thuốc điều trị tăng huyết áp trên bệnh thận đái tháo đường - bs phạm văn...
TRANSCRIPT
HYPERTENSION
&
THE KIDNEY Prof Pham Van Bui
PNT University of Medicine
NTP Hospital, Viet Nam
Invited Professor, Liège University, Belgium

HYPERTENSION & KIDNEY



8
4 questions in pts with HT
Primary or secondary?
Pathophysiology ?
CV Risk factors& co-morbidities?
Primary or secondary prevention:
Target –organ involvement?
Heart(LVH)
Kidney(proteinuria) Bakris LG (2013). CME. Med Educ
9
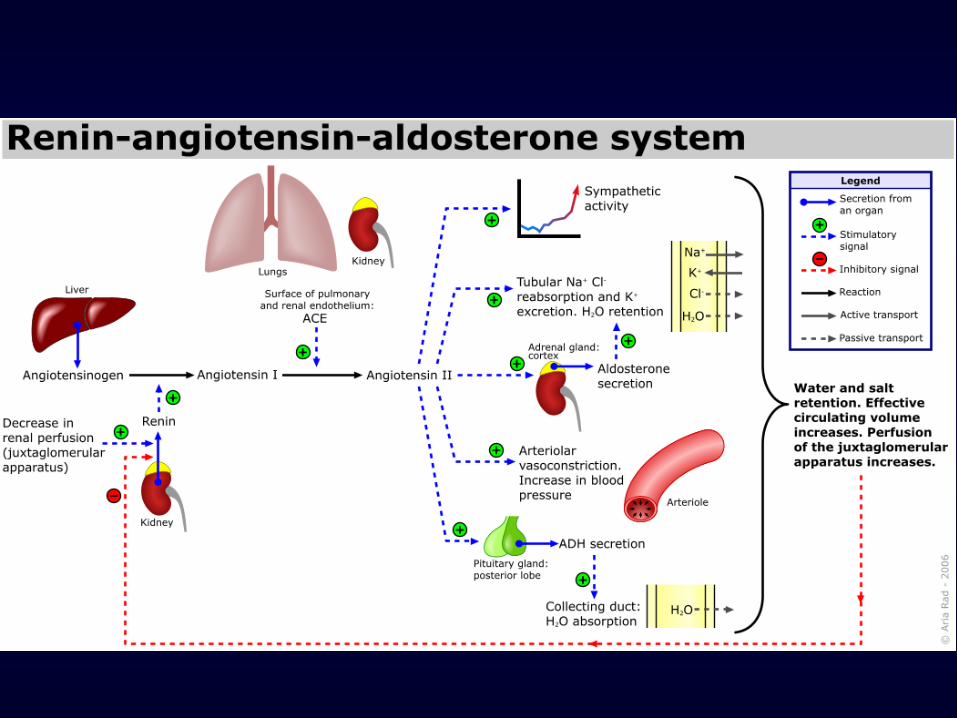
Key considerations in pathophysiology of HT
Volume, sodium loading, volume status
Renin-angiotensin-aldosterone system(RAS)
Sympathetic nervous system
Comorbidities
Other vasoactive substances(NO, PGl, endothelin,
EDHF) → endothelial dysfunction
Genetic components
Bakris LG (2013). CME. Med Educ
10
Key considerations in pathophysiology of HT
Volume, sodium loading, volume status
Renin-angiotensin-aldosterone system(RAS)
Sympathetic nervous system
Comorbidities
Other vasoactive substances(NO, PGl, endothelin,
EDHF) → endothelial dysfunction
Genetic components
Bakris LG (2013). CME. Med Educ

• Salt retention along w/ volume overload:
major cause of HT in patients with CKD
• Verdalles et al. used BIS to assess fluid status
and guided the use of diuretics to treat HT in
CKD patients not on dialysis.
• 30 patients w/ ECV expansion treated =
diuretic
• 20 patients w/o ECV expansion receiving
another additional antiHT medication
Verdalles U, et al(2012). Nephrol Dial Transplant 2012; 27 (Suppl 4):iv31–iv35.

