0.0001) with DEB-TACE despite administering a higher mean dose of doxorubi-cin than what was used in the cTACE patients. In a subgroup of 135 patients with more advanced disease (Child–Pugh B, ECOG 1, or bilobar or recurrent disease), objective response (52.4 vs 34.7%, DEB-TACE vs cTACE) and control rates (63.5 vs 44.4%) were significantly higher with DEB-TACE than with cTACE groups (p = 0.038 and p = 0.026 for objective response and control rates, respectively) [28]. Since this was a subset
Table 2. Summary of objective response and overall survival outcomes in observational and interventional studies with conventional transarterial chemoembolization in patients with hepatocellular carcinoma.
Study (year) Level of evidence
Study population
Child–Pugh class (%)†
Objective response, Pr and Cr; % (criteria)
Overall survival from cTACe (%)
p-value ref.
Total cTACE A B C 1 year 2 years
GETCH (1995) 1iiA 96 50 –‡ –‡ –‡ NA 62 38 NS [40]
Pelletier et al. (1998) 1iiA 73 37 70 30 0 24 (WHO) 51 24 NS [41]
Lo et al. (2002) 1iiA 80 40 –‡ –‡ –‡ 35 (WHO) 57 31 0.002 [14]
Llovet et al. (2002) 1iiA 112 40 0 87.5 12.5 39 (WHO) 82 63 0.009 [13]
Yuen et al. (2003) 2A 96 80 80 20 0 28 (tumor size on angiography)
93.8 86.3 0.002 [42]
Brown et al. (2008) 3iiA 209 209 65.7 32.3 2.0 NA –§ –§ NA [43]
Barone et al. (2003) 3iiA 193 110 –‡ –‡ –‡ NA –§ –§ <0.001 [44]
Takayasu et al. (2006) 3iiiA 8510 8510 41 39 10 NA 82 NA [45]
Comparators to cTACE included conservative management or best supportive care. Strength of evidence categories were stratified according to National Cancer Institute Physician Data Query® levels of evidence for pediatric and adult cancer treatment studies [101] and ranked by level of evidence. †Child–Pugh scores were the most common indicator of severity of disease in the majority of studies published, and offered a comparison of patients receiving different modalities of treatment. ‡Child–Pugh class breakdown was unavailable for these studies. GETCH: 94% of cTACE patients had Okuda stage I disease; 6% had Okuda stage II disease. Lo et al.: 47.5% of cTACE patients had Okuda stage I disease; 52.5% had Okuda stage II disease. §Breakdowns of 1- and 2-year survival data were unavailable for these studies. Barone et al.: median survival was 26 months. Brown et al.: median survival was 12.6 months. CR: Complete response; cTACE: Conventional transarterial chemoembolization; GETCH: Groupe d’Etude et de Traitement du Carcinome Hépatocellulaire; NA: Not applicable; NS: Not significant; PR: Partial response. Data taken from [13,14,43–48].

90Y radioembolization versus chemoembolization in the treatment of hepatocellular carcinoma review
future science group www.futuremedicine.com 439
analysis with limited numbers, further prospective randomized studies with both time-to-progression and survival data are necessary to draw definitive conclusions about the superiority of DEB-TACE to cTACE in intermediate and advanced HCC.
■ Transarterial radioembolizationTransarterial radioembolization involves admin-istration of 90Y-labeled embolic microspheres. 90Y is a pure b-emitter with mean liver tissue penetra-tion of 2.5 mm (maximum 10 mm) and a half-life of 64.2 h (2.67 days). 90Y radioembolization can deliver high levels of radiation (200–300 Gy) via selective permeation of vessels while minimiz-ing exposure to nontumorous liver parenchyma [29]. TheraSpheres® (glass microsphere; MDS Nordion, Kanata, ON, Canada) were approved by the US FDA in 1999 under a humanitarian device exemption for the treatment of unresect-able HCC in patients with appropriately posi-tioned hepatic arterial catheters. SIR-Spheres® (resin microsphere; Sirtex Medical, Lane Cove, Australia) were granted full premarketing approval in 2002 by the FDA for the treatment
of colorectal metastases in conjunction with intra-hepatic floxuridine (FDUR). Given the mean diameter of <60 µm for both products, absolute contraindications to therapy include excessive hepatopulmonary and demonstrable gastrointes-tinal deposition that may cause radiation pneumo-nitis and gastrointestinal ulceration, respectively [30]. Extensive pretreatment planning including mesenteric and visceral angiography, dosimetry planning (transarterial 99Tc-macroaggregated albumin [MAA] study for pulmonary shunting), and occlusion of potential enteric channels, such as the g astroduodenal artery, are thus required [31].
