pleomorphicadenomaofthesalivaryglands...
TRANSCRIPT
Pleomorphic Adenoma of the Salivary Glands:Correlation Between Gallium-67 Uptake andHistopathological ComponentsTomonori Yoshikai, Nobuhisa Yonemitsu, Junichiro Ishimaru, Makoto Mihara, Takemoto Shin and Sho KudoDepartments of Radiolog)', Pathology and Otolanmgology, Saga Medical School, Saga, Japan
We correlated 67Ga uptake and histopathological findings in pleo-morphic adenomas of the salivary glands. Methods: Sixty-twopleomorphic adenomas of the salivary glands were visually gradedby degree of 67Ga uptake as negative, weakly positive or strongly
positive in comparison to uptake in the nasal cavity. Tiiese adenomas were re-examined pathologically and classified as epithelial,intermediate or mesenchymal type according to their dominanthistological components. The pathological presence of marginalinvasion or associated sialoadenitis was also re-examined. Results:Eighteen adenomas were classified as strongly positive, eight asweakly positive and 36 as negative. Nine (50%) of the 18 stronglypositive adenomas were of the epithelial type and the other nine(50%) strongly positive adenomas were of the intermediate type.While none of the strongly positive adenomas were of the mesenchymal type, 27 (75%) of the 36 negative adenomas were of themesenchymal type. Six (75%) of the eight weakly positive adenomas were of the intermediate type. About half of the adenomasshowed marginal invasion regardless of the grade of 67Ga uptake.
None of the strongly positive adenomas were associated withsialoadenitis. Conclusion: The epithelial component of pleomorphicadenomas may be responsible for 67Ga uptake. The presence of
marginal invasion or associated sialoadenitis has little relation to67Ga uptake in pleomorphic adenomas.
Key Words: gallium-67; pleomorphic adenoma; salivarygland
J NucÃMed 1998; 39:537-541
JL leomorphic adenoma is the most common salivary glandtumor and represents 70%-80% of all benign salivary glandtumors ( / ). Pleomorphic adenoma has various degrees of 67Gauptake. While most pleomorphic adenomas have negative 67Ga
uptake, some show high tracer uptake. Pleomorphic adenomahas a biphasic appearance resulting from an intimate admixtureof epithelial and myxochondroid components (2), and eachadenoma contains these components at various rates. In thisstudy, we examined whether the difference in 67Ga uptake
correlates with the variation in histopathological components ofpleomorphic adenomas or with other pathological factors.
MATERIALS AND METHODS
SubjectsSixty-two pleomorphic adenomas of the salivary glands of 61
patients were reviewed. The adenomas were studied by preoperative gallium scintigraphy and were all confirmed pathologicallyafter surgical removal. Forty-eight adenomas originated in theparotid glands, 13 in the submandibular glands and 1 was from aminor salivary gland. Sialography was not performed prior toscintigraphy in these cases.
Received Mar. 14, 1997; accepted Apr. 22,1997.For correspondence or reprints contact: Tomonori Yoshikai, MD, Department of
Radiology, Saga Medical School, Nabeshima 5-1-1, Saga 849-8501, Japan.
Gallium ScintigraphyGallium scintigraphy was performed 3 days after injection of
111 MBq 67Ga-citrate. Anterior and bilateral lateral images of the
head and neck were obtained using a Toshiba gamma camera(Tokyo Shibaura Co., Ltd., Tokyo, Japan) and a medium-energycollimator with a preset time of 450 kcts. The 67Ga uptake of
pleomorphic adenomas was visually graded into three groups:negative (the uptake in tumor was not depicted), weakly positive(the uptake in tumor was definite but lower than that in nasalcavity) and strongly positive (the uptake in tumor was equal to orhigher than that in nasal cavity).
Tumor SizeTumor size was defined as an average of long and short
diameters of the adenoma measured by CT or magnetic resonanceimaging (MRI). The unpaired t-test was used for statistical analysisof tumor size.
