update of understanding of fibromyalgia dr. jad okais hotel dieu de france november 2009
TRANSCRIPT

Update of Understanding of Fibromyalgia
Dr. Jad OKAISHotel Dieu de France
November 2009

Diagnostics to roll out Inflammatory disorders:
SA ( enthesopathy)
Sjogren disease (30% association)
Lupus (22% association)
RA; PPR;syn. Hyper eosinophilia
Infectious diseases:
viral infections (Parvo;Hepatitis C,..)
post streptococcus
rheumatism
Metabolic diseases:
Hypothyroid
VIT- D deficiency multiple calcificationMetabolic syndrome ( obesity)
Constitutional anomalies :
Hyper laxity
poly articular dysplesia

Fibromyalgia and Depression
Pain Depression
Definition of FibromyalgiaFibromyalgia syndrome (FMS) is a common rheumatologic condition characterized by chronic widespread pain and reduced pain threshold, with hyperalgesia and allodynia. Associated features include fatigue, depression, anxiety, sleep disturbance, headache, migraine, variable bowel habits, diffuse abdominal pain and urinary frequency
Hudson JI, et al. Comorbidity of fibromyalgia with medical and psychiatric disorders. American Journal of Medicine 1992;92:363-367Mease P. Fibromyalgia syndrome: review of clinical presentation, pathogenesis, outcome measures, and treatment. Journal of Rheumatology 2005;6-21..

1990 ACR fibromyalgia criteria:
the core research standard 1. History of widespread pain 1. History of widespread pain
for at least 3 months in 4 for at least 3 months in 4 quadrants of the body quadrants of the body along with axial skeletal along with axial skeletal painpain
2. Pain at 11 or more of 18 2. Pain at 11 or more of 18 specifically designated specifically designated muscle-tendon sites called muscle-tendon sites called “tender points” . Palpation “tender points” . Palpation force of about 4 Kg.force of about 4 Kg.
3. Appropriate Rule/outs 3. Appropriate Rule/outs
Note: Tender points are sites that are normally more Note: Tender points are sites that are normally more tender i.e. sensitive to pressuretender i.e. sensitive to pressure

Clinical definition DescriptiveBased on subjective symptomsAbsence of psychopathological definition reflecting the specificity of this disease

Stressors Associated with the onset of Fibromyalgia
Early life stressorsChildren with stressors were 1.5- 2 x more likely to have a chronic widespread pain.
Certain catastrophic eventsPsychological stressTriggering events

Physical Symptoms Common In Psychiatric
Patients
Data from Kellner R, Sheffield BF. The one-week prevalence of symptoms in neurotic patients and normals. Am J Psychiatry 1973;130:102–105
Psychiatric Healthy Symptom Patients (%) Subjects (%)
Tiredness, lack of energy 85 40Headache, head pains 64 48Dizziness or faintness 60 14Feeling of weakness in parts of body 57 23Muscle pains, aches, rheumatism 53 27Stomach pains 51 20Chest pains 46 14
Hudson JI, et al.: Comorbidity of fibromyalgia with medical and psychiatric disorders. Am J Med 1992, 92:363–367

Fibromyalgia and depression differ in brain activation
patternsHealthy controls and patients FM without depression :
Activations in:In primary somatosensory cortexIn secondary somatosensory cortexAnterior insula
Patients FM with depression:
Activations inSame structuresAmygdalaMore act. In anterior insula

Physiopathology Troubles of nociception (peripheral theory):
Nociceptive Stimuli
Troubles of pain’s Modulation is a central matter:
Reduced pain thresholdPain’s amplificationExpansion of pain beyond affected organ or dermatome
Wolf 1994

Trouble of Nociception:peripheral stressors associated with fibromyalgia and chronic widespread
pain
Peripheral pain syndromes (RA,SLE,osteoarthritis)
Physical trauma or stressInfectionsHyperlaxity Whiplash-associated injuries
1.Clawn et al. J.Clin rheumatology 1995;1:335-422. Harkness EF, et al.AR & Rheum. 2004; 50:1665-1664.3. Albin JN; et al. J Autoimmun 2006,27: 145-152.4. Nef W, Gerber NJ: Schweiz Med Wochenschr 1998, 128:302–3105. Elert J, Kendall SA,et al.: J Rheumatol 2001, 28:1361–1368..

