post operative ultrasound evaluation of the neck in thyroid cancer patients stephen d. chapman, d.o....
TRANSCRIPT
Post operative ultrasound evaluation of the neck in Thyroid cancer patients
Stephen D. Chapman, D.O.
Lansing Radiology Associates, P.C.
Well differentiated thyroid cancer
Thyroid cancer is the most common endocrine cancer
Papillary and follicular types are classified as well-differentiated thyroid arising from thyroid follicular cells.
Account for approximately 80% to 90% of all thyroid cancers.
Well differentiated thyroid cancer
Sonography can detect recurrent disease as small as 2 to 3 mm; before they become palpable and visualized with other imaging modalities or before laboratory values become abnormal

Lymph node anatomy
Normal lymph nodes are composed of a cortex and a medulla covered by a fibrous capsule
Each lymph node contains a main artery that enters at the hilus and branches into multiple arterioles.
Cortex contains tightly packed lymphocytes and is hypoechoic.
Medulla is made of trabeculae and medullary cords and sinuses and is echogenic
Lymph node anatomy
Normal cervical lymph nodes are typically oblong, oval, cigar, or kidney bean shaped.
Reported size criteria are variable; normal nodes have a short- to long-axis ratio of less than 0.5.
The presence of an echogenic hilus is a strong predictor of a benign node
Lymph node anatomy
Small nodes, less than 5 mm, often appear to be avascular.
Flow within the larger submandibular and upper cervical lymph nodes may be increased.
Peripheral vascularity should not be seen in normal lymph nodes.
Lymph node anatomy
Multiple characteristics should be visualized to confirm benignity.
A sole benign criterion is not sufficient for an accurate diagnosis.

Well differentiated thyroid cancer
When recurrent disease is present, the lymph node will lose its ovoid, elliptical shape and become more rounded.
Lymph nodes that are increasing in size on serial sonograms should be concerning for metastases.
Well differentiated thyroid cancer
In addition to a lack of a fatty hilum, malignant lymph nodes typically are hypoechoic when compared with the surrounding tissues. This is the case with medullary thyroid cancer and lymphoma.
With recurrent papillary thyroid cancer, however, the lymph node is commonly hyperechoic. This hyperechoic appearance is likely due to the presence of thyroglobulin within the lymph node.
Peripheral or mixed (peripheral and hilar) flow has been shown to be highly suggestive of malignancy.
Well differentiated thyroid cancer
Calcifications are typically small (microcalcifications) and peripherally located.
Shadowing from the calcification may or may not be visualized.
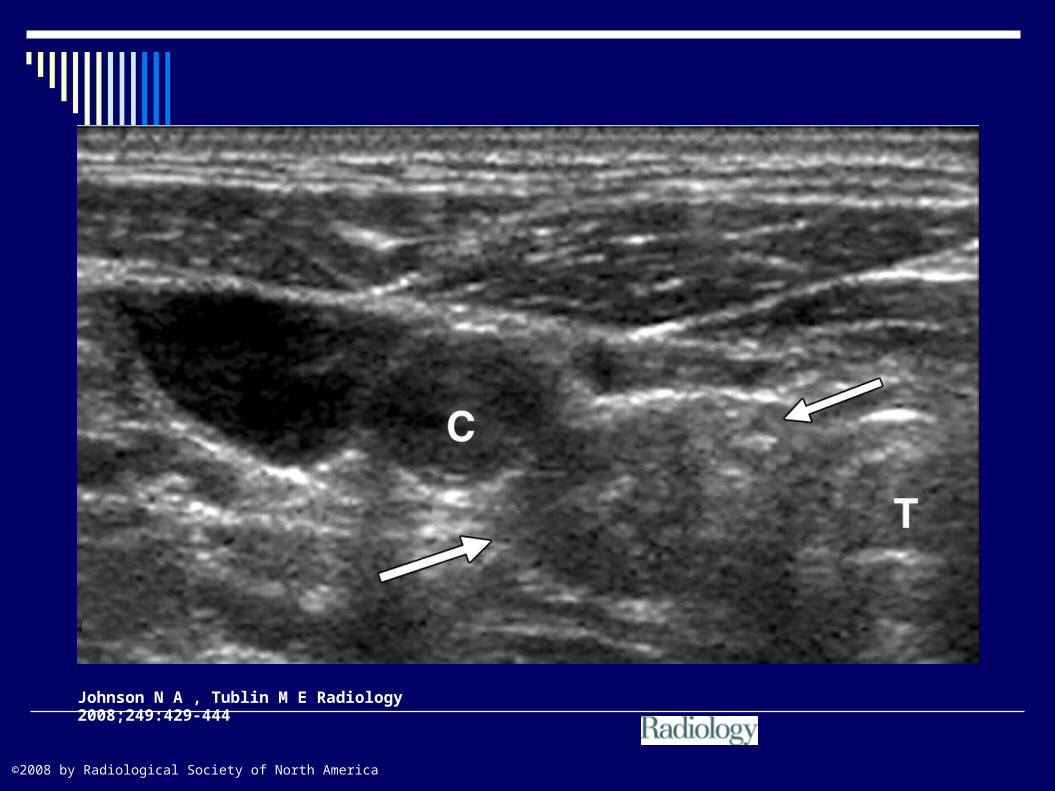
When the cervical lymph node becomes cystic, it is highly suggestive of recurrent papillary thyroid cancer
The cystic change is caused by necrosis secondary to tumor invasion.
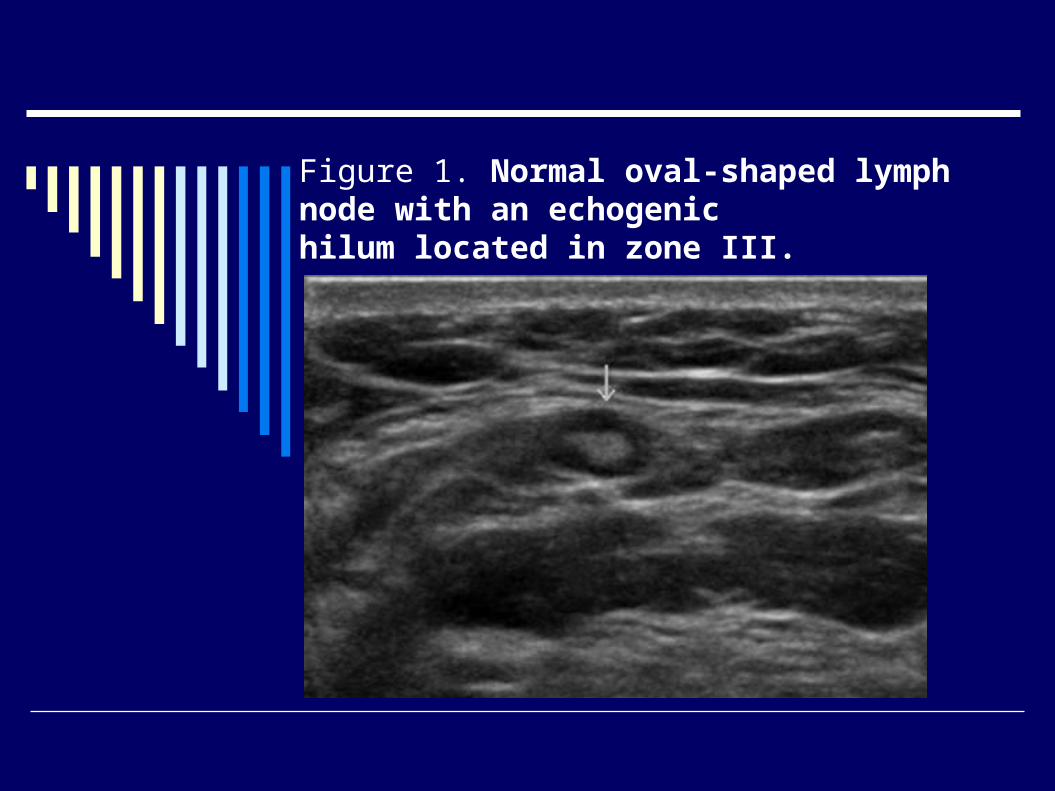
Figure 1. Normal oval-shaped lymph node with an echogenichilum located in zone III.
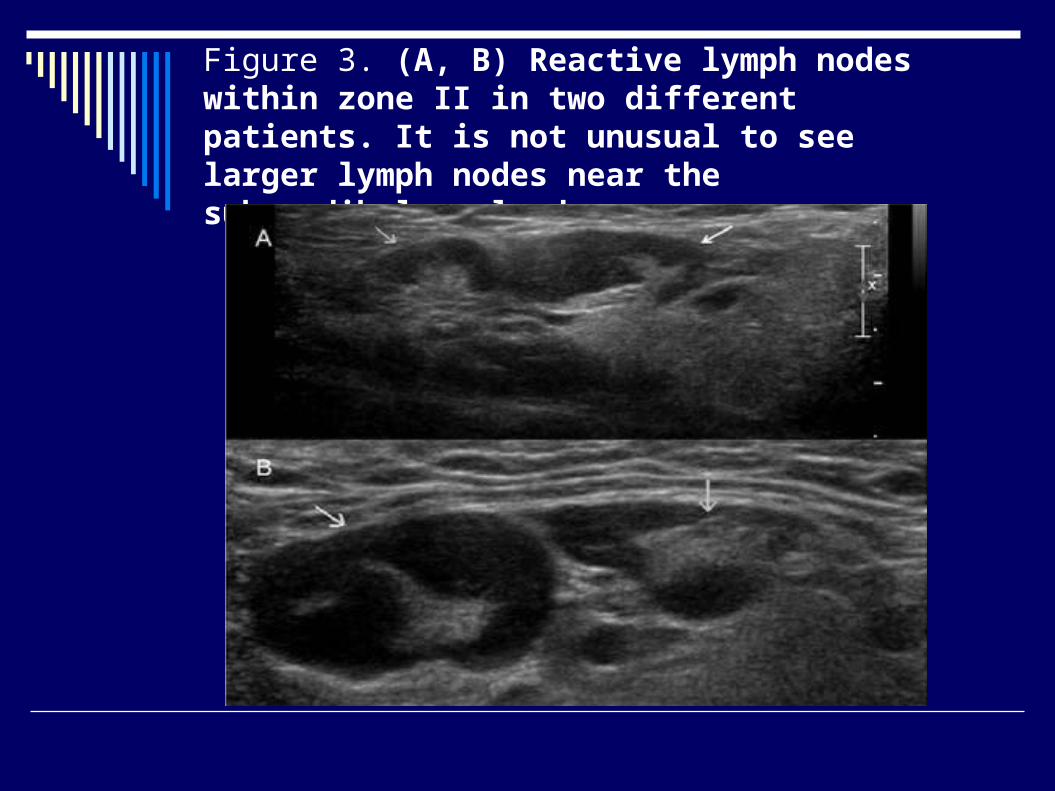
Figure 3. (A, B) Reactive lymph nodes within zone II in two different patients. It is not unusual to see larger lymph nodes near the submandibular gland.
