the role of tofac (1)
TRANSCRIPT

New chapter in RA therapyPresented By Nehal El Ghobashy

The role of kinase inhibitors in Ra

introductionRheumatoid arthritis (RA) is a systemic multifactorial immune-mediated disease with circadian clinical symptomatology. It is mainly characterized by synovial tissue proliferation and subintimal infiltration of inflammatory cells, followed by progressive and symmetrical damage of the joints [McInnes and Schett, 2011)

Over the last ten years• The use of biologics has improved the outcomes for RA
patients, however Challenge remains because:-• a significant percentage of patients either cannot
tolerate or obtain incomplete relief from these medications.
• Additionally, the cost of therapy remains very high, and the patients have to undergo either intravenous or subcutaneous injections.

More recently,• a new category of drugs targeting small signaling molecules
(kinases) found in cytokine receptors expressed on Tcells & Bcells is now used for treatment of resistant rheumatoid arthritis.
• In case of rheumatoid arthritis:- kinases play a central role in the aberrant immune system activation & they are:-
• Mitogen-activated phosphokinase p38 (MAPK) • spleen tyrosine kinase (Syk) • Janus kinases (JAKs)
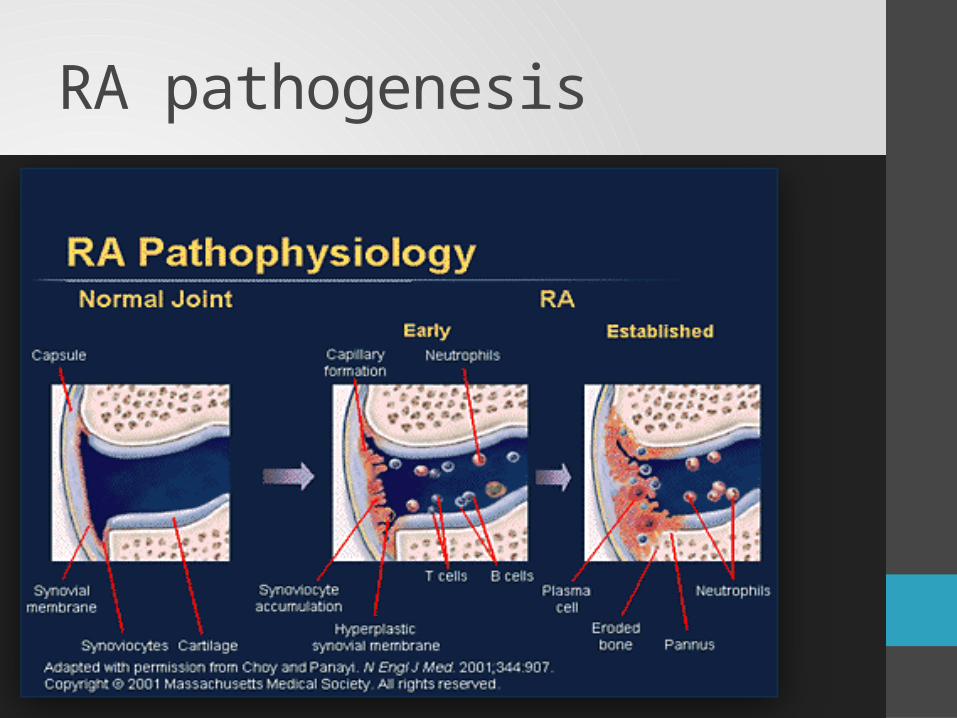
RA pathogenesis

T cell activation
• Antigen recognition
• Cytokine binds to Tcell receptor which leads to T cell proliferation and differintiation. This occurs through many pathways , one of them is jak stat pathway.
signal1
Signal 2

JAK-STAT signaling pathway
• The JAK-STAT signaling pathway :-transmits information from chemical signals outside the cell, through the cell membrane, and into gene promoters on the DNA in the cell nucleus, which causes DNA transcription and activity in the cell. The JAK-STAT system is a major signaling alternative to the second messenger system.
• Many JAK-STAT pathways are expressed in white blood cells, and are therefore involved in regulation of the immune system.
• The JAK-STAT system consists of three main components: • (1) a receptor .• (2) Janus kinase (JAK). • (3) Signal Transducer and Activator of Transcription.

