cat fetalcellcount by flow cytometry - uz leuven · casus (2) rhd neg mother & rhd‐neg...
TRANSCRIPT

CATCAT
Fetal Cell Countby Flow Cytometry
17‐6‐2008
De Vos NathalieDe Vos Nathalie

INTRODUCTIONINTRODUCTION
B l i 121 382 bi th i 2006• Belgium n = 121 382 births in 2006• 15% Rhesus D negative mothers (n = 18 207 in 2006)
Kenniscentrum Statistiek – Vlaamse Overheid2004 KCE Nationale richtlijn prenatale zorg
IgM IgG
sensitisingevent
HDNevent

HISTORYHISTORY
300 µg = 1500 IU
1960s: routine postnatal anti‐D prophylaxis Sensitization decreased from 14 7% to 1 6% 2003 NVOG; 2003 Vox SangSensitization decreased from 14,7% to 1,6% 2003 NVOG; 2003 Vox Sang
1998 in NL, 2002 in UK: routine antenatal anti‐D prophylaxis (RAADP)Sensitization decreased from 1,5% to 0,2%2006 Proefschrift Pelikan ; 1999 Lee Guidelines Tranfus Med, 2003 NVOG, 2003 Vox Sang

RAADP to all non‐sensitized RhD‐negative pregnant women in a first pregnancy
W k AUSTR / NZ UK NL CAN / BWeek AUSTR / NZ UK NL CAN / B
28 625 IU 500 IU 1500 IU
30 1000 IU
34 625 IU 500 IU
2003 NBA ; 2002 ANZSBT
2006 BCSH; 2002 NICE
2003 NVOG 2003 SOGC; 2006 CEBAM2002 ANZSBT 2002 NICE;
1999 Lee ea.2006 CEBAM; 2004 KCE; RhoGAM ® product insertproduct insert

T ½ = 18dT ½ = 18d
~5 ng/ml
Neutralising power ~2,5 ml fetal blood
5 ng/ml
2003 Bichler ea BJOG Week after antiD administration

QUESTIONSQUESTIONS
I. CLINICAL RELEVANCE: Which clinical indication(s) do Guidelines propose for fetal cell count in maternal blood?
II. DIAGNOSTIC‐THERAPEUTIC IMPACT: Is it necessary to have FCM 24h/24h 7d/7d available? If not what is clinicallyFCM 24h/24h 7d/7d available? If not, what is clinically acceptable?
What is the benefit of follow‐up samples?What is the benefit of follow up samples?
III TECHNICAL PERFORMANCE: Is FCM a reliable method for theIII. TECHNICAL PERFORMANCE: Is FCM a reliable method for the detection of fetal cells in routine laboratory? Is it more accurate than the KBB method? Can the limit of detection (analytical sensitivity) reach the clinical relevance?

I CLINICAL RELEVANCEI. CLINICAL RELEVANCE
Calculate RhoGAM dose for massive FMT:IIb‐B BCSH 2006; III‐B SOGC 2003; B RCOG 2002
– Potentially sensitising events during pregnancy: • Macro‐trauma
I i t l di i / I t th ti i t ti• Invasive prenatal diagnosis / In‐utero therapeutic intervention
• External cephalic version
• Ectopic pregnancyEctopic pregnancy
• Intrauterine death, miscarriage, termination of pregnancy
d2006 BCSH; 2003 SOGC; 2003 NBA; 1999 Lee ea; Uptodate
– Spontaneous in 3d trim
– At delivery (0 3 – 1 7% have massive FMT > 30 ml fetal blood)At delivery (0,3 1,7% have massive FMT > 30 ml fetal blood)2002 Ochsenbein ea; 2002 Chen ea

NOT RELEVANTNOT RELEVANT
Fetal cell detection in minor traumata:
2003 SOGC
Sensitization when FMT ≥ 0,1 ml fetal blood
2003 SOGC
overlap
Natural process of fetal cell release 0,05 – 0,12 ml fetal blood
1997 Warzynski ea; 1984 Medearis ea

II. DIAGNOSTIC‐THERAPEUTIC IMPACT
• Failure to prevent alloimmunization:1. Insufficent dose of RhoGAM
2. Administered too late

II. DIAGNOSTIC‐THERAPEUTIC IMPACT
• Failure to prevent alloimmunization:1. Insufficent dose of RhoGAM
> f ll l h FMT > 15 l f t l bl d=> follow‐up samples when FMT > 15 ml fetal blood
48h after RhoGAM administrationG id li 1999 BCSH i h i bilit t dGuidelines 1999 BCSH; in‐house variability study
2. Administered too late

