spina bifida
DESCRIPTION
Human Growth Development report.TRANSCRIPT

SPINA BIFIDA
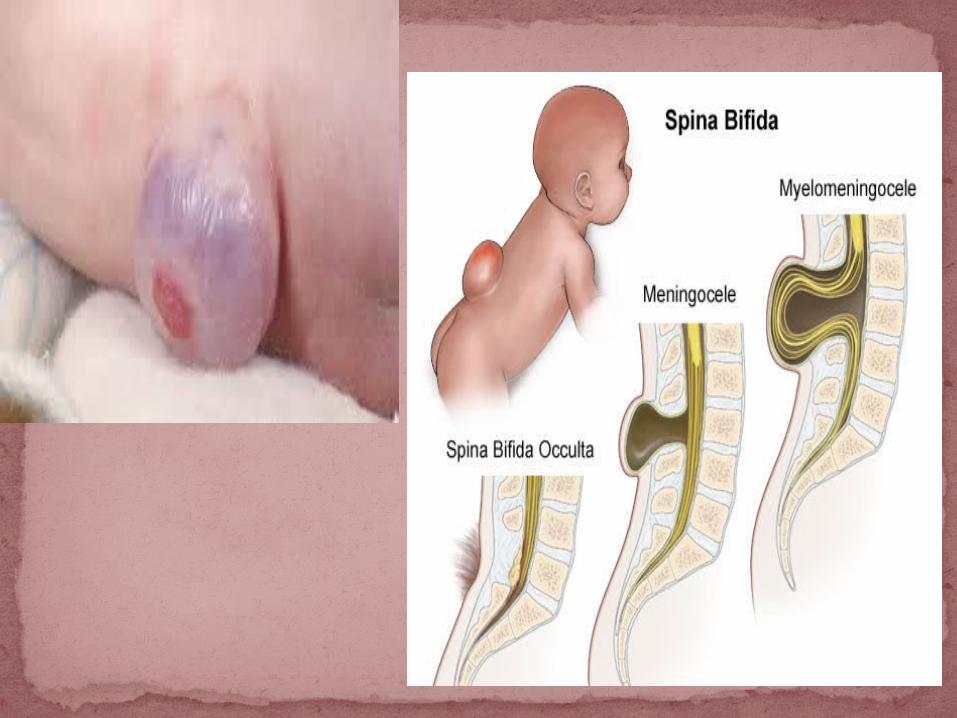
SPINA BIFIDA is a spinal defect usually diagnosed at birth by the presence of an external sac on the infant’s back.
The sac contains meninges and spinal chord tissue protruding through a dorsal defect in the vertebrae.
This defect may occur at any point along the spine but it is most commonly located in the lumbar region.

Spina BifidaThe sac covered by a transparent
membrane with neural tissue attached to its inner surface or the sac maybe open with the neural tissue exposed.
The lateral border of the sac has bony protrusions formed by the unfused neural arches of the vertebrae.
The defect maybe large, with many vertebrae involved, or it maybe small, involving only one or two segments. The size of the lesion is not by itself predictive of the child’s functional deficit.

EtiologyEtiology of spina bifida is complex; both
polygenics inheritance and environmental influences seem to contribute in a multifactorial manner.
. The malformation are attributed to
abnormal interaction of several regulating and modifying genes in nearly fetal development. The female to female prevalence ratio was 1.2 in two United States Surveillance System.

it helps to understand the anatomy of the spine and spinal cord. The back includes the spine and the structures that surround the spine.
The spine is an upright row of stacked bones, called the vertebral column. Individual bones of the spine are called vertebrae.
The vertebral column starts under the skull and continues to the buttocks.
Bones of the spine: a.)Bones of the cervical, b.) Thoracic and c.) Lumbar spine(Lower spine).
ANATOMY

