weight management practices among heart and vascular...
TRANSCRIPT

July-August 2012 • Vol. 21/No. 4222
Melly Turner, BSN, RN-BC, is Clinician 4, Cardiology Practice Nurse, Heart and Vascular Center,University of Virginia Health System, Charlottesville, VA.
Suzanne M. Burns, MSN, RN, RRT, ACNP, CCRN, FAAN, FCCM, FAANP, is Professor ofNursing, Acute and Specialty Care APN2, Critical Care, University of Virginia Health System,Charlottesville, VA.
Laura Knight, BSN, RN-BC, is Clinician 3, Cardiology Practice Nurse, Heart and Vascular Center,University of Virginia Health System, Charlottesville, VA.
Kathryn Ward, MSN, APRN, BC, CDE, is Medical Center Manager, Heart and Vascular Center,University of Virginia Health System, Charlottesville, VA.
Adrienne Garo, MSN, RN, is Clinician 3, Cardiology Practice Nurse, Heart and Vascular Center,University of Virginia Health System, Charlottesville, VA.
Theresa Morris, LPN, is Patient Care Technician, Heart and Vascular Center, University of VirginiaHealth System, Charlottesville, VA.
Elizabeth Hooper, MSN, RN, is Clinician 3, Thoracic and Cardiovascular Surgery Clinic, Heart andVascular Center, University of Virginia Medical Center, Charlottesville, VA.
Mark Conaway, PhD, is Professor and Director, Division of Biostatistics and Epidemiology,University of Virginia Health System, Charlottesville, VA.
Acknowledgment: The authors wish to thank Dr. Gayle Timmerman for permission to use theWeight Management Practices among Primary Care Providers survey.
Weight Management Practices amongHeart and Vascular Health Care
Providers in an Ambulatory Setting
In response to the alarmingincrease in obesity and thenumber of overweight individ-uals, professional organiza-
tions published guidelines for themanagement of obesity. Theseinclude the National Institutes ofHealth (NIH) National Heart, Lung,and Blood Institute (NHLBI) (1998;release of updated guidelines expect-ed in late 2012), the World HealthOrganization (2000), and the U.S.Preventive Services Task Force(McTigue et al., 2003). Overweight orobese physical states are a significanthealth problem, affecting an estimat-ed 206,000,000 people, according tothe American Heart Association 2007Heart Disease and Stroke Statistics(Rosamond et al., 2007). These indi-viduals are at increased risk for manyco-morbid health conditions, includ-ing hypertension, osteoarthritis, dys-lipidemia, type 2 diabetes, coronaryheart disease, stroke, gallbladder disease, sleep apnea and respiratoryproblems, and some cancers (endo -metrial, breast, and colon) (NHLBI,1998). According to the NationalHealth and Nutrition ExaminationSurvey (NHANES III) (National Cen -ter for Health Statistics, 1994), mor-bidity for a number of health condi-tions increases with an increase inbody mass index (BMI) in both menand women. In persons with cardio-vascular disease, BMI of 20 or greaterincreases mortality rates by 50%-100% (NHLBI,1998).
Literature Review
Demographics of ObesityMadala and colleagues (2008)
found the overall incidence of over-
weight has increased 2-fold and ofobesity more than 3-fold over thepast 50 years. The prevalence ofextreme and super-obesity (bodymass index > 40 or 50 kg/m2, respec-tively) has increased by 50% and75%. A report by the Robert WoodJohnson Foundation and The Trustfor American Health (Levi, Vinter, St.Laurent, & Segal, 2008) indicated theincidence of adult obesity had risenin 37 states. Obesity rates nowexceed 25% in more than half the
states. These data are sobering givenevidence that health care attitudesmay contribute to negative out-comes in patients who are obese(Ruelaz et al., 2007).
Health Care Attitudes andTheir Effect on Outcomes
Literature suggests patients andhealth care providers (HCPs) vary intheir attitudes and beliefs about fac-tors affecting the etiology of obesity,and about the role of the medical
Research for PracticeResearch for Practice
Melly Turner, Suzanne M. Burns, Laura Knight, Kathryn Ward, Adrienne Garo, Theresa Morris, Elizabeth Hooper, and Mark Conaway
In this study, health care providers’ assessment, intervention practices,and perceived barriers to weight management approaches in anambulatory adult heart and vascular setting are reported. Their knowl-edge of the National Institutes of Health National Heart, Lung andBlood Institute’s The Practical Guide: Identification, Evaluation, andTreatment of Overweight and Obesity in Adults are also described.

July-August 2012 • Vol. 21/No. 4 223
system and its ability to intervene(Ruelaz et al., 2007). These beliefsaffect providers’ frequency andmethods of assessment. In addition,the weight loss interventions are notimplemented as often in the patientswho are obese (Lyznicki, Young,Riggs, & Davis, 2001; Timmerman,Reifsnider, & Allan, 2000).
Galuska, Will, Serdula, and Ford(1999) used data from the 1996Behavioral Risk Factor SurveillanceSystem, a random-digit telephonesurvey conducted by the Centers forDisease Control, as well as statehealth departments in all 50 statesand the District of Columbia, todetermine the health informationgiven to patients by providers. The1996 Behavioral Risk Factor Ques -tionnaire included queries about cur-rent behaviors that affect health(e.g., tobacco use, weight control,women’s health) and questions ondemographic characteristics. Section7 (titled “Weight Control”) listed thefollowing questions: Are you tryingto lose weight? Are you trying tomaintain your current weight, thatis, to keep from gaining weight? Areyou eating either fewer calories orless fat to lose weight or keep fromgaining weight? Are you using phys-ical activity or exercise to lose weightor keep from gaining weight? In thepast 12 months, has a doctor, nurse,or other health professional givenyou advice about your weight? Theanalytic sample included 12,835adults, age 18 and older, classified asobese (BMI ≥ 30 kg/m2), who had vis-ited their physician for a routinecheckup during the previous 12months. Less than half (42%,n=5,391) of survey respondentsreported they had been told by adoctor, nurse, or other HCP to loseweight. A strong association wasfound between measures of healthand reporting of received advice.Results suggested HCPs may be selec-tive in whom they advise because (a)they identify a patient’s weight-relat-ed condition such as diabetes; (b)they target persons whom they per-ceive may be most likely to comply,such as women, the highly educated,and patients who are most over-weight; and (c) they are more likelyto advise weight loss when they have
more frequent patient contact, aswith those persons who are over-weight and/or have diabetes.