II. DIAGNOSTIC‐THERAPEUTIC IMPACT
• Failure to prevent alloimmunization:1. Insufficent dose of RhoGAM
2. Administered too late

II. DIAGNOSTIC‐THERAPEUTIC IMPACT
• Failure to prevent alloimmunization:1. Insufficent dose of RhoGAM
2. Administered too late
=> administer RhoGAM ASAP within 72h;
up to 10d (28d)
‘at no time anti‐D should be withheld based upon,
d h l f f ’
Guidelines 2004 BCSH; 2003 NBA; 2003 SOGC; 2002 RCOG
or pending, the results of a test to quantify FMT’
=> fetal cell count TAT: report result ASAP within 72hGuidelines 2002 ANZSBT
=> fetal cell count TAT: report result ASAP within 72hGuidelines 2004 BCSH; 2002 ANZSBT

Diagnostic actionsDiagnostic actions2006 BCSH Guideline
weeks of gestation transfusion tests fetal cell count
< 16 NVOG No recommendations are specified
< 20 BCSHdetermine ABOD/anti-D of mother when potentially sensitising episode /
> 20 BCSH or 1) determine ABOD/anti-D of mother> 20 BCSH or > 16 NVOG
1) determine ABOD/anti D of mother when potentially sensitising episode 2) administer 1 dose of RhoGAM®
3) asses FMT when potentially sensitising episode
4) administer supplemental RhoGAM® if needed
28 BCSH or determine ABOD/anti-D of mother prior to RAADP administration to
30 NVOGpmother /
birth 1) determine ABOD neonatus + mother if neonatus is RhD-positive:
2) administer 1 dose of RhoGAM®2) administer 1 dose of RhoGAM®
3) asses FMT
4) administer supplemental RhoGAM® if needed

Diagnostic actionsDiagnostic actions2006 BCSH Guideline
weeks of gestation transfusion tests fetal cell count
< 16 NVOG No recommendations are specified
< 20 BCSHdetermine ABOD/anti-D of mother when potentially sensitising episode /
> 20 BCSH or 1) determine ABOD/anti-D of mother> 20 BCSH or > 16 NVOG
1) determine ABOD/anti D of mother when potentially sensitising episode 2) administer 1 dose of RhoGAM®
3) asses FMT when potentially sensitising episode
4) administer supplemental RhoGAM® if needed
28 BCSH or determine ABOD/anti-D of mother prior to RAADP administration to
30 NVOGpmother /
birth 1) determine ABOD neonatus + mother if neonatus is RhD-positive:
2) administer 1 dose of RhoGAM®2) administer 1 dose of RhoGAM®
3) asses FMT
4) administer supplemental RhoGAM® if needed

III TECHNICAL PERFORMANCEIII. TECHNICAL PERFORMANCE
CV Analytical sensitivity(at least 0 6% fRBC or 30 ml fetal blood)(at least 0,6% fRBC or 30 ml fetal blood)
KBB 39,5% ‐ 71,8% 5 ml fetal blood
FCM(50 000 events)
< 15 % 0,1% fRBC or5 ml fetal blood
FCM :2003 Lafferty; 1998 Davis; 2002 Chen; 2002 Ochsenbein; 2006 Pelikan
• 500 000 events will lower CV < 10% & increase sensitivity
• target anti‐HbF versus anti‐D
• 2 parameters HbF/CA

ESTIMATED QUANTITY OF FMT1800 ml maternal RBC volume
ESTIMATED QUANTITY OF FMT2004 BCSH Guideline1800 ml maternal RBC‐volume
corrected for fetal RBC (22% larger than adult RBC) corrected for staining efficiency of 92%
2004 BCSH Guideline2002 ANZSBT Guideline
# ml FMT = (1800 ml x F / A) x 1.22 x 1.09
Shortcut method 1993 Mollison eds. Blood Transfusion in Clinical Medicine
Corrected # ml FMT = 2400 x F / A