Pathologic ExaminationEach resected pleomorphic adenoma was re-examined patholog
ically. Area ratio of the epithelial component to the whole specimen of the adenoma was measured microscopically, and alladenomas were classified into three types: epithelial (the epithelialcomponent occupies 70% or more of the whole specimen), intermediate (the epithelial component occupies between 30% and 70%of the whole specimen) and mesenchymal (the epithelial component occupies less than 30% of the whole specimen). The presenceof marginal invasion and associated sialoadenitis was also examined pathologically in each case.
RESULTSThe results from all patients are shown in Table 1, arranged
according to the grade of 67Ga uptake and tumor size. Eighteen
of 62 pleomorphic adenomas (29.0%) were strongly positive andeight (12.9%) were weakly positive. A total of 41.9% of theadenomas were positive. The remaining 36 adenomas were negative.
The mean size and s.d. was 2.9 ±0.7 cm in the stronglypositive adenomas (n = 18), 2.3 ± 0.7 cm in the weaklypositive adenomas (n = 8) and 2.4 ±0.8 cm in the negativeadenomas (n = 36). The strongly positive adenomas weresignificantly larger than either the weakly positive or negativeadenomas (p < 0.05). Weakly positive and negative adenomasdid not show a significant difference in size.
Pathological examination revealed that 50% of the stronglypositive adenomas were of the epithelial type and 50% were ofthe intermediate type; none were of the mesenchymal type.However, 75% of the negative adenomas were of the mesenchymal type, and 75% of the weakly positive adenomas were ofthe intermediate type. About half of the adenomas showedmarginal invasion regardless of the grade of 67Ga uptake. None
of the strongly positive adenomas were associated with sialoadenitis. A few cases of the weakly positive or negative adenomasshowed associated sialoadenitis (Table 2).
GALLiuM-67UPTAKEIN PLEOMORPHICADENOMA•Yoshikai et al. 537
by on July 2, 2018. For personal use only. jnm.snmjournals.org Downloaded from

TABLE 1Patients, Lesions and Results
Patientno.1234567S'91011121314151617*181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162Age(yr)4051462328244773193637315536525273551352291466626640466052452968584276367555588262326443696438176950415151303166604273591862GenderFFFMMMMFFMMMFFMFFFMFMFFFFMMFMMMMMMMFMFFMFFFFFFFMFMMFFFFFMFFFMFLocationL.
PR.PLSR.PLPLPLPR.
SLPLPR.
SR.PR.PR.PLPLPR.
PLPR.
PL.SR.SR.SR.PR.SLPR.
PLPR.
PR.PLPL.
PLPR.
SLSR.PR.PLPLPLPR.
PL.SL.SL.SR.PLPR.
PR.PR.PLPLPL.
PR.PR.PLPLPR.
PMinSLSR.
PR.PR.PLPSize(cm)4.54.33.23.13.13.02.92.92.82.82.82.82.82.32.32.32.02.03.52.82.72.22.11.81.81.55.04.03.53.53.43.33.02.82.82.52.52.52.52.52.32.32.22.22.12.12.12.02.02.02.02.02.01.91.81.81.81.81.61.51.41.467Ga
Dominant Marginal
uptake histologyinvasion+
++++++
+++E+
++++
+E++++++++E++E++ E+++I++ E+++I++E++ E+++ E++
I++I++E++
I+M+|+
I++I+M
+IM
+MMM
ncMMEME
+M+I
+MMM
+M+ME
+M+M+M+MI
+MM
+MM
+M+I+IMM
+M+M+EAssociated
sialoadenitisnc----nc-----ncnc-nc----+nc---+-+-nc-ncnc--+-----+-+-------nc-—-—-+----—
"Lésionsin the same patient.R = right; L = left; P = parotid gland; S = submandibular gland; MinS = minor salivary gland; + + = strongly positive; + = weakly positive; - = negative;
E = epithelial type; I = intermediate type; M = mesenchymal type; marginal invasion: + = positive, - = negative, nc = not clear; associated sialoadenitis:+ = positive, - = negative, nc = not clear.