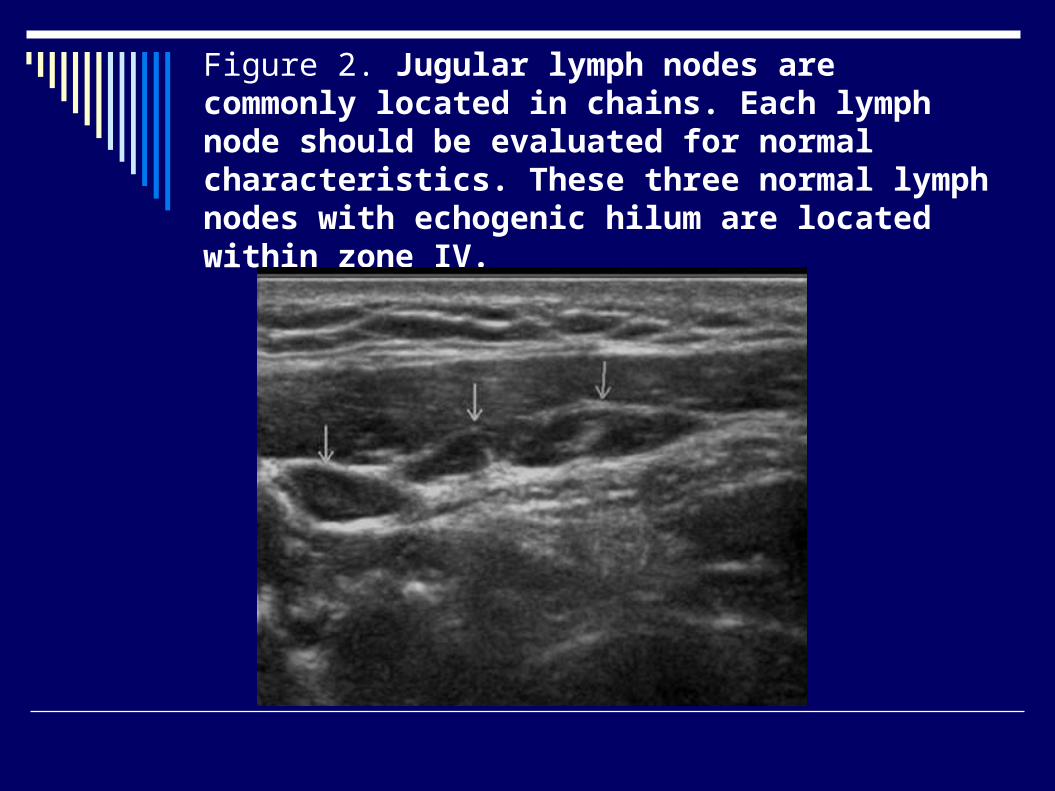
Figure 2. Jugular lymph nodes are commonly located in chains. Each lymph node should be evaluated for normal characteristics. These three normal lymph nodes with echogenic hilum are located within zone IV.
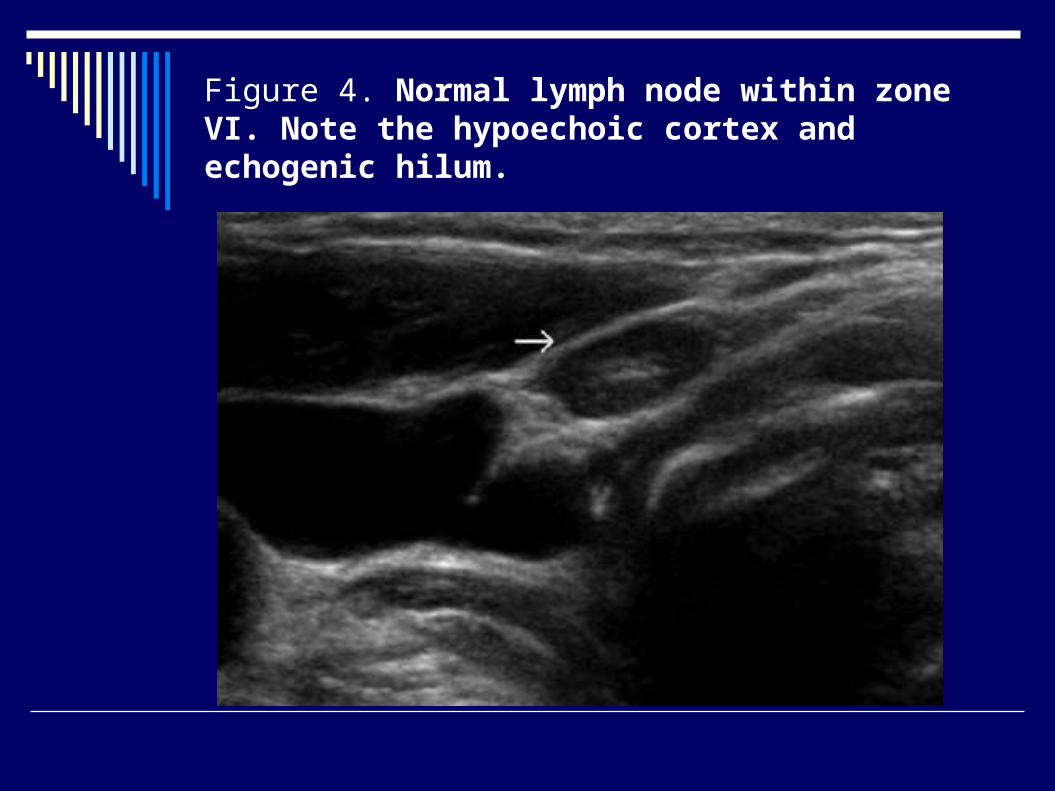
Figure 4. Normal lymph node within zone VI. Note the hypoechoic cortex and echogenic hilum.
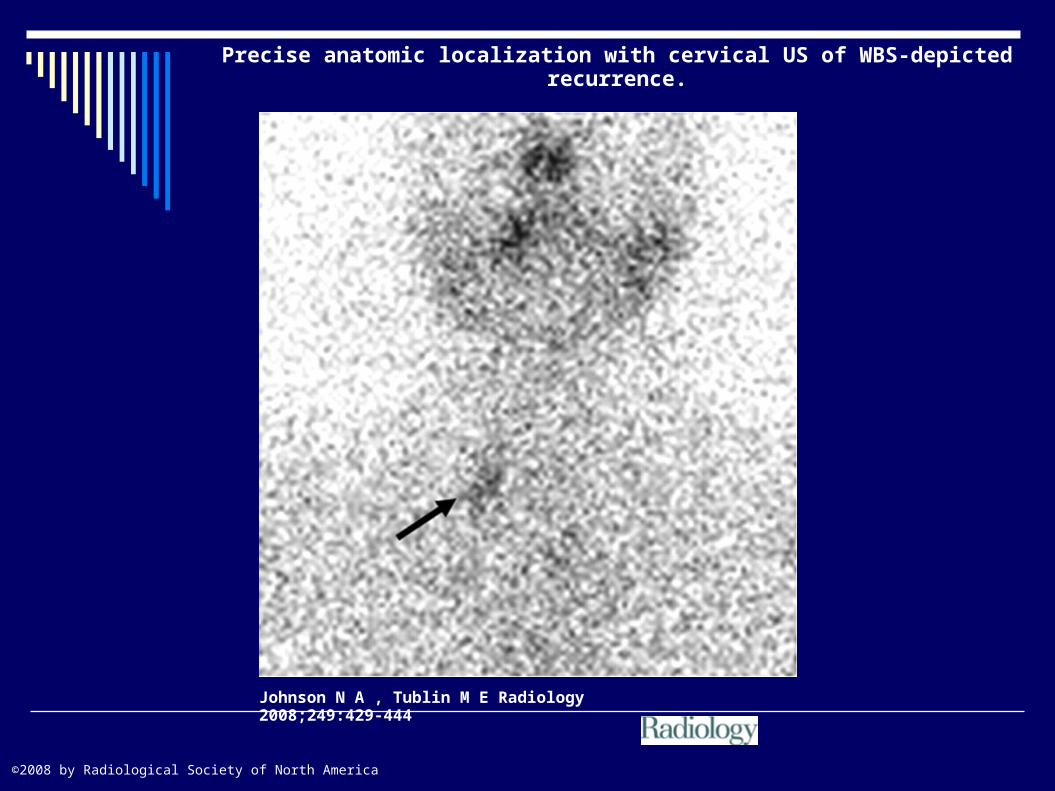
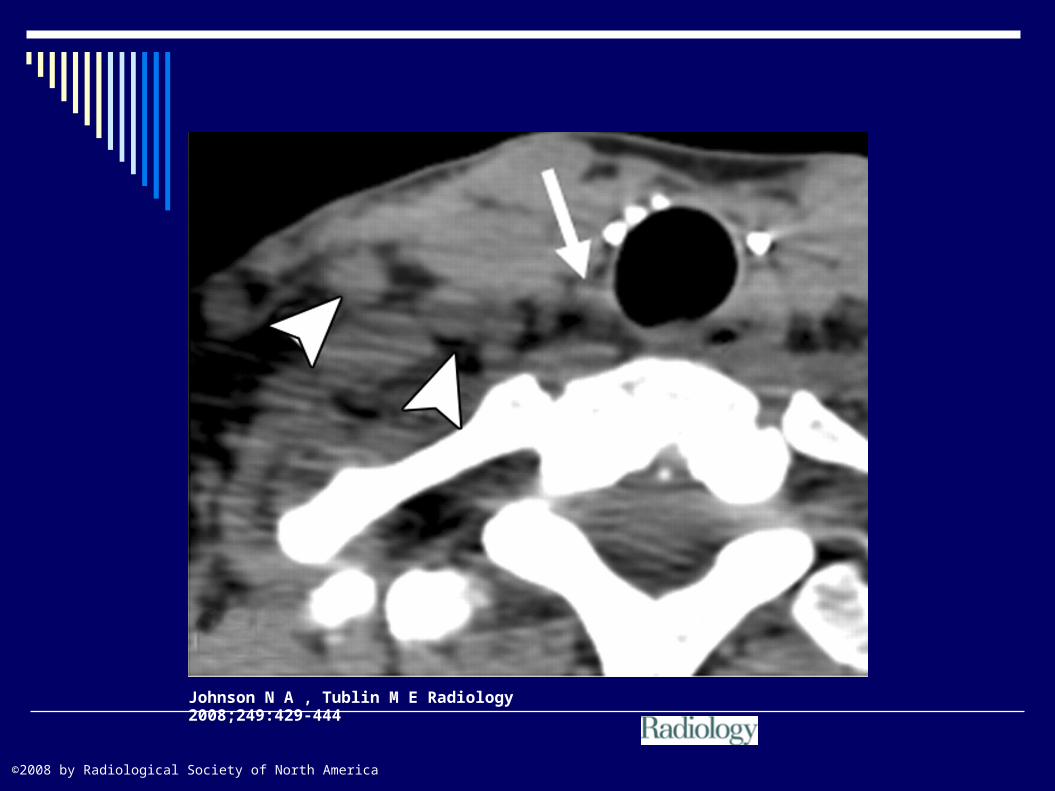
Precise anatomic localization with cervical US of WBS-depicted recurrence.