At 6 months of follow-up, :
Pts w/ ECV expansion (30
treated=diuretic)
Pts w/o ECV expansion (20
treated =
another antiHT
med. )
P
↓sBlood
Pressure
21 mmHg 09 mmHg < 0.01
Target BP <
140/90 mmHg 09/30 pts 02/20 pts < 0.01
Verdalles U, et al(2012). Nephrol Dial Transplant 2012; 27 (Suppl 4):iv31–iv35.
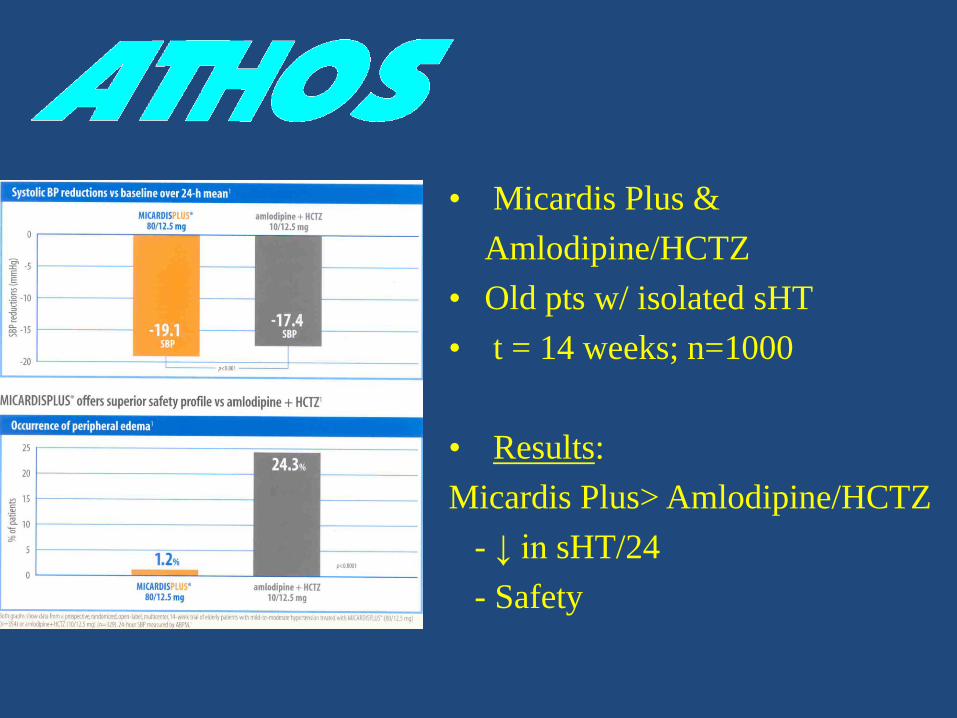
• Micardis Plus &
Amlodipine/HCTZ
• Old pts w/ isolated sHT
• t = 14 weeks; n=1000
• Results:
Micardis Plus> Amlodipine/HCTZ
- ↓ in sHT/24
- Safety
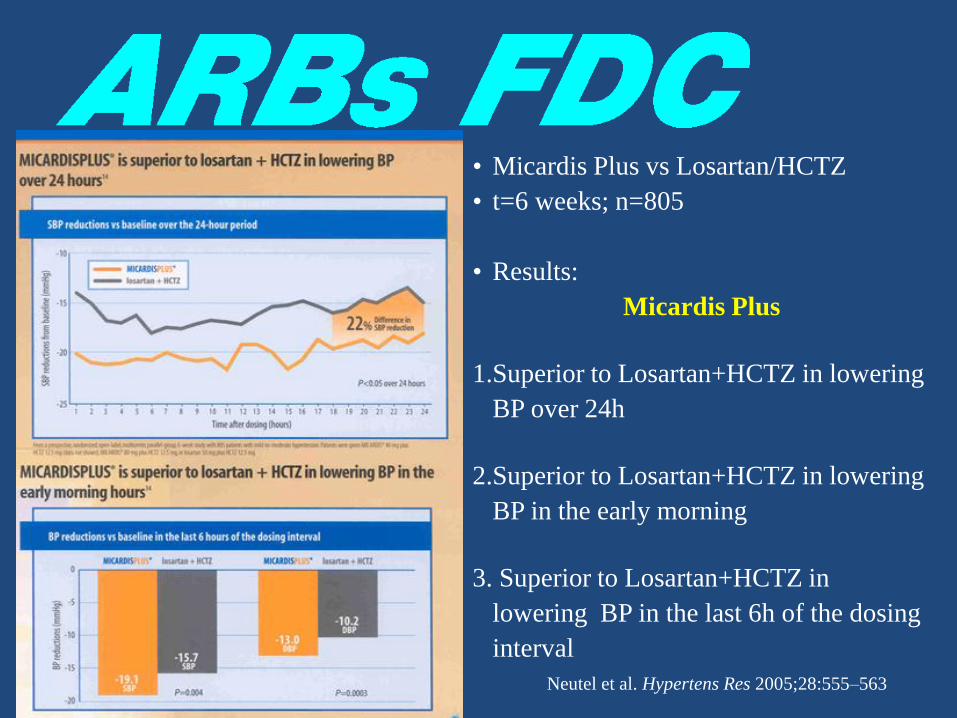
• Micardis Plus vs Losartan/HCTZ
• t=6 weeks; n=805
• Results:
Micardis Plus
1.Superior to Losartan+HCTZ in lowering
BP over 24h
2.Superior to Losartan+HCTZ in lowering
BP in the early morning
3. Superior to Losartan+HCTZ in
lowering BP in the last 6h of the dosing
interval
Neutel et al. Hypertens Res 2005;28:555–563

Thiazides in CKD
• The traditional teaching has been that
thiazides become ineffective when
GFR< 30ml/min whereas loop
diuretics remain effective in
advanced CKD. Although widely
accepted, this traditional notion has
been called into question by a recent
pilot study
Opie HL.(2013). Diuretics. In Drugs for the Heart
A Pilot Study Comparing Furosemide
and HCTZ in Patients With Hypertension
and Stage 4 or 5 CKD
• RCT, crossover trial of 23 pts w/ HT & CKD
G4/5, 3 months ttt w/ either HCTZ(25mg/d)
or long acting furosemide (60mg/d)
• No differences between furosemide and
HCTZ with respect to natriuresis and BP
control in patients with HT and CKD.
Bertrand Dussol et al(2012). J Clin Hypertens (Greenwich)

In Advanced CKD,
Thiazide May Help Control BP
Dialogue b/w Bakris GL & Agarwal R:
• 7 studies of thiazides in patients with CKD.
We found that there may be some evidence
that Thiazides may work, even for people
with advanced kidney disease
Bakris GL, Agarwal R(2014).lIn Advanced CKD, Thiazide May Help Control BP. Medscape. May 20, 2014.

Chlorthalidone for Poorly Controlled HT in CKD:
An Interventional Pilot Study
• 14 subjects 67.5 years, taking median of 4
antihypertensive drug (incl RAS blockers)
• eGFR :26.8 ± 8.8 ml/min/1.73 m2 (20-45 )
• Chlorthalidone
• 25 mg/day added to existing medications
• dose doubled every 4w if BP still high
• Twelve subjects completed the 12-week
treatment phase
Agarwal R et al(2014).Am J Nephrol (Abst(

