dipartimento di oncoematologia pediatrica e medicina ... · il ruolo dell’intesivista pediatrico...
TRANSCRIPT

Il ruolo dell’intesivista pediatrico nella gestione dei
pazienti sottoposti a trapianto di cellule staminali
ematopoietiche
Dipartimento di oncoematologia pediatrica e medicina
trasfusionale
Pietro Merli
Pietro Merli

Indications for HSCT

Introduction

Complications

ICU admission for HSCT patients
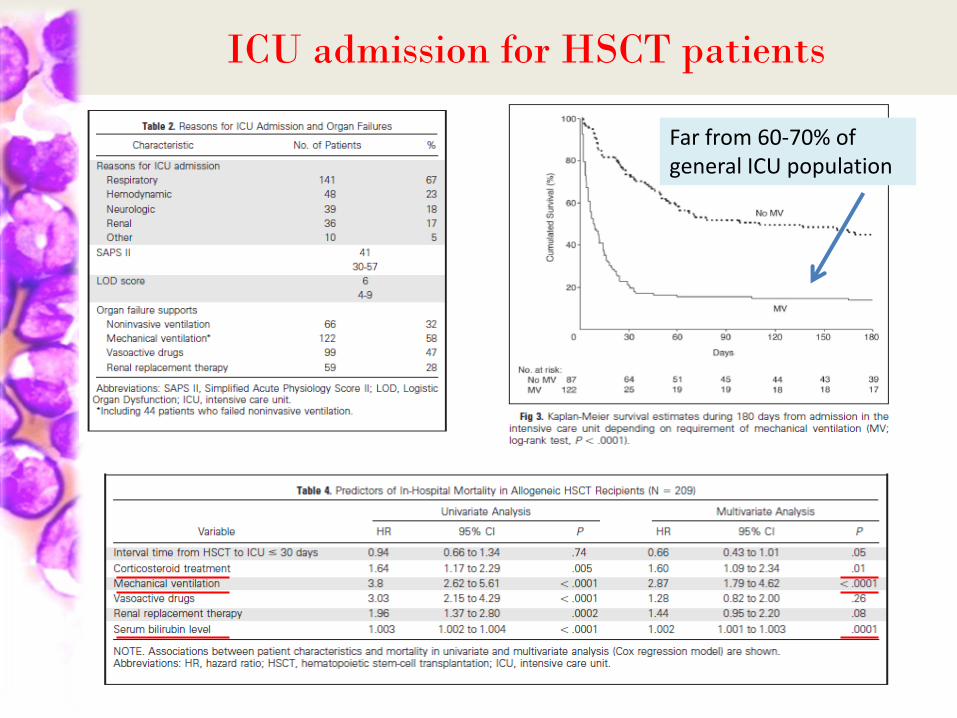
- The overall in-ICU, in-hospital, 6-month, and 1-year survival rates were 48.3%, 32.5%, 27.2%, and 21%, respectively; - Mechanical ventilation, elevated bilirubin level (and corticosteroid treatment for the indication of active graft-versus-host disease (GVHD)) were independent predictors of death in the whole cohort; - In the subgroup of patients requiring mechanical ventilation, associated organ failures, such as shock and liver dysfunction, were independent predictors of death; - ICU admission during engraftment period was associated with acceptable outcome in mechanically ventilated patients, whereas patients with late complications of HSCT in the setting of active GVHD had a poor outcome
Neither disease status at transplantation nor transplantation-related characteristics influenced the in-hospital outcome in allogeneic HSCT recipients
ICU admission for HSCT patients
Far from 60-70% of general ICU population