Johnson N A , Tublin M E Radiology 2008;249:429-444
©2008 by Radiological Society of North America
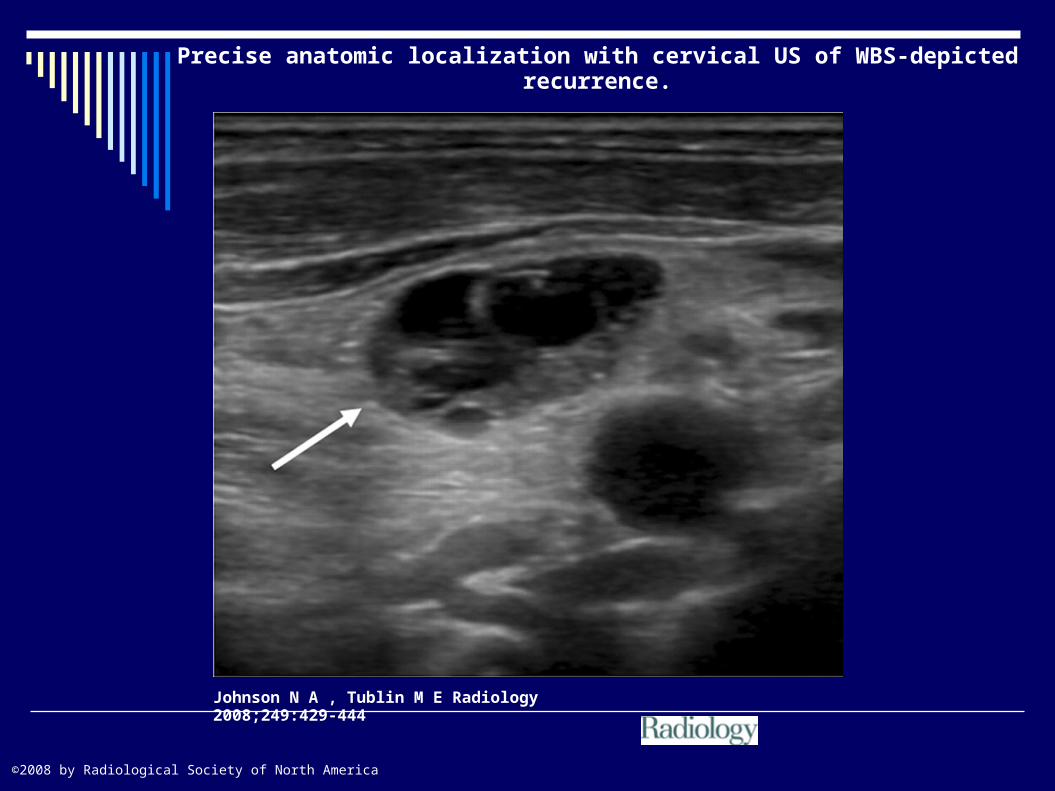
Precise anatomic localization with cervical US of WBS-depicted recurrence.
Johnson N A , Tublin M E Radiology 2008;249:429-444
©2008 by Radiological Society of North America
Technique
The patient is positioned supine with the neck hyperextended.
Typically, a 10 to12-MHz or higher linear array transducer is used.
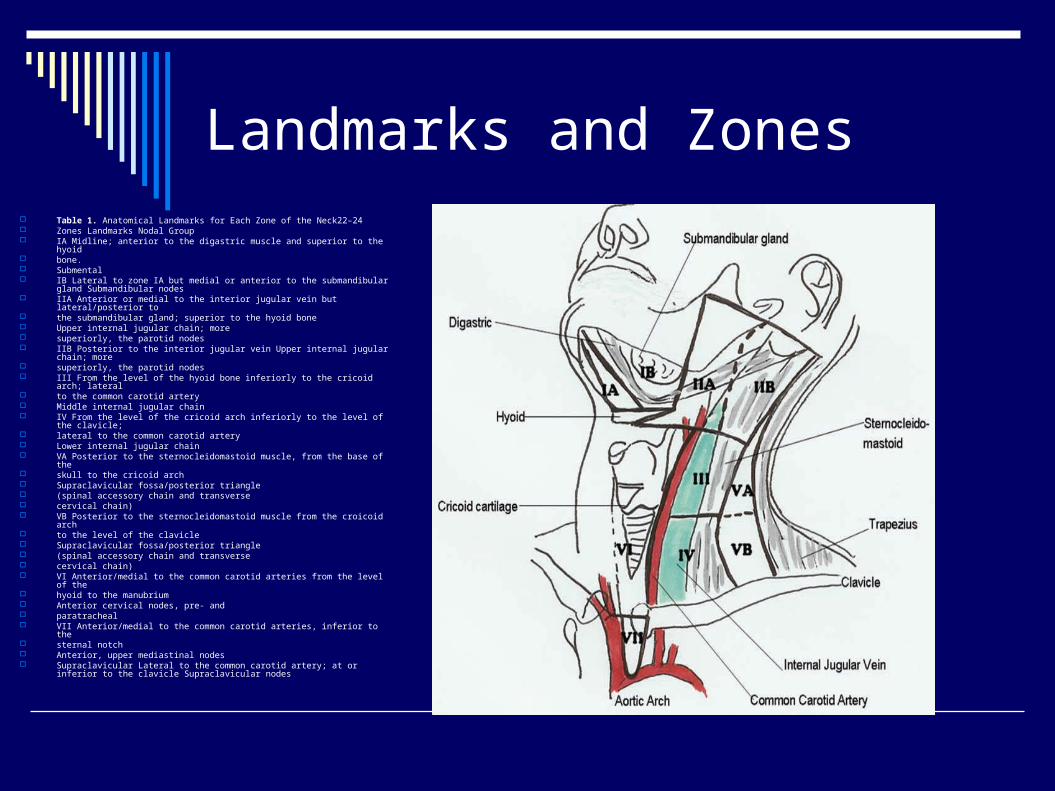
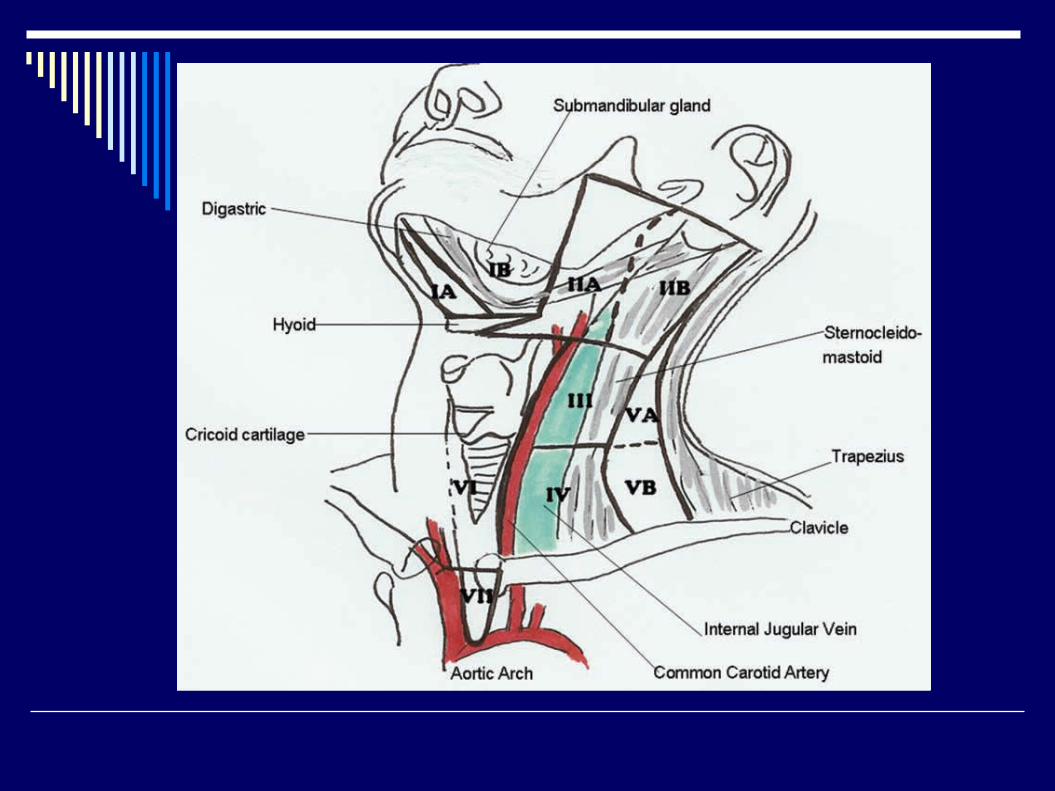
Landmarks and Zones Table 1. Anatomical Landmarks for Each Zone of the Neck22–24 Zones Landmarks Nodal Group IA Midline; anterior to the digastric muscle and superior to the hyoid bone. Submental IB Lateral to zone IA but medial or anterior to the submandibular gland
Submandibular nodes IIA Anterior or medial to the interior jugular vein but lateral/posterior to the submandibular gland; superior to the hyoid bone Upper internal jugular chain; more superiorly, the parotid nodes IIB Posterior to the interior jugular vein Upper internal jugular chain; more superiorly, the parotid nodes III From the level of the hyoid bone inferiorly to the cricoid arch; lateral to the common carotid artery Middle internal jugular chain IV From the level of the cricoid arch inferiorly to the level of the clavicle; lateral to the common carotid artery Lower internal jugular chain VA Posterior to the sternocleidomastoid muscle, from the base of the skull to the cricoid arch Supraclavicular fossa/posterior triangle (spinal accessory chain and transverse cervical chain) VB Posterior to the sternocleidomastoid muscle from the croicoid arch to the level of the clavicle Supraclavicular fossa/posterior triangle (spinal accessory chain and transverse cervical chain) VI Anterior/medial to the common carotid arteries from the level of the hyoid to the manubrium Anterior cervical nodes, pre- and paratracheal VII Anterior/medial to the common carotid arteries, inferior to the sternal notch Anterior, upper mediastinal nodes Supraclavicular Lateral to the common carotid artery; at or inferior to the clavicle
Supraclavicular nodes

Standardized neck imaging classification scheme for reporting findings in lymph nodes is critical for effective communication with
referring clinicians and surgeons.