Vertebral column
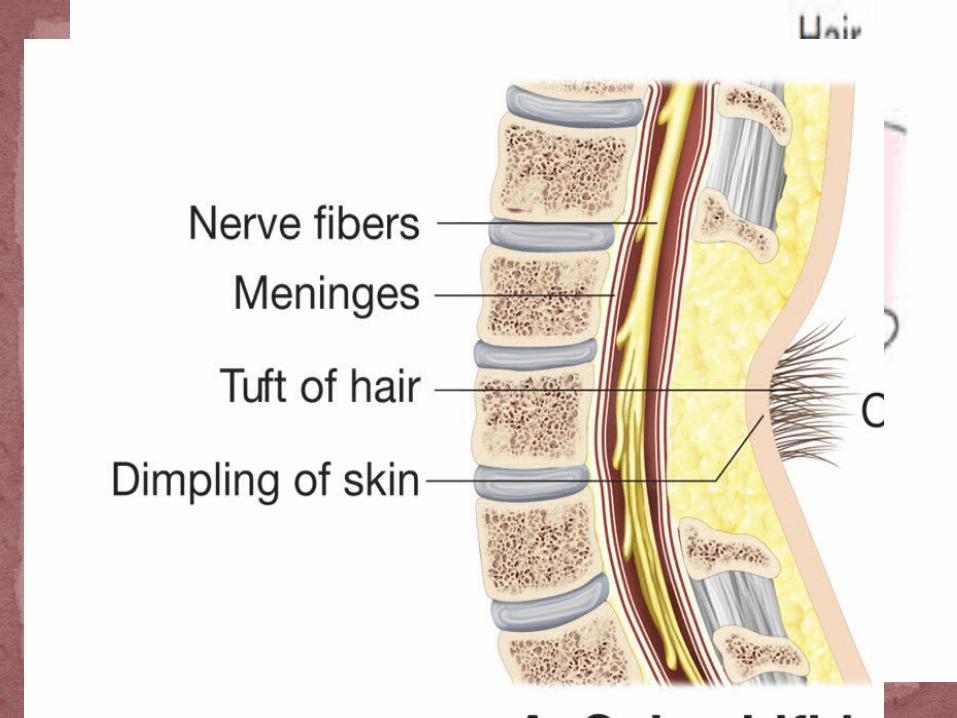
1.Spina Bifida Occulta – an abnormality is confined to the vertebrae only and is due to an unclosed posterior vertebral arch.
Approximately 40% of all Americans may have spina bifida occulta, but because they experience little or no symptoms, very few of them ever know that they have it.
Types of Spina Bifida
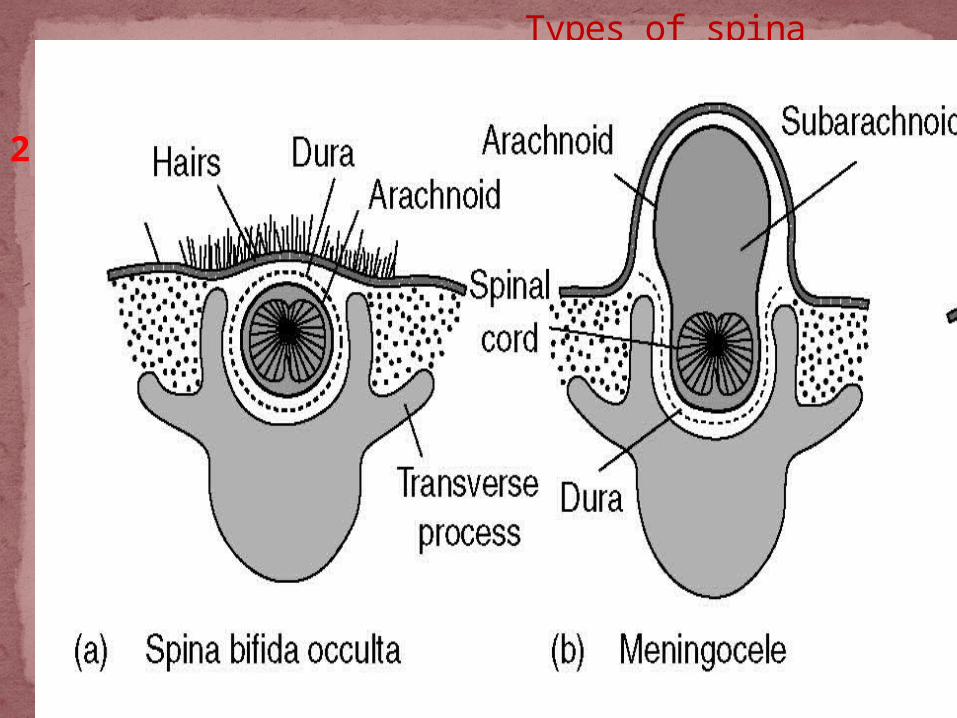
2. Meningocele-In this instance, the vertebrae are malformed, forming a passageway for the lining of the spinal cord. The spinal cord lining protrudes through the opening, forming a bulge under the skin in the back. The bulge may not contain any nerve tissue. This is the least common form of spina bifida.
Types of spina bifida