ICU admission for HSCT patients
Legline et al, BMT 2015
PICU admission for Pediatric HSCT patients
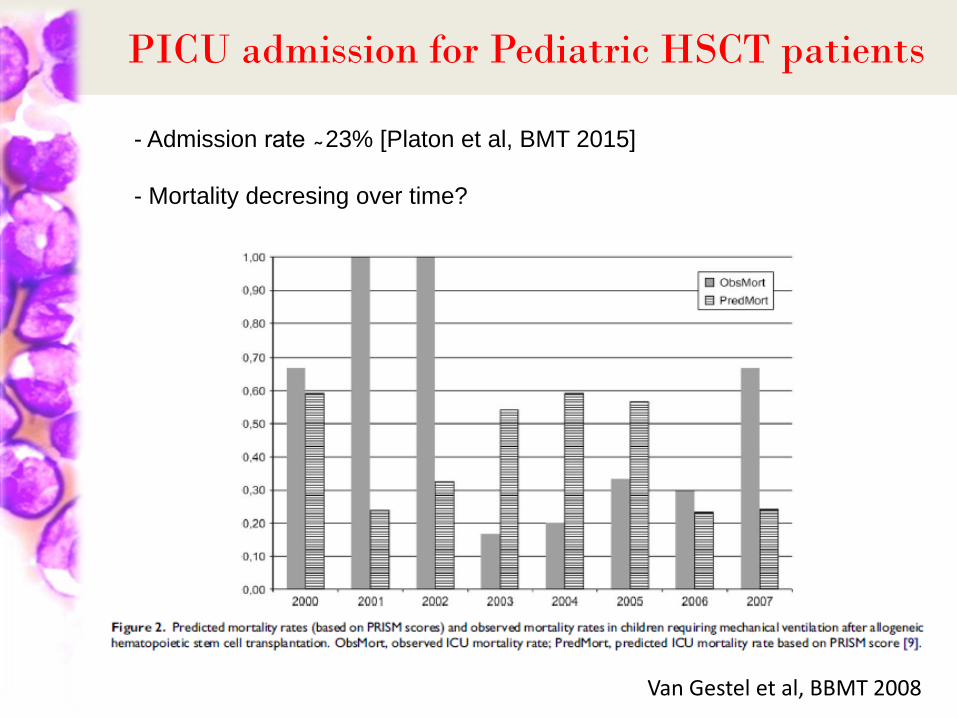
- Admission rate ̴ 23% [Platon et al, BMT 2015]
- Mortality decresing over time?
Van Gestel et al, BBMT 2008

Mortality during PICU permanence for HSCT patients
Van Gestel et al, Crit Care Med2008

PICU hospitalization for Pediatric HSCT patients
Van
Ge
stel
et
al, C
rit
Car
e M
ed2
00
8

Intensive Care for Pediatric HSCT patients
McA
rth
ur
et a
l, B
MT
20
11

Intensive Care for Pediatric HSCT patients
McArthur et al, BMT 2011
Indications for PCCM physician consultation

ECMO for Pediatric HSCT patients
ECMO should be considered in: 1) HSCT patients with either nonmalignant disorders or with malignancies at low risk of recurrence 2) when engraftment is acquired 3) when an effective etiologically targeted treatment of the HSCT complications is available
29 patients (ELSO registry between 1991-2012): -23 (79%) died during ECMO - 6 (21%) survived ECMO - 3 (10%) discharged

PICU for HSCT patients: OPBG experience
Study period: 01/06/2015-30/11/2015
Number/ median
Percentage/ range
Total number of patients 54 100%
Male/Female 32/22 59%/41%
Age at diagnosis (years) 8.5 0.6-23
Malignant/Non-Malignant 28/26 52%/48%
MAC/RIC* 34/20 63%/37%
* MAC, MyeloAblativeConditioning; RIC, Reduced-Intensity Conditioning
Update 15/12/2015