Johnson N A , Tublin M E Radiology 2008;249:429-444
©2008 by Radiological Society of North America
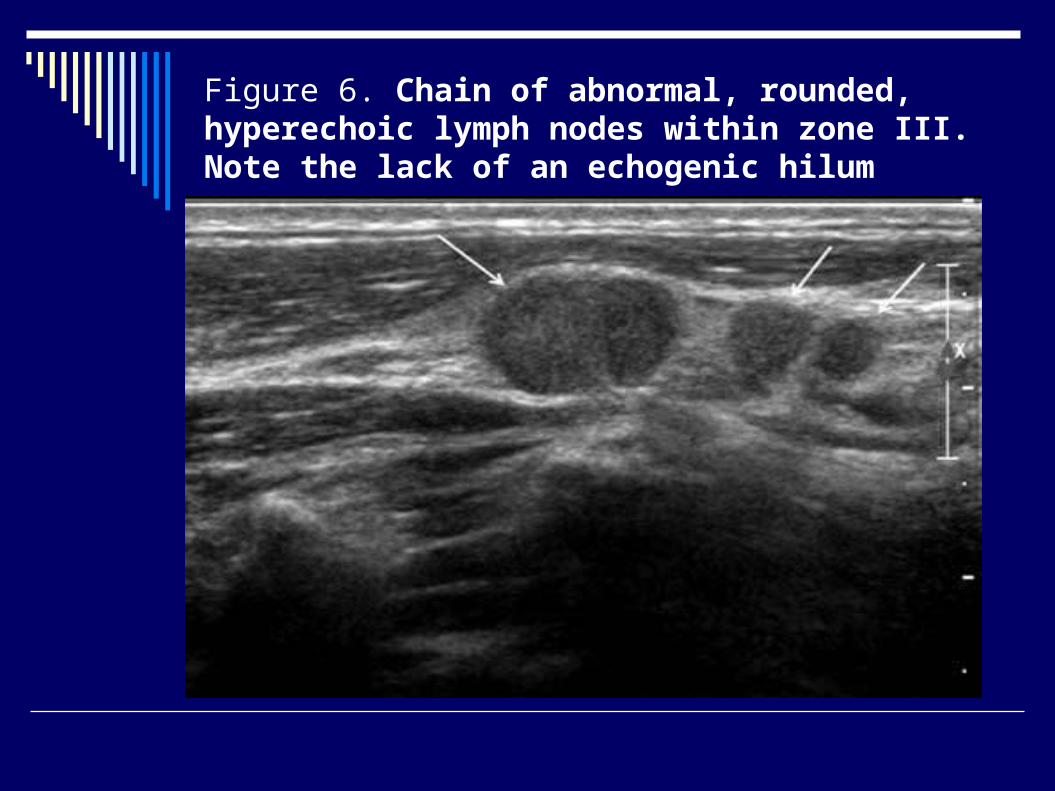
Figure 6. Chain of abnormal, rounded, hyperechoic lymph nodes within zone III. Note the lack of an echogenic hilum
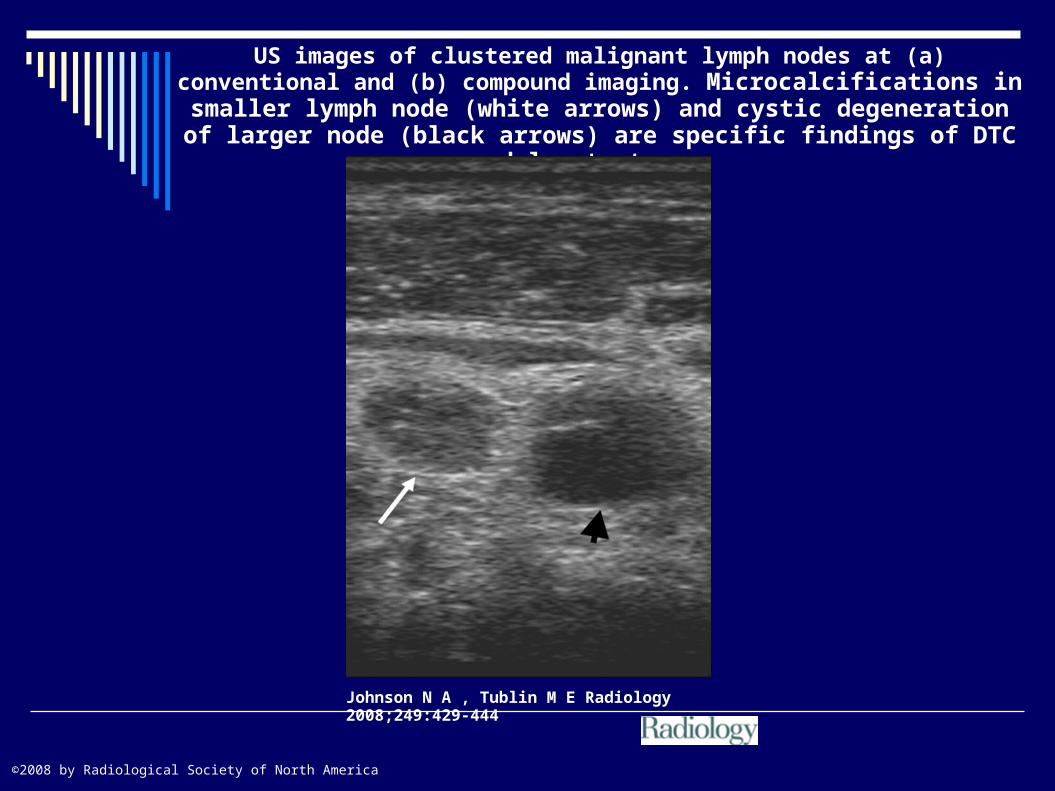
US images of clustered malignant lymph nodes at (a) conventional and (b) compound imaging. Microcalcifications in smaller lymph node (white
arrows) and cystic degeneration of larger node (black arrows) are specific findings of DTC nodal metastases.
Johnson N A , Tublin M E Radiology 2008;249:429-444
©2008 by Radiological Society of North America
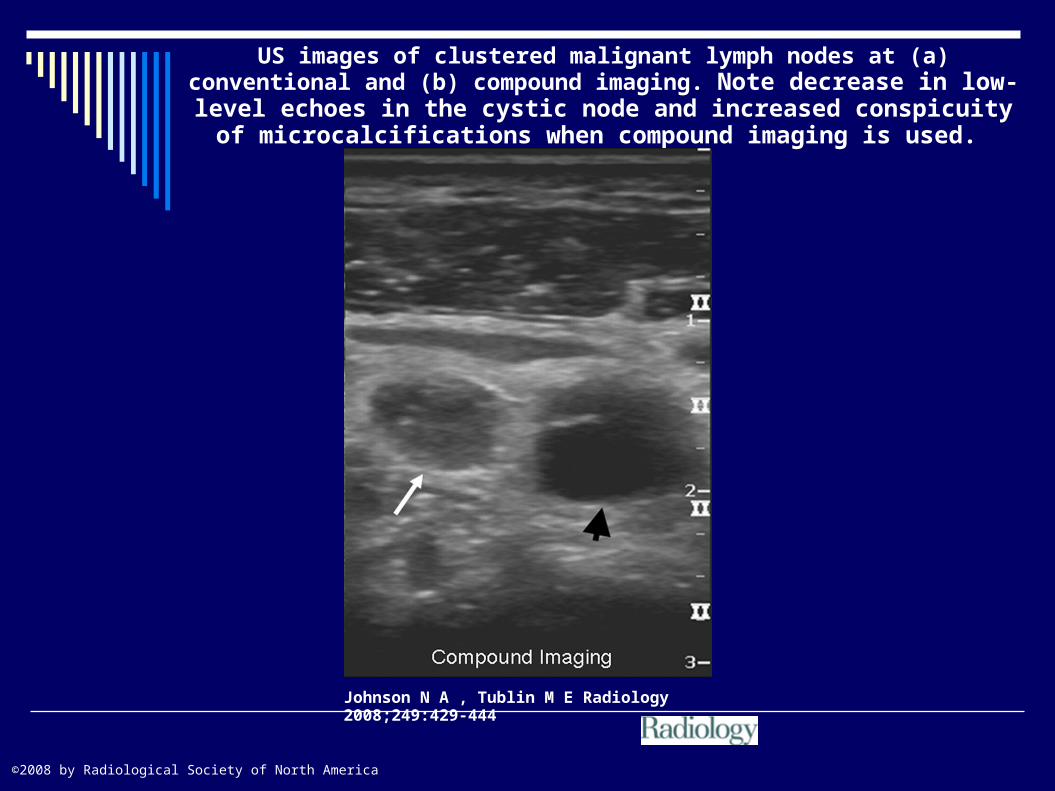
US images of clustered malignant lymph nodes at (a) conventional and (b) compound imaging. Note decrease in low-level echoes in the cystic node
and increased conspicuity of microcalcifications when compound imaging is used.