538 THE JOURNALOFNUCLEARMEDICINE•Vol. 39 •No. 3 •March 1998
by on July 2, 2018. For personal use only. jnm.snmjournals.org Downloaded from
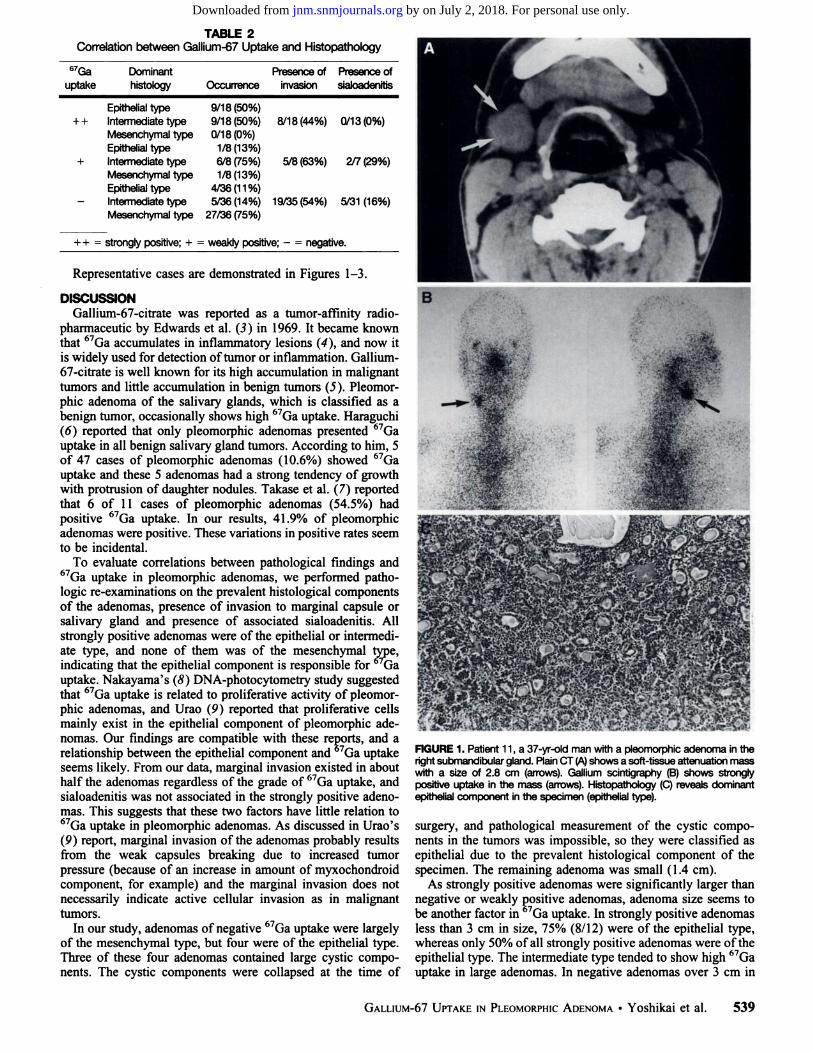
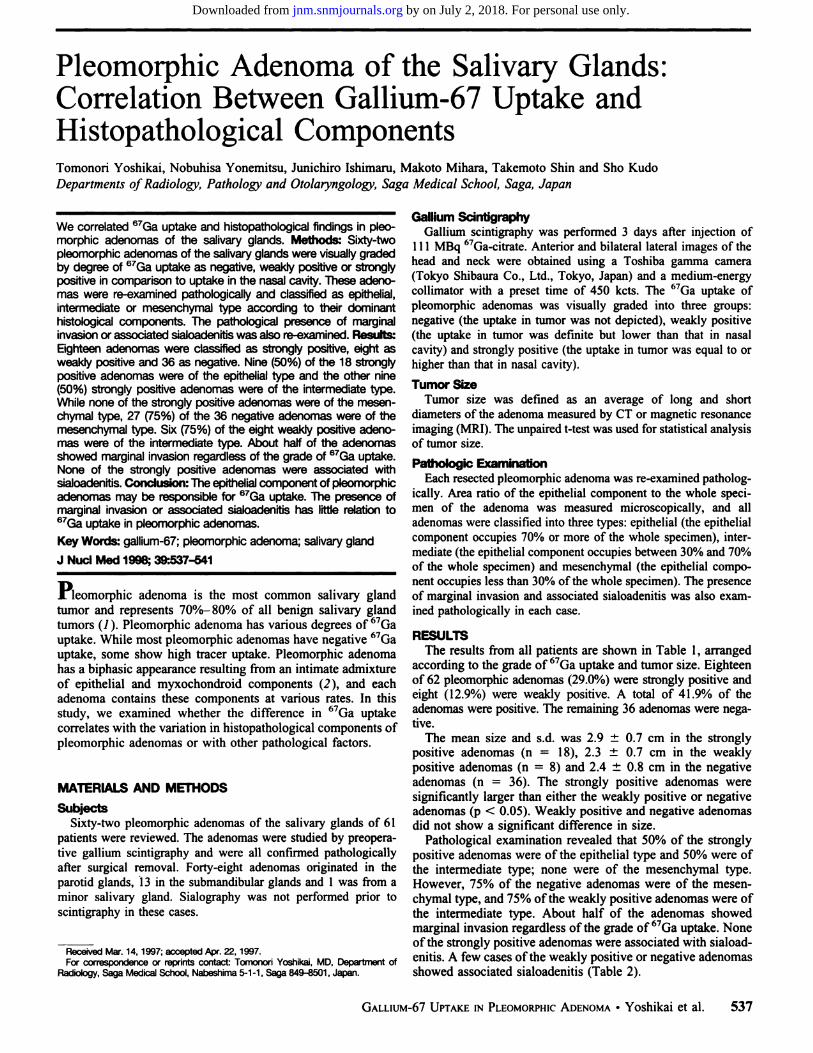
TABLE 2Correlation between Galh'um-67 Uptake and Histopathology
67Ga
uptake+
+
+Dominant
histologyEpithelial
typeIntermediate typeMesenchymal typeEpithelial typeIntermediate typeMesenchymal typeEpithelial typeIntermediate typeOccurrence9/18(50%)
9/18(50%)0/18(0%)
1/8(13%)6/8 (75%)1/8(13%)
4/36(11%)5/36(14%)Presence
ofinvasion8/18(44%)
5/8 (63%)
19/35(54%)Presence
ofsialoadenitis0/13(0%)
2/7 (29%)
5/31 (16%)Mesenchymal type 27/36 (75%)
+ + = strongly positive; + = weakly positive; - = negative.
Representative cases are demonstrated in Figures 1-3.
DISCUSSIONGallium-67-citrate was reported as a tumor-affinity radio-
pharmaceutic by Edwards et al. (3) in 1969. It became knownthat 67Ga accumulates in inflammatory lesions (4), and now it
is widely used for detection of tumor or inflammation. Gallium-67-citrate is well known for its high accumulation in malignanttumors and little accumulation in benign tumors (5). Pleomor-phic adenoma of the salivary glands, which is classified as abenign tumor, occasionally shows high 67Ga uptake. Haraguchi(6) reported that only pleomorphic adenomas presented 67Ga
uptake in all benign salivary gland tumors. According to him, 5of 47 cases of pleomorphic adenomas (10.6%) showed 67Ga
uptake and these 5 adenomas had a strong tendency of growthwith protrusion of daughter nodules. Takase et al. (7) reportedthat 6 of 11 cases of pleomorphic adenomas (54.5%) hadpositive 67Ga uptake. In our results, 41.9% of pleomorphic
adenomas were positive. These variations in positive rates seemto be incidental.
