a comparison of chemoembolization endpoints using angiographic versus transcatheter intraarterial...
TRANSCRIPT

A Comparison of ChemoembolizationEndpoints Using Angiographic versusTranscatheter Intraarterial Perfusion/MRImaging MonitoringRobert J. Lewandowski, MD, Dingxin Wang, BS, James Gehl, BBA, Bassel Atassi, MD, Robert K. Ryu, MD,
Kent Sato, MD, Albert A. Nemcek, Jr, MD, Frank H. Miller, MD, Mary F. Mulcahy, MD, Laura Kulik, MD,Andrew C. Larson, PhD, Riad Salem, MD, MBA, and Reed A. Omary, MD, MS
PURPOSE: Transcatheter arterial chemoembolization (TACE) is an established treatment for unresectable liver cancer.This study was conducted to test the hypothesis that angiographic endpoints during TACE are measurable andreproducible by comparing subjective angiographic versus objective magnetic resonance (MR) endpoints of TACE.
MATERIALS AND METHODS: The study included 12 consecutive patients who presented for TACE for surgicallyunresectable HCC or progressive hepatic metastases despite chemotherapy. All procedures were performed witha dedicated imaging system. Angiographic series before and after TACE were reviewed independently by threeboard-certified interventional radiologists. A subjective angiographic chemoembolization endpoint (SACE)classification scheme, modified from an established angiographic grading system in the cardiology literature, wasdesigned to assist in reproducibly classifying angiographic endpoints. Reproducibility in SACE classificationlevel was compared among operators, and MR imaging perfusion reduction was compared with SACE levels foreach observer.
RESULTS: Twelve patients successfully underwent 15 separate TACE sessions. SACE levels ranged from I through IV.There was moderate agreement in SACE classification (� � 0.46 � 0.12). There was no correlation between SACE leveland MR perfusion reduction (r � 0.16 for one operator and 0.02 for the other two).
CONCLUSIONS: Angiographic endpoints during TACE vary widely, have moderate reproducibility among operators,and do not correlate with functional MR imaging perfusion endpoints. Future research should aim to determine idealangiographic and functional MR imaging endpoints for TACE according to outcome measures such as imagingresponse, pathologic response, and survival.
J Vasc Interv Radiol 2007; 18:1249–1257
Abbreviations: AUC � area under the curve, DSA � digital subtraction angiography, HCC � hepatocellular carcinoma, SACE � subjective angiographic chemoem-bolization endpoint, TACE � transcatheter arterial chemoembolization, TIMI � Thrombolysis In Myocardial Infarction, TRIP � transcatheter intraarterial perfusion.
PRIMARY and secondary hepatic ma-lignancies continue to plague clinicaloncologists. Unfortunately, most pa-
From the Departments of Radiology (R.J.L., D.W.,J.G., B.A., R.K.R., K.S., A.A.N., F.M., M.F.M., L.K.,A.C.L., R.S., R.A.O.), Biomedical Engineering (D.W.,A.C.L., R.A.O.), and Medicine (M.F.M., L.K., R.S.),Feinberg School of Medicine, and Robert H. LurieComprehensive Cancer Center (M.F.M., A.C.L., R.S.,R.A.O.), Northwestern University, 676 North St.
Clair Street, Suite 800, Chicago, Illinois 60611. Re-ceived April 2, 2007; final revision received June 18,tients are not candidates for an opera-tive cure at presentation (1,2). Tradi-tional chemotherapeutic regimens
2007; accepted June 20, 2007. Address correspondenceto R.J.L.; E-mail: [email protected]
None of the authors have identified a conflict ofinterest.
© SIR, 2007
DOI: 10.1016/j.jvir.2007.06.028
offer no survival benefit comparedwith best supportive care for patientswith hepatocellular carcinoma (HCC)(3–9). Liver-directed therapies, ofwhich transcatheter arterial chemoem-bolization (TACE) is the most widelyaccepted, have evolved in the treat-ment of HCC. Recent randomized con-trolled studies have demonstrated im-proved survival benefit for thoseundergoing TACE versus best sup-portive care (10,11). TACE has also be-come an established treatment for
those with progressive hepatic metas-1249

1250 • Subjective Angiographic vs Objective MR Endpoints of TACE October 2007 JVIR
tases despite standard-of-care chemo-therapy (12–20). However, there is nopublished consensus regarding thepreferred angiographic endpoint forTACE: stasis to antegrade blood flowor to a substasis level (21). Althoughunproven, a substasis endpoint maybe safer and more efficacious becauseexcessive embolization may result inarterial occlusion or liver failure (22).