90Y radioembolization has been noted to be particularly appealing for patients in-between intermediate and advanced disease, as well as for patients who minimally exceed resection, abla-tion or transplant criteria [32], and may be useful for patient progression to TACE or sorafenib. The efficacy and safety of 90Y radioembolization is increasingly being evidenced in single- and multi-center observational studies [33,34]. Table 4 illus-trates available data on 90Y radioembolization and compares its efficacy and outcomes to cTACE.
Table 3. Summary of objective response and overall survival outcomes in observational and interventional studies with drug-eluting bead transarterial chemoembolization in patients with hepatocellular carcinoma.
Study (year) Level of evidence
Study population Child–Pugh class (%)†
Objective response, Pr and Cr; % (criteria)
Overall survival at 2 years from DeB-TACe (%)
ref.
Total DEB‑TACE A B C
Sacco et al. (2011) 1iiA 67 33 29 4 0 100 (RECIST) 86.8 [46]
Lammer et al. (2010) PRECISION V
1iiDiv 212 102 83 19 0 53 (RECIST) NA [28]
Forner et al. (2009) 2Div 55 24 24 0 0 50 (RECIST) NA [47]
Reyes et al. (2009) 2Div 20 20 15 5 0 10 (RECIST), 60 (EASL) 55 [48]
Dhanasekaran et al. (2010)
3iiA 71 45 22 11 12 NA 40 [49]
Prajapati et al. (2012) 3iiA 121 121 60.3 39.7 0 NA –‡ [27]
Kalva et al. (2011) 3iiiA 54 54 27 25 2 21 (RECIST), 68 (EASL) 32 [50]
Varela et al. (2007) 3iiDiv 27 27 27 0 0 75 (EASL) 88.9 [24]
Poon et al. (2007) 3iiDiv 30 30 30 0 0 50 (RECIST), 70 (EASL) NA [25]
Kettenbach et al. (2008) 3iiDiv 30 30 26 4 0 40 (RECIST), 44 (EASL) –‡ [51]
Grosso et al. (2008) 3iiiDiv 50 50 46 4 0 74.8 (EASL) NA [52]
Strength of evidence categories were stratified according to National Cancer Institute Physician Data Query® levels of evidence for pediatric and adult cancer treatment studies [101] and ranked by level of evidence. †Child–Pugh scores were the most common indicator of severity of disease in the majority of studies published, and offered a comparison of patients receiving different modalities of treatment. ‡Overall survival at 2 years was unavailable for these studies. Kettenbach et al.: mean overall survival was 12.5 months; Prajapati et al.: median overall survival was 13.5 months. CR: Complete response; DEB‑TACE: Drug‑eluting bead transarterial chemoembolization; EASL: European Association for the Study of the Liver; NA: Not applicable; PR: Partial response; RECIST: Response Evaluation Criteria in Solid Tumors.

J. Compar. Effect. Res. (2013) 2(4) future science group440
review Xing, Kokabi, Camacho, Kooby, El-Rayes & Kim
■ Comparing objective response & survivalBased on analysis of 90Y radioembolization stud-ies, median overall survival with 90Y radioem-bolization in HCC patients ranges from 8 to 26.6 months (Table 4). Although few studies have investigated overall survival differences
between 90Y radioembolization and cTACE, a number of retrospective studies have found similar efficacy, as defined by tumor response and patient survival, between 90Y radioemboliza-tion and cTACE [10,34–36]. A highly significant predictor of clinical outcome has been found to
Table 4. Assessment of efficacy of yttrium-90 radioembolization and comparisons with conventional transarterial chemoembolization.
Study Level of evidence
Study population
Child–Pugh class (%)†
Objective response Pr and Cr (%; criteria)
Overall survival at 2 years (%)
Median overall survival (months)
ref.