Ambulatory BP
Response
Ag
arwal R
et al(20
14
).Am
J Nep
hro
l (Ab
st)
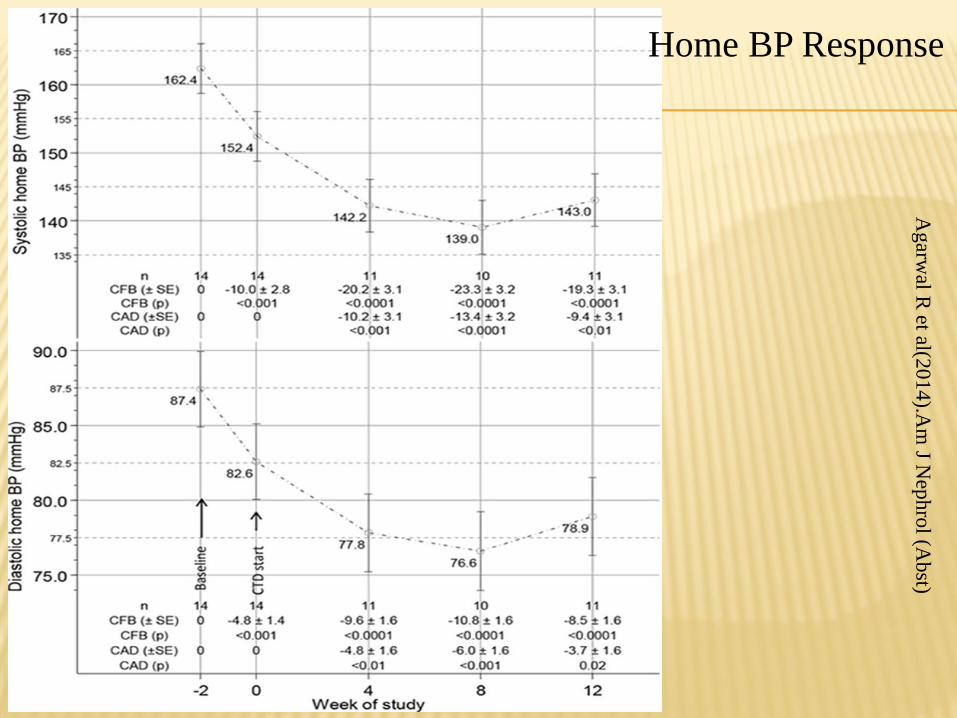
Home BP Response A
garw
al R et al(2
01
4).A
m J N
eph
rol (A
bst)
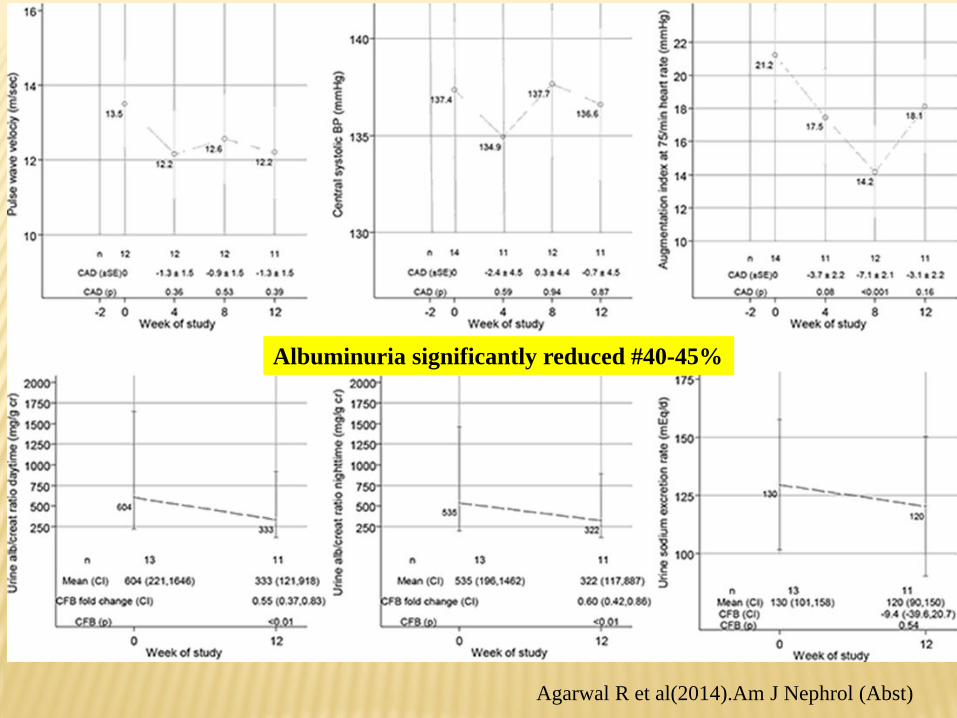
Albuminuria significantly reduced #40-45%
Agarwal R et al(2014).Am J Nephrol (Abst)


KDIGO Clinical Practice Guideline for the
Management of BP in CKD 2013
• Thiazides: one of the first 2 or 3 drugs used for
BP lowering in CKD, particularly :
• Edema
• Add-on ACE-Is/ARBs
• Potentiate the effect of other
antihypertensive agents, particularly
ACE-Is/ARBs
• ↓ risk of hyperkalemia
• ↓ Albuminuria

25
Key considerations in pathophysiology of HT
Volume, sodium loading, volume status
Renin-angiotensin-aldosterone system(RAS)
Sympathetic nervous system
Comorbidities
Other vasoactive substances(NO, PGl, endothelin,
EDHF) → endothelial dysfunction
Genetic components
Bakris LG (2013). CME. Med Educ
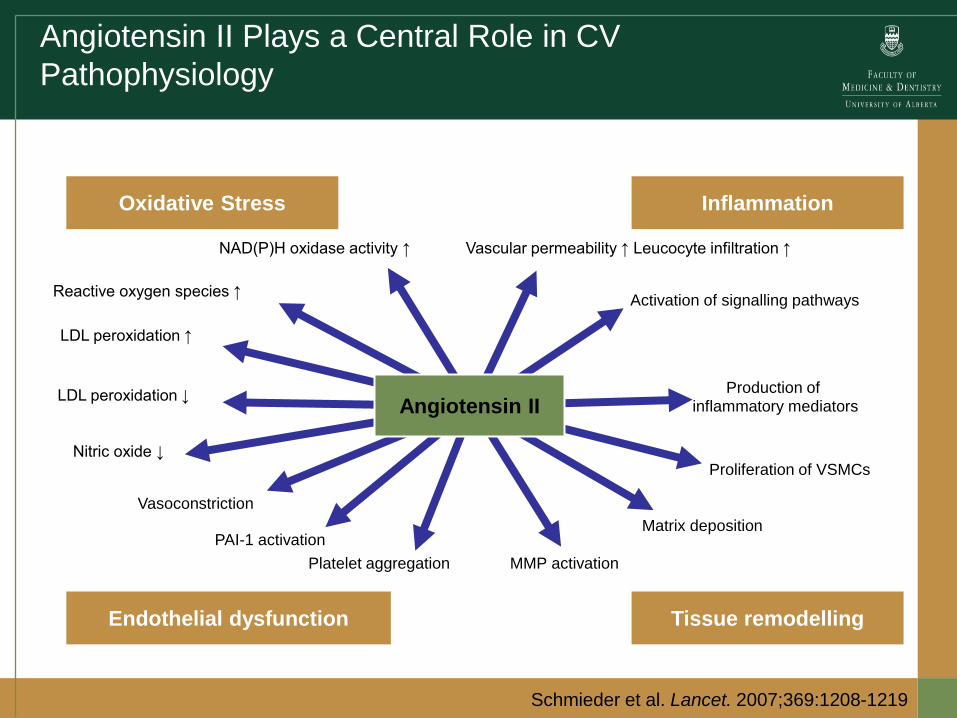
Angiotensin II Plays a Central Role in CV
Pathophysiology
Oxidative Stress Inflammation
Endothelial dysfunction Tissue remodelling
Vascular permeability ↑ Leucocyte infiltration ↑
Activation of signalling pathways
Production of inflammatory mediators
Proliferation of VSMCs
Matrix deposition
MMP activation Platelet aggregation
PAI-1 activation
Vasoconstriction
Nitric oxide ↓
LDL peroxidation ↓
LDL peroxidation ↑
Reactive oxygen species ↑
NAD(P)H oxidase activity ↑
Angiotensin II
Schmieder et al. Lancet. 2007;369:1208-1219
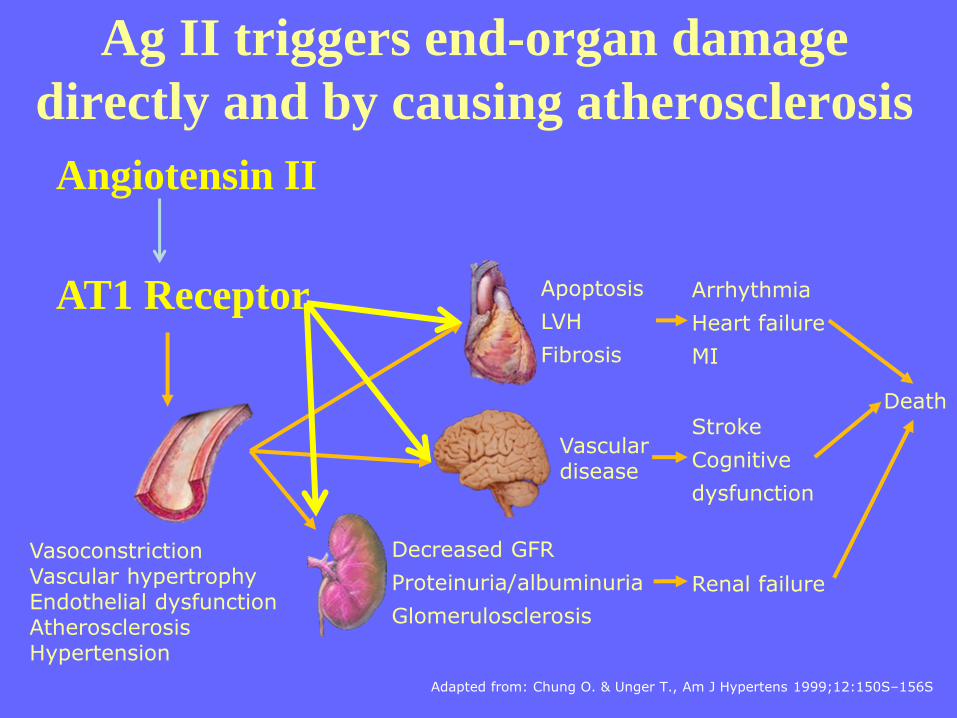
Ag II triggers end-organ damage
directly and by causing atherosclerosis
Adapted from: Chung O. & Unger T., Am J Hypertens 1999;12:150S–156S
Angiotensin II
Vasoconstriction Vascular hypertrophy Endothelial dysfunction Atherosclerosis Hypertension
Decreased GFR
Proteinuria/albuminuria
Glomerulosclerosis
Vascular disease
Apoptosis
LVH
Fibrosis
Arrhythmia
Heart failure
MI
Stroke
Cognitive
dysfunction
Renal failure
Death
AT1 Receptor

