lisa schilling, rn, mph vice president, cmi center for...
TRANSCRIPT

Leadership Lessons for Spread and Scale Lisa Schilling, RN, MPH Vice President, CMI Center for Health Systems Performance
IHI Forum
Orlando, FL
December9, 2014
Session Objectives
Engage in discussion about learning and challenges in spread
Describe how initiative complexity and local culture impact spread
Identify strategies to address challenges

Disclosures
Faculty have nothing to disclose

“The Greatest glory in living lies not in never falling,
but in rising every time we fall.” - Nelson Mandela

The Framework P5
Adoption
Mechanisms
Set-up Build Scalable
Unit
Test Scale-
Up
Go to Full-Scale
& Sustain
Support
Systems
Phases of
Scale-up
Best
Practice
exists
New Scale-
up Idea
Leadership, communication, social networks, culture of urgency
and persistence
Learning systems, data systems, infrastructure for scale-up,
human capacity for scale-up, capability for scale-up
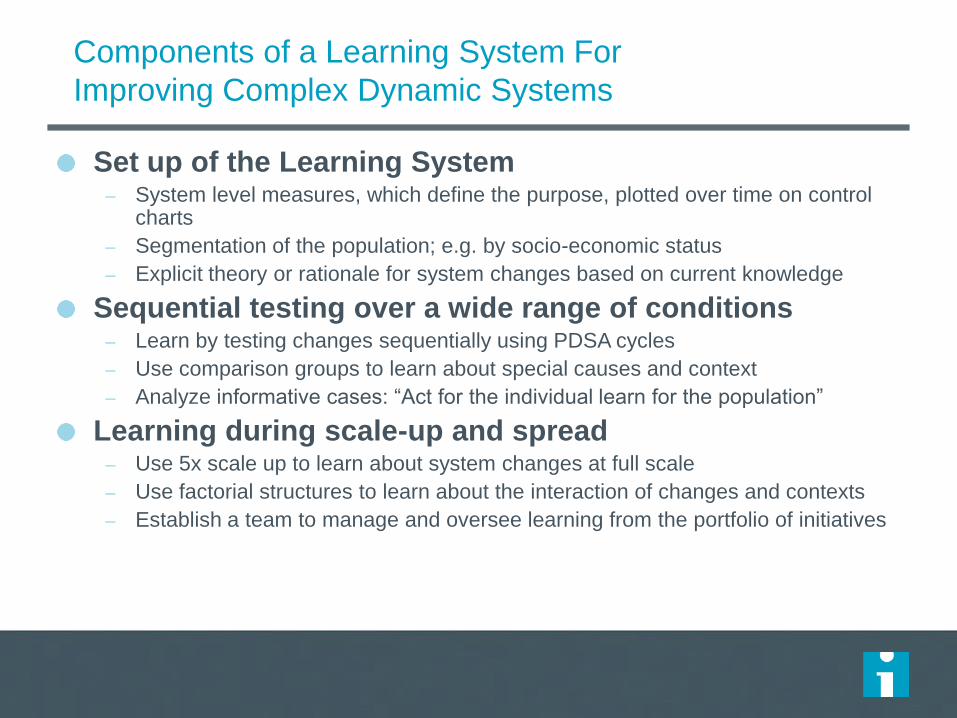
Components of a Learning System For
Improving Complex Dynamic Systems
Set up of the Learning System – System level measures, which define the purpose, plotted over time on control