Study arm
n A B C
Dancey et al. (2000)
3iiiA 90Y 22 –‡ –‡ –‡ 20 (WHO) 20 12.6 [53]
Carr et al. (2004) 3iiiA 90Y 65 –‡ –‡ –‡ 38.4 (WHO) –§ 21.6 (Okuda stage I); 10 (Okuda stage II)
[54]
Geschwind et al. (2004)
3iiiA 90Y 80 90 10 0 NA –§ 18.9 (Child–Pugh A); 8.2 (Child–Pugh B)
[55]
Salem et al. (2005) 3iiiA 90Y 43 62.8 34.9 2.3 47 (WHO) –§ 20.5 (Child–Pugh A); 13.8 (Child–Pugh B/C)
[56]
Kulik et al. (2006) 3iiiA 90Y 35 –‡ –‡ –‡ 50 (WHO) 54 26.6 [57]
Kulik et al. (2008) 3iiiB 90Y 82 65.9 32.9 1.2 42.2 (RECIST), 70 (EASL) –§ 15.6 [58]
Lewandowski et al. (2009)
3iiiA 90Y 43 56 44 0 61 (WHO), 86 (EASL) 59 35.7 [4]
cTACE 43 53 42 5 37 (WHO), 71 (EASL) 28 18.7
Kooby et al. (2010) 3iiiA 90Y 27 48 52 0 11 (RECIST) 10 6.0 [10]
cTACE 44 50 50 0 6 (RECIST) 15 6.0
Carr et al. (2010) 3iiiA 90Y 99 –‡ –‡ –‡ 41 (WHO) 29.2 11.5 [35]
cTACE 691 –‡ –‡ –‡ 60 (WHO) 20.1 8.5
Hilgard et al. (2010) 3iA 90Y 108 77 22 0 15 (WHO), 41 (mRECIST), 40 (EASL)
30 16.4 [59]
Salem et al. (2010) 3iiA 90Y 291 45 52.2 2.8 42 (WHO), 57 (EASL) 40 17.2 (Child–Pugh A), 7.7 (Child–Pugh B)
[33]
Sangro et al. (2011) 3iA 90Y 325 82.5 17.5 0 NA –§ 12.8 [37]
Salem et al. (2011) 3iiiA 90Y 123 55 44 1 49 (WHO), 72 (EASL) 45 20.5 [34]
cTACE 122 55 43 2 36 (WHO), 69 (EASL) 35 17.4
Lance et al. (2011) 3iiiA 90Y 38 81.6 18.4 0 46.1(AFP) 30 8.0 [36]
cTACE 35 68.6 31.4 0 30 (AFP) 15 10.3
Moreno-Luna et al. (2012)
3iiiA 90Y 61 87 13 0 51 (mRECIST) 30 15 [6]
cTACE 55 80 20 0 51 (mRECIST) 24 14.4
Strength of evidence categories stratified according to National Cancer Institute Physician Data Query® levels of evidence for pediatric and adult cancer treatment studies [101]. Overall survival at 2 years and median overall survival indicate survival from the time of 90Y radioembolization procedure.
†Child–Pugh scores were the most common indicator of severity of disease in the majority of studies published, and offered a comparison of patients receiving different modalities of treatment. ‡Child–Pugh class was unavailable for these studies. Dancey et al.: Okuda stage I (45%), Okuda stage II (55%). Carr et al. (2004): Okuda stage I (64.6%), Okuda stage II (32.3%), Okuda stage III (4.8%). Kulik et al. (2006): all patients stage T3 (United Network for Organ Sharing). §Overall survival data at 2 years were unavailable for these studies.
AFP: a-fetoprotein levels; CR: Complete response; cTACE: Conventional transarterial chemoembolization; EASL: European Association for the Study of the Liver; mRECIST: Modified Response Evaluation Criteria in Solid Tumors criteria; NA: Not applicable; PR: Partial response; RECIST: Response Evaluation Criteria in Solid Tumors; 90Y: Yttrium-90.

90Y radioembolization versus chemoembolization in the treatment of hepatocellular carcinoma review
future science group www.futuremedicine.com 441
be BCLC stage, with large multicenter analyses demonstrating that median survival decreases from 24.4 months (BCLC A) to 16.9 months (BCLC B) and 10.0 months (BCLC C) depend-ing on BCLC [37].