Cleator and colleagues (2002)conducted a retrospective analysis of615 hospital records from three spe-cialty outpatient clinics to determinereported prevalence of obesity andthe action taken. The number ofclinic records by specialty were asfollows: cardiology=257, rheumatol-ogy=108, orthopedics=250. Becausethe retrospective analysis did notinclude the patients’ heights, theinvestigators undertook a prospec-tive study of 570 patients from thesame three specialty outpatient clin-ics to determine the true prevalenceof BMI by direct measurement ofheight and weight. In this analysisthe breakdown by specialty clinicpatients was as follows: cardiolo-gy=283, rheumatology=188, ortho-pedics=179. The author identified“missed opportunities for diagnosisand treatment of obesity in outpa-tient departments” (p. 582). In addi-tion, Cleator and co-authors suggest-ed inaccurate identification and doc-umentation of prevalence of thediagnosis lead to hindrances in theHCP’s ability to integrate obesitytreatment and disease managementinto the plan of care. Evidence clear-ly indicated efforts to change healthcare attitudes about obesity areimportant, especially becauseresearch findings suggest a proactiveapproach to the care of obesepatients improves outcomes (NHLBI,1998).
Effect of TreatmentPrograms on Obesity
A physician office-based studyconducted by Ashley and colleagues(2001) examined effects of incorpo-rating meal replacements into tradi-tional lifestyle interventions as anadditional weight-reduction strategyfor overweight patients. Participantsin the 1-year study (26 sessions)included 113 overweight, pre-menopausal women ages 25-50 withBMIs of 25-30. The women wereassigned randomly to three differentlifestyle-based groups: (a) dietitian-led 1-hour group intervention, (b)dietitian-led 1-hour group interven-tion incorporating meal replace-
ments (shakes or bars), or (c) primarycare office visit incorporating mealreplacements with individual physi-cian and nurse visits (10-15 minutesper visit). Of the 113 initial subjects,74 (65%) completed the 1-yearstudy. Findings showed the brief pri-mary care visit incorporating mealreplacements achieved the sameresult as the dietitian-directed tradi-tional group without meal replace-ments (mean weight loss 4.3% vs.4.1% respectively). Of the two dieti-tian-led groups, the women usingmeal replacements vs. those who didnot maintained a greater weight loss(9.1% vs. 4.1% respectively, p=0.03).Analysis across groups showed aweight loss of 5%-10% was associat-ed with significant reduction in thepercentage of body fat, body massindex, waist circumference, restingenergy expenditure, insulin level,total cholesterol level, and low-den-sity lipoprotein cholesterol level(p=0.01). Incorporation of a mealreplacement into a traditionallifestyle intervention thus was anindependent contributor to out-comes. The study’s main finding sug-gested the primary care physiciancan lead a successful lifestyle inter-vention for weight control, withinthe time constraints in a generaloffice practice, with the appropriatetools (meal replacements and life -style instruction materials).
Dick (2004) reviewed a meta-analysis of 493 randomized con-trolled trials (RCTs) and an addition-al five RCTs on the topic of the ther-apeutic effectiveness of diet, exercise,and diet plus exercise programs inthe management and treatment ofobesity in adults. Studies were cri-tiqued for quality and conclusionsfor clinical management. Whilesome discrepancies existed in howinstruments for measurements weremade in study patients, the authorconcluded the studies were wellpowered for size, had good studydesigns and controls, and were con-sistent in the use of appropriateinstruments for analysis. She alsoobserved overall findings revealedintervention, including diet plusexercise, is more effective for sus-tained weight loss over time thandiet or exercise alone.
Weight Management Practices among Heart and Vascular Health Care Providers in an Ambulatory Setting

July-August 2012 • Vol. 21/No. 4224
Ruelaz and collegues (2007) notedprevalent attitudes related to poten-tial barriers to weight control includepatients’ lack of self-control to stayon a diet, availability of fatteningfood, and time for physical activity.Timmerman and co-authors (2000)suggested such attitudes may resultin high relapse rates of patients withweight problems, lack of patientinterest in changing behaviors, lackof provider time, and lack of appro-priate educational materials for thetreatment of obesity. Thus, applica-tion of the obesity managementguidelines (NHLBI, 1998) shouldbegin with the routine assessment ofpatients for obesity as the first step inaddressing these attitudes and barri-ers to weight control.
Assessment of ObesityAnthropometric measurements
and/or self-reporting may be usedto collect height and weight in theambulatory setting, but they are not standardized or obtained consistently. Niedhammer, Bugel,Bonenfant, Goldberg, and Leclerc(2000) concluded self-reportedheight tends to be overestimatedand weight tends to be underesti-mated, while Hendershot and col-leagues (2006) found HCPs’ esti-mates of heights, weights, and BMIwere highly inaccurate. Akhtar-Danesh, Dehghan, Merchant, andRainey (2008) concluded the use ofmeasured height and weight ispreferable to the use of self-reportedvalues in estimating the prevalenceof obesity. In their study, femalesand heavier respondents under-reported BMI more frequently thanothers.