charts
– Segmentation of the population; e.g. by socio-economic status
– Explicit theory or rationale for system changes based on current knowledge
Sequential testing over a wide range of conditions – Learn by testing changes sequentially using PDSA cycles
– Use comparison groups to learn about special causes and context
– Analyze informative cases: “Act for the individual learn for the population”
Learning during scale-up and spread – Use 5x scale up to learn about system changes at full scale
– Use factorial structures to learn about the interaction of changes and contexts
– Establish a team to manage and oversee learning from the portfolio of initiatives
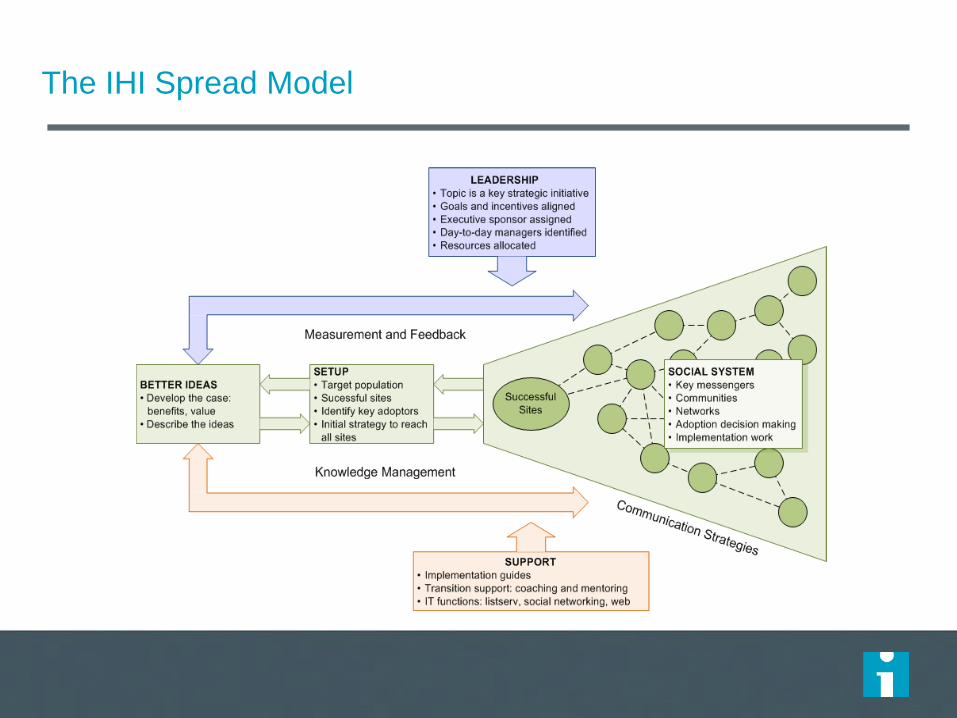
The IHI Spread Model
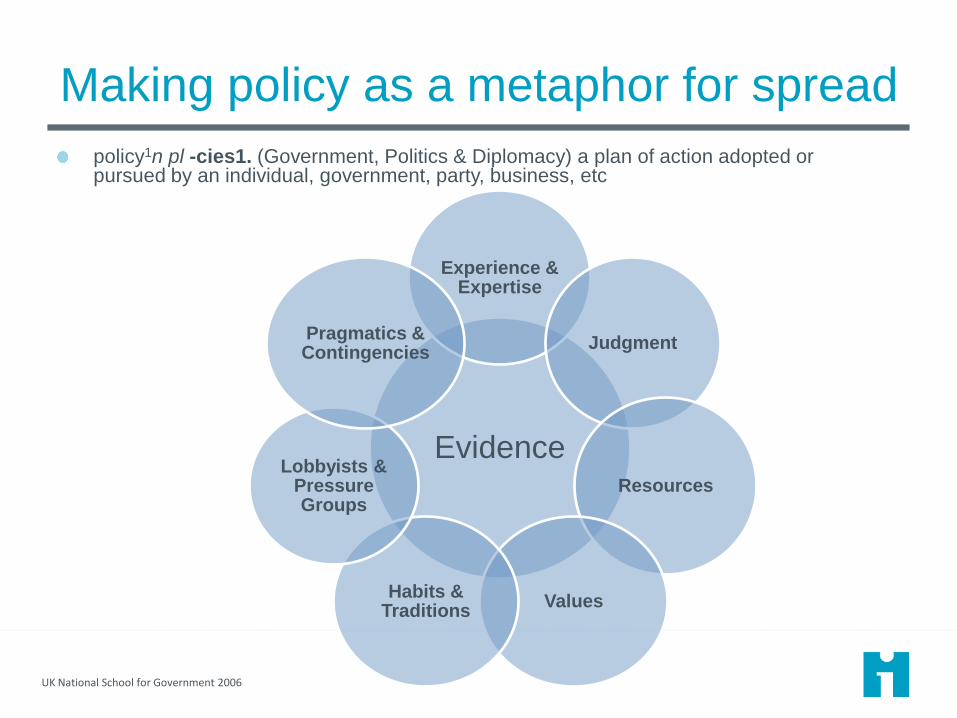
Making policy as a metaphor for spread
policy1n pl -cies1. (Government, Politics & Diplomacy) a plan of action adopted or pursued by an individual, government, party, business, etc
UK National School for Government 2006
Evidence
Experience & Expertise
Judgment
Resources
Values Habits &
Traditions
Lobbyists & Pressure Groups
Pragmatics & Contingencies