To evaluate correlations between pathological findings and67Ga uptake in pleomorphic adenomas, we performed patho
logic re-examinations on the prevalent histological componentsof the adenomas, presence of invasion to marginal capsule orsalivary gland and presence of associated sialoadenitis. Allstrongly positive adenomas were of the epithelial or intermediate type, and none of them was of the mesenchymal type,indicating that the epithelial component is responsible for Gauptake. Nakayama's (8) DNA-photocytometry study suggestedthat 67Ga uptake is related to proliferative activity of pleomor
phic adenomas, and Urao (9) reported that proliferative cellsmainly exist in the epithelial component of pleomorphic adenomas. Our findings are compatible with these reports, and arelationship between the epithelial component and 67Ga uptake
seems likely. From our data, marginal invasion existed in abouthalf the adenomas regardless of the grade of 67Ga uptake, and
sialoadenitis was not associated in the strongly positive adenomas. This suggests that these two factors have little relation to67Ga uptake in pleomorphic adenomas. As discussed in Urao's
(9) report, marginal invasion of the adenomas probably resultsfrom the weak capsules breaking due to increased tumorpressure (because of an increase in amount of myxochondroidcomponent, for example) and the marginal invasion does notnecessarily indicate active cellular invasion as in malignanttumors.
In our study, adenomas of negative 67Ga uptake were largely
of the mesenchymal type, but four were of the epithelial type.Three of these four adenomas contained large cystic components. The cystic components were collapsed at the time of
FIGURE 1. Patient 11, a 37-yr-old man with a pleomorphic adenoma in theright submandibular gland. Plain CT (A)shows a soft-tissue attenuation mass
with a size of 2.8 cm (arrows). Gallium scintigraphy (B) shows stronglypositive uptake in the mass (arrows). Histopathology (C) reveals dominantepithelial component in the specimen (epithelial type).
surgery, and pathological measurement of the cystic components in the tumors was impossible, so they were classified asepithelial due to the prevalent histological component of thespecimen. The remaining adenoma was small (1.4 cm).