Peripheral changes at primary afferent neurons
after partial nerve lesion, leading to peripheral sensitization. Some axons are damaged and degenerate whereas others are still intact and connected with the peripheral end organ. The lesion triggers the expression of sodium channels on damaged C-fibers. Furthermore, products such as nerve growth factor triggering channel and receptor expression (sodium channels, TRPV1 receptors, adrenoceptors) on uninjured fibers.
Ralf Baron (2006) Mechanisms of Disease: neuropathic pain—a clinical perspective.Nat Clin Pract Neurol 2: 95–105 doi:10.1038/ncpneuro0113
Figure 2 Mechanisms of peripheral and central sensitization in neuropathic pain
Baron R. Nat Clin Pract Neurol 2: 95–105. 2006
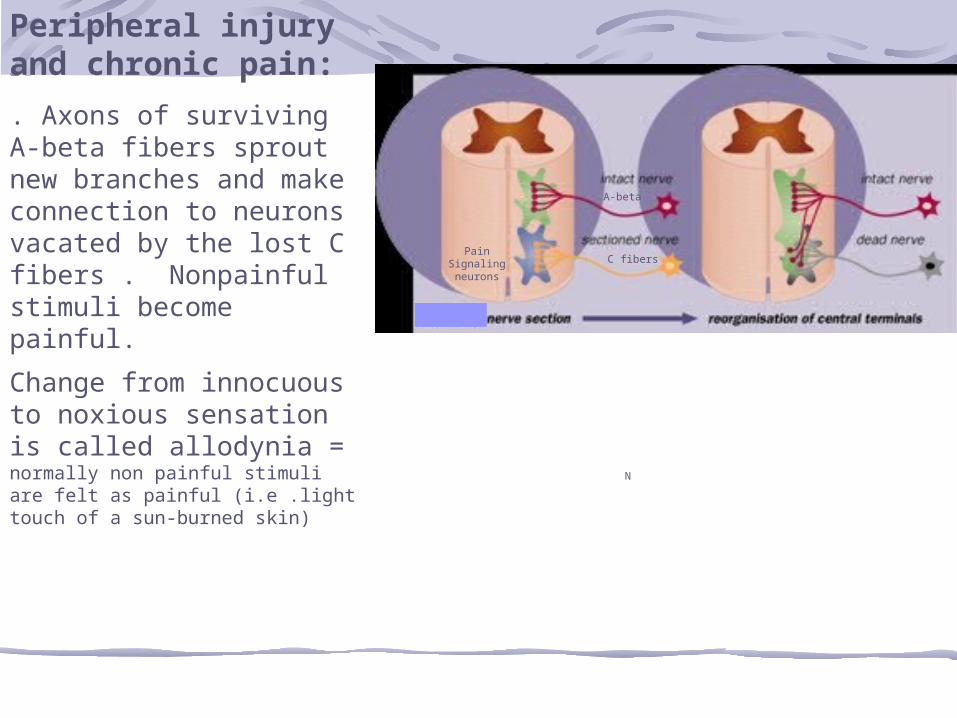
Peripheral injury and chronic pain:
. Axons of surviving A-beta fibers sprout new branches and make connection to neurons vacated by the lost C fibers . Nonpainful stimuli become painful.
Change from innocuous to noxious sensation is called allodynia = normally non painful stimuli are felt as painful (i.e .light touch of a sun-burned skin)
A-beta
C fibersPain
Signalingneurons
N