ESTIMATED QUANTITY OF FMTESTIMATED QUANTITY OF FMTCorrected # ml FMT 2400 x F / ACorrected # ml FMT = 2400 x F / A
1800 ml arbitrary volume of maternal RBC (postpartum)1800 ml arbitrary volume of maternal RBC (postpartum)
LAG UZ Leuven:
ml FMT = 4500 ml x F / A
4500 ml arbitrary volume of maternal blood
/
ml FMT = 4500 ml x F / 150000
ml FMT = F x 0.03
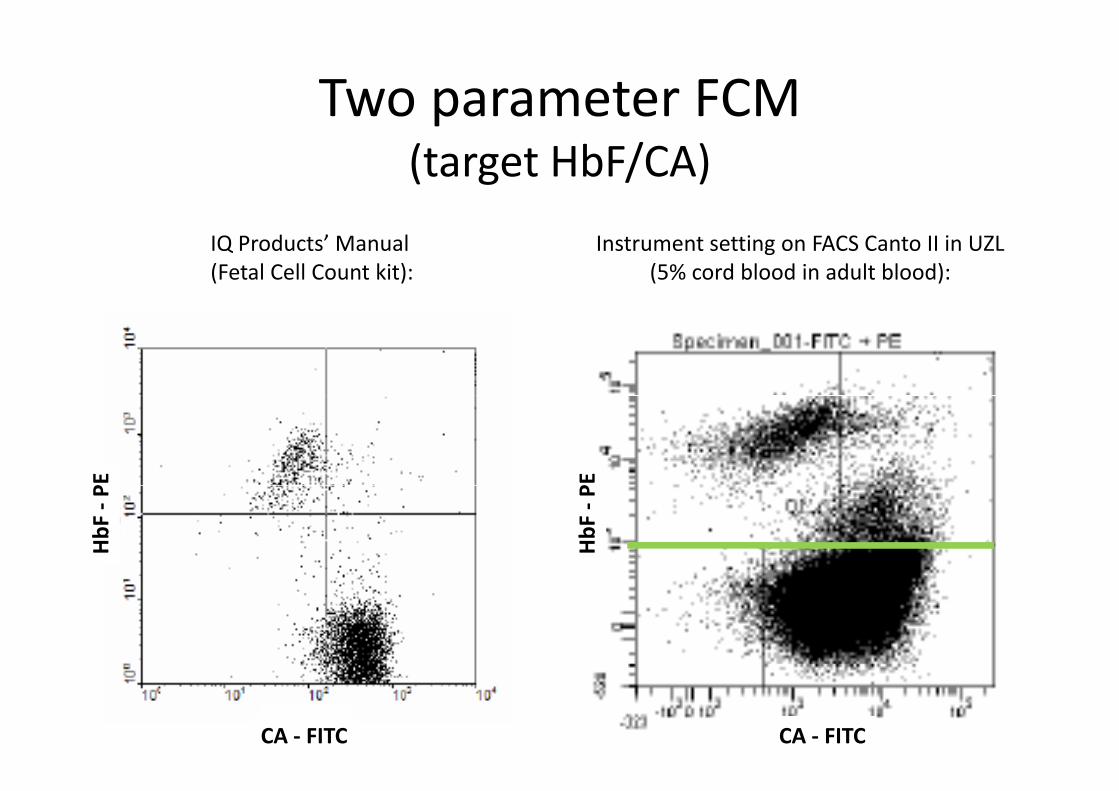
Two parameter FCM p(target HbF/CA)
Instrument setting on FACS Canto II in UZL(5% cord blood in adult blood):
IQ Products’ Manual(Fetal Cell Count kit):
PE PE
HbF
‐P
HbF
‐P
CA ‐ FITCCA ‐ FITC

Two parameter FCM p(target HbF/CA)
Instrument setting on FACS Canto II in UZL(5% cord blood in adult blood):
fRBC fRBC
PEHbF
‐P
CA ‐ FITCHbF ‐ PE

Two parameter FCM p(target HbF/CA)
Routine sample (KBB 11,7 ml fetal blood or 0,3% fRBC):
fRBC 0,5%fRBC
PEHbF
‐P
0,5%
CA ‐ FITCHbF ‐ PE

CORRELATION FCM KBBCORRELATION FCM ‐ KBB
• Target HbF:
r 2 = 0,99 (N = 170)r 0,99 (N 170)
randomised controlled trial 2007 Fernandes ea. Pren Diagn
• Target RhD (indirect FCM) and HbF (KBB):Target RhD (indirect FCM) and HbF (KBB):
r 2 = 0,714 1995 Johnson ea. J Clin Pathol