Abdominal adiposity obtained asa waist circumference provides ameasurement for assessing a pa -tient’s abdominal fat content,which is an independent predictorof risk factors and morbidity(NHLBI, 1998). Abdominal fat alsoappears to be an independent riskfactor when BMI is not increasedmarkedly. Madala and co-authors(2008) concluded excess adiposity isstrongly related to first non-ST ele-vation myocardial infarction asabdominal fat is related directly to
increased inflammatory markers aswell as pathogenesis of atheroscle-rotic plaque accumulation and rup-ture.
Some limited evidence suggestsattitudes of health care providersmay have negative impact on accessto care and provision of appropriatecare for obese persons (Ruelaz et al.,2007). The prevalence of obesity, aswell as its effect on individuals andsociety, requires health care profes-sionals to work to prevent and man-age obesity more aggressively. Animportant initial step is to reviewcurrent practices to determine if obe-sity assessment and management areincorporated into routine care.
Study RationaleIn the researchers’ ambulatory
cardiology setting, 47% (n=8,440) of
cardiology patients seen during fiscalyear 2008 were overweight (20%,n=3,606), obese (22%, n=3,911), ormorbidly obese (5%, n=923). How -ever, the recommended screening(height, weight, BMI, waist circum-ference, and risk factor assessment)of these physical states varied with-out standardized interventions.With each clinic encounter, apatient’s height and weight may bemeasured or identified by patientstatement; weight could be meas-ured on either digital or manualscales. Waist circumferences weremeasured sporadically. Researchersbelieved a study to determine thedegree to which practitioners fol-lowed recommended guidelines forthe assessment and management ofobesity would be an important con-tribution to the institution and oth-ers as well. In addition, they believed
Source: Adapted from NHLBI, 1998.
TABLE 1.Expert Panel’s Treatment Algorithm for Overweight and Obese Adults
Step Algorithm Process
1 Patient encounter
2Determine if the patient has a history of being overweight or recorded BMI≥ 25.
3 Determine if BMI has been measured in the past 2 years.
4 Measure weight, height, and waist circumference, then calculate BMI.
5Determine if BMI ≥ 25 or waist circumference >35 inches (88 cm) (F) > 40inches (102 cm) (M). If yes, proceed to step 6; if no, proceed to step 14.
6 Assess risk factors.
7Determine if BMI ≥ 30 or BMI 25-29.9 or waist circumference > 35 inches(F) > 40 inches (M) and ≥ 2 risk factors. If yes, proceed to step 8; if no, pro-ceed to step 12.
8 Devise goals/ treatment strategy for weight loss and risk factor control.
9Determine progress being made and if weight loss goal was achieved. Ifyes, proceed to step 11; if no, proceed to step 10.
10 Assess reasons for inability to lose weight.
11Provide maintenance counseling: dietary therapy, behavior therapy, physicalactivity.
12 Determine if the patient wants to lose weight.
13 Advise to maintain current weight and address other risk factors.
14 Determine if BMI ≥ 25.
15 Provide brief reinforcement and educate on weight management.
16 Provide periodic weight, BMI, and waist circumference checks.
Research for Practice

July-August 2012 • Vol. 21/No. 4 225
such a study may serve as an impetusfor evidence-based practice changes.
Study ObjectivesThe specific objectives of the
study were to determine (a) ambula-tory cardiology (AC) practices relatedto weight management, (b) differ-ences in practice patterns regardingweight management by practice set-ting, (c) perceived barriers to imple-menting weight management inter-ventions in the AC practice and, (d) providers’ familiarity with the
NHLBI Practical Guide: Identification,Evaluation, and Treatment of Over -weight and Obesity in Adults (NHLBI,2000).
Study Site and Sample
This study was conducted in theambulatory cardiovascular clinic at a750-bed academic medical center inthe mid-Atlantic region of theUnited States. The study receivedapproval from the institutionalreview board of the hospital. Thesurvey population included health
care providers (surgeons, cardiolo-gists, cardiology fellows, registerednurses, nurse practitioners, physi-cian assistants, registered dieticians)who managed specific aspects ofpatient care, and worked in theambulatory adult heart and vascularsetting.
Materials and MethodsThe study investigators selected
The Practical Guide: Identification,Evaluation, and Treat ment of Over -
TABLE 2.Assessment of Patients with Weight Management Problems
During the past 30 days, as a part of routine health maintenance visits or ongoing follow-up visits with patients who have weightmanagement problems, how often did you assess the following? Circle one number:
Never (0%) = 0 Sometimes (< 50%) = 1 Often (≥50%) = 2 Usually (≥80%) = 3
Routine or Follow-Up Visits
Never Sometimes Often Usually
I. HISTORY
Weight history (History of weight gain losses/regains or previousattempts at weight loss)*
0 1 2 3
Past weight management history 0 1 2 3
Nutrition assessment (e.g., 24-hour recall, food frequency) 0 1 2 3
Physical activity or exercise patterns 0 1 2 3
Binge eating behavior 0 1 2 3
Risk Factors:
Neuroendocrine disorders (thyroid disorders, polycystic ovariansyndrome, diabetes)*
0 1 2 3
Family history of obesity 0 1 2 3
Age of obesity onset 0 1 2 3
Depression 0 1 2 3
High stress levels or life crises 0 1 2 3
Smoking 0 1 2 3
II. PHYSICAL ASSESSMENT
Weight 0 1 2 3
Height* 0 1 2 3
Waist circumference* 0 1 2 3
Body mass index (kg/m2) 0 1 2 3
Lab Work:
Lipid profile 0 1 2 3
TSH 0 1 2 3
FBS 0 1 2 3
Hemoglobin A1C* 0 1 2 3
Note: *Denotes items modified from Timmerman et al., 2000.