Carr et al. examined 932 patients in two non-concurrent cohorts, using concurrent untreated patients as controls. Stratification of patients based on bilirubin <1.5 mg/dl, a-fetoprotein <25 IU/ml, and the absence of PVT yielded equivalent outcomes for both cTACE and 90Y radioembolization in this study [35]. A direct comparison of treatment efficacy by Salem et al. in 122 patients who underwent cTACE and 123 patients who underwent 90Y radioemboliza-tion established similar overall survival times over a period of 9 years [34]. However, a significantly longer time-to-progression (13.3 vs 8.4 months, p = 0.046) and lower toxicity with 90Y compared with cTACE was observed in the same study [34]. Similarly, Moreno-Luna et al. found no difference in overall survival and tumor response between cTACE and 90Y radioembolization, with 90Y patients requiring fewer hospitalization days [6]. The decreased embolic effect of 90Y radioemboli-zation may be beneficial for patients with occlu-sive PVT compared with cTACE [36]. In patients with intermediate and advanced disease who are not considered ideal candidates for transplanta-tion, radioembolization has also demonstrated promising outcomes for tumor downstaging to meet the Milan (T2) criteria. Lewandowski et al. retrospectively compared 90Y radioembolization with cTACE in 86 intermediate and advanced HCC patients (BCLC Stage B, C and D) with T3 disease (no conferred listing advantage via United Network for Organ Sharing, UNOS) [4]. A higher conversion rate from T3 to T2 was observed with 90Y (58 vs 31%, p = 0.028), dem-onstrating greater efficacy for downstaging to meet the Milan criteria for OLT as compared with cTACE; larger prospective randomized studies are required to validate the effectiveness of 90Y for pretransplant downstaging.
■ Comparing safety & toxicityIn comparing the toxicity profiles of cTACE and 90Y radioembolization in a concurrent cohort (44 patients undergoing cTACE and 27 patients undergoing 90Y radioembolization) according to the National Cancer Institute common toxicity criteria, Kooby et al. found cTACE to be asso-ciated with statistically greater overall toxicity, with hematologic toxicity occurring exclusively
in patients treated with cTACE [10]. However, no difference in the incidence of major toxici-ties between both groups was observed. Salem et al. described a significantly higher rate of abdominal pain and hepatic transaminase eleva-tion in patients undergoing cTACE compared with 90Y radioembolization [34]. In addition, a significantly shorter postprocedural hospital stay with 90Y has been observed in numerous studies, and has been attributed to a lower incidence of postembolization syndrome and a greater toler-ance of therapy with 90Y treatment [6,10,34,36].
■ Comparing cost–effectivenessAlthough objective response and survival has been investigated in the comparison of 90Y radioembolization and cTACE, few studies have described the cost–effectiveness of either inter-vention in detail. It is not currently known if the cost of preprocedural angiography with 90Y radio-embolization outweighs the cost of additional hospitalization associated with cTACE. Ray et al. examined cost of RFA, cTACE and 90Y radio-embolization using Monte Carlo simulations and sensitivity analysis by running the model 100,000 times to simulate the same number of patients [38]. The authors found that although cTACE cost less than 90Y radioembolization in the majority of possible cases, 90Y treatment was less expensive than cTACE in 33.4% of simula-tions. Average allowable Medicare charges were found to be dependent on the number of repeat procedures required for each intervention ($9362 vs $30,107 vs $35,629 for RFA, cTACE, and 90Y radioembolization; p<0.001) [38]. A cost analysis study by Naugler and Sonnenberg established that immediate treatment with cTACE or RFA in patients with compensated cirrhosis resulted in similar or longer survival and decreased cost compared with expectant monitoring for intended liver transplantation [39]. It was pro-posed that improvements in HCC locoregional treatments would increase the feasibility and cost–effectiveness of early therapy for HCC [39].
Conclusion & future perspectiveSimilar efficacy and survival outcomes have been reported between cTACE and 90Y radioemboli-zation for HCC in retrospective cohort studies only, and there is not sufficient evidence thus far for 90Y radioembolization to be definitively rec-ommended over cTACE as the standard of care for patients with intermediate and advanced HCC. Prospective, randomized controlled trials

J. Compar. Effect. Res. (2013) 2(4) future science group442
review Xing, Kokabi, Camacho, Kooby, El-Rayes & Kim
investigating response, patient survival and toxic-ity are required for definitive recommendations to be made. Further comparisons of cTACE and 90Y radioembolization for both locoregional control and as a bridge to transplant are required to con-firm the effectiveness of 90Y radioembolization and define the optimal populations in which each treatment should be used. In addition, patient-based analysis is required to establish whether the risk and cost of additional hospitalization associated with cTACE outweigh the risk and cost of the additional preprocedural angiography that is required for 90Y radioembolization. Given the similarities observed in efficacy and survival,
econometric cost analyses comparing inpatient cTACE, outpatient DEB-TACE and outpatient 90Y radioembolization would be useful for future patient stratification and optimizing therapy.