CORRELATION FCM KBBCORRELATION FCM ‐ KBB
‘FCM d FMT 4 l fRBC h h d b i l ifi d b KBB’• ‘FCM can detect FMT < 4 ml fRBC that had been incorrectly quantified by KBB’
• ‘KBB could lead to inadequate anti‐D prophylaxis when FMT > 10ml fetal blood’(2003 Lafferty ea Am J Clin Pathol)
(Lubenko 1999)
• ‘FCM was more sensitive and more timely than KBB’
(2003 Lafferty ea. Am J Clin Pathol)
(2007 Fernandes Pren Diagn)
• ‘FCM produces results within a narrower range, smaller SD & CV compared to KBB’
• ‘FCM is accepted as the most accurate quantitative test for assessing FMT’
(2002 ANZSBT GUIDELINES)
• ‘FCM is the method of choice for quantification if readily available’
(Guidelines 2003 NBA; 2002 ANZSBT; 2001 NCCLS/CLSI; 1999 Lee ea Transfus Med)
(Guidelines 2003 NBA; 2002 ANZSBT )
• ‘FCM is useful for follow‐up of large FMT’(1999 Lee ea. Transfus Med)

KBBKBB
Nieuwe ‘Kleihauer Kit’ (Immucor Gamma)– validatiedossier d.d. 05‐05‐2008
– SOP‐042 (bijlage 1) d.d. 08‐05‐2008

median [IQR] = 0,03 [0 – 0,06] median [IQR] = 12 [10,5 ‐ 13]
8 10 12 14 16 18
sample_approximately_12_ml_fetal_blood
0,00 0,05 0,10 0,15
negative_sample
median [IQR] = 15 [15 ‐ 21] median [IQR] = 44 [34 ‐ 47]
10 20 30 40 50 60
strongly_positive_control
5 10 15 20 25 30 35
strongly_positive_sample

KBB sources of errorsKBB sources of errors
• Assumptions in the formula for calculating FMT
• Variability in thickness of bloodfilm• Variability in thickness of bloodfilm
• Staining efficiency only 92%g y y
• Inter‐individual variability:• A different microscopic field for counting contains a different number of RBC’s
b f h f f l ll h• Subjectivity for the interpretation of a fetal cell: the difficulty of classifying cells of intermediate staining.

FETALtrol CONTROLFETALtrol CONTROL(Trillium Diagnostics)
• € 368 per set• stability 3 months
00 00 00
y• suitable for FCM and for KBB
300
350
40
Adult_RBCs
300
350
40
Adult_RBCs
030
035
040
Adult_RBCs
150
200
250
Num
ber
150
200
250
Num
ber
150
200
250
Num
ber
050
100
Fetal_RBCs
050
100
Fetal_RBCs
050
100
Fetal_RBCs
10 1 10 2 10 3 10 4
anti-HbF10 1 10 2 10 3 10 4
anti-HbF10 1 10 2 10 3 10 4
anti-HbF
Level 1 (0‐0,02% fRBC) Level 2 (0,12‐0,24% fRBC) Level 3 (0,79‐1,58% fRBC)=> Negative => detectable => detectable

Query fetal cell countQuery fetal cell count• dec 2005 ‐ dec 2007 N = 1913 requests (~ 1000/year)q y
• follow‐up samples 26% (no massive FMT)
FMT (ml fetal blood) N %( )
< 5 ml 1892/1913 98,9
5 – 15 ml 13/1913 0,7
15 ‐ 20 ml 1/1913 0,05
> 20 ml 7/1913 0,4
• range of massive FMT 16,4 – 90 ml fetal bloodCasus (1) 51,3 ml was HPFH
Casus (2) RhD pos motherCasus (2) RhD pos mother
Casus (2) RhD neg mother & RhD‐neg neonatus
Casus (1) 22,5 ml received 2 doses RhoGAM
Casus (1) 29 3 ml received 1 dose RhoGAM => enough ?Casus (1) 29,3 ml received 1 dose RhoGAM => enough ?
Casus (1) 90 ml with anaemic neonatus => ?