Johnson N A , Tublin M E Radiology 2008;249:429-444
©2008 by Radiological Society of North America
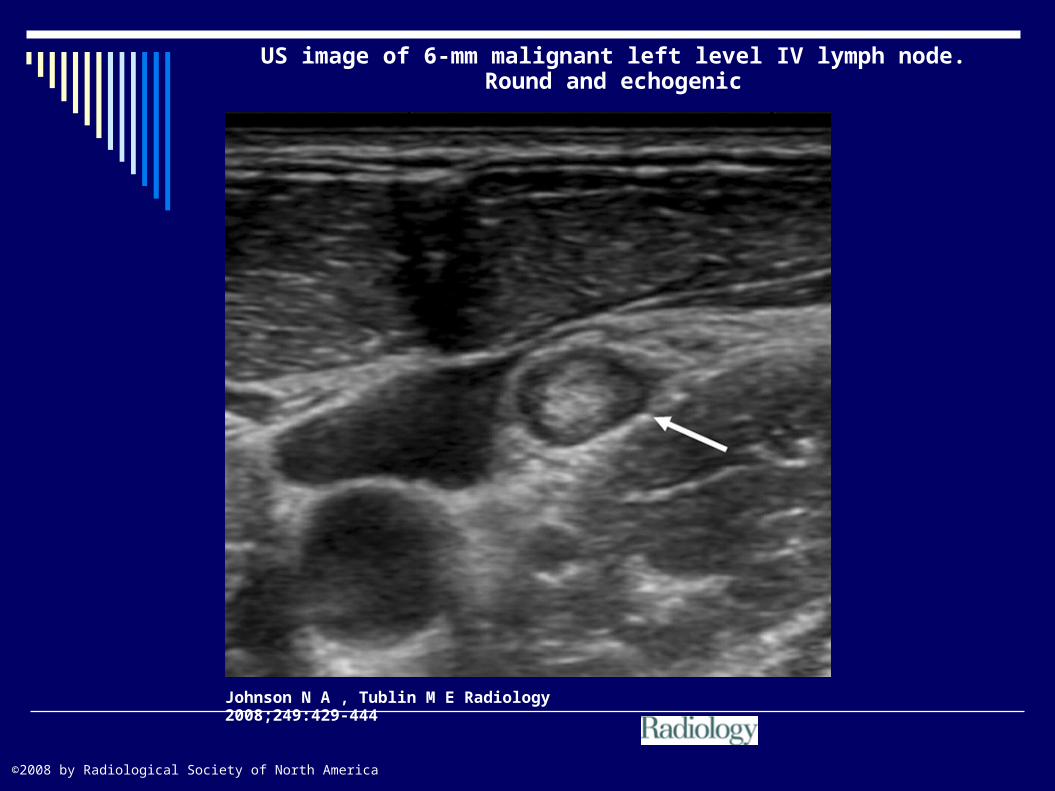
US image of 6-mm malignant left level IV lymph node.Round and echogenic
Johnson N A , Tublin M E Radiology 2008;249:429-444
©2008 by Radiological Society of North America
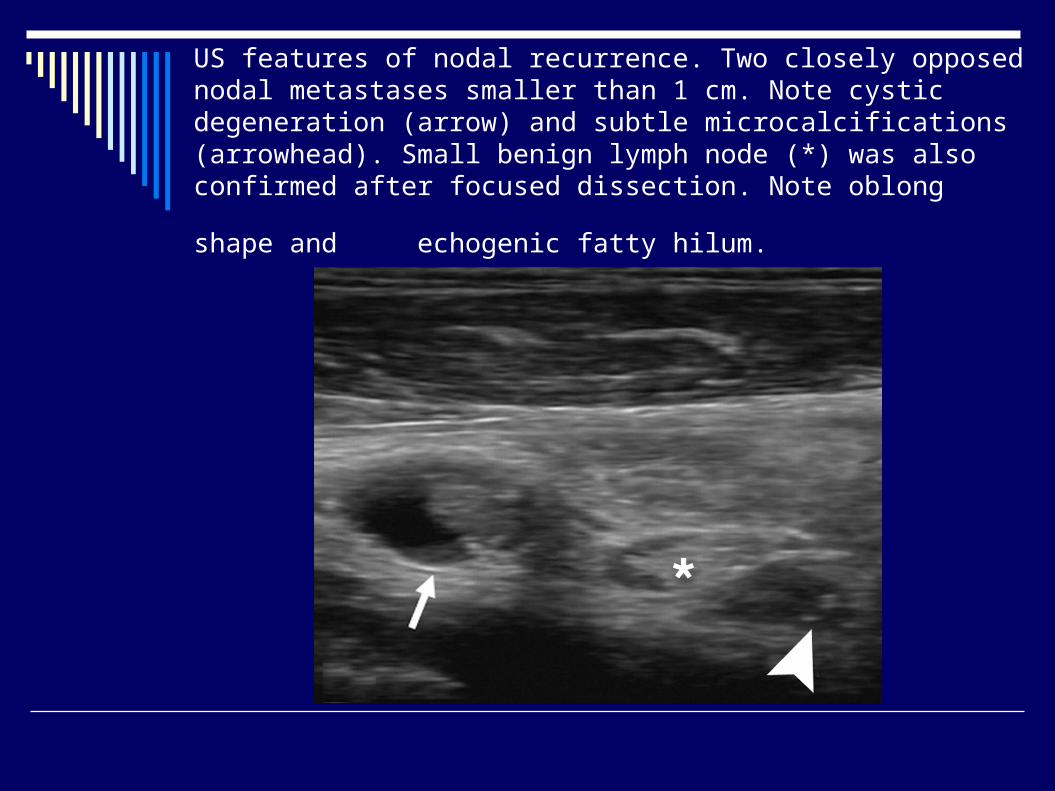
US features of nodal recurrence. Two closely opposed nodal metastases smaller than 1 cm. Note cystic degeneration (arrow) and subtle microcalcifications (arrowhead). Small benign lymph node (*) was also confirmed after focused dissection. Note oblong shape and
echogenic fatty hilum.
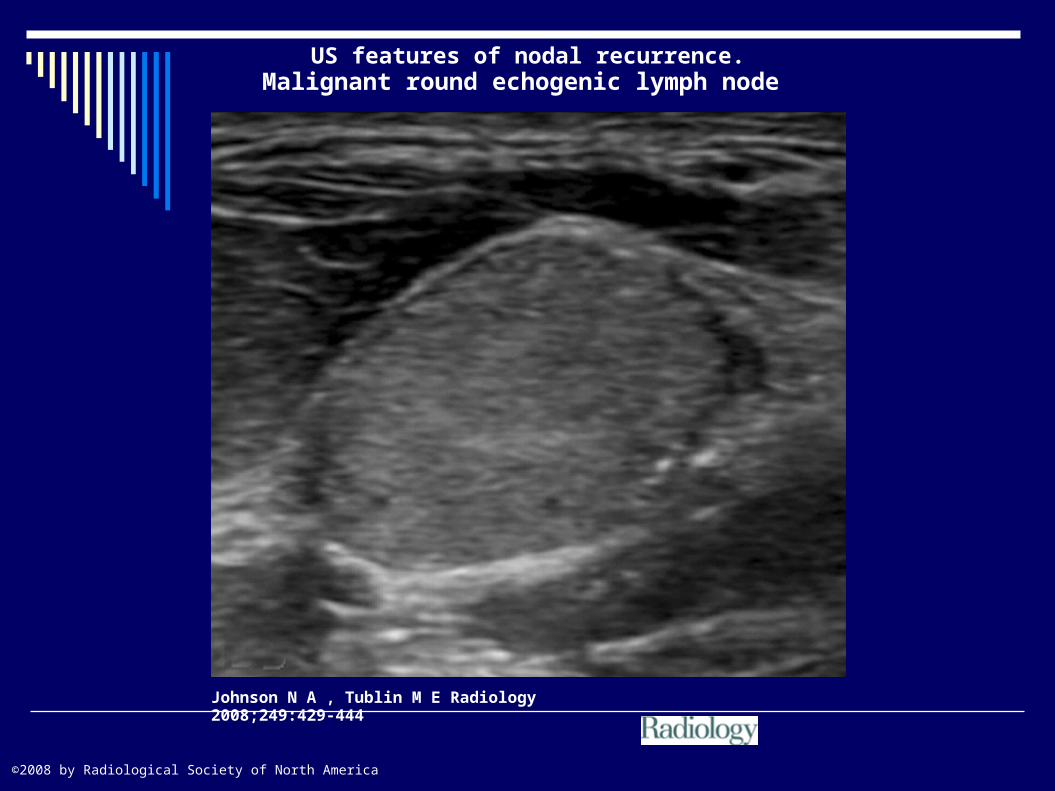
US features of nodal recurrence.Malignant round echogenic lymph node
Johnson N A , Tublin M E Radiology 2008;249:429-444
©2008 by Radiological Society of North America
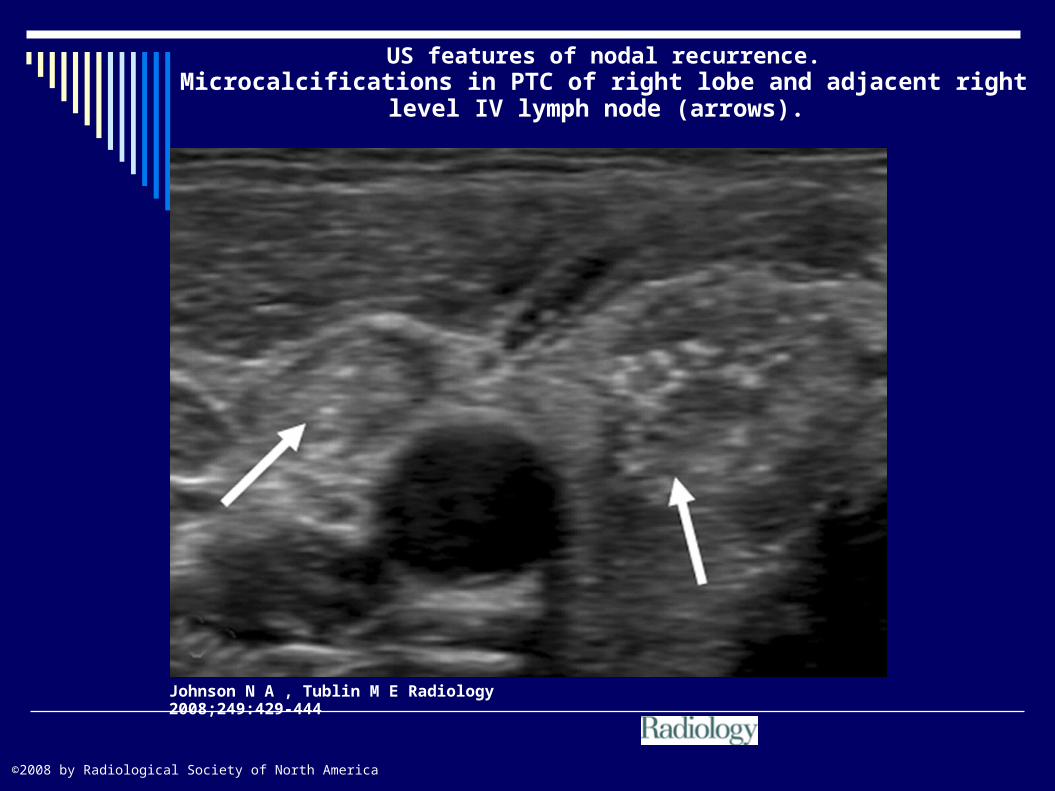
US features of nodal recurrence.Microcalcifications in PTC of right lobe and adjacent right level IV lymph
node (arrows).