Transcatheter intraarterial perfu-sion (TRIP) magnetic resonance (MR)imaging is an innovative first-passperfusion technique that employs di-rect catheter-based intraarterial injec-tions of contrast agent into the tar-geted hepatic artery before and afterTACE. TRIP MR imaging can be usedto verify distribution of injected che-moembolic material before deliveryand to monitor changes in tumor per-fusion after liver embolotherapy (23).It differs from conventional dynamiccontrast agent–enhanced MR imagingbecause TRIP MR imaging uses cathe-ter-directed intraarterial injections ofgadolinium, whereas dynamic con-trast agent–enhanced MR imaginguses intravenous injections of gadolin-ium. A preclinical study in the VX2rabbit liver tumor model has validatedthe utility of TRIP MR imaging tomonitor iterative changes in liver tu-mor perfusion during embolization(23). This technique has been trans-lated clinically in the context of inter-ventional radiologic MR suites, whichcombine interventional radiologic ra-diographic digital subtraction angiog-raphy (DSA) with adjacent MR imag-ing scanners. TRIP MR imaging offersan objective, quantitative intraproce-dural method to compare subjectiveangiographic endpoints of TACE.
Current radiographic methodscannot assess functional endpoints ofTACE. By fusing intraproceduralTRIP MR imaging information withtraditional radiographically guideddelivery of TACE, we aim to im-prove the success and reduce thevariability of such therapies. In thisprospective clinical study, we testedthe hypothesis that angiographicendpoints during TACE for HCC orprogressive hepatic metastases aremeasurable and reproducible. To ac-complish this, we compared subjec-tive radiographic versus objective
MR endpoints of TACE.MATERIALS AND METHODS
Clinical Setting and Patients
Our local institutional review boardapproved this prospective study.From March through November 2006,we enrolled 12 consecutive patientswith surgically unresectable HCC orprogressive hepatic metastases despitestandard-of-care chemotherapy whopresented at a single university-affili-ated hospital in a large metropolitanarea. All patients were deemed TACEcandidates at a weekly institutionalmultidisciplinary tumor conference.Inclusion and exclusion criteria weremodified from the report of Brown etal (24). Included patients met the fol-lowing criteria: (i) age greater than 18years, (ii) Eastern Cooperative Oncol-ogy Group performance status nogreater than 2, (iii) Child-Pugh classA/B disease in cases of HCC, (iv) focalor multifocal hepatic malignancy, (v)no contraindications to MR imaging,and (vi) informed consent. We ex-cluded patients with (i) life expectancyless than 6 months, (ii) Eastern Coop-erative Oncology Group performancestatus of 3 or greater, (iii) Child-Pughclass C disease, (iv) uncorrectable co-agulopathy (International NormalizedRatio �1.5), (v) total bilirubin levelgreater than 4.0 mg/dL, (vi) serumcreatinine �2.0 mg/dL; (vii) uncor-rectable thrombocytopenia (plateletcount �50,000/�L), or (viii) contrain-dications to MR imaging (eg, pace-maker, cochlear implant). Patientswith portal vein thrombosis were en-rolled if superselective segmental
Table 1Study Sample Demographics
Demographics No. of Patients
Age (y)�69 10 (83)�69 2 (17)
Ethnic groupWhite 8 (67)Black 1 (8)Asian 2 (17)Hispanic 1 (8)
SexMale 7 (58)Female 5 (42)
Note.—Values in parentheses arepercentages.
TACE was technically feasible (25).
Demographics, tumor characteristics,baseline liver function, and staging ofenrolled patients’ disease are detailedin Tables 1–3.
The diagnosis of HCC was estab-lished by biopsy and/or noninva-sively based on a tumor larger than 2cm in diameter with characteristic im-aging findings (26) in the setting ofcirrhosis with an serum �-fetoproteinlevel of at least 400 ng/mL (27). Pa-tients were deemed to have unresect-able disease by an attending trans-plant surgeon or surgical oncologistfor the following reasons: (i) concur-rent comorbidities including cardiacor respiratory compromise, (ii) recur-rent or multilobar disease, (iii) cirrho-sis or portal hypertension, (iv) vascu-lar invasion, (v) high tumor burden,and/or (vi) contraindications to gen-eral anesthesia. The diagnosis of pro-gressive hepatic metastatic diseasewas established by biopsy and cross-sectional imaging.
MR Procedure Suite
We performed all TACE proce-
Table 2Tumor Characteristics of StudySample
Tumor CharacteristicsNo. of
Patients
Lesion distribution(measurable)
Unilobar 6 (50)Bilobar 6 (50)
Replacement (%)0–25 10 (84)26–50 1 (8)51–75 1 (8)�75 0 (0)
MorphologyUninodular and �50% 9 (75)Multinodular and �50% 3 (25)Massive or �50% 0 (0)
Portal vein thrombosisNone 11 (92)Unilobar 0 (0)Main 1 (8)
CirrhosisNo 2 (17)Yes 10 (83)
InfiltrativeNo 10 (83)Yes 2 (17)
Note.—Values in parentheses arepercentages.
dures with use of a dedicated inter-

Lewandowski et al • 1251Volume 18 Number 10
ventional radiologic MR system(Miyabi; Siemens, Erlangen, Germany)that contains an Artis–dTA flat-panelradiographic DSA unit integrated witha 1.5-T Espree MR imaging scanner viaa moving table (Fig 1).