Financial & competing interests disclosureThe authors have no relevant affiliations or financial involve-ment with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, con-sultancies, honoraria, stock ownership or options, expert tes-timony, grants or patents received or p ending, or royalties.
No writing assistance was utilized in the production of this manuscript.
executive summary
Background ■ Hepatocellular carcinoma is the third leading cause of cancer mortality worldwide, with a rapidly rising global disease burden. ■ Curative therapy (i.e., surgical resection, transplant and radiofrequency ablation) is offered for tumors diagnosed at early Barcelona Clinic Liver Cancer stages. However, the majority of hepatocellular carcinoma diagnosed at Barcelona Clinic Liver Cancer intermediate or advanced stages, precluding these curative treatment options.
■ For Barcelona Clinic Liver Cancer Stage B and C tumors, both US and European clinical guidelines endorse sorafenib and transarterial chemoembolization (TACE).
Conventional TACE ■ Conventional TACE (cTACE) is the accepted standard of care regional therapy for hepatocellular carcinoma in nonoperable patients with well-preserved liver function.
■ cTACE has also been used to downstage patients prior to liver transplantation, as a bridge to liver transplant to prevent disease progression beyond the Milan criteria.
Comparing objective response & survival ■ Similar efficacy, defined by tumor response and patient survival, between yttrium-90 (90Y) radioembolization and cTACE, has been found in a number of studies, with a significantly lower time-to-progression and toxicity with 90Y radioembolization having been observed.
Comparing safety & toxicity ■ Compared with 90Y radioembolization, cTACE has been associated with statistically greater overall toxicity, a higher rate of abdominal pain and hepatic transaminase elevation post procedure.
■ A significantly shorter post-procedural hospital stay with 90Y radioembolization compared with cTACE has been observed in numerous studies, and has been attributed to a lower incidence of postembolization syndrome and a greater tolerance of therapy with 90Y treatment.
Comparing cost–effectiveness ■ Cost analysis simulation of both cTACE and 90Y has shown that, although cTACE costs less than 90Y radioembolization in the majority of cases, 90Y treatment was less expensive compared with cTACE in 33.4% of simulations.
Conclusion & future perspective ■ Further analysis is required to establish whether the risk and cost of additional hospitalization associated with cTACE outweigh the risk and cost of the additional preprocedural angiography that is required for 90Y radioembolization.
■ Given the similarities observed in efficacy and survival, cost analysis comparing inpatient cTACE, outpatient drug-eluting bead-TACE and outpatient 90Y radioembolization would be useful for future patient stratification and optimizing therapy.
ReferencesPapers of special note have been highlighted as:n of interest
1 Altekruse SF, McGlynn KA, Reichman ME. Hepatocellular carcinoma incidence, mortality, and survival trends in the United States from 1975 to 2005. J. Clin. Oncol. 27(9), 1485–1491 (2009).
2 Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. Cancer 61(2), 69–90 (2011).
3 El-Serag HB, Davila JA, Petersen NJ, McGlynn KA. The continuing increase in the incidence of hepatocellular carcinoma in the United States: an update. Ann. Intern. Med. 139(10), 817–823 (2003).
4 Lewandowski RJ, Kulik LM, Riaz A et al. A comparative analysis of transarterial downstaging for hepatocellular carcinoma: chemoembolization versus radioembolization. Am. J. Transpl. 9(8), 1920–1928 (2009).
n Recent data comparing efficacy and safety of yttrium-90 (90Y) radioembolization

90Y radioembolization versus chemoembolization in the treatment of hepatocellular carcinoma review
future science group www.futuremedicine.com 443
versus conventional transarterial chemoembolization (cTACE).
5 Villanueva A, Hernandez-Gea V, Llovet JM. Medical therapies for hepatocellular carcinoma: a critical view of the evidence. Nat. Rev. Gastroenterol. Hepatol. 10(1), 34–42 (2012).
6 Moreno-Luna LE, Yang JD, Sanchez W et al. Efficacy and safety of transarterial radioembolization versus chemoembolization in patients with hepatocellular carcinoma. Cardiovasc. Intervent. Radiol. 36(3), 714–723 (2012).
n Recent data comparing efficacy and safety of 90Y radioembolization versus cTACE.