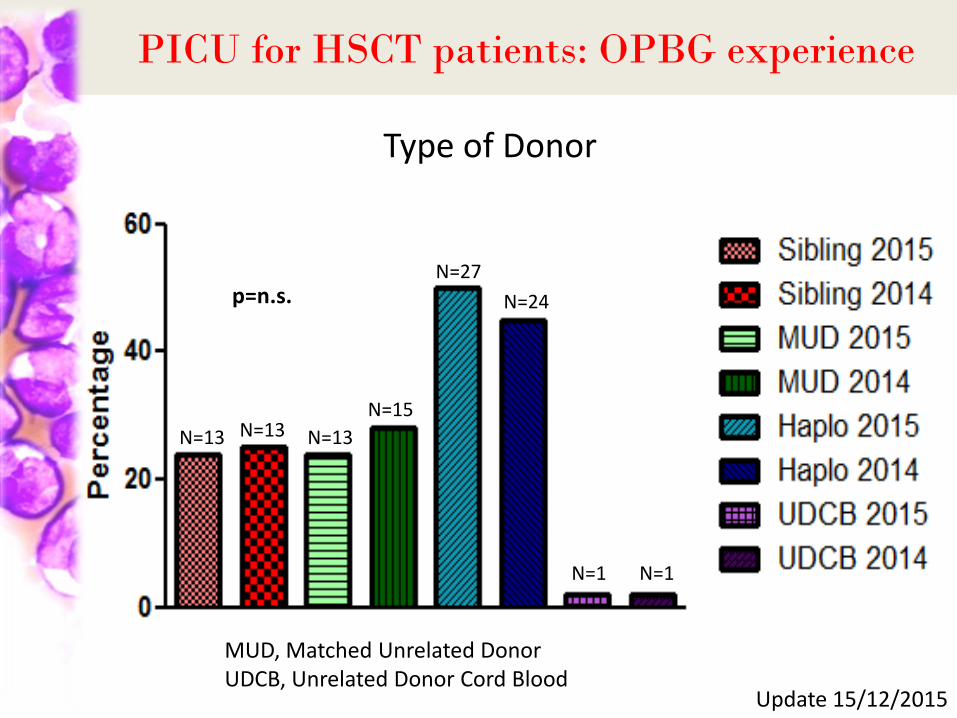
PICU for HSCT patients: OPBG experience
Type of Donor
N=13 N=13
N=27
N=1
MUD, Matched Unrelated Donor UDCB, Unrelated Donor Cord Blood
Update 15/12/2015
PICU for HSCT patients: OPBG experience
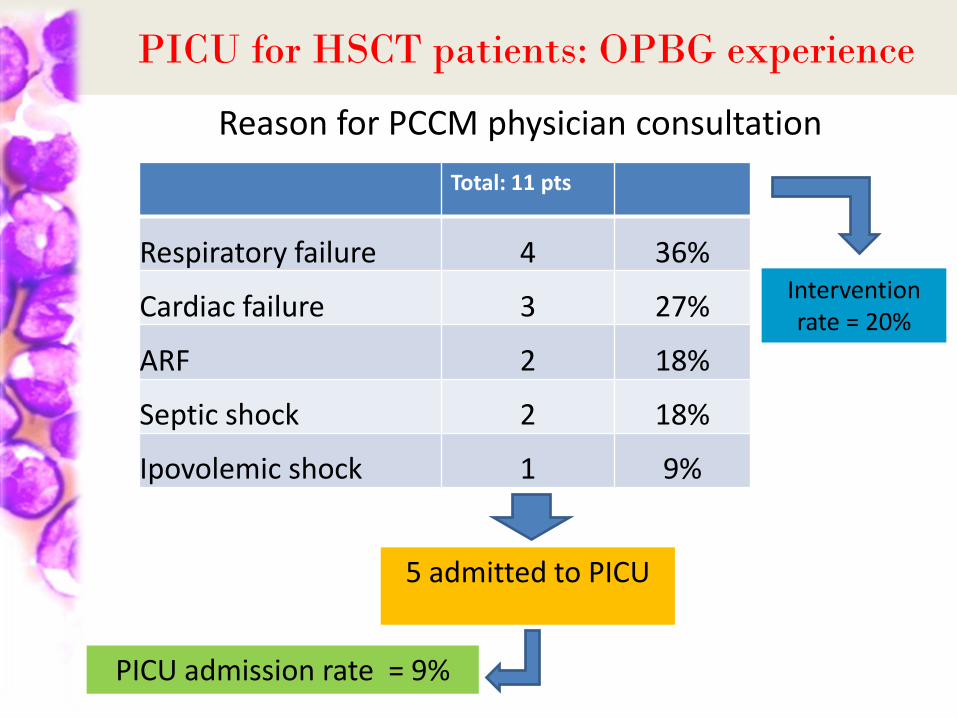
Reason for PCCM physician consultation
Total: 11 pts
Respiratory failure 4 36%
Cardiac failure 3 27%
ARF 2 18%
Septic shock 2 18%