Neurogenic Inflammation In neurogenically inflammed tissue in Fibromyalgia, Enthesopathie, irritable bowel syndrome etc biopsy specimens can show:
Vasodilatation and plasma extravasationAbnormal sprouting of peripheral nerve terminalsMast cell accumulation
In patients with fibromyalgia, skin tissue RT-PCR positive signals were detected in:
19/50 for IL-1β14/51 for IL-617/53 for TNF-αIn healthy skin, none of these cytokines were detected
1.Sprott H, et al A&R 1997; 40: 1450-42.Salemi S, et al. J Rheumatology 2003; 30:146-50

CGRP
CGRP
Peripheral sensitization to pain:
Some definitions:Hyperalgesia increased sensitivity to an already painful stimulusAllodynia normally non painful stimuli are felt as painful (i.e .light touch of a sun-burned skin)

sensitization of the dorsal horn
Aβ - Aδ Afferents(pressure)
C-fibre nociceptor with resting activity
Wind-up at Widedynamic range -neuron
Descending inhibition; Diffuse noxious inhibitory control (DNIC) N-METHYL-D-ASPARTAT
Wind-up
externally applied stimulus evokes hyperalgesia (Aδ) and allodynia (Aβ) due to sensitization
KETAMIN
Baron 2004

Modulating Pain Pathways:unbalance between facilitation and
inhibition
Facilitation• Substance P•Glutamate and EAA•Serotonin (5HT 2a,3a)•Neurotensin•Nerve growth factor•Cholecystokinin
Inhibition•Descending anti-nociceptive pathways
•Norepinephrine•Serotonine (5HT 1a,b)•Dopamine•opoids
•GABA•Cannabinoids•Adenosine
EAA = Excitatory amino acids , GABA = gamma-aminobutyric acid
Chronic pain resultsIncrease excitation Decrease inhibition
N-methyl-D-aspartate

Evolution of Allodynia & Hyperalgesia
Effects of NMDA receptor activation:Spinal neurons carrying pain signal can be stimulated with less peripheral inputLess glutamate is required to transmit pain signalMore anti-nociceptive input to stop it
Endomorphins and other naturally occuring pain-relievers cannot keep up with the demand and essentially lose their effectiveness
Dickerson AH. 1994N-methyl-D-aspartate

Serotonin Deficiency Serotonin
Inhibits release of spinal cord substance P by afferents neurons
Low concentrations of serum tryptophan and serotonin exist in chronic pain patients
Correlates with their number of myofascial tender pointIn fibromyalgia, low serotonin manifests specifically in peripheral platelets
Russel IJ: Z Rheumatol 1998, 57(Suppl 2):63–68.

Serotonin Deficiency CSF substance P levels in patients with fibromyalgia:
Are 2-3 x than controlsAre not increasing by the induction of noxious stimuli to tender points
SP levels are normal or low in a variety of chronic painful conditions (low back pain, diabetic neuropathy etc.)

Expansion of pain beyond affected organ
Widespread versus localized

Model of central pain sensitization
Intense or prolonged impulses from afferents depolarize dorsal horn
There is an flux of extracellular Ca into neurons.
An exaggerated release of substance P and glutamate leads
to neuronal hyperexcitability
Amplified pain signal is sent to the brain from the dorsal horn

NMDA Receptor ActivationActivation of NMDA receptors:
Cause neural cells to sprout new connective endingsNeural remodeling adds new dimensions to old sensations
Emotional component of painMay be increased if the new connections channel more of the pain signal to the brain’s reticular activating systemThe signal’s pathways into the cerebral cortex is more splayedConsequently, pain signals is more diffuse and difficult to localize

Apoptosis from NMDA Receptor Activation
NMDA receptor activation normal apoptosis trough a series of events involving multiple interdependent events:
Neurotrauma mediates neuronal death Data suggest that chronic pain follows a similar destructive processus The requires timely treatment to limit damage that glutamate-mediated excito-toxicity incites.
Arundine M. et al. Cell Mol Life Sci. 2004; 61: 657-68