Johnson N A , Tublin M E Radiology 2008;249:429-444
©2008 by Radiological Society of North America

US features of nodal recurrence. Cystic degeneration. Thick septations and nodular solid components are typical of DTC recurrence.
Johnson N A , Tublin M E Radiology 2008;249:429-444
©2008 by Radiological Society of North America

Figure 8. Multiple examples of abnormal lymph nodesshowing microcalcifications. (A) Complex lymph node thatis recurrent papillary carcinoma by biopsy. (B) Hypoechoiclymph node with microcalcifications that was biopsy-provenrecurrent medullary carcinoma. (C) Hyperechoic lymphnode with microcalcifications. This lymph node was recurrentpapillary carcinoma.
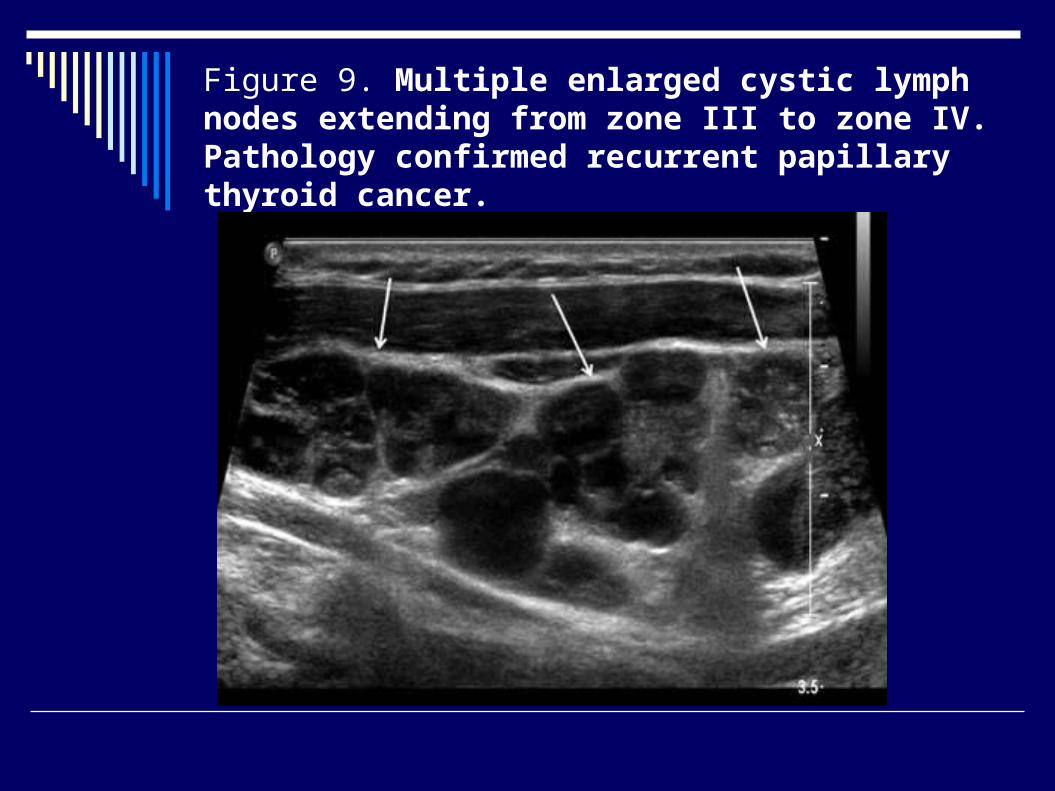
Figure 9. Multiple enlarged cystic lymph nodes extending from zone III to zone IV. Pathology confirmed recurrent papillary thyroid cancer.
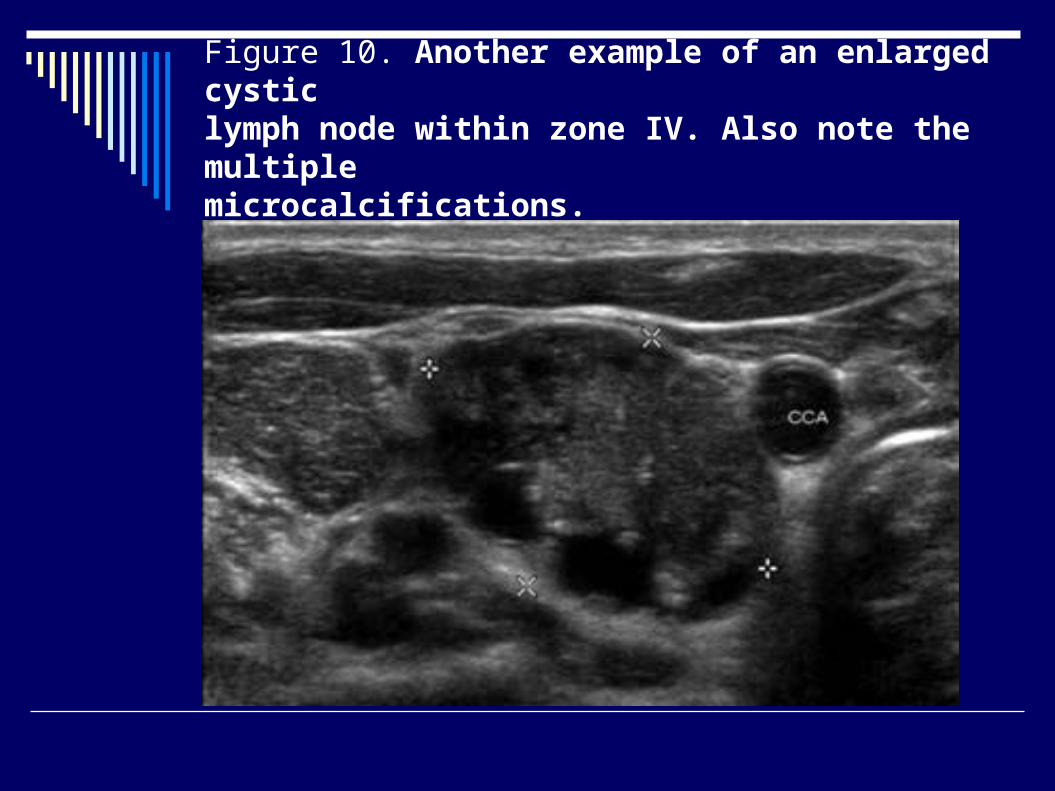
Figure 10. Another example of an enlarged cysticlymph node within zone IV. Also note the multiplemicrocalcifications.