Ipovolemic shock 1 9%
PICU admission rate = 9%
5 admitted to PICU
Intervention rate = 20%
PICU for HSCT patients: OPBG experience
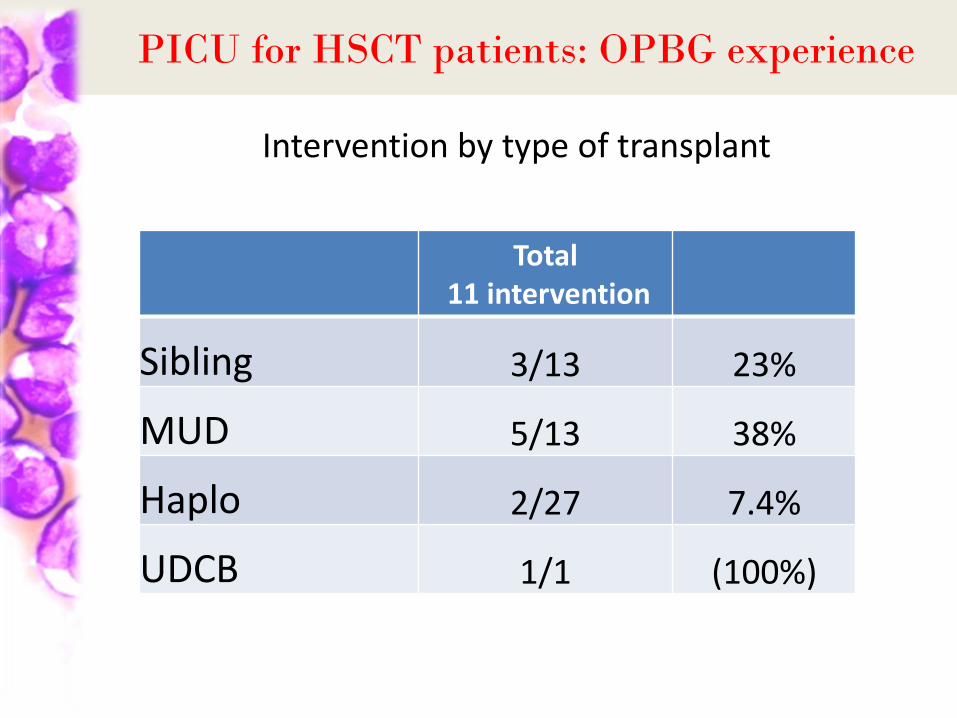
Intervention by type of transplant
Total 11 intervention
Sibling 3/13 23%
MUD 5/13 38%
Haplo 2/27 7.4%
UDCB 1/1 (100%)
PICU for HSCT patients: OPBG experience
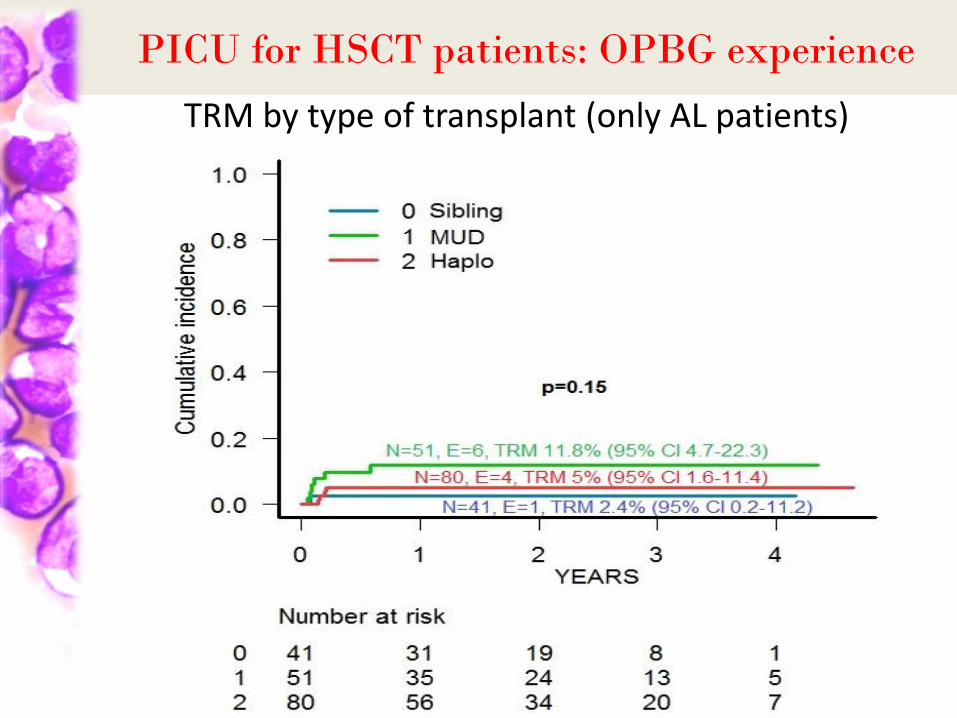
TRM by type of transplant (only AL patients)