Weight Management Practices among Heart and Vascular Health Care Providers in an Ambulatory Setting
July-August 2012 • Vol. 21/No. 4226
weight and Obesity in Adults (NHLBI,2000) as the blueprint for assessmentand management strategies in thestudy as it was the oldest of the exist-ing guidelines and thus presumablythe most familiar to health care pro-fessionals. In addition, it containedrecommendations consistent withthose of the World Health Organi -zation (2000) and the U.S. Pre -ventive Services Task Force (McTigueet al., 2003). Finally, it was the mostusable of the existing guidelines, withresources such as “Expert Panel’sTreatment Algorithm,” which detailsassessment and management direc-tions for the patients in a step-by-stepapproach (see Table 1). Informationon the health care participants wascollected by a self-report surveyadapted from the Weight ManagementPractices among Primary Care Pro -viders Survey with permission ofTimmerman and co-authors (2000)(see Tables 2, 3, and 4).
The survey was divided into fourpages, beginning with baseline infor-mation, including questions aboutthe providers’ familiarity with the
NHLBI practical guide (2000). Asnoted in Tables 2, 3, and 4, theproviders then were questioned abouttheir assessment of weight manage-ment problems, weight managementinterventions, and barriers to imple-menting weight management inter-ventions. Participants were instructedto answer questions based on the past30 days, either as part of routinehealth maintenance visits or ongoingfollow-up visits for patients with con-firmed weight management difficulty(see Table 2). Participants were askedhow often they answered the practicequestions by using a Likert-type scale,with responses ranging from 0 (never)to 3 (usually).
Questions answered by the healthcare providers regarding health sta-tus included weight history, pastweight history, nutritional assess-ment, physical activity, and bingeeating behavior. Questions to assessrisk factors included presence of neu-roendocrine disorders, family historyof obesity, age of obesity onset, pres-ence of depression or high stress lev-els, and history of smoking. Physical
assessment included weight, height,waist circumference, and body massindex. Laboratory assessment in -cluded lipid profile, thyroid stimu-lating hormone, fasting blood glu-cose, and hemoglobin A1C (seeTable 2).
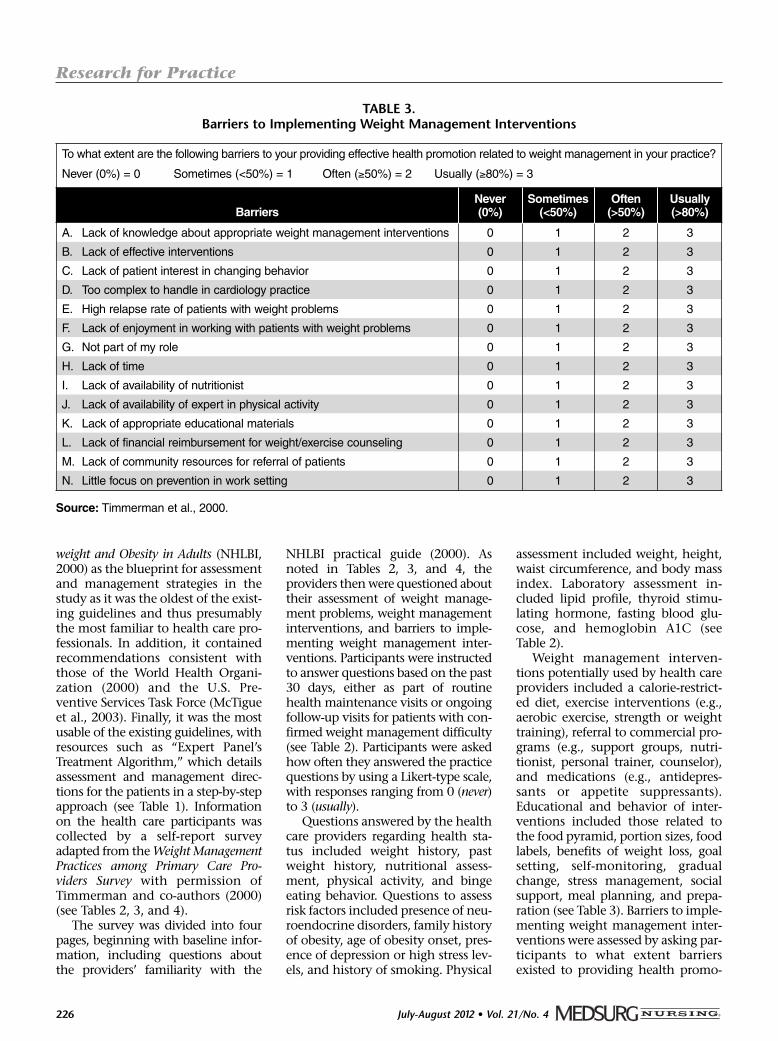
Weight management interven-tions potentially used by health careproviders included a calorie-restrict-ed diet, exercise interventions (e.g.,aerobic exercise, strength or weighttraining), referral to commercial pro-grams (e.g., support groups, nutri-tionist, personal trainer, counselor),and medications (e.g., antidepres-sants or appetite suppressants).Educational and behavior of inter-ventions included those related tothe food pyramid, portion sizes, foodlabels, benefits of weight loss, goalsetting, self-monitoring, gradualchange, stress management, socialsupport, meal planning, and prepa-ration (see Table 3). Barriers to imple-menting weight management inter-ventions were assessed by asking par-ticipants to what extent barriersexisted to providing health promo-
TABLE 3.Barriers to Implementing Weight Management Interventions
To what extent are the following barriers to your providing effective health promotion related to weight management in your practice?