Where Are We in Diabetic Nephropathy
MicroRNAs and Biomarkers?
McClelland et al. Curr Opin Nephrol Hypertens. 2014

It appears that AngII-induced hypertension
increases miR-132 and miR-212 in organs
associated with blood pressure control, including
the kidney.
Significant decrease in miR-132 and miR-212
were observed in arteries of angiotensin
receptor blocker (ARB)-treated patients, but
treatment with β-blockers had no effect.
McClelland et al. Curr Opin Nephrol Hypertens. 2014

INTERNATIONAL GUIDELINES
R8. In the general
population aged ≥18y w/
CKD, initial(or add-on )
antihypertensive treatment
should include an ACEI
or ARB to improve
kidney outcome. This
applies to all CKD
patients w/ hypertension
regardless of race or
diabetic state (Moderate
Recommendation- Grade
B)
Pharmacological
therapy for patients
w/ diabetes and
hypertension should
comprise a regimen
that includes either
an ACEI or ARB. If
one class is not
tolerated, the other
should be substitued .
C
CKD ND pts w/o DM
ARB /ACEI use in adults
w/ CKD ND and UAE of
30-300mg/24h(S-2D)or
>300mg/24h(R-1B) in
whom treated w/ BP-
lowering drugs is indicated
CKD ND pts w/ DM
ARB /ACEI use in adults
w/ diabetes and CKD ND
w/ UAE of 30-300mg/24h
(S) or UAE > 300mg/24h
(R)
JNC 8, 2014 DIABETIC CARE
2014 KDIGO 2013:

Antihypertensives May Delay
Kidney Disease Progression
Hsu TW et al(2013). JAMA Dec
In advanced stage of CKD + stable HT by RAA
blocking medicines →lower risk of advancing to
long-term dialysis or dying ?
Prospective cohort study: 28,497 predialysis
patients with advanced CKD, HT, and anemia.
B/w January 1, 2000, and June 30, 2009,
20,152 pts (70.7%) requiring long-term
dialysis
5696 (20.0%) died before progressing ESRD
Antihypertensives May Delay Kidney
Disease Progression
• Compared w/ pts not using ACEIs/ARBs Use of
ACEIs/ARBs :
• ↓ 6% risk for long-term dialysis ( HR 0.94;
95% CI, 0.91 - 0.97)
• ↓ 6% risk in the composite outcome of
long-term dialysis or death (HR, 0.94; 95%
CI, 0.92 - 0.97).
Hsu TW et al(2013). JAMA Dec

KDIGO Clinical Practice Guideline for the
Management of BP in CKD 2013
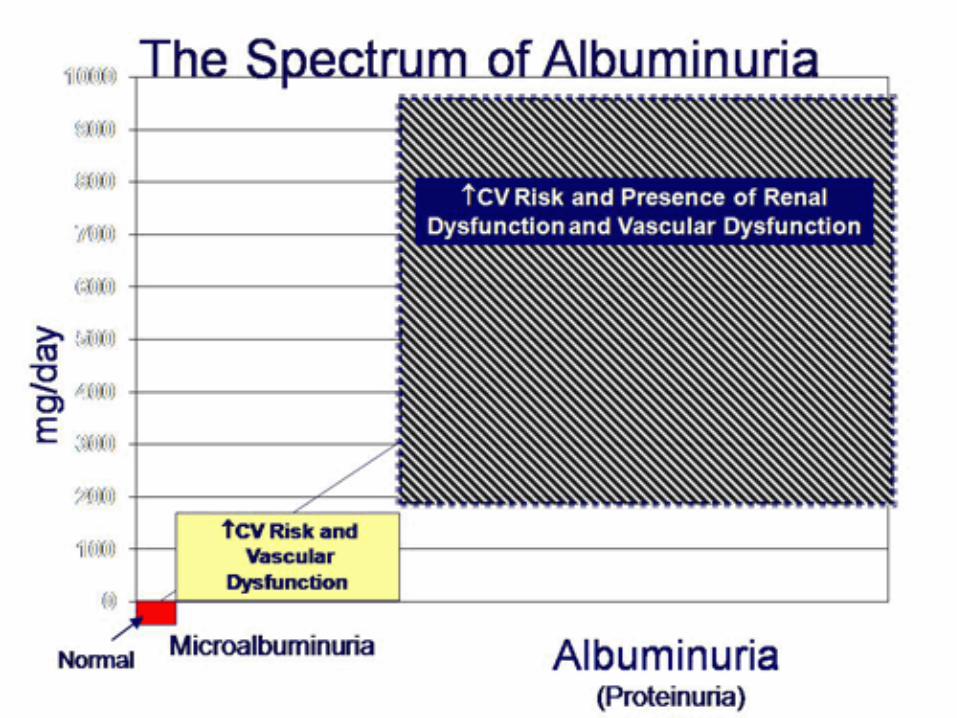
• Albuminuria. The level of
albuminuria in CKD
predicts not only the
prognosis with respect to
kidney function but also
morbidity and mortality
from CVD events including
stroke.