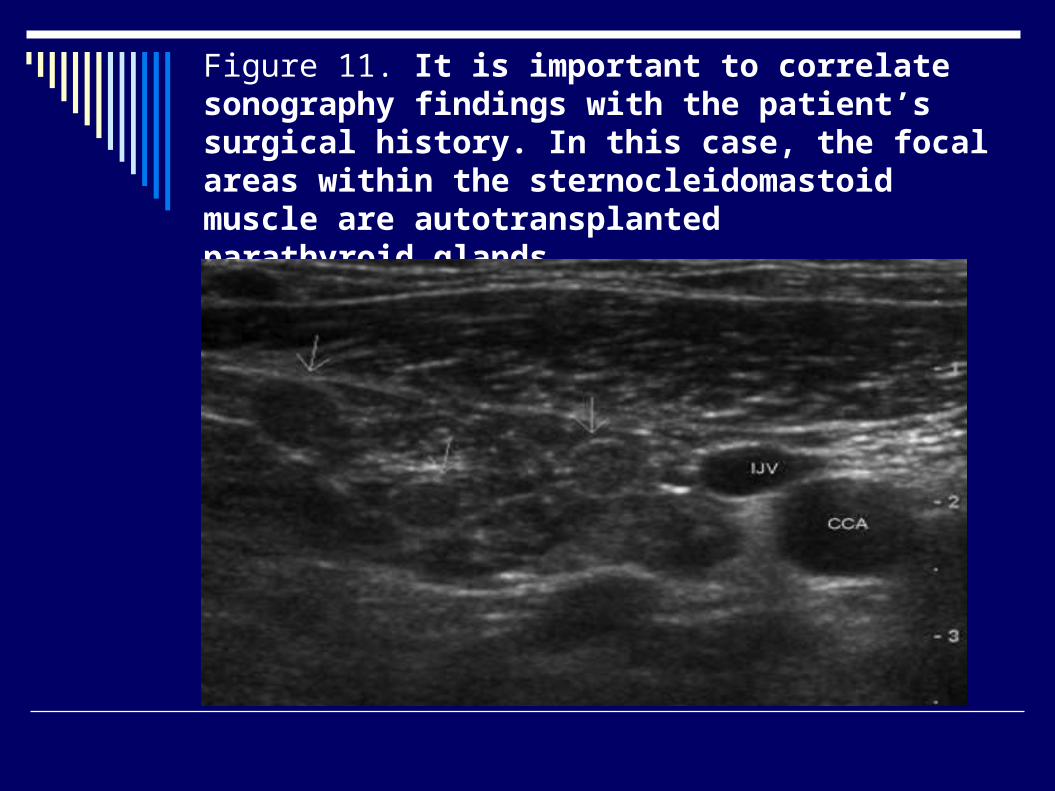
Figure 11. It is important to correlate sonography findings with the patient’s surgical history. In this case, the focal areas within the sternocleidomastoid muscle are autotransplantedparathyroid glands.

Figure 5. Normal hilar flow within a cervical lymph node.
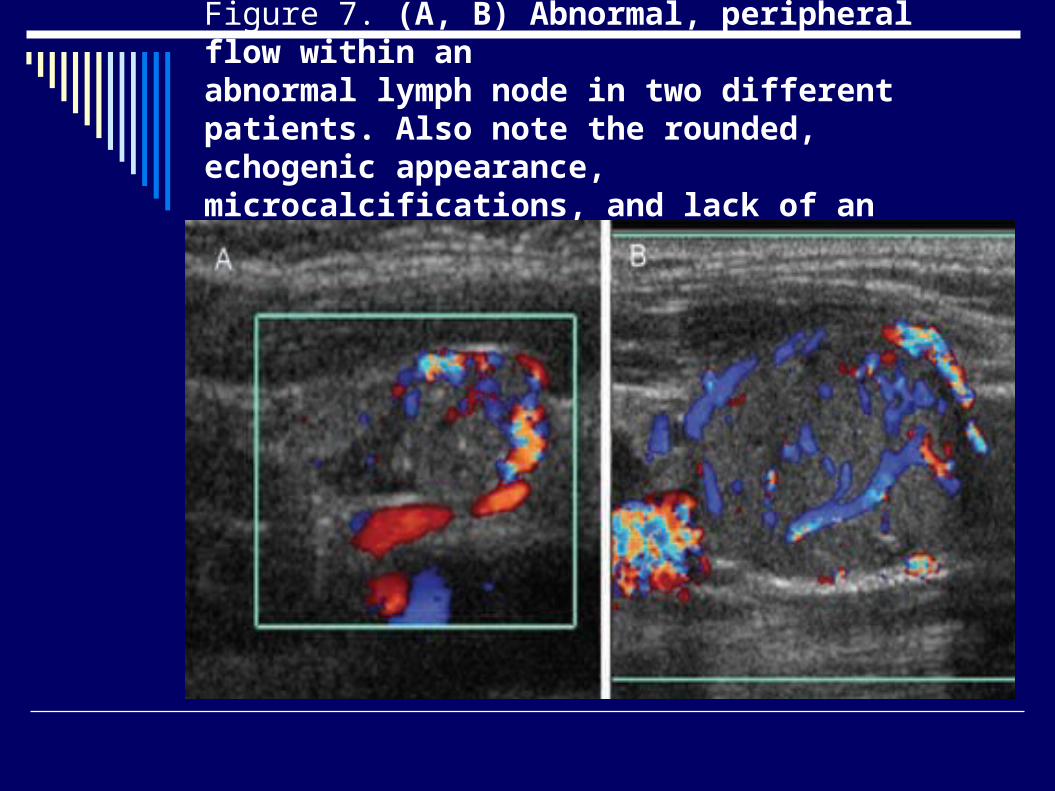
Figure 7. (A, B) Abnormal, peripheral flow within anabnormal lymph node in two different patients. Also note the rounded, echogenic appearance, microcalcifications, and lack of an echogenic hilum.
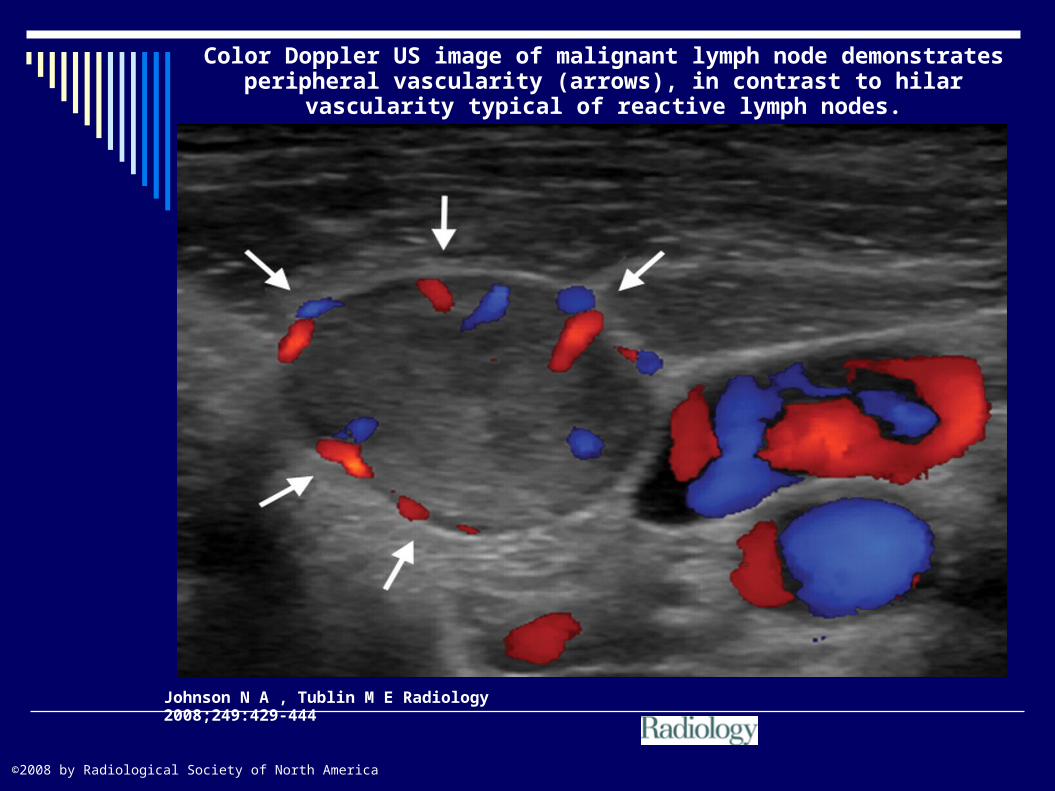
Color Doppler US image of malignant lymph node demonstrates peripheral vascularity (arrows), in contrast to hilar vascularity typical of reactive lymph
nodes.
Johnson N A , Tublin M E Radiology 2008;249:429-444
©2008 by Radiological Society of North America

Well differentiated thyroid cancer
Zone VI masses can include postoperative scarring, muscle, necrosing fat, suture granulomas, parathyroid glands, lymph nodes, remnant tissue, and metastasis
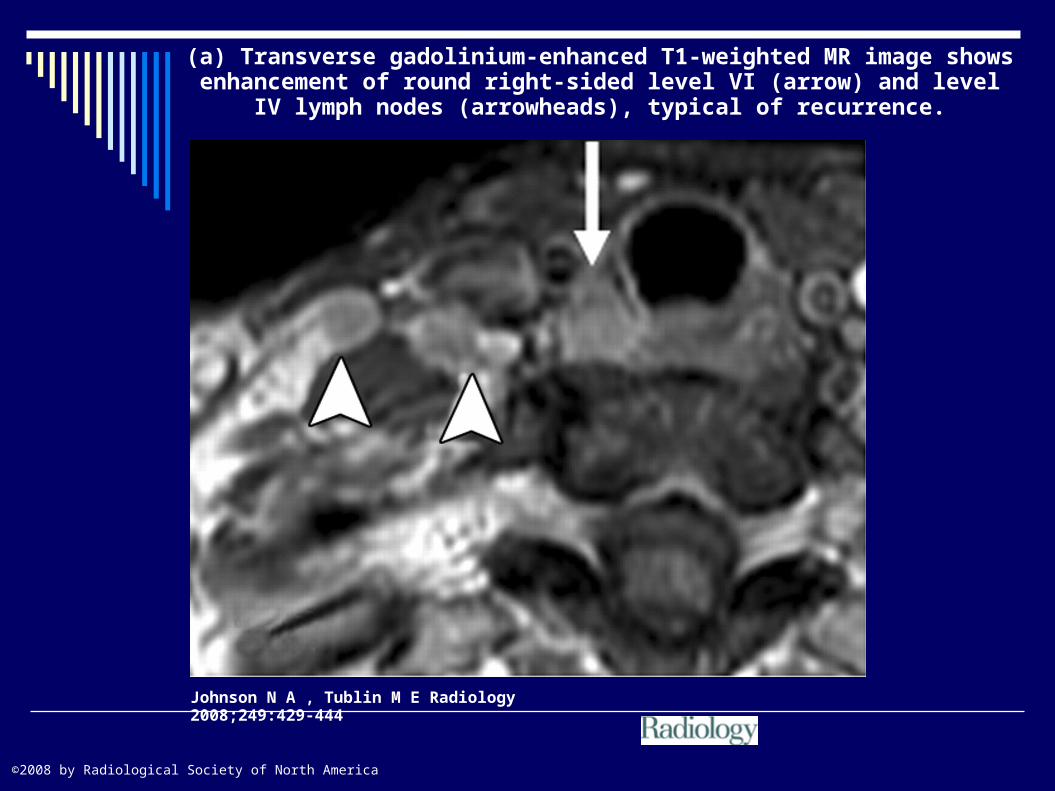
(a) Transverse gadolinium-enhanced T1-weighted MR image shows enhancement of round right-sided level VI (arrow) and level IV lymph nodes
(arrowheads), typical of recurrence.