TACE
All TACE procedures were per-formed by four board-certified attend-ing interventional radiologists whospecialize in interventional oncology.Patients were prepared and draped insterile fashion in the interventional ra-diology suite. A 5.5-F vascular sheathwas placed into the common femoralartery. After initial mapping, visceralradiographic DSA with a selective 5-Fvisceral catheter (typically Simmonsor Cobra shapes), a 2.8-F microcath-eter (Renegade Hi-Flo; Boston Scien-tific, Natick, Mass) was coaxially in-serted over a 0.016-inch-diameterguide wire (Headliner; Terumo, To-kyo, Japan) to superselect the hepaticlobar or segmental hepatic artery sup-plying the targeted tumor. ThreeTACE procedures were segmental and12 were lobar. DSA was performedwith iohexol injection (Omnipaque350; Amersham Health, Princeton,
Table 3Baseline Liver Function of StudySample
ParameterNo. of
Patients
AscitesNo 9 (75)Yes 3 (25)
Bilirubin (total)�ULN 7 (58)�ULN 5 (42)
Albumin�LLN 2 (17)�LLN 10 (83)
Aspartate aminotransferase�ULN 1 (8)�ULN 11 (92)
Alanine aminotransferase�ULN 6 (50)�ULN 6 (50)
Alfa-fetoprotein (ng/mL)�400 11 (92)�400 1 (8)
Note.—LLN � lower limit of normal;ULN � upper limit of normal. Valuesin parentheses are percentages.
NJ).
After the attending interventionalradiologist selected the final catheterposition for TACE, patients weretransferred on the moving table to theadjacent MR imaging unit. A steriledrape was applied on top of the exist-ing catheter system, allowing subse-quent placement of the MR chest arraycoil. We performed baseline MR imag-ing before TACE, which was then per-formed back in the interventionalsuite. We created a 1:1 solution ofemulsifying contrast agent and che-motherapeutic agent by mixing 10 mLof Ethiodol (Savage Laboratories,Melville, NY) with a 10-mL mixture ofthree chemotherapy drugs: cisplatin100 mg, doxorubicin 30 mg, and mito-mycin-C 30 mg. Under direct radio-graphic monitoring, we instilled thismixture in 1–3-mL aliquots, typicallyuntil there was some slowing of ante-grade blood flow. We then completedTACE by injecting 500–700-�m-diam-eter Embospheres (Biosphere Medical,Rockland, Mass) mixed with iohexol.The angiographic endpoint was deter-mined at the discretion of the attend-ing interventional radiologist. AfterTACE, patients were transferred to theadjacent MR suite for completion MRimaging. After this final MR imagingstudy, we transferred patients back tothe interventional suite, where thevascular sheath was removed and he-mostasis was achieved with manualcompression. After TACE, all patients
Figure 1. MR/interventional suite at invallows rapid transfer of patients duringimaging.
were admitted to the hospital on the
attending oncologist’s clinical service.They were discharged 1–2 days laterafter verification of adequate pain con-trol, ambulation, and oral intake.
MR Imaging
Immediately after patient transferfrom the interventional suite to theMR imaging unit, we performed axialand coronal T2-weighted and T1-weighted turbo spin-echo localizationstudies to determine optimal slice po-sition(s) for subsequent TRIP MR im-aging. Localization scans were repeatedwith each between-unit transfer to en-sure consistent slice positions for serialTRIP MR imaging measurements.
TRIP MR imaging was performedwith breath-hold two-dimensional sat-uration-recovery gradient-echo imag-ing in axial orientations, providing fullspatial coverage of the targeted liversegment(s). This sequence is relativelymotion-insensitive, allows rapid serialacquisition of T1-weighted images forfirst-pass contrast agent–enhancedMR imaging, and provides strong T1weighting with a relatively linear rela-tionship between signal and contrastagent concentration (28). TRIP MR im-aging parameters included a repeti-tion time of 2.4 msec, echo time of 1.2msec, matrix of 192 � 128, field ofview of 300–340 mm, slice thickness of8 mm, generalized autocalibratingpartially parallel acquisition factor of
igators’ institution. Moving table (arrow)CE between radiographic DSA and MR
estTA
2, inversion time of 90 msec, and

1252 • Subjective Angiographic vs Objective MR Endpoints of TACE October 2007 JVIR
10–14 slices. These slice positions wererepeatedly sampled for 40 seconds(2.5-second sampling rate for eachstack of two-dimensional slices). Fiveseconds after beginning this image acqui-sition, the interventional radiologist in-jected 4–10 mL of 20% gadopentetatedimeglumine solution (Magnevist; Ber-lex, Montville, NJ) at a rate of 1–2 mL/sec through the existing hepatic arterycatheter. Each TRIP MR imaging con-trast agent injection was tailored em-pirically based on the targeted vesselcaliber and blood flow rates, as well asthe targeted volume, to avoid reflux ofinjected gadopentetate dimeglumineinto nontargeted angiographic territo-ries. Before and after TACE, each pa-tient underwent the same TRIP MRimaging scanning and contrast agentinjection protocol, as quantitativechanges are relative.