QUESTIONSQUESTIONS
I. CLINICAL RELEVANCE: Which clinical indication(s) do Guidelines propose for fetal cell count in maternal blood?M i FMT
II. DIAGNOSTIC‐THERAPEUTIC IMPACT: Is it necessary to have FCM 24h/24h 7d/7d available? If not what is clinically
Massive FMT
FCM 24h/24h 7d/7d available? If not, what is clinically acceptable?
What is the benefit of follow‐up samples?
Within 72h
Confirm massive FMTWhat is the benefit of follow up samples?
III TECHNICAL PERFORMANCE: Is FCM a reliable method for the
Confirm massive FMT
III. TECHNICAL PERFORMANCE: Is FCM a reliable method for the detection of fetal cells in routine laboratory? Is it more accurate than the KBB method? Can the limit of detection (analytical sensitivity) reach the clinical relevance?
0,6% fRBC0,1% fRBCYes.

IV COST IMPACTIV. COST IMPACT
KBB FCM
Reagent cost per test (direct cost) € 1,29 € 45,15(incl. controls)
Primary activity of MLT € 30,21 (50 min) € 66,46 (1h50)
THEORETICAL COST PER TEST € 31,50 € 111,61
• ‘erythrocyten – foetale, telling in het bloed van de moeder’
• B200 > honorarium € 5 82• B200 => honorarium € 5,82
• Tarief voor gehospitaliseerde & ambulante patiënt € 1,45

V DECISION MAKINGV. DECISION MAKING
• Guidelines suggest FCM for accurate estimation of massive FMT
• Arguments against FCM implementation:– in UZ Leuven only 0 4% FMT > 15 ml fetal blood (~ 4 samples a year);in UZ Leuven only 0,4% FMT > 15 ml fetal blood ( 4 samples a year);
– no expertise;
– difficult interpretation of cytograms.

RhD+ mother RhD- mother
RhD- foetus
free fetal DNA in maternal blood unknown RhD foetus
check motherABOD/anti D
delivery (FMT)RAADP at week 28*No RhoGAM > week 16**potentially sensitizing
ABOD/anti-D
1500 I.U.potentially sensitizing event (FMT) Rhesus typing
on cord bloodcheck
1500 I.U. RhD+ neonatus RhD- neonatusmotherABODanti-D
No RhoGAMFetal cell count + follow-up if FMT > 15 ml fetal blood***
FMT < 20 ml fetal blood FMT ≥ 20 ml fetal blood
No extra RhoGAMNo extra RhoGAMextra dose

RhD+ mother RhD- mother
RhD- foetus
free fetal DNA in maternal blood unknown RhD foetus
check motherABOD/anti D
delivery (FMT)RAADP at week 28*No RhoGAM > week 16**potentially sensitizing
ABOD/anti-D
1500 I.U.potentially sensitizing event (FMT) Rhesus typing
on cord bloodcheck
1500 I.U. RhD+ neonatus RhD- neonatusmotherABODanti-D
No RhoGAMFetal cell count + follow-up if FMT > 15 ml fetal blood***
FMT < 20 ml fetal blood FMT ≥ 20 ml fetal blood
No extra RhoGAMNo extra RhoGAMextra dose

RhD+ mother RhD- mother
RhD- foetus
free fetal DNA in maternal blood unknown RhD foetus
check motherABOD/anti D
delivery (FMT)RAADP at week 28*No RhoGAM > week 16**potentially sensitizing
ABOD/anti-D
1500 I.U.potentially sensitizing event (FMT) Rhesus typing
on cord bloodcheck
1500 I.U. RhD+ neonatus RhD- neonatusmotherABODanti-D
No RhoGAMFetal cell count + follow-up if FMT > 15 ml fetal blood***
FMT < 20 ml fetal blood FMT ≥ 20 ml fetal blood
No extra RhoGAMNo extra RhoGAMextra dose

Cell‐free fetal DNAin maternal plasma
D Mi t l 04 223 87 81Dr. Minon, tel 04 223 87 81 2008 Minon JM ea. Transf

RhD+ mother RhD- mother
RhD- foetus
free fetal DNA in maternal blood unknown RhD foetus
check motherABOD/anti D
delivery (FMT)RAADP at week 28*No RhoGAM > week 16**potentially sensitizing
ABOD/anti-D
1500 I.U.potentially sensitizing event (FMT) Rhesus typing
on cord bloodcheck
1500 I.U. RhD+ neonatus RhD- neonatusmotherABODanti-D
No RhoGAMFetal cell count + follow-up if FMT > 15 ml fetal blood***
FMT < 20 ml fetal blood FMT ≥ 20 ml fetal blood
No extra RhoGAMNo extra RhoGAMextra dose