7 Bruix J, Sherman M, Llovet JM et al. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL Conference. J. Hepatol. 35(3), 421–430 (2001).
8 Bruix J, Sala M, Llovet JM. Chemoembolization for hepatocellular carcinoma. Gastroenterology 127(5 Suppl. 1), S179–S188 (2004).
9 Llovet JM, Ricci S, Mazzaferro V et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 359(4), 378–390 (2008).
10 Kooby DA, Egnatashvili V, Srinivasan S et al. Comparison of yttrium-90 radioembolization and transcatheter arterial chemoembolization for the treatment of unresectable hepatocellular carcinoma. J. Vasc. Interv. Radiol. 21(2), 224–230 (2010).
n Recent data comparing efficacy and safety of 90Y radioembolization versus cTACE.
11 Yamada R, Nakatsuka H, Nakamura K et al. Hepatic artery embolization in 32 patients with unresectable hepatoma. Osaka City Med. J. 26(2), 81–96 (1980).
12 Liapi E, Georgiades CC, Hong K, Geschwind JFH. Transcatheter arterial chemoembolization: current technique and future promise. Tech. Vasc. Interv. Radiol. 10(1), 2–11 (2007).
13 Llovet JM, Real MI, Montaña X, Planas R, Coll S. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet 18(359), 1734–1739 (2002).
14 Lo CM, Ngan H, Tso WK et al. Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology 35(5), 1164–1171 (2002).
15 Schwarz RE, Alfa GA, Geschwind JF et al. Nonoperative therapies for combined modality treatment of hepatocellular cancer: expert consensus statement. HPB (Oxford) 12(5), 313–320 (2010).
16 Yao FY, Kerlan RK, Hirose R et al. Excellent outcome following down-staging of hepatocellular carcinoma prior to liver transplantation: an intention-to-treat analysis. Hepatology 48(3), 819–827 (2008).
17 Ravaioli M, Grazi GL, Piscaglia F et al. Liver transplantation for hepatocellular carcinoma: results of down-staging in patients initially outside the Milan selection criteria. Am. J. Transplant. 8(12), 2547–2557 (2008).
18 Chapman WC, Majella Doyle MB, Stuart JE et al. Outcomes of neoadjuvant transarterial chemoembolization to downstage hepatocellular carcinoma before liver transplantation. Ann. Surg. 248(4), 617–625 (2008).
19 Jarnagin W, Chapman WC, Curley S et al. Surgical treatment of hepatocellular carcinoma: expert consensus statement. HPB (Oxford) 12(5), 302–310 (2010).
20 Kim WR, Stock PG, Smith JM et al. OPTN/SRTR 2011 annual data report: liver. Am. J. Transplant. 13(Suppl. 1), S73–S102 (2013).
21 Pelletier SJ, Fu S, Thyagarajan V et al. An intention-to-treat analysis of liver transplantation for hepatocellular carcinoma using organ procurement transplant network data. Liver Transpl. 15(8), 859–868 (2009).
22 Bargellini I, Vignali C, Cioni R et al. Hepatocellular carcinoma: CT for tumor response after transarterial chemoembolization in patients exceeding Milan criteria – selection parameter for liver transplantation. Radiology 255(1), 289–300 (2010).
23 Luo J, Peng ZW, Guo RP et al. Hepatic resection versus transarterial lipiodol chemoembolization as the initial treatment for large, multiple, and resectable hepatocellular carcinomas: a prospective nonrandomized analysis. Radiology 259(1), 286–295 (2011).
24 Varela M, Real MI, Burrel M et al. Chemoembolization of hepatocellular carcinoma with drug eluting beads: efficacy and doxorubicin pharmacokinetics. J. Hepatol. 46(3), 474–481 (2007).
25 Poon RTP, Tso WK, Pang RWC et al. A Phase I/II trial of chemoembolization for hepatocellular carcinoma using a novel intra-arterial drug-eluting bead. Clin. Gastroenterol. Hepatol. 5(9), 1100–1108 (2007).
26 Prajapati HJ, Dhanasekaran R, El-Rayes BF et al. Safety and efficacy of doxorubicin drug-
eluting bead transarterial chemoembolization in patients with advanced hepatocellular carcinoma. J. Vasc. Interv. Radiol. 24(3), 307–315 (2013).