PICU for HSCT patients: OPBG experience
Intervention
Indication
Respiratory failure
4
Cardiac failure
3
ARF
2
Septic shock
2
Hypovolemic/ hemorrhagic shock
1
HFNC - 2 CPAP - 2 MV
Inotropic support
- 1 CRRT - 1 fenoldopam
Vasoactive support
Replacement therapy Vasoactive support

PICU in HSCT patients: OPBG experience
OS of patients requiring PICU admission

PICU in HSCT patients: OPBG experience
OS of patients receiving PCCM physician evaluation
PICU in HSCT patients: OPBG experience
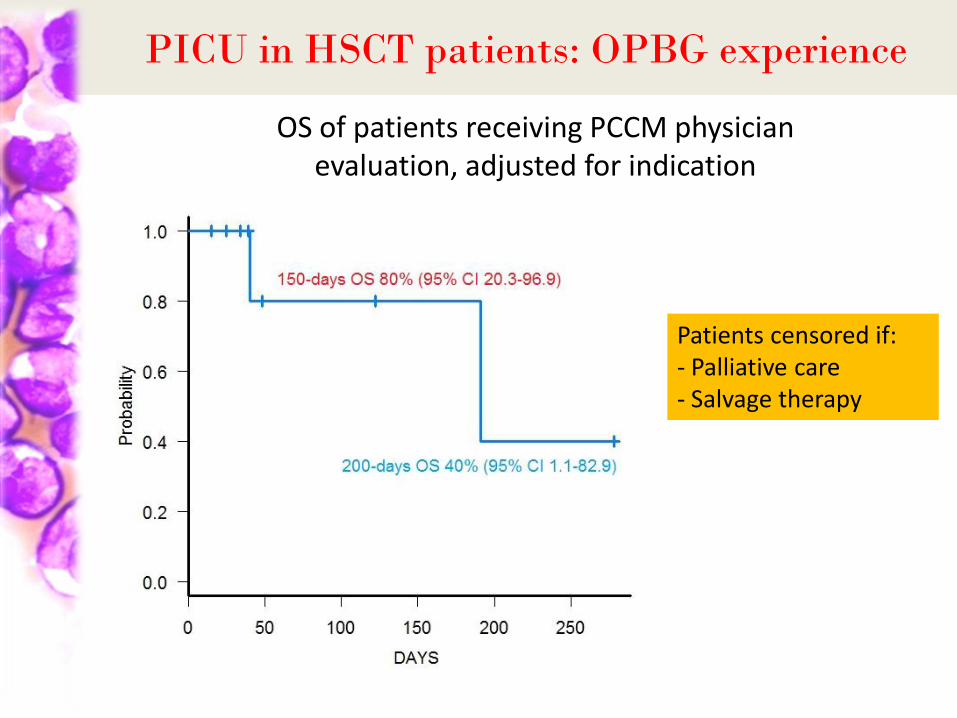
OS of patients receiving PCCM physician evaluation, adjusted for indication
Patients censored if: - Palliative care - Salvage therapy