| © 2011 Kaiser Foundation Health Plan, Inc. For
internal
December 7,
2014
9
What Really Matters
PRACTICE TRANSFERRABILITY
December 7,
2014
What Really Matters
PRACTICE TRANSFERRABILITY

| © 2011 Kaiser Foundation Health Plan, Inc. For
internl us only.
December 7,
2014
What Really Matters
PRACTICE TRANSFERRABILITY
Your Biggest Challenges
Buy in from staff and executive leadership
Speed of adoption
Standardizing vs customizing
Sustaining or “making it stick”
Large complex program adoption and management
Discussion Groups
Identify biggest challenges to spread
Move to a table on this topic
Discuss 3 items:
– Challenges
– Ideas
– One change you will try
Appendix

Phase 1 Determine Organizational Readiness
Start with the
end in mind
Align
improvement to
strategic objects
Assess site
readiness
to receive
© Kaiser Permanente 2014 reproduce by permission only
15
Start with the
end in mind
Determine what
is being spread
Define target
population &
end state
Establish
timeframe to
achieve scale
Define
measurement
strategy
including spread
measures
Align improvement to
strategic objects
Determine if
improvement links
with strategic goals
Craft a
compelling
message “start
with why”
Determine key
members of
chartered teams -
who are the key
stakeholders &
sponsorship
Assess practice
readiness to spread
Complete
assessment of
host site
readiness to
spread
Plan for or
identify sites
based on
learnings
Revisit scale,
scope and speed
Assess site
readiness
to receive
Complete
readiness to
receive
assessment
tool
Plan for
sequencing
based on
learnings
Create monitor
and review plan

How Does
It Work?
Simplicity
Cultural Fit
Business Case
Tools
Implementation Support
Practice readiness to spread
Demonstrated Sustainability
Demonstrated Transfer
Adaptability
Unintended Consequences
Does It Work? Will It Work
Elsewhere?
Comparative Performance
Outcome vs. Process
Improvement Attributable to Practice
Strength of Evidence
Logic Model
Key Components
Specific Processes
OrganizationalEnablers
Barriers and Risks
Will It Spread?
16
© Kaiser Permanente 2014 reproduce by permission only

Organizational
Culture
Project Management & Championship
Training
Measurement and Monitoring
Site readiness to receive
Staff Capacity & Competency
Space
Technology
Operational Infrastructure (# of units involved, relationships)
Leadership
Alignment
Operational
Resources
Strategic Alignment with Goals and Priorities
Sponsorship & Leadership
Oversight Infrastructure
Cultural Readiness for Change
Implementation
Infrastructure
17
© Kaiser Permanente 2014 reproduce by permission only

How much variation? Adapt locally vs. copy exactly
Adapt locally
Theory (Paul Plsek)
– Health care is a Complex Adaptive System
– Find local Attractors
– Use only Simple Rules
Strength
– Spread is more likely to occur if importers can adapt to their needs
Copy exactly
Theory (Gabriel Szulanski)
– We’re not as smart as we think
– Experience beats cleverness
– First import, then improve
Strength
– Spread is more likely to get results if importers work with exporters to learn a proven model
© Kaiser Permanente 2014 reproduce by permission only
18

Key components ≈ Minimum specifications
NW Transition Care Bundle ElementsWhat does the patient need? Transition Bundle
I will have what I need when I
return home
Risk Stratification with tailored care
I know when I should call and what
number to use when I need help
Specialized phone number on DC
Instructions
My regular doctor will know what
happened to me in the hospital
Standardized Same Day Discharge Summary
I understand my medications, how
to take them, and why I need them
Pharmacist reviewing medications in
hospital
PharmD phone call (high risk)
I will see my doctor soon after my
hospitalization
I know someone will check on me
when I am home.
MD appointments made in hospital within 5
(high risk) to 10 days.
RN follow up Call within 48 hours.
RN case mgmt 30 days (high risk)
2012 National Quality Conference9
19 © Kaiser Permanente 2014 reproduce by permission only