Never (0%) = 0 Sometimes (<50%) = 1 Often (≥50%) = 2 Usually (≥80%) = 3
BarriersNever (0%)
Sometimes(<50%)
Often (>50%)
Usually(>80%)
A. Lack of knowledge about appropriate weight management interventions 0 1 2 3
B. Lack of effective interventions 0 1 2 3
C. Lack of patient interest in changing behavior 0 1 2 3
D. Too complex to handle in cardiology practice 0 1 2 3
E. High relapse rate of patients with weight problems 0 1 2 3
F. Lack of enjoyment in working with patients with weight problems 0 1 2 3
G. Not part of my role 0 1 2 3
H. Lack of time 0 1 2 3
I. Lack of availability of nutritionist 0 1 2 3
J. Lack of availability of expert in physical activity 0 1 2 3
K. Lack of appropriate educational materials 0 1 2 3
L. Lack of financial reimbursement for weight/exercise counseling 0 1 2 3
M. Lack of community resources for referral of patients 0 1 2 3
N. Little focus on prevention in work setting 0 1 2 3
Source: Timmerman et al., 2000.
Research for Practice

July-August 2012 • Vol. 21/No. 4 227
TABLE 4.Weight Management Interventions
During the past 30 days, as a part of weight management interventions you use in your practice during new patient visits, routinehealth maintenance visits, or on-going follow-up visits, how often do you advise the following? (Circle one number for each inter-vention.):
Never (0%) = 0 Sometimes (< 50%) = 1 Often (≥50%) = 2 Usually (≥80%) = 3
Routine or Follow-Up Visits
Never Sometimes Often Usually
1. Dietary Interventions
Calorie-restricted diet 0 1 2 3
Low-fat diet 0 1 2 3
Increased fiber diet 0 1 2 3
Other (Mediterranean, South Beach, etc.) * 0 1 2 3
2. Exercise Interventions
Increase activity (30 minutes of daily moderate activity) 0 1 2 3
Aerobic exercise 0 1 2 3
Strength or weight training 0 1 2 3
3. Referrals
Commercial programs (e.g., Weight Watchers, Jenny Craig) 0 1 2 3
Support groups (e.g., OA, TOPS, NAAFA) 0 1 2 3
Nutritionist / Dietitian / Diabetic cardiovascular clinic 0 1 2 3
Interdisciplinary team (IDT) *
Personal trainer or exercise physiologist 0 1 2 3
Counseling (psychologist, psychiatrist, counselor) 0 1 2 3
Medically supervised weight loss program 0 1 2 3
4. Medications
Antidepressant medications 0 1 2 3
Appetite suppressants * 0 1 2 3
Other (List) 0 1 2 3
5. Educational Interventions
Food pyramid 0 1 2 3
Portion sizes 0 1 2 3
Food labels 0 1 2 3
Benefits of weight loss, exercise, or nutritious eating 0 1 2 3
6. Behavioral Interventions
Goal setting 0 1 2 3
Self-monitoring / food diaries 0 1 2 3
Gradual change 0 1 2 3
Stress management 0 1 2 3
Social support (get significant other involved) 0 1 2 3
Discourage perfectionist attitudes 0 1 2 3
Behavior modification (e.g. eating at table only, cue restriction) 0 1 2 3
Meal planning and preparation 0 1 2 3
Note: *Denotes items added to instrument by Timmerman et al., 2000.
Weight Management Practices among Heart and Vascular Health Care Providers in an Ambulatory Setting

July-August 2012 • Vol. 21/No. 4228
tion related to weight management.The barrier questions included lackof knowledge, lack of effective inter-ventions, lack of patient interest inchanging behavior, too complex tohandle in cardiology clinic, highrelapse rate, lack of enjoyment work-ing with, not part of my role, lack oftime, lack of availability of a nutri-tionist or expert in physical activity,lack of educational materials, finan-cial reimbursement, communityresources, and little focus on preven-tion in the work setting (see Table 4).
The Primacy Care Survey (Tim -merman et al., 2000) was modifiedslightly by adding assessment ques-tions concerning risk factors thatidentified neuroendocrine disorders(e.g., thyroid disorders, polycysticovarian syndrome, diabetes), heightand waist circumference, and hemo-globin A1C. Finally, percentage ofideal body weight, percentage ofbody fat, and waist/hip ratio weredeleted (Table 2 denotes modifieditems with an asterisk). Other ques-tions were added in three categories.In the weight management interven-tion category, questions were addedto the dietary intervention section as“other” (e.g., Mediterranean, SouthBeach). In the referral category, dia-betic cardiovascular clinic interdisci-plinary team were added. In addi-tion, appetite suppressants wereincluded in the medication section(Table 4 denotes added items with anasterisk). These alterations reflectedchoices available in the authors’ prac-tice environment.