As strongly positive adenomas were significantly larger thannegative or weakly positive adenomas, adenoma size seems tobe another factor in 67Ga uptake. In strongly positive adenomas
less than 3 cm in size, 75% (8/12) were of the epithelial type,whereas only 50% of all strongly positive adenomas were of theepithelial type. The intermediate type tended to show high 67Ga
uptake in large adenomas. In negative adenomas over 3 cm in
GALLiuM-67UPTAKEIN PLEOMORPHICADENOMA•Yoshikai et al. 539
by on July 2, 2018. For personal use only. jnm.snmjournals.org Downloaded from
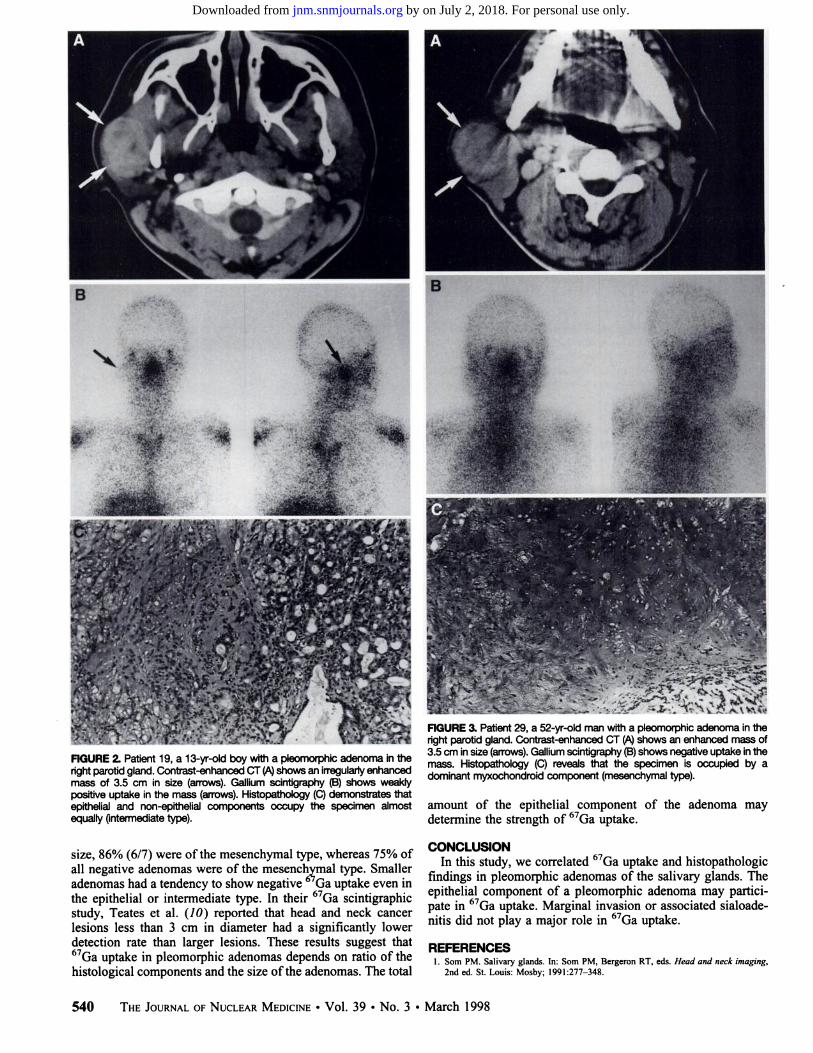
FIGURE 2. Patient 19, a 13-yr-old boy with a pleomorphic adenoma in theright parotid gland. Contrast-enhanced CT (A)shows an irregularly enhancedmass of 3.5 cm in size (arrows). Gallium scintigraphy (B) shows weaklypositive uptake in the mass (arrows). Histopathology (C) demonstrates thatepithelial and non-epithelial components occupy the specimen almost
equally (intermediate type).
size, 86% (6/7) were of the mesenchymal type, whereas 75% ofall negative adenomas were of the mesenchymal type. Smalleradenomas had a tendency to show negative 67Ga uptake even inthe epithelial or intermediate type. In their 67Ga scintigraphic
study, Teates et al. (10) reported that head and neck cancerlesions less than 3 cm in diameter had a significantly lowerdetection rate than larger lesions. These results suggest that67Ga uptake in pleomorphic adenomas depends on ratio of the
histological components and the size of the adenomas. The total
FIGURE 3. Patient 29, a 52-yr-old man with a pleomorphic adenoma in theright parotid gland. Contrast-enhanced CT (A) shows an enhanced mass of
3.5 cm in size (arrows). Gallium scintigraphy (B) shows negative uptake in themass. Histopathology (C) reveals that the specimen is occupied by adominant myxochondroid component (mesenchymal type).
amount of the epithelial component of the adenoma maydetermine the strength of 67Ga uptake.
CONCLUSIONIn this study, we correlated 67Ga uptake and histopathologic
findings in pleomorphic adenomas of the salivary glands. Theepithelial component of a pleomorphic adenoma may participate in 67Ga uptake. Marginal invasion or associated sialoade-nitis did not play a major role in 67Ga uptake.
REFERENCES1. Som PM. Salivary glands. In: Som PM. Bergeron RT, eds. Head and neck imaging,
2nd ed. St. Louis: Mosby; 1991:277-348.