RhD+ mother RhD- mother
RhD- foetus
free fetal DNA in maternal blood unknown RhD foetus
check motherABOD/anti D
delivery (FMT)RAADP at week 28*No RhoGAM > week 16**potentially sensitizing
ABOD/anti-D
1500 I.U.potentially sensitizing event (FMT) Rhesus typing
on cord bloodcheck
1500 I.U. RhD+ neonatus RhD- neonatusmotherABODanti-D
No RhoGAMFetal cell count + follow-up if FMT > 15 ml fetal blood***
FMT < 20 ml fetal blood FMT ≥ 20 ml fetal blood
No extra RhoGAMNo extra RhoGAMextra dose

RhD+ mother RhD- mother
RhD- foetus
free fetal DNA in maternal blood unknown RhD foetus
check motherABOD/anti D
delivery (FMT)RAADP at week 28*No RhoGAM > week 16**potentially sensitizing
ABOD/anti-D
1500 I.U.potentially sensitizing event (FMT) Rhesus typing
on cord bloodcheck
1500 I.U. RhD+ neonatus RhD- neonatusmotherABODanti-D
No RhoGAMFetal cell count + follow-up if FMT > 15 ml fetal blood***
FMT < 20 ml fetal blood FMT ≥ 20 ml fetal blood
No extra RhoGAMNo extra RhoGAMextra dose

RhD+ mother RhD- mother
RhD- foetus
free fetal DNA in maternal blood unknown RhD foetus
check motherABOD/anti D
delivery (FMT)RAADP at week 28*No RhoGAM > week 16**potentially sensitizing
ABOD/anti-D
1500 I.U.potentially sensitizing event (FMT) Rhesus typing
on cord bloodcheck
1500 I.U. RhD+ neonatus RhD- neonatusmotherABODanti-D
No RhoGAMFetal cell count + follow-up if FMT > 15 ml fetal blood***
FMT < 20 ml fetal blood FMT ≥ 20 ml fetal blood
No extra RhoGAMNo extra RhoGAMextra dose

RhD+ mother RhD- mother
RhD- foetus
free fetal DNA in maternal blood unknown RhD foetus
check motherABOD/anti D
delivery (FMT)RAADP at week 28*No RhoGAM > week 16**potentially sensitizing
ABOD/anti-D
1500 I.U.potentially sensitizing event (FMT) Rhesus typing
on cord bloodcheck
1500 I.U. RhD+ neonatus RhD- neonatusmotherABODanti-D
No RhoGAMFetal cell count + follow-up if FMT > 15 ml fetal blood***
FMT < 20 ml fetal blood FMT ≥ 20 ml fetal blood
No extra RhoGAMNo extra RhoGAMextra dose

RhD+ mother RhD- mother
RhD- foetus
free fetal DNA in maternal blood unknown RhD foetus
check motherABOD/anti D
delivery (FMT)RAADP at week 28*No RhoGAM > week 16**potentially sensitizing
ABOD/anti-D
1500 I.U.potentially sensitizing event (FMT) Rhesus typing
on cord bloodcheck
1500 I.U. RhD+ neonatus RhD- neonatusmotherABODanti-D
No RhoGAMFetal cell count + follow-up if FMT > 15 ml fetal blood***
FMT < 20 ml fetal blood FMT ≥ 20 ml fetal blood
No extra RhoGAMNo extra RhoGAMextra dose

RhD+ mother RhD- mother
RhD- foetus
free fetal DNA in maternal blood unknown RhD foetus
check motherABOD/anti D
delivery (FMT)RAADP at week 28*No RhoGAM > week 16**potentially sensitizing
ABOD/anti-D
1500 I.U.potentially sensitizing event (FMT) Rhesus typing
on cord bloodcheck
1500 I.U. RhD+ neonatus RhD- neonatusmotherABODanti-D
No RhoGAMFetal cell count + follow-up if FMT > 15 ml fetal blood***
FMT < 20 ml fetal blood FMT ≥ 20 ml fetal blood
No extra RhoGAMNo extra RhoGAMextra dose

RhD+ mother RhD- mother
RhD- foetus
free fetal DNA in maternal blood unknown RhD foetus
check motherABOD/anti D
delivery (FMT)RAADP at week 28*No RhoGAM > week 16**potentially sensitizing
ABOD/anti-D
1500 I.U.potentially sensitizing event (FMT) Rhesus typing
on cord bloodcheck
1500 I.U. RhD+ neonatus RhD- neonatusmotherABODanti-D
No RhoGAMFetal cell count + follow-up if FMT > 15 ml fetal blood***
FMT < 20 ml fetal blood FMT ≥ 20 ml fetal blood
No extra RhoGAMNo extra RhoGAMextra dose