3.) Myelomeningocele-aka-meningomyelocele-is the most severe form of SB. In this type, the involved area is represented by a flattened, plate-like mass of nervous tissue with no overlying membrane.
The exposure of these nerves and tissues make the baby more prone to life-threatening infections such as meningitis or hydrocephalus.
Elements of the cord also protrude through the defect, resulting in severe neural deficits.
1 out of 1,000 births
Types of spina bifida

Race & sexMedically diagnosed obesity.Use of certain anti-seizure
medications.High temperatures in early pregnancy
(prolonged fevers). A previous pregnancy with a defect
increases the chances.
RISK FACTORS
Low preconceptional intakes of plant proteins, iron, magnesium, and niacin are associated with a 2 - 5 fold increased risk of spina bifida.
Women with diabetes are more likely to have a baby with spina bifida, compared to other females.
Folate deficiency-folic acid
RISK FACTORS

In previous generation long-term of survival of children with spina bifida was reported to range from as low as 1% without treatment to 50% with treatment.
A survival rate of more than 90% is not expected when aggressive treatment is provided to the spinal defect and its associated problems.
This chapter represents the primary problems for this population of children, including hydrocephalus, motor and sensory deficits in the lower extremities and urologic impairments as well as the secondary issues that are of clinical significance.
Prognosis

The use of antibiotics to limit infection in the open spine starting in 1947, and the surgical insertion of ventricular shunts in 1960 to limit hydrocephalus were major advances in the treatment of spina bifida.
Early and consistent use of clean, intermittent catherization to completely empty the bladder has also dramatically improved the survival rate by controlling urinary infection and the renal deterioration, both of which have been major causes of mortality.
The measure along with the practice of early back closure, continue to improve the chances of survival of children with spina bifida.

The number of severely affected children who have survived has increase. Additionally, there is an increased number of less severely involved individuals who would have not have lived with earlier, less aggressive treatment protocols.
Therefore, the full spectrum and complexity of the disability can now be appreciated. Clinicians have the opportunity, unavailable in previous eras, to work with and learn a great deal from this heterogeneous group.
As the survival rate improved, an increased awareness evolved for the associated problems that were neither evident nor priority for the treatment in the past.
Diagnosing spina bifida In the majority of cases, spina bifida is detected when the pregnant mother has a routine ultrasound scan pregnant women may be offered spina bifida and other birth defect screening tests.
The tests are not 100% accurate. MSAFP (maternal serum alpha-fetoprotein) test - this is a blood test. Blood is sent to the lab and tested for AFP (alpha-fetoprotein). AFP is a protein the fetus produces. AFP does not usually get into the mother's bloodstream, if it does it usually means the fetus has abnormally high levels and probably has a neural tube defect, which could include anencephaly (incomplete skull and underdeveloped brain) or spina bifida.
Cranial imaging using ultrasonography, CT scan, or MRI is done to look for hydrocephalus.
Diagnosis

Women of childbearing are were to consume 0.4 mg of folic acid prior to becoming pregnant and during the first trimester of pregnancy, the incidence of folic acid preventable spina bifida and anencephaly could be reduced by up to 75%.
Folic acid= a common water soluble B vitamin, is essential for the functioning of the human body.
Folic acid can be found in multivitamins, fortified breakfast cereals, dark green leafy vegetables such as broccoli and spinach, egg yolks, and some fruits and fruit juices.
With proper care, most children with SB live well into adulthood.
Prevention
A.) surgery - this is usually done to repair the spine within two days of birth. The surgeon replaces the spinal cord and any exposed tissues or nerves back into the patient's body. The gap in the vertebrae will then be closed and the spinal cord sealed with muscle and skin. If the child develops problems with bone development, such as scoliosis or dislocated joints, further corrective surgery may be needed (orthopedic surgery).
For scoliosis a back-brace may be used. Meningocele- involves surgery to put the
meninges back in place and close the opening in the vertebrae.
Myelomeningocele- also requires surgery, usually within 24 to 48 hours after birth
treatment
Hydrocephalus - surgery will be required to treat a buildup of CSF (cerebrospinal fluid) in the brain. The surgeon implants a shunt (thin tube) in the baby's brain. The shunt drains away excess fluid, usually to the abdomen. The patient will probably need a permanent shunt. Further surgery may be needed if the shunt becomes blocked or infected, or a larger one is needed as the child grows.
B.)Prenatal surgery- In this procedure which takes place before the 26th week of pregnancy surgeons expose a pregnant mother's uterus surgically, open the uterus and repair the baby's spinal cord.
C.)Ongoing care- Treatment doesn't end with the initial surgery, though. In babies with myelomeningocele, irreparable nerve damage has already occurred and ongoing care from a multidisciplinary team of surgeons, physicians and therapists is usually needed. Babies with myelomeningocele may need further operations for a variety of complications. Paralysis and bladder and bowel problems often remain, and treatment for these conditions typically begins soon after birth.
D.)Physical therapy (UK: physiotherapy)- this is a vital part of the child's treatment, which will help him/her become as independent as possible, as well as preventing the lower limb muscles from weakening. Special leg braces may help keep the muscles strong.
E.)Occupational therapy - the aim here is to help the child perform everyday activities more effectively, such as getting dressed. Occupational therapy helps with self-esteem and independence.
treatment
F.)Assistive technologies - a patient with total paralysis of the legs will need a wheelchair. Although electric wheelchairs are more convenient, manual ones help maintain upper-body strength and general fitness. Those with partial paralysis may need leg braces. Computers and specialized software may help children with learning problems.
treatment