Immunology of Pain & Hyperalgesia
Astrocytes and microglia release key mediators of hyperalgesia
NONMDACytokines (TNF IL-1..)NGF
Watkins LR, et al. 1999

Neural Plasticity & RemodlingThe presence of c-fos protein in spinal cord cells:
Marker for neuron activationC-fos may also indicate central hypersensitizationAlternatively, c-fos-expressing neurons may be inhibitory interneurons activated by noxious stimuli
Protein products of these genes
Function as a transcriptor factorsTrigger long-lasting plastic changes in CNS neurons
Harris JA 1998N-methyl-D-aspartate, alpha-amino-3-hydroxy 5-methyloxzazole-4-proprionate

Neural Plasticity and Remodeling
With persistent of pain, c-fos protein spreads to progressively higher levels of the spinal cord
Eventually reach the thalamus, at witch pain may be untreatable Explain why patient with chronic suffering find their pain has spread beyond affected organ or dermatomeThat why we can make a false conclusion that the patient’s pain is psychogenic

Neurogenic Inflammation evoke the Role of SP
In neurogenically inflammed tissue in Fibromyalgia, Enthesopathie, irritable bowel syndrome etc biopsy specimens can show:
Vasodilatation and plasma extravasationAbnormal sprouting of peripheral nerve terminalsMast cell accumulationWithout infiltration of the site by the inflammatory cells
Wolf 1994Weihe 1991

Afferents may become Efferent
Neurons can carry signals in afferent or afferent directionWith the prolonged generation of pain signals, a dorsal root reflex can become pathologically establishedAfferent cells in the dorsal horn release mediators that cause action potentials to fire antidromicallyAn antidromic impulse in an axon refers to conduction opposite to the normal
Dimitriadou V. et al. neuroscience 1997;77: 829-39

Neuron inflammationThe release of SP & NGF into the periphery causes a tissue reaction
Driven by CNS eventsNot depending of inflammation’s cellsSubstance P causes mast cell degranulationVascular endothelial effects : release of bradikinin and production of NO and that lead to vasodilatation of vessels
Antidromic
stim
ulation
NGF
Chronic pain
Dimitriadou V. et al. neuroscience 1997;77: 829-39

Why stress can generate and increase pain?
Stress influences pain transmission and stress can produce central analgesiaThe stress response is primarily mediated trough the HPA axis and the automatic nervous systemAbnormalities of the HPA axis found in pain syndrome
One third of adult fibromyalgia patients are growth hormone deficient
HPA: HYPOTHALAMIC-PITUATIRY-ADRENAL

Peripheral stressors
Exposures syndromes
Hyperalgesia/allodynia and/or central sensitization.
Long-term neuroplastic changes
Chronic pain

Mechanistic Classification of Chronic Pain Disorders
Peripheral (nociceptive)
Neuropathic Central
( non noxious)
•Inflammatory ormechanical damage:
•Osteoarthritis•Rheumatoid arthritis
•Damage or entrapment ofperipheral nerve:
•Diabetic neuropathy•Post-herpetic neuralgia
•Central disturbance in pain processing:
•Fibromyalgia •Irritable bowel syn.•Headache•Idiopathic low back pain•Temporomandibular disorder•Others ….

Fibromyalgia It’s not a real illness, it’s in the
“patient’s head”
It’s a real illness, it’s in the’’ patient’s brain’’

Peripheral tissueNSAIDS OPOIDS
Peripheral nerveNa channels blockers
Anti-epileptics
Dorsal horn descendingMonoamine reuptake
InhibitorsGABA agonists
Dorsal horn ascendingNMDA antogonists
Substance P antogonistsNGF antagonists
Nitric oxide
Midbrain Opoids
Alpha-2adrenergic agonistsTramadol
Supraspinal OpoidsSSRIs
Serotonine Dopamine
Adrenergic agonists