Shaded areas represent 95% CIs.
Models included spline eGFR, categorical
albuminuria, and their interaction terms
as well as adjustment for age, sex, ethnic
origin, history of cardiovascular disease,
systolic blood pressure, diabetes,
smoking, and total cholesterol. The
reference (diamond) was eGFR 95
mL/min/1.73 m² plus ACR less than 3.4
mg/mmol (30 mg/g) or dipstick test result
negative or trace. Circles represent
statistically significant and triangles
represent not significant.
Decline in eGFR and albumin:creatinine ratio are
closely linked to CV mortality
CKDPC Lancet 2010;375:2073-2081.
Guideline 6: Management of Albuminuria
in Normotensive Patients with Diabetes
Treatments that produce a lasting
decrease in urinary albumin
excretion may slow the
progression of DKD even in the
absence of hypertension.
NFK KDOQI CLINICAL PRACTICE GUIDELINE FOR DIABETES AND CKD:
2012 UPDATE

KDIGO Clinical Practice Guideline for the
Management of BP in CKD 2013
• Some BP-lowering agents are particular
effective at reducing albuminuria or
proteinuria, suggesting that BP management
should differ depending on the amount
of albumin or protein in the urine
• ACE-Is and ARBs are valuable BP-
reducing agents in CKD patients, are
indicated if urinary albumin excretion is
elevated and are safe to combine with
most other BP-reducing agents.

• The transition RR to overt
nephropathy ↓ # 66%
(telmisartan 80mg) 55%(
telmisartan 40 mg)/ placebo (a)
• The renoprotective benefit of
telmisartan also apparent in
normotensive patients at
baseline (b), suggesting a BP-
independent effect
(The INcipieNt to OVert: AII receptor blocker,
Telmisartan, Investigation On type 2 diabetic Nephropathy)
Makino et al. Diabetes Care 2007

*P<0.05 vs losartan not attributed
to BP control, as reductions in
systolic and diastolic BP similar in
both treatment arms
Proteinuria reduction at 1 year
-35
-30
-25
-20
-15
-10
-5
0
Telmisartan 40-80 mg Losartan 50-100 mg
Pro
tein
uri
a-a
dju
ste
d m
ea
n c
ha
ng
e (
%)
29%
reduction*
20%
reduction
Bakris et al . Kidney International 2008 74:364-369
• Telmisartan vs. Losartan
• t = 52 weeks
• 1566 Hyertensive diabetic pts w/ overt nephropathy
After a 2-month period in
which both drugs were
stopped: a sustained and
persistent antiproteinuric
effect with the novel
ARB(Telmisartan).
A trial to compare telMisartan 40 mg titrated to 80 mg versus
losArtan 50 mg titrated to 100 mg in hypertensive type 2
DiabEtic patients with Overt nephropathy: 1566 patients
Telmisartan more renoprotective than losartan
Micardis reduces proteinuria
significantly better than losartan
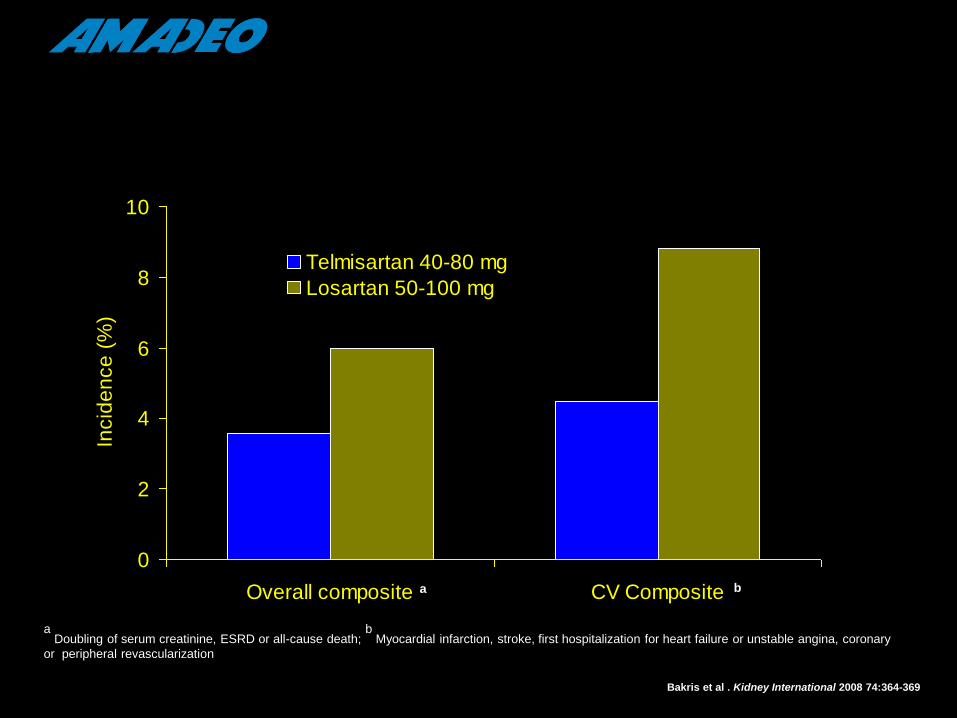
0
2
4
6
8
10
Overall composite CV Composite
Incid
en
ce
(%
)
Telmisartan 40-80 mg
Losartan 50-100 mg
a Doubling of serum creatinine, ESRD or all-cause death;
b Myocardial infarction, stroke, first hospitalization for heart failure or unstable angina, coronary
or peripheral revascularization
a b
Bakris et al . Kidney International 2008 74:364-369
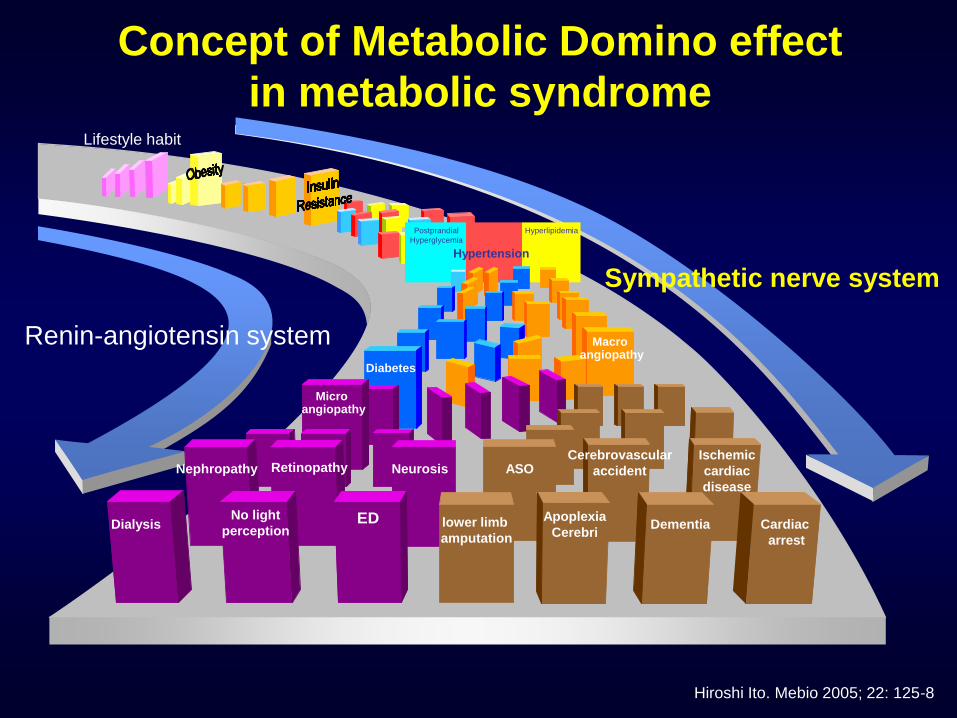
Concept of Metabolic Domino effect
in metabolic syndrome
Hiroshi Ito. Mebio 2005; 22: 125-8
Cardiac
arrest
Hyperlipidemia
Dementia Apoplexia
Cerebri lower limb
amputation
ED No light
perception Dialysis
Nephropathy Retinopathy Neurosis ASO Cerebrovascular
accident
Ischemic
cardiac
disease
Micro angiopathy
Diabetes
Macro angiopathy
Hypertension
Postprandial
Hyperglycemia
Lifestyle habit
Sympathetic nerve system
Renin-angiotensin system