After each TRIP MR imaging scan,we performed two-dimensional multi-slice T1-weighted gradient-echo studiesto provide conventional delayed-phasecontrast agent–enhanced depiction ofthe liver in axial and coronal orienta-tions.
Data Analysis
TACE.—Selective angiographic im-ages before and after TACE were ar-chived to a picture archiving systemand reviewed independently by threeboard-certified attending interven-tional radiologists. All were blinded toTRIP MR imaging results. A subjectiveangiographic chemoembolization end-point (SACE) classification schemewas designed to assist in reproduciblyclassifying angiographic endpoints(Table 4). This classification system wasmodified from an established angio-graphic grading system: the Thrombol-
Table 4TIMI (29) versus SACE Grading System
TIMI
GradeAntegrade Arterial
Flow Level
0 No flow I1 Minimal flow II2 Partial flow III3 Complete flow IV
ysis In Myocardial Infarction (TIMI)
flow grade used in coronary angiogra-phy (29).
TRIP MR imaging.—TRIP MR im-age series for each patient were ex-ported to a laptop workstation (Mac-Book Pro; Apple, Cupertino, Calif)with MatLab image processing soft-ware (Mathworks, Natick, Mass).Based on localization and delayed-phase contrast agent–enhanced ana-tomic images, we selected TRIP MRimaging slice positions at the center ofeach tumor. At these slice positions weselected a region of interest encom-passing the entire tumor and mea-sured time–intensity curves for allvoxels. For each tumor, we evaluatedthe TRIP MR imaging series obtainedbefore TACE to determine the optimaltime interval after injection for our ar-ea-under-the-curve (AUC) semiquan-titative perfusion measurements. Wefirst plotted the composite time–inten-sity curves formed by averaging allvoxelwise curves within the tumor re-gion of interest and selected a signalintegration interval beginning withthe initiation of signal enhancementand closing at peak signal enhance-ment. After selecting the integrationinterval and subtracting baseline sig-nal intensity, we calculated the AUCfor each voxelwise time–intensitycurve to produce a spatially resolvedperfusion map within the targetedvascular territory. Within perfusionmaps, each voxel was assigned a colorcorresponding to relative perfusion atthat image location.
For measurements after TACE, weanalyzed corresponding TRIP MR im-age series in similar fashion by em-ploying identical duration of AUC in-tegration. We defined the functionalTRIP MR imaging embolic endpoint asthe percent reduction in tumor perfu-
SACE
Antegrade ArterialFlow Tumor Blush
Normal Normal/reducedReduced ReducedReduced NoneNone None
sion after TACE. These measurements
were all calculated blinded to angio-graphic classification.
Outcome Measures
For each individual interventionalradiologist, we graphed the SACElevel versus TRIP MR imaging perfu-sion and determined correlation withuse of the Spearman correlation test.We compared the reproducibility inSACE classification level among oper-ators with use of the � statistic. Meanchanges in tumor perfusion before andafter TACE were assessed with apaired t test. Statistical significancewas judged at a P value less than .05.
RESULTS
TACE
Twelve patients successfully under-went a total of 15 separate TACE ses-sions within the MR/interventionalprocedure suite. Ten patients hadHCC (13 total TACE sessions) and twohad hepatic neuroendocrine metasta-ses (one TACE session each). The typ-ical time to complete the entire moni-tored MR/interventional procedurewas 3 hours, with the transfer timebetween interventional and MR unitsaveraging 10 minutes.
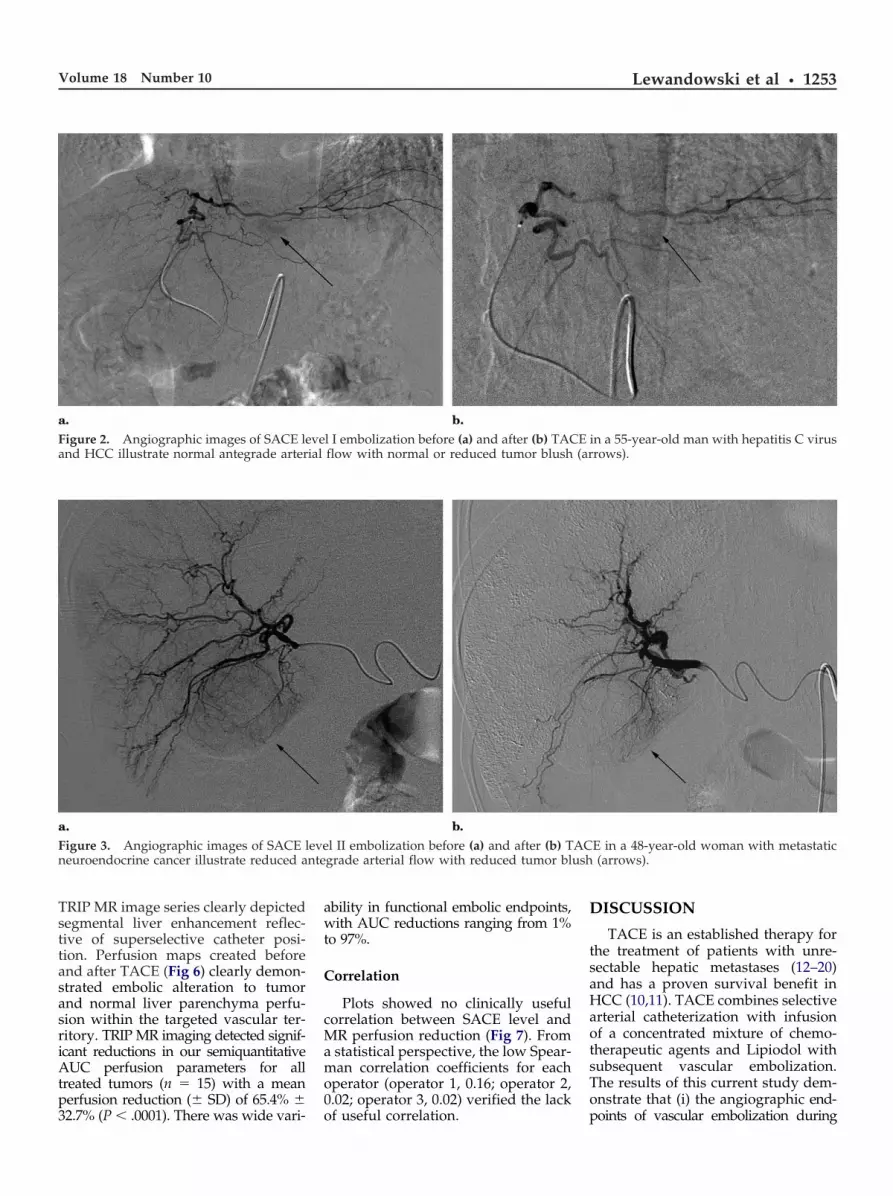