Procedure
The survey was distributed at themonthly faculty and staff meeting aswell as during clinic hours (for thosewho were not reached in the meet-ings). The survey took 15-20 minutesto complete. To enhance surveyresponse rate, researchers sent areminder email approximately 1week after the initial survey distribu-tion. To maintain anonymity, thesurvey form contained no identi-fiers; respondents gave completedsurveys to a research team member,who placed them in a folder, alsowithout identifiers. All data were
TABLE 5.Weight Management Assessment Addressed 50%
of the Time by Clinic Staff
Assessment CategoryGeneral
Cardiology Subspecialty TCV
Weight history X X
Past weight history X
Nutrition X
Exercise X X X
Neuroendocrine X X X
Family history of obesity X X X
Depression X X
High stress level X X
Smoking X X X
Height X X X
Waist circumference X
BMI X X
Serum lipids X X
Thyroid stimulating hormone (TSH), fastingblood glucose X X
Hemoglobin A1c X X X
TCV = thoracic cardiovascular surgery
TABLE 6.Weight Management Interventions Scored as Occurring 50%
of the Time by Clinic Staff
InterventionGeneral
Cardiology Subspecialty TCV
Calorie restriction X X
Low-fat diet X X X
Increased fiber diet X X
Mediterranean or South Beach diet X X
Increase activity 30 minutes/day X X X
Aerobic activity X X X
Strength or weight training X
Referral to nutritionist X
Personal trainer or exercise physiologist X
Portion size X
Food labels X
Benefits of weight loss X X X
Goal setting X X
Food diary X
Gradual change X X
Stress management X X
Social support X X
Behavior modification X
Meal planning and preparation X
TCV = thoracic cardiovascular surgery
Research for Practice

July-August 2012 • Vol. 21/No. 4 229
reviewed for completeness thenentered into a spreadsheet. Each dataentry was validated for accuracy by asecond research team member.
Data AnalysisResults were tabulated by type of
respondent (attending, fellow, ornon-MD HCP) and/or service (tho-racic cardiovascular surgery [TCV],cardiology, and sub-specialty). Chi-squared tests were used to test differ-ences by respondent or group.
Results
Demographics Of the 61 respondents (78%
return rate), 36 were MDs (9 sur-geons, 27 cardiologists) with an aver-age age of 45 and average 16 years ofexperience. The 25 non-MD partici-pants included 11 RNs, 7 nurse prac-titioners, 4 physician assistants, and2 registered dieticians. Mean age ofthe non-MD group was 45; thegroup averaged 19 years of experi-ence. The majority of respondents inall categories were not familiar withNHLBI Obesity Guidelines. Whenasked if they could list steps in thetreatment algorithm, only sevencould name 4 of the 16 steps. Thosewho were familiar with the guide-lines by category were as follows:attending (30%), fellows (6%), non-MD HCPs (32%).
Assessment of WeightManagement Problems byProvider
No significant differences amongproviders were noted in the percent-age of time devoted to different cate-gories of assessment. However, cate-gories that were scored as usually oroften at least 50% of the time includ-ed all but nutritional assessment, ageof onset of obesity, and family histo-ry of obesity. Differences in providersby service area existed, with surgicalservices adopting the fewest recom-mended assessment steps. Membersof surgical services reported they didnot screen for weight history, pastweight management history, nutri-tional assessment, depression, high
stress levels, waist circumference,serum lipids, thyroid stimulatinghormone, and fasting blood sugars(see Table 5).
Weight ManagementAssessment Categories byClinic Type
Assessment categories by clinicreported to be addressed more than50% of the time are found in Table 5.Significant differences existed be -tween TCV and the other two clinicsin the following categories of man-agement assessments: weight history(p=0.001), past weight history(p=0.005), nutritional assessment(p=0.003), physical activity exercise(p=0.015), high stress levels or lifecrisis (p≤0.001), waist circumference(p=0.006), BMI (p≤0.001), lipids(p≤0.001), and TSH (p≤0.001). Per -ceived frequency of these assess-ments by TCV was lower than theother specialties.
Weight ManagementInterventions by Clinic
Weight management interven-tions by clinic reported to beaddressed more than 50% of thetime are found in Table 6. Significantdifferences between weight manage-ment interventions by clinic includ-ed the following: calorie-restricteddiet (p=0.001), increased fiber diet(p=0.003), “other diet” (p=0.003), aer-obic exercise (p=0.008), personal train-er or exercise physiologist (p≤0.001),refer to counseling (p=0.015), portionsizes (p=0.012), food labels (p≤0.001),goal setting (p≤0.001), gradualchange (p≤0.001), stress manage-ment (p≤0.001), and meal planning
and preparation (p=0.004). As notedpreviously, TCV providers tended toaddress interventions less often thanproviders in subspecialty clinics andgeneral cardiology.
Barriers to ImplementingWeight ManagementInterventions
Barriers were described in the sur-vey as the extent to which theyaffect weight management healthpromotion. Barriers scored as beingpresent 50% of the time by clinic arefound in Table 7. Significant differ-ences existed between TCV respons-es and the other two specialties forthe following perceived barriers: notpart of my role (p=0.010), lack ofavailability of nutritionist (0.042),and little focus on prevention inwork setting (p=0.014). TCV pro -viders did not see implementingweight management interventionsas part of their role (p=0.010).
DiscussionThe majority of providers in
ambulatory heart and vascular clin-ics were not familiar with the NHLBIPractical Guide (2000). Anecdotally,a query of other ambulatory clinicsin the setting confirmed the trendsdemonstrated in this study. Thisfinding is somewhat surprising asthe NHLBI Guidelines are the oldestof the three published to date andthe most prescriptive. The authorssuspect findings may be similar aswell in other clinics beyond thehealth care system. While the use ofevidence-based guidelines may as -sure application of information that
TABLE 7.Barriers to Implementing Weight Management Interventions by
Specialty Scored as Present >50% of the Time
InterventionGeneral
Cardiology Subspecialty TCV
Lack of patient interest in changing behavior X X X
High relapse rate X X
Lack of time X
Lack of nutritionists X
TCV = thoracic cardiovascular surgery
Weight Management Practices among Heart and Vascular Health Care Providers in an Ambulatory Setting

July-August 2012 • Vol. 21/No. 4230
Weight Loss StrategiesDo I Need to Lose Weight?
The Body Mass Index (BMI) is a tool that estimates your total body fat using your height and weight. Your BMI is calculatedduring every visit.
How Do I Lose Weight?Maintaining a healthy weight requires a balance of energy. You must balance the calories you get from food and beverageswith the calories you use to keep your body going and be physically active.