Hypertension
/ARB
, CCB
Samir G Mallat. Cardiovasc Diabetol. 2012;11(32):1-12.; Mancia G . J Hypertens 2009,
27(11):2121–2158 ; K/DOQI. Am J Kidney Dis 2004, 43(5 Suppl 1):S1–S290.
• ASH indicated a preference for RAS
blockers in combination with either a
diuretic or CCB, with selection
dependent on individual patient F*,
including additional CV risk factors &
comorbidities
What is a Preferred ARB-based Combination
Therapy for BP Control in HT Patients With
Diabetic and Non-diabetic Renal Impairment
What is a Preferred ARB-based Combination
Therapy for BP Control in HT Patients With
Diabetic and Non-diabetic Renal Impairment
Samir G Mallat. Cardiovasc Diabetol. 2012;11(32):1-12.; Mancia G . J Hypertens 2009,
27(11):2121–2158 ; K/DOQI. Am J Kidney Dis 2004, 43(5 Suppl 1):S1–S290.
• In pts with evidence of renal disease or in those with a
greater risk of developing renal disease(pts w/ DM & high-
normal BP or overt HT), guidelines clearly recommend
RAS blocker-based combination therapy superior
renoprotective effects
• ARB-based preferred > ACE inhibitors:
• Superior tolerability& adherence
• Delay the progression of DKD
• Delay development of diabetes in at-risk patients
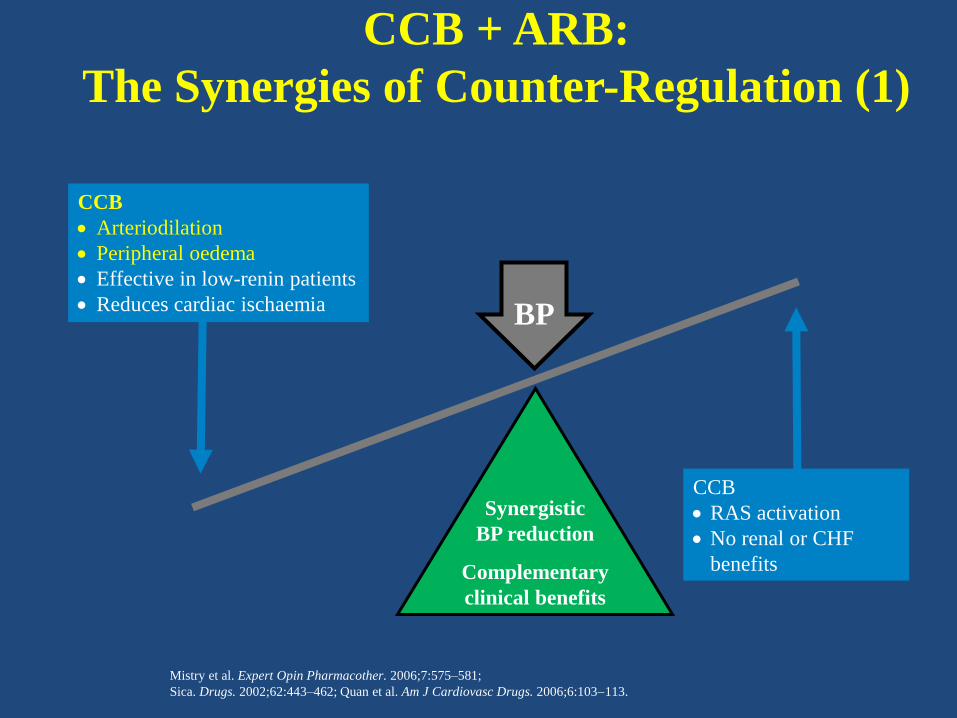
CCB + ARB:
The Synergies of Counter-Regulation (1)
Synergistic
BP reduction
Complementary
clinical benefits
CCB
Arteriodilation
Peripheral oedema
Effective in low-renin patients
Reduces cardiac ischaemia
CCB
RAS activation
No renal or CHF
benefits
BP
Mistry et al. Expert Opin Pharmacother. 2006;7:575–581;
Sica. Drugs. 2002;62:443–462; Quan et al. Am J Cardiovasc Drugs. 2006;6:103113.
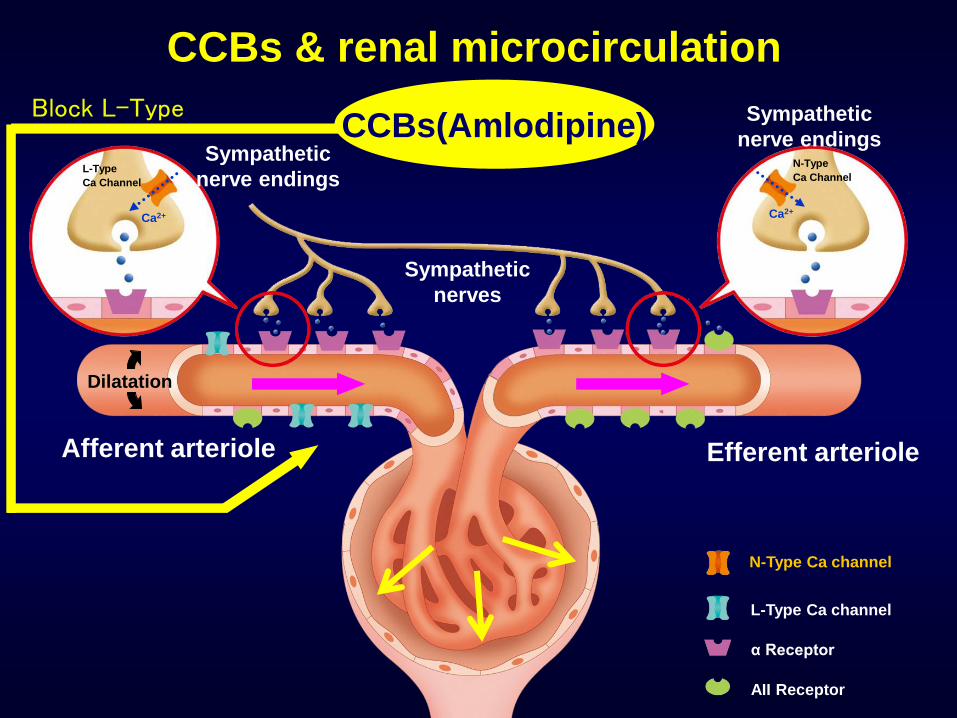
Afferent arteriole Efferent arteriole
CCBs(Amlodipine) Block L-Type
Dilatation
N-Type Ca channel
L-Type Ca channel
α Receptor
AII Receptor
CCBs & renal microcirculation
Sympathetic
nerve endings
Ca2+ Ca2+
N-Type
Ca Channel L-Type
Ca Channel
Sympathetic
nerve endings
Sympathetic
nerves