Mechanism• Cytokine signaling:• Inactive janus kinase associate with cytokine receptor• They are attached to cytoplasmic domains of cytokine
receptors.
jaky
Cell membrane
Cytokine receptors
jaky

Cytokine attached to receptor
y yjj
cy
to
ki
ne
• Activation of of jak
• Recuritment of signal transducers and activators of transcription(STAT)
• Phosphorylation of tyrosine residue of cytoplasmic receptor
• Phosphorylation ofSTAT
p p
stat p statp
y y
After phosphorylation• The phosphorylated proteins dissociate from receptors the
bind to each other to form STAT dimer
y
yp
p
STAT dimer

finally• STAT dimer migrates to nucleus where it binds to region of
cytokine responsive genes.• Gene transcription occurs which lead to cell activation and
proliferation.
gene transcription.
Nucleus

Jak family• The JAK family consist of four types of tyrosine kinase
enzymes: JAK1, JAK2, JAK3 and TyK2. • IL-3 and IL-5 use JAK2, • IL-6, IL-10, IL-11, IL-9, IL-20, IL-22 and interferon [IFN]-γ use
JAK1 and JAK2. • IL-2, IL-4, IL-7, IL-9, IL-15 and IL-21 use JAK3 [Karaman et
al. 2008]. These cytokines are critically involved in T- and NK-cell development, B-cell function and proliferation [Kawamura et al. 1994).

Tofacitinib
• Tofacitinib (trade name Xeljanz)
• It is an inhibitor of the enzyme janus kinase 3 (JAK3), which means that it interferes with the JAK-STAT signaling pathway, which transmits extracellular information into the cell nucleus, influencing DNA transcription
• This inhibition will result in suppression of multiple cytokines involved in the disease process
• In November 2012, the U.S. Food and Drug Administration (FDA) approved tofacitinib for treatment of rheumatoid arthritis.
• However in 2013 it was not approved by European medicine agency as amonotherapy for rheumatoid arthritis.


Dose
• 5-10 mg twice daily (oral)• 1st oral biologic.• a half-life of approximately 3 h• The drug is cleared by both hepatic (70%) and renal
metabolism (30%).• According to new EULAR 2013 rheumatoid arthritis guide
lines tofacitinib recommended to be used after 2 biologic failures.

Effiacy• Tofacitinib was shown to be effective in preventing cartilage
damage in mouse and rat models of experimental arthritis.• Six RCTs evaluating TOFA in RA have been presented as abstracts or
published.[The initial three trials were dose-ranging trials evaluating TOFA as a monotherapy or in combination with MTX, with adalimumab (the placebo) as a comparator in one trial.
• Kremer et al conducted a six-week Phase IIa study that evaluated patients who either could not tolerate or did not respond to methotrexate and/or one tumor necrosis factor-alpha inhibitor.
• The patients were randomized to TOFA 5 mg twice a day, 15 mg twice a day, 30 mg twice a day, or placebo. The investigators described a rapid (within 1–2 weeks) response to the drug, with ACR20 responses of 70.5%, 81.2%, and 76.4% in the 5 mg, 15 mg, and 30 mg dose groups, as opposed to 29.2% in the placebo group.

In a Phase IIb study• Tofacitinib at various doses (20 mg once a day or 1 mg, 3 mg,
5 mg, 10 mg, and 15 mg twice daily) or placebo was added onto stable background methotrexate. patients enrolled in the study had active disease despite methotrexate at a mean dose of 16–17 mg per week.
• Treatment with 3 mg twice daily or more of tofacitinib resulted in higher response rates than for placebo starting as early as week 2 and sustained through to week 24 of treatment. In particular, the ACR20 response rate was 52.9% for the 3 mg twice-daily group compared with 33.3% for the placebo group.

In another study, Fleischmann et al • compared tofacitinib with adalimumab, in patients with
active RA.• Impressively, tofacitinib monotherapy resulted in a dose-
dependent response that was better than both adalimumab or placebo. At week 12, the ACR20 responses were between 39.2% for the 3 mg twice-daily dose and 71.9% for the 15 mg twice-daily dose. This compared with 22% for placebo and 35.9% for adalimumab.