540 THEJOURNALOFNUCLEARMEDICINE•Vol. 39 •No. 3 •March 1998
by on July 2, 2018. For personal use only. jnm.snmjournals.org Downloaded from

2. Rosai J. Major and minor salivary glands. In: Rosai J. ed. Ackerman 's surgical
pathology, vol. 1. 8th ed. St. Louis: Mosby; 1996:815-856.3. Edwards CL, Hayes RL. Tumor scanning with "Ga-citrate. J NucÃMed 1969;10:103-
105.4. Lavender JP. Lowe J, Barker JR, Burn JI, Chaudhuri MA. Gallium-67-citrate scanning
in neoplastic and inflammatory lesions. Br J Radial 1971;44:361-366.
5. Hirakata R, Nakayama C. Watanabe H, Nakata H, Suzuki K, Nishio K. Clinicalevaluation of 67Ga scintigraphy on superficial soft-tissue diseases. Jpn J Clin Radiol1986;31:1429-1434.
6. Haraguchi S. Diagnostic evaluation of RI scintigraphy in parotid gland tumors. NipponJibiinkoka Gakkai Kaiho 1985:88:520-534.
7. Takase H, Toyama M. Eguchi T, Maeda K. Evaluation of Ga-67 scintigraphy forsalivary gland tumors. Jpn J Med Imaging 1993;12:217-224.
8. Nakayama N. Analysis of proliferative activity of pleomorphic adenoma of salivarygland with DNA-photocytometry. Nippon Jihiinkoka Gakkai Kaiho 1988:91:1274-
1284.9. Urao Y. Evaluation of proliferative activity of pleomorphic adenoma arising from the
salivary glands using anti BrdU monoclonal antibody. Nippon Jibiinkoka GakkaiKaiho 1989;92:420-430.
10. Teates CD, Preston DF, Boyd CM. Gallium-67-citrate imaging in head and necktumors: report of cooperative group. J NucÃMed 1980:21:622-627.
Pentavalent Technetium-99m-DimercaptosuccinicAcid Scintigraphy in Renal OsteodystrophyTetsuya Higuchi, Tsuneo Mirano, Tornio Inoue, Jun Aoki, Kazue Ueki, Ryoji Wakamatsu, Shintarou Yano, Takuji Naruse andKeigo EndoDepartments of Nuclear Medicine, Diagnostic Radiology and Internal Medicine, Gunma University School of Medicine,Gunma, Japan
Pentavalent 99mTc-dimercaptosuccinic acid (DMSA) scintigraphyand ""Tc-hydroxymethylene diphosphonate (HMDP) bone scan
were performed in one patient with renal osteodystrophy (ROD)before and after vitamin D3 pulse therapy. The bone scan showeddiffusely increased tracer uptake in the whole skeleton, and nochange of tracer distribution was noted before or after vitamin D3pulse therapy. However, 99mTc(V)-DMSA scintigraphy revealed dif
fusely increased tracer uptake in the whole skeleton before therapy,and markedly decreased tracer uptake in the bones was seen at 5mo after therapy. Increased uptake of 99nTc(V)-DMSA was ob
served at 7 mo after therapy, which reflected the laboratory findings.Technetium-99m-(V)-DMSA scintigraphy appeared to be more sensitive than the conventional ""Tc-HMDP bone scan in assessing
the characteristics and therapeutic effect of bone disease in ROD.Key Words: technetium-99m; dimercaptosuccinic acid; renal osteodystrophy; hemodialysis; 1, 25-dihydroxyvitamin D3
J NucÃMed 1998; 39:541-543
IVenal osteodystrophy (ROD) is a common and serious complication for uremie patients receiving hemodialysis. The recentprogress and widespread clinical use of hemodialysis hasprolonged the mean survival rate for patients with uremia;however, some problems such as ROD have appeared. A widelyused treatment in patients with ROD is vitamin D3 pulsetherapy, which is very effective especially in ROD related tosecondary hyperparathyroidism (1,2).