CCB + ARB:
The Synergies of Counter-Regulation (2)
ARB
Venodilation
Attenuates peripheral oedema
Effective in high-renin patients
No effect on cardiac ischaemia
ARB
RAS blockade
CHF and renal
benefits
Mistry et al. Expert Opin Pharmacother. 2006;7:575–581; Sica. Drugs. 2002;62:443–462; Quan et al. Am J Cardiovasc Drugs. 2006;6:103113.
Synergistic
BP reduction
Complementary clinical benefits
BP
CCB
Arteriodilation
Peripheral oedema
Effective in low-renin patients
Reduces cardiac ischaemia
CCB
RAS activation
No renal or CHF
benefits
The Two Key Components of BP Regulation
Grassi. J Hypertens. 2001;19:1713–1716; modified.
© Theodore Kurtz, MD
all rights reserved
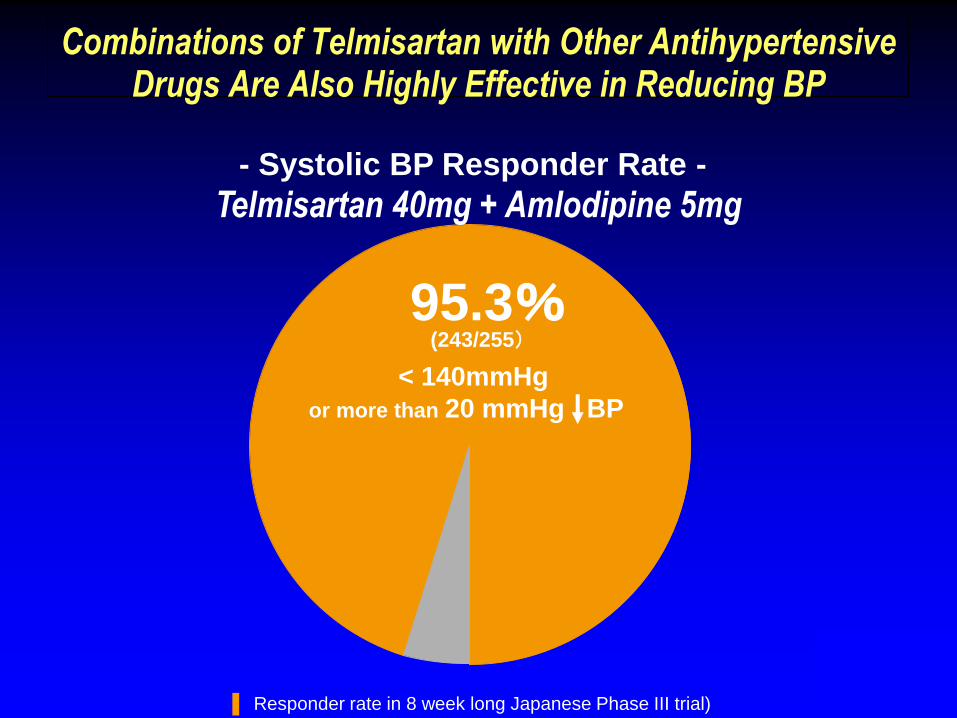
Combinations of Telmisartan with Other Antihypertensive Drugs Are Also Highly Effective in Reducing BP
▐ Responder rate in 8 week long Japanese Phase III trial)
- Systolic BP Responder Rate -
< 140mmHg
or more than 20 mmHg BP
(243/255)
Telmisartan 40mg + Amlodipine 5mg
95.3%