Phase III trials• Patients who failed at least one biologic or conventional
DMARD were randomized to receive placebo or tofacitinib 5 mg twice a day (low dose) or 10 mg twice a day (high dose) for 6 months.
• Patients on the placebo arm were switched to active medication at three months.
• The primary endpoint of ACR20 was met in the study, with the two tofacitinib groups reaching ACR20 responses of 59.8% (low dose) and 65.7% (high dose) versus 26.7% for the placebo group.

In a parallel 12-month study• patients on methotrexate were assigned to the same two
doses of tofacitinib as above, adalimumab 40 mg every other week, or placebo.
• The patients on placebo who did not achieve an improvement of at least 20% by three months were switched to tofacitinib.
• At month 6, tofacitinib was found to be equivalent to adalimumab with ACR20 responses of 51.5%, 52.6%, and 47.2% for low-dose tofacitinib, high-dose tofacitinib, and adalimumab, respectively. This was in contrast with a 28.3%ACR20 response rate in the placebo group.

At the 2011 ACR annual meeting• Phase III RCT was evaluating 887 patients with RA with an
inadequate response to MTX.• The study was designed to evaluate the impact of TOFA on
radiographic progression and patients enrolled were required to have at baseline at least three erosions by x-ray or to be seropositive for rheumatoid factor or anti-citrullinated protein antibodies

• Enrolled patients had longstanding disease (mean 8.8–9.5 years) and at baseline had modified Total Sharp Score (30.1–37.3).
• At month 3 patients who were nonresponders were randomized in a blinded fashion to TOFA and at 6 months all placebo patients were randomized to TOFA.
• At month 6 the modified Total Sharp Score progressed 0.47 in the placebo group,
• 0.12 in the 5-mg TOFA patients • 0.06 in the 10-mg TOFA patients.

Tofacitinib radiographic outcome in the 12-month study of rheumatoid arthritis patients with active disease, despite methotrexate

Safety• The most common AEs were nasopharyngitis, upper
respiratory infections, urinary tract infections (UTIs), headache, and gastrointestinal complaints.
• A reduction in overall neutrophil counts similar to that seen with TNF and IL-6 inhibitors was reported. Rare (1–2%) cases of neutrophil counts below 2000 were seen but no cases of grade 4 neutropenia (<500) have been reported. No relationship between neutropenia and infection has been reported.

• Rare cases of anemia were seen in the clinical trials, possibly related to Jak2 inhibition as erythropoietin signals through this Jak. This was primarily seen in the Phase II RCTs at doses of TOFA greater than 10 mg b.i.d
• Liver function test elevations were seen more commonly with TOFA compared with the placebo groups. More frequent elevations were reported in combination with MTX than monotherapy. Rare patients had transaminase elevations of more than three-times the upper limit of normal, requiring dose modification. These elevations resolved with dose modification or drug discontinuation and no cases of hepatic failure have been reported.

• A peculiar elevation in serum creatinine levels has been reported in the RCTs. These were generally in the range of less than 30% and not associated with other signs and symptoms of renal injury
• Approximately 15% of patients in the RCTs had an increase in total cholesterol that occurred early and plateaued by 3 months. In general, both the low-density lipoprotein and high-density lipoprotein levels were elevated with no change in the ratio.
• Herpes zoster was reported more frequently in the TOFA treated patients with a rate which is higher than previously reported with other biologic therapies for RA.

• Ten cases of tuberculosis (TB) were reported .There were 20 patients with other opportunistic infections. These included esophagealcandidiasis(seven),cytomegalovirusinfection/viremia (four), Pneumocystis jiroveci pneumonia (three), non-TB mycobacterium lung infection (two) and one case each of cryptococcal pneumonia, cryptococcal meningitis, multidermatomal herpes zoster and encephalitis.
• The rate of lymphomas or other lymphoproliferative disorders in the tofacitinib RA clinical studies was 0.07 per 100 patients which is consistent with the rates of lymphoma among all RA patients and among those treated with biological DMARDs

THANK YOU




























