SACE levels ranged from I throughIV. SACE level I denotes normal ante-grade arterial flow with normal or re-duced tumor blush (Fig 2). SACE levelII denotes reduced antegrade arterialflow with reduced tumor blush (Fig 3),SACE level III denotes reduced ante-grade arterial flow with no tumorblush (Fig 4), and SACE level IV isreserved for cases of no antegrade ar-terial flow and no tumor blush (Fig 5).
There was moderate agreement inSACE classification, with a � value of0.46 � 0.12. In four of 16 cases (25%),one operator classified the endpoint ascomplete stasis (ie, SACE level IV),whereas the remaining two operatorsclassified the same patients at substa-sis endpoints (SACE level II or III).The most common endpoint wasSACE level III, which was seen in 24 of45 classifications (53%).
MR Imaging
All patients successfully underwentTRIP MR imaging perfusion measure-
s
ments before and after TACE. Each
ial (ar
nte ush
Lewandowski et al • 1253Volume 18 Number 10
TRIP MR image series clearly depictedsegmental liver enhancement reflec-tive of superselective catheter posi-tion. Perfusion maps created beforeand after TACE (Fig 6) clearly demon-strated embolic alteration to tumorand normal liver parenchyma perfu-sion within the targeted vascular ter-ritory. TRIP MR imaging detected signif-icant reductions in our semiquantitativeAUC perfusion parameters for alltreated tumors (n � 15) with a meanperfusion reduction (� SD) of 65.4% �
Figure 2. Angiographic images of SACE leand HCC illustrate normal antegrade arter
Figure 3. Angiographic images of SACE lneuroendocrine cancer illustrate reduced a
32.7% (P � .0001). There was wide vari-
ability in functional embolic endpoints,with AUC reductions ranging from 1%to 97%.
Correlation
Plots showed no clinically usefulcorrelation between SACE level andMR perfusion reduction (Fig 7). Froma statistical perspective, the low Spear-man correlation coefficients for eachoperator (operator 1, 0.16; operator 2,0.02; operator 3, 0.02) verified the lack
l I embolization before (a) and after (b) TACflow with normal or reduced tumor blush
l II embolization before (a) and after (b) Tgrade arterial flow with reduced tumor bl
of useful correlation.
DISCUSSION
TACE is an established therapy forthe treatment of patients with unre-sectable hepatic metastases (12–20)and has a proven survival benefit inHCC (10,11). TACE combines selectivearterial catheterization with infusionof a concentrated mixture of chemo-therapeutic agents and Lipiodol withsubsequent vascular embolization.The results of this current study dem-onstrate that (i) the angiographic end-
in a 55-year-old man with hepatitis C virusrows).
E in a 48-year-old woman with metastatic(arrows).
ve E
eve AC
points of vascular embolization during

E, ith
de
1254 • Subjective Angiographic vs Objective MR Endpoints of TACE October 2007 JVIR
TACE vary widely; (ii) interventionalradiologists have only moderate re-producibility in classifying these end-points when using subjective angio-graphic criteria; and (iii) there is no
Figure 4. Angiographic images of SACEcomplicated by multifocal HCC. After TAC
Figure 5. Angiographic images of SACE leand HCC. After TACE, there is no antegra
correlation between angiographic and
TRIP MR imaging functional perfu-sion endpoints. These results aresomewhat unexpected because theyfail to confirm our hypothesis that an-giographic endpoints during TACE
el III embolization before (a) and after (bthere is reduced antegrade arterial flow w
IV embolization before (a) and after (b) TAarterial flow and no tumor blush.
for HCC or progressive hepatic metas-
tases are measurable and reproduc-ible.