Afferent arteriole Efferent arteriole
CCBs Block L-Type
Dilatation Dilatation
RAS inhibitors
N-Type Ca channel
L-Type Ca channel
α Receptor
AII Receptor
MOA of CCBs & RASIs on renal microcirculation
Sympathetic
nerve endings
Ca2+ Ca2+
N-Type
Ca Channel
Additive
effect
L-Type
Ca Channel
Sympathetic
nerve endings
Sympathetic
nerves
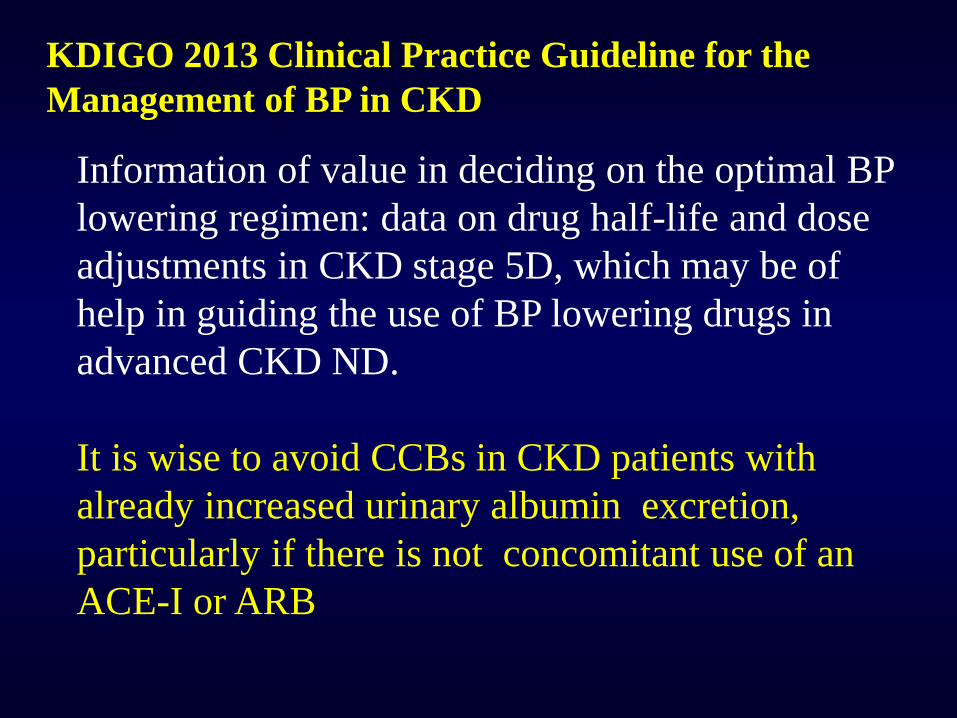
KDIGO 2013 Clinical Practice Guideline for the
Management of BP in CKD
Information of value in deciding on the optimal BP
lowering regimen: data on drug half-life and dose
adjustments in CKD stage 5D, which may be of
help in guiding the use of BP lowering drugs in
advanced CKD ND.
It is wise to avoid CCBs in CKD patients with
already increased urinary albumin excretion,
particularly if there is not concomitant use of an
ACE-I or ARB
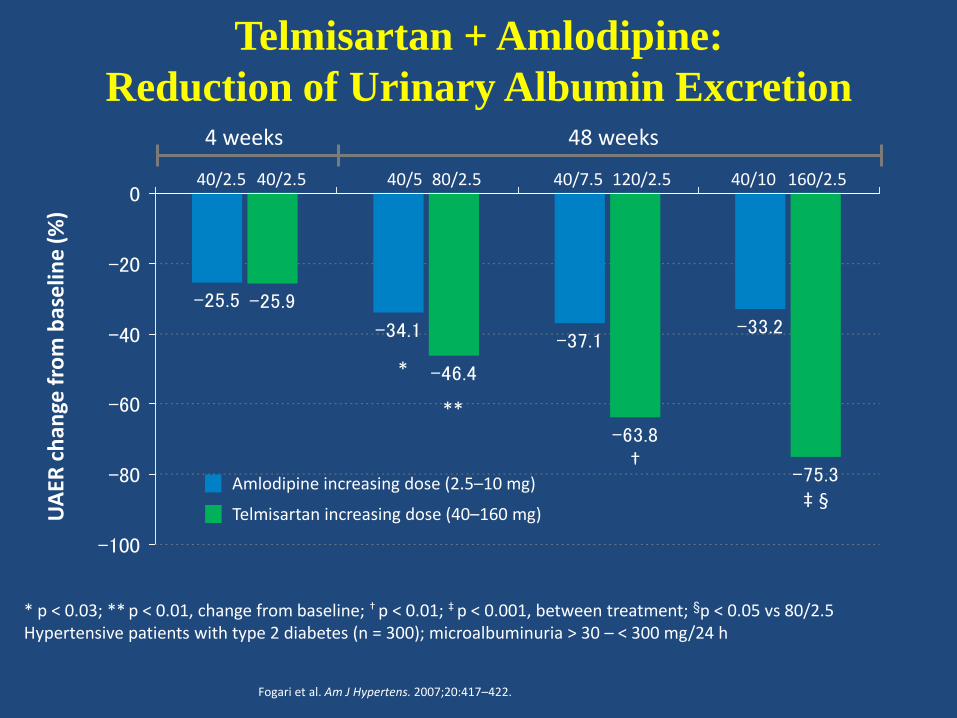
Telmisartan + Amlodipine:
Reduction of Urinary Albumin Excretion
-25.5
-34.1-37.1
-33.2
-25.9
-46.4
-63.8
-75.3
-100
-80
-60
-40
-20
0
* p < 0.03; ** p < 0.01, change from baseline; † p < 0.01; ‡ p < 0.001, between treatment; §p < 0.05 vs 80/2.5 Hypertensive patients with type 2 diabetes (n = 300); microalbuminuria > 30 – < 300 mg/24 h
*
†
**
‡ §
Fogari et al. Am J Hypertens. 2007;20:417–422.
UA
ER c
han
ge f
rom
bas
elin
e (%
)
Telmisartan increasing dose (40–160 mg)
40/2.5 40/5 40/7.5 40/10
4 weeks 48 weeks
40/2.5 80/2.5 120/2.5 160/2.5
Amlodipine increasing dose (2.5–10 mg)

DIABETIC CARE 2014
• Multiple-drug therapy(two or more
agents at maximal doses) is generally
required to achieve BP target. B
• Administer one or more
antihypertensive medications at
bedtime. A
AMAZING KIDNEYS !