27 Prajapati HJ, Rafi S, El-Rayes BF, Kauh JS, Kooby DA, Kim HS. Safety and feasibility of same-day discharge of patients with unresectable hepatocellular carcinoma treated with doxorubicin drug-eluting bead transcatheter chemoembolization. J. Vasc. Interv. Radiol. 23(10), 1286–1293.e1281 (2012).
28 Lammer J, Malagari K, Vogl T et al. Prospective randomized study of doxorubicin-eluting-bead embolization in the treatment of hepatocellular carcinoma: results of the PRECISION V study. Cardiovasc. Intervent. Radiol. 33(1), 41–52 (2010).
29 Campbell AM, Bailey IH, Burton MA. Analysis of the distribution of intra-arterial microspheres in human liver following hepatic yttrium-90 microsphere therapy. Phys. Med. Biol. 45(4), 1023–1033 (2000).
30 Murthy R, Kamat P, Nunez R, Salem R. Radioembolization of yttrium-90 microspheres for hepatic malignancy. Semin. Intervent. Radiol. 25(1), 48–57 (2008).
31 Salem R, Thurston KG. Radioembolization with 90Yttrium microspheres: a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies. J. Vasc. Interv. Radiol. 17(8), 1251–1278 (2006).
32 Sangro B, Inarrairaegui M, Bilbao JI. Radioembolization for hepatocellular carcinoma. J. Hepatol. 56(2), 464–473 (2012).
33 Salem R, Lewandowski RJ, Mulcahy MF et al. Radioembolization for hepatocellular carcinoma using yttrium-90 microspheres: a comprehensive report of long-term outcomes. Gastroenterology 138(1), 52–64 (2010).
34 Salem R, Lewandowski RJ, Kulik L et al. Radioembolization results in longer time-to-progression and reduced toxicity compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology 140(2), 497–507.e492 (2011).
n Recent data comparing efficacy and safety of 90Y radioembolization versus cTACE.
35 Carr BI, Kondragunta V, Buch SC, Branch RA. Therapeutic equivalence in survival for hepatic arterial chemoembolization and yttrium 90 microsphere treatments in unresectable hepatocellular carcinoma: a two-cohort study. Cancer 116(5), 1305–1314 (2010).
n Recent data comparing efficacy and safety of 90Y radioembolization versus cTACE.

J. Compar. Effect. Res. (2013) 2(4) future science group444
review Xing, Kokabi, Camacho, Kooby, El-Rayes & Kim
36 Lance C, McLennan G, Obuchowski N et al. Comparative analysis of the safety and efficacy of transcatheter arterial chemoembolization and yttrium-90 radioembolization in patients with unresectable hepatocellular carcinoma. J. Vasc. Interv. Radiol. 22(12), 1697–1705 (2011).
n Recent data comparing efficacy and safety of 90Y radioembolization versus cTACE.
37 Sangro B, Carpanese L, Cianni R et al. Survival after yttrium-90 resin microsphere radioembolization of hepatocellular carcinoma across Barcelona clinic liver cancer stages: a European evaluation. Hepatology 54(3), 868–878 (2011).
n Recent data comparing efficacy and safety of 90Y radioembolization versus cTACE.
38 Ray J, Charles E, Battaglia C et al. Interventional radiologic treatment of hepatocellular carcinoma – a cost analysis from the payer perspective. J. Vasc. Interv. Radiol. 23(3), 306–314 (2012).
39 Naugler WE, Sonnenberg A. Survival and cost-effectiveness analysis of competing strategies in the management of small hepatocellular carcinoma. Liver Transpl. 16(10), 1186–1194 (2010).
40 A comparison of lipiodol chemoembolization and conservative treatment for unresectable hepatocellular carcinoma. Groupe d’Etude et de Traitement du Carcinome Hepatocellulaire. N. Engl. J. Med. 332(19), 1256–1261 (1995).
41 Pelletier G, Ducreux M, Gay F et al. Treatment of unresectable hepatocellular carcinoma with lipiodol chemoembolization: a multicenter randomized trial. Groupe CHC. J. Hepatol. 29(1), 129–134 (1998).
42 Yuen MF, Chan AOO, Wong BCY et al. Transarterial chemoembolization for inoperable, early stage hepatocellular carcinoma in patients with Child–Pugh grade A and B: results of a comparative study in 96 Chinese patients. Am. J. Gastroenterol. 98(5), 1181–1185 (2003).