• The same amount of energy IN and energy OUT over time = weight stays the same• More IN than OUT over time = weight gain• More OUT than IN over time = weight loss
To lose weight, you must either:• Decrease your intake by consuming fewer caloriesOr• Increase the amount of calories you burn through exercise
Healthy weight loss is 1-2 lbs per week. That means you need to burn roughly 500-1,000 more calories per day than youconsume.
Ways to Decrease Caloric IntakeSubstitution:One of the easiest ways to decrease the amount of calories you take in during the day is to slowly substitute healthy, low-calorie foods for the foods you are already eating. Consulting with a nutritionist can help you identify healthy and tasty sub-stitutions.
Portion Control:People often greatly overestimate the size of a portion of food and in the process, eat many more calories than they wereintending.
Some Strategies for Decreasing Portion Size Are:• When eating out, choose small portions, share an entrée with a friend, or take some of the food home. • Check a product’s Nutrition Facts label to learn how much food is considered a serving and how many calories, fat grams,
and other nutrients are in the item. • Limit portion sizes of such high-calorie foods as cookies, cakes, and other sweets; French fries; and oils. • Use smaller plates. We eat most of what is on our plate, no matter what the size. Smaller plates can mean smaller por-
tions.
How Should I Start?• Discuss exercise plans with your doctor. He or she will be able to address your unique health concerns. • If you’ve been inactive for a while, you may want to start with walking, biking, or swimming at a comfortable pace.
Beginning with less-strenuous activities will allow you to become gradually more fit without straining your body. • If you’re not sure how physically fit you are, you may want to visit a qualified exercise professional to receive a fitness
assessment. This can give you a good picture of the shape you’re in and allow you to choose activities and goals that areright for you.
• Cardiac rehabilitation is also a good option for those who have been diagnosed with heart conditions.
continued on next page
If your BMI is: Then you are considered: And you should:<18.5 Underweight Gain weight18.5-24.9 Normal Maintain current weight
25.0-29.9 Overweight Lose weight, especially if you haveother risk factors for heart disease
>30.0 Obese Lose weight
APPENDIX 1.
Research for Practice

July-August 2012 • Vol. 21/No. 4 231
results in improved outcomes, adher-ence must be assured. Findings suchas these are important because theysuggest awareness of the guidelines,which must be present before adher-ence is assured, is a missing first step.
Overall, practice patterns relatedto weight management among car-diovascular practices were similarexcept for TCV provider practices.Weight history related to obesityand risk factors, physical assess-ment, and related laboratory testswere done. Waist circumference,however, was measured only inter-mittently. Some small positive dif-ferences were noted by providers insub-specialty areas where additionalresources were available to accom-plish the measurements and inter-ventions (exercise physiologist, reg-istered dietician).
The main barrier in the surgicalclinics appeared to be the perceptionthat addressing these issues was notthe role of the provider treating a spe-cific surgical condition. A beliefappears to exist that medical issues
are the purview of the primary physi-cian. Clinicians also may believe theydo not have the knowledge, skills, ortime to address weight managementduring the office outpatient visit.Along with time, these may be barri-ers in cardiology and other clinics aswell. However, this study did not testall these perceptions; further work inthe area is needed. In addition, use ofreferrals to allied health profession-als, such as nutritionists, exercisephysiologists, and/or obesity clinicsto provide essential weight manage-ment teaching, should be encour-aged as a means to provide essentialinformation without increasing actu-al clinic time spent by the health careprovider.
The study was limited by its sam-ple size and the fact that the surveyis a self-reported instrument. Self-reports may represent over-reportingor under-reporting from the respon-dents, not practice reality. However,the content was carefully scripted tofollow the NHLBI guideline manage-ment elements.
Health Care ProviderImplications andImplementing the NHLBIGuidelines
Because study results could helpvalidate the importance of screeningfor overweight or obese patients andserve as a stimulus for a change inpractice, they were distributed local-ly via newsletters and staff meetings,and at the evidence-based nursingpractice annual conference. Simplestrategies to educate staff aboutweight management practices alsohelped to incorporate these practicesinto care in the ambulatory settings.These included teaching staff aboutthe NHLBI Practical Guide (2000)through a bulletin board in-service,retraining health care providers onthe correct steps of waist circumfer-ence measurement with returndemonstration, assuring properequipment to measure height andweights was present in all clinics(with emphasis on measuring vs.self-reporting at each visit), calculat-ing BMI using the electronic medical
APPENDIX 1. (continued)
How Much Should I Get?Any exercise is better than no exercise, but…• To reduce risk of heart disease, get at least 30 minutes of moderate activity on most, and preferably all, days of the week.• For weight loss, try to get 60-90 minutes of moderate-intensity activity daily, without taking in extra calories.
What Kind of Exercise Should I Do?It’s less about exercising, and more about just increasing physical activity. Walking is one of best forms of exercise, and walk-ing with friends or family can be a great opportunity to strengthen social ties. If time is an issue, you can break any activityinto shorter periods of at least 10 minutes each and still get many of the same health benefits.
When Should I Contact My Doctor?Consult your doctor immediately if you experience sudden dizziness, cold sweats, paleness, fainting, extreme breathless-ness, or pain or pressure in your upper body during or just after an activity.
Examples of Moderate Exercise Examples of Vigorous Exercise
• Bicycling (less than 10 mph)• Downhill skiing• Dancing• Gardening• Golf (on foot)• Hiking (flat ground)
• Aerobic dancing• Basketball• Bicycling (more than 10 mph)• Cross-county skiing• Hiking (uphill)• Logging/running (at least 5 mph)
Source: Used with permission of the University of Virginia Patient Education Repository.