PICU for HSCT patients: OPBG experience
Comparison with historical cohort Study period: 01/06-30/11/2015 vs 01/06-30/11/2014
Number/ Median yr 2015
Number/ Median yr 2014
P-value
Total number of patients 54 53
Male/Female 32/22 34/19 0.69
Age at diagnosis (years) 8.5 (0.6-23) 10.1 (0.7-22.2) 0.09
Malignant/Non-Malignant 28/26 32/21 0.43
MAC/RIC* 34/20 24/29 0.08
* MAC, MyeloAblativeConditioning; RIC, Reduced-Intensity Conditioning
Update 15/12/2015
PICU for HSCT patients: OPBG experience
Type of Donor
N=13
MUD, Matched Unrelated Donor UDCB, Unrelated Donor Cord Blood
Update 15/12/2015
N=13 N=13
N=15
N=1 N=1
N=27
N=24 p=n.s.
PICU for HSCT patients: OPBG experience
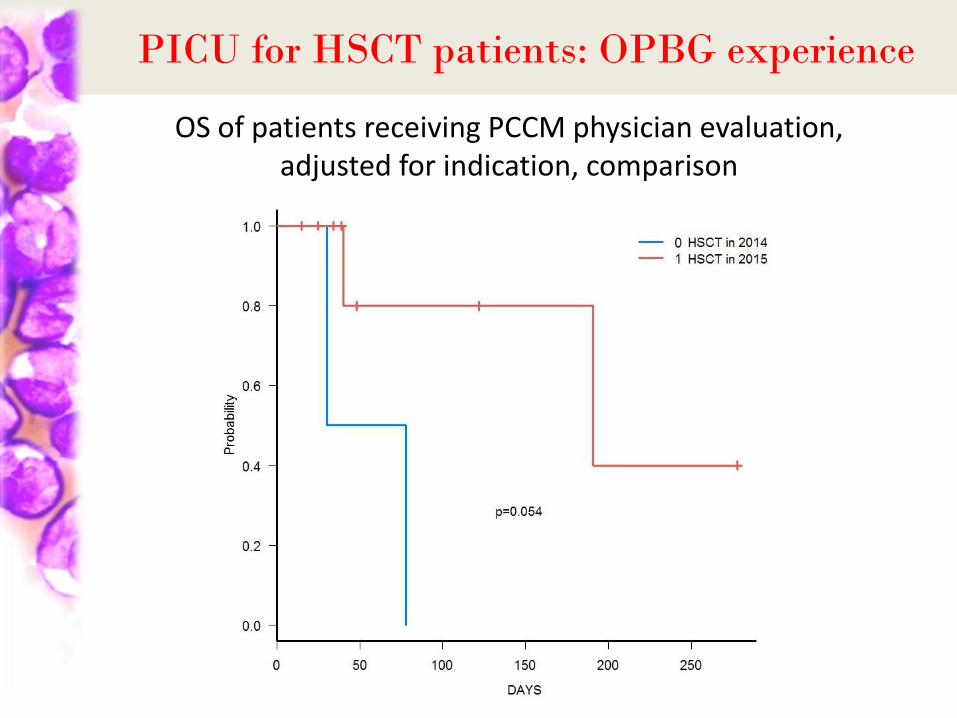
OS of patients receiving PCCM physician evaluation, adjusted for indication, comparison

Proposal for new Intensive Care approach for
Pediatric HSCT patients requirind PICU admission
time
time
inte
nsi
ty o
f ca
re OLD model (“progressive intensity”)
NEW model (“top-down”)
Example: HFNC
Intubation
BMT unit
PICU Example: HFNC
NIV
Intubation
NIV

Conclusions
- PCCM physician plays an important role in the management of pediatric patients undergoing HSCT;
- A tight cooperation between PCCM and BMT physician seems to ameliorate the outcome of children who received an HSCT;
- Despite improvements in supportive care, mortality remains high; thus, new approaches/treatment strategies are desirable;
- Since robust data on PICU admission for pediatric patients undergoing HSCT are lacking, well-designed studies will clarify indications to (and timing for) PICU admission, prognostic factors and optimal treatment program in this setting.