Johnson N A , Tublin M E Radiology 2008;249:429-444
©2008 by Radiological Society of North America
Johnson N A , Tublin M E Radiology 2008;249:429-444
©2008 by Radiological Society of North America
Johnson N A , Tublin M E Radiology 2008;249:429-444
©2008 by Radiological Society of North America
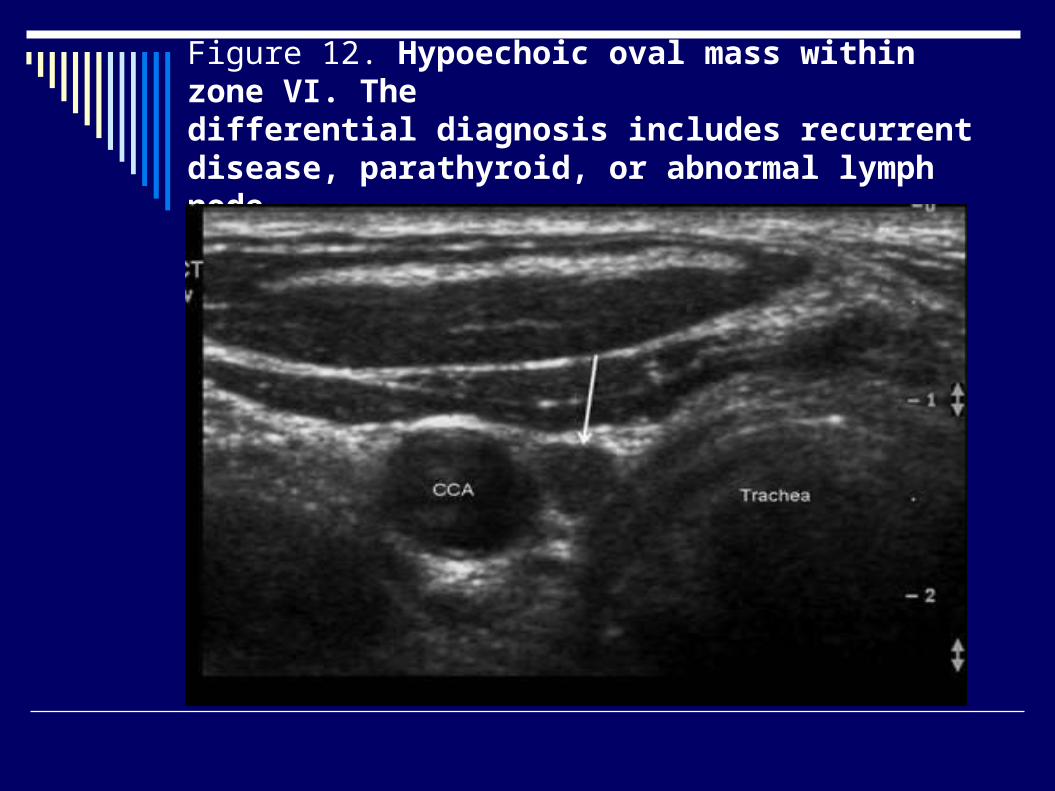
Figure 12. Hypoechoic oval mass within zone VI. Thedifferential diagnosis includes recurrent disease, parathyroid, or abnormal lymph node.
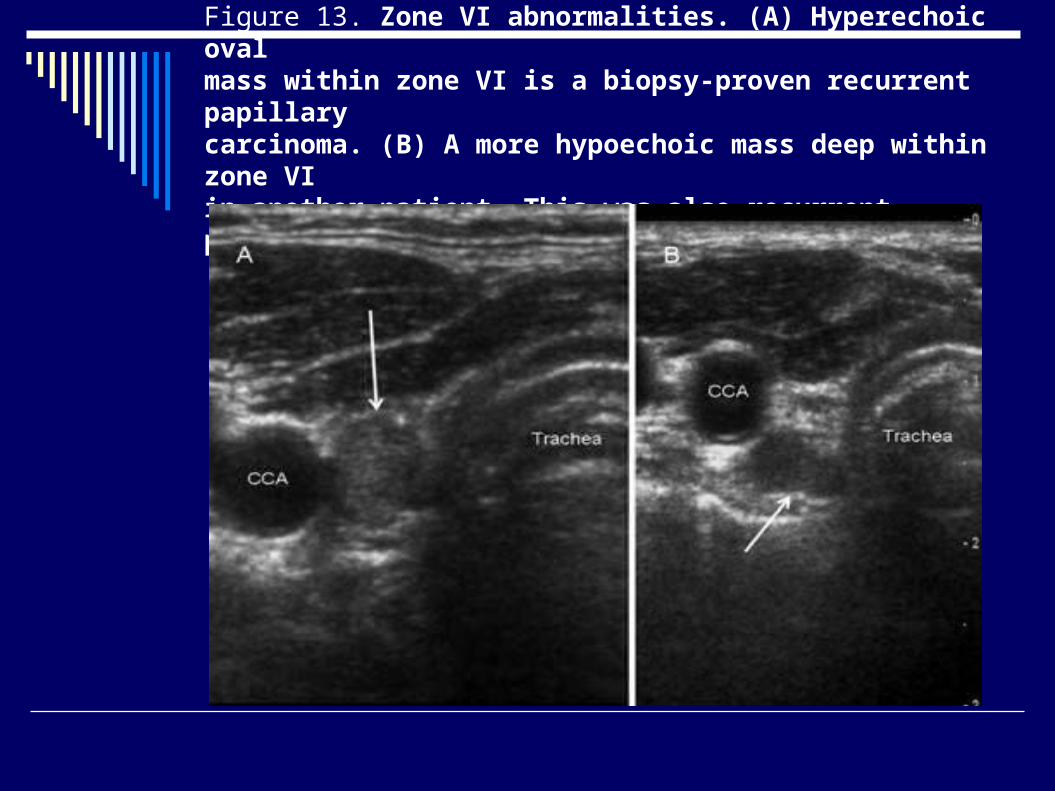
Figure 13. Zone VI abnormalities. (A) Hyperechoic ovalmass within zone VI is a biopsy-proven recurrent papillarycarcinoma. (B) A more hypoechoic mass deep within zone VIin another patient. This was also recurrent papillary carcinoma.
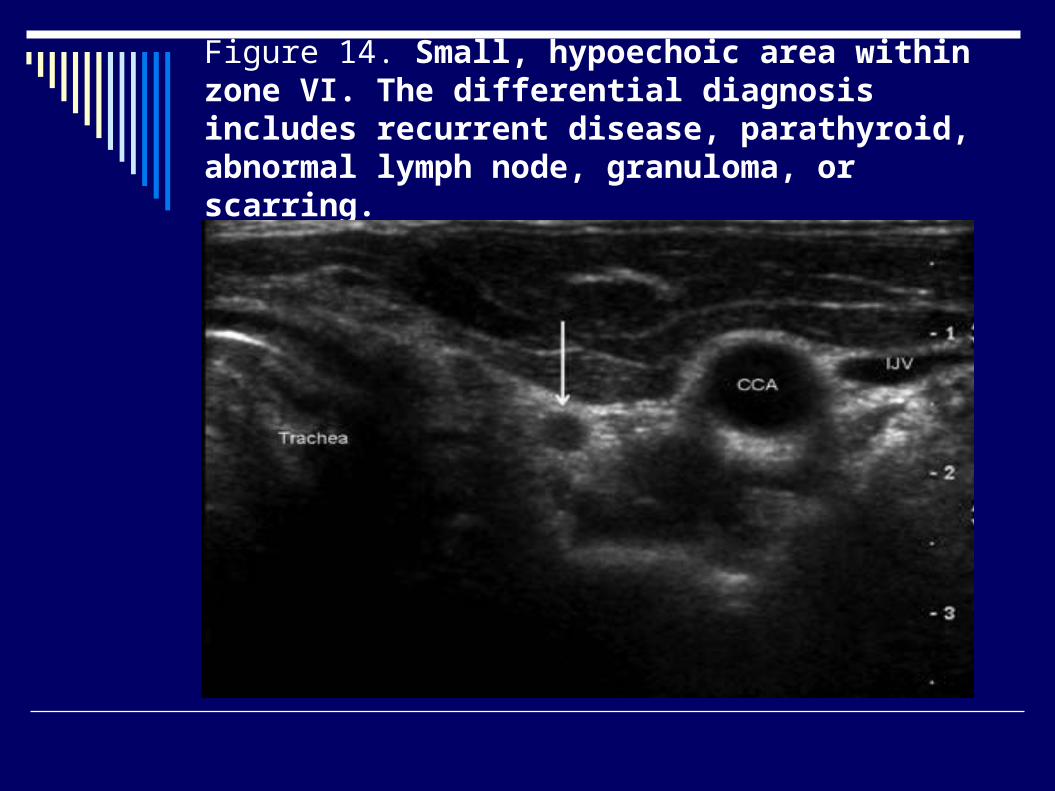
Figure 14. Small, hypoechoic area within zone VI. The differential diagnosis includes recurrent disease, parathyroid, abnormal lymph node, granuloma, or scarring.

Well differentiated thyroid cancer
US was found to be far more sensitive than WBS for the detection of local recurrence (sensitivity, 70% for US vs 20% for WBS); when thyroglobulin measurement was combined with US, the sensitivity and specificity were 96.2% and 100%, respectively, versus 92.7% and 100% for thyroglobulin measurement combined with WBS