Pentavalent 9 mTc-dimercaptosuccinic acid (DMSA) has
been used in detecting tumors, such as medullary carcinoma ofthe thyroid and soft-tissue tumors, and in evaluating thelocalization of primary amyloidosis (3-6). The bone scanningagent "Tc-hydroxymethylene diphosphonate (HMDP) has also
been used to evaluate ROD (7,8). Its clinical use complementedthe assessment of lesions in patients with symptomatic hemodialysis bone disease. We report one case with renal osteodystrophy (ROD) evaluated by using 99mTc(V)-DMSA scintigra
phy both before and at 7 and 15 mo after vitamin D3 pulsetherapy.
TABLE 1Laboratory Data in a Patient with CRF Before and After Vitamin D3
Pulse Therapy
Beforetherapy8mo aftertherapy1
5 mo after therapyC-PTH*(ng/ml)32627AU*(IU/I)767123268Intact-PTH*(pg/ml)1770—1546
Received Mar. 11, 1997; revision accepted May 2, 1997.For correspondence or reprints contact: Tetsuya Higuchi. MD, Department of Nuclear
Medicine, Gunma University School of Medicine, 3-39-22 Showamachi, Mebashi,
Gunma, 371, Japan.
'Normal range = less than 1.3 ng/ml, measured by C-PTH kit (Incstar Co.
Stillwater, MM).formal range = 70-240 IU/I.*Normal range = 10-65 pg/ml, measured by alegro intact PTH kit (Nichols
Institute, San Juan Capistrano, CA).
CASE REPORT
The patient was a 44-yr-old woman with chronic renal failuresecondary to chronic glomerular nephritis who had receivedcontinuous ambulatory peritoneal dialysis for 8 yr. She had been onhemodialysis for 3 yr.
She had developed low back and shoulder pain 3 mo earlier. Inthe laboratory data (Table 1), elevated serum levels of alkalinephosphatase (ALP), C-parathyroid hormone (PTH) and intact-PTH were noted. The radiograph of the hand revealed subperi-
osteal résorptionand a thin osteal cortex. On CT scans andradionuclide imagings using 201T1C1and 99rnTc-pertechnetate in
the cervix, no enlarged parathyroid gland was seen. On the bonescan using 740 MBq 99mTc-HMDP, diffusely increased tracer
uptake was observed in the whole skeleton (Fig. 1A). Thesefindings led to the diagnosis of ROD associated with secondaryhyperparathyroidism. A 99mTc(V)-DMSA whole-body scan,
prepared as previously described by Hirano et al. (3), was done1 wk after the bone scan, and it revealed diffusely increasedtracer uptake in the skeletal bones, especially the skull andmandible (Fig. 2A).
A weekly dose of 4-jig calcitriol was started to treat ROD. Aftervitamin D3 pulse therapy, serum levels of ALP, C-PTH, intact-PTHgradually decreased and were almost normalized at 6 mo. Therewas no obvious change in the bone scan (Fig. IB); however, clearly
TECHNETiUM-99m-DMSASCINTIGRAPHYIN ROD •Higuchi et al. 541
by on July 2, 2018. For personal use only. jnm.snmjournals.org Downloaded from
1998;39:537-541.J Nucl Med. Tomonori Yoshikai, Nobuhisa Yonemitsu, Junichiro Ishimaru, Makoto Mihara, Takemoto Shin and Sho Kudo and Histopathological ComponentsPleomorphic Adenoma of the Salivary Glands: Correlation Between Gallium-67 Uptake
http://jnm.snmjournals.org/content/39/3/537This article and updated information are available at:
http://jnm.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNM can be found at:
http://jnm.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0161-5505, Online ISSN: 2159-662X)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published monthly.The Journal of Nuclear Medicine
© Copyright 1998 SNMMI; all rights reserved.
by on July 2, 2018. For personal use only. jnm.snmjournals.org Downloaded from