G.)Urinary incontinence - the patient will probably be referred to a urologist for assessment. The child may be taught to use CIC (clean intermittent catherterization), a technique to empty the bladder at regular intervals in which the child and/or parent place the catheter through the urethra and into the bladder to empty it.
The child may be prescribed antimuscarinics, medications used for urinary incontinence in adults - these medications increase the amount of urine the bladder can hold, thus reducing the number of times the child has to pee.

If the child's bladder contracts abnormally (hyper-reflexic bladder), the doctor may recommend a botulinum toxin injection, which paralyzes the muscles. If it works, the patient will need repeat treatment every six months.
Artificial urinary sphincter (AUS) - this is surgically implanted. It has a silicone cuff, surrounded by a liquid, a pump and a balloon. It is attached to the urethra and the balloon is placed in the abdomen. The pump is placed under the skin of the scrotum in males and under the skin of the labia in females. When the child wants to pee they press the pump, which temporarily empties the fluid from the cuff into the balloon, releasing the pressure on the cuff and opening the urethra, allowing urine to be released.
H.)Bowel incontinence - this may involve having to go on special diets and some toilet training techniques. A healthy-balanced diet with plenty of fiber is essential to avoid constipation However; the patient must not go to the other extreme and end up with diarrhea. A food diary will help the parent and/or child know which foods are best for him/her.
Anal plugs can prevent soiling. They are made of foam and inserted into the anus. As soon as it gets wet it expands, thus blocking the passage of any feces and liquid. Anal plugs work for about 12 hours; they can be taken out by pulling an attached string.
A colostomy involves diverting a section of the colon so that it connects to a stoma, which is attached to a pouch. The pouch collects stools. If the diversion is at the end of the small intestine the procedure is called an ileostomy.
Teaching gross motor and spatial skills to facilitate coordination.
Developing and maintaining fitness and flexibility to emphasize self sufficiency.
Encouraging movement and fitness to overcome susceptibility to obesity.
Developing physical skills that generalize to activities of daily living and vocational skills.
Promoting social development in recreational and group play activities, such as aquatics.
Providing appropriate social outlets for enjoyment and self satisfaction on an individual basis as well as with family or peers within the community.
Goals of Intervention
The range of problems requires a multidisciplinary treatment team. Specific concerns of comprehensive functional rehabilitation are prevention of deformities.
There's good reason to hope, however, because most people with spina bifida live active, productive and full lives - especially with encouragement and support from loved ones.
most children can walk for at least short distances, usually with the assistance of braces, canes or crutches, although they may require wheelchairs for longer distances. Using these devices can help a child compensate for his or her condition and gain more independence.
Conclusion

Presented by: Ann Dimco Noime Joy, Javerle

PEDIATRIC REHABILITATION. 3rd edition book by Gabriells E. Molnar,MD & Michael A Alexander,MD
PEDIATRIC PHYSICAL THERAPY . 4rth edition by Jan S Tecklin.
http://www.mayoclinic.org/diseases-conditions/spina-bifida/basics/risk-factors/con-20035356
http://www.medicalnewstoday.com/articles/220424.php
Google.comhttp://www.merckmanuals.com/professional/
pediatrics/congenital_neurologic_anomalies/spina_bifida.html#v1098579
References