43 Brown DB, Chapman WC, Cook RD et al. Chemoembolization of hepatocellular
carcinoma: patient status at presentation and outcome over 15 years at a single center. Am. J. Roentgenol. 190(3), 608–615 (2008).
44 Barone M, Ettorre GC, Ladisa R et al. Transcatheter arterial chemoembolization (TACE) in treatment of hepatocellular carcinoma. Hepatogastroenterology 50(49), 183–187 (2003).
45 Takayasu K, Arii S, Ikai I et al. Prospective cohort study of transarterial chemoembolization for unresectable hepatocellular carcinoma in 8510 patients. Gastroenterology 131(2), 461–469 (2006).
46 Sacco R, Bargellini I, Bertini M et al. Conventional versus doxorubicin-eluting bead transarterial chemoembolization for hepatocellular carcinoma. J. Vasc. Interv. Radiol. 22(11), 1545–1552 (2011).
47 Forner A, Ayuso C, Varela M et al. Evaluation of tumor response after locoregional therapies in hepatocellular carcinoma: are response evaluation criteria in solid tumors reliable? Cancer 115(3), 616–623 (2009).
48 Reyes DK, Vossen JA, Kamel IR et al. Single-center phase II trial of transarterial chemoembolization with drug-eluting beads for patients with unresectable hepatocellular carcinoma: initial experience in the United States. Cancer J. 15(6), 526–532 (2009).
49 Dhanasekaran R, Kooby DA, Staley CA, Kauh JS, Khanna V, Kim HS. Comparison of conventional transarterial chemoembolization (TACE) and chemoembolization with doxorubicin drug eluting beads (DEB) for unresectable hepatocelluar carcinoma (HCC). J. Surg. Oncol. 101(6), 476–480 (2010).
50 Kalva SP, Iqbal SI, Yeddula K et al. Transarterial chemoembolization with Doxorubicin-eluting microspheres for inoperable hepatocellular carcinoma. Gastrointest. Cancer Res. 4(1), 2–8 (2011).
51 Kettenbach J, Stadler A, Katzler IV et al. Drug-loaded microspheres for the treatment of liver cancer: review of current results. Cardiovasc. Intervent. Radiol. 31(3), 468–476 (2008).
52 Grosso M, Vignali C, Quaretti P et al. Transarterial chemoembolization for hepatocellular carcinoma with drug-eluting microspheres: preliminary results from an Italian multicentre study. Cardiovasc. Intervent. Radiol. 31(6), 1141–1149 (2008).
53 Dancey JE, Shepherd FA, Paul K et al. Treatment of nonresectable hepatocellular carcinoma with intrahepatic 90Y-microspheres. J. Nucl. Med. 41(10), 1673–1681 (2000).
54 Carr BI. Hepatic arterial 90yttrium glass microspheres (Therasphere) for unresectable hepatocellular carcinoma: interim safety and survival data on 65 patients. Liver Transpl. 10(2 Suppl. 1), S107–S110 (2004).
55 Geschwind JFH, Salem R, Carr BI et al. Yttrium-90 microspheres for the treatment of hepatocellular carcinoma. Gastroenterology 127(5 Suppl. 1), S194–S205 (2004).
56 Salem R, Lewandowski RJ, Atassi B et al. Treatment of unresectable hepatocellular carcinoma with use of 90Y microspheres (TheraSphere): safety, tumor response, and survival. J. Vasc. Interv. Radiol. 16(12), 1627–1639 (2005).
57 Kulik LM, Atassi B, Van Holsbeeck L et al. Yttrium-90 microspheres (TheraSphere) treatment of unresectable hepatocellular carcinoma: downstaging to resection, RFA and bridge to transplantation. J. Surg. Oncol. 94(7), 572–586 (2006).
58 Kulik LM, Carr BI, Mulcahy MF et al. Safety and efficacy of 90Y radiotherapy for hepatocellular carcinoma with and without portal vein thrombosis. Hepatology 47(1), 71–81 (2008).
59 Hilgard P, Hamami M, Fouly AE et al. Radioembolization with yttrium-90 glass microspheres in hepatocellular carcinoma: European experience on safety and long-term survival. Hepatology 52(5), 1741–1749 (2010).
■ Website101 National Cancer Institute. Levels of Evidence
for Adult and Pediatric Cancer Treatment Studies (PDQ®). www.cancer.gov/cancertopics/pdq/levels-evidence-adult-treatment/healthprofessional