TO DO / ACTIONSTO DO / ACTIONS
l f f l b h1. No implementation of FCM. KBB training of laboratory technicians.
2 Report limit FMT < 5 ml fetal blood2. Report limit FMT < 5 ml fetal blood.
3. Alarm value of FMT > 15 ml fetal blood => phone & FU.
4. Fetal cell count introduction in Diagnostic Prenatal Care Path.
Do the gynaecologists consider using the
clinical‐diagnostic‐therapeutic algorithm?clinical diagnostic therapeutic algorithm?

Diagnostic prenatal care pathConsultatie 20-24 weken
Diagnostic prenatal care path
2082 Cytomegalovirus IgG (zo IgG niet gekend positief)
2084 Cytomegalovirus IgM (zo IgG niet gekend positief preconceptie)
2087 Toxoplasma IgG (zo negatief bij begin zwangerschap)
2089 Toxoplasma IgM (zo IgG niet gekend positief)Consultatie 28 weken
71 Hemoglobineg72 RBC telling + hematocriet80 Trombocytentelling84 WBC telling
4234 Ferritine4234 Ferritine253 Challenge met 50g Glc (zwangere)
8240 Indirecte coombs (zo bloedgroep rhesusnegatief.)
2087 T pl I G ( ti f bij b i h p)2087 Toxoplasma IgG (zo negatief bij begin zwangerschap)
2089 Toxoplasma IgM (zo IgG niet gekend positief)
4215 Urinezuur
1780 Neisseria gonorrhoeae cult.+microscopie op vaginale wisserConsultatie 36 weken
1784 Screening voor S. agalactiae op vaginorectale wisser

Consultatie 20-24 weken
2082 Cytomegalovirus IgG (zo IgG niet gekend positief)
2084 Cytomegalovirus IgM (zo IgG niet gekend positief preconceptie)
2087 Toxoplasma IgG (zo negatief bij begin zwangerschap)
2089 Toxoplasma IgM (zo IgG niet gekend positief)
9316 Foetale cellenConsultatie 28 weken
71 Hemoglobineg72 RBC telling + hematocriet80 Trombocytentelling84 WBC telling
4234 Ferritine4234 Ferritine253 Challenge met 50g Glc (zwangere)
8240 Indirecte coombs (zo bloedgroep rhesusnegatief.)
2087 T pl I G ( ti f bij b i h p)2087 Toxoplasma IgG (zo negatief bij begin zwangerschap)
2089 Toxoplasma IgM (zo IgG niet gekend positief)
4215 Urinezuur
1780 Neisseria gonorrhoeae cult.+microscopie op vaginale wisser
9316 Foetale cellenConsultatie 36 weken
1784 Screening voor S. agalactiae op vaginorectale wisser
9316 Foetale cellen

TO DO / ACTIONSTO DO / ACTIONS
l f f l b h1. No implementation of FCM. KBB training of laboratory technicians.
2 Report limit FMT < 5 ml fetal blood2. Report limit FMT < 5 ml fetal blood.
3. Alarm value of FMT > 15 ml fetal blood => phone & FU.
4. Fetal cell count introduction in Diagnostic Prenatal Care Path.
Do the gynaecologists consider using the
clinical‐diagnostic‐therapeutic algorithm?clinical diagnostic therapeutic algorithm?
5. Acquisition of the commercial FETALtrol control would be an improvement.

Positive control (blood of a 1‐month‐old baby)
Example of adequate control Often inadequate control⇒ make new slides (30?)⇒ stain again⇒ time consuming

TO DO / ACTIONSTO DO / ACTIONS
l f f l b h1. No implementation of FCM. KBB training of laboratory technicians.
2 Report limit FMT < 5 ml fetal blood2. Report limit FMT < 5 ml fetal blood.
3. Alarm value of FMT > 15 ml fetal blood => phone & FU.
4. Fetal cell count introduction in Diagnostic Prenatal Care Path.
Do the gynaecologists consider using the
clinical‐diagnostic‐therapeutic algorithm?clinical diagnostic therapeutic algorithm?
5. Acquisition of the commercial FETALtrol control would be an improvement.