Interventional radiologists haveadopted no standard angiographic cri-teria to describe flow in blood vessels.
ACE in a 74-year-old man with cirrhosisno tumor blush (arrows).
in a 55-year-old man with hepatitis C virus
lev ) T
vel CE
This makes it difficult when discuss-

sio .
Lewandowski et al • 1255Volume 18 Number 10
ing or comparing procedures such asTACE that may alter the flow of bloodto a particular region of interest. Incontrast, cardiologists have estab-lished the widely accepted TIMI an-giographic system for grading bloodflow. TIMI criteria initially character-ized coronary flow after thrombolytictherapy for myocardial infarction.TIMI grade 0 implies no flow, grade 1minimal flow, grade 2 partial flow,and grade 3 complete flow (29). TheSACE scale described in this article isbased on the TIMI scale, and it is anattempt to reproducibly classify angio-graphic endpoints for interventionalradiologists (Table 4). Although thisproposed classification scheme hadmoderate reproducibility among oper-ators, it still did not correlate with ob-jective MR reductions in perfusionchange. This finding suggests that theproposed SACE scale was not able tofunction as a surrogate for the actualfunctional changes in tumor perfusionthat occurred during TACE. Future re-search will need to resolve whether amodification of the proposed SACEscale may allow it to function as a
Figure 6. TRIP MR imaging perfusion mathe right hepatic lobe. (a) T1-weighted anatand after (c) TACE show a 40% perfusion revoxel, with red indicating maximum perfu
surrogate for functional MR imaging
perfusion changes. If not, there will bestrong evidence that radiographicDSA can not be used to predict alter-ations in tumor perfusion after embo-lotherapy.
There is controversy regarding notonly the ideal embolization agent forTACE (30,31), but also the ideal TACEangiographic endpoint. The Society ofInterventional Radiology Standards ofPractice document for TACE does notaddress this issue (21). Stasis to for-ward blood flow may increase toxicityand induce expression of angiogenicgrowth factors that can promote tu-mor growth, including vascular endo-thelial growth factor (32,33) and hyp-oxia inducible factor–1� (34). HCCcells have also been shown to havecompensatory mechanisms to surviveor even proliferate more efficientlywhen placed in a hypoxic environ-ment (35,36). Overembolization (ie,embolization to a level beyond anytherapeutic benefit) or repeated embo-lizations may lead to arterial occlusionor accelerate liver failure (22). There-fore, an angiographic endpoint short
from a 55-year-old man with hepatitis C viric MR imaging depicts enhancing tumor intion. The adjacent color-coded scale (in arb
n and blue indicating minimum perfusion
of stasis may be safer and more effica-
cious, but this postulate remains un-proven.
The MR interventional suite used inthis study combines radiographic DSAwith an adjacent MR imaging scanner,allowing comparisons between ob-served angiographic endpoints of theprocedure with objective, measuredperfusion endpoints. The concept is touse radiographic guidance for catheterplacement and to use MR imaging foriterative intraprocedural monitoring ofthe functional effect of therapy. Withthis technology, TRIP MR imaging of-fers an objective, quantitative method tocompare subjective angiographic end-points of TACE. In this study, there wasa wide variability in functional embolicendpoints, with AUC reductions rang-ing from 1% to 97%. This variability islikely related to intrinsic differences inperfusion to the targeted tumors.
This study has several importantlimitations. First, our sample size wasnot large enough to correlate long-term clinical outcomes with intrapro-cedural TACE endpoints. However, inan ongoing study, we hope to accom-plish this objective. Second, there is no
and multifocal HCC treated with TACE topatic segment 8. Perfusion maps before (b)ry units) depicts relative perfusion for each
ps usom heduc itra
Society of Interventional Radiology–

1256 • Subjective Angiographic vs Objective MR Endpoints of TACE October 2007 JVIR
approved angiographic classificationsystem to describe blood flow in targetvessels. We addressed this shortcom-ing by modifying a well establishedclassification scheme from the cardiol-ogy literature. However, other classifi-cation schemes could be proposed thatmight lead to different results. Finally,TACE research that focuses on func-tional MR imaging endpoints relies onthe availability of clinical MR/inter-ventional units, which are currentlyavailable at only a few large academicmedical centers. However, this type ofresearch can be expanded as theseunits become disseminated.