Weight Management Practices among Heart and Vascular Health Care Providers in an Ambulatory Setting

July-August 2012 • Vol. 21/No. 4232
record, and developing a two-pagepatient education tool (see Appendix1). While these interventions haveresulted in positive changes in studyclinics, challenges remain to thescreening and management of over-weight or obese patients.
ConclusionThe burden of obesity-related car-
diovascular disease is likely to increasethrough direct adverse health effectsof obesity and indirectly through itseffects on cardiovascular risk factors.Findings of this study suggest oppor-tunities for weight management diag-nosis and treatment are missed frequently. Although measurementalone does not alter practice, it doesoffer an opportunity to raise aware-ness of weight management amongpatients with cardiovascular diag-noses.
REFERENCESAkhtar-Danesh, N., Dehghan, M., Merchant,
A.T., & Rainey, J.A. (2008). Validity ofself-reported height and weight formeasuring prevalence of obesity. OpenMedicine, 2(3), e83-e88.
Ashley, J.M., St Jeor, S.T., Schrage, J.P.,Perumean-Chaney, S.E., Gilbertson,
M.C., McCall, N.L., & Bovee, V. (2001).Weight control in the physician’s office.Archives of Internal Medicine, 161(13),1599-1604.
Cleator, J., Richman, E., Leong, K.S.,Mawdsley, L., White, S., & Wilding, J.(2002). Obesity: Under-diagnosed andunder-treated in hospital outpatientdepartments. International Associationfor the Study of Obesity, 26(4), 581-584.
Dick, J.J. (2004). Weight loss interventions foradult obesity: Evidence for practice.Worldviews on Evidence-Based Nursing,1(4), 209-214.
Galuska, D.A., Will, J.C., Serdula, M.K., &Ford, E.S. (1999). Are health care profes-sionals advising obese patients to loseweight? Journal of the American MedicalAssociation, 282(16), 1576-1578.
Hendershot, K.M., Robinson, L., Roland, J.,Vaziri, K., Rizzo, A.G., & Fakhry, S.M.(2006). Estimated height, weight, andbody mass index: Implications forresearch and patient safety. Journal ofthe American College of Surgeons,203(6), 887-893.
Levi, J., Vinter, S., St. Laurent, R., & Segal,L.M. (2008). F as in fat: How obesity poli-cies are failing in America. Retrievedfrom http://healthyamericans.org/reports/obesity2008/Obesity2008Report.pdf
Lyznicki, J.M., Young, D.C., Riggs, J.A., &Davis, R.M. (2001). Obesity: Assessmentand management in primary care.American Family Physician, 63(11),2185-2196.
Madala, M.C., Franklin, B.A., Chen, A.Y.,Berman, A.D., Roe, M.T., Peterson, E.D.,… McCullough, P.A. (2008). Obesity and
age of first non-ST-segmet elevationmyocardial infarction. Journal of theAmerican College of Cardiology, 52(12),979-985. doi:10.1016/.jacc.2008.04.067
McTigue, K.M., Harris, R., Hemphill, B., Lux,L., Sutton, S., Bunton, A.J., & Lohr, K.N.(2003). Screening and interventions forobesity in adults: Summary of the evi-dence for the U.S. preventive servicestask force. Annals of Internal Medicine,139(11), 933-949.
National Center for Health Statistics. (1994).Vital health statistics: Plan and operationof the third national health and nutritionexamination survey, 1988-1994.Retrieved from http://www.cdc.gov/nchs/data/series/sr_01/sr01_032.pdf
National Institutes of Health (NIH) NationalHeart, Lung, and Blood Institute(NHLBI). (1998). Clinical guidelines onthe identification, evaluation, and treat-ment of overweight and obesity in adults:The evidence report. Retrieved fromwww.nhlbi.nih.gov/guidelines/obesity/ob_gdlns.pdf
National Institutes of Health (NIH) NationalHeart, Lung, and Blood Institute(NHLBI). (2000). The practical guide:Identification, evaluation, and treatmentof overweight and obesity in adults.Retrieved from www.nhlbi.nih.gov/guidelines/obesity/prctgd_c.pdf
Niedhammer, I., Bugel, I., Bonenfant, S.,Goldberg, M., & Leclerc, A. (2000).Validity of self-reported weight andheight in the French GAZEL cohort.International Journal of Obesity RelatedMetabolic Disorders, 24(9), 1111-1118.
Rosamond, W., Flegal, K., Friday, G., Furie, K.,Go, A., Greenlund, K., … American HeartAssociation Statistics Committee andStroke Statistics Subcommittee. (2007).Heart disease and stroke statistics –2007 update: A report from the AmericanHeart Association Statistics Committeeand Stroke Statistics Subcommittee.Circulation, 115(5), e69-171. d oi:10.1161/CIRCULATION.106.179918
Ruelaz, A.R., Diefenback, P., Simon, B., Lanto,A., Arterburn, D., & Shekelle, P.G. (2007).Perceived barriers to weight manage-ment in primary care-perspectives ofpatients and providers. Journal ofGeneral Internal Medicine, 22(4), 518-522. doi:10.1007/s11606-007-0125-4
Timmerman, G.M., Reifsnider, E., & Allan, J.D.(2000). Weight management practicesamong primary care providers. Journalof the American Academy of NursePractitioners, 12(4), 113-116.
World Health Organization. (2000). Obesity:Preventing and managing the global epi-demic: Report of a WHO consultation.Geneva, Switzerland: Author.
ADDITIONAL READINGSimkin-Silverman, L.R., Conroy, M.B., & King,
W.C. (2008). Treatment of overweightand obesity in primary care practice:Current evidence and future directions.American Journal of Lifestyle Medicine,2(4), 296-304.
Research for Practice