Our study shows that angiographicendpoints during TACE vary widely,have moderate reproducibility amongoperators, and do not correlate withfunctional MR imaging perfusion end-points. We recommend that futurepublications focused on TACE pro-vide more details regarding the angio-graphic endpoint employed, includingsome mention of the reproducibilityamong different operators to classifythese endpoints. We invite the inter-ventional radiology community to em-
MR Perfusion Change vs. SACE
0
10
20
30
40
50
60
70
80
90
100
1 320
Subjective Angiographic Chemoemoblization E
MR
Per
fusi
on C
han
ge
I II III
MR Perfusion Change vs. SACE
0
10
20
30
40
50
60
70
80
90
100
3210
Subjective Angiographic Chemoemoblization E
MR
Per
fusi
on
Ch
ang
e
I IIIII
.a
c.
ploy and/or refine an angiographic
tumor embolization endpoint scalesimilar to the TIMI scale used by car-diologists. An improved angiographicclassification scheme that correlateswith TRIP MR imaging perfusion re-duction would be especially desirable.Future research should also aim to de-termine the ideal angiographic andfunctional MR imaging endpoints forTACE with use of outcome measuressuch as imaging response, pathologicresponse, and survival.
References1. Marcos-Alvarez A, Jenkins RL, Wash-
burn WK, et al. Multimodality treat-ment of hepatocellular carcinoma in ahepatobiliary specialty center. ArchSurg 1996; 131:292–298.
2. Bramhall SR, Gur U, Coldham C, et al.Liver resection for colorectal metasta-ses. Ann R Coll Surg Engl 2003; 85:334–339.
3. Okada S, Okazaki N, Nose H, YoshimariM, Aoki K. Prognostic factors in patientswith hepatocellular carcinoma receivingsystemic chemotherapy. Hepatology 1992;16:112–117.
4. Colleoni M, Bajetta E, Nelli P, et al.Prognostic factors in patients affectedby hepatocellular carcinoma treated
l
54
oint (SACE) level
IR 1
MR
0
10
20
30
40
50
60
70
80
90
100
10
Subjective Angio
MR
Per
fusi
on C
han
ge
I
l
54
oint (SACE) level
IR 3
.b
Figure 7. Raw comand MR tumor perserver (n � 3) andoperator 2, and (c)
with systemic chemotherapy: the expe-
rience of the National Cancer Instituteof Milan. Ann Oncol 1993; 4:489–493.
5. Boucher E, Corbinais S, Brissot P, Boud-jema K, Raoul JL. Treatment of hepato-cellular carcinoma (HCC) with systemicchemotherapy combining epirubicin, cis-platinum and infusional 5-fluorouracil(ECF regimen). Cancer Chemother Phar-macol 2002; 50:305–308.
6. Llovet JM, Sala M, Castells L, et al.Randomized controlled trial of inter-feron treatment for advanced hepato-cellularcarcinoma.Hepatology2000;31:54–58.
7. Chow PK, Tai BC, Tan CK, et al.High-dose tamoxifen in the treatmentof inoperable hepatocellular carci-noma: a multicenter randomized con-trolled trial. Hepatology 2002; 36:1221–1226.
8. Lai CL, Wu PC, Chan GC, Lok AS, LinHJ. Doxorubicin versus no antitumortherapy in inoperable hepatocellularcarcinoma: a prospective randomizedtrial. Cancer 1988; 62:479–483.
9. Mulcahy MF. Management of hepa-tocellular cancer. Curr Treat OptionsOncol 2005; 6:423–435.
10. Llovet JM, Real MI, Montana X, et al.Arterial embolisation or chemoembolisa-tion versus symptomatic treatment in pa-
fusion Change vs. SACE level
5432
hic Chemoemoblization Endpoint (SACE) level
IR 2
IIII I IV
risons between angiographic endpointion reduction percentage for each ob-CE session (n � 15). (a) Operator 1, (b)rator 3.
leve
ndp
Per
grap
leve
ndp
pafusTAope
tients with unresectable hepatocellular car-

Lewandowski et al • 1257Volume 18 Number 10
cinoma: a randomised controlled trial.Lancet 2002; 359:1734–1739.
11. Lo CM, Ngan H, Tso WK, et al.Randomized controlled trial of transar-terial lipiodol chemoembolization forunresectable hepatocellular carcinoma.Hepatology 2002; 35:1164–1171.
12. Mavligit GM, Charnsangavej C, Car-rasco CH, et al. Regression of ocularmelanoma metastatic to the liver afterhepatic arterial chemoembolizationwith cisplatin and polyvinyl sponge.JAMA 1988; 260:974–976.
13. Tellez C, Benson AB 3rd, Lyster MT, etal. Phase II trial of chemoemboliza-tion for the treatment of metastaticcolorectal carcinoma to the liver andreview of the literature. Cancer 1998;82:1250–1259.
14. Soulen MC. Chemoembolization ofhepatic malignancies. Oncology (Will-iston Park) 1994; 8:77–84.
15. Salman HS, Cynamon J, Jagust M, et al.Randomized phase II trial of embo-lization therapy versus chemoemboli-zation therapy in previously treatedpatients with colorectal carcinoma met-astatic to the liver. Clin Colorectal Can-cer 2002; 2:173–179.
16. Therasse E, Breittmayer F, Roche A, etal. Transcatheter chemoembolizationof progressive carcinoid liver metasta-sis. Radiology 1993; 189:541–547.
17. Stokes KR, Stuart K, Clouse ME.Hepatic arterial chemoembolization formetastatic endocrine tumors. J Vasc In-terv Radiol 1993; 4:341–345.
18. Gupta S, Yao JC, Ahrar K, et al.Hepatic artery embolization and che-moembolization for treatment of pa-tients with metastatic carcinoid tu-mors: the M.D. Anderson experience.Cancer J 2003; 9:261–267.
19. Giroux MF, Baum RA, Soulen MC.Chemoembolization of liver metastasisfrom breast carcinoma. J Vasc IntervRadiol 2004; 15:289–291.
20. Rajan DK, Soulen MC, Clark TW, et al.Sarcomas metastatic to the liver: re-
sponse and survival after cisplatin, doxo-rubicin, mitomycin-C, Ethiodol, andpolyvinyl alcohol chemoembolization. JVasc Interv Radiol 2001; 12:187–193.
21. Brown DB, Geschwind JF, Soulen MC,Millward SF, Sacks D. Society of In-terventional Radiology position state-ment on chemoembolization of hepaticmalignancies. J Vasc Interv Radiol2006; 17:217–223.
22. Geschwind JF, Ramsey DE, van derWal BC, et al. Transcatheter arterialchemoembolization of liver tumors: ef-fects of embolization protocol on inject-able volume of chemotherapy and sub-sequent arterial patency. CardiovascIntervent Radiol 2003; 26:111–117.
23. Larson A WD, Atassi B, Sato K, et al.Transcatheter intraarterial first-passperfusion (TRIP)—MRI monitoring ofchemoembolization for hepatocellularcarcinoma. Radiology 2007 (in press).
24. Brown DB, Cardella JF, Sacks D, et al.Quality improvement guidelines fortranshepatic arterial chemoemboliza-tion, embolization, and chemothera-peutic infusion for hepatic malignancy.J Vasc Interv Radiol 2006; 17:225–232.
25. Georgiades CS, Hong K, D’Angelo M,Geschwind JF. Safety and efficacy oftransarterial chemoembolization in pa-tients with unresectable hepatocellularcarcinoma and portal vein thrombosis.J Vasc Interv Radiol 2005; 16:1653–1659.
26. Bruix J, Sherman M, Llovet JM, et al.Clinical management of hepatocellularcarcinoma. Conclusions of the Barce-lona-2000 EASL conference. EuropeanAssociation for the Study of the Liver.J Hepatol 2001; 35:421–430.
27. Soresi, M, Magliarisi C, Campagna P,et al. Usefulness of alpha-fetoproteinin the diagnosis of hepatocellular car-cinoma. Anticancer Res, 2003; 23:1747–1753.
28. Materne, R, Smith AM, Peeters F, et al.Assessment of hepatic perfusion pa-rameters with dynamic MRI. Magn Re-
son Med 2002; 47:135–142.29. TIMI Study Group. The Thromboly-sis in Myocardial Infarction (TIMI)trial. Phase I findings. N Engl J Med1985; 312:932–936.
30. Brown DB, Pilgram TK, Darcy MD, etal. Hepatic arterial chemoemboliza-tion for hepatocellular carcinoma: com-parison of survival rates with differentembolic agents. J Vasc Interv Radiol,2005; 16:1661–1666.
31. Hong, K, Kobeiter H, Georgiades CS,Torbenson MS, Geschwind JF. Effectsof the type of embolization particles oncarboplatin concentration in liver tu-mors after transcatheter arterial che-moembolization in a rabbit model ofliver cancer. J Vasc Interv Radiol 2005;16:1711–1717.
32. Kobayashi, N, Ishii M, Ueno Y, et al.Co-expression of Bcl-2 protein and vas-cular endothelial growth factor in hep-atocellular carcinomas treated by che-moembolization. Liver 1999; 19:25–31.
33. Xiong ZP, Yang SR, Liang ZY, et al.Association between vascular endothe-lial growth factor and metastasis aftertranscatheter arterial chemoemboliza-tion in patients with hepatocellular car-cinoma. Hepatobiliary Pancreat Dis Int2004; 3:386–390.
34. Rhee TK, Young JY, Larson AC, et al.Effect of transcatheter arterial emboli-zation on levels of hypoxia induciblefactor-1 alpha in rabbit VX2 liver tu-mors. J Vasc Interv Radiol 2007; 18:639–645.
35. Gwak GY, Yoon JH, Kim KM, et al.Hypoxia stimulates proliferation of hu-man hepatoma cells through the induc-tion of hexokinase II expression.J Hepatol 2005; 42:358–364.
36. Vali M, Liapi E, Kowalski J, et al.Intraarterial therapy with a new potentinhibitor of tumor metabolism (3-bro-mopyruvate): identification of therapeu-tic dose and method of injection in ananimal model of liver cancer. J Vasc In-
terv Radiol 2